Choosing Wisely Canada 5 things NOT to do in the ICU
|
|
|
- Albert Lewis
- 6 years ago
- Views:
Transcription




1 Choosing Wisely Canada 5 things NOT to do in the ICU Andre Amaral, MD on behalf of the CWC Critical Care Task Force Assistant Professor Interdepartmental Division of Critical Care Medicine University of Toronto Sunnybrook Health Sciences Centre


2
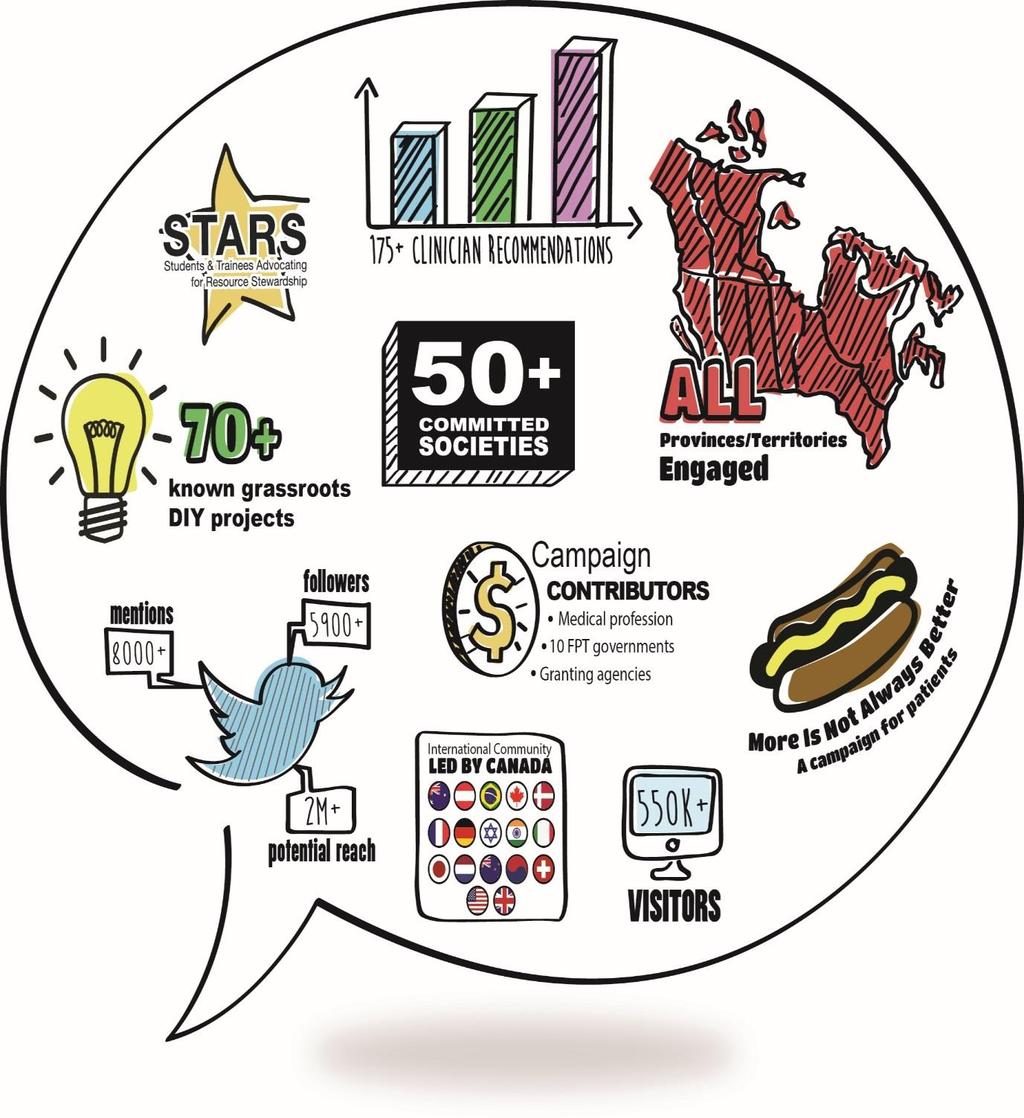
3 Choosing Wisely Canada is a campaign to help clinicians and patients engage in conversations about unnecessary tests and treatments and make smart and effective choices to ensure high-quality care.
4 What is unique about CWC? Clinician led Bottom up approach Focused on common clinical conditions Simple Remarkably rapid uptake
5 Campaign approach Clinicians Societies develop lists Disseminate through multiple channels Patients Develop patient materials Disseminate broadly through multiple channels Media Coordinated approach toward media Multiple voices, a common message Stakeholders Work through health care stakeholder organizations to implement and support adoption
6
7 Online resources Clinician website: Patient website: Twitter: Facebook:

8
9 Methodology Task force from Canadian Critical Care Society Canadian Association of Critical Care Nurses Canadian Society of Respiratory Therapists Representatives from pharmacy, physiotherapy and dietitian
10 Methodology and YOUR opinion! During this presentation we will survey you via SMS and your participation in this survey infers you agree to have results included in the CWC Critical Care Recommendations once ready for publication
11 TASK FORCE MEMBERS Halfkenny-Zellas, C Bazinet, K O Callaghan, N Huberdeau, C Morgan, B Buttazzoni, L Wickson, P Newman, A Downar, J Amaral, A Martin, C Mahan, N McCall, M Zygun, D Cheng, D Granton, J Martin, J Kanji, S Muscedere, J Dhanani, S Fowler, R Fox-Robichaud, A Ménard, C Toma, A
12 1. ITEM GENERATION 1. CCCS Google-groups list 2. Members of the task force
13 Treatments 1. Parenteral nutrition 2. RBC Transfusion 3. Antimicrobials for septic shock 4. Duration of empiric antibiotics 5. HES for resuscitation 6. ino for ARDS 7. Glucose control 8. EPO for critically ill patients without CKD 9. Early goal directed therapy 10. Broad-spectrum antimicrobials 11. Steroids for sepsis 12. Steroids for spinal cord injuries 13. Steroids for patients with TBI 14. Omega-3 fish oils for ARDS/ALI 15. Hyperventilation in TBI 16. Continuous sedation 17. Bronchoscopy for atelectasis 18. End-of-life care 19. Sleep preservation 20. Targeted temperature control post cardiac arrest Procedures 21. NIV for ALI 22. Holding feeds for OR 23. PACs to guide hemodynamic management 24. Craniectomy for TBI 25. Line insertion under US 26. Early mobility 27. Physical and pharmacological restraints Tests 28. Routine CXR 29. Routine blood work 30. BAL for the diagnosis of VAP 31. Follow-up CT scans in CVAs 32. Delirium screening Other 33. Consideration for organ donation 34. Goals of care discussion 35. Physician Assistants in ICU 36. C-spine clearance after trauma 37. Establishing daily goals 38. Family participation in daily rounds
14 2. ITEM SELECTION Task force members prioritized 10 items from this list For the 10 selected items, task force members wrote a DON T statement and brief summary focused on: Existing evidence Extent of overutilization Potential cost-impact
15 2. ITEM SELECTION 1. Don t routinely hold feeds in intubated patients for OR 2. Don t use hydroxyethyl starches in the critically ill 3. Don t limit interactions between the patients and their family 4. Don t routinely keep critically ill patients under bed rest 5. Don t maintain mechanically ventilated patients deeply sedated 6. Don t prolong mechanical ventilation without attempting an SBT 7. Don t transfer a patient out without discussing goals of care 8. Don t withdraw life support before discussing organ donation 9. Don t initiate life support therapies for terminally ill patients 10. Don t order routine chest X-rays, unless to inform a specific decision 11. Don t routinely transfuse PRBC in patients with a Hb > 70 g/l
16
17
18
19 3. ITEM SELECTION (2ND ROUND) Task force members ranked items on: Evidence Prevalence Relevance Ease of implementation Prevention of harm Innovation Cost savings
20 Evidence Prevalence Relevance Ease of Prevention Innovation Cost Average of harm savings (no costs) CXR Sedation Transfusion Early Mobility GOC Discussion SBT Family Interaction HES LST for terminal illness Enteral nutrition Organ Donation
21 Evidence Prevalence Relevance Ease of Prevention Innovation Cost Average of harm savings (no costs) CXR Sedation Transfusion Early Mobility GOC Discussion SBT Family Interaction HES LST for terminal illness Enteral nutrition Organ Donation
22 Evidence Prevalence Relevance Ease of Prevention Innovation Cost Average of harm savings (no costs) CXR Sedation Transfusion Early Mobility GOC Discussion SBT Family Interaction HES LST for terminal illness Enteral nutrition Organ Donation
23 Evidence Prevalence Relevance Ease of Prevention Innovation Cost Average of harm savings (no costs) CXR Sedation Transfusion Early Mobility GOC Discussion SBT Family Interaction HES LST for terminal illness Enteral nutrition Organ Donation
24 #1 DON T LIMIT INTERACTIONS BETWEEN THE PATIENT AND THEIR FAMILY Access for families on rounds, visitation and resuscitation Stickney J Pediatr 2014, Wyskiel Families, systems and health 2015, Oczkowski J Intens Care 2015 Highly valued by families Stelson Am J Crit Care 2016 In the US: 80% units restrict visitation Liu Crit Care 2013
25 #2 DON T PROLONG MECHANICAL VENTILATION BY PRACTICES FACILITATING IMMOBILITY, OVER-USE OF SEDATIVES AND DELAYED ASSESSMENT OF ABILITY TO LIBERATE FROM VENTILATION 58% of patients in Canada did not receive a sedation interruption Burry Can J Anaesth 2014 Adherence to SBTs in US: 9-55% Robertson CCM 2008 Mobility not performed in 60-80% of eligible days in Canada Fan, Amaral. Unpublished data
26 #3 DON T TRANSFER A PATIENT WITH END-STAGE OR TERMINAL ILLNESS OUT OF THE ICU WITHOUT A DISCUSSION ABOUT GOALS OF CARE Overutilization of ICU beds for patients that may not benefit (6.7% in the US) Huyhn, JAMA Int Med 2013 Physicians don t always elicit the preferences of dying patients Downar CCM 2015 Ward physicians may defer conversations to a clinician with ICU experience Jones CCM 2014
27 #4 DON T ORDER ROUTINE CHEST RADIOGRAPHS FOR CRITICALLY ILL PATIENTS, EXCEPT TO ANSWER A SPECIFIC CLINICAL QUESTION RCTs and observational studies find that routine CXRs do not improve outcomes compared with an ondemand CXR strategy Oba Radiology 2010 Meta-analysis of eliminating daily routine CXRs: no affect on mortality (OR 0.92) no effect on ICU LOS (difference = 0.19 days) no effect on ventilator days (difference = 0.33 days) Ganapathy Crit Care 2012
28 #5 DON T ROUTINELY TRANSFUSE RED BLOOD CELLS IN HEMODYNAMICALLY STABLE ICU PATIENTS WITH A HEMOGLOBIN CONCENTRATION GREATER THAN 70 G/L* *A threshold of 80 g/l may be considered for patients undergoing cardiac or orthopedic surgery and those with active cardiovascular disease Unnecessary transfusion of RBCs is more harmful than helpful Carson JAMA 2016 In certain populations, the restrictive arm tested Hb of 80g/L (cardiac surgery, orthopedics, active CV disease)
29
30
31
32 THANK YOU!
Barriers to Early Rehabilitation in Critically Ill Patients. Shannon Goddard, MD Sunnybrook Health Sciences Centre
 Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
5/9/2015. Disclosures. Improving ICU outcomes and cost-effectiveness. Targets for improvement. A brief overview: ICU care in the United States
 Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
ICU. Rotation Goals & Objectives for Urology Residents
 THE UNIVERSITY OF BRITISH COLUMBIA Department of Urologic Sciences Faculty of Medicine Gordon & Leslie Diamond Health Care Centre Level 6, 2775 Laurel Street Vancouver, BC, Canada V5Z 1M9 Tel: (604) 875-4301
THE UNIVERSITY OF BRITISH COLUMBIA Department of Urologic Sciences Faculty of Medicine Gordon & Leslie Diamond Health Care Centre Level 6, 2775 Laurel Street Vancouver, BC, Canada V5Z 1M9 Tel: (604) 875-4301
Penn State Milton S. Hershey Medical Center. Division of Trauma, Acute Care & Critical Care Surgery
 Curriculum Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-SICU The Section Chief for the Emergency General Surgery section within the Division
Curriculum Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-SICU The Section Chief for the Emergency General Surgery section within the Division
1. Receives report from EMS and/or outlying facility. 5. Adheres to safety and universal precaution guidelines.
 Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Getting Operational Leaders on Board to Deliver the Triple Aim
 Session #37 Getting Operational Leaders on Board to Deliver the Triple Aim Lauren Anthony, MD System Medical Director Allina Health Clinical Laboratories Learning Objectives Recognize the three most important
Session #37 Getting Operational Leaders on Board to Deliver the Triple Aim Lauren Anthony, MD System Medical Director Allina Health Clinical Laboratories Learning Objectives Recognize the three most important
a Canadian Critical Care Knowledge Translation Network ac 3 KTion Net
 a Canadian Critical Care Knowledge Translation Network ac 3 KTion Net 1 Learning Objectives To understand the need for knowledge translation (KT) in Critical Care To review the need for measurement as
a Canadian Critical Care Knowledge Translation Network ac 3 KTion Net 1 Learning Objectives To understand the need for knowledge translation (KT) in Critical Care To review the need for measurement as
TheValues History: A Worksheet for Advance Directives Courtesy of Somerset Hospital s Ethics Committee
 TheValues History: A Worksheet for Advance Directives Courtesy of Somerset Hospital s Ethics Committee Advance Directives Living Wills Power of Attorney The Values History: A Worksheet for Advanced Directives
TheValues History: A Worksheet for Advance Directives Courtesy of Somerset Hospital s Ethics Committee Advance Directives Living Wills Power of Attorney The Values History: A Worksheet for Advanced Directives
1. CRITICAL CARE. Preamble. Adult and Pediatric Critical Care
 1. CRITICAL CARE Complete understanding of the following paragraphs is essential to appropriate billing of the critical care fees. Members of the team billing the Critical Care Payment Schedule can not
1. CRITICAL CARE Complete understanding of the following paragraphs is essential to appropriate billing of the critical care fees. Members of the team billing the Critical Care Payment Schedule can not
Critical Care Curriculum for Two-Month Rotation as Part of an Anesthesiology Residency
 DEPARTMENT OF ANESTHESIA Critical Care Curriculum for Two-Month Rotation as Part of an Anesthesiology Residency 1. An anesthesiology resident, during a two month rotation should gain exposure to the scope
DEPARTMENT OF ANESTHESIA Critical Care Curriculum for Two-Month Rotation as Part of an Anesthesiology Residency 1. An anesthesiology resident, during a two month rotation should gain exposure to the scope
Pandemic Planning for Critical Care. Stephen Lapinsky Mount Sinai Hospital Toronto
 Pandemic Planning for Critical Care Stephen Lapinsky Mount Sinai Hospital Toronto Outline Pandemic planning Why plan? What do we expect? Increasing ICU capacity Protecting ICU staff ICU management Ethical
Pandemic Planning for Critical Care Stephen Lapinsky Mount Sinai Hospital Toronto Outline Pandemic planning Why plan? What do we expect? Increasing ICU capacity Protecting ICU staff ICU management Ethical
Quality Improvement in the ICU: A Way Forward
 Quality Improvement in the ICU: A Way Forward Ognjen Gajic M.D. Mayo Clinic Rochester MN, USA Multidisciplinary Epidemiology and Translational Research in Intensive Care, Emergency and Perioperative Medicine
Quality Improvement in the ICU: A Way Forward Ognjen Gajic M.D. Mayo Clinic Rochester MN, USA Multidisciplinary Epidemiology and Translational Research in Intensive Care, Emergency and Perioperative Medicine
Course: Acute Trauma Care Course Number SUR 1905 (1615)
") Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
Barriers to Early Rehabilitation in Critically Ill Patients. Shannon Goddard, MD Sunnybrook Health Sciences Centre
 Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
2014 ANCC National Magnet Conference. Safeguarding Valuable Resources through Partnership, Technology, and Education
 2014 ANCC National Magnet Conference Safeguarding Valuable Resources through Partnership, Technology, and Education Session # C707, 8:00AM 9:00AM Friday, October 10, 2014 Michelle L. Kopp, RN, MSN, AOCNS,
2014 ANCC National Magnet Conference Safeguarding Valuable Resources through Partnership, Technology, and Education Session # C707, 8:00AM 9:00AM Friday, October 10, 2014 Michelle L. Kopp, RN, MSN, AOCNS,
COBAFOLIO: DOCUMENTING THE EVIDENCE OF COMPETENCE
 COBAFOLIO: DOCUMENTING THE EVIDENCE OF COMPETENCE (2006) The CoBaTrICE Collaboration: 1 st September 2006. European Society of Intensive Care Medicine (ESICM) Avenue Joseph Wybran 40, B-1070,Brussels.
COBAFOLIO: DOCUMENTING THE EVIDENCE OF COMPETENCE (2006) The CoBaTrICE Collaboration: 1 st September 2006. European Society of Intensive Care Medicine (ESICM) Avenue Joseph Wybran 40, B-1070,Brussels.
Louise Rose RN, BN, ICU Cert, Adult Ed Cert, MN, PhD
 Louise Rose RN, BN, ICU Cert, Adult Ed Cert, MN, PhD TD Nursing Professor in Critical Care Research, Sunnybrook Health Sciences Centre Associate Professor, LSBFON, University of Toronto CIHR New Investigator
Louise Rose RN, BN, ICU Cert, Adult Ed Cert, MN, PhD TD Nursing Professor in Critical Care Research, Sunnybrook Health Sciences Centre Associate Professor, LSBFON, University of Toronto CIHR New Investigator
Communication with Surrogate Decision Makers. Shannon S. Carson, MD Associate Professor University of North Carolina
 Communication with Surrogate Decision Makers Shannon S. Carson, MD Associate Professor University of North Carolina Role of Communication with Families in the ICU Sharing information about illness and
Communication with Surrogate Decision Makers Shannon S. Carson, MD Associate Professor University of North Carolina Role of Communication with Families in the ICU Sharing information about illness and
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department
 Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
In a common ICU situation like this, there are two main questions we have to answer daily:
 MICU ROUNDING PLAN // 12.3.2014 This document contains 4 sections: 1. Rationale 2. Assumptions and ground rules 3. Detailed plan for rounding structure 4. 1-page outline of rounding structure 1. Rationale
MICU ROUNDING PLAN // 12.3.2014 This document contains 4 sections: 1. Rationale 2. Assumptions and ground rules 3. Detailed plan for rounding structure 4. 1-page outline of rounding structure 1. Rationale
SICU Curriculum for CA2 West Virginia University Department of Anesthesiology
 SICU Curriculum for CA2 West Virginia University Department of Anesthesiology Description of Rotation or Educational Experience One month rotation in SICU as CA1 and another month in SICU as a CA2. During
SICU Curriculum for CA2 West Virginia University Department of Anesthesiology Description of Rotation or Educational Experience One month rotation in SICU as CA1 and another month in SICU as a CA2. During
The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Jefferson Health
 The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Jefferson Health 2. Title Of Initiative Implementation of a Patient Blood Management
The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Jefferson Health 2. Title Of Initiative Implementation of a Patient Blood Management
ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY)
") July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
End of Life Care in the ICU
 End of Life Care in the ICU C.M. Stafford, MD, FCCP Medical Director, Intensive Care Unit Chairman, Healthcare Ethics Committee Naval Medical Center San Diego The views expressed in this presentation are
End of Life Care in the ICU C.M. Stafford, MD, FCCP Medical Director, Intensive Care Unit Chairman, Healthcare Ethics Committee Naval Medical Center San Diego The views expressed in this presentation are
Pediatric ICU Rotation
 Pediatric Anesthesia Fellowship Program Department of Anesthesiology 800 Washington Street, Box 298 Boston, MA 02111 Tel: 617 636 6044 Fax: 617 636 8384 Pediatric ICU Rotation ROTATION DIRECTOR: RASHED
Pediatric Anesthesia Fellowship Program Department of Anesthesiology 800 Washington Street, Box 298 Boston, MA 02111 Tel: 617 636 6044 Fax: 617 636 8384 Pediatric ICU Rotation ROTATION DIRECTOR: RASHED
@ncepod #tracheostomy
 @ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
@ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
Barriers to Early Mobilization in Critically Ill Patients
 Barriers to Early Mobilization in Critically Ill Patients Shannon Goddard, MD Department of Critical Care Medicine, Sunnybrook Health Sciences Centre PhD Student, Institute of Health Policy, Management
Barriers to Early Mobilization in Critically Ill Patients Shannon Goddard, MD Department of Critical Care Medicine, Sunnybrook Health Sciences Centre PhD Student, Institute of Health Policy, Management
ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221. I. Title Trauma team Activation Protocol/Roles & Responsibilities of the Trauma Team
 Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221 Subject: Trauma Team Activation Protocol/Roles & Responsibilities of the Trauma Team Trauma Coordinator UTMB respects the diverse culture
Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221 Subject: Trauma Team Activation Protocol/Roles & Responsibilities of the Trauma Team Trauma Coordinator UTMB respects the diverse culture
Implementation of Clinical Practice Guidelines for Nutrition in the Critical Care Setting:
 Implementation of Clinical Practice Guidelines for Nutrition in the Critical Care Setting: Time to narrow the gap! Daren K. Heyland Professor of Medicine Queen s University, Kingston General Hospital Kingston,
Implementation of Clinical Practice Guidelines for Nutrition in the Critical Care Setting: Time to narrow the gap! Daren K. Heyland Professor of Medicine Queen s University, Kingston General Hospital Kingston,
Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014
 Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014 Ryan Arnold, MD Department of Emergency Medicine and Value Institute Christiana Care Health System, Newark, DE Susan Niemeier, RN Chief Nursing
Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014 Ryan Arnold, MD Department of Emergency Medicine and Value Institute Christiana Care Health System, Newark, DE Susan Niemeier, RN Chief Nursing
Penn State Milton S. Hershey Medical Center. Division of Trauma, Acute Care & Critical Care Surgery
 Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
UNMH Anesthesiology Clinical Privileges
 For eligibility to request privileges in Anesthesiology, applicants must have appointment as a Faculty member of the UNM Department of Anesthesiology & Critical Care Medicine. All new applicants must meet
For eligibility to request privileges in Anesthesiology, applicants must have appointment as a Faculty member of the UNM Department of Anesthesiology & Critical Care Medicine. All new applicants must meet
Administration of blood components. Denise Watson Patient Blood Management Practitioner 11th January, 2016
 Administration of blood components Denise Watson Patient Blood Management Practitioner 11th January, 2016 Introduction British Committee for Standards in Haematology guidelines Administration process Case
Administration of blood components Denise Watson Patient Blood Management Practitioner 11th January, 2016 Introduction British Committee for Standards in Haematology guidelines Administration process Case
HONG KONG SANATORIUM AND HOSPITAL INTENSIVE CARE UNIT (ICU) GUIDELINES ON ADMISSIONS AND DISCHARGES
 GUIDELINES ON ADMISSIONS AND DISCHARGES") HONG KONG SANATORIUM AND HOSPITAL INTENSIVE CARE UNIT (ICU) GUIDELINES ON ADMISSIONS AND DISCHARGES I. Principle The intensive care unit is operated on the principles of high turnover; ready accessibility
HONG KONG SANATORIUM AND HOSPITAL INTENSIVE CARE UNIT (ICU) GUIDELINES ON ADMISSIONS AND DISCHARGES I. Principle The intensive care unit is operated on the principles of high turnover; ready accessibility
Presenters. Tiffany Osborn, MD, MPH. Laura Evans, MD MSc. Arjun Venkatesh, MD, MBA, MHS
 Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
Trauma Rotation UMASS Memorial University Campus
 Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring
 Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Clinical and Financial Successes at Advocate Health Care Utilizing our
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
CARDIOVASCULAR SURGERY PHYSICIAN ASSISTANT CLINICAL PRIVILEGES
 Notice to Applicant: Applicants have the burden of producing information deemed adequate by University of Mississippi Medical Center (UMMC) for a proper evaluation of current competence, current clinical
Notice to Applicant: Applicants have the burden of producing information deemed adequate by University of Mississippi Medical Center (UMMC) for a proper evaluation of current competence, current clinical
MEDICAL DIRECTIVE Critical Care Outreach Team (CCOT) Abdominal Pain
 Abdominal Pain") Authorizing physician(s) Intensivists who are part of the Critical Care Physician Section Authorized to who CCOT Responders (RRTs and RNs) that have the knowledge, skill and judgment and who have successfully
Authorizing physician(s) Intensivists who are part of the Critical Care Physician Section Authorized to who CCOT Responders (RRTs and RNs) that have the knowledge, skill and judgment and who have successfully
Observation Unit. Romil Chadha
 Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
The curriculum is based on achievement of the clinical competencies outlined below:
 ANESTHESIOLOGY CRITICAL CARE MEDICINE FELLOWSHIP Program Goals and Objectives The curriculum is based on achievement of the clinical competencies outlined below: Patient Care Fellows will provide clinical
ANESTHESIOLOGY CRITICAL CARE MEDICINE FELLOWSHIP Program Goals and Objectives The curriculum is based on achievement of the clinical competencies outlined below: Patient Care Fellows will provide clinical
Mobile Communications
 Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
CHHP Management, LLC dba Community Hospital of Huntington Park
 Training Proposal for: CHHP Management, LLC dba Community Hospital of Huntington Park Agreement Number: ET13-0394 Panel Meeting of: May 23, 2013 ETP Regional Office: North Hollywood Analyst: J. Romero
Training Proposal for: CHHP Management, LLC dba Community Hospital of Huntington Park Agreement Number: ET13-0394 Panel Meeting of: May 23, 2013 ETP Regional Office: North Hollywood Analyst: J. Romero
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program April 30, 2016 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate Health
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program April 30, 2016 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate Health
Ethics and Health Care: End of Life and Critical Care Decisions: Legal and Ethical Considerations. Helga D. Van Iderstine
 Ethics and Health Care: End of Life and Critical Care Decisions: Legal and Ethical Considerations Helga D. Van Iderstine Legal Framework Breach of Fiduciary Duty Battery Negligence Breach of standard of
Ethics and Health Care: End of Life and Critical Care Decisions: Legal and Ethical Considerations Helga D. Van Iderstine Legal Framework Breach of Fiduciary Duty Battery Negligence Breach of standard of
A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals
 A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals Joshua Dunn, Pharm.D. Anne Teichman, Pharm.D. School of Pharmacy University of Charleston Charleston WV Corresponding author:
A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals Joshua Dunn, Pharm.D. Anne Teichman, Pharm.D. School of Pharmacy University of Charleston Charleston WV Corresponding author:
"Working Smartly: Better Communication and Reduced Error through Improved Clinical Informatics"
 "Working Smartly: Better Communication and Reduced Error through Improved Clinical Informatics" Healthcare Transformation Services Lisa Pahl, MSN, Principal, Practice Lead Alarm Management May, 2017 Data,
"Working Smartly: Better Communication and Reduced Error through Improved Clinical Informatics" Healthcare Transformation Services Lisa Pahl, MSN, Principal, Practice Lead Alarm Management May, 2017 Data,
Improving communication of the daily care plan in a teaching hospital intensive care unit
 Improving communication of the daily care plan in a teaching hospital intensive care unit Dharshi Karalapillai, Ian Baldwin, Gillian Dunnachie, Cameron Knott, Glenn Eastwood, John Rogan, Erin Carnell and
Improving communication of the daily care plan in a teaching hospital intensive care unit Dharshi Karalapillai, Ian Baldwin, Gillian Dunnachie, Cameron Knott, Glenn Eastwood, John Rogan, Erin Carnell and
MEMORANDUM FOR MTN PALS PROGRAM DIRECTORS/ADMINISTRATORS. SUBJECT: Hostile Environments Life-Saving Pediatrics (HELP)
") UNIFORMED SERVICES UNIVERSITY OF THE HEALTH SCIENCES 4301 JONES BRIDGE ROAD BETHESDA, MARYLAND 20814-4799 www.usuhs.mil MEMORANDUM FOR MTN PALS PROGRAM DIRECTORS/ADMINISTRATORS SUBJECT: Hostile Environments
UNIFORMED SERVICES UNIVERSITY OF THE HEALTH SCIENCES 4301 JONES BRIDGE ROAD BETHESDA, MARYLAND 20814-4799 www.usuhs.mil MEMORANDUM FOR MTN PALS PROGRAM DIRECTORS/ADMINISTRATORS SUBJECT: Hostile Environments
NMHS National Foundation Module Critical Care Nursing. Module overview. Module leader: Katie Wedgeworth
 Module overview Module leader: Katie Wedgeworth Katie.wedgeworth@ucd.ie 017166447 Module web link Module Objectives and Learning Outcomes The objective of this module is that students will be able to safely
Module overview Module leader: Katie Wedgeworth Katie.wedgeworth@ucd.ie 017166447 Module web link Module Objectives and Learning Outcomes The objective of this module is that students will be able to safely
Team collabora+on: an impera+ve for early mobiliza+on Dr Louise Rose BN, ICU Cert, MN, PhD, FAAN TD Nursing Professor in Cri+cal Care Research
 Team collabora+on: an impera+ve for early mobiliza+on Dr Louise Rose BN, ICU Cert, MN, PhD, FAAN TD Nursing Professor in Cri+cal Care Research Sunnybrook Health Sciences Centre; Associate Professor, University
Team collabora+on: an impera+ve for early mobiliza+on Dr Louise Rose BN, ICU Cert, MN, PhD, FAAN TD Nursing Professor in Cri+cal Care Research Sunnybrook Health Sciences Centre; Associate Professor, University
ADVANCE DIRECTIVE FOR HEALTH CARE
 ADVANCE DIRECTIVE FOR HEALTH CARE This document includes a list of definitions and the two types of Advance Directives (together called a Combined Directive). Some people choose to fill out only one portion.
ADVANCE DIRECTIVE FOR HEALTH CARE This document includes a list of definitions and the two types of Advance Directives (together called a Combined Directive). Some people choose to fill out only one portion.
PATIENT RIGHTS, PRIVACY, AND PROTECTION
 REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
Department of Critical Care Restricted Registration Proposal for Call Coverage by Residents in TOH Intensive Care Units
 Department of Critical Care Restricted Registration Proposal for Call Coverage by Residents in TOH Intensive Care Units Background: In 2004, the CPSO adopted a model for a pilot project to institute limited
Department of Critical Care Restricted Registration Proposal for Call Coverage by Residents in TOH Intensive Care Units Background: In 2004, the CPSO adopted a model for a pilot project to institute limited
TRAUMA CENTER REQUIREMENTS
 California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
the victorian paediatric emergency transport service pets
 the victorian paediatric emergency transport service pets The Victorian Paediatric Emergency Transport Service The Victorian Paediatric Emergency Transport Service (PETS) is based at the Paediatric Intensive
the victorian paediatric emergency transport service pets The Victorian Paediatric Emergency Transport Service The Victorian Paediatric Emergency Transport Service (PETS) is based at the Paediatric Intensive
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016
 Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Disclosure. I have no conflict of interest with this event because I have no affiliations, sponsorships, honoraria, monetary support or conflict of
 The RBC Audit: What s in your closet? Yulia Lin, MD, FRCPC Transfusion Medicine & Hematology, Sunnybrook HSC Assistant Professor, Dept of LMP, University of Toronto On behalf of the RBC Audit Working Group
The RBC Audit: What s in your closet? Yulia Lin, MD, FRCPC Transfusion Medicine & Hematology, Sunnybrook HSC Assistant Professor, Dept of LMP, University of Toronto On behalf of the RBC Audit Working Group
Saving Lives with Best Practices and Improvements in Sepsis Care
 Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
ABOUT THE CONE HEALTH NETWORK OF SERVICES
 THE MOSES H. CONE MEMORIAL HOSPITAL (536 beds) Critical Care Services All system ICU patients are monitored with the help an electronic ICU monitoring system (VISICU ). Emergency Services Medical Intensive
THE MOSES H. CONE MEMORIAL HOSPITAL (536 beds) Critical Care Services All system ICU patients are monitored with the help an electronic ICU monitoring system (VISICU ). Emergency Services Medical Intensive
Lost in translation: challenges in handing over critical care
 Lost in translation: challenges in handing over critical care Andre Amaral, MD Assistant Professor Interdepartmental Division of Critical Care Medicine University of Toronto Sunnybrook Health Sciences
Lost in translation: challenges in handing over critical care Andre Amaral, MD Assistant Professor Interdepartmental Division of Critical Care Medicine University of Toronto Sunnybrook Health Sciences
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
TeleICU And What It Means To You
 Vanderbilt Department of Anesthesiology TeleICU And What It Means To You Dr. L. Weavind MBBCh Associate Professor Anesthesia and Surgery Director Critical Care Fellowship Vanderbilt University Former Director
Vanderbilt Department of Anesthesiology TeleICU And What It Means To You Dr. L. Weavind MBBCh Associate Professor Anesthesia and Surgery Director Critical Care Fellowship Vanderbilt University Former Director
DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Rhode Island Version) You must be at least eighteen (18) years of age.
 You must be at least eighteen (18) years of age.") MASSASOIT INTERNAL MEDICINE (401) 434-2704 massasoitmed.com DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Rhode Island Version) THE DURABLE POWER OF ATTORNEY FOR HEALTH CARE DOCUMENT lets you appoint someone
MASSASOIT INTERNAL MEDICINE (401) 434-2704 massasoitmed.com DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Rhode Island Version) THE DURABLE POWER OF ATTORNEY FOR HEALTH CARE DOCUMENT lets you appoint someone
Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways
 For Patients not eligible for other TICKER Clinical Pathways") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Part II. The CCT in. Intensive Care Medicine. Assessment System. The Faculty of. Intensive Care Medicine
 Part II The CCT in Intensive Care Medicine Assessment System The Faculty of Intensive Care Medicine Contents 1. Principles of Assessment... 3 1.1 Training Stage Records... 3 1.2 How many workplace-based
Part II The CCT in Intensive Care Medicine Assessment System The Faculty of Intensive Care Medicine Contents 1. Principles of Assessment... 3 1.1 Training Stage Records... 3 1.2 How many workplace-based
Co C as a t s Pro r v o i v nce nc G eneral Hospi s tal Le L v e e v l 5 R 5 e R fe f rr r al a F ac a i c lity *** 9/2/2015 1
 Coast Province General Hospital Level 5 Referral Facility *** 9/2/2015 1 Background Coast Province General Hospital was founded in 1908 as the Native Civil Hospital in the Makadara area of Mombasa Island.
Coast Province General Hospital Level 5 Referral Facility *** 9/2/2015 1 Background Coast Province General Hospital was founded in 1908 as the Native Civil Hospital in the Makadara area of Mombasa Island.
HOW TO DO POST-HOC RESPONSE REVIEWS
 HOW TO DO POST-HOC RESPONSE REVIEWS Ken Hillman 6 th International Symposium on Rapid Response Systems and Medical Emergency Teams Pittsburgh, USA, 11 th -12 th May 2010 ACUTE HOSPITAL SYSTEM AUDIT OF
HOW TO DO POST-HOC RESPONSE REVIEWS Ken Hillman 6 th International Symposium on Rapid Response Systems and Medical Emergency Teams Pittsburgh, USA, 11 th -12 th May 2010 ACUTE HOSPITAL SYSTEM AUDIT OF
Trauma Center Pre-Review Questionnaire Notes Title 22
 This Pre-Review Questionnaire is designed to accompany the spread sheet appropriate for the Trauma Center being reviewed For use with review of Level III Trauma Center with American College of Surgeons'
This Pre-Review Questionnaire is designed to accompany the spread sheet appropriate for the Trauma Center being reviewed For use with review of Level III Trauma Center with American College of Surgeons'
Policies and Procedures. ID Number: 1138
 Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
ICU Nurses Perceptions of Nutrition Education and Training. October 17, 2011 Gwynne MacDonald, Cathy Alberda and Leah Gramlich
 ICU Nurses Perceptions of Nutrition Education and Training October 17, 2011 Gwynne MacDonald, Cathy Alberda and Leah Gramlich Why bother feeding? Increased energy and protein associated with lower mortality
ICU Nurses Perceptions of Nutrition Education and Training October 17, 2011 Gwynne MacDonald, Cathy Alberda and Leah Gramlich Why bother feeding? Increased energy and protein associated with lower mortality
UNM SRMC CRITICAL CARE PRIVILEGES
 UNM SRMC INSTRUCTIONS All new applicants must meet the following requirements as approved by the UNM SRMC Board of Directors effective May 24, 2017 Applicant: Check off the "Requested" box for each privilege
UNM SRMC INSTRUCTIONS All new applicants must meet the following requirements as approved by the UNM SRMC Board of Directors effective May 24, 2017 Applicant: Check off the "Requested" box for each privilege
Responding to Patients and Families that Want Everything Done
 Responding to Patients and Families that Want Everything Done Steven Pantilat, MD Professor of Clinical Medicine Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care Director, Palliative
Responding to Patients and Families that Want Everything Done Steven Pantilat, MD Professor of Clinical Medicine Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care Director, Palliative
A New, National Approach to Surveillance for Ventilator-associated Events; Challenges and Opportunities
 A New, National Approach to Surveillance for Ventilator-associated Events; Challenges and Opportunities Linda R.Greene,RN,MPS,CIC Manager of Infection Prevention Highland Hospital Rochester, NY Affiliate
A New, National Approach to Surveillance for Ventilator-associated Events; Challenges and Opportunities Linda R.Greene,RN,MPS,CIC Manager of Infection Prevention Highland Hospital Rochester, NY Affiliate
Beth Israel Deaconess Medical Center Perioperative Services Manual. Guidelines for Perioperative Handoffs from OR to receiving units.
 Beth Israel Deaconess Medical Center Perioperative Services Manual Title: Guidelines for Perioperative Handoffs from OR to receiving units. Policy #: PSM 100-102A Purpose: This guideline provides a standard
Beth Israel Deaconess Medical Center Perioperative Services Manual Title: Guidelines for Perioperative Handoffs from OR to receiving units. Policy #: PSM 100-102A Purpose: This guideline provides a standard
SUPERVISION POLICY. Roles, Responsibilities and Patient Care Activities of Subspecialty Residents (Fellows)
") Roles, Responsibilities and Patient Care Activities of Subspecialty Residents (Fellows) Definitions Pediatric Critical Care Medicine Fellowship Program Seattle Children s Hospital and Harborview Medical
Roles, Responsibilities and Patient Care Activities of Subspecialty Residents (Fellows) Definitions Pediatric Critical Care Medicine Fellowship Program Seattle Children s Hospital and Harborview Medical
UNIVERSITY OF COLORADO HEALTH SCIENCES CENTER PULMONARY ELECTIVE HOUSESTAFF ROTATION CURRICULUM AND OBJECTIVES
 January 2007 UNIVERSITY OF COLORADO HEALTH SCIENCES CENTER PULMONARY ELECTIVE HOUSESTAFF ROTATION CURRICULUM AND OBJECTIVES This paragraph only applies if you are rotating at the University of Colorado
January 2007 UNIVERSITY OF COLORADO HEALTH SCIENCES CENTER PULMONARY ELECTIVE HOUSESTAFF ROTATION CURRICULUM AND OBJECTIVES This paragraph only applies if you are rotating at the University of Colorado
Minor/technical revision of existing policy X Major revision of existing policy Reaffirmation of existing policy
 Name of Policy: Policy Number: 3364-100-45-06 Department: Approving Officer: Responsible Agent: Scope: Heart and Vascular Center, Hospital Clinics, the George Isaac Outpatient Surgical Center, the First
Name of Policy: Policy Number: 3364-100-45-06 Department: Approving Officer: Responsible Agent: Scope: Heart and Vascular Center, Hospital Clinics, the George Isaac Outpatient Surgical Center, the First
Pediatric Fundamental Critical Care Support (PFCCS)
") Provided By: Pediatric Fundamental Critical Care Support (PFCCS) Center for Advanced Medical Learning and Simulation (CAMLS) 124 S. Franklin, Tampa, Florida 33602 Need and Course Description: Early identification
Provided By: Pediatric Fundamental Critical Care Support (PFCCS) Center for Advanced Medical Learning and Simulation (CAMLS) 124 S. Franklin, Tampa, Florida 33602 Need and Course Description: Early identification
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers
 Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers Melissa A. Fitzpatrick, RN, MSN, FAAN VP & Chief Clinical Officer, Hill-Rom Trends Driving Our Industry Aging
Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers Melissa A. Fitzpatrick, RN, MSN, FAAN VP & Chief Clinical Officer, Hill-Rom Trends Driving Our Industry Aging
Fundamental Critical Care Support (FCCS)
") Provided By: Fundamental Critical Care Support (FCCS) Center for Advanced Medical Learning and Simulation (CAMLS) 124 S. Franklin, Tampa, Florida 33602 Needs Statement and Educational Gap: Early identification
Provided By: Fundamental Critical Care Support (FCCS) Center for Advanced Medical Learning and Simulation (CAMLS) 124 S. Franklin, Tampa, Florida 33602 Needs Statement and Educational Gap: Early identification
Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation
 Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation Potential and Mobility Plan Amy Dean, MS, RN, CCRN Kristin
Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation Potential and Mobility Plan Amy Dean, MS, RN, CCRN Kristin
CA-1 CRITICAL CARE ROTATION University of Minnesota Medical Center Fairview (UMMC) Rotation Site Director: Dr. Martin Birch Rotation Duration: 4 weeks
 Rotation Site Director: Dr. Martin Birch Rotation Duration: 4 weeks") CA-1 CRITICAL CARE ROTATION Medical Center Fairview (UMMC) Rotation Site Director: Dr. Martin Birch Rotation Duration: 4 weeks Introduction: Critical Care is an integral aspect of anesthesiology training.
CA-1 CRITICAL CARE ROTATION Medical Center Fairview (UMMC) Rotation Site Director: Dr. Martin Birch Rotation Duration: 4 weeks Introduction: Critical Care is an integral aspect of anesthesiology training.
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management
 SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
The Davies Award Is: The HIMSS Nicholas E. Davies Award of Excellence. Awarding IT. Improving Healthcare.
 The Davies Award Is: Since 1994, the Nicholas E. Davies Award of Excellence is HIMSS highest global recognition of hospitals, ambulatory practices and clinics, community health organizations, and public
The Davies Award Is: Since 1994, the Nicholas E. Davies Award of Excellence is HIMSS highest global recognition of hospitals, ambulatory practices and clinics, community health organizations, and public
RCT CONSORT CONSORT Introduction CONSORT Method RCT
 RCT 2018/01/09 ICU RCT CONSORT CONSORT Introduction CONSORT Method RCT RCT CONSORT CONSORT Introduction CONSORT Method RCT / Intervention Outcome Intervention, Outcome I O Patients Intervention Patient
RCT 2018/01/09 ICU RCT CONSORT CONSORT Introduction CONSORT Method RCT RCT CONSORT CONSORT Introduction CONSORT Method RCT / Intervention Outcome Intervention, Outcome I O Patients Intervention Patient
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
ADVANCED HEALTH CARE DIRECTIVE OF LAWRENCE HALL JR.
 ADVANCED HEALTH CARE DIRECTIVE OF LAWRENCE HALL JR. Identification. I, Lawrence Hall Jr., being a competent adult of sound mind, having the capacity to make health care decisions, willfully and voluntarily
ADVANCED HEALTH CARE DIRECTIVE OF LAWRENCE HALL JR. Identification. I, Lawrence Hall Jr., being a competent adult of sound mind, having the capacity to make health care decisions, willfully and voluntarily
Policy for Admission to Adult Critical Care Services
 Policy Number: CCaNNI 008 Title: Policy for Admission to Adult Critical Care Services Operational Date: Review Date: December 2009 December 2012 Type of Document: EQIA Screening Date: Corporate x Clinical
Policy Number: CCaNNI 008 Title: Policy for Admission to Adult Critical Care Services Operational Date: Review Date: December 2009 December 2012 Type of Document: EQIA Screening Date: Corporate x Clinical
REMOVING WASTE FROM HEALTH CARE: LESSONS FROM CHOOSING WISELY AND THE RIGHT CARE ALLIANCE
 REMOVING WASTE FROM HEALTH CARE: LESSONS FROM CHOOSING WISELY AND THE RIGHT CARE ALLIANCE D e c e m b e r 9, 2 0 1 3 I n s t i t u t e f o r H e a l t hc a r e I m p r o v e m e nt O r l a n d o, F L S
REMOVING WASTE FROM HEALTH CARE: LESSONS FROM CHOOSING WISELY AND THE RIGHT CARE ALLIANCE D e c e m b e r 9, 2 0 1 3 I n s t i t u t e f o r H e a l t hc a r e I m p r o v e m e nt O r l a n d o, F L S
The Heart and Stroke Foundation of Canada and the Canadian Institutes of Health Research s Institute of Circulatory and Respiratory Health (ICRH)
") The Heart and Stroke Foundation of Canada and the Canadian Institutes of Health Research s Institute of Circulatory and Respiratory Health (ICRH) Objectives Request for Applications (RFA) for Team Grants
The Heart and Stroke Foundation of Canada and the Canadian Institutes of Health Research s Institute of Circulatory and Respiratory Health (ICRH) Objectives Request for Applications (RFA) for Team Grants
The deteriorating patient recognition and management Dave Story
 The deteriorating patient recognition and management Dave Story MBBS, MD, BMedSci, FANZCA Professor and Foundation Chair of Anaesthesia Head of Anaesthesia, Perioperative and Pain Medicine Unit (APPMU)
The deteriorating patient recognition and management Dave Story MBBS, MD, BMedSci, FANZCA Professor and Foundation Chair of Anaesthesia Head of Anaesthesia, Perioperative and Pain Medicine Unit (APPMU)
Position Paper on Anesthesia Assistants: An Official Position Paper of the Canadian Anesthesiologists Society
 Can J Anesth/J Can Anesth (2018) Appendix 5 Position Paper on Anesthesia Assistants: An Official Position Paper of the Canadian Anesthesiologists Society Background Medical and surgical care has become
Can J Anesth/J Can Anesth (2018) Appendix 5 Position Paper on Anesthesia Assistants: An Official Position Paper of the Canadian Anesthesiologists Society Background Medical and surgical care has become
Anesthesia Elective Curriculum Outline
 Department of Internal Medicine Texas Tech University Health Sciences Center Odessa, Texas Anesthesia Elective Curriculum Outline Revision Date: July 10, 2006 Approved by Curriculum Meeting September 19,
Department of Internal Medicine Texas Tech University Health Sciences Center Odessa, Texas Anesthesia Elective Curriculum Outline Revision Date: July 10, 2006 Approved by Curriculum Meeting September 19,
Improving Outcomes for High Risk and Critically Ill Patients
 Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The