CRITICAL ACCESS HOSPITAL SWING BED PROGRAM
|
|
|
- Colleen Price
- 5 years ago
- Views:
Transcription



1 CRITICAL ACCESS HOSPITAL SWING BED PROGRAM Operational and Management Strategies March 1, 2016 Andrea Elliott, CPA Senior Managing Consultant Suzy Harvey, RN-BC, RAC-CT Managing Consultant
2 Agenda Coverage Criteria Swing Bed Management & Utilization Important items for SB Cost Reports CAH Financial Ratios CCJR Questions 2
3 Skilled Nursing Facility vs CAH Swing Bed Level of Care

4 Level of Care Swing beds must meet same level of care criteria as Skilled Nursing Facilities SB SNF
5 Operational Benefits Provides viable option to local community Increased in-house services for the community Physicians can easily monitor their patients without moving them Keeps patients in the community Helps to manage Nursing hours with less drastic fluctuation in the census Cost-based reimbursement No length of stay requirements
6 Patient Benefits of Swing Bed Improved Patient Care Opportunity to identify patient needs to assure safe and sustainable return home More time for training, demonstration, return demonstration, education to patients and family Extra time to put post-acute discharge plan in place Increased patient/family satisfaction ( not thrown out ) Willingness to go to a skilled level of care while meeting their needs for a longer inpatient stay
7 Resources The policies for extended care services in a Swing- Bed are the same as a SNF. Medicare General Information, Eligibility and Entitlement Manuals Chapter 3, Section 10.4 Chapter 4, Section 40 Medicare Benefit Policy Manual Chapter 8, Sections 10,20,& 30 Chapter 15, Section 220 State Operations Manual Appendix W
8 Coverage Criteria
9 Technical Eligibility Medicare Part A available days Medicare Advantage Plan or Managed Care Three consecutive day qualifying stay in acute hospital (3 midnights) within the last 30 days 30 day Transfer Rule Medically appropriate exception Physician Certification
10 Clinical Eligibility Skilled Services performed or supervised by a qualified technical or professional health personnel For a condition, which arose while receiving care for a conditions for which he received inpatient hospital services Services required Daily Skilled Nursing Services 7 X week Skilled Rehabilitation Services at least 5 X week Reasonable and necessary
11 Skilled Services Defined Nursing or Therapy services Furnished per physician order Require skills an d qualification of professional personnel Provided directly by or under supervision of skilled personnel
12 Determining Skilled Services Skilled level of care is usually required because of the patient s condition, which may: Be unstable Require complex treatment Be associated with multiple unskilled problems which demand professional management Be a chronic situation that confines the patient and requires ongoing nursing decisions about services on a daily basis or Terminal, meeting the requirements of skilled care.

13 Nursing Services - Skilled Direct Skilled Nursing Services Care Plan Management Observation and Assessment Teaching and Training


14 Questionable Situations Situations that do not support evidence of daily skilled service Primary services needed is oral medications Patient is capable of independent ambulation, dressing, feeding and hygiene Therapy for strength and endurance Passive ROM
15 Swing Bed Management & Utilization
16 Inquiry/Initial Pre-Assessment Process Process should begin day 1 of acute hospital stay. Hospital discharge planner, along with UR committee, review all acute patients-daily Identify patients eligible for SB Notify Physician of SB eligibility Notify Patient or Representative
17 Patients in ER/Observation Utilizing the 30 Day Transfer Rule Has the patient been in the hospital or received skilled care in the past 30 days? Is the reason for ER/Observation related to the most recent hospital stay? Admit to Swing Bed 17
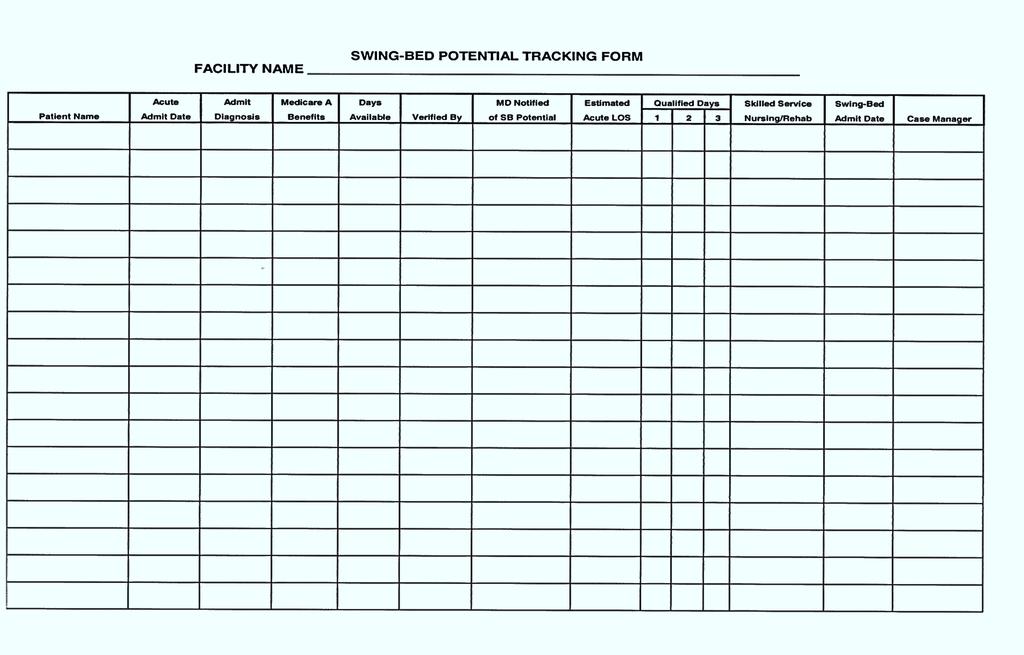
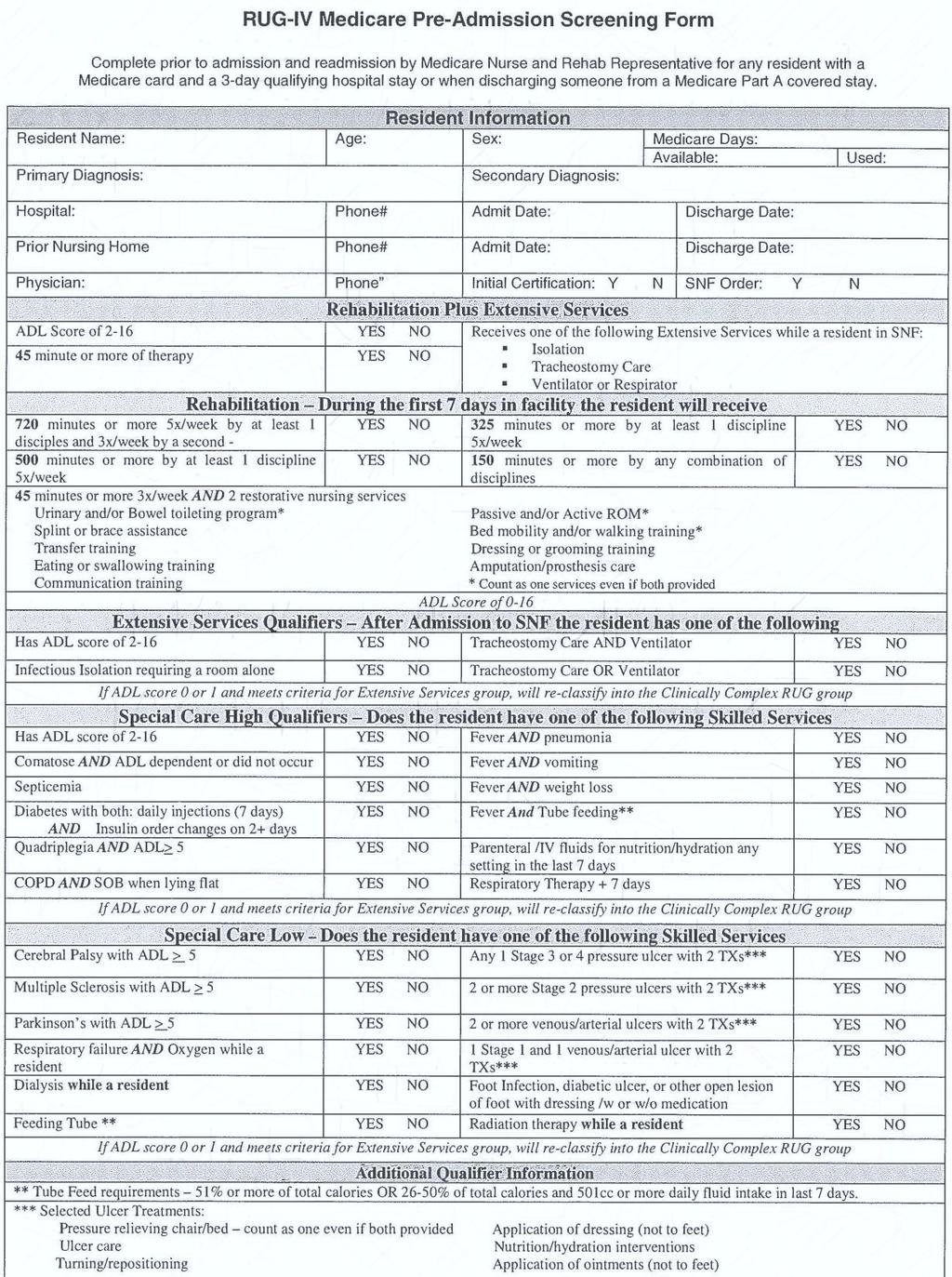
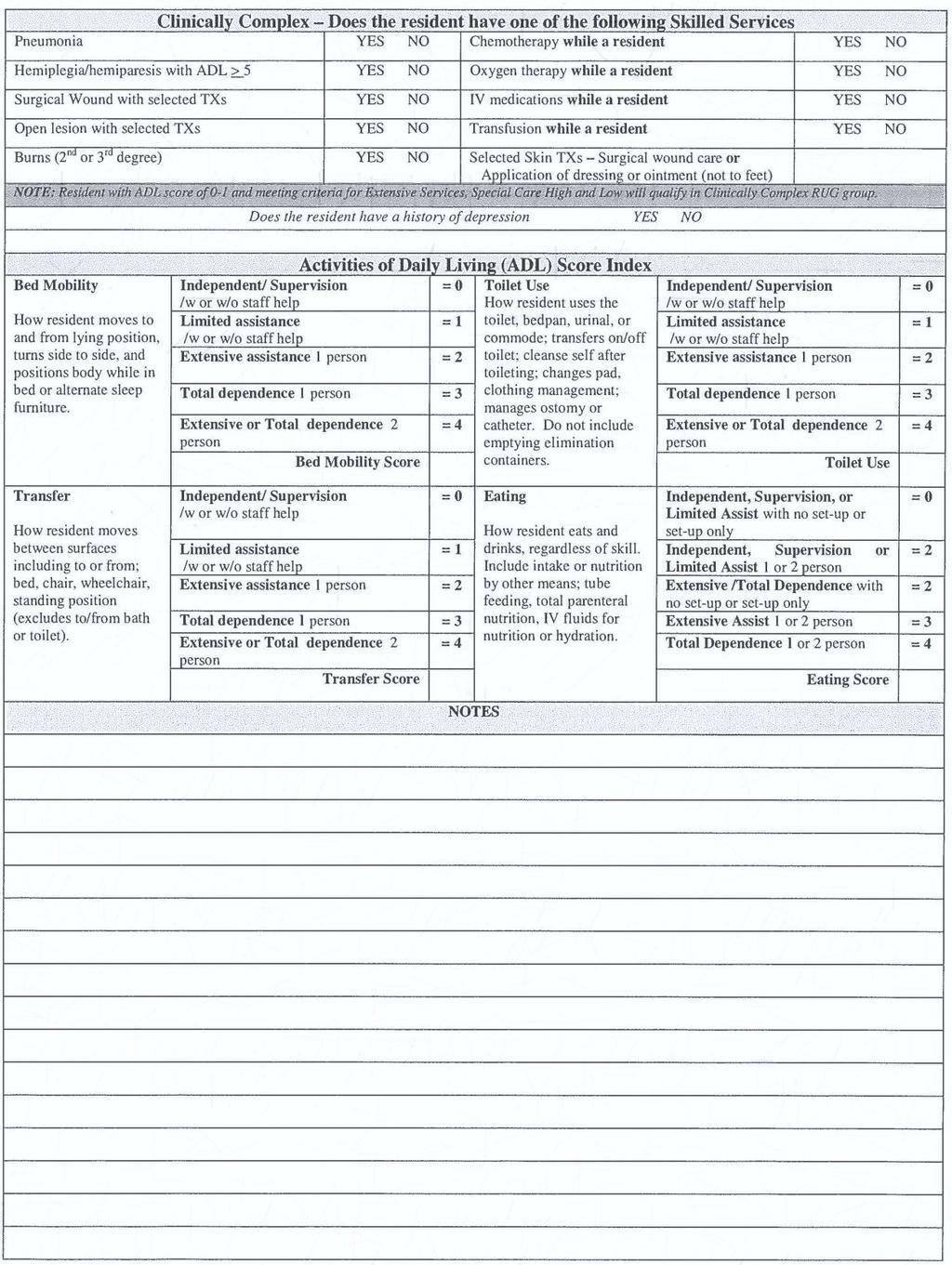
18 Swing Bed Tracking Form Recommend use of; Tracking form Good way to determine type of patients not being admitted Great for marketing Pre-screening form Examples of both included in handout
19 19
20 20

21 21
22 Manage care needs Utilization Review Ensure stability prior to discharge Monitoring acute stay for 96 hour requirement or GMLOS of diagnosis Look at length of stay Typically less than 5 days Increase to 7-10 days for safe and sustainable discharge 22
23 Summary Risk management is essential for effective utilization of Swing Beds Verify all eligibility criteria is met Documentation to Support Skilled Care Manage the patient stay Ensure safe and sustainable discharge Increase length of stay as appropriate to prevent rehospitalizations 23
24 Swing Bed Financial Implications
25 CAH Cost Report Important Items Importance of reporting correct patient days: CAH cost per day Observation days (typically calculated based upon hours patient is in observation) must be correct to allocate costs for this service outpatient service Report Medicare HMO days (Acute Part C) to increase Medicare utilization for EHR payments
26 CAH Cost Report Important Items Importance of reporting correct patient days: Should also segregate Medicaid HMO days from straight Medicaid for those receiving Medicaid DSH (for tie out to audits by the state) Exclude days related to self-insured insurance plan NF days paid consistent with Medicare rates should be included on the SNF line
27 CAH Cost Report Important Items Importance of reporting correct patient discharges: Discharges must be correct for CAH average length of stay calculations Plan to track hours patients are in-house as acute, if length of stay is approaching 96 hours EHR importance for Medicaid
28 CAH Cost Report Important Items Reporting correct days example: Routine cost $ 984,560 Routine days total 1,075 (error of 10 days) Cost per day $
 Cost per day $ 924.")
29 CAH Cost Report Important Items Reporting correct days example: Routine cost $ 984,560 Routine days total 1,065 (correct days) Cost per day $
30 CAH Cost Report Important Items Reporting correct days example: Routine cost per day (correct) $ Routine cost per day (error of 10 days) $ Error per day $8.60 Medicare acute/swing bed days 635 Reimbursement impact $5,461
31 CAH Cost Report Important Items Accurate matching revenue and expense Revenues and expenses should be properly matched on the cost report (line numbers) Proper and consistent cut-off of both revenue and expenses for your year-end Following asset capitalization policy for new assets and repairs
32 CAH Cost Report Important Items Physicians Important to be proactive to correctly capture all physician costs for the cost report. ER availability time studies (write into contract that this is a requirement) Medical Director time studies or contract language ER Call Pay contract language and time study
33 CAH Cost Report Important Items Statistics B part I is a summary of all costs as allocated by the B-1 statistics. The data can be used for more than just the cost report. Review these allocations for changes from year to year and also what is going to non-reimbursable cost centers.
34 CAH Financial Ratios What is your total occupancy rate? What is your length of stay? What is your swing bed length of stay? What is your opportunity?

35 CAH Financial Review

36 CAH Financial Review

37 CAH Financial Review
38 CAH Financial Ratios Occupancy rate (4,021/9,125) 44.1% Length of stay (4,021/1,018) 3.95 Swing bed length of stay (557/93) 5.99 Medicare Percentage (2,311/4,021) 57.5% There appears opportunity to increase patient utilization of the swing beds, as many SNF providers see ALOS of days. If could add 4 days to LOS would result in 372 additional days.
39 CAH Financial Revised Ratios Occupancy rate (4,393/9,125) 48.1% Length of stay (4,393/1,018) 4.32 Swing bed length of stay (929/93) 9.99 Medicare Percentage (2,683/4,393) 61.1%
40 CAH Financial Results Medicare Days Medicare Discharges Medicare ALOS Total Days Medicare Days Medicare Discharges Medicare ALOS Total Days Acute/ICU 1, ,464 1, ,464 Swing Bed - SNF Swing Bed - NF Observation Total Days 2,311 4,549 2,683 4,921 Total Routine Cost 4,879,006 4,879,006 Less: Swing Bed - NF Costs - - Adjusted Total Routine Cost 4,879,006 4,879,006 Total Days (Less Swing Bed - NF) 4,549 4,921 Total Routine Cost Per Day 1, Medicare Days 2,311 2,683 Medicare Acute & Swing Bed SNF Cost 2,478,651 2,660,136 Medicare Routine Cost Reimbursement % 51% 55% 181,485
41 Comprehensive Care for Joint Replacement (CCJR) CAH s are not subject to CCJR HOWEVER CAH s in CCJR MSA s should not expect admissions into their swing beds from other acute hospitals based on the high cost of service (as compared to skilled nursing facilities and home health agencies) CAH s should monitor legislation as other MSA s and other DRG s are added which could impact referral sources
42 Summary Cost report is important for more than just the settlement Provides important management information It is important that the individuals involved in preparing the cost report understand the importance of all the issues surrounding CAH reimbursement Monitor CAH reimbursement on an interim basis to avoid significant under/over payments at year end
43 QUESTIONS?

44 THANK YOU! FOR MORE INFORMATION Andrea Elliott, CPA Suzy Harvey, RN-BC
45
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals
 Rural Hospitals under 100 Beds and Critical Access Hospitals") SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
Illinois Department of Public Health Critical Access Hospital Program Certification Process Preparation
 Illinois Department of Public Health Critical Access Hospital Program Certification Process Preparation Overview of the process The Critical Access Hospital (CAH) program is an opportunity for rural hospitals
Illinois Department of Public Health Critical Access Hospital Program Certification Process Preparation Overview of the process The Critical Access Hospital (CAH) program is an opportunity for rural hospitals
More than a Century of Legal Experience
 Swing Bed Services: 3 Day Qualifying Stays, Medically Necessary Admissions, and Observation Services Oh My!!! August 13, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience This
Swing Bed Services: 3 Day Qualifying Stays, Medically Necessary Admissions, and Observation Services Oh My!!! August 13, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience This
8/6/2013. More than a Century of Legal Experience. Agenda
 Swing Bed Services: 3 Day Qualifying Stays, Medically Necessary Admissions, and Observation Services Oh My!!! August 13, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience This
Swing Bed Services: 3 Day Qualifying Stays, Medically Necessary Admissions, and Observation Services Oh My!!! August 13, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience This
Objectives. Observation: Exploring the MOON and Charge Capture. Aurora Health Care 10/11/2016
 Observation: Exploring the MOON and Charge Capture Lynn Sisler, Senior Director Case Management Manpreet Lehn, Manager Revenue Assurance Objectives Understand the CMS requirements for the Medicare Outpatient
Observation: Exploring the MOON and Charge Capture Lynn Sisler, Senior Director Case Management Manpreet Lehn, Manager Revenue Assurance Objectives Understand the CMS requirements for the Medicare Outpatient
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
CRS Report for Congress Received through the CRS Web
 CRS Report for Congress Received through the CRS Web Order Code RS20386 Updated April 16, 2001 Medicare's Skilled Nursing Facility Benefit Summary Heidi G. Yacker Information Research Specialist Information
CRS Report for Congress Received through the CRS Web Order Code RS20386 Updated April 16, 2001 Medicare's Skilled Nursing Facility Benefit Summary Heidi G. Yacker Information Research Specialist Information
CMS -1599F. The 2 Midnight Rule Effective October 1, 2013
 Joseph Nitti, M.D. Medical Director/Physician Advisor Continuum of Care Dept. Morristown Medical Center 973-971-4004 CMS -1599F The 2 Midnight Rule Effective October 1, 2013 Determination of Inpatient
Joseph Nitti, M.D. Medical Director/Physician Advisor Continuum of Care Dept. Morristown Medical Center 973-971-4004 CMS -1599F The 2 Midnight Rule Effective October 1, 2013 Determination of Inpatient
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services. Discharge Planning
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services ICN 908184 October 2014 This booklet was current at the time it was published or uploaded onto the web. Medicare policy
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services ICN 908184 October 2014 This booklet was current at the time it was published or uploaded onto the web. Medicare policy
Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1
 PEPPER to Support Auditing and Monitoring Efforts: Session 1") Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER IPF PEPPER target
Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER IPF PEPPER target
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services. Discharge Planning
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services ICN 908184 October 2013 This page intentionally left blank. This booklet was current at the time it was published or uploaded
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services ICN 908184 October 2013 This page intentionally left blank. This booklet was current at the time it was published or uploaded
Medi-Pak Advantage: Reimbursement Methodology
 Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
Observation vs. Inpatient: How to Get it Right. November 5, 2013
 Observation vs. Inpatient: How to Get it Right November 5, 2013 Learning Objectives Understand how the Inpatient Prospective Payment System (IPPS) Final Rule impacts your facility Integrate leading practice
Observation vs. Inpatient: How to Get it Right November 5, 2013 Learning Objectives Understand how the Inpatient Prospective Payment System (IPPS) Final Rule impacts your facility Integrate leading practice
May 3, 2018 Rick Reid Director, Provider Payment Analytics Michael Felczak Director, Provider Payment Analytics
 Hot Reimbursement Topics Rural Area Hospitals May 3, 2018 Rick Reid Director, Provider Payment Analytics Michael Felczak Director, Provider Payment Analytics RICHARD S. REID, MPA, FHFMA, CPA, Director,
Hot Reimbursement Topics Rural Area Hospitals May 3, 2018 Rick Reid Director, Provider Payment Analytics Michael Felczak Director, Provider Payment Analytics RICHARD S. REID, MPA, FHFMA, CPA, Director,
2014 Hospital Admission Criteria
 2014 Hospital Admission Criteria Created on 11/20/2013 Audio and/or Video Recording of this Educational Session is Prohibited Agenda Inpatient vs. observation 2-midnight benchmark and presumption Admission
2014 Hospital Admission Criteria Created on 11/20/2013 Audio and/or Video Recording of this Educational Session is Prohibited Agenda Inpatient vs. observation 2-midnight benchmark and presumption Admission
Inpatient Psychiatric Facility (IPF) Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016
 Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016") Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
Regulatory Compliance Risks. September 2009
 Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
routine services furnished by nursing facilities (other than NFs for individuals with intellectual Rev
 4025.1 FORM CMS-2552-10 11-16 When an inpatient is occupying any other ancillary area (e.g., surgery or radiology) at the census taking hour prior to occupying an inpatient bed, do not record the patient
4025.1 FORM CMS-2552-10 11-16 When an inpatient is occupying any other ancillary area (e.g., surgery or radiology) at the census taking hour prior to occupying an inpatient bed, do not record the patient
IMAGES & ASSOCIATES O UR S ERVICES OPERATIONAL REVIEW AND ENHANCEMENT
 O UR S ERVICES OPERATIONAL REVIEW AND ENHANCEMENT The Prospective Payment System (PPS) for Inpatient Rehabilitation Facilities creates both opportunities and challenges for facilities that provide comprehensive
O UR S ERVICES OPERATIONAL REVIEW AND ENHANCEMENT The Prospective Payment System (PPS) for Inpatient Rehabilitation Facilities creates both opportunities and challenges for facilities that provide comprehensive
CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
paymentbasics Defining the inpatient acute care products Medicare buys Under the IPPS, Medicare sets perdischarge
 Hospital ACUTE inpatient services system basics Revised: October 2007 This document does not reflect proposed legislation or regulatory actions. 601 New Jersey Ave., NW Suite 9000 Washington, DC 20001
Hospital ACUTE inpatient services system basics Revised: October 2007 This document does not reflect proposed legislation or regulatory actions. 601 New Jersey Ave., NW Suite 9000 Washington, DC 20001
paymentbasics The IPPS payment rates are intended to cover the costs that reasonably efficient providers would incur in furnishing highquality
 Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Section A Identification Information
 r Minimum Data Set (MDS) 3.0 Instructor Guide Section A Identification Information Objectives State the intent of Section A Identification Information. Describe the information required to complete Section
r Minimum Data Set (MDS) 3.0 Instructor Guide Section A Identification Information Objectives State the intent of Section A Identification Information. Describe the information required to complete Section
Reimbursement Models of the Future A Look at Proposed Models
 Experience the Eide Bailly Difference Reimbursement Models of the Future A Look at Proposed Models Ralph J. Llewellyn, CPA, CHFP Partner rllewellyn@eidebailly.com 701.239.8594 Introduction CAH reimbursement
Experience the Eide Bailly Difference Reimbursement Models of the Future A Look at Proposed Models Ralph J. Llewellyn, CPA, CHFP Partner rllewellyn@eidebailly.com 701.239.8594 Introduction CAH reimbursement
Prepared for North Gunther Hospital Medicare ID August 06, 2012
 Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Hospital Rate Setting
 Hospital Rate Setting Calendar Year 2014 Wisconsin Department of Health Services Division of Health Care Access and Accountability Bureau of Fiscal Management September 6, 2013 1 Agenda 1. Introduction
Hospital Rate Setting Calendar Year 2014 Wisconsin Department of Health Services Division of Health Care Access and Accountability Bureau of Fiscal Management September 6, 2013 1 Agenda 1. Introduction
Webinar Etiquette. Webinar Resources
 Georgia State Office of Rural Health & HomeTown Health, LLC Welcome you to the: Best Practices for Compliance & Efficiency 2016-2017 Rural Swing Bed Management (RSBM) Training Program Use of Swing Beds
Georgia State Office of Rural Health & HomeTown Health, LLC Welcome you to the: Best Practices for Compliance & Efficiency 2016-2017 Rural Swing Bed Management (RSBM) Training Program Use of Swing Beds
LifeWise Reference Manual LifeWise Health Plan of Oregon
 11 UB-04 Billing Description This chapter contains participation, claims and billing information for providers who bill on a UB-04 (CMS 1450) claim form. This chapter supplements information contained
11 UB-04 Billing Description This chapter contains participation, claims and billing information for providers who bill on a UB-04 (CMS 1450) claim form. This chapter supplements information contained
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Rural Provider Types and Payment Models
 Rural Provider Types and Payment Models Emily Jane Cook, JD, MSPH McDermott Will & Emery LLP American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues Baltimore, MD March 28,
Rural Provider Types and Payment Models Emily Jane Cook, JD, MSPH McDermott Will & Emery LLP American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues Baltimore, MD March 28,
Appendix B: Formulae Used for Calculation of Hospital Performance Measures
 Appendix B: Formulae Used for Calculation of Hospital Performance Measures ADJUSTMENTS Adjustment Factor Case Mix Adjustment Wage Index Adjustment Gross Patient Revenue / Gross Inpatient Acute Care Revenue
Appendix B: Formulae Used for Calculation of Hospital Performance Measures ADJUSTMENTS Adjustment Factor Case Mix Adjustment Wage Index Adjustment Gross Patient Revenue / Gross Inpatient Acute Care Revenue
Payment Methodology. Acute Care Hospital - Inpatient Services
 Grid Medi-Pak Advantage generally reimburses deemed providers the amount they would have received under Original Medicare for Medicare covered services, minus any amounts paid directly by Original Medicare
Grid Medi-Pak Advantage generally reimburses deemed providers the amount they would have received under Original Medicare for Medicare covered services, minus any amounts paid directly by Original Medicare
Medical Care Meets Long-Term Services and Supports (LTSS)
") Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
EMERGENCY DEPARTMENT CASE MANAGEMENT
 EMERGENCY DEPARTMENT CASE MANAGEMENT By Linda Sallee, Haley Rhodes, Sapna Patel, Cathleen Trespasz Healthcare consumers are becoming more empowered to have healthcare on their terms. With telemedicine,
EMERGENCY DEPARTMENT CASE MANAGEMENT By Linda Sallee, Haley Rhodes, Sapna Patel, Cathleen Trespasz Healthcare consumers are becoming more empowered to have healthcare on their terms. With telemedicine,
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
Overview of Alaska s Hospitals and Nursing Homes. House HSS Committee March 1, 2012
 Overview of Alaska s Hospitals and Nursing Homes House HSS Committee March 1, 2012 Alaska Hospital and Nursing Homes Testifying Today Fairbanks Memorial Hospital Mike Powers Central Peninsula Hospital
Overview of Alaska s Hospitals and Nursing Homes House HSS Committee March 1, 2012 Alaska Hospital and Nursing Homes Testifying Today Fairbanks Memorial Hospital Mike Powers Central Peninsula Hospital
Clinical. Financial. Integrated.
 Clinical. Financial. Integrated. April 2015 Table of Contents When are the rule changes effective? What is changing? What requirements must be met to avoid payment at the site neutral rate? How is the
Clinical. Financial. Integrated. April 2015 Table of Contents When are the rule changes effective? What is changing? What requirements must be met to avoid payment at the site neutral rate? How is the
Transitions of Care. Scott Clark, President Leading Edge Health Care
 Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
A1600 A1800: Most Recent Admission/Entry or Reentry into this Facility
 A1550: Conditions Related to Intellectual Disability/Developmental Disability (ID/DD) Status (cont.) Code E: if an ID/DD condition is present but the resident does not have any of the specific conditions
A1550: Conditions Related to Intellectual Disability/Developmental Disability (ID/DD) Status (cont.) Code E: if an ID/DD condition is present but the resident does not have any of the specific conditions
907 KAR 10:815. Per diem inpatient hospital reimbursement.
 907 KAR 10:815. Per diem inpatient hospital reimbursement. RELATES TO: KRS 13B.140, 205.510(16), 205.637, 205.639, 205.640, 205.641, 216.380, 42 C.F.R. Parts 412, 413, 440.10, 440.140, 447.250-447.280,
907 KAR 10:815. Per diem inpatient hospital reimbursement. RELATES TO: KRS 13B.140, 205.510(16), 205.637, 205.639, 205.640, 205.641, 216.380, 42 C.F.R. Parts 412, 413, 440.10, 440.140, 447.250-447.280,
MEDICARE COMPREHENSIVE CARE FOR JOINT REPLACEMENT MODEL (CCJR) Preparing for Risk-Based Outcomes of Bundled Care 8/12/2015.
 Preparing for Risk-Based Outcomes of Bundled Care 8/12/2015.") MEDICARE COMPREHENSIVE CARE FOR JOINT REPLACEMENT MODEL (CCJR) Preparing for Risk-Based Outcomes of Bundled Care August 13, 2015 Eric M. Rogers MEd RT(R) Managing Consultant erogers@bkd.com Jeff Bond President
MEDICARE COMPREHENSIVE CARE FOR JOINT REPLACEMENT MODEL (CCJR) Preparing for Risk-Based Outcomes of Bundled Care August 13, 2015 Eric M. Rogers MEd RT(R) Managing Consultant erogers@bkd.com Jeff Bond President
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW OHA Finance/PFS Webinar Series. May 10, 2016
 MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
Abbreviated Client Stay means an Inpatient stay ending in client death or in which the client leaves against medical advice.
 DEPARTMENT OF HEALTH CARE POLICY AND FINANCING Medical Services Board MEDICAL ASSISTANCE - SECTION 8.300 10 CCR 2505-10 8.300 [Editor s Notes follow the text of the rules at the end of this CCR Document.]
DEPARTMENT OF HEALTH CARE POLICY AND FINANCING Medical Services Board MEDICAL ASSISTANCE - SECTION 8.300 10 CCR 2505-10 8.300 [Editor s Notes follow the text of the rules at the end of this CCR Document.]
William J. Ennis D.O.,MBA University of Illinois at Chicago Professor Clinical Surgery, Chief Section wound healing and tissue repair
 William J. Ennis D.O.,MBA University of Illinois at Chicago Professor Clinical Surgery, Chief Section wound healing and tissue repair What are the revenue streams What are the expenses How does the hospital
William J. Ennis D.O.,MBA University of Illinois at Chicago Professor Clinical Surgery, Chief Section wound healing and tissue repair What are the revenue streams What are the expenses How does the hospital
Medicare Cost Report Hot Topics!
 Medicare Cost Report Hot Topics! Montana HFMA April 2017 Presented by: Shar Sheaffer, Owner Outline Occupational mix Swing bed days Uncompensated care costs Common cost report issues Medicare bad debts
Medicare Cost Report Hot Topics! Montana HFMA April 2017 Presented by: Shar Sheaffer, Owner Outline Occupational mix Swing bed days Uncompensated care costs Common cost report issues Medicare bad debts
Medicare Cost Reporting and PPS FFY 2015 Proposed Rule Why it Still Matters. Glenn Grigsby, CPA OACHC 2014 Annual Spring Conference March 11, 2014
 Medicare Cost Reporting and PPS FFY 2015 Proposed Rule Why it Still Matters Glenn Grigsby, CPA OACHC 2014 Annual Spring Conference March 11, 2014 Agenda Medicare cost report myths Common cost reporting
Medicare Cost Reporting and PPS FFY 2015 Proposed Rule Why it Still Matters Glenn Grigsby, CPA OACHC 2014 Annual Spring Conference March 11, 2014 Agenda Medicare cost report myths Common cost reporting
What is CDI? 2016 HTH FL Boot Camp. HIM/Documentation: Endurance in the Clinical Documentation Improvement (CDI) Race
 Race") HIM/Documentation: Endurance in the Clinical Documentation Improvement (CDI) Race Presented By: Sandy Sage Developed by Annie Lee Sallee Endurance in the Clinical Documentation Improvement (CDI) Race Learning
HIM/Documentation: Endurance in the Clinical Documentation Improvement (CDI) Race Presented By: Sandy Sage Developed by Annie Lee Sallee Endurance in the Clinical Documentation Improvement (CDI) Race Learning
10/12/2017 COST REPORTING 201. October 18, Michael K. Westerfield, CPA, FHFMA Senior Manager
 COST REPORTING 201 October 18, 2017 Michael K. Westerfield, CPA, FHFMA Senior Manager 1 AGENDA Cost Report 101 Review Wage Index Disproportionate Share S-10 Indirect Medical Education (IME) Graduate Medical
COST REPORTING 201 October 18, 2017 Michael K. Westerfield, CPA, FHFMA Senior Manager 1 AGENDA Cost Report 101 Review Wage Index Disproportionate Share S-10 Indirect Medical Education (IME) Graduate Medical
CLINICAL CRITERIA FOR UM DECISIONS Skilled Nursing Facilities
 COMMERCIAL CLINICAL CRITERIA FOR UM DECISIONS Skilled Nursing Facilities Capital Health Plan (CHP) will provide coverage for care in a skilled nursing facility, subject to the benefit limitations of the
COMMERCIAL CLINICAL CRITERIA FOR UM DECISIONS Skilled Nursing Facilities Capital Health Plan (CHP) will provide coverage for care in a skilled nursing facility, subject to the benefit limitations of the
Health Management Policy
 Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
State of California Health and Human Services Agency Department of Health Care Services
 State of California Health and Human Services Agency Department of Health Care Services TOBY DOUGLAS Director EDMUND G. BROWN JR. Governor DATE: OCTOBER 28, 2013 ALL PLAN LETTER 13-014 SUPERSEDES ALL PLAN
State of California Health and Human Services Agency Department of Health Care Services TOBY DOUGLAS Director EDMUND G. BROWN JR. Governor DATE: OCTOBER 28, 2013 ALL PLAN LETTER 13-014 SUPERSEDES ALL PLAN
PROVIDER POLICIES & PROCEDURES
 PROVIDER POLICIES & PROCEDURES EXTENDED NURSING SERVICES The purpose of this document is to provide guidance to providers enrolled in the Connecticut Medical Assistance Program (CMAP) on the requirements
PROVIDER POLICIES & PROCEDURES EXTENDED NURSING SERVICES The purpose of this document is to provide guidance to providers enrolled in the Connecticut Medical Assistance Program (CMAP) on the requirements
District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions
 District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions Version Date: July 20, 2017 Updates for October 1, 2017 Effective October 1, 2017 (the District s fiscal year
District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions Version Date: July 20, 2017 Updates for October 1, 2017 Effective October 1, 2017 (the District s fiscal year
ALABAMA MEDICAID AGENCY ADMINISTRATIVE CODE CHAPTER 560-X-46 HOSPICE CARE TABLE OF CONTENTS
 Medicaid Chapter 560-X-46 ALABAMA MEDICAID AGENCY ADMINISTRATIVE CODE CHAPTER 560-X-46 HOSPICE CARE TABLE OF CONTENTS 560-X-46-.01 560-X-46-.02 560-X-46-.03 560-X-46-.04 560-X-46-.05 560-X-46-.06 560-X-46-.07
Medicaid Chapter 560-X-46 ALABAMA MEDICAID AGENCY ADMINISTRATIVE CODE CHAPTER 560-X-46 HOSPICE CARE TABLE OF CONTENTS 560-X-46-.01 560-X-46-.02 560-X-46-.03 560-X-46-.04 560-X-46-.05 560-X-46-.06 560-X-46-.07
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability
 Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
May 2007 Provider Bulletin Number 753. Hospice Providers. Changes to ICF/MR Room and Board Charges for Hospice Beneficiaries
 May 2007 Provider Bulletin Number 753 Hospice Providers Changes to ICF/MR Room and Board Charges for Hospice Beneficiaries This is an update to bulletin 743. A correction has been made regarding how to
May 2007 Provider Bulletin Number 753 Hospice Providers Changes to ICF/MR Room and Board Charges for Hospice Beneficiaries This is an update to bulletin 743. A correction has been made regarding how to
Michigan. Source: Data collected by George Washington University for MACPAC Back to Summary. Date Last Searched. Documentation Date
 Medicaid Nursing Facility Payment Policy Landscapes - Note: Data is based on publicly available policy documentation identified in March, April, May of 2014. Follow-up contact was made with state Medicaid
Medicaid Nursing Facility Payment Policy Landscapes - Note: Data is based on publicly available policy documentation identified in March, April, May of 2014. Follow-up contact was made with state Medicaid
Overview of the Federal 340B Drug Pricing Program
 Overview of the Federal 340B Drug Pricing Program Presented by: James A. Raley, CPA Senior Manager Health Care Services Arnett Carbis Toothman LLP 345 340B Program: Overview Provides discounts on outpatient
Overview of the Federal 340B Drug Pricing Program Presented by: James A. Raley, CPA Senior Manager Health Care Services Arnett Carbis Toothman LLP 345 340B Program: Overview Provides discounts on outpatient
Looking at Patient Flow in Hours and Days
 This presenter has nothing to disclose Looking at Patient Flow in Hours and Days Getting Patients to the Right Level of Care at the Right Time October 23, 2014 Session Objectives Understand the differences
This presenter has nothing to disclose Looking at Patient Flow in Hours and Days Getting Patients to the Right Level of Care at the Right Time October 23, 2014 Session Objectives Understand the differences
Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid
 Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid Information posted on October 8, 2010 Effective for dates of service on or after December 1, 2010, the benefit criteria
Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid Information posted on October 8, 2010 Effective for dates of service on or after December 1, 2010, the benefit criteria
RESPITE CARE LEGACY HOSPICE
 RESPITE CARE LEGACY HOSPICE THE BASICS OF RESPITE CARE WHAT IS RESPITE? Short-term inpatient care provided only when necessary to relieve the family members or other persons caring for the individual at
RESPITE CARE LEGACY HOSPICE THE BASICS OF RESPITE CARE WHAT IS RESPITE? Short-term inpatient care provided only when necessary to relieve the family members or other persons caring for the individual at
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model
 Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
Prior Authorization form for Post-Acute Care Admission and Recertification for SNF,LTAC and Rehab
 Prior Authorization form for Post-Acute Care Admission and Recertification for SNF,LTAC and Rehab (Required for all Rehab, SNF, LTAC admits) Providers must request authorization for initial admissions
Prior Authorization form for Post-Acute Care Admission and Recertification for SNF,LTAC and Rehab (Required for all Rehab, SNF, LTAC admits) Providers must request authorization for initial admissions
The Medicare Admissions Process and Strategies for Success. Your Speakers
 The Medicare Admissions Process and Strategies for Success Leading Age Michigan 2014 Annual Leadership Institute Thursday, August 14, 2014 10:45 am 11:45 am 1 Your Speakers Betsy Anderson, President FR&R
The Medicare Admissions Process and Strategies for Success Leading Age Michigan 2014 Annual Leadership Institute Thursday, August 14, 2014 10:45 am 11:45 am 1 Your Speakers Betsy Anderson, President FR&R
Course Module Objectives
 Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1
 Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER PEPPER target areas Percents and percentiles Comparison
Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER PEPPER target areas Percents and percentiles Comparison
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Hospital Transitions: A Guide for Professionals.
 Hospital Transitions: A Guide for Professionals 2017 www.medicarerights.org Medicare Rights Center The Medicare Rights Center is a national, nonprofit consumer service organization that works to ensure
Hospital Transitions: A Guide for Professionals 2017 www.medicarerights.org Medicare Rights Center The Medicare Rights Center is a national, nonprofit consumer service organization that works to ensure
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Section 4 - Referrals and Authorizations: UM Department
 Section 4 - Referrals and Authorizations: UM Department Primary Care Referral Process 1 Referrals to In-Network Specialists 1 Referrals to Out-Of-Network Specialists 2 Consultation Referral Forms 2 Consultation
Section 4 - Referrals and Authorizations: UM Department Primary Care Referral Process 1 Referrals to In-Network Specialists 1 Referrals to Out-Of-Network Specialists 2 Consultation Referral Forms 2 Consultation
Critical Access Hospitals and Cost-Based Reimbursement
 Critical Access Hospitals and Cost-Based Reimbursement Jared Heim, CPA, Partner jheim@eidebailly.com 563.557.6169 Agenda for Today Overview of Critical Access Hospitals Overview of Health Care Reform Behavioral
Critical Access Hospitals and Cost-Based Reimbursement Jared Heim, CPA, Partner jheim@eidebailly.com 563.557.6169 Agenda for Today Overview of Critical Access Hospitals Overview of Health Care Reform Behavioral
Chapter 9 Section 1. Ambulatory Surgical Center (ASC) Reimbursement
 Reimbursement") Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Comparison of Bundled Payment Models. Model 1 Model 2 Model 3 Model 4. hospitals, physicians, and post-acute care where
 Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Medicare Advantage Outreach and Education Bulletin
 Medicare Advantage Outreach and Education Bulletin December 2010 To: All Medicare Advantage (MA) Physicians & Practitioners, Hospitals & Facilities* *Contracting physicians & practitioners, hospitals &
Medicare Advantage Outreach and Education Bulletin December 2010 To: All Medicare Advantage (MA) Physicians & Practitioners, Hospitals & Facilities* *Contracting physicians & practitioners, hospitals &
INPATIENT HOSPITAL REIMBURSEMENT
 HCRA CLAIMS PROCESSING Reimbursement: HCRA is not Medicaid; however, HCRA covered services are reimbursed at the hospital s outpatient or inpatient reimbursement rate allowed for Florida Medicaid. The
HCRA CLAIMS PROCESSING Reimbursement: HCRA is not Medicaid; however, HCRA covered services are reimbursed at the hospital s outpatient or inpatient reimbursement rate allowed for Florida Medicaid. The
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
The Regulatory Focus. Critical Access Hospitals The Regulatory Process
 Critical Access Hospitals The Regulatory Process Montana DPHHS Quality Assurance Division Roy Kemp, Deputy Administrator rkemp@mt.gov The Regulatory Focus The fundamental principal of the state regulatory
Critical Access Hospitals The Regulatory Process Montana DPHHS Quality Assurance Division Roy Kemp, Deputy Administrator rkemp@mt.gov The Regulatory Focus The fundamental principal of the state regulatory
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Working Paper Series
 The Financial Benefits of Critical Access Hospital Conversion for FY 1999 and FY 2000 Converters Working Paper Series Jeffrey Stensland, Ph.D. Project HOPE (and currently MedPAC) Gestur Davidson, Ph.D.
The Financial Benefits of Critical Access Hospital Conversion for FY 1999 and FY 2000 Converters Working Paper Series Jeffrey Stensland, Ph.D. Project HOPE (and currently MedPAC) Gestur Davidson, Ph.D.
06-01 FORM HCFA WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the
 06-01 FORM HCFA-1728-94 3204 3203. WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the initial cost report (first cost report filed for the
06-01 FORM HCFA-1728-94 3204 3203. WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the initial cost report (first cost report filed for the
Index. Bone densitometry, 20. Family caregivers. See Informal care Functional impairment factors, 4,51 I 91
 Index A Activities of daily living functional impairment and, 50-51 ADLs. See Activities of daily living Age factors. See also Patients age 65 and over; Patients age 50 to 64 discharge to rehabilitation
Index A Activities of daily living functional impairment and, 50-51 ADLs. See Activities of daily living Age factors. See also Patients age 65 and over; Patients age 50 to 64 discharge to rehabilitation
August 25, Dear Ms. Verma:
 Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
Medicaid Hospital Incentive Payments Calculations
 Medicaid Hospital Incentive Payments Calculations Note: This guidance is intended to assist hospitals and others in understanding Medicaid hospital incentive payment calculations. However, all hospitals
Medicaid Hospital Incentive Payments Calculations Note: This guidance is intended to assist hospitals and others in understanding Medicaid hospital incentive payment calculations. However, all hospitals
Rural Medicare Provider Types and Payment Provisions
 Rural Medicare Provider Types and Payment Provisions American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues March 25-27, 2015 Emily Jane Cook I. What is Rural?- Common Rural
Rural Medicare Provider Types and Payment Provisions American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues March 25-27, 2015 Emily Jane Cook I. What is Rural?- Common Rural
MANAGED CARE IS HERE
 MANAGED CARE IS HERE Survive or Thrive Susie Mix CEO/President Mix Solutions Inc. 1 Nursing Home (NH) Industry Transformation Senior Care Industry Trends & Strategies Why do we care about change? Finances
MANAGED CARE IS HERE Survive or Thrive Susie Mix CEO/President Mix Solutions Inc. 1 Nursing Home (NH) Industry Transformation Senior Care Industry Trends & Strategies Why do we care about change? Finances
Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A
 Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A Sec. 15001. Development of Medicare study for HCPCS versions of MS-DRG codes
Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A Sec. 15001. Development of Medicare study for HCPCS versions of MS-DRG codes
Palmetto GBA Hospice Coalition Questions August 7, 2001
 Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Understanding the PEPPER
 Understanding the PEPPER and What It Means to Your IRF FIM, UDS-PRO, and UDSMR are trademarks of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc. Sue Gehrman,
Understanding the PEPPER and What It Means to Your IRF FIM, UDS-PRO, and UDSMR are trademarks of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc. Sue Gehrman,
The Medicare Hospice Benefit. What Does It Mean to You and Your Patients?
 The Medicare Hospice Benefit What Does It Mean to You and Your Patients? The Medicare Hospice Benefit By the time Congress established the Medicare Hospice Benefit in 1982, hundreds of organizations in
The Medicare Hospice Benefit What Does It Mean to You and Your Patients? The Medicare Hospice Benefit By the time Congress established the Medicare Hospice Benefit in 1982, hundreds of organizations in
PROPOSED POLICY AND PAYMENT CHANGES FOR INPATIENT STAYS IN ACUTE-CARE HOSPITALS AND LONG-TERM CARE HOSPITALS IN FY 2014
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
CAH/FQHC Collaboration
 1 2017 FLEX PROGRAM REVERSE SITE VISIT BETHESDA, MD CAH/FQHC Collaboration A Community s Success Story Coal Country Community Health Center Sakakawea Medical Center 2 Presentation Agenda & Objectives Rural
1 2017 FLEX PROGRAM REVERSE SITE VISIT BETHESDA, MD CAH/FQHC Collaboration A Community s Success Story Coal Country Community Health Center Sakakawea Medical Center 2 Presentation Agenda & Objectives Rural
CURRENT OIG ENFORCEMENT INITIATIVES: A ROAD MAP FOR HIGH RISK COMPLIANCE AREAS
 10 th Annual HCCA Compliance Institute Session Las Vegas, NV April 25, 2006 CURRENT OIG ENFORCEMENT INITIATIVES: A ROAD MAP FOR HIGH RISK COMPLIANCE AREAS MARK HARDIMAN HOOPER, LUNDY & BOOKMAN, INC. 1875
10 th Annual HCCA Compliance Institute Session Las Vegas, NV April 25, 2006 CURRENT OIG ENFORCEMENT INITIATIVES: A ROAD MAP FOR HIGH RISK COMPLIANCE AREAS MARK HARDIMAN HOOPER, LUNDY & BOOKMAN, INC. 1875
08/07/2015. Next Generation ACO Model. What is an ACO? Preliminary Beneficiary Engagement Timeline
 Next Generation ACO Model National Training Program RO V and RO VII St. Louis August 10-11, 2015 What is an ACO? Accountable Care Organizations (ACOs) are groups of doctors, hospitals, and other health
Next Generation ACO Model National Training Program RO V and RO VII St. Louis August 10-11, 2015 What is an ACO? Accountable Care Organizations (ACOs) are groups of doctors, hospitals, and other health
AHLA. Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions
 AHLA Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Joan C. Ragsdale CEO MedManagement LLC Vestavia,
AHLA Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Joan C. Ragsdale CEO MedManagement LLC Vestavia,
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate