Medical Decision Making
|
|
|
- Opal Ford
- 6 years ago
- Views:
Transcription

1 Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com February 2012

2 What s he thinking?
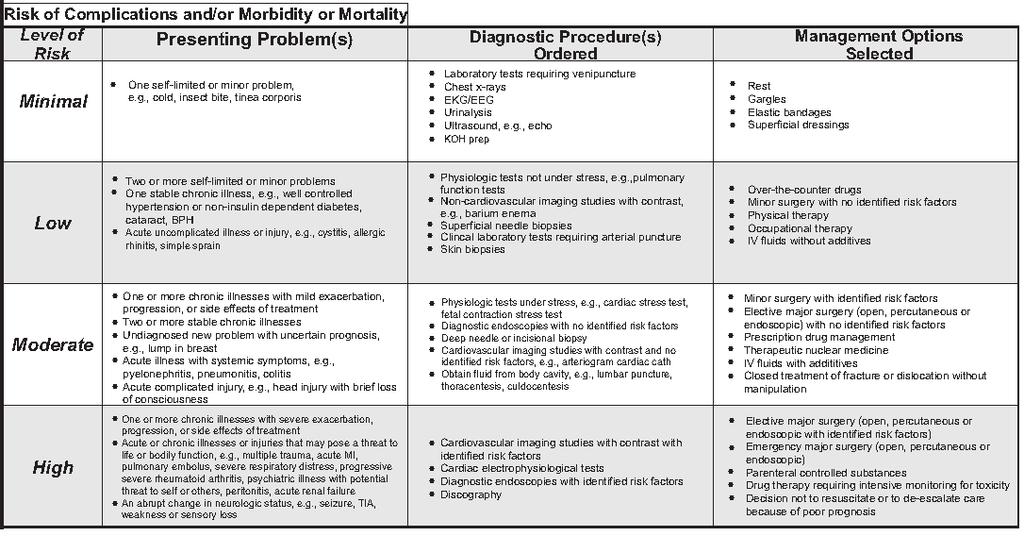
3 What Is the Table of Risk? 1 of 7 tables in the 1995 and 1997 E/M Documentation and Coding Guidelines. 1 of 3 preliminary tables that you can use along with the problem categories table and the type of data table, to determine the level of decision-making

4 Table of Risk
5 Why Should I Use the Sheets? support for your physician s code selection check your physicians levels Watch out: You might have to use a different audit tool for some carriers. TrailBlazer (Medicare Part B carrier for Texas, Virginia, Maryland and Delaware) has developed its own counting system

6
7 How Does Risk Tie Into MDM? Medical decision-making (MDM) is comprised of: 1. Number of diagnoses or management options 2. Amount and/or complexity of data to be reviewed 3. Risk of complications and/or morbidity or mortality physician must meet or exceed 2 of the 3 elements


8 How Should I Evaluate Type? You can t read your physician s mind They can help you see what was involved by completely documenting the process include all diagnoses and any suspected problems or concerns, including rule-outs Don t overlook: You won t code the rule-outs, but documenting them shows a more involved MDM type.
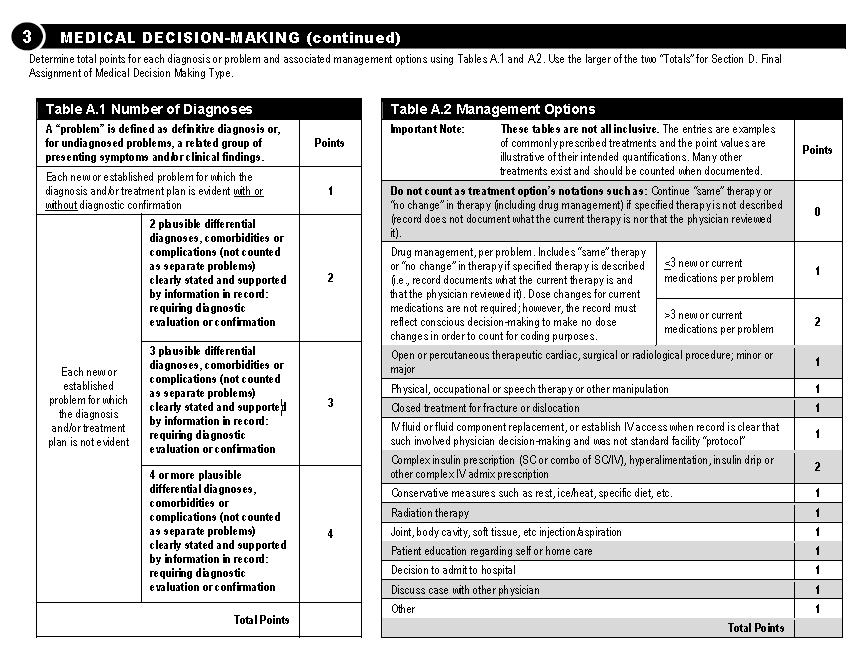
9 What Should I Look For? To weigh the type of risk, zoom in on: 1. Diagnosis 2. Status 3. Risks, treatments or management Map these to the CMS medical point-making system.
10
11 Example An ENT sees a patient with a diagnosis of otitis media (OM) and decides the patient requires tubes. The physician orders no tests and reviews no records. The patient is scheduled for tympanostomy (69436, Tympanostomy [requiring insertion of ventilating tube], general anesthesia).
12 Classify Problem s Status - Table 1 Follow these rules: If the ENT has previously treated the patient for OM, CMS considers the problem established and awards 2 points for an established problem that is inadequately controlled, worsening or failing to progress as expected If this is the first time the ENT is treating the patient for OM, you should consider the diagnosis a new problem, which is worth three points
13 Table 1 con t Why is there a point difference? CMS expects that the decision-making for a known problem is less than that of a new problem Who is the problem new to? The sheet indicates to the examiner. The problem has to be new to that provider. The increased score for a new problem is given because working up a new problem involves more work than assessing a problem that is established or familiar to the physician.
14 Self-Limited or Minor Examples on Table of Risk: Cold Insect Bite Tinea Corporosis assign 1 point
15 Self-Limited or Minor Definition: A problem that runs a definite and prescribed course, is transient in nature, and is not likely to permanently alter health status OR has a good prognosis with management/compliance.
16 Table 1 cont d CMS guidelines state, The assessment of risk of the presenting problem(s) is based on the risk related to the disease process anticipated between the present encounter and the next one. Risk measures the chance of the patient becoming worse from the time he leaves the physician s care to the next visit. A common cold carries minimal risk, consistent with the definition of a minor or self-limited problem.
17 Example An established male patient previously diagnosed as a controlled-diabetic presents with complaints of a runny nose and congestion without any other symptoms. Ignoring the co morbidities and listing only the presenting problem diagnosis, will make the visit qualify for the lowest risk level. The physician should also consider the effect the patient s diabetes has on management options, and if the physician treats the condition, they should report (Diabetes mellitus ) for addressing the underlying disease. Documentation guidelines state, Co morbidities/underlying diseases or other factors that increase the complexity of medical decision making by increasing the risk of complications, morbidity, and/or mortality should be documented.
18 Example An ENT sees a patient with a diagnosis of otitis media (OM) and decides the patient requires tubes. The physician orders no tests and reviews no records. The patient is scheduled for tympanostomy (69436, Tympanostomy [requiring insertion of ventilating tube], general anesthesia).
19 Calculate Reviewed Data The ENT did not review any data so he receives a 0 in this table. Remember to map your CPT codes to the areas listed in the Amount and/or Complexity of Data Reviewed table. Give 1 point for clinical lab tests like urinalysis or a strep test. (80000 series codes) Don t miss: The table counts medicine tests (90000 codes) separately. If a physician reviews an x-ray and orders an ECG, give 1 point for each of these tests.
20 Don t Double Dip! If the physician is coding the service like an x-ray, allergy testing, or an ENG at this service or another, they are already receiving credit for the review in the test code. Give points for work the physician could not otherwise get credit for. ei: a strep test that an outside lab is reading or an x-ray that an outside radiologist reads Do not report [E/M] services for test interpretation and report.
21 Data cont d Poor historian record who the historian is why the patient is not giving the history.

22 Example A babysitter attempting to give the history for a small child. If time doesn t dominate these encounters qualifying them for time-based coding, consider giving a point in this table for decision to obtain history from someone other than parent. The Coding Institute LLC, 2222 Sedwick Drive, Durham, NC Phone: (866) customerservice@supercoder.com 22
23 Select Risk Level based on the single highest element identified in the table of risk s three columns (1 of 3). Do not need one element in each column.
24
25 Look to History OM Patient Should you classify OM with a decision for tubes as a presenting problem that is stable chronic (low), acute uncomplicated illness (low), or acute illness with systemic symptoms (moderate)? If there is documented hearing loss, balance dysfunction, speech/language delay, tympanic membrane rupture, you could argue that it represents an acute or chronic illness that may pose a risk to loss of function, classifying the presenting problem as high.
26 Count Tests/Labs - Column 2 To calculate the diagnostic procedures level, you ll focus on any workup the Otolaryngologist ordered. Because the physician in the OM case study did not order or review any diagnostic procedures, you have no circle in column two.
27

28 Tip: Check Hx check if the patient has any identified risk factors refers to the patient s unique medical history that might affect the outcome. Asthma example: circle "minor surgery with identified risk factors ups level from low to moderate.
29 Jump to High for Risk Exceptions diagnostic endoscopies with no identified risk factors = moderate risk diagnostic endoscopies with identified risk factors = high risk Don t increase the risk factor just because the patient s undergoing a scope.
30 Jump to High for Risk Exceptions Do this: Usually give a physician moderate risk credit for ordering a scope. All patients undergoing an endoscopy face a certain amount of risk, so the ordering of the endoscopy is always the same. Exception: If a patient has identified risk factors, increase the risk factor from moderate to high.
31 Weighing Medication = Moderate Giving samples involves this same process. How AMA Weighs Managing Drugs The table of risk in the AMA-approved 1995 E/M guidelines lists prescription drug management as a common clinical example of moderate risk. The provider has to evaluate the suitability of the patient for the medication and weigh the benefits and risks.
32 Weighing Medication cont d What Counts as Prescription/Drug? Giving samples with or without a prescription all falls under prescription drug management. The process of prescription drug management would include giving the patient the actual meds as samples, the thought process and risk would remain the same as writing it down on a piece of paper. Example: A female patient has allergic rhinitis. The allergist gives her samples of Astelin to try as needed. He tells the patient to call in for a prescription if she feels the prescription helps. This case constitutes prescription management.


33 OTC = low risk Risk assessment relates to the disease process anticipated between the present encounter and the next one.
 and documentation support a chronic illness with progression, child who is new to the ENT has no comorbidities.")
34 Identify Risk With Highest Circle chronic otitis media with effusion (381.3) and documentation support a chronic illness with progression, child who is new to the ENT has no comorbidities. Assign the level based on the highest circle. The highest level is moderate.

35 Tally Final MDM enter the 3 tables scores in the Final Result for Complexity table. Determine the final score using 2/3 elements.
36 No Column Has 2 Circles draw a line down the column with the second circle from the left Example: A patient has allergic rhinitis that s usually controlled with Allegra-D but weather changes trigger the patient s allergies, which precipitates her sinusitis. The patient s sinusitis is a new problem to the pediatrician and he plans no additional work-up and orders no tests. The patient, an adolescent, gives her own history. The pediatrician has previously treated the patient s allergies and writes her a prescription telling her to fill it if after she finishes the samples provided. She decides the Xyzal is decreasing her sinusitis and allergic rhinitis exacerbations.

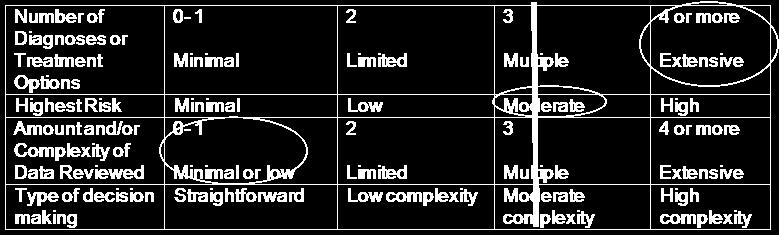
37 No Column Has 2 Circles
38 Combining History, Exam, MDM Example: When a patient comes into the office complaining of chest pain, we often order lab work, an ECG, and send the patient to the hospital. These instances involve moderate to high risk but we do not perform a complete review of systems (ROS) due to the presenting problem s emergent nature. Will these be level 4 or 5 established patient office visits?
39 Answer: Choose level based on the medically necessary history, exam, and medical decision making (MDM) that is performed and documented at each encounter. Probable combos: detailed history + detailed/comprehensive exam + mod/high MDM MDM, plus the amount of exam, ultimately determine whether or
40 MDM 4 points in the "Number of Diagnoses or Treatment Options" area for the new problem to provider with additional work-up planned total of 2 points in the "Amount and/or Complexity of Data to be Reviewed" section. 1 point for ordering lab work 1 point for ordering the ECG Because the diagnoses level puts you at a high level and the data amount is at a low level, the risk will determine whether the MDM is high complexity (if risk is high) or moderate complexity (if risk is moderate).
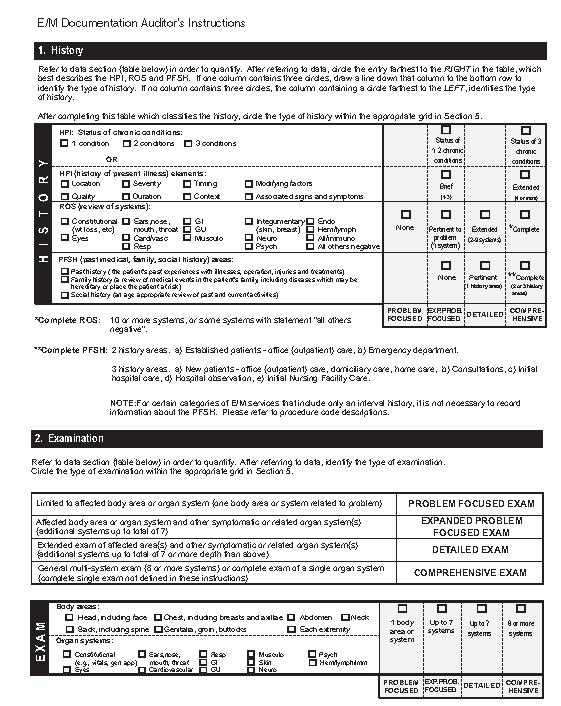
41 History Extended HPI - asking the patient about the severity, duration, quality, context, etc. of the pain Pertinent PFSH - any past personal or family history of heart disease Detailed ROS - questions about the constitutional and cardiac systems Extended HPI + extended ROS + pertinent PFSH = detailed history.
42 Which Exam Level? Comprehensive exam - 8 or more systems -- such as constitutional, eyes, ENT, detailed cardio, respiratory, skin, neurological, and psychological Detailed exam - If the severity didn t allow for anything other than constitutional (vitals, general appearance) and detailed cardio, you may still be at a detailed exam.

43 Visit SuperCoder.com Get mini ICD-10 Training Jen Godreau AAPC April 1-4 AHIMA certified ICD-10 training instructor Suzanne Leder, CPC, COBGC Win SuperCoder T-shirts, mouse pads, & more! Booth 100

44 Thank you SuperCoder.com Better Coding!
Start with the Problem
 Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Medical Necessity verses Medical Decision Making. Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC
 Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Evaluation & Management
 Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
6/14/2017. Evaluation and Management Coding. Jeffrey D. Lehrman, DPM, FASPS, MAPWCA
 Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Evaluation and Management Auditing Back to the Basics. Objectives. Audit Start with the benchmarks CMS MEDPAR by specialty 4/22/2013
 Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
NEXTGEN E&M CODING DEMONSTRATION
 NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
Presented for the AAPC National Conference April 4, 2011
 Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC
 Service in RHC") How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
NEXTGEN E&M CODING DEMONSTRATION
 NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
Evaluation and Management
 Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
E/M Auditing: History is the Key
 E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation
 A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
CODING vs AUDITING Does it all boil down to Medical Necessity?
 PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
E/M: Coding Opportunities- Documentation is key
 E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
The World of Evaluation and Management Services and Supporting Documentation
 The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
Demonstrating the Chain of Medical Necessity. Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President
 Demonstrating the Chain of Medical Necessity Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science,
Demonstrating the Chain of Medical Necessity Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science,
Anthem Blue Cross and Blue Shield Commercial Professional Reimbursement Policy
 Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
Advanced E/M Auditing: Secrets to Success
 Advanced E/M Auditing: Secrets to Success Presented by Carrie Severson CPC, CPC-H, CPMA, CPC-I Senior Auditor, AAPC Client Services Why We Are Here OIG Report (OEI-04-10-00180) Coding Trends of Medicare
Advanced E/M Auditing: Secrets to Success Presented by Carrie Severson CPC, CPC-H, CPMA, CPC-I Senior Auditor, AAPC Client Services Why We Are Here OIG Report (OEI-04-10-00180) Coding Trends of Medicare
Getting Paid for What You Do! Coding 2010
 Getting Paid for What You Do! Coding 20 Children s Mercy Health Network 11/17/09 Richard H. Tuck, MD, FAAP Disclosure I have financial relationships or interests with proprietary entities producing health
Getting Paid for What You Do! Coding 20 Children s Mercy Health Network 11/17/09 Richard H. Tuck, MD, FAAP Disclosure I have financial relationships or interests with proprietary entities producing health
Evaluation & Management 101 for Clinicians
 Evaluation & Management 101 for Clinicians Kerin Draak, MSN, WHNP BC, CPC, CEMC, COBGC, CPC I System Director of Clinical & Financial Integration Hospital Sisters Health System This is the Full Title of
Evaluation & Management 101 for Clinicians Kerin Draak, MSN, WHNP BC, CPC, CEMC, COBGC, CPC I System Director of Clinical & Financial Integration Hospital Sisters Health System This is the Full Title of
SPECIALTY TIP #13 Evaluation and Management (E&M)
") ICD- 10 SPECIALTY TIPS SPECIALTY TIP #13 Evaluation and Management (E&M) This topic is being addressed in our Specialty Tips series as most providers rate Evaluation and Management as one of the more challenging
ICD- 10 SPECIALTY TIPS SPECIALTY TIP #13 Evaluation and Management (E&M) This topic is being addressed in our Specialty Tips series as most providers rate Evaluation and Management as one of the more challenging
Few non-clinical issues have created as
 from October 2001 How to Get All the 99214s You Deserve It s easier than you might think to get what s coming to you. Emily Hill, PA-C Few non-clinical issues have created as much controversy as the CPT
from October 2001 How to Get All the 99214s You Deserve It s easier than you might think to get what s coming to you. Emily Hill, PA-C Few non-clinical issues have created as much controversy as the CPT
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule. Grace Wilson, RHIA
 Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Care Transition Strategies: The 2013 Transition Care Management Codes
 Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
Documentation for ED Visits with "Additional Work-Up" Planned. Presented by Rae Jimenez, CPC, CDEO, CPB, CPMA, CPPM, CPC-I, CCS
 Documentation for ED Visits with "Additional Work-Up" Planned Presented by Rae Jimenez, CPC, CDEO, CPB, CPMA, CPPM, CPC-I, CCS Course Objectives Discuss gray areas for E/M selection for the professional
Documentation for ED Visits with "Additional Work-Up" Planned Presented by Rae Jimenez, CPC, CDEO, CPB, CPMA, CPPM, CPC-I, CCS Course Objectives Discuss gray areas for E/M selection for the professional
follow-up for pneumonia
 Questions How long can I access the on demand version. Where can I ask questions after the webinar? Can the CC be used as an element of HPI? I have a co-worker who believes it cannot be used at all towards
Questions How long can I access the on demand version. Where can I ask questions after the webinar? Can the CC be used as an element of HPI? I have a co-worker who believes it cannot be used at all towards
Transition Care Management Update: Practical Applications for 2016
 60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
Documenting & Coding for Compliance
 Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Preventive and Sick Visits Same Day. Objectives
 Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
Code Assignment & Validation
 Code Assignment & Validation Evaluation & Management Services Presenter Santa Allaire, RHIT, CCS, CPC, CIRCC, CEMC Disclaimer This presentation is for general education purposes only. The information contained
Code Assignment & Validation Evaluation & Management Services Presenter Santa Allaire, RHIT, CCS, CPC, CIRCC, CEMC Disclaimer This presentation is for general education purposes only. The information contained
Exam. Jen Godreau, BA, CPC, CPEDC. Director of Development & Operations Supercoder.com January 2012
 Exam Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com January 2012 Agenda 1. Embrace the GRAY! 2. Put your clinical savvy to the TEST 3. Make your
Exam Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com January 2012 Agenda 1. Embrace the GRAY! 2. Put your clinical savvy to the TEST 3. Make your
Medical Necessity: Not just LCD. Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC
 Medical Necessity: Not just LCD Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC Medical Necessity In The Law Social Security Act, Title XVIII Section 1862 (a) (1)
Medical Necessity: Not just LCD Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC Medical Necessity In The Law Social Security Act, Title XVIII Section 1862 (a) (1)
Getting paid properly requires a thorough knowledge of the rules.
 Selecting E/M Codes For Established Patients Getting paid properly requires a thorough knowledge of the rules. Kenneth F. Malkin, D.P.M. Bio: Dr. Malkin is a diplomate of the American Board of Quality
Selecting E/M Codes For Established Patients Getting paid properly requires a thorough knowledge of the rules. Kenneth F. Malkin, D.P.M. Bio: Dr. Malkin is a diplomate of the American Board of Quality
Evaluation & Management Documentation Training Tool
 Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table, which
Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table, which
Evaluation and Management Services
 Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
How to Write a Medical Note for the. Foundations of Doctoring Course and Beyond: Demystifying the Focused (SOAP) Note
 Note") How to Write a Medical Note for the Foundations of Doctoring Course and Beyond: Demystifying the Focused (SOAP) Note and the Comprehensive (H&P) Note by Todd Guth, MD Overview of the Medical Note Medical
How to Write a Medical Note for the Foundations of Doctoring Course and Beyond: Demystifying the Focused (SOAP) Note and the Comprehensive (H&P) Note by Todd Guth, MD Overview of the Medical Note Medical
How does one report the performance of both a screening mammogram on the right breast and a diagnostic on the left breast at the same encounter?
 1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
See the Time chapter for complete instructions regarding how to code using time as the controlling E/M factor.
 2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
EVALUATION & MANAGEMENT SERVICES CODING. Part I: What is an E&M? Where do you start? Jennifer Jones, CPC, CPC-I
 DOTHAN AL CHAPTER AAPC FALL WORKSHOP Friday November 17, 2017 REGISTRATION BEGINS AT 7:15 am PROGRAM TIME IS 8:00 am 12:30 pm Earn 4 CEU s for a Fee of only $50.00 per attendee (Snacks will be provided
DOTHAN AL CHAPTER AAPC FALL WORKSHOP Friday November 17, 2017 REGISTRATION BEGINS AT 7:15 am PROGRAM TIME IS 8:00 am 12:30 pm Earn 4 CEU s for a Fee of only $50.00 per attendee (Snacks will be provided
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
Evaluation & Management Documentation Training Tool
 A MS Medicare Administrative ontractor Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest
A MS Medicare Administrative ontractor Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest
Focus On Observation
 Focus On Observation Introduction CPT and CMS Requirements CPT Codes Documentation Requirements Observation Coding: Facility Considerations 2 LogixHealth s unsurpassed service stems from the fact that
Focus On Observation Introduction CPT and CMS Requirements CPT Codes Documentation Requirements Observation Coding: Facility Considerations 2 LogixHealth s unsurpassed service stems from the fact that
See the Time chapter for complete instructions on how to code using time as the controlling factor when selecting an E/M code.
 2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
9/17/2018. Place of Service Type of Service Patient Status
 Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Evaluation and Management Services Guide
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide November 2014 / ICN: 006764 PREFACE This guide is offered as a reference tool
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide November 2014 / ICN: 006764 PREFACE This guide is offered as a reference tool
Institute on Medicare and Medicaid Payment Issues March 28 30, 2012 Robert A. Pelaia, JD, CPC
 I. Introduction Institute on Medicare and Medicaid Payment Issues March 28 30, 2012 Robert A. Pelaia, JD, CPC Senior University Counsel for Health Affairs - Jacksonville 904-244-3146 robert.pelaia@jax.ufl.edu
I. Introduction Institute on Medicare and Medicaid Payment Issues March 28 30, 2012 Robert A. Pelaia, JD, CPC Senior University Counsel for Health Affairs - Jacksonville 904-244-3146 robert.pelaia@jax.ufl.edu
Coding for the Practitioner
 Coding for the Practitioner Prepared for Coalition of State Rheumatology Organizations National Rheumatology Fellows Conference February 2018 Presented by: Jean Acevedo, LHRM, CPC, CHC, CENTC Disclaimer
Coding for the Practitioner Prepared for Coalition of State Rheumatology Organizations National Rheumatology Fellows Conference February 2018 Presented by: Jean Acevedo, LHRM, CPC, CHC, CENTC Disclaimer
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
E & M Coding. Welcome To The Digital Learning Center. Today s Presentation. Course Faculty. Beyond the Basics. Presented by
 Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Charting for Midwives. Getting Credit For the Work You Do
 Charting for Midwives Getting Credit For the Work You Do Moving Beyond S.O.A.P. The U.S. health care system is moving past fee-for-service billing. In the future, the providers will be reimbursed based
Charting for Midwives Getting Credit For the Work You Do Moving Beyond S.O.A.P. The U.S. health care system is moving past fee-for-service billing. In the future, the providers will be reimbursed based
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
*OB/Gyn. Hospital Billing. April 2, 2014 Erika Bloomquist, CPC
 OB/Gyn Hospital Billing April 2, 2014 Erika Bloomquist, CPC Initial Date Diagnoses Billing Level Code Patient Label ZK 3/1 1,2 A1 Or two patient identifiers BB 3/2 1,2 S2 TS 3/3 1,2 D1 Inpt. Obs Transfer
OB/Gyn Hospital Billing April 2, 2014 Erika Bloomquist, CPC Initial Date Diagnoses Billing Level Code Patient Label ZK 3/1 1,2 A1 Or two patient identifiers BB 3/2 1,2 S2 TS 3/3 1,2 D1 Inpt. Obs Transfer
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
Coding Complexities of Critical Care
 Coding Complexities of Critical Care Jill Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing.
Coding Complexities of Critical Care Jill Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing.
The E/M Essentials Pocket Guide
 The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CCS-P, CEMC The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CEMC, CCS-P The E/M Essentials Pocket Guide is published by HCPro, a division
The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CCS-P, CEMC The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CEMC, CCS-P The E/M Essentials Pocket Guide is published by HCPro, a division
Man s mind, once stretched by a new idea, never returns to its original dimensions. Oliver Wendell Holmes
 Man s mind, once stretched by a new idea, never returns to its original dimensions. Oliver Wendell Holmes This education is Part 7 of a 9-part series on documenting and selecting the level of service for
Man s mind, once stretched by a new idea, never returns to its original dimensions. Oliver Wendell Holmes This education is Part 7 of a 9-part series on documenting and selecting the level of service for
E/M Fast Finder. CPT only 2012 American Medical Association. 1 All Rights Reserved.
 E/M Fast Finder The E/M Fast Finder is a carry-along reference to assist in assigning the Evaluation and Management (E/M) codes that are part of the 99000 series of Current Procedural Terminology (CPT
E/M Fast Finder The E/M Fast Finder is a carry-along reference to assist in assigning the Evaluation and Management (E/M) codes that are part of the 99000 series of Current Procedural Terminology (CPT
SERVICE CODE CLARIFICATIONS
 SERVICE CODE CLARIFICATIONS Service Description Assertive Community Treatment (ACT) Assisted Outpatient Treatment (AOT) HCPCS Code Description Explanation of Code Utilization H0039 ACT Report only face-to-face
SERVICE CODE CLARIFICATIONS Service Description Assertive Community Treatment (ACT) Assisted Outpatient Treatment (AOT) HCPCS Code Description Explanation of Code Utilization H0039 ACT Report only face-to-face
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
NEW YORK STATE MEDICAID PROGRAM PODIATRY PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM PODIATRY PROCEDURE CODES Table of Contents GENERAL INFORMATION AND INSTRUCTIONS... 3 MMIS MODIFIERS... 12 LABORATORY SERVICES PERFORMED IN A PODIATRIST'S OFFICE... 13 MEDICAL
NEW YORK STATE MEDICAID PROGRAM PODIATRY PROCEDURE CODES Table of Contents GENERAL INFORMATION AND INSTRUCTIONS... 3 MMIS MODIFIERS... 12 LABORATORY SERVICES PERFORMED IN A PODIATRIST'S OFFICE... 13 MEDICAL
Walk-in Clinic. Dear Patients. Frequently Asked Questions (FAQ)
") Walk-in Clinic Klamath Tribal Health & Family Services 330 Chiloquin Boulevard Chiloquin, OR 97624 (541) 882-1487 Frequently Asked Questions (FAQ) Monday Friday, 8:00 a.m. 3:30 p.m. * First Wednesday of
Walk-in Clinic Klamath Tribal Health & Family Services 330 Chiloquin Boulevard Chiloquin, OR 97624 (541) 882-1487 Frequently Asked Questions (FAQ) Monday Friday, 8:00 a.m. 3:30 p.m. * First Wednesday of
8/19/2017. The OIG Report
 This presentation was created by me with the best intentions and believable resources. I however am not a lawyer, doctor or self-proclaimed expert, but I have watched plenty on TV. The information and
This presentation was created by me with the best intentions and believable resources. I however am not a lawyer, doctor or self-proclaimed expert, but I have watched plenty on TV. The information and
Message Response Message
 Message If established pt wouldn't 2 out of 3 still require the level for slide 5? Response Message Can you re-state your question? I am unclear on what you are asking. Thanks You stated that even when
Message If established pt wouldn't 2 out of 3 still require the level for slide 5? Response Message Can you re-state your question? I am unclear on what you are asking. Thanks You stated that even when
FindACode.com Presents: Integrating NPP into E/M for Compliance and Quality Care. Excerpts from:
 FindACode.com Presents: Integrating NPP into E/M for Compliance and Quality Care Excerpts from: Practical E/M: Documentation and Coding Solutions for Quality Patient Care by Dr. Stephen R. Levinson To
FindACode.com Presents: Integrating NPP into E/M for Compliance and Quality Care Excerpts from: Practical E/M: Documentation and Coding Solutions for Quality Patient Care by Dr. Stephen R. Levinson To
Billing & Coding. Tim Shope, MD, MPH General Academic Pediatrics Continuity Clinic Conference Week of August 14, 2017
 Billing & Coding Tim Shope, MD, MPH General Academic Pediatrics Continuity Clinic Conference Week of August 14, 2017 Learning Objectives After interacting with these materials, the learner should be able
Billing & Coding Tim Shope, MD, MPH General Academic Pediatrics Continuity Clinic Conference Week of August 14, 2017 Learning Objectives After interacting with these materials, the learner should be able
Protocol: Name of supervising ED provider: Name of RDTC Faculty: Disposition: Date: / / Time: : (military)
") RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
CPT Coding Changes in 2013: Billing, Reimbursement and IT
 CPT Coding Changes in 2013: Billing, Reimbursement and IT Texas Council of Community Centers Presented by: David R. Swann, MA, LCAS, CCS, LPC, NCC Senior Healthcare Integration Consultant Phone: 336-386-9801
CPT Coding Changes in 2013: Billing, Reimbursement and IT Texas Council of Community Centers Presented by: David R. Swann, MA, LCAS, CCS, LPC, NCC Senior Healthcare Integration Consultant Phone: 336-386-9801
Are they coming to get you! Todd Thomas, CCS-P
 Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
History of CPT. History of CPT. History of CPT. History of CPT. History of E&M. Workshop Evaluation and Management Coding on the River 2010
 Workshop Evaluation and Management Coding on the River 2010 Presented By: Freda Brinson, CPC, CPC-H, CEMC Freda.brinson@aapcca.org or brinsonfr@sjchs.org Faye Grile, CPC, CPMA, CEMC grilefa1@memorialhealth.com
Workshop Evaluation and Management Coding on the River 2010 Presented By: Freda Brinson, CPC, CPC-H, CEMC Freda.brinson@aapcca.org or brinsonfr@sjchs.org Faye Grile, CPC, CPMA, CEMC grilefa1@memorialhealth.com
Presented by Teresa Thompson, CPC TM Consulting, Inc
 Presented by Teresa Thompson, CPC TM Consulting, Inc Teresathom@aol.com I have no disclosure to report Disclosure information No relevant relationships disclosed Tips for Improving Your Revenue Coding
Presented by Teresa Thompson, CPC TM Consulting, Inc Teresathom@aol.com I have no disclosure to report Disclosure information No relevant relationships disclosed Tips for Improving Your Revenue Coding
Urgent Care Coding. Webinar Subscription Access Expires December 31.
 Urgent Care Coding Questions Answers Webinar Subscription Access Expires December 31. How long can I access the on demand version? You will find that in the same instructions box you utilized to access
Urgent Care Coding Questions Answers Webinar Subscription Access Expires December 31. How long can I access the on demand version? You will find that in the same instructions box you utilized to access
Electronic Health Records - Advantages and Pitfalls of Documentation
 Electronic Health Records - Advantages and Pitfalls of Documentation Kansas City, KS HCCA Regional Conference September 25, 2015 1:00 P.M. 2:00 P.M. Presented by: Cynthia A. Swanson, RN, CPC, CEMC, CHC,
Electronic Health Records - Advantages and Pitfalls of Documentation Kansas City, KS HCCA Regional Conference September 25, 2015 1:00 P.M. 2:00 P.M. Presented by: Cynthia A. Swanson, RN, CPC, CEMC, CHC,
Cigna Medical Coverage Policy
 Cigna Medical Coverage Policy Subject Observation Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 5 Effective Date... 10/15/2014 Next Review
Cigna Medical Coverage Policy Subject Observation Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 5 Effective Date... 10/15/2014 Next Review
Meet the Presenter. Welcome to PMI s Webinar Presentation. E/M Auditing - Telling an Accurate Patient Story. On the topic:
 Welcome to PMI s Webinar Presentation Brought to you by: Practice Management Institute pmimd.com Meet the Presenter On the topic: Pam Joslin, MM, CMC, CMIS, CMOM E/M Auditing - Telling an Accurate Patient
Welcome to PMI s Webinar Presentation Brought to you by: Practice Management Institute pmimd.com Meet the Presenter On the topic: Pam Joslin, MM, CMC, CMIS, CMOM E/M Auditing - Telling an Accurate Patient
Pediatric Coding and Billing. Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC
 Pediatric Coding and Billing Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Evaluation and Management Office Hospital Counseling Well-child Care
Pediatric Coding and Billing Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Evaluation and Management Office Hospital Counseling Well-child Care
Advanced Evaluation and. AAPC Regional Conference Chicago 10/27/12
 Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
OVERVIEW OF ESSENTIAL CHARTING ELEMENTS FOR THE EMERGENCY DEPARTMENT
 OVERVIEW OF ESSENTIAL CHARTING ELEMENTS FOR THE EMERGENCY DEPARTMENT ALL CHARTING NEEDS TO BE FINISHED AT THE END OF YOUR SHIFT PRIOR TO LEAVING THE ED IF YOU HAVE ANY QUESTIONS, ASK FOR HELP! All of the
OVERVIEW OF ESSENTIAL CHARTING ELEMENTS FOR THE EMERGENCY DEPARTMENT ALL CHARTING NEEDS TO BE FINISHED AT THE END OF YOUR SHIFT PRIOR TO LEAVING THE ED IF YOU HAVE ANY QUESTIONS, ASK FOR HELP! All of the
Basic Teaching Physician Presence and Documentation
 Basic Teaching Physician Presence and Documentation Welcome to the Children s University Medical Group (CUMG) training on the Teaching Physician Presence and Documentation. The goal of this module is to
Basic Teaching Physician Presence and Documentation Welcome to the Children s University Medical Group (CUMG) training on the Teaching Physician Presence and Documentation. The goal of this module is to
FAQ for Coding Encounters in ICD 10 CM
 FAQ for Coding Encounters in ICD 10 CM Topics: Encounter for Routine Health Exams Encounter for Vaccines Follow Up Encounters Coding for Injuries Encounter for Suture Removal External Cause Codes Tobacco
FAQ for Coding Encounters in ICD 10 CM Topics: Encounter for Routine Health Exams Encounter for Vaccines Follow Up Encounters Coding for Injuries Encounter for Suture Removal External Cause Codes Tobacco
Risk Adjustment and Hierarchial Condition Category Coding and Auditing
 December 2, 2016 Risk Adjustment and Hierarchial Condition Category Coding and Auditing Risk Adjustment (RA) and Hierarchical Condition Category (HCC) coding is a payment model mandated by CMS in 1997,
December 2, 2016 Risk Adjustment and Hierarchial Condition Category Coding and Auditing Risk Adjustment (RA) and Hierarchical Condition Category (HCC) coding is a payment model mandated by CMS in 1997,
RVU KILLERS The Most Common Reimbursement Documentation Errors. Michael Granovsky MD CPC CEDC FACEP President LogixHealth
 RVU KILLERS The Most Common Reimbursement Documentation Errors Michael Granovsky MD CPC CEDC FACEP President LogixHealth Documentation-Why Does It Matter? Must communicate to the payer your concerns and
RVU KILLERS The Most Common Reimbursement Documentation Errors Michael Granovsky MD CPC CEDC FACEP President LogixHealth Documentation-Why Does It Matter? Must communicate to the payer your concerns and
News SEPTEMBER. Hospital Outpatient Quality Reporting Program. Support Contractor
 Volume 1, Issue 4 Hospital Outpatient Quality Reporting Program Support Contractor News SEPTEMBER 2011 In This Issue... Emergency Department Arrival and Departure Times Page 2 Hospital OQR Benchmarks Page
Volume 1, Issue 4 Hospital Outpatient Quality Reporting Program Support Contractor News SEPTEMBER 2011 In This Issue... Emergency Department Arrival and Departure Times Page 2 Hospital OQR Benchmarks Page
HEALTH DEPARTMENT BILLING GUIDELINES
 HEALTH DEPARTMENT BILLING GUIDELINES Acknowledgement: Current Procedural Terminology (CPT ) is copyright 2017 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative
HEALTH DEPARTMENT BILLING GUIDELINES Acknowledgement: Current Procedural Terminology (CPT ) is copyright 2017 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative
HC 1930 HC 1930 ICD-9-CM III/CPT Coding II
 South Central College HC 1930 HC 1930 ICD-9-CM III/CPT Coding II Course Information Description Total Credits 4.00 Total Hours 80.00 Types of Instruction This course is a continuation of HC 1920, 1925,
South Central College HC 1930 HC 1930 ICD-9-CM III/CPT Coding II Course Information Description Total Credits 4.00 Total Hours 80.00 Types of Instruction This course is a continuation of HC 1920, 1925,
Health Assessment Student Handbook
 Health Assessment Student Handbook Fall 2017 Your guide to the Shadow Health Digital Clinical Experience UGV.1 Table of Contents WELCOME!... 3 HEALTH HISTORY Instructions... 4 HEENT Instructions... 5 RESPIRATORY
Health Assessment Student Handbook Fall 2017 Your guide to the Shadow Health Digital Clinical Experience UGV.1 Table of Contents WELCOME!... 3 HEALTH HISTORY Instructions... 4 HEENT Instructions... 5 RESPIRATORY
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
Crash Course in Medical Necessity for E/M Coders
 Crash Course in Medical Necessity for E/M Coders Stephanie Cecchini, CPC, CEMC, CHISP About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing solutions
Crash Course in Medical Necessity for E/M Coders Stephanie Cecchini, CPC, CEMC, CHISP About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing solutions
Office of Compliance. Complete & Accurate Documentation Core Curriculum for GWU Residents
 Office of Compliance Complete & Accurate Documentation Core Curriculum for GWU Residents December 3, 2014 Medical Record The medical record tells the story of the patient from start to finish. If the story
Office of Compliance Complete & Accurate Documentation Core Curriculum for GWU Residents December 3, 2014 Medical Record The medical record tells the story of the patient from start to finish. If the story
Crash Course in Medical Necessity for E/M Coders. Regional Conference
 Crash Course in Medical Necessity for E/M Coders Regional Conference About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing solutions that allow coders
Crash Course in Medical Necessity for E/M Coders Regional Conference About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing solutions that allow coders
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice
 Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Patient Health Education: What Physicians Need to Know to Thrive in Today s Healthcare Environments
 Patient Health Education: What Physicians Need to Know to Thrive in Today s Healthcare Environments Prepared by National Institute of Whole Health www.niwh.org Accredited by the Institute for Credentialing
Patient Health Education: What Physicians Need to Know to Thrive in Today s Healthcare Environments Prepared by National Institute of Whole Health www.niwh.org Accredited by the Institute for Credentialing
Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims
 March 8, 2018 Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims By Kristi Pollard, RHIT, CCS, CPC, CIRCC, AHIMA-approved ICD-10- CM/PCS trainer There is
March 8, 2018 Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims By Kristi Pollard, RHIT, CCS, CPC, CIRCC, AHIMA-approved ICD-10- CM/PCS trainer There is
Implementation Date: January 2018 Clinical Operations
 Magellan Healthcare Clinical guidelines RECORD KEEPING AND DOCUMENTATION STANDARDS Original Date: November 2015 Page 1 of 11 Physical Medicine Clinical Decision Making Last Review Date: June 2017 Guideline
Magellan Healthcare Clinical guidelines RECORD KEEPING AND DOCUMENTATION STANDARDS Original Date: November 2015 Page 1 of 11 Physical Medicine Clinical Decision Making Last Review Date: June 2017 Guideline
Chapter 9 Worksheet Code It
 Class: Date: Chapter 9 Worksheet 3 2 1 Code It True/False Indicate whether the statement is true or false. 1. Notes located beneath headings and/or subheadings apply to all codes in the categories or subcategories.
Class: Date: Chapter 9 Worksheet 3 2 1 Code It True/False Indicate whether the statement is true or false. 1. Notes located beneath headings and/or subheadings apply to all codes in the categories or subcategories.
Paula LeSueur MSN, CNP
 HEDIS Measures 2014 Presented at Envision NM Telehealth April 24, 2014 Paula LeSueur MSN, CNP 1 NEW To connect audio, please telephone 1-877-551-7185. Conference Code 1578316654# Please mute/un-mute your
HEDIS Measures 2014 Presented at Envision NM Telehealth April 24, 2014 Paula LeSueur MSN, CNP 1 NEW To connect audio, please telephone 1-877-551-7185. Conference Code 1578316654# Please mute/un-mute your
2019 Evaluation and Management Coding Advisor. Advanced guidance on E/M code selection for traditional documentation systems
 2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
Risk Adjusted Diagnosis Coding:
 Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare