Avoiding 30-day Readmissions of Acute MI Patients Utilizing Cardiac Rehabilitation
|
|
|
- Myrtle Carr
- 6 years ago
- Views:
Transcription

1 The University of San Francisco USF Scholarship: a digital Gleeson Library Geschke Center Doctor of Nursing Practice (DNP) Projects Theses, Dissertations, Capstones and Projects Fall Avoiding 30-day Readmissions of Acute MI Patients Utilizing Cardiac Rehabilitation Patricia T. Forsberg University of San Francisco, rpforsberg@sbcglobal.net Follow this and additional works at: Part of the Health and Medical Administration Commons, Nursing Administration Commons, and the Other Rehabilitation and Therapy Commons Recommended Citation Forsberg, Patricia T., "Avoiding 30-day Readmissions of Acute MI Patients Utilizing Cardiac Rehabilitation" (2014). Doctor of Nursing Practice (DNP) Projects This Project is brought to you for free and open access by the Theses, Dissertations, Capstones and Projects at USF Scholarship: a digital Gleeson Library Geschke Center. It has been accepted for inclusion in Doctor of Nursing Practice (DNP) Projects by an authorized administrator of USF Scholarship: a digital Gleeson Library Geschke Center. For more information, please contact repository@usfca.edu.
2 Running head: AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 1 Avoiding 30-day Readmissions of Acute MI Patients Utilizing Cardiac Rehabilitation Patricia Forsberg University of San Francisco N 789 DNP Project
3 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 2 Table of Contents Section I Title and Abstract Title 1 Abstract 4 Section II Introduction Background knowledge 5 Local problem 6 Intended improvement/purpose of Change 8 Review of the evidence 9 Conceptual/Theoretical framework 11 Section III Methods Ethical issues 12 Setting 13 Planning the intervention 15 Implementation of the project 22 Planning the study of the intervention 22 Methods of evaluation 25 Analysis 26 Section IV Results Program evaluation/outcomes 27 Section V Discussion Summary 29 Relation to other evidence 29 Barriers to implementation/limitations 31 Interpretation 32 Conclusions 32 Section VI Other Information Funding 33 Section VII References 34
4 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 3 Section VIII Appendices Appendix A Medicare Data 38 Appendix B Discharge Phone Call Breakdown 39 Appendix C Discharge Phone Call Issues 40 Appendix D Evidence Table 41 Appendix E AACVPR Core Competencies 46 Appendix F Hospital Based CR Questionnaire 53 Appendix G Comparison of Questionnaire Feedback 55 Appendix H Number of Hospital Discharges 56 Appendix I In House CR Experts 57 Appendix J ROI Budget Projections 58 Appendix K GANTT Chart 60 Appendix L GAP Analysis 61 Appendix M SWOT Analysis 62 Appendix N Educational Power Point 63 Appendix O Feedback from Educational Power Point 71
5 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 4 Abstract A significant number of Acute Myocardial Infarction (AMI) patients were readmitted to an urban San Francisco Medical Center within 5-7 days post discharge this year. Two of the main identified causes were symptom management issues and medication instructions, both of which are part of the discharge instructions. It s not surprising that 80% of all discharge teaching is forgotten by patients by the time they hit the parking lot. With the recommended timeframe for post discharge follow up appointments at 48 to 72 hours post discharge and as those appointments are not typically available within the recommended timeframe, patients are more likely to be readmitted unless an alternative for post discharge follow up can be created. The intent of this project is to propose the implementation of a hospital based Cardiac Rehabilitation (CR) program that allows AMI patients to participate as early as hours post discharge. This first part, or intake to the CR program would reinforce discharge teaching inclusive of medication reconciliation, symptom management, and all other components taught at discharge. The evidence to be duplicated is that enrollment in a certified cardiac rehab program as early as 48 hours post discharge can prevent readmissions by enhancing the patient/family s retention and understanding of discharge instructions that include symptom management and medication reconciliation, resulting in fewer hospital readmissions.
6 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 5 Avoiding 30-day Readmissions of Acute MI Patients Utilizing Cardiac Rehabilitation Section II Introduction Background The Medical Center (MC) is a 600 bed academic medical center recognized throughout the world for innovative patient care, advanced technology and pioneering research. It is one of the nation's top 10 hospitals, according to the 2014 annual survey by U.S. News and World Report with about 38,000 admissions per year. In calendar year 2013, there were a total of 67 Medicare Fee for Service (FFS) AMI discharges with a 30-day readmission rate of 25.4%. Of those readmissions, 52% of those patients were readmitted within 1-7 days after discharge and another 29.4% were readmitted 8-14 days post discharge for a total of 81.4% of patients readmitted within 14 days of discharge (Appendix A). MC has an active post discharge call back program. From April 2014 to July 2014, 479 discharged cardiology service patients were called by the auto-calling program Cipher. Of those patients, 386 (81%) were reached and of those 386 patients, 140 (36%) requested a callback. Of those requesting a call back, the majority of their concerns were of a clinical nature (66%) and the rest were satisfaction issues (Appendix B). Of the clinical issues, medication questions and concerns about symptoms were the top two reasons patient requested a call back (Appendix C). The literature cites that there are three essential keys to reducing hospital readmissions; medication reconciliation, discharge teaching that begins at admission, and adequate discharge follow up. Part of that effective discharge follow up includes discharge phone calls and ensuring that the patients are seen either by their primary care provider (PCP) or newly referred provider as soon as possible after discharge. How soon after discharge that first outpatient visit occurs is also a concern. In the Improvement Map, Improving Transitions to Reduce Readmissions, the
7 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 6 Institute for Healthcare Improvement (IHI) recommends that high-risk patients are seen within 48 hours of discharge and moderate risk patients are seen within five days (2013). These appointments should be scheduled prior to discharge, and in the high-risk patients, with a faceto-face interaction. This post discharge visit is essential to the care continuum and should include a review of medications, assuring the patient is on the correct treatment trajectory, and offering additional education and support to the patient and family. It is through these outpatient encounters that true healthcare can take place by referring patients to programs that can promote wellness and avoiding stressful hospitalizations. Patients who were prescribed enrollment in a CR program after discharge are referred to programs at surrounding hospitals; St. Mary s Hospital, California Pacific Medical Center, and Seton Hospital as the MC discontinued their in house program in This decision was made after the merger between the MC and another large academic medical center came to an end in 1999 as a cost cutting initiative in an attempt to regain some of the money that was lost as a result of the split. Local Problem With a significant amount of post AMI patients being referred to outside and even competing facilities for care, oversight and potential control of these patients could be lost to these facilities with a resulting loss in continuity of care and potential revenue loss. Readmissions of Medicare FFS AMI patients were high and contributed to the MC having to pay a fine (over $125,000) last year for a higher than average readmission rate of these patients. The literature suggests that early post discharge follow up appointments within a week of discharge have been found to reduce emergency department visits and hospital readmissions (Andrews, 2011). Hospital readmissions can be attributed to three major issues. Readmitting for
8 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 7 complications of a procedure during the initial hospitalization, readmission due to poorly managed processes in transitioning the patient from the hospital, and readmission due to the recurrence of a chronic condition that is not well managed outside the hospital (Jones & Ringquist, 2013). The MC has been challenged to meet the goal of early post discharge provider appointments as the cardiology clinic has been so impacted that patients can wait up to 30 days to get a follow up appointment after a cardiac event such as an AMI. Initially the focus was on streamlining and providing better access to post discharge appointments, but it became clear that the main obstacle around access was that there was a severe shortage of providers in the clinic. There is a Nurse Practitioner (NP) in the clinic but her focus is supporting the work of the existing provider staff and sees few patients independently. The providers have competing priorities between hospital care of patients, research, and clinical time, that the number of appointments could not be increased. All University of California (UC) medical centers have united in their approach to reduce inpatient readmissions and have started the initiative by targeting patients with an index admission of sepsis. Transitions leaders from all five campuses met in September 2014 to complete a best practice survey and identified three tactics to be implemented across all 5 UC campuses. Tactic #1 is the development of a standardized UC readmission assessment tool and applies that questionnaire to evaluate 20 readmissions per hospital with an index admission of sepsis from those questionnaires. Trends and opportunities will be summarized. Tactic #2 includes an alert or readmissions flag in the electronic medical record at all UC hospitals that would signal Emergency Department (ED) physicians of the potential readmission and allow for early and real time intervention and stronger consideration of admission. Tactic #3 is the
9 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 8 creation of a new standard for providers that all discharge summaries would be completed within 48 hours of the patient s discharge ensuring that information is shared in a timelier manner as a means to improve the communication between providers. Intended Improvement The overall AIM of this project is, can the MC financially implement and sustain a cardiac rehabilitation program in the next fiscal year so that AMI patients can enroll soon after discharge and potentially prevent their 30-day readmissions? As a way to ensure a quality program at MC, collaborative activities with local cardiac rehabilitation (CR) programs were performed, along with an evidence based educational presentation to ensure local programs are up to date on the benefits of early admission to CR to decrease readmissions. The presentation would also highlight some of the area programs best practices that would also be used in the development of the CR program at the MC. A group of providers, cardiologists, case managers, transitions managers, hospital and nursing leaders has been established to review the readmission rates for primarily Medicare FFS AMI patients and heart failure (HF) patients. This Cardiology Service Transitions of Care and Readmission Task Force has come to consensus that post discharge follow up is necessary to prevent readmissions of these patients. Currently the majority of AMI patients are discharge to home or to home with home care services. This group of patients has a higher 30-day readmission rate than those discharged to skilled nursing facility (SNF) or to hospice. A significant number of these patients (81.4%) were also readmitted between 1 to 14 days post discharge (Appendix A). Taking into consideration the breakdown in discharge phone callback issues, the group identified that a more aggressive post discharge follow up and reinforcement of
10 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 9 discharge teaching including medication reconciliation and symptom management needed to occur. Review of the Evidence Searches using key words, cardiac rehabilitation, AMI, cardiovascular disease, and readmissions in CINAHL, PubMed, Joanna Briggs, and Cochrane produced only one experimental control study comparing post AMI patients participating in a CR program post discharge to those that didn t participate in such a program. That study found that the treatment group (those that participated in a CR program post discharge) did indeed have a lower incidence of 30-day readmission to the hospital as well as a shorter length of stay during that readmission (Meshgin, 2008). All other case reviews and practice guideline publications suggest that better discharge instruction methods and early post discharge follow up appointments can reduce avoidable hospital readmissions post AMI. Of the evidence reviewed related to better retention of discharge instructions, methods, and reduction of readmissions, 50% were systematic reviews and clinical practice guidelines with 35% being experimental studies, meta analysis and non experimental studies. The remaining search results were case studies and literature reviews. The findings can be placed into four categories: reasons for readmission, identifying hospital environmental issues preventing the retention of discharge education, successful implementation strategies that resulted in decreased readmissions, and the benefits of a CR program. One of the highest evidence level and quality study was conducted over a year and involved over 38,000 AMI discharges in 1088 hospitals. There was a 20.3% readmission rate overall and the study identified the need for an improvement in palliative care referrals, having a post discharge follow appointment within 14 days of discharge and better medication reconciliation as a means to decrease hospital readmissions (Brown, et al. 2014). Another non-
11 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 10 experimental study of discharged vascular surgery patients revealed that only 65% of discharged patients were able to answer 4 questions correctly about their discharge instructions only 3 days after they were discharged (Lee, et al. 2005). A decreased length of stay (LOS) was not associated with higher readmission rates, whereas an increased LOS was associated with higher readmission rates (Saczynsk, et al. 2010) that lead into the hospital environment itself being a contributing factor to readmissions. A condition called post hospital syndrome can occur as a result of the stress of hospitalization and can contribute to the lack of information retention (Detsky, 2014). During the hospitalization many stressors and influence the patient. They include lack of sleep, presence of pain, deconditioning, anxiety about a new diagnosis and how the patient will cope with this new illness or condition when home. Although short-term stress can actually sharpen our mind, long term or chronic stress limits our ability to focus, concentrate, and remember facts (Law, 2012). Some facilities with lower readmission rates have implemented successful strategies. Tallahassee Medical Center implemented a discharge clinic for high risk for readmission patients in which patients were seen 1-2 days post discharge for clarification of discharge instructions and medication reconciliation. As a result, their ED visits and hospital readmissions decreased by 61% (Andrews, 2011). Best practices were identified by 5 of the top performers in the University Health Care (UHC) academic medical centers. They included interdisciplinary team interactions during hospitalization, discharge tools such as teach back, during education, and a 7 day post discharge plan and follow up with their primary care physician (UHC Field Brief, 2011).
12 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 11 The highest evidence level and quality experimental studies involved cardiac and cardiac surgical patients randomized to enroll or not to enroll in CR programs. Out of a total of 308 cardiac patients, 198 were in the control group, and 110 patients were in the treatment group and participated in a CR program while the control group did not. Six percent of the patients in the CR program were readmitted while 19% in the control group were readmitted within the same 1 year period (Meshgin, 2008). A similar result was seen in 147 post CABG patients where 32% of the 98 patients in the control group who did not participate in a CR program were readmitted while only 14% of the 49 patients in the treatment group who enrolled in a CR program were readmitted (Perk, et al. 1990). A review of the strength of the literature using the Johns Hopkins Nursing Evidenced-based Practice tool can be found in Appendix D. Conceptual Framework For the purpose of the proposal to implement the CR program at the MC, in addition to the community CR program survey and educational power point, Aristotle s modes of persuasion will be utilized. The three modes of persuasion include ethos, pathos, and logos. Ethos deals with the character of the presenter to appear credible with the following characteristics; competence, good intention, and empathy. Competence refers to the background knowledge, research on the issue, and accuracy of information presented. Good intention is the concept that the proposal or information being presented is for the betterment of a population and would benefit a group without causing harm to another. Empathy is the ability to communicate the information in a sensitive manner and have a genuine interest and concern for the content being presented. When conducting the survey questionnaires, and introduction started the interview with my background, formal education, and interest in their CR program.
13 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 12 Pathos refers to the emotional influence of the presenter to the audience. The goal is to persuade the audience and it is therefore necessary to put the audience in the appropriate emotional state. The intent of the questionnaire was to learn about the individual programs and give them an opportunity to share some of their best practices while at the same time, remark on some of their achievements such as readmission and survival rates from the hospital compare website. Logos is the appeal towards logical reason. In the case of the community CR program survey, the intent of the survey started the conversation with the participants. Later, the evidence was shared with the different CR programs that participation in a CR program can lead to fewer hospital readmissions. All the CR programs were not consistently aware of this, but it made sense to them. One of the participants even remarked that perhaps the patients that are in a CR program are more self managing and would more likely call their physician before going to the ED for care. Logos would also be utilized when presenting this proposal to the MC leadership team. It is in this manner that the logical reasoning that implementing a CR program would not only produce revenue to the MC, but also save the hospital money in terms of CMS fines for readmissions and loss of reimbursement for those readmissions. Section III Methods Ethical Issues Although the proposal to implement a CR program at the MC itself does not impose any ethical implications, the question needs to be asked, if we have the capacity and the service is reimbursable for a number of discharge diagnoses, why would we not implement such a program as a benefit to our patients and the general health of the population that we serve? The answer is
14 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 13 yes if the program can be implemented without additional cost to the facility, or if there is a cost, then it should be less than the readmission fines paid by the hospital. Setting In FY14 at this 600 bed academic MC, there were a total of 84 patients discharged with the diagnosis of AMI. The overall payor mix was approximately 45% Medicare, 21% Medi-Cal, 33% commercial, and 1% self pay. If CR is ordered for these patients they are referred to programs at either California Pacific Medical Center (CPMC) or St. Mary s hospital, both nearby medical centers in the city of San Francisco. Much work is being done in the Medicare Fee for Service (FFS) and Transitions of Care programs at the MC for AMI, CHF, Chronic Obstructive Pulmonary Disease (COPD), Pneumonia, and Total Knee and Total Hip Arthroplasty as these diagnoses, if readmitted 30 days post discharge will result in fines to the hospital if the total percentage is higher than Center for Medicare and Medicaid Services (CMS) allows. A Cardiology Service Transitions of Care and Readmissions Committee was formed to analyze readmission data, review the discharge phone call results, and establish best practices for the MC. This committee is made of up Cardiologists, Transitions in Care leadership, Case Managers, and hospital leadership. Goals for the group include; understanding how cardiology patients transition at the MC, promote what is working well, and identifying areas for improvement, while involving key stakeholders in the improvement process. This work is in response to a University of California Medical Center (UC) quality goal of a 1.5% reduction in all readmissions involving all five of its medical facilities; the MC, UC Davis, UC San Diego, UC Los Angeles, and UC Irvine. Current strategies include; implementing a robust readmission tool to assess why patients are readmitted,
15 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 14 designing a readmission notification flag in the electronic medical record, and ensuring that all discharge summary notes are completed and in the chart within 48 hours of the patient discharge. Early efforts were focused on increasing the availability and access to post discharge provider clinic visits. The outpatient Cardiology Clinic at Mission Bay is a full service outpatient clinic with noninvasive diagnostics, meeting rooms, and 12 exam rooms. A Master s prepared Nurse Manager has administrative oversight of staff that includes a Nurse Practitioner, Medical Assistants, and Receptionist. The Cardiology Attending physicians see patients and their time is split between clinic hours, classroom lectures, rounding with residents and their ongoing research activities. These competing priorities make it impossible to increase the number of discharge appointments currently and no opportunity to entertain any additional full time equivalents (FTEs) to be hired into the clinic during this fiscal year. Examining the possibility of a CR program was an idea discussed at one of the Cardiology Service Transitions of Care and Readmission Committees and was embraced by the medical staff committee members. The committee also identified the challenge of appointing a Medical Director due to the same time constraints mentioned above. The proposed CR program was conceptually tied to the current outpatient pulmonary rehabilitation (PR) program located at the Mount Zion campus. The PR program is currently being funded and costs are being offset by a grant with an active Medical Director. It was clear that a physician champion would have be identified in addition to the financial business plan and space allocation proposal needed to convince hospital administration of the cost benefit of such a program at the MC. As mentioned earlier, the MC at one time did have a CR program that was not creating revenue for the medical center. It was discontinued due to fiscal constraints resulting from the Stanford split in early The objective of this project is to establish a clear and convincing business proposal to re
16 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 15 create a CR program that would be revenue producing or at least cost neutral benefitting the patient population and reducing 30-day hospital readmissions of the AMI patients. A lot of focus has been directed to the Ciphor centralized automated discharge phone call system. The current process includes discharged patients receiving an automated phone call giving them prompts if they desire a return call and follow up information. Then one of the centralized discharge phone call RNs returns the patient s call and answers the patients question while concurrently viewing the patient s medical record in APeX, the MC s electronic health record (EHR) Data from the system can be extracted to determine the reason the patient requested a call back, and the response of the call back RNs. While these interventions have answered patients concerns timely, the total 30-day readmission rate for Medicare FFS AMI patients continues to not be improving, from 12.3% in FY12, 15.8% in FY13, to 14.8% in FY14 to date. Of those patients readmitted in FY14 to date, 39% were readmitted in 1-7 days post discharge and 20.3% between 8-14 days post discharge supporting the need for early post discharge appointments and/or outpatient referrals. By offering a hospital based CR program, patients can be seen as early as 3-5 days post discharge for intake assessment that can include medication reconciliation and review of the discharge instructions. Planning the Intervention Lack of access to outpatient care can lead to higher readmissions (UHC, 2013). Kaiser Health News, August 2, 2013 reported that hospitals with the highest share of low-income patients had the highest readmission rates while hospitals with the lowest share of low-income patients had some of the lowest readmission rates. The federal Agency for Healthcare Research and Quality (AHRQ, 2013) noted that adverse events occur in approximately one in five adult medical patients within three weeks of discharge and that nearly 20% of Medicare patients will
17 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 16 be readmitted within 30 days of being discharged from acute care. The Patient Protection and Affordable Care Act (PPACA) contains regulation that focuses on decreasing preventable readmissions by improving care transitions. Through this legislation, hospitals have even greater incentives to improve transitional care at hospital discharge. Preventable readmissions can be placed in four categories and are due to; the provision of quality care in the initial hospitalization, adequate discharge planning, adequate post-discharge follow-up, or improved coordination between inpatient and outpatient health care teams (Goldfield et al., 2008). According to patients and their caregivers, four similar factors were expressed as the most essential contributors to post hospitalization follow up (Taverner, 2013). These four common factors are associated with readmissions within 30 days and include; medication self-management, having a patient centered medical record, getting primary care and specialist follow up, and knowledge of red flags or warning symptoms of a worsening condition. In his white paper, Taverner also cited a 2007 Journal of the American Medical Association study that found that direct communication between hospital physicians and primary doctors occurred in less than 20% of cases. Having pertinent medical record information from the hospitalization is also problematic. The discharge summary was available to the primary care physician at the first post hospitalization visit only 12%-34% of the time (Kripalani et al., 2007). By implementing a hospital based CR program many of the main causes for readmission could be addressed during the intake appointment. Patients could be seen in a timely manner, there would be efficient communication between the program and the patient s provider through the common EMR, and medication reconciliation, and symptom management teaching would occur.
18 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 17 In order to pursue the proposal for a CR program, eligible participants, reimbursement, capitol equipment needs and staffing needs must be assessed. In terms of staffing, the number and type of staff needs to be considered as well as their competencies as related to CR. The American Association of Cardiovascular and Pulmonary Rehabilitation, (AACVPR) defines specific core competencies for staff in the domains of patient assessment, nutritional counseling, weight management, blood pressure management, lipid management, diabetes, management, tobacco cessation, psychological management, physical activity counseling, and exercise training evaluation (Appendix E). In addition to these competencies, the CR staff must also demonstrate excellent communication skills and a commitment to improving the health and well being of the patients they serve. In addition to staffing, equipment and monitoring capabilities costs must be established. As Phase II consists of monitored exercise, there should be a variety of exercise equipment available. Typically equipment consists of treadmills, stationary bicycles, elliptical machine(s), adequate numbers of telemetry transmitters to accommodate the projected size of the class, and emergency equipment such as a crash cart and portable defibrillator. AACVPR regulations state that there must be at least one CR staff member present for every 5 monitored patients. Location is also an important consideration. With the opening of the new hospital in Mission Bay in February 2015, there may be opportunity for additional space in the next fiscal year once all the patient units are relocated. The emphasis of this intervention, a CR proposal, will focus on a business plan and budget to present to hospital administration for approval and location will be determined afterward. Eligible patients also must be considered. Up until recently, CMS only reimbursed patients with a discharge diagnosis of AMI, CABG, or other cardiac surgery, stents, and angina.
19 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 18 HF was recently added to the list of reimbursable participants in a CR program by CMS. As CR enrollment historically remains low, 20% to 30% in most eligible populations as mentioned, accurate enrollment projections are needed to best anticipate capacity requirements for the new program. The sample budget takes both 20% and 30% enrollment figures into the equation for a budget projection (Appendix J). Understanding the duration of enrollment in a CR needs to be understood. CR typically consists of three phases. Phase I, in patient teaching that can be accomplished prior to discharge as an introduction to the program. Phase II, a monitored exercise program where 36 sessions are reimbursed both by Medicare and private insurance companies and is typically completed within 18 weeks. Phase III is unmonitored exercise and is reimbursed at a much lower rate. As a critical piece of understanding current practice and to ensure proper implementation of the program, community programs were assessed and compared to gain a better understanding. A questionnaire (Appendix F) was sent to CPMC, St. Mary s, Seton Hospital, and UC Davis, another University of California medical center. The purpose was two fold, to gain an understanding of what each program consisted of and identifying best practices that could or should be implemented in the newly proposed program for the MC. Based on the assessment an educational session was developed to ensure these sites were aware of the best evidence based practices to decrease hospital readmissions. Four of the five programs were certified by AACVPR and the manager at Seton, participated in the development of the national AACVPR guidelines and is an active member of the pulmonary rehabilitation professional organization. All programs offer Phase II monitored exercise and 4 of the 5 programs offer phase III, non-monitored exercise (Appendix G). Phase I, in hospital education, is less consistent among the programs based on the patient s shorter length of stay and availability of staff to teach
20 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 19 patients in house. This feedback provided the important information necessary to ensure that MC s program will be best in class. In these CR programs, much of the medication teaching and reconciliation is done during the intake portion of Phase II after the patient is discharged from the hospital. This can be a crucial time for the patient as they are typically discharged on several new medications, and those medications need to be reconciled with any previous medications the patients are taking. This is also a crucial time after discharge when the patient is no longer in the hospital with the continued support and may have questions that if go unanswered, may contribute to a potential readmission. Risk factor, diet and exercise education are taught in various methods while the patient is participating in their Phase II program. Most of the programs utilize a nutritionist to teach patients about diet and risk factor modification. In determining the cost benefit analysis of the program proposal, CMS reimbursement of CR and the eligible participants must be acknowledged. In their CMS Decision Memo for Cardiac Rehabilitations Programs (CAG-00089R) it was determined that the evidence is adequate to conclude that CR is reasonable and necessary following AMI, coronary bypass graft (CABG), stable angina pectoris, heart valve repair or replacement, percutaneous transluminal coronary angioplasty (PTCA) or coronary stenting, and heart or heart lung transplant. CMS recently, (July 18, 2014) published a National Coverage Determination (CAG-00437N) and instructions to include heart failure (HF) patients in CR programs with reimbursement. They categorize HF patients as stable HF with left ventricular ejection fraction of 35% or less and still have class II-IV symptoms despite being on optimal heart failure therapy for at least 6 weeks.
21 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 20 For purposes of the proposal the volume predictions will include potential patients from all of these discharge diagnoses. In FY14, there were 69 AMI discharges, 124 PTCA and stent discharges, 253 CABG, valve and other cardiac surgical discharges, and 22 heart transplants. Adding HF and Advanced HF to this population, the total discharges eligible for CR is 943 (Appendix H). Based on the volume of patients discharged with diagnoses that are eligible and covered by their insurance program for cardiac rehab, the projection is for a five-day/week program, Monday to Friday, operating eight hours/day. The center would run two 4-hour sessions daily, the first from 7:00 am to 11:00 am and the second from 12:00 pm to 4:00 pm. The program would include both Phase II and Phase III. Phase II consists of outpatient monitored exercise sessions that patients participate in twice a week for a total of 36 sessions usually over 18 weeks. This phase is reimbursed at a slightly higher rate than Phase III. Phase III consists of unmonitored sessions and considered the maintenance segment of CR. The staffing would include 1.5 FTE of RN and 1.0 FTE of an exercise physiologist. During monitored Phase II sessions, the ratio of RN to patients is 1:5, so there must be 2 RNs present during monitored exercise for 6 to 10 patients per session. Phase II sessions would be held in the morning session, 7:00 am to 11:00 am and Phase III sessions held in the afternoon session, 12:00 pm to 4:00 pm. Oversight and availability of a cardiologist is also a requirement for the program. This would be dependent on the location of the CR program and the participation of available attending physicians. Currently the MC has on staff two cardiologists with CR experience and expertise. (Appendix I). Start up costs also include treadmills, stationary bicycles, emergency cart with defibrillator, and potentially a telemetry monitoring system for up to 12 channels if the prior
22 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 21 equipment is not up to standard requirements. Return on Investment (ROI) was calculated utilizing a spreadsheet that includes the capitol equipment costs along with the labor and nonlabor costs of running the CR as described (Appendix J). The projected budget includes two different scenarios. The more conservative approach assumes a patient population and enrollment in CR to 189 patients/year. That is 20% of the total eligible patient population. It also assumes that the payor mix is 55% Medicare and 45% Commercial. Commercial reimbursement is a much higher figure at an average of $89.83 per monitored session as compared to Medicare s $15.89 per monitored session. Salary expenses included 1.5 FTE RN, 1.0 FTE Exercise Technician, Registered Dietician to teach nutrition classes weekly and a medical director fee of $12,500 which is typically 5% of an attending physician s annual salary. With equipment depreciation for the first year of a little over $7,000 and supply and marketing costs, the net revenue over expenses was over $66,000. With a larger patient enrollment, 30% of eligible patients equating to 283 patients, that net revenue after expenses goes to over $225,000. Capacity must also be considered given the ratios needed for monitored exercise in Phase II. In the first scenario, 189 patients are eligible for 36 sessions in Phase II for a total of 6790 sessions. Spread over a year, the average patient per session would be 12 requiring 3 staff members present during monitored exercise sessions assuming that there are 2 sessions daily, 5 times/week for 56 weeks in a year. If the patient enrollment expands to 30% eligible patients, or 283 patients, then the average patients per session would increase to 18 patients making it difficult to staff at the budgeted level and additional staffing would have to be considered. Compared to other programs, the first scenario is more likely and could easily be accommodated with positive net revenue over expenses.
23 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 22 Implementation of the Project Due to the institution s primary focus of the move to the Mission Bay campus February 1, 2015 and the timing of new program budgeting, the final proposal for implementing the CR program will be presented for implementation in FY16, after July 1, In addition to the financial proposal, a GANTT chart, (Appendix K) will be included to plan the actual timeline associated with equipment procurement, hiring and training of staff, any room modification, and state licensing requirements. As a means to implement best practices for our program, a survey was taken of local CR programs to assess their programs and their knowledge. (Appendix F) With the results of the survey, a power point presentation was developed (Appendix N) and provided to the sites as an educational outreach activity to assist them in understanding the need for timely follow up to potentially prevent patients from being readmitted to the hospital. Feedback from the educational session was reviewed and analyzed (Appendix O). Findings from the literature review, community CR program survey and the feedback from the education will be utilized in the development of the future CR program at the MC. Planning the Study of the Intervention Efforts to reduce 30-day readmission rate for AMI patients in addition to CHF, COPD and Pneumonia patients are embraced not only by the MC, but hospitals across the nation as CMS increases the penalties hospital will pay if the cumulative readmission rate is higher than the national average. The MC has been subjected to this fine of over $100,000 and the AMI readmission rate being the highest was responsible for the fine. A gap analysis was completed comparing the identified evidence based best practices and strategies to decrease hospital readmissions to current practices at the MC (Appendix L). Much work towards these practices
24 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 23 has occurred with the exception of an internal CR program or creation of a discharge clinic. Discharge teaching continues to be a challenge as bedside nurses who are tasked with this have been trained in the teach back method, but it s effectiveness are yet to be determined as the nurse is busy with his/her other 3 patients while anticipating the next admission. Patients are also in a hurry to get home, and can be anxious about self care after hospitalization as well as the discharge process itself. This stress can also alter the retention of the discharge information that is being taught to the patient and the longer the patient is hospitalized, the more deconditioned and potentially dependent on the services provided during hospitalization which increases anxiety about self care ability when discharged. The complexity of the discharge instructions can also lead to readmission if the instructions are not clear and concise. APeX, the MC s EHR provides a detailed seven to eight page discharge instruction document called the After Visit Summary (AVS). This document details the medication list that the patient is being discharged with, along with wound care, basic symptom management and instructions on how to activate the emergency response. The essential vulnerability after discharge occurs when the patient is home, and has to recall those instructions and reviews the AVS document for information on their new medication. It s no wonder that a significant number of discharge phone call return calls are about medication questions. Implementing a hospital based CR program consists of five essential functions of initiation, planning, execution, control, and closeout. A GANTT chart in increments of weeks outlines the processes within each function so that the progress of the implementation can be tracked and multiple processes can be initiated at one time if they are not interdependent upon each other (Appendix K).
25 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 24 The function of initiation includes the assessment, design, and proposal of the program with the final task being submission and approval of the project. The proposal consists of evidenced based rationale for the program in addition to a robust financial plan and budget that includes a cost benefit analysis. The planning function consists of identifying the state and facilities requirements, selecting and ordering capitol equipment, recruiting and training staff, and developing work flows and any order sets for the program. Execution involves creating the project kick off team, observing the actual work potentially at other cardiac rehab centers, and participating in day in the life dress rehearsals of actual or simulated patients to identify and correct work flow patterns. Control is about monitoring the clinical and financial measures of the CR program. Monthly or quarterly meetings to review patient outcomes such as readmission rates for participating discharge diagnoses and financial reports can be helpful. During the initiation phase, the development of the proposal was completed with the assistance of Jeff Kalin, the Director of Cardiology Operations at the MC. He provided a good historical perspective as well as reimbursement numbers for the different payors. Prior to the presentation to administration, this proposal will be vetted by the Cardiology physician leaders and the Cardiology Service Transitions of Care and Readmission Committee as they are very supportive of the initiative and can add valuable insight to the content. Once the proposal is approved and the formal planning function starts, a task force will be established consisting of a potential medical director, nursing leadership, and a content expert with CR knowledge or experience. This workgroup will continue to meet to review outcomes, both clinical and operational in the control phase. Clinical outcome measures will include readmission rates for those patient populations enrolled in the program and patient satisfaction. Another consideration will be the survey results from the surrounding community CR programs
26 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 25 and realizing their best practices and potential gaps in the delivery of CR care and the impact they can have on the readmission rates. Methods of Evaluation Readmission rates for AMI will one of the main outcome measures to evaluate the effectiveness of the newly implemented CR program. Other diagnoses can also be monitored if they are included in the CR enrollment. In order for the program to be sustained, the financial budget must also be maintained. Efforts must be made to contain extraneous costs with the program and if enrollment is lower during specific weeks, then staffing must flex down to keep the program financially sustainable. With a $66,000 margin, close monitoring of labor cost and payor mix must occur. If Medicare patients exceed the 55% projected percent of patient enrollment, then revenue will be less than projected and adjustments must be made. A SWOT analysis of the current state without a CR program was completed (Appendix M). Strengths are no additional equipment to purchase or maintain and no additional FTEs to hire and send through the orientation process. Weaknesses are that our own patients are referred to competing hospitals in the city for their rehabilitation. The MC is at the top in AMI care and exceeds the national standards for percutaneous coronary intervention (PCI) within 90 minutes of arrival and aspirin and statins prescribed at discharge, and why isn t CR provided at the facility post discharge? An additional weakness is that our own MC cardiology fellows in order to complete their CR rotation are going to competing hospitals to fulfill this requirement. Opportunities are that the MC is in the top 10 hospitals again this year according to the US News and World Report and with that, Dr. Dean Ornish s Intensive Cardiac Rehabilitation Program has reached out to hospital leadership in an effort to implement their program at the MC. San Francisco is also know for being a very fit city and there is potential to incorporate a wellness
27 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 26 component to the program. Threats include patients referred to outside CR programs are subject to leave their UC alliance depending on their experience at competing hospitals programs. Measurement of readmission rates as a determination of a success of the CR program must not be limited to Medicare FFS patients and should include all discharge diagnoses participating the CR program. Medicare FFS patients must be encouraged to participate in the program, as their 30-day readmissions are what place the hospital at risk for penalties. Patient satisfaction will also be measured quarterly to ensure that patient s needs and expectations are being met and will lead to better program adherence and potentially lower dropout rates. The community CR survey that was performed and the resulting power point educational program will also be used in the development in the program. Feedback from the power point was analyzed to determine if the educational information was useful and if changes in the community CR programs would be implemented based on the education provided (Appendix O). Analysis The findings from the survey performed along with the work that the Cardiology Service Transitions of Care and Readmissions Committee that has been done so far has provided the groundwork for a potentially viable program to provide a needed service to the patients who are discharged from the MC. A plan for full implementation of the project will be provided to key leadership and there is great interest in moving this project forward from the committee. Key findings of the survey included an interest in enrolling patients earlier after discharge and engaging them while they are hospitalized as part of the Phase I program in half of the respondents. All respondents felt that the information provided in the power point was helpful and one of the other facilities was experiencing some of the same barriers with their providers
28 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 27 having competing priorities and outside distractions. Another outcome of the educational session was an invitation to attend the kick off meeting of one of the facilities participating in the American College of Cardiology s Patient Navigator Program. This program addresses issues such as stresses within the hospital, fragility on discharge, lack of understanding of discharge instructions and inability to carry out discharge instructions through a personalized approach focused on meeting the needs of heart disease patients before and after they leave the hospital. The program will support a team of caregivers dedicated to helping patients overcome challenges during their hospital stay and in the weeks following discharge when they are most vulnerable and can prevent hospital readmissions. One of the more interesting feedback comments was the consideration of the types of patients that attend cardiac rehab and the associated reduced readmission rate. It was suggested by one of the sites that patients that are active participants in CR may be higher functioning, have fewer medication issues and can better advocate for themselves, which may lead to fewer hospital readmissions. Section IV Results Program Evaluation/Outcomes Although the program at the MC is yet to be established, local hospital based CR programs were assessed and some best practices were identified in the community CR questionnaire that will be incorporated into the proposal for the new program at the MC. Appendix G illustrates the characteristics of the 4 programs assessed. All programs had a Phase II, 36 session monitored exercise program, three of the programs did limited Phase I in patient teaching and all but one had an un monitored Phase III program with some very long term participants. Three of the four programs were certified by AACVPR and all were open five
29 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 28 days/week. The biggest variable was the length of time between hospital discharge and enrollment in the program. Some programs were as soon as 9-10 days and others as long as 4 weeks for AMI patients. Although much of the enrollment timing is physician driven, review of discharge information and medication reconciliation can occur prior to monitored exercise sessions and is an essential strategy to reduce readmissions. Some best practices were identified including a discharge order set with an automatic CR referral, which the discharging provider can opt out, but rarely does. Other best practices include a healthy heart program open to the public with a nominal fee, and offering CR to privately insured diabetic patients for risk reduction. From this assessment and the evidence supporting CR programs can lead to fewer AMI readmissions, an educational power point was prepared and distributed to those programs involved in the assessment (Appendix N). Best practices that were also shared as a part of the power point and include incorporating a referral for CR in the discharge order set for appropriate discharges, offering the CR program to diabetic patients for risk reduction, and a fee for service health heart lifestyle program. Feedback from the community CR programs after the educational power point was positive. All participants felt that the information provided was useful and helpful to their programs. Initiatives that the programs will take back to their programs include, better surveillance of post discharge follow up via their EHR, consideration of seeing patients earlier post discharge, and overcoming some of the inertia of the cardiologists at their facility (Appendix O).
30 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 29 Section V Discussion Summary Once the financial cost benefit analysis was completed, it was promising to see that implementing this program as designed would not be a cost burden to the facility. If run efficiently and the Medicare payor mix does not exceed 55% of the patient population, then a net revenue gain of a little over $66,000 annually can be achieved. Certain variables may arise during the approval process, but much effort was put into creating a realistic budget projection. Staffing includes an Advance Practice Nurse, (NP) as the main full time clinical member of the team. This clinician will have advanced pathophysiology and assessment skills. Along with the NP the other team members will be able to provide optimal care to this population that needs quick follow up to decrease the chance of the patient needing to be readmitted. The survey provided tremendous information that as a budding program will be helpful to mitigate issues that other programs have encountered. The other sites appreciated the evidence based information about how Phase 1 can be key to decreasing readmissions of this vulnerable population. Relation to Other Evidence Of the evidence outlined in the table in Appendix D, only two studies actually compared patients enrolled in a CR program to those that were not and the differences in readmission rates. One study involved CABG patients and the other AMI patients. Both studies demonstrated lower readmission rates for those patients enrolled in a CR program and when they were admitted, their LOS was much shorter and they had better outcomes. Other evidence described best practices and practice guidelines for the care of AMI patients that contribute to lower readmission rates. The main strategy that can be accomplished by early CR enrollment is post
31 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 30 discharge follow up within 7 days and reviewing of discharge instructions that include medication reconciliation and symptom management. A gap in practice a the MC demonstrated that patients were waiting over 14 days for their follow up appointments and that readmissions were occurring between 2-7 days post discharge. Comparing our discharge phone call data, it does appear that there is lack of clarity and understanding the medications that patients are discharged in addition to symptom management, as they are the majority of the reasons that patients request a call back. These are two of the main reasons patients are readmitted to the hospital according to the literature, and as evidenced at the MC. The evidence does support that stress of hospitalization does contribute to a lack of information retention and that reinforcement of this information in the intake assessment during their first visit to CR when the patient is less stressed can lead to better retention. The evidence also supports that nurse led education is associated with a reduced rate of complications anxiety, and readmissions of patients when they have a cardiac event, versus from a physician provider. At the MC, the nursing staff mainly provides the discharge education. A barrier previously identified at the MC is that this education is rushed due to the patient being anxious to get home in addition to the nurse s time competing with other priorities and anticipating the next admission. A case study at Tallahassee Medical Center demonstrated that a discharge clinic run by an advanced practice nurse targeted high-risk patients for readmission and were able to decrease ED visits and hospital readmissions by 61%. These results provide the needed evidence to pursue programmatic replication at the MC.
32 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 31 Barriers to Implementation/Limitations Creating the proposal was a robust exercise, but the larger barriers to successful implementation of the program are space allocation and identification of a medical director. Space is currently at a high premium, but the team is optimistic that with the opening of the new hospital in Mission Bay on February 1, 2015, and the relocation of several inpatient units both at the Parnassus and Mount Zion location, that adequate space can be identified. Program location consideration includes, easy patient access and parking, proximity to the medical director or other cardiologist for emergencies, and transport issues in case patients need to be admitted as an inpatient following any emergency event. Early discussions in the Cardiology Readmission Transitions meeting included the identification and salary of a medical director. Both cardiologists in attendance at the meeting reiterated the competing priorities between teaching, rounding with students and residents, clinic time, and participation in research. These were the same issues preventing additional clinic appointments that would increase patient access to post discharge follow up and stimulated the idea of a CR as an option for early post discharge follow up. In spite of these limitations, there is a spirit of optimism that this program proposal will be accepted and implemented in FY16. During the community CR program survey, one barrier was mentioned in all of the programs. That barrier was the ability to see patients while they are in the hospital, Phase I, due to shorter LOS and the lack of available CR personnel to see the patients. Many of the CR program managers felt that this could reduce patient drop out or non-participation in their CR program. The team will be taking this feedback and work to ensure there are ways to increase the use of Phase 1 with the patients in their program.
33 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 32 Interpretation Much of the evidence can be duplicated by the implementation of a hospital based CR program at the MC. The evidence that most patients are readmitted due to medication reconciliation and symptom management coincide with the discharge phone call responses from patients seeking clarification in those two areas. It is also worth mentioning that the data from the discharge phone calls are not a strategy to reduce readmissions, but an indicator of what areas patients lack understanding of the information provided to them at discharge and represent a strong indicator of potential readmissions. Early review of this information at the intake appointment in a CR program where the patient is more at ease and has better potential to information retention can result in fewer readmissions. As a result of the community CR educational power point, some CR programs will consider enrolling their patients earlier post discharge as a strategy to decrease hospital readmissions. Other adaptable strategies identified by the community CR programs include closer follow up post discharge by the CR staff via the patient s HER, enrolling patients in the CR program as soon as possible, and maintaining enthusiasm for the program with the medical staff by keeping them involved in the program. Conclusions Given the fact that access to post discharge physician follow up appointments currently cannot occur within 7-14 days at the MC, enrollment in a CR program can provide an intake appointment within that timeframe. During that intake assessment, medications can be reviewed along with the information provided to the patient at discharge that includes symptom management. The evidence indicates that these are two of the main reasons patients are readmitted and is supported by the discharge phone call feedback from the MC. The main
34 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 33 reasons patients are requesting return calls at the MC are due to questions regarding their medication, symptom management, and their follow up appointments. The implementation of a CR program at the MC could replicate the evidence and decrease 30-day hospital readmissions in eligible patient populations including AMI, Cardiac Surgery, Heart Transplant, post Stent placement, and CHF. The cost benefit analysis illustrates that the program would be revenue generating and not be a loss to the MC. Add the benefit of a decrease in 30-day readmissions of AMI and even CHF patients; the potential savings of not paying CMS fines make this proposal even more appealing in addition to the lack of reimbursement of care provided if the patient is readmitted 30 days post discharge. Once the CR program is established, future plans can also include a cardiac risk reduction program for diabetic patients, a privately funded wellness program, as well as a partnership with Dr. Dean Ornish s Intensive Cardiac Rehab Program, a reimbursable program by the CMS. Section VI Other Information Funding There was no need for funding the proposal activities and supporting evidence, nor the community CR program surveys. Once the proposal is accepting by the MC administration, the start up capital would be $145,000 and would be paid by the MC capital budget
35 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 34 References Andrews, M. (2011). Some hospitals turn to post-discharge clinics to help hold down readmissions [Issue brief]. Retrieved from Bean, P., & Waldron, K. (1995, September). Readmission study leads to continuum of care. Nursing Management, 26(9), Brown, J. R., Chang, C., Zhou, W., MacKenzie, T. A., Malenka, D. J., & Goodman, D. C. (2014, May 20). Health system characteristics and rates of readmission after acute myocardial infarction in the United States. Journal of the American Heart Association, Chugh, A., Williaims, M. V., Grigsby, J., & Coleman, E. A. (n.d.). Better transitions: improving comprehension of discharge instructions. Frontiers of Health Services Management, 25(3), Retrieved from Desai, M. M., Stauffer, B. D., Feringa, H. H., & Schreiner, G. C. (2009). Statistical models and patient predictors of readmission for acute myocardial infarction: a systematic review. Circulation Cardiovascular Quality and Outcomes, Detsky, A. S., & Krumholz, H. M. (2014, June 4). Reducing the trauma of hospitalization. JAMA, Goldfield, N. I., McCullough, E. C., Hughes, J. S., Tang, A. M., Eastman, B., Rawlins, L. K., & Averill, R. F. (2008, Fall). Identifying potentially preventable readmissions []. Health Care Financing Review, 30(1),
36 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 35 Jones, D., & Ringquist, L. (n.d.). Integrating medical homes and hospitals to reduce avoidable readmissions. Retrieved from Dorland Health: Kadda, O., Marvaki, C., & Panagiotakos, D. (2012, October 12). The role of nursing education after a cardiac event. Health Science Journal, 6, Retrieved from Kripalani, S., LeFevre, F., Phillips, C. O., Williams, M. V., Basaviah, P., & Baker, D. W. (2007, February 28). Deficits in communication and information transfer between hospital-based and primary care physicians. Journal of the American Medical Association, 297, Krumholz, H. M. (2013, January 10). Post-hospital syndrome - an acquired transient condition of generalized risk. New England Journal of Medicine, Lamb, G., & Carrier, D. (2013). Multipronged approach to reducing readmissions [Case study]. 155 North Wacker Drive, Chicago Illinois 60606: UHC. Law, D. (2012). Stress and learning - how prolonged stress damages our ability to focus and remember what we study. Natural Stress Care. Retrieved from Lee, T. L., & Bokovoy, J. (2005). Understanding discharge instructions after vascular surgery: an observational study. Journal of Vascular Nursing, XXIII(1), Meshgin, N. (2008, July). Cardiac rehabilitation reducing hospital readmissions through community based programs. Australian Family Physician, 37, Newsad, N. (2014). Cardiac rehab emerges as readmission reduction solution as Medicare targets hospital readmissions with payment policies. Retrieved from
37 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS Perk, J., Hedback, B., & Engvall, J. (1990, March). Effects of cardiac rehabilitation after coronary bypass grafting on readmissions, return to work, and physical fitness: a case control study. Scandinavian Journal of Public Health, Russell, S. S. (2006, October). An overview of adult learning processes. Urological Nursing, 26, Saczynski, J. S., Lessard, D., Spencer, F. A., Gurwitz, J. H., Gore, J. M., Yarzebski, J., & Goldberg, R. J. (2010). Declining length of stay for patients hospitalized with AMI: impact on mortality and readmissions. The American Journal of Medicine, Sanderson, B. K., Thompson, J., Brown, T. M., Tucker, M., & Bittner, V. (2009, November/December). Assessing patient recall of discharge instructions for acute myocardial infarction. Journal for Healthcare Quality, 31(6), Sharing the care: managing the myocardial infarct patient post discharge [Supplemental material]. (2011). Practicing Clinicians. Retrieved from Taverner, K. (2013). White paper hospital readmission rate reduction: building better interfaces within the community. North Wales, PA: Vree Health. University Health Care. (2002). Reducing readmissions benchmarking project [Issue brief]. 155 North Wacker Drive Chicago Illinois 60606: UHC.
38 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 37 VanSuch, M., Naessens, J. M., Stroebel, R. J., Huddleston, J. M., & Williams, A. R. (2006). Effect of discharge instructions on readmission of hospitalized patients with heart failure: do all of the joint commission on accreditation of healthcare organizations heart failure core measures reflect better care? Quality and Safe Health Care, 15, Walker, T. (2012, October). Take charge of medication reconciliation to reduce readmission rates [News capsules]. Formulary, 47, Retrieved from Ziaeian, B., Araujo, K. L., VanNess, P. H., & Horwitz, L. I. (2012, July 14). Medication reconciliation accuracy and patient understanding of intended medication changes on hospital disharge. Journal of General Internal Medicine, 27,

39 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 38 Appendix A Medicare(Data(
40 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 39 Appendix B Cardiology*Post.Discharge*Call:*Breakdown*April*2014* *July*2014* Home*Discharges* 479*paGents* discharged*to*home* Reach*Rates* 386*paGents*reached* (81%)* 93*paGents*not* reached*(19%)* Issue*Rates* 140*(36%)*paGents* required*callback* * 237*issues*captured* (auto*+*live*calls)* 246*(64%)*of*paGents* were*found*to*have* no*issues*with*auto* calls* Issue*Breakdown* 156*Clinical*Issues* 66%* 81*SaGsfacGon*Issues* 34%*

* 1%* Care**")
*")


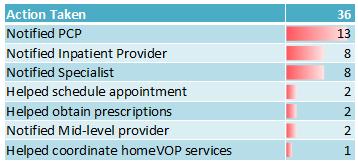
41 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 40 Appendix C Wound/* Incision*(1)* 1%* Care** CoordinaAon*(14)* 9%* Other*D/C* InstrucAons*(3)* 2%* MedicaAon** Class** (11)* 7%* Cardiology*Issue*Breakdown:*Clinical*Issues** * AcAon** Taken*(36)* 23%* 156*Clinical*Related* Issues* Symptoms*(49)* 31%* MedicaAons** (22)* 14%* PrescripAons** (20)* 13%*
42 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 41 Appendix D Johns Hopkins Nursing Evidenced-based Practice Individual Evidence Summary Tool Author & Date 1 Andrews Bean, et al Evidence Type Case study Clinical practice guidelines Sample, Sample Size, & Setting 600 patients discharged from Tallahassee Medical Center 503 patients discharged from Lakes Region Hospital Study Findings Discharge clinic established Targeted at high risk patients for readmission ED visits and hospital readmissions decreased by 61% 11% readmitted 88% of those had chronic conditions Lack of recall of discharge instructions Unable to find printed instructions Evidence Level & Quality 5B 4B 3 Brown, et al Chugh, et al. 5 Desai, et al Detsky 2014 Non Experimental Research Systematic Review Systematic Review Systematic Review 38,350 AMI readmissions in 1088 hospitals in one year 20.3% readmission rate overall Improve palliative care PCP visit within 14 days of discharge Medication reconciliation Shorter LOS and complexity of discharge instructions lends itself to likelihood of readmissions Effect of health literacy and cognitive function on comprehension of discharge instruction Found few patient predictors or characteristics consistently associated with readmissions Identified post hospital syndrome as result of stress of hospitalization 3A 4B 4A 4B
43 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 42 Author & Date 7 Kadda, et al Jones, et al Krumhol z Law 2012 Evidence Type Systematic Review Expert Opinion Systematic Review Expert opinion Sample, Sample Size, & Setting Study Findings which could lead to lack of information retention Stressors include lack of sleep, pain, deconditioning & anxiety Nurse led education is associated with a reduced rate of complications, anxiety, and readmissions of patients with a cardiac event 3 categories of readmissions o Complications during stay o Poorly managed discharge processes to home of other facility o Recurrence of chronic condition Must not do any additional harm to patients while hospitalized and increase their stress levels Efforts to be made to decrease their vulnerability after discharge by improving the hospital stay by o Reducing disruption of sleep o Minimizing pain o Emphasize physical activity o Enhancing cognitive and physical function Chronic or long term stress limits ability to focus, concentrate, and remember facts Evidence Level & Quality 11 Lee, et al. Non 24 patients 65% of patients were able 3B 4B 5A 4B 5B
44 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 43 Author & Date 12 Meshgin Newsad Perk et al Evidence Type Sample, Sample Size, & Setting 2005 Experimental post vascular surgery 15 Practicin g Clinician s Russell 2006 Experimental Clinical Practice guidelines Experimental Clinical Practice Guidelines Literature Review 308 post cardiac patients 147 post CABG patients Study Findings to answer 4 questions about their discharge instructions 3 days post discharge 198 patients in control group no CR o 19% were readmitted 110 patient in treatment group CR o 6% were readmitted CR prevents a recurring event Can help to reduce hospital readmissions after cardiac event CR enrollment remains low especially with women, minorities, and impoverished patients 98 patients in control group no CR o 32% of patients were readmitted 49 patients in treatment group CR o 14% of patients were readmitted Reinforced the AHA & ACC post MI care guidelines Emphasized the need for timely post discharge review of medications to reduce readmissions o Aspirin o Beta blockers o Lipid lowering agents Identified barriers to learning according to Knowles theory of adult Evidence Level & Quality 1A 4C 1B 4A 5B
45 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 44 Author & Date 17 Saczynsk i et al Sanderso n et al UHC Field Brief UHC 2013 Evidence Type Non Experimental Case Study Clinical Practice Guidelines Case Study Sample, Sample Size, & Setting 4184 post AMI patients for 6 years 159 post AMI patients in academic medical centers Survey of 36 academic medical centers 500 bed academic medical center reduced readmissions by 14% Study Findings learning o Learner does not see the need for change Decreased LOS not associated with higher readmission rates Prolonged LOS was associated with higher readmission rates Patients had better recall of medications than lifestyle recommendations from their discharge instructions 5 best performers were identified based on their lower than average readmission rates o Interdisciplinary team interaction during hospitalization o DC tools used for teaching teachback o 7 day post discharge plan and follow up with PCP Most common 30 day readmissions were CHF and sickle cell disease Due to lack of engagement by primary care physicians o Created an outpatient clinic for high risk discharged patients o Clinic also did call backs to patients Evidence Level & Quality 21 VanSuch Meta 782 patients 68% of patients received 1A 3A 5B 4A 5B
46 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 45 Author & Date et al Walker Ziaeian etal.2012 Evidence Type Analysis Clinical Practice Guidelines Meta Analysis Sample, Sample Size, & Setting eligible to receive discharge instructions 377 patients discharged with CHF, ACS, or PNE Study Findings all instructions o less likely to be readmitted for any cause Described H2H, program endorsed by ACC and IHI for patients with CHF and AMI o Follow up to occur within 7 days post DC o Mind your Meds post discharge medication management o Signs and Symptoms patient recognition of signs and symptoms Assessed patient understanding of intended medication changes through post DC interviews Medication reconciliation and patient understanding are inadequate in older patients post discharge Evidence Level & Quality 4A 1A
47 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 46 Appendix E AACVPR Core Competencies for Cardiac Rehabilitation & Secondary Prevention Professionals Competency Knowledge Skills Patient Assessment Nutritional Counseling Nutritional Counseling Demonstrates an understanding of: Cardiovascular anatomy, physiology, & pathophysiology Cardiac arrhythmias & their influence on physical activity & symptoms Cardiac device therapies (pacemakers, defibrillators, VADs) Cardiovascular assessments, diagnostic tests, & procedures Signs & symptoms of CVD Appropriate emergency responses to changing signs & symptoms Effective lifestyle management ot CVD & associated risk factors Pharmacological approaches for CVD & risk factor management Comorbidities limiting or otherwise influencing function or treatment strategies Side effect from pharmacologic therapies Psychosocial factors related to CVD Adult learning principles, theoretical models for behavior change, adherence, coping, disease management strategies Compliance & adherence to therapeutic regimens Effective communication to referral sources & the interdisciplinary team to promote care coordination Principles & methods for outcome assessment and reporting Demonstrate an understanding of: Role and impact of diet & CVD progression & risk factor Ability to perform the following: Obtain a comprehensive medical, social, & family history through interview, review of medical records, & questionnaires Physical examination of cardiovascular system (HR, BP, heart tones, lung sounds, pulses, signs of DVT, PAD, & wounds) Develop risk factor profile & CVD risk reduction strategies Basic tests & assessments, 12 lead ECG, oximetry, blood glucose, & lipids Obtain information on patient preferences &goals Interactive communication & counseling with patient & family on treatment plan through shared decision making Develop an ITP Document and communicate ITP & progress reports to physicians & ID team Quantify patient outcomes assessment through pre & post program assessment Ability to perform the following: Dietary intake assessment to estimate total calories,
48 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 47 Competency Knowledge Skills (con t) management Analysis of diet composition with specific emphasis on total caloric intake & dietary content that influences risk factors Potential risks & benefits of nonprescription nutritional amounts of saturated fats, trans fat, cholesterol, sodium, fruits & vegetables, whole grains, fiber, & fish, number of meals & snacks, portion size, frequency of eating out, alcohol consumption supplements & alcohol intake Education & counseling on Target goals for dietary modification and nutrition specific dietary modifications needed to achieve target goals interventions for identified risk Behavior interventions to factors & co morbidities (HTN, diabetes, HF, kidney disease) Effective behavior change promote adherence & self management skills in dietary habits strategies based on common Measure & report outcomes of theoretical models & adult learning strategies nutritional management goals at the conclusion of the Weight management Weight management (con t) Demonstrates an understanding of: Physiological & pathological effects of overweight & obesity & those of low body weight Principles of weight management through the balance of caloric intake & caloric expenditure Awareness of fad diets & possible risks to CVD patients Current guidelines & recommendations for healthy body weight and & secondary prevention Weight loss interventions that promote gradual, sustainable weight loss (5-10%) over 3 to 6 months Medication & surgeries for weight loss Nutritional & medical risks associate with rapid weight loss & cyclical weight gain & weight loss Recognition that weight loss and weight maintenance is often complex & difficult & requires ongoing dietary management, physical activity, & behavioral program Ability to perform the following: Measure body weight, height, & waist circumference Calculate BMI & determine proper category, normal, overweight, or obese Develop short and long term weight loss goals for those in overweight or obese categories Assess nutritional & dietary habits as well as daily energy intake & expenditure to help guide individualized education & counseling for weight management Behavioral interventions to promote adherence & selfmanagement skills in weight management Measure and report outcomes of weight management at the conclusion of the program
49 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 48 Competency Knowledge Skills management Importance & efficacy of regular physical activity, modification of dietary patterns, changes in caloric balance, & drug therapy in weight management Effective behavior change strategies based on common theoretical models & adult learning strategies Blood Pressure management Lipid management Demonstrate an understanding of: HTN as a risk factor for atherosclerotic vascular disease Signs & symptoms of hypotension and hypertension Normal range of BP at rest & during exercise Current BP targets for secondary prevention Home BP monitoring Actions of classes of antihypertensive medications & common side effects Postural & post exercise hypotension Elements of the DASH diet for treating HTN Principles of measurement & operation for BP measurement devices Recognition that BP control is often complex & difficult & may require ongoing medication adjustments, dietary management, physical activity & behavioral management Importance & efficacy of sodium restriction, weight management, physical activity, smoking cessation, alcohol moderation, & drug therapy in the control of BP Demonstrate an understanding of: Definitions of LDL-C, HDL-C, VLDL-C, TG, non HDL-C Ability to perform the following: Accurate BP determinations at rest (seated, supine, & standing) & during exercise Recognize significant BP deviation from the expected range or targeted outcome Assess compliance with BP medications and management plan Measure & report outcomes for BP management at the conclusion of the rehabilitation program Ability to perform the following: Interpret LDL-C, HDL-C, non- HDL-C, VLDL-C, & TG
50 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 49 Competency Knowledge Skills Physiological role of lipids in the atherosclerotic disease process Elements of the Therapeutic Lifestyle Change Diet and the Mediterranean diet Action of classes of anti hyperlipidemia medications, including non prescription, & side effects Types of dietary fats & simple carbohydrates & their effect on serum lipid levels Current serum lipid target clause for secondary prevention Importance & efficacy of weight management, physical activity & exercise, smoking cessation, alcohol moderation, & drug therapy in the control of serum lipids Diabetes management Demonstrate an understanding of: Type I & type II diabetes Fasting & casual BG values that define hypoglycemia & hyperglycemia Importance of & recommended target value for HbA1c Complications related to diabetes Signs & symptoms related to hypoglycemia & hyperglycemia Use of carbohydrates for hypoglycemia Actions of glucose-lowering medications and insulin Importance of monitoring BG values, before & after exercise Contradictions to exercise based on BG values Importance of compliance with diabetic medications & dietary, body weight, & exercise recommendations Importance of recognizing & managing the metabolic syndrome values in light of secondary prevention target values Assess compliance with anti hyperlipidemia medications & management plan Assess compliance with lifestyle intervention for the management of serum lipid values Provide patient education information concerning serum lipids Develop a risk reduction plan for abnormal serum lipids & communicate the plan to the patient & family Measure & report outcomes for serum lipid at the conclusion of the rehabilitation Ability to perform the following: History of complications related to diabetes, including frequency & triggers of hyperglycemia and hypoglycemia Calibration & proper use of glucometers Assess signs & symptoms of hyperglycemia & hypoglycemia & take appropriate actions Provide patient education concerning the effects of lifestyle & medications on glycemic control Referral of the [patient to a diabetic educator or clinical dietician as needed Measure & report outcomes for glucose control at the conclusion of rehabilitation, including episodes of hyperglycemia & hypoglycemia during and after
51 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 50 Competency Knowledge Skills & the associated CVD risk factors exercise Importance & efficacy of weight management, physical activity & exercise, alcohol moderation, & drug therapy in the control of BG Tobacco cessation Psychosocial management Demonstrate an understanding of: Current guidelines for treating tobacco use & secondary prevention goal Biochemical & physiological consequences of smoking on CVD Exposure to second hand smoke as a risk factor for cardiovascular events Effective behavior change strategies based on common theoretical models Available services to support smoking cessation, community programs, counselors, psychologists Physiological & psychological aspects of tobacco addiction Efficacy of pharmacologic interventions, including risks & benefits Demonstrate an understanding of: Influence of psychosocial factors on the pathophysiology of CVD & adherence to treatment Depression & its major association with recurrent CAD events, poorer outcomes, & adherence to treatment Other psychological indicators that may affect treatment response such as anxiety, anger, hostility, & social isolation Actions of pharmacologic & lifestyle interventions for psychological distress Socioeconomic factors that may Ability to perform the following: Assessment of use & categories of tobacco use, never, former, recent, or current Behavioral interventions to promote tobacco cessation & long term tobacco free adherence Measure & report outcomes of tobacco cessation at the conclusion of the program Ability to perform the following: Screening & assessment for psychological distress, especially depression, anxiety, anger, hostility, social isolation, marital or family distress, sexual dysfunction, and substance abuse Appropriate referrals for psychiatric or psychological care when needs are recognized as beyond the scope of usual care Individual & group education & counseling interventions that address stress management & coping
52 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 51 Competency Knowledge Skills serve as barriers to treatment strategies adherence such as educational or Measure & report outcomes of income level, lack of resources or psychosocial management at support the conclusion of the program Available support services to augment psychological interventions, psychologists, counselors, social workers, clergy Effective behavior change strategies based on common theoretical models & adult learning strategies Physical activity counseling Demonstrate an understanding of: Lack of regular physical activity & sedentary behavior as a risk factor for CAD Negative health consequences of time spent being sedentary Current recommendations for intensity frequency & duration for regular physical activity in persons with CVD Preexisting musculoskeletal & neuromuscular conditions that may affect physical activity Identifying physical activities that may increase the risk of an untoward cardiovascular event & environmental condition that may also increase the risk Barriers to increasing physical activity Metabolic requirements for recreational, occupational, & sexual activities Recommendations to avoid musculoskeletal injury related to physical activity Effective behavior change strategies based on common theoretical models & adult learning strategies Ability to perform the following: Assess current physical activity level using both questionnaires & available activity monitoring devices Assist patients in setting realistic incremental goals for future physical activity Recommendations for increasing the level of safe & appropriate daily physical activity & structured exercise Assess physical & metabolic requirements for activities of daily living & occupational & recreational activities Communication & behavioral strategies that will improve compliance with regular physical activity recommendations Measure & report outcomes for physical activity at the conclusion of rehabilitation Exercise Demonstrate an understanding of: Ability to perform the following:
53 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 52 Competency Knowledge Skills training evaluation Normal & abnormal responses to exercise including signs & symptoms of exercise intolerance, myocardial ischemia, acute coronary syndrome, & ventricular arrhythmias Physiological responses to acute exercise & adaptations to chronic exercise Risk stratification according to patient assessment & exercise test results Exercise prescription methodology for cardiovascular endurance exercise & resistance training in a broad range of patients with heart disease Absolute & relative contraindications for exercise Absolute & relative indications to terminate an exercise session Recognize life-threatening cardiac arrhythmias, myocardial ischemia, or infarction, hypoxemia, hypotension, hypoglycemia, & other signs & symptoms of exercise intolerance Risk stratify each patient according to AHA & AACVPR criteria Develop an individualized, safe, & effective cardiovascular endurance exercise prescription including modes, intensity, duration, frequency, & progression Develop an individualized, safe, & effective exercise prescription for resistance training including load, number of repetitions, frequency, and progression for appropriate muscle groups Include warm-up, cool-down, & exercises flexibility & balance in the exercise prescription As needed, accommodate existing comorbidities within the exercise prescription Skin preparation & electrode placement for exercise ECG monitoring Measure & report outcomes for exercise training at the conclusion of the rehabilitation
54 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 53 Facility Appendix F Hospital Based Cardiac Rehabilitation (CR) Questionnaire Contact Person Phone 1. Is your program certified by AACVPR? Yes No Title 2. What phases of CR do you offer? Phase I Phase II Phase III 3. How long do patients participate in each program? Phase I: Phase II: Phase III: 4. What educational topics are covered during CR and when? Topic Medications When Taught Diet Exercise Symptom Management Other: Other: 5. Patients with the following discharge diagnoses participate in CR: Angina Cardiac Surgery (either CABG or Valve) Heart Failure
55 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 54 Acute Myocardial Infarction (AMI) Other 6. How soon after hospital discharge do patients enter the program? 7. Is there any contact by the CR team prior to the patient s discharge? 8. What is your current staffing and operating hours 9. Do you monitor if your patients are readmitted to the hospital during their CR enrollment? Yes No 10. Other
56 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 55 Appendix G Facility Comparison of Hospital Based Cardiac Rehab Programs Diagnoses Served AACVPR Certified Phases Offered AMI Angina Cardiac Surgery Heart Failure Earliest Enrollment for AMI post Discharge CPMC X I, II X X X 9-10 days M-F 8-4:30p Seton X I, II, III X X X X 2-3 weeks St. Marys I, II, III X X X 4 weeks Hours of Operation Comments and Best Practices MWF 7-5p TTh 7-11a MWF 7-4:30p TTh 7-11a UC Davis X II, III X X X X 2 weeks M-F 7-4:30p Discharge order set includes CR referral automatically Also offer Healthy Heart Program to public Some Phase III participants have been participating for over 10 years. Oldest patient is 98. Offer CR for privately insured diabetic patients for risk reduction
57 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 56 Appendix H Numbers of Discharges Discharges by Diagnosis FY13 FY14 AMI CABG Other Heart Surgery Valve Surgery Cardiac Transplant Stents HF/Shock Advanced Heart Failure Patients per session 5 Total # sessions year Phase II Days/week Annually % % % % % Phase II = 36 sessions and Cardiac Rehabilitation Enrollment Projections


58 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 57 Anne Thorson, M.D. Cardiologist Appendix I In House Cardiac Rehabilitation Experts Dr. Anne Thorson, a cardiologist, is co-director of the UCSF Center for Prevention of Heart and Vascular Disease at Mission Bay and the supervising physician in the Non-invasive Cardiac Stress Laboratory, which evaluates patients for heart disease. An expert in women's heart health, she specializes in assessing and treating cardiovascular disease in women. Thorson is interested in early diagnosis and treatment of patients at potential risk of heart and vascular disease and in noninvasive imaging technology to diagnose and monitor heart conditions. Prior to joining UCSF in 1999, Thorson was in private practice for 10 years. She was director of Cardiac Rehabilitation Services at California Pacific Medical Center in San Francisco and medical director for the "Health Champions" to promote wellness among San Francisco school children. Thorson earned a medical degree at Stanford University School of Medicine. At UCSF, she is an associate clinical professor of medicine in the Division of Cardiology. Gordon Fung, M.P.H., M.D. Cardiologist Dr. Gordon L. Fung, a cardiologist, is an expert in the treatment of heart disease with a special interest in cardiac rehabilitation, cardiovascular pharmacology, echocardiography and preventive cardiology. At UCSF Medical Center at Mount Zion, he is director of the Cardiology Consultation Service, the Cardiac Noninvasive Laboratory and the Enhanced External Counterpulsation Unit. At the medical center's Parnassus location, he directs the Electrocardiography Laboratory and is the associate director of the Non-Invasive Laboratory. Fung's research explores advances in preventive cardiology and end stage heart disease. Fung earned a master's degree in public health in hospital economics and administration at the University of California, Berkeley and a medical degree at the University of California, San Francisco. He completed an internal medicine residency and was chief resident at Highland General Hospital in Oakland. He completed a cardiology fellowship at the Veterans Administration Medical Center in Martinez, Calif. He has been active in the activities American Heart Association and has served on the association's national board of directors. Fung is an associate clinical professor of medicine and cardiology at UCSF.
59 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 58 Medical Center Capital Budget Request - ROI Appendix J ROI Budget Projections Cost Center #/Name Request Name Request Description Outpatient Cardiac Rehabilitation Program Pat Forsberg/Jeff Kalin Program for new outpatient service to include cardiac discharge diagnoses including, AMI, CABG, Valves, Stents, ACS, and HF Justification Reduced 30 day re-admissions and improving population health Capital Cost Summary Unit Cost 12 Channel Telemetry with Central $80,000 Station 10 3,000 $30,000 1 Recumbant Exercise Bicycle $1,800 4 Airdyne Exercise 900 $3,600 1 Eliptical $2,500 Emergency Code Cart with Defibrillator $10,000 Subtotal: $127,900 Sales Tax & 13.5% $17,267 Other costs $145,167 Additional Capital (Below) Additional IT Additional Construction Other Less Trade In: (enter as pos number) Total Capital Request: $145,167
60 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 59 FINANCIALS 189 Patients 283 Patients 20% of eligible patients 30% of eligible patients Medicare Revenue $59,492 $89,032 Enter UOS--- 55% of patients Volume: >>> x 36 sessions 3,744 5,603 Rate: $15.89 $15.89 Commercial Revenue $274,880 $411,871 Enter UOS--- 45% of patients Volume: >>> x 36 sessions 3,060 4,585 Rate: $89.83 $89.83 Gross Patient Revenue $334,372 $500,902 Deductions Net Patient Revenue $334,372 $500,902 Other Operating Revenue $0 $0 Total Operating Revenue $334,372 $500,902 Salaries $187,200 $187,200 FTEs - RN Rate: $60.00 $60.00 FTEs - Exercise Tech Rate: $39.50 $39.50 Benefits 30.00% $56,160 $56,160 Contract Labor - RD 1 hour/week $2,500 $2,500 Professional Fees - MD Director $12,500 $12,500 Contract Labor Expenses $15,000 $15,000 Total Labor Expenses $258,360 $258,360 life Depreciation --->> Enter Useful 10 Half Year $7,258 $14,517 Interest $0 $0 Bad Debt $0 $0 Other Expenses $2,500 $2,500 Service Contract $0 Rent $0 $0 Supplies $1,500 $1,500 Marketing $1,000 $1,000 Total Expenses $268,118 $275,377 Excess Revenue over Expenses $66,254 $225,526
61 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 60 Appendix K GANTT Chart Implemen'ng)a)Cardiac)Rehabilita'on)Program)at)UCSFMC) Weeks) Ini$a$on' 1) 2) 3) 4) 5) 6) 7) 8) 9) 10) 11) 12) 13) 14) 15) 16) 17) 18) 19) 20) 21) 22) 23) 24) 25) 26) 27) Assessment)&)Recommenda'ons))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Create)proposal*))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Finalize)budget)projec'ons))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Submit))proposal)to)Administra'on))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Administra've)approval)obtained*))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Planning' )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Review)state)requirements))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Order)Equipment))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Modify)exis'ng)space))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Equipment)procurement))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Hire),)orient,)and)train)staff))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Develop)work)flows)and)order)sets#))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Execu$on' )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Project)tem)kickoff)mee'ng))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Work)observa'on)(Gemba)))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Prac'ce)"Day)in)the)Life"))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Implement)small)test(s))of)change))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Meaure)short)term)results))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) ReEvaluate)as)necessary))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Control' )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Project)status)mee'ngs))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Monitor)outcome)repor'ng))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Adjust)or)redirect)as)necessary))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Closeout' )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Report)out)on)process/outcomes*))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Plan)on)sustaining)improvement))) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) )) Assump'ons)include:) Week)8)star'ng)July)1,)2014) *) Milestones) #) Deliverables)
62 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 61 Appendix L Gap Analysis Identified Best Practices Nurse led education associated with reduced rate of complications, anxiety, and readmissions of patients with cardiac event (Kadda et al. 2012) Identified barriers to learning according to Knowles if learner does not see the need for change (Russell 2006). Decreased LOS not associated with higher readmission rates and prolonged LOS was associated with higher readmission (Sacsynski et al. 2009) 7 day post discharge plan and follow up with PCP (UHC Field Brief 2011) Creation of an outpatient clinic for high risk patients (UHC 2013) Discharge Clinic established for patient at high risk of readmission (Andrews 2011) Shorter LOS and complexity of discharge instructions lends itself to likelihood of readmissions (Chugh, et al.) Cardiac Rehab (CR) prevents recurring event and can help to reduce hospital readmission after a cardiac event (Newsad 2014) Need for timely post discharge review of medications to reduce readmissions, medications include aspirin, beta blockers, and lipid lowering agents (Practicing Clinicians 2011) H2H Program endorsed by American College of Cardiology (ACC) and IHI include follow up within 7 days post discharge, mind your meds, and signs and symptoms review at that time (Walker 2012) UCSFMC Discharge teaching is done by bedside RN usually on day of discharge and questions answered post discharge when prompted by automated discharge phone call. If new diagnosis for patient and patient does not embrace new diagnosis or is in denial, patient does not see the need for additional education. Cardiology service struggles with balance of keeping patient longer to ensure stabilization while continued hospitalization contributes to deconditioning and stress Access to cardiology clinic and/or PCP at UCSF impacted and takes longer than 14 days to get appointment. No clinic established Admission Visit Summary (AVS) is a 7-8 page document provided to the patient that outlines discharge instructions and medication list. If patients are prescribed CR, they are referred to outside and potentially competing facilities. Unknown when actual medication review takes place after discharge prior to post discharge follow up appointment which can occur after 14 days post discharge. No follow up appointment in 7 days post discharge and discharge phone call data suggests that most patients have questions about medications and symptoms management.
63 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS 62 Appendix M SWOT Analysis Current State without Cardiac Rehab Program Strengths Weaknesses Opportunities Threats No capitol outlay Patients prescribed CR are referred to outside and competing hospitals In top 10 hospitals in nation with cardiovascular center of excellence. No additional FTEs UCSFMC demonstrates excellent AMI care higher than national average for PCI within 90minutes Aspirin at discharge Statins at discharge Why not complement with a CR program? UCSF cardiology fellows must complete their CR rotation off site either at St. Mary s or CPMC Dean Ornish s Intensive CR program, reimbursed by CMS, has approached UCSFMC to collaborate on establishing program Creation of on site wellness center for San Francisco population Draw patients currently accessing services at other medical centers in the city of San Francisco Support the referral of patients back to the MC for other cardiology patients Patients could leave UC system based on their experience at competing hospitals CR program


64 AVOIDING 30-DAY READMISSIONS OF ACUTE MI PATIENTS Appendix N Educational Power Point to Local CR Programs Can Participation in a Cardiac Rehabilitation Program Decrease AMI Readmissions? Pat Forsberg, DNPc, MBA, RN, NE-BC October
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Significance of Timing of Patient Daily Weights and the Barriers
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 The
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 The
Improving Nurse-patient Communication about New Medicines
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Improving
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
paymentbasics The IPPS payment rates are intended to cover the costs that reasonably efficient providers would incur in furnishing highquality
 Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs
 Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
MAC J-15 Cardiac & Pulmonary Probe Audit / Ohio & Kentucky (March 2012) J. Rosneck MAC 15 Chairperson
 J. Rosneck MAC 15 Chairperson") Greetings All, MAC J-15 Cardiac & Pulmonary Probe Audit / Ohio & Kentucky (March 2012) I discovered late last week from the AACVPR, prior to presenting at the Kentucky state meeting, that the RAC probe
Greetings All, MAC J-15 Cardiac & Pulmonary Probe Audit / Ohio & Kentucky (March 2012) I discovered late last week from the AACVPR, prior to presenting at the Kentucky state meeting, that the RAC probe
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
 Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
VAP Prevention in the CTICU
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-22-2015 VAP
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-22-2015 VAP
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Intermediate Coronary Care Unit Rotation
 1 Intermediate Coronary Care Unit Rotation Section of Cardiology Dartmouth-Hitchcock Medical Center (2008-2009) I. Overview of Rotation The cardiology-specific critical care experience is in the Intermediate
1 Intermediate Coronary Care Unit Rotation Section of Cardiology Dartmouth-Hitchcock Medical Center (2008-2009) I. Overview of Rotation The cardiology-specific critical care experience is in the Intermediate
Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting
 Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting Chris Kane SVP, Strategic Business Development WellStar
Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting Chris Kane SVP, Strategic Business Development WellStar
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Home Health. Improving Patient Outcomes & Reducing Readmissions. Home Health: Improving Outcomes & Reducing Readmissions
 Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
CKHA Quality Improvement Plan (QIP) Scorecard
 Scorecard") CKHA Quality Improvement Plan () Scorecard 217-18 Quality dimension Performance Indicator 217-18 Performance Goals results where available Current Value Page Safety Medication Reconciliation completed
CKHA Quality Improvement Plan () Scorecard 217-18 Quality dimension Performance Indicator 217-18 Performance Goals results where available Current Value Page Safety Medication Reconciliation completed
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
HOSPITAL QUALITY MEASURES. Overview of QM s
 HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Regulatory Advisor Volume Eight
 Regulatory Advisor Volume Eight 2018 Final Inpatient Prospective Payment System (IPPS) Rule Focused on Quality by Steve Kowske WEALTH ADVISORY OUTSOURCING AUDIT, TAX, AND CONSULTING 2017 CliftonLarsonAllen
Regulatory Advisor Volume Eight 2018 Final Inpatient Prospective Payment System (IPPS) Rule Focused on Quality by Steve Kowske WEALTH ADVISORY OUTSOURCING AUDIT, TAX, AND CONSULTING 2017 CliftonLarsonAllen
Specialty Payment Model Opportunities Assessment and Design
 Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
OMC Strategic Plan Final Draft. Dear Community, Working together to provide excellence in health care.
 Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Evaluation of a Pharmacist-Led Bedside Medication Delivery Service for Cardiology Patients at Hospital Discharge
 Evaluation of a Pharmacist-Led Bedside Medication Delivery Service for Cardiology Patients at Hospital Discharge Julianna Burton, Pharm.D., BCPS, BCACP, FCSHP Assistant Chief, Ambulatory Clinical Services
Evaluation of a Pharmacist-Led Bedside Medication Delivery Service for Cardiology Patients at Hospital Discharge Julianna Burton, Pharm.D., BCPS, BCACP, FCSHP Assistant Chief, Ambulatory Clinical Services
HCAHPS: Background and Significance Evidenced Based Recommendations
 HCAHPS: Background and Significance Evidenced Based Recommendations Susan T. Bionat, APRN, CNS, ACNP-BC, CCRN Education Leader, Nurse Practitioner Program Objectives Discuss the background of HCAHPS. Discuss
HCAHPS: Background and Significance Evidenced Based Recommendations Susan T. Bionat, APRN, CNS, ACNP-BC, CCRN Education Leader, Nurse Practitioner Program Objectives Discuss the background of HCAHPS. Discuss
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
Quality Based Impacts to Medicare Inpatient Payments
 Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
DRAFT Complex and Chronic Care Improvement Program Template. (Not approved by CMS subject to continuing review process)
") DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
Reducing Avoidable Readmissions Within 30 Days of Discharge
 Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING
 MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
Factors that Impact Readmission for Medicare and Medicaid HMO Inpatients
 The College at Brockport: State University of New York Digital Commons @Brockport Senior Honors Theses Master's Theses and Honors Projects 5-2014 Factors that Impact Readmission for Medicare and Medicaid
The College at Brockport: State University of New York Digital Commons @Brockport Senior Honors Theses Master's Theses and Honors Projects 5-2014 Factors that Impact Readmission for Medicare and Medicaid
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
STATE OF KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES OSAWATOMIE STATE HOSPITAL OPERATIONS ASSESSMENT EXECUTIVE SUMMARY
 STATE OF KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES OSAWATOMIE STATE HOSPITAL OPERATIONS ASSESSMENT Prepared by: THE BUCKLEY GROUP, L.L.C. OVERVIEW The Osawatomie State Hospital (OSH) in Osawatomie
STATE OF KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES OSAWATOMIE STATE HOSPITAL OPERATIONS ASSESSMENT Prepared by: THE BUCKLEY GROUP, L.L.C. OVERVIEW The Osawatomie State Hospital (OSH) in Osawatomie
Creating Care Pathways Committees
 Presentation Creating Care Title Pathways Committees December 12, 2012 December 12, 2012 Creating Care Pathways Committees LeadingAge Indiana Integrated Care & Payment Executive Series 1 2012 Health Dimensions
Presentation Creating Care Title Pathways Committees December 12, 2012 December 12, 2012 Creating Care Pathways Committees LeadingAge Indiana Integrated Care & Payment Executive Series 1 2012 Health Dimensions
Expression of Interest for Wound Care Project
 Expression of Interest for Wound Care Project November 11, 2016 Telewound Care EOI Page 1 of 12 Contents 1 Introduction... 3 2 Telewound Care Project Background... 4 2.1 Background... 4 2.2 Purpose...
Expression of Interest for Wound Care Project November 11, 2016 Telewound Care EOI Page 1 of 12 Contents 1 Introduction... 3 2 Telewound Care Project Background... 4 2.1 Background... 4 2.2 Purpose...
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
National Patient Safety Goals & Quality Measures CY 2017
 National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
Chronic Care Taking Disease Management Beyond Hospital Walls
 Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
CMS Quality Program- Outcome Measures. Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018
 CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions for Myocardial Infarctions with Early Access to Clinic: An Innovative Approach
 Reducing Readmissions for Myocardial Infarctions with Early Access to Clinic: An Innovative Approach Kathryn Ward, MSN, PHCNS-BC, DNPc 2016 Ninth Annual DNP Conference, Baltimore, MD October 5-7, 2016
Reducing Readmissions for Myocardial Infarctions with Early Access to Clinic: An Innovative Approach Kathryn Ward, MSN, PHCNS-BC, DNPc 2016 Ninth Annual DNP Conference, Baltimore, MD October 5-7, 2016
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Hospital Inpatient Quality Reporting (IQR) Program
 Program") Hospital IQR Program Hybrid Hospital-Wide 30-Day Readmission Measure Core Clinical Data Elements for Calendar Year 2018 Voluntary Data Submission Questions and Answers Moderator Artrina Sturges, EdD, MS
Hospital IQR Program Hybrid Hospital-Wide 30-Day Readmission Measure Core Clinical Data Elements for Calendar Year 2018 Voluntary Data Submission Questions and Answers Moderator Artrina Sturges, EdD, MS
Webinar. Reducing Readmissions with BI and Analytics. 23 March 2018 Copyright 2016 AAJ Technologies All rights reserved.
 Webinar Reducing Readmissions with BI and Analytics Copyright Reducing 2016 Readmissions AAJ Technologies with BI and All rights Analytics reserved. www.aajtech.com Hospital Readmissions Michele Russell,
Webinar Reducing Readmissions with BI and Analytics Copyright Reducing 2016 Readmissions AAJ Technologies with BI and All rights Analytics reserved. www.aajtech.com Hospital Readmissions Michele Russell,
Medical Appropriateness and Risk Adjustment
 Medical Appropriateness and Risk Adjustment Medical Appropriateness David Rzeszutko, MD Medical Director November 10, 2017 Objectives Medical necessity Value equation Medical appropriateness Why? To improve
Medical Appropriateness and Risk Adjustment Medical Appropriateness David Rzeszutko, MD Medical Director November 10, 2017 Objectives Medical necessity Value equation Medical appropriateness Why? To improve
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
FirstHealth Moore Regional Hospital. Implementation Plan
 FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
1 Title Improving Wellness and Care Management with an Electronic Health Record System
 HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
A Multi-Prong Fall Awareness Program to Reduce the Occurrence of Falls in a Skilled Nursing Unit
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 A Multi-Prong
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 A Multi-Prong
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Innovation. Successful Outpatient Management of Kidney Stone Disease. Provider HealthEast Care System
 Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Caring for the Whole Patient Predictive Analytics Technology, Socio-demographic Insights, and Improved Patient Outcomes Randy K.
 WHITE PAPER Caring for the Whole Patient Randy K. Hawkins, MD Caring for the Whole Patient Socio-demographic data, not normally present in the electronic health record, and not routinely found in the hands
WHITE PAPER Caring for the Whole Patient Randy K. Hawkins, MD Caring for the Whole Patient Socio-demographic data, not normally present in the electronic health record, and not routinely found in the hands
Provider Guide. Medi-Cal Health Homes Program
 Medi-Cal Health Provider Guide This provider guide provides information on the California Medi-Cal Health (HHP) for Community-Based Care Management Entities (CB-CMEs), providers, community-based organizations,
Medi-Cal Health Provider Guide This provider guide provides information on the California Medi-Cal Health (HHP) for Community-Based Care Management Entities (CB-CMEs), providers, community-based organizations,
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017
 Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Hendrick Center for Extended Care. Community Health Needs Assessment Implementation Plan
 Hendrick Center for Extended Care Community Health Needs Assessment Implementation Plan - 2014-2016 Overview: Hendrick Center for Extended Care ( HCEC ) is a Long Term Acute Care Hospital, within Hendrick
Hendrick Center for Extended Care Community Health Needs Assessment Implementation Plan - 2014-2016 Overview: Hendrick Center for Extended Care ( HCEC ) is a Long Term Acute Care Hospital, within Hendrick
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
Clinical Operations. Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012
 Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
AACVPR Update for. Tom Draper, MBA, FAACVPR President, AACVPR
 AACVPR Update for Tom Draper, MBA, FAACVPR President, AACVPR Mission To reduce morbidity, mortality, and disability from cardiovascular and pulmonary disease through education, prevention, rehabilitation,
AACVPR Update for Tom Draper, MBA, FAACVPR President, AACVPR Mission To reduce morbidity, mortality, and disability from cardiovascular and pulmonary disease through education, prevention, rehabilitation,
PG snapshot Nursing Special Report. The Role of Workplace Safety and Surveillance Capacity in Driving Nurse and Patient Outcomes
 PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
Introduction and Executive Summary
 Introduction and Executive Summary 1. Introduction and Executive Summary. Hospital length of stay (LOS) varies markedly and persistently across geographic areas in the United States. This phenomenon is
Introduction and Executive Summary 1. Introduction and Executive Summary. Hospital length of stay (LOS) varies markedly and persistently across geographic areas in the United States. This phenomenon is
California Pacific Medical Center Outpatient Dialysis Transition Proposition Q Hearing San Francisco Health Commission September 7, 2010
 California Pacific Medical Center Outpatient Dialysis Transition Proposition Q Hearing San Francisco Health Commission September 7, 2010 Overview Presenter: Delvecchio Finley, FACHE Vice President,Operations
California Pacific Medical Center Outpatient Dialysis Transition Proposition Q Hearing San Francisco Health Commission September 7, 2010 Overview Presenter: Delvecchio Finley, FACHE Vice President,Operations
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
# December 29, 2000
 #00-53-3 December 29, 2000 Minnesota Department of Human Services 444 Lafayette Rd. St. Paul, MN 55155 OF INTEREST TO! County Social Service Directors/Supervisors! County Designated LMHA for PASRR! County
#00-53-3 December 29, 2000 Minnesota Department of Human Services 444 Lafayette Rd. St. Paul, MN 55155 OF INTEREST TO! County Social Service Directors/Supervisors! County Designated LMHA for PASRR! County
Cutting Avoidable Readmissions Starts in the Emergency Department
 WHITE PAPER Cutting Avoidable Readmissions Starts in the Emergency Department SMARTER EMERGENCY CARE: EVERYWHERE, EVERY TIME. Our experience and innovative approach offers smarter solutions for emergency
WHITE PAPER Cutting Avoidable Readmissions Starts in the Emergency Department SMARTER EMERGENCY CARE: EVERYWHERE, EVERY TIME. Our experience and innovative approach offers smarter solutions for emergency
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients
 Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients Overview of Project A drive to Population Health and changes in reimbursement have prompted the need to
Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients Overview of Project A drive to Population Health and changes in reimbursement have prompted the need to
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter