CPT Coding Basic Principles & Practice 2016
|
|
|
- Brittany Rich
- 6 years ago
- Views:
Transcription
1 CPT Coding Basic Principles & Practice 2016 Peter A. Hollmann, MD

2 Avoid this

3 And this


4 Somewhere between this


5 And this
6 Utility of Coding Systems Billing Research Quality Improvement Public Health Risk Adjustment (HCC) Predictive Modeling Productivity assessment/practice management
7 Key Systems to Know CPT AMA: to describe physician services HCPCS Level II CMS: supplies, selected procedures, PQRS (G codes) Place of Service Codes ICD-10 Diagnosis nomenclature (facilities use for procedures)
8 Payer policies It s Not Just Coding CMS is not the only payer Medicare Advantage plans match benefits, not payment rules Bundling, correct coding edits, globals Site of service, diagnosis, provider type Fee schedule differences Modifier acceptance Local Medicare contractor rules
9 CMS Medical Necessity In general, Medicare pays for services that are considered medically reasonable and necessary to the overall diagnosis and treatment of the patient s condition. Services or supplies are considered medically necessary if they: Are proper and needed for diagnosis or treatment of the patient s medical condition Are furnished for the diagnosis, direct care, and treatment of the patient s medical condition Meet standards of good medical practice and Are not mainly for convenience of the patient, provider, or supplier Medicare pays for provider professional services that are furnished in the U.S. and in the home, office, institution, or at the scene of an accident.
10 Important caveats Do not undercode nor upcode consider your profile It is not wrong to get paid for your service, but sometimes you will not Billing rules seem a lot like the tax code variability, risk/reward Medical necessity matters more than possible coding; coding is supported, not defined by documentation Insurance (especially Medicare) does not cover everything there is patient liability (ABN) Pay attention to your charges and payer fee schedules/allowances.
11 Freq Profiling Pattern Estab OV Distribution 2015 Medicare Level
12 CPT Updated annually to reflect changes in medicine Organized by body system logical sequence in general Evaluation & Management section Modifiers Clinical examples (early 1990 s) Unlisted procedures (select only accurate codes)
13 Medicare Proposed Rule July Final Rule November and Par Status HCPCS Codes Quarterly, but main changes effective January 1 Codes semi organized MedLearn Matters, Internet Only Manuals Benefits are Statutory
14 CPT/CMS etc Changes 2016 Transitional Care Management bill day of E/M Advance Care Planning Prolonged Clinical Staff Services (99415, 99416) Cerumen Removal (69209, 69210) Rules for Quality Programs (Value Based Purchasing) Fee Changes Annually check for coding and benefit changes and decide participation status
15 Participation Options Par: 100% PFS less copay and deductibles Nonpar/accept assignment: 95% less copay and deductibles Nonpar/ do not accept assignment: 115% of 95% (109.25%) and you must collect from patient Opt out: neither provider or beneficiary get Medicare funds
16 Overview to E/M Codes in CPT Place/type of service Key elements: History, exam, complexity of medical decision making Contributory: time, nature of presenting problem Select a level: Some services require all three components, some only two Definitions and documentation criteria Does it take a scorecard?
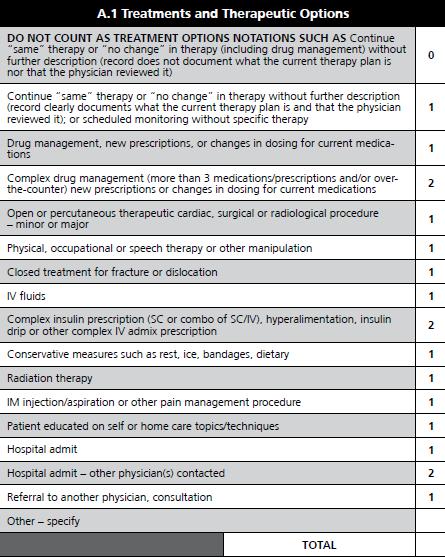
17 99214 (DG s) Hx Detail 4HPI 2-9 ROS PE Detail 6 Organ 2 each MDM Mod Mult Diags Mod Data 1/3 PFSH 2 organ 6 each Mod Risk TIME 25 KEY 2/3
18 Documentation Guideline Support clinical care Why is the patient present What was done in history and exam What were your thoughts What are you planning to do, did you do Credit is given for Hx elements when patient cannot provide info eg coma
19 Extent of History (CPT) Problem Focused: chief complaint; brief history of present illness or problem Expanded problem focused: chief complaint; brief history of present illness; problem pertinent system review Detailed: chief complaint; extended history of present illness; problem pertinent system review extended to include a review of a limited number of additional systems; pertinent past, family, and/or social history directly related to the patient s problems Comprehensive: chief complaint; extended history of present illness; review of systems which is directly related to the problem(s) identified in the history of the present illness plus a review of all additional body systems; complete past, family, and social history
20 Example: History 1997 DGs History Type HPI PFSH ROS EPF brief n/a Problem pertinent Detailed Extended Pertinent Extended ROS and PFSH may in HPI ROS and PFSH can be noted as no changes ROS and PFSH can be obtained on form if confirmed Brief HPI: Extended HPI: Pertinent ROS: Extended ROS: 1-3 elements* 4 or more elements the system directly related to the HPI direct and limited number of additional systems (2-9) *Elements: Location; quality; severity; duration; timing; context; modifying factors; associated signs/symptoms
21 Extent of Examination (CPT) Problem focused: a limited examination of the affected body area or organ system Expanded problem focused: a limited examination of the affected body area or organ system and other symptomatic or related organ system(s) Detailed: an extended examination of the affected body area(s) and other symptomatic or related organ system(s) Comprehensive: a general multi-system examination or a complete examination of a single organ system Note: preventive medicine evaluation and management service is multi-system, but its extent is based on age and risk factors identified
22 Medical Decision Making (CPT) Medical decision making refers to the complexity of establishing a diagnosis and/or selecting a management option as measured by: the number of possible diagnoses and/or the number of management options that must be considered; the amount and/or complexity of medical records, diagnostic tests, and/or other information that must be obtained, reviewed, and analyzed; and the risk of significant complications, morbidity, and/or mortality, as well as comorbidities, associated with the patient s presenting problem(s), the diagnostic procedure(s) and/or the possible management options.
23 Medical Decision Making (CPT) (Continued) Four types of medical decision making are recognized: straightforward; low complexity; moderate complexity; and high complexity. To qualify for a given type of decision making, two of the three elements in the following table must be met or exceeded. Cormorbidities/underlying diseases, in and of themselves, are not considered in selecting a level of E/M services unless their presence significantly increases the complexity of the medical decision making.
24 Number of Diagnoses or Management Options Complexity of Medical Decision Making Amount and/or Complexity of Data to be Reviewed Risk of Complications and/or Morbidity or Mortality Type of Decision Making minimal minimal or none minimal Straightforward limited limited low Low complexity multiple moderate moderate Moderate complexity extensive extensive high High complexity
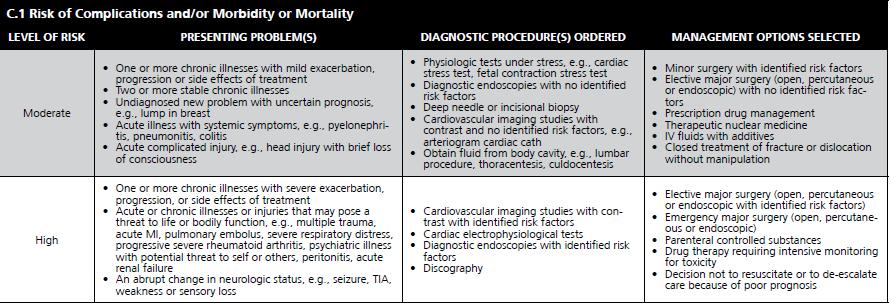
25 CMS DG Table of Risk Risk Level low Example 2 or more self limited 1 stable (e.g. HTN) minor acute (UTI) moderate 1 illness w/ exacerbation 2 chronic stable 1 Acute with systemic risk (e.g. pyelo)
26 Trailblazer Example Patient Condition (Medical Necessity) determines H/PE/MDM and assuming you provide appropriate care determines code Use Level 4 or 5 ONLY IF 3 or more problems managed OR A problem had 50%+ chance of worsening, death or disability Use Level 5 ONLY IF 4 or more problems managed OR A problem has 50%+ chance of worsening, death or disability
27 Trailblazer Pocket Guide Reiterates CMS 1995 or 1997 Documentation Guidelines Quantifies Medical Decision Making more specifically than the DGs.

28
29

30

31
32 Example: 99213, office or other outpatient visit 99213, office or other outpatient visit for the evaluation and management of an established patient, which requires at least two of these three key components: an expanded problem focused history; an expanded problem focused examination; medical decision made of low complexity Counseling and coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient s and/or family s needs. Usually, the presenting problem(s) are of low to moderate severity. Physicians typically spend 15 minutes face-to-face with the patient and/or family.
33 Big Picture Did not see physician/qhcp Did not need to see Stable problem All the geriatric patients Time based or need for complete reassessment
34 Time When counseling and/or coordination of care dominated (more than 50%) the physician/patient and/or family encounter (face-to-face time in the office or other outpatient setting or floor/unit time in the hospital or nursing facility), then time may be considered the key or controlling factor to qualify for a particular level of E/M services. This includes time spent with parties who have assumed responsibility for the care of the patient and decision making whether or not they are family members (e.g., foster parents, person acting in locum parentis, legal guardian). The extent of counseling and/or coordination of care must be documented in the medical record.
35 99213 Clinical Examples Office visit for the quarterly follow-up of a 45-yearold male with stable chronic asthma requiring regular drug therapy. (Allergy & Immunology) Office visit for a 62-year-old female, established patient, for follow-up for stable cirrhosis of the liver. (Internal Medicine/Family Medicine) Office visit for an 80-year-old female, established patient, to evaluate medical management of osteoarthritis of the temporomandibular joint. (Rheumatology)
36 Other Key Rules in E/M New (vs. established): new or not seen in 3 years, or if a group, it is a new/different specialty Consults: requested by a physician or other appropriate source (not patient or family) with written report back Consults can be done by you on your patients (ER, pre-op) CMS does not recognize Consult Codes Domicilliary Care is not Home Care Observation care/same day discharge Report OBS if same day discharge or facility designates OBS CMS expects >8 hrs for combined code Preventive Medicine ( ) is non-covered and billable to the beneficiary in traditional Medicare (be careful as most components are now covered). Admissions services typically bundle OV, ER services (see CPT) Hospital Discharge and Nursing facility Admission may be reported same day
37 E/M times are closest CPT vs. CMS CMS: Times are thresholds E/M codes mention face to face with the patient and/or family CMS: Patient must be present Prolonged Services Inpatient refer to unit time CMS: Count only face to face time?? Consultation Codes ( , ) Invalid for Medicare
38 Bundling, CCI, Modifiers Certain services or procedures are considered part of another service/procedure or in global period CMS uses Correct Coding Initiative claims systems edits Modifiers signal that CCI and other edits do not apply and must be used properly or it may be fraud/abuse
39 Modifier 25 Significant, Separately Identifiable Evaluation and Management Service by the Same Physician on the Same Day of the Procedure or Other Services: The physician may need to indicate that on the day a procedure or service identified by a CPT code was performed, the patient s condition required a significant, separately identifiable E/M service above and beyond the other service provided or beyond the usual preoperative and postoperative care associated the procedure that was performed. The E/M service may be prompted by the symptom or condition for which the procedure and/or service was provided. As such, different diagnoses are not required for reporting of the E/M services on the same date. This circumstance by be reported by addition the modifier 25 to the appropriate level of E/M service. Note: This modifier is not used to report an E/M service that resulted in a decision to perform surgery. See modifier 57.
40 Bill All Services Not just E/M codes Some are member liability (family conference) CPT procedure codes, G codes, supply/drugs Bill for all services of team (MNT, H&B) ($20.05) Critical Care codes Manpower shortage regions
41 Get up and Go/MMSE describes timed get up and go test Separately reported if. 15 minutes (8 minute threshold) Separate Written Report Otherwise is Physical Exam MMSE is NOT CNS testing It is PE
42 Coding Comprehensive Geriatric Assessment S Code: CGA and Planning by Team Coding by parts may be better Multiple visits or single visit / prolonged service Covered/non-covered services screenings, case management Teams Medical nutrition therapy neuropsych, health and behavior assessment PT/OT evaluations
43 Noncovered Services Advance beneficiary notice advised/ required --GY not covered --GA not necessary, ABN on file, written reason supplied Not all medically appropriate services are covered Rule of thumb: check fee schedule status
44 NON FACE TO FACE A major Source of Uncompensated Work Each Service has Pre and Post Time Most are not Bene Liability - Some are. Try to Tie the Work to a Billed Service CPT vs. CMS re: Family Family Psychotherapy (w/o patient present)
45 G0180 Tip: Home Health Certification Certification ($54.06) / 60d G0179 Recertification ($41.53) / 60d G : Physician [re-certification] [certification] services for Medicare-covered services provided by a participating home health agency (patient not present), including review of initial or subsequent reports of patient status, review of patient s responses to the Oasis assessment instrument, contact with the home health agency to ascertain the initial implementation plan of care, and documentation in the patient s office record, per certification period Documentation requirements not specified Not for MLP Date must match 485 start date
46 Face to Face Requirements Effective May 12, 2011 F2F encounter 90 days prior of 30 days thereafter Physician can certify, but encounter may be by NPP Hospital or SNF physician can certify and transfer Benefits Manual CH
47 Tip: CPO Hospice/HHA CMS rejected CPT due to time with nonprofessionals G0181 CPO-HHA ($108.85) G0182 CPO-Hospice ($109.20) G : Physician supervision of a patient receiving Medicare covered services provided by a participate [home health agency] [hospice](patient not present) requiring complex and multidisciplinary care modalities involving regular physician development and/or revision of care plans, review of subsequent reports of patient status, review of laboratory and other studies, communication (including telephone calls) with other health care professionals involved in the patient s car, integration of new information into the medical treatment plan and/or adjustment of medical therapy, within a calendar month, 30 minutes or more
48 Requirement for Modifier Hospice Enrollee Services require a GV or GW modifier GV Attending physician not employed or paid under arrangement by the patient's hospice provider GW Service not related to the hospice patient's terminal condition Deny claims for all other services related to the terminal illness furnished by individuals or entities other than the designated attending physician, who may be a nurse practitioner.
49 CPO Rules Requirement for a timesheet documenting over 30 minutes exclusive of certification and discussion with nonprofessionals (e.g., family) time No financial relationship with agency or hospice medical director Only one physician, not in post op global if surgeon Prior face to face encounter (was 6 months now 90d) 30 minutes/month minimum MLPs using their number may bill for these services Box 23 agency number Only Hospice and Home Health Covered G codes, not CPT
50 Transitional Care Management (99495, 99496) ICN Reflect work of reporting professional and clinical staff Day of D/C and next 29 days Report the date of service as 30 th day or day of F2F If dies before day 30 may not report If readmitted before day 30 may report MDM for the 30 days, not the E/M Place of service is where F2F occurs Home from Hospital or NF
51 TCM: Required Services Interactive contact within 2 business days of D/C (attempted) Face to Face service within 14 days Medication Reconciliation by the time of F2F visit MDM of at least Moderate Complexity over the 30 days not every patient

52 TCM: Code Selection New or Established Patient both the same Timing of F2F and MDM for month
53 TCM: Included/Separate Can report Discharge codes, but not use them as the required F2F by day 14 Only first F2F is bundled. Later E/M reported separately May not report CPO/Cert (no requirement that Home Care be in place either) 99495: $ :$ G0180+G0181= $ : add $ : add $100
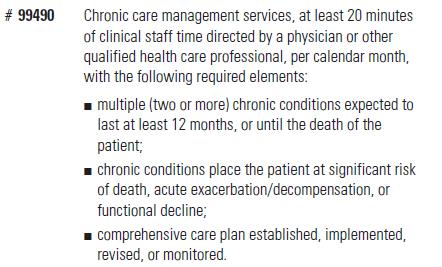
54 Chronic Care Management TCM and CCM codes created by CPT for 2013 Medicare accepts TCM and CCM is B status 2014 Fee Schedule CMS proposes paying a single G code for CCM of 20 minutes or more in a 30 days period, for persons with 2 or more chronic conditions Lots of other issues included, eg PCMH and EMR certification and no link to a face to face service Apparent goal was high volume, low dollar payments for a large proportion of beneficiaries CPT responds with Medicare code Value $42 54


55 Chronic Care Management 55
56 CCM and Complex CCM CODE # Chronic Conditions >2 >2 Duration of Conditions 12 months or until death 12 months or until death Clinical Staff Time > 20 minutes > 60 minutes Period of service Calendar Month Calendar Month Comprehensive Care Plan Established, implemented, revised or monitored Established or substantial revision MDM No requirement Moderate or High Medicare Payment $40.84 B Status 56

57 CCM- Who Qualifies 57
58 Role of Physician or QHCP Oversees the management and/or coordination of services, as needed, for: All medical conditions, Psychosocial needs and Activities of daily living Incident to By appropriately qualified clinical staff Or personally by provider 58

59 CCM Services 59

60 CCM Services 60
61 CCM Care Plan 61

62 CCM- Practice Requirements 62
63 CCM Initiation and Consent 63

64 CCM- EMR Requirements 64
65 CCM- EMR Requirements 65


66 CCM- EMR Requirements 66
67 CCM - Restrictions Not in an Advanced Primary Care Demonstration Project the Specific Patient Not with other Care Management Service Codes for same time period 67
")
68 CCM Resource (ICN May 2015) 68



69 Advance Care Planning ( ) 69
70 Advance Care Planning 70 For CY 2016, CMS has changed assignment of CPT codes and PFS status to indicator A, (defined as: Active code). The presence of an A indicator does not mean that Medicare has made a national coverage determination regarding the service. Contractors remain responsible for local coverage decisions in the absence of a national Medicare policy. Medicare allowance is $85.99 and $74.88 for and respectively.
71 Advance Care Plan 2016 Final Rule Separately payable with AWV; use modifier -33 so beneficiary has no cost sharing If done with AWV can also be a team service Also separately payable with E/M; use modifier -25 on E/M (does not include Critical Care) CMS allows that the service be incident to with some significant direct supervision 71
72 Final Rule
73 ACP - additional points Standard CPT Time Rules (more than ½ way to midpoint) Do not count any time that was part of determining level of E/M as ACP time Does not require execution of a legally recognized advance directive No predetermined frequency limits No specific special training/specialty restrictions 73
74 Tip: Incident To General rule: Incident To Billing Physician bills as the provider of service, even though major elements of the service were performed by MLP. The payment amount is at the physician level. Certain conditions must be met: MLP is employee Physician must provide direct personal supervision. In office this means being immediately available in office; inpatient use shared visit concept only. Physician must see patient if inpatient. No incident to for SNF. Physician must initiate course of treatment and remain involved in patient s care. All the supervision rules are independent of any licensure requirement, i.e., less restrictive licensure rules are irrelevant.
75 Nursing Facility Services Delegation to RNP/PA Physician may not delegate initial comprehensive assessment in SNF RNP/CNS/PA may perform services prior to initial comprehensive If state law allows, non facility level - employee may do initial comprehensive for NF level Employee RNP/CNS may not certify SNF. All NF certification rules up to state. (PAs now can certify) NO incident to or shared visits in SNF MedLearn Matters: SE0418
76 Tip: Prolonged Services First 29 minutes free Must be face-to-face ( ) Office and inpatient settings have their own set In addition to other services, including E/M at any level May be appropriate when multiple hospital visits are required as only one is allowed
77 TIP:TEAM CONFERENCES Team conference with patient present is E/M Can report as counseling and coordination of care Cautions documentation, same tax ID
78 Tip:Tobacco Cessation For services furnished on or after March 22, 2005, Medicare Part B covers two new levels of counseling -- intermediate and intensive -- for smoking and tobacco use cessation counseling. This coverage is beyond the minimal smoking and tobacco use cessation counseling that is already considered to be covered at each evaluation and management visit. Coverage is limited to beneficiaries who: Are competent and alert at the time services are provided and Use tobacco AND Have a disease or adverse health effect found by the U.S. Surgeon General to be linked to tobacco use or Are taking certain therapeutic agents whose metabolism or dosage is affected by tobacco use based on Food and Drug Administrationapproved information. Two cessation attempts are covered each year. Each attempt may include a maximum of 4 intermediate or intensive sessions, up to 8 sessions in a 12- month period ($13.95) 3-10 minutes; ($26.88) over 10 minutes
79 Preventive and Wellness Visits Initial Preventive Physical Exam First 12 months of enrollment First Annual Wellness Visit Only after first 12 months of enrollment Subsequent Annual Wellness Visit Is this a yearly physical? No Is IPPE and Initial AWV for established patients? Yes
80 Initial Preventive Physical Exam (IPPE) (G0402) Once per life within 12 months of effective date of Part B coverage. Fee $ Extensive: full H&P including modifiable risk factors, depression, function (minimally: hearing, falls, ADL, home safety, visual acuity, BMI, EOL) EKG (G0403-5) Not req d. Education/counseling with written plan for prevention services Can bill , modifier 25, also G codes except rectal Physicians and NPP s Medlearn Matters Number: MM6223
81 Initial Annual Wellness Visit (G0438) (ICN905706) History: HRA, Medical/FH; Risk/History Mood Disorder; ask or observe hearing, ADL, fall risk, home safety; Provider & Caregiver list Exam: BMI, BP, cognition Counsel: Written Screening Schedule 5-10 yrs, Risk Factors (incl. mental health), Personalized Health Advice (lifestyle, community resources, weight, physical activity, falls, nutrition $172.58; One per lifetime
82 Subsequent Wellness Visit (G0439) All elements same as initial, but updates only required $117.08; one per year
83 AWV and HRA Health risk assessment screening tool completed by patient workforhra.pdf Suggestions about what to use (not required to follow)
84 Services Separately Reported AWV Definition of Separately Identifiable and expectation of frequency Labs, EKG s, Immunizations (rules on co-pays and deductibles vary) Tobacco Cessation Many Preventive Services G Codes Screening Pap test/pelvic exam DRE ( except with IPPE)
85 It adds up Code Service Allowance G0402 IPPE $ G0436 Tobacco 3-10 min $14.68 G0437 Tobacco over 10 min $27.93 G0438 AWV Initial $ G0439 AWV Subseq $ G0442 Alcohol Screen $18.26 G0443 Alcohol Counsel $26.14 G0444 Depression Screen $18.26 G0445 STI Counseling $27.12 G0446 IBT for CVD $26.14 G0447 Obesity $26.14

86
87
88 Tobacco Counseling Preventative Benefit For those without symptoms of disease G0436 ($14.68), G0437 ($27.93) Must use diagnosis codes Four sessions, two attempts per year
89 Alcohol (MM 7633) Annual Screen (G0442) If positive then 4 brief F2F counseling visits (G0443) Misuse, not dependency Men 14/week or 4 on any occasion Women 7/week or 3 on any occasion Primary Care only 5 A s 99408, Invalid for Medicare
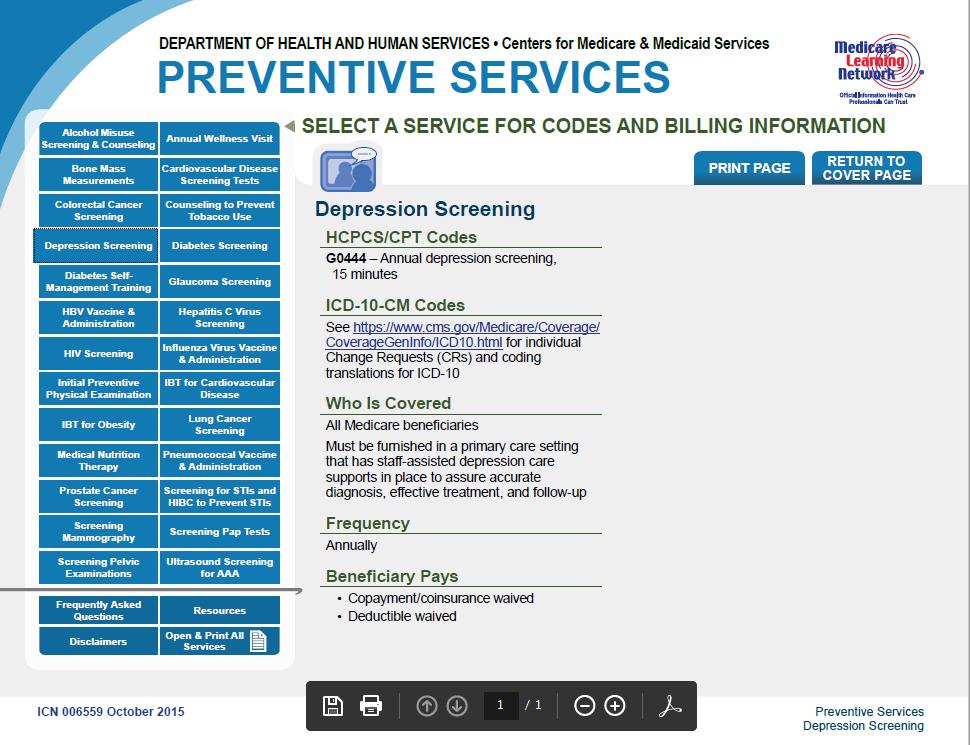
90 Depression Annual Screen (G0444) Primary Care Reviewed by Physician/NPP
91 Intensive Behavioral Therapy for Cardiovascular Disease G0446 One annually Intensive??? 15 minutes ASA BP check Counseling on diet, risk factors
92 IBT for Obesity (MM7641) >30 BMI, 22 visits max in 12 months G0447 ($26.14) 1 weekly F2F month one 1 QOW F2F months QMo F2F months 7-12, if lost 3 kg Dx codes for BMI Primary Care 5 A s
93 Preventive Services Challenges How do you know AWV history of services? Benefits for Preventive Visits and Cost Sharing Not always obvious or relevant Specifications for diagnosis AAA screen no longer ONLY if IPPE related Annual Physicals
94 Little things? ($73.04) vs ($108.13) ($73.40) vs ($108.13) ($104.91) vs 99291($225.93, office $277.44) ($100.97) and ($98.10)

95 Electronic Record Warning! Only you can select the correct code Replicate notes are gaining a lot of attention Documentation must reflect actual services, including review of unchanged areas Copy and Paste has other risk management issues
96 Resources CMS Website: cms.hhs.gov Medicare Physician Guide: A resource for Residents, Practicing Physicians and Other Health Care Professionals (Medicare Learning Network) AMA publications Contractor Medical Director AGS GAYF Coding page
97 Case One A 68-year-old female is seen in the office for follow-up treatment of diabetes and hypertension. History indicated that glucometer fasting readings run each morning. She has had no spells of weakness or diaphoresis and continues to tolerate her metformin. She follows her diet and saw the ophthalmologist for her routine exam last month. She is tolerating her lisinopril and has a mild cough, which does not bother her. She has no CP or SOB. She notes chronic left knee pain, worse with activity. No trauma. It is swelling a little. No fevers. Tylenol is ineffective.
98 On exam BP is 130/80, HR 68 Reg, weight is 142 stable, lungs clear, COR neg, ext no edema. Left knee FROM, stable, small effusion, no calor or erythema. The knee is tapped for 12cc of straw colored fluid and 40 mg of Aristospan and one cc of 1% lido are instilled. She is instructed to continue her current meds, to get a HgA1C and FBS. She is to report increased pain or redness in the knee or fever. She is to return in 3 months.
99 Questions Case 1 What E/M code should be reported? Are there any other codes for which you can get paid? Is a modifier necessary? What would one code if the whole reason the patient was there was to get an intraarticular injection?
100 Answers Case 1 What E/M code should be reported? D or PF history (ROS, PFSH), D or PF PE, Options/Data/Risk; 2/3; separation from injection A case can be made for or Are there any other codes for which you can get paid? 20610, J3303 (8 units) Is a modifier necessary? Modifier 25 on E/M What would one code if the whole reason the patient was there was to get an intra-articular injection? There is always some E/M in every procedure that is not separately reported.
101 Case Three Mrs. Smith is a 79-year-old woman with a history of CAD who presents to the office with a history of shortness of breath that is progressive. Last night she had chest heaviness and difficulty breathing. On exam she is tachypneic, has rales ½ way up and increased pedal edema. Her pulse ox is 78%. You call 911 and have the patient transported to the hospital. The ER is contacted, a med list and past EKG is faxed. She has been on ASA, a statin and metoprolol. You document the visit. After you finish with the other patients you go to the hospital.
102 You visit her in the hospital. A comprehensive history and exam are performed. Data indicates CHF and a small rise in troponin without EKG changes. By the time you see her she has been treated with nitrates, diuretics and ASA. She is more comfortable. Her BP is in the low 90 s systolic. Her glucose is 480 without an anion gap. Her urine had 4-10 WBCs.
103 Questions Case 3 What E/M is reported for the hospital admission? What E/M is reported for the office visit? What if you did the admission note the next day? What if your partner is on call for hospital admits and does the admit? What if your PA does the admit and then you come in later and complete the visit?
104 Answers Case 3 What E/M is reported for the hospital admission? 99223, see next question What E/M is reported for the office visit? All same day services roll up into one service, but was this critical care? Critical care can occur outside the ICU What if you did the admission note the next day? Report by date of service, not date of admission. You could report both outpatient and inpatient in this case. What if your partner is on call for hospital admits and does the admit? Your partner is the same as you What if your PA does the admit and then you come in later and complete the visit? Shared visit concept is applicable to inpatient care other than consults.
105 Case Four Mr. Atlas is a 68-year-old male who you last saw 4 years ago for a checkup. He states he feels great, walks 5 miles a day, lifts weights, but felt he should see you because he knew your daughter was in college and you had tuition payments to make. You review the interval history, which is negative. You confirm the past social and family histories. He does not smoke, only drinks if he goes out to dinner. He limits it to 2 glasses of wine. His diet does not include sodium rich foods and he never adds salt. A ROS checklist he filled out is negative and you confirm this. He never got a Pneumovax and his only medication is an aspirin a day, a multivitamin, and 400 IU of vitamin E. He has never had a colonoscopy or sig.
106 On exam, you note his BP to be This is confirmed in both arms and after rest. You do and document a complete PE which is all negative including a negative rectal exam and stool OB. His EKG is normal. You ask him to come back in a month for a follow-up visit. You ask him to stop by a couple of times to have his BP checked before then. You order a Hematocrit, fasting lipid panel and basic metabolic profile. You give him the Pneumovax.
107 Questions Case 4 What E/M code(s) are reported? Is this a new patient? What other codes are reported? Is this the IPPE exam? An Annual Wellness? Do I bill the patient or the payer?
108 Answers Case 4 What E/M code(s) are reported? for elevated BP, for Preventive Exam. Not HTN, but is elevated BP. If comes back for BP check 99211? Is this a new patient? Yes What other codes are reported? FOBT (CRC screen) not performed, stool OB not medically necessary; G0102 (prostate) performed, but cannot report with E/M (CCI edit); pneumovax admin G0009 (or CPT if not Medicare) and supply 90732; (EKG). Is this the IPPE exam? AWV? Not IPPE-not new to Medicare. Not AWV- services did not conform Do I bill the patient or the payer? Who is the payer? May get paid for BOTH and by some, one E/M by others. Medicare: bill to CMS and deduct charge for from charge for and bill patient the difference. Will this be allowed with AWV benefits?
109 Case Five You are a carrier medical director. You note that a local geriatrician new to practice is billing 90% of his visits at a level 5. While 30% are new patients, he is billing most of his follow-up exams at You ask for five records of patients who received more than one You note he has an electronic medical record. HPI was thorough. Each visit the doctor confirms medications, PFSH, and ROS. Each PE is extremely thorough and other than rectal/genital/breast exams is complete. One patient had moderate dementia with severe behavioral problems. Phone documentation was extensive between visits. Two patients had mild-moderate dementia and were fairly stable, seen every 3-4 months.
110 He documented good caregiver education. One patient had compensated CHF as her primary reason for visits every 3 months. Another patient had severe COPD and anxiety. Even when seen monthly, she still was in the ER a couple of times. The records documented ER contact and retrieval of labs/x-rays however, she actually was not unstable and it appeared she needed constant reassurance. The treatment course was not changing. The doctor indicates he uses an electronic record and the computer suggested visit codes.
111 Question Case 5 Is this physician coding correctly?
112 Answer Case 5 No. All services must be medically necessary to count for each key element. An electronic carry forward of problem lists and drug lists is not taking a history. Computers really cannot assess medical decision making and relevant elements of history or exam.
113 Case 6 A 74 y/o male is day 2 after being admitted for CP. You see him at 7AM and he is doing well on an increased dose of beta blocker and nitrates. You spent 17 minutes on the unit. Later that day he develops more CP and ST changes are noted. He is moved to the ICU, receives heparin and intravenous NTG. You return to the hospital. You spend 48 minutes on the unit reviewing records, history/exam, talking to the cardiologist and patient/family.
114 Questions Case 6 How do I report two visits on one day?
115 Answer Case 6 As a general rule only one E/M per day may be reported. Look at descriptor per day for inpatients. Two office visits can be reported, but will look like a duplicate claim. Hospital discharge and nursing facility admit same day may both be reported. Prolonged services may apply. (NB: NF is inpatient). Record your time. CMS rules all Prolonged Service is F2F only.
116 Case 7 A 83 y/o patient is treated by you at a hospital. You discharge her to a nursing home where you intend to follow her. This facility has a RNP who works with all staff physicians and is available to see patients on a daily basis. The RNP sees the patient that day and does a comprehensive assessment. You review the treatment plan with the RNP and plan to personally assess the patient in 48 hrs. When you come in you document a detailed history and perform a problem focused exam given the recent complete assessment in the hospital as well as that of the RNP. Your plan is for rehab services for her THR, continuation of anticoagulation therapy,
117 order checking of PVRs for follow-up of a question of retention, as well as continue her HTN treatment and consider whether she requires an antidepressant for some mood problems that you feel may be limiting her recovery.
118 Questions Case 7 How do I code when my service does not meet 3/3 elements? Is this a shared visit? Who gets to bill, me or the RNP or both? What if I saw the patient the day of admission?
119 Answers Case 7 How do I code when my service does not meet 3/3 elements? Unlisted codes are technically correct. Should you add nonsense documentation or just code or use 2/3? Is this a shared visit? There are no shared visits in the SNF/NF. Some may argue that you can confirm the key components of the RNP work in your documentation in selecting the correct E/M. Who gets to bill, me or the RNP or both? Same day only one could claim. An RNP may report services prior to the admission assessment, if medically necessary. What if I saw the patient the day of admission? See above
120 Teaching Rules No allowance for med students Bill for what you do, not what you write or rely upon combined documentation supports the code time based codes: your time only If primary care center can bill lower codes (1-3) Even if not present in room, prompt review 4:1, PGY over 6 months Psych must have visual. Surg must be present for key component of surgery Modifiers -GC resident involved -GE ambulatory care ctr, if physician not F2F
121 Teaching Rules Both residents and teaching physicians may document physician services in the patient s medical record. The documentation must be dated and contain a legible signature or identity and may be dictated and transcribed, typed, hand-written, or computer-generated. The attending physician who bills Medicare for evaluation and management (E/M) services in the teaching setting must, at a minimum, personally document his or her participation in the management of the patient and that he or she performed the service or was physically present during the critical or key portion(s) of the service performed by the resident (the resident s certification that the attending physician was present is not sufficient). Students may also document services in the patient s medical record. The teaching physician may refer only to a student s E/M documentation that is related to a review of systems (ROS) and/or past, family, and/or social history (PFSH). If the student documents E/M services, the teaching physician must verify and repeat documentation of the physical examination and medical decision making activities of the service.
122 Teaching Rules For initial hospital care, emergency department visits, office visits for new patients, and office and hospital consultations, the teaching physician must enter a personal notation that demonstrates the appropriate level of service that the patient requires and documents his or her participation in the three key components. The three key components are history, examination, and medical decision making. If the teaching physician repeats key elements of the service components that the resident previously obtained and documented, his or her note may be brief, summarize comments that relate to the resident s entry, and confirm or revise these key elements: Relevant history of present illness (HPI) and prior diagnostic tests Major finding(s) of the physical examination Assessment, clinical impression, or diagnosis and Plan of care
123 Teaching Rules For subsequent hospital care and office visits for established patients, the teaching physician must enter a personal notation that highlights two of the three key components of these services. These components are history, physical examination, and medical decision making. For follow-up visits for established patients, the guidelines for initial hospital care, emergency department visits, office visits for new patients, and office and hospital consultations guidelines must also be followed.
124 Teaching Rules Medicare may grant a primary care exception within an approved Graduate Medical Education Program in which the teaching physician is paid for certain E/M services the resident performs when the teaching physician is not present. The primary care exception applies to the following lower and mid-level E/M services: New Patient - CPT Codes 99201, 99202, and and Established Patient - CPT Codes 99211, 99212, and Effective January 1, 2005, the primary care exception also applies to the initial preventive physical examination, also known as the Welcome to Medicare Physical - Healthcare Common Procedure Coding System code G3044, the initial preventive physical examination, face-to-face visit, services limited to new beneficiary during the first six months of Medicare enrollment.
3/28/2016. Evaluation and Management. Evaluation and Management Emerging Trends. Disclosures. Evaluation and Management The History
 Evaluation and Management Emerging Trends Peter Hollmann MD Past CPT Panel Chair Disclosures Ambassador for AMA CPT Member RBRVS Update Committee 2 Evaluation and Management The History Evaluation and
Evaluation and Management Emerging Trends Peter Hollmann MD Past CPT Panel Chair Disclosures Ambassador for AMA CPT Member RBRVS Update Committee 2 Evaluation and Management The History Evaluation and
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
Coding and Billing for Lifestyle Medicine
 Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21.
 How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21. If only some of the charges are noncovered, per CMS Internet-Only Manual,
How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21. If only some of the charges are noncovered, per CMS Internet-Only Manual,
Reimbursement Environment
 Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
Evaluation and Management
 Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Presented for the AAPC National Conference April 4, 2011
 Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
TIPS FROM OUR CONSULTANT By: Joy Newby, LPN, CPC, PCS Newby Consulting
 TIPS FROM OUR CONSULTANT By: Joy Newby, LPN, CPC, PCS Newby Consulting CONFUSED ABOUT MEDICARE PREVENTATIVE VISITS? SO ARE YOUR PATIENTS! Congress legislated coverage for two preventive visits for Medicare
TIPS FROM OUR CONSULTANT By: Joy Newby, LPN, CPC, PCS Newby Consulting CONFUSED ABOUT MEDICARE PREVENTATIVE VISITS? SO ARE YOUR PATIENTS! Congress legislated coverage for two preventive visits for Medicare
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule. Grace Wilson, RHIA
 Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Evaluation and Management Auditing Back to the Basics. Objectives. Audit Start with the benchmarks CMS MEDPAR by specialty 4/22/2013
 Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
See the Time chapter for complete instructions regarding how to code using time as the controlling E/M factor.
 2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
E/M Auditing: History is the Key
 E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
PEARLS OF THE ACC CV SUMMIT: THOUGHTS FROM THE OYSTER BED OF CLINICAL PRACTICE
 PEARLS OF THE ACC CV SUMMIT: THOUGHTS FROM THE OYSTER BED OF CLINICAL PRACTICE IN-ACC October 13, 2018 Linda Gates-Striby CCS-P, ACS-CA St. Vincent Medical Group Director Quality Assurance Lggates@ascension.org
PEARLS OF THE ACC CV SUMMIT: THOUGHTS FROM THE OYSTER BED OF CLINICAL PRACTICE IN-ACC October 13, 2018 Linda Gates-Striby CCS-P, ACS-CA St. Vincent Medical Group Director Quality Assurance Lggates@ascension.org
IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY
 Global Surgery Policy Number GLS03272013RP Approved By UnitedHealthcare Medicare Committee Current Approval Date 04/09/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
Global Surgery Policy Number GLS03272013RP Approved By UnitedHealthcare Medicare Committee Current Approval Date 04/09/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
The World of Evaluation and Management Services and Supporting Documentation
 The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
Evaluation and Management Services
 Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
E & M Coding. Welcome To The Digital Learning Center. Today s Presentation. Course Faculty. Beyond the Basics. Presented by
 Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Procedure Code Job Aid
 Procedure Code 99211 Job Aid Definition for 99211: Office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician. Usually,
Procedure Code 99211 Job Aid Definition for 99211: Office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician. Usually,
Start with the Problem
 Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Leveraging Wellness Visit with Medicare: Improving Income and Patient Outcomes
 Leveraging Wellness Visit with Medicare: Improving Income and Patient Outcomes Overview Why Medicare Wellness Exams What are the Medicare Wellness Exams Annual Wellness Exam Components What is covered
Leveraging Wellness Visit with Medicare: Improving Income and Patient Outcomes Overview Why Medicare Wellness Exams What are the Medicare Wellness Exams Annual Wellness Exam Components What is covered
Getting Paid for What You Do! Coding 2010
 Getting Paid for What You Do! Coding 20 Children s Mercy Health Network 11/17/09 Richard H. Tuck, MD, FAAP Disclosure I have financial relationships or interests with proprietary entities producing health
Getting Paid for What You Do! Coding 20 Children s Mercy Health Network 11/17/09 Richard H. Tuck, MD, FAAP Disclosure I have financial relationships or interests with proprietary entities producing health
2019 Evaluation and Management Coding Advisor. Advanced guidance on E/M code selection for traditional documentation systems
 2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
E/M: Coding Opportunities- Documentation is key
 E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
Are they coming to get you! Todd Thomas, CCS-P
 Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Provider-Based RHC Billing June 8, 2018
 Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
9/17/2018. Place of Service Type of Service Patient Status
 Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Primary Care Setting Behavioral Health Billing Codes
 Primary Care Setting s Medicaid Medicare Third Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though
Primary Care Setting s Medicaid Medicare Third Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though
Medicare Preventive Services
 Medicare Preventive Services Presented by Part B Provider Outreach & Education December 16, 2015 Event Instructions Today s event is a teleconference Slides will not be advanced during the presentation
Medicare Preventive Services Presented by Part B Provider Outreach & Education December 16, 2015 Event Instructions Today s event is a teleconference Slides will not be advanced during the presentation
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011
 PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
FQHC Behavioral Health Billing Codes
 FQHC s Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though process clearly reflected in assessment
FQHC s Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though process clearly reflected in assessment
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
1:35. NPP April Young Medical Consulting, LLC. Non-Physician Practitioner Coding and Billing. Disclaimer
 Non-Physician Practitioner Coding and Billing Jill Young - CPC, CEDC, CIMC, East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing. The information
Non-Physician Practitioner Coding and Billing Jill Young - CPC, CEDC, CIMC, East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing. The information
How does one report the performance of both a screening mammogram on the right breast and a diagnostic on the left breast at the same encounter?
 1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
Advanced Evaluation and. AAPC Regional Conference Chicago 10/27/12
 Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Deleted Codes. Agenda 1/31/ E/M Codes Deleted Codes New Codes Changed Codes
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February Jean C. Russell, MS, RHIT Richard Cooley, BA, CCS
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
Charting for Midwives. Getting Credit For the Work You Do
 Charting for Midwives Getting Credit For the Work You Do Moving Beyond S.O.A.P. The U.S. health care system is moving past fee-for-service billing. In the future, the providers will be reimbursed based
Charting for Midwives Getting Credit For the Work You Do Moving Beyond S.O.A.P. The U.S. health care system is moving past fee-for-service billing. In the future, the providers will be reimbursed based
Preventive and Sick Visits Same Day. Objectives
 Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
PREVENTIVE MEDICINE AND SCREENING POLICY
 UnitedHealthcare Oxford Reimbursement Policy PREVENTIVE MEDICINE AND SCREENING POLICY Policy Number: ADMINISTRATIVE 238.19 T0 Effective Date: July 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
UnitedHealthcare Oxford Reimbursement Policy PREVENTIVE MEDICINE AND SCREENING POLICY Policy Number: ADMINISTRATIVE 238.19 T0 Effective Date: July 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
RHC Billing for Provider-Based RHCs. Charles A. James, Jr. President and CEO North American Healthcare Management Services
 RHC Billing for Provider-Based RHCs Charles A. James, Jr. President and CEO North American Healthcare Management Services Presentation Objectives Provider-Based Requirements Provider-based Enrollment Issues
RHC Billing for Provider-Based RHCs Charles A. James, Jr. President and CEO North American Healthcare Management Services Presentation Objectives Provider-Based Requirements Provider-based Enrollment Issues
RHC Billing RHC and nonrhc Services Janet Lytton, Director of Reimbursement Rural Health Development
 RHC Billing RHC and nonrhc Services Janet Lytton, Director of Reimbursement Rural Health Development 308-647-6455 janet.lytton@rhdconsult.com SEPTEMBER 18, 2014 1 Understand the billing of the various
RHC Billing RHC and nonrhc Services Janet Lytton, Director of Reimbursement Rural Health Development 308-647-6455 janet.lytton@rhdconsult.com SEPTEMBER 18, 2014 1 Understand the billing of the various
Observation Coding and Billing Compliance Montana Hospital Association
 Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
9/17/2018. Critical to Practices
 Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Reporting Preventive Services & Problem-Oriented E & M in RHCs
 Reporting Preventive Services & Problem-Oriented E & M in RHCs John Burns, CPMA, CEMC, CPC, CPC-I Vice President, Audit and Compliance Services John.Burns@RuralHealthCoding.com Your Faculty John F. Burns,
Reporting Preventive Services & Problem-Oriented E & M in RHCs John Burns, CPMA, CEMC, CPC, CPC-I Vice President, Audit and Compliance Services John.Burns@RuralHealthCoding.com Your Faculty John F. Burns,
Coding Guidance for HIV Clinical Practices: Care Management Services
 Coding Guidance for HIV Clinical Practices: Care Management Services HIV medical practices and clinicians provide many services outside of a face-to-face encounter with a patient. Some of these services
Coding Guidance for HIV Clinical Practices: Care Management Services HIV medical practices and clinicians provide many services outside of a face-to-face encounter with a patient. Some of these services
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
Telehealth. Administrative Process. Coverage. Indications that are covered
 Telehealth These services may or may not be covered by your HealthPartners plan. Please see your plan documents for your specific coverage information. If there is a difference between this general information
Telehealth These services may or may not be covered by your HealthPartners plan. Please see your plan documents for your specific coverage information. If there is a difference between this general information
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice
 Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC
 Service in RHC") How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
February Jean C. Russell, MS, RHIT Richard Cooley, BA, CCS
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
Rural Health Clinic Overview
 TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC Disclaimer
 Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
Coding and Billing with Confidence! Elizabeth Keltner, CPC, CHCA MCW Compliance Education Coordinator
 2016 Winter Refresher Course Coding and Billing with Confidence! Elizabeth Keltner, CPC, CHCA MCW Compliance Education Coordinator Disclosure The Speaker Has No Financial Relationships to Disclose 2 1
2016 Winter Refresher Course Coding and Billing with Confidence! Elizabeth Keltner, CPC, CHCA MCW Compliance Education Coordinator Disclosure The Speaker Has No Financial Relationships to Disclose 2 1
Everybody s Favorite Form: New Advance Beneficiary Notice of Noncoverage (ABN) Form Begins in 2012
 Form Begins in 2012") Everybody s Favorite Form: New Advance Beneficiary Notice of Noncoverage (ABN) Form Begins in 2012 NOTE: We have just added an educational webinar on using the ABN form. This is an expanded webinar with
Everybody s Favorite Form: New Advance Beneficiary Notice of Noncoverage (ABN) Form Begins in 2012 NOTE: We have just added an educational webinar on using the ABN form. This is an expanded webinar with
Initial Preventive Physical Examination (IPPE) Presented by Provider Outreach and Education (POE) December 2016
 Presented by Provider Outreach and Education (POE) December 2016") Initial Preventive Physical Examination (IPPE) Presented by Provider Outreach and Education (POE) December 2016 DISCLAIMER This information release is the property of Noridian Healthcare Solutions, LLC
Initial Preventive Physical Examination (IPPE) Presented by Provider Outreach and Education (POE) December 2016 DISCLAIMER This information release is the property of Noridian Healthcare Solutions, LLC
Protocol: Name of supervising ED provider: Name of RDTC Faculty: Disposition: Date: / / Time: : (military)
") RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
Specific Payment Codes for the Federally Qualified Health Center (FQHC) PPS
 PPS") Specific Payment Codes for the Federally Qualified Health Center (FQHC) PPS In accordance with Section 1834(o)(1)(A) and 1834(o)(2)(C) of the Social Security Act, we established specific payment codes
Specific Payment Codes for the Federally Qualified Health Center (FQHC) PPS In accordance with Section 1834(o)(1)(A) and 1834(o)(2)(C) of the Social Security Act, we established specific payment codes
E/M Fast Finder. CPT only 2012 American Medical Association. 1 All Rights Reserved.
 E/M Fast Finder The E/M Fast Finder is a carry-along reference to assist in assigning the Evaluation and Management (E/M) codes that are part of the 99000 series of Current Procedural Terminology (CPT
E/M Fast Finder The E/M Fast Finder is a carry-along reference to assist in assigning the Evaluation and Management (E/M) codes that are part of the 99000 series of Current Procedural Terminology (CPT
See the Time chapter for complete instructions on how to code using time as the controlling factor when selecting an E/M code.
 2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid s MLN Matters Number: MM9269 Revised Related CR Release : January 26, 2016 Related Transmittal #: R1596OTN Change Request (CR) #:
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid s MLN Matters Number: MM9269 Revised Related CR Release : January 26, 2016 Related Transmittal #: R1596OTN Change Request (CR) #:
Care Plan Oversight Services and Physician Services for Certification
 Education Makes the Difference Care Plan Oversight Services and Physician Services for Certification and Recertification of Medicare-Covered Home Health Services A CMS CONTRACTED INTERMEDIARY CARRIER The
Education Makes the Difference Care Plan Oversight Services and Physician Services for Certification and Recertification of Medicare-Covered Home Health Services A CMS CONTRACTED INTERMEDIARY CARRIER The
Billing and Coding Tidbits for Not Leaving $$ on the Table
 Billing and Coding Tidbits for Not Leaving $$ on the Table Presented by Sarah Reed BSE, CPC, CPC-I Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Presentation Objectives Review some
Billing and Coding Tidbits for Not Leaving $$ on the Table Presented by Sarah Reed BSE, CPC, CPC-I Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Presentation Objectives Review some
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Global Surgery Fact Sheet
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Global Surgery Fact Sheet Definition of a Global Surgical Package This fact sheet is designed to provide education on the
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Global Surgery Fact Sheet Definition of a Global Surgical Package This fact sheet is designed to provide education on the
Documenting & Coding for Compliance
 Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
BILLING AND CODING IN POST-ACUTE AND LONG-TERM CARE CONTINUUM ALVA S. BAKER, MD, CMDR, HMDC
 BILLING AND CODING IN POST-ACUTE AND LONG-TERM CARE CONTINUUM ALVA S. BAKER, MD, CMDR, HMDC SPEAKER DISCLOSURES Dr. Baker has disclosed that he has no relevant financial relationship(s). LEARNING OBJECTIVES:
BILLING AND CODING IN POST-ACUTE AND LONG-TERM CARE CONTINUUM ALVA S. BAKER, MD, CMDR, HMDC SPEAKER DISCLOSURES Dr. Baker has disclosed that he has no relevant financial relationship(s). LEARNING OBJECTIVES:
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation
 A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
Statement of Financial Responsibility
 Statement of Financial Responsibility Patient Name: Date: Acct : BIR JV, LLP including; Out-Patient, In-Patient and, Home Health Rehab appreciates the confidence you have shown in choosing us to provide
Statement of Financial Responsibility Patient Name: Date: Acct : BIR JV, LLP including; Out-Patient, In-Patient and, Home Health Rehab appreciates the confidence you have shown in choosing us to provide
Coding Guidelines for Certain Respiratory Care Services January 2018 (updates in red)
") Coding Guidelines for Certain Respiratory Care Services (updates in red) Overview From time to time the AARC receives inquiries about respiratory-related coding and coverage issues through its Help Line
Coding Guidelines for Certain Respiratory Care Services (updates in red) Overview From time to time the AARC receives inquiries about respiratory-related coding and coverage issues through its Help Line
Medical Decision Making
 Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
Coding for the Practitioner
 Coding for the Practitioner Prepared for Coalition of State Rheumatology Organizations National Rheumatology Fellows Conference February 2018 Presented by: Jean Acevedo, LHRM, CPC, CHC, CENTC Disclaimer
Coding for the Practitioner Prepared for Coalition of State Rheumatology Organizations National Rheumatology Fellows Conference February 2018 Presented by: Jean Acevedo, LHRM, CPC, CHC, CENTC Disclaimer
2/28/2017 NO DISCLOSURES. K 1/Partner
 NO DISCLOSURES LaMon Norton NP Participant will recognize origin & role of Relative Value Unit (RVU) in coding and reimbursement. Participant will be able to link documentation points to coding and RVU
NO DISCLOSURES LaMon Norton NP Participant will recognize origin & role of Relative Value Unit (RVU) in coding and reimbursement. Participant will be able to link documentation points to coding and RVU
Third Party Payer Days. IMGMA February 25, 2015
 Third Party Payer Days IMGMA February 25, 2015 Agenda 2015 Medicare Physician Fee Schedule Medicare Physician Fee Schedule Database Transitional Care Management - Reminder Medicare - Coverage Guidelines
Third Party Payer Days IMGMA February 25, 2015 Agenda 2015 Medicare Physician Fee Schedule Medicare Physician Fee Schedule Database Transitional Care Management - Reminder Medicare - Coverage Guidelines
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT
 Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Focus On Observation
 Focus On Observation Introduction CPT and CMS Requirements CPT Codes Documentation Requirements Observation Coding: Facility Considerations 2 LogixHealth s unsurpassed service stems from the fact that
Focus On Observation Introduction CPT and CMS Requirements CPT Codes Documentation Requirements Observation Coding: Facility Considerations 2 LogixHealth s unsurpassed service stems from the fact that
Message Response Message
 Message If established pt wouldn't 2 out of 3 still require the level for slide 5? Response Message Can you re-state your question? I am unclear on what you are asking. Thanks You stated that even when
Message If established pt wouldn't 2 out of 3 still require the level for slide 5? Response Message Can you re-state your question? I am unclear on what you are asking. Thanks You stated that even when
Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT
 1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
The In and Out of the Medicare Two Midnight Rule. Disclaimer. Objectives 3/31/2014
 The In and Out of the Medicare Two Midnight Rule Brenda Keeling, RN, CPHQ, CCM Patient Response, Inc. 1 Disclaimer Information enclosed was current at the time it was presented. Medicare policy changes
The In and Out of the Medicare Two Midnight Rule Brenda Keeling, RN, CPHQ, CCM Patient Response, Inc. 1 Disclaimer Information enclosed was current at the time it was presented. Medicare policy changes
JOHNS HOPKINS HEALTHCARE
 Page 1 of 16 ACTION: New Policy Effective Date: 10/01/2013 Revising : Review Dates: 03/29/16, 06/29/17, Superseding 09/01/17, 12/01/17 Archiving Retiring Johns Hopkins HealthCare LLC (JHHC) provides a
Page 1 of 16 ACTION: New Policy Effective Date: 10/01/2013 Revising : Review Dates: 03/29/16, 06/29/17, Superseding 09/01/17, 12/01/17 Archiving Retiring Johns Hopkins HealthCare LLC (JHHC) provides a
PSYCHIATRY SERVICES: MD FOCUSED
 PSYCHIATRY SERVICES: MD FOCUSED CY2013 Risk Based Scheduled Review Agenda 2 Overview of New Risk Based Scheduled Reviews Initial review findings PhD summary MD summary Examples Template/Psychotherapy Time
PSYCHIATRY SERVICES: MD FOCUSED CY2013 Risk Based Scheduled Review Agenda 2 Overview of New Risk Based Scheduled Reviews Initial review findings PhD summary MD summary Examples Template/Psychotherapy Time
MLN Matters Number: MM6740 Revised Related Change Request (CR) #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010
 #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010") News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
ELIGIBILITY & CERTIFICATION THE CONTINUING SAGA
 1 ELIGIBILITY & CERTIFICATION THE CONTINUING SAGA Hospice Fundamentals Charlene Ross, MSN, MBA, RN Consultant / Educator 2 What You Will Learn Today The regulatory requirements of certification, recertification
1 ELIGIBILITY & CERTIFICATION THE CONTINUING SAGA Hospice Fundamentals Charlene Ross, MSN, MBA, RN Consultant / Educator 2 What You Will Learn Today The regulatory requirements of certification, recertification
ICD-9 (Diagnosis) Coding
 Coding") 1 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University.
1 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University.
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Transitional Care Management We provide these services a-la-carte...
 Transitional Care Management We provide these services a-la-carte... Initial Patient Outreach* This must be done within 2 days of the patient s discharge from the hospital. During this call patient s medications
Transitional Care Management We provide these services a-la-carte... Initial Patient Outreach* This must be done within 2 days of the patient s discharge from the hospital. During this call patient s medications
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM. November 20, 2015
 THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
Rural Health Clinic Billing
 Critical Access Hospital and Rural Health Clinic Billing September 12, 2017 1 Rural Health Clinic Overview Rural Health Clinic Services Preventive Services in the RHC Non-RHC Services/Non-Covered Services
Critical Access Hospital and Rural Health Clinic Billing September 12, 2017 1 Rural Health Clinic Overview Rural Health Clinic Services Preventive Services in the RHC Non-RHC Services/Non-Covered Services