Adult Retrieval Victoria ANNUAL REVIEW
|
|
|
- Denis May
- 5 years ago
- Views:
Transcription


1 Adult Retrieval Victoria ANNUAL REVIEW

2 ADULT RETRIEVAL VICTORIA Ambulance Victoria Unit 4/12 Larkin Court, Essendon Fields, VIC, 3041 Phone: arvadmin@ambulance.vic.gov.au Released: 06 November Ambulance Victoria Values Being Respectful Working Together Being Accountable Openly Communicating Driving Innovation 2
3 Contents 1. Introduction Clinical Lead Highlights of Recent Publications RETRIEVAL TRAUMA TRANSFER OUTCOME STUDY (RTTOS) CIVILIAN AEROMEDICAL TRANSFER RETRIEVAL REMS SCORE VALIDATION CRITICAL AIRWAY MANAGEMENT OXFORD HANDBOOK OF RETRIEVAL MEDICINE Preparation for retrieval Data: Activity and Performance CASE AND RETRIEVAL ACTIVITY Case Rate by Region and Date Activity Rates by Time of Day and Day of Week REFERRAL SITE Referring Hospital (highest referral rates) Top 50 referral hospitals Referral Hospital by Region CASE TYPE Clinical Problem Patient Age and Gender TRAUMA CASE ACTIVATION TIME (ARRIVAL TO REFERRAL TO ARV) CASE DURATION DESTINATION HOSPITAL Destination Unit REASON FOR CASE REFERRAL Reason for Transfer vs. Region of Origin Service Unavailable vs. Problem Type vs. Referral Region RETRIEVAL RETRIEVAL PLATFORM CREW MIX VS. PLATFORM QUALITY MEASURES Performance Times ARV Coordinator Contact Time Crew Appropriateness Clinical Variations Critical Care Access Restriction
4 1. Introduction The current year has presented challenges and opportunities for ARV. The reorganisation of structure within the department has provided additional leadership and operational capability to ARV, in particular by providing more accessible staff, rostered more flexibly for case management. Inclusion of additional registrar and fellow positions though roster reorganisation has allowed case volume growth and greater around-the-clock responsiveness. Consequently case activity has grown in response to increased demand for both metropolitan and rural and regional retrieval services, as well as additional AV support for clinicians, early warning activation of cases and support for prehospital thrombolysis. Despite the reorganisation, ARV continues to grow consistently as demonstrated in the graph below, and consequently, service delivery is becoming more challenging within the current physical and fiscal environment. To address this continued growth, particularly in coordination and 24 hour responsiveness, continued work on redesign and caseload management capability will require ongoing review and rework of material and human resources, physical environment and accommodations, and fiscal resources Total Cases Total Retrieval Cases The current year has also seen expanded scope of practice: Beyond conventional retrieval services, ARV has demonstrated a capability, and met a need to provide broader outreach services. If such growth is to continue, it is recommended that this be in the context of a formally re-planned program of development. Growth areas and potential future expansion areas include: Outreach support for urgent care centres via telehealth and existing modalities Coordination of hyper-specialty patient transfer: cerebral clot retrieval, neurosurgical emergencies, cardiac patients (within the context of the developing state services plan), major trauma transfer Education and training (Trauma Victoria) IT and systems support: REACH development of applications for Mental Health Beds, Neonatal Critical Care bed management. ARVIS development of applications for PIPER for acute case management and coordination. Telehealth coordination and governance Potentially expanded clinical roles: ECMO, REBOA, other Other potential system roles Collaboration with paediatric retrieval services (PIPER), to investigate opportunity to work more closely in research, education and training and clinical case management. As Ambulance Victoria progresses through appointment of a new Board and CEO in 2015, ARV has transferred within the organisational structure to sit in the newly formed Clinical and Community Services Division. 2. Clinical Lead Appointment of Dr Charlotte Evans as ARV Clinical Lead The Clinical Lead role is a new ½ time leadership position within the department, commencing May 25th The primary objective of this position is to lead the Retrieval Team including Retrieval Registrars and Consultants to provide highest standard, and consistent clinical coordination and retrieval services in line with AV & DHHS standards thereby increasing value to customers and the organisation. In addition the position will provide specialist advice and support to a range of stakeholders including the following specific areas: 4

5 Provide leadership and innovation in development and implementation of clinical retrieval practice, including advanced contemporary and developing interventional critical care and retrieval practice Provide consultation, expert opinion and guidance on Audit and incident review including review of ARV cases/incidents and trends in incident reporting as requested by the Director or Medical Advisor(s) Provide supervision, clinical advice and support to Retrieval Consultants undertaking Critical Care Coordination and Retrieval Response Develop and maintain positive relationships with various stakeholders to assist in the delivery of a safe and seamless service to the community Liaise with other AV departments and key external stakeholders in the decision making process with respect to retrieval mission coordination and execution Contribute to the development of retrieval practice as a professional discipline in external settings such as: learned colleges (e.g. ACEM), academic and research environments Charlotte has extensive experience in emergency medicine, trauma and retrieval medicine, and is co-author of the soon to be published Oxford Handbook of Retrieval Medicine. She also has interests in education and simulation training systems and delivery. She has a range of formal qualifications including: MBBS, BSc, MRCS, MCEM (UK), FACEM, GCEH (Aeromedical & Retrieval), GCCS. 3. Highlights of Increased activity and services delivered: Cases 11.3%, Retrieval Total 4.95%, Medical Retrieval 5.1% ARV has been re-accredited by the Australasian College for Emergency Medicine for advanced training for registrars (six-months special skills). To replace previous on-call night registrar arrangements, 24 hour registrar on-shift staffing commenced from February ARV consultant coordinators are now on-base 16 ½ hours per day (08:00-22:30) and provide on-call cover overnight. Trauma Victoria successfully launched Moodle-based learning modules for all of the Victorian State Trauma Committee guidelines. These are available to clinicians across the state. ARV has provided support for about 50% of AV prehospital thrombolysis cases as a part of the AV trial of this new intervention. ARV now has telehealth and tele radiology linkages to most health services in the state. Electronic case referral was launched, allowing referral sites to save clinician time and increase accuracy of case referrals directly into ARVIS : 5
6 4. Recent Publications 4.1 Retrieval Trauma Transfer Outcome Study (RTTOS) Impact of the Introduction of an Integrated Adult Retrieval Service on Major Trauma Outcomes Kennedy, Marcus P, Gabbe, Belinda J, McKenzie, Ben A Emergency Medicine Journal (BMJ), 2015 The primary aim of this study was to examine the impact of the introduction of an integrated adult critical care patient retrieval system in Victoria, Australia on early clinical outcomes for major trauma patients who undergo inter-hospital transfer. The secondary aims were to examine the impact on quality and process measures for inter-hospital transfers in this population, and on longer term patient-reported outcomes. Method: This is a cohort study utilising data contained in the Victorian State Trauma Registry (VSTR) for major trauma patients >18 years of age between 2009 and 2013 who had undergone inter-hospital transfer. For eligible patients, data items were extracted from the VSTR for analysis: demographic, injury details, hospital details, transfer details, Adult Retrieval Victoria (ARV) coordination indicator and transfer indicator, key clinical observations and outcomes. Results: There were 3,009 major trauma inter-hospital transfers in the state with a transfer time less than 24 hours. ARV was contacted for 1,174 (39.0%) transfers. ARV coordinated metropolitan transfers demonstrated lower adjusted odds of in-hospital mortality compared to metropolitan transfers occurring without ARV coordination (OR 0.39, ). Adjusting for destination hospital type demonstrates that this impact was principally due to ARV facilitation of a Major Trauma Service as the destination for transferred patients (OR 0.41, ). The median time spent at the referral hospital was lower for ARV coordinated transfers: 5.4 hours ( ) vs 6.1 ( ), p< Conclusion: In a mature trauma system, an effective retrieval service can further reduce mortality and improve long-term outcomes. 4.2 Civilian aeromedical transfer Civilian aeromedical retrievals (the Australian experience) R Ramadas, S Hendel, A MacKillop BJA Education, 2015, 1 5 doi: /bjaed/mkv040 Retrieval medicine is the process by which suitably qualified and trained personnel utilize appropriate equipment and transport platforms to clinically manage and safely transport a patient from one location to another. Retrievals can be subclassified into primary, secondary, and tertiary. Primary retrieval is the transport of patients to their initial hospital reception. This may be their nearest hospital, or directly to a larger and more distant centre such as a designated trauma centre. Secondary retrievals move patients from a non- specialized hospital to a higher level of clinical care such as for neurosurgery, interventional cardiology, complex obstetrics, or paediatrics. Tertiary retrievals transport patients between two similarly specialized hospitals. In modified primary retrievals, an injured or unwell patient has already been taken to an initial health facility that has minimal capacity to increase the level of care to that provided in the prehospital environment. In these circumstances, the retrieval team apply similar practices to a true primary retrieval, albeit in a more controlled clinical environment. In Australia, owing to the large land mass and relatively low population density, specialized medical services are clustered mostly in coastal urban centres. Therefore, many referrals are from rural and remote areas where access to specialist medical services is limited. Journeys range from a few kilometres and a few minutes in major capital cities to several thousand kilometres over many hours from isolated rural communities. While distance might not be limiting, other access issues such as terrain and weather extremes play roles in the structure of services. Most retrieval occurs within state health system jurisdictions or within state boundaries. If there is need to transfer patients interstate or internationally, pre-existing agreements between the relevant authorities are important to safely facilitate transfer. These patients have often received initial medical care at the place of presentation. With the increased ease and popularity of travel, particularly to developing nations with limited healthcare capacity, international retrievals/repatriations are becoming common. They bring with them unique logistic and cultural issues for the retrieval team, in addition to the challenges of medical retrieval. 6
7 4.3 Retrieval REMS Score Validation The Retrieval Rapid Emergency Medical Score in Retrieval Medicine Kennedy, Marcus P, Wilson, Krystle, Gabbe, Belinda J, Straney, Lahn, Michael Bailey Emergency Medicine Australasia, 2015 Objective: Prognostic models are commonly used in the clinical setting. The objective of the study is to evaluate the prognostic accuracy of the Rapid Emergency Medical Score (REMS) or alternate models. Methods: A retrospective cohort study of critical care patients who underwent retrieval service transfer to an Intensive Care Unit (ICU) in a single state-wide service in Victoria, Australia. All patients aged 18 years and over transferred to an ICU between 01/1/2010 and 30/6/2013. Retrieval and ICU datasets were probabilistically linked. Multivariable logistic regression modelling was used to investigate the capacity of physiological markers and patient characteristics to predict in hospital mortality in the ICU population. The prediction performance was evaluated using measures of discrimination (C-statistic) and calibration (Hosmer-Lemeshow (H-L statistic)). Results: There were 1776 ICU patients who were transferred and 1749 (98.5%) had complete data. Of the 1749 patients with complete data, 257 (14.7%) died in-hospital. The REMS calculated at the time of retrieval referral demonstrated borderline predictive capability (C-statistic 0.69, 95% CI ). Following logistic regression analysis of the REMS components, final variables included in the Retrieval REMS model were age, mean arterial pressure and Glasgow Coma Score. This model demonstrated acceptable predictive capability (C-statistic % CI ). The median (IQR) Retrieval REMS for survivors and non-survivors respectively was 7 (5,10) and 9 (7,11) p<0.01. Conclusions: The availability of a validated tool such as Retrieval REMS assists recognition of high risk patients and consideration of this risk in retrieval mission planning and response. 4.4 Critical Airway Management Prospective observational study of emergency airway management in the critical care environment of a tertiary hospital in Melbourne J. F. Dyett, M. S. Moser, A. E. Tobin Anaesth Intensive Care :5 The objective of this study is to describe the population of patients receiving emergency airway management outside operating theatres at our institution, a tertiary referral centre in Melbourne. A registry of all patients receiving emergency airway management in the emergency department, ICU and on the wards as part of Medical Emergency Response teams care, was prospectively collected. There were 128 adults and one paediatric patient requiring emergency airway management recruited to the study. Data for analysis included patient demographics, preoxygenation and apnoeic oxygenation, staff, drugs, details of laryngoscopic attempts, adjuncts, airway manoeuvres, complications sustained and method of confirmation of endotracheal tube placement. Over a 12-month period, there were 139 intubations of 129 patients, requiring a total of 169 attempts. Respiratory failure was the most common indication for intubation. Intubation was successful on the first episode of laryngoscopy in 116 (83.5%) patients. Complications occurred in 48 patients. In the cohort of patients without respiratory failure, nasal cannulae apnoeic oxygenation significantly reduced the incidence of hypoxaemia (0 out of 31 [0.0%] versus 10 out of 60 [16.7%], P=0.016; absolute risk reduction 16.7%; number needed to treat: 6). Waveform capnography was used to confirm endotracheal tube placement in 133 patients and there were four episodes of oesophageal intubation, all of which were recognised immediately. In the critical care environment of our institution, emergency airway management is achieved with a first-attempt success rate that is comparable to overseas data. Nasal cannulae apnoeic oxygenation appears to significantly reduce the risk of hypoxaemia in patients without respiratory failure and the use of waveform capnography eliminates episodes of unrecognised oesophageal intubation. 7




8 4.5 Oxford Handbook of Retrieval Medicine Edited by Charlotte Evans, Anne Creaton and Marcus Kennedy, the first edition of this text is now in production, for release early in This is the first text of its type and draws on the work of many experts in the area of Retrieval Medicine in Australia and the UK. Published by Oxford University Press Forward to the First Edition: Retrieval medicine has existed in various guises for many decades however in recent years has become more systematised as an area of specialist clinical practice and an area of clinical medicine which requires its own body of literature, educational systems, qualifications and recognition. The days are gone where retrieval was critical care transfer by junior staff, with ad hoc equipment and monitoring, non specialised transport platforms, all enveloped by a clinical governance void! In contradistinction, around the world we now have specialist training systems that are established or developing, formal qualifications and defined standards and accreditation in many settings. University courses and qualifications in aeromedical, prehospital and retrieval medicine have emerged, and research activity is progressing positively. In addition, governance systems, regulation, accreditation, data sharing and benchmarking are also appearing worldwide. This progress is however not uniform, and indeed retrieval medicine is practised in a vast range of models around the world. We have approached this textbook from the perspective that there is international commonality at the core of this discipline, and that systems of patient care and clinical retrieval medicine are similar in many countries. We have consulted widely with international colleagues and adopted generic approaches where possible, and feel confident that the contents of this work will be of value and relevance to all retrieval practitioners from those working in high volume critical care retrieval services to those who are occasional retrievalists or need to maintain low volume patient transfer capability. It is our aim to add to the knowledge that drives standards of patient care and the quality of clinical outcomes. Each of us has seen the difference between non-systematised patient transfer, and the transfer of patients via professional retrieval services who deploy well trained, educated and supported staff. We hope that this work will contribute further to these systems, this quality of retrieval care, and the health of our communities. 8

9 5. Preparation for retrieval 9
10 6. Data: Activity and Performance Case and Retrieval Activity Case Rate b y Region and Date Total Cases Retrieval ARV case activity Total Cases Retrieval Region Total Region Total Metro 967 Metro 21.13% Gippsland 890 Gippsland 19.45% Loddon Mallee 708 Loddon Mallee 15.47% Hume 662 Hume 14.46% Barwon South West 548 Barwon South West 11.97% Grampians 450 Grampians 9.83% Undefined (eg prehosp consult) 262 Undefined (eg prehosp consult) 5.75% New South Wales 79 New South Wales 1.73% Australian Capital Territory 3 Australian Capital Territory 0.07% Tasmania 3 Tasmania 0.07% Northern Territory 2 Northern Territory 0.04% South Australia 1 South Australia 0.02% Queensland 1 Queensland 0.02% Grand Total 4577 Grand Total % A case is any occasion of service provided for a patient by ARV. It may involve critical care or other advice, retrieval, or facilitation of access to a critical care bed. ARV cases originate from all parts of the State of Victoria, with small numbers from interstate (particularly southern NSW). Case rates have increased by 11.3% from The geographical distribution of case origins remains similar to previous years, with the exception of the number of Metro referrals which has increased by 21%. Ongoing support to AV staff, clinicians and AAV (including authorisation of transfusion and early / prehospital notification of cases) has continued to increase through Case rates in winter months are somewhat higher than summer months. 10

11 Cases per annum 12 AM 1 AM 2 AM 3 AM 4 AM 5 AM 6 AM 7 AM 8 AM 9 AM 10 AM 11 AM 12 PM 1 PM 2 PM 3 PM 4 PM 5 PM 6 PM 7 PM 8 PM 9 PM 10 PM 11 PM Cases per annum Cases per annum Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Activity Rates b y Time of Da y and Da y of Week Distribution of calls through the day shows relatively uniform spread of cases through day and evening hours possibly reflecting earlier activation of retrieval. The pattern of calls (by time and day) has not altered in the current year. ARV continues to advocate for early referral of cases likely to need transfer. ARV performs 6-7 retrievals per day which are evenly spread throughout the week. Distribution of retrievals through the day shows relatively even spread from hrs, with lower rates overnight Day of Week Monday Tuesday Wednesday Thursday Friday Saturday Sunday ARV receives approximately cases per day which are evenly spread throughout the week. Case rates at peak periods during winter months can reach critical care cases within 24 hours and at times concurrent cases. This case volume creates significant pressure on current single Call taker/coordinator capacity and requires flex of additional administrative and support staff into these roles.
12 6.2 Referral Site Referring Hospital (highest referral rates) Referral Hospital Total Bairnsdale Regional Health Service 222 Bendigo Hospital, The 211 Goulburn Valley Health [Shepparton] 195 Mercy Public Hospitals Inc [Werribee] 185 Latrobe Regional Hospital [Traralgon] 179 Northeast Health Wangaratta 168 New Mildura Base Hospital 168 University Hospital Geelong 151 Ballarat Health Services [Base Campus] 149 South West Healthcare [Warrnambool] 139 Echuca Regional Health 136 Wimmera Base Hospital [Horsham] 131 West Gippsland Healthcare Group [Warragul] 125 Albury Wodonga Health - Albury 125 Bass Coast Health 118 The 15 highest volume referral sites for ARV cases shows a significant variation in hospital types and service needs. Over 85% of transfers are due to lack of availability of specialised clinical services. Some additional caseload in this year relates to primary response support for Ambulance Victoria where the ARV coordinator provides advice to the AV clinician, authorises procedures (eg blood administration), consults on prehospital thrombolysis, or receives early warning of a major trauma patient being transported to a small hospital. There is little overall change in pattern in Top 50 referral hospitals Albury Wodonga Health - Albury 125 Mansfield District Hospital 20 Albury Wodonga Health - Wodonga 43 Maroondah Hospital [East Ringwood] 60 Alexandra District Hospital 23 Maryborough District Health Service [Maryborough] 41 Alfred, The [Prahran] 27 Mercy Public Hospitals Inc [Werribee] 185 Angliss Hospital 39 Monash Medical Centre [Clayton] 28 Austin Hospital 19 New Mildura Base Hospital 168 Bairnsdale Regional Health Service 222 Northeast Health Wangaratta 168 Ballarat Health Services [Base Campus] 149 Northern Hospital, The [Epping] 80 Bass Coast Health 118 Orbost Regional Health 37 Bendigo Hospital, The 211 Portland District Health 80 Box Hill Hospital 81 Rosebud Hospital 24 Casey Hospital 35 Seymour Health 23 Central Gippsland Health Service [Sale] 84 South Gippsland Hospital [Foster] 37 Colac Area Health 58 South West Healthcare [Camperdown] 23 Dandenong Campus 55 South West Healthcare [Warrnambool] 139 Deniliquin Hospital & Community Health Services 52 St John of God Geelong Hospital 18 East Grampians Health Service [Ararat] 28 Stawell Regional Health 35 East Wimmera Health Service [St Arnaud] 18 Sunshine Hospital 49 Echuca Regional Health 136 Swan Hill District Health [Swan Hill] 80 Frankston Hospital 105 University Hospital Geelong 151 Goulburn Valley Health [Shepparton] 195 West Gippsland Healthcare Group [Warragul] 125 Hamilton Base Hospital 57 West Wimmera Health Service [Nhill] 17 Kerang District Health 22 Western Hospital [Footscray] 47 Latrobe Regional Hospital [Traralgon] 179 Wimmera Base Hospital [Horsham] 131 Leongatha Memorial Hospital 34 Yarram & District Health Service 20 (by referral count, arranged alphabetically)
 Cardiac 1118 24.51% Trauma 922 20.21% Neurological_Neurosurgical 688 15.08% Respiratory 517 11.33% Gastrointestinal 306 6.")

. A significant component of this caseload is related to interventional cardiology needs.")
 is yet to result in alteration in this pattern. Trauma has increased as a proportion of ARV workload (from 19.")
13 6.2.3 Referral Hospital b y Region Gippsland, 890, 21% Metro, 967, 22.47% Loddon Mallee, 708, 16% New South Wales, 79, 2% Grampians, 450, 10% Hume, 662, 15% Barwon South West, 548, 13% 6.3 Case Type Clinical Problem Principal Problem (referral site) Cardiac % Trauma % Neurological_Neurosurgical % Respiratory % Gastrointestinal % Sepsis % Toxicological % Vascular (not neuro) % Renal % Other % Oncology % Endocrine % Immune_Allergy % Haematological % Obstetric/Gynaecological % ENT % Genitourinary % Metabolic % Dermatology % Psychosocial % Musculoskeletal % All ARV cases are classified according to clinical problem type. The range of clinical problems defined at the referral point is consistent across the State. Cardiac problems account for 25% of cases across the system (unchanged from 14-15). A significant component of this caseload is related to interventional cardiology needs. Given the time criticality of this type of case, the need for efficient retrieval and transfer services is highlighted. Recently increasing regional capability for acute cardiac intervention (PCI) is yet to result in alteration in this pattern. Trauma has increased as a proportion of ARV workload (from 19.11% in 14-15) and in absolute volume (from 786 cases to 922 cases) as gains continue to be made in improving processes to encourage early referral to ARV for coordination of interhospital transfer of major trauma patients. There has been a slight decrease in the number of neurosurgical and acute neurological referrals.
14 Problem Type Cardiac Trauma Neurological_Neurosurgical Respiratory Gastrointestinal Sepsis Toxicological Vascular (not neuro) Renal Other Oncology Endocrine Immune_Allergy Haematological Obstetric/Gynaecological ENT Genitourinary Metabolic Dermatology Psychosocial Musculoskeletal Patient Age and Gender Gender Total Female 37.89% Male 61.94% Unknown 0.17% Males are significantly more commonly in need of retrieval or critical care transfer services, with patients over 60 years forming 48% of the ARV caseload. Distribution remains unchanged. Gender imbalance is less pronounced in younger groups. Mean Age = (SD 19.27) Female Male
15 Minutes 6.4 Trauma Case activation time (arrival to referral to ARV) ARV promotes early activation of the retrieval system this ensures most efficient organisation of retrieval and early delivery of the patient to a point of definitive care provision. This is known to be of importance to outcomes in major trauma in particular. Data presented in the table below represents trauma cases referred to ARV (from Victorian Health Services, with complete time data, time from patient arrival to referral < 12 hours). Data reported is mean minutes to referral (patient arrival at hospital to time of ARV contact), with standard deviation, 90 th percentile, proportion of cases referred within 60 minutes (major trauma referral time goal). Trauma Cases Referred to ARV ALL ARV CASES BSW Gippsland Grampians Hume Loddon Mallee Metro All Trauma Cases Mean Std dev th %ile %<60min 16% 21% 16% 18% 16% 9% 16% 22% Number mean std dev Mean time for referral of trauma patients is 181 minutes (vs 194 for all ARV referrals) across Victoria. Trauma guidelines suggest <60 minutes as a threshold target for referral time. Considerable variability is seen between regions, with metro referral times for trauma patients averaging almost 4 hours. 25% 20% 15% 10% 5% 0% % referred <60min %<60min Trauma guidelines suggest <60 minutes as a threshold target for referral of major trauma patients. The data indicates considerable opportunity for more urgent activation of trauma referrals for consultation or transfer. Less than 10% of metro trauma transfers are referred to retrieval within 60 minutes.
16 6.5 Case duration Principal Problem Average case duration (min) Cardiac 349 Dermatology 353 Endocrine 331 ENT 252 Gastrointestinal 402 Genitourinary 392 Haematological 344 Immune_Allergy 316 Metabolic 304 Neurological_Neurosurgical 356 Obstetric/Gynaecological 236 Oncology 380 Other 313 Psychosocial 438 Renal 379 Respiratory 399 Sepsis 398 Toxicological 327 Trauma 379 Vascular (not neuro) 311 Region Average case duration (min) Barwon South West 332 Gippsland 372 Grampians 402 Hume 364 Loddon Mallee 412 Metro 308 New South Wales 375 Tasmania 595 Case duration is the time from initial call to ARV until a case is closed generally after confirmation of arrival of a patient at a destination hospital. Data is limited to ARV standard cases (excluding prehospital early notifications, AV authorisations etc) This data is presented for the first time in to illustrate the resource application to ARV cases (retrieved and non-retrieved) vs problem type and by health region. Typically, assessment, coordination and transfer of critical care retrieval patients takes a total of 5-6 hours, during which up to phone calls or logistic conversations occur in the management of each patient. Tasmania New South Wales Metro Loddon Mallee Hume Grampians Gippsland Barwon South West Case Duration Minutes
17 6.6 Destination Hospital Total Alfred, The [Prahran] 804 Royal Melbourne Hospital - City Campus 486 St Vincent s Hospital 401 University Hospital Geelong 256 Monash Medical Centre [Clayton] 231 Austin Hospital 212 Western Hospital [Footscray] 99 Dandenong Campus 87 Bendigo Hospital, The 78 Latrobe Regional Hospital [Traralgon] 74 Ballarat Health Services [Base Campus] 68 Frankston Hospital 67 Box Hill Hospital 64 Northern Hospital, The [Epping] 57 Epworth Hospital [Richmond] 38 Note: Data presented in this table represents standard retrieval cases (excludes categories such as AV support, early prehospital notification of trauma cases etc) The Alfred, St. Vincent s and The Royal Melbourne Hospitals are the most common receiving sites, consistent with previous years data. Geelong Hospital maintains a reasonably strong regional and geographical catchment. Additional trauma load is a likely key factor in this change in distribution. Non Tertiary Metro hospitals and regional hospitals receive 23% of ARV case distribution. This distribution is consistent year on year. (Geelong Hospital is counted as a Tertiary Hospital in the above calculations) Destination Unit Destination Unit Adult General 6.96% 4.23% Angio_Cath Lab 1.50% 1.13% Burns N/A 0.15% CCU 14.75% 14.82% ED 41.27% 41.31% HDU 2.43% 3.30% ICU 30.38% 33.15% Isolation (shared) N/A 0.03% Theatre 0.56% 0.54% Other 2.15% 1.34% The most common destination unit is the ED (41%) with ICU/HDU (33%) next. It is preferred that transferred patients be received into a critical care ward setting to decrease impact on congested emergency departments. Major trauma patients and other unstable patients are normally and appropriately transferred to the MTS ED for initial trauma team workup. 6.7 Reason for Case Referral Reason for Transfer Specialised Clinical Service not available 3601 Prehospital Notification 302 ICU bed not available 243 Clinical advice 154 Appropriate Medical Staff not available 71 CCU bed not available 52 AV Interventions Authorisation 51 HDU bed not available 40 Other 26 Uninsured Patient in Private Hospital 10 Back Transfer 5 General Ward bed not available 4 Appropriate Nursing Staff not available 3 There has been significant change in recorded reason for referral. More cases have been recorded in with reasons for transfer of specialised clinical service unavailable This classification now includes major trauma transfers which in previous years had been reported separately. Local ICU bed availability appears less of a driver for transfers than service availability a consistent finding in previous years. Prehospital early notification appears as a reason for referral for the first time in this year s data.
18 6.7.1 Reason for Transfer vs. Region of Origin Barwon South West Gippsland Grampians Hume Loddon Mallee Metro Grand Total Specialised Clinical Service not available 11.43% 17.74% 9.36% 13.78% 13.99% 17.10% 83.40% ICU bed not available 0.33% 0.55% 0.10% 0.21% 0.90% 3.68% 5.77% Notification 0.45% 0.90% 0.48% 0.62% 0.43% 0.26% 3.14% Clinical advice 0.33% 0.74% 0.36% 0.45% 0.57% 0.31% 2.76% Appropriate Medical Staff not available 0.21% 0.40% 0.17% 0.24% 0.36% 0.29% 1.66% CCU bed not available 0.10% 0.43% 0.10% 0.19% 0.26% 0.17% 1.24% HDU bed not available 0.07% 0.19% 0.05% 0.05% 0.12% 0.48% 0.95% Other 0.07% 0.07% 0.05% 0.12% 0.10% 0.14% 0.55% Uninsured Patient in Private Hospital 0.00% 0.00% 0.02% 0.00% 0.00% 0.21% 0.24% Back Transfer 0.00% 0.00% 0.00% 0.00% 0.00% 0.10% 0.10% General Ward bed not available 0.00% 0.05% 0.00% 0.00% 0.00% 0.05% 0.10% Appropriate Nursing Staff not available 0.02% 0.00% 0.00% 0.00% 0.05% 0.00% 0.07% Authorisation 0.00% 0.00% 0.00% 0.05% 0.00% 0.00% 0.05% Availability of specialised services (especially cardiac and neurological-neurosurgical) remains a much greater contributor to reason for transfer in non-metro settings. (Cardiac = 24.83%, Trauma = 18.39% and Neuro 13.04%) Lack of local availability of ICU and HDU beds was a significantly higher factor in transfer in the metro region Service Unavailable vs. Problem T ype vs. Referral Region When patients are transferred due to lack of locally available specialty services it is useful to understand what services may need to be considered in future strategic planning, and in which regions. Principle Problem (accounting for 85% of transfers) by region of origin Barwon SW Gippsland Grampians Cardiac Trauma Neurological_Neurosurgical Respiratory Gastrointestinal Sepsis Vascular (not neuro) Toxicological Renal Hume Loddon Mallee Metro Total
19 6.8 Retrieval Retrieval: Retrieval is the transfer of a patient from one hospital to another in which specialised clinical teams and transport platforms and equipment are used. These teams may include medical, nursing, paramedic or MICA paramedic personnel. Patient retrieval provides specialised assessment and management, prior to and during transfer of time critical or critically ill patients. Retrieval occurs from facilities where resources or services are inappropriate for ongoing care to facilities that are able to provide definitive care for the patient. During transfer, a retrieval team provides the same or higher standard of care than that available at the point of referral. Time Critical: In respect of Retrieval Transfer, a patient is considered time critical if the patient has a clinical condition which presents an immediate threat to life, limb, cognition or future quality of life, and: Delay in definitive treatment will significantly increase that outcome risk, and; Definitive management of that condition or threat is likely to be achieved by urgent transfer to another hospital, or; Management of that condition definitively, or for a prolonged interim period, is beyond the resource capacity or clinical skill capacity of the current provider (or would result in unacceptable resource drain and exposure of other patients to risk). Region Number of cases retrieved Australian Capital Territory 2 Barwon South West 339 Gippsland 480 Grampians 243 Hume 446 Loddon Mallee 466 Metro 404 New South Wales 49 Medical (& paramedic) crew Tasmania 2 Crew Consultant Registrar Total Overall approximately 53% of ARV cases (55% ) progress to a coordinated retrieval (the remainder receiving bed coordination services or isolated clinical advice). For regional cases this proportion is considerably higher, with 63% progressing to retrieval. Retrieval crewing is mixed, with the distribution trending slightly towards paramedic crewing: 43% doctor and paramedic crew and 57% paramedic (MICA) only crew. Medical crews are despatched from Essendon where 24 hour on-base staffing is now maintained. Medical crewed cases have increased by 5% in the current year Registrars previously based part-time at Geelong are now located at Essendon (from February 2015) and have contributed to the increased response capability seen in Paramedic only crew Grand Total
20 6.9 Retrieval Platform Principal Transport Platform used for patient movement AAV Fixed Wing HATS HEMS HEMS HEMS HEMS HEMS CPAV Emerg Road Other (blank) Principal Retrieval Transport Platform Total Air 66.39% HATS 15.94% Emerg Road 14.80% Notes: HEMS: Helicopter, HEMS 5 is the Retrievaldedicated helicopter HATS: High acuity transport service Private sector provided ambulance with critical care nurse crew (+/- ARV staff) CPAV: Complex patient ambulance large ambulance capable of additional crew load and bariatric patient care Emerg Road: standard emergency ambulance Air transport is utilised in 66% of retrieval cases. HEMS 5 (retrieval helicopter) accounted for only 8.1% of retrievals (cf 7.3% ) whilst other rotary transfers account for 14% of retrievals indicating that there may be significant scope for review of utilisation of rotary platforms for medical retrieval Crew Mix vs. Platform Principal Transport Platform utilisation Dr + Paramedic Crew Paramedic Only Crew AV Fixed Wing HATS HEMS HEMS HEMS HEMS HEMS CPAV 22 2 Emerg Distribution of AV road vs. air platform use for retrieval cases is split between Dr/Paramedic and Paramedic-only crew types with a higher proportion of medical retrieval utilising the road platforms. As is expected from crew geographical distribution, regional HEMS is largely Paramedic-only crewed. The data continues to demonstrate marked differences in crew mix practices based on geographical distribution of helicopters, with regional patients experiencing significantly lower crewing intensity when transferred by regionally based rotary platforms. Some 469 (increased from 442 in ) HEMS critical care interhospital transfers were completed with paramedic-only crewing. Ideally such patients would be managed by a combined doctor paramedic crew to optimise clinical standards. This data strongly suggests that improvement in access to rotary wing platforms and optimised paramedic-doctor team crewing of missions remains an opportunity for improvement for Ambulance Victoria. Formal analysis of the reasons for this distribution will be undertaken in and remedial recommendations will be developed. All platforms crewmix proportions : retrieval cases 100% 80% 60% 40% 20% 0% AV Fixed Wing HATS HEMS1 HEMS2 HEMS3 HEMS4 HEMS5 CPAV Emerg Paramedic Only Crew Dr + Paramedic Crew
21 6.11 Quality Measures ARV collects a comprehensive range of clinical and performance data and reports a suite of quality measures internally to Ambulance Victoria and externally to stakeholders. The subset below are presented annually to the sector Performance Times Jul- Sep Oct- Dec Jan- Mar Apr- Jun Jul- Sep Oct- Dec Jan- Mar Apr- Jun Mean Mobilisation time (min) for time critical cases (1) Mobilisation time (min) for time critical cases: 90th percentile (2) Mean Mobilisation time (min) for acute cases (3) Mobilisation time (min) for acute cases: 90th percentile (4) Median At Patient Time (min) (5) Proportion of Cases with At Patient (clinical) Time < 90 Minutes (6) n/a 89% 86% 88% 87% 82% 83% Improvements are noted by green shading no significant deterioration is seen in any of these quality measures 1) Time critical cases have a recommended mobilisation time (call received to en route) <30 minutes 2) Measure of performance spread (proportion within performance goal) 3) Acute cases have a recommended mobilisation time (call received to en route) <90 minutes 4) Measure of performance spread (proportion within performance goal) 5) At patient clinical time (at patient to ready to depart) Goal is 60 minutes. 6) Measure of performance spread (proportion within performance goal) : % <90 minutes, with a 90% threshold or target ARV Coordinator Contact Time Jul-Sep Oct-Dec Jan-Mar Apr-Jun Mean Coordinator contact time % cases with Coordinator contact time 15min 91.8% 92.5% 95.0% 90.3% Mean Time from call received to coordinator in discussion with referrer. Goal is less than 15 minutes. Measure of performance spread (proportion within performance goal target is 95%) ARV aim to provide referrers with access to a specialist critical care coordinator within 15 minutes of initiating a call. Some slippage has been noted in the performance of this indicator related to the overall workload increases experienced this year. Overall caseload has increased by 11%, with peak month growth (Apr-Jun) increasing by 17.3%. Strategies to manage this growth efficiently are being implemented including electronic streamlined referral processes and additional call taking and coordination staffing.
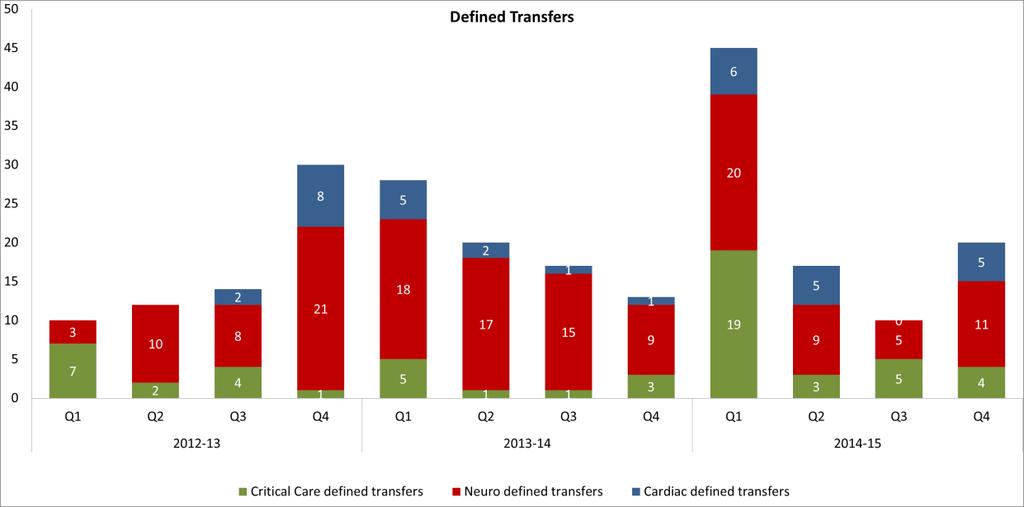
22 Crew Appropriateness Jul- Sep Oct- Dec Jan- Mar Apr- Jun Jul- Sep Oct- Dec Jan- Mar Apr- Jun Proportion of High Complexity cases with medical crewed retrieval (1) 76% 70% 63% 73% 70% 67% 69% 67% Despatch of second retrieval crew (required due to patient need for higher skill set) (2) (1) High complexity retrieval cases represent the group of patients most in need of maximised crew skill sets. In such cases coordinators attempt to task combined medical and paramedic crews (usually MICA). The (arbitrary) performance threshold for this indicator is 80%. Reasons for inability to medically crew high complexity cases includes platform availability (see previous data). (2) Initial crew dispatched is unable to provide the required level of care, and a second crew is required (with higher skill set). This is a key indicator for the quality of clinical coordination, case assessment and planning. ARV patients are by their nature critically unwell and often unstable, and as such it is expected that this measure would not be zero, but would be small and stable as a proportion of caseload. Performance against this indicator is stable Clinical Variations July-Sep Oct-Dec Jan-Mar Apr-Jun Very serious (Levels 1) Moderately serious (Level 2) Minor documentation (Level 3-4) No variation All cases where medical staff provides crewing are reviewed by ARV. Staff receive feedback on the findings of the review of each case they perform. Minor variations to documentation or guideline adherence are managed by ARV clinical advisor feedback to medical staff. More serious variations where patient harm may (or does) occur are referred for external clinical review and reported to the Clinical Review Committee Critical Care Access Restriction In August 2008, DHHS implemented an Interim Critical Care Access Guideline which provided a mechanism to manage situations where critical care bed occupancy was extremely high. ARV developed a system of early warning of low ICU bed capacity via a group fax and system. In early 2009, this system was modified to provide earlier warning (resulting in increased rates of notification). In 2010, this system was moved to a combination of and SMS alert messaging when system occupancy is critical. Where no ICU bed can be identified for a patient who requires time critical transfer, ARV will define a destination for that patient and ensure transfer of the patient (rather than have the patient wait for an extended time in a setting which is unable to provide the required level of care). Such distribution is managed carefully across the system and reported regularly to DHHS. In January 2010 this process was expanded to include defined transfer for acute neurosurgical patients who though not critical, have time urgent neurosurgical problems and require transfer to a neurosurgical unit. Similarly in January 2013, a system for defined transfer of cardiac patients was introduced. The rate of defined transfers is somewhat seasonal, and has decreased from year to year due to improvement in critical care patient distribution and access management, and to increased ICU bed capacity in Victoria. The peak in critical care defined transfers noted in Quarter 1 of this year is likely due to seasonal pressures and increased rates of respiratory disease and ICU ventilation days. This safety and quality initiative has resulted in more timely transfer of a number of patients whose clinical outcomes may have become compromised due to inability to access specialist care. It has also raised awareness of this issue and the need to ensure access queues manage both acuity and urgency for optimised clinical outcomes.
23
24
PIPER. Defined transfer (Time Critical Newborn)
") PIPER Paediatric Infant Perinatal Emergency Retrieval Defined transfer (Time Critical Newborn) Review date: June 2018 1 P a g e Defined transfer (Time Critical Newborn) Retrieval System Paediatric Infant
PIPER Paediatric Infant Perinatal Emergency Retrieval Defined transfer (Time Critical Newborn) Review date: June 2018 1 P a g e Defined transfer (Time Critical Newborn) Retrieval System Paediatric Infant
PETS Activity Report The Victorian Paediatric Emergency Service
 PETS Activity Report 2012-2013 The Victorian Paediatric Emergency Service The Victorian The Victorian Victorian Paediatric Emergency Transport Service Paediatric Emergency Transport Service Activity Activity
PETS Activity Report 2012-2013 The Victorian Paediatric Emergency Service The Victorian The Victorian Victorian Paediatric Emergency Transport Service Paediatric Emergency Transport Service Activity Activity
Safe Patient Care (Nurse to Patient and Midwife to Patient Ratios) Bill 2015
 Bill 2015") Version No. 001 Safe Patient Care (Nurse to Patient and Midwife to Patient Ratios) Act 2015 No. 51 of 2015 Version as at 23 December 2015 Safe Patient Care (Nurse to Patient and Midwife to Patient Ratios)
Version No. 001 Safe Patient Care (Nurse to Patient and Midwife to Patient Ratios) Act 2015 No. 51 of 2015 Version as at 23 December 2015 Safe Patient Care (Nurse to Patient and Midwife to Patient Ratios)
Adult Retrieval Victoria -An update. DR EMMELINE FINN Clinical lead (Acting)
") Adult Retrieval Victoria -An update DR EMMELINE FINN Clinical lead (Acting) My Background Emergency Physician by trade Pre-hospital and Retrieval Medicine Specialist Disaster Management MIMMS and EMERGO
Adult Retrieval Victoria -An update DR EMMELINE FINN Clinical lead (Acting) My Background Emergency Physician by trade Pre-hospital and Retrieval Medicine Specialist Disaster Management MIMMS and EMERGO
Haematology Registrar (clinical) Registrar Appointments for 2011
 Registrar Appointments for 2011") Studley Road, Heidelberg, 3084 Haematology Registrar (clinical) Registrar Appointments for 2011 Name of Unit / Specialty: Head of Unit: CSU / Department: Haematology Cancer services Contact person for
Studley Road, Heidelberg, 3084 Haematology Registrar (clinical) Registrar Appointments for 2011 Name of Unit / Specialty: Head of Unit: CSU / Department: Haematology Cancer services Contact person for
Critical Care HMO/PGY
 Studley Road, Heidelberg, 3084 Critical Care HMO/PGY 3 2018 Thank you for your interest in applying for a position in the Critical Care HMO/PGY3 stream at Austin Health (AH). Introduction There will be
Studley Road, Heidelberg, 3084 Critical Care HMO/PGY 3 2018 Thank you for your interest in applying for a position in the Critical Care HMO/PGY3 stream at Austin Health (AH). Introduction There will be
Employee name: Positions reporting to this one:
 MERCY PUBLIC HOSPITALS INC POSITION DESCRIPTION Core Mercy Values: Compassion, Hospitality, Respect, Innovation, Stewardship, Teamwork Position title: Entity/Group: Business Unit/Department: Position reports
MERCY PUBLIC HOSPITALS INC POSITION DESCRIPTION Core Mercy Values: Compassion, Hospitality, Respect, Innovation, Stewardship, Teamwork Position title: Entity/Group: Business Unit/Department: Position reports
Cardiology Registrar 2013
 Studley Road, Heidelberg, 3084 Cardiology Registrar 2013 Registrar Appointments for 2013 Name of Unit / Specialty: Head of Unit: CSU / Department: CARDIOLOGY A/PROF OMAR FAROUQUE SPECIALTY SERVICES/CARDIOLOGY
Studley Road, Heidelberg, 3084 Cardiology Registrar 2013 Registrar Appointments for 2013 Name of Unit / Specialty: Head of Unit: CSU / Department: CARDIOLOGY A/PROF OMAR FAROUQUE SPECIALTY SERVICES/CARDIOLOGY
Cardiology Registrar 2011
 Studley Road, Heidelberg, 3084 Cardiology Registrar 2011 Registrar Appointments for 2011 Name of Unit / Specialty: Head of Unit: CSU / Department: CARDIOLOGY A/PROF OMAR FAROUQUE SPECIALTY SERVICES/CARDIOLOGY
Studley Road, Heidelberg, 3084 Cardiology Registrar 2011 Registrar Appointments for 2011 Name of Unit / Specialty: Head of Unit: CSU / Department: CARDIOLOGY A/PROF OMAR FAROUQUE SPECIALTY SERVICES/CARDIOLOGY
Emergency department presentations of Victorian Aboriginal and Torres Strait Islander people
 Emergency department presentations of Victorian Aboriginal and Torres Strait Islander people Nadia Costa, Mary Sullivan, Rae Walker and Kerin M Robinson Abstract This paper explains how routinely collected
Emergency department presentations of Victorian Aboriginal and Torres Strait Islander people Nadia Costa, Mary Sullivan, Rae Walker and Kerin M Robinson Abstract This paper explains how routinely collected
VICTORIAN PUBLIC HOSPITALS REFEREE ASSESSMENT FORM NEONATAL REGISTRAR POSITIONS
 VICTORIAN PUBLIC HOSPITALS REFEREE ASSESSMENT FORM NEONATAL REGISTRAR POSITIONS INSTRUCTIONS TO APPLICANT: 1. Three (3) Referee Assessments are required. At least two (2) should be from Consultants. Registrars
VICTORIAN PUBLIC HOSPITALS REFEREE ASSESSMENT FORM NEONATAL REGISTRAR POSITIONS INSTRUCTIONS TO APPLICANT: 1. Three (3) Referee Assessments are required. At least two (2) should be from Consultants. Registrars
PARLIAMENT OF VICTORIA. Safe Patient Care (Nurse to Patient and Midwife to Patient Ratios) Bill 2015
 Bill 2015") PARLIAMENT OF VICTORIA Safe Patient Care (Nurse to Patient and Midwife to Patient Ratios) Bill 1 Clause TABLE OF PROVISIONS Page Part 1 Preliminary 1 1 Purposes 1 2 Commencement 2 3 Definitions 2 4 Objective
PARLIAMENT OF VICTORIA Safe Patient Care (Nurse to Patient and Midwife to Patient Ratios) Bill 1 Clause TABLE OF PROVISIONS Page Part 1 Preliminary 1 1 Purposes 1 2 Commencement 2 3 Definitions 2 4 Objective
STREAMLINING FOR GROWTH PROGRAM 2016/17 REGIONAL PACKAGE
 STREAMLINING FOR GROWTH PROGRAM 2016/17 REGIONAL PACKAGE The Victorian Government is supporting strategic planning projects that will stimulate economic growth and boost jobs, infrastructure and housing
STREAMLINING FOR GROWTH PROGRAM 2016/17 REGIONAL PACKAGE The Victorian Government is supporting strategic planning projects that will stimulate economic growth and boost jobs, infrastructure and housing
Paediatric Critical Care and Specialised Surgery in Children Review. Paediatric critical care and ECMO: interim update
 Gateway Reference: 06662 Paediatric Critical Care and Specialised Surgery in Children Review Paediatric critical care and ECMO: interim update June 2017 Contents Executive summary 1. Introduction 2. Context
Gateway Reference: 06662 Paediatric Critical Care and Specialised Surgery in Children Review Paediatric critical care and ECMO: interim update June 2017 Contents Executive summary 1. Introduction 2. Context
Pilot Retrieval Practitioner MedSTAR - Opportunities & Barriers
 Pilot Retrieval Practitioner Journey @ MedSTAR - Opportunities & Barriers Deirdre Clarke Clinical Practice Nursing Director Retrieval Practitioners Retrieval Practitioners MedSTAR > What do we do? > Communication
Pilot Retrieval Practitioner Journey @ MedSTAR - Opportunities & Barriers Deirdre Clarke Clinical Practice Nursing Director Retrieval Practitioners Retrieval Practitioners MedSTAR > What do we do? > Communication
GUIDE TO SUBMITTING STEPOUT PRISON REFERRALS TO COATS
 GUIDE TO SUBMITTING STEPOUT PRISON REFERRALS TO COATS 1. What is the name of the referral form? The StepOut referral form for general prison staff is called COATS Prison Referral StepOut. 2. What is StepOut?
GUIDE TO SUBMITTING STEPOUT PRISON REFERRALS TO COATS 1. What is the name of the referral form? The StepOut referral form for general prison staff is called COATS Prison Referral StepOut. 2. What is StepOut?
We have an experienced and knowledgeable team. Biruu.Health has a deep understanding of this domain
 Towards certainty Decisions are more robust and accurate if they are based on thorough, practical and clearlypresented analysis, supported by data. We transform information and experience into insights
Towards certainty Decisions are more robust and accurate if they are based on thorough, practical and clearlypresented analysis, supported by data. We transform information and experience into insights
2018 Optional Special Interest Groups
 2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
Allied Health Review Background Paper 19 June 2014
 Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
aeromedical transport, critical care, intensive care, mortality, retrieval, transfer.
 bs_bs_banner Emergency Medicine Australasia (2013) 25, 260 267 doi: 10.1111/1742-6723.12075 PREHOSPITAL AND RETRIEVAL MEDICINE Factors involved in intensive care unit mortality following medical retrieval:
bs_bs_banner Emergency Medicine Australasia (2013) 25, 260 267 doi: 10.1111/1742-6723.12075 PREHOSPITAL AND RETRIEVAL MEDICINE Factors involved in intensive care unit mortality following medical retrieval:
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Public sector EBA campaign update #12
 Public sector EBA campaign update #12 29 APRIL 2016 Protected industrial action starts - red, red, red! 1. Status of EBA negotiations Following the negotiations with senior Victorian Government representatives
Public sector EBA campaign update #12 29 APRIL 2016 Protected industrial action starts - red, red, red! 1. Status of EBA negotiations Following the negotiations with senior Victorian Government representatives
MINIMUM STANDARDS FOR INTENSIVE CARE UNITS SEEKING ACCREDITATION FOR TRAINING IN INTENSIVE CARE MEDICINE
 College of Intensive Care Medicine of Australia and New Zealand ABN: 16 134 292 103 Document type: Policy Date established: 1994 Date last reviewed: 2015 MINIMUM STANDARDS FOR INTENSIVE CARE UNITS SEEKING
College of Intensive Care Medicine of Australia and New Zealand ABN: 16 134 292 103 Document type: Policy Date established: 1994 Date last reviewed: 2015 MINIMUM STANDARDS FOR INTENSIVE CARE UNITS SEEKING
RETRIEVAL AND CRITICAL HEALTH INFORMATION SYSTEM
 RETRIEVAL AND CRITICAL HEALTH INFORMATION SYSTEM USER GUIDE May 2017 Contents Introduction... 3 Access to REACH... 3 Homepage... 3 Roles within REACH... 4 Hospital Administrator... 4 Hospital User... 4
RETRIEVAL AND CRITICAL HEALTH INFORMATION SYSTEM USER GUIDE May 2017 Contents Introduction... 3 Access to REACH... 3 Homepage... 3 Roles within REACH... 4 Hospital Administrator... 4 Hospital User... 4
Anaesthesia Registrars
 Studley Road, Heidelberg, 3084 Anaesthesia Registrars - 2017 Name of Unit / Specialty: Head of Unit: CSU / Department: Anaesthesia A/Prof Larry McNicol Anaesthesia Contact person: Dr Shiva Malekzadeh,
Studley Road, Heidelberg, 3084 Anaesthesia Registrars - 2017 Name of Unit / Specialty: Head of Unit: CSU / Department: Anaesthesia A/Prof Larry McNicol Anaesthesia Contact person: Dr Shiva Malekzadeh,
the victorian paediatric emergency transport service pets
 the victorian paediatric emergency transport service pets The Victorian Paediatric Emergency Transport Service The Victorian Paediatric Emergency Transport Service (PETS) is based at the Paediatric Intensive
the victorian paediatric emergency transport service pets The Victorian Paediatric Emergency Transport Service The Victorian Paediatric Emergency Transport Service (PETS) is based at the Paediatric Intensive
RETRIEVAL AND CRITICAL HEALTH INFORMATION SYSTEM
 RETRIEVAL AND CRITICAL HEALTH INFORMATION SYSTEM USER GUIDE November 2014 Contents Introduction... 4 Access to REACH... 4 Homepage... 4 Roles within REACH... 5 Hospital Administrator... 5 Hospital User...
RETRIEVAL AND CRITICAL HEALTH INFORMATION SYSTEM USER GUIDE November 2014 Contents Introduction... 4 Access to REACH... 4 Homepage... 4 Roles within REACH... 5 Hospital Administrator... 5 Hospital User...
Metro South Health Intensive Care Services Strategy
 Metro South Health Intensive Care Services Strategy Draft for Consultation May 2017 Page 1 of 14 Introduction The availability of and access to intensive care services is vital to the health of the community
Metro South Health Intensive Care Services Strategy Draft for Consultation May 2017 Page 1 of 14 Introduction The availability of and access to intensive care services is vital to the health of the community
overview Indicative ATAR ATARs listed in this document are from the 2018 intake and may change for the 2019 intake. Please only use them as a guide.
 overview This document has been developed to assist students and their families in researching undergraduate Nursing, Midwifery and Paramedicine courses at Victorian universities. Students are encouraged
overview This document has been developed to assist students and their families in researching undergraduate Nursing, Midwifery and Paramedicine courses at Victorian universities. Students are encouraged
Board Briefing. Board Briefing of Nursing and Midwifery Staffing Levels. Date of Briefing January 2018 (December 2017 data)
") Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
VICTORIAN AMBULANCE CARDIAC ARREST REGISTRY
 7 VICTORIAN AMBULANCE CARDIAC ARREST REGISTRY [Cover Page] ANNUAL REPORT 2013-2014 VACAR Annual Report 2013-2014 Page 1 VACAR Annual Report 2013-2014 Page 2 Victorian Ambulance Cardiac Arrest Registry
7 VICTORIAN AMBULANCE CARDIAC ARREST REGISTRY [Cover Page] ANNUAL REPORT 2013-2014 VACAR Annual Report 2013-2014 Page 1 VACAR Annual Report 2013-2014 Page 2 Victorian Ambulance Cardiac Arrest Registry
Inpatient, Day case and Outpatient Stage of Treatment Waiting Times
 Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 30 June 2017 Publication date 29 August 2017 A National Statistics Publication for Scotland
Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 30 June 2017 Publication date 29 August 2017 A National Statistics Publication for Scotland
Supplementary Online Content
 Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
Transferring critically ill patients in North West London. Transfer data analysis
 Transferring critically ill patients in North West London Transfer data analysis 2010 11 Picture: A typical intensive care (Level 3) patient with a selection of equipment and monitors that would need to
Transferring critically ill patients in North West London Transfer data analysis 2010 11 Picture: A typical intensive care (Level 3) patient with a selection of equipment and monitors that would need to
ABOUT US. Service system and program development Policy development Financial reviews, business planning and feasibility studies
 C O M P A N Y P R O F I L E ABOUT US. Aspex is a specialist consulting group with a strong focus on health and human services. We tailor solutions to meet the needs and goals of large and smaller organisations.
C O M P A N Y P R O F I L E ABOUT US. Aspex is a specialist consulting group with a strong focus on health and human services. We tailor solutions to meet the needs and goals of large and smaller organisations.
The impact of an ICU liaison nurse service on patient outcomes
 The impact of an ICU liaison nurse service on patient outcomes Suzanne J Eliott, David Ernest, Andrea G Doric, Karen N Page, Linda J Worrall-Carter, Lukman Thalib and Wendy Chaboyer Increasing interest
The impact of an ICU liaison nurse service on patient outcomes Suzanne J Eliott, David Ernest, Andrea G Doric, Karen N Page, Linda J Worrall-Carter, Lukman Thalib and Wendy Chaboyer Increasing interest
STREAMLINING FOR GROWTH PROGRAM 2016/17 FUNDING REPORT
 STREAMLINING FOR GROWTH PROGRAM 2016/17 FUNDING REPORT The Victorian Government is accelerating the delivery of land projects that will stimulate economic growth and boost jobs, infrastructure and housing
STREAMLINING FOR GROWTH PROGRAM 2016/17 FUNDING REPORT The Victorian Government is accelerating the delivery of land projects that will stimulate economic growth and boost jobs, infrastructure and housing
Understanding Monash Health s environment
 Understanding Monash Health s environment Context for developing our 2018-2023 Strategic Plan Working draft September 2017 Introduction Monash Health is a health care, teaching and research institution
Understanding Monash Health s environment Context for developing our 2018-2023 Strategic Plan Working draft September 2017 Introduction Monash Health is a health care, teaching and research institution
Part 3. Condition of medical equipment
 Part 3 Condition of medical equipment 27 INTRODUCTION 3.1 As medical equipment assets have to be replaced or upgraded at some point in time, it is important to identify the life expectancy of each item
Part 3 Condition of medical equipment 27 INTRODUCTION 3.1 As medical equipment assets have to be replaced or upgraded at some point in time, it is important to identify the life expectancy of each item
Redesigning the Acute Coronary Syndrome (NSTE- ACS) pathway at Morriston Cardiac Centre - The case for change
 pathway at Morriston Cardiac Centre - The case for change") Redesigning the Acute Coronary Syndrome (NSTE- ACS) pathway at Morriston Cardiac Centre - The case for change 4 th July 2012 Dr D Smith & Dr S Dorman Introduction... 2 NSTE-ACS Where are we now?... 2 NSTE-ACS
Redesigning the Acute Coronary Syndrome (NSTE- ACS) pathway at Morriston Cardiac Centre - The case for change 4 th July 2012 Dr D Smith & Dr S Dorman Introduction... 2 NSTE-ACS Where are we now?... 2 NSTE-ACS
Hard Truths Public Board 29th September, 2016
 Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Strategic Plan
 Strategic Plan 2016-2020 Our Vision: Supporting a healthy community. Our Mission: The purpose of Benalla Health is to facilitate a healthy and resilient community through the provision of integrated, lifelong
Strategic Plan 2016-2020 Our Vision: Supporting a healthy community. Our Mission: The purpose of Benalla Health is to facilitate a healthy and resilient community through the provision of integrated, lifelong
WAITING TIMES AND ACCESS TARGETS
 NHS Board Meeting Tuesday 17 February 2015 Chief Officer (Acute Services) Board Paper No.15/08 WAITING TIMES AND ACCESS TARGETS Recommendation: The NHS Board is asked to note progress against the national
NHS Board Meeting Tuesday 17 February 2015 Chief Officer (Acute Services) Board Paper No.15/08 WAITING TIMES AND ACCESS TARGETS Recommendation: The NHS Board is asked to note progress against the national
Inpatient, Day case and Outpatient Stage of Treatment Waiting Times
 Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 30 June 2016 Publication date 30 August 2016 A National Statistics Publication for Scotland
Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 30 June 2016 Publication date 30 August 2016 A National Statistics Publication for Scotland
Regional Development Australia Fund and Federal Budget overview. Information for Grants Network Victoria
 Regional Development Australia Fund and 2011-12 Federal Budget overview Information for Grants Network Victoria Winter 2011 This presentation includes: Commitment to Regional Australia RDA Committees and
Regional Development Australia Fund and 2011-12 Federal Budget overview Information for Grants Network Victoria Winter 2011 This presentation includes: Commitment to Regional Australia RDA Committees and
Alfred Health Pharmacy Internships 2019
 Alfred Health Pharmacy Internships 2019 Alfred Health 55 Commercial Road Melbourne VIC 3004 Campuses at which pharmacy intern will work The Alfred, Caulfield Hospital & Sandringham Hospital Hospital Information
Alfred Health Pharmacy Internships 2019 Alfred Health 55 Commercial Road Melbourne VIC 3004 Campuses at which pharmacy intern will work The Alfred, Caulfield Hospital & Sandringham Hospital Hospital Information
Goulburn Valley Health Position Description
 Goulburn Valley Health Position Description Position Title: Operationally reports to: Professionally reports to: Department: Directorate: Cost centre: Code & classification: Performance review: Employment
Goulburn Valley Health Position Description Position Title: Operationally reports to: Professionally reports to: Department: Directorate: Cost centre: Code & classification: Performance review: Employment
Successes and Failures in Telehealth 2017
 How the VST Program works Transitioning from a single-site pilot project to a state-wide regional telehealth service: the experience from the Victorian Stroke Telemedicine program Stroke symptom onset
How the VST Program works Transitioning from a single-site pilot project to a state-wide regional telehealth service: the experience from the Victorian Stroke Telemedicine program Stroke symptom onset
National Cardiac Arrest Audit Report
 National Cardiac Arrest Audit Report St Elsewhere Hospital 1 April 212 to 3 September 212 (n = 122) Date of report: 14/1/213 ncaa@icnarc.org Supported by Resuscitation Council (UK) and Intensive Care National
National Cardiac Arrest Audit Report St Elsewhere Hospital 1 April 212 to 3 September 212 (n = 122) Date of report: 14/1/213 ncaa@icnarc.org Supported by Resuscitation Council (UK) and Intensive Care National
Inpatient, Day case and Outpatient Stage of Treatment Waiting Times
 Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 31 December 2016 Publication date 28 February 2017 A National Statistics Publication
Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 31 December 2016 Publication date 28 February 2017 A National Statistics Publication
THE DETERIORATING PATIENT IN THE SUB-ACUTE SETTING. Australasian Rehabilitation Nurses Association June 26 th 2015
 THE DETERIORATING PATIENT IN THE SUB-ACUTE SETTING Australasian Rehabilitation Nurses Association June 26 th 2015 Conflict of Interest and affiliations No conflicts of interest regarding this topic. Current
THE DETERIORATING PATIENT IN THE SUB-ACUTE SETTING Australasian Rehabilitation Nurses Association June 26 th 2015 Conflict of Interest and affiliations No conflicts of interest regarding this topic. Current
HOME CARE PACKAGES PROGRAM
 HOME CARE PACKAGES PROGRAM Data Report 27 February 30 June 2017 September 2017 Table of Contents Key Messages... 3 Introduction... 4 Home Care Packages Program... 4 Increasing Choice in Home Care... 4
HOME CARE PACKAGES PROGRAM Data Report 27 February 30 June 2017 September 2017 Table of Contents Key Messages... 3 Introduction... 4 Home Care Packages Program... 4 Increasing Choice in Home Care... 4
OPTIONS APPRAISAL PAPER FOR DEVELOPING A SUSTAINABLE AND EFFECTIVE ORTHOPAEDIC SERVICE IN NHS WESTERN ISLES
 Highland NHS Board 9 August 2011 Item 4.3 OPTIONS APPRAISAL PAPER FOR DEVELOPING A SUSTAINABLE AND EFFECTIVE ORTHOPAEDIC SERVICE IN NHS WESTERN ISLES Report by Sheila Cascarino, Divisional Manager, Surgical
Highland NHS Board 9 August 2011 Item 4.3 OPTIONS APPRAISAL PAPER FOR DEVELOPING A SUSTAINABLE AND EFFECTIVE ORTHOPAEDIC SERVICE IN NHS WESTERN ISLES Report by Sheila Cascarino, Divisional Manager, Surgical
MET CALLS IN A METROPOLITAN PRIVATE HOSPITAL: A CROSS SECTIONAL STUDY
 MET CALLS IN A METROPOLITAN PRIVATE HOSPITAL: A CROSS SECTIONAL STUDY Joyce Kant, A/Prof Peter Morley, S. Murphy, R. English, L. Umstad Melbourne Private Hospital, University of Melbourne Background /
MET CALLS IN A METROPOLITAN PRIVATE HOSPITAL: A CROSS SECTIONAL STUDY Joyce Kant, A/Prof Peter Morley, S. Murphy, R. English, L. Umstad Melbourne Private Hospital, University of Melbourne Background /
Clinical Use of Blood The AIM II Trial. Challenges of Near-Live Organisational Blood Use Monitoring
 Clinical Use of Blood The AIM II Trial Challenges of Near-Live Organisational Blood Use Monitoring Goals for AIM Assist hospitals in complying with timely metric driven standards Create an inclusive approach
Clinical Use of Blood The AIM II Trial Challenges of Near-Live Organisational Blood Use Monitoring Goals for AIM Assist hospitals in complying with timely metric driven standards Create an inclusive approach
Improving Care, Delivering Quality Reducing mortality & harm in Welsh Ambulance Services NHS Trust
 National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service E08/S/b Neonatal Intensive Care Transport Commissioner Lead Provider Lead Period Date of Review 12 Months 1. Population
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service E08/S/b Neonatal Intensive Care Transport Commissioner Lead Provider Lead Period Date of Review 12 Months 1. Population
Approved Diploma of Nursing Programs
 Approved Diploma of Nursing Programs Table 1 Approved Diploma of Nursing Programs as at 3 September 2018 Owner: Accreditation 3 September 2018 Australian Nursing and Midwifery Education Centre Diploma
Approved Diploma of Nursing Programs Table 1 Approved Diploma of Nursing Programs as at 3 September 2018 Owner: Accreditation 3 September 2018 Australian Nursing and Midwifery Education Centre Diploma
Anaesthesia Fellow. Position Description. Department : Department of Anaesthesia & Perioperative Medicine
 Job Title : Anaesthesia Fellow Department : Department of Anaesthesia & Perioperative Medicine Location : Waitemata District Health Board Reporting To : Clinical Director Anaesthesia Direct Reports : Anaesthesia
Job Title : Anaesthesia Fellow Department : Department of Anaesthesia & Perioperative Medicine Location : Waitemata District Health Board Reporting To : Clinical Director Anaesthesia Direct Reports : Anaesthesia
Monthly and Quarterly Activity Returns Statistics Consultation
 Monthly and Quarterly Activity Returns Statistics Consultation Monthly and Quarterly Activity Returns Statistics Consultation Version number: 1 First published: 08/02/2018 Prepared by: Classification:
Monthly and Quarterly Activity Returns Statistics Consultation Monthly and Quarterly Activity Returns Statistics Consultation Version number: 1 First published: 08/02/2018 Prepared by: Classification:
Same day emergency care: clinical definition, patient selection and metrics
 Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Phases of staged response to an increased demand for Paediatric Intensive Care in the event of pandemic or other disaster.
 Phases of staged response to an increased demand for Paediatric Intensive Care in the event of pandemic or other disaster. Working document The Critical Care Contingency Plan in the event of an emergency
Phases of staged response to an increased demand for Paediatric Intensive Care in the event of pandemic or other disaster. Working document The Critical Care Contingency Plan in the event of an emergency
Specialist Family Violence Advisor Capacity Building Program Stage 1. Program Framework
 Specialist Family Violence Advisor Capacity Building Program Stage 1 Program Framework Specialist Family Violence Advisor Capacity Building Program Stage 1 Program Framework Contents About the Program
Specialist Family Violence Advisor Capacity Building Program Stage 1 Program Framework Specialist Family Violence Advisor Capacity Building Program Stage 1 Program Framework Contents About the Program
Re: Victorian Pre-budget submission 2017/18 RANZCP Victorian Branch priority budget consideration
 8 August 2016 Dr Margaret Grigg A/g Director, Mental Health Department of Health and Human Services 50 Lonsdale Street MELBOURNE VIC 3000 By email to: margaret.grigg@health.vic.gov.au Dear Dr Grigg Re:
8 August 2016 Dr Margaret Grigg A/g Director, Mental Health Department of Health and Human Services 50 Lonsdale Street MELBOURNE VIC 3000 By email to: margaret.grigg@health.vic.gov.au Dear Dr Grigg Re:
NUTRITION SCREENING SURVEY IN THE UK AND REPUBLIC OF IRELAND IN 2010 A Report by the British Association for Parenteral and Enteral Nutrition (BAPEN)
") NUTRITION SCREENING SURVEY IN THE UK AND REPUBLIC OF IRELAND IN 2010 A Report by the British Association for Parenteral and Enteral Nutrition (BAPEN) HOSPITALS, CARE HOMES AND MENTAL HEALTH UNITS NUTRITION
NUTRITION SCREENING SURVEY IN THE UK AND REPUBLIC OF IRELAND IN 2010 A Report by the British Association for Parenteral and Enteral Nutrition (BAPEN) HOSPITALS, CARE HOMES AND MENTAL HEALTH UNITS NUTRITION
Ambulatory Emergency Care in South Wales
 Ambulatory Emergency Care in South Wales The Ambulatory Care Score ( Amb Score) Les Ala Consultant Acute Physician Royal Glamorgan Hospital LLantrisant, South Wales ROYAL GLAMORGAN HOSPITAL Format Our
Ambulatory Emergency Care in South Wales The Ambulatory Care Score ( Amb Score) Les Ala Consultant Acute Physician Royal Glamorgan Hospital LLantrisant, South Wales ROYAL GLAMORGAN HOSPITAL Format Our
A ANNUAL WORK PLAN DECEMBER
 After Hours DRAFT ONLY 12/04/17 ANNUAL WORK PLAN DECEMBER 2017 Eastern Melbourne PHN 1 3. (b) Planned PHN Activities After Hours Primary Health Care 2017-19 Proposed Activities After Hours Primary Health
After Hours DRAFT ONLY 12/04/17 ANNUAL WORK PLAN DECEMBER 2017 Eastern Melbourne PHN 1 3. (b) Planned PHN Activities After Hours Primary Health Care 2017-19 Proposed Activities After Hours Primary Health
STRATIFICATION GUIDE 2018
 STRATIFICATION GUIDE 2018 The ACHS, in collaboration with relevant medical colleges, associations and specialty societies have developed the following stratification variables to enable like organisations
STRATIFICATION GUIDE 2018 The ACHS, in collaboration with relevant medical colleges, associations and specialty societies have developed the following stratification variables to enable like organisations
Wales Critical Care & Trauma Network (North)
") Wales Critical Care & Trauma Network (North) CRITICAL CARE ADMISSION & DISCHARGE GUIDELINES Revised 2016 1 CONTENTS: 1.0 Introduction 1.1 Scope of the Guideline 1.2 Levels of Care 2.0 Admission Guidance
Wales Critical Care & Trauma Network (North) CRITICAL CARE ADMISSION & DISCHARGE GUIDELINES Revised 2016 1 CONTENTS: 1.0 Introduction 1.1 Scope of the Guideline 1.2 Levels of Care 2.0 Admission Guidance
Countywide Emergency Department Ambulance Patient Transfer of Care Report Performance Report
 Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/28/2017 Patient Transfer
Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/28/2017 Patient Transfer
Australasian Health Facility Guidelines. Part B - Health Facility Briefing and Planning Medical Assessment Unit - Addendum to 0340 IPU
 Australasian Health Facility Guidelines Part B - Health Facility Briefing and Planning 0330 - Medical Assessment Unit - Addendum to 0340 IPU Revision 2.0 01 March 2016 COPYRIGHT AND DISCLAIMER Copyright
Australasian Health Facility Guidelines Part B - Health Facility Briefing and Planning 0330 - Medical Assessment Unit - Addendum to 0340 IPU Revision 2.0 01 March 2016 COPYRIGHT AND DISCLAIMER Copyright
POLICIES AND PROCEDURE MANUAL
 POLICIES AND PROCEDURE MANUAL Policy: MP017 Section: Medical Benefit Policy Subject: Ambulance Transport Service I. Policy: Ambulance Transport Service II. Purpose/Objective: To provide a policy of coverage
POLICIES AND PROCEDURE MANUAL Policy: MP017 Section: Medical Benefit Policy Subject: Ambulance Transport Service I. Policy: Ambulance Transport Service II. Purpose/Objective: To provide a policy of coverage
2018 Graduate Nurse /Midwifery Program (GNMP) Match Business Rules
 Match Business Rules") The Postgraduate Medical Council of Victoria (PMCV) conducts the GNMP Match on behalf of the Department of Health & Human Services. Business rules and guidelines for the 2018 GNMP Match 1. GENERAL RULES
The Postgraduate Medical Council of Victoria (PMCV) conducts the GNMP Match on behalf of the Department of Health & Human Services. Business rules and guidelines for the 2018 GNMP Match 1. GENERAL RULES
Boarding Impact on patients, hospitals and healthcare systems
 Boarding Impact on patients, hospitals and healthcare systems Dan Beckett Consultant Acute Physician NHSFV National Clinical Lead Whole System Patient Flow Project Scottish Government May 2014 Important
Boarding Impact on patients, hospitals and healthcare systems Dan Beckett Consultant Acute Physician NHSFV National Clinical Lead Whole System Patient Flow Project Scottish Government May 2014 Important
Management of surge and escalation in critical care services: standard operating procedure for adult respiratory extra corporeal membrane oxygenation
 Management of surge and escalation in critical care services: standard operating procedure for adult respiratory extra corporeal membrane oxygenation 1 NHS England INFORMATION READER BOX Directorate Medical
Management of surge and escalation in critical care services: standard operating procedure for adult respiratory extra corporeal membrane oxygenation 1 NHS England INFORMATION READER BOX Directorate Medical
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Cause of death in intensive care patients within 2 years of discharge from hospital
 Cause of death in intensive care patients within 2 years of discharge from hospital Peter R Hicks and Diane M Mackle Understanding of intensive care outcomes has moved from focusing on intensive care unit
Cause of death in intensive care patients within 2 years of discharge from hospital Peter R Hicks and Diane M Mackle Understanding of intensive care outcomes has moved from focusing on intensive care unit
Unit length of stay and APACHE II scores for ventilated admissions to critical care in England, Wales and Northern Ireland
 Unit length of stay and APACHE II scores for ventilated admissions to critical care in England, Wales and Northern Ireland Questions What was the unit length of stay and APACHE II scores for ventilated
Unit length of stay and APACHE II scores for ventilated admissions to critical care in England, Wales and Northern Ireland Questions What was the unit length of stay and APACHE II scores for ventilated
Emergency department overcrowding, mortality and the 4-hour rule in Western Australia. Abstract. Methods
 Research Gary C Geelhoed FRACP, FACEM, MD, Director, 1 and Professor, 2 Nicholas H de Klerk BSc, MSc, PhD, Head of Biostatistics and Bioinformatics 3,4 1 Emergency Department, Princess Margaret Hospital
Research Gary C Geelhoed FRACP, FACEM, MD, Director, 1 and Professor, 2 Nicholas H de Klerk BSc, MSc, PhD, Head of Biostatistics and Bioinformatics 3,4 1 Emergency Department, Princess Margaret Hospital
Managing the Morbidly Obese ED Perspective
 Managing the Morbidly Obese ED Perspective Dr Stuart Young Director of Emergency Medicine, Logan Hospital Currently on secondment to Retrieval Services Queensland Acknowlegements: Justine Powell NUM, RFDS
Managing the Morbidly Obese ED Perspective Dr Stuart Young Director of Emergency Medicine, Logan Hospital Currently on secondment to Retrieval Services Queensland Acknowlegements: Justine Powell NUM, RFDS
Evaluation of NHS111 pilot sites. Second Interim Report
 Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
Palliative Care/Palliative Medicine Registrar
 Monash Doctors Workforce Monash Medical Centre 246 Clayton Road Clayton Victoria 3168 Australia Palliative Care/Palliative Medicine Registrar Role Information: Postal address: Locked Bag 29 Clayton South
Monash Doctors Workforce Monash Medical Centre 246 Clayton Road Clayton Victoria 3168 Australia Palliative Care/Palliative Medicine Registrar Role Information: Postal address: Locked Bag 29 Clayton South
Advanced practice in emergency care: the paediatric flow nurse
 Advanced practice in emergency care: the paediatric flow nurse Development and implementation of a new liaison role in paediatric services in Australia has improved services for children and young people
Advanced practice in emergency care: the paediatric flow nurse Development and implementation of a new liaison role in paediatric services in Australia has improved services for children and young people
Pricing and funding for safety and quality: the Australian approach
 Pricing and funding for safety and quality: the Australian approach Sarah Neville, Ph.D. Executive Director, Data Analytics Sean Heng Senior Technical Advisor, AR-DRG Development Independent Hospital Pricing
Pricing and funding for safety and quality: the Australian approach Sarah Neville, Ph.D. Executive Director, Data Analytics Sean Heng Senior Technical Advisor, AR-DRG Development Independent Hospital Pricing
Consumer engagement plan. Engaging with our consumers
 Consumer engagement plan 2017 Engaging with our consumers Contents 02 Message from the Chair of the Community Advisory Committee and Chief Executive 04 About Us 05 Our Facilities 06 Our Community 07 Our
Consumer engagement plan 2017 Engaging with our consumers Contents 02 Message from the Chair of the Community Advisory Committee and Chief Executive 04 About Us 05 Our Facilities 06 Our Community 07 Our
STREAMLINING FOR GROWTH PROGRAM 2016/17 FUNDING REPORT
 STREAMLINING FOR GROWTH PROGRAM 2016/17 FUNDING REPORT The Victorian Government is accelerating the delivery of land projects that will stimulate economic growth and boost jobs, infrastructure and housing
STREAMLINING FOR GROWTH PROGRAM 2016/17 FUNDING REPORT The Victorian Government is accelerating the delivery of land projects that will stimulate economic growth and boost jobs, infrastructure and housing
St. James s Hospital, Dublin.
 Position Fellowship in Anaesthesia for Advanced Airway Management Assignment Department of Anaesthesia, St. James s Hospital. Commencement Date Monday, 09 th July, 2018. Purpose of the Post The St. James
Position Fellowship in Anaesthesia for Advanced Airway Management Assignment Department of Anaesthesia, St. James s Hospital. Commencement Date Monday, 09 th July, 2018. Purpose of the Post The St. James
April Clinical Governance Corporate Report Narrative
 April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
Hub Team Leader. Dependent upon qualifications and experience, plus superannuation and the ability to salary package up to $15,899 tax free (pro-rata)
") Hub Team Leader The Hub Team Leader will lead a team of Hub Practitioners working within the integrated Hub team who are responsible for the delivery of high quality, safe and effective responses to Victorians
Hub Team Leader The Hub Team Leader will lead a team of Hub Practitioners working within the integrated Hub team who are responsible for the delivery of high quality, safe and effective responses to Victorians
Service Mapping Report
 Service Mapping Report Background and purpose One of the roles of the Southern Melbourne Integrated Cancer Service (SMICS) is to map cancer services provided to adults by Alfred Health, Cabrini Health,
Service Mapping Report Background and purpose One of the roles of the Southern Melbourne Integrated Cancer Service (SMICS) is to map cancer services provided to adults by Alfred Health, Cabrini Health,
NHS Electronic Referrals Service. Paper Switch Off an update Digital Health Webinar 4 May 2018
 NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
Position Description Western Victoria Primary Health Network
 Position Description Western Victoria Primary Health Network POSITION TITLE: Primary Care Consultant (Population Health Planning) DIVISION: REPORTS TO: Regional Manager - Geelong DIRECT REPORTS: Nil LOCATION:
Position Description Western Victoria Primary Health Network POSITION TITLE: Primary Care Consultant (Population Health Planning) DIVISION: REPORTS TO: Regional Manager - Geelong DIRECT REPORTS: Nil LOCATION:
Approved Diploma of Nursing Programs
 Approved Diploma of Nursing Programs Owner: Accreditation 17 April 2018 Table 1 Approved Diploma of Nursing Programs as at 17 April 2018 Australian Nursing and Midwifery Education Centre Diploma of Nursing
Approved Diploma of Nursing Programs Owner: Accreditation 17 April 2018 Table 1 Approved Diploma of Nursing Programs as at 17 April 2018 Australian Nursing and Midwifery Education Centre Diploma of Nursing
NHS Emergency Planning Guidance
 NHS Emergency Planning Guidance Planning for the development and deployment of Medical Emergency Response Incident Teams in the provision of advanced medical care at the scene of an incident NHS Emergency
NHS Emergency Planning Guidance Planning for the development and deployment of Medical Emergency Response Incident Teams in the provision of advanced medical care at the scene of an incident NHS Emergency
M D S. Report Medical Practice in rural & remote Australia: National Minimum Data Set (MDS) Report as at 30th November 2006
 Report as at 30th November 2006") M D S Report 2006 Medical Practice in rural & remote Australia: National Minimum Data Set (MDS) Report as at 30th November 2006 Health Workforce Queensland and New South Wales Rural Doctors Network 2008
M D S Report 2006 Medical Practice in rural & remote Australia: National Minimum Data Set (MDS) Report as at 30th November 2006 Health Workforce Queensland and New South Wales Rural Doctors Network 2008
Newborn bloodspot screening
 Policy HUMAN GENETICS SOCIETY OF AUSTRALASIA ARBN. 076 130 937 (Incorporated Under the Associations Incorporation Act) The liability of members is limited RACP, 145 Macquarie Street, Sydney NSW 2000, Australia
Policy HUMAN GENETICS SOCIETY OF AUSTRALASIA ARBN. 076 130 937 (Incorporated Under the Associations Incorporation Act) The liability of members is limited RACP, 145 Macquarie Street, Sydney NSW 2000, Australia
Requesting Ambulance Transport (999 or Urgent) A Guide for Healthcare Professionals
 A Guide for Healthcare Professionals") Requesting Ambulance Transport (999 or Urgent) A Guide for Healthcare Professionals Contents Page No. Introduction... 3 Glossary of terms... 4 Which patients should have 999 or urgent ambulance transport
Requesting Ambulance Transport (999 or Urgent) A Guide for Healthcare Professionals Contents Page No. Introduction... 3 Glossary of terms... 4 Which patients should have 999 or urgent ambulance transport
Strengthening Men s Sheds Program. Guidelines for applying for grants to refurbish existing Men s Sheds
 Strengthening Men s Sheds Program Guidelines for applying for grants to refurbish existing Men s Sheds March 2014 Minister s foreword Strengthening Men s Sheds Program The Victorian Government recognises
Strengthening Men s Sheds Program Guidelines for applying for grants to refurbish existing Men s Sheds March 2014 Minister s foreword Strengthening Men s Sheds Program The Victorian Government recognises