BILLING AND CODING IN POST-ACUTE AND LONG-TERM CARE CONTINUUM ALVA S. BAKER, MD, CMDR, HMDC
|
|
|
- Samson Barrett
- 6 years ago
- Views:
Transcription

1 BILLING AND CODING IN POST-ACUTE AND LONG-TERM CARE CONTINUUM ALVA S. BAKER, MD, CMDR, HMDC
2 SPEAKER DISCLOSURES Dr. Baker has disclosed that he has no relevant financial relationship(s).
3 LEARNING OBJECTIVES: By the end of the presentation, participants will be able to: 1. Describe the differences in billing related to Place of Service 2. Delineate constraints on visit services for patients receiving Medicare Part A benefits 3. Review recent changes in billing and coding requirements
4 Billing and Coding in Post-Acute and Long-Term Care Continuum DESCRIBE THE DIFFERENCES IN BILLING RELATED TO PLACE OF SERVICE OBJECTIVE 1
5
6
7
8 PA/LTC BILLING CODES Code Time History Exam Decision Initial Det/Comp Det/Comp Strt/Low Comp Comp Moderate Comp Comp High Subsequent Prob. Foc. Prob. Foc. Straight Exp. PF Exp. PF Low Detailed Detailed Moderate Comp Comp High =<30 xxx xxx xxx >30 xxx xxx xxx Detailed Comp Low/Mod


9 PA/LTC BILLING CODES Initial/Subsequent vs. New/Established care codes Initial/Subsequent PA/LTC New/Established Office/Hospital/etc. Admission/episode of care Longitudinal relationship
10 PA/LTC BILLING CODES Other recurrent troublesome concepts All codes apply both SNF and NF All require face-to-face visit Medical necessity must be documented Physician must do initial evaluation in SNF (POS 31); NPP may do in NF (POS 32) NPP visit in SNF prior to MD eval is billed as subsequent care Documentation for visit must include adequate E/M items as required for code
11 Billing and Coding in Post-Acute and Long-Term Care Continuum DELINEATE CONSTRAINTS ON VISIT SERVICES FOR PATIENTS RECEIVING MEDICARE PART A BENEFITS OBJECTIVE 2
12
13
14 14 MEDICARE CLAIMS PROCESSING MANUAL, PUB SEC Selection of Level of Evaluation and Management Service A. Use of CPT Codes Medical necessity of a service is the overarching criterion for payment in addition to the individual requirements of a CPT code. The volume of documentation should not be the primary influence upon which a specific level of service is billed. Documentation should support the level of service reported. AMDA White Paper
15 15 MEDICARE CLAIMS PROCESSING MANUAL, PUB , Nursing Facility Services Medically Necessary Visits Medically necessary E/M visits for the diagnosis or treatment of an illness or injury or to improve the functioning of a malformed body member are payable under the physician fee schedule under Medicare Part B
16 16 VISITS BY QUALIFIED NONPHYSICIAN PRACTITIONERS State Regulations, State Scope of Practice All E/M visits shall be within the State scope of practice and licensure requirements where the visit is performed and all the requirements for physician collaboration and physician supervision shall be met when performed and reported by qualified NPPs. General physician supervision and employer billing requirements shall be met for PA services in addition to the PA meeting the State scope of practice and licensure requirements where the E/M visit is performed.
17 17 VISITS BY QUALIFIED NONPHYSICIAN PRACTITIONERS Medically Necessary Visits Qualified NPPs may perform medically necessary E/M visits prior to and after the physician s initial visit in both the SNF and NF. A physician or NPP may bill the most appropriate initial nursing facility care code (CPT codes ) or subsequent nursing facility care code (CPT codes ), even if the E/M service is provided prior to the initial federally mandated visit.
18 A VISITS TO PERFORM THE INITIAL COMPREHENSIVE ASSESSMENT AND ANNUAL ASSESSMENTS Definition of Initial Federally Mandated Visit is: the initial comprehensive visit during which the physician: completes a thorough assessment, develops a plan of care, and writes or verifies admitting orders for the nursing facility resident.
19 A VISITS TO PERFORM THE INITIAL COMPREHENSIVE ASSESSMENT AND ANNUAL ASSESSMENTS Prior to/ after Initial Federally Mandated Visit: other medically necessary E/M visits may be performed and reported prior to and after the initial visit, if the medical needs of the patient require an E/M visit. Qualified NPP may perform. Medically necessary E/M visits for the diagnosis or treatment of an illness or injury or to improve the functioning of a malformed body member are payable under the physician fee schedule under Medicare Part B.
20 A VISITS TO PERFORM THE INITIAL COMPREHENSIVE ASSESSMENT AND ANNUAL ASSESSMENTS READMISSION A readmission to a SNF or NF shall have the same payment policy requirements as an initial admission in both the SNF and NF settings. Definition of readmission unclear Patient needs to be officially discharged from the facility to be able to use another Initial Visit code, otherwise a Subsequent Visit code should be used
21 21 MEDICARE CLAIMS PROCESSING MANUAL, PUB Nursing Facility Services B. Visits to Comply With Federal Regulations (42 CFR ) Payment is made under the physician fee schedule by Medicare Part B for federally mandated visits. Following the initial federally mandated visit by the physician, or qualified NPP where permitted, payment shall be made for federally mandated visits that monitor and evaluate residents at least once every 30 days for the first 90 days after admission and at least once every 60 days thereafter. Subsequent Nursing Facility Care, per day, ( ) shall be used to report federally mandated physician E/M visits and medically necessary E/M visits.
22 22 MEDICARE CLAIMS PROCESSING MANUAL, PUB Nursing Facility Services B. Visits to Comply With Federal Regulations (42 CFR ) Medicare Part B payment policy does not pay for additional E/M visits that may be required by State law for a facility admission or for other additional visits to satisfy facility or other administrative purposes.
23 I SNF/NF DISCHARGE DAY MANAGEMENT Requires a face-to-face visit Reported for the date of the actual visit by the physician or qualified NPP even if the patient is discharged from the facility on a different calendar date
24 I SNF/NF DISCHARGE DAY MANAGEMENT Death may be reported using CPT code or 99316, depending on the code requirement, for a patient who has expired, but only if the physician or qualified NPP personally performed the death pronouncement.
25 25 VISITS BY QUALIFIED NONPHYSICIAN PRACTITIONERS Federally Mandated Visits SNF (31) Following the initial federally mandated visit by the physician, the physician may delegate alternate federally mandated physician visits to a qualified NPP who meets collaboration and physician supervision requirements and is licensed as such by the State and performing within the scope of practice in that State.
26 26 VISITS BY QUALIFIED NONPHYSICIAN PRACTITIONERS Federally Mandated Visits NF (32) Per the regulations at 42 CFR (f), a qualified NPP, who meets the collaboration and physician supervision requirements, the State scope of practice and licensure requirements, and who is not employed by the NF, may at the option of the State, perform the initial federally mandated visit in a NF, and may perform any other federally mandated physician visit in a NF in addition to performing other medically necessary E/M visits.
27 27 Order to Admit Admission Treatment Orders Initial Comprehe nsive Visit Other Required Visits SNF PA, NP & CNS employed by facility N N N PA, NP & CNS not a facility employee N N N Y (alternate) Y (alternate) NF PA, NP, CNS employed by facility N N N N PA, NP, CNS not a facility employee Y Y Y Y
28 28 SNF Other Medically Necessary Visits Other Medically Necessary Orders Certification/ Recertificatio n PA, NP & CNS employed by facility Y Y N PA, NP & CNS not a facility employee Y Y Y NF PA, NP, CNS employed by facility Y Y NA PA, NP, CNS not a facility employee Y Y NA
29 Billing and Coding in Post-Acute and Long-Term Care Continuum REVIEW RECENT CHANGES IN BILLING AND CODING REQUIREMENTS OBJECTIVE 3
30
31 CODES, CODES, AND MORE CODES Transitional Care Management (TCM) Chronic Care Management (CCM) Advance Care Planning (ACP) Proposed codes
32 TCM
33 TRANSITIONAL CARE MANAGEMENT Transition Care Management (TCM): 99495, for discharge from hospital, SNF, or CMHC stay; outpatient observation; partial hospitalization covers 30 days, starting with discharge day and ending 29 days later (date of service for billing is the 30 th day) POS code is for the site of service of the required face-to-face visit
34 TRANSITIONAL CARE MANAGEMENT Can only be billed by one provider Covers non-face-to-face physician and non-physician time/work
35 TRANSITIONAL CARE MANAGEMENT communication: by end of 2 nd business day face-to-face by end of 14 th day medical decision making: moderate communication by end of 2 nd business day face-to-face by end of 7 th day medical decision making: high
36 TRANSITIONAL CARE MANAGEMENT for both med reconciliation no later than date of f2f visit medical decision making required

37 TRANSITIONAL CARE MANAGEMENT NEW IN 2016: may now submit bill on date of F2F visit and not have to wait until the 30 th day

38 TRANSITIONAL CARE MANAGEMENT NEW IN 2016: may now submit bill on date of F2F visit and not have to wait until the 30 th day Payment/PhysicianFeeSched/Downloads/FAQ-TCMS.pdf
39 TRANSITIONAL CARE MANAGEMENT NEW IN 2016: may now submit bill on date of F2F visit and not have to wait until the 30 th day. Must still track the patient for 30 days If the patient is readmitted within 30 days, and the practice has already billed TCM for that patient, they cannot bill for TCM when the patient is discharged the second time. If the patient is readmitted and the practice has not yet billed, they can wait until the patient is discharged the second time, track the patient for TCM, and bill after the second face-toface visit.
40
41 CCM
42 CHRONIC CARE MANAGEMENT (CCM) Two or more significant chronic conditions Non face-to-face work Billed no more frequently than once per month per qualified patient Started January 1, 2015
43 CHRONIC CARE MANAGEMENT (CCM) Services covered include Regular development and revision of a electronic plan of care Communication with other treating health professionals Medication management 24-hour-a-day, 7-day-a-week access to address a patient s acute chronic care needs.
44 CHRONIC CARE MANAGEMENT (CCM) Services covered include Continuity of care with a designated practitioner or member of the care team with whom the patient is able to get successive routine appointments. Care management for chronic conditions including systematic assessment and development of a patient centered plan of care. Management of care transitions within health care.
45 CHRONIC CARE MANAGEMENT (CCM) Services covered include Coordination with home and community based clinical service providers. Enhanced opportunities for a patient to communicate with the provider through telephone and secure messaging, internet or other asynchronous non face-to-face consultation methods.
46 CHRONIC CARE MANAGEMENT (CCM) Electronic Care Plan - components establish, implement, revise, or monitor and manage an electronic care plan that addresses the physical, mental, cognitive, psychosocial, functional and environmental needs of the patient maintain an inventory of resources and supports that the patient needs
47 CHRONIC CARE MANAGEMENT (CCM) Electronic Care Plan - components The practice must use a certified EHR to bill CCM codes. The electronic care plan must be directly available to anyone providing CCM services fax not allowed 24/7 A copy of the electronic care plan must be provided to the patient
48 CHRONIC CARE MANAGEMENT (CCM) Billing The practice must have the patient s written consent CPT code (avg: $42.60) Co-pays do apply Only one clinician can be paid for CCM services in a calendar month Duke it out
49 CHRONIC CARE MANAGEMENT (CCM) Billing The following codes cannot be billed during the same month as CCM (CPT 99490): Transition Care Management (TCM) CPT and Home Healthcare Supervision HCPCS G0181 Hospice Care Supervision HCPCS G9182 Certain ESRD services CPT
50 CHRONIC CARE MANAGEMENT (CCM) Benefit get paid for work already being done, but not reimbursed billed monthly for 20 eligible patients = $10k/year Downside many practices may not meet requirements

51 CHRONIC CARE MANAGEMENT (CCM) Downside not billable for patients living in facility NEW IN 2016: Clarification of facility
52 52 CHRONIC CARE MANAGEMENT (CCM) Resources Medicare MLN Education/Medicare-Learning-Network- MLN/MLNProducts/Downloads/ChronicCareMa nagement.pdf Medicare MLN Connects: National Provider Call Education/Outreach/NPC/Downloads/ Chronic-Care-Presentation.pdf
53 53 CHRONIC CARE MANAGEMENT (CCM) Resources ACP toolkit AAFP e/payment_coding/medicare/chronic_care_ management_toolkit.pdf Moore, K: Chronic Care Management and Other New CPT Codes. Fam Pract Manag Jan-Feb;22(1):7-12.
54
55 ACP Payment/PhysicianFeeSched/Downloads/FAQ-Advance-Care-Planning.pdf
56 56 ADVANCE CARE PLANNING Beginning January 1, 2016, Medicare pays healthcare providers for advance care planning (ACP) discussions with Medicare beneficiaries. ACP: the face-to-face service between a physician or other qualified healthcare professional (QHCP) and a patient, family member, or surrogate in counseling and discussing advance directives, with or without completing relevant legal forms.

57 57 ADVANCE CARE PLANNING Two codes 99497: first 30 minutes 99498: each additional 30 minutes
58 CPT Code Description CY 2016 WRVU Advance care planning including the explanation and discussion of advance directives such as standard forms (with completion of such forms, when performed), 1.50 by the physician or other qualified health care professional; first 30 minutes, face-to-face with the patient, family member(s), and/or surrogate. Advance care planning including the explanation and discussion of advance directives such as standard forms (with completion of such forms, when performed), by the physicians or other qualified health care professional; each additional 30 minutes (List separately in addition to code for primary procedure). Approx. Amount $86 in doctor s office $80 in hospital 1.40 $75
59 AND 99498: BILLABLE WITH new and established patient office visits ( ), observation initial, subsequent and discharge care codes ( , ), initial, subsequent and discharge hospital service codes ( , ), observation or inpatient admit and discharge on the same date ( ), outpatient and inpatient consultations ( ), emergency department visit codes ( ), initial, subsequent and discharge nursing facility care codes ( ), annual nursing facility assessment code (99318), new, established and discharge domiciliary or rest home visit codes ( ), new and established patient home visit codes ( ), initial and periodic preventive medicine codes ( ), and Transitional Care Management Service codes ( )

60 AND 99498: DIAGNOSIS
61 PROPOSED UPDATES AND NEW CODES
62 PROPOSED UPDATES AND NEW CODES New codes for primary care payments Psychiatric collaborative care model Four separate codes. Not pertinent to us but allows for broader application of care management benefits for those with psychiatric conditions. Temporary G codes until CPT codes/process finalized Code for Assessment / Care Planning Services for Cognitively Impaired SNF/NF not included office, home, domiciliary or rest home covered. May help set a precedence for us in the future or help a dementia APM Adjusted Payment for routine visits for those with mobility impairments SNF/NF not included as relates primarily to need for specialty equipment needs in the outpatient setting
63 PROPOSED UPDATES AND NEW CODES New codes for primary care payments Comprehensive assessment for chronic care management Allows for comprehensive assessment and care planning by physician or other qualified health professional for patients requiring CCM services, including assessment during the provision of a face to face service billed separately.
64 PROPOSED UPDATES AND NEW CODES CMS Recognition of CPT Codes for Primary Care Previously not Paid for Prolonged non-face to Face Service Codes 99358/9 First 60 min, then every 30 min thereafter (2.1 and 1.0 wrvu respectively). Allows for billing of time spent before and/or after direct patient care. Vignette gives example of extensive review of subsequently received record and communication thereafter with daughter. CMS proposes to require service to be furnished on the same day by the same physician as the companion E/M code, and not on the same day as CCM or TCM codes. CMS request comment on the potential intersection of these prolonged service codes with the proposed comprehensive assessment for and care planning for patient requiring CCM service.
65 PROPOSED UPDATES AND NEW CODES CMS Recognition of CPT Codes for Primary Care Previously not Paid for Complex Chronic Care Management Codes / 89 CMS noted that in order to more accurately pay for services based on the relative resources required, that the original somewhat more stringent CCCM codes would now be paid for. These codes require the patient be at significant risk of death, acute exacerbation/decompensation or functional decline, and requires the establishment or substantial revision of a comprehensive care plan or moderate or high complexity medical decision making, 60 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month is for the first 60 minutes per month, is for each additional 30 minutes.
66 PROPOSED UPDATES AND NEW CODES Telehealth Codes Advance Care Planning added to telehealth on basic AWE allowed, although no formal request was made. Rural/underserved areas only
67 PROPOSED UPDATES AND NEW CODES Telehealth Codes ICU consultative visits added to telehealth. May help form basis for allowing specialty consultations in PA/LTC in the future. CMS is considering such requests on a yearly basis. Submitted evidence requires a description of relevant clinical studies that demonstrate the service provided by telehealth improves the diagnosis or treatment of illness or injury or improves the functioning of a malformed body part.
68 Billing and Coding in Post-Acute and Long-Term Care Continuum ICD-10 CONSIDERATIONS

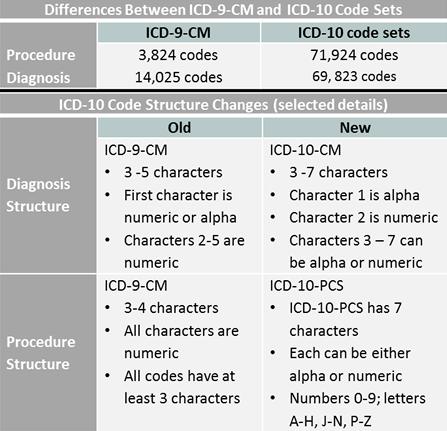
69 ICD-10 The Devil is in the Details
70 ICD-10
71 ICD-10: WHAT DETAILS: Laterality Severity Complexity Injuries (cause, how, where happened) Pregnancy trimester Operative (intra-, post- complications) New concepts not in ICD-9 (under dosing, blood type, the Glasgow Coma Scale, and alcohol level.)
72 HOW DETAILED?? 16. V97.33XD: Sucked into jet engine, subsequent encounter. 15. W51.XXXA: Accidental striking against or bumped into by another person, sequela. 14. V00.01XD: Pedestrian on foot injured in collision with rollerskater, subsequent encounter. 13. Y93.D: Activities involved arts and handcrafts. 12. Z99.89: Dependence on enabling machines and devices, not elsewhere classified. 11. Y92.146: Swimming-pool of prison as the place of occurrence of the external cause. 10. S10.87XA: Other superficial bite of other specified part of neck, initial encounter. 9. W55.41XA: Bitten by pig, initial encounter.
73 HOW DETAILED?? 8. W61.62XD: Struck by duck, subsequent encounter. 7. Z63.1: Problems in relationship with in-laws. 6. W220.2XD: Walked into lamppost, subsequent encounter. 5. Y93.D: V91.07XD: Burn due to water-skis on fire, subsequent encounter. 4. W55.29XA: Other contact with cow, subsequent encounter. 3. W22.02XD: V95.43XS: Spacecraft collision injuring occupant, sequela. 2. W61.12XA: Struck by macaw, initial encounter. 1. R46.1: Bizarre personal appearance.
74 TOP CODING CHALLENGES (AHIMA, JULY 2016) Incorrectly applying 7 th character for trauma and fracture Improperly using procedure codes that drive a diagnostic related group Misidentifying respiratory failure Mistaking the use of guidance tools Insufficiently documenting devices, components, and grafting material
75 ICD-10: BILLING IMPLICATIONS Correct code Adequate level of detail Initial/subsequent encounters Staff training Timely response to rejections

76 SUCCEEDING WITH IDC-10
77
78 Billing and Coding in Post-Acute and Long-Term Care Continuum SUMMARY
79 SUMMARY Differences in billing related to Place of Service Constraints on visit services for patients receiving Medicare Part A benefits Recent changes in billing and coding requirements Impact of ICD-10 implementation


80 Billing and Coding in Post-Acute and Long-Term Care Continuum
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011
 PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
3/28/2016. Evaluation and Management. Evaluation and Management Emerging Trends. Disclosures. Evaluation and Management The History
 Evaluation and Management Emerging Trends Peter Hollmann MD Past CPT Panel Chair Disclosures Ambassador for AMA CPT Member RBRVS Update Committee 2 Evaluation and Management The History Evaluation and
Evaluation and Management Emerging Trends Peter Hollmann MD Past CPT Panel Chair Disclosures Ambassador for AMA CPT Member RBRVS Update Committee 2 Evaluation and Management The History Evaluation and
Updates in Coding & Billing Strategies.
 Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Updates in Coding & Billing Strategies. Drew Keister MD, FAAFP Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow
Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Updates in Coding & Billing Strategies. Drew Keister MD, FAAFP Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow
Transitional Care Management - Mistakes, CCM Interface, and the 2016 Fee Schedule Changes
 Transitional Care Management - Mistakes, CCM Interface, and the 2016 Fee Schedule Changes Stephen Canon, M.D. Program Director & Associate Professor UAMS Department of Urology Chief, Division of Pediatric
Transitional Care Management - Mistakes, CCM Interface, and the 2016 Fee Schedule Changes Stephen Canon, M.D. Program Director & Associate Professor UAMS Department of Urology Chief, Division of Pediatric
Coding Guidance for HIV Clinical Practices: Care Management Services
 Coding Guidance for HIV Clinical Practices: Care Management Services HIV medical practices and clinicians provide many services outside of a face-to-face encounter with a patient. Some of these services
Coding Guidance for HIV Clinical Practices: Care Management Services HIV medical practices and clinicians provide many services outside of a face-to-face encounter with a patient. Some of these services
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE
 CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Transitional Care Management (TCM) and Chronic Care Management (CCM) Overview and Billing Process. April 19, :00 PM
 and Chronic Care Management (CCM) Overview and Billing Process. April 19, :00 PM") Transitional Care Management (TCM) and Chronic Care Management (CCM) Overview and Billing Process April 19, 2016 2:00 PM 2 Discussion Topics TCM Requirements TCM Services and C247 Process Medical Decision
Transitional Care Management (TCM) and Chronic Care Management (CCM) Overview and Billing Process April 19, 2016 2:00 PM 2 Discussion Topics TCM Requirements TCM Services and C247 Process Medical Decision
Disclosure Statement
 2017 Coding and Medicare Changes for Physician Fee Schedule Billing Presented by Jean Acevedo, CHC CPC CENTC LHRM Disclosure Statement No financial relationships to disclose. 1 Disclaimer The information
2017 Coding and Medicare Changes for Physician Fee Schedule Billing Presented by Jean Acevedo, CHC CPC CENTC LHRM Disclosure Statement No financial relationships to disclose. 1 Disclaimer The information
Chronic Care Management Coding Guidelines Effective January 1, 2017
 Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
Transitional Care Management We provide these services a-la-carte...
 Transitional Care Management We provide these services a-la-carte... Initial Patient Outreach* This must be done within 2 days of the patient s discharge from the hospital. During this call patient s medications
Transitional Care Management We provide these services a-la-carte... Initial Patient Outreach* This must be done within 2 days of the patient s discharge from the hospital. During this call patient s medications
The Business Case for Chronic Care Management in the Ambulatory Care Practice
 The Business Case for Chronic Care Management in the Ambulatory Care Practice Debbie Rozanski, CMC Practice Transformation Coach Michigan Rural Health Association Soaring Eagle Casino & Resort May 4-5,
The Business Case for Chronic Care Management in the Ambulatory Care Practice Debbie Rozanski, CMC Practice Transformation Coach Michigan Rural Health Association Soaring Eagle Casino & Resort May 4-5,
Provider-Based RHC Billing June 8, 2018
 Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
Chronic Care Management (CCM): An Overview for Pharmacists. March Developed Through a Collaboration Among:
: An Overview for Pharmacists. March Developed Through a Collaboration Among:") Chronic Care Management (CCM): An Overview for Pharmacists March 2017 Developed Through a Collaboration Among: Overview of CCM and Complex CCM Beginning January 1, 2015, the Medicare Physician Fee Schedule
Chronic Care Management (CCM): An Overview for Pharmacists March 2017 Developed Through a Collaboration Among: Overview of CCM and Complex CCM Beginning January 1, 2015, the Medicare Physician Fee Schedule
Multi-payer G and CPT Care Management Code Summary v7
 Purpose This document is a guide to help care management team members quickly understand the requirements and documentation fields required for billing care management-related G and CPT codes. Please note
Purpose This document is a guide to help care management team members quickly understand the requirements and documentation fields required for billing care management-related G and CPT codes. Please note
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes
 CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Clinically Focused. Outcomes Oriented. Technology Driven. Chronic Care Management. eqguide. (CPT Codes 99490, 99487, 99489)
") Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
WHAT YOU NEED TO KNOW! CMS (Medicare)! and! The Joint Commission CSC! Updates!
! and! The Joint Commission CSC! Updates!") !!! Lombardi Hill Consulting Group WHAT YOU NEED TO KNOW!! CMS (Medicare)! and! The Joint Commission CSC! Updates! Debbie Lombardi Hill, FAHA Dunedin, Florida w May 4, 2016 Lombardi Hill Consulting Group!
!!! Lombardi Hill Consulting Group WHAT YOU NEED TO KNOW!! CMS (Medicare)! and! The Joint Commission CSC! Updates! Debbie Lombardi Hill, FAHA Dunedin, Florida w May 4, 2016 Lombardi Hill Consulting Group!
Presented for the AAPC National Conference April 4, 2011
 Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Fact Sheet: Advance Care Planning as a Billable Medicare Service starting Jan. 1, 2016
 Fact Sheet: Advance Care Planning as a Billable Medicare Service starting Jan. 1, 2016 What constitutes Advance Care Planning? Getting information on the types of life-sustaining treatments that are available
Fact Sheet: Advance Care Planning as a Billable Medicare Service starting Jan. 1, 2016 What constitutes Advance Care Planning? Getting information on the types of life-sustaining treatments that are available
Telehealth. Administrative Process. Coverage. Indications that are covered
 Telehealth These services may or may not be covered by your HealthPartners plan. Please see your plan documents for your specific coverage information. If there is a difference between this general information
Telehealth These services may or may not be covered by your HealthPartners plan. Please see your plan documents for your specific coverage information. If there is a difference between this general information
Prolonged Services With Direct Face-to-Face Patient Contact Service (Codes ) (ZZZ codes)
 (ZZZ codes)") 30.6.15.1 - Prolonged Services With Direct Face-to-Face Patient Contact Service (s 99354-99357) (ZZZ codes) (Rev.1490, Issued: 04-11-08, Effective: 07-01-08, Implementation: 07-07-08) A. Definition Prolonged
30.6.15.1 - Prolonged Services With Direct Face-to-Face Patient Contact Service (s 99354-99357) (ZZZ codes) (Rev.1490, Issued: 04-11-08, Effective: 07-01-08, Implementation: 07-07-08) A. Definition Prolonged
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
PEARLS OF THE ACC CV SUMMIT: THOUGHTS FROM THE OYSTER BED OF CLINICAL PRACTICE
 PEARLS OF THE ACC CV SUMMIT: THOUGHTS FROM THE OYSTER BED OF CLINICAL PRACTICE IN-ACC October 13, 2018 Linda Gates-Striby CCS-P, ACS-CA St. Vincent Medical Group Director Quality Assurance Lggates@ascension.org
PEARLS OF THE ACC CV SUMMIT: THOUGHTS FROM THE OYSTER BED OF CLINICAL PRACTICE IN-ACC October 13, 2018 Linda Gates-Striby CCS-P, ACS-CA St. Vincent Medical Group Director Quality Assurance Lggates@ascension.org
2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES
 2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES 2017 Physician Fee Schedule Impact on Medicare ACOs 1. Allowing ACO Participants to report PQRS separately from ACO 2. ACO Quality
2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES 2017 Physician Fee Schedule Impact on Medicare ACOs 1. Allowing ACO Participants to report PQRS separately from ACO 2. ACO Quality
Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT
 1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
Telehealth 101. Telehealth Summit May 24, 2018
 Telehealth 101 Telehealth Summit May 24, 2018 Tim Bickel Telehealth Director, University of Louisville Deborah Burton, Telehealth Program Manager, KentuckyOne Health, Lexington; Chair, Kentucky Teleheath
Telehealth 101 Telehealth Summit May 24, 2018 Tim Bickel Telehealth Director, University of Louisville Deborah Burton, Telehealth Program Manager, KentuckyOne Health, Lexington; Chair, Kentucky Teleheath
CPT Pediatric Coding Updates 2013
 (TNAAP) CPT Pediatric Coding Updates 2013 The 2013 Current Procedural Terminology (CPT) codes are effective as of January 1, 2013. This is not an all inclusive list of the 2013 changes. TNAAP has listed
(TNAAP) CPT Pediatric Coding Updates 2013 The 2013 Current Procedural Terminology (CPT) codes are effective as of January 1, 2013. This is not an all inclusive list of the 2013 changes. TNAAP has listed
Central Ohio HFMA Fall Education Hot Topics: Maintaining Compliance in Times of Change. November 22, 2013
 Central Ohio HFMA Fall Education Hot Topics: Maintaining Compliance in Times of Change November 22, 2013 Agenda IPPS Final rule inpatient status changes Proposed OPPS changes to reporting hospital evaluation
Central Ohio HFMA Fall Education Hot Topics: Maintaining Compliance in Times of Change November 22, 2013 Agenda IPPS Final rule inpatient status changes Proposed OPPS changes to reporting hospital evaluation
Monday, October 24, :15 a.m. to 10:45 a.m. Great Halls 1 & 2
 Expanding Pharmacy Impact: Transitional Care Management and Chronic Care Management Activity Number: 0217-0000-16-1118-L04-P 1.50 hours of CPE credit; Activity Type: A Knowledge-Based Activity Monday,
Expanding Pharmacy Impact: Transitional Care Management and Chronic Care Management Activity Number: 0217-0000-16-1118-L04-P 1.50 hours of CPE credit; Activity Type: A Knowledge-Based Activity Monday,
MEDICAL POLICY No R2 TELEMEDICINE
 Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Telemedicine Guidance
 Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21.
 How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21. If only some of the charges are noncovered, per CMS Internet-Only Manual,
How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21. If only some of the charges are noncovered, per CMS Internet-Only Manual,
JOHNS HOPKINS HEALTHCARE
 Page 1 of 16 ACTION: New Policy Effective Date: 10/01/2013 Revising : Review Dates: 03/29/16, 06/29/17, Superseding 09/01/17, 12/01/17 Archiving Retiring Johns Hopkins HealthCare LLC (JHHC) provides a
Page 1 of 16 ACTION: New Policy Effective Date: 10/01/2013 Revising : Review Dates: 03/29/16, 06/29/17, Superseding 09/01/17, 12/01/17 Archiving Retiring Johns Hopkins HealthCare LLC (JHHC) provides a
MEDICAL POLICY No R1 TELEMEDICINE
 Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Telemedicine and Reimbursement
 Telemedicine and Reimbursement Presented for : March 14 th 2018 About Acevedo Consulting Incorporated Acevedo Consulting Incorporated prides itself on not providing cookie-cutter programs, but a quality
Telemedicine and Reimbursement Presented for : March 14 th 2018 About Acevedo Consulting Incorporated Acevedo Consulting Incorporated prides itself on not providing cookie-cutter programs, but a quality
E. Improving Payment Accuracy for Primary Care, Care Management and Patient-Centered
 CMS-1654-F 212 E. Improving Payment Accuracy for Primary Care, Care Management and Patient-Centered Services 1. Overview In recent years, we have undertaken ongoing efforts to support primary care and
CMS-1654-F 212 E. Improving Payment Accuracy for Primary Care, Care Management and Patient-Centered Services 1. Overview In recent years, we have undertaken ongoing efforts to support primary care and
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
Rural Health Clinic Billing
 Critical Access Hospital and Rural Health Clinic Billing September 12, 2017 1 Rural Health Clinic Overview Rural Health Clinic Services Preventive Services in the RHC Non-RHC Services/Non-Covered Services
Critical Access Hospital and Rural Health Clinic Billing September 12, 2017 1 Rural Health Clinic Overview Rural Health Clinic Services Preventive Services in the RHC Non-RHC Services/Non-Covered Services
Third Party Payer Days. IMGMA February 25, 2015
 Third Party Payer Days IMGMA February 25, 2015 Agenda 2015 Medicare Physician Fee Schedule Medicare Physician Fee Schedule Database Transitional Care Management - Reminder Medicare - Coverage Guidelines
Third Party Payer Days IMGMA February 25, 2015 Agenda 2015 Medicare Physician Fee Schedule Medicare Physician Fee Schedule Database Transitional Care Management - Reminder Medicare - Coverage Guidelines
Chronic Care Management
 Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
The New Medicare DME Face-To- Face Rule: What Referral Sources Need to Know
 The New Medicare DME Face-To- Face Rule: What Referral Sources Need to Know What is the Face-to-Face Rule? Section 6407(b) of the 2009 Health Care Reform law (Affordable Care Act) mandates that there must
The New Medicare DME Face-To- Face Rule: What Referral Sources Need to Know What is the Face-to-Face Rule? Section 6407(b) of the 2009 Health Care Reform law (Affordable Care Act) mandates that there must
Care Plan Oversight Services and Physician Services for Certification
 Education Makes the Difference Care Plan Oversight Services and Physician Services for Certification and Recertification of Medicare-Covered Home Health Services A CMS CONTRACTED INTERMEDIARY CARRIER The
Education Makes the Difference Care Plan Oversight Services and Physician Services for Certification and Recertification of Medicare-Covered Home Health Services A CMS CONTRACTED INTERMEDIARY CARRIER The
1:35. NPP April Young Medical Consulting, LLC. Non-Physician Practitioner Coding and Billing. Disclaimer
 Non-Physician Practitioner Coding and Billing Jill Young - CPC, CEDC, CIMC, East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing. The information
Non-Physician Practitioner Coding and Billing Jill Young - CPC, CEDC, CIMC, East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing. The information
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
CPT Coding Changes in 2013: Billing, Reimbursement and IT
 CPT Coding Changes in 2013: Billing, Reimbursement and IT Texas Council of Community Centers Presented by: David R. Swann, MA, LCAS, CCS, LPC, NCC Senior Healthcare Integration Consultant Phone: 336-386-9801
CPT Coding Changes in 2013: Billing, Reimbursement and IT Texas Council of Community Centers Presented by: David R. Swann, MA, LCAS, CCS, LPC, NCC Senior Healthcare Integration Consultant Phone: 336-386-9801
2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of
 2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company
2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company
Strategies for Coding, Billing and Getting Paid Appropriately
 Strategies for Coding, Billing and Getting Paid Appropriately 2015 Monograph Update California Academy of Family Physicians Another new year and time to make sure your practice is doing everything possible
Strategies for Coding, Billing and Getting Paid Appropriately 2015 Monograph Update California Academy of Family Physicians Another new year and time to make sure your practice is doing everything possible
Cognitive Emotional Social Behavioral functioning
 TIP SHEET Health and Behavior Assessment and Intervention (HBAI) Services Coverage of Chronic Disease Self-Management Education Medicare and Medicare Advantage Purpose: The HBAI services are used to identify
TIP SHEET Health and Behavior Assessment and Intervention (HBAI) Services Coverage of Chronic Disease Self-Management Education Medicare and Medicare Advantage Purpose: The HBAI services are used to identify
Documentation for CCC Reimbursement
 Section 4.6 Implement Documentation for CCC Reimbursement This tool describes the importance of documentation and potential workflow changes to take advantage of any opportunity for reimbursement of services
Section 4.6 Implement Documentation for CCC Reimbursement This tool describes the importance of documentation and potential workflow changes to take advantage of any opportunity for reimbursement of services
Transitional Care Management Services: New Codes, New Requirements
 Transitional Care Management Services: New Codes, New Requirements hospital 99496 99495 99496 family practice o n Jan. 1, 2013, the much anticipated transitional care management (TCM) Two new codes will
Transitional Care Management Services: New Codes, New Requirements hospital 99496 99495 99496 family practice o n Jan. 1, 2013, the much anticipated transitional care management (TCM) Two new codes will
Shared and Incident To Billing of E/M Services in Radiation Oncology Updated November 2017
 ASTRO Guidance on Shared and Incident To Billing of Evaluation and Management Services in Radiation Oncology The Centers for Medicare and Medicaid Services (CMS) establishes Medicare policy for the payment
ASTRO Guidance on Shared and Incident To Billing of Evaluation and Management Services in Radiation Oncology The Centers for Medicare and Medicaid Services (CMS) establishes Medicare policy for the payment
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Chronic Care Management Services. Presented by Noridian Part B Medicare Provider Outreach and Education April 2015
 Chronic Care Management Services Presented by Noridian Part B Medicare Provider Outreach and Education April 2015 Continuing Education Unit (CEU) When registering, add all additional attendees First and
Chronic Care Management Services Presented by Noridian Part B Medicare Provider Outreach and Education April 2015 Continuing Education Unit (CEU) When registering, add all additional attendees First and
Case Management Model Act Supporting Case Management Programs
 Case Management Model Act Supporting Case Management Programs CMSA 2017 Page 1 Case Management Model Act Revised 2017 i (CM Model Act) The Case Management Model Act, revised version, was adopted by the
Case Management Model Act Supporting Case Management Programs CMSA 2017 Page 1 Case Management Model Act Revised 2017 i (CM Model Act) The Case Management Model Act, revised version, was adopted by the
Updated Only for Logo and Branding Provider Notice
 Updated Only for Logo and Branding Provider Notice To: From: PerformCare Network Providers Sheryl M. Swanson, MBA, Project Manager Date: December 21, 2012 Subject: AD12 112 2013 CPT Code Update IMPLEMENTATION
Updated Only for Logo and Branding Provider Notice To: From: PerformCare Network Providers Sheryl M. Swanson, MBA, Project Manager Date: December 21, 2012 Subject: AD12 112 2013 CPT Code Update IMPLEMENTATION
Critical Care What Makes this so Difficult
 Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
CPT & MEDICARE CHANGES FOR RHEUMATOLOGY
 CPT & MEDICARE CHANGES FOR RHEUMATOLOGY PRESENTOR: Candice Fenildo, CPC, CPMA, CPB, CENTC, CPC-I Presented in Partnership with NORM and Crescendo Bioscience Developed & Hosted by Acevedo Consulting Incorporated
CPT & MEDICARE CHANGES FOR RHEUMATOLOGY PRESENTOR: Candice Fenildo, CPC, CPMA, CPB, CENTC, CPC-I Presented in Partnership with NORM and Crescendo Bioscience Developed & Hosted by Acevedo Consulting Incorporated
Providing and Billing Medicare for Chronic Care Management
 Providing and Billing Medicare for Chronic Care Management 2015 Medicare Physician Fee Schedule Final Rule November 2014 (PYA). No portion of this white paper may be used or duplicated by any person or
Providing and Billing Medicare for Chronic Care Management 2015 Medicare Physician Fee Schedule Final Rule November 2014 (PYA). No portion of this white paper may be used or duplicated by any person or
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Primary Care Setting Behavioral Health Billing Codes
 Primary Care Setting s Medicaid Medicare Third Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though
Primary Care Setting s Medicaid Medicare Third Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though
MLN Matters Number: MM6740 Revised Related Change Request (CR) #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010
 #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010") News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
OUTPATIENT BEHAVIORAL HEALTH CSHCN SERVICES PROGRAM PROVIDER MANUAL
 OUTPATIENT BEHAVIORAL HEALTH CSHCN SERVICES PROGRAM PROVIDER MANUAL APRIL 2018 CSHCN PROVIDER PROCEDURES MANUAL APRIL 2018 OUTPATIENT BEHAVIORAL HEALTH Table of Contents 29.1 Enrollment......................................................................
OUTPATIENT BEHAVIORAL HEALTH CSHCN SERVICES PROGRAM PROVIDER MANUAL APRIL 2018 CSHCN PROVIDER PROCEDURES MANUAL APRIL 2018 OUTPATIENT BEHAVIORAL HEALTH Table of Contents 29.1 Enrollment......................................................................
2019 Evaluation and Management Coding Advisor. Advanced guidance on E/M code selection for traditional documentation systems
 2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Deleted Codes. Agenda 1/31/ E/M Codes Deleted Codes New Codes Changed Codes
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February Jean C. Russell, MS, RHIT Richard Cooley, BA, CCS
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
SERVICE CODE CLARIFICATIONS
 SERVICE CODE CLARIFICATIONS Service Description Assertive Community Treatment (ACT) Assisted Outpatient Treatment (AOT) HCPCS Code Description Explanation of Code Utilization H0039 ACT Report only face-to-face
SERVICE CODE CLARIFICATIONS Service Description Assertive Community Treatment (ACT) Assisted Outpatient Treatment (AOT) HCPCS Code Description Explanation of Code Utilization H0039 ACT Report only face-to-face
Patient Health Education: What Physicians Need to Know to Thrive in Today s Healthcare Environments
 Patient Health Education: What Physicians Need to Know to Thrive in Today s Healthcare Environments Prepared by National Institute of Whole Health www.niwh.org Accredited by the Institute for Credentialing
Patient Health Education: What Physicians Need to Know to Thrive in Today s Healthcare Environments Prepared by National Institute of Whole Health www.niwh.org Accredited by the Institute for Credentialing
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT
 Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Care Transition Strategies: The 2013 Transition Care Management Codes
 Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
See the Time chapter for complete instructions regarding how to code using time as the controlling E/M factor.
 2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
CMS Changes Expanding Coverage of Telehealth
 CMS Changes Expanding Coverage of Telehealth WASHINGTON Saturday, Nov. 30, 2013 -- Medicare beneficiaries received good news on the eve of Thanksgiving as the Centers for Medicare and Medicaid Services
CMS Changes Expanding Coverage of Telehealth WASHINGTON Saturday, Nov. 30, 2013 -- Medicare beneficiaries received good news on the eve of Thanksgiving as the Centers for Medicare and Medicaid Services
The New World of Value Driven Cardiac Care
 1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
Evaluation and Management Services
 Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
8/1/2017. Services and Description
 Index of CPT Codes for Medical Home The following index was originally published in November 2003 in Medical Home Crosswalk To Reimbursement. The information was developed by Margaret McManus, Alan Kohrt,
Index of CPT Codes for Medical Home The following index was originally published in November 2003 in Medical Home Crosswalk To Reimbursement. The information was developed by Margaret McManus, Alan Kohrt,
WHY SHOULD A CHC/FQHC CARE?
 Suzanne Niemi, CPA, CMPE, CCE Alaska Primary Care Association April 2017 Medicare Part A & Part B MACRA / MIPS Chronic Care Management Billing WHY SHOULD A CHC/FQHC CARE? 2 DEFINITIONS FQHC Federally Qualified
Suzanne Niemi, CPA, CMPE, CCE Alaska Primary Care Association April 2017 Medicare Part A & Part B MACRA / MIPS Chronic Care Management Billing WHY SHOULD A CHC/FQHC CARE? 2 DEFINITIONS FQHC Federally Qualified
JOHNS HOPKINS HEALTHCARE
 Page 1 of 19 ACTION: New Policy Effective Date: 10/01/2013 Revising : Review Dates: 03/29/16, 06/29/17, Superseding 09/01/17, 12/01/17, 05/15/18 Archiving Retiring Johns Hopkins HealthCare LLC (JHHC) provides
Page 1 of 19 ACTION: New Policy Effective Date: 10/01/2013 Revising : Review Dates: 03/29/16, 06/29/17, Superseding 09/01/17, 12/01/17, 05/15/18 Archiving Retiring Johns Hopkins HealthCare LLC (JHHC) provides
Medicare Chronic Care Management. November 8, 2017
 Medicare Chronic Care Management November 8, 2017 2 Overview 1) Overview of the Medicare CCM program 2) Chronic Care Management 2018 Service Update 3) Implementing at your Organization 1) Key Questions
Medicare Chronic Care Management November 8, 2017 2 Overview 1) Overview of the Medicare CCM program 2) Chronic Care Management 2018 Service Update 3) Implementing at your Organization 1) Key Questions
Personally Providing Services Primary Care Exception Physicians AT Teaching Hospital
 Personally Providing Services Primary Care Exception Physicians AT Teaching Hospital Agenda Services Primary Care Exception (PCE) Physicians AT Teaching Hospital (PATH) 2 Personally Provided Services 3
Personally Providing Services Primary Care Exception Physicians AT Teaching Hospital Agenda Services Primary Care Exception (PCE) Physicians AT Teaching Hospital (PATH) 2 Personally Provided Services 3
COMPLIANCE ALERT. Department Chairs, Compliance Leaders, and UFJPI Management
 UNIVERSITY OF FLORIDA COLLEGE OF MEDICINE - JACKSONVILLE Office of Physician Billing Compliance 653-1 West 8 th Street, LRC-3 Jacksonville, Florida 32209 Phone: (904) 244-2158 Fax: (904) 244-5323 COMPLIANCE
UNIVERSITY OF FLORIDA COLLEGE OF MEDICINE - JACKSONVILLE Office of Physician Billing Compliance 653-1 West 8 th Street, LRC-3 Jacksonville, Florida 32209 Phone: (904) 244-2158 Fax: (904) 244-5323 COMPLIANCE
2017 Proposed Rule Physician Fee Schedule in the Federal Register
 2017 Proposed Rule Physician Fee Schedule in the Federal Register Thursday, December 15, 2016 Noon 1:00 Pacific / 1:00 2:00 Mountain / 2:00 3:00 Central / 3:00-4:00 PM Eastern Lucy Zielinski, Vice President
2017 Proposed Rule Physician Fee Schedule in the Federal Register Thursday, December 15, 2016 Noon 1:00 Pacific / 1:00 2:00 Mountain / 2:00 3:00 Central / 3:00-4:00 PM Eastern Lucy Zielinski, Vice President
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
THE TELEMEDICINE MARKET LANDSCAPE
 How Telehealth is Changing the Care Provided to Patients Anne Cadwell, The Permanente Medical Group THE TELEMEDICINE MARKET LANDSCAPE Approximately 1 million virtual doctor visits in the U.S. in 2015 1
How Telehealth is Changing the Care Provided to Patients Anne Cadwell, The Permanente Medical Group THE TELEMEDICINE MARKET LANDSCAPE Approximately 1 million virtual doctor visits in the U.S. in 2015 1
Telemedicine Policy Annual Approval Date
 Policy Number 2017R0046A Telemedicine Policy Annual Approval Date 7/13/2016 Approved By REIMBURSEMENT POLICY CMS-1500 Payment Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You
Policy Number 2017R0046A Telemedicine Policy Annual Approval Date 7/13/2016 Approved By REIMBURSEMENT POLICY CMS-1500 Payment Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You
Initial Preventive Physical Examination (IPPE) Presented by Provider Outreach and Education (POE) December 2016
 Presented by Provider Outreach and Education (POE) December 2016") Initial Preventive Physical Examination (IPPE) Presented by Provider Outreach and Education (POE) December 2016 DISCLAIMER This information release is the property of Noridian Healthcare Solutions, LLC
Initial Preventive Physical Examination (IPPE) Presented by Provider Outreach and Education (POE) December 2016 DISCLAIMER This information release is the property of Noridian Healthcare Solutions, LLC
FQHC Behavioral Health Billing Codes
 FQHC s Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though process clearly reflected in assessment
FQHC s Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though process clearly reflected in assessment
Medicare Preventive Services
 Medicare Preventive Services Presented by Part B Provider Outreach & Education December 16, 2015 Event Instructions Today s event is a teleconference Slides will not be advanced during the presentation
Medicare Preventive Services Presented by Part B Provider Outreach & Education December 16, 2015 Event Instructions Today s event is a teleconference Slides will not be advanced during the presentation
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC
 Service in RHC") How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
NARHC Spring Institute
 NARHC Spring Institute Tuesday, March 15, 2016 San Antonio Conference Breakouts Your choice Regency Ballroom E Mac Discussion: Novitas Kim Robinson Live Oak Mac Discussion: Noridian Tana Williams You are
NARHC Spring Institute Tuesday, March 15, 2016 San Antonio Conference Breakouts Your choice Regency Ballroom E Mac Discussion: Novitas Kim Robinson Live Oak Mac Discussion: Noridian Tana Williams You are
Coding and Billing for Lifestyle Medicine
 Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers. Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW
 Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW Objectives Answer questions specific to FQHC and Primary
Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW Objectives Answer questions specific to FQHC and Primary