Psychiatric Emergencies: A Continuum of Solutions
|
|
|
- Clifton Miles
- 5 years ago
- Views:
Transcription
1 C30 These presenters have nothing to disclose Psychiatric Emergencies: A Continuum of Solutions Margie Balfour, MD, PHD John Santopietro, MD William Tucker, MD Facilitator: Mara Laderman, MSPH December 6, :30 2:45 PM #IHIFORUM
2 Session Objectives P2 Describe the challenges that emergency departments face in caring for patients with behavioral health needs. Compare different approaches to addressing psychiatric emergencies in health care and community settings. Understand how to reconfigure their current resources to reduce the number of psychiatric emergencies in the first place. #IHIFORUM
3 Psychiatric emergencies are prevalent P3 In 2007, 12 million, or 12.5% of total ED visits, were related to mental health and substance abuse. In 2014, 84 percent of EDs reported boarding psychiatric patients with over half reporting at least daily boarding. 91% of physicians who report psychiatric boarding in the ED say that boarding has resulted in harm to other patients or staff.
4 and lead to poorer outcomes and P4 higher costs Overcrowding in the ED Delays in treatment for psychiatric patients which increases the probability of inpatient admissions Treatment delays for other ED patients Increased stress for patients and families Increased pressure and stress for ED teams Safety concerns for health care professionals Financial issues
5 Session Format P5 Panel discussion: Each presenter will speak for 15 minutes Q&A and discussion

6 Caring for ED Patients Virtually : A Local Story John Santopietro, MD, DFAPA Carolinas HealthCare System IHI December 6 th, 2016

7 W H E R E W E A R E
8 Carolinas HealthCare System 39 hospitals and 900+ care locations in North Carolina, South Carolina and Georgia More than 7,800 licensed beds More than 11 million patient encounters in ,000+ system-employed physicians, 14,000+ nurses and more than 60,000 employees $1.5 billion in community benefit in 2013 More than $8 billion in annual revenue The region s only Level I trauma center One of five academic medical centers in North Carolina One of the largest HIT and EMR systems in the country Cerner s largest contract


9 A good place to start

10 Source: Anne M. Hakenewerth, PhD, Texas Cancer Registry, Texas Department of State Health Svcs. Judith E. Tintinalli, MD, Anna E. Waller, ScD, Amy Ising, MSIS, Tracy DeSelm, MD, Carolina Center for Health Informatics, Department of Emergency Medicine, University of North Carolina at Chapel Hill
11
12
13

14

15 Behavioral Health is another vital sign Normalize Destigmatize Systematize
")


16 Virtual Behavioral Health Footprint Tele-psychiatry and Patient Placement Collaborate with 20 Emergency Departments Behavioral Health Integration (BHI) Collaborate with 50 + Primary Care sites* Behavioral Health Call Center Map Key Received 175,954 calls in 2015 Active Tele-psychiatry and Patient Placement Site Future Tele-psychiatry and Patient Placement Site Active BHI Site Future BHI Site BH Call Center *Note: Numbers include care management. There are 16 fully integrated PCP sites.

17 A new idea?

18

19
20 Department Evolution FTE Shortage The Plan Scheduling Capacity with Current FTEs (not including OT & PRN) Patient Placement Monday Friday 7 am to 11 pm Actual Scheduling by 2014 Year End 24/7 Telepsych Monday Friday 7 am to 11 pm Weekdays: hrs* Weekends: hrs* 2014 OT & PRN Hours 5,926 2, Physician Supplemental Pay n/a *need data* *Currently, telepsych clinician and MD scheduling times differ Director 2014 Jan Feb Mar April May June July Aug Sept Oct Nov Dec 1.0 FTE Nurse Manager 25% Admin Prog. Coordinator 50% Admin Telepsych Clinician Placement Coordinator MD Coverage 3.0 FTEs 1.0 FTE 1.0 FTE 1.0 FTE 1.0 FTE.5 FTE 1.0 FTE 1.0 FTE 1.0 FTE 3.0 FTEs 1.0 FTE 1.0 FTE Incremental Existing 11/28/


21
22 2014 Incremental CHS Investment $ 40,873 for.96 Admission Transfer Coordinator (annualized) $ 85,003 for 1.17 Telepsych Clinicians (annualized) $ 151,689 for overtime and PRN (patient placement & telepsych) $ 339,300 for G4S Patient Transport Contract $ 0 for Providers (utilized existing ED Physicians) $ 629,991 in incremental expense to CHS in /28/

23
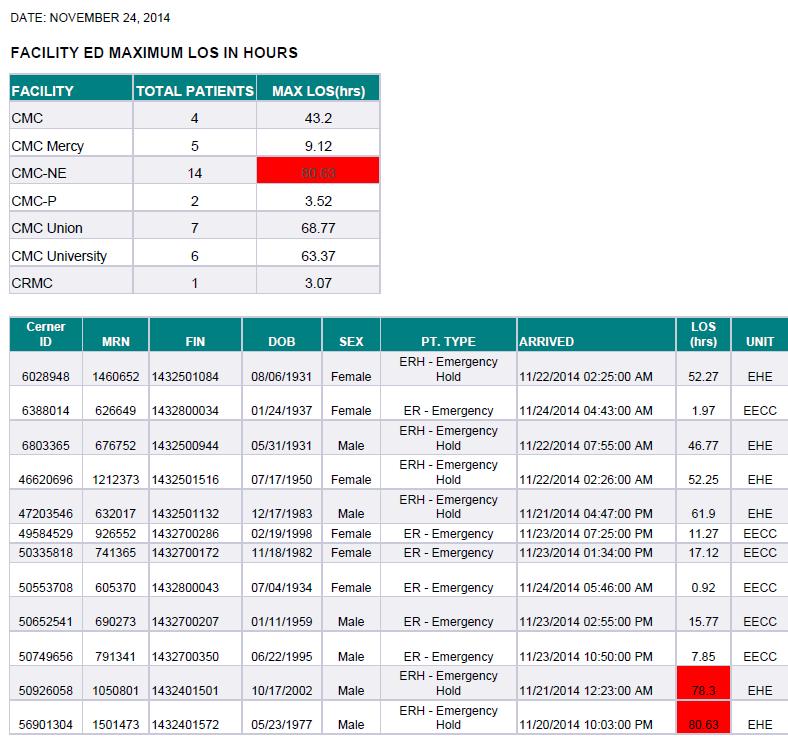
24 ED Length of Stay Reduction 50 ALOS for CMC Pineville ED BH Patients 24

25


26
27 No rest for the weary 8000 Acute Care ED Patients (excluding psych ED) % September 2014 YTD Acute Care ED Patients (excluding psych ED) September 2016 YTD Linear (Acute Care ED Patients (excluding psych ED))


28 .
29 Workshop C30 This presenter has nothing to disclose Facility-based behavioral health crisis services as an alternative to ED boarding and jail Margie Balfour, MD, PhD VP for Clinical Innovation & Quality, ConnectionsAZ Chief Clinical Officer, Crisis Response Center Asst Professor of Psychiatry, University of Arizona Tucson, AZ Tue Dec :30-2:45 #IHIFORUM

30 The path to psychiatric boarding P30 People in crisis are often unable to immediately access care or they don t know where to go So they go to the ED Which is not equipped for psychiatric evaluation, stabilization, or discharge planning So they get put on a list to be admitted to an inpatient psychiatric unit And then they wait and wait




31 How do people get to the ED? P31 First Responders Walk-in For psych emergencies, first responders are often the police
 each year.")
 Prevalence of serious mental illness among jail inmates. Psychiatric Services. 60(6):761-5.")
32 P32 The path to jail Officers want the person to get treatment But they don t know where else to take them except the ED Where they have to wait. Cops are busy and have crimes to fight So they take the person to jail instead. There are over 2 million jail bookings of people with serious mental illness (SMI) each year. 1 Nearly half of people with SMI have been arrested at least once. 2 SMI 3 -Men -Women Prevalence of Mental Illness Jail US Adults % 34.3% 4% Any mental disorder 4 76% 18% + Co-occurring substance use 4 49% 3.3% 6 1. Steadman HJ et al. (2009) Prevalence of serious mental illness among jail inmates. Psychiatric Services. 60(6): %. Hall LL et al. (2003) TRIAD Report: Shattered Lives: Results of a National Survey of NAMI Members Living with Mental Illnesses and Their Families. 3. Includes PTSD. Excluding PTSD rates are 14.5% for men and 31.0% for women. Steadman HJ, Osher FC, Robbins PC, Case B, Samuels S. (2009) Prevalence of serious mental illness among jail inmates. Psychiatric Services. 60(6): Glaze LE, James DJ. (2006) Mental Health Problems Of Prison And Jail Inmates. Bureau of Justice Statistics. 5. NIMH Statistics 6. SAMHSA (2015). Behavioral Health Trends in the United States: Results from the 2014 National Survey on Drug Use and Health.

33 An alternative model P33 A facility-based behavioral health crisis program that provides 24/7 on-demand access A safe and welcoming environment Rapid triage and psychiatric assessment Crisis Stabilization: Via counseling, medications, peer groups, family engagement, etc. Connection to community resources Studies show this model reduces: ED boarding 1,2 Inpatient hospitalization 1,2 Arrest 3 1. Little-Upah P et al. (2013). The Banner psychiatric center: a model for providing psychiatric crisis care to the community while easing behavioral health holds in emergency departments. Perm J 17(1): Zeller S et al. (2014). Effects of a dedicated regional psychiatric emergency service on boarding of psychiatric patients in area emergency departments. West J Emerg Med 15(1): 1-6.Steadman HJ et al (2001). A specialized crisis response site as a core element of police-based diversion programs. Psychiatr Serv 52: Steadman HJ et al (2001). A specialized crisis response site as a core element of police-based diversion programs. Psychiatr Serv 52:219-22
 Inpatient psych hospital that provides court-ordered evaluations Emergency")
34 An example: Crisis Response Center 34 Built with county bond funds in 2011 to serve Pima County (Tucson, AZ) 12,000 adults + 2,200 youth per year Alternative to jail, ED, hospitals Co-located crisis call center Mobile team dispatch Bed board Space for community partners Adjacent to Mental health court (civil commitment) Inpatient psych hospital that provides court-ordered evaluations Emergency Department ConnectionsAZ/Banner University Medical Center Crisis Response Center in Tucson, AZ

35 24/7 Access to Psychiatric Emergency Services 35 Patients arrive via: Walk-in Law enforcement Emergency rooms transfers Mobile Crisis Teams Referrals from clinics, foster care, group homes, etc. Services include: Urgent care clinic 23-observation unit Short-term (3-5 day) inpatient stabilization We address any behavioral health need at any time.

36 Low clinical barriers to access 36 No wrong door We do our best to take everyone: No such thing as too agitated Highly intoxicated Voluntary or involuntary Fewer medical exclusionary criteria than many inpatient psych hospitals No refusal policy for law enforcement Otherwise, where would these patients go?


37 37 The CRC provides safe environment where people can be under continuous observation and lack the means to hurt themselves or others, while being as comfortable and welcoming as possible Crisis Response Center, Tucson AZ



38 Gated Sally Port for Secure Law Enforcement Drop-offs 38 Crisis Response Center, Tucson AZ


39 39 23-Hour Observation Unit Staffed 24/7 with MDs, NPs, PAs Medical necessity criteria similar to that of inpatient psych (danger to self, other, etc.) Diversion from inpatient: 60-70% discharged to the community the following day Early intervention Median door to doc time is ~90 min Interdisciplinary team Including peers with lived experience Aggressive discharge planning Collaboration and coordination with community & family partners Assumption that the crisis can be resolved

40 Outcomes: Police Turnaround Time 40 Half of our patients arrive via law enforcement. They are an important customer and quick turnaround time is critical to providing a viable alternative to jail. (Our Phoenix facility achieves similar results with twice the volume.)
41 Outcomes: Urgent Care Clinic 41 Patients are able to walk in and quickly get their needs met without going to an ED (med refills, connection to services, etc.)
42 Outcomes: Obs Unit Door-to-Doc 42 Early assessment and treatment is critical to avoiding hospitalization and preventing adverse outcomes such as restraints and assaults.
43 Outcomes: Community Dispositions 43 Only a fraction of the observation patients are admitted to an inpatient unit. Instead, they can be discharged (diverted) to less-restrictive communitybased care. In an ED, many more would board waiting for beds.
44 44 More outcomes and data We developed a set of quality measures for our organization Endorsed by the American Association for Emergency Psychiatry The Joint Commission will have a project in 2017 to develop a core measure set for behavioral health crisis services. We also created daily data feeds to the Regional Behavioral Health Authority to assist them more real time management of network performance, identify high-utilizers, etc. Balfour ME, Tanner K, Jurica PS, Rhoads R, Carson C. (2016) Community Mental Health Journal. 52(1):



45 45 More outcomes and data Internal Quality Metrics We developed a set of quality measures for our organization Endorsed by American Association for Emergency Psychiatry Joint Commission project in 2017 will develop core measures for crisis services. System Performance Data Crisis utilization is a canary in the coal mine performance indicator of the overall behavioral health system We developed daily data feeds for the Regional Behavioral Health Authority (our primary payer) Real time analysis of network performance Identification of high utilizers Balfour ME, Tanner K, Jurica PS, Rhoads R, Carson C. (2016) Community Mental Health Journal. 52(1):

.")
: 45-49. https://doi.")
46 Other applications of this model 46 Urgent Psychiatric Center Our flagship facility in Phoenix, serving 2000 patients per month We adapted this model to service a hospital system with EDs across metro Phoenix We have also assisted in the design and implementation of similar programs in more rural areas such as Flagstaff and Prescott Valley Little-Upah P et al. (2013). The Banner psychiatric center: a model for providing psychiatric crisis care to the community while easing behavioral health holds in emergency departments. Perm J 17(1):
47 Lessons Learned P47 The solution is not always more beds. Inpatient admission is often the default when less-restrictive alternatives are unavailable or ineffective. Quickly meeting people s needs leads to positive outcomes. Figure out how to say yes. When crisis centers exclude patients, they end up in EDs/jails. Safety is the prime directive. Processes and facilities must be designed to safely care for the most acute. A multidisciplinary approach and community partnerships are critical to success. There will never be a rule for every scenario. When in doubt: 1) be safe, and 2) follow the golden rule.
48 How to Reduce Pressure on Psychiatric Emergency Services Promote Recovery Instead of Compliance William Tucker, MD
49 Problems with Current Services Former inmates, mental hospital dischargees, and the homeless are NOT YET engaged in community services Clinics to which the above are referred have no motivation to hold onto them. Institutions themselves have no resources to promote community engagement ER is always the default option (+/- hosp.) Hence, the revolving door is the rule
50 Sources of Increasing Pressure 1) increased access provided by funding through the Affordable Care Act 2) increased rate of early discharge from mental hospitals and from prisons (high cost of institutionalization->closures)
51 Alternative to Revolving Door : Stabilization and Recovery Stabilization=independent living, financial stability, acceptance of [selected] traditional services [e.g., meds, programs], avoidance of ER s, reduction/ cessation of substance abuse Recovery=pursuit of personal goals (patients have provided a standard list of these shelter, transportation, meaningful relationships, etc; more specifically: living undisturbed, independence from family, pursuit of pleasurable activities, college completion, freedom from agency interference, gender identity transformation)
52 How Outreach Works to Promote Recovery It provides traditional services (psychopharm, supportive psychotherapy) + non-traditional ones (making home visits and visits to ER s, in-patient sites, PMD s, job sites) It requires getting to know each patient intimately (i.e., personal goals rather than symptoms) It requires hanging on until stabilization and recovery begin (note: Promoting compliance leaves responsibility with the clinician, rather than with the patient)
53 Resources and Outcomes 1) I treated 30 patients at a time, working 2d/wk +consulted to a Psych NP treating another 30. 2) Medicaid contract paid $1500/mo. for mental health and housing (SSI supplemented housing). 3) Half of my patients recovered. 4) Hospitalizations and ER visits plummeted for all patients, more than off-setting costs.
54 Problems with Outreach It requires working in the community, which is not as safe, secure, and predictable as in traditional institutional or clinic settings. It requires lots of LEGWORK! It s an open-ended contract: there are no discharges or hand-offs to other services. It takes a team. 50% of patients will require enhanced interventions, but you don t know which 50%.
55 How to Get Outreach Started Get administrative support for market-rate community housing, not group homes. Divert a SMALL amount of current resources to ACT teams, or set up referral networks. Have ER assign new patients to ACT teams. Help families connect early to services promoting recovery. Check out programs for enhanced firstepisode services (RAISE, OnTrack).
56 My Questions to You About Systems Change Does outreach sound possible within your system? What changes would you require to try it out? Have you been thinking of outreach for a long time already, waiting for your system to catch up?

57 Questions?
Psychiatric Emergencies: A Continuum of Solutions Margie Balfour, MD, PHD John Santopietro, MD William Tucker, MD Facilitator: Mara Laderman, MSPH
 C30 These presenters have nothing to disclose Psychiatric Emergencies: A Continuum of Solutions Margie Balfour, MD, PHD John Santopietro, MD William Tucker, MD Facilitator: Mara Laderman, MSPH December
C30 These presenters have nothing to disclose Psychiatric Emergencies: A Continuum of Solutions Margie Balfour, MD, PHD John Santopietro, MD William Tucker, MD Facilitator: Mara Laderman, MSPH December
More Than Emergency Response:
 More Than Emergency Response: The Tucson Model's Preventative Approach to Crisis and Public Safety Margie Balfour, MD, PhD Connections Health Solutions VP for Clinical Innovation & Quality Chief Clinical
More Than Emergency Response: The Tucson Model's Preventative Approach to Crisis and Public Safety Margie Balfour, MD, PhD Connections Health Solutions VP for Clinical Innovation & Quality Chief Clinical
Behavioral Health Division JPS Health Network
 Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE
 EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
Speaker: Ruby Qazilbash. Ruby Qazilbash Associate Deputy Director Bureau of Justice Assistance Office of Justice Programs U.S. Department of Justice
 1 2 Speaker: Ruby Qazilbash Ruby Qazilbash Associate Deputy Director Bureau of Justice Assistance Office of Justice Programs U.S. Department of Justice 3 Today s Webinar Council of State Governments Justice
1 2 Speaker: Ruby Qazilbash Ruby Qazilbash Associate Deputy Director Bureau of Justice Assistance Office of Justice Programs U.S. Department of Justice 3 Today s Webinar Council of State Governments Justice
TARRANT COUNTY DIVERSION INITIATIVES
 TARRANT COUNTY DIVERSION INITIATIVES Texas Council June 2015 Ramey C. Heddins, CCHP Director Mental Health Support Services Kathleen Carr Rae, Public Policy Specialist WHAT IS THE PROBLEM? Prison 3-year
TARRANT COUNTY DIVERSION INITIATIVES Texas Council June 2015 Ramey C. Heddins, CCHP Director Mental Health Support Services Kathleen Carr Rae, Public Policy Specialist WHAT IS THE PROBLEM? Prison 3-year
ABC s of PES. Greg Miller, MD MBA CMO Unity Center for Behavioral Health
 ABC s of PES Greg Miller, MD MBA CMO Unity Center for Behavioral Health Content Outline Overview of Unity Services Emergency Psychiatry: Historical Perspective Emergency Psychiatry: Current Service Delivery
ABC s of PES Greg Miller, MD MBA CMO Unity Center for Behavioral Health Content Outline Overview of Unity Services Emergency Psychiatry: Historical Perspective Emergency Psychiatry: Current Service Delivery
Arizona Mental Health Criminal Justice Coalition. Goal is to reduce court involvement when possible (criminal AND civil)
") Arizona Mental Health Criminal Justice Coalition Goal is to reduce court involvement when possible (criminal AND civil) Arizona Mental Health Criminal Justice Coalition 2 million seriously mentally ill
Arizona Mental Health Criminal Justice Coalition Goal is to reduce court involvement when possible (criminal AND civil) Arizona Mental Health Criminal Justice Coalition 2 million seriously mentally ill
How can we provide the same world class care to patients with psychiatric disorders? 11/27/2016. Dec 2016 Orlando, FL
 The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
How Can Emergency Departments Improve Care for Patients with Mental Health Issues?
 D1/E1 These presenters have nothing to disclose How Can Emergency Departments Improve Care for Patients with Mental Health Issues? Robin Henderson, PsyD Mara Laderman, MSPH Arpan Waghray, MD December 13,
D1/E1 These presenters have nothing to disclose How Can Emergency Departments Improve Care for Patients with Mental Health Issues? Robin Henderson, PsyD Mara Laderman, MSPH Arpan Waghray, MD December 13,
A Model for Psychiatric Emergency Services
 A Model for Psychiatric Emergency Services Improving Access and Quality Reducing Boarding, Re-Hospitalizations and Costs Scott Zeller, MD Chief, Psychiatric Emergency Services Alameda Health System, Oakland,
A Model for Psychiatric Emergency Services Improving Access and Quality Reducing Boarding, Re-Hospitalizations and Costs Scott Zeller, MD Chief, Psychiatric Emergency Services Alameda Health System, Oakland,
Behavioral Health Services. San Francisco Department of Public Health
 Behavioral Health Services San Francisco Department of Public Health Slide 2 Agenda Behavioral Health Services in San Francisco Mental Health Services Substance Use Disorder Services Levels of Care Behavioral
Behavioral Health Services San Francisco Department of Public Health Slide 2 Agenda Behavioral Health Services in San Francisco Mental Health Services Substance Use Disorder Services Levels of Care Behavioral
GOB Project 193 Mental Health Diversion Facility Service Capacity and Fiscal Impact Estimates June 9, 2016
 GOB Project 193 Mental Health Diversion Facility Service Capacity and Fiscal Impact Estimates June 9, 2016 I. SUMMARY The purpose of the Mental Health Diversion Facility (Facility) is to create a comprehensive
GOB Project 193 Mental Health Diversion Facility Service Capacity and Fiscal Impact Estimates June 9, 2016 I. SUMMARY The purpose of the Mental Health Diversion Facility (Facility) is to create a comprehensive
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT
 NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT Provider will comply with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT Provider will comply with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
Options for cost savings through regionalizing community-based services, and discussion of data needs. Michael Flaum, MD
 Legislative Task Force Des Moines, IA Oct 21, 2009 Options for cost savings through regionalizing community-based services, and discussion of data needs Michael Flaum, MD Director, Iowa Consortium for
Legislative Task Force Des Moines, IA Oct 21, 2009 Options for cost savings through regionalizing community-based services, and discussion of data needs Michael Flaum, MD Director, Iowa Consortium for
Julie Kelley, MSW, MPH Program Chief, Mental Heath/Psychiatry Contra Costa Regional Medical Center Martinez, CA
 Julie Kelley, MSW, MPH Program Chief, Mental Heath/Psychiatry Contra Costa Regional Medical Center Martinez, CA Patients and Families as Care Partners April 20, 2011 Little about us Contra Costa Regional
Julie Kelley, MSW, MPH Program Chief, Mental Heath/Psychiatry Contra Costa Regional Medical Center Martinez, CA Patients and Families as Care Partners April 20, 2011 Little about us Contra Costa Regional
6/27/2014. THE NEW TECHNOLOGY LANDSCAPE Presentation Objectives. The Landscape Drives Metrics. Issues: Responding to Need. AZ Drivers/Priorities
 x == 6/27/2014 THE NEW TECHNOLOGY LANDSCAPE Presentation Objectives Using Business Analytics & Health Information Exchanges to Improve Practice & Sustain Organizations Business Metric Development Strategies
x == 6/27/2014 THE NEW TECHNOLOGY LANDSCAPE Presentation Objectives Using Business Analytics & Health Information Exchanges to Improve Practice & Sustain Organizations Business Metric Development Strategies
Miami-Dade County Mental Health Diversion Facility July 2016
 Miami-Dade County Mental Health Diversion Facility July 2016 I. SUMMARY The purpose of the Mental Health Diversion Facility is to create a comprehensive and coordinated system of care for individuals with
Miami-Dade County Mental Health Diversion Facility July 2016 I. SUMMARY The purpose of the Mental Health Diversion Facility is to create a comprehensive and coordinated system of care for individuals with
PSYCHIATRY SERVICES UPDATE
 PSYCHIATRY SERVICES UPDATE Mark Leary MD, Interim Chief Kathy Ballou RN, Director of Nursing Anton Nigusse Bland MD, PES Medical Director Emily Lee MD, Inpatient Psychiatry Medical Director TRUE NORTH
PSYCHIATRY SERVICES UPDATE Mark Leary MD, Interim Chief Kathy Ballou RN, Director of Nursing Anton Nigusse Bland MD, PES Medical Director Emily Lee MD, Inpatient Psychiatry Medical Director TRUE NORTH
The Behavioral Health System. Presentation to the House Select Committee on Mental Health
 The Behavioral Health System Presentation to the House Select Committee on Mental Health John Hellerstedt, M.D. Commissioner Lauren Lacefield Lewis Assistant Commissioner Division for Mental Health and
The Behavioral Health System Presentation to the House Select Committee on Mental Health John Hellerstedt, M.D. Commissioner Lauren Lacefield Lewis Assistant Commissioner Division for Mental Health and
Crisis Now: Transforming Services is Within Our Reach. August 9, 2017
 Disclaimer The views, opinions, and content expressed in this presentation do not necessarily reflect the views, opinions, or policies of the Center for Mental Health Services (CMHS), the Substance Abuse
Disclaimer The views, opinions, and content expressed in this presentation do not necessarily reflect the views, opinions, or policies of the Center for Mental Health Services (CMHS), the Substance Abuse
San Francisco Whole Person Care California Medi-Cal 2020 Waiver Initiative
 San Francisco Whole Person Care California Medi-Cal 2020 Waiver Initiative Update April 3, 2018 Health Commission Maria X Martinez, Director Whole Person Care Barry Zevin, MD, Medical Director Street Medicine
San Francisco Whole Person Care California Medi-Cal 2020 Waiver Initiative Update April 3, 2018 Health Commission Maria X Martinez, Director Whole Person Care Barry Zevin, MD, Medical Director Street Medicine
Psychiatric Patient Boarding Problems in the Emergency Department
 Psychiatric Patient Boarding Problems in the Emergency Department IMPROVING TIMELINESS, ACCESS, AND QUALITY LOWERING COSTS AND RE-HOSPITALIZATIONS Scott Zeller, MD Chief, Psychiatric Emergency Services
Psychiatric Patient Boarding Problems in the Emergency Department IMPROVING TIMELINESS, ACCESS, AND QUALITY LOWERING COSTS AND RE-HOSPITALIZATIONS Scott Zeller, MD Chief, Psychiatric Emergency Services
The Scope and Impact of the Metropolitan St. Louis Psychiatric Center (MPC) Emergency Department (ED)/Acute Care Closure
 Emergency Department (ED)/Acute Care Closure") The Scope and Impact of the Metropolitan St. Louis Psychiatric Center (MPC) Emergency Department (ED)/Acute Care Closure Draft Prepared by the Short-Term Crisis Management Team June 23, 2010 Background
The Scope and Impact of the Metropolitan St. Louis Psychiatric Center (MPC) Emergency Department (ED)/Acute Care Closure Draft Prepared by the Short-Term Crisis Management Team June 23, 2010 Background
Urgent Matters Learning Webinar December 16, 2010
 Urgent Matters Learning Webinar December 16, 2010 Providing Health Care for the Acute Mentally Ill: A Community Response San Antonio, Texas David A. Hnatow, MD, FAAEM, FACEP Emergency Medicine Physician,
Urgent Matters Learning Webinar December 16, 2010 Providing Health Care for the Acute Mentally Ill: A Community Response San Antonio, Texas David A. Hnatow, MD, FAAEM, FACEP Emergency Medicine Physician,
Southwest Texas Regional Advisory Council
 Executive Summary In 1989, the Texas legislature identified a need to ensure trauma resources were available to every person in Texas. The Omni Rural Health Care Rescue Act, directed the Bureau of Emergency
Executive Summary In 1989, the Texas legislature identified a need to ensure trauma resources were available to every person in Texas. The Omni Rural Health Care Rescue Act, directed the Bureau of Emergency
Critical Time Intervention (CTI) (State-Funded)
 (State-Funded)") Critical Time (CTI) (State-Funded) Service Definition and Required Components Critical Time (CTI) is an intensive 9 month case management model designed to assist adults age 18 years and older with mental
Critical Time (CTI) (State-Funded) Service Definition and Required Components Critical Time (CTI) is an intensive 9 month case management model designed to assist adults age 18 years and older with mental
1. November RN VACANCY RATE: Overall 2320 RN vacancy rate for areas reported is 12.5%
 PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, December 2013 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. November 2013-2320 RN VACANCY RATE: Overall 2320 RN
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, December 2013 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. November 2013-2320 RN VACANCY RATE: Overall 2320 RN
A CALL TO ACTION East Baton Rouge Parish s Plan for Behavioral Health Crisis Management
 Jan M. Kasofsky, PH.D. Executive Director, Capital Area Human Services Clinical Design Committee Chair A CALL TO ACTION East Baton Rouge Parish s Plan for Behavioral Health Crisis Management BATON ROUGE
Jan M. Kasofsky, PH.D. Executive Director, Capital Area Human Services Clinical Design Committee Chair A CALL TO ACTION East Baton Rouge Parish s Plan for Behavioral Health Crisis Management BATON ROUGE
Emanuel Medical Center adult behavioral health ED visits
 Learning objectives Learn about Psychiatric Emergency Service Models and Need Learn about the Alameda Model study A Regional Approach to Addressing ED Psychiatric Boarding Learn about Unity Center for
Learning objectives Learn about Psychiatric Emergency Service Models and Need Learn about the Alameda Model study A Regional Approach to Addressing ED Psychiatric Boarding Learn about Unity Center for
Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Brian Sheitman MD
 Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Professor of Family Medicine UNC School of Medicine & Associate Medical Director Primary Care Services
Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Professor of Family Medicine UNC School of Medicine & Associate Medical Director Primary Care Services
What is the Judge Guy Herman Center for Mental Health Crisis Care?
 FAQs: Judge Guy Herman Center for Mental Health Crisis Care What is the Judge Guy Herman Center for Mental Health Crisis Care? The Judge Herman Center for Mental Health Crisis Care provides short term
FAQs: Judge Guy Herman Center for Mental Health Crisis Care What is the Judge Guy Herman Center for Mental Health Crisis Care? The Judge Herman Center for Mental Health Crisis Care provides short term
AHP Patient Centered Care Models and Unity Center Psychiatric Emergency Service
 AHP Patient Centered Care Models and Unity Center Psychiatric Emergency Service CHRIS FARENTINOS, MD, MPH VICE PRESIDENT, UNITY CENTER FOR BEHAVIORAL HEALTH 1 Emanuel Medical Center adult behavioral health
AHP Patient Centered Care Models and Unity Center Psychiatric Emergency Service CHRIS FARENTINOS, MD, MPH VICE PRESIDENT, UNITY CENTER FOR BEHAVIORAL HEALTH 1 Emanuel Medical Center adult behavioral health
Behavioral Wellness. Garden Fountain by Bridget Hochman RECOMMENDED BUDGET & STAFFING SUMMARY & BUDGET PROGRAMS CHART
 Garden Fountain by Bridget Hochman RECOMMENDED BUDGET & STAFFING SUMMARY & BUDGET PROGRAMS CHART Operating $ 133,861,700 Capital $ 0 FTEs 384.4 Alice Gleghorn, PhD Director Administration & Support Mental
Garden Fountain by Bridget Hochman RECOMMENDED BUDGET & STAFFING SUMMARY & BUDGET PROGRAMS CHART Operating $ 133,861,700 Capital $ 0 FTEs 384.4 Alice Gleghorn, PhD Director Administration & Support Mental
Aurora will expand its geographic coverage within Wisconsin to achieve its mission to: Aurora Health Care 1991 Strategic Plan
 Objectives To describe the 20-year evolution of Aurora Medical Group within Aurora Health Care To identify the cultural characteristics necessary to improve patient access from the patient s perspective
Objectives To describe the 20-year evolution of Aurora Medical Group within Aurora Health Care To identify the cultural characteristics necessary to improve patient access from the patient s perspective
Implementation and Outcomes from Connecticut s Mobile Crisis Intervention Service
 Implementation and Outcomes from Connecticut s Mobile Crisis Intervention Service Jeffrey J. Vanderploeg, Ph.D. Vice President for Mental Health Child Health & Development Institute of Connecticut Tim
Implementation and Outcomes from Connecticut s Mobile Crisis Intervention Service Jeffrey J. Vanderploeg, Ph.D. Vice President for Mental Health Child Health & Development Institute of Connecticut Tim
Managing Psychiatric Patient Throughput in the Emergency Department
 Managing Psychiatric Patient Throughput in the Emergency Department Heartland Healthcare Executive Group (HHEG) October 22, 2015 Agenda Introductions U.S. Mental Health Access Crisis Risks to Patients,
Managing Psychiatric Patient Throughput in the Emergency Department Heartland Healthcare Executive Group (HHEG) October 22, 2015 Agenda Introductions U.S. Mental Health Access Crisis Risks to Patients,
Assertive Community Treatment (ACT)
") Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Acute Crisis Units. Shelly Rhodes, Provider Relations Manager
 Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
Department of Vermont Health Access Department of Mental Health. dvha.vermont.gov/ vtmedicaid.com/#/home
 Department of Vermont Health Access Department of Mental Health dvha.vermont.gov/ vtmedicaid.com/#/home ... 2 INTRODUCTION... 3 CHILDREN AND ADOLESCENT PSYCHIATRIC ADMISSIONS... 7 VOLUNTARY ADULTS (NON-CRT)
Department of Vermont Health Access Department of Mental Health dvha.vermont.gov/ vtmedicaid.com/#/home ... 2 INTRODUCTION... 3 CHILDREN AND ADOLESCENT PSYCHIATRIC ADMISSIONS... 7 VOLUNTARY ADULTS (NON-CRT)
Widespread prescribing, distribution and availability of naloxone for high risk individuals and as rescue medication 2
 Co Occurring Collaborative Serving Maine Expanding Medication Assisted Recovery Services & Building a Stronger Recovery Oriented System for SUD Treatment in Maine April 2018 Introduction: With support
Co Occurring Collaborative Serving Maine Expanding Medication Assisted Recovery Services & Building a Stronger Recovery Oriented System for SUD Treatment in Maine April 2018 Introduction: With support
Bridging the Gap Between Crisis and Care: How to Effectively Integrate Psychiatric Emergency Care Within a Community Hospital Emergency Department.
 Bridging the Gap Between Crisis and Care: How to Effectively Integrate Psychiatric Emergency Care Within a Community Hospital Emergency Department. Jeannine Loucks, MSN, RN BC PMHN Laura Derr, BSN, RN
Bridging the Gap Between Crisis and Care: How to Effectively Integrate Psychiatric Emergency Care Within a Community Hospital Emergency Department. Jeannine Loucks, MSN, RN BC PMHN Laura Derr, BSN, RN
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November 2017
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Justice-Involved Veterans
 Justice-Involved Veterans Jessica Blue-Howells, LCSW National Coordinator, Health Care for Reentry Veterans National Program Manager, Project CHALENG May 2014 Agenda Who are justice involved Veterans Why
Justice-Involved Veterans Jessica Blue-Howells, LCSW National Coordinator, Health Care for Reentry Veterans National Program Manager, Project CHALENG May 2014 Agenda Who are justice involved Veterans Why
Medicaid and the. Bus Pass Problem
 Medicaid and the Bus Pass Problem PRESENTED BY: Cardinal Innovations Healthcare Richard F. Topping, Chief Executive Officer Leesa Bain, Vice President, Care Coordination & Quality Management September
Medicaid and the Bus Pass Problem PRESENTED BY: Cardinal Innovations Healthcare Richard F. Topping, Chief Executive Officer Leesa Bain, Vice President, Care Coordination & Quality Management September
An Update on Our Work
 An Update on Our Work Improving the psychiatric crisis and emergency services system in Central Ohio Franklin County Psychiatric Crisis and Emergency System Task Force (PCES) May 2017 The need for emergency
An Update on Our Work Improving the psychiatric crisis and emergency services system in Central Ohio Franklin County Psychiatric Crisis and Emergency System Task Force (PCES) May 2017 The need for emergency
Nevada County Behavioral Health. Crisis, Access, and Linkage Services. Welfare & Institutions Code Section 5150 et al.
 Nevada County Behavioral Health Crisis, Access, and Linkage Services Welfare & Institutions Code Section 5150 et al. Darryl Quinn, PhD Program Manager Adult Services Nevada County Behavioral Health Joy
Nevada County Behavioral Health Crisis, Access, and Linkage Services Welfare & Institutions Code Section 5150 et al. Darryl Quinn, PhD Program Manager Adult Services Nevada County Behavioral Health Joy
Transforming Healthcare Delivery, the Challenges for Behavioral Health
 Transforming Healthcare Delivery, the Challenges for Behavioral Health Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: mtmserve@aol.com
Transforming Healthcare Delivery, the Challenges for Behavioral Health Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: mtmserve@aol.com
National Association of State Mental Health Program Directors Research Institute
 Goal: 100% of Consumers have access without delay to the most appropriate 24/7 emergency, crisis stabilization, inpatient or recovery bed: Lessons Learned from States with On-Line Registries of Available
Goal: 100% of Consumers have access without delay to the most appropriate 24/7 emergency, crisis stabilization, inpatient or recovery bed: Lessons Learned from States with On-Line Registries of Available
EMERGENCY PSYCHIATRY PROCESSES AND PROCEDURES
 EMERGENCY PSYCHIATRY PROCESSES AND PROCEDURES 1. On Call Team and Coverage a. The on call team consists of a junior resident, senior resident and staff psychiatrist. There is also usually a clinical clerk.
EMERGENCY PSYCHIATRY PROCESSES AND PROCEDURES 1. On Call Team and Coverage a. The on call team consists of a junior resident, senior resident and staff psychiatrist. There is also usually a clinical clerk.
CRISIS INTERVENTION SERVICES
 Erie County Medical Center Corporation RFP # 21809 Addendum Number 1 Erie County Medical Center Corporation Addendum Number 1 to RFP # 21809 CRISIS INTERVENTION SERVICES The deadline for submission still
Erie County Medical Center Corporation RFP # 21809 Addendum Number 1 Erie County Medical Center Corporation Addendum Number 1 to RFP # 21809 CRISIS INTERVENTION SERVICES The deadline for submission still
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
Cenpatico Crisis Protocol for Yuma County
 2015-2016 Cenpatico Crisis Protocol for Yuma County Table of Contents Overview & Purpose:... 1 Definitions... 2 Crisis During Business Hours... 6 Crisis Services... 7 The NurseWise Crisis Line... 7 Crisis
2015-2016 Cenpatico Crisis Protocol for Yuma County Table of Contents Overview & Purpose:... 1 Definitions... 2 Crisis During Business Hours... 6 Crisis Services... 7 The NurseWise Crisis Line... 7 Crisis
IV. Clinical Policies and Procedures
 A. Introduction The role of ValueOptions NorthSTAR is to coordinate the delivery of clinical services. There are three parties to this care coordination process: the Enrollee, the Provider(s), and the
A. Introduction The role of ValueOptions NorthSTAR is to coordinate the delivery of clinical services. There are three parties to this care coordination process: the Enrollee, the Provider(s), and the
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE. Tennessee Primary Care Association Annual Conference October 25 26, 2012.
 IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
INTEGRATED CASE MANAGEMENT ANNEX A
 INTEGRATED CASE MANAGEMENT ANNEX A NAME OF AGENCY: CONTRACT NUMBER: CONTRACT TERM: TO BUDGET MATRIX CODE: 32 This Annex A specifies the Integrated Case Management services that the Provider Agency is authorized
INTEGRATED CASE MANAGEMENT ANNEX A NAME OF AGENCY: CONTRACT NUMBER: CONTRACT TERM: TO BUDGET MATRIX CODE: 32 This Annex A specifies the Integrated Case Management services that the Provider Agency is authorized
FAQs: Judge Guy Herman Center for Mental Health Crisis Care
 FAQs: Judge Guy Herman Center for Mental Health Crisis Care A new approach to psychiatric crisis care in Travis County Integral Care offers a new type of mental health crisis care for adults living in
FAQs: Judge Guy Herman Center for Mental Health Crisis Care A new approach to psychiatric crisis care in Travis County Integral Care offers a new type of mental health crisis care for adults living in
FY 2016 PERFORMANCE PLAN
 Program Purpose Program Information PM1: How much did we do? FY 2016 PERFORMANCE PLAN BHD/CSE Alexis Mapes, x4889 Leslie Weisman, x4888 Maintain safety of individuals experiencing mental health crises
Program Purpose Program Information PM1: How much did we do? FY 2016 PERFORMANCE PLAN BHD/CSE Alexis Mapes, x4889 Leslie Weisman, x4888 Maintain safety of individuals experiencing mental health crises
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2
 Program Grantees: Part 2") SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
Acute Psychiatry Solutions
 Acute Psychiatry Solutions Expert care when patients need it most We believe psychiatric emergencies are medical emergencies. We also believe the best psychiatric care is delivered when patients are treated
Acute Psychiatry Solutions Expert care when patients need it most We believe psychiatric emergencies are medical emergencies. We also believe the best psychiatric care is delivered when patients are treated
Defining the Nathaniel ACT ATI Program
 Nathaniel ACT ATI Program: ACT or FACT? Over the past 10 years, the Center for Alternative Sentencing and Employment Services (CASES) has received national recognition for the Nathaniel Project 1. Initially
Nathaniel ACT ATI Program: ACT or FACT? Over the past 10 years, the Center for Alternative Sentencing and Employment Services (CASES) has received national recognition for the Nathaniel Project 1. Initially
n/a n/a n/a n/a CEO Engage in professional search firms to recruit additional FNP s and additional primary care physicians CEO
 Identified Priority Area: Access to Care Plan not to address: Provider reimbursement, high deductible plans/ co-pay costs/ lack of health insurance The hospital does not have the ability to change reimbursement
Identified Priority Area: Access to Care Plan not to address: Provider reimbursement, high deductible plans/ co-pay costs/ lack of health insurance The hospital does not have the ability to change reimbursement
STATE OF KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES OSAWATOMIE STATE HOSPITAL OPERATIONS ASSESSMENT EXECUTIVE SUMMARY
 STATE OF KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES OSAWATOMIE STATE HOSPITAL OPERATIONS ASSESSMENT Prepared by: THE BUCKLEY GROUP, L.L.C. OVERVIEW The Osawatomie State Hospital (OSH) in Osawatomie
STATE OF KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES OSAWATOMIE STATE HOSPITAL OPERATIONS ASSESSMENT Prepared by: THE BUCKLEY GROUP, L.L.C. OVERVIEW The Osawatomie State Hospital (OSH) in Osawatomie
Mental Health
 Mental Health - 23 - Mental Health The Legislative Budget Board estimates that the 2016-2017 General Appropriations Act allocates $3.6 billion to behavioral health (mental health and substance use) services.
Mental Health - 23 - Mental Health The Legislative Budget Board estimates that the 2016-2017 General Appropriations Act allocates $3.6 billion to behavioral health (mental health and substance use) services.
Arizona Department of Corrections
 Arizona Department of Corrections March 5, 2016 Nicole Taylor, J.D., Ph.D. Arizona Department of Corrections VISION Safer communities through effective corrections. MISSION To serve and protect the people
Arizona Department of Corrections March 5, 2016 Nicole Taylor, J.D., Ph.D. Arizona Department of Corrections VISION Safer communities through effective corrections. MISSION To serve and protect the people
SAMHSA Expert Panel on Best Practices in Statewide Real-time Crisis Bed Databases
 SAMHSA Expert Panel on Best Practices in Statewide Real-time Crisis Bed Databases David Morrissette, PhD, LCSW Captain, US Public Health Service Office of the Chief Medical Officer Substance Abuse and
SAMHSA Expert Panel on Best Practices in Statewide Real-time Crisis Bed Databases David Morrissette, PhD, LCSW Captain, US Public Health Service Office of the Chief Medical Officer Substance Abuse and
Grady Health System, Atlanta GA. Upstream Crisis Intervention
 2014 Changes EMS Leadership Conference Augusta, Ga Grady Health System, Atlanta GA. Upstream Crisis Intervention Michael Colman, MPA, NRP, Director of EMS Operations at Grady Health Systems Arthur H. Yancey,
2014 Changes EMS Leadership Conference Augusta, Ga Grady Health System, Atlanta GA. Upstream Crisis Intervention Michael Colman, MPA, NRP, Director of EMS Operations at Grady Health Systems Arthur H. Yancey,
What s the BIG DEAL? Behavioral Health Integration Throughout the Continuum
 What s the BIG DEAL? Behavioral Health Integration Throughout the Continuum NCAHQ April 5, 2017 Monica Cooke MA, RNC, CPHQ, CPHRM, FASHRM Quality Plus Solutions LLC Objectives Describe the prevalence of
What s the BIG DEAL? Behavioral Health Integration Throughout the Continuum NCAHQ April 5, 2017 Monica Cooke MA, RNC, CPHQ, CPHRM, FASHRM Quality Plus Solutions LLC Objectives Describe the prevalence of
Division of Mental Health, Developmental Disabilities & Substance Abuse Services NC Mental Health and Substance Use Service Array Survey
 Table 1 Service Name Include any subcategories of service on a separate line In Table 2, please add service description and key terms Outpatient Treatment Behavioral Health Urgent Care (a type of outpatient)
Table 1 Service Name Include any subcategories of service on a separate line In Table 2, please add service description and key terms Outpatient Treatment Behavioral Health Urgent Care (a type of outpatient)
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August 2016
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August By: Terry Dentoni, MSN, RN, CNL, SFGH Chief Nursing Officer 1. Professional Nursing..1 2. Emergency Department
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August By: Terry Dentoni, MSN, RN, CNL, SFGH Chief Nursing Officer 1. Professional Nursing..1 2. Emergency Department
Nathaniel Assertive Community Treatment: New York County Alternative to Incarceration Program. May 13, 2011 ACT Roundtable Meeting
 Nathaniel Assertive Community Treatment: New York County Alternative to Incarceration Program May 13, 2011 ACT Roundtable Meeting Consumer Characteristics Average Age 43 Male 84% African American 60% Latino
Nathaniel Assertive Community Treatment: New York County Alternative to Incarceration Program May 13, 2011 ACT Roundtable Meeting Consumer Characteristics Average Age 43 Male 84% African American 60% Latino
Border Region Mental Health & Mental Retardation Community Center Adult Jail Diversion Action Plan FY
 ATTACHMENT 3 b Border Region Mental Health & Mental Retardation Community Center Adult Jail Diversion Action Plan FY 2010086 The Border Region MHMR Community Center developed a Jail Diversion Plan for
ATTACHMENT 3 b Border Region Mental Health & Mental Retardation Community Center Adult Jail Diversion Action Plan FY 2010086 The Border Region MHMR Community Center developed a Jail Diversion Plan for
Clinical Operations in a Service Line Model
 Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line Development Jill Castaneda Project Manager,
Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line Development Jill Castaneda Project Manager,
CCBHCs 101: Opportunities and Strategic Decisions Ahead
 CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
Taming Length of Stay Challenges Through Analytics
 Taming Length of Stay Challenges Through Analytics March 3, 2016 Dr. Michelle Pezzani, Medical Director Utilization Management at El Camino Hospital & Palo Alto Medical Foundation (PAMF) Petrina Griesbach
Taming Length of Stay Challenges Through Analytics March 3, 2016 Dr. Michelle Pezzani, Medical Director Utilization Management at El Camino Hospital & Palo Alto Medical Foundation (PAMF) Petrina Griesbach
Mental Health Board Member Orientation & Training
 1 Mental Health Board Member Orientation & Training See Tab 1 Mental Health Timeline 1957 Sources: California Legislative Analyst Office & California Department of Health Care Services to Prior to 1957
1 Mental Health Board Member Orientation & Training See Tab 1 Mental Health Timeline 1957 Sources: California Legislative Analyst Office & California Department of Health Care Services to Prior to 1957
Forensic Assertive Community Treatment Team (FACT) A bridge back to the community for people with severe mental illness
 A bridge back to the community for people with severe mental illness") Forensic Assertive Community Treatment Team (FACT) A bridge back to the community for people with severe mental illness Gary Morse, Ph.D. Katie Thumann, L.C.S.W. Places for People: Community Alternatives
Forensic Assertive Community Treatment Team (FACT) A bridge back to the community for people with severe mental illness Gary Morse, Ph.D. Katie Thumann, L.C.S.W. Places for People: Community Alternatives
EMERGENCY SERVICES PROGRAM (ESP)
") EMERGENCY SERVICES PROGRAM (ESP) Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally,
EMERGENCY SERVICES PROGRAM (ESP) Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally,
INTEGRATED CRISIS RESPONSE SYSTEM (ICRS) TRAINING MODULE
 TRAINING MODULE") North Sound Behavioral Health Organization, LLC 301 Valley Mall Way, Suite 110, Mount Vernon, WA 98273 http://northsoundbho.org 360.416.7013 800.684.3555 Fax 360.416.7017 INTEGRATED CRISIS RESPONSE SYSTEM
North Sound Behavioral Health Organization, LLC 301 Valley Mall Way, Suite 110, Mount Vernon, WA 98273 http://northsoundbho.org 360.416.7013 800.684.3555 Fax 360.416.7017 INTEGRATED CRISIS RESPONSE SYSTEM
Integrated Behavioral Health Services
 Integrated Behavioral Health Services Anitra Walker, LCSW Liz Frye, MD, MPH Integrated Behavioral Health Background SHLI Integrated Care Initiative started in July 2011 2 initial demonstration sites; Focus
Integrated Behavioral Health Services Anitra Walker, LCSW Liz Frye, MD, MPH Integrated Behavioral Health Background SHLI Integrated Care Initiative started in July 2011 2 initial demonstration sites; Focus
Stakeholder input is gathered in several ways. Patients are given the opportunity to provide feedback, the SWOT analysis is based on information from
 Strategic Plan 27 Executive Summary The following is a summary of the information shared in this Operations Review and Plan. This plan highlights operational achievements and challenges, clinical outcomes
Strategic Plan 27 Executive Summary The following is a summary of the information shared in this Operations Review and Plan. This plan highlights operational achievements and challenges, clinical outcomes
MBHP Massachusetts Emergency Services Program Overview Presentation. August 2016
 MBHP Massachusetts Emergency Services Program Overview Presentation August 2016 Emergency Services Program (ESP) Mission and Purpose The Mission of ESP is to: Deliver high-quality, culturally competent,
MBHP Massachusetts Emergency Services Program Overview Presentation August 2016 Emergency Services Program (ESP) Mission and Purpose The Mission of ESP is to: Deliver high-quality, culturally competent,
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives
 Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
The Reduction of Seclusion & Restraint in the University of Michigan Psychiatric Emergency Services with the Introduction of 24/7 Nurse Staffing
 The Reduction of Seclusion & Restraint in the University of Michigan Psychiatric Emergency Services with the Introduction of 24/7 Nurse Staffing Sharon P. Stetz MSN Marvella M. Muzik, MS PMHNP, BC Objectives
The Reduction of Seclusion & Restraint in the University of Michigan Psychiatric Emergency Services with the Introduction of 24/7 Nurse Staffing Sharon P. Stetz MSN Marvella M. Muzik, MS PMHNP, BC Objectives
Leaving No Veteran Behind: The Policy Implications Identified at the 5th Annual Justice Involved Veterans Conference. Andrew Keller, PhD May 14, 2014
 Leaving No Veteran Behind: The Policy Implications Identified at the 5th Annual Justice Involved Veterans Conference Andrew Keller, PhD May 14, 2014 About the Meadows Mental Health Policy Institute Our
Leaving No Veteran Behind: The Policy Implications Identified at the 5th Annual Justice Involved Veterans Conference Andrew Keller, PhD May 14, 2014 About the Meadows Mental Health Policy Institute Our
WAY BEHIND: Report on the State of Mental Health in 2014 DMH Budget: Last in Growth in New England since 2009
 WAY BEHIND: Report on the State of Mental Health in 2014 Authored by Caity Stuhan, Intern, Graduate Student at Harvard School of Public Health Revised Edition: May 27, 2014 In 2009, the National Alliance
WAY BEHIND: Report on the State of Mental Health in 2014 Authored by Caity Stuhan, Intern, Graduate Student at Harvard School of Public Health Revised Edition: May 27, 2014 In 2009, the National Alliance
Accomplishments and Challenges in Medicaid Mental Health Services
 Accomplishments and Challenges in Medicaid Mental Health Services Innovation, Financing and Change June 5, 2008 Richard H. Dougherty, Ph.D. Accomplishments There has been significant reductions in state
Accomplishments and Challenges in Medicaid Mental Health Services Innovation, Financing and Change June 5, 2008 Richard H. Dougherty, Ph.D. Accomplishments There has been significant reductions in state
APNA 27th Annual Conference Session 3023: October 11, 2013
 Beth Phoenix, RN, PhD Aaron Miller, RN, MS, PMHNP Sherri Borden, RN, MS, ANP Matt Tierney, RN, MS, NP UCSF School of Nursing None of the presenters has any conflicts of interest to disclose Beth Phoenix,
Beth Phoenix, RN, PhD Aaron Miller, RN, MS, PMHNP Sherri Borden, RN, MS, ANP Matt Tierney, RN, MS, NP UCSF School of Nursing None of the presenters has any conflicts of interest to disclose Beth Phoenix,
LOUISIANA MEDICAID LEVEL OF CARE GUIDELINES
 Optum By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) LOUISIANA MEDICAID LEVEL OF CARE GUIDELINES Effective
Optum By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) LOUISIANA MEDICAID LEVEL OF CARE GUIDELINES Effective
 Relationships: The Behavioral Health Consultant, Primary Care Physician, and Psychiatrist i t Healthcare Integration Webinar National Council for Community Behavioral Healthcare February 25, 2010 The Status
Relationships: The Behavioral Health Consultant, Primary Care Physician, and Psychiatrist i t Healthcare Integration Webinar National Council for Community Behavioral Healthcare February 25, 2010 The Status
David Folsom, MD, MPH Medical Director St. Vincent de Paul Village Associate Professor Psychiatry and Family Medicine UC San Diego
 David Folsom, MD, MPH Medical Director St. Vincent de Paul Village Associate Professor Psychiatry and Family Medicine UC San Diego Describe need for programs targeting homeless high utilizers of emergency
David Folsom, MD, MPH Medical Director St. Vincent de Paul Village Associate Professor Psychiatry and Family Medicine UC San Diego Describe need for programs targeting homeless high utilizers of emergency
The Integration of Behavioral Health and Primary Care: A Leadership Perspective
 The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
-OPTUM PIERCE BEHAVIORAL HEALTH ORGANIZATION
 -OPTUM PIERCE BEHAVIORAL HEALTH ORGANIZATION CARE MANAGEMENT AND SERVICE PLANNING POLICY Policy: CM-10 Section: Care Management and Service Planning Approved by Bea Dixon, Executive Director Effective
-OPTUM PIERCE BEHAVIORAL HEALTH ORGANIZATION CARE MANAGEMENT AND SERVICE PLANNING POLICY Policy: CM-10 Section: Care Management and Service Planning Approved by Bea Dixon, Executive Director Effective
Harris County Mental Health Jail Diversion Program Harris County Sequential Intercept Model
 Harris County Mental Health Jail Diversion Program Harris County Sequential Intercept Model 12/31/2015 1 Harris County Mental Health Jail Diversion Program Sequential Intercept Model The Sequential Intercept
Harris County Mental Health Jail Diversion Program Harris County Sequential Intercept Model 12/31/2015 1 Harris County Mental Health Jail Diversion Program Sequential Intercept Model The Sequential Intercept
Community-Based Psychiatric Nursing Care
 Community-Based Psychiatric Nursing Care 1 The goal of the mental health delivery system is to help people who have experienced a psychiatric illness live successful and productive lives in the community
Community-Based Psychiatric Nursing Care 1 The goal of the mental health delivery system is to help people who have experienced a psychiatric illness live successful and productive lives in the community
Louisville Metro Police Department: A Review of Our Crisis Intervention Team and De-escalation Training
 Louisville Metro Police Department: A Review of Our Crisis Intervention Team and De-escalation Training Executive Summary Due to various high profile incidents around the country, on December 18, 2014,
Louisville Metro Police Department: A Review of Our Crisis Intervention Team and De-escalation Training Executive Summary Due to various high profile incidents around the country, on December 18, 2014,
The North Carolina Behavioral Health Crisis Referral System
 The North Carolina Behavioral Health Crisis Referral System Krista Ragan, MA BH-CRSys Program Manager, NC Division of Mental Health, Developmental Disabilities & Substance Abuse Services November 6 th,
The North Carolina Behavioral Health Crisis Referral System Krista Ragan, MA BH-CRSys Program Manager, NC Division of Mental Health, Developmental Disabilities & Substance Abuse Services November 6 th,
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES
 EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
Behavioral Wellness. Garden Fountain by Bridget Hochman BUDGET & FULL-TIME EQUIVALENTS SUMMARY & BUDGET PROGRAMS CHART
 Garden Fountain by Bridget Hochman BUDGET & FULL-TIME EQUIVALENTS SUMMARY & BUDGET PROGRAMS CHART Operating $ 109,040,762 Capital $ 46,000 FTEs 432.10 Alice Gleghorn, PhD Director Administration & Support
Garden Fountain by Bridget Hochman BUDGET & FULL-TIME EQUIVALENTS SUMMARY & BUDGET PROGRAMS CHART Operating $ 109,040,762 Capital $ 46,000 FTEs 432.10 Alice Gleghorn, PhD Director Administration & Support
MAGELLAN UNIVERSAL SERVICES LIST - Includes Preferred HIPAA Compliant Codes. UB-04 Revenue Codes
 Service Name & Detailed Magellan Description (see column heading explanations at end of this document) MAGELLAN UNIVERSAL SERVICES LIST - Includes Preferred HIPAA Compliant Codes Codes Used to Determine
Service Name & Detailed Magellan Description (see column heading explanations at end of this document) MAGELLAN UNIVERSAL SERVICES LIST - Includes Preferred HIPAA Compliant Codes Codes Used to Determine