ACUTE MEDICINE HIGHER TRAINING PROGRAMME
|
|
|
- Jade Barton
- 6 years ago
- Views:
Transcription


1 ACUTE MEDICINE HIGHER TRAINING PROGRAMME StR HANDBOOK WALES DEANERY
2 WELCOME! CROESO Acute medicine is a vibrant, rewarding, and rapidly developing medical speciality, concerned with the assessment, diagnosis and management of adults presenting to secondary care with acute medical illness. It also involves the management of busy acute medical units (AMUs) to ensure they deliver high-quality, efficient and patientcentred care. This handbook provides an overview of the Acute Medicine Specialist Training scheme and details the essential information required for trainees. The Welsh Higher Training Programme in Acute Medicine fulfils all the recommendations of the Royal College of Physicians and GMC for accreditation in this speciality and aims to offer the highest quality training in hospitals situated throughout Wales. The four-year programme is designed to provide trainees with a Certificate of Completion of Training (CCT) in Acute Internal Medicine (AIM) with the option of extending training to a fifth year in General internal Medicine (GIM), or to dually accredit in another speciality. Core trainees from both Core Medical Training (CMT) and Acute Care Common Stem (ACCS) are eligible to apply for the Acute Medicine StR programme. We hope you enjoy your time in Wales and look forward to working with you. Note: If you spot any errors, omissions, contradictions, or if any updates are needed please contact Dr Nia Rathbone (Nia.Rathbone@Wales.nhs.uk) or Dr Aled Huws (Aled.Huws@Wales.nhs.uk). The definitive guides for training and curriculum matters remain the Gold Guide and the speciality curricula. 2
3 CONTENTS Acute Medicine Training Overview Wales Deanery...6 Acute Medicine Specialist Training Committee (STC)...7 Wales Higher Training Programme in Acute Medicine....8 Entry Criteria Training Programme General Comments Postgraduate Training Pathway Speciality Experience ST placements...12 Sample Rotations Hospitals participating in training...14 Acute Consultants / Associate Specialists in Wales Educational and Clinical Supervisors...16 Educational supervisors...16 Clinical supervisors...17 Patient safety concerns...17 Undermining/bullying...17 Specialist Skill Curricula...19 E-portfolio (JRCPTB)...20 Key points...21 Overview of AIM training requirements 22 Overview of GIM training requirements Work Based Placed Assessments (WBPAs)...25 Supervised Learning Events (SLEs)...25 Mini-clinical evaluation exercise (mini-cex)...25 Case-based discussion (CbD)...25 Direct observation of procedural skills (DOPS)...25 Acute care assessment tool (ACAT)...25 Multi-source feedback (MSF)...26 Patient survey...26 Audit Assessment
4 Quality Improvement Project Assessment Tool...26 Teaching observation...26 Multiple consultant report (MCR)...27 Audits...27 Firth calculator...27 Personal library Training quality surveys Annual calendar...28 Training days and leave...29 Acute Medicine Summer School...29 Welsh Acute Physicians Society (WAPS).29 GIM Training...29 Study Leave...30 Annual leave...30 Speciality Certificate Examination (SCE)...31 Annual Review of Competence Progression (ARCP)...34 Principal ARCP outcomes...35 Penultimate Year Assessment (PYA)...36 Completion of training...37 Out of Programme (OOP) requests...38 Acting up as a consultant (AUC)...39 Flexible / Less Than Full Time Training (LTFT)...40 Professional Support Unit (PSU)...40 Useful training related websites...41 Society for Acute Medicine Journals...41 Other societies and organisations...41 Useful training resources...42 Appendix 1: AIM/GIM ARCP Checklist.43 Appendix 2: GIM PYA Checklist.44 4
5 Acute Medicine Training Overview Acute Internal Medicine (AIM) was formally recognised as a speciality in 2009, having previously been a subspeciality of General Internal Medicine (GIM). This was in response to the growing need for a senior medical presence supervising acute medical takes within an Acute Medical Unit (AMU) environment and has resulted in a massive expansion of Consultant Acute Physicians along with the development of Acute Medicine training programmes. Over recent years, the Wales Deanery has expanded the number of training posts in this evolving field in recognition of the increasing number of appointments of Acute Physicians nationally. In Wales we currently have 13 training posts of 4 years duration with the option of dual accreditation. Entry to the Acute Medicine training programme can either be from Core Medical Training (CMT) or Acute Care Common Stem (ACCS). Our training programme is exciting and varied. The experience it offers is unique as it allows rotation through many different specialties at registrar level in a variety of work settings and intensities. It also offers the opportunity for trainees to develop their own area of interest or special skill whilst satisfying the core curriculum requirements. AIM is a hospital-based speciality, with the majority of the work involving care of medical patients around the time of admission to hospital. The spectrum of clinical problems encountered in the AMU is very wide, and this variability enables trainees to become experts in assessment, investigation, diagnosis and management across multiple disciplines. The posts are a mixture of AMU, ambulatory care, elderly medicine, respiratory, cardiology and intensive care medicine rotations. Training concentrates on the recognition and management of medical emergencies, the development of acute medical services and the acquisition of skills in leadership and management of the AMU as a whole. The requirement to obtain an additional specialist skill or interest during higher training enables acute medicine trainees to pursue a professional qualification, diagnostic skill or research interest that will enhance their clinical practice. These interests can be maintained throughout their career as an Acute Physician, adding another dimension to the speciality. 5
6 Wales Deanery The aim of the Wales Deanery is to commission, quality assure and support the education and training of trainees in Wales. The Deanery manages out of programme experience, flexible or less than full time training, inter-deanery transfers and ARCPs in conjunction with the Acute Medicine STCs. There are several important people within the Deanery who will monitor and help support your training: Acute Internal Medicine (AIM) Trudy McMullin Telephone number: General Internal Medicine (GIM) Robert McGowan Telephone number: Speciality Training Manager Hilary Williams Telephone number:
7 Acute Medicine Specialist Training Committee (STC) The main role of the STC is to organise the speciality training programme in Wales. It consists of Acute Medicine consultants from each of the Health Boards within Wales, consultants from the specialties through which our trainees rotate along with a trainee representative. A Chair and a Training Programme Director (TPD) oversee the STC. TPDs are responsible for managing the speciality training programme including recruitment, placements and ARCPs. They also assist the Deanery with managing trainees in difficulty. Acute Medicine STC Chair Dr Nia Rathbone Consultant Acute Physician Royal Glamorgan Hospital, Llantrisant Nia.Rathbone@Wales.nhs.uk Training Programme Director (TPD) Dr Tom Cozens Consultant Acute Physician Royal Gwent Hospital, Newport Thomas.Cozens@Wales.nhs.uk StR Trainee Representative Appointed on annual basis 7
 or Acute Care Common Stem (ACCS).")
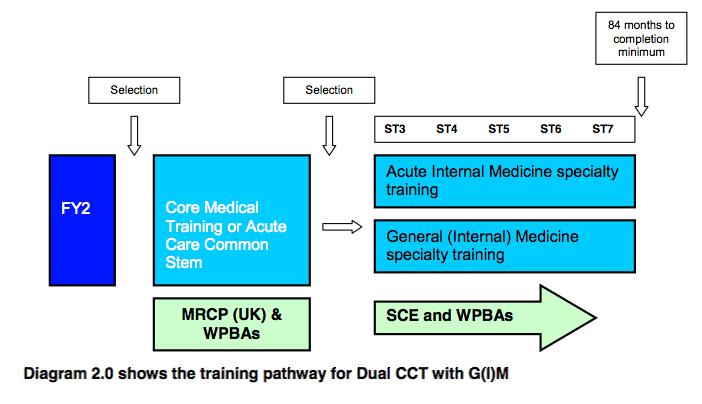
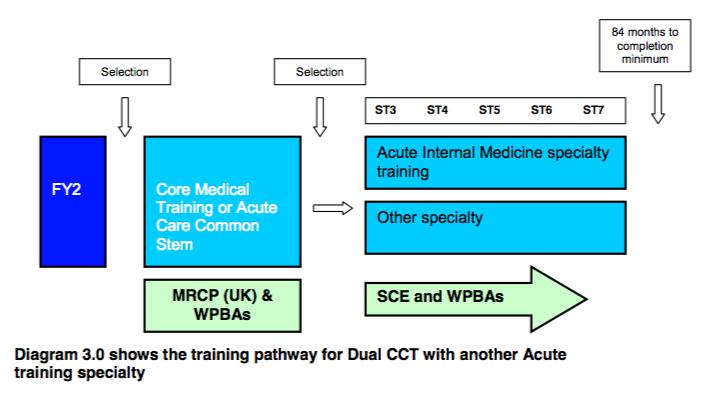
8 Wales Higher Training Programme in Acute Medicine Entry Criteria Entry into Acute Medicine higher speciality training is possible following successful completion of both a Foundation Programme and a Core Training programme - either Core Medical Training (CMT) or Acute Care Common Stem (ACCS). The minimum experience in CMT posts in Medicine is 24 months or months in ACCS posts of which at least 12 months must include the care of acute medical inpatients. Full membership of the Royal College of Physicians (MRCP) is a minimum educational requirement for entry to the programme at ST3 grade. The other qualities considered essential or desirable are detailed in the ST3 Acute Internal Medicine Person Specification, which can be found via the following link: Postgraduate Training Pathway The following diagrams illustrate the different postgraduate training pathways in Acute Internal Medicine leading to single or dual CCT: 8
9 9

10 The following diagram shows an example programme for dual CCT in ICM and AIM: 10
11 Specialty Experience The program has been constructed to ensure exposure to specialities relevant to Acute Medicine. Training includes time on AMU and Ambulatory Care as well as attachments in other relevant specialties, with a focus on managerial AMU experience towards the end of higher specialist training. The trainees will gain experience in the following fields: Acute Internal Medicine, including experience working in o Acute Medical Units (AMUs) = Medical Admissions Units (MAUs) or Clinical Decisions Units (CDUs) o Ambulatory care (AECU or MDUs) o Acute non-selected takes Cardiology Critical Care (ITU, HDU, CCU) General Internal Medicine including acute non-selected takes (minimum 4 months): o Respiratory Medicine o Care of the Elderly Out Patient experience o Rapid Access Medical outpatient clinics / Hot Clinics o Acute Medicine review clinics o Speciality based clinics - Cardiology, Respiratory Medicine, and Medicine for the Elderly The final year of training should include at least 6 months experience within an Acute Medical Unit that is led by an Acute Physician. This should include training in management and leadership skills as well as taking a more senior, but supervised, role within the running of the acute medical take. Throughout training the trainee should be aware of the need to acquire a special competency or skill that is specifically relevant to Acute Internal Medicine. Acquisition of one of these competencies is a mandatory part of training and trainees should review with their educational supervisor as early as possible in their training which of these would be most relevant for their career development, and sustainable in the long term. This is detailed in the Specialist Skill chapter on page 18 of this handbook. The trainee will be required to take part in organised, relevant courses particularly those which form part of the Core Curriculum, and the regional GIM Training sessions. The trainee will be expected to keep abreast of current developments within the speciality, to practice evidence-based medicine and to help to change practice within the department where appropriate. Computer literacy is essential in order to ensure effective audit of all clinical / managerial aspects of the work of the department. 11
12 ST Placements Each clinical placement usually commences in the first week of August each year. However, should a trainee leave the programme outside this changeover interval, the start date of a newly appointed ST3 may be brought forward or delayed to match the timing of the vacancy left by the departing trainee. The trainee will be placed in one LHB (usually one hospital) for the whole year though trainees may rotate between specialties at various intervals throughout the year. Most trainees rotate to North Wales for at least one year of their training. The TPD will endeavour to inform trainees of as many of their future placements with as much advance notice as is reasonably possible. It may occasionally be possible, if circumstances permit, to inform some trainees of their placements for the entire 4/5 year training programme though this has to date proved difficult given the fluctuating number and staggered CCT dates of trainees, as well as the expanding number of hospitals participating in training over recent years. Trainees will usually rotate through ICU/Cardiology in the early part of training. Those trainees rotating through North Wales will usually do so in the earlier years of their training. The final year is usually in South Wales and should include at least 6 months experience within an AMU led by an Acute Physician. Thus, there will be a degree of certainty about where the trainee will be geographically located for the duration of their training although this is not totally guaranteed. A Survival Guide to Cardiology & ICU has been produced by one of the current trainees and contains invaluable tips and practical advice to help prepare trainees for what is often regarded as a rather daunting year. This handout, along with a host of other useful documents, will be given to trainees at the beginning of their training and can be accessed via the WAPS cloud account. If trainees step out of programme for any reason, it is anticipated that they will return to the rotation they left. If a grace period is required, trainees may need to go back to the beginning of their rotation. It is very important for trainees to arrange a meeting with their educational supervisor within the first couple of weeks of their first rotation to discuss their personal development plan and educational needs for that year this should be recorded on an induction appraisal form on the NHS e-portfolio. The StR s weekly timetable will vary significantly with each placement. It is acknowledged by the STC that the trainees are entitled to one protected session per week for specialist skill / service improvement / admin. The following table shows sample training rotations (5-year, for those aiming for dual accreditation with GIM). Please note: these examples are meant only as a guide to illustrate the usual locations and sequence of the rotations. The actual rotations allocated by the TPD will depend on placement availability, service demand and training needs of the individual. 12
13 Trainee 1 Trainee 2 Trainee 3 Trainee 4 Year 1 - ST3 UHW Cardiology ICU UHW ICU Cardiology Princess of Wales CDU Stroke Wrexham Maelor MAU Year 2 ST4 Royal Glamorgan AECU Resp 4/12 COTE 2/12 Royal Glamorgan Resp 4/12 COTE 2/12 AECU UHW Cardiology ICU UHW ICU Cardiology Sample Rotations: Year 3 ST5 Princess of Wales CDU Stroke Princess of Wales Stroke CDU Royal Glamorgan Resp 4/12 COTE 4/12 AECU Royal Glamorgan AECU Resp 4/12 COTE 2/12 Year 4 ST6 Ysbyty Glan Clwyd MAU Royal Gwent MAU Ysbyty Gwynedd MAU Nevill Hall MAU Year 5 ST7 Royal Gwent MAU Nevill Hall MAU Prince Charles CDU Princess of Wales Stroke CDU 13
14 Hospitals participating in training Training is provided in 9 hospitals in 5 Health Boards across Wales. The post holder will be required to work at any of the following Health Boards in Wales: Abertawe Bro Morgannwg University Health Board Aneurin Bevan Health Board Betsi Cadwaladr University Health Board Cardiff and Vale University Health Board Cwm Taf Health Board Hospital Speciality / Experience Clinical Placement Coordinators - *May 2016 Ysbyty Gwynedd, Bangor AMU Dr Chris Subbe Ysbyty Glan Clwyd, Rhyl Wrexham Maelor Hospital, Wrexham Nevill Hall Hospital, Abergavenny Royal Gwent Hospital, Newport Princess of Wales Hospital, Bridgend Royal Glamorgan Hospital, Llantrisant Prince Charles Hospital, Merthyr Tydfil University Hospital of Wales, Cardiff AMU, A&E Majors, AMU, MDU MAU MAU CDU Stroke Medicine / COTE AECU (Ambulatory Care) AMU Respiratory COTE CDU, MDU ICU Cardiology Dr Hari Nair Dr Sarah Dyer Dr Matt Brouns Dr Tom Cozens Dr John Hounsell Dr Harish Bhat (Stroke) Dr Les Ala / Dr Chris Hodcroft Dr Amit Benjamin (Resp) Dr Biswas (COTE) Dr Aled Huws Dr Chris Hingston (ICU) Dr Richard Wheeler (Cardio) * Note: The list of Clinical Placement Coordinators (CPC) is subject to change. Trainees will be informed of their CPC by the TPD upon commencing each placement. 14
15 Acute Consultants / Associate Specialists in Wales Note: This list is subject to change. Updated 31/8/15. Royal Gwent Hospital (RGH), Newport: o Hannah Brothers o Tom Cozens o Paul Mizen o Llifon Edwards o Haris Saleem o Emma Mason o Ferran Cavalle o Anna Lewis Nevill Hall Hospital (NHH), Abergavenny: o Matt Brouns Ysbyty Ystrad Fawr (YYF), Ystrad Mynach: o Mohamed Adlan University Hospital of Wales (UHW), Cardiff: o Dave Thomas o Anil Kumar University Hospital Llandough (UHL), Cardiff: o Ahmed Osman o Anna De Lloyd o Nolan Arulraj Princess of Wales Hospital (POW), Bridgend: o John Hounsell Royal Glamorgan Hospital (RGL), Llantrisant: o Les Ala o Nia Rathbone o Chris Hodcroft o Kate Speed o Nerys Conway o Atul Kalhan o Eugene Tabiowo Prince Charles Hospital (PCH), Merthyr Tydfil o Mohamed Hassan o Mark Stephens o Aled Huws o Vikas Lodhi o Joanne Morris Morriston Hospital (MH), Swansea (not currently participating in ST training): o Steve Lennox 15
16 o Ali Al Hassani Ysbyty Gwynedd (YG), Bangor o Hassan Mohammed o Anwar Khan o Chris Subbe Ysbyty Glan Clwyd (YGC), Rhyl o Aye Nyunt o Hari Nair o Atanu Basu o Sarah Davies Wrexham Maelor Hospital (WMH), Wrexham o Sarah Dyer o James Kilbane Educational & Clinical Supervisors Each trainee will have two nominated supervisors who will be named at the beginning of their rotation; one clinical placement coordinator (who will change with the various placements listed on page 14) and one educational supervisor (who should remain the same for the entire training). Note: there will be a number of clinical supervisors within each post but only one clinical placement coordinator. Educational supervisors It is your responsibility to arrange regular meetings with your educational supervisor (ES) and ensure the e-portfolio is up to date and reviewed. If you have difficulty arranging meetings with your educational or clinical placement coordinator (CPC) or have any other concerns you should speak with your TPD. You should have four meetings with your ES during each placement, with documentation completed on the e-portfolio: 1. Induction appraisal within initial 4 weeks of the post 2. Mid-point review (optional but recommended) 3. ES report / review (prior to ARCP) 4. End of attachment appraisal end of July prior to rotation to next post A formal process of appraisals and reviews underpins training. This process ensures adequate supervision during training, provides continuity between posts and different supervisors and is one of the main ways of providing feedback to trainees. All appraisals should be recorded in the eportfolio. For those who are dually accrediting, it is important to look at and complete your training requirements for both AIM and GIM this includes audits, SLEs and attendance at training days. 16
17 The supervisor s main responsibilities are to use e-portfolio evidence such as outcomes of assessments, reflections and personal development plans to inform appraisal meetings. They are also expected to update the trainee s record of progress through the curriculum, write end-of-attachment appraisals and supervisor s reports. Clinical supervisors Clinical supervisors (CS) are responsible for overseeing your day-to-day clinical work, such as inpatient work and outpatient clinics, and providing constructive feedback during a training placement. Your ES will also seek feedback about your progress and performance from your CPC or CS this will be recorded in your multiple consultant reports (MCRs). In some cases your CPC will also be your ES i.e. the roles will be merged. All elements of work in training posts must be supervised with the level of supervision varying depending on the experience of the trainee and the clinical exposure and case mix undertaken. Outpatient and referral supervision must routinely include the opportunity to personally discuss all cases if required. It is required that the clinical supervisor devotes at least one hour per week in their timetable per trainee for this work. As training progresses the trainee should have the opportunity for increasing autonomy, consistent with safe and effective care for the patient. Any concerns or problems (either personal or related to your job) that you experience during your placement can be discussed with your clinical placement coordinator or educational supervisor or any other member of the department you feel comfortable approaching. If there are any issues with your placement or job plan, you should approach your CP/CPC as the first point of contact, who will then inform your ED who will in turn contact the TPD. If you do not feel comfortable discussing or are unable to resolve any concerns raised you are welcome to contact the TPD directly. There is also in each hospital a tutor of the Royal College of Physicians, who is available for discussion. Patient safety concerns Any concerns you have relating to patient safety should be discussed with either your clinical placement coordinator or educational supervisor. If these concerns potentially relate to your supervisors they should be discussed with the head of department or local clinical director. Undermining / bullying If you encounter or witness any undermining or bullying during your placements you should discuss this with either your clinical placement coordinator or educational supervisor. If you feel this involves your supervisors you can discuss this with the TPD. 17
18 Specialist Skill The development of an additional skill or qualification is a mandatory requirement of training in Acute Medicine. This specialist skill must be acquired before the date of the trainees CCT. For some trainees, this may be a procedural skill or a practical interest such as echocardiography, ultrasonography or scoping; while for others it may be an academic interest where they ll gain a qualification in healthcare management, leadership or medical education, or it could be developing an interest in another medical field such as stroke, intensive care medicine or medical toxicology. Some may choose to undertake a serious bit of medical research during their training years. Note: Please refer to the corresponding section in the AIM curriculum for a more exhaustive list of the types of specialist skills that may be acquired by trainees. The new Specialist Skill section on the SAM website also has a comprehensive list and detailed information on 23 possible options for specialist skill: In considering which specialist skill to develop, the trainee should consider how the acquisition of the skill may benefit the delivery of the Acute Medicine service overall. Choice of skill should take place as early in Acute Internal Medicine training as is possible. The skill should be one that can be used and developed throughout the physician s career. We try to accommodate the trainees choice of special skill and the sooner the decision is made the sooner we will be able to support this choice. However, if there is specific skill desired by the trainee before application but falls outside the options listed on the SAM website, trainees are encouraged to contact the programme director as early as possible. It is recommended that a trainee should choose only ONE specialist skill in which to achieve competence. It is not anticipated that any trainee should be trying to adopt extensive experience in multiple skills during the training programme. Whichever specialist skill the trainee chooses there must be robust arrangements for training, assessment of competence, and maintenance of competence as defined by the relevant authority for each skill (e.g. BSE for echocardiography or JAG for endoscopy). It is important that an individual trainee recognises that continued exposure to and practise of a procedural skill is the only way to sustain competence in that skill. The choice of procedural skill should therefore be made whilst taking into account which is most likely to be required by the health service after training is complete. Discussion with the programme director or Educational Supervisor is recommended when making this decision. 18
19 Curricula Both the AIM and GIM curricula along with respective ARCP decision aids are available on the JRCPTB website or accessible through links on your e-portfolio. These documents outline the competencies required to achieve your CCT, including the requirements for assessments and progress at each stage of your training. It is important to ensure that evidence of your training is uploaded to your e- portfolio on a regular basis, with adequate linking between your assessments or reflections and relevant parts of the curriculum (NB: you can link to more than one part of your curriculum). AIM Curriculum AIM curriculum 2009 (amended 2012) & decision aid (revised November 2014) The AIM curriculum has been designed to enable StRs on completion of CCT to apply for Acute Medicine consultant posts armed with competencies for the delivery of high quality medical care to acutely ill patients and also the managerial skills required to run AMUs. The curriculum emphasises the skills and competencies that must be acquired in the acute medical settings but also reflects those that are relevant to the inpatient and outpatient settings including ambulatory care. Specific competencies in the management of patients requiring level 2 care are also mandatory for trainees undertaking training in AIM. It also details how these competencies will be assessed as a trainee progresses through the syllabus. GIM Curriculum GIM curriculum 2009 (amended 2012) & decision aid (revised November 2014) Within the GIM curriculum there is an emphasis on the training of physicians with the ability to investigate, treat and diagnose patients with chronic medical symptoms, with the provision of high quality review skills for inpatients and outpatients fulfilling the requirement of consultant-led continuity of care. While these attributes are not emphasised in the AIM curriculum it is clear that these are competencies that must be acquired for those pursuing a dual CCT in AIM and GIM. It is recognised that there is a hierarchy of competencies within each curriculum. It is expected that the breadth and depth of evidence presented for the emergency presentations, top symptom presentations and procedures will be greater than that for the common competencies and the other important presentations which should be sampled to a lesser extent i.e. work place assessment evidence is not required for all of these competencies. However, there must be evidence of engagement with that section of the curriculum. 19
20 E-portfolio (JRCPTB) Trainees are required to register for specialist training with JRCPTB at the start of their training programmes. Enrolment with JRCPTB is mandatory and has an enrolment fee, which can either be paid to the JRCPTB with an upfront one off payment of 845 (tax deductible) in 2016, or as instalments of 169 per annum paid alongside collegiate membership. The maximum duration of payment is 5 years (even if you take longer to complete your training). Trainees can enrol online at On enrolling with JRCPTB trainees will be given access to the e-portfolio. This web-based e-portfolio is where trainees should record their assessments, appraisals, reflections on learning experiences, acquisition of competencies and progress through training. It allows evidence to be built up to inform decisions on a trainee s progress and provides tools to support trainees education and development. Note: the JRCPTB will not provide a paper-based alternative to the e-portfolio. It is important to become familiar with the different components of the e-portfolio early in your training, as it provides evidence of adequate progression, assessed at your annual ARCP. It includes a record of meetings with your educational supervisor, Clinical supervisor, examination and certificates, personal library (80MB limit), workplace based assessments (WPBAs) / Supervised Learning Events (SLEs) with links to your curriculum and Annual Review of Competence Progression (ARCP) outcomes. It is primarily the trainee s responsibility to ensure the e-portfolio is kept up to date though supervisors also have access to shared parts of the portfolio and have a responsibility to record appraisal outcomes and sign off the record of competence. The trainee must also arrange assessments and ensure they are recorded, prepare drafts of appraisal forms, maintain their personal development plan, record their reflections on learning and record their progress through the curriculum. If you have any difficulties in engaging your ES in the e-portfolio you must inform the TPD immediately it will not be accepted as a reason for incomplete information provided at your ARCPs. 20
21 E-Portfolio - Key points Ensure that all of your personal details including address are kept up to date within the Profile section. You should complete a PDP (personal development plan) at the start of each clinical attachment and prior to your ARCP to outline your objectives for your next placement (this information will be used to plan the rotation) Each review meeting and report entered by your ES must include that it covers both Acute Medicine & GIM (if working towards dual accreditation) You should review the decision aids for both Acute Medicine & GIM at the start of each placement so that you are aware of your requirements for the forthcoming year this includes the appropriate number of SLEs Your e-portfolio and assessments should be updated regularly throughout the year and linked to the relevant parts of the curriculum. The number of times an SLE can be linked to curriculum competencies is limited to eight for each ACAT and two for CbD & mini-cexs Your ES should sign off the different components of your curriculum. This can be very time consuming but can now be done as a group sign off or sampling of the curriculum rather that exhaustively sign off every competence. It is worth using the Royal College of Physicians diary to record your CPD activity an annual summary can be uploaded as a PDF to your personal library (it is also recommended at your GIM PYA) Courses etc can only be validated if certificates are uploaded to your e-portfolio (this usually requires completion of feedback) Any absences from work should be recorded on your e-portfolio. You will be required to complete a trainee absence form, sent to you by the deanery, ahead of your ARCP every year. Your TPD should be notified of periods > 2 weeks, which may potentially require an extension to your CCT date. The assessments required for stage of the training programme is summarised in the AIM and GIM decision aids (see links in Curricula chapter). An overview is provided below, however this is not exhaustive: 21
22 Overview of AIM training requirements 1. Educational Supervisor (ES) report to cover training year since last ARCP Multiple Consultant Report (MCR) must be completed annually each MCR must be completed by either the trainee s clinical supervisor / clinical placement coordinator or consultants who the trainee has regular working contact with (not consultants that trainees have fleeting contact with e.g. on-call). For dual accrediting trainees, 2 MCRs must include feedback on GIM clinical abilities. Summary of the MCR and any actions resulting to be recorded in ES report 3. Specialist Certificate Exam (SCE) AIM SCE usually taken in years 3 or 4 and achieved by CCT 4. Valid ALS throughout training (these are valid for 4 years) evidenced in the Certificate and Exams section of your e-portfolio. 5. Supervised Learning Events (SLEs) - Minimum of 10 SLEs (ACATs, CbDs and mini CEX) per year of training to include a minimum of 6 ACATs SLEs should be performed proportionately throughout each training year by a number of different assessors across the breadth of the curriculum. Structured feedback should be given to aid the trainee s personal development 6. Multi-source feedback (MSF) - Minimum of 12 raters including 3 consultants and a mixture of other staff (medical and non-medical) Replies should be received within 3 months for a valid MSF. If significant concerns are raised then arrangements should be made for a repeat MSF. An MSF should be completed per year. Don t forget your self-assessment! 7. A Patient Survey should be completed in the first two years and another in the last two years e.g. during years 2 and 4 (i.e. ST4 and ST6). 8. AIM Audit or AIM Quality Improvement projects 4 before CCT one of which must complete the loop. Ideally a Quality Improvement assessment (QIPAT) or Audit assessment should be performed 9. Teaching observation 1 before PYA 10. Signed off for: common competencies, emergency presentations, top presentations & other important presentations. One assessment in each major domain should be covered during your placement 11. Common competencies - Confirmation by educational supervisor that level 3 or 4 achieved. Ten do not require linked evidence unless concerns are identified. Evidence of engagement with 75% of remaining competencies to be determined by sampling and level achieved recorded in the ES report 22
23 12. Emergency presentations Evidence of engagement required for all 4 emergency presentations by end of AIM training. ES to confirm level achieved and complete rating for each presentation. Evidence to include ACATs, mini-cexs and CbDs 13. Top presentations. Evidence of engagement required for all top presentations by end of AIM training. Level achieved to be determined by sampling and recorded in ES report 14. Practical procedures - summative DOPS evidence required for each of the following: a. Clinically independent by completion of ST3 for: i. Central venous cannulation (by femoral approach as a minimum) with ultrasound guidance where appropriate* ii. Abdominal paracentesis* iii. DC cardioversion iv. Knee aspiration b. Clinically independent by completion of year 3 AIM for: i. Intercostal drainage (1) Pneumothorax insertion using Seldinger technique* ii. Intercostal drainage (2) Pleural Effusion using Seldinger technique following ultrasound guidance* iii. By PYA: signed off for CVP line insertion, intercostal drain insertion using ultrasound c. Clinically independent by PYA for: i. Arterial line d. Competent in skills lab by PYA for (these have been removed from the curriculum though there may be a delay until the decision aid is updated): i. Temporary cardiac pacing via transvenous route* ii. Sengstaken- Blakemore Tube insertion* Summative sign off for routine procedures to be undertaken on one occasion with one assessor to confirm clinical independence. Summative DOPS sign off for potentially life threatening procedures (marked with asterisk) to be undertaken on at least two occasions with two different assessors (one assessor per occasion) 15. Clinical activity - Annual Summary of Training Calculator uploaded to your personal library: a. Acute take: 1250 patients seen before CCT b. Ambulatory Care: 300 new patients seen before CCT 16. Clinical experience with relevant competencies in AMU, Cardiovascular medicine, Respiratory Medicine, Geriatric Medicine, Intensive Care Medicine Specialist Skill training 17. Teaching satisfactory record of teaching attendance (should be specified at induction but evidence of attendance at a minimum of 70% of deanery training days 23
24 should be achieved) with 100 hours external AIM teaching (including regional teaching days) before CCT Overview of GIM training requirements For dually accrediting trainees - as per AIM requirements except: / in addition to AIM requirements 1. GIM Audit or GIM Quality Improvement projects Need to have lead one before CCT one of which must complete the loop. Quality Improvement assessment tool (QIPAT) or Audit assessment (AA) to be performed 2. Multiple Consultant Reports (MCR) of the 4-6 MCRs that must be completed annually, 2 MCRs must include feedback on GIM clinical abilities for dual accrediting trainees 3. Clinical activity: o GIM Acute Take: 1000 patients seen before CCT o Outpatients clinics (or equivalent): 186 clinics performed before CCT (approximately 1500 outpatients) Please note: AIM trainees dually accrediting with GIM can count new ambulatory care patient contact experience as outpatients for the GIM curriculum. Each SLEs can be linked to both AIM and GIM curriculums i.e. the SLEs do not need to be duplicated for the purposes of satisfying both curriculum requirements. Similarly, though the absolute number required for each curriculum differs, the same patient contact experience can be counted towards the clinical activity requirements for both curriculums. 24
25 Workplace-based Assessments (WPBAs) The various workplace based assessment methods are described below. More information about these methods including guidance for trainees and assessors is available in the eportfolio and on the JRCPTB website These assessment tools are available online in the eportfolio and assessments should be recorded in the trainee s eportfolio. Printable versions of some of the forms can be found in the document library on this website. Supervised Learning Events (SLEs) Trainees should aim for at least 10 SLEs (ACATs, CbDs and mini CEX) - to include a minimum of 6 ACATs. SLEs should be performed proportionately throughout each training year by a number of different assessors across the breadth of the curriculum. Structured feedback should be given to aid the trainee s personal development mini-clinical Evaluation Exercise (mini-cex) This supervised learning event tool evaluates a clinical encounter with a patient to provide feedback on skills essential for good clinical care such as history taking, examination and clinical reasoning. The trainee receives immediate feedback to aid learning. It can be used at any time and in any setting when there is a trainee and patient interaction and an assessor is available. Case-based Discussion (CbD) The CbD is a tool for supervised learning events based on a trainee's management of a patient and provides feedback on clinical reasoning, decision-making and application of medical knowledge in relation to patient care. It also serves as a method to document conversations about, and presentations of, cases by trainees. The CbD should focus on a written record (such as written case notes, out-patient letter, discharge summary). A typical encounter might be when presenting newly referred patients in the outpatient department. Direct Observation of Procedural Skills (DOPS) A DOPS is an assessment tool designed to evaluate the performance of a trainee in undertaking a practical procedure, against a structured checklist. The trainee receives immediate feedback to identify strengths and areas for development. DOPS have been separated into two categories for routine and life-threatening procedures, with a clear differentiation of formative and summative sign off. Formative DOPS for routine and potentially life threatening procedures should be undertaken before doing a summative DOPS and can be undertake as many times as the trainee and their supervisor feel is necessary. Summative DOPS should be undertaken as follows: Acute Care Assessment Tool (ACAT) The ACAT is designed to be used for supervised learning events on the acute medical take (but may be on a ward round or covering a day's management of admissions and 25
26 ward work). The ACAT looks at clinical assessment and management, decision-making, team working, time management, record keeping and handover for the whole time period and multiple patients. There should be a minimum of 5 cases for an ACAT assessment. Multi-source feedback (MSF) This tool is a method of assessing generic skills such as communication, leadership, team working, reliability etc, across the domains of Good Medical Practice. This provides objective systematic collection and feedback of performance data on a trainee, derived from a number of colleagues. Raters' are individuals with whom the trainee works, and includes doctors, administration staff, and other allied professionals. The trainee will not see the individual responses by raters, feedback is given to the trainee by the Educational Supervisor. Trainees are also required to complete a self-assessment form. If significant concerns are raised then arrangements should be made for a repeat MSF Patient Survey (PS) Patient Survey address issues, including behaviour of the doctor and effectiveness of the consultation, which are important to patients. It is intended to assess the trainee's performance in areas such as interpersonal skills, communication skills and professionalism by concentrating solely on their performance during one consultation. Patient survey guidance, survey forms and summary forms are available in the assessment section of the JRCPTB website. The summary form must be completed and signed off by your ES and then uploaded to your personal library as evidence. Audit Assessment (AA) The Audit Assessment tool is designed to assess a trainee's competence in completing an audit. The Audit Assessment can be based on review of audit documentation or on a presentation of the audit at a meeting. If possible the trainee should be assessed on the same audit by more than one assessor Quality improvement project assessment tool (QIPAT) The QIP Assessment tool is designed to assess a trainee's competence in completing a quality improvement project. The trainee should be given immediate feedback to identify strengths and areas for development. All workplace-based assessments are intended primarily to support learning so this feedback is very important. The QIP Assessment can be based on review of QIP documentation OR on a presentation of the QIP at a meeting. If possible the trainee should be assessed on the same QIP by more than one assessor. Assessors can be any doctor with suitable experience - for trainees in higher speciality training this is likely to be consultants. Teaching Observation (TO) The Teaching Observation is designed to provide structured, formative feedback to trainees on their competence at teaching. The Teaching Observation can be based on any instance of formalised teaching by the trainee which has been observed by the assessor. The process should be trainee-led (identifying appropriate teaching sessions and assessors) and one TO should be completed before PYA in AIM & GIM 26
27 Multiple Consultant Report (MCR) The Multiple Consultant Report (MCR) was introduced in 2013 and is designed to capture the views of consultant supervisors on a trainee's clinical performance. It must be completed by a minimum of 4 consultants (maximum of six) or associate specialists / speciality doctors (not trainees) who are able to provide feedback on a trainee's clinical performance. Educational supervisors should not be asked to complete an MCR for their own trainees as they will complete the ES report. Note these are different to MSF assessments. Each MCR form is completed by a single consultant who should either be the trainee s clinical supervisor (or clinical placement coordinator) or a consultant who the trainee has regular working contact with and not a consultant who the trainee may have fleeting contact with e.g. on-call. For dual accrediting trainees with GIM, 2 MCRs must include feedback on GIM clinical abilities. A summary of the MCR and any actions resulting is to be recorded in the ES s report. Therefore if four MCRs are required, four consultants should complete a form each resulting in four MCR forms. The MCRs will be automatically collated and summarised in the MCR Year Summary Sheet that will inform the ES report at the end of the training year. The MCR requests feedback on clinical performance and must be completed in addition to the Multi Source Feedback (MSF) tool. The same consultant may be approached to complete both forms. Out of programme trainees are also advised to complete these reports. Trainees who are less than full time should complete the number of MCRs pro rata following discussion with their education supervisor. Further information is available in the assessment section of the JRCPTB website. Audits AIM trainees are required to complete four audits or quality improvement projects (QIP) prior to CCT (one per year), one of which must complete the loop. These should be uploaded to the personal library. An audit assessment tool or QIPAT assesses a trainee s competency in completing an audit / QIP and must be completed after review of the documentation or presentation at a meeting. Those trainees dually accrediting with GIM are also required to complete a single GIM audit / QIP prior to CCT (and complete an audit assessment tool). Ideally an audit should be commenced near the start of the placement so there is an opportunity to perform a second/further cycle later in the year. Involvement in a local service development is also equally acceptable. Annual Summary of Training Calculator This calculator calculates your acute medical and outpatient experience. It is available for download from the GIM section of the Wales deanery website (see below link), with an alternative version downloadable from the GIM section of the JRCPTB website: 27
28 It should be updated annually and uploaded to your personal library. The AIM decision aid stipulates that 1250 acute take patients and 300 new Ambulatory care patients should be seen prior to CCT, whilst the GIM decision aid states that 1000 patients should be seen on the acute intake and 186 outpatient clinics attended (approx 1500 outpatients) before a trainees CCT date. Personal library This section of the e-portfolio allows you to upload electronic documents to provide evidence of your training (ALS/SCE/CPD certificates, audits etc). You can upload any file type, however it is limited to 80MB of space. The files can be organised into folders & subfolders. Training quality surveys The national GMC training survey serves to monitor the quality of medical education and training in the UK. In addition an online placement survey is sent out towards the end of each rotation. Completion is a mandatory requirement of training and allows the quality and balance of the training rotations to be maintained. Annual calendar February: AIM Trainee Survey March : ST Applications April: ST3 Interviews May: Society for Acute Medicine Spring Conference May: Spring Meeting of the Society of Physicians in Wales (Portmeirion) May: AIM ARCPs May/June : Acute Medicine Summer School May/June: Welsh Acute Physicians Society Spring Symposium June: Society of Acute Medicine Benchmarking Audit (SAMBA) June/July: Acute Medicine Awareness Week September: Society for Acute Medicine International Conference September: GIM ARCPs October: Welsh Acute Physicians Society Autumn Symposium November: Society of Physicians of Wales and Royal College of Physicians Joint Update in General and Acute Medicine (Cardiff) 28
29 Training days and leave Acute Medicine Summer School The Acute Medicine Summer School is an annual training week arranged for Acute Medicine trainees and is held alternately between North and South Wales, usually at a rural hotel location. It provides a varied programme of activities including service improvement workshops, video simulation sessions on emergency clinical scenarios, practical procedure workshops, debates on contentious clinical issues, a journal club, guideline updates and a number of talks by distinguished local and national speakers on a range of different topics. One of the training days is a national Acute Medicine Symposium organised by WAPS. Attendance is mandatory and it is the responsibility of the trainee to ensure that any oncall commitments are swapped to allow attendance. Any difficulty in obtaining leave for the mandatory training week should be reported to the TPD as soon as possible. Welsh Acute Physicians Society (WAPS) The recently formed Welsh Acute Physicians' Society is dedicated to furthering Acute Medicine and supporting trainees in Wales. The group was set up predominantly by a group of acute medicine trainees to raise the profile of the speciality across Wales but is open to all those with an interest in acute medical care and education. The society organises educational events such as the Acute Medicine Symposium, which provides 6 CPD points. Trainees joining the training programme will automatically gain membership to this society and free entry to all symposiums. GIM Training Several GIM core curriculum training courses are available each year, with dates advertised in your e-portfolio. The mandatory GIM core curriculum training days required for CCT are: Core Management & Leadership Training Teaching Techniques Communication Skills Medical Law Assessing Trainees Medical Ethics Trainees are also required to attend at least 3 GIM generic curriculum regional StR teaching days (around 4 per year). These courses are arranged by the deanery and take 29
30 place in South Wales with video link available to North Wales trainees. You may need to contact the organisers to find out dates and get onto lists. If the trainee does not comply with the minimum attendance percentage of 70%, they will obtain an unsatisfactory ARCP outcome. Currently the North Wales days are organised by Dr. Ben Thomas or Dr. David Glover in Wrexham Maelor Hospital. Booking contact: or The South Wales teaching days are managed by Dr Aled Roberts (STC Chair) & Dr Biju Mohamed (TPD). Any enquiries, should be directed to Dr Roberts or Dr Mohamed GIM courses are advertised on the e-portfolio and RCP / Wales deanery website. For full information on dates or to book your place on the training days, please contact Miss Ceri Cook at the Wales Deanery: McGowanR@cardiff.ac.ukTel no: You are required to provide evidence of 100 hours of external GIM CPD points prior to your CCT. We advise registering for the RCP CPD diary a summary of your CPD for each year can be uploaded to your personal library as a PDF (this is also recommendation at your GIM PYA). Study Leave The Wales Deanery defines the study leave budget annually (currently capped at around 800 per trainee). Each specialist trainee is entitled to 30 days study leave per annum. Attendance at ARCPs and core curriculum for specialist trainees is mandatory and therefore not deducted from your annual study leave. All study leave must be requested and authorised using the INTREPID 10 online system. This database keeps a record of all leave taken throughout your training and remaining study leave budget available. Study leave will be granted at the discretion of your departmental leave coordinator. Most hospitals require a minimum of 6 weeks notice to allow cancellation of outpatient clinics and other clinical commitments, although this can vary between different Health Boards (this should be discussed at your local induction meeting). Annual leave Trainees in their first five years of NHS employment are entitled 27 days of annual leave, increasing to 32 days thereafter. Similar to study leave, at least 6 weeks notice is often required to allow cancellation of your clinical commitments. The process for gaining annual leave will vary between Health Boards and should be discussed at your local induction meeting at the start of your placement. 30
General Internal Medicine (GIM) ARCP Decision Aid AUGUST 2017
 ARCP Decision Aid AUGUST 2017") General Internal Medicine (GIM) ARCP Decision Aid AUGUST 2017 The ARCP decision aid documents the targets to be achieved for a satisfactory ARCP outcome at the end of each training level. This document
General Internal Medicine (GIM) ARCP Decision Aid AUGUST 2017 The ARCP decision aid documents the targets to be achieved for a satisfactory ARCP outcome at the end of each training level. This document
Core Medical Training (CMT) ARCP Decision Aid revised November 2014
 ARCP Decision Aid revised November 2014") Core Medical Training (CMT) ARCP Decision Aid revised November 2014 The table that follows includes a column for each training year within core medical training, documenting the targets that have to be
Core Medical Training (CMT) ARCP Decision Aid revised November 2014 The table that follows includes a column for each training year within core medical training, documenting the targets that have to be
RESPIRATORY REGISTRAR TRAINEE INDUCTION PACK
 Page1 RESPIRATORY REGISTRAR TRAINEE INDUCTION PACK The British Thoracic Society (BTS) and its Specialist Trainees Advisory Group (STAG) feel it is very important to have high quality induction packs for
Page1 RESPIRATORY REGISTRAR TRAINEE INDUCTION PACK The British Thoracic Society (BTS) and its Specialist Trainees Advisory Group (STAG) feel it is very important to have high quality induction packs for
Wales Foundation School
 Wales Foundation School A guide for Foundation Doctors commencing August 2017 Contents: Welcome and contact details Assessments & e-portfolio TAB guidance Progression and sign off ARCP Absence from Training
Wales Foundation School A guide for Foundation Doctors commencing August 2017 Contents: Welcome and contact details Assessments & e-portfolio TAB guidance Progression and sign off ARCP Absence from Training
GUIDANCE NOTES, PROCESS & APPLICATION FORM FOR FOUNDATION YEAR 1 APPLICANTS WITH SPECIAL CIRCUMSTANCES MATCHING TO LOCATION AND PROGRAMME 2018/19
 This document describes the allocation process for Foundation Year 1 applicants with special circumstances, once they have been allocated to the Wales Foundation School. The national process for allocating
This document describes the allocation process for Foundation Year 1 applicants with special circumstances, once they have been allocated to the Wales Foundation School. The national process for allocating
SPECIALTY TRAINING CURRICULUM FOR NUCLEAR MEDICINE AUGUST 2010
 SPECIALTY TRAINING CURRICULUM FOR NUCLEAR MEDICINE AUGUST 200 Joint Royal Colleges of Physicians Training Board 5 St Andrews Place Regent s Park London NW 4LB Telephone: (020) 793574 Facsimile: (020)7486
SPECIALTY TRAINING CURRICULUM FOR NUCLEAR MEDICINE AUGUST 200 Joint Royal Colleges of Physicians Training Board 5 St Andrews Place Regent s Park London NW 4LB Telephone: (020) 793574 Facsimile: (020)7486
Curriculum for Internal Medicine Stage 1 Training
 Curriculum for Internal Medicine Stage 1 Training Implementation August 2019 Contents 1. Introduction 3 2. Purpose 3 2.1 Purpose statement 3 2.2 Rationale 4 2.3 Development 7 2.4 Training Pathway 7 2.5
Curriculum for Internal Medicine Stage 1 Training Implementation August 2019 Contents 1. Introduction 3 2. Purpose 3 2.1 Purpose statement 3 2.2 Rationale 4 2.3 Development 7 2.4 Training Pathway 7 2.5
106,717 people accessed mental health. 192,192 access A&E. 1,011,942 patient contacts with community staff. 2,245,439 patient contacts
 Employs 15,285 2,245,439 patient contacts 192,192 Assisted 91,360 Dispensed 13,598,605 prescription items** 38,107 1,011,942 patient contacts with Across 11 clusters, 540,850 people are registered with
Employs 15,285 2,245,439 patient contacts 192,192 Assisted 91,360 Dispensed 13,598,605 prescription items** 38,107 1,011,942 patient contacts with Across 11 clusters, 540,850 people are registered with
Palliative Medicine ARCP Decision Aid REVISED SEPTEMBER 2015
 Palliative Medicine ARCP Decision Aid REVISED SEPTEMBER 2015 The guidance below documents the targets that have to be achieved for a satisfactory ARCP outcome at the end of each training year. This decision
Palliative Medicine ARCP Decision Aid REVISED SEPTEMBER 2015 The guidance below documents the targets that have to be achieved for a satisfactory ARCP outcome at the end of each training year. This decision
STROKE MEDICINE SUB SPECIALTY TRAINING
 STROKE MEDICINE SUB SPECIALTY TRAINING ENTRY CRITERIA ESSENTIAL CRITERIA Qualifications Applicants must have: MBBS or equivalent medical qualification MRCP (UK) full diploma or EEA eligibility ii at time
STROKE MEDICINE SUB SPECIALTY TRAINING ENTRY CRITERIA ESSENTIAL CRITERIA Qualifications Applicants must have: MBBS or equivalent medical qualification MRCP (UK) full diploma or EEA eligibility ii at time
Title of the Health Board Report
 AGENDA ITEM 3.2 Title of the Health Board Report IMPLEMENTING THE OUTCOME OF THE SOUTH WALES PROGRAMME THROUGH ACUTE CARE ALLIANCES AND DEVELOPMENT OF THE SOUTH WALES HEALTH COLLABORATIVE Executive Lead:
AGENDA ITEM 3.2 Title of the Health Board Report IMPLEMENTING THE OUTCOME OF THE SOUTH WALES PROGRAMME THROUGH ACUTE CARE ALLIANCES AND DEVELOPMENT OF THE SOUTH WALES HEALTH COLLABORATIVE Executive Lead:
CARDIOLOGY ST3 ESSENTIAL CRITERIA
 ENTRY CRITERIA CARDIOLOGY ST3 ESSENTIAL CRITERIA Applicants must have: MBBS or equivalent medical qualification Qualifications MRCP (UK) Part 1 or EEA eligibility ii at time of application MRCP (UK) full
ENTRY CRITERIA CARDIOLOGY ST3 ESSENTIAL CRITERIA Applicants must have: MBBS or equivalent medical qualification Qualifications MRCP (UK) Part 1 or EEA eligibility ii at time of application MRCP (UK) full
HAEMATOLOGY ST3 ESSENTIAL CRITERIA
 ENTRY CRITERIA HAEMATOLOGY ST3 ESSENTIAL CRITERIA Applicants must have: MBBS or equivalent medical qualification Qualifications MRCP (UK) Part 1 or MRCPCH Part 1 A and B or EEA eligibility ii at time of
ENTRY CRITERIA HAEMATOLOGY ST3 ESSENTIAL CRITERIA Applicants must have: MBBS or equivalent medical qualification Qualifications MRCP (UK) Part 1 or MRCPCH Part 1 A and B or EEA eligibility ii at time of
Your local NHS and you
 South Wales Programme Local Engagement Document Your local NHS and you Local NHS services in Cardiff and the Vale of Glamorgan are run by Cardiff and Vale University Health Board (UHB). The UHB is one
South Wales Programme Local Engagement Document Your local NHS and you Local NHS services in Cardiff and the Vale of Glamorgan are run by Cardiff and Vale University Health Board (UHB). The UHB is one
RHEUMATOLOGY ST3 ESSENTIAL CRITERIA
 ENTRY CRITERIA RHEUMATOLOGY ST3 ESSENTIAL CRITERIA Applicants must have: MBBS or equivalent medical qualification Qualifications MRCP (UK) Part 1 or EEA eligibility ii at time of application MRCP (UK)
ENTRY CRITERIA RHEUMATOLOGY ST3 ESSENTIAL CRITERIA Applicants must have: MBBS or equivalent medical qualification Qualifications MRCP (UK) Part 1 or EEA eligibility ii at time of application MRCP (UK)
Visit to Hull & East Yorkshire Hospitals NHS Trust
 Yorkshire and the Humber regional review 2014 15 Visit to Hull & East Yorkshire Hospitals NHS Trust This visit is part of a regional review and uses a risk-based approach. For more information on this
Yorkshire and the Humber regional review 2014 15 Visit to Hull & East Yorkshire Hospitals NHS Trust This visit is part of a regional review and uses a risk-based approach. For more information on this
Training capacity and Rostering
 GUIDANCE FOR TRAINING UNITS IN INTENSIVE CARE MEDICINE This guidance pertains to trainees undertaking blocks in Intensive Care Medicine while pursuing the 2011 standalone curriculum for a CCT in ICM either
GUIDANCE FOR TRAINING UNITS IN INTENSIVE CARE MEDICINE This guidance pertains to trainees undertaking blocks in Intensive Care Medicine while pursuing the 2011 standalone curriculum for a CCT in ICM either
The Trainee Doctor. Foundation and specialty, including GP training
 Foundation and specialty, including GP training The duties of a doctor registered with the General Medical Council Patients must be able to trust doctors with their lives and health. To justify that trust
Foundation and specialty, including GP training The duties of a doctor registered with the General Medical Council Patients must be able to trust doctors with their lives and health. To justify that trust
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine
 Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Supporting revalidation: methods and evidence
 PROFESSIONAL ISSUES Supporting revalidation: methods and evidence Kirstyn Shaw and Mary Armitage Kirstyn Shaw BSc PhD, Clinical Standards Project Manager, Clinical Effectiveness and Evaluation Unit, Royal
PROFESSIONAL ISSUES Supporting revalidation: methods and evidence Kirstyn Shaw and Mary Armitage Kirstyn Shaw BSc PhD, Clinical Standards Project Manager, Clinical Effectiveness and Evaluation Unit, Royal
Curriculum for Specialty Training in Medical Virology
 Curriculum for Specialty Training in Medical Virology Incorporating Combined Infection Training, developed in conjunction with the JRCPTB Approved 6 May 204 Contents INTRODUCTION... 3. RATIONALE... 3 2.
Curriculum for Specialty Training in Medical Virology Incorporating Combined Infection Training, developed in conjunction with the JRCPTB Approved 6 May 204 Contents INTRODUCTION... 3. RATIONALE... 3 2.
Multi-Professional Deanery
 Multi-Professional Deanery SCHOOL VISIT REPORT Visiting School Date visited Medicine April 18 th 2013 Local Education Provider (LEP) visited Princess Alexandra Hospital NHS Trust Visiting team Ian Barton,
Multi-Professional Deanery SCHOOL VISIT REPORT Visiting School Date visited Medicine April 18 th 2013 Local Education Provider (LEP) visited Princess Alexandra Hospital NHS Trust Visiting team Ian Barton,
SPECIALTY TRAINING CURRICULUM FOR NUCLEAR MEDICINE
 SPECIALTY TRAINING CURRICULUM FOR NUCLEAR MEDICINE Approved 3 August 204 (updated October 206) To be implemented August 205 Joint Royal Colleges of Physicians Training Board 5 St Andrews Place Regent s
SPECIALTY TRAINING CURRICULUM FOR NUCLEAR MEDICINE Approved 3 August 204 (updated October 206) To be implemented August 205 Joint Royal Colleges of Physicians Training Board 5 St Andrews Place Regent s
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Intensive Care Medicine (ST3)
") Intensive Care Medicine (ST3) Entry Criteria Qualifications Eligibility Essential Criteria When Evaluated 1 AND MBBS or equivalent medical qualification Anaesthetics via CAT or ACCS (Anaesthetics) or equivalent:
Intensive Care Medicine (ST3) Entry Criteria Qualifications Eligibility Essential Criteria When Evaluated 1 AND MBBS or equivalent medical qualification Anaesthetics via CAT or ACCS (Anaesthetics) or equivalent:
Supervision of Trainee Doctors
 Appendix 13 Supervision of Trainee Doctors Good Medical Practice Supervision of Trainee Doctors Teaching, training, appraising and assessing doctors and students are important for the care of patients
Appendix 13 Supervision of Trainee Doctors Good Medical Practice Supervision of Trainee Doctors Teaching, training, appraising and assessing doctors and students are important for the care of patients
PAEDIATRIC CARDIOLOGY ST4
 ENTRY CRITERIA PAEDIATRIC CARDIOLOGY ST4 ESSENTIAL CRITERIA Applicants must have: MBBS or equivalent medical qualification Qualifications MRCPCH full diploma or on GMC specialist register for paediatrics
ENTRY CRITERIA PAEDIATRIC CARDIOLOGY ST4 ESSENTIAL CRITERIA Applicants must have: MBBS or equivalent medical qualification Qualifications MRCPCH full diploma or on GMC specialist register for paediatrics
IMPLEMENTING THE OUTCOME OF THE SOUTH WALES PROGRAMME THROUGH ACUTE CARE ALLIANCES AND DEVELOPMENT OF THE SOUTH WALES HEALTH COLLABORATIVE
 AGENDA ITEM 3.3 9 September 2014 IMPLEMENTING THE OUTCOME OF THE SOUTH WALES PROGRAMME THROUGH ACUTE CARE ALLIANCES AND DEVELOPMENT OF THE SOUTH WALES HEALTH COLLABORATIVE Executive Lead: Chief Executive
AGENDA ITEM 3.3 9 September 2014 IMPLEMENTING THE OUTCOME OF THE SOUTH WALES PROGRAMME THROUGH ACUTE CARE ALLIANCES AND DEVELOPMENT OF THE SOUTH WALES HEALTH COLLABORATIVE Executive Lead: Chief Executive
INTENSIVE CARE MEDICINE ST3
 INTENSIVE CARE MEDICINE ST3 ENTRY CRITERIA ESSENTIAL CRITERIA Applicants must have: MBBS or equivalent medical qualification Qualifications WHEN EVALUATED i Applicants from an Anaesthetics training background,
INTENSIVE CARE MEDICINE ST3 ENTRY CRITERIA ESSENTIAL CRITERIA Applicants must have: MBBS or equivalent medical qualification Qualifications WHEN EVALUATED i Applicants from an Anaesthetics training background,
HEALTH EDUCATION NORTH WEST ANNUAL ASSESSMENT VISIT
 Health Education North West HEALTH EDUCATION NORTH WEST ANNUAL ASSESSMENT VISIT VISITORS:- Postgraduate Dean: Professor David Graham PUBLIC HEALTH ith 9" October 2013 Associate Director of Postgraduate
Health Education North West HEALTH EDUCATION NORTH WEST ANNUAL ASSESSMENT VISIT VISITORS:- Postgraduate Dean: Professor David Graham PUBLIC HEALTH ith 9" October 2013 Associate Director of Postgraduate
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Contents. Foundation Programme Reference Guide 2016
 Reference Guide May 2016 Contents 1. Introduction and background... 5 2. Foundation Programme: policy and organisation... 6 THE UK FOUNDATION PROGRAMME OFFICE (UKFPO)... 6 UK HEALTH DEPARTMENTS... 6 HEALTH
Reference Guide May 2016 Contents 1. Introduction and background... 5 2. Foundation Programme: policy and organisation... 6 THE UK FOUNDATION PROGRAMME OFFICE (UKFPO)... 6 UK HEALTH DEPARTMENTS... 6 HEALTH
Mental Health training in Foundation Programmes
 Mental Health training in Foundation Programmes Paul Baker Deputy Postgraduate Dean Health Education North West Overview What is foundation training? National and regional context Role of clinical supervisor
Mental Health training in Foundation Programmes Paul Baker Deputy Postgraduate Dean Health Education North West Overview What is foundation training? National and regional context Role of clinical supervisor
GUIDANCE ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY
 ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
An Overview for F2 Doctors of Foundation Programme attachments to General Practice
 An Overview for F2 Doctors of Foundation Programme attachments to General Practice July 2011 Contents Page GP Placements 2 Guidance on Educational Agreements 4 Key facts about F2 Placements 6 The Foundation
An Overview for F2 Doctors of Foundation Programme attachments to General Practice July 2011 Contents Page GP Placements 2 Guidance on Educational Agreements 4 Key facts about F2 Placements 6 The Foundation
MORTALITY OF POWYS CITIZENS. Medical Director. This paper supports:
 MORTALITY OF POWYS CITIZENS QUALITY & SAFETY COMMITTEE 05 MAY 2016 AGENDA ITEM 2.2 Report of Medical Director Paper prepared by Safety & Quality Improvement Manager Purpose of Paper Action/Decision required
MORTALITY OF POWYS CITIZENS QUALITY & SAFETY COMMITTEE 05 MAY 2016 AGENDA ITEM 2.2 Report of Medical Director Paper prepared by Safety & Quality Improvement Manager Purpose of Paper Action/Decision required
Rheumatology. Opportunities in UK
 Rheumatology Training Opportunities in UK Dr S Venkatachalam Consultant Rheumatologist, Cannock, UK Vice Chair Rheumatology Speciality Advisory Committee, UK Chair Rheumatology Speciality Training Committee,
Rheumatology Training Opportunities in UK Dr S Venkatachalam Consultant Rheumatologist, Cannock, UK Vice Chair Rheumatology Speciality Advisory Committee, UK Chair Rheumatology Speciality Training Committee,
CORE MEDICAL TRAINING PROGRAMME, WESSEX DEANERY
 CORE MEDICAL TRAINING PROGRAMME, WESSEX DEANERY This is a 2-year training programme in Core Medicine aimed at doctors who can demonstrate the essential competences to enter at the CT1 level of training.
CORE MEDICAL TRAINING PROGRAMME, WESSEX DEANERY This is a 2-year training programme in Core Medicine aimed at doctors who can demonstrate the essential competences to enter at the CT1 level of training.
Part II. The CCT in. Intensive Care Medicine. Assessment System. The Faculty of. Intensive Care Medicine
 Part II The CCT in Intensive Care Medicine Assessment System The Faculty of Intensive Care Medicine Contents 1. Principles of Assessment... 3 1.1 Training Stage Records... 3 1.2 How many workplace-based
Part II The CCT in Intensive Care Medicine Assessment System The Faculty of Intensive Care Medicine Contents 1. Principles of Assessment... 3 1.1 Training Stage Records... 3 1.2 How many workplace-based
Guidance on supporting information for revalidation
 Guidance on supporting information for revalidation Including specialty-specific information for medical examiners (of the cause of death) General introduction The purpose of revalidation is to assure
Guidance on supporting information for revalidation Including specialty-specific information for medical examiners (of the cause of death) General introduction The purpose of revalidation is to assure
PAEDIATRIC CARDIOLOGY ST4
 ENTRY CRITERIA PAEDIATRIC CARDIOLOGY ST4 ESSENTIAL CRITERIA Applicants must have: MBBS or equivalent medical qualification Qualifications MRCPCH full diploma or on GMC specialist register for paediatrics
ENTRY CRITERIA PAEDIATRIC CARDIOLOGY ST4 ESSENTIAL CRITERIA Applicants must have: MBBS or equivalent medical qualification Qualifications MRCPCH full diploma or on GMC specialist register for paediatrics
Non-emergency patient transport: the picture across Wales
 Non-emergency patient transport: the picture across Wales January 2018 0 P a g e Accessible formats If you would like this publication in an alternative format and/or language, please contact us. You can
Non-emergency patient transport: the picture across Wales January 2018 0 P a g e Accessible formats If you would like this publication in an alternative format and/or language, please contact us. You can
Supporting information for appraisal and revalidation: guidance for psychiatry
 Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Dartford and Gravesham NHS Trust Darent Valley Hospital INDUCTION HANDBOOK FOR THE ANAESTHETIC FACULTY GROUP
 Dartford and Gravesham NHS Trust Darent Valley Hospital INDUCTION HANDBOOK FOR THE ANAESTHETIC FACULTY GROUP August 2015 Page 1 KENT SURREY AND SUSSEX POSTGRADUATE DEANERY FOR MEDICAL AND DENTAL EDUCATION
Dartford and Gravesham NHS Trust Darent Valley Hospital INDUCTION HANDBOOK FOR THE ANAESTHETIC FACULTY GROUP August 2015 Page 1 KENT SURREY AND SUSSEX POSTGRADUATE DEANERY FOR MEDICAL AND DENTAL EDUCATION
SPECIALTY TRAINING PROGRAMME IN PALLIATIVE MEDICINE IN WESSEX DEANERY
 SPECIALTY TRAINING PROGRAMME IN PALLIATIVE MEDICINE IN WESSEX DEANERY This is a 4 year training programme in Palliative Medicine at ST3 level aimed at doctors who can demonstrate the essential competencies
SPECIALTY TRAINING PROGRAMME IN PALLIATIVE MEDICINE IN WESSEX DEANERY This is a 4 year training programme in Palliative Medicine at ST3 level aimed at doctors who can demonstrate the essential competencies
MEDICAL OPHTHALMOLOGY ST3
 ENTRY CRITERIA MEDICAL OPHTHALMOLOGY ST3 ESSENTIAL CRITERIA Applicants must have: Qualifications MBBS or equivalent medical qualification, and one of the following pathways Medical training MRCP (UK) Part
ENTRY CRITERIA MEDICAL OPHTHALMOLOGY ST3 ESSENTIAL CRITERIA Applicants must have: Qualifications MBBS or equivalent medical qualification, and one of the following pathways Medical training MRCP (UK) Part
Curriculum for Training for Advanced Critical Care Practitioners
 Edition 1 2015 Curriculum for Training for Advanced Critical Care Practitioners The Faculty of Intensive Care Medicine The Faculty of Intensive Care Medicine. This guidance may be reproduced for training
Edition 1 2015 Curriculum for Training for Advanced Critical Care Practitioners The Faculty of Intensive Care Medicine The Faculty of Intensive Care Medicine. This guidance may be reproduced for training
Postgraduate Quality Assurance Visit. Report on Wales Deanery 2011/12
 Postgraduate Quality Assurance Visit Report on Wales Deanery 2011/12 Contents Executive summary... 3 Summary of key findings... 5 Good practice... 5 Requirements... 7 Recommendations... 7 The Report...
Postgraduate Quality Assurance Visit Report on Wales Deanery 2011/12 Contents Executive summary... 3 Summary of key findings... 5 Good practice... 5 Requirements... 7 Recommendations... 7 The Report...
Supporting information for appraisal and revalidation: guidance for Supporting information for appraisal and revalidation: guidance for ophthalmology
 FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
Global Health Fellowships
 Global Health Fellowships APPLY NOW for an exciting opportunity to expand your horizons in Global Health in South Africa and enhance your GP competencies. Global Health Fellowships APPLY NOW for an exciting
Global Health Fellowships APPLY NOW for an exciting opportunity to expand your horizons in Global Health in South Africa and enhance your GP competencies. Global Health Fellowships APPLY NOW for an exciting
GP School Quality Monitoring Visits to GPSPT Programmes and Trusts
 Visiting Team Educational Roles GP Deputy Dean Associate GP Dean Training Programme Director GPST3 Name Dr Rebecca Viney Dr Roger Tisi Dr Sanjana Banka Dr Tutu Adewole Programme/Trust Team Educational
Visiting Team Educational Roles GP Deputy Dean Associate GP Dean Training Programme Director GPST3 Name Dr Rebecca Viney Dr Roger Tisi Dr Sanjana Banka Dr Tutu Adewole Programme/Trust Team Educational
Competencies in practice. A curriculum for internal medicine
 Competencies in practice A curriculum for internal medicine Drivers for Change Shape of Training Increased generalism Changing demography etc Published 2013 Generic Professional Capabilities (GMC) To be
Competencies in practice A curriculum for internal medicine Drivers for Change Shape of Training Increased generalism Changing demography etc Published 2013 Generic Professional Capabilities (GMC) To be
Level 2: Exceptional LEP Review Visit by School Level 3: Exceptional LEP Trigger Visit by Deanery with Externality... 18
 Postgraduate Training Ongoing Quality Review and Enhancement Framework Version 1: 2010 Contents Contents... 2 PMET Quality Review Framework Introduction... 3 Introduction... 3 Postgraduate Training Quality
Postgraduate Training Ongoing Quality Review and Enhancement Framework Version 1: 2010 Contents Contents... 2 PMET Quality Review Framework Introduction... 3 Introduction... 3 Postgraduate Training Quality
Professional Support for Doctors in Training
 Professional Support for Doctors in Training Guidance and support for trainees and trainers Professional Support for Doctors in Training 1. Introduction Almost all medical and dental trainees will complete
Professional Support for Doctors in Training Guidance and support for trainees and trainers Professional Support for Doctors in Training 1. Introduction Almost all medical and dental trainees will complete
Reproduced with kind permission from the Joint Programmes Board
 Multi-Source Feedback (MSF) The description and documentation described below is applicable to workplace based assessment. Self mini-pat (Peer Assessment Tool) for General Level Pharmacists Purpose Self
Multi-Source Feedback (MSF) The description and documentation described below is applicable to workplace based assessment. Self mini-pat (Peer Assessment Tool) for General Level Pharmacists Purpose Self
PTP Certificate of Equivalence
 PTP Certificate of Equivalence Programme Handbook 2014/15 18 September 2014 Version 4.0 For further information please contact the Academy for Healthcare Science: Academy for Healthcare Science - Registration
PTP Certificate of Equivalence Programme Handbook 2014/15 18 September 2014 Version 4.0 For further information please contact the Academy for Healthcare Science: Academy for Healthcare Science - Registration
Gynaecology Services Escalation Policy
 Gynaecology Services Escalation Policy Author: Women & Child Health Specialty: Gynaecology Date Approved: 18 th September 2013 Approved by: W&CH Quality & Safety Committee Date for Review: August 2016
Gynaecology Services Escalation Policy Author: Women & Child Health Specialty: Gynaecology Date Approved: 18 th September 2013 Approved by: W&CH Quality & Safety Committee Date for Review: August 2016
Ayrshire and Arran NHS Board
 Paper 12 Ayrshire and Arran NHS Board Monday 30 January 2017 Medical Education and Training: Update on Enhanced monitoring status of University Hospital Ayr Medical Department Author: Hugh Neill, Director
Paper 12 Ayrshire and Arran NHS Board Monday 30 January 2017 Medical Education and Training: Update on Enhanced monitoring status of University Hospital Ayr Medical Department Author: Hugh Neill, Director
14 May Armed Forces Covenant Framework for Wales
 14 May 2015 Armed Forces Covenant Framework for Wales Armed Forces Covenant Framework Background The first duty of the UK Government is the defence of the realm. The Armed Forces fulfill that responsibility
14 May 2015 Armed Forces Covenant Framework for Wales Armed Forces Covenant Framework Background The first duty of the UK Government is the defence of the realm. The Armed Forces fulfill that responsibility
British Cardiovascular Society. Revalidation of cardiologists: Standards and Content of a portfolio for revalidation
 Page 1 of 8 British Cardiovascular Society Revalidation of cardiologists: Standards and Content of a portfolio for revalidation David Hackett Vice-President, Clinical Standards Division August 2009 Introduction:
Page 1 of 8 British Cardiovascular Society Revalidation of cardiologists: Standards and Content of a portfolio for revalidation David Hackett Vice-President, Clinical Standards Division August 2009 Introduction:
Reference Guide. has bee. July 2012
 Reference Guide ument This doc n has bee for updated 2014 August July 2012 Contents 1. Introduction 4 2. The purpose of the Foundation Programme 5 3. Organisation of postgraduate training 7 4. Shape of
Reference Guide ument This doc n has bee for updated 2014 August July 2012 Contents 1. Introduction 4 2. The purpose of the Foundation Programme 5 3. Organisation of postgraduate training 7 4. Shape of
Equivalence Guidance for GMP Domain 1
 Equivalence Guidance for GMP Domain 1 From 1 st August 2011 the new GMC approved curriculum in Intensive Care Medicine (ICM) came into effect. As a result of this new curriculum, all equivalence applications
Equivalence Guidance for GMP Domain 1 From 1 st August 2011 the new GMC approved curriculum in Intensive Care Medicine (ICM) came into effect. As a result of this new curriculum, all equivalence applications
Care and Children and Young People's Services (England) (Children and Young People s Management) Entry code 10397
 (Children and Young People s Management) Entry code 10397") QCF Leadership for Health and Social Care Services Centre Handbook OCR Level 5 Diploma In Leadership for Health and Social Care and Children and Young People's Services (England) (Children and Young People
QCF Leadership for Health and Social Care Services Centre Handbook OCR Level 5 Diploma In Leadership for Health and Social Care and Children and Young People's Services (England) (Children and Young People
EMERGENCY MEDICINE ST4
 EMERGENCY MEDICINE ST4 ENTRY CRITERIA ESSENTIAL CRITERIA WHEN EVALUATED i Qualifications Applicants must have: MBBS or equivalent medical qualification MRCEM by time of appointment iv Applicants must:
EMERGENCY MEDICINE ST4 ENTRY CRITERIA ESSENTIAL CRITERIA WHEN EVALUATED i Qualifications Applicants must have: MBBS or equivalent medical qualification MRCEM by time of appointment iv Applicants must:
Care and Children and Young People's Services (England) (Adults Management) Entry code 10394
 (Adults Management) Entry code 10394") QCF Leadership for Health and Social Care Services Centre Handbook OCR Level 5 Diploma In Leadership for Health and Social Care and Children and Young People's Services (England) (Adults Residential Management)
QCF Leadership for Health and Social Care Services Centre Handbook OCR Level 5 Diploma In Leadership for Health and Social Care and Children and Young People's Services (England) (Adults Residential Management)
Revalidation Annual Report
 Paper 31 14 Revalidation Annual Report 2013-14 Purpose of Document: To provide the Board with a report on the first year s experience with medical revalidation in Public Health Wales. Board/Committee to-
Paper 31 14 Revalidation Annual Report 2013-14 Purpose of Document: To provide the Board with a report on the first year s experience with medical revalidation in Public Health Wales. Board/Committee to-
Initial education and training of pharmacy technicians: draft evidence framework
 Initial education and training of pharmacy technicians: draft evidence framework October 2017 About this document This document should be read alongside the standards for the initial education and training
Initial education and training of pharmacy technicians: draft evidence framework October 2017 About this document This document should be read alongside the standards for the initial education and training
Visit report on Royal Cornwall Hospital NHS Trust
 South West Regional Review 2016 Visit report on Royal Cornwall Hospital NHS Trust This visit is part of the South West regional review to ensure organisations are complying with the standards and requirements
South West Regional Review 2016 Visit report on Royal Cornwall Hospital NHS Trust This visit is part of the South West regional review to ensure organisations are complying with the standards and requirements
JOB DESCRIPTION. Dr Joble Joseph, Clinical Director for Medicine. Dan Gibbs, Interim Divisional Manager, Trauma, Emergency and Medicine (TEaM)
") JOB DESCRIPTION JOB TITLE: GRADE: International Fellow in Medicine Junior Clinical Fellow (JCF) HOURS: 40 Hours (Band 1A) RESPONSIBLE TO: ACCOUNTABLE TO: Dr Joble Joseph, Clinical Director for Medicine
JOB DESCRIPTION JOB TITLE: GRADE: International Fellow in Medicine Junior Clinical Fellow (JCF) HOURS: 40 Hours (Band 1A) RESPONSIBLE TO: ACCOUNTABLE TO: Dr Joble Joseph, Clinical Director for Medicine
INVESTIGATION UNDER SECTION 17 OF THE WELSH LANGUAGE ACT Betsi Cadwaladr University Local Health Board
 INVESTIGATION UNDER SECTION 17 OF THE WELSH LANGUAGE ACT 1993 Betsi Cadwaladr University Local Health Board Background The main aim of the Welsh Language Commissioner, an independent role created in accordance
INVESTIGATION UNDER SECTION 17 OF THE WELSH LANGUAGE ACT 1993 Betsi Cadwaladr University Local Health Board Background The main aim of the Welsh Language Commissioner, an independent role created in accordance
Visit to The Queen Elizabeth Hospital King s Lynn NHS Foundation Trust
 East of England regional review 2015 Visit to The Queen Elizabeth Hospital King s Lynn NHS Foundation Trust This visit is part of a regional review and uses a risk-based approach. For more information
East of England regional review 2015 Visit to The Queen Elizabeth Hospital King s Lynn NHS Foundation Trust This visit is part of a regional review and uses a risk-based approach. For more information
WESSEX DEANERY OUT OF HOURS GUIDELINES (Aug 2013)
") WESSEX DEANERY OUT OF HOURS GUIDELINES (Aug 2013) Introduction 1. Emergency and unscheduled work remains an essential part of Primary Health Care services and all General Practice Trainees must gain experience
WESSEX DEANERY OUT OF HOURS GUIDELINES (Aug 2013) Introduction 1. Emergency and unscheduled work remains an essential part of Primary Health Care services and all General Practice Trainees must gain experience
Programme Specification for the Post-graduate certificate in Cardiac Nursing
 Programme Specification for the Post-graduate certificate in Cardiac Nursing. PLEASE NOTE. This specification provides a concise summary of the main features of the programme and the learning outcomes
Programme Specification for the Post-graduate certificate in Cardiac Nursing. PLEASE NOTE. This specification provides a concise summary of the main features of the programme and the learning outcomes
Together for Health A Delivery Plan for the Critically Ill
 Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
EMERGENCY PRESSURES ESCALATION PROCEDURES
 OP48 EMERGENCY PRESSURES ESCALATION PROCEDURES INITIATED BY: Director of Therapies & Health Sciences / Chief Operating Officer APPROVED BY: Executive Board DATE APPROVED: 21 September 2016 VERSION: 3 OPERATIONAL
OP48 EMERGENCY PRESSURES ESCALATION PROCEDURES INITIATED BY: Director of Therapies & Health Sciences / Chief Operating Officer APPROVED BY: Executive Board DATE APPROVED: 21 September 2016 VERSION: 3 OPERATIONAL
Supporting the acute medical take: advice for NHS trusts and local health boards
 Supporting the acute medical take: advice for NHS trusts and local health boards Purpose of the statement The acute medical take has proven to be a challenge across acute hospital trusts and health boards
Supporting the acute medical take: advice for NHS trusts and local health boards Purpose of the statement The acute medical take has proven to be a challenge across acute hospital trusts and health boards
General practice education and training in the UK a thematic review
 General practice education and training in the UK a thematic review Introduction This report provides a snapshot of medical education and training in general practice (GP). It is based on visits to five
General practice education and training in the UK a thematic review Introduction This report provides a snapshot of medical education and training in general practice (GP). It is based on visits to five
Minimum Requirements for Assessments and Assessors of Foundation Doctors
 Minimum Requirements for Assessments and Assessors of Foundation Doctors Author: Foundation Programme Unit/Quality & Committee Services Version number: FP 01/03 Applicable to: All Foundation Schools and
Minimum Requirements for Assessments and Assessors of Foundation Doctors Author: Foundation Programme Unit/Quality & Committee Services Version number: FP 01/03 Applicable to: All Foundation Schools and
CLINICAL RADIOLOGY - ST1
 ENTRY CRITERIA CLINICAL RADIOLOGY - ST1 ESSENTIAL CRITERIA WHEN EVALUATED i Applicants must have: Qualifications MBBS or equivalent medical qualification Applicants must: Eligibility Be eligible for full
ENTRY CRITERIA CLINICAL RADIOLOGY - ST1 ESSENTIAL CRITERIA WHEN EVALUATED i Applicants must have: Qualifications MBBS or equivalent medical qualification Applicants must: Eligibility Be eligible for full
GP School Quality Monitoring Visits to GPSPT Programmes Name of GPST Programme: WEST HERTFORDSHIRE Date of visit: 31 st July 2014
 Report compiled by: (on behalf of the visiting team) Professor John Howard Directors, Tutors, Admin Staff & GPST Registrars visited East of England Multi-Professional Deanery Educational Roles Name Contact
Report compiled by: (on behalf of the visiting team) Professor John Howard Directors, Tutors, Admin Staff & GPST Registrars visited East of England Multi-Professional Deanery Educational Roles Name Contact
Regulation and Inspection of Social Care (Wales) Act 2016 Re-registration guidance for providers
 Act 2016 Re-registration guidance for providers") Regulation and Inspection of Social Care (Wales) Act 2016 Re-registration guidance for providers October 2017 Mae r ddogfen yma hefyd ar gael yn Gymraeg. This document is also available in Welsh. Crown
Regulation and Inspection of Social Care (Wales) Act 2016 Re-registration guidance for providers October 2017 Mae r ddogfen yma hefyd ar gael yn Gymraeg. This document is also available in Welsh. Crown
Australian Medical Council Limited
 Australian Medical Council Limited Procedures for Assessment and Accreditation of Specialist Medical Programs and Professional Development Programs by the Australian Medical Council 2017 Specialist Education
Australian Medical Council Limited Procedures for Assessment and Accreditation of Specialist Medical Programs and Professional Development Programs by the Australian Medical Council 2017 Specialist Education
Review of Management Arrangements within the Microbiology Division Public Health Wales NHS Trust. Issued: December 2013 Document reference: 653A2013
 Review of Management Arrangements within the Microbiology Division Public Health Issued: December 2013 Document reference: 653A2013 Status of report This document has been prepared for the internal use
Review of Management Arrangements within the Microbiology Division Public Health Issued: December 2013 Document reference: 653A2013 Status of report This document has been prepared for the internal use
Curriculum for Specialty Training in Infectious Diseases
 Curriculum for Specialty Training in Infectious Diseases Incorporating Combined Infection Training, developed in conjunction with the Royal College of Pathologists Approved 6 May 204 Table of Contents
Curriculum for Specialty Training in Infectious Diseases Incorporating Combined Infection Training, developed in conjunction with the Royal College of Pathologists Approved 6 May 204 Table of Contents
SPECIALTY TRAINING PROGRAMME IN OPHTHALMOLOGY IN WESSEX DEANERY
 SPECIALTY TRAINING PROGRAMME IN OPHTHALMOLOGY IN WESSEX DEANERY This is a 7 year training programme in Ophthalmology for which 4 posts are available at ST1 level, starting August 2014. The programme is
SPECIALTY TRAINING PROGRAMME IN OPHTHALMOLOGY IN WESSEX DEANERY This is a 7 year training programme in Ophthalmology for which 4 posts are available at ST1 level, starting August 2014. The programme is
Local CPD and Training Opportunities for Trainers
 Local and Training Opportunities for Trainers This quarterly publication provides details of the local and training opportunities that are on offer to trainers across NHS Wales to assist them in meeting
Local and Training Opportunities for Trainers This quarterly publication provides details of the local and training opportunities that are on offer to trainers across NHS Wales to assist them in meeting
A Reference Guide to Core Medical Training in Iceland
 A Reference Guide to Core Medical Training in Iceland Applicable to all trainees taking up appointments in Core Medical Training, which commence on or after 1. September 2015 The Icelandic Gold Guide First
A Reference Guide to Core Medical Training in Iceland Applicable to all trainees taking up appointments in Core Medical Training, which commence on or after 1. September 2015 The Icelandic Gold Guide First
Removal of Annual Declaration and new Triennial Review Form. Originated / Modified By: Professional Development and Education Team
 Review Circulation Application Ratificatio n Author Minor Amendment Supersedes Title DOCUMENT CONTROL PAGE Title: Mentorship in Nursing and Midwifery Policy Version: 14.1 Reference Number: Supersedes:.14.0
Review Circulation Application Ratificatio n Author Minor Amendment Supersedes Title DOCUMENT CONTROL PAGE Title: Mentorship in Nursing and Midwifery Policy Version: 14.1 Reference Number: Supersedes:.14.0
CT Scanner Replacement Nevill Hall Hospital Abergavenny. Business Justification
 CT Scanner Replacement Nevill Hall Hospital Abergavenny Business Justification Version No: 3 Issue Date: 9 July 2012 VERSION HISTORY Version Date Brief Summary of Change Owner s Name Issued Draft 21/06/12
CT Scanner Replacement Nevill Hall Hospital Abergavenny Business Justification Version No: 3 Issue Date: 9 July 2012 VERSION HISTORY Version Date Brief Summary of Change Owner s Name Issued Draft 21/06/12
NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET
 NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET Version: 1.0 Date: 17 th August 2017 Data Set Title Admitted Patient Care data set (APC ds) Sponsor Welsh Government
NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET Version: 1.0 Date: 17 th August 2017 Data Set Title Admitted Patient Care data set (APC ds) Sponsor Welsh Government
SPECIALTY TRAINING CURRICULUM FOR GASTROENTEROLOGY AUGUST 2010 AMENDMENTS AUGUST 2013
 SPECIALTY TRAINING CURRICULUM FOR GASTROENTEROLOGY AUGUST 200 AMENDMENTS AUGUST 203 Version Change Approval Implementation V 22 August 203 22 August 203 V2 Amendment of name of the specialist exam to European
SPECIALTY TRAINING CURRICULUM FOR GASTROENTEROLOGY AUGUST 200 AMENDMENTS AUGUST 203 Version Change Approval Implementation V 22 August 203 22 August 203 V2 Amendment of name of the specialist exam to European
University of Bradford
 UNIVERSITY OF BRADFORD Academic Year 2014-15 School of Health Studies Division of Service Development and Improvement Programme title: PG Dip in Respiratory Medicine for Practitioners with a Special Interest
UNIVERSITY OF BRADFORD Academic Year 2014-15 School of Health Studies Division of Service Development and Improvement Programme title: PG Dip in Respiratory Medicine for Practitioners with a Special Interest
Continuing Professional Development Supporting the Delivery of Quality Healthcare
 714 CPD Supporting Delivery of Quality Healthcare I Starke & W Wade Continuing Professional Development Supporting the Delivery of Quality Healthcare I Starke, 1 MD, MSc, FRCP, W Wade, 2 BSc (Hons), MA
714 CPD Supporting Delivery of Quality Healthcare I Starke & W Wade Continuing Professional Development Supporting the Delivery of Quality Healthcare I Starke, 1 MD, MSc, FRCP, W Wade, 2 BSc (Hons), MA
SPECIALTY TRAINING CURRICULUM FOR GASTROENTEROLOGY AND SUB-SPECIALTY TRAINING CURRICULUM FOR HEPATOLOGY AUGUST 2010 (AMENDMENTS AUGUST 2013)
") SPECIALTY TRAINING CURRICULUM FOR GASTROENTEROLOGY AND SUB-SPECIALTY TRAINING CURRICULUM FOR HEPATOLOGY AUGUST 200 (AMENDMENTS AUGUST 203) Joint Royal Colleges of Physicians Training Board 5 St Andrews
SPECIALTY TRAINING CURRICULUM FOR GASTROENTEROLOGY AND SUB-SPECIALTY TRAINING CURRICULUM FOR HEPATOLOGY AUGUST 200 (AMENDMENTS AUGUST 203) Joint Royal Colleges of Physicians Training Board 5 St Andrews
Proposal to seek approval for an Innovative Post
 Proposal to seek approval for an Innovative Post This template offers a means of providing a standard approach to achieving approval by the GP Education Subcommittee. You are strongly recommended to refer
Proposal to seek approval for an Innovative Post This template offers a means of providing a standard approach to achieving approval by the GP Education Subcommittee. You are strongly recommended to refer
HEALTHCARE INSPECTORATE WALES SAFEGUARDING AND PROTECTING CHILDREN IN WALES:
 HEALTHCARE INSPECTORATE WALES SAFEGUARDING AND PROTECTING CHILDREN IN WALES: A Review of the arrangements in place across the Welsh National Health Service ACTION PLAN - UPDATED August 2010 RECOMMENDATION
HEALTHCARE INSPECTORATE WALES SAFEGUARDING AND PROTECTING CHILDREN IN WALES: A Review of the arrangements in place across the Welsh National Health Service ACTION PLAN - UPDATED August 2010 RECOMMENDATION
Action Plan for Health Education Kent, Surrey and Sussex
 Action Plan for Health Education Kent, Surrey and Sussex Requirements Report HEKSS1 HEKSS must work with East Kent Hospitals University NHS Foundation Trust to address the patient safety concern identified
Action Plan for Health Education Kent, Surrey and Sussex Requirements Report HEKSS1 HEKSS must work with East Kent Hospitals University NHS Foundation Trust to address the patient safety concern identified
GUIDELINES FOR JUNIOR DOCTORS USING THE NATIONAL ASSESSMENT TOOLS
 GUIDELINES FOR JUNIOR DOCTORS USING THE NATIONAL ASSESSMENT TOOLS This training manual contains materials which are intended to be used to assist JUNIOR DOCTORs in using the National Assessment Tools.
GUIDELINES FOR JUNIOR DOCTORS USING THE NATIONAL ASSESSMENT TOOLS This training manual contains materials which are intended to be used to assist JUNIOR DOCTORs in using the National Assessment Tools.
Paper for the Health Board Quality and Safety Committee. Out of Hours Upper GI Haemorrhage
 Paper for the Health Board Quality and Safety Committee Out of Hours Upper GI Haemorrhage This short paper describes the current pathways within the Health Board for the management of out of hours emergency
Paper for the Health Board Quality and Safety Committee Out of Hours Upper GI Haemorrhage This short paper describes the current pathways within the Health Board for the management of out of hours emergency
Work Schedule. Employing organisation: Anyplace Acute NHS Trust (Lead Employing Trust for GPST)
") Work Schedule Trainee Name: Dr Motors Training Programme: General Practice Specialty placement: General Practice Grade: ST3 Length of placement: 1 year Employing organisation: Anyplace Acute NHS Trust
Work Schedule Trainee Name: Dr Motors Training Programme: General Practice Specialty placement: General Practice Grade: ST3 Length of placement: 1 year Employing organisation: Anyplace Acute NHS Trust