Patient Safety Event Review Process & Tools
|
|
|
- Jade Richards
- 5 years ago
- Views:
Transcription
1 Patient Safety Event Review Process & Tools
2 Event Occurs Patient Safety Event Review Process Immediate actions are taken to care for the patient, make the situation safer for others and sequester equipment/products Entered into Reporting System (VOICE) Opened for investigation by Patient Safety & Unit Manager Patient Safety reviews the events daily for events needing scoring committee review. May require gathering additional information during this phase. Patient Safety Prepares SBAR for potential Serious Safety Events (SSEs) Event Response Prioritization tool should direct the type of response/review that will be used SSE Scoring Committee sets SEC harm scale and response Could be RCA, or ACA Each event should have one strong, or two intermediate actions in addition to any other identified weaker actions. SSE Committee is comprised of leadership and is actively involved in the RCA and actions by supporting the process, approving and periodically reviewing the status of actions, understanding what a thorough assessment report should include, and acting when reviews do not meet minimum requirements. Owners are identified for every action item and responsible for implementation and measurement. Patient Safety follows-up on action items for status updates. Event Response/Review Conducted SSE Committee Reviews and endorses (or not) the action plan Implementation, Measurement & Feedback
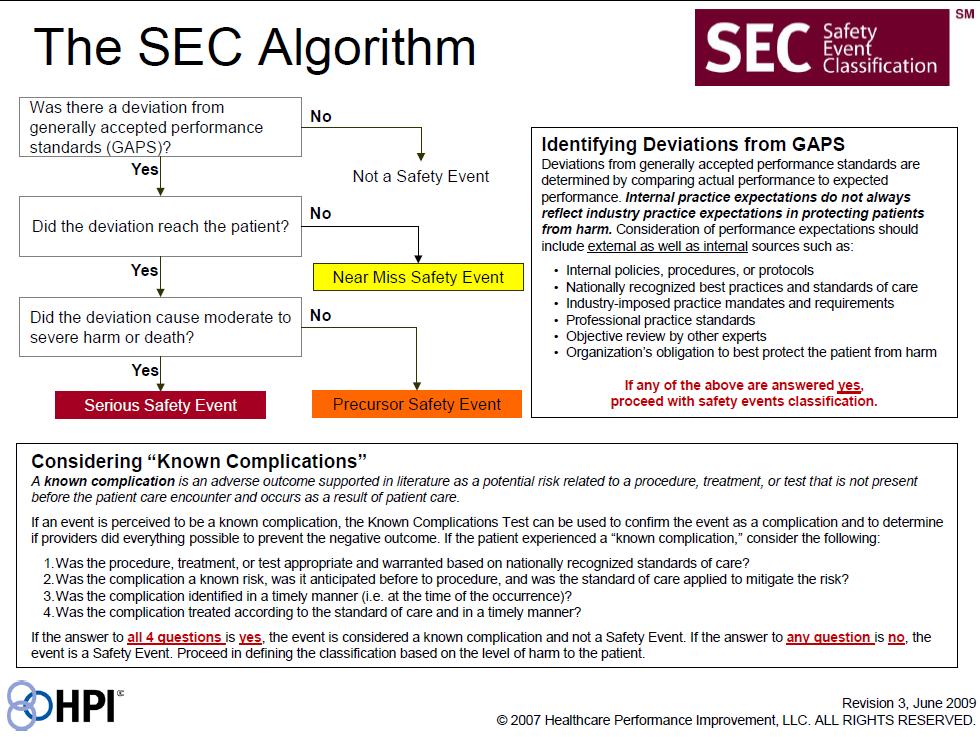
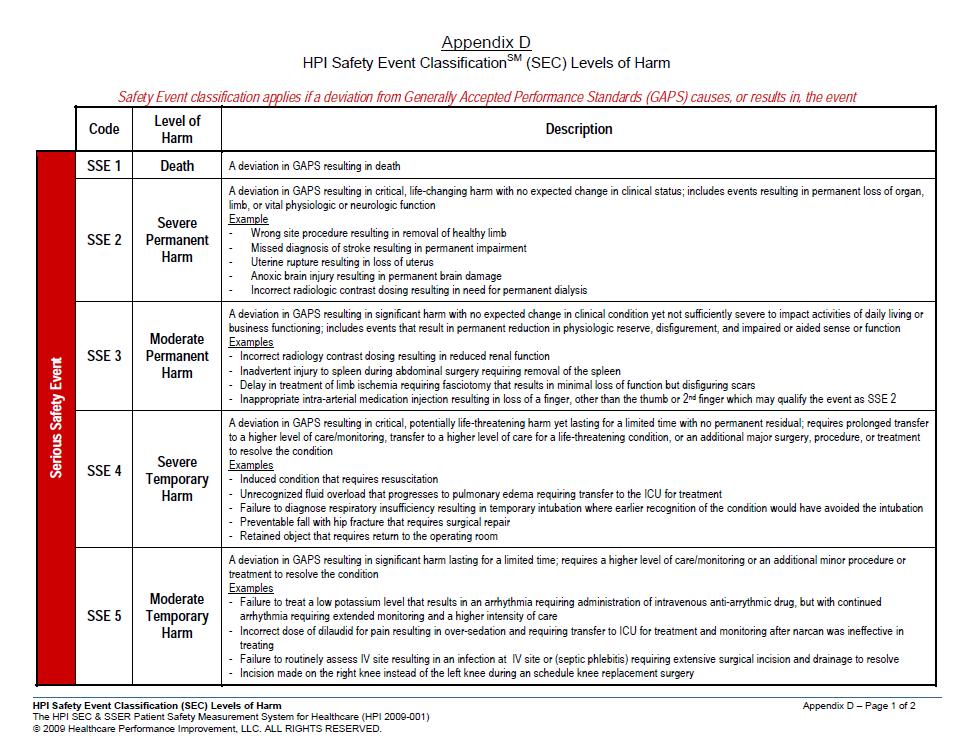
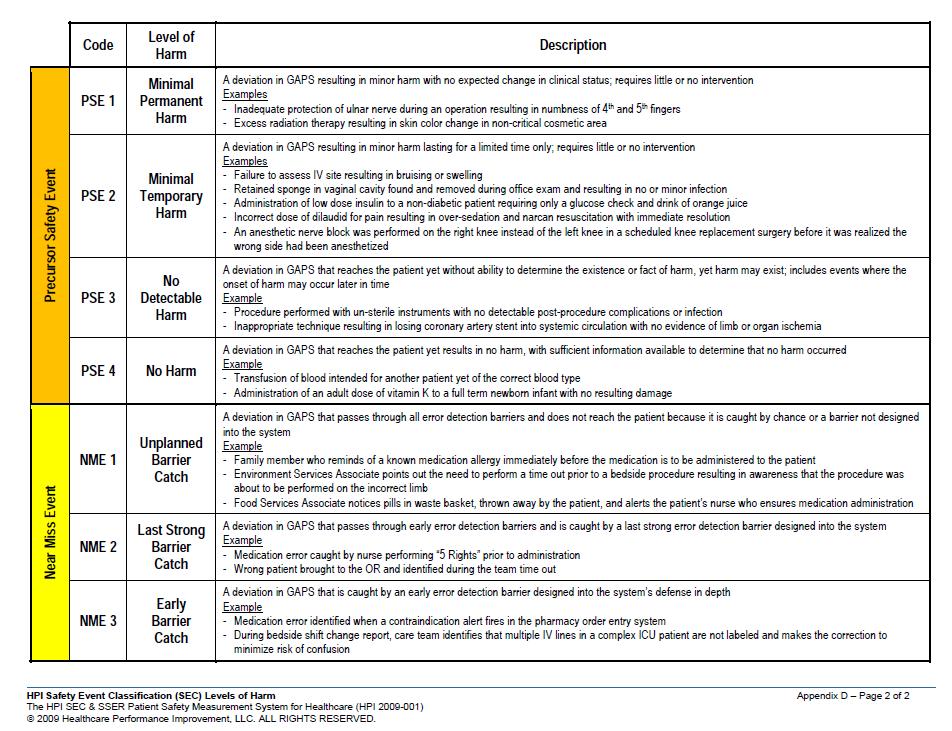
3 Severity Event Response Prioritization Severity and Frequency Evaluation Matrix to Prioritize Response Are there system issues present? Is this a patient safety concern? If yes: 1. Determine priority based on severity and frequency 2. Determine appropriate response based on matrix 3. Determine if event meets TJC Sentinel Event definition Catastrophic Major Moderate Minor Frequency Historical Event Occurrence Consider Rare Less than one event each year Frequency should be specific: by service, by location, by equipment or med type, by procedure type. If we Unlikely One event per year, annually see trends in event-type throughout the institution, consider aggregation. Possible 3-4 times per year, quarterly Likely Monthly or every other month Almost Certain Weekly or daily Severity Actual Harm Intervention SSE Range Minor No injury or minimal, temporary injury No intervention or minimal intervention NME or PSE 3, 4 + Moderate Major (Serious) Catastrophic Rare Unlikely Possible Likely Almost Certain Moderate level of harm that is temporary or minor permanent Serious Harm, Severe temporary or moderate permanent harm resulting in long term disability Death-unexpected and not related to underlying condition (or hastened), severe permanent harm 1 3 Priority Extreme High Moderate Low Meets TJC sentinel event definition? Requires additional monitoring or testing, minimal surgical intervention (sutures) Major interventions include escalation in level of care, surgical interventions, and prolonged length of stay Requires heroic life-saving measures unrelated to patient s expected medical course, amputation 2 PSE 1, 2 or SSE 5 SSE 3, 4 SSE 1, 2 Response * RCA 1 : Multidisciplinary review, SSE Committee review. Action plan within 45 business days. Local Review with required follow up: Local review and action plan sent to SSE Committee for review of action plan within 60 business days. Aggregate and/or Committee: Consider for aggregation. If appropriate committee exists, send for review. Findings entered into VOICE or sent to SSE Committee as directed. Local Review, Optional Follow Up: Findings entered into VOICE. S Sentinel Events: Regardless of response-type above action plans must be developed within 45 business days. *If concerns about individual performance are discovered, consider sending for case review or to HR for performance review. 1 May be facilitated by an existing institutional team, if deemed more appropriate by the SSE Scoring Committee. + Potential: Consider near miss or precursor with potential for catastrophic harm as catastrophic rating at the discretion of SSE Scoring Committee members
4
5 5
6 6
7 Debrief Form Content Situation: Description of event, approximately one or two sentences. Background: Provide some background information related to this problem or situation. Include pertinent medical information. What is the frequency of occurrence? Assessment: What is your assessment of the current situation or problem? Focus on system processes positive and/or negatives; what went well/what could have gone better. Consider the following as potentially contributing to the event: Teamwork Availability of Information Technology Equipment/Supplies Staffing Environment Communication Processes Recommendation(s): Consider immediate interventions to prevent /minimize harm. Additional Considerations: Notify your chain of command? Is there a need to secure equipment, supplies, medical devices, and/or medication? Any patient or family ongoing support needed? Do we need to involve Social Services, Pastoral Care or Patient Liaison? Care for the caregiver? Is there a need for disclosure?
8 What happened? Root Cause Analysis Process 1-2 sentences include impact to the patient and/or Flow diagram Identify RCA Team Including executive sponsor & RCA lead Document/ Record Review RCA Lead 1 st Meeting: Identify Interview Plan 2 nd Meeting: Identify Contributing Factors Identify interviewees Identify triggering questions Schedule future meeting Build from the initial flow diagram Contributing Factors from Initial Interviews 14 days or less 3 rd Meeting: Contributing Factors & Countermeasure s 4 th Meeting Cont. Contributing Factors Identify Countermeasures Identify metric(s) to gauge success Final Edit of Report Discuss process owners feedback Prepare leadership briefing
9 Action Hierarchy Less memory or reliance on individual performance More memory and reliance on individual performance Stronger Actions Intermediate Actions Weaker Actions Architectural/physical plant changes New devices with usability testing before purchasing Engineering control or interlock (forcing functions) Simplify the process and remove unnecessary steps Standardize equipment or process Tangible involvement and action by leadership in support of patient safety Redundancy Increase in staffing/decrease in workload Software enhancements/modifications Education using simulation-based learning with a competency assessment completed on a recurring basis Eliminate/reduce distractions (sterile medical environment) Checklist/cognitive aid Eliminate look and sound-alikes Repeat-back/Read-back Enhanced documentation/communication Double checks Warnings and labels New procedure/memorandum/policy Traditional training Additional study/analysis 9

10 10

11 Munson Medical Center Patient Safety Team 11
12 Foundations of Safety Culture Trainers Site Coord MMC Cadillac Grayling POMH Kalkaska Charlevoix Manistee Rachel Stein Lindsey Mack Amanda Rommell Jessica Blazok Joanna Benchley Kathryn Bandfield- Keough Jeremy Carlson Theresa Schepers Roberta Bellinger Dawn Cupp Susan Kilbourn Nancy Goodyear Julie Banktson Ann Holmes Kris Thomas Judy Spoor Kim Babcock Christine Bissonette Connie Farrier Allyssa Brooks Mike Aenis Allen Stout Grace Berry Diane Valley Gina Hodges Michelle Ruhser Mellissa (Missy) Hilliard- John 4 Kassidy Fleis Ben Elliott Heather Kage Alexi (Alex) Callaway 5 John Bolde Theresa Feldhauser Pam Walsh Delaney Bachman Melanie Engels Claudia Orth Frank Mancuso Diane Barton Julie Botsford 11 Penny Hawkins Wendy Hunt Tiffany Fortin Katherine Parrish Kathy Sahs Kristen Horton Cathy Munoz Beth Workman Grover Raymond Jennifer Fuhrman Rebecca Reda Jessica Fultz Amanda Trudgeon Michael Hodnett Tonimaree Verville John Charette Kristen King 12
Appendix G: The LFD Tool
 Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
Title: Learning from Defects Learning from and Preventing adverse events
 Title: Learning from Defects Learning from and Preventing adverse events Armstrong Institute for Patient Safety and Quality Presented by: David A. Thompson DNSc, MS, RN Title: Associate Professor The Johns
Title: Learning from Defects Learning from and Preventing adverse events Armstrong Institute for Patient Safety and Quality Presented by: David A. Thompson DNSc, MS, RN Title: Associate Professor The Johns
How effective and sustainable are Root. HFESA Conference
 How effective and sustainable are Root Cause Analysis (RCA) investigations 27 th November 2017 HFESA Conference Peter Hibbert, Matthew Thomas, Anita Deakin, Bill Runciman, Jeffrey Braithwaite Acknowledgements:
How effective and sustainable are Root Cause Analysis (RCA) investigations 27 th November 2017 HFESA Conference Peter Hibbert, Matthew Thomas, Anita Deakin, Bill Runciman, Jeffrey Braithwaite Acknowledgements:
Root Cause Analysis. Why things happen
 Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA
 Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Moving Towards RCA 2 : See One, Do One, Take it Home!
 ML16 The presenters have nothing to disclose Moving Towards RCA 2 : See One, Do One, Take it Home! IHI National Forum Orlando, Florida December 11, 2017 Elizabeth Mort, MD, MPH Brian Cummings, MD; Jana
ML16 The presenters have nothing to disclose Moving Towards RCA 2 : See One, Do One, Take it Home! IHI National Forum Orlando, Florida December 11, 2017 Elizabeth Mort, MD, MPH Brian Cummings, MD; Jana
Root Cause Analysis (Part I) event/rca_assisttool.doc
 event/rca_assisttool.doc") (Part I) http://www.jcaho.org/accredited+organizations/sentinel+ event/rca_assisttool.doc Edited by Dr. E. Terry DIO Dr. S.K. Oliver OME Examines the reasons an error occurred Suggests changes to the system
(Part I) http://www.jcaho.org/accredited+organizations/sentinel+ event/rca_assisttool.doc Edited by Dr. E. Terry DIO Dr. S.K. Oliver OME Examines the reasons an error occurred Suggests changes to the system
Proactive Risk Assessment Models. March 7, MHA Patient Safety and Quality Symposium. Joseph DeRosier, PE, CSP 1
 2017 MHA Patient Safety and Quality Symposium Healthcare Failure Mode and Effect Analysis (HFMEA) Proactive Risk Assessment Joseph DeRosier, PE, CSP derosierjm@gmail.com Why conduct proactive risk assessments?
2017 MHA Patient Safety and Quality Symposium Healthcare Failure Mode and Effect Analysis (HFMEA) Proactive Risk Assessment Joseph DeRosier, PE, CSP derosierjm@gmail.com Why conduct proactive risk assessments?
Department of Defense INSTRUCTION. SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP)
 Patient Safety Program (PSP) (MHSPSP)") Department of Defense INSTRUCTION NUMBER 6025.17 August 16, 2001 SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP) ASD(HA) References: (a) Sections 742 and 754 of the Floyd D.
Department of Defense INSTRUCTION NUMBER 6025.17 August 16, 2001 SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP) ASD(HA) References: (a) Sections 742 and 754 of the Floyd D.
QAPI Making An Improvement
 Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN
 UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
Root Cause Analysis. Responding to a Sentinel Event
 2.1 HOURS Root Cause Analysis Responding to a Sentinel Event Brenda M. Ewen, MSN, RN, CPHRM, and Gale Bucher, MSN, RN, COS-C rors. Root cause analysis (RCA) provides an evidence-based structure for methodical
2.1 HOURS Root Cause Analysis Responding to a Sentinel Event Brenda M. Ewen, MSN, RN, CPHRM, and Gale Bucher, MSN, RN, COS-C rors. Root cause analysis (RCA) provides an evidence-based structure for methodical
Hospital Survey on Patient Safety Culture: Debrief and Action Planning
 Hospital Survey on Patient Safety Culture: Debrief and Action Planning August 7, 2018 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association 1 Three
Hospital Survey on Patient Safety Culture: Debrief and Action Planning August 7, 2018 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association 1 Three
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
Root Cause Analysis: The NSW Health Incident Management System
 Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Hand out 1 Incident decision tree. Per person-in pack Handout 2 YCFF habd out (2 sided with explanations) per person in pack Handout 3 NPSA quick ref
 per person in pack Handout 3 NPSA quick ref") Hand out 1 Incident decision tree. Per person-in pack Handout 2 YCFF habd out (2 sided with explanations) per person in pack Handout 3 NPSA quick ref guide to SEA. per person in pack Handout 4 Our SEA
Hand out 1 Incident decision tree. Per person-in pack Handout 2 YCFF habd out (2 sided with explanations) per person in pack Handout 3 NPSA quick ref guide to SEA. per person in pack Handout 4 Our SEA
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
uncovering key data points to improve OR profitability
 REPRINT March 2014 Robert A. Stiefel Howard Greenfield healthcare financial management association hfma.org uncovering key data points to improve OR profitability Hospital finance leaders can increase
REPRINT March 2014 Robert A. Stiefel Howard Greenfield healthcare financial management association hfma.org uncovering key data points to improve OR profitability Hospital finance leaders can increase
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
Designing for Safety
 2014 FGI Guidelines Update Series FGI Guidelines Update #1 July 11, 2013 Designing for Safety Ellen Taylor, AIA, MBA, EDAC In 2010 one of the topics introduced to the Guidelines for Design and Construction
2014 FGI Guidelines Update Series FGI Guidelines Update #1 July 11, 2013 Designing for Safety Ellen Taylor, AIA, MBA, EDAC In 2010 one of the topics introduced to the Guidelines for Design and Construction
Table of Contents. TeamSTEPPS Framework and Competencies Key Principles. Team Structure Multi-Team System For Patient Care
 Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Joint Commission Update for Ambulatory Clinics
 Joint Commission Update for Ambulatory Clinics Mary Beth McLellan, RN, BSN Manager of Clinical Operations Rapid City Regional Hospital Family Medicine Residency Program Objectives: Participants will understand
Joint Commission Update for Ambulatory Clinics Mary Beth McLellan, RN, BSN Manager of Clinical Operations Rapid City Regional Hospital Family Medicine Residency Program Objectives: Participants will understand
Hospital Adverse Event Reporting Program: an Initial Evaluation
 Hospital Adverse Event Reporting Program: an Initial Evaluation When the Patient Safety Commission began the Adverse Event Reporting Program in May, 2006, we promised hospitals we would complete an evaluation
Hospital Adverse Event Reporting Program: an Initial Evaluation When the Patient Safety Commission began the Adverse Event Reporting Program in May, 2006, we promised hospitals we would complete an evaluation
Design Principles for Learning and Caring in Patient-Centered Primary Care Homes
 The H.R. Bob Brettell, MD, Memorial Lectureship January 29, 2013 Design Principles for Learning and Caring in Patient-Centered Primary Care Homes Judith L. Bowen, MD, FACP Professor of Medicine Oregon
The H.R. Bob Brettell, MD, Memorial Lectureship January 29, 2013 Design Principles for Learning and Caring in Patient-Centered Primary Care Homes Judith L. Bowen, MD, FACP Professor of Medicine Oregon
The Patient Safety Act Reporting and RCA Requirements
 The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
INTEGRATING CHRONIC CARE MANAGEMENT INTO COMMUNITY PHARMACY PRACTICE
 INTEGRATING CHRONIC CARE MANAGEMENT INTO COMMUNITY PHARMACY PRACTICE ACPE UAN: 0107-9999-17-101-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon completion
INTEGRATING CHRONIC CARE MANAGEMENT INTO COMMUNITY PHARMACY PRACTICE ACPE UAN: 0107-9999-17-101-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon completion
Page 1 of 5 Version No: 6 Authorised by: General Counsel
 Feedback Action Analysis Prioritisation Classificattion Notification Identification INCIDENT MANAGEMENT Patient informed / Family informed if required Event occurs If staff injury form must be printed,
Feedback Action Analysis Prioritisation Classificattion Notification Identification INCIDENT MANAGEMENT Patient informed / Family informed if required Event occurs If staff injury form must be printed,
Using Transparency to Drive Patient Safety
 Session Code These presenter s have nothing to disclose Using Transparency to Drive Patient Safety Doug Salvador, MD MPH Chief Quality Officer, Baystate Health Chief Medical Officer, Baystate Medical Center
Session Code These presenter s have nothing to disclose Using Transparency to Drive Patient Safety Doug Salvador, MD MPH Chief Quality Officer, Baystate Health Chief Medical Officer, Baystate Medical Center
Wrong PSV Found Installed in Field
 Wrong PSV Found Installed in Field Lessons Learned Volume 04 Issue 12 2004 USW Wrong PSV Found Installed in Field Purpose To conduct a small group lessons learned activity to share information gained from
Wrong PSV Found Installed in Field Lessons Learned Volume 04 Issue 12 2004 USW Wrong PSV Found Installed in Field Purpose To conduct a small group lessons learned activity to share information gained from
Accident Investigation: Root Cause Analysis
 Accident Investigation: Root Cause Analysis Prepared for: Alabama Health Care Association SUMMARY and OBJECTIVES Accident Investigation: Root Cause Analysis Prepared for: Alabama Health Care Association
Accident Investigation: Root Cause Analysis Prepared for: Alabama Health Care Association SUMMARY and OBJECTIVES Accident Investigation: Root Cause Analysis Prepared for: Alabama Health Care Association
Development and assessment of a Patient Safety Culture Dr Alice Oborne
 Development and assessment of a Patient Safety Culture Dr Alice Oborne Consultant pharmacist safe medication use March 2014 Outline 1.Definitions 2.Concept of a safe culture 3.Assessment of patient safety
Development and assessment of a Patient Safety Culture Dr Alice Oborne Consultant pharmacist safe medication use March 2014 Outline 1.Definitions 2.Concept of a safe culture 3.Assessment of patient safety
9/9/2016. How Respiratory Therapist Enhance Patient Safety. Introduction. Raise your hand. Tawana Shaffer CPHRM, MBA, BSc, CRT
 How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
Objectives. Key Elements. ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management 5/20/2014
 ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
POLICY NAME POLICY # Sentinel, Adverse Event and Near Miss. CSP Reporting and Investigation
 Purpose To outline a reporting system that promotes client safety by learning from experiences and utilizing the results of investigations and data analysis to prepare and disseminate recommendations for
Purpose To outline a reporting system that promotes client safety by learning from experiences and utilizing the results of investigations and data analysis to prepare and disseminate recommendations for
Auditing and Monitoring Focusing Your Resources
 Auditing and Monitoring Focusing Your Resources Subscriber Webinar June 13, 2014 Today s Plan Why a hospice should devote resources to auditing and monitoring Setting priorities Guidelines for developing
Auditing and Monitoring Focusing Your Resources Subscriber Webinar June 13, 2014 Today s Plan Why a hospice should devote resources to auditing and monitoring Setting priorities Guidelines for developing
Risk Assessment Scoring and Matrix
 Risk Assessment Scoring and Matrix Appendix 2 Consequence score (severity levels) and examples of descriptors 1 2 3 4 5 Domains Negligible Minor Moderate Major Catastrophic Impact on the safety of patients,
Risk Assessment Scoring and Matrix Appendix 2 Consequence score (severity levels) and examples of descriptors 1 2 3 4 5 Domains Negligible Minor Moderate Major Catastrophic Impact on the safety of patients,
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager
 Ratchada Prakongsai Senior Manager") Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Survey Analysis for Evaluating Risk (SAFER ) Insights July 13, 2017
 Insights July 13, 2017") Survey Analysis for Evaluating Risk (SAFER ) Insights July 13, 2017 Caroline Heskett, MPH The Joint Commission, Accreditation & Certification Operations Project Manager, Business Transformation Objectives
Survey Analysis for Evaluating Risk (SAFER ) Insights July 13, 2017 Caroline Heskett, MPH The Joint Commission, Accreditation & Certification Operations Project Manager, Business Transformation Objectives
Subject:Alaris/Care Fusion Syringe Pumps. Dear Colleagues,
 From: Hupp, Diane Sent: Friday, April 17, 2015 8:51 PM To: Davis, Peter (ANES); Cain, James G; Ambrose, Heather; Bojtos, Brooke; Brytus, Jeanne M; Butler, Gabriella; Cales, Rebecca; Cancilla, Diane; Carlson,
From: Hupp, Diane Sent: Friday, April 17, 2015 8:51 PM To: Davis, Peter (ANES); Cain, James G; Ambrose, Heather; Bojtos, Brooke; Brytus, Jeanne M; Butler, Gabriella; Cales, Rebecca; Cancilla, Diane; Carlson,
University of Washington School of Nursing - Continuing Nursing Education 1
 A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
Human Factors. Frank Federico, RPh. This presenter has nothing to disclose.
 Human Factors Frank Federico, RPh This presenter has nothing to disclose. 25 February 2015 Culture Learning System Improvement and Measurement Transparency Continuous Learning Accountability Teamwork &
Human Factors Frank Federico, RPh This presenter has nothing to disclose. 25 February 2015 Culture Learning System Improvement and Measurement Transparency Continuous Learning Accountability Teamwork &
TeamSTEPPSCM. Strategies & Tools to Enhance Performance and Patient Safety
 TeamSTEPPSCM Strategies & Tools to Enhance Performance and Patient Safety Agency for Healthcare Research and Quality Advancing Exce fence in Health Care www.ahrq.gov TeamSTEPPS Team Competency Outcomes
TeamSTEPPSCM Strategies & Tools to Enhance Performance and Patient Safety Agency for Healthcare Research and Quality Advancing Exce fence in Health Care www.ahrq.gov TeamSTEPPS Team Competency Outcomes
Case Study Comprehensive Analysis: Elopement from a Long- Term Care Home
 CANADIAN INCIDENT ANALYSIS FRAMEWORK Case Study Comprehensive Analysis: Elopement from a Long- Term Care Home 2012 Canadian Patient Safety Institute All rights reserved. Permission is hereby granted to
CANADIAN INCIDENT ANALYSIS FRAMEWORK Case Study Comprehensive Analysis: Elopement from a Long- Term Care Home 2012 Canadian Patient Safety Institute All rights reserved. Permission is hereby granted to
COOK COUNTY HEALTH & HOSPITALS SYSTEM
 COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
PROPOSAL FORMAT FOR REQUEST OF AFS RESEARCH FUNDS SPONSORING TECHNICAL COMMITTEE/DIVISION FORM
 PROPOSAL FORMAT FOR REQUEST OF AFS RESEARCH FUNDS SPONSORING TECHNICAL COMMITTEE/DIVISION FORM Sponsoring Committee: : Division Nos. Approval Communication Submitted for Proposal Yes No Project Title:
PROPOSAL FORMAT FOR REQUEST OF AFS RESEARCH FUNDS SPONSORING TECHNICAL COMMITTEE/DIVISION FORM Sponsoring Committee: : Division Nos. Approval Communication Submitted for Proposal Yes No Project Title:
TIME OUT! A Patient Safety Strategy. Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service
 TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
Event Based Nursing Peer Review: Knowing Harm to No Harm
 Event Based Nursing Peer Review: Knowing Harm to No Harm Arkansas Children s Hospital Mitch Highfill, BSN, RN Debra Jeffs, PhD, RN-BC Stephanie Benning, MSN, APRN, PCNS-BC, CPN Ellen Mallard, MSN, APRN,
Event Based Nursing Peer Review: Knowing Harm to No Harm Arkansas Children s Hospital Mitch Highfill, BSN, RN Debra Jeffs, PhD, RN-BC Stephanie Benning, MSN, APRN, PCNS-BC, CPN Ellen Mallard, MSN, APRN,
Improving the Pre-Empted Medication Error Reporting System at St. Charles Hospital, Port Jefferson, NY
 Improving the Pre-Empted Medication Error Reporting System at St. Charles Hospital, Port Jefferson, NY Contributed by Kathleen LeDoux, MS, RN, BC, CPHQ Performance Improvement Nurse, St. Charles Hospital,
Improving the Pre-Empted Medication Error Reporting System at St. Charles Hospital, Port Jefferson, NY Contributed by Kathleen LeDoux, MS, RN, BC, CPHQ Performance Improvement Nurse, St. Charles Hospital,
Risk Management in the ASC
 1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
High Reliability Organizations The Key to Improving Quality and Safety
 High Reliability Organizations The Key to Improving Quality and Safety William B Munier, MD, MBA Acting Director Center for Quality Improvement and Patient Safety Agency for Healthcare Research and Quality
High Reliability Organizations The Key to Improving Quality and Safety William B Munier, MD, MBA Acting Director Center for Quality Improvement and Patient Safety Agency for Healthcare Research and Quality
Patient Care Coordination Variance Reporting
 Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
Identifying Solutions for Nurses Health IT Pain Points March 1, 2016 at 2:30 PM
 Identifying Solutions for Nurses Health IT Pain Points March 1, 2016 at 2:30 PM Nancy Staggers, PhD, RN, FAAN, Entrepreneur & Professor, Summit Health Informatics & University of Utah Ellen Makar, MSN,
Identifying Solutions for Nurses Health IT Pain Points March 1, 2016 at 2:30 PM Nancy Staggers, PhD, RN, FAAN, Entrepreneur & Professor, Summit Health Informatics & University of Utah Ellen Makar, MSN,
National Patient Safety Agency Root Cause Analysis (RCA) Investigation
 Investigation") National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
Incident Reporting and Investigation Guideline
 Incident Reporting and Investigation Guideline Guideline Owner: Director Human Resources Services Centre Keywords: 1) Accident 2) Investigation 3) Reporting 4) Incident 5) Guideline Intent Organisational
Incident Reporting and Investigation Guideline Guideline Owner: Director Human Resources Services Centre Keywords: 1) Accident 2) Investigation 3) Reporting 4) Incident 5) Guideline Intent Organisational
LEVEL 2 REPORTING IN PACE.
 LEVEL 2 REPORTING IN PACE. MEDICAL DIRECTOR ROLE AND RESPONSIBILITIES, Stephen Ryan, MD, MPH Sr Medical Director PACE & Managed LTC Medical Director ElderONE, RRH WHO ARE WE? Geriatrician Medical Director
LEVEL 2 REPORTING IN PACE. MEDICAL DIRECTOR ROLE AND RESPONSIBILITIES, Stephen Ryan, MD, MPH Sr Medical Director PACE & Managed LTC Medical Director ElderONE, RRH WHO ARE WE? Geriatrician Medical Director
SUPPORT FOR VULNERABLE GP PRACTICES: PILOT PROGRAMME
 Publications Gateway Reference 04476 For the attention of: NHS England Directors of Commissioning Operations Clinical Leaders and Accountable Officers, NHS Clinical Commissioning Groups Copy: NHS England
Publications Gateway Reference 04476 For the attention of: NHS England Directors of Commissioning Operations Clinical Leaders and Accountable Officers, NHS Clinical Commissioning Groups Copy: NHS England
INCIDENT INVESTIGATION PROGRAM
 INCIDENT INVESTIGATION PROGRAM 1.0 PURPOSE The purpose of this program is to prevent the recurrence of an incident and to eliminate or minimize the risks associated with the incident. 2.0 SCOPE This procedure
INCIDENT INVESTIGATION PROGRAM 1.0 PURPOSE The purpose of this program is to prevent the recurrence of an incident and to eliminate or minimize the risks associated with the incident. 2.0 SCOPE This procedure
GUIDELINES FOR THE USE OF ASSISTIVE TECHNOLOGY EQUIPMENT IN COMMUNITY INPATIENT UNITS
 GUIDELINES FOR THE USE OF ASSISTIVE TECHNOLOGY EQUIPMENT IN COMMUNITY INPATIENT UNITS Guideline Reference: 1666 Version: 2.1 Status: Adopted Type: Clinical Guideline Guideline applies to (Staff Group)
GUIDELINES FOR THE USE OF ASSISTIVE TECHNOLOGY EQUIPMENT IN COMMUNITY INPATIENT UNITS Guideline Reference: 1666 Version: 2.1 Status: Adopted Type: Clinical Guideline Guideline applies to (Staff Group)
Improving Student Critical Thinking Skills through a Root Cause Analysis (RCA) Pilot Project
 Pilot Project") Improving Student Critical Thinking Skills through a Root Cause Analysis (RCA) Pilot Project Dana Tschannen, PhD, RN Michelle Aebersold, PhD, RN University of Michigan, School of Nursing June 3, 2010 Presentation
Improving Student Critical Thinking Skills through a Root Cause Analysis (RCA) Pilot Project Dana Tschannen, PhD, RN Michelle Aebersold, PhD, RN University of Michigan, School of Nursing June 3, 2010 Presentation
Learning from Actual & Near Miss Events
 POST-EVENT DEBRIEFING TOOL & INTERVIEW GUIDE Learning from Actual & Near Miss Events Using Debriefing Methodology Jeffrey Klenklen, MS, RN, NE-BC, CPHQ, CPHRM Senior Director of Patient Safety & Clinical
POST-EVENT DEBRIEFING TOOL & INTERVIEW GUIDE Learning from Actual & Near Miss Events Using Debriefing Methodology Jeffrey Klenklen, MS, RN, NE-BC, CPHQ, CPHRM Senior Director of Patient Safety & Clinical
Barriers to a Positive Safety Culture. Donna Zankowski MPH RN
 Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
These Things (Don t Have to) Happen Patient Safety Tami Minnier Chief Quality Officer Friday, April 5, 2013
 Happen Patient Safety Tami Minnier Chief Quality Officer Friday, April 5, 2013") These Things (Don t Have to) Happen Patient Safety 2013 Tami Minnier Chief Quality Officer Friday, April 5, 2013 Agenda Review the current state of healthcare Define and understand the concept of reliability
These Things (Don t Have to) Happen Patient Safety 2013 Tami Minnier Chief Quality Officer Friday, April 5, 2013 Agenda Review the current state of healthcare Define and understand the concept of reliability
Gantt Chart. Critical Path Method 9/23/2013. Some of the common tools that managers use to create operational plan
 Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Unique Identifier: Review Date: November Issue Status: Approved Version No: 1.4 Issue Date: November 2017
 Policy Authors Name & Title: Dr Mark Jackson, Director of Research & Informatics Dr Raphael Perry, Medical Director Scope: Trust Wide Classification: Non Clinical Replaces: version 1.3 To be read in conjunction
Policy Authors Name & Title: Dr Mark Jackson, Director of Research & Informatics Dr Raphael Perry, Medical Director Scope: Trust Wide Classification: Non Clinical Replaces: version 1.3 To be read in conjunction
Quality Assessment and Assurance. Guidance Training (F520) (o)
 (o)") Quality Assessment and Assurance Guidance Training (F520) 483.75(o) 2006 1 Today s Agenda! Regulation! Interpretive Guidelines! Investigative Protocol! Determination of Compliance! Deficiency Categorization
Quality Assessment and Assurance Guidance Training (F520) 483.75(o) 2006 1 Today s Agenda! Regulation! Interpretive Guidelines! Investigative Protocol! Determination of Compliance! Deficiency Categorization
Overview of Root Cause Analysis
 Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
Policy for the Investigation, Analysis and Learning from Incidents, Complaints and Claims
 Policy for the Investigation, Analysis and Learning from Incidents, Complaints and Claims Please be aware that this printed version of the Policy may NOT be the latest version. Staff are reminded that
Policy for the Investigation, Analysis and Learning from Incidents, Complaints and Claims Please be aware that this printed version of the Policy may NOT be the latest version. Staff are reminded that
HRSA/Bureau of Primary Health Care (BPHC) Presentation
 Presentation") HRSA/Bureau of Primary Health Care (BPHC) Presentation Educational Webinar September 14, 2017 Valerie Henriques, MA, M.Ed., RN Joint Commission Clinical Surveyor 1 Webinar Objectives: Discuss the theory
HRSA/Bureau of Primary Health Care (BPHC) Presentation Educational Webinar September 14, 2017 Valerie Henriques, MA, M.Ed., RN Joint Commission Clinical Surveyor 1 Webinar Objectives: Discuss the theory
Continuity of Care in General Practice Registrar Training: Results from the ReCEnT study
 Continuity of Care in General Practice Registrar Training: Results from the ReCEnT study Mr James W Pearlman 1,2 Dr Parker Magin 1,2 Dr Simon Morgan 2 Dr Cathy Regan 2 Ms Kim Henderson 2 Ms Amanda Tapley
Continuity of Care in General Practice Registrar Training: Results from the ReCEnT study Mr James W Pearlman 1,2 Dr Parker Magin 1,2 Dr Simon Morgan 2 Dr Cathy Regan 2 Ms Kim Henderson 2 Ms Amanda Tapley
Effective Incident Command System
 Effective Incident Command System Public Health Response to Katrina Evacuees Pam Blackwell, RN Director, Center for Emergency Preparedness and Response Alpha Bryan, MD District Health Director Cobb & Douglas
Effective Incident Command System Public Health Response to Katrina Evacuees Pam Blackwell, RN Director, Center for Emergency Preparedness and Response Alpha Bryan, MD District Health Director Cobb & Douglas
The following tables define the impact and likelihood scoring options and the resulting score: - Risk score. Category
 LIKELIHO OD NHS Eastern Cheshire Clinical Commissioning Group: Quality Impact Assessment Tool v1 Overview This tool involves an initial assessment (stage 1) to quantify potential impacts (positive or negative)
LIKELIHO OD NHS Eastern Cheshire Clinical Commissioning Group: Quality Impact Assessment Tool v1 Overview This tool involves an initial assessment (stage 1) to quantify potential impacts (positive or negative)
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
3/30/2015. Objectives. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
MLK MACC Organizational Structure (Deliverable #3)
") MLK MACC Organizational Structure (Deliverable #3) February 29, 2008 Introduction The complexity of the transition from a fully functioning hospital to an ambulatory care center should not be under-estimated.
MLK MACC Organizational Structure (Deliverable #3) February 29, 2008 Introduction The complexity of the transition from a fully functioning hospital to an ambulatory care center should not be under-estimated.
EP7f, CN III OB Hemorrhage.pdf OBSTETRIC HEMORRHAGE. Amelia Indig RN Clinical Nurse III Candidate December 17, 2009
 OBSTETRIC HEMORRHAGE Amelia Indig RN Clinical Nurse III Candidate December 17, 2009 1 OBJECTIVE OF THE PROJECT EP7f, CN III OB Hemorrhage.pdf Determine opportunities to improve patient safety and quality
OBSTETRIC HEMORRHAGE Amelia Indig RN Clinical Nurse III Candidate December 17, 2009 1 OBJECTIVE OF THE PROJECT EP7f, CN III OB Hemorrhage.pdf Determine opportunities to improve patient safety and quality
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
improvement program to Electronic Health variety of reasons, experts suggest that up to
 Reducing Hospital Readmissions March/2017 The readmission rate for patients discharged to a skilled nursing facility is 25% within 30 days1. What can senior care providers do to reduce these hospital readmissions?
Reducing Hospital Readmissions March/2017 The readmission rate for patients discharged to a skilled nursing facility is 25% within 30 days1. What can senior care providers do to reduce these hospital readmissions?
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE CLINICAL ADVERSE EVENTS SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND
TITLE CLINICAL ADVERSE EVENTS SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND
TELLIGENCE. Workflow Solutions. Integrated Workflow Intelligence. Ascom
 Ascom TELLIGENCE Workflow Solutions Integrated Workflow Intelligence Ascom Telligence workflow solutions The next evolution in nurse call systems is here: designed to help staff be more productive, enhance
Ascom TELLIGENCE Workflow Solutions Integrated Workflow Intelligence Ascom Telligence workflow solutions The next evolution in nurse call systems is here: designed to help staff be more productive, enhance
Policy for the Reporting and Management of Incidents Including Serious Incidents. Version Number: 006
 CONTROLLED DOCUMENT Policy for the Reporting and Management of Incidents Including Serious Incidents CATEGORY: CLASSIFICATION: PURPOSE Controlled Number: Document Policy Governance To set out the principles
CONTROLLED DOCUMENT Policy for the Reporting and Management of Incidents Including Serious Incidents CATEGORY: CLASSIFICATION: PURPOSE Controlled Number: Document Policy Governance To set out the principles
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
RECENT DEVELOPMENTS 3/17/2015
 Trends, Challenges, and Best Practices for an Effective Home Health Compliance Program Asha Scielzo, Special Counsel Pillsbury Winthrop Shaw Pittman Tina Rao, Chief Counsel of Healthcare Maxim Healthcare
Trends, Challenges, and Best Practices for an Effective Home Health Compliance Program Asha Scielzo, Special Counsel Pillsbury Winthrop Shaw Pittman Tina Rao, Chief Counsel of Healthcare Maxim Healthcare
Muskoka Algonquin Healthcare Patient Safety Plan
 Muskoka Algonquin Healthcare Patient Safety Plan Muskoka Algonquin Healthcare s (MAHC) three year patient safety plan is designed to support and promote the mission, vision, and values of its organization,
Muskoka Algonquin Healthcare Patient Safety Plan Muskoka Algonquin Healthcare s (MAHC) three year patient safety plan is designed to support and promote the mission, vision, and values of its organization,
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Baler Gone Wild! Lessons Learned. Volume 03 Issue USW
 Baler Gone Wild! Lessons Learned Volume 03 Issue 29 2004 USW Baler Gone Wild! Purpose To conduct a small group lessons learned activity to share information gained from incident investigations. To understand
Baler Gone Wild! Lessons Learned Volume 03 Issue 29 2004 USW Baler Gone Wild! Purpose To conduct a small group lessons learned activity to share information gained from incident investigations. To understand
1.0 Standard. Title: Date of Issue: Feb Incident Investigation Policy & Procedure. Approved By: Review/ Revision Date. 1-Nov-10.
 Title: Incident Investigation Policy & Procedure Date of Issue: Feb 2001 Approved By: Mark Runciman Review/ Revision Date 1-Nov-10 Location: All Locations Ref. No: HS-002 1.0 Standard 1.1 Purpose To ensure
Title: Incident Investigation Policy & Procedure Date of Issue: Feb 2001 Approved By: Mark Runciman Review/ Revision Date 1-Nov-10 Location: All Locations Ref. No: HS-002 1.0 Standard 1.1 Purpose To ensure
Journal Club. Medical Education Interest Group. Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety.
 Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB
 Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient Safety
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient Safety
Monday, August 15, :00 p.m. Eastern
 Monday, August 15, 2016 2:00 p.m. Eastern Dial In: 888.863.0985 Conference ID: 34874161 Slide 1 Speakers Deb Kilday, MSN, RN Senior Performance Partner Performance Services Quality & Safety Premier, Inc.
Monday, August 15, 2016 2:00 p.m. Eastern Dial In: 888.863.0985 Conference ID: 34874161 Slide 1 Speakers Deb Kilday, MSN, RN Senior Performance Partner Performance Services Quality & Safety Premier, Inc.
February New Zealand Health and Disability Services National Reportable Events Policy 2012
 February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
A Systems Approach to Patient Safety at the VA
 BRIGHT IDEAS A Systems Approach to Patient Safety at the VA Erika Hatva The Department of Veterans Affairs (VA) operates the largest integrated healthcare system in the United States, serving 8.76 million
BRIGHT IDEAS A Systems Approach to Patient Safety at the VA Erika Hatva The Department of Veterans Affairs (VA) operates the largest integrated healthcare system in the United States, serving 8.76 million
ECRI Patient Safety Organization HFACS and Healthcare
 October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
Transfer Information. Your transfer to Munson Medical Center
 Transfer Information Your transfer to Munson Medical Center Important Phone Numbers Munson Medical Center can be reached by calling: (231) 935-5000 or 1-800-4-MUNSON (1-800-468-6766) Additional Notes:
Transfer Information Your transfer to Munson Medical Center Important Phone Numbers Munson Medical Center can be reached by calling: (231) 935-5000 or 1-800-4-MUNSON (1-800-468-6766) Additional Notes:
UPMC Passavant POLICY MANUAL
 UPMC Passavant POLICY MANUAL SUBJECT: Quality Plan 2017 POLICY: 04.078 DATE: July 2016 INDEX TITLE: Administrative PURPOSE/OBJECTIVES: To continuously improve the quality healthcare we provide in our community
UPMC Passavant POLICY MANUAL SUBJECT: Quality Plan 2017 POLICY: 04.078 DATE: July 2016 INDEX TITLE: Administrative PURPOSE/OBJECTIVES: To continuously improve the quality healthcare we provide in our community