Lost in translation: challenges in handing over critical care
|
|
|
- Brett Holmes
- 6 years ago
- Views:
Transcription


1 Lost in translation: challenges in handing over critical care Andre Amaral, MD Assistant Professor Interdepartmental Division of Critical Care Medicine University of Toronto Sunnybrook Health Sciences Centre
2 Objectives 1. To understand the relevance of handovers for patient safety 3. To review possible threats to effective handovers 5. To think about simple things you can do to improve your


3 WHAT IS A HANDOVER? 1.Exchange of patient information: Allow for continuity of care Increased effectiveness Increased safety of actions Better clinical understanding Cohen MD and Amaral AC Crit Care 2011 (in press)


4 ARE HANDOVERS A SAFETY

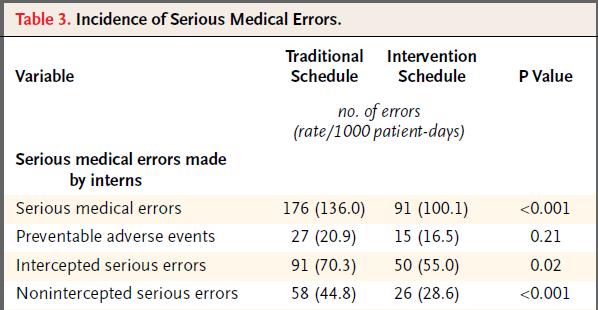
5 WE KNOW FATIGUE IS 1. Libby Zion, 18: Oct. 4, 1984 with fever, agitation and jerking movements 2. A first-year intern was charged with her care 3. Meperidine to calm her degree fever, then fatal heart attack 5. Cause of death: serotonin syndrome
6 LIBBY S FATHER BLAMED INADEQUATE HOSPITAL STAFFING Libby s father, Sidney Zion, wrote in The New York Times: You don t need kindergarten to know that a resident working a 36-hour shift is in no condition to make any kind of judgment call. Washington Post. Nov 28, 2006.
7 REFORMS FOLLOW LIBBY S DEATH 1. Blue-ribbon commission report: New York State s residency duty requirements : ACGME : revised ACGME Washington Post. Nov 28, 2006.
8
9
10 To the Editor:... However, having experienced the intervention schedule firsthand as intern subjects in the study, we have serious concerns about the authors' conclusions. Residents in the study worked traditional every-threeday on-call schedules and routinely worked extra hours to cover for the interns. Worried residents and attending physicians, aware that the interns on the intervention schedule were poorly informed, took a more active role in patient care, making the majority of decisions and more closely supervising the interns' actions. This hypervigilance may have strongly biased the study toward a positive result
11
12 Traditional Interventio n Total Serious Medication Errors (Rate/1000 patientdays) Wrong Medication (Rate/1000 patient-days)
13 Traditional Interventio n Total Serious Medication Errors (Rate/1000 patientdays) Wrong Medication (Rate/1000 patient-days)
14 Academic Pre-Reform Year 2 Pre-Reform Year 1 Post-Reform Year 1 Post-Reform Year 2

15 Academic Non-Teaching Pre-Reform Year 2 Pre-Reform Year 1 Post-Reform Year 1 Post-Reform Year 2
16
17 MALPRACTICE CLAIMS
18 MALPRACTICE CLAIMS 1. Failed handovers: 28% of surgical errors (Gawande AA Surgery 2003) 20% of ambulatory care errors (Gandhi TK Ann Intern Med 2006)
19 MALPRACTICE CLAIMS 1. Failed handovers: 28% of surgical errors (Gawande AA Surgery 2003) 20% of ambulatory care errors (Gandhi TK Ann Intern Med 2006) 24% E.D. errors (Kachalia A Ann Emerg Med 2007)
20 MALPRACTICE CLAIMS 1. Failed handovers: 28% of surgical errors (Gawande AA Surgery 2003) 20% of ambulatory care errors (Gandhi TK Ann Intern Med 2006) 24% E.D. errors (Kachalia A Ann Emerg Med 2007)
21 MALPRACTICE CLAIMS 1. Failed handovers: 28% of surgical errors (Gawande AA Surgery 2003) 20% of ambulatory care errors (Gandhi TK Ann Intern Med 2006) 24% E.D. errors (Kachalia A Ann Emerg Med 2007) 2. What is worse: a fumbled handover or being fatigued?
22 MALPRACTICE CLAIMS 1. Failed handovers: 28% of surgical errors (Gawande AA Surgery 2003) 20% of ambulatory care errors (Gandhi TK Ann Intern Med 2006) 24% E.D. errors (Kachalia A Ann Emerg Med 2007) 2. What is worse: a fumbled handover or being fatigued?
23 MALPRACTICE CLAIMS 1. Failed handovers: 28% of surgical errors (Gawande AA Surgery 2003) 20% of ambulatory care errors (Gandhi TK Ann Intern Med 2006) 24% E.D. errors (Kachalia A Ann Emerg Med 2007) 2. What is worse: a fumbled handover or being fatigued? 4. Handovers 6x > fatigue in claims! (Singh Arch
24 ARE HANDOVERS A SAFETY
25 ARE HANDOVERS A SAFETY 1.23% of handovers may contain: errors (incorrect information) surprises (omitted information) Philibert I Qual Saf Health Care 2009
26 ARE HANDOVERS A SAFETY 1.23% of handovers may contain: errors (incorrect information) surprises (omitted information) Philibert I Qual Saf Health Care Trainees not prepared for 80% of nighttime events
27 ARE HANDOVERS A SAFETY 1.23% of handovers may contain: errors (incorrect information) surprises (omitted information) Philibert I Qual Saf Health Care Trainees not prepared for 80% of nighttime events 75% of which could have been anticipated and discussed during handovers Borowitz SM Qual Saf Health Care 2008

28 Variable OR p Value Crosscovering Apache II 1.2 <0.001
29 OBJECTIVE 1: TO UNDERSTAND HANDOVERS IN PATIENT SAFETY 1.Handovers are frequently seen as an important factor in adverse events 3.Handovers may be more important than fatigue!
30 ELEMENTS OF A HANDOVER (1) Background clinical information (2) Course of the acute illness (3) To-dos / Tasks (4) Uncertainty (5) Anticipation of events
31 ELEMENTS OF A HANDOVER Objectiv e (1) Background clinical information (2) Course of the acute illness (3) To-dos / Tasks (4) Uncertainty (5) Anticipation of events
32 ELEMENTS OF A HANDOVER Objectiv e Subjectiv e (1) Background clinical information (2) Course of the acute illness (3) To-dos / Tasks (4) Uncertainty (5) Anticipation of events
33 THREAT 1: DEFAULT (1)Background clinical information COPD and hypertension (2) Course of the acute illness septic shock from perforated ischemic bowel, who had acute lung injury and acute kidney injury. He has been extubated for the past 24 hours and is starting to diurese spontaneously (3) To-dos He needs to have a new catheter inserted to re-start dialysis tomorrow (4) Uncertainty He was slightly hypotensive overnight. I think we might have made him hypovolemic with the ultrafiltration. He was on low dose of pressors this morning, but he is off pressors now after a fluid challenge. I am not sure whether he is becoming septic again (5) Anticipation of events
34 THREAT 1: DEFAULT (1)Background clinical information COPD and hypertension (2) Course of the acute illness septic shock from perforated ischemic bowel, who had acute lung injury and acute kidney injury. He has been extubated for the past 24 hours and is starting to diurese spontaneously (3) To-dos He needs to have a new catheter inserted to re-start dialysis tomorrow (4) Uncertainty He was slightly hypotensive overnight. I think we might have made him hypovolemic with the ultrafiltration. He was on low dose of pressors this morning, but he is off pressors now after a fluid challenge. I am not sure whether he is becoming septic again (5) Anticipation of events
35 THREAT 1: DEFAULT (1)Background clinical information COPD and hypertension (2) Course of the acute illness septic shock from perforated ischemic bowel, who had acute lung injury and acute kidney injury. He has been extubated for the past 24 hours and is starting to diurese spontaneously (3) To-dos He needs to have a new catheter inserted to re-start dialysis tomorrow (4) Uncertainty He was slightly hypotensive overnight. I think we might have made him hypovolemic with the ultrafiltration. He was on low dose of pressors this morning, but he is off pressors now after a fluid challenge. I am not sure whether he is becoming septic again (5) Anticipation of events
36 THREAT 1: DEFAULT (1)Background clinical information COPD and hypertension (2) Course of the acute illness septic shock from perforated ischemic bowel, who had acute lung injury and acute kidney injury. He has been extubated for the past 24 hours and is starting to diurese spontaneously (3) To-dos He needs to have a new catheter inserted to re-start dialysis tomorrow (4) Uncertainty He was slightly hypotensive overnight. I think we might have made him hypovolemic with the ultrafiltration. He was on low dose of pressors this morning, but he is off pressors now after a fluid challenge. I am not sure whether he is becoming septic again (5) Anticipation of events
37 THREAT 1: DEFAULT (1)Background clinical information COPD and hypertension (2) Course of the acute illness septic shock from perforated ischemic bowel, who had acute lung injury and acute kidney injury. He has been extubated for the past 24 hours and is starting to diurese spontaneously (3) To-dos He needs to have a new catheter inserted to re-start dialysis tomorrow (4) Uncertainty he was hypovolemic, I gave him a fluid bolus (5) Anticipation of events
38 THREAT 1: DEFAULT (1)Background clinical information COPD and hypertension (2) Course of the acute illness septic shock from perforated ischemic bowel, who had acute lung injury and acute kidney injury. He has been extubated for the past 24 hours and is starting to diurese spontaneously (3) To-dos He needs to have a new catheter inserted to re-start dialysis tomorrow (4) Uncertainty he was hypovolemic, I gave him a fluid bolus (5) Anticipation of events Default option

39 THE DEFAULT OPTION
40 THREAT 2: OUR MENTAL
41 THREAT 2: OUR MENTAL (1)Background clinical information COPD and hypertension (2) Course of the acute illness septic shock from perforated ischemic bowel, who had acute lung injury and acute kidney injury. He has been extubated for the past 24 hours and is starting to diurese spontaneously (3) To-dos He needs to have a new catheter inserted to re-start dialysis tomorrow (4) Uncertainty He was slightly hypotensive overnight. I think we might have made him hypovolemic with the ultrafiltration. He was on low dose of pressors this morning, but he is off pressors now after a fluid challenge. I am not sure whether he is becoming septic again (5) Anticipation of events In case he gets worse again, I d re-start antibiotics and arrange for an abdominal CT scan
42 THREAT 2: OUR MENTAL
43 THREAT 2: OUR MENTAL Next morning s handover to the team: Mr MM was OK overnight, he is just on a very low-dose of levo. 2.When CT was ordered in the next day he was found to have acalculous cholecystitis Diagnosis/Rx were delayed by approximately 18 hrs!
44 THREAT 3: HIERARCHY 1.63 yo, elective pelvic exenteration for colorectal cancer 2.Low urine output and elevated lactate in the first 24 hrs of ICU, but resolved with fluid resuscitation 3.On transfer to the floor the ICU fellow thought the AXR looked a bit different, then called Surg Resident

45 THREAT 2: MRS HIERARCHY
46 THREAT 3: HIERARCHY
47 THREAT 3: HIERARCHY 1.Surg resident: Oh, it is not worrisome 2.ICU Fellow: OK, if you say so Pt found to have a gastric volvulus and required reoperation
48 OBJECTIVE 2: TO REVIEW
49 OBJECTIVE 2: TO REVIEW 1.Handovers: information exchange
50 OBJECTIVE 2: TO REVIEW 1.Handovers: information exchange
51 OBJECTIVE 2: TO REVIEW 1.Handovers: information exchange 3.Multiple types of handovers
52 OBJECTIVE 2: TO REVIEW 1.Handovers: information exchange 3.Multiple types of handovers
53 OBJECTIVE 2: TO REVIEW 1.Handovers: information exchange 3.Multiple types of handovers 5.It is not a simple task, as it involves several subjective components
54 OBJECTIVE 2: TO REVIEW 1.Handovers: information exchange 3.Multiple types of handovers 5.It is not a simple task, as it involves several subjective components It is a clinical skill that needs to be
55 LITTLE THINGS YOU CAN 1. When there is uncertainty, we see only what we have been trained to see 3. Avoid creating diagnoses, there is no shame in saying I don t know what this patient has
56 LITTLE THINGS YOU CAN 2. Mental models are the visualization of concepts and their relationship 3. Who is receiving handover from you? 4. Do they share mental models with you? Yes more efficient and safer handover No less efficient, BUT opportunity to increase knowledge about a patient 5. Do they already know the patients? 7. If you are receiving a handover, questions are NEEDED
57 LITTLE THINGS YOU CAN 3. Hierarchy may hinder discussion of differences in mental models 5. If you see a problem, don t be afraid to voice it!
58 Objectives 1. To understand the relevance of handovers for patient safety 3. To review possible threats to effective handovers 5. To think about simple things you can do to improve your
59 THANK YOU!
60 Riesenberg, Am J Med Qual 2009 SBAR

61 Riesenberg, Am J Med Qual 2009 SBAR

62 SBAR

63 No Standardized Handover Standardized Handover Recall of Clinical Information 56.6% 49.2%
Improving Sign-Outs in Hospital Medicine
 Improving Sign-Outs in Hospital Medicine Arpana R. Vidyarthi, MD Assistant Professor of Medicine Division of Hospital Medicine Director of Quality, Division of Hospital Medicine Director, Patient Safety
Improving Sign-Outs in Hospital Medicine Arpana R. Vidyarthi, MD Assistant Professor of Medicine Division of Hospital Medicine Director of Quality, Division of Hospital Medicine Director, Patient Safety
10/23/2015. Don t drop the baton: Improving handover communication from the CMPA s perspective
 Don t drop the baton: Improving handover communication from the CMPA s perspective This is an abridged version of presentation with cases and videos removed Dr Janet Nuth, Physician Risk Manager CMPA Associate
Don t drop the baton: Improving handover communication from the CMPA s perspective This is an abridged version of presentation with cases and videos removed Dr Janet Nuth, Physician Risk Manager CMPA Associate
When and How to Introduce Palliative Care
 When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
TRANSITIONS OF CARE: HOSPITAL HANDOFFS. Intern Orientation
 TRANSITIONS OF CARE: HOSPITAL HANDOFFS Intern Orientation Avoiding the Overnight Handover Fumble Objectives After today, you will be able to: Understand the importance of communication around care transitions
TRANSITIONS OF CARE: HOSPITAL HANDOFFS Intern Orientation Avoiding the Overnight Handover Fumble Objectives After today, you will be able to: Understand the importance of communication around care transitions
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
Goals today 6/14/2011. Disclosures, 2004-May Sepsis A Medical Emergency. Jim O Brien, MD, MSc So what is sepsis anyway?
 Jim O Brien, MD, MSc James.OBrien@osumc.edu Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Jim O Brien, MD, MSc James.OBrien@osumc.edu Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Emergency. Best Critical Care Practices
 Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Jim O Brien, MD, MSc James.OBrien@osumc.edu Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Jim O Brien, MD, MSc James.OBrien@osumc.edu Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Diagnostics for Patient Safety and Quality of Care
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD Vice President Institute for Healthcare Improvement Cindy Hupke, BSN, MBA Director Institute for Healthcare Improvement Objectives
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD Vice President Institute for Healthcare Improvement Cindy Hupke, BSN, MBA Director Institute for Healthcare Improvement Objectives
Greetings from Michelle & Katie QUALITY IMPROVEMENT DIVISION OF HOSPITAL MEDICINE
 IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
Case 1 Standard of Care. Disclosures. Defending Critical Care: Navigating Through the Malpractice Maze 5/9/2015. Defending Critical Care:
 Defending Critical Care: Navigating Through the Malpractice Maze Defending Critical Care: Navigating Through the Malpractice Maze Joseph Picchi, JD Richard Schoenberger, JD Critical Care Medicine Update
Defending Critical Care: Navigating Through the Malpractice Maze Defending Critical Care: Navigating Through the Malpractice Maze Joseph Picchi, JD Richard Schoenberger, JD Critical Care Medicine Update
at OU Medicine Leadership Development Institute August 6, 2010
 Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Coroner's Corner - Inquest into the death of Gwendoline Mead
 Coroner's Corner - Inquest into the death of Gwendoline Mead Date of Findings: 22 June 2017 Coroner: Ainslie Kirkegaard Inquest Place: Brisbane Date of Death: 1 March 2015 Factual Summary: Gwendoline Mead
Coroner's Corner - Inquest into the death of Gwendoline Mead Date of Findings: 22 June 2017 Coroner: Ainslie Kirkegaard Inquest Place: Brisbane Date of Death: 1 March 2015 Factual Summary: Gwendoline Mead
Think proactively = prevent codes Elective intubation better than PEA arrest
 Kyla Terhune, MD Treat all the same Think proactively = prevent codes Elective intubation better than PEA arrest Floor patient going to ICU? Treat if you are waiting! Rapid Response if Needed Does this
Kyla Terhune, MD Treat all the same Think proactively = prevent codes Elective intubation better than PEA arrest Floor patient going to ICU? Treat if you are waiting! Rapid Response if Needed Does this
ICU - Sepsis, CAUTI and CLABSI Less May Be Better. HRET HIIN ICU Virtual Event April 11, 2017
 ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU)
") Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Station Name: Mrs. Smith. Issue: Transitioning to comfort measures only (CMO)
") Station Name: Mrs. Smith Issue: Transitioning to comfort measures only (CMO) Presenting Situation: The physician will meet with Mrs. Smith s children to update them on her condition and determine the future
Station Name: Mrs. Smith Issue: Transitioning to comfort measures only (CMO) Presenting Situation: The physician will meet with Mrs. Smith s children to update them on her condition and determine the future
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Quality Improvement/Systems-based Practice. Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery
 Quality Improvement/Systems-based Practice Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery Objectives Define and understand the importance of Systems Based Practice
Quality Improvement/Systems-based Practice Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery Objectives Define and understand the importance of Systems Based Practice
Busy Lots of variety Chance to do Procedures Mix of didactics and practical experience Amount of practical experience is up to you Trauma and General
 Busy Lots of variety Chance to do Procedures Mix of didactics and practical experience Amount of practical experience is up to you Trauma and General Surgery Trauma bay, ICU, OR, floor, clinic In your
Busy Lots of variety Chance to do Procedures Mix of didactics and practical experience Amount of practical experience is up to you Trauma and General Surgery Trauma bay, ICU, OR, floor, clinic In your
I WOULD RECOMMEND INCORPORATING RECOMMENDATIONS INTO SHARED DECISION MAKING
 I WOULD RECOMMEND INCORPORATING RECOMMENDATIONS INTO SHARED DECISION MAKING JENNY WEI DO UNIVERSITY OF UTAH SCHOOL OF MEDICINE DEPARTMENT OF INTERNAL MEDICINE NOTHING TO DISCLOSE DISCLOSURES OBJECTIVES
I WOULD RECOMMEND INCORPORATING RECOMMENDATIONS INTO SHARED DECISION MAKING JENNY WEI DO UNIVERSITY OF UTAH SCHOOL OF MEDICINE DEPARTMENT OF INTERNAL MEDICINE NOTHING TO DISCLOSE DISCLOSURES OBJECTIVES
Sepsis Screening Tools
 ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
DESC Script. E Express your concerns about the action. S Suggest other alternatives. C Consequences should be stated
 DESC Script What is it? A structured, assertive, communication approach for managing and resolving conflict. D Describ e the specific situation ti E Express your concerns about the action S Suggest other
DESC Script What is it? A structured, assertive, communication approach for managing and resolving conflict. D Describ e the specific situation ti E Express your concerns about the action S Suggest other
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Kate Beaumont. Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign.
 Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring
 Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
INTERN BOOT CAMP 2017
 Sign Out INTERN BOOT CAMP 2017 Objectives Review importance of sign outs Touch on less than ideal examples of verbal and written sign outs Review the IPASS system of sign outs Review disease-specific details
Sign Out INTERN BOOT CAMP 2017 Objectives Review importance of sign outs Touch on less than ideal examples of verbal and written sign outs Review the IPASS system of sign outs Review disease-specific details
Choosing Wisely Canada 5 things NOT to do in the ICU
 Choosing Wisely Canada 5 things NOT to do in the ICU Andre Amaral, MD on behalf of the CWC Critical Care Task Force Assistant Professor Interdepartmental Division of Critical Care Medicine University of
Choosing Wisely Canada 5 things NOT to do in the ICU Andre Amaral, MD on behalf of the CWC Critical Care Task Force Assistant Professor Interdepartmental Division of Critical Care Medicine University of
CONSENT FOR SURGERY OR SPECIAL PROCEDURES
 Admission Date THE VALLEY HOSPITAL CONSENT FOR SURGERY OR SPECIAL PROCEDURES - Colonoscopy 1. Authorization. I hereby authorize Dr. (" my Doctor") and any such assistants or designees as may be selected
Admission Date THE VALLEY HOSPITAL CONSENT FOR SURGERY OR SPECIAL PROCEDURES - Colonoscopy 1. Authorization. I hereby authorize Dr. (" my Doctor") and any such assistants or designees as may be selected
Focus on Diagnostic Errors: Understanding and Prevention
 Focus on Diagnostic Errors: Understanding and Prevention Tejal Gandhi, MD MPH CPPS President, National Patient Safety Foundation Associate Professor, Harvard Medical School Thanks to Dr. Mark Graber for
Focus on Diagnostic Errors: Understanding and Prevention Tejal Gandhi, MD MPH CPPS President, National Patient Safety Foundation Associate Professor, Harvard Medical School Thanks to Dr. Mark Graber for
5/9/2015. Disclosures. Improving ICU outcomes and cost-effectiveness. Targets for improvement. A brief overview: ICU care in the United States
 Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Sepsis Care in the ED. Graduate EBP Capstone Project
 Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
MEDICAL DIRECTIVE Management of Intravenous Fluid Therapy by Anesthesia Assistants. Approved by/date: Medical Advisory Comm.
 MEDICAL DIRECTIVE Management of Intravenous Fluid Therapy by Anesthesia Assistants Approved by/: Medical Advisory Comm. May 24, 2011 Authorizing physician(s) Anesthetists, Lakeridge Health Oshawa, Department
MEDICAL DIRECTIVE Management of Intravenous Fluid Therapy by Anesthesia Assistants Approved by/: Medical Advisory Comm. May 24, 2011 Authorizing physician(s) Anesthetists, Lakeridge Health Oshawa, Department
9/17/2018. Place of Service Type of Service Patient Status
 Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Pediatric Surgery Curriculum Clinical Base Year
 Pediatric Surgery Curriculum Clinical Base Year Collaborating Faculty: Cindi Graves, MD Residency Program Director Department of Surgery Purpose and Educational Value The purpose of the Pediatric Surgery
Pediatric Surgery Curriculum Clinical Base Year Collaborating Faculty: Cindi Graves, MD Residency Program Director Department of Surgery Purpose and Educational Value The purpose of the Pediatric Surgery
9/9/2016. How Respiratory Therapist Enhance Patient Safety. Introduction. Raise your hand. Tawana Shaffer CPHRM, MBA, BSc, CRT
 How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
Auckland District Health Board Summary 1 July 2011 to 30 June 2012 Serious and Sentinel Events
 DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
2. Unlicensed assistive personnel: any personnel to whom nursing tasks are delegated and who work in settings with structured nursing organizations.
 XVII. MANAGEMENT AND DELEGATION A. General Information: The judgments that you make in management and delegation situations have to be based on knowledge. You MUST know your content, and then you can move
XVII. MANAGEMENT AND DELEGATION A. General Information: The judgments that you make in management and delegation situations have to be based on knowledge. You MUST know your content, and then you can move
A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care
 A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care Gordy Schiff, MD, Associate Director of Brigham and Women s Center for Patient Safety Research
A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care Gordy Schiff, MD, Associate Director of Brigham and Women s Center for Patient Safety Research
Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital
 Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital A doctor tends to a mortally ill child in Sir Luke Fildes s 1891 painting The Doctor. The Rise
Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital A doctor tends to a mortally ill child in Sir Luke Fildes s 1891 painting The Doctor. The Rise
Some Practical Tips on Being a Senior Pediatric Resident at McMaster
 Some Practical Tips on Being a Senior Pediatric Resident at McMaster This document is meant to provide practical information to help Junior pediatric residents transition to the Senior pediatric resident
Some Practical Tips on Being a Senior Pediatric Resident at McMaster This document is meant to provide practical information to help Junior pediatric residents transition to the Senior pediatric resident
Sepsis The Silent Killer in the NHS
 Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Patient Safety and Quality Measures for CRRT: The UAB Experience. Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012
 Patient Safety and Quality Measures for CRRT: The UAB Experience Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012 Quality Healthcare Quality is the extent to which health services for
Patient Safety and Quality Measures for CRRT: The UAB Experience Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012 Quality Healthcare Quality is the extent to which health services for
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Recognising i & Simple, yet. complex. Professor Gary B Smith, FRCA, FRCP
 GB Smith 2012 Recognising i & responding to deterioration Simple, yet surprisingly complex Professor Gary B Smith, FRCA, FRCP Centre of Postgraduate Medical Research & Education School of Health and Social
GB Smith 2012 Recognising i & responding to deterioration Simple, yet surprisingly complex Professor Gary B Smith, FRCA, FRCP Centre of Postgraduate Medical Research & Education School of Health and Social
Justifying Medicare Inpatient Admissions RAC Response and Appeals Tactics
 Justifying Medicare Inpatient Admissions RAC Response and Appeals Tactics Gregory Palega, MD JD MedManagement LLC Medical Director of Regulatory Affairs gpalega@medmanagementllc.com Objectives Learn the
Justifying Medicare Inpatient Admissions RAC Response and Appeals Tactics Gregory Palega, MD JD MedManagement LLC Medical Director of Regulatory Affairs gpalega@medmanagementllc.com Objectives Learn the
Teamwork, Communication, Briefing, Checklists, & O.R. Safety
 Teamwork, Communication, Briefing, Checklists, & O.R. Safety E. Patchen Dellinger, MD, FACS Professor of Surgery, Chief of General Surgery, Chief of Staff, University of Washington Medical Center (UWMC),
Teamwork, Communication, Briefing, Checklists, & O.R. Safety E. Patchen Dellinger, MD, FACS Professor of Surgery, Chief of General Surgery, Chief of Staff, University of Washington Medical Center (UWMC),
Developing an ED Facility Charge Calculator March 3, :00pm
 Developing an ED Facility Charge Calculator March 3, 2016 4:00pm Neal Kothe, The Ohio State University Wexner Medical Center Carol Gray, The Ohio State University Wexner Medical Center Conflict of Interest
Developing an ED Facility Charge Calculator March 3, 2016 4:00pm Neal Kothe, The Ohio State University Wexner Medical Center Carol Gray, The Ohio State University Wexner Medical Center Conflict of Interest
SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING
 SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING Dr. Duncan Hargreaves QI Fellow Worthing Hospital Allied Health Sciences Network 2017 SEPSIS IMPROVEMENT AT WSHFT QUESTcollaboration ->
SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING Dr. Duncan Hargreaves QI Fellow Worthing Hospital Allied Health Sciences Network 2017 SEPSIS IMPROVEMENT AT WSHFT QUESTcollaboration ->
To ensure oversight of resident supervision and graded authority and responsibility, the following levels of supervision are recognized:
 Roles, Responsibilities and Patient Care Activities of Residents University of Washington Boise Internal Medicine and Saint Luke s Health Care System and Saint Alphonsus Health Care System Definitions
Roles, Responsibilities and Patient Care Activities of Residents University of Washington Boise Internal Medicine and Saint Luke s Health Care System and Saint Alphonsus Health Care System Definitions
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration
 One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration Presented by: Marla Husch Northwestern Memorial Hospital Northwestern Memorial Hospital Chicago, Illinois
One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration Presented by: Marla Husch Northwestern Memorial Hospital Northwestern Memorial Hospital Chicago, Illinois
This matter was initiated by a letter from the complainant received on March 20, A response from Dr. Justin Clark was received on May 11, 2017.
 COLLEGE OF PHYSICIANS AND SURGEONS OF NOVA SCOTIA SUMMARY OF DECISION OF INVESTIGATION COMMITTEE C Dr. Justin Clark License Number: 016409 Investigations Committee C of the College of Physicians and Surgeons
COLLEGE OF PHYSICIANS AND SURGEONS OF NOVA SCOTIA SUMMARY OF DECISION OF INVESTIGATION COMMITTEE C Dr. Justin Clark License Number: 016409 Investigations Committee C of the College of Physicians and Surgeons
Introduction of an advanced practice nurse endoscopist program to Victoria
 Introduction of an advanced practice nurse endoscopist program to Victoria Melodie Heland, Director Surgical Clinical Services Unit Sylvia Constantinou, Program Manager, State Endoscopy Training Centre
Introduction of an advanced practice nurse endoscopist program to Victoria Melodie Heland, Director Surgical Clinical Services Unit Sylvia Constantinou, Program Manager, State Endoscopy Training Centre
Course: Acute Trauma Care Course Number SUR 1905 (1615)
") Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
Observation Unit. Romil Chadha
 Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
To disclose, or not to disclose (a medication error) that is the question
 that is the question") To disclose, or not to disclose (a medication error) that is the question Jennifer L. Mazan, Pharm.D., Associate Professor of Pharmacy Practice Ana C. Quiñones-Boex, Ph.D., Associate Professor of Pharmacy
To disclose, or not to disclose (a medication error) that is the question Jennifer L. Mazan, Pharm.D., Associate Professor of Pharmacy Practice Ana C. Quiñones-Boex, Ph.D., Associate Professor of Pharmacy
Rapid Response Team Building
 Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Independent investigation into the death of Mr Jeffrey Rookes a prisoner at HMP Erlestoke on 14 June 2017
 Independent investigation into the death of Mr Jeffrey Rookes a prisoner at HMP Erlestoke on 14 June 2017 Crown copyright 2017 This publication is licensed under the terms of the Open Government Licence
Independent investigation into the death of Mr Jeffrey Rookes a prisoner at HMP Erlestoke on 14 June 2017 Crown copyright 2017 This publication is licensed under the terms of the Open Government Licence
In a common ICU situation like this, there are two main questions we have to answer daily:
 MICU ROUNDING PLAN // 12.3.2014 This document contains 4 sections: 1. Rationale 2. Assumptions and ground rules 3. Detailed plan for rounding structure 4. 1-page outline of rounding structure 1. Rationale
MICU ROUNDING PLAN // 12.3.2014 This document contains 4 sections: 1. Rationale 2. Assumptions and ground rules 3. Detailed plan for rounding structure 4. 1-page outline of rounding structure 1. Rationale
Statement of Financial Responsibility
 Statement of Financial Responsibility Patient Name: Date: Acct : BIR JV, LLP including; Out-Patient, In-Patient and, Home Health Rehab appreciates the confidence you have shown in choosing us to provide
Statement of Financial Responsibility Patient Name: Date: Acct : BIR JV, LLP including; Out-Patient, In-Patient and, Home Health Rehab appreciates the confidence you have shown in choosing us to provide
Guidance on the Enhanced Recovery Programme in Colorectal Surgery Surgery Patient Information Leaflet
 Guidance on the Enhanced Recovery Programme in Colorectal Surgery Surgery Patient Information Leaflet Originator: Mr Raj Patel Date: May 2011 Version: 2 Date for Review: May 2014 DGOH Ref No: DGOH/PIL/00364
Guidance on the Enhanced Recovery Programme in Colorectal Surgery Surgery Patient Information Leaflet Originator: Mr Raj Patel Date: May 2011 Version: 2 Date for Review: May 2014 DGOH Ref No: DGOH/PIL/00364
Update on the Maryland Patient Safety Program
 Update on the Maryland Patient Safety Program Department of Heath and Mental Hygiene Wendy Kronmiller, Director Renee Webster, Assistant Director Anne Jones RN, Nurse Surveyor Fifth Annual Maryland Patient
Update on the Maryland Patient Safety Program Department of Heath and Mental Hygiene Wendy Kronmiller, Director Renee Webster, Assistant Director Anne Jones RN, Nurse Surveyor Fifth Annual Maryland Patient
University of South Dakota Vermillion, South Dakota Department of Nursing
 Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Transitions of Care: Vital to Quality Patient Care. Erica Shaver, MD WVU GME Orientation June 2017
 Transitions of Care: Vital to Quality Patient Care Erica Shaver, MD WVU GME Orientation June 2017 Goals of Session Define transition of care What makes for a good or bad handoff? ACGME expectations WVU
Transitions of Care: Vital to Quality Patient Care Erica Shaver, MD WVU GME Orientation June 2017 Goals of Session Define transition of care What makes for a good or bad handoff? ACGME expectations WVU
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD
 Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
FOCUS CHARTING. The Focus Charting System is the accepted documentation system at Windsor Regional Hospital.
 FOCUS CHARTING The Focus Charting System is the accepted documentation system at Windsor Regional Hospital. Advantages of Focus Charting Flexible enough to adapt to any clinical practice setting and promotes
FOCUS CHARTING The Focus Charting System is the accepted documentation system at Windsor Regional Hospital. Advantages of Focus Charting Flexible enough to adapt to any clinical practice setting and promotes
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Patient Safety Time for a change in design
 World Congress of Sterilization Milan Italy June 4-7, 2008 Patient Safety Time for a change in design Gina Pugliese, RN, MS Vice President, Premier Safety Institute Associate Faculty University of Illinois
World Congress of Sterilization Milan Italy June 4-7, 2008 Patient Safety Time for a change in design Gina Pugliese, RN, MS Vice President, Premier Safety Institute Associate Faculty University of Illinois
APHA CONFERENCE March 2014
 APHA CONFERENCE March 2014 Richard Royle Executive Director - UnitingCare Health Dr Luis Prado Chief Medical Officer - UnitingCare Health and Director of Medical Services - The Wesley Hospital The Wesley
APHA CONFERENCE March 2014 Richard Royle Executive Director - UnitingCare Health Dr Luis Prado Chief Medical Officer - UnitingCare Health and Director of Medical Services - The Wesley Hospital The Wesley
Application of Simulation to Improve Clinical Efficiency Systems Integration
 Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
Case study: how reliable are our healthcare systems?
 Case study: how reliable are our healthcare systems? CMSSQ Centre for Medication Safety & Service Quality Professor Bryony Dean Franklin Centre for Medication Safety and Service Quality Imperial College
Case study: how reliable are our healthcare systems? CMSSQ Centre for Medication Safety & Service Quality Professor Bryony Dean Franklin Centre for Medication Safety and Service Quality Imperial College
Just Culture Toolkit Scenarios
 Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
Laparoscopic Radical Nephrectomy
 Urology Department Laparoscopic Radical Nephrectomy Information Aims of this leaflet To give information on the intended benefits and potential risks of kidney surgery To guide you in the decisions you
Urology Department Laparoscopic Radical Nephrectomy Information Aims of this leaflet To give information on the intended benefits and potential risks of kidney surgery To guide you in the decisions you
DUKE INTERNAL MEDICINE RESIDENCY PROGRAM. GASTROENTEROLOGY SUBSPECIALTY CONSULTS (ELECTIVE) ROTATION DESCRIPTION Biliary, General GI and Hepatology
 ROTATION DESCRIPTION Biliary, General GI and Hepatology") Department of Medicine Internal Medicine Residency Program DUKE INTERNAL MEDICINE RESIDENCY PROGRAM GASTROENTEROLOGY SUBSPECIALTY CONSULTS (ELECTIVE) ROTATION DESCRIPTION Biliary, General GI and Hepatology
Department of Medicine Internal Medicine Residency Program DUKE INTERNAL MEDICINE RESIDENCY PROGRAM GASTROENTEROLOGY SUBSPECIALTY CONSULTS (ELECTIVE) ROTATION DESCRIPTION Biliary, General GI and Hepatology
A Resident-led PICU Morbidity and Mortality Conference
 A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
4/4/2012. Sign Out Competence: Easier Said Than Done. Hypothesis: Introduction. Our Program
 Introduction Information sign out is essential to patient care Sign Out Competence: Easier Said Than Done Sarah A Rawstron M.B.,B.S., Sajad Khazal M.B.,Ch.B., Cynthia Katz M.D. Duty hour restrictions (more
Introduction Information sign out is essential to patient care Sign Out Competence: Easier Said Than Done Sarah A Rawstron M.B.,B.S., Sajad Khazal M.B.,Ch.B., Cynthia Katz M.D. Duty hour restrictions (more
End Of Life Decision Making - Who s Decision Is It Anyway?
 End Of Life Decision Making - Who s Decision Is It Anyway? Kara Livy RN MN NP Critical Care Nurse Practitioner Royal Alexandra Hospital Edmonton, Alberta Kara.livy@albertahealthservices.ca End-Of-Life
End Of Life Decision Making - Who s Decision Is It Anyway? Kara Livy RN MN NP Critical Care Nurse Practitioner Royal Alexandra Hospital Edmonton, Alberta Kara.livy@albertahealthservices.ca End-Of-Life
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
The investigation of a complaint by Dr A against Cardiff and Vale University Health Board
 The investigation of a complaint by Dr A against Cardiff and Vale University Health Board A report by the Public Services Ombudsman for Wales Case: 201401302 Contents Page Introduction 3 Summary 4 The
The investigation of a complaint by Dr A against Cardiff and Vale University Health Board A report by the Public Services Ombudsman for Wales Case: 201401302 Contents Page Introduction 3 Summary 4 The
The Multidisciplinary aspects of JCI accreditation
 The Multidisciplinary aspects of JCI accreditation Saleem Kiblawi MD, FCCP, Physician consultant, Joint Commission International Oakbrook, Illinois USA Lebanese American University April 15, 2016 Beirut,
The Multidisciplinary aspects of JCI accreditation Saleem Kiblawi MD, FCCP, Physician consultant, Joint Commission International Oakbrook, Illinois USA Lebanese American University April 15, 2016 Beirut,
Penn State Milton S. Hershey Medical Center. Division of Trauma, Acute Care & Critical Care Surgery
 Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
How to Help Write a Good Consent Form: MOVING FROM! INFORMED CONSENT to INFORMED CHOICE
 How to Help Write a Good Consent Form: MOVING FROM! INFORMED CONSENT to INFORMED CHOICE Peggy Devine Founder & President Cancer Information & Support Network (CISN) C3 ASCO advocate training January 19,
How to Help Write a Good Consent Form: MOVING FROM! INFORMED CONSENT to INFORMED CHOICE Peggy Devine Founder & President Cancer Information & Support Network (CISN) C3 ASCO advocate training January 19,
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
2. Unlicensed assistive personnel: any personnel to whom nursing tasks are delegated and who work in settings with structured nursing organizations.
 XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
Massachusetts Eye and Ear Infirmary CA-3 Rotation in Anesthesiology for Otorhinolaryngologic & Ophthalmolic (ENT) procedures
 procedures") Massachusetts Eye and Ear Infirmary CA-3 Rotation in Anesthesiology for Otorhinolaryngologic & Ophthalmolic (ENT) procedures I. Medical Knowledge A. Cognitive objectives 1. Know age and size appropriate
Massachusetts Eye and Ear Infirmary CA-3 Rotation in Anesthesiology for Otorhinolaryngologic & Ophthalmolic (ENT) procedures I. Medical Knowledge A. Cognitive objectives 1. Know age and size appropriate
ACGME Institutional Requirements
 Graduate Medical Education : Focusing on Quality and Safety in a Clinical Learning Environment Developing a Standardized and Sustainable Resident Sign Out Process Better Hand Off = Safer Care Ron Amedee,
Graduate Medical Education : Focusing on Quality and Safety in a Clinical Learning Environment Developing a Standardized and Sustainable Resident Sign Out Process Better Hand Off = Safer Care Ron Amedee,
West Middlesex Junior Doctors Handbook in Colorectal Surgery
 West Middlesex Junior Doctors Handbook in Colorectal Surgery Page 1 of 10 INTRODUCTION Welcome to surgery and to the colorectal team! This guide is meant to be just that, a guide and has been principally
West Middlesex Junior Doctors Handbook in Colorectal Surgery Page 1 of 10 INTRODUCTION Welcome to surgery and to the colorectal team! This guide is meant to be just that, a guide and has been principally
ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY)
") July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD September 2012 This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies: - Blame - Denial - And the
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD September 2012 This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies: - Blame - Denial - And the