FALL PREVENTION PROGRAM
|
|
|
- Jeffry Blankenship
- 6 years ago
- Views:
Transcription
1 The Guam Memorial Hospital Authority Proudly Presents: FALL PREVENTION PROGRAM CAUTION: FALL RISK Roseann Apuron, RNC-OB & Jasmin Tanglao, RN February 2018
2 OBJECTIVES: AT THE END OF THE PRESENTATION STAFF WILL BE ABLE TO: 1. Recall the key elements of the GMHA Fall Prevention Program 2. Identify components of the Fall Risk Assessment Tools in the Clinical Setting for adult and pediatric populations. 3. Describe current and new nursing interventions for each risk level, for adults and the pediatric populations 4. Describe what to do after a fall incident. 5. Explain how everyone can be a team player in preventing falls here at GMHA.
3 IMPORTANCE OF THE PROGRAM: Patient Safety! Comply with Joint Commission Requirements: Reduce the risk of patient harm resulting from falls Initiate evidence-based practices to reduce the incidence of falls Continue to implement an Interdisciplinary approach to Fall Prevention Hospital-wide Continue our Mission: To Provide Quality Patient Care in a Safe Environment
4 WHAT IS A FALL? It is an unplanned descent to the floor (or extension of the floor, with or without injury to the patient: All types of falls are to be included whether they result from physiological reasons (fainting) or environmental reasons (slippery floor). Include assisted falls when a staff member attempts to minimize the impact of the fall.
5 STATS ABOUT FALLS IN HC FACILITIES: Patient falls affect between 700,000 to 1 million patients each year. Falls rank among the most frequently reported incidence in hospitals and other healthcare facilities. In acute care and rehab hospitals, between 30-51% of falls result in some injury. Up to 44% of those injuries are ones that may lead to death (i.e. fractures, subdural hematomas, or excessive bleeding). Injured patients require additional treatment and sometimes prolonged hospital stays. The average cost for a fall with injury was about $14,000 in Today, falls with serious injuries cost hospitals an additional $27,000. Falls with serious injury are consistently among the Top 10 sentinel events reported to The Joint Commission s Sentinel Event database. Falls must now be reported to the Hospital Improvement Innovation Network (HIIN) led by CMS.
6 WHAT CONTRIBUTES TO A FALL: Analysis of falls with injury in the Joint Commission Sentinel Event database reveals the most common contributing factors pertain to: Inadequate assessment Communication failures Lack of adherence to protocols and safety practices Inadequate staff orientation, supervision, staffing levels or skill mix Deficiencies in the physical environment Lack of leadership
7 CONTRIBUTING FACTORS TO A FALL: EXTRINSIC FACTORS INTRINSIC FACTORS
8 EXTRINSIC FACTORS: INADEQUATE ASSISTIVE DEVICES FURNITURE/ STRUCTURAL DESIGN FOOTWEAR POOR LIGHTING EXTRINSIC FACTORS EQUIPMENT MALFUNCTION MEDICATIONS EXCESSIVE CLUTTER FLOOR SURFACES Poor Lighting Medications Floor Surfaces Excessive Clutter Equipment Malfunction Footwear Inadequate Assistive Devices Furniture/ Structural Design
9 INTRINSIC FACTORS: Previous Falls Reduced vision Unsteady Gait Musculoskeletal System Mental Status Age and Gender Urinary Incontinence Illness Inadequate Nutrition ILLNESS INADEQUATE NUTRITION URINARY INCONTINENCE AGE & GENDER PREVIOUS FALLS INTRINSIC FACTORS MENTAL STATUS REDUCED VISION UNSTEADY GAIT MUSCULO- SKELETAL SYSTEM
10 PATIENT ASSESSMENT: Upon admission, and every shift, or with any ACOC, Fall Risk Assessment Tool: Adults: The Morse Fall Scale (18 years and older). Pediatrics: The Humpty Dumpty Falls Scale (age 3 months to 17 years). An Acute Change of Condition is a sudden, clinically important deviation from a resident s baseline in physical, cognitive, behavioral, or functional domains. Clinically important means a deviation that, without intervention, may result in complications or death.
11 ADULT TOOL: Morse Fall Scale Evidence- Based 6 areas of assessment: Fall History Secondary Diagnosis Ambulatory Aid Saline Lock / IV Gait Transferring Mental Status
12 MORSE FALL SCALE RISK LEVELS: Low Risk: 0-24 Moderate Risk: High Risk: Greater then 45

13 ADULT MEDICATION ASSESSMENT: HIGH ALERT MEDS:

14 ADULT MEDICATION ASSESSMENT : CAUTION MEDS: Note: Thrombolytics should be considered due to the risk of bleeding related to a fall incident... Important info to share in post fall huddle!
15 PEDIATRIC TOOL: The Humpty Dumpty Scale Evidence-Based 7 assessment criteria: Age Gender Diagnosis Environmental Factors Response to Surgery/Sedation/ Anesthesia Medication Usage

16 HUMPTY DUMPTY FALL SCALE RISK LEVELS: Only 2 Levels Low Risk: 7-11 High Risk: 12 or Above
17 PLAN OF CARE (POC): Implement POC based on the risk assessment score. A Fall Risk Care Plan will be initiated for patients indicated as High Risk. Risk level is either low risk, moderate risk, or high risk. POC shall be modified based on changes in the patient s condition. Any significant changes in the patient s condition must be communicated to all staff members involved in the patient s care. Discontinue POC if no longer considered a fall risk
18 NURSING INTERVENTIONS (ADULT): Low Risk (score of 0-24): Implement the Standard Fall Precautions: 1. Environmental orientation/re-orientation. 2. Call light use demonstrated and within reach. 3. Personal possessions within safe patient reach. 4. Handrails (bathrooms, room, and hallway). 5. Hospital bed in low position (while resting in bed); raise bed (when the patient is transferring out of bed). 6. Bed brakes locked. 7. Wheelchair wheel locks in "locked" position when stationary. 8. Patient footwear (nonslip, well-fitting). 9. Use night lights or supplemental lighting. 10. Floor surfaces kept clean and dry. 11. Keep care areas uncluttered. 12. Follow safe patient handling practices. 13. Place Call Don t Fall visual cues in patient rooms. 14. Encourage daily exercise or ambulation to maintain strength and reduce risk of debilitation if possible.
19 NURSING INTERVENTIONS (ADULT): Moderate Risk (score of 25-44): Implement the Standard Fall Precautions and the following: 1. Family members stay with patient or inform staff if leaving. 2. An Alert clasp identifier for fall (YELLOW clasp) will be placed on the patient s ID bracelet. 3. Place a Caution: Fall Risk sign in front of the patient s room. This is to alert hospital staff to monitor the patient closely for falls, and do spot-checks if passing by. 4. Inform Rehabilitative Services via imed application of patient s risk level for Balance Screening. 5. Emphasize on preventing falls, stress patient education, elaborating more on obtaining assistance when getting out of bed.
20 NURSING INTERVENTIONS (ADULT): High Risk (score of 45 and above): Implement the Standard Fall Precautions, Moderate Risk Interventions, and the following High Risk Preventative Measures: 1. Communicate High Risk Status. Initiate Plan of Care (POC). Notify the Physician. 2. Include Fall Precaution in patient s indicator profile (imed). 3. Re-educate patient and family on Fall Prevention Interventions-notify nurses if patient will be left alone in room. 4. If situation permits, relocate patient closer to nurses station. 5. Referrals or consults to address individual assessed problems (rehabilitative, dietary, social services, and pharmacy). 6. Environmental checklist (every shift) to ensure the safety of the patient. Any nursing staff can perform this checklist and inform the appropriate department of the deficiency for corrective action.
21 NURSING INTERVENTIONS (PEDIATRICS): Low Risk (score of 7-11): Implement the Standard Fall Precautions: 1. Assess elimination needs and assist as needed. 2. Keep call light within reach and educate on its functionality. 3. Place Call Don t Fall visual cues in patient rooms. 4. Keep environment clear (unused equipment or hazards). 5. Orient/re-orient patient and family to room and unit. 6. Keep bed in low position with brakes on. 7. Place side rails X2, assess large gaps, use additional safety precautions. 8. Use of non-skid footwear for ambulating patients. 9. Use of appropriate size clothing to prevent risk of tripping. 10. Assess for adequate lighting, leave nightlights on. 11. Ensure patient and family education (parents and patients).
22 NURSING INTERVENTIONS (PEDIATRICS): High Risk (score of 12 and above): Implement the Standard Fall Precautions and the following: 1. Place a Caution: Fall Risk sign in front of the patient s room and initiate POC. 2. Accompany patient with ambulation. 3. Family member involvement. 4. Educate Patient/Family regarding falls prevention: fall risk factors, appropriate transfer/ambulation needs, appropriate use of side rails. 5. Remove all unused equipment out of room. 6. Apply protective barriers if possible to close off spaces or gaps in the bed. 7. Evaluate medication administration times. Optimize medication administration times around safe functional independence of patient (ie. toileting, ambulating, etc.) 8. Location: Move patient closer to nurses station, if possible. 9. Environmental checklist (every shift) to ensure the safety of the patient. Any nursing staff can perform this checklist and inform the appropriate department of the deficiency for corrective action.


23 SIGNS IN ALL PATIENT ROOMS/AREAS:
24 ALERT CLASP: For Moderate Risk Patients Nursing Staff: Please place alert clasp on patient if applicable!
25 FOR MODERATE/HIGH FALL ALERT PATIENTS: For Moderate Risk (Adult) or High Risk (Pediatric) Patients Nursing Staff place this sign on the door to alert ALL STAFF of the patient s risk for fall. CAUTION: FALL RISK

26 NO PASS ZONE: On you tube, please watch this 2:27min video: The No Pass Zone- UC Health
27 NO PASS ZONE:(AS PER GMHA CLINICAL ALARMS POLICY (A-PS900) IT is the job OF ALL HOSPITAL EMPLOYEES to assist patients, their families, our visitors and each other. A call light/bell indicates a need. All employees are expected stop and check when a call light is on. The NO PASS rule shall apply
28 NO PASS RULE Never pass them by Observe patient privacy Provide what they are asking for if you can, OR Access someone who can Safety first, never put patients at risk Smile and use AIDET
29 AIDET Acknowledge: knock on door, wash hands, address by patient name, state purpose Introduce: staff name & occupation Duration: report to patient how long before someone can assist, stay with them Explanation: what you re doing and why, in understandable language, ask if any questions Thank you: thank them for alerting staff and wash hands
30 WHAT ALL STAFF CAN DO: Reposition call light, telephone, bedside table, chairs, trash can, tissues or other personal items within reach Assist with making phone calls or answering the telephone Change TV channels or turn TV on or off Turn lights on or off Obtain personal items such as blanket, pillow, towel, washcloth, slippers and toiletries Obtain other items such as pens, pencils, books, magazines, etc Open and/or close privacy curtains Reduce clutter If entering an isolation room, follow proper PPE requirements
31 WHAT NON-CLINICAL STAFF CANNOT DO: Only NURSING STAFF can do the following: Manage an IV and/or infusion pump Offer pain relief Remove meal trays or water pitchers Assist patients with eating and drinking Physically assist a patient Turn off any alarms Explain clinical matters/treatments, unless appropriate to your discipline Raise or lower a patient bed Transfer a patient between bed to bathroom, bed to chair, chair to bed, etc If you are a non-clinical staff member responding to an alarm and determine if the patient is in immediate distress, call for help IMMEDIATELY!
32 NO PASS ZONE REMINDERS: Do NOT Pass the patient s room, ignoring the call light Notify nursing staff of the patient s call if you do no notice anyone responding Knock on the patient s door, ensure privacy, and as what the patient may need In LR or OBW Do Not Enter the patient s room, please alert staff that the patient is calling

33 ENVIRONMENTAL CHECKLIST: Any nursing staff can complete the checklist Inform the appropriate department of any deficiency for corrective action
34 OTHER NURSING INTERVENTIONS: Shift Huddles to identify high risk patients on the floors Communication Boards Hourly rounding checking the 5 Ps: Pain, Position, Proximity- Personal Belongings/Call light, Pathway, Potty, 4 bed alarms: Tele-PCU, MSW, SW, SNU

35 ROUNDS CONDUCTED IN MED-SURG WARD:

36 NEW BED ALARMS:
37 PATIENT/FAMILY EDUCATION: Upon admission- instruct on how to prevent falls. Outcomes of this education shall be documented appropriately. In the event of a fall- the patient s family shall be notified. Upon discharge- patients identified as moderate or high risk for falls shall have discharge instructions provided to the patient and/or family regarding preventing falls at home.
38 PATIENT/FAMILY EDUCATION ON ADMISSION:

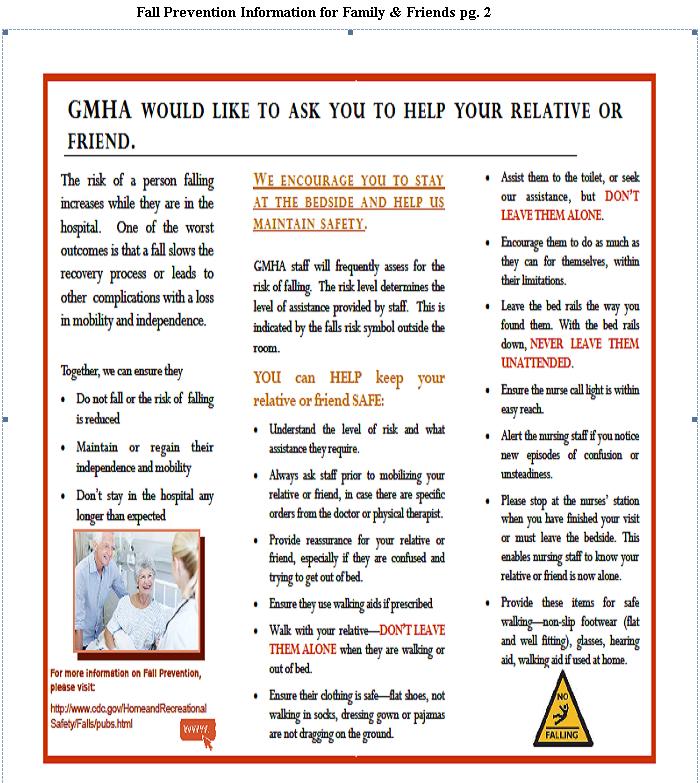
39 EDUCATION FOR FAMILY/FRIENDS:
40 WHAT TO DO AFTER A FALL INCIDENT: Immediate assessment by a registered nurse, rendering necessary first aid and treatment. Assess the level of injury: i. No injuries ii. Minor Injury: Bruise, abrasion, minor laceration iii. Major Injury: Fracture(s), head trauma, loss of function iv. Death related to fall The patient s vital signs and level of consciousness shall be monitored and documented for the next 24 hours as follows: First Hour: Every 15 minutes Next Four Hours: Every 2 hours Remaining Hours (in 24 period): Every 4 hours The attending physician shall be notified immediately. Inform the physician of the extent of the injury (if any), the neurological status of the patient, and the current vital signs.
41 WHAT DO NURSES DOCUMENT? In the event a fall has occurred, the following shall be documented in the patient s notes (imed): Remember: PALLOR Physician notification of fall incident Medical and nursing Actions that were taken. Level of injury with descriptions Location of the fall Observations: Patient appearance at the time they were discovered Patient s Response to the fall, such as altered mental status, or presence of pain.
42 WHAT TO DO AFTER A FALL INCIDENT: Complete the Patient Safety Form and the Post Fall Information Report (as soon as possible and before the end of the shift). The completion of the Post-Fall Information Report shall involve the charge nurse, the patient s primary nurse and nurse assistant, and any other staff member who witnessed the fall. A Post-Fall Huddle shall occur immediately. The Fall Prevention Team including the Interdisciplinary members will be notified of the fall through the Post-Fall Information Report attached in the Nursing Supervisor s 24 hour report. The Fall Prevention Team will meet to discuss reported falls and determine corrective actions to improve patient outcomes. Any death or major loss of function related to a fall shall be reported immediately to the Patient Safety Officer/Risk Manager, Associate Administrator of Nursing Services and the Hospital Administrator.
43 POST FALL HUDDLE: Who: Primary nurse, Charge nurse, Nurse assistant, Hospital Nurse Supervisor on-duty and any other staff who witnessed the fall What: Discuss events surrounding the fall Where: At or Near Fall Location When: Immediately after the fall How: Use Post Fall Information Report to guide discussion Why: To try determine cause for fall and immediate corrective action

44 POST FALL INFORMATION REPORT:
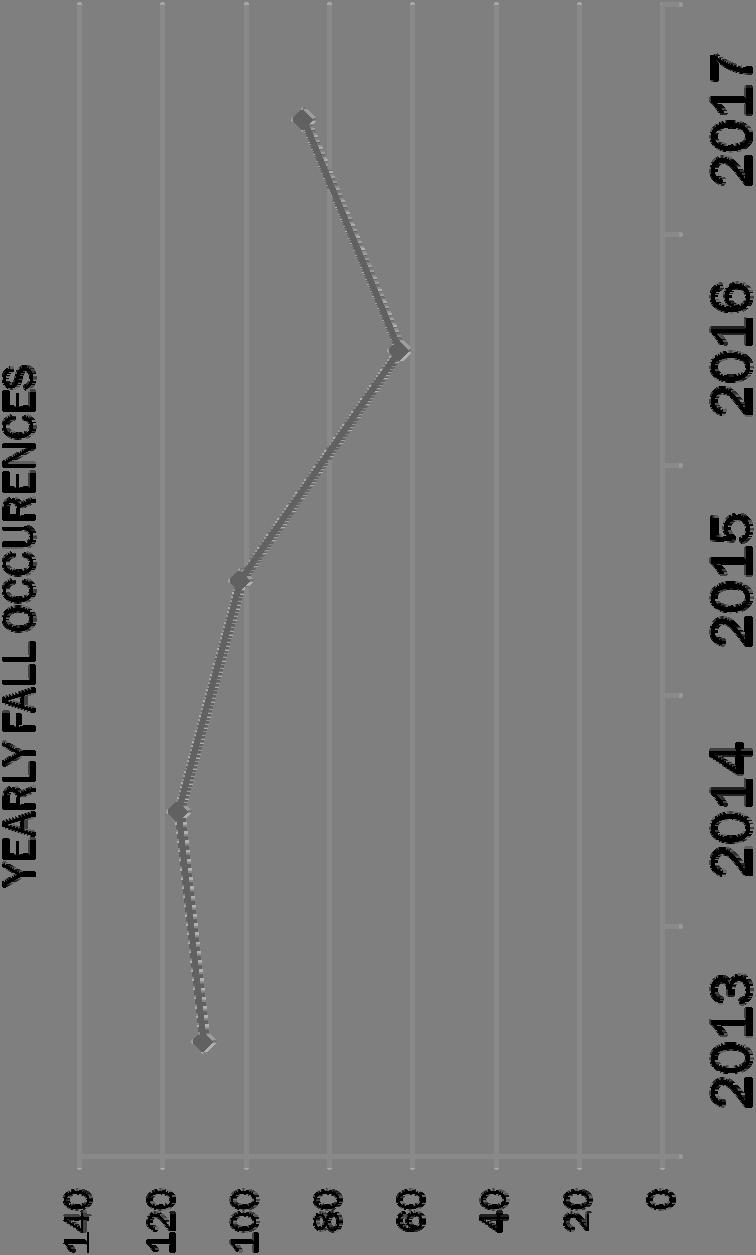
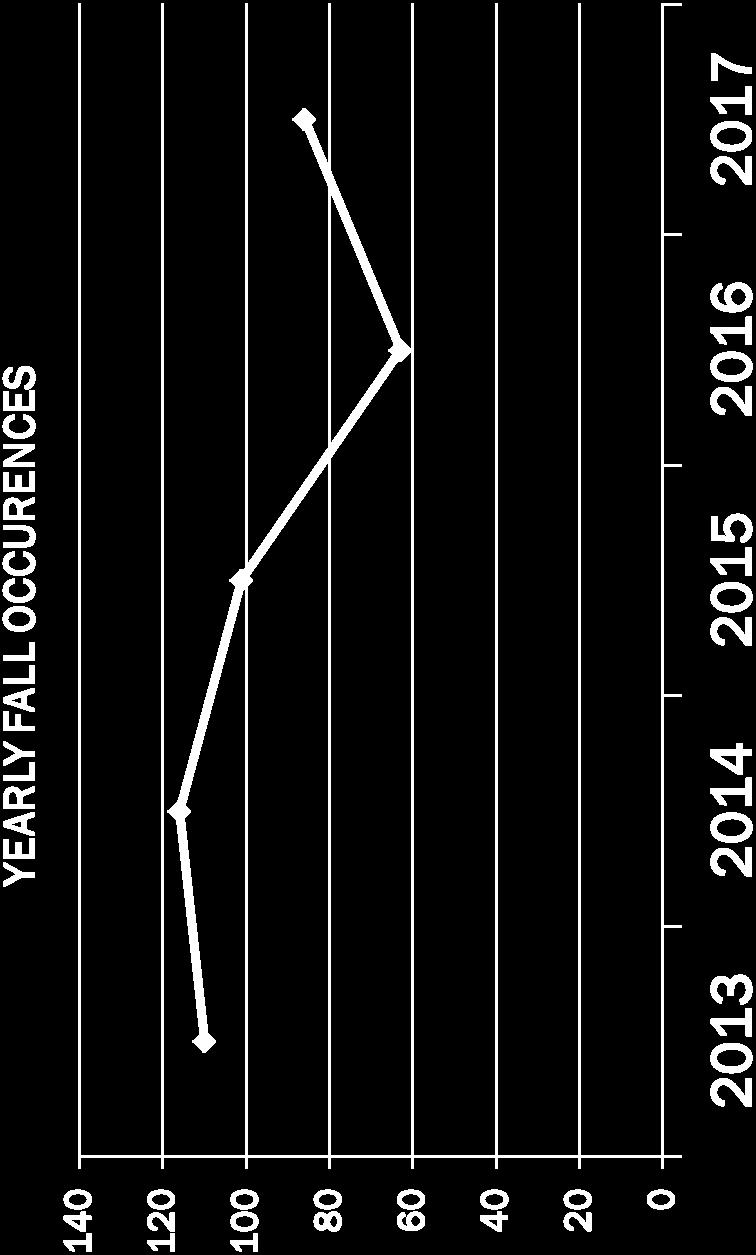
45 PERFORMANCE IMPROVEMENT: All fall occurrences are monitored by the Patient Safety Officer/Risk Manager and reported to Nursing Management, Patient Safety Committee, and the Performance Improvement Committee. The Interdisciplinary Team shall identify opportunities to reduce the risk associated with falls through preventative strategies, alternatives and process improvements.

46 PERFORMANCE IMPROVEMENT DATA: Total Falls: 101 MONTHLY FALL OCCURENCES BY NURSING UNITS 2016 JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC TOTAL ICU MSW TELE/PCU PEDS/PICU SURG HEMO ER ANCILLARY SNU MONTHLY FALL OCCURENCES BY NURSING UNITS JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC TOTAL ICU MSW TELE/PCU PEDS/PICU SURG HEMO ER ANCILLARY SNU Total Falls: 63 Total Falls: 86


47 PERFORMANCE IMPROVEMENT DATA: CY 15 CY 16 CY 17 CY 15 CY 16 CY
48 PERFORMANCE IMPROVEMENT DATA:

49 AN INTERDISCIPLINARY APPROACH: Nursing Services Department Rehabilitative Services Dietetic Services Pharmacy Department Social Services Medical Services
50 INTERDISCIPLINARY ROLES: Rehabilitative Services Will perform a functional screening on the identified patients. Dietetic Services All inpatients are screened for nutritional risk by a member of the health care team within hours of admission. Pharmacy Department Review, Verification, Interpretation of Medication Orders. The pharmacist shall interpret all medication orders and resolve all questions or problems prior to dispensing medications. Social Services Will conduct a Social evaluation of family or home situation for safe and secure placement at discharge. Medical Services ** New component to team, important component for patient care.
51 YOUR INTERDISCIPLINARY FALL PREVENTION TEAM: INTERDISCIPLINARY TEAM Nursing: Roseann Apuron & Jasmin Tanglao (Fall Committee Co-Chairpersons) Rehab Dept: Nora Garces Social Services: Ciena Materne Dietetic Services: Kristy Joy Mary Pharmacy: Jason Boyd Medical Staff: Dr. Kozue NURSING UNIT REPRESENTATIVES: ER: Essel Kerr SSD/UC/Radiology: Belle Rada ICU: Alvin Resurreccion Hemo: Veronica Censon L&D: Carlo Losinio MSW: Sherena Rosadino NICU: Avelina Opena OBW: Joanna Morales OR: Sr. Seville Cabuhat Peds: Rosa Segovia SNU: Elizabeth Camacho SW: Maria Blanquita Torres Tele-PCU: Raven Agpaoa
52 5 KEY TAKE AWAY POINTS Patient Safety is EVERYONE S responsibility NO PASS ZONE- if you hear a call- check the pt Licensed staff are responsible for completing assessments, including adult medication assessments, and initiating care plans. All Nursing Staff can help with interventions Post Fall Huddles must occur!

53 THANK YOU. FROM YOUR FALL TEAM!! Questions and Suggestions??

54 THANK YOU! To ensure comprehension of this online course please complete the online examination on our GMHA Portal: GMHA Fall Prevention Program Exam Your URL is: testmoz.com/ Please follow instructions on the next page in order to login A score of 80% or greater is necessary to pass the exam. If you do not pass the exam, please re-take the exam until a passing score is achieved. Exams are timed and any questionable submissions will be reported to your Supervisors for disciplinary action.
55 USER NAME & PASSWORD: In ALL CAPS, Please Indicate your Unit as one of the following: For Nursing: ADMN, ADMNNL (for non-licensed), SSD, RAD, ER, ICU, HEMO, LR, MSW, NICU, OBW, OR, PEDS, SNU,SW, TELE For all other Depts: enter the first four letters of your department in ALL CAPS: For example: PHAR for Pharmacy staff followed by your first initial, full last name and employee ID number (found on your ID badge) with NO SPACES in between. For Example: ADMNRAPURON Student Quiz Passcode:GMHA
Guidelines for Care: Suicide Precautions: a Two-Tiered Approach
 GMHA Nursing Services Department Guidelines for Care: Suicide Precautions: a Two-Tiered Approach Roseann Apuron, RNC OB, Staff Nurse Training Officer Objectives: 1. Discuss suicide precautions for GMHA
GMHA Nursing Services Department Guidelines for Care: Suicide Precautions: a Two-Tiered Approach Roseann Apuron, RNC OB, Staff Nurse Training Officer Objectives: 1. Discuss suicide precautions for GMHA
Definition of fall any unplanned descent to the floor, assisted or unassisted, with or without injury.
 1 Springfield, Illinois Patient Care Policy/Procedure Date: April, 2014 Subject: FALL PREVENTION AND MANAGEMENT: REDUCING HARM Policy: All patients are evaluated for risk of falls by the nurse on admission,
1 Springfield, Illinois Patient Care Policy/Procedure Date: April, 2014 Subject: FALL PREVENTION AND MANAGEMENT: REDUCING HARM Policy: All patients are evaluated for risk of falls by the nurse on admission,
Fall Prevention Program. St. Catherine Hospital East Chicago, Indiana Paula Swenson Chief Nursing Officer
 Fall Prevention Program St. Catherine Hospital East Chicago, Indiana Paula Swenson Chief Nursing Officer St. Catherine Hospital 189 bed community hospital, located in East Chicago Indiana Member of Community
Fall Prevention Program St. Catherine Hospital East Chicago, Indiana Paula Swenson Chief Nursing Officer St. Catherine Hospital 189 bed community hospital, located in East Chicago Indiana Member of Community
Fall Prevention. Falls 1
 Falls 1 Fall Prevention A fall is defined as an unplanned descent to the floor with or without injury. Patient falls contribute to mortality and increased morbidity in the general patient population. Implementation
Falls 1 Fall Prevention A fall is defined as an unplanned descent to the floor with or without injury. Patient falls contribute to mortality and increased morbidity in the general patient population. Implementation
EXPERIENCE OF NH HOSPITALS: FALLS DATA NH FALLS RISK REDUCTION TASK FORCE ANNUAL DATA MEETING MARCH 7, 2017 PRESENTED BY: ANNE DIEFENDORF FOUNDATION
 EXPERIENCE OF NH HOSPITALS: FALLS DATA NH FALLS RISK REDUCTION TASK FORCE ANNUAL DATA MEETING MARCH 7, 2017 PRESENTED BY: ANNE DIEFENDORF FOUNDATION FOR HEALTHY COMMUNITIES Objectives Review 2015 NH Adverse
EXPERIENCE OF NH HOSPITALS: FALLS DATA NH FALLS RISK REDUCTION TASK FORCE ANNUAL DATA MEETING MARCH 7, 2017 PRESENTED BY: ANNE DIEFENDORF FOUNDATION FOR HEALTHY COMMUNITIES Objectives Review 2015 NH Adverse
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: PEDIATRIC FALL PREVENTION EFFECTIVE DATE: REVISED DATE: POLICY TYPE: Job Title of Reviewer: Director, Women & Children s Department (pediatrics)
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: PEDIATRIC FALL PREVENTION EFFECTIVE DATE: REVISED DATE: POLICY TYPE: Job Title of Reviewer: Director, Women & Children s Department (pediatrics)
Fall Prevention Protocol
 Fall Prevention Protocol I. Assessment Each patient should be assessed for fall risk: On admission to the facility On any transfer from one unit to another within the facility Following any change of status
Fall Prevention Protocol I. Assessment Each patient should be assessed for fall risk: On admission to the facility On any transfer from one unit to another within the facility Following any change of status
Current Status: Active PolicyStat ID: Fall Prevention, 3F 01.5 COPY
 Current Status: Active PolicyStat ID: 4273244 Origination: 10/2000 Last Approved: 01/2017 Last Revised: 12/2016 Next Review: 01/2020 Owner: Damian Gulbransen: Dir, Nursing Area: Clinical (Patient Care)
Current Status: Active PolicyStat ID: 4273244 Origination: 10/2000 Last Approved: 01/2017 Last Revised: 12/2016 Next Review: 01/2020 Owner: Damian Gulbransen: Dir, Nursing Area: Clinical (Patient Care)
Preventing Falls in the Home
 ~ VOLUME I ISSUE V LESSON PLAN ~ OBJECTIVES Upon completion of this program, the home health aide will be able to:» Identify four variables that increase the likelihood of falls» List three common hazards
~ VOLUME I ISSUE V LESSON PLAN ~ OBJECTIVES Upon completion of this program, the home health aide will be able to:» Identify four variables that increase the likelihood of falls» List three common hazards
ATTENTION ALL C.N.A S
 ATTENTION ALL C.N.A S October s monthly Education Manual will not be the usual booklet. You will find a different handout with required reading and a post test. This handout will meet your required units
ATTENTION ALL C.N.A S October s monthly Education Manual will not be the usual booklet. You will find a different handout with required reading and a post test. This handout will meet your required units
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: PEDIATRIC FALL PREVENTION EFFECTIVE DATE: REVISED DATE: POLICY TYPE: Job Title of Reviewer: Director, Women & Children s Department (pediatrics)
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: PEDIATRIC FALL PREVENTION EFFECTIVE DATE: REVISED DATE: POLICY TYPE: Job Title of Reviewer: Director, Women & Children s Department (pediatrics)
Falls Prevention In Rehabilitation
 Falls Prevention In Rehabilitation Robyn Walker Rankin Park Centre Greater Newcastle Cluster March 2008 1 Frequency of Falls A total of 157 patients fell in Rankin Park Centre during the 12 months from
Falls Prevention In Rehabilitation Robyn Walker Rankin Park Centre Greater Newcastle Cluster March 2008 1 Frequency of Falls A total of 157 patients fell in Rankin Park Centre during the 12 months from
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Patient-Centered Fall Prevention Toolkit Paper Fall TIPS Instruction Sheet for Nurses
 Overview Patient-Centered Fall Prevention Toolkit Paper Fall TIPS Instruction Sheet for Nurses Preventing falls is a three step process * : 1) identifying risk factors; 2) developing a tailored or personalized
Overview Patient-Centered Fall Prevention Toolkit Paper Fall TIPS Instruction Sheet for Nurses Preventing falls is a three step process * : 1) identifying risk factors; 2) developing a tailored or personalized
Patient Safety: Fall Prevention. Unlicensed Assistive Personnel
 Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
NorthCrest Medical Center Amanda Costello RN, BSN, CMSRN
 NorthCrest Medical Center Amanda Costello RN, BSN, CMSRN Robertson County is located approximately 30 miles north of Nashville. Robertson county sits between Cheatham, Davidson and Sumner counties and
NorthCrest Medical Center Amanda Costello RN, BSN, CMSRN Robertson County is located approximately 30 miles north of Nashville. Robertson county sits between Cheatham, Davidson and Sumner counties and
Purpose and Objectives
 Fall Prevention Purpose and Objectives Purpose: Review the UC Health Fall Prevention Program. Objectives: 1. Present evidence about patient safety and falls. 2. Review the UC Health Fall Prevention Policy
Fall Prevention Purpose and Objectives Purpose: Review the UC Health Fall Prevention Program. Objectives: 1. Present evidence about patient safety and falls. 2. Review the UC Health Fall Prevention Policy
The Joint Commission and Facility Design: A Partnership for Patient Safety and Quality Care
 The Joint Commission and Facility Design: A Partnership for Patient Safety and Quality Care A Webinar Presentation for the AIA AAH 8 January 2013 1 Topic 1: Driving Safety through Good Design Presenter:
The Joint Commission and Facility Design: A Partnership for Patient Safety and Quality Care A Webinar Presentation for the AIA AAH 8 January 2013 1 Topic 1: Driving Safety through Good Design Presenter:
REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL
 Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
WRHA Constant Care Guidelines for Acute Care 2018
 WRHA Constant Care Guidelines for Acute Care 8. PURPOSE To establish standardized guidelines and support appropriate use of constant care in acute care settings. Separate guidelines apply to residents
WRHA Constant Care Guidelines for Acute Care 8. PURPOSE To establish standardized guidelines and support appropriate use of constant care in acute care settings. Separate guidelines apply to residents
KENT HOSPITAL POLICY/PROCEDURE SUBJECT: AUTHORS: APPROVAL DATE: POLICY NUMBER: January 2012 EFFECTIVE DATE: January January 2013 NPP600-E-6
 KENT HOSPITAL POLICY/PROCEDURE SUBJECT: AUTHORS: APPROVAL DATE: POLICY NUMBER: January 2012 Fall Prevention Barbara Bird, MSN, RN-BC, CCNS EFFECTIVE DATE: 8310-0005 Falls Council/ Prevention Committee
KENT HOSPITAL POLICY/PROCEDURE SUBJECT: AUTHORS: APPROVAL DATE: POLICY NUMBER: January 2012 Fall Prevention Barbara Bird, MSN, RN-BC, CCNS EFFECTIVE DATE: 8310-0005 Falls Council/ Prevention Committee
Reducing and Discontinuing Resident Alarms. The False Reassurance of Personal Alarms
 Across the country, state health organizations, nursing homes, private and government quality improvement organizations have all been studying the impact of personal alarms on the lives of residents in
Across the country, state health organizations, nursing homes, private and government quality improvement organizations have all been studying the impact of personal alarms on the lives of residents in
IHI Expedition: Smart Use of Resources: Nurses' Time. IHI Support Staff
 IHI Expedition: Smart Use of Resources: Nurses' Time Session 6 June 28, 2012 Content: Designing new care delivery models IHI Support Staff Tracy Jacobs Director Kayla DeVincentis Project Coordinator 2
IHI Expedition: Smart Use of Resources: Nurses' Time Session 6 June 28, 2012 Content: Designing new care delivery models IHI Support Staff Tracy Jacobs Director Kayla DeVincentis Project Coordinator 2
Patient Fall Prevention Orientation Module. Wheaton Franciscan Healthcare
 Patient Fall Prevention Orientation Module Wheaton Franciscan Healthcare Learning Objectives Define the goals of fall prevention Define a fall Identify patients at risk for falls Identify factors that
Patient Fall Prevention Orientation Module Wheaton Franciscan Healthcare Learning Objectives Define the goals of fall prevention Define a fall Identify patients at risk for falls Identify factors that
Alberta First Nations Continuing Care Needs Assessment - Health and Home Care Program Staff Survey -
 Alberta First Nations Continuing Care Needs Assessment p. 1 Alberta First Nations Continuing Care Needs Assessment - Health and Home Care Program Staff Survey - Definition of Terms Continuing Care: As
Alberta First Nations Continuing Care Needs Assessment p. 1 Alberta First Nations Continuing Care Needs Assessment - Health and Home Care Program Staff Survey - Definition of Terms Continuing Care: As
SUMMARY OF INDICATOR CHANGES FOR VERSION 3 INTELLIGENT MONITORING REPORTS Acute and Specialist NHS Trusts 23 June Final Draft, Subject to Change
 Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
CH Patient Fall Prevention
 GUIDELINES/PLANS/POLICIES & PROCEDURES CH Patient Fall Prevention Summary: Every patient presenting to the hospital will be assessed in order to determine the patient's potential for falls. Effective Date:
GUIDELINES/PLANS/POLICIES & PROCEDURES CH Patient Fall Prevention Summary: Every patient presenting to the hospital will be assessed in order to determine the patient's potential for falls. Effective Date:
Pharmaceutical Services Report to Joint Conference Committee September 2010
 Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
FALL PREVENTION ASSESSING THE 5P S OF HOURLY ROUNDING. Katie Souviney, RN BSN and Jennifer Posnick RN
 FALL PREVENTION ASSESSING THE 5P S OF HOURLY ROUNDING Katie Souviney, RN BSN and Jennifer Posnick RN ARE FALLS REALLY A PROBLEM? Here are the facts Each year between 700,000 and 1,000,000 people in the
FALL PREVENTION ASSESSING THE 5P S OF HOURLY ROUNDING Katie Souviney, RN BSN and Jennifer Posnick RN ARE FALLS REALLY A PROBLEM? Here are the facts Each year between 700,000 and 1,000,000 people in the
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
AT THE UNIVERSITY OF ILLINOIS HOSPITAL AND HEALTH SCIENCES SYSTEM
 PARENT HANDBOOK A PATIENT CENTERED ORGANIZATION The University of Illinois Hospital and Clinics is a patient centered organization. Providing safe, high-quality and cost-effective care for our patients
PARENT HANDBOOK A PATIENT CENTERED ORGANIZATION The University of Illinois Hospital and Clinics is a patient centered organization. Providing safe, high-quality and cost-effective care for our patients
Prevention of Pediatric Patient Falls. Instruction Packet
 Prevention of Pediatric Patient Falls Instruction Packet University of Minnesota Children s Hospital, Fairview M Turner/ 1/07 1 Dear UMCH, F, patient care staff, As you are aware, reduction of patient
Prevention of Pediatric Patient Falls Instruction Packet University of Minnesota Children s Hospital, Fairview M Turner/ 1/07 1 Dear UMCH, F, patient care staff, As you are aware, reduction of patient
University of Akron College of Nursing 370-Care of Older Adult Home Safety Checklist
 University of Akron College of Nursing 370-Care of Older Adult Home Safety Checklist Patient: 1. 2. 3. 4. Living Room/- Family Room Yes No Can you turn on a light without having to walk into a dark room?
University of Akron College of Nursing 370-Care of Older Adult Home Safety Checklist Patient: 1. 2. 3. 4. Living Room/- Family Room Yes No Can you turn on a light without having to walk into a dark room?
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Solution Title: Sustaining Fall Prevention Over Time, Is It Possible?
 Organization: Sinai Hospital of Maryland Solution Title: Sustaining Fall Prevention Over Time, Is It Possible? Focus rea: Preventing Falls with Injury Program/Project Description, Including Goals: In 2010,
Organization: Sinai Hospital of Maryland Solution Title: Sustaining Fall Prevention Over Time, Is It Possible? Focus rea: Preventing Falls with Injury Program/Project Description, Including Goals: In 2010,
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
HCAHPS. Presented by: Bill Sexton. Proudly recognized as one of the Nation s Top 100 Critical Access Hospitals - ivantage Health Analytics
 HCAHPS Presented by: Bill Sexton HCAHPS results will impact your organization's reimbursement in the era of health care reform HCAPHS results are a quality metric, not just a patient satisfaction metric
HCAHPS Presented by: Bill Sexton HCAHPS results will impact your organization's reimbursement in the era of health care reform HCAPHS results are a quality metric, not just a patient satisfaction metric
Utilization of a Nursing Bundle to Improve the Patient Experience
 Utilization of a Nursing Bundle to Improve the Patient Experience Tina Prescott, MBA, BSN, RN, NEA-BC Chief Nursing Officer West Tennessee Healthcare Our Healthcare System Locations across West Tennessee
Utilization of a Nursing Bundle to Improve the Patient Experience Tina Prescott, MBA, BSN, RN, NEA-BC Chief Nursing Officer West Tennessee Healthcare Our Healthcare System Locations across West Tennessee
Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound)
") Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound) Problem: Surveys showed that the noise level made it difficult for patients to rest. Innovation: Implemented a culture of quiet.
Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound) Problem: Surveys showed that the noise level made it difficult for patients to rest. Innovation: Implemented a culture of quiet.
Northern Health - Acute Services. Evidence Based Practice Venous Thromboembolism Prevention
 Northern Health - Acute Services Evidence Based Practice Venous Thromboembolism Prevention (VTE) Jeannette Kamar Christine Lamotte, Liam Carter Improving Patient Safety Preventing and Managing Venous Thromboembolism
Northern Health - Acute Services Evidence Based Practice Venous Thromboembolism Prevention (VTE) Jeannette Kamar Christine Lamotte, Liam Carter Improving Patient Safety Preventing and Managing Venous Thromboembolism
FALLS RISK REDUCTION & MANAGEMENT OF INPATIENT FALLS - STANDARDS
 STANDARDS TO BE MET 1. Safe Mobilisation and Falls Prevention Assessment 1.1 The multidisciplinary team will: a) Conduct the Safe Mobilisation and Fall Prevention Assessment; b) Initiate appropriate interventions
STANDARDS TO BE MET 1. Safe Mobilisation and Falls Prevention Assessment 1.1 The multidisciplinary team will: a) Conduct the Safe Mobilisation and Fall Prevention Assessment; b) Initiate appropriate interventions
BOARD OF DIRECTORS PAPER COVER SHEET. Meeting Date: 1 st December 2010
 BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
PRINTED: 10/13/2017 FORM APPROVED CENTERS FOR MEDICARE & MEDICAID SERVICES OMB NO (X2) MULTIPLE CONSTRUCTION A.
 MULTIPLE CONSTRUCTION A.") ENTERS FOR MEDIARE & MEDIA SERVIES OMB NO. 0938-0391 (X2) MULTIPLE ONSTRUTION STATEMENT OF DEFIIENIES AND PLAN OF ORRETION NAME OF PROVER OR SUPPLIER (X1) PROVER/SUPPLIER/LIA ENTIFIATION NUMBER: JAMES
ENTERS FOR MEDIARE & MEDIA SERVIES OMB NO. 0938-0391 (X2) MULTIPLE ONSTRUTION STATEMENT OF DEFIIENIES AND PLAN OF ORRETION NAME OF PROVER OR SUPPLIER (X1) PROVER/SUPPLIER/LIA ENTIFIATION NUMBER: JAMES
Recommendations for Adoption
 North Carolina Hospital Association Recommendations for Adoption ALLERGY FALL RISK 7 Recommendations for Adoption August 2009 Do Not Resuscitate Recommendation: It is recommended that hospitals adopt the
North Carolina Hospital Association Recommendations for Adoption ALLERGY FALL RISK 7 Recommendations for Adoption August 2009 Do Not Resuscitate Recommendation: It is recommended that hospitals adopt the
APPENDIX I HOSPICE INPATIENT FACILITY (HIF)
") INTRODUCTION APPENDIX I HOSPICE INPATIENT FACILITY (HIF) The principles and standards in all chapters of the Standards of Practice for Hospice Programs apply to hospice care provided in an inpatient facility.
INTRODUCTION APPENDIX I HOSPICE INPATIENT FACILITY (HIF) The principles and standards in all chapters of the Standards of Practice for Hospice Programs apply to hospice care provided in an inpatient facility.
The Patient Experience at Florida Hospital Learning Module for Students
 The Patient Experience at Florida Hospital Learning Module for Students 1 Introduction Adventist Health System and its East Florida Region hospitals welcome the privilege to provide a wellrounded learning
The Patient Experience at Florida Hospital Learning Module for Students 1 Introduction Adventist Health System and its East Florida Region hospitals welcome the privilege to provide a wellrounded learning
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
CAUTI Reduction A Clinton Memorial Presentation
 CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
University of Arkansas, Fayetteville. Loribeth Alexander University of Arkansas, Fayetteville
 University of Arkansas, Fayetteville ScholarWorks@UARK The Eleanor Mann School of Nursing Undergraduate Honors Theses The Eleanor Mann School of Nursing 12-2014 A Quality Improvement Study Concerning the
University of Arkansas, Fayetteville ScholarWorks@UARK The Eleanor Mann School of Nursing Undergraduate Honors Theses The Eleanor Mann School of Nursing 12-2014 A Quality Improvement Study Concerning the
Elaine Andrews, Assistant Director of Nursing & Safety and Caroline Booton Quality Analyst Jill Asbury, Acting Director of Nursing
 Report to: Board of Directors Date of Meeting: 26 th October 2016 Report Title: Inpatient Falls Report Status: Mark relevant box with X Prepared by: Executive Sponsor (presenting): For information x Discussion
Report to: Board of Directors Date of Meeting: 26 th October 2016 Report Title: Inpatient Falls Report Status: Mark relevant box with X Prepared by: Executive Sponsor (presenting): For information x Discussion
ACTIVITIES OF DAILY LIVING (ADL) DECLINE Facility Assessment Checklists
 DECLINE Facility Assessment Checklists") ACTIVITIES OF DAILY LIVING (ADL) DECLINE Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to activities of daily living
ACTIVITIES OF DAILY LIVING (ADL) DECLINE Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to activities of daily living
Chapter 11. Preventing Falls. Copyright 2019 by Elsevier, Inc. All rights reserved.
 Chapter 11 Preventing Falls Copyright 2019 by Elsevier, Inc. All rights reserved. Lesson 11.1 Define the key terms and key abbreviations in this chapter. Identify the causes and risk factors for falls.
Chapter 11 Preventing Falls Copyright 2019 by Elsevier, Inc. All rights reserved. Lesson 11.1 Define the key terms and key abbreviations in this chapter. Identify the causes and risk factors for falls.
Departments to Improve. February Chad Faiella RN, Terri Martin RN. 1 Process Excellence
 Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November 2017
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
The Reduction of Seclusion & Restraint in the University of Michigan Psychiatric Emergency Services with the Introduction of 24/7 Nurse Staffing
 The Reduction of Seclusion & Restraint in the University of Michigan Psychiatric Emergency Services with the Introduction of 24/7 Nurse Staffing Sharon P. Stetz MSN Marvella M. Muzik, MS PMHNP, BC Objectives
The Reduction of Seclusion & Restraint in the University of Michigan Psychiatric Emergency Services with the Introduction of 24/7 Nurse Staffing Sharon P. Stetz MSN Marvella M. Muzik, MS PMHNP, BC Objectives
The Value of Nursing: Implementation of Video Monitoring to Decrease 1:1 Sitter Cost
 The Value of Nursing: Implementation of Video Monitoring to Decrease 1:1 Sitter Cost 2010 NDNQI Conference January 20-22, 2010 New Orleans, Louisiana Janet Davis, RN, BSN, MS, NE-BC Tampa General Hospital
The Value of Nursing: Implementation of Video Monitoring to Decrease 1:1 Sitter Cost 2010 NDNQI Conference January 20-22, 2010 New Orleans, Louisiana Janet Davis, RN, BSN, MS, NE-BC Tampa General Hospital
Welcome to the Rehabilitation (Rehab) Unit
 Unit") Welcome to the Rehabilitation (Rehab) Unit How to contact the Rehab Unit Page 2 What to expect with your child s care Page 3 Daily rounds Page 5 Staying overnight and visiting hours Page 8 Keeping your
Welcome to the Rehabilitation (Rehab) Unit How to contact the Rehab Unit Page 2 What to expect with your child s care Page 3 Daily rounds Page 5 Staying overnight and visiting hours Page 8 Keeping your
Falls With Injury. Change Package 2015 UPDATE PREVENTING HARM FROM INJURIES DUE TO FALLS AND IMMOBILITY
 Falls With Injury Change Package 2015 UPDATE PREVENTING HARM FROM INJURIES DUE TO FALLS AND IMMOBILITY ACKNOWLEDGEMENTS We would like to recognize the contributions of the American Hospital Association
Falls With Injury Change Package 2015 UPDATE PREVENTING HARM FROM INJURIES DUE TO FALLS AND IMMOBILITY ACKNOWLEDGEMENTS We would like to recognize the contributions of the American Hospital Association
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017
 HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
From Big Data to Big Knowledge Optimizing Medication Management
 From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
Welcome to E4 and F4
 Welcome to E4 and F4 Surgery and Surgical Oncology Juravinski Hospital We are surgical units that care for people who may need surgery and are recovering from surgery. The staff on E4 and F4 welcome you
Welcome to E4 and F4 Surgery and Surgical Oncology Juravinski Hospital We are surgical units that care for people who may need surgery and are recovering from surgery. The staff on E4 and F4 welcome you
Resident Rights in Nursing Facilities
 Your Guide to Resident Rights in Nursing Facilities 1-800-499-0229 1 Table of Contents The Ombudsman Advocate...3 You Take Your Rights with You...4 Federal Regulations Protect You...5 Medical Assessment
Your Guide to Resident Rights in Nursing Facilities 1-800-499-0229 1 Table of Contents The Ombudsman Advocate...3 You Take Your Rights with You...4 Federal Regulations Protect You...5 Medical Assessment
UCLA Newborn Screening Symposium 2018
 UCLA Newborn Screening Symposium 2018 Facility Feedback HEPP Reports and Graphs How to Best Utilize These Reports for Optimal Outcomes Timeliness in Specimen Collection and Transit TRF Completion Early/Missing
UCLA Newborn Screening Symposium 2018 Facility Feedback HEPP Reports and Graphs How to Best Utilize These Reports for Optimal Outcomes Timeliness in Specimen Collection and Transit TRF Completion Early/Missing
Case Study Comprehensive Analysis: Elopement from a Long- Term Care Home
 CANADIAN INCIDENT ANALYSIS FRAMEWORK Case Study Comprehensive Analysis: Elopement from a Long- Term Care Home 2012 Canadian Patient Safety Institute All rights reserved. Permission is hereby granted to
CANADIAN INCIDENT ANALYSIS FRAMEWORK Case Study Comprehensive Analysis: Elopement from a Long- Term Care Home 2012 Canadian Patient Safety Institute All rights reserved. Permission is hereby granted to
Penticton & District Community Resources Society. Child Care & Support Services. Medication Control and Monitoring Handbook
 Penticton & District Community Resources Society Child Care & Support Services Medication Control and Monitoring Handbook Revised Mar 2012 Table of Contents Table of Contents MEDICATION CONTROL AND MONITORING...
Penticton & District Community Resources Society Child Care & Support Services Medication Control and Monitoring Handbook Revised Mar 2012 Table of Contents Table of Contents MEDICATION CONTROL AND MONITORING...
North Carolina Division of Medical Assistance
 North Carolina Division of Medical Assistance Medicaid Clinical Policy and Programs Update on Medicaid In-Home Personal Care Services (PCS) Presented Larry Nason, Ed.D. Chief, Medicaid Facility by: and
North Carolina Division of Medical Assistance Medicaid Clinical Policy and Programs Update on Medicaid In-Home Personal Care Services (PCS) Presented Larry Nason, Ed.D. Chief, Medicaid Facility by: and
Welcome Providers. Thursday, November 11, Page 1
 Welcome Providers Thursday, November 11, 2010 Page 1 What is a 3 Share Plan? The 3 Share Plan is an affordable health plan for small businesses. Cost is shared among employers, their employees, and one
Welcome Providers Thursday, November 11, 2010 Page 1 What is a 3 Share Plan? The 3 Share Plan is an affordable health plan for small businesses. Cost is shared among employers, their employees, and one
Simulation Design Template. Date: May 7, 2008 File Name: Group 4
 Simulation Design Template Date: May 7, 2008 File Name: Group 4 Discipline: Nursing, medicine, radiology, EMT, possible consultant (specialist ie neurosurgeon via conference call), possible social work/pastoral
Simulation Design Template Date: May 7, 2008 File Name: Group 4 Discipline: Nursing, medicine, radiology, EMT, possible consultant (specialist ie neurosurgeon via conference call), possible social work/pastoral
The CAUTI Can-Can. Hennepin County Medical Center August Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion
 Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
OhioHealth s Mission: To Improve the Health of Those We Serve
 Enhancing SAFE SKIN Through Computer Utilization OhioHealth s Mission: To Improve the Health of Those We Serve 2 1 3 Grant Medical Center 21,000 patient discharges/year Average daily census of 260 Magnet
Enhancing SAFE SKIN Through Computer Utilization OhioHealth s Mission: To Improve the Health of Those We Serve 2 1 3 Grant Medical Center 21,000 patient discharges/year Average daily census of 260 Magnet
After the Hospital Where Do I Go From Here?
 After the Hospital Where Do I Go From Here? Prepared by: Abigail Dignadice, RN, BSN Geriatric-Psychiatric Unit, Palomar Medical Center Poway Edited and approved by: Diane Loehner, Licensed Clinical Social
After the Hospital Where Do I Go From Here? Prepared by: Abigail Dignadice, RN, BSN Geriatric-Psychiatric Unit, Palomar Medical Center Poway Edited and approved by: Diane Loehner, Licensed Clinical Social
Change Management at Orbost Regional Health
 Change Management at Orbost Regional Health Our change management journey 1 Medication Change System Meds at Beds 2 The slightly exaggerated before process 3 Project Goals The purpose of the Meds at Beds
Change Management at Orbost Regional Health Our change management journey 1 Medication Change System Meds at Beds 2 The slightly exaggerated before process 3 Project Goals The purpose of the Meds at Beds
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Interprofessional Model of Care Redesign
 Interprofessional Model of Care Redesign Betty Anne Whelan, RN, MSN Project Manager Interprofessional Model of Care redesign Model of Care Review 2013 Summary of Findings( Completed by Professional Practice)
Interprofessional Model of Care Redesign Betty Anne Whelan, RN, MSN Project Manager Interprofessional Model of Care redesign Model of Care Review 2013 Summary of Findings( Completed by Professional Practice)
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Decreasing Nosocomial C. diff
 Decreasing Nosocomial C. diff Our journey to decreasing nosocomial C. diff Jennifer Conti BSN, RN, CIC Nicole Rabic MSN, RN, CIC 4.21.2016 Nosocomial C. diff Use of the CDC standardized definition Review
Decreasing Nosocomial C. diff Our journey to decreasing nosocomial C. diff Jennifer Conti BSN, RN, CIC Nicole Rabic MSN, RN, CIC 4.21.2016 Nosocomial C. diff Use of the CDC standardized definition Review
Cohort 20 Team 7. Improving Care Of The Pediatric Patient With A Tracheostomy
 Cohort 20 Team 7 Improving Care Of The Pediatric Patient With A Tracheostomy Team Members & Participants Marisa Earley, MD / Medical Resource Carlos Montano / Respiratory Resource Nelia Acuna / Nursing
Cohort 20 Team 7 Improving Care Of The Pediatric Patient With A Tracheostomy Team Members & Participants Marisa Earley, MD / Medical Resource Carlos Montano / Respiratory Resource Nelia Acuna / Nursing
Readmission Reduction: Patient Interviews. KHA Quality Conference March, 2018
 Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
ADMISSION CARE PLAN. Orient PRN to person, place, & time
 ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
ABC s of PES. Greg Miller, MD MBA CMO Unity Center for Behavioral Health
 ABC s of PES Greg Miller, MD MBA CMO Unity Center for Behavioral Health Content Outline Overview of Unity Services Emergency Psychiatry: Historical Perspective Emergency Psychiatry: Current Service Delivery
ABC s of PES Greg Miller, MD MBA CMO Unity Center for Behavioral Health Content Outline Overview of Unity Services Emergency Psychiatry: Historical Perspective Emergency Psychiatry: Current Service Delivery
PATIENT AGGRESSION & VIOLENCE BEST PRACTICES NCQC PSO Safe Table July 2015
 PATIENT AGGRESSION & VIOLENCE BEST PRACTICES NCQC PSO Safe Table July 2015 Minimize the impact of patient aggression and violence by focusing on various phases of the care process. RECOGNITION Understand
PATIENT AGGRESSION & VIOLENCE BEST PRACTICES NCQC PSO Safe Table July 2015 Minimize the impact of patient aggression and violence by focusing on various phases of the care process. RECOGNITION Understand
Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach
 Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach July 18, 2016 AAMI Foundation Vision: To drive the safe
Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach July 18, 2016 AAMI Foundation Vision: To drive the safe
Patient Safety (PS) 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.
 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.") Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
Care Coordination in the New CoP s. Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017
 Care Coordination in the New CoP s Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting,
Care Coordination in the New CoP s Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting,
Pedi-CSI: Pediatric Clinical Safety Investigation Through Virtual Patient Safety Rounds
 Pedi-CSI: Pediatric Clinical Safety Investigation Through Virtual Patient Safety Rounds Training Manual Boston Children s Hospital Medicine Patient Services and Boston College William F. Connell School
Pedi-CSI: Pediatric Clinical Safety Investigation Through Virtual Patient Safety Rounds Training Manual Boston Children s Hospital Medicine Patient Services and Boston College William F. Connell School
Transforming Care Delivery: Redesigning Case Management and Primary Care Roles in Population Health Management
 Transforming Care Delivery: Redesigning Case Management and Primary Care Roles in Population Health Management PCPCC June 26, 2014 Karen Jones MD FACP VP, Chief Medical Officer, WMG Laurie Brown BSN, MBA
Transforming Care Delivery: Redesigning Case Management and Primary Care Roles in Population Health Management PCPCC June 26, 2014 Karen Jones MD FACP VP, Chief Medical Officer, WMG Laurie Brown BSN, MBA
Overcoming Common Barriers to Successful Safe Patient Handling Programs
 Overcoming Common Barriers to Successful Safe Patient Handling Programs Strategies for Gaining Support with Leadership at All Levels Ed Hall, Chief Operating Officer, The Risk Authority Strategies for
Overcoming Common Barriers to Successful Safe Patient Handling Programs Strategies for Gaining Support with Leadership at All Levels Ed Hall, Chief Operating Officer, The Risk Authority Strategies for
FUNCTIONAL PROGRAM for General Hospital
 FUNCTIONAL PROGRAM for General Hospital 1 General Considerations 1.1 Applicability As discussed with WY Dept of Health, it is anticipated that this facility will be surveyed and licensed as a General Hospital.
FUNCTIONAL PROGRAM for General Hospital 1 General Considerations 1.1 Applicability As discussed with WY Dept of Health, it is anticipated that this facility will be surveyed and licensed as a General Hospital.
MDS Essentials. MDS Essentials: Content. Faculty Disclosures 5/22/2017. Educational Activity Completion
 MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
Fall Protection and Prevention Program. Wendy Bauer, MSN, NHA, NEA-BC St. Elizabeth Healthcare
 Fall Protection and Prevention Program Wendy Bauer, MSN, NHA, NEA-BC St. Elizabeth Healthcare Objectives & About Us St. Elizabeth is a multi-facility Health Care System in Northern Kentucky hospitals,
Fall Protection and Prevention Program Wendy Bauer, MSN, NHA, NEA-BC St. Elizabeth Healthcare Objectives & About Us St. Elizabeth is a multi-facility Health Care System in Northern Kentucky hospitals,
Auchinlea Care Home Care Home Service
 Auchinlea Care Home Care Home Service 10-12 Scott Street Largs KA30 9NU Telephone: 01475 673500 Type of inspection: Unannounced Inspection completed on: 20 September 2017 Service provided by: Bertinaley
Auchinlea Care Home Care Home Service 10-12 Scott Street Largs KA30 9NU Telephone: 01475 673500 Type of inspection: Unannounced Inspection completed on: 20 September 2017 Service provided by: Bertinaley
The Effects of an Electronic Hourly Rounding Tool on Nurses Steps
 The Effects of an Electronic Hourly Rounding Tool on Nurses Steps Dr. Aimee Burch, DNP, APRN-CNS CHI Health St. Francis Katie Hottovy, Co-founder and Director of Client Services, Nobl Disclosures to Participants
The Effects of an Electronic Hourly Rounding Tool on Nurses Steps Dr. Aimee Burch, DNP, APRN-CNS CHI Health St. Francis Katie Hottovy, Co-founder and Director of Client Services, Nobl Disclosures to Participants
NCQC PSO Safe Tables Fall Prevention July 2016
 NCQC PSO Safe Tables Fall Prevention July 2016 Background Role of a PSO Share Learn Improve Protection under the and Quality Improvement Act of 2005 It s like Vegas Safe Table Objectives Support our commitment
NCQC PSO Safe Tables Fall Prevention July 2016 Background Role of a PSO Share Learn Improve Protection under the and Quality Improvement Act of 2005 It s like Vegas Safe Table Objectives Support our commitment
PART I - ALL APPLICANTS MUST COMPLETE
 APPLICATION FOR NURSING HOME, ASSISTED LIVING AND HEALTHCARE FACILITIES PROFESSIONAL AND GENERAL LIABILITY INSURANCE (Claims Made Basis) APPLICANT S INSTRUCTIONS: 1. Answer all questions. If the answer
APPLICATION FOR NURSING HOME, ASSISTED LIVING AND HEALTHCARE FACILITIES PROFESSIONAL AND GENERAL LIABILITY INSURANCE (Claims Made Basis) APPLICANT S INSTRUCTIONS: 1. Answer all questions. If the answer
Improve the Efficiency and Service of the Emergency Room at North Side Hospital
 Improve the Efficiency and Service of the Emergency Room at North Side Hospital John Melton, VP and CEO Washington County Operations meltonjw@msha.com Kerry Vermillion, CFO Washington County Operations
Improve the Efficiency and Service of the Emergency Room at North Side Hospital John Melton, VP and CEO Washington County Operations meltonjw@msha.com Kerry Vermillion, CFO Washington County Operations
University of Colorado Hospital Policy and Procedure Fall Prevention
 University of Colorado Hospital Policy and Procedure Fall Prevention Related Policies and Procedures: Patient Occurrence Reporting Process Restraint Use: Acute Medical Surgical (Non-Violent, Non-Self Destructive
University of Colorado Hospital Policy and Procedure Fall Prevention Related Policies and Procedures: Patient Occurrence Reporting Process Restraint Use: Acute Medical Surgical (Non-Violent, Non-Self Destructive