On the CUSP: STOP CAUTI. Teamwork & Reducing CAUTI in the Emergency Department
|
|
|
- Beatrix Carpenter
- 6 years ago
- Views:
Transcription
1 On the CUSP: STOP CAUTI Teamwork & Reducing CAUTI in the Emergency Department Indiana HEN May 1, 2014 Eugene S. Chu, MD, FHM Director of Hospital Medicine Boulder Community Hospital Associate Clinical Professor of Medicine University of Colorado School of Medicine 1
2 Objectives Understand how teamwork improves health care outcomes Learn teamwork theory Apply teamwork and culture change theory to decreasing CAUTI in the Emergency Department 2
3 Project Overview Project Goals for CAUTI are to: 1. reduce mean CAUTI rates in participating clinical units by 25 percent; and 2. improve safety culture as evidenced by improved teamwork and communication by employing CUSP methodology.

4 Positive Outcomes of Effective Teamwork on Health Care Reduced length of stay Higher quality of care Better patient outcomes Greater ability to meet family member needs Improved patient experience with care scores Lower nurse turnover Shortell SM, Marstellar JA, Lin M et al. The role of perceived team effectiveness in improving chronic illness care. Med Care 2004 Nov; 42:

5 Communication in Health Care
6 6 Coordination of Care
7 % of respondents reporting above adequate teamwork Physicians and RN Collaboration % 88% 90% 93% % 48% 54% 59% L&D RN/MD ICU RN/MD OR RN/Surg CRNA/Anesth RN rates Physician Physician rates RN L&D RN/OB OR RN/Surgeon ICU RN/MD CRNA/Anesthesiologist
8 Teamwork Disconnect MD: Good teamwork means the nurse does what I say RN: Good teamwork means I am asked for my input 8



9 % of respondents reporting above adequate teamwork The strongest predictor of clinical excellence: caregivers feel comfortable speaking up if they perceive a problem with patient care No BSI = 5 months or more w/ zero No BSI 21% No BSI 31% No BSI 44% Health Services Research, 2006;41(4 Part II): % of respondents within an ICU reporting good teamwork climate Teamwork Climate Across Michigan ICUs
10 % reporting positive teamwork climate TEAMWORK CLIMATE & ANNUAL NURSE TURNOVER High Turnover 16.0% Mid Turnover10.8% 10 Low Turnover 7.9%
11 Barriers Frankly, our health care professionals are not trained to be team members, they are trained to be individual heroes. - John Troussaint, MD President and CEO ThedaCare, Inc.
12 Objectives Understand how teamwork improves health care outcomes Learn teamwork theory Apply teamwork and culture change theory to decreasing CAUTI in the Emergency Department 12
13 Exercise Think of a high performing team you have either been a part of or witnessed in action. 13
14 High Performance Teams Trivia
15 What is the name of this team? A.The Fantastic Four B.The X-Men C.The Avengers D.The Super Friends
16 What is the name of this team? A.The Fantastic Four B.The X-Men C.The Avengers D.The Super Friends



17
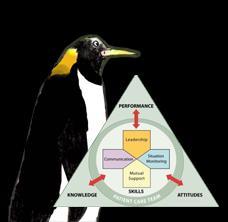
18 Characteristics Common Purpose Clear Roles Accepted Leadership Effective Processes Solid Relationships Excellent Communication Thiel D. A process to build high performance teams. 2007
19 Productivity/Performance Stages of Team Development Forming Sign up Little understanding of mission Roles and Responsibiities unclear No processes Dependent on leaderdirective Storming Sort it out Uncertainties on purpose persist Team members vie for position Power struggles Decisions difficult Leader critical Norming Focus Commitment and unity strong Roles and Resp clear/accepted Agreement on big decisions Develop processes Leader facilitates Performing Deliver Cohesion and pride Shared Vision and Independent Focus on overachieving goals Make most decisions and deal with issues internally Breakeven Whole = parts 19 Time
20 Common Purpose Clear Relevant Achievable Significant Urgent Thiel D. A process to build high performance teams. 2007



21 What is our purpose? Clear Relevant Achievable Significant Urgent Thiel D. A process to build high performance teams. 2007
22 Clear Roles Design Division Deployment Discussion Thiel D. A process to build high performance teams. 2007
23 Key Roles and Responsibilities to Prevent CAUTI Role or Responsibility Project coordinator Nurse champion (engage and educate nursing personnel, implement nursing processes) Physician champion (engage and educate medical personnel, implement physician processes) Data collection, monitoring, reporting Example of Personnel to Consider IP, quality manager, nurse manager, nurse educator Bedside nurse, nurse educator, unit manager, charge nurse Urologist, ID physician, hospital epidemiologist, hospitalist Infection preventionist, quality manager, utilization manager (Modified from
24 Accepted Leadership Appreciate collective intelligence Believe in the power of diversity See leadership as a service Thiel D. A process to build high performance teams. 2007
25 Quiz
26 Which team would you pick to defend Earth? A B C D E
27 Which team would you pick to defend Earth? A B C D E

28 Effective Processes Working Processes Thinking Processes Thiel D. A process to build high performance teams. 2007
29 Excellent Communication Fast I PASS the BATON S Clear Timely Accurate Straight Talk H U D D L E SBAR SAIF-IR Read Back O A P Thiel D. A process to build high performance teams. 2007


30 Four Key Components of Effective Communication 1 Complete Clear Brief Timely As seen in TeamSTEPPS 30
31 Solid Relationships Trust Acceptance Understanding Respect Courtesy Thiel D. A process to build high performance teams. 2007
32 Which is the sine qua non of solid relationships? Trust Acceptance Understanding Respect Courtesy Simply put, trust means confidence. The opposite of trust distrust is suspicion. Stephen MR Covey The Speed of Trust Thiel D. A process to build high performance teams. 2007
33 Productivity/Performa nce Stages of Team Development Forming Sign up Little understanding of mission Roles and Responsibiities unclear No processes Dependent on leaderdirective Storming Sort it out Uncertainties on purpose persist Team members vie for position Power struggles Decisions difficult Leader critical Norming Focus Commitment and unity strong Roles and Resp clear/accepted Agreement on big decisions Develop processes Leader facilitates Performing Deliver Cohesion and pride Shared Vision and Independent Focus on overachieving goals Make most decisions and deal with issues internally Breakeven Whole = parts 33 Time
34 Characteristics Common Purpose Clear Roles Accepted Leadership Effective Processes Solid Relationships Excellent Communication Team members are so devoted to their purpose that they will surmount any barrier to achieve the team's goals. Katzenbach et al.: The Wisdom of Teams, HarperBusiness, 2003
35 Objectives Understand how teamwork improves health care outcomes Learn teamwork theory Apply teamwork and culture change theory to decreasing CAUTI in the Emergency Department 35
36 The CAUTI Emergency Department Improvement Intervention What is the On the CUSP: STOP CAUTI ED Improvement Intervention? Expanding the reach of the On the CUSP: STOP CAUTI national collaborative Instilling a culture of partnership between emergency departments and in-patient units Broadening exposure to national experts Emergency Nurses Association (ENA) American College of Emergency Physicians (ACEP) 36
37 ED Improvement Intervention Goals: Best practice techniques for CAUTI Prevention Technical change (Process): Determine catheter appropriateness Preventing unnecessary placement Promoting compliance with institutional guidelines Promoting proper insertion techniques Culture change (CUSP): Teamwork and communication amongst frontline staff Identify nurse and physician champions for leadership and buy-in Collaboration with in-patient units 37







38 Opportunities for Improvement: Multi-disciplinary and Multi-departmental Efforts PACU/OR Follow criteria for placement in the OR Remove promptly after surgery before transfer out if appropriate ICU Evaluate for continued need Discontinue no longer needed before transfer out Non-ICU Evaluate need on admission Evaluate for continued need ED Avoid initial placement Reevaluate for continued need after patient stabilizes
39 CAUTI Culture in the ED CAUTI Indications Orders HICPAC Insertion and Maintenance Technique Competency Removal Process Structure 39
40 Can you get people to start behaving in a new way? educate engage execute and evaluate 40

41 Case Scenario educate engage 41
42 CAUTI effects mortality by OR 1.99 ICU LOS by 12 days non-icu LOS by 21 days 42 Crit Care Med May;39(5): Relationship of catheter-associated urinary tract infection to mortality and length of stay in critically ill patients: a systematic review and meta-analysis of observational studies. Chant C 1, Smith OM, Marshall JC, Friedrich JO.
43 Can you get people to start behaving in a new way? educate engage execute and evaluate 43
44 Appropriate Indications for Indwelling Appropriate Indications Urinary Catheter Use Patient has acute urinary retention or obstruction Need for accurate measurements of urinary output in critically ill patients. Perioperative use for selected procedures: urologic surgery or other surgery on contiguous structures of genitourinary tract, anticipated prolonged surgery duration (removed in post-anesthesia unit), anticipated to receive large-volume infusions or diuretics in surgery, operative patients with urinary incontinence, need to intraoperative monitoring of urinary output. To assist in healing of open sacral or perineal wounds in incontinent patients. Requires prolonged immobilization (e.g., potentially unstable thoracic or lumbar spine) To improve comfort for end of life care if needed. Gould C, et al. Infect Control Hosp Epidemiol 2010;31:






45 Common Conditions where the UC is Placed Inappropriately Elderly (especially women) Immobility Incontinence Physician and Nurse Practice 45 Morbid obesity? Inappropriate Catheter Placement Use in noncritically ill cardiac and renal patients Debility
46 Common Patterns of ED Urinary Catheter Misuse Measuring urine output in stable patients CHF Assessing bladder volume Urinary retention from spinal injury Protocolized care for trauma Incontinence without open sacral or perineal wounds Pre-operative Mental status Delirium Dementia Existing catheter use 46
47 educate Issues to Clarify A chronic indwelling UC present on admission to the ED would not be counted as engage placed in the ED (even if the catheter is changed there). Some patients have a UC upon admission, prior to presentation to the ED (for example, obstructive uropathy). Again, these may represent appropriate indications for utilization, but would not be counted as originally placed in the ED. 47
48 Examples of Common Conditions where Catheter May Be Placed Inappropriately Who is Critically Ill? Admitted to ICU Requiring high amounts of Oxygen (e.g., >4 liters, >6 liters, or on 100% O2 nonrebreather)? Emergent Pelvic Ultrasound for Pregnancy? Placing UC would increase the risk for introducing bacteria to the bladder. Patients can drink fluids and will have a full bladder without risk. It is usually an issue with workflow in the ED. Unconsciousness versus Agitation Agitated patients may have a higher risk of trauma related to UC, if placed. Evaluate whether you have any standing orders for UC placement as a part of the treatment of acute stroke. Frail and Immobile patients The UC reduces mobility, and makes patients at a higher risk for pressure ulcers. Frail patients may become more deconditioned with a UC and infectious complications (CAUTI) may result in poor outcomes. 48
49 CAUTI Myths Facilitates I/O measurement Alternatives are available with less risk (e.g., urinals, daily weights) Prevents falls from getting up to urinate Increases risk to fall, especially in the confused patient Protects skin in the incontinent patient Increases risk of skin breakdown from immobility, muscle loss, and catheter-related trauma Saves time for the bedside nurse Extended LOS, infection complications, and other risks, it does not 49
50 Can you get people to start behaving in a new way? educate engage execute and evaluate 50


51 Urinary Catheter Insertion Kits
52
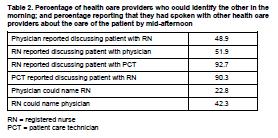
53 Data Collection in the Emergency Department A form is completed by the ED nurse transferring the patient to the hospital unit: 1. Patient with or without catheter 2. Reason for use of catheter (for internal evaluation) 3. If no appropriate reason, nurse to evaluate removal 53
54 54
55 Metrics to Evaluate Improvements Measurement Calculation Required for reporting to national project: ED UC Placement Rate = Optional recommended to internal evaluation: Inappropriately Placed UC Rate Documented Physician Order to Place UC Rate = = (Number of ED admissions with a newly-placed indwelling UC, including observation patients) (Number of ED admits from the ED, including observation patients) (Number of UCs placed in the ED without appropriate indication) (Total number UCs placed in the ED) (Number of UCs placed in the ED without a documented physician s order) (Total number of UCs placed in the ED) X 100 X 100 X





56 Urinary Catheter ED Avengers 1. ED physician champion 2. ED nurse champion 3. Infection Preventionist 4. ICU, Floor, OR? 5. Trauma? 6. Cardiology? 7. Urology? 8. Patient?
57 Characteristics Common Purpose Clear Roles Accepted Leadership Effective Processes Solid Relationships Excellent Communication Team members are so devoted to their purpose that they will surmount any barrier to achieve the team's goals. Katzenbach et al.: The Wisdom of Teams, HarperBusiness, 2003
58 educate Purpose Improve the compliance with the appropriate indications engage for UC placement in the emergency department. Improve the compliance with proper technique for placement. Goal is to have less UCs placed in the ED, contributing to a lower utilization rate throughout inpatient units. 58
59 Characteristics Common Purpose Clear Roles Accepted Leadership Effective Processes Solid Relationships Excellent Communication Team members are so devoted to their purpose that they will surmount any barrier to achieve the team's goals. Katzenbach et al.: The Wisdom of Teams, HarperBusiness, 2003
60 ED Nursing Role Obtain support from ED nurse director, nurse manager, and nurse educator ED nurse champion identified Responsible for peer-to-peer coaching and education Should be an approachable person who is well-versed in ED functions and is available as a resource Educated nursing staff Appropriate indications, alternatives to UC Focused on working with physicians to determine UC necessity (patient-specific, patient-focused) Stressed importance of a corresponding, written physician order
61 ED Physician Role Promote reduction of catheter use by championing appropriateness Encourage interdisciplinary conversation around catheter use Engage other services around patterns of catheter use All urinary catheters require an order Encourage communication at the time of catheter ordering/placement Huddle re: need for catheter Acknowledge nursing s deeper knowledge of patient and ability to care for self 61
62 Infection Preventionist Role Team leader Data collection and entry Facilitate implementation Project coordinator 62
63 Characteristics Common Purpose Clear Roles Accepted Leadership Effective Processes Solid Relationships Excellent Communication Team members are so devoted to their purpose that they will surmount any barrier to achieve the team's goals. Katzenbach et al.: The Wisdom of Teams, HarperBusiness, 2003
64 Champion Roles Share data on catheter use with medical staff Break out by physician if possible Circulate descriptive summaries of any CAUTIs that are attributed to ED placement Communicate with other medical services about specific patterns of care 64
65 Characteristics Common Purpose Clear Roles Accepted Leadership Effective Processes Solid Relationships Excellent Communication Team members are so devoted to their purpose that they will surmount any barrier to achieve the team's goals. Katzenbach et al.: The Wisdom of Teams, HarperBusiness, 2003
66 What is the Process? Physician and nurse evaluate patient. Decision to place a UC based on appropriate indication. Patient s ED nurse reevaluates need for UC and reason for use before transfer to unit. 66


67 Is the patient critically ill and will require accurate output measurement? Other indications for urinary catheter: Urinary retention/obstruction? o Use bladder scanner first Immobilization needed for trauma or surgery? Incontinent with open sacral/perineal wounds? End of life/hospice? Chronic or existing catheter use? o Re-evaluate need and discuss with provider Insert catheter and treat signs of shock: Hypotension Decreased cardiac output/function Decreased renal function Hypovolemia Hemorrhage Re-assess after intervention Do NOT insert Explore alternatives Still critically ill, requiring accurate output measurement? 67 Insert or maintain catheter Remove catheter prior to admission
68 Simplified Insertion Checklist for UC Placement Components of Checklist Hand hygiene before and after procedure? Sterile gloves, drapes, sponges, aseptic sterile solution for cleaning, and single use packet lubricant used? Aseptic insertion technique (no contamination during placement)? Proper securement of urinary catheter postprocedure? Closed drainage system and bag is below patient post-procedure? Yes Compliant Yes, after correction 68
69 Characteristics Common Purpose Clear Roles Accepted Leadership Effective Processes Solid Relationships Excellent Communication Team members are so devoted to their purpose that they will surmount any barrier to achieve the team's goals. Katzenbach et al.: The Wisdom of Teams, HarperBusiness, 2003
70 Relationships and Communication ICU PACU/OR Non-ICU ED
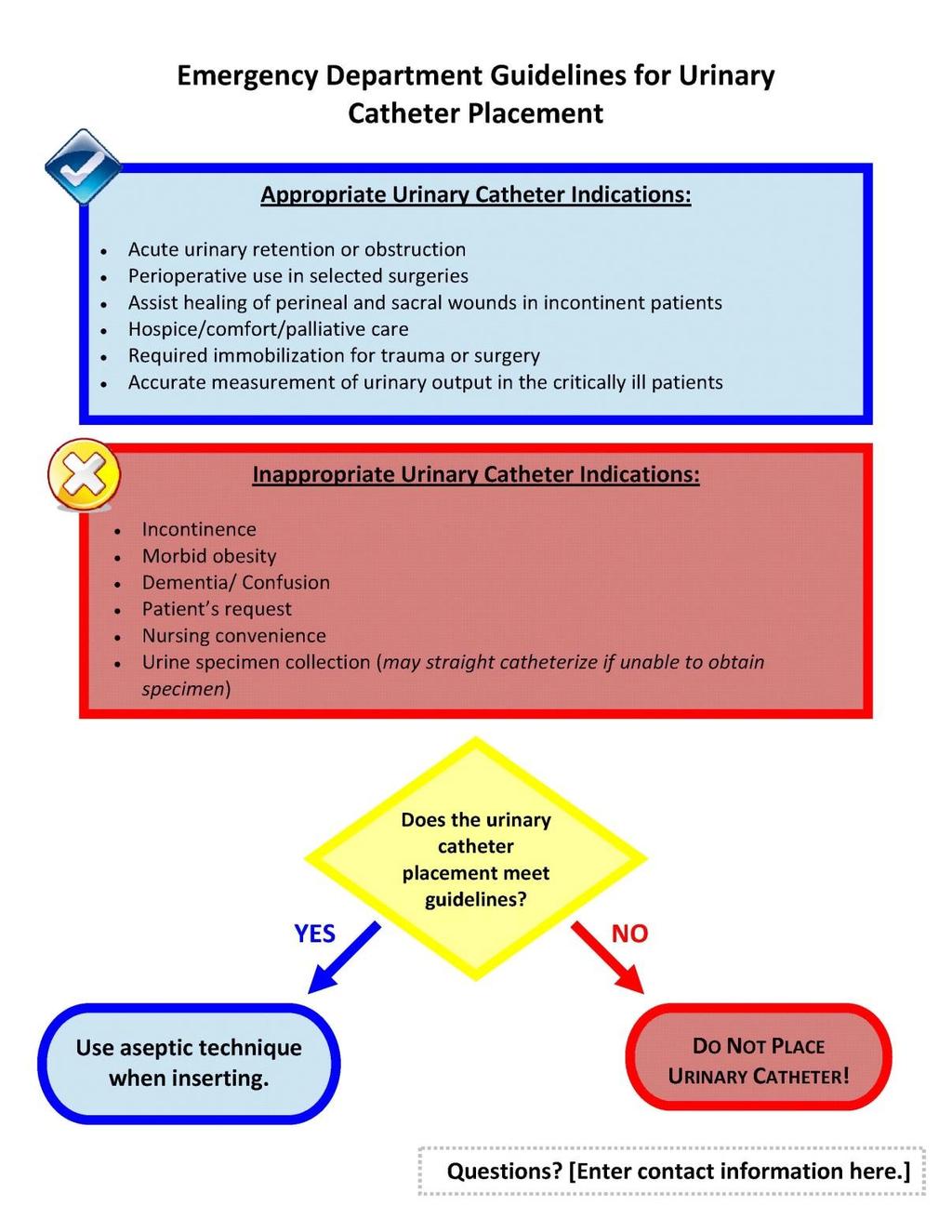
71 How to Spread the Message Pocket cards, posters, lectures, and algorithms describing the appropriate indications. Make sure the information is shared with nurses and nursing assistants, staff physicians, physicians-intraining, and mid-level providers DO NOT PLACE URINARY CATHETERS UNLESS NEEDED! Emergency Department-Specific Guidelines Appropriate Urinary Catheters Indications: Acute urinary retention or obstruction Perioperative use in selected surgeries Assist healing of perineal and sacral wounds in incontinent patients Hospice/ comfort/ palliative care Required immobilization for trauma or surgery Accurate measurement of urinary output in the critically ill patients Urinary catheters may also be used for: Place your additional institutional indications if different from above Always obtain a physician order before placement of a urinary catheter. For questions, please contact [Enter contact information here]. 71

72 What is the Process? Physician and nurse evaluate patient. Decision to place a UC based on appropriate indication. Patient s ED nurse reevaluates need for UC and reason for use before transfer to unit. 72

73 educate engage execute and evaluate 73

74 Example of Success: AH Pilot- 18 EDs (Fakih et al, ID week 2013, abstract 1073) 10% 8% 6% 4% 2% 0% Catheter Placed in ED Baseline Intervention Sustainability Catheter avoidance translates into preventing exposure to the catheter for thousands of patients 100% 80% 60% 40% 20% 0% Reduction in catheter use by a third! The results were sustained for more than 6 months Appropriate reason for placement Baseline Intervention Sustainability 74
75 75 Thank You
Mohamad Fakih, MD, MPH
 Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
CAUTI reduction at Mayo Clinic
 CAUTI reduction at Mayo Clinic Priya Sampathkumar, MD, FIDSA, FSHEA Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester Jean (Wentink) Barth, MPH, RN, CIC Director,
CAUTI reduction at Mayo Clinic Priya Sampathkumar, MD, FIDSA, FSHEA Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester Jean (Wentink) Barth, MPH, RN, CIC Director,
From Defeating CAUTI to Preventing Urinary Catheter Harm
 From Defeating CAUTI to Preventing Urinary Catheter Harm Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University Senior Medical Director, Center of Excellence for Antimicrobial Stewardship
From Defeating CAUTI to Preventing Urinary Catheter Harm Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University Senior Medical Director, Center of Excellence for Antimicrobial Stewardship
Driving CAUTI Rates to ZERO. Nada Nassar, BSN, MSN Nurse Quality Manager-AUBMC
 Driving CAUTI Rates to ZERO Nada Nassar, BSN, MSN Nurse Quality Manager-AUBMC I. Background: 1. Impact of CAUTI Outline 2. Urinary Catheter Use II. FOCUS PI tool for CAUTI 1. Find the problem 2. Organize
Driving CAUTI Rates to ZERO Nada Nassar, BSN, MSN Nurse Quality Manager-AUBMC I. Background: 1. Impact of CAUTI Outline 2. Urinary Catheter Use II. FOCUS PI tool for CAUTI 1. Find the problem 2. Organize
What are the Barriers and Facilitators to Nurses Utilization of a Nurse Driven Protocol for Indwelling Urinary Catheter Removal?
 What are the Barriers and Facilitators to Nurses Utilization of a Nurse Driven Protocol for Indwelling Urinary Catheter Removal? Brenda Clark, BSN, RN, CMSRN Clinical Nurse II Co-chair Interprofessional
What are the Barriers and Facilitators to Nurses Utilization of a Nurse Driven Protocol for Indwelling Urinary Catheter Removal? Brenda Clark, BSN, RN, CMSRN Clinical Nurse II Co-chair Interprofessional
Physician Engagement
 On the CUSP: STOP CAUTI Physician Engagement Mohamad Fakih, MD, MPH St John Hospital and Medical Center Detroit, MI February 7, 2012 Acknowledgments Special thanks to Drs Sanjay Saint and Sarah Krein for
On the CUSP: STOP CAUTI Physician Engagement Mohamad Fakih, MD, MPH St John Hospital and Medical Center Detroit, MI February 7, 2012 Acknowledgments Special thanks to Drs Sanjay Saint and Sarah Krein for
Indwelling Urinary Catheters: A One- Point Restraint?
 Broadcast live from... Outline The Technical & Socio-Adaptive Aspects of Preventing -Associated Urinary Tract Infection Sanjay Saint, MD, MPH George Dock Professor of Internal Medicine Ann Arbor VAMC &
Broadcast live from... Outline The Technical & Socio-Adaptive Aspects of Preventing -Associated Urinary Tract Infection Sanjay Saint, MD, MPH George Dock Professor of Internal Medicine Ann Arbor VAMC &
Our Journey Towards CAUTI Freedom. Johnson City Medical Center
 Our Journey Towards CAUTI Freedom Johnson City Medical Center Objectives List two of the HICPAC appropriate indications for indwelling urinary catheters List two obstacles we encountered that prevented
Our Journey Towards CAUTI Freedom Johnson City Medical Center Objectives List two of the HICPAC appropriate indications for indwelling urinary catheters List two obstacles we encountered that prevented
AHA/HRET HEN 2.0 CAUTI WEBINAR: OVERCOMING BARRIERS TO ASEPTIC CATHETER INSERTION. August 9, :00 a.m. 12:00 p.m. CT
 AHA/HRET HEN 2.0 CAUTI WEBINAR: OVERCOMING BARRIERS TO ASEPTIC CATHETER INSERTION August 9, 2016 11:00 a.m. 12:00 p.m. CT 1 WELCOME AND INTRODUCTIONS Marina Levin, Program Manager HRET 11:00 11:05AM 2
AHA/HRET HEN 2.0 CAUTI WEBINAR: OVERCOMING BARRIERS TO ASEPTIC CATHETER INSERTION August 9, 2016 11:00 a.m. 12:00 p.m. CT 1 WELCOME AND INTRODUCTIONS Marina Levin, Program Manager HRET 11:00 11:05AM 2
Eliminating Catheter-Associated Urinary Tract Infections: Implementing a Quality Improvement Project
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Nurse Driven Foley Removal Protocol. Cathy Moore, MSN, ACNS-BC, CCRN 2009
 Nurse Driven Foley Removal Protocol Cathy Moore, MSN, ACNS-BC, CCRN 2009 Abstract Text Nosocomial urinary tract infections (UTI) are common and costly occurrences for hospitalized patients. Patients may
Nurse Driven Foley Removal Protocol Cathy Moore, MSN, ACNS-BC, CCRN 2009 Abstract Text Nosocomial urinary tract infections (UTI) are common and costly occurrences for hospitalized patients. Patients may
Running head: EBN & CAUTIS 1
 Running head: EBN & CAUTIS 1 Evidence-Based Nursing & Reducing Catheter-Associated Urinary Tract Infections Dana L Knoll Ferris State University EBN & CAUTIS 2 Evidence-Based Nursing & Reducing Catheter-Associated
Running head: EBN & CAUTIS 1 Evidence-Based Nursing & Reducing Catheter-Associated Urinary Tract Infections Dana L Knoll Ferris State University EBN & CAUTIS 2 Evidence-Based Nursing & Reducing Catheter-Associated
Goal Statement: Achieve reduction in CAUTI events by review and implementation of best practices for utilization and management.
 Organization: Medstar Good Samaritan Hospital Title: Call for Action: Prevention of CAUTI in the Acute Care Setting Program/Project Description, including Goals: According to the Centers for Disease Control
Organization: Medstar Good Samaritan Hospital Title: Call for Action: Prevention of CAUTI in the Acute Care Setting Program/Project Description, including Goals: According to the Centers for Disease Control
ICU - Sepsis, CAUTI and CLABSI Less May Be Better. HRET HIIN ICU Virtual Event April 11, 2017
 ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
CAUTI Prevention Case Study
 CAUTI Prevention Case Study University of Missouri Health One Hospital Drive Columbia, Missouri 65212 Primary Contact: Linda S. Johnson, RN, MSN, CIC Manager, Infection Prevention and Control University
CAUTI Prevention Case Study University of Missouri Health One Hospital Drive Columbia, Missouri 65212 Primary Contact: Linda S. Johnson, RN, MSN, CIC Manager, Infection Prevention and Control University
The CAUTI Can-Can. Hennepin County Medical Center August Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion
 Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W.
 Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W.") Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W. Bourg, PhD, RN, TCRN, FAEN Learning Objectives Explain the importance
Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W. Bourg, PhD, RN, TCRN, FAEN Learning Objectives Explain the importance
CAUTI Reduction A Clinton Memorial Presentation
 CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
Exemplary Professional Practice CARE DELIVERY SYSTEM(S)
") Exemplary Professional Practice CARE DELIVERY SYSTEM(S) EP7EO s systematically evaluate professional organizations standards of practice, incorporating them into the organization s professional practice
Exemplary Professional Practice CARE DELIVERY SYSTEM(S) EP7EO s systematically evaluate professional organizations standards of practice, incorporating them into the organization s professional practice
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Kathleen S. Hall-Meyer, RN, MBA, CIC Saint Luke s Health System Kansas City, Missouri
 Kathleen S. Hall-Meyer, RN, MBA, CIC Saint Luke s Health System Kansas City, Missouri Nothing to disclose At the conclusion of this program, the learner will be able to: -Describe how a partnership with
Kathleen S. Hall-Meyer, RN, MBA, CIC Saint Luke s Health System Kansas City, Missouri Nothing to disclose At the conclusion of this program, the learner will be able to: -Describe how a partnership with
Strategies to Prevent Catheter-Associated Urinary Tract Infections in Acute Care Hospitals: 2014 Update
 INFECTION CONTROL A HOSPITAL EPIDEMIOLOGY MAY 2014, VOL. 35, NO. S2 SHEA/lDSA PRACTICE RECOMMEATION Strategies to Prevent Catheter-Associated Urinary Tract Infections in Acute Care Hospitals: 2014 Update
INFECTION CONTROL A HOSPITAL EPIDEMIOLOGY MAY 2014, VOL. 35, NO. S2 SHEA/lDSA PRACTICE RECOMMEATION Strategies to Prevent Catheter-Associated Urinary Tract Infections in Acute Care Hospitals: 2014 Update
Clinical Intervention Overview: Objectives
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
Advanced Measurement for Improvement Prework
 Advanced Measurement for Improvement Prework IHI Training Seminar Boston, MA March 20-21, 2017 Faculty: Richard Scoville PhD; Gareth Parry PhD Thank you for enrolling in IHI s upcoming seminar on designing
Advanced Measurement for Improvement Prework IHI Training Seminar Boston, MA March 20-21, 2017 Faculty: Richard Scoville PhD; Gareth Parry PhD Thank you for enrolling in IHI s upcoming seminar on designing
Critical Thinking Steps
 CAA s = Critical Thinking CAROL SIEM, MSN, RN, BC, GNP Clinical Educator/Team Leader for QIPMO Critical Thinking Steps Recognition/Assessment Gather essential information about the individual Problem definition
CAA s = Critical Thinking CAROL SIEM, MSN, RN, BC, GNP Clinical Educator/Team Leader for QIPMO Critical Thinking Steps Recognition/Assessment Gather essential information about the individual Problem definition
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
CHANGING BEHAVIOR BY DESIGN.
 CHANGING BEHAVIOR BY DESIGN. One Layer IUC Tray Designed to intuitively guide evidenced-based practices Putting Evidence Into Practice. UTI is one of the most common healthcare-associated infections.
CHANGING BEHAVIOR BY DESIGN. One Layer IUC Tray Designed to intuitively guide evidenced-based practices Putting Evidence Into Practice. UTI is one of the most common healthcare-associated infections.
The Culture of Culturing: The Importance of Knowing When to Order Urine Cultures. Today s Presenters
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI The Culture of Culturing: The Importance of Knowing When to Order Urine Cultures National Content Webinar Series October 15, 2015 Today s Presenters Barbara
AHRQ Safety Program for Long-term Care: HAIs/CAUTI The Culture of Culturing: The Importance of Knowing When to Order Urine Cultures National Content Webinar Series October 15, 2015 Today s Presenters Barbara
Jennifer A. Meddings, MD, MSc
 CAUTI progress reports: How was this data collected? Jennifer A. Meddings, MD, MSc University of Michigan Medical School Disclosures: Research Grant Funding: AHRQ, BCBSFM Honorariums: SHEA, RAND, CSCR
CAUTI progress reports: How was this data collected? Jennifer A. Meddings, MD, MSc University of Michigan Medical School Disclosures: Research Grant Funding: AHRQ, BCBSFM Honorariums: SHEA, RAND, CSCR
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
19th Annual. Challenges. in Critical Care
 19th Annual Challenges in Critical Care A Multidisciplinary Approach Friday August 22, 2014 The Hotel Hershey 100 Hotel Road Hershey, Pennsylvania 17033 A continuing education service of Penn State College
19th Annual Challenges in Critical Care A Multidisciplinary Approach Friday August 22, 2014 The Hotel Hershey 100 Hotel Road Hershey, Pennsylvania 17033 A continuing education service of Penn State College
E: Nursing Practice. Alberta Licensed Practical Nurses Competency Profile 51
 E: Nursing Practice Alberta Licensed Practical Nurses Competency Profile 51 Competency: E-1 Critical Thinking E-1-1 E-1-2 E-1-3 Demonstrate knowledge and ability to apply critical thinking concepts throughout
E: Nursing Practice Alberta Licensed Practical Nurses Competency Profile 51 Competency: E-1 Critical Thinking E-1-1 E-1-2 E-1-3 Demonstrate knowledge and ability to apply critical thinking concepts throughout
Changing ICU culture to reduce catheter-associated urinary tract infections
 QI IN IPAC Changing ICU culture to reduce catheter-associated urinary tract infections Marcia Maxwell RN, MS, CNS, CCNS, CCRN, Kristy Murphy RN, BSN, MSc & Maude McGettigan RN, BA, CIC SCL Health Good
QI IN IPAC Changing ICU culture to reduce catheter-associated urinary tract infections Marcia Maxwell RN, MS, CNS, CCNS, CCRN, Kristy Murphy RN, BSN, MSc & Maude McGettigan RN, BA, CIC SCL Health Good
OHA HEN 2.0 Partnership for Patients Letter of Commitment
 OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
The percent of skilled nursing facility (SNF) residents who have
 residents who have") Implementation of the FIRM (Foley Insertion, Removal, and Maintenance) protocol in skilled nursing facilities Murthy Gokula a and Phyllis M. Gaspar a 1 a University of Toledo Health Science Campus, Toledo,
Implementation of the FIRM (Foley Insertion, Removal, and Maintenance) protocol in skilled nursing facilities Murthy Gokula a and Phyllis M. Gaspar a 1 a University of Toledo Health Science Campus, Toledo,
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Engaging Residents and Families in HAIs/CAUTI Prevention. Presenters
 AHRQ Safety Program for Long term Care: Engaging Residents and Families in Prevention National Content Webinar Series for Core Team January 21, 2016 Presenters Kathy Bradley, Family Member CEO and Executive
AHRQ Safety Program for Long term Care: Engaging Residents and Families in Prevention National Content Webinar Series for Core Team January 21, 2016 Presenters Kathy Bradley, Family Member CEO and Executive
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition
 Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
BUGS BE GONE: Reducing HAIs and Streamlining Care!
 BUGS BE GONE: Reducing HAIs and Streamlining Care! SUSAN WHITNEY, RN, PCCN, MM, BME FLORIDA HOSPITAL ORLANDO, FL SUWHIT@AOL.COM LEARNING OUTCOMES 1. Describe HAI s and the impact disposable ECG leads have
BUGS BE GONE: Reducing HAIs and Streamlining Care! SUSAN WHITNEY, RN, PCCN, MM, BME FLORIDA HOSPITAL ORLANDO, FL SUWHIT@AOL.COM LEARNING OUTCOMES 1. Describe HAI s and the impact disposable ECG leads have
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017
 HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
VERNON COLLEGE SYLLABUS. DIVISION: Allied Health and Human Services DATE:
 VERNON COLLEGE SYLLABUS DIVISION: Allied Health and Human Services DATE: 2011-2012 CREDITS HRS: 4 HRS/WK LEC: 2 HRS/WK LAB: 6 LEC/LAB COMB: 8 I. VERNON COLLEGE GENERAL EDUCATION PHILOSOPHY STATEMENT General
VERNON COLLEGE SYLLABUS DIVISION: Allied Health and Human Services DATE: 2011-2012 CREDITS HRS: 4 HRS/WK LEC: 2 HRS/WK LAB: 6 LEC/LAB COMB: 8 I. VERNON COLLEGE GENERAL EDUCATION PHILOSOPHY STATEMENT General
Effective Date: August 31, 2006 SUBJECT: PRESSURE SORE (DECUBITUS ULCER), PREVENTION AND TREATMENT
, PREVENTION AND TREATMENT") COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION - Treatments POLICY NUMBER: 420 Effective Date: August 31, 2006 SUBJECT: PRESSURE SORE (DECUBITUS ULCER), PREVENTION AND TREATMENT 1.
COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION - Treatments POLICY NUMBER: 420 Effective Date: August 31, 2006 SUBJECT: PRESSURE SORE (DECUBITUS ULCER), PREVENTION AND TREATMENT 1.
Creating Sustainable Change to Prevent Harm in the ICU: Culture Matters
 Creating Sustainable Change to Prevent Harm in the ICU: Culture Matters Pat Posa RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Health Sytem Ann Arbor, MI patposa@gmail.com Objectives Understand
Creating Sustainable Change to Prevent Harm in the ICU: Culture Matters Pat Posa RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Health Sytem Ann Arbor, MI patposa@gmail.com Objectives Understand
Describe the impact of CLABSI on patients and their families. Discuss three methods of reducing CLABSIs
 Describe the impact of CLABSI on patients and their families. Discuss three methods of reducing CLABSIs Explore the essential elements of maintaining decreased CLABSIs 1 2001-43,000 CLABSIs In ICUs 2009-18,000
Describe the impact of CLABSI on patients and their families. Discuss three methods of reducing CLABSIs Explore the essential elements of maintaining decreased CLABSIs 1 2001-43,000 CLABSIs In ICUs 2009-18,000
Goal Elements of Performance APIC Comments APIC Recommendations
 Association for Professionals in Infection Control and Epidemiology, Inc. Comments on the Joint Commission s Proposed 2012 National Patient Safety Goals The Joint Commission Practice Guidance Team Accreditation
Association for Professionals in Infection Control and Epidemiology, Inc. Comments on the Joint Commission s Proposed 2012 National Patient Safety Goals The Joint Commission Practice Guidance Team Accreditation
CLABSI Prevention Hardwiring Improvement
 CLABSI Prevention Hardwiring Improvement Brian Koll MD, FACP, FIDSA Executive Director, Infection Prevention Mount Sinai Health System Professor of Medicine, Icahn School of Medicine September 29, 2014
CLABSI Prevention Hardwiring Improvement Brian Koll MD, FACP, FIDSA Executive Director, Infection Prevention Mount Sinai Health System Professor of Medicine, Icahn School of Medicine September 29, 2014
Bundle Me Up! Using Central Line Bundles to Decrease Infection
 Bundle Me Up! Using Central Line Bundles to Decrease Infection Organization Name: Peninsula Regional : Acute Care Hospital Medical Center Contact Person: Regina Kundell Title: Dir, Women s and Children
Bundle Me Up! Using Central Line Bundles to Decrease Infection Organization Name: Peninsula Regional : Acute Care Hospital Medical Center Contact Person: Regina Kundell Title: Dir, Women s and Children
URINARY CATHETER MANAGEMENT CARE PLAN
 URINARY CATHETER MANAGEMENT CARE PLAN Care planning: Clear set of actions that enable a patient/ client and nurse to achieve a goal in relation to a specific problem or need. Focus for care Continuity
URINARY CATHETER MANAGEMENT CARE PLAN Care planning: Clear set of actions that enable a patient/ client and nurse to achieve a goal in relation to a specific problem or need. Focus for care Continuity
Core Elements of Antibiotic Stewardship for Nursing Homes
 Core Elements of Antibiotic Stewardship for Nursing Homes Welcome! Holly Harmon, RN, MBA, LNHA Senior Director Clinical Services 1 Leonard Russ Immediate Past Chair AHCA Board of Governors Antibiotic Stewardship
Core Elements of Antibiotic Stewardship for Nursing Homes Welcome! Holly Harmon, RN, MBA, LNHA Senior Director Clinical Services 1 Leonard Russ Immediate Past Chair AHCA Board of Governors Antibiotic Stewardship
You have joined the CUSP Communication & Teamwork Tools Informational Session!
 You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers
 Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers Melissa A. Fitzpatrick, RN, MSN, FAAN VP & Chief Clinical Officer, Hill-Rom Trends Driving Our Industry Aging
Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers Melissa A. Fitzpatrick, RN, MSN, FAAN VP & Chief Clinical Officer, Hill-Rom Trends Driving Our Industry Aging
Canadian Surgical Site Infection Prevention Audit Month
 Canadian Surgical Site Infection Prevention Audit Month February 2016 CONTENTS KEY FACTS...3 SSI PREVENTION AUDIT RESULTS...3 BACKGROUND...4 METHODOLOGY...4 Data Scores... 5 How to Interpret the Indicator
Canadian Surgical Site Infection Prevention Audit Month February 2016 CONTENTS KEY FACTS...3 SSI PREVENTION AUDIT RESULTS...3 BACKGROUND...4 METHODOLOGY...4 Data Scores... 5 How to Interpret the Indicator
Strategies to Address All Types of Harm. Objectives. Share implementation process for a successful large scale harm reduction campaign
 C20 These presenters have nothing to disclose Strategies to Address All Types of Harm Jack Jordan, Partnership for Patients, CMMI William Conway, MD Henry Ford Health System Sam Watson, Michigan Hospital
C20 These presenters have nothing to disclose Strategies to Address All Types of Harm Jack Jordan, Partnership for Patients, CMMI William Conway, MD Henry Ford Health System Sam Watson, Michigan Hospital
Device Utilization and CAUTI Prevention. Lori Fornwalt, RN, CIC Infection Prevention Coordinator October 4, 2016
 Device Utilization and CAUTI Prevention Lori Fornwalt, RN, CIC Infection Prevention Coordinator October 4, 2016 DISCLOSURES Nothing to disclose OBJECTIVES Explain relationship between catheterassociated
Device Utilization and CAUTI Prevention Lori Fornwalt, RN, CIC Infection Prevention Coordinator October 4, 2016 DISCLOSURES Nothing to disclose OBJECTIVES Explain relationship between catheterassociated
Text-based Document. Downloaded 25-Apr :55:57.
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Rehabilitation Readiness. Lane Brown, PhD Magee Rehabilitation at Jefferson March 1,2018
 Rehabilitation Readiness Lane Brown, PhD Magee Rehabilitation at Jefferson March 1,2018 Today s Rehabilitation Readiness Discussion: Rehabilitation settings Characteristics of inpatient settings Characteristics
Rehabilitation Readiness Lane Brown, PhD Magee Rehabilitation at Jefferson March 1,2018 Today s Rehabilitation Readiness Discussion: Rehabilitation settings Characteristics of inpatient settings Characteristics
INFECTION of the urinary tract caused
 J Nurs Care Qual Vol. 00, No. 00, pp. 1 6 Copyright c 2016 Wolters Kluwer Health, Inc. All rights reserved. Incorporation of Leadership Rounds in CAUTI Prevention Efforts Suzanne Purvis, DNP, RN, GCNS-BC;
J Nurs Care Qual Vol. 00, No. 00, pp. 1 6 Copyright c 2016 Wolters Kluwer Health, Inc. All rights reserved. Incorporation of Leadership Rounds in CAUTI Prevention Efforts Suzanne Purvis, DNP, RN, GCNS-BC;
A QUALITY IMPROVEMENT NURSE LED INITIATIVE TO DECREASE THE RATE OF CATHETER ASSOCIATED URINARY TRACT INFECTIONS AT A LONG TERM ACUTE CARE HOSPITAL.
 A QUALITY IMPROVEMENT NURSE LED INITIATIVE TO DECREASE THE RATE OF CATHETER ASSOCIATED URINARY TRACT INFECTIONS AT A LONG TERM ACUTE CARE HOSPITAL. Jacqueline F. Mawoneke A project submitted to the faculty
A QUALITY IMPROVEMENT NURSE LED INITIATIVE TO DECREASE THE RATE OF CATHETER ASSOCIATED URINARY TRACT INFECTIONS AT A LONG TERM ACUTE CARE HOSPITAL. Jacqueline F. Mawoneke A project submitted to the faculty
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
Infection Prevention - Changing Practice in Catheter Management
 Infection Prevention - Changing Practice in Catheter Management Keywords: Urinary catheters, catheter specimen of urine, antibiotics Duration of project: April 2007 March 2009 Report received for publication:
Infection Prevention - Changing Practice in Catheter Management Keywords: Urinary catheters, catheter specimen of urine, antibiotics Duration of project: April 2007 March 2009 Report received for publication:
On the Road to Eliminating CAUTI at a Community Hospital Lessons Learned
 On the Road to Eliminating CAUTI at a Community Hospital Lessons Learned Getting Started CDC guidelines LeverageIT Capabilities Ordering, documenting and tracking Develop education SimLab observations
On the Road to Eliminating CAUTI at a Community Hospital Lessons Learned Getting Started CDC guidelines LeverageIT Capabilities Ordering, documenting and tracking Develop education SimLab observations
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core
 Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through Telemedicine
 PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
Why Shepherd? Shepherd Center Patients. Here s How We Measure Up: Shepherd Patient Population
 Center Patients Total Patients ABI Patients SCI Patients Other Patients Center specializes in medical treatment, research and rehabilitation for people with spinal cord and brain injury. In CY, had 911
Center Patients Total Patients ABI Patients SCI Patients Other Patients Center specializes in medical treatment, research and rehabilitation for people with spinal cord and brain injury. In CY, had 911
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
Willamette Valley Medical Center Carla Galbraith RN, BSN, CIC Manager Patient Safety/Infection Control November 1, 2013
 Willamette Valley Medical Center Carla Galbraith RN, BSN, CIC Manager Patient Safety/Infection Control November 1, 2013 About Us Willamette Valley Medical Center McMinnville, Oregon Acute Care Facility
Willamette Valley Medical Center Carla Galbraith RN, BSN, CIC Manager Patient Safety/Infection Control November 1, 2013 About Us Willamette Valley Medical Center McMinnville, Oregon Acute Care Facility
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Chasing Zero Infections Coaching Call Strategies to Reduce Surgical Site Infections March 14, 2018
 Chasing Zero Infections Coaching Call Strategies to Reduce Surgical Site Infections March 14, 2018 Agenda Welcome & FHA Mission to Care HIIN Trends and Progress: Surgical Site Infections Cheryl Love, RN,
Chasing Zero Infections Coaching Call Strategies to Reduce Surgical Site Infections March 14, 2018 Agenda Welcome & FHA Mission to Care HIIN Trends and Progress: Surgical Site Infections Cheryl Love, RN,
The Life and Times of the Urinary Catheter Mar4n Kiernan, Southport and Ormskirk Hospital NHS Trust Broadcast Live from IPS 2013 Conference
 Broadcast live from... Disclosures 2 Martin Kiernan Nurse Consultant, Southport and Ormskirk Hospital NHS Trust Member of advisory boards for Carefusion, Pfizer, Gama and Vernacare and have presented at
Broadcast live from... Disclosures 2 Martin Kiernan Nurse Consultant, Southport and Ormskirk Hospital NHS Trust Member of advisory boards for Carefusion, Pfizer, Gama and Vernacare and have presented at
In 2008, the Centers for Medicare & Medicaid Services
 Reducing catheter-associated urinary tract infections: standardising practice Amy Cartwright ABSTRACT Inspired by innovations in catheter practice from the USA, in 2014 Nottingham University Hospitals
Reducing catheter-associated urinary tract infections: standardising practice Amy Cartwright ABSTRACT Inspired by innovations in catheter practice from the USA, in 2014 Nottingham University Hospitals
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Infection Prevention and Control: How to Meet the Conditions of Participation for Home Health
 Infection Prevention and Control: How to Meet the Conditions of Participation for Home Health Mary McGoldrick, MS, RN, CRNI Home Care and Hospice Consultant Saint Simons Island, GA Nothing to Disclose
Infection Prevention and Control: How to Meet the Conditions of Participation for Home Health Mary McGoldrick, MS, RN, CRNI Home Care and Hospice Consultant Saint Simons Island, GA Nothing to Disclose
Achieving the Triple Aim: Decreasing Use of Inappropriate Telemetry Monitoring
 Achieving the Triple Aim: Decreasing Use of Inappropriate Telemetry Monitoring Marylynn Hippe, MSN, RN, ACNS-BC, CMSRN St. Luke s Health System Boise, Idaho Objectives Learners will understand the appropriate
Achieving the Triple Aim: Decreasing Use of Inappropriate Telemetry Monitoring Marylynn Hippe, MSN, RN, ACNS-BC, CMSRN St. Luke s Health System Boise, Idaho Objectives Learners will understand the appropriate
Effects of a fluid intake encouragement program in elderly Koreans
 , pp.113-118 http://dx.doi.org/10.14257/astl.2015.88.24 Effects of a fluid intake encouragement program in elderly Koreans Sung Jung Hong 1 *, Eun Hee Kim 2 1 Department of Nursing, Semyung University,
, pp.113-118 http://dx.doi.org/10.14257/astl.2015.88.24 Effects of a fluid intake encouragement program in elderly Koreans Sung Jung Hong 1 *, Eun Hee Kim 2 1 Department of Nursing, Semyung University,
THE ROLE OF HUMAN FACTORS FOR INFECTION PREVENTION IN THE EMERGENCY DEPARTMENT
 THE ROLE OF HUMAN FACTORS FOR INFECTION PREVENTION IN THE EMERGENCY DEPARTMENT Connie Savor Price, MD Director, Infection Prevention and Chief, Division of Infectious Diseases Denver Health and Hospital
THE ROLE OF HUMAN FACTORS FOR INFECTION PREVENTION IN THE EMERGENCY DEPARTMENT Connie Savor Price, MD Director, Infection Prevention and Chief, Division of Infectious Diseases Denver Health and Hospital
Evidence Based Practices to Prevent HAIs/CAUTI and Improve Resident Safety
 AHRQ Safety Program for Long term Care: HAIs/CAUTI Evidence Based Practices to Prevent HAIs/CAUTI and Improve Resident Safety Objectives Upon completion of this module, participants will be able to: Describe
AHRQ Safety Program for Long term Care: HAIs/CAUTI Evidence Based Practices to Prevent HAIs/CAUTI and Improve Resident Safety Objectives Upon completion of this module, participants will be able to: Describe
Reducing Central Line Associated Blood Stream Infection (C.L.A.B.S.I.) System and Patient Tracer
 System and Patient Tracer") Reducing C.L.A.B.S.I.: SYSTEM Tracer Begin with Large Group General Questions: 1. Describe your surgical and then medical process related to the prevention of C.L.A.B.S.I. 2. Create questions that come
Reducing C.L.A.B.S.I.: SYSTEM Tracer Begin with Large Group General Questions: 1. Describe your surgical and then medical process related to the prevention of C.L.A.B.S.I. 2. Create questions that come
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Outline 1. Infection Prevention Program Bloodborne Pathogens/Exposure Prevention & Management Standard Precautions 2. Hand Hygiene 3. Isolation Precau
 Erlanger Infection Prevention Resident and df Fellow Orientation June 2011 1 Outline 1. Infection Prevention Program Bloodborne Pathogens/Exposure Prevention & Management Standard Precautions 2. Hand Hygiene
Erlanger Infection Prevention Resident and df Fellow Orientation June 2011 1 Outline 1. Infection Prevention Program Bloodborne Pathogens/Exposure Prevention & Management Standard Precautions 2. Hand Hygiene
HIMSS Submission Leveraging HIT, Improving Quality & Safety
 HIMSS Submission Leveraging HIT, Improving Quality & Safety Title: Making the Electronic Health Record Do the Heavy Lifting: Reducing Hospital Acquired Urinary Tract Infections at NorthShore University
HIMSS Submission Leveraging HIT, Improving Quality & Safety Title: Making the Electronic Health Record Do the Heavy Lifting: Reducing Hospital Acquired Urinary Tract Infections at NorthShore University
Missed Nursing Care: Errors of Omission
 Missed Nursing Care: Errors of Omission Beatrice Kalisch, PhD, RN, FAAN Titus Professor of Nursing and Chair University of Michigan Nursing Business and Health Systems Presented at the NDNQI annual meeting
Missed Nursing Care: Errors of Omission Beatrice Kalisch, PhD, RN, FAAN Titus Professor of Nursing and Chair University of Michigan Nursing Business and Health Systems Presented at the NDNQI annual meeting
Chasing Zero Infections Webinar: CAUTI Coaching Call March 21, 2017
 Chasing Zero Infections Webinar: CAUTI Coaching Call March 21, 2017 Agenda Welcome & HIIN Update Sally Forsberg, RNC-OB, BSN, MBA, NEA-BC, CPHQ, Clinical Performance Improvement Advisor, FHA Hospital Best
Chasing Zero Infections Webinar: CAUTI Coaching Call March 21, 2017 Agenda Welcome & HIIN Update Sally Forsberg, RNC-OB, BSN, MBA, NEA-BC, CPHQ, Clinical Performance Improvement Advisor, FHA Hospital Best
RELIAFIT MALE URINARY DEVICE. Case Study
 RELIAFIT MALE URINARY DEVICE Case Study Quality Improvement Initiative Successful in Achieving CAUTI Reduction Mary Fitzwater, RN INTRODUCTION Catheter-associated urinary tract infections (CAUTI) negatively
RELIAFIT MALE URINARY DEVICE Case Study Quality Improvement Initiative Successful in Achieving CAUTI Reduction Mary Fitzwater, RN INTRODUCTION Catheter-associated urinary tract infections (CAUTI) negatively
2015 Executive Overview
 An Independent Licensee of the Blue Cross and Blue Shield Association 2015 Executive Overview Criteria for the Blue Cross and Blue Shield of Alabama Hospital Tiered Network will be updated effective January
An Independent Licensee of the Blue Cross and Blue Shield Association 2015 Executive Overview Criteria for the Blue Cross and Blue Shield of Alabama Hospital Tiered Network will be updated effective January
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals
 Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Guidelines for Supervising Residents Updated July 2017
 NORTHWESTERN UNIVERSITY FEINBERG SCHOOL OF MEDICINE DEPARTMENT OF SURGERY POLICIES & PROCEDURES Guidelines for Supervising Residents Updated July 2017 PURPOSE To clearly define the level of patient care
NORTHWESTERN UNIVERSITY FEINBERG SCHOOL OF MEDICINE DEPARTMENT OF SURGERY POLICIES & PROCEDURES Guidelines for Supervising Residents Updated July 2017 PURPOSE To clearly define the level of patient care
2017 Nicolas E. Davies Enterprise Award of Excellence
 2017 Nicolas E. Davies Enterprise Award of Excellence Agenda Memorial Hermann Health System Overview Journey to High Reliability Case study review CLABSI Prevention 2 Memorial Hermann Health System Woodlands
2017 Nicolas E. Davies Enterprise Award of Excellence Agenda Memorial Hermann Health System Overview Journey to High Reliability Case study review CLABSI Prevention 2 Memorial Hermann Health System Woodlands
Patient Experience of Care Survey Results Hospital Consumer Assessment of Healthcare Providers and Systems (Inpatient)
") Patient Experience of Care Survey Results Hospital Consumer Assessment of Healthcare Providers and Systems (Inpatient) HCAHPS QUESTION DESCRIPTION (April 2016 - March 2017) Patients who reported that their
Patient Experience of Care Survey Results Hospital Consumer Assessment of Healthcare Providers and Systems (Inpatient) HCAHPS QUESTION DESCRIPTION (April 2016 - March 2017) Patients who reported that their
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Right Sizing Healthcare-Associated Infection Prevention Measures for Critical Access Hospitals. Bonnie M. Barnard, MPH, CIC
 Right Sizing Healthcare-Associated Infection Prevention Measures for Critical Access Hospitals Bonnie M. Barnard, MPH, CIC Objectives Describe the features of critical access hospitals (CAHs) Describe
Right Sizing Healthcare-Associated Infection Prevention Measures for Critical Access Hospitals Bonnie M. Barnard, MPH, CIC Objectives Describe the features of critical access hospitals (CAHs) Describe
RCFE ADMINISTRATOR INITIAL CERTIFICATION PROGRAM
 RCFE ADMINISTRATOR INITIAL CERTIFICATION PROGRAM Day 5 DAY 5 1) Physical Needs Monitoring residents for changes in condition Health-related services Allowable, restricted, and prohibited conditions Diabetes
RCFE ADMINISTRATOR INITIAL CERTIFICATION PROGRAM Day 5 DAY 5 1) Physical Needs Monitoring residents for changes in condition Health-related services Allowable, restricted, and prohibited conditions Diabetes
Preventing Urinary Tract Infections in the Acute Care Setting
 Walden University ScholarWorks Walden Dissertations and Doctoral Studies Walden Dissertations and Doctoral Studies Collection 2016 Preventing Urinary Tract Infections in the Acute Care Setting Charlotte
Walden University ScholarWorks Walden Dissertations and Doctoral Studies Walden Dissertations and Doctoral Studies Collection 2016 Preventing Urinary Tract Infections in the Acute Care Setting Charlotte
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Partnering with the Care Management Department. Medical Staff and Allied Health Practitioner Orientation
 Partnering with the Care Management Department Medical Staff and Allied Health Practitioner Orientation 10/2015 Department of Care Management Medical Directors of Care Coordination Inpatient Case Managers
Partnering with the Care Management Department Medical Staff and Allied Health Practitioner Orientation 10/2015 Department of Care Management Medical Directors of Care Coordination Inpatient Case Managers
Implementation Guide for Central Line Associated Blood Stream Infection
 Implementation Guide for Central Line Associated Blood Stream Infection March 27, 2013 Contents 1. Introduction... 3 2. Central Line Associated Blood Stream Infection Prevention Evidence-Based Practices...
Implementation Guide for Central Line Associated Blood Stream Infection March 27, 2013 Contents 1. Introduction... 3 2. Central Line Associated Blood Stream Infection Prevention Evidence-Based Practices...
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Thinking Differently Acting Differently. Higher staff satisfaction = better patient outcomes & better patient experience
 Thinking Differently Acting Differently Higher staff satisfaction = better patient outcomes & better patient experience Staff Satisfaction is the best indicator of a High Quality Culture Nursing contribution
Thinking Differently Acting Differently Higher staff satisfaction = better patient outcomes & better patient experience Staff Satisfaction is the best indicator of a High Quality Culture Nursing contribution
LEAN HEALTHCARE: Elimination of CAUTI on 8 East Providence St. Vincent Medical Center. Purdue Research Foundation
 LEAN HEALTHCARE: Elimination of CAUTI on 8 East Providence St. Vincent Medical Center 1 About Us Providence St. Vincent Medical Center PSVMC is located Portland, Oregon. We are a level 2 trauma center
LEAN HEALTHCARE: Elimination of CAUTI on 8 East Providence St. Vincent Medical Center 1 About Us Providence St. Vincent Medical Center PSVMC is located Portland, Oregon. We are a level 2 trauma center