Medicare Shared Savings Program ACO Learning System
|
|
|
- Ferdinand McDowell
- 5 years ago
- Views:
Transcription



1 Medicare Shared Savings Program ACO Learning System Leveraging Community Resources and Addressing Beneficiaries Social Needs Wednesday, September 14, :30 4:00 PM ET Audio for this session can be streamed through your computer, or accessed by phone by dialing ; access code:
2 Disclaimer The comments made on this call are offered only for general informational and educational purposes. As always, the agency s positions on matters may be subject to change. CMS s comments are not offered as and do not constitute legal advice or legal opinions, and no statement made on this call will preclude the agency and/or its law enforcement partners from enforcing any and all applicable laws, rules and regulations. ACOs are responsible for ensuring that their actions fully comply with applicable laws, rules and regulations, and we encourage you to consult with your own legal counsel to ensure such compliance. Furthermore, to the extent that we may seek to gather facts and information from you during this call, we intend to gather your individual input. CMS is not seeking group advice.
3 Past Webinar Materials Interested in past Learning System events? Go to to access recordings and summaries of past webinars, including: Advancing Primary Care 11/14/14 Beneficiary Engagement 10/22/14 Beneficiary Engagement and Annual Wellness Visits 8/19/15 Care Coordinator Roundtable Session 1 9/30/15 Care Coordinator Roundtable Session 2 10/14/15 Coordinating Care for Beneficiaries with Complex Care Needs 6/24/15 Coordinating with Hospitals and Specialists 12/15/14 Coordinating with Post-Acute Care Providers 11/21/14, 11/19/15 Engaging Office Managers in ACOs 12/10/15 Engaging Pharmacists in Accountable Care 7/19/16 3
4 Past Webinar Materials (cont.) Evidence-Based Medicine 1/7/14, 1/24/14 Internal Cost and Quality Reporting 4/17/14, 5/22/14 Lessons from GPRO Reporting 1/17/14, 10/28/14, 10/28/15 Lessons Learned from the Million Hearts Initiative 7/29/15 Provider Engagement 9/9/14, 10/1/14 Strategies of SSP ACOs Achieving Interim Savings 4/4/14, 4/11/14, 5/2/14, 5/16/14 Strategies of SSP ACOs Achieving Shared Savings 4/15/15, 4/29/15, 5/12/15, 5/19/15, 1/7/16 Using Data to Drive Performance 6/8/15, 5/19/16 In the ACO portal, materials for these and other webinars are located in the Events Calendar, and Program Announcements section, under Learning System Webinar Materials 4
5 Webinar Agenda Housekeeping items Welcome from CMS Presentations: Broward Guardian Mission Health Partners Chautauqua Region Associated Medical Partners Questions and answers Wrap-up 5
6 The widget menu located at the bottom of the event console contains various resources for the webcast. You can resize a widget by clicking on the maximize icon on the top right of the widget or dragging the bottom right corner of the widget panel. Q&A: Pose questions to the presenters or submit technical questions. Help: Access technical information about the webinar platform and test your system. Resource List: Download documents related to this webcast. Closed Captioning: Access the live closed captioning feed for the webcast. Survey: Submit feedback about the webcast via the post-event survey. For audio: Listen via your device s speakers, or join the teleconference at (toll number); Access Code:
7 Welcome from CMS Featured topic Upcoming events Polling questions Thank you! 7

8 Broward Guardian John Harkins Executive Director 8
9 A Holistic Approach to Improving Beneficiary Health Medicare Shared Savings Program ACO Learning System

10 ACO Background Start Date: January 2014 Track 1 Model No Advance Payment Memorial Healthcare System (MHS) is Participating Provider 75 Participating Providers 9,000 Attributed Beneficiaries 95% EHR Penetration with 15 different platforms (most common EHR is eclinicalworks promoted by MHS)

11 Broward Guardian Culture Collaboration between Memorial Healthcare System (MHS) and Community based Primary Care Physicians. MHS is the 4 th largest public health system in the country and the only hospital provider in the market Located in Southern Broward County, boarding Miami- Dade County. Geographically small, but diverse population mix Extremely high benchmark MA (Medicare Advantage) Risk penetration is high (preferred method of contracting for providers and payers)
12 Focusing on the Three-Part Aim (Quality/Access/Costs) Strategy Driven by Limited Access to Capital Reality: Generate Savings or Close up Shop Focus on Short Term Savings Strategies Cost verses Benefit Short Term verses Long Term Physicians understand the relationship between Quality and Savings More Primary Care Utilization Avoid Unnecessary/Avoidable Utilization
13 Overall Performance 2014* Attributed Lives: 5,800 Benchmark: $17,038*** 2015 Actual Performance: $16,619*** ($16,436 before adjustment) Attributed Lives: 9,788** Benchmark: $15,540*** Actual Performance: $14,402*** Savings per Beneficiary: $1,138 ($11 million) *Because of delays, the Broward Guardian Care Coordination program did not begin until October 1, **We added 25 participating providers in ***Benchmark and Actual Performance numbers are presented as per beneficiary numbers.
14 Broward Guardian Care Coordination Model Engage High-Risk Patients High Cost and High Risk Develop Individual Care Plans Beneficiary/Caregiver/Provider Include Personal Goals Frequent Interaction and Contact Right service, Right Time, Right Place Reduce Avoidable Readmissions Reduce Unnecessary ED Utilization Eyes and Ears of the PCP
15 The Care Team Director of Nursing(1) Clinician and Manager Inpatient Care Coordinators(2) (Navigators) Visit every patient that present at the 2 main Memorial Hospitals. Critical Strength is ability to effectively communicate Care Coordinators(3) LPNs or MAs 1 Coordinator to Every 150 Active High-Risk Beneficiaries Telephonic Follow-Ups on ALL Hospital Patients Telephonic Chronic Case Management (CCM Program) Ongoing Coordination for Long-Term High-Risk Beneficiaries Assessments and Care Plan Development
16 What is a High-Risk patient? High-Cost Multiple Admissions/Readmissions Multiple Co-Morbidities Poly-Pharmacy High ED Utilization Low Encounters Demographics (age, socio-economics) WHAT ABOUT THE NON-CLINICAL FACTORS?
 Home and Community Based Services Caregiver Engagement")
17 Borrowing from the Managed Care Community Chronic SNP(Special Needs Plans) Management Comprehensive Assessment Risk Stratification Individualized Care Plans Manage/Evaluate/Reassess Managed Long Term Care (MLTC) Home and Community Based Services Caregiver Engagement Holistic Approach
18 Traditional Data-Driven Risk Models Generate Quarterly Reports Identifying High-Risk Beneficiaries and Distribute to Each Practice High, Medium and Low Risk differentiated by Red, Yellow and Green Based Only on Claims Data No Subjective Input Individual DOB Gender # of Admissions # of Re-admissions* # of ER Visits # of Office Visits Highest Paid Diagnosis Total Paid Risk Score Please schedule an appointment with the following Medicare beneficiaries immediately and every month thereafter DOE, JOHN 01/01/1900 M Retinal Disorders $ 73, DOE, JOHN 01/01/1900 F Colorectal Cancer $ 34, DOE, JOHN 01/01/1900 F Cataract $ 10, Please schedule an appointment with the following Medicare beneficiaries as soon as possible and every 3 months thereafter DOE, JOHN 01/01/1901 F Rheumatoid Arthritis $ 59, DOE, JOHN 01/01/1901 M Osteoarthritis $ 55, DOE, JOHN 01/01/1901 M Multiple Myeloma $ 26, Please schedule an appointment with the following Medicare beneficiaries every 6 months DOE, JOHN 01/01/1901 F Hernias $ 20, DOE, JOHN 01/01/1901 F Osteoarthritis $ 25, DOE, JOHN 01/01/1901 F Gall Bladder Diseases $ 10, DOE, JOHN 01/01/1901 F Misc Cancers $ 8, DOE, JOHN 01/01/1901 F Musculoskeletal Disorders $ 13,

19 Comprehensive Assessment Looking Beyond the Clinical Florida 701B Assessment Tool Medicaid Qualification Managed Long-Term Care Holistic Approach Mental Health/Behavioral/Cognition Nutrition Health Conditions Specialized Services Medications Caregiver Information


20 The Hidden Risk A Real Life Example Patient Smith age 70 Diabetic/CHF (non-compliant) Patient Constantly Rescheduling Visits Does not get lab work when ordered Inconsistent Medication administration No glucose records Reports poor eating decisions The REAL Risk Factors Patient is primary caregiver for disabled spouse No extended family Struggles to put food on the table No air conditioning Only available transportation is neighbor

21 Empower the Coordinators to Think Outside of the Box!!! Success in any Disease Management or Care Management model is dependent on Patient Engagement and Self-Management. What can we do to help enable the patient to be more engaged?
 and the Aging and Disability Resource")

22 Community Partnership Area Agency on Aging (AAA) and the Aging and Disability Resource Center (ADRC) Provide and Coordinate Services Free to the Beneficiary Free to the ACO Added Resource
23 Integrating and Coordinating Comprehensive Care Plan Clinical Interventions Non-Clinical Interventions Direct Referrals to Community Agencies Assistance with locating, qualifying, applying for services Meals on Wheels Transportation Social Programs Self-Management Training Programs Diabetes Self-Management Chronic Disease Self-Management Falls Prevention Program More Eyes On The Beneficiary
24 Key Areas of Focus - Summary Reducing Unnecessary and Avoidable Hospital Utilization Reduce ER/ED Utilization Reduce Readmission Rate (24%) Promote Primary Care Utilization Identify Gaps in Care Facilitate the Flow of Information Remove Barriers Identify Risk Factors Develop Comprehensive Care Plan Utilize Community Resources Become a Beneficiary Advocate
25 Contact Information John Harkins Executive Director Broward Guardian (954) Thank You!
26 Questions & Answers Please submit questions through the Q&A panel/widget 26

27 Mission Health Partners Robert Fields Medical Director 27


28 It Takes a Village: Community Resource Use by a Medicare Shared Savings Program ACO Community Resources in the MSSP I 28 Rob Fields, MD Medical Director Mission Health Partners Asheville, NC
29 Mission Health Partners Track and Start date: Track 1, 2015 State(s): North Carolina Advance Payment or ACO Investment Model? No Are any of the ACO participants hospitals? Yes Number of practitioners: 1,100 Number of assigned beneficiaries: 47,000 MSSP; 75,000 total 100% EHR penetration; 15 platforms within primary care alone Community Resources in the MSSP I 29
30 ACO Formation, Culture and Background Our formation was a collaboration between independent primary care physicians and our largest hospital system, Mission Health Provider-led with a majority of our Board seats held by independent physicians Semi-Urban Total population 800,000 in 18-county service area Total population 250,000 in Buncombe County (largest) Community Resources in the MSSP I 30
31 Formation and Collaboration Community interest in partnership with Mission Health Mission recognized the need for partnership outside of ownership Shared perspective and mutual respect within our governance structure Community Resources in the MSSP I 31
32 Care Coordination The foundation of population health Typically condition focused MHP motivated by an upstream approach Pathways Community HUB approach as the foundational model * * More information on the HUB model can be found in the AHRQ manual: Community Resources in the MSSP I 32


33 Community Resources in the MSSP I 33
34 Pathways & ACO Care Management Accountability model Begins with an assessment of needs during intake process Marry a social determinant need with a community agency that does the work E.g. Legal aid organizations Community Resources in the MSSP I 34
35 Pathways & ACO Care Management Agencies assigned one or more social determinant pathway(s) Tool tracks completion of those pathways Collected data could lead to development of advocacy efforts e.g. transportation, housing, nutrition, med access Community Resources in the MSSP I 35
36 Community Partner Motivation Interest in ACO/health system alignment Data collection??shared savings?? Community Resources in the MSSP I 36
37 Barriers to Success Buy in using the tool Appropriate agreements need to be in place to allow access Long-term incentives for community partners Community Resources in the MSSP I 37
38 Contact Information Robert W. Fields, MD Medical Director, Mission Health Partners (828) Community Resources in the MSSP I 38
39 Questions & Answers Please submit questions through the Q&A panel/widget 39

40 Chautauqua Region Associated Medical Partners Ann Morse Abdella Executive Director 40
41 Chautauqua Region Associated Medical Partners (AMP) ACO Learning System: Leveraging Community Resources and Addressing Beneficiaries Social Needs Wednesday, September 14, 2016
42 AMP Profile MSSP participation only, July 2012 cohort; renewed contract , Track 1 Rural upstate New York 6,600 beneficiaries Physician-Hospital Partnership 11 Independent PCPs (5 different EHRs) 4 Independent Hospital Organizations (3 different EHRs) 2 Independent SNF Organizations 3 facilities (2 different EHRs) No advance payment Shared Savings in 2014; saved 6.4%, 92% quality score
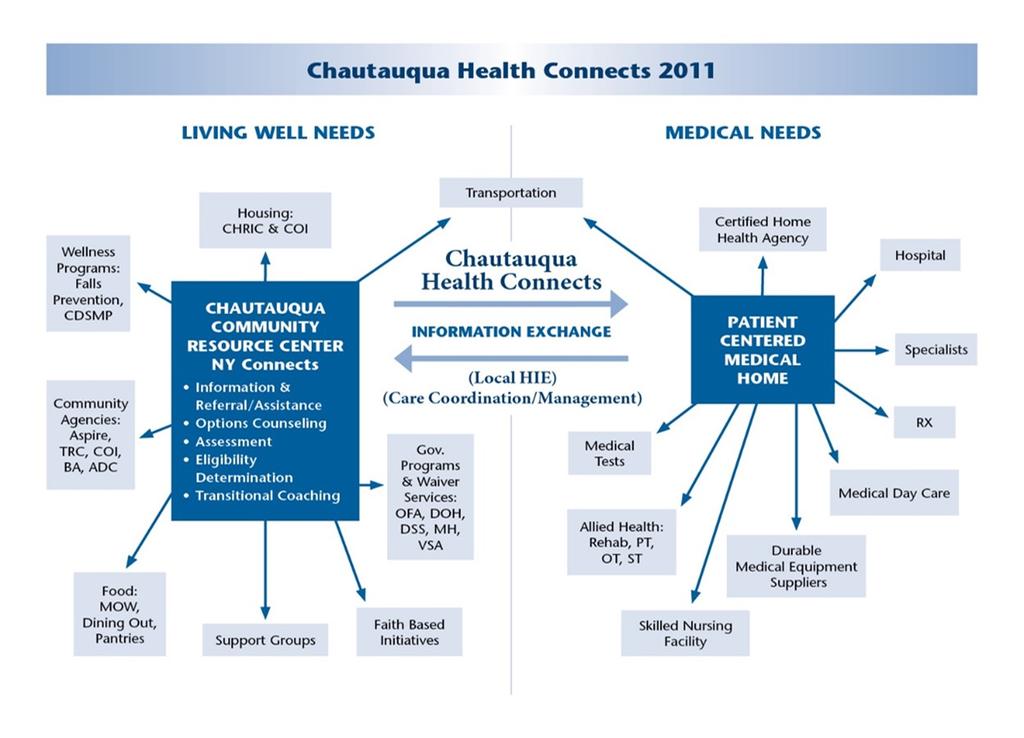
43 Conventional Wisdom Differing Approaches to Integration Chautauqua Health Connects
44 Our Plan Build Patient Centered Medical Homes and Centralize the Medical Neighborhood (Community) to Support Them Focus: Medicare Beneficiaries

45 Strengthening the local Health Care and Wellness Delivery System Our Strategies: Clinical Integration and Collective Impact Systemness and Relationships
46 Accountable Care Communities Coordinate health care inside AND outside the doctor s office Improve care and promote healthier choices in people s daily lives Policy ~ System ~ Environment
47 Some Things We Think We Are Doing Right Accountable Care Communities taking Geographic and Public Health Approach to design and delivery Patient Centered Medical Home and Neighborhood Continuum of Care and Community Collaborations Performance Targets and Plans: Citizenship + Quality Data Driven-reporting, structured data, and transparency Social Determinants of Health Collective Impact Framework Alignment with Other Public Health Initiatives Patient Engagement Building Care Management Capacity


48
49 Roles for NY Connects (ADRC) in an ACO Community Care Coordination: Access point for community supports & services (all ages) Ensure two-way communication with medical providers Support seamless care transitions at discharge Partner with Physicians and CBOs in new, collaborative ways, i.e. Community Services Plans (ACA) and Million Lives Initiative Non-medical services become part of the medical care plan Support for PCMH Retooling of care management to include community care & behavioral health Deploy Chronic Disease Self-Management Education & other EBI Support Advance Care Planning and Palliative Care
50 Projects We are Working on Together Increasing data sharing among participants Reducing readmissions Building Care Management Consumer Engagement Self-Management Aging in Place Area Agency on Aging (AAA) gradually integrating as part of the PCMH care team Long Term Care Council Advises
51 AAA Key Partner Area Agency on Aging Addressing Social Determinants of Health Care Transitions beyond CMMI Training & Adoption of best practices (falls, LTSS) Health Care Proxy Registry Collaboration on Complex Clients in Crisis Feedback on Community Referrals PCP staff involved in EBI
52 Secure Referrals In-service staff and make referrals part of their performance measures EHR Referral templates built EHR turns referral into a fax AAA fax number built-in Fax goes to AAA secure mail box AAA Acknowledges receipt 2 month follow-up report Fall screens faxed to PCP
53 AAA Menu of Services Referrals to EBI Stepping On Home falls assessment Tai Chi Powerful Tools for Caregivers CDSMP Community based LTSS Health Insurance Counseling Medicare & Medicaid Health Care Proxy Registry Examples of other nonmedical services that impact care: Meals on Wheels OFA Home Care Services Transportation Adult Day Care
54 Sharing Info with PCPs LTSS (frequency & provider) Meals PCA I or II PERs Dietician consults Home repairs/access Health & wellness classes Fall prevention (TUG scores) Exercise CDSME ADLs & IADLs Deficits only Caregiver Information Clean Medication List

55 Sample Clinical Measures Experience Measure Fall Screening Medication Reconciliation All Cause Readmissions Source: CMS MSSP Performance Reports
56 Financial Support Leverage existing county services AMP subscribes for secure messaging and referral service; Direct may replace DUA and BAA with OFA; approved by CMS AMP subcontracts for CTI coaching AMP sister rural health network assists with staff education and training
57 AAA ADRC expansion under Medicaid (1115 waiver) NY Statewide PeerPlace Direct communication capability is increasing Import/Export automatic reports from service data to healthcare EHRs not set up to capture Caregiver info Exploring a pilot to expand LTSS to a wider group of beneficiaries NYS Alzheimer s Caregivers Initiative Future In the Works Just launched partnership with Hospice and Palliative Care Building connections between PCMH and Behavioral Health Homes Building Community Health Teams with hospitals Just beginning discussions with County Health Department
58 Acronyms Used EHR: Electronic Health Record ADRC: Aging and Disabilities Resource Center AAA: Area Agency on Aging is the same as Office for the Aging EBI: Evidenced based intervention LTSS: long term services and supports ADL: Activities of Daily Living IADL: instrumental Activities of Daily Living TUG: timed up and go test. A measure used to assess falls risk PCA I: Personal care level one PCA II: Personal Care level two PERs: Personal Emergency Reporting System CDSMP and CDSME: Chronic disease self-management program or education CTI: Care Transition Intervention Program
59 Contact Ann Morse Abdella Executive Director AMP (716) x1202 Special thanks to: Mary Ann Spanos Director Chautauqua County Office for the Aging (716)
60 Questions & Answers Please submit questions through the Q&A panel/widget 60

61 Please give us your feedback! Open the survey widget located in the widget menu at the bottom of your event console. Don t forget to press the submit button when finished! 61
62 Thank you! Slides and a link to the webinar recording will be posted to the ACO portlet. A recording will also be available tomorrow from the audience link that you used to attend. Please complete the webinar evaluation. Fee free to send questions, comments, and suggestions for future topics to ACOLearningActivities@mathematica-mpr.com 62
Medicare Shared Savings Program ACO Learning System
 Medicare Shared Savings Program ACO Learning System Coordinating Care for Beneficiaries with Complex Care Needs Wednesday, June 24, 2015 2:30 4:00 PM ET Audio for this session can be streamed through your
Medicare Shared Savings Program ACO Learning System Coordinating Care for Beneficiaries with Complex Care Needs Wednesday, June 24, 2015 2:30 4:00 PM ET Audio for this session can be streamed through your
Planning a Course to Population Health Management
 Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community. Stewards of Change June 11, 2013
 An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM. November 20, 2015
 THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
Chronic Care Management
 Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
SWAN Alerts and Best Practices for Improved Care Coordination
 SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
Monarch HealthCare, a Medical Group, Inc.
 Monarch HealthCare, a Medical Group, Inc. Accountable Care in the Independent Practice Model June 7, 2010 Jay J. Cohen, MD, MBA President/Chairman Monarch HealthCare Monarch HealthCare, a Medical Group,
Monarch HealthCare, a Medical Group, Inc. Accountable Care in the Independent Practice Model June 7, 2010 Jay J. Cohen, MD, MBA President/Chairman Monarch HealthCare Monarch HealthCare, a Medical Group,
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Pharmacists Improve Care Through Team Collaboration
 Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
State Leadership for Health Care Reform
 State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
What Have we Learned from the Pioneer ACO Model?
 What Have we Learned from the Pioneer ACO Model? Sherly Binu, CMMI December 7, 2016 Disclaimers 2 This presentation was prepared as a tool to assist providers and is not intended to grant rights or impose
What Have we Learned from the Pioneer ACO Model? Sherly Binu, CMMI December 7, 2016 Disclaimers 2 This presentation was prepared as a tool to assist providers and is not intended to grant rights or impose
Care Integration and Network Models: How to Become a Player
 Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States
: Reform Strategies for States") Advancing innovations in health care delivery for low-income Americans Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States March 6, 2018 Michelle Herman Soper and Alexandra
Advancing innovations in health care delivery for low-income Americans Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States March 6, 2018 Michelle Herman Soper and Alexandra
Webinar Instructions. A nonprofit service and advocacy organization National Council on Aging
 Webinar Instructions 1 Health Care and Community-Based Organizations: A Win-Win Partnership Sue Lachenmayr, MPH, CHES Program Director Center for Healthy Aging National Council on Aging Pam Piering Consultant,
Webinar Instructions 1 Health Care and Community-Based Organizations: A Win-Win Partnership Sue Lachenmayr, MPH, CHES Program Director Center for Healthy Aging National Council on Aging Pam Piering Consultant,
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Denise Hudson, NR-CMA Health Informatics Specialist Health Services Advisory Group (HSAG) April 13, 2018
 April 13, 2018") Learning Forum Fridays Countdown to MIPS* Data Submission Webinar Series Spring Into Action Using Your First Quarter Data Denise Hudson, NR-CMA Health Informatics Specialist Health Services Advisory Group
Learning Forum Fridays Countdown to MIPS* Data Submission Webinar Series Spring Into Action Using Your First Quarter Data Denise Hudson, NR-CMA Health Informatics Specialist Health Services Advisory Group
Accountable Care and Governance Challenges Under the Affordable Care Act
 Accountable Care and Governance Challenges Under the Affordable Care Act The First National Congress on Healthcare Clinical Innovations, Quality Improvement and Cost Containment October 26, 2011 Doug Hastings
Accountable Care and Governance Challenges Under the Affordable Care Act The First National Congress on Healthcare Clinical Innovations, Quality Improvement and Cost Containment October 26, 2011 Doug Hastings
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare
 Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Partnering with Public Health Departments in Managed Care. THIS AREA CAN BE LEFT BLANK or ADD A PICTURE
 Partnering with Public Health Departments in Managed Care THIS AREA CAN BE LEFT BLANK or ADD A PICTURE 2/3/2017 The Value of Medicaid Managed Care States Have Seen the Value of Medicaid Managed Care 75
Partnering with Public Health Departments in Managed Care THIS AREA CAN BE LEFT BLANK or ADD A PICTURE 2/3/2017 The Value of Medicaid Managed Care States Have Seen the Value of Medicaid Managed Care 75
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Primary Care Transformation in the Era of Value
 Primary Care Transformation in the Era of Value CMS Innovation Center & Primary Care Bruce Finke, MD Janel Jin, MSPH Gabrielle Schechter, MPH Center for Medicare & Medicaid Innovation Centers for Medicare
Primary Care Transformation in the Era of Value CMS Innovation Center & Primary Care Bruce Finke, MD Janel Jin, MSPH Gabrielle Schechter, MPH Center for Medicare & Medicaid Innovation Centers for Medicare
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Findings from ACL s Process Evaluation of the Chronic Disease Self-Management Program (CDSMP)
") Findings from ACL s Process Evaluation of the Chronic Disease Self-Management Program (CDSMP) Introduction Susan Jenkins, PhD Social Science Analyst with the Administration for Community Living Who is
Findings from ACL s Process Evaluation of the Chronic Disease Self-Management Program (CDSMP) Introduction Susan Jenkins, PhD Social Science Analyst with the Administration for Community Living Who is
Denise Hudson, NR-CMA Health Informatics Specialist Health Services Advisory Group (HSAG) August 10, 2018
 August 10, 2018") Countdown to MIPS* Data Submission Webinar Series Preparing for Fall Without Falling Behind Denise Hudson, NR-CMA Health Informatics Specialist Health Services Advisory Group (HSAG) August 10, 2018 *Merit-based
Countdown to MIPS* Data Submission Webinar Series Preparing for Fall Without Falling Behind Denise Hudson, NR-CMA Health Informatics Specialist Health Services Advisory Group (HSAG) August 10, 2018 *Merit-based
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Implementing the Affordable Care Act:
 Implementing the Affordable Care Act: Making it Easier For Individuals to Navigate Their Health and Long Term Care 26 th National Home and Community Based Services Conference Tuesday, September 28, 2010
Implementing the Affordable Care Act: Making it Easier For Individuals to Navigate Their Health and Long Term Care 26 th National Home and Community Based Services Conference Tuesday, September 28, 2010
Ministry of Health Patients as Partners Provincial Dialogue Report
 Ministry of Health Patients as Partners 2017 Provincial Dialogue Report Contents Executive Summary 4 Introduction 6 Balanced Participation: Demographics and Representation at the Dialogue 8 Engagement
Ministry of Health Patients as Partners 2017 Provincial Dialogue Report Contents Executive Summary 4 Introduction 6 Balanced Participation: Demographics and Representation at the Dialogue 8 Engagement
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Engaging Providers in Integrated Care Programs
 Engaging Providers in Integrated Care Programs November 6, 2014 4:00 PM Eastern The Integrated Care Resource Center, an initiative of the Centers for Medicare & Medicaid Services Medicare-Medicaid Coordination
Engaging Providers in Integrated Care Programs November 6, 2014 4:00 PM Eastern The Integrated Care Resource Center, an initiative of the Centers for Medicare & Medicaid Services Medicare-Medicaid Coordination
Why Are We Doing This?
 ALIGNING PAYMENT WITH PATIENT-CENTERED CARE AND VALUE-BASED PAY Craig Hostetler MPCA Annual Conference August 5 th, 2013 Why Are We Doing This? Why Take the Risk? Our stakeholders wanted something better
ALIGNING PAYMENT WITH PATIENT-CENTERED CARE AND VALUE-BASED PAY Craig Hostetler MPCA Annual Conference August 5 th, 2013 Why Are We Doing This? Why Take the Risk? Our stakeholders wanted something better
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow
 One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement. Craig J. Wilson
 Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Explaining the Value to Payers
 Explaining the Value to Payers Explaining the Value to Payers This document has been created to provide talking points for EMS agencies to explain to payers the value of EMS 3.0 services. Please review
Explaining the Value to Payers Explaining the Value to Payers This document has been created to provide talking points for EMS agencies to explain to payers the value of EMS 3.0 services. Please review
Lessons from the States: Oregon s APM Model
 Lessons from the States: Oregon s APM Model F R I D AY, N O V E M B E R 6, 2 0 1 5 2 : 0 0 P M E T C R A I G H O S T E T L E R, E X E C U T I V E D I R E C T O R, O P C A K E R S T E N B U R N S L A U
Lessons from the States: Oregon s APM Model F R I D AY, N O V E M B E R 6, 2 0 1 5 2 : 0 0 P M E T C R A I G H O S T E T L E R, E X E C U T I V E D I R E C T O R, O P C A K E R S T E N B U R N S L A U
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
Best Practices in Care Coordination & Transitions of Care Communications
 Best Practices in Care Coordination & Transitions of Care Communications Jessica Carpenter, MS, RD, LDN Director, Disability and Community Services University of Massachusetts Medical School Overview/Agenda
Best Practices in Care Coordination & Transitions of Care Communications Jessica Carpenter, MS, RD, LDN Director, Disability and Community Services University of Massachusetts Medical School Overview/Agenda
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Mission Health Care Network. April 2017
 Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network. Monday, September 12, 2011
 Care Coordination and the Role of the Aging Network. Monday, September 12, 2011") National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
DRAFT Complex and Chronic Care Improvement Program Template. (Not approved by CMS subject to continuing review process)
") DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
Building the Universal Roadmap to Population Health Management
 Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
Chronic Care Management Services. Presented by Noridian Part B Medicare Provider Outreach and Education April 2015
 Chronic Care Management Services Presented by Noridian Part B Medicare Provider Outreach and Education April 2015 Continuing Education Unit (CEU) When registering, add all additional attendees First and
Chronic Care Management Services Presented by Noridian Part B Medicare Provider Outreach and Education April 2015 Continuing Education Unit (CEU) When registering, add all additional attendees First and
LONG TERM CARE INTEGRATION
 LONG TERM CARE INTEGRATION Kristen D Smith, MPH Aging Program Administrator Aging & Independence Services County of San Diego Health and Human Services 1/11/2017 1 COUNTY OF SAN DIEGO Building Better Health
LONG TERM CARE INTEGRATION Kristen D Smith, MPH Aging Program Administrator Aging & Independence Services County of San Diego Health and Human Services 1/11/2017 1 COUNTY OF SAN DIEGO Building Better Health
HOUSEKEEPING. Slides were sent this morning Webinar is being recorded Please use the telephone option
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
Patient Engagement in the Population Health Management Era
 Patient Engagement in the Population Health Management Era Creagh Milford, DO, MPH President, Population Health Services A Catholic healthcare ministry serving Ohio and Kentucky Agenda Agenda I. Overview
Patient Engagement in the Population Health Management Era Creagh Milford, DO, MPH President, Population Health Services A Catholic healthcare ministry serving Ohio and Kentucky Agenda Agenda I. Overview
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees
 TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
Rural and Independent Primary Care.
 Rural and Independent Primary Care www.caravanhealth.com Agenda 2015 Results from Rural ACO Participants Fundamental population health programs. Overview of additional rural value-based payments Opportunities
Rural and Independent Primary Care www.caravanhealth.com Agenda 2015 Results from Rural ACO Participants Fundamental population health programs. Overview of additional rural value-based payments Opportunities
Model Of Care: Care Coordination Interdisciplinary Care Team (ICT)
") Cal MediConnect 2017 Model Of Care: Care Coordination Interdisciplinary Care Team (ICT) 2017 CMC Annual Training Learning Objectives Define the L.A. Care Cal MediConnect (CMC) Model of Care Describe the
Cal MediConnect 2017 Model Of Care: Care Coordination Interdisciplinary Care Team (ICT) 2017 CMC Annual Training Learning Objectives Define the L.A. Care Cal MediConnect (CMC) Model of Care Describe the
NextGen Population Health TEN TEN TEN TEN TE. Prevent Patients from Falling Through the Cracks in 10 Easy Steps
 NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
CHCANYS NYS HCCN ecw Webinar
 CHCANYS NYS HCCN ecw Webinar Meaningful Use, V10 and UDS January 30, 2013 Stephanie Rose, Project Director Desiree Railine, HIT Implementation Specialist/Trainer Agenda Meaningful Use Stage 1 2014 Review
CHCANYS NYS HCCN ecw Webinar Meaningful Use, V10 and UDS January 30, 2013 Stephanie Rose, Project Director Desiree Railine, HIT Implementation Specialist/Trainer Agenda Meaningful Use Stage 1 2014 Review
Streamlining care processes with a data-driven approach
 Streamlining care processes with a data-driven approach With Innovaccer s efficient and end-to-end care management solution Case Study Leading Iowa-based Mercy ACO deployed InCare to enable every member
Streamlining care processes with a data-driven approach With Innovaccer s efficient and end-to-end care management solution Case Study Leading Iowa-based Mercy ACO deployed InCare to enable every member
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement?
 Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Healthcare Service Delivery and Purchasing Reform in Connecticut
 Healthcare Service Delivery and Purchasing Reform in Connecticut Presentation to National Association of Medicaid Directors November 9, 2011 Mark Schaefer Director, Medical Care Administration Health Purchasing
Healthcare Service Delivery and Purchasing Reform in Connecticut Presentation to National Association of Medicaid Directors November 9, 2011 Mark Schaefer Director, Medical Care Administration Health Purchasing
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Improving Care and Lowering Costs: The Use of Clinical Data by Medicaid Managed Care Organizations. April 26, 2018
 Improving Care and Lowering Costs: The Use of Clinical Data by Medicaid Managed Care Organizations April 26, 2018 Agenda Welcome and Overview of Interview Results Claudia Ellison, Director of Programs,
Improving Care and Lowering Costs: The Use of Clinical Data by Medicaid Managed Care Organizations April 26, 2018 Agenda Welcome and Overview of Interview Results Claudia Ellison, Director of Programs,
Model of Care Heritage Provider Network & Arizona Priority Care Model of Care 2018
 Model of Care Model of Care 2018 Learning Objectives Program participants will be able to: List two differences between the Complex Care Management (CCM), and Special Needs Program (SNP) programs. Identify
Model of Care Model of Care 2018 Learning Objectives Program participants will be able to: List two differences between the Complex Care Management (CCM), and Special Needs Program (SNP) programs. Identify
Quality Measurement and Reporting Kickoff
 Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
2.b.iii ED Care Triage for At-Risk Populations
 2.b.iii ED Care Triage for At-Risk Populations Project Objective: To develop an evidence-based care coordination and transitional care program that will assist patients to link with a primary care physician/practitioner,
2.b.iii ED Care Triage for At-Risk Populations Project Objective: To develop an evidence-based care coordination and transitional care program that will assist patients to link with a primary care physician/practitioner,
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Updates October 2, 2012 Rick Hoover & Andy Finnegan
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Updates October 2, 2012 Rick Hoover & Andy Finnegan What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of meaningful use New
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Updates October 2, 2012 Rick Hoover & Andy Finnegan What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of meaningful use New
Trends in Home Care: Everybody Wants to Be There. Barbara A McCann Chief Industry Officer
 Trends in Home Care: Everybody Wants to Be There Barbara A McCann Chief Industry Officer Trend 1: The Medicare Home Health Benefit: Limiting Positive Innovation and Comfort It is an acute illness benefit
Trends in Home Care: Everybody Wants to Be There Barbara A McCann Chief Industry Officer Trend 1: The Medicare Home Health Benefit: Limiting Positive Innovation and Comfort It is an acute illness benefit
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Core Item: Hospital. Cover Page. Admissions and Readmissions. Executive Summary
 Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Medicaid Innovation Accelerator Project
 Medicaid Innovation Accelerator Project 2016-2017 Technical Expert Panel In-Person Meeting Community Integration Community-Based Long-Term Services and Supports Breakout Session April 18-19, 2017 Community
Medicaid Innovation Accelerator Project 2016-2017 Technical Expert Panel In-Person Meeting Community Integration Community-Based Long-Term Services and Supports Breakout Session April 18-19, 2017 Community
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
CLINICAL INTEGRATION STRATEGY
 CLINICAL INTEGRATION STRATEGY ABSTRACT The Suffolk Care Collaborative Clinical Integration Strategy focuses on the ability to coordinate care across the continuum through clinically interoperable systems.
CLINICAL INTEGRATION STRATEGY ABSTRACT The Suffolk Care Collaborative Clinical Integration Strategy focuses on the ability to coordinate care across the continuum through clinically interoperable systems.
Monday, October 24, :15 a.m. to 10:45 a.m. Great Halls 1 & 2
 Expanding Pharmacy Impact: Transitional Care Management and Chronic Care Management Activity Number: 0217-0000-16-1118-L04-P 1.50 hours of CPE credit; Activity Type: A Knowledge-Based Activity Monday,
Expanding Pharmacy Impact: Transitional Care Management and Chronic Care Management Activity Number: 0217-0000-16-1118-L04-P 1.50 hours of CPE credit; Activity Type: A Knowledge-Based Activity Monday,
Molina Medicare Model of Care
 Molina Medicare Model of Care Provider Network Molina Healthcare 2018 1 Molina s Mission and Vision Our Vision: We envision a future where everyone receives quality health care Our Mission: To provide
Molina Medicare Model of Care Provider Network Molina Healthcare 2018 1 Molina s Mission and Vision Our Vision: We envision a future where everyone receives quality health care Our Mission: To provide
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Quality Improvement: Utilization Measures
 Home Health Value-Based Purchasing (HHVBP) Quality Improvement: Utilization Measures June 9, 2016 As prepared by the Centers for Medicare & Medicaid Services HHVBP Technical Assistance contract number
Home Health Value-Based Purchasing (HHVBP) Quality Improvement: Utilization Measures June 9, 2016 As prepared by the Centers for Medicare & Medicaid Services HHVBP Technical Assistance contract number
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
DSRIP Demonstration Year 1, Quarter 1-2 Domain 1 Patient Engagement Data Request
 DSRIP Demonstration Year 1, Quarter 1-2 Domain 1 Patient Engagement Data Request Webinar: Monday, October 5, 2015 Time: 1:30pm-3:00pm Presented by Suffolk Care Collaborative (SCC) Suffolk County Performing
DSRIP Demonstration Year 1, Quarter 1-2 Domain 1 Patient Engagement Data Request Webinar: Monday, October 5, 2015 Time: 1:30pm-3:00pm Presented by Suffolk Care Collaborative (SCC) Suffolk County Performing
Policy & Providers. for Managing Chronic Care Patients. Mary Alexander Strategic Alliances Director - Home Instead, Inc. Kelly Funk.
 Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Medical Home Summit September 20, 2011
 Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
Coordinated Care Initiative DRAFT Assessment and Care Coordination Standards November 20, 2012
 Coordinated Care Initiative DRAFT Assessment and Care Coordination Standards November 20, 2012 Table of Contents CARE COORDINATION GENERAL REQUIREMENTS...4 RISK STRATIFICATION AND HEALTH ASSESSMENT PROCESS...6
Coordinated Care Initiative DRAFT Assessment and Care Coordination Standards November 20, 2012 Table of Contents CARE COORDINATION GENERAL REQUIREMENTS...4 RISK STRATIFICATION AND HEALTH ASSESSMENT PROCESS...6
Jeffrey B. Klein, FACHE President & CEO
 Jeffrey B. Klein, FACHE President & CEO THE ROAD TO REVOLUTION How serious will the trajectory of demographic shifts and the effects of the health care delivery system change be on America s most vulnerable
Jeffrey B. Klein, FACHE President & CEO THE ROAD TO REVOLUTION How serious will the trajectory of demographic shifts and the effects of the health care delivery system change be on America s most vulnerable
The Collaborative to Advance Social Health Integration (CASHI)
") The Collaborative to Advance Social Health Integration (CASHI) "Let me tell you the story of one patient we worked with in Boston. He was screened for unmet health-related social needs as part of a newly
The Collaborative to Advance Social Health Integration (CASHI) "Let me tell you the story of one patient we worked with in Boston. He was screened for unmet health-related social needs as part of a newly
Medicare Advantage in Practice: Enhanced Care Models for High Need Patients
 Medicare Advantage in Practice: Enhanced Care Models for High Need Patients Rebekah Dube, Pharm.D. VP, Health Plan Clinical Programs & Interim VP, Health Plan Products Who is Martin s Point Health Care?
Medicare Advantage in Practice: Enhanced Care Models for High Need Patients Rebekah Dube, Pharm.D. VP, Health Plan Clinical Programs & Interim VP, Health Plan Products Who is Martin s Point Health Care?
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs
 2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
MEDICAL HOMES Arkansas Hospital Association
 MEDICAL HOMES Arkansas Hospital Association Framing our discussion Environmental snapshot of health care Hospitals and the PCMH Arkansas Medical Homes Patients/Consumers 2 1 Health Policy is changing Budget
MEDICAL HOMES Arkansas Hospital Association Framing our discussion Environmental snapshot of health care Hospitals and the PCMH Arkansas Medical Homes Patients/Consumers 2 1 Health Policy is changing Budget
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered