MEETING OF THE TRUST BOARD OF STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST
|
|
|
- Joleen Short
- 6 years ago
- Views:
Transcription
1 Enc 00 MEETING OF THE TRUST BOARD OF STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST Wednesday 27 January 2016 at 10.00hrs to 13.15hrs Brampton Room, Morston House, Newcastle under Lyme AGENDA Item Enc Description Time 1. Verbal Welcome and Apologies David Pearson Verbal Questions from Members of the Public David Pearson Verbal Declarations of Interest David Pearson Minutes of the last Staffordshire and Stoke on Trent Partnership NHS Enc 01 Trust Board meeting held on 25 November 2015 and matters arising David Pearson 5. Enc 01A Ambassador for Cultural Change Report Helene Donnelly Enc 02 Chief Executive Officer Report Stuart Poynor Assurance Reports Chairs of the Quality Governance, Finance Enc 03 Investment and Performance, Workforce Matters and Audit Committees David Pearson, John Scarpello, Andy Talbot and Gary Crowe Break Assurance 8. Enc 04 Corporate Risk Register Rose Goodwin Enc 05 Safe Nursing Staffing Rose Goodwin Enc 06 Quality Report Rose Goodwin Enc 07 Integrated Performance Report Month 8 Jonathan Tringham Enc 08 Finance Report Month 8 Jonathan Tringham Enc 09 Responsible Officer Medical Revalidation Q3 Report James Shipman Enc 10 Workforce Partnership Approach Tina Harkin/Julie Tanner Page 1 of 2
2 Enc Verbal Any Other Business Review of meeting and outcomes Review of risks David Pearson lunch Verbal Break for lunch Date of Next Meeting: Wednesday 24 February 2016, Boardroom 1, Edric House, Rugeley, WS15 1UW Page 2 of 2
3 Enc 01 Enclosure: 01 REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD TO BE HELD ON: WEDNESDAY 27 JANUARY 2016 Subject: Minutes of the Staffordshire and Stoke on Trent Partnership NHS Trust Board Meeting on Wednesday 25 November 2015 Strategic Goal: (tick as applicable) x We will provide high quality and safe services which provide an excellent experience and best possible outcomes x x x x We will work with users and carers to deliver integrated systems, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Director Lead: Mr David Pearson, Interim Chairman Recommendation: For Approval & Assurance x For Discussion For Information PURPOSE OF THE REPORT: The unapproved draft minutes of the Staffordshire and Stoke on Trent Partnership NHS Trust Board meeting held on Wednesday 25 November 2015 are enclosed for review and approval. INTER DEPENDENCIES: Legal and/or Risk The Trust Board reviews the outcomes of each meeting and considers whether any risks should be referred to the Executive Risk Management Committee for review and reporting onto the Corporate Risk Register. Clinical Financial HR Staff and Trade Union involvement actions undertaken/planned Social Care See content of Sub-Committee meeting minutes See content of Sub-Committee meeting minutes See content of Sub-Committee meeting minutes See content of Sub-Committee meeting minutes See content of Sub-Committee meeting minutes Page 1 of 20
4 Enc 01 Patient & Public Involvement Equality Impact Information exempt from Disclosure Requirement for further review The Patient/Staff story informs the Trust Board of any developments or improvements to the Services that we provide See content of Sub-Committee meeting minutes This is a public document Action arising from the Minutes are tracked and reviewed each month RECOMMENDATIONS: The Trust Board is requested to appraise and approve the minutes of the Trust Board Meeting held on Wednesday 25 November 2015 and to review and discuss progress or further action for the outstanding actions. Page 2 of 20
5 Enc 01 Meeting of the Trust Board of Directors of Staffordshire and Stoke on Trent Partnership NHS Trust Wednesday 27 January 2016 Morston House, The Midway, Newcastle under Lyme, Staffordshire, ST5 1BQ Overdue On Target Action Complete ACTION TRACKER Action No. Date of Meeting Action Status/ Due Date Comments (incl. interface with/ reference to another Committee/ Sub Committee/Working Group) Responsible Officer RAG Rating Deep dive workshop on patient experience to be set up The Medical Director to incorporate patient and carer experience into the Clinical Strategy Head of Service User and Carer Experience Medical Director Assurance to be provided regarding the reduction in the number of social care unallocated cases Complete. This is covered within the Social Care programme and updates provided to the QGC meetings. Director of Operations Page 3 of 20
6 Enc 01 Action No. Date of Meeting Action Status/ Due Date Comments (incl. interface with/ reference to another Committee/ Sub Committee/Working Group) Responsible Officer RAG Rating Re-ablement to be added to the Corporate Risk Register This was not able to be added to the Corporate Risk Register due to timing issues of the Executive Risk Management Committee. It will be referred to the Executive Risk Management Committee for review on the 14 th December Associate Director of Quality Weekly briefing to be prepared for Non- Executive Directors to update them on CQC and any other matters. This briefing would start in December Chief Executive Officer Column to be added to the safer staffing report to include actual bed numbers on wards Interim Director of Nursing & Quality to raise the issue of flexing the ratios by utilizing Health Care Support Workers on those wards where the acuity of the patients is lower at the Financial Recovery Group and report the outcomes of this work to the next meeting of the Board Interim Director of Nursing & Quality Completed. Reviewed at EMT Interim Director of Nursing & Quality The Interim Director of Nursing & Quality would raise the health and safety Completed. The Chair of Falls Committee will report any issues Interim Director of Nursing & Quality Page 4 of 20
7 Enc 01 Action No. Date of Meeting Action Status/ Due Date Comments (incl. interface with/ reference to another Committee/ Sub Committee/Working Group) Responsible Officer RAG Rating element linked with falls with the Chair of the Falls Prevention Panel. relating to Health & Safety Interim Director of Nursing & Quality arrange a deep dive into Falls at a Quality Governance Committee meeting in this year s cycle of business This is already included in the cycle of business Interim Director of Nursing & Quality Page 5 of 20
8
9 Enc 01 MEETING OF THE TRUST BOARD OF STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST Wednesday 25 November 2015 Brampton Room, Morston House, Newcastle under Lyme Present: David Pearson DP Interim Chairman Gary Crowe GC Non-Executive Director Jane Gaddum JG Non-Executive Director Rosie Goodwin RG Interim Director of Nursing & Quality Geraint Griffiths GG Deputy Chief Executive Kieron Murphy KM Director of Operations Elizabeth Jarrett EJ Non-Executive Director Stuart Poynor SP Chief Executive Officer Dr James Shipman JSh Medical Director (part) Julie Tanner JkT Director of Workforce & Development Jonathan Tringham JT Director of Finance & Resources Paul Weston PW Non-Executive Director Designate Apologies: Dr John Scarpello JS Non-Executive Director Andy Talbot AT Non-Executive Director Designate In attendance Andrew Errington AE Professional Head of Social Work Nic Glover NG Executive Assistant to Chairman and CEO Chris Beswick CB Staffside Representative Melanie Print MP Company Secretary Welcome and Apologies The Interim Chairman welcomed Board Members, Staff Members and Members of the Public. Apologies were received from John Scarpello and Andy Talbot Questions from Members of the Public The Interim Chairman invited questions from the members of the public, confirming that there would be a further opportunity at the end of the Board to ask questions of the Board Declarations of Interest The Interim Chairman asked if Trust Board Members had any declarations of Page 6 of 20
10 Enc 01 interest to declare. The Medical Director referred to his standing declaration that he is employed (part time) as a salaried GP within the local health economy. Non-Executive Director Designate, Mr Weston declared he was the Chief Financial Officer for Housing and Care 21 Ltd. The Interim Chairman welcomed Claire Neill the Trust s new Associate Director of Communications to the Trust. The Interim Chairman informed Board Members that Keele University School of Nursing and Midwifery s Mentor of the Year Award has been won by Hannah Beech from Clayton District Nursing Team, who was highly praised by two students with comments I have nothing but praise for Hannah and I was genuinely disappointed when I left the placement area. She is a fantastic mentor in a fantastic placement area and feel very lucky to have been able to work there and Hannah is an inspiration, very patient centred and knowledgeable. She has given me much needed confidence to progress in my career and I have gained skills and knowledge that have proved invaluable. The Interim Chairman informed Board Members that Steve Kenyon, Clinical Lead for the Continence Team in the North was one of a small number of specialist clinicians, MPs and other stakeholders from across the UK to be invited to a Parliamentary Reception at the House of Commons on 4 November The Interim Chairman informed Board Members of the very sad news that Sarah Whittingham, one of the Trust s Community Staff Nurse/Specialist Practitioner Student in Alrewas had passed away tragically and unexpectedly at the weekend. The Interim Chairman informed Board Members that Sarah s Team were being supported Minutes of the meeting and matters arising The Interim Chairman referred Trust Board Members to the minutes of the Trust Board meeting held on 28 October 2015 and Board Members agreed the minutes as a correct record apart from the following changes: Page 5 title change, Interim Medical Director to Medical Director Page 5 title change Paul Weston, Non-Executive Director to Non- Executive Director Designate Page 5 title change Andrew Errington from Professional Head of Social Care to Professional Head of Social Work Page 10, , first sentence should read Board Members which now annexed (for this month a sample) instead of Board Members which now annexed (fir this month a sample) Page 15, , fourth paragraph last sentence should read preparing a report as SIRO for the FIP Committee and not FIP Commitment Board Members went through the action tracker and noted that all actions were either on target or complete Patient story Page 7 of 20
11 Enc 01 The Interim Chairman Mr Pearson welcomed Mr and Mrs Abbotts to the meeting. Mr and Mrs Abbotts informed Board Members that Mr Abbots had been receiving care for many years from the Bucknall ILCT and has remained highly independent, with support from Mrs Abbotts as his carer; they can contact the Community Matron, Morlich Barnett, should Mr Abbotts symptoms change but they generally manage his COPD. Mr and Mrs Abbotts informed Board Members that Mr Abbotts had been diagnosed with terminal liver cancer and that Bucknall ILCT immediately contacted the cancer and supportive therapies team to provide guidance and assistance to Mr and Mrs Abbotts, as well as the oncology specialists at the Royal Stoke Hospital. Following oral chemotherapy, Mr Abbotts experienced a number of severe side effects which required additional medication and the Douglas Macmillan Hospice provide palliative care and support. Around the time of the diagnosis, Mrs Abbotts suffered from a back injury; she was unable to continue caring for Mr Abbotts. Bucknall ILCT worked with the Intermediate Care Team to provide ongoing personal care, support and assistance to Mr Abbotts. The two teams, along with the Douglas Macmillan, offered support and comfort to Mr & Mrs Abbotts, as they had lost a significant element of their independence, whilst also having to come to terms with the diagnosis of terminal liver cancer. Following the involvement of the Douglas Macmillan, Bucknall ILCT worked with Mr Abbotts GP to arrange a DS1500, providing them with end of life care funding. Mr Abbotts said that whilst he is still suffering from COPD and terminal liver cancer, he continues to be as independent as he can with the aid of Mrs Abbots and attributes this to the continued, outstanding care which went above and beyond what was expected from the Partnership Trust teams. Mr and Mrs Abbotts noted that during such a time of crisis for the couple, the stability offered to them both by Community Matron Barnett and her team was exceptional. The Interim Chairman thanked Mr and Mrs Abbotts for attending the Trust Board to inform Board Members of their story and personally thanked Morlich Barnett for the exemplary care and support that she had provided to them Chief Executive Officer Report The Chief Executive Officer referred Members of the Board to his report which highlighted a number of national and local items as follows: Matters of national significance: NHS Confederation; Government response to the House of Commons Health Select Committee report on End of Life Care; CQC s proposed changes to fees and the move to a risk based regime; NHS bodies proposals on changes to safe staffing guidance; NHS Employers welcomes lifting of restrictions on nurses being recruited from outside the EU; Public health cuts in the upcoming spending review; NHS Clinical Commissioners and NHS Providers news; Changes to the National tariff; Ofsted ratings for CCGs; Patient power; Page 8 of 20
12 Enc 01 Neglect claims for older people rise as services are cut; Nurse validation faces two year delay; NHS to remove names from job applications to prevent discrimination; News from NHS England. Matters of local significance: HSJ award; National award for Stoke Speech and Language Therapist; User Carer Experience; CQC visit; Offender Health. The Chief Executive Officer appraised the Board of the initial feedback from CQC; the recognition that staff were caring and compassionate and the steps that had been implemented to address matters highlighted by CQC; and the prospective timeline for the publication of the Inspection Report; CQC had highlighted that staff were a credit to our Trust but there are a number of concerns that we have committed to address as a priority. The Chief Executive Officer informed Board Members that the Trust was finding itself in a very challenging position; appraised them of the outcomes of the limited assurance report of the Internal Auditors which had been discussed at the Executive Management Team on the 24 th November; reporting that a more directed financial recovery would be implemented and that he would continue to drive the financial recovery and CIP recovery through his chairmanship of the Financial Recovery Group and the CIP Scrutiny Panel. The Director of Finance & Resources would discuss in further detail in his report. The Chief Executive Officer informed Board Members that the Trust had not been successful in its tender bid for offender health; the bid had been awarded to a private company. Non-Executive Director, Mrs Gaddum asked for feedback on why the Trust had not won the tender. The Deputy Chief Executive reported that successful bidder could demonstrate better partnership working with a mental health partner and drug and alcohol support. The Chief Executive Officer informed Board Members that Staffordshire County Council had asked for and been granted an extension with regard to the Quarter 2 review of the Section 75 agreement; there would be a need for an extra-ordinary Board meeting to discuss the outcome of the Quarter 2 review. Board members discussed availability and it was agreed that an extra-ordinary Board meeting would be convened for the 16 th December The Interim Chairman urged that the reports to be made to this meeting are referred to Board members well in advance of the meeting. The Chief Executive Officer informed Board Members that there were ongoing challenges within the local health economy at the current time due to the continuing negotiations around the Step Up and Step Down specifications and the localities for these services; no contract variation had yet been agreed with the commissioners. Non-Executive Director Designate, Mr Weston asked for more clarity regarding information in the report and the context for the Trust. Non-Executive Director, Mrs Jarrett asked if the information in the report could be Page 9 of 20
13 Enc 01 put together in sections. The Chief Executive Officer agreed that the contents of the report needed to be reframed within a context which is meaningful and relevant to the Trust. The Trust Board noted the contents of the Chief Executive Officer report Assurance Reports Quality Governance Committee Quality Governance Committee The Interim Chairman and Chairman of the Quality Governance Committee, Mr Pearson presented the assurance report for the Quality Governance Committee in relation to the matters and business of the meeting of 11 November 2015 and reported the following items of business which the Committee had agreed to refer to the Board for its consideration and required action as appropriate: The Committee received an escalation report from the Safety & Effectiveness Sub-committee concerning a trend in the cancellation of secondary care appointments for offenders as a result of insufficient escorts. All cancelled visits have been logged as an incident. The Committee was appraised of the actions taken to mitigate this risk, including notification to the Commissioners and the Prison Governors of the need for additional escorts. The Specialist Divisional Business Meeting will maintain oversight of this risk. The Committee reviewed an assurance report into the outcomes of the reviews undertaken by the Mortality Review Group; there has been an increase in the number of deaths principally due to the high numbers of palliative care patients. The Medical Director reported that as the Trust had had to flex the Grange Ward criteria to receive palliative care cases from Royal Stoke the Chair of the Clinical Quality Review Meeting has agreed to review palliative care provision. This report is shared with Commissioners through the Clinical Quality Review Meeting. The Committee has requested that the learning actions which relate to the admission of frail patients outside normal medical staffing hours are addressed in the Hospital Transfers Meeting and through the Discharge Policy (which is due to be submitted to the Committee in January 2016) so as to ensure that any discharges are safe. The Committee received an outline of the Healthcheck early warning system and were not assured that this had been embedded into the governance of quality; the Committee recommended that the Director of Operations report back to the Committee in January with a flow chart which maps the reporting, triggers and escalations of the early warning system into the governance of quality and confirmation as to the thresholds which would trigger a quality visit, together with the timeline as to when this process is to be fully implemented. The Committee received a verbal update as to the initial overview of the Care Quality Commission; they were assured by the Chief Executive Officer that immediate action has been taken to address the initial concerns raised by the Care Quality Commission; Executive Director leads have been assigned to each of these actions and a full report will be made to the next meeting of the Committee. The Executive Management Team will monitor weekly progress and will escalate any risks to the Board. Non-Executive Director, Mrs Gaddum asked for clarification on the point regarding Page 10 of 20
14 Enc 01 the escalations from the CQC Inspection, and the need for oversight by the Board. The Chief Executive Officer assured Mrs Gaddum and the Board that there would be a weekly briefing prepared for Non-Executive Directors to update them on CQC and any other matters. This briefing would start in December. SP The Trust Board received the assurance report of the Chair of the Quality Governance Committee into the matters and business arising from the meeting of the Committee on the 11 November Audit Committee The Chairman of the Audit Committee, Mr Crowe presented the assurance report for the Audit Committee in relation to the matters and business of the meeting of 13 November 2015 and he referred the Board to the following items of business for its consideration and required action as appropriate: The Committee reviewed the Internal Audit Progress report. It recommended that the actions relating to the limited assurance audit of the Burton Agency Account are prioritised for closure and it has reiterated its expectation that all actions are responded to and closed within the timeframes agreed with the Internal Auditors. The Committee would advise the Board that the meeting took some time to review and consider the Internal Auditors report into financial management and CIP arrangements ; the Committee welcomed the fact that audit testing has confirmed that each CIP is supported by a Project Initiation Document and a Quality Impact Assessment and that improved delivery and accountability is delivered through the Chief Executive Officer s chairmanship of the CIP Scrutiny Committee; these actions address the concerns highlighted by the Internal Auditors earlier in the year. It is of concern that this report is of limited assurance. The Committee has recommended that the outcomes of the Internal Auditors review are reported to the Executive Management Team for immediate implementation of those actions required to address the limited assurance, with an update report to the Board by the Chief Executive Officer. The Committee has welcomed the assurances of the Director of Finance & Resources that the performance management framework is re-instated as an immediate priority. The Deputy Chief Executive urged that a full response is made to the Internal Audit report at the next Audit Committee so that we can mitigate the limited assurances that were reviewed at the Executive Management Team meeting on the 25 th November. The Chief Executive Officer reported that he will personally review all Schemes prior to the next meeting of the CIP Scrutiny Panel and he will respond to those recommendations in the Report which have been assigned to him as the Accountable Officer. Non-Executive Director Gary Crowe sought confirmation that all Executive Directors understood the context of the limited assurances and urged that a collective response is made. The Chief Executive Officer reported that he will secure that a collective response is Page 11 of 20
15 Enc 01 made. Councillor Jones noted that the Trust s liquidity score had decreased and asked whether the External Auditors had expressed any concerns as to whether the Trust could continue to demonstrate that it was a going concern. The Director of Finance & Resources responded that the liquidity score is 2; we have a cash balance of 8.7M which has decreased as a result of outstanding debts, principally monies due from Stoke on Trent City Council; no concerns have been raised by the External Auditors and no conditions were applied in their audit of the Accounts for 2014/15. The Trust Board received the assurance report of the Chair of the Audit Committee into the matters and business arising from the meeting of the Committee on the 13 November 2015 and noted the steps that were being taken to address the limited assurances reported in the Internal Auditors report into financial management and CIP Corporate Risk Register The Interim Director of Nursing & Quality presented the Corporate Risk Register to Board Members for their review; informing the Board that the Risk Register has been reviewed and the following changes were made at the Executive Risk Management Committee on 9 November One risk was identified for de-escalation from the Corporate Risk Register: Lack of integrated management information to support planning and delivery of services. The Interim Director of Nursing & Quality informed Board Members that the Committee reviewed the quarterly review report of all risks 12 and above. The Committee discussed the emerging risks and reviewed the risks so as to identify any new risks for escalation to the Corporate Risk Register. Two risks were identified for further review prior to escalation onto the Corporate Risk Register and will be reviewed at the next Committee. The Trust Board noted the updated version of the Corporate Risk Register appended to this Report and noted the actions that are being taken to manage the reported risks Safer Nursing Staffing The Interim Director of Nursing & Quality presented the Safer Nursing Staffing report to Board Members providing an overview of nurse staffing levels in the Community Hospitals of the Partnership NHS Trust during October The Interim Director of Nursing & Quality informed Board Members that key points to note in the report are: Safe staffing has been maintained throughout October 2015 across all 4 Community Hospitals operated by the Partnership Trust. The number of shifts being characterised as being of professional concern (red) has increased to from 7 to 16. Late transfers of patients (after 9pm), late notice sickness and unpredicted changes in patient acuity have all contributed to this change. The number of shifts characterised as amber has risen by 3% from 19.4% to Page 12 of 20
16 22.4% The number of shifts with only 1 RN on duty has doubled to 18 from September 2015 s figures. Ward 2 at Cheadle remains an outlier against registered nurse to patient ratios during day time shifts and Cottage Ward at Leek Moorlands Hospital exceeds the best practice ratio for night time shifts. There have been no patient safety issues reported on these wards related to staffing. There has been an increase in shifts not meeting the agreed establishment figures for registered nursing staff as a result of vacancies, sickness and the agreed D2A project establishment profile. The number of shifts with additional care worker on duty continues to climb in response to the need to carry out close supervision and monitoring for those at risk of falls. The Interim Chairman was concerned about the late transfers of care and the reported information on the decrease in the successful recruitment to nurse vacancies. The Interim Director of Nursing and Quality assured the Interim Chairman that these late transfers are monitored; three late transfers had happened on one late shift; and one patient had required 1:1 care; all late transfers are incident reported and the handovers monitored. The Director of Workforce & Development reported that special measures had been applied to the recruitment to these vacancies but we remained in competition with other providers. Non-Executive Director, Mrs. Jarrett asked how we systematically reviewed the patient experience for those patients who had been subject to the late transfers? The Interim Director of Nursing and Quality responded that patients and families were met with and the patient experience information was triangulated with safer staffing reports. Enc 01 Non-Executive Director Designate, Mr. Weston asked if there was any scope to tighten up on the staffing ratios due to the financial predicament the Trust found itself in. The Interim Director of Nursing & Quality responded that there is a recognition that we need to flex the ratios by utilizing Health Care Support Workers on those wards where the acuity of the patients is lower; she will raise this at the Financial Recovery Group and report the outcomes of this work to the next meeting of the Board. RG The Medical Director reported that we are achieving a ratio of 1:7 which is better that many Acute Trusts and that only 1.5% of the Trust s shifts were of professional concern. Councillor Jones asked what actions the Trust was undertaking regarding its use of agency staff. The Director of Workforce & Development reported that the national caps for agency staff were now in force and that she was confident that with the implementation of the Trust wide Bank the agency bill will be significantly reduced. The Medical Director asked for a column to be added to the report to include the actual bed numbers. Page 13 of 20
17 Enc 01 The Director of Operations reported to the Board that whilst there were no mandated safe staffing ratios in community nursing he had recognized that it is operationally imperative that we assure ourselves that the ratios in community nursing are safe; he indicated that Operations had developed a template for the 32 teams which looked at a range of indicators, such as sickness, incidents, staffing and complaints; these are RAG rated and assigned to managers and he reviews the actions taken to make the teams safe. This had been approved at the Executive Management Team and is now reported to the Clinical Quality Review Meeting. The Company Secretary advised the Board that in the context of the discussions today the recommendations that the Trust be assured that the Trust is compliant with safe staffing nursing cannot be endorsed; as such the Board can only endorse the proposition that there are controls in place to systematically monitor compliance with safe staffing guidance.. Board Members agreed and recommended that the report content is noted and that the Board is assured that the organisation has controls in place to systematically monitor its compliance with safe nurse staffing guidance for October Quality Report The Interim Director of Nursing & Quality presented the Quality report to Board Members which provide the experience, safety, and effectiveness data of service users and carers during September The Interim Director of Nursing & Quality outlined the key points of note in the report, reporting that there had been an increase in falls (with no increase in harm) and that this is due to the need to get patients mobilised so that they can become independent; it is part and parcel of their rehabilitation before they are discharged. The Medical Director asked whether we captured other harm such as a loss of confidence and a decline in mobility as a result of increased length of stays. The Interim Director of Nursing & Quality reported that we can examine these issues at a deep dive into Falls at the Quality Governance Committee. Board members agreed and asked that the Interim Director of Nursing & Quality arrange a deep dive into Falls at a Quality Governance Committee meeting in this year s cycle of business. RG Non-Executive Director Designate, Mr Weston asked for clarification on social care complaints in relation to the quality of care and services provided by other providers. The Company Secretary reported that the County Council undertake quality monitoring of those providers with which we contract for services such as domiciliary care and residential care, as the County Council manage these contracts; any concerns are reported to the Quality Team. The Board discussed and noted the quality indicators in the dashboard of the key points for September Page 14 of 20
18 Enc Integrated Performance Report Month 7 The Director of Finance and Resources presented the Month 7 Integrated Performance Report to Board Members which provided a concise integrated view of performance across the organisation for October 2015; informing Board Members that of the 59 performance indicators with targets attached, 40 are green, 5 are amber and 14 are red. There is to be a review of the suite of the KPIs that the Trust reports against so that there is a more proportionate and contextual overview of the key areas of performance that the Board should be concerned with. The Director of Finance and Resources informed Board Members that key areas of strong performance improvement include: Customer satisfaction with social care support increased from 66% to 73% in October against a target of 72%. For the first time in the year we have no red indicators in the Quality section of the quadrant. The Director of Finance and Resources informed Board Members that key performance concerns include: The only indicator rated red in the Quality Assessment continues to be the percentage of harm free care in the safety thermometer (90.9% against a target of 95%). Social care delayed transfers of care still show no sign of improvement, and deteriorated slightly further in September. Most other underperforming social care indicators remain fairly static with no signs of decisive improvement. This includes: reablement leading to no need for on-going support, proportion of clients in receipt of direct payments, and reviews. New performance improvement plans were launched in October and are now being embedded at Team level. Agreement has been made to an increase in interim capacity to support reviews. CIP delivery is ahead of schedule (130%), financial performance has deteriorated, mostly due to adult social care demand pressures. Despite stable patterns of improvement, appraisals (73.65%) and training compliance (83.29%) remain below their respective targets (95%, and 90%). The Director of Finance & Resources referred the Board to Annex 5 the Self Certification Board Statement; reporting that he and the Company Secretary had appraised the Finance & Performance Committee that the report could not report compliance with statement 10 having regard to the deteriorating financial position and the limited assurance report of the Internal Auditors as reported in the context of the Finance Report (Agenda item 8 refers). The Board agreed that a non-compliance statement should be reported. The Chief Executive Officer asked what this meant for the Trust. The Company Secretary reported that on reporting non-compliance it is necessary for a report to be made to the TDA as to the steps that will be taken to enable the Board to report compliance with this statement; this can then be monitored by the Board; the report would need to be made by the Chief Executive Officer as the Accountable Officer. Page 15 of 20
19 Enc 01 The Interim Chairman asked the Director of Operations what was being done to improve operational performance in relation to each of the areas against which operational performance continued to perform poorly; were their improvement plans in place; and who monitored them? The Director of Operations assured the Board that there was a detailed improvement plan in place for each indicator which is supported by an implementation group; the Executive Management Team had supported investment in additional OTs (contracted through a supplier on a framework) to secure the delivery of quicker assessments and reviews; he recognises his own accountability to deliver better operational performance; and he reported that he was confident that these measures would significantly improve the performance of the red indicators, The Trust Board noted the content of the executive summary and performance scorecard and endorsed the proposal that non-compliance with statement 10 should be reported against the Self-certification Board Statement Finance Report Month 7 The Director of Finance and Resources presented the Month 7 Finance Report to Board Members and asked them to consider the financial outlook arising from this. The Director of Finance and Resources informed Board Members that the Trust is reporting an actual deficit of 4.920m at the end of Month 7, representing an adverse variance of 3.871m against an internal budgeted deficit to date of 1.049m. This compares to the revised planning position submitted to the Trust Development Authority (TDA) of 4.114m deficit at this stage; performance at Month 7 has drifted seriously above the level expected, with much of this attributable to Adult Social Care (ASC) demand pressures in the South of the county, particularly in residential care where there remained continuing difficulties in finding beds into which placements could be made. The Director of Finance and Resources informed Board Members that as highlighted in the planning and monitoring reports presented to the Trust Board over previous months, the risks in delivering the Cost Improvement Programme (CIP) target, and ASC spend within the resource provided under the second term of the Section 75 Agreement with Staffordshire County Council (SCC), are critical to the Trust s financial prospects for the financial year. He appraised the Board of the in-month ( run-rate ) deficit of 1.1m, representing an increase over the run-rate at Month 6 ( 0.5m deficit). It is in excess of the planned deficit of 0.3m; this position includes the full YTD value of the Trust s negotiating stance with regard to the closure of wards at Longton Cottage Hospital and the Trust s evaluation of the funding due from Staffordshire County Council under the inflationary provisions of the risk-share agreement; he appraised Board Members that this is predicated on the recovery of 1.5M. The forecast deficit in Adult Social Care will be 3.9M unless both the full risk share is secured from the County Council and the Social Care Transformation Plan delivers to the quantum that has been reported to the Board. The Director of Finance and Resources informed Board Members that the best Page 16 of 20
20 case position of 2.015m submitted to the TDA in September has to now be regarded as daunting and that the achievement of this position is dependent upon full delivery of best case scenarios in relation to CIP savings, financial recovery programmes, the risk-share negotiations with the County Council, and containment of the underlying run rate. He reported to the Board that contractual pressures will increase over the next Quarter and that the disparity that existed between the parties in negotiating the contract variation relating to the re-design of services in the North economy ( stepup/step-down ), as articulated to the Trust Board last month, has been mitigated through the Commissioners accepting the Trust s cost model, subject to an independent due diligence of the model. The Director of Finance and Resources informed Board Members that it is imperative that every opportunity is taken to maximise cost reductions and increase income. The Chief Executive Officer reported that it had been agreed that all corporate and managerial vacancies in Operations are frozen subject to a business case which is predicated on invest to save principles. Councillor Jones noted that the Council was also in a difficult financial position; it could not rely on its reserves to cover off the Adult Social Care deficit; the risk share was not agreed and he would question the capability of the Trust to deliver the benefits of integration as evidenced by the static performance in undertaking reviews and the need to better show the benefits of Reablement services; the driver for the variance appears to solely relate to the failure to deliver the CIP? The Chief Executive Officer reported to Councillor Jones that the Trust delivered on its contract with the Council over the three years from 2012 to 2015 at a cost to the Trust of 1M; a matter of public record, as evidenced by our Public Accounts; the accountability for delivering the Adult Social Care Transformation Programme was joint as between the Director of Operations and the Interim DASS; and he will appreciate that the new Section 75 Agreement had been redrawn so as to emphasis better partnership working. The Director of Finance & Resources reiterated the principles of joint partnership and reported to the Board that in recent years the Trust has moved from an investment of 1,190 per client to 890 per client; this is the cost to the County Council of commissioning Adult Social Care; it benchmarks within the lowest quartile of Councils In England and that fundamentally there is a need to agree what level of commissioned investment (per client) is sufficient to deliver the services and care that the Trust is commissioned to deliver; the Trust has invested in additional OTs to undertake reviews so as to ascertain whether the cost of care (against assessed need) can be reduced. The Chief Executive Officer reported that the Council had recently agreed that the Trust could become a provider of domiciliary care; a position they had resisted until recently as they had been keen to manage this market. Councillor Jones reported that Healthwatch had undertaken a review of a residential home in a morning could the Trust do this? Non-Executive Director, Mrs Jarrett reported that Healthwatch do not do full reviews such as a review of records, care and medicines and asked what was driving the Enc 01 Page 17 of 20
21 Enc 01 demand in the South as it is focussed on Adult Social Care. The Director of Finance & Resources reported that it is a different model in the South with fewer Community Hospitals and limited Discharge to Assess capacity; this meant that patients were discharged from Acute Care to their homes or Residential/Nursing Care. Non-Executive Director Mr Crowe asked whether we can be confident that we will deliver the best case scenario? The Director of Finance & Resources informed the Board that we approaching the end of Quarter 3 and unless the financial recovery can be ramped up and the savings from the Transformation Programme for Adult Social Care start to rapidly deliver then we will not achieve the best case scenario. Non-Executive Director Designate, Mr Weston asked if the 9.7m was a projected best or worst case scenario and the Director of Finance & Resources confirmed this figure was if the Trust continued with the current run rate. The Medical Director asked if the domiciliary care issue was on the Corporate Risk Register for both the Council and the Trust. Non-Executive Director Mrs Gaddum asked whether the loss of recent tenders in Offender Heath and East Staffordshire would impact on this year s financial position or next year s financial position? The Director of Finance & Resources confirmed that the school nursing tender would affect this year s financial position and the East Staffs and Offender Health would affect next year. Councillor Jones commented that the Clinical Commissioning Groups in North Staffordshire were ineffective. The Interim Chairman stated that we need absolute clarity as to what can be delivered under the Transformation Programme for Adult Social Care; that the report into the Quarter 2 review (for Adult Social Care) needs to be made available to Board Members well in advance of the Extraordinary Board Meeting and that the principles of partnership will need to be reinforced at the forthcoming Trust Board to Cabinet meeting in early December. The Interim Chairman asked for assurance that a more directed approach to financial recovery be agreed by the Executive Directors. The Chief Executive Officer reiterated that he would be chairing the Financial Recovery Group and he would reiterate to all members of that Group as to the imperative to secure financial recovery in the terms outlined to the Board today. The Company Secretary advised the Board that the recommendations were seeking their active consideration as what steps should be implemented to secure financial recovery; reiterating that the Board has agreed to report non-compliance with statement 10 of the Self-certification Statement and as such the Board need actively consider what actions they should endorse to secure the best prospects of financial recovery. The Trust Board reviewed in detail the forecast financial performance of the Page 18 of 20
22 Enc 01 Trust at the end of October 2015 (Month 7) and fully endorsed the following actions to achieve a best case position of a deficit of 2.015m: Review of all Agency Staff Ensure appropriate accounting for capital expenditure Review of 2016/17 CIP schemes for pull forward Review areas for invest to save in ASC Review of Nursing levels in Community Hospitals Income Maximisation Review of over performing services Cost benefit analysis for recruitment Freeze on Management posts above Band 7 subject to demonstrating ROI Ensure recovery under Risk share with SCC Review Consultant job plans Acceleration of Social Care Transformation Directed control of discretionary expenditure Board Assurance Framework The Company Secretary presented the Board Assurance Framework to Board Members informing them that the Board Assurance Framework (BAF), annexed to the report is the second iteration of the BAF, changes having been made as a consequence of an advisory review by the Internal Auditors. This report highlights the changes made and the next steps to secure implementation of those changes. The Company Secretary outlined the changes that had been made following the interim review by the Internal Auditors and the agreement of the Audit Committee to the same, as follows: High signifying full assurance has been provided over the effectiveness of the reported controls supported by independent testing; Medium signifying that some assurances are in place and/or the controls are still maturing so the effectiveness of the same cannot be fully assessed. The presumption is that the efficacy of the controls will improve; Low signifying that the assurance that has been provided is showing poor effectiveness of controls, this maybe evidenced by independent testing by the Internal Auditors, other agencies and regulators. This iteration of the BAF applies an indicative confidence rating to the relevant controls. The interim review of the BAF by the Internal Auditors has reported that: Currently the level of comfort in the assurances provided is not recorded in the BAF. This is considered to be good practice. Assurances which are categorised as low will be prioritised for review by the Audit Committee. The next iteration of the BAF (to be reported to the Audit Committee and Board In January 2016) and will incorporate revised and clear actions with a cross reference to any supporting evidence e.g. positive assurance report from the Internal Auditors. Non-Executive Director Gary Crowe endorsed the changes that had been approved Page 19 of 20
23 at the Audit Committee, the continuing support and input from the Company Secretary in improving the BAF and pointed out the Committee would be looking for better operational assurance, the Director of Operations having attended the Committee to assure them that this is a priority; the Committee will test these assurances, over the next Quarter of its business cycle, by reference to the confidence score that has been assigned to the assurances received. The Trust Board: reviewed this iteration of the BAF and endorsed the proposition that the assurance level assigned to each assurance is reviewed and confirmed by the relevant Executive Director; endorsed a review of the assurances assigned to the relevant principal Committees by the sponsor Committee supported by an assurance report to the Audit Committee by the Chair of each Committee; supported a development session of the Board with CW Audit Services, the Chair of the Audit Committee and the Company Secretary into the further development of the Board Assurance Framework and the supporting escalation framework for risks and assurances early in Any Other Business None. Review of meeting and outcomes The Interim Chairman, Mr Pearson asked Board Members for any comments regarding the meeting; Members of the Board responded that they had felt it was a much more focussed and positive meeting. Enc Date of next meeting The next Public Trust Board Meeting will be held on Wednesday 27 January 2016 at Morston House, Newcastle under Lyme. Page 20 of 20
24
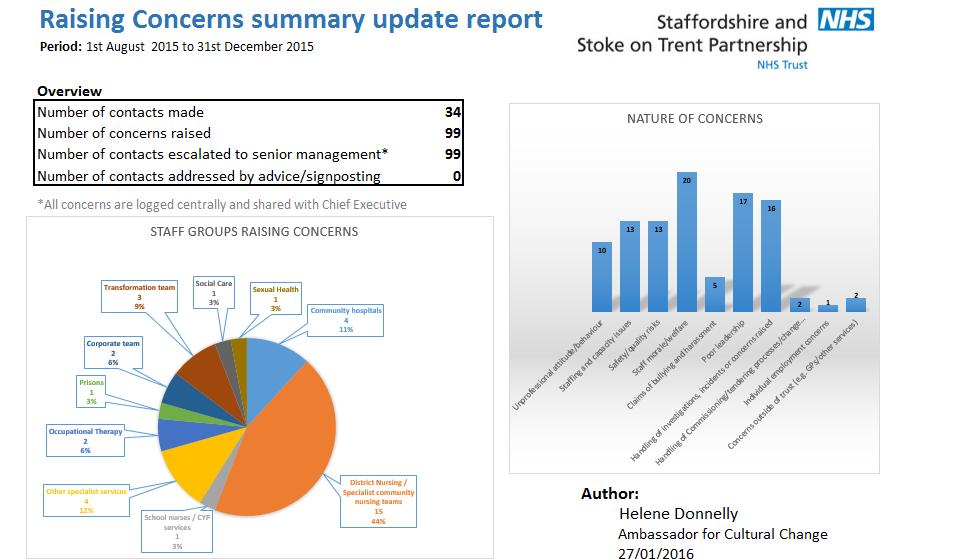
25 Enc 01A REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD TO BE HELD ON: WEDNESDAY 27 JANUARY 2016 Enclosure: Subject: 01A Report of the Ambassador for Cultural Change Quarter 3 Raising Concerns Strategic Goal: (tick as applicable) x We will provide high quality and safe services which provide an excellent experience and best possible outcomes x x x x We will work with users and carers to deliver integrated systems, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Director Lead: Helene Donnelly, Ambassador for Cultural Change Recommendation: For Approval & Assurance For Discussion x For Information PURPOSE OF THE REPORT: To provide an overview and update to the Trust Board on Raising Concerns to the period ending on 31 December INTER DEPENDENCIES: Legal and/or Risk A national framework for raising concerns Freedom to Speak Up has been the subject of consultation. Once launched the Trust will need to ensure that its procedures and supporting policies for raising concerns are aligned to the national framework. Clinical Financial HR Staff and Trade Union involvement Clinical risks that are highlighted within any concern raised are referred to the Medical Director / Interim Director of Nursing & Quality for review. Some concerns may require additional investment to mitigate the risks of low staff morale/capacity. Workforce risks that are highlighted within any concern raised are referred to Director of Workforce & Development for review. None at this time Page 1 of 2
26 Enc 01A actions undertaken/planned Social Care Patient & Public Involvement Equality Impact Information exempt from Disclosure Requirement for further review None at this time. Patient concerns are addressed through PALs/Complaints and frontline staff. An equality impact assessment of the new Freedom to Speak Up framework will be undertaken. None. Quarterly report to the Board RECOMMENDATIONS: The Trust Board is requested to review and discuss the Raising Concerns report of the Ambassador for Cultural Change. Page 2 of 2
27
28
29 Enc 02 REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD TO BE HELD ON: 27 January 2015 Enclosure: 02 Subject: Chief Executive Officer Report Strategic Goal: (tick as applicable) We will provide high quality and safe services which provide an excellent experience and best possible outcomes We will work with users and carers to deliver integrated services, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Director Lead: Stuart Poynor, Chief Executive Officer Recommendation: For Approval & Assurance For Discussion For Information x PURPOSE OF THE REPORT To provide members of the Partnership Trust Board with an update from the Chief Executive Officer. KEY POINTS LOCAL We put quality first We submitted the first response to the Care Quality Commission on time and have received three draft reports (Brighton House, Living Independently Staffordshire) Good partnership working helped manage winter pressures World Aids Day and HIV testing week were both celebrated A lot of work has been done to raise the profile of preventing pressure ulcers 1
30 Our therapy services have been recognised in a number of different ways We focus on people After almost 30 years pioneering rehabilitation medicine, Professor Ward retires All 14 community nurses supported by the Trust to undertake the Specialist Practitioner Qualification are now in district nursing sister positions Keele University recognised our practice educator mentors Our visual impairment rehabilitation officers secured the NHS Collaboration award for their work with Staffordshire Fire and Rescue Service. The family nurse partnership celebrated the latest cohort of mums to graduate from the programme The New Year gave us the opportunity to promote our healthy lifestyle service, Together 4 Health Our joint social care transformation programme with Staffordshire County Council is progressing well Bronze, silver and gold awards made. We take responsibility What our patients, service users and carers can expect from us when things go wrong Following national changes to the way health visiting is commissioned, we are organising our staff along the boundaries of the two local authorities within which we work We are leading the way on integration by delivering the multi-specialist community provider model set out in the five year forward view, published October NATIONAL 2015 spending review offered local authorities the opportunity to increase council tax by 2% to contribute to the funding of social care. The NHS will receive a real-terms funding increase of 10bn between now and 2020/21 The latest planning guidance has been issued and introduces the requirement for a health economy-wide five year sustainability and transformation plan Boards have been asked to consider quality and finances on equal footing 1.8bn sustainability fund announced Lord Carter has written to the Secretary of State saying that the NHS will be able to generate 5bn of efficiency savings by 2020, if certain conditions are in place Additional arrangements have been put in place relating to agency costs A national Freedom to Speak up Guardian has been appointed A consultation on the Care Quality Commission s fee structure is open CCG leaders have called for the ban on mergers to be lifted The latest workforce data shows that district nursing has seen a fall. The majority of extra nurses have been employed by the acute sector. Health visitor numbers have increased nationally. Enc 02 INTER DEPENDENCIES: Legal and/or risk Clinical Financial None None None 2
31 HR Social care Patient & public involvement Staff and Trade Union involvement actions undertaken/ planned None None Patients, family members and carers inform the CEO of the details of their experience of receiving care during his visits to frontline services None Enc 02 Information exempt from disclosure Requirement for further review The report is a public document and available to members of the public via the Partnership Trust website None RECOMMENDATIONS / ACTION REQUIRED The Trust Board is asked to note the contents of the Chief Executive Officer s report. 3
32
33 Local We put quality first: we deliver quality and do the very best we can. Care Quality Commission We responded to the first deadline of the Care Quality Commission s warning notice on time. A steering group is meeting weekly to monitor the actions in our improvement plan, which is being delivered by the operational delivery group. The steering group escalates issues to the Executive Management Team, if necessary, following each meeting. Overall oversight is provided by the Quality Governance Committee. There is a lot to do before the final deadline of 29 th February, but progress is being made at pace. We have received draft inspection reports for Brighton House and the Living Independently Staffordshire teams in the North and South of the county. These are registered separately, as required by the CQC. We have until 25 th January to check for factual accuracy and they will be published on or shortly after 25th. Managing winter pressures At the beginning of December, the health and care economy hosted a press conference to explain to the people of North Staffordshire, how we would manage winter pressures. As expected, the two Bank Holiday weekends led to increased demand for health and care services. Our staff worked with University Hospitals North Midlands NHS Trust (UHNM), and neighbouring Acute Trusts, to identify people suitable for care at home, in line with our Home First philosophy. Our community teams also worked hard to maintain people in their own home. When the pressure at Royal Stoke Hospital became really great, we opened an additional ward at Cheadle Hospital. Despite everyone s best efforts, some patients at UHNM still experienced trolley waits. Celebrating sexual health services World Aids Day is marked every December and last month saw Leicester sexual health team up with Leicester City Council, local MPs and local voluntary sector organisations LASS and Trade to sign the Halve It pledge a national pledge committing Leicester, Leicestershire and Rutland to halve late HIV diagnoses by The month before was national HIV testing week and the Trust s sexual health teams offered free and confidential HIV testing in a variety of locations to residents of Stoke-on-Trent and North Staffordshire. An art exhibition titled HIV Unfolded was held at AirSpace Gallery in Hanley, with artists and local people sharing a snapshot of HIV from their perspective. Profiling pressure ulcers Since the last Board meeting, we have done a lot to raise the profile of pressure ulcers. Staff form the tissue viability team helped spread key prevention messages to patients and members of the public at Haywood Hospital as part of World Pressure Ulcer Day on 19 November. We have since launched our pressure ulcer campaign, React to Red. The Trust s tissue viability team offered advice and information about how to prevent pressure ulcers in their early stages at a series of drop-in sessions at Haywood Hospital on Thursday 17 December. Tissue viability specialists also went e on to wards to discuss with staff, patients and their carers and families, the signs and actions to be taken if you React to Red. Enc 02 4
34 Recognition for our physiotherapists At the end of November, members of the Trust s Integrated Physiotherapy and Pain Service (IPOPS) had the opportunity to share their expertise with 180 GPs from Coventry and Rugby CCG at an education workshop. Six Extended Scope Practitioners from the IPOPS team were invited to share their knowledge by Dr Ralph Mitchell. Last month, the same team was visited by the Chartered Society of Physiotherapy (CSP) and the European Senior Golf Tour. The service welcomed Steve Tolan, Head of Practice and Development at CSP and Orlaith Buckley, Consultant Physiotherapist at European Senior Golf Tour. Steve Tolan offered mentorship to the service s clinical leads Denise Softley and Paula Deacon during his visit to the Lichfield and Tamworth based team. Steve, who described IPOPS as the most famous musculoskeletal management service in the UK, looked at the clinical data that the team has collected over the last five years and discussed how they could share this information both nationally and internationally. In November, the Trust s Occupational Therapy service for children rolled out a training package on Developmental Coordination Disorder (DCD), designed for teaching staff and Special Educational Needs Coordinators in primary schools in Staffordshire and Stoke on Trent. The training afforded an important opportunity to develop and strengthen partnership working between health and educational services. It is anticipated that the strengthening of this partnership will enable better working and more effective outcomes for the children and families we work with. In October, the Trust welcomed four senior physiotherapists from Hong Kong who were selected by Hong Kong Health Authority to complete a training programme in the UK. The group of physiotherapists spent 10 days with Keele University and the Trust. During their time here, they had the opportunity to complete the Biopsychosocial Management of Complex Patients with Back Pain course with the Trust s Consultant Physiotherapist, Gail Sowden at Keele University. They also undertook an international learning package at Haywood Hospital and got the chance to shadow physiotherapists at various musculoskeletal (MSK) outpatient clinics across the Trust. This serves us well as we look to recruit more allied health professionals. Enc 02 We focus on people: we treat people as individuals and take time to respect and understand their point of view. Celebrating excellence awards The shortlisting has now taken place for our annual awards, the ceremony for which will take place on Friday 11 th March. There were 279 nominations across the 12 categories. Professor Ward retires Professor Anthony Ward, retired at the end of last month. For almost 30 years, he pioneered cutting edge rehabilitation medicine and training at our North Staffordshire Rehabilitation Centre, gaining international reputation for his expertise and research in the management of spasticity and in brain injury and stroke rehabilitation. Professor Ward founded the North Staffordshire Rehabilitation Centre in 1988 as the sole consultant in rehabilitation medicine in the West Midlands region and only the 5
35 seventh to be appointed in the country. The centre is now recognised as a pioneer for research, training, innovation and exemplar clinical service. Investing in our nurses We have always valued specialist practice and in recent years have encouraged community nursing staff to take the Specialist Practitioner Qualification (SPQ) course to enhance their skills. A recent study by the Queen s Nursing Institute highlights the value of the SPQ. The work, funded by the Department of Health, identifies key themes including direct benefits to patient care, personal and professional development, the benefit to employing organisations, and cost savings. We have supported 14 community nurses to completing the course so far and all are now in District Nursing Sister positions. These practitioners hold the NMC recordable qualification of a specialist practitioner which supports them in exercising higher levels of judgement, specialist knowledge and decision making in clinical practice. Their training could not have been achieved without the support and dedication of their Community Practice Educators and Community Practice Teachers who facilitate the learning in practice throughout the 12 month programme. Practice Educator Mentor awards Last year, Keele University School of Health and Rehabilitation launched their Practice Educator Mentor awards. Physiotherapy students had the opportunity to nominate a Practice Educator who they felt had been outstanding in their educator role in supporting student education and providing an exceptional physiotherapy placement experience. Four of these awards were given to physiotherapists from the Partnership Trust. Elizabeth Hallam Physiotherapist, Biddulph Primary Care Centre Janet Smith Physiotherapist, Community Respiratory Team, Greyfriars Therapy Centre Vanessa Clayton Physiotherapist, Longton Cottage Hospital Joseph Wright Physiotherapist, Bentilee Neighbourhood Centre Recognition for visual impairment Visual impairment rehabilitation officers from the Trust won a national award in recognition of their joined up working with Staffordshire Fire and Rescue Service to raise awareness of the difficulties people living with visual impairments experience on a daily basis. The NHS Collaboration award is given to the NHS Trust which has worked best with other public/private sector organisations to engage the local community in preventative campaigns. The collaborative working involves the rehabilitation team providing practical and interactive training to firefighters in Staffordshire to help build a greater understanding of how conditions such as blindness or partial sightedness affect a person s livelihood. Success of the Family Nurse Partnership programme Last month, more than a dozen young mums joined family nurses at Cannock Chase Children s Centre to celebrate their graduation from the Family Nurse Partnership programme. The Family Nurse Partnership provides a wide range of pre and postnatal support to first time mothers aged between 16 and 19, who access the service before week 29 of pregnancy. The family nurses provide weekly and fortnightly sessions which are one-to-one and tailored to the needs of the mother and child, until the child reaches the age of two. Enc 02 6
36 Together 4 Health We took advantage of the New Year to promote our healthy lifestyle service. The service is commissioned by public health at Staffordshire County Council and comprises services we used to provide such as Healthy Kid5 and Time to Quit. Social care transformation The joint transformation programme with Staffordshire County Council is progressing well. Strategic priorities have been identified and investment, both time and money, has been made in the actions identified for this financial year. The personalisation agenda continues to be seen as important with the recognition that service users show greater levels of satisfaction and reduced costs wherever direct payments are used. We have launched a staff engagement programme to raise the profile of independence as part of the social care transformation programme. Staff will be supported to focus on delivering creative solutions to promoting independence with service users. Service user and carer experience GOLD is awarded to North DESMOND Team For the completion of their monthly target sample of Service User and Carer experience surveys Achieving a Friends and Family Test score of 99% of respondents who would recommend the service SILVER is awarded to Sycamore Ward - Palliative Care For the completion of their monthly target sample of Service User and Carer experience surveys Achieving a Friends and Family Test score of 100% of respondents who would recommend the service BRONZE is awarded to Cannock LIS For the completion of their monthly target sample of Service User and Carer experience surveys Achieving a Friends and Family Test score of 100% of respondents who would recommend the service Enc 02 We take responsibility: we take personal ownership of things and see them through; we focus on finding solutions. Saying sorry when things go wrong Our patients, service users and carers can expect us to say sorry when things go wrong and harm is caused while in our care. The most common form of harm that occurs are falls and pressure ulcers. If harm is identified, the staff member involved in giving care and support will: Reduce any risk of further harm Give a verbal apology/acknowledgement of the harm to the patient and explain what has gone wrong Complete incident report including information on Duty of Candour Document discussion in medical records. 7
37 Within 10 days, the staff member must send a letter to the patient detailing the incident and explaining that an investigation is underway. An investigation will take place and written feedback is given to the patient and or relative/carer if the patient lacks capacity. Changes to health visiting Following a national change in commissioning arrangements, Stoke on Trent City Council and Staffordshire County Council now commission our health visiting service. In response to this, Staffordshire County Council issued a revised service specification, which requires us, as provider, to work within their boundaries. This will mean that families who are registered with a GP in Staffordshire but live in a different local authority will experience a change in health visitor. We are starting to receive records from neighbouring authorities, who are making the same change. The new model will allow us to focus resources where they are needed most, in areas of highest deprivation. It will also allow our health visitors to work with a defined community to develop local solutions to their needs. We are already working in this way in Stoke on Trent. Leading the way on integration Last month saw over 70 staff from health and social care gather together to start to plan a future model of integrated care. The event was jointly hosted by Jane Gaddum, Non-Executive Director at the Trust, Dr Chandra Kanneganti, from Goldenhill Medical Practice and Practice Manager, Linda Allen, from Millrise Medical Practice. It brought together community health services, patient representatives, and adult social care, with federations of GP practices and mental health to discuss a new model of care called a multi-specialist community provider (MSCP). The aim of multi-specialist community providers is to improve co-ordinated care, to provide care closer to home, and to reduce the number of unnecessary trips to hospital as a result. This is in line with the NHS Five Year Forward View, published in October last year. As part of this, five different models are being tested by 50 sites (called Vanguard sites) across the country. We are taking the learning from the national Vanguards and are hoping to set up four Early Implementer Sites within Staffordshire and Stoke on Trent, the first one to be established covers the North East (NEB) area of Stoke on Trent. Enc 02 National 2015 Spending Review A concise joint briefing has been produced by Health Foundation, The King's Fund and the Nuffield Trust. On care, its analysis is that new powers to raise Council Tax by up to 2 per cent to spend on social care will provide flexibility for local authorities but are unlikely to raise as much as the government suggests and could disadvantage deprived areas with low tax bases. It asserts that the additional funding will not be enough to close the social care funding gap which they estimate will be somewhere between 2 billion and 2.7 billion in 2019/20, depending on how much is raised through the Council Tax precept. Social care also faces additional cost pressures from implementing the National Living Wage which will add another 800 million to these estimates, leaving an estimated total funding gap of between 2.8 billion and 3.5 billion by the end of the parliament. Public spending on social care as a proportion of GDP will fall back to around 0.9 per cent by 2019/20, despite the ageing population and rising demand for services. 8
38 On health, the Spending Review announced that the NHS will receive a real-terms funding increase of 10 billion over the period from 2014/15 to 2020/21. It also announced that 6 billion of this funding would be front-loaded by 2016/17. The government argued that this delivers the 8 billion it had promised to fund the NHS five year forward view. The rest of the stated increase comprises additional funding for the current year announced in last year's Autumn Statement. Other inclusions: Bursaries for student nurses to be removed and replaced with student loans. Creation of up to 10,000 new nursing training places. More than 5bn for health research, including genomics and dementia. State pension to increase to per week next year. A new single tier pension payment of for new pensioners from next year An apprenticeship levy to raise 3bn a year, set at 0.5 per cent of the payroll bill but with a 15,000 allowance for employers to offset the levy. Planning guidance This year, we will be required to produce two plans: 1. A five year sustainability and transformation plan (STP), covering the period October 2016 to March 2021 subject to a formal assessment in July 2016 following submission in June This plan is being submitted by the pan-staffordshire transformation programme being led by Rita Symons. We have contributed the section on out of hospital care/long term conditions. 2. One year operational plans for 2016/17. These plans will need to be consistent with the emerging STP and in time to enable contract sign off by end of March The planning guidance articulates nine must do s for the year ahead: 1. Develop a high quality and agreed STP and subsequently deliver agreed milestones in 2016/17 2. Return the system to aggregate financial balance, including NHS providers engaging with Lord Carter s productivity work programme, and complying with agency rules, and CCGs delivering savings by tackling unwarranted variation in demand through implementing the RightCare programme in every locality 3. Developing and implementing a local plan to address the sustainability and quality of general practice including workforce and workload issues 4. Getting back on track with access standards for A&E and ambulance waits (95% patients wait no more than four hours in A&E and that ambulances respond to 75% of Category A calls within eight minutes) 5. Improvement and maintenance of NHS Constitution standards for referral to treatment (more than 92% patients on non emergency pathways wait no more than 18 weeks from referral to treatment) including offering patient choice 6. Deliver Constitutional standards on cancer care, including the 62 day cancer waiting standard and the constitutional two week and 31 day cancer standards, making progress in earlier diagnosis and improving one year survival rates 7. Achieve and maintain the two new mental health access standards (more than 50% people experiencing a first episode of psychosis will commence treatment with a NICE approved package within two weeks of referral; 75% referrals to IAPT will be treated within six weeks and 95% within 18 weeks). Continue to meet dementia diagnosis targets Enc 02 9
39 Enc Deliver actions in local plans to transform care for people with learning disabilities including enhanced community provision, reducing inpatient capacity and rolling out care and treatment reviews 9. Develop and implement an affordable plan to make improvements in quality particularly for organisations in special measures. In addition providers are required to participate in the annual publication of avoidable mortality rates by individual trust. Boards asked to consider quality and finances on equal footing A joint letter from Jim Mackey and Professor Sir Mike Richards to all trust boards, asks them to consider quality and finances on equal footing in their planning decisions. This highlights that in due course Monitor, together with CQC and NHS England, will be publishing revised National Quality Board staffing guidance and a new metric looking at care hours per patient day, as part of CQC s new assessment on the use of resources. Further details on this will be published in the coming months. Our share of the 1.8bn sustainability fund We have received notification that we will be getting a share of this fund. This funding will be dependent on having: A recovery plan with NHS Improvement and agreed control total for 2016/17 including capital and revenue limits A plan for maintaining agreed performance trajectories for delivering quality and access standards Development of sustainability and transformation plans, including adherence to the planning timetable Compliance with all staff agency rules Tangible progress towards achieving seven-day services. Preliminary recommendations from Lord Carter s review in to operational productivity This will be published at the end of this month or early February. In the meantime he has written to the Secretary of State and in this letter he reemphasises that the NHS will be able to generate 5bn of efficiency savings by the end of the parliament, but only with: a. A single reporting framework is adopted for all trusts based on benchmarked best practice, which in turn will also reduce and rationalise the data reporting burden currently placed on providers by commissioners and regulators b. Support for addressing delayed transfers for care, which is leading to suboptimal use of clinical resources c. National support and coverage to help providers unlock the productivity improvements linked to redesigning clinical services, to enable rapid adoption and implementation by providers of the review s recommendations d. Substantial improvements in workforce productivity. A 1% improvement in workforce productivity could represent around 400m in savings. Additional arrangements from NHS Improvement to tackle agency costs A letter from NHS Improvement sets out: 10
40 Enc 02 a. The plan to lower the agency price caps for medical and clinical staff on 1 Feb has been restated. b. The ban on using agency frameworks not approved by NHS Improvement will be extended to all staff groups from 1 April. Currently, it only applies to nursing staff. c. NHS Improvement has recognised that framework suppliers renegotiations or retenderings with agencies will extend beyond 1 Apr. In the meantime, suppliers must strongly support the price caps. d. NHS Improvement will in time move towards expressing price caps in a way that defines the amount the worker receives equivalent to standard NHS t&c and agencies will bid to be on-framework on the basis of their agency fees. e. NHSI will also take steps to stop agency workers using personal services companies to avoid taxes. f. A requirement on providers to use e-rostering National guardian for freedom to speak up appointed The Care Quality Commission has appointed Dame Eileen Sills DBE, chief nurse at Guy s and St Thomas NHS Foundation Trust, as its first national guardian for the freedom to speak up safely in the NHS. Dame Eileen, whose post will be independent, will work in partnership with the CQC, NHS England and NHS Improvement to help in leading a cultural change, initially within NHS foundation trusts and trusts, with the aim of ensuring that healthcare staff always feel confident and supported to raise concerns about patient care. Dame Eileen will provide advice and support to a network of individuals within foundation trusts and trusts appointed as local freedom to speak up guardians. Helené Donnelly is our freedom to speak up guardian. Helené is soon to go on maternity leave and an internal secondment is being offered to cover the period of her leave. Bringing the Care Quality Commission's comprehensive inspections within scope of its fee raising power The Department of Health is consulting on a proposal to extend the CQC s fee raising power to cover all aspects of its comprehensive inspection programme. Its budget is to be cut by 25% over the next four years. Its overall budget is set to fall by 13%, with the cut in its government funding balanced by an increase in the fees the CQC charges to those it regulates. Currently, the CQC s fees may only cover those activities which relate to assessing whether providers are compliant with registration requirements. The CQC's new comprehensive inspections consider the quality of care above and beyond the registration requirements, highlighting good and outstanding care. The inspections therefore go beyond the scope of the CQC s fee setting power. In a separate consultation, the CQC is asking whether it should move to a position of full cost recovery over two years or four years. In order to proceed with the plans to move to full cost recovery, the Department of Health must introduce these regulations to allow the CQC to charge fees for its full inspection programme. CCG leaders call for merger ban to be lifted A survey by HSJ revealed that more than half of clinical commissioning group leaders would like NHS England to lift its informal ban on CCGs merging. Forty-six leaders took part in the latest HSJ CCG Barometer. Fifty-nine per cent said they believed NHS England should lift its informal ban on CCG mergers, however more than half said mergers were unlikely to take place by Respondents were given possible options for how CCG responsibilities might shift by April 2017 and were asked to rate how likely these were. Almost 60% said it was likely or very likely that their responsibilities would be transferred to a provider or groups of providers, while 11
41 45% said sharing responsibilities and budgets with local government under devolution arrangements was likely or very likely, and 59% said sharing budgets and responsibilities across groups of CCGs would take place. NHS England has not formally banned CCG mergers, but chief executive Simon Stevens has indicated he does not want any more to take place. National district nurse reductions According to the latest workforce data, the NHS is continuing to recruit record levels of qualified nursing staff, although some groups such as district nursing have seen double digit falls. Workforce data published by the Health and Social Care Information Centre reveals the number of full-time qualified nursing, midwifery and health visiting staff employed in the NHS in September 2015 rose to 317,023 almost 2,300 more than in August. In September 2015, 3,508 more nursing staff were employed in the NHS compared to September 2014, with majority of the extra staff being employed in the acute sector. While community services saw an increase of 1,405 staff, this was largely in health visitors, which increased by 1,210. The Royal College of Nursing has shown there are more than 10,000 vacancies for nursing posts in London. The shortage of nurses worsened last year, with 17% of all London's registered nursing jobs vacant, up from 14% in 2014 and 11% in The figure is much higher than the national average of 10%. Enc 02 12
42
43 Enc 03i REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD MEETING TO BE HELD ON: WEDNESDAY 27 JANUARY 2016 Enclosure: 03 Subject: Assurance Report of the Chair of the Quality Governance Committee Strategic Goal (tick as appropriate): x x We will provide high quality and safe services which provide an excellent experience and best possible outcomes We will work with users and carers to deliver integrated services, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Director Lead: Melanie Print, Company Secretary Recommendation: For Approval & Assurance x For Discussion For Information PURPOSE OF THE REPORT: To receive an assurance report from the Chair of the Quality Governance Committee as to the matters and business of the meeting of the Committee of the 13 January 2016 referred to the Board for its consideration and action (as required). KEY POINTS: Items of Business for Review by the Trust Board The following matters are referred to the Trust Board, following the meeting of the Committee on the 13 January 2016, for its consideration and action as required: The Committee reviewed the report into the procedures and control processes that have been implemented to manage the unallocated cases in social care, noting that the waiting list for allocation has improved and performance increased; Team Leaders have oversight of the allocation of high priority cases; and the Divisional Business Meetings will now review the improvement plans put in place to reduce the waiting list, any related incidents and the impact on the care and assessment of the service user as a consequence of any incident. The Committee has recommended that the continued delays in implementing a fix to Care Director so as to enable Social Workers and Social Care Assessors to effectively and efficiently manage social care allocations Teams have had to revert to a paper based system are escalated by the Director of Operations to the next Cabinet to Trust Board meeting. They commended the Chief Operating Officer Social Care on her report and the Page 1 of 3
44 improvements that have been made in reducing the waiting list for social care allocations. Enc 03i The Committee ratified a number of key policies and changes to the training of staff which underpin the Partnership Trust s response to the CQC Warning Notice and the embedding of best practice. The Committee recommended that the Director of Workforce & Development secure that the Duty of Candour training is mandated as mandatory for Nursing, Clinical and other relevant staff and that a report is made to the Board to that effect. This is an agenda item for the meeting of the Board. The Committee has direct oversight of the actions and steps that are being taken to secure the required improvements sought by the Care Quality Commission. The Committee has directed that if additional investment is required so as to secure that the training and development of staff, in relation to the Duty of Candour and the Mental Capacity Act, is undertaken promptly and effectively, then this investment must be made. The Committee deferred consideration of the Healthcheck Assurance Report; it is to be presented by the Director of Operations to the next meeting of the Committee in February with confirmation as to how the risks and actions referred to in the Team Plans are escalated and referenced within the governance framework of the Partnership Trust, together with a timeline as to when the early warning system is to be implemented. The Committee reviewed the Transfer of Patients and Service Users Policy; it has approved this Policy as a time limited working draft so that its application can be tested. Changes are to be made so as to ensure that this Policy is linked to the Discharge Policy; the Hospitals Full Policy and the admissions (to Community Hospitals) criteria. The Committee has directed that this work is undertaken by the Director of Operations with the support of the Interim Director of Nursing & Quality and the Medical Director. The Committee has emphasized that the changes to the policy are worked up from a ward level and patient experience context and tested with staff who receive and transfer patients. A further assurance report is to be made by the Director of Operations to the meeting of the Committee is March. The Committee directed that the risks highlighted in the Health & Safety Quarterly Report are reported to the Executive Risk Management Committee by the Director of Operations so that this Committee can review the impact on staff and services. The Committee welcomed the first iteration of the new Quality Dashboard; it will provide improved oversight and quality assurance of the services and quality indicators of the Partnership Trust; improving the governance of quality and performance in a more streamlined and succinct manner. This work is linked to the changes to the reporting and supporting governance of the Committee which will be made in this quarter and which are aligned to the Well Led Framework work. INTER DEPENDENCIES: Legal and/or Risk Clinical Financial HR Regulatory and reputational risk as a consequence of the issue of a warning notice by the Care Quality Commission. The Committee has an oversight function in relation to the actions taken to address the required improvements referenced in the warning notice. Clinical risks are highlighted in the Safety & Effectiveness report. None at this time. None at this time. Page 2 of 3
45 Enc 03i Social Care Staff and Trade Union involvement actions undertaken/planned Patient & Public Involvement Equality Impact Information exempt from Disclosure Requirement for further review The functionality of Care Director is impacting on the efficiency and effectiveness of Social Workers and Social Care Assessors. Staff have been kept appraised of the changes to services. The experience of Patients and Services Users and their families is considered in the experience and effectiveness reports to the Committee. The Committee has directed that an equality impact assessment is referenced in the Transfers Policy with regards to what actions are required to mitigate the risks of transfers into and from our care. None at this time. None at this time. RECOMMENDATIONS: The Trust Board is recommended to receive the assurance report of the Chair of the Quality Governance Committee into the matters and business arising from the meeting of the Committee on the 13 January 2016 and to consider whether any further action is required to address the matters highlighted in the key points above. Page 3 of 3
46
47 Enc 03ii REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD MEETING TO BE HELD ON: WEDNESDAY 27 JANUARY 2016 Enclosure: Subject: Strategic Goal (tick as appropriate): Director Lead: 03ii Assurance of Report of the Chair of the Audit Committee X X We will provide high quality and safe services which provide an excellent experience and best possible outcomes We will work with users and carers to deliver integrated services, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Melanie Print, Company Secretary Recommendation: For Approval & Assurance X For Discussion For Information PURPOSE OF THE REPORT: To receive an assurance report from the Chair of the Audit Committee in relation to the matters and business of the meeting of the Committee of the 15 January 2016 referred to the Board for its review and action. KEY POINTS: Items of Business for Review by the Trust Board The following matters are referred to the Trust Board, following the meeting of the Committee on the 15 January 2016, for its consideration and required action as appropriate: The Committee has directed that the actions arising from the Internal Auditors limited assurance report into financial management and CIP arrangements are the subject of a formal assurance report to the March meeting of the Committee, so that it can be confident that the culture of delivery of CIP has been embedded into the cycle of Cost Improvement Plans for 2016/17. The Committee reviewed all outstanding actions arising from Internal Audit reports and expressed its concern that a number of outstanding actions, ranked with a high risk rating, have not been responded to. The Committee has recommended that the Director of Finance & Resources reports their concerns to the Chief Executive Officer as the Accountable Officer of the Partnership Trust. It is the Committee s expectation that a closure report will be made to it confirming what action has been taken to secure that Page 1 of 3
48 Enc 03ii Internal Audit recommendations are closed down on time, particularly those actions which are allocated a high risk score. The Committee welcomed the significant assurance that has been provided by the Internal Auditors into the Financial Systems of the Partnership Trust. It has recommended that the risks highlighted in relation to overpayments to staff are addressed by the Workforce Matters Committee and that an assurance report is made by the Chair of that Committee to the next meeting of the Audit Committee confirming what steps have been taken to minimise overpayments and to secure recovery of the same, having regard to the volume and value of overpayments made. The Committee reviewed the limited assurances that had been made by the Internal Auditors into the internal audit of Care Director (Client Income). It noted that the actions to secure that full assurance can be applied to this function of Care Director, and the efficient management of Client Income will be monitored through the Social Care Transformation Programme; performance against this Programme is reported by the Director of Operations to the Finance Investment & Performance Committee. The Committee reiterated its expectation that actions arising from limited assurance reports are completed as a matter of priority. The Committee reviewed the Board Assurance Framework (Quarter 3 review), focussing on those assurances which underpin the response to the CQC Warning Notice. It recommended that those assurances which are the subject of low confidence ratings are formally referred to the sponsor Committees with a direction that the relevant Committee reviews the assurances and the actions taken to improve the confidence rating; a separate report is to be provided by the Chair and lead Executive Director of each Committee to the next convenient meeting of the Audit Committee. INTER DEPENDENCIES: Legal and/or Risk Clinical Financial HR Social Care Staff and Trade Union involvement actions undertaken/planned Patient & Public Involvement Equality Impact Information exempt from Disclosure Requirement for further review Regulatory and reputational risk as a consequence of the issue of a warning notice by the Care Quality Commission. The Committee has an oversight function in relation to the actions taken to address the required improvements referenced in the warning notice. Service risks are a subset of the CQC Warning Notice. These are monitored through the CQC Steering Group. The risks to CIP delivery as highlighted in the limited assurance internal audit report are monitored by the Audit Committee and Board. None at this time. The actions taken to mitigate the limited assurance applied to the audit of Care Director is being managed through the Social Care Transformation Programme. None at this time. None at present. None at present. None The implementation of the actions arising from the internal audit into financial management and CIP will be reviewed at the Audit Committee in March 2016 Page 2 of 3
49 Enc 03ii RECOMMENDATIONS: The Trust Board is recommended to receive the assurance report of the Chair of the Audit Committee into the matters and business arising from the meeting of the Committee of the 15 January 2016 and to consider whether any further action is required to address the matters highlighted in the key points above. Page 3 of 3
50
51 Enc 03 REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD MEETING TO BE HELD ON: WEDNESDAY 27 th JANUARY 2016 Enclosure: Enc 03 Subject: Strategic Goal (tick as appropriate): Director Lead: Assurance Report of the Chair of the Workforce Matters Committee x x x x We will provide high quality and safe services which provide an excellent experience and best possible outcomes We will work with users and carers to deliver integrated services, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Andrew Talbot Non Executive Director/Julie Tanner Director of Workforce & Developoment Recommendation: For Approval & Assurance x For Discussion For Information PURPOSE OF THE REPORT: To receive an assurance report from the Chair of the Workforce Matters Committee in relation to the matters and business of the meeting of the Committee on the 2 nd December KEY POINTS: Items of Business for Review by the Trust Board The following matters are referred to the Trust Board, following the meeting of the Committee on the 2 nd December 2015, for its consideration and required action as appropriate. Equality Impact Assessments The Equality and Inclusion Manager raised an issue relating to the inconsistency of policies within the Trust not having a robust Equality Impact assessment completed on production of new policies or the review of current versions. There is a legal requirement on us as an organisation to ensure that this process is carried out. The Equality and Inclusion Manager confirmed that there was work commencing with the Corporate Governance Lead to ensure that a new process was put in place to ensure compliance. The E& I Page 1 of 3
52 Enc 03 Manager was also going to draft a set of questions which this committee could use to test the robustness of future EIA on workforce polices brought to the committee. Recruitment Process The Associate Director of Human Resources advised that from the original 65 action points on the SBS Recruitment Action Plan, 38 have been closed and 27 remain in progress. Assurance was given that the remaining 27 actions should be closed by the end of December 2015 then the intention is to give SBS an improvement period until the end of March 2016 to reach the KPI of 14 weeks advert to fill time. The Trust also needs to make improvements at the front end of the process with the approval of vacancies and turn round of actions. An exception sheet has been compiled by SBS which will go to the AD for Human Resources to indicate where there are blockages in the system attributed to Trust Managers so that these can be followed up. As District Nursing and Community Hospitals Nursing staff is a high risk and needs a fast turnaround these roles have been taken out of the SBS process for the time being and being dealt with by a temporary internal recruitment team. It was reported that there were concerns about the quality of the data being produced from the Stepchange System administered by NHS SBS. However, a workshop had been arranged for early January with key people attending where this will be resolved and an agreed suite of reports identified. These reports would be reviewed at the next meeting of this committee. Previously, all calls to SBS Recruitment were being received at a general helpdesk by staff with very little knowledge of recruitment processes. SBS have worked with their staff and now have recruitment specialists answering calls who have detailed knowledge and can answer queries in a more timely manner. Feedback is showing that this seems to be working much better but will continue to be reviewed via the Welcome Day Feedback Sheets. Central Bank Team (renamed to Temporary Staffing Bureau - TSB) It was reported that this newly established team had made considerable progress with recruiting suitable people to the Trust internal bank arrangements. They had in the last 6 months doubled the number of people available and were starting to build capacity across nearly all staff groups. They were reporting on average an 80% fill rate across all requests. In addition this team had taken on the role of co-ordinating all agency reuests and ensuring that wherever possible, where bank was not available, bookings were within the tolerances set by the Trust Development Authority/Monitor of on framework and below the financial cap. In addition the team are co-ordinating the weekly return to the TDA on non-compliance with these requirements. Plans for the implementation of a neutral vendor arrangement to co-ordinate better access to approved agencies and to provide more detailed management information was on trajectory for going live before the end of the financial year. INTER DEPENDENCIES: Legal and/or Risk Clinical Financial HR Social Care Inefficient recruitment processes can lead to patient safety risks and Trust reputational risk. None None None None Page 2 of 3
53 Enc 03 Staff and Trade Union involvement actions undertaken/planned Patient & Public Involvement Equality Impact Information exempt from Disclosure Requirement for further review Staff side are members of the Workforce Matters Committee. None None None Recruitment processes under regular scrutiny by Executive Management Team and Workforce Information and Planning Committee. RECOMMENDATIONS: The Trust Board is recommended to receive the assurance report of the Chair of the Workforce Matters Committee into the matters and business arising from the meeting of the Committee on the 2 nd December 2015 and to consider whether any further action is required to address the matters highlighted in the key points above Page 3 of 3
54
55 Enc 03iv REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD MEETING TO BE HELD ON: WEDNESDAY 27 JANUARY 2016 Enclosure: Subject: Strategic Goal (tick as appropriate): Director Lead: 03iv Assurance of Report of the Chair of the Finance Investment & Performance Committee X X We will provide high quality and safe services which provide an excellent experience and best possible outcomes We will work with users and carers to deliver integrated services, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Melanie Print, Company Secretary Recommendation: For Approval & Assurance X For Discussion For Information PURPOSE OF THE REPORT: To receive an assurance report from the Chair of the Finance Investment & Performance Committee in relation to the matters and business of the meeting of the Committee of the 21 January 2016 referred to the Board for its review and action. KEY POINTS: Items of Business for Review by the Trust Board The following matters are referred to the Trust Board, following the meeting of the Committee on the 21 January 2016, for its consideration and required action as appropriate. The Committee took some time to consider the Finance Report for Month 9, the Financial Outlook for 2016/17 and the financial assumptions that underpin the proposed control total of a (net) 2.1M deficit. The Committee recommends to the Board the following proposals to support the Trust s operational plan for 2016/17 under the terms of the Sustainability and Transformation Plan: A CIP of 4% for 2016/17, the full plans for which will be reported to the Board at its February meeting; Break even in Adult Social Care; Revised planning assumptions to support an overall break/even position; and A reduction / review of loss making services consistent with the Core Services Strategy which is to be approved by the Board. Page 1 of 2
56 Enc 03iv INTER DEPENDENCIES: Legal and/or Risk Clinical Financial HR Social Care Staff and Trade Union involvement actions undertaken/planned Patient & Public Involvement Equality Impact Information exempt from Disclosure Requirement for further review A failure to meet the control total reported by the TDA will put the Trust at risk of breaching its statutory duty to break even. The Core Service Strategy, of which the clinical strategy will be a component part, will assist the Board in agreeing the financial and service assumptions which underpin achievement of the control total. The financial assumptions that underpin the financial outlook for 2016/17 are to be agreed by the Board. The governance and delivery of CIP is being improved to address the limited assurances reported to the Audit Committee. None at this time. The renegotiation of the Section 75 Adult Social Care quantum and outcomes of the Section 75 Agreement are integral to the delivery of the control total for the Trust. None at this time. None at present. None at present. None The CIP Programme for 2016/17 will be presented to the Board in February. RECOMMENDATIONS: The Trust Board is recommended to receive the assurance report of the Chair of the Finance Investment & Performance Committee and to endorse the proposal referred to in the key points above. Page 2 of 2
57 Enc 04 REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD MEETING TO BE HELD ON: 27 JANUARY 2016 Enclosure: 04 Subject: Strategic Goal (tick as appropriate): Director Lead: Corporate Risk Register We will provide high quality and safe services which provide an excellent experience and best possible outcomes We will work with users and carers to deliver integrated services, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Rose Goodwin Interim Director of Nursing and Quality Recommendation: For Approval & Assurance X For Discussion For Information PURPOSE OF THE REPORT: The Corporate Risk Register is appended to this Report for review and note of the changes that have taken placed through the Executive Risk Management Committee at its meetings on 14 December 2015 and 18 January The Board is asked to take assurance that the reported risks are the subject of risk controls and actions to mitigate the residual risk reported on the Register. KEY POINTS: Corporate Risk Register The Risk Register has been reviewed and the following changes have been made at the Executive Risk Management Committee. December 2015: Risk Register discussed and agreed. One risk identified for de-escalation: o Risk Ref 13 ~ sustainable plan for service delivery 2015/16 January 2016: Two new risks discussed and agreed for inclusion on the Corporate Risk Register: o Risk Ref 608 ~ risk staff not fully competent and applying the principles of Mental Capacity Act in practice o Risk Ref 625 ~ non-compliance issues identified by Care Quality Commission which, Page 1 of 2
58 Enc 04 if not addressed, could result in possible enforcement action Risk Register Review Presentations: The Committee signed off the following reviewed risk registers at the December 2015 and January 2016 meetings: o Nursing & Quality Directorate o Finance Directorate o Workforce Directorate o Specialised Services Division INTER DEPENDENCIES: Legal and/or Risk An effective Risk Management Strategy linked to the Board Assurance Framework and the Corporate Risk Register will mitigate risks the organisation s Strategic Objectives and provides assurance that risks are being managed. Clinical Financial HR Social Care Staff and Trade Union involvement actions undertaken/planned Patient & Public Involvement Equality Impact Information exempt from Disclosure Requirement for further review RECOMMENDATIONS: Those risks which are clinical are assigned to the relevant Directorate for mitigation with updates through the governance of the Quality Governance Committee. Financial risks or risk with financial implications are escalated onto the corporate risk register No HR risks are reported in this month s Corporate Risk Register. The impact of the evolution of the integration is the subject of ongoing review by the Executive Risk Management Committee. Staff and trade union involvement is through either Committee (eg workforce and health and safety) as risk are escalated/de-escalated or through local discussions within Divisions. We are engaging with those patients and their families who are affected by decisions to decommission services. The impact on services which are decommissioned is assessed by the CCGs None The Corporate Risk Register is reviewed monthly. The Trust Board is recommended to: Note the updated version of the Corporate Risk Register appended to this Report; Note the actions that are being taken to manage the reported risks. Page 2 of 2
59 Risk Register - Corporate Risks Number CQC Domain Strategic Objective Division, Direcotrate, Department Added to Register Review Cycle and Last Updated Description of Risk Cause Effect Impact Initial Impact Initial Likelihood Initial Risk Rating Details of Risk Control Actions Planned Action Progress Current Impact Current Likelihood Residual Rating Lead Officer Lead Manager Lead Director Target Impact Target Likelihood Target Risk Rating Risk Proximty 01 Corporate Operations Directorate Responsive Safe SG2 01/08/2012 Monthy 11/01/2016 Insufficient standard domiciliary care and enhanced domiciliary care packages. It should be noted that this is predominantly a risk in the North. Cause: Qualified staff (Band 5 and above) inappropriately delivering care that could be provided by non-qualified staff (Band 2 or 3) Effect: Referrals of unmet need back to community services Impact: Additional impact on the capacity of community services. Delays to discharge from acute and community inpatient wards. Concerns about compromise to patient safety Social Care Transformation Programme has work streams in place to control the risk Continue to monitor and review actions set out in the Social Care Transformation plan Monitoring has continued throughout the previous month. Non-availability of Dom Care has been the biggest single factor impacting on patient flow Date Entered : 14/01/ :18 Director Of Operations Director Of Operations Director Of Operations 3-6 Months 02 Corporate Operations Directorate Safe SG5 01/10/2013 Monthy 11/01/2016 (PMO Work stream - Social Care Transformation Programme) Risk of delayed social care assessments and service provisions as a result of the issues/problems experienced with the implementation and ongoing use of Care Director and associated loss of income. Cause: Care Director as a system is reported as difficult/cumbersome to use by staff, issues with IM&T connectivity Effect: Staff capacity reduced due to loss of productivity whilst using the new system. Impact: Under recovery of income (PMO Work stream - Social Care Transformation Programme) Action plan agreed to address issues with the way the system is working. Additional capacity secured to support Social Care staff Monitor impact of actions implemented for one month then review with view to possibly reducing the residual risk score. Jan 16: Report to Quality Governance Committee 13/01/2016 illustrates improvement. Issues remain in relation to Care Director. Teams are utilising manual recording where necessary. User group established to identify business process changes Change control group established Specific controls have been included in the transformation programme Jan 16: Continue with transformation plan actions including revision of Care Director. The next up-grade for Care Director will be actioned by 2017 and although we have a range of activities in train to improve inputting the system changes will not have the required impact until next year. We have a number of meetings in place to review and improve our performance but this is dependent on some extra admin staff inputting Service Provisions etc. Director Of Operations Director Of Operations Director Of Operations 0-3 Months Date Entered : 14/01/ :24 Date Printed: 21/01/2016 Page 1 of 8
60 Risk Register - Corporate Risks Number CQC Domain Strategic Objective Division, Direcotrate, Department Added to Register Review Cycle and Last Updated Description of Risk Cause Effect Impact Initial Impact Initial Likelihood Initial Risk Rating Details of Risk Control Actions Planned Action Progress Current Impact Current Likelihood Residual Rating Lead Officer Lead Manager Lead Director Target Impact Target Likelihood Target Risk Rating Risk Proximty 03 Corporate Operations Directorate Safe Effective SG2 01/04/2014 Monthy 11/01/2016 Medium term risk for the Trust based on the re commissioning plans of the County Council for Domiciliary Care provision and the decision to extend the existing arrangements. Co-dependency with Risk 1. Cause: Not within the control of SSOTP - commissioning led by the County Council Effect: No change/improvements to provision - for a 12 month period from April 15-March 16. Impact: No change or enhancements to current service provision from third party providers Task and finish group to review the effectiveness of the current frameworks and the capacity of the Dom Care market place to respond to current demand and enhanced packages of care. Task and finish group reports into the Social Care Transformation Programme who forecast future activity so that a new service can be commissioned. Monitor impact of actions taken for one month with a view to possibly reducing residual risk score. Jan 16: Continue to monitor and review actions set out in Social Care Transformation Plan Monitoring has continued throughout the previous month. Non-availability of Dom Care has been the biggest single factor impacting on patient flow Date Entered : 14/01/ : Director Of Operations Director Of Operations Chief Executive Officer 6-9 Months Proposals have been presented to SCC and the Trust. 04A Effective Safe SG2 Corporate Operations Directorate 01/10/2014 Monthy 11/01/2016 Risks to level (capacity) of service provision in the District Nursing service - North Division Cause: Inability to recruit staff to vacancies funded by Commissioners. Effect: High pressure on services. Impact on Day and Night provision as care carried across where visits have not been achieved. Impact: Concerns about safety and quality of care. Low morale amongst staff. (PMO Work stream - Workforce) Workforce Planning Toolkit. Safer Staffing implementation programme. To continue to monitor over Stoke Longton team have a band 6 in place, reviewed need to have more people in clinics, new starter in next 4 weeks Commissioning Intentions for 15/16 - service specifications for district nursing which will inform the strategic approach by SSOTP to provision and staffing the coming months to ensure that recruitment exceeds the numbers of staff leaving the service. To reduce residual score once staffing levels sustained. Porthill and Chesterton have appointed a permanent band 6 and work started to put in place new team Date Entered : 14/01/ :26 Chief Operating Officer (North) Director Of Operations Director Of Operations 0-3 Months Safer Staffing dashboards and monitoring. Date Printed: 21/01/2016 Page 2 of 8
61 Risk Register - Corporate Risks Number CQC Domain Strategic Objective Division, Direcotrate, Department Added to Register Review Cycle and Last Updated Description of Risk Cause Effect Impact Initial Impact Initial Likelihood Initial Risk Rating Details of Risk Control Actions Planned Action Progress Current Impact Current Likelihood Residual Rating Lead Officer Lead Manager Lead Director Target Impact Target Likelihood Target Risk Rating Risk Proximty 04B Effective Safe SG2 South Division Operations Directorate 01/10/2014 Monthy 11/01/2016 Risks to level (capacity) of service provision in the District Nursing service - South Division Cause: Changes in the commissioning arrangements for the community nursing workforce. Staff turnover and sickness. Underfunding of services by Commissioners. Effect: High pressure on services. Impact on Day and Night provision as care carried across where visits have not been achieved. Impact: Concerns about safety and quality of care. Low morale amongst staff. Impact on a large number of patients. (PMO Work stream - Workforce) Workforce Planning Toolkit. Safer Staffing implementation programme. Impact of actions implemented to be monitored over the coming month to ensure effectiveness and then review residual risk score with Cannock - DN issues in a view to possible reduction. Commissioning Intentions for 15/16 - service specifications for district nursing which will inform the strategic approach by SSOTP to provision and staffing Safer Staffing dashboards and monitoring. Some areas have achieved staffing levels and skill mix in line with WPT. All red and red+ teams have buddy system in place. Cannock reducing - Hednesford resolved - Great Wyrley easing as vacancies filled - Rugeley Still staffing pressures due to staff sickness. East - Day time teams have minimal vacancies remaining, Main challenge remains OOHs due to the size of the team. Stafford - ILCT 2 - Risk reduced to 9 as a residual risk, as staffing levels are improving, bank is being used to support ongoing vacancies. Lichfield/Tamworth - Risk remains unchanged. Agency nurses continue to support the area and are moved to support the need as indicated. Vacancies now recruited to and continue to go through recruitment checks Seisdon CIS - Risk 313 on the divisional plan - Budget remains overspent and is now an unsustainable cost pressure. Reorganisation of boundaries is planned by the end of January which will further streamline pathways and increase efficiencies, however this will again reduce the overall team size as establishment is adjusted in line with geographical areas. Chief Operating Officer - South Director Of Operations Director Of Operations 0-3 Months Date Entered : 21/01/ :25 Date Printed: 21/01/2016 Page 3 of 8
62 Risk Register - Corporate Risks Number CQC Domain Strategic Objective Division, Direcotrate, Department Added to Register Review Cycle and Last Updated Description of Risk Cause Effect Impact Initial Impact Initial Likelihood Initial Risk Rating Details of Risk Control Actions Planned Action Progress Current Impact Current Likelihood Residual Rating Lead Officer Lead Manager Lead Director Target Impact Target Likelihood Target Risk Rating Risk Proximty 06 Corporate Workforce Directorate Workforce & Development Direct Safe SG2 07 Corporate Workforce Directorate Workforce & Development Direct Safe Effective SG2 11/11/ /11/2014 Monthy 06/01/2016 Monthy 06/01/2016 Inability to sustain staffing levels in the Trust due to turnover of staff. Cause: Increased turnover of staff - with particular focus on district nursing and ward based nursing staff. Effect: Increased number of vacancies and/or skills gaps within operational teams. Low staff morale. Impact: Compromise to patient care and safety, less able to deliver to contract specifications. Breach of contract delivery - penalties/fines. Staff support systems compromised, e.g. appraisals. (PMO Work stream - Workforce) Risk to operational delivery as vacancies are not filled in a timely manner. Cause: Slow process means that the time to recruit new members of staff into the organisation has elongated. Effect: Vacancy gaps within teams. Impact: Services working with a reduced workforce for longer than they would ordinarily do so impacting on morale and quality of care. Increased agency spend as the staffing shortfall is managed in the short term. (PMO Work stream - Workforce) Regular monitoring through EMT and Workforce Matters Committee Information obtained through New process has been Wellbeing and Engagement Group - has been on hold until new Deputy to Director of Workforce in post. New Deputy to Director of Workforce to commence in post., All vacancies notified to Director of Workforce to rapidly identify trends. the new exit interview process is to be collated and sorted by Division, themes etc. A report will be prepared and presented to the Workforce Matters Committee in February 2016 launched and feedback will be provided to Workforce Matters Committee at the end of February 2016 Date Entered : 19/01/ : Workforce Matters Three month monitoring There is currently a 3 month SBS contract including KPIs Detailed Divisional/Directorate reports to enable performance management. Activity reports from SBS Monthly employment services board meeting to review progress against KPIs, weekly operational calls. period to commence following implementation of all improvement measures (end of December 2015) monitoring period in operation that is due for completion end of March Fill rate is currently 18 weeks with a target fill rate of 14 weeks to be achieved by the end of March 2016 Date Entered : 19/01/ :33 Associate Director Of Training & Transformation Associate Director Of Human Resources Director Of Workforce & Development Director Of Workforce & Development Director Of Workforce And Deve Director Of Workforce And Deve 0-3 Months 3-6 Months Improvement Work stream: Director Led Project Group and Project Plan New Deputy to Director of Workforce to commence in post., All vacancies notified to Director of Workforce to rapidly identify trends. Weekly conference calls to internal Recruitment Team Date Printed: 21/01/2016 Page 4 of 8
63 Risk Register - Corporate Risks Number CQC Domain Strategic Objective Division, Direcotrate, Department Added to Register Review Cycle and Last Updated Description of Risk Cause Effect Impact Initial Impact Initial Likelihood Initial Risk Rating Details of Risk Control Actions Planned Action Progress Current Impact Current Likelihood Residual Rating Lead Officer Lead Manager Lead Director Target Impact Target Likelihood Target Risk Rating Risk Proximty 09 Corporate Transformation Directorate Financial Management Well-Led SG5 11 Corporate Operations Directorate Responsive SG2 01/01/ /02/2015 Monthy 13/01/2016 Monthy 11/01/2016 Risk of non-delivery of the CIP Target for 15/16. Target for health set at a minimum of 13.7 million (approx. 6% of Trust health budget). In year risk. Cause: Insufficient programmes identified to deliver the full CIP target. In addition failure of CIP programmes to deliver against the targets identified Effect: Trust will be in a position of overspend. Impact: Failure to deliver will mean that the Trust is unable to deliver a breakeven at year end. (PMO Work stream - CIP) Potential delay to implement findings and potential solutions of the Toolkit for AHP's Cause: Inability (capacity and skills gap) of some operational managers to implement the toolkit Effect: Services not operating as efficiently as they could Impact: Significant impact on CIP Delivery (approx. costing savings of 2.5m not achieved/gap) Use of Bank staff. Staff being asked if they wish to join the Bank on induction CIP Scrutiny Panel in place reporting to FIP on a monthly basis. Monitoring of progress against targets - escalated to FIP Committee Process undertaken to identify and allocate projects to Directorates. Targets and initial project plans sign off process in place. Business planning workshops to were held during November and following these a CIP engagement session for each division will take place between January 2016 and March Discussed at Senior Management Team meeting and no change or update at this time Date Entered : 14/01/ : North and South Implementation Groups - reporting to Workforce Planning and Information (sub of Workforce Matters). Awaiting amendments agreed On the divisional risk register CIP Scrutiny Panel to be applied to individual budgets concerned. Potential for small cost pressure (initial estimate 25k) on SLT budget but will confirm once budgets rectified. Potential work force model described to be implemented as vacancies arise. Jan 16: Ongoing work to address OT issues Corporate risk, deviation templates were completed and agreed for all AHP services with the exception of OT. No cost pressures or inefficiencies have resulted for the changes made to the teams and all teams now have an agreed skill mix to work towards with no additional cost pressures. OT remains outstanding current cost pressure 500k. Workforce model and required establishment now modelled with finance OT budget/establishment remains outstanding Output of WPT does not reflect the skill mix required within the Team. Transformation of Social Care and Care Act have increased demand on the team. Date Entered : 21/01/ :29 Director Of Operations & Service Transformation Director Of Operations Director Of Operations & Service Transformation Director Of Operations Deputy Chief Executive Officer Director Of Operations 3-6 Months 0-3 Months Date Printed: 21/01/2016 Page 5 of 8
64 Risk Register - Corporate Risks Number CQC Domain Strategic Objective Division, Direcotrate, Department Added to Register Review Cycle and Last Updated Description of Risk Cause Effect Impact Initial Impact Initial Likelihood Initial Risk Rating Details of Risk Control Actions Planned Action Progress Current Impact Current Likelihood Residual Rating Lead Officer Lead Manager Lead Director Target Impact Target Likelihood Target Risk Rating Risk Proximty Templates need to be presented to WPIG. Division not currently in a position to safely progress. Jan 16: Work ongoing in relation to implementation of toolkit We have not made any progress re AHP toolkit. Exception reports been completed by division and professional lead. This will mean deviation form the toolkit recommendations 14 Corporate Workforce Directorate Workforce & Development Direct Safe SG3 01/01/2015 Monthy 06/01/2016 Risk of non-compliance with appraisals and mandatory training, in accordance with Trust guidance Cause: Uptake of appraisals has reduced primarily due to 1) capacity within the workforce and 2) changes to reporting periods to reflect increments, although the quality of appraisals has improved Effect: Less face2face time between managers and staff for staff dialogue. Negative impact on planning for training and development. Impact: Negative impact on staff morale and team understanding/ownership. Reduced awareness of individual's role in the organisational context. Potential compromise to patient care This risk has a co-dependency with Risks CRR 6 staff turnover, and CRR 7 timely filling of vacancies. Risk discussed at WIPG 18 January There are significant financial implications attached to this process. A deviation template needs to be presented and discussed at EMT 19 January 2016 Date Entered : 14/01/ : Workforce Matters and EMT Priority work stream Monthly dashboard with performance data. Monitoring of re-registration Ongoing monitoring of mandatory training compliance (likely to drop in January due to winter pressures and no mandatory training sessions being scheduled). Implementation plan for Trust wide appraisal process being developed No further update at this time. Date Entered : 06/01/ : Feedback on process through staff opinion survey. Associate Director Of Training & Transformation Director Of Workforce & Development Director Of Workforce And Deve 0-3 Months Date Printed: 21/01/2016 Page 6 of 8
65 Risk Register - Corporate Risks Number CQC Domain Strategic Objective Division, Direcotrate, Department Added to Register Review Cycle and Last Updated Description of Risk Cause Effect Impact Initial Impact Initial Likelihood Initial Risk Rating Details of Risk Control Actions Planned Action Progress Current Impact Current Likelihood Residual Rating Lead Officer Lead Manager Lead Director Target Impact Target Likelihood Target Risk Rating Risk Proximty 15 Specialist Services Division Sexual Health City of Leicester, Leics and R Well-Led SG5 608 Corporate Nursing And Quality Adult Safeguarding Effective Safe Caring SG1 01/03/ /12/2015 Monthy 04/12/2015 Monthy 18/01/2016 Risk that the computer system will compromise the delivery of the LLR Sexual Health services against contract Cause: The IT system is provided by three different providers therefore a very complex system. IT investigation carried out but no system improvements. Effect: Telephony system with intermittent cut out (or no phone system at all at times), limits access to clinical system, stress to staff/low morale, ad hoc use of a paper based system Impact: Unable to report against contract KPIs. Patient experience due to delays - complaints. Short term risk to clinical care and patient safety due to move to paper based system as and when required. Issue has been cited in some staff turnover. There is a risk that some staff are not fully competent and not applying the principles of the Mental Capacity Act in practice. Cause: Lack of full provision of training and policy guidance available to staffeffect: There are some staff that haven't received the necessary training on MCAImpact: There may be some patients/service users that havent received the appropriate assessments Contract with activity levels and KPIs Contracts with IT providers - not supporting the service delivery Contract monitoring bimonthly with three Local Authority providers. Trial of new IT system to be completed Jan 16: Confirmed date required for commencement of new IT roll out Few minor issues are being addressed and tested. Roll out to commence in February 2016 but no confirmed date as yet. Computers out of stock and therefore only able to provide 20 computers at a time (approx. 60 computers need replacing) and therefore roll out may take some time depending on how quickly new computers can be obtained Date Entered : 14/01/ : Adult Safeguarding team and Professional Leads Social worker available for advice and support. Briefings distributed to all staff Limited number of taught sessions available to staff Drafting of the MCA policy Provision of additional taught sessions Updating the Training needs analysis Uploading an updated ELearning package Additional staff to be identified to deliver MCA training Training needs analysis updated and sent to the training department The MCA presentation (Safeguarding Board Approved) has been sent to the training team and is awaiting upload as an ELearning package. Date Entered : 23/12/ : Senior Programme Manager Head Of Adult Safeguarding Strategic Sexual Health Service Lead Director Of Nursing & Quality Chief Operating Officer - Spec Director Of Nursing And Qualit 0-3 Months 0-3 Months Date Printed: 21/01/2016 Page 7 of 8
66 Risk Register - Corporate Risks Number CQC Domain Strategic Objective Division, Direcotrate, Department Added to Register Review Cycle and Last Updated Description of Risk Cause Effect Impact Initial Impact Initial Likelihood Initial Risk Rating Details of Risk Control Actions Planned Action Progress Current Impact Current Likelihood Residual Rating Lead Officer Lead Manager Lead Director Target Impact Target Likelihood Target Risk Rating Risk Proximty 625 Corporate Nursing And Quality Caring Effective Responsive Safe Well-Led SG1 19/01/2016 Monthy 19/01/2016 Non compliance issues have been identified by the Care Quality Commission which, if not addressed, could lead to possible enforcement action Cause: CQC did not receive adequate assurance in all areas during an inspection in November 2015Effect: Non-compliance issues identifiedimpact: Possible enforcement action if non-compliance issues not addressed Detailed action plan in place to address areas of non-compliance. Action plan reviewed and updated weekly at Steering Group meeting and Operational Delivery Group meetings and any slippage escalated to EMT weekly Ongoing work to complete actions identified in detailed action plan Weekly actions continue to be monitored through the operational delivery group with escalations identified by the steering group to Executive Management Team. Progress towards the delivery of actions together with assurance testing of outcomes is on track for delivery Date Entered : 21/01/ :32 Associate Director Of Quality And Nursing Director Of Nursing & Quality Director Of Nursing And Qualit 0-3 Months Date Printed: 21/01/2016 Page 8 of 8
67 Enc 05 REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD MEETING TO BE HELD ON: WEDNESDAY 27 JANUARY 2016 Enclosure: Enc 05 Subject: Strategic Goal: (tick as applicable) Director Lead: Safe Nurse Staffing in Community Hospitals X We will provide high quality and safe services which provide an excellent experience and best possible outcomes We will work with users and carers to deliver integrated services, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Rose Goodwin - Director of Nursing & Quality (Interim) Recommendation: For Approval & Assurance X For Discussion For Information PURPOSE OF THE REPORT: This paper provides an overview of nurse staffing levels in the Community Hospitals of the Partnership NHS Trust during November 2015 and December KEY POINTS: The nurse staffing levels summary is attached for both November 2015 (Appendix 1) and December 2015 (Appendix 2). November 2015 Safe staffing has been maintained throughout November 2015 across all 4 Community Hospitals operated by the Partnership Trust. Day time fill rate for registered nurses has increased by 2% to 98.1%; care worker fill rate remains unchanged. The number of shifts being characterised as being of professional concern (red) has fallen from 16 to 10. The number of shifts with only 1 RN on duty has fallen to 6 from 18. Ward 2 at Cheadle remains an outlier against registered nurse to patient ratios (day time shifts). There have been no patient safety issues reported on the ward related to staffing. The number of shifts with additional care worker on duty continues to rise in response to the need to carry out close supervision and monitoring for those at risk of falls. Page 1 of 8
68 Vacancies have increased within the service. There are challenges in recruitment due to interest in the roles and poor calibre of applicants at interview. Staff sickness for care workers has risen to 6.81% from 3.92% (October 2015) and can be attributed to seasonal illness and pre-existing health problems requiring surgical interventions. Enc 05 December 2015 Safe staffing has been maintained throughout December 2015 across all 4 Community Hospitals operated by the Partnership Trust. Day time fill rate for registered nurses has fallen slightly (1%) to 97.4% and for care workers to 99.3%. Night time fill rate remains unchanged. The number of shifts being characterised as being of professional concern (red) has risen from 10 (November 2015) to 16, which is a return to October 2015 s position. There have been no patient safety issues as a result of staffing. The number of shifts with only 1 RN on duty has risen from 6 to 16 (in line with October s position) and includes four shifts for Scotia Ward where bed occupancy was low (4 and 5 patients) that it was deemed safe to have only one registered nurse on duty. Wards 1 and 2 at Cheadle Hospital are reporting day time registered to patient ratios in excess of national best practice guidance, (1:9 and 1:10 respectively). There have been no patient safety issues reported on the ward related to staffing. The number of shifts with additional care worker on duty has fallen by 4% in December 2015 but additional staff continue to be needed to undertake close supervision and monitoring of those at risk of falls. Vacancies remain relatively unchanged during December INTER DEPENDENCIES: Legal and/or Risk It is a requirement of NHS England to provide monthly updates on safe staffing levels. Failure to comply will risk reputational damage with the public. Clinical Financial HR Staff and Trade Union involvement actions undertaken/planned Social Care Patient & Public Involvement Equality Impact Information exempt The link between safe nurse staffing levels is clear. Ensuring that the right staff are on duty to deliver care in a timely manner is a priority for the Partnership Trust There are no direct financial implications associated with this paper however there are additional costs associated with temporary staff usage. On-going recruitment and management of staff sickness is reliant upon HR support. The Staffing Establishment has been approved by and supported by the Board Support from staff side colleagues is essential in managing staff absence and supporting safe recruitment practices. This paper relates to safe nurse staffing levels in Community Hospitals only. There has been no direct involvement of public groups in the development of this paper. Safe staffing information is available to the wider public through NHS Choices and the organisations website. Safe nurse staffing levels has an impact on all users of service regardless of culture or ethnicity. This paper describes how a safe staffing profile is monitored and this is available to the public via the organisations website. None. This paper will be published on the Partnership Trust website to Page 2 of 8
69 Enc 05 from Disclosure Requirement for further review allow public scrutiny. Safe nurse staffing levels will continue to be monitored on a monthly basis RECOMMENDATIONS / ACTION REQUIRED: The Trust Board is requested to: 1. Note the report content and be assured that the organisation is compliant with safe nurse staffing level guidance for both November and December Page 3 of 8
70
71 Enc 05 Report on Safe Nurse Staffing in Community Hospitals November 2015 Safe Nurse Staffing Safe staffing has been maintained during November 2015 across the community hospital in-patient wards. Fill Rate NHS England requires all NHS organisations to provide information relating to Fill Rate for both day and night time shifts. The term Fill Rate relates to the total planned hours (staff scheduled to work on roster) versus actual hours worked and not to the number or skill mix required in agreed shift establishment. The fill rate during day time shifts for registered nurses in November 2015 is reported at 98.1% (96.0% in October 2015) and 101.3% for care workers, which is unchanged from October Night time fill rate has increased slightly for registered nurses from 98.7% in October to 99.1% in November At night the fill rate for care workers has also risen to 102.5% (October %) and reflects the additional staff used to support care for those at risk of falls. RN to Patient Ratio The overall registered nurse (RN) to patient ratio remains within acceptable parameters (1:7 - day time and 1:10 - night time). A ratio of one registered nurse to nine patients (day time) has been reported at on Ward 2 at Cheadle Hospital on three successive occasions from September to November The ward has a relatively high vacancy factor (5.19WTE) for registered nurses, has staff on maternity leave as well as an above average rate of sickness for both care workers and registered nurses. The Hospital Matrons and Community Hospitals Manager are working with HR colleagues in the active recruitment to these and posts across the service. Night time shifts are staffed so as to ensure a minimum of two registered nurses on duty and therefore the night time patient to registered nurse ratio will vary from ward to ward, with the average ratio for night time being reported as 1:10 across the service. There are no wards during November which have exceeded the agreed standard for each ward at night. The number of shifts where there is only one registered nurse on duty has fallen from eighteen (October 2015) to six in November 2015; all of these shifts were night shifts. On 1 November 2015 severe fog affected the area and was cited as a reason as to why three registered nurses failed to report for duty, resulting in only one registered nurse being available. It was fortunate that additional care staff were on duty to support individuals at risk of falls, thus reducing some of the risk associated with only one registered nurse being on duty. Number of Shifts Deviating from Agreed Staffing Levels Each ward has a staffing establishment and skill mix developed from safe staffing reviews which is based on patient acuity. The number of instances where the shift by shift establishment is deviated from is reported as part of the summary dashboard. The number of shifts falling below agreed staffing for registered nurses was 289 in November (24.7%) a slight fall from October s figure (28.8%) and for care workers this figure was 36 (3.07%) which is unchanged from October s figure (3.22%). The number of shifts above agreed establishment for registered nurses was 62 (5.29%) which is an increase compared to the October percentage (3.06%). The reported increase can be attributed to Page 4 of 8
72 Enc 05 issues with supply and demand for temporary staff. There have been a number of occasions during November 2015 where requests have been made to the internal Bank for care workers but none could be provided for the dates/shifts required, there was however registered nurse availability and these staff were utilised, despite a lower band being required, so as not to impact safety. Additional care workers continue to be utilised across the service and there has been a further rise in the number of shifts above the agreed establishment for this staff group to 57.09%. These staff have been utilised to support individuals who, due to cognitive impairment and increased frailty, are at increased risk of falls and harm and to fill gaps in registered nurse rota s where this staff group cannot be sourced. Professional Concerns There were ten shifts reported as being of professional concern during November 2015 a fall from October (16). The majority (9 shifts) of these shifts were night shifts and one was a late shift. Three of the night shifts related to temporary staff failing to report for duty due to inclement weather (fog). Five of the shifts where professional concern was raised were shifts with only one registered nurse on duty. The short notice absence coupled with high patient demand put additional pressure on the teams; in the majority of cases there were no patient safety incidents although there were a small number of no harm falls where staffing levels were considered a factor. In the remaining instances concerns related to increased care needs of those on the wards. Mitigation of risk has been achieved by reprioritising work activities and support provided by other staff on site. The number of amber shifts reported has fallen slightly to 21.88% (256 shifts) from 22.41% in October 2015 and those classed as been of no concern (green) have correspondingly increased to 77.26% from 76.26% in October Agency Staff Usage Agency usage has remained relatively unchanged during November 2015; registered nurse agency staff 8% (9% in October 2015), care worker 11% (10% in October 2015). Wards are required to utilise the internal Bank to supply temporary staff in the first instance before agency resources can be considered. Where agency staff are used senior manager agreement is required. Care workers form the majority of agency staff usage so as to support individuals at risk of falls. There are some wards where registered nurse agency use is high and reflects vacancy and sickness in this staff group. Recruitment The number of registered nurse and care worker vacancies within the Community Hospitals service (hands on care) has increased to 32.77WTE (RN WTE and HCSW 6.15WTE) from WTE. Recruitment continues, however suitable candidates both in number and suitability for the position offered continues to be a challenge. Sickness The average percentage sickness absence in November 2015 remains relatively unchanged for registered staff (2.69% - Nov/ 2.77% - Oct) and has increased for care workers (6.81% Nov/ Oct 3.92%). The majority of sickness relates to short term illness, often associated with the time of year however there are a number of staff awaiting surgery and are precluded from work as a result of their health needs. Page 5 of 8
73 Enc 05 Report on Safe Nurse Staffing in Community Hospitals December 2015 Safe Nurse Staffing Safe staffing has been maintained during December 2015 across the community hospital in-patient wards. Fill Rate NHS England requires all NHS organisations to provide information relating to Fill Rate for both day and night time shifts. The term Fill Rate relates to the total planned hours (staff scheduled to work on roster) versus actual hours worked and not to the number or skill mix required in agreed shift establishment. The fill rate during day time shifts for registered nurses in December 2015 is reported at 97.4% (98.1% in November 2015) and 99.3% for care workers, which is a slight fall from November 2015 where care worker fill rate (day) was reported at 101.3%. Night time fill rate remains relatively unchanged for registered nurses, 98.1% in December and 99.1% in November 2015, and care workers, 103.9% in December and 102.5% in November Overfill rates (above 100%) reflect the additional care worker staff utilised to fill gaps in the rota where registered nursing staff cannot be sourced and to support care for those at risk of falls, thus mitigating risk. RN to Patient Ratio The overall registered nurse (RN) to patient ratio remains within acceptable parameters (1:7 - day time and 1:10 - night time). A day time ratio of one registered nurse to nine patients has been reported on Ward 1 and a ratio of one registered nurse to ten patients reported for Ward 2 both wards are at Cheadle Hospital. Night time ratios (registered nurse to patient) on these wards are within normal parameters (1:10). Staff sickness and registered nurse vacancies are all key contributors to an inability to meet the ratios recommended nationally. In addition the hospital s rural location, away from public transport links means attracting temporary staff to fill registered nurse gaps in the rota is difficult. Recruitment options continue to be pursued but the future transfer to University Hospital of North Midlands is seen by prospective candidates as a detractor and reducing interest in available posts. The hospital manager and matrons are working closely to reallocate staffing from other sites to improve cover however the ability to achieve this is hampered by absences on other wards and sites. Night time shifts are staffed so as to ensure a minimum of two registered nurses on duty and therefore the night time patient to registered nurse ratio will vary from ward to ward, with the average ratio for night time being reported as 1:10 across the service. The number of shifts where there is only one registered nurse on duty has risen during December 2015 from 6 to 16. The majority of shifts where there was only one registered nurse on duty were night shifts (13). Four of these shifts relate to Scotia Ward, as a result of staff sickness and additional registered nurse cover could not be sourced; ward occupancy was low, four and five patients, and following a risk review it was determined by operational managers that the remaining staffing levels were sufficient to maintain safety, particularly with the available support from wards on site on these occasions. Nine of the instances where there was one registered nurse on duty were classed as being of professional concern. Four of these were night shifts, one early shift and one late shift and were of concern due the lateness that staff were made aware that registered nurse cover would be diminished. There were no patient safety incidents as a result of staffing on any of the wards reporting professional concern or reduced registered nurse cover. Number of Shifts Deviating from Agreed Staffing Levels Each ward has a staffing establishment and skill mix developed from safe staffing reviews which is based on patient acuity. The number of instances where the shift by shift establishment is deviated from is reported as part of the summary dashboard. Page 6 of 8
74 Enc 05 The number of shifts falling below agreed staffing for registered nurses was 336 in December 2015, an increase compared to November s data (289/24.7%), and represents 27.8% of all shifts; for care workers this figure was 59 (4.9%), again an increase from November 2015 (36/3.07%). No excessive annual leave was taken in December 2015 and the fall in shifts below agreed staffing levels is thought to relate to a reduction in availability from temporary staff (Bank and Agency) due to the Christmas and New Year holiday period. The number of shifts above the agreed establishment for registered nurses has remained relatively unchanged at 66 shifts (5.4%) for December 2015 (62/5.29% in November 2015). There have been a number of shifts where care worker cover was required but availability was limited to registered nursing staff; in these instances the more qualified individual was utilised to ensure safety rather than accept a gap in the service. For care workers there were 645 shifts (53.3%) where additional staff were utilised, which is a slight reduction on November s figure of 57.09%. This staff group have supported additional care needs, particularly those at risk of falls and also to mitigate risk where registered nurse cover cannot be sourced. Professional Concerns There were sixteen shifts reported as being of professional concern during December 2015 compared to ten shifts in November 2015 but this figure is equal to that reported in October The majority of these shifts (11) were night shifts; four were late shifts and one an early shift. The majority of shifts were deemed as being of professional concern as a result of short notice absence, either sickness or failure of temporary staff to report for duty, or where patient care needs exceeded nursing capacity. There were no patient safety incidents relating to staffing on these shifts but nursing staff felt pressured and as they continued to strive for high quality care with reduced resources. The number of amber shifts has increased from 256 (21.88% - November 2015) to 380 (31.4%) in December This change is a reflection in the increased activity associated with the winter and holiday period and associated increase in patient acuity. It is important to note that an amber shift is one where there is a disparity between agreed and actual staffing numbers/skill mix or between demand and capacity however the concern or disparity concern has been resolved or appropriate mitigation in place to maintain safety. Agency Staff Usage Agency usage for December 2015 is reported as 8% for registered nursing staff, which is no change from previous months and 12% for care worker staff, a slight increase (Nov 11%, Oct 10%) from previous months and reflects the need to provide support for those at risk of harm whilst in an inpatient area. Use of Agency staff is agreed through the operational management team for the hospitals and can only be considered when all other avenues have been exhausted. Recruitment The number of vacancies for both registered nursing and care worker staff has remained relatively unchanged (RN: Nov 26.62WTE & Dec 25.15WTE and HCSW: Nov 6.15WTE & Dec 4.66WTE). A rolling programme of recruitment continues however perceived uncertainty about the future of this service and the impending transfer of some services to University Hospitals of North Midlands has resulted in a low level of interest in available posts. Sickness The average percentage sickness absence for December 2015 is reported at 39.68WTE (7.27%) for care workers and 5.5WTE (2.82%) for registered staff. The overall small increase in sickness amongst care workers is a likely reflection of seasonal illnesses e.g. colds, flu like symptoms and winter vomiting. There are some ward areas that are reporting high levels of sickness absence again due to seasonal health problems but also long term health issues, some of whom require surgery before they are able to return to work. Page 7 of 8
75 Enc 05 Recommendations The Trust Board is requested to: 1. Note the report content and be assured that the organisation was compliant with safe nurse staffing level guidance for both November and December Page 8 of 8
76
77 Hospital Ward Bed Numbers Green Amber Red RN - Day HCSW - Day RN - Night HSCW - Night Day Night RN HCSW RN HCSW Bradwell Only 1 RN on Shift RN HCSW RN HCSW Vacancies - RN Bennion % 97.7% 98.2% 100.9% 1:6 1: % 5% Oak % 98.1% 101.9% 100.0% 1:7 1: % 1% Sycamore % 100.0% 100.0% 100.0% 1:6 1: % 2% Total Bradwell % 98.6% 100.0% 100.5% 1:6 1: % 3% Cheadle Ward One % 97.8% 100.0% 100.0% 1:8 1: % 18% Ward Two % 98.8% 98.3% 100.0% 1:9 1: % 7% Total Cheadle % 98.3% 99.2% 100.0% 1:8 1: % 13% Leek Cottage % 99.1% 100.0% 96.8% 1:8 1: % 1% Saddler % 99.6% 96.8% 97.2% 1:8 1: % 9% Total Leek % 99.4% 98.4% 97.0% 1:8 1: % 5% Haywood Safe Staffing (Community Hospitals) Nov-15 Professional Judgement Monthly Fill Rate (NHS Choices) Staffing Ratios Establishment Low Staffing No of shifts RAG rated by nurse in charge Actual V Rostered Staffing (Hours) Average RN to Patient Ratio Ward Establishment (WTE) Number of shifts BELOW agreed establishment High Staffing Number of shifts ABOVE agreed establishment Agency Staff Average % of Actual Staffing Agency Staff Broadfield % 108.6% 100.0% 125.0% 1:8 1: % 17% Chatterley % 99.1% 100.0% 99.0% 1:7 1: % 27% Grange % 109.1% 96.6% 103.3% 1:6 1: % 26% Vacancies - HCSW Vacancies and Leave WTEs vacant or not filled due to sickness/maternity leave Posts appointed to but not yet started Maternity Leave Sickness HSCW (11.88%) RN (0.41%) HSCW (10.49%) RN (0.41%) HSCW (6.11%) RN (8.00%) HSCW (9.49%) RN (2.94%) HSCW (0.48%) 0 - RN (0.00%) HSCW (13.72%) RN (4.47%) HSCW (7.10%) RN (2.24%) HSCW (7.06%) RN (5.23%) HSCW (7.84%) RN (1.52%) HSCW (7.45%) RN (3.38%) HSCW (2.17%) RN (9.16%) HSCW (14.51%) RN (6.36%) HSCW (11.08%) RN (7.25%) Professional Assurance Professional Assurance Statement Safe staffing has been maintained throughout November There was only one shift (Night) which was of professional concern and also resulted in one RN on duty. A Bank member of staff failed to report for duty due to adverse weather (fog). A near miss event (fall without injury) occured on this shift and staffing was thought to be a contributing factor. Safe staffing has been maintained throughout November There were no shifts with only one RN on duty or where professional concern was raised. Safe staffing has been maintained throughout November There were no shifts with only one RN on duty or where professional concern was raised. The ward is unable to meet the RN staffing levels set out as part of the D2A project and where gaps in RN provision cannot be filled, care worker staff have been utilised to mitigate risk. Additional care worker staff have also been used to support close supervision and monitoring of those individuals at risk of falls. There have been no patient safety incidents relating to staffing. Safe staffing has been maintained throughout November There were no shifts with only one RN on duty or where professional concern was raised. Additional staff have been utilised to provide close monitoring and supervision for those individuals at risk of falls. There have been instances where care worker staff could not be sourced and RN's were available; in these instances they were redeployed to another ward area, with RN gaps. Safe staffing has been maintained throughout November There was only one shift (Night) which was of professional concern and also resulted in one RN on duty. An Agency member of staff failed to report for duty due to adverse weather (fog). Mutual aid was provided from the adjacent ward and there were no patient safety issues relating to staffing reported. Additional care worker staff have also been used to support close supervision and monitoring of those individuals at risk of falls. Safe staffing has been maintained throughout November There were no shifts with only one RN and only one shift (Night) where professional concern was raised. Short notice sickness absence from the care worker staff and an inability to find alternative cover placed additional pressure on the team, whilst caring for patients with complex care needs. There were no patient safety issues relating to staffing. Additional care worker staff have been used to support close supervision and monitoring of those individuals at risk of falls and to mitigate risk where RN gaps cannot be filled. Safe staffing has been maintained throughout November There were four shifts where professional concern was raised (1x Late and 3 x Night) with two of the night shifts resulting in only one RN on duty. All shifts where concern was raised resulted from late notice absence, making sourcing additional staff challenging. The majority of absences related to sicknes but one shift was challenged due to poor weather and the Agency nurse did not report for duty as a result. There were two instances of no harm falls on these shifts and staffing was thought to be a contributing factor. Safe staffing has been maintained throughout November There were no shifts where professional concern was raised and one shift (Night) with only one RN on duty due to failure of an Agency nurse failing to report for duty. Gaps in RN provision were filled by additional care worker staff when RN's could not be sourced. Additional care worker staff were also utilised to reduce risk of harm amongst individuals with unpredictable and risky behaviours. Safe staffing has been maintained throughout November There were no shifts with only one RN on duty or where professional concern was raised. Additional care workers were utilised to provide close monitoring for those at risk of falls. Safe staffing has been maintained throughout November There were no shifts with one RN on duty and two shifts (Night) where professional concern was raised. Late notice sickness absence resulted in RN gap's not been filled adding additional pressure on to the team, caring for individuals with complex health needs. There were no patient safety incidents relating to staffing reported onthese shifts. Additional care workers were utilised to provide close monitoring for those at risk of falls. Where care workers were requested and none available but a RN was sourced these staff were utilised on wards with RN gaps in the rota. Jackfield % 97.7% 98.3% 98.8% 1:6 1: % 15% Scotia % 99.3% 100.0% 100.0% 1:4 1: % 0% Sneyd % 108.7% 100.0% 114.1% 1:6 1: % 11% Total Haywood % 104.0% 99.0% 105.4% 1:6 1: % 16% Overall % 101.3% 99.1% 102.5% 1:7 1: % 11% Total HSCW (2.61%) RN (0.16%) HSCW (12.38%) 0 - RN (0.00%) HSCW (8.69%) RN (0.14%) HSCW (8.57%) RN (3.85%) HSCW (6.81%) RN (2.69%) Safe staffing has been maintained throughout November There was one shift (Night) with only one RN on duty and where professional concern was raised as a result of late notice sickness. Additional care workers were utilised to provide close monitoring for those at risk of falls and those who require the support of more than 2 members of staff to move safely. Safe staffing has been maintained throughout November There were no shifts with only 1 RN on duty or where professional concern was raised Safe staffing has been maintained throughout November Safe staffing has been maintained throughout November There were no shifts with only 1 RN on duty or where professional concern was raised. Additional care workers were utilised to provide close monitoring for those at risk of falls.
78 Safe Staffing (Community Hospitals) Dec-15 Professional Judgement Monthly Fill Rate (NHS Choices) Staffing Ratios Establishment Low Staffing Ward Establishment Number of shifts BELOW agreed No of shifts RAG rated by nurse in charge Actual V Rostered Staffing (Hours) Average RN to Patient Ratio (WTE) establishment High Staffing Number of shifts ABOVE agreed establishment Agency Staff Average % of Actual Staffing Agency Staff Vacancies and Leave WTEs vacant or not filled due to sickness/maternity leave Professional Assurance Hospital Ward Bed Numbers Green Amber Red RN - Day HCSW - Day RN - Night HSCW - Night Day Night RN HCSW RN HCSW Only 1 RN on Shift RN HCSW RN HCSW Vacancies - RN Vacancies - HCSW Posts appointed to but not yet started Maternity Leave Sickness Professional Assurance Statement Bennion % 102.2% 100.0% 100.0% 1:6 1: % 5% HSCW (8.49%) RN (2.60%) Safe staffing has been maintained throughout December There were no shifts with only one registered nurse on duty or where professional concern was raised. Acuity of patients remains high and additional staff are being utilised to reduce risk of falls in those at risk. Additional care worker staff were utilised to fill gaps in the roster where registered nursing staff could not be sourced and to support individuals at risk of falls. Bradwell Oak % 100.5% 98.4% 100.0% 1:6 1: % 9% HSCW (17.68%) RN (1.12%) Safe staffing has been maintained throughout December There was one shift (Night shift) with only one registered nurse on duty as a result of late notice sickness. Bed capacity was slightly reduced (2 empty beds) and measures were taken to reduce risk. Support was provided from colleagues on site and reprioritising work activities reduced risk. There was one shift (Night Shift) where professional concern was raised due to increased demand following deterioration in a patient's health. There were no patient safety incidents as a result of staffing concerns. Additional staff have been used to support close supervision and monitoring of those at risk of falls. Sycamore % 98.5% 98.4% 96.7% 1:7 1: % 4% HSCW (6.90%) RN (0.41%) Safe staffing has been maintained throughout December There were was one shift (Night shift) with only one registered nurse on duty which was also of professional concern. Short notice sickness and increased patient care needs were key factors on this shift. There were no patient safety incidents as a result of staffing concerns. Where gaps in registered nursing cover cannot be filled additional care workers have been sourced to maintain patient safety. Total Bradwell % 100.4% 98.9% 99.0% 1:7 1: % 6% HSCW (11.02%) RN (1.38%) Ward One % 97.4% 100.0% 106.4% 1:9 1: % 23% HSCW (5.95%) RN (2.65%) Safe staffing has been maintained throughout December There were no shifts with only one registered nurse on duty or where professional concern was raised. Additional care worker staff were utilised to fill gaps in the roster where registered nursing staff could not be sourced and to support individuals at risk of falls. Cheadle Ward Two % 99.4% 98.4% 96.3% 1:10 1: % 8% HSCW (15.15%) RN (4.17%) Safe staffing has been maintained throughout December There was only one shift (Night shift) with only one registered nurse on duty, which was also of professional concern. Short notice staff sickness and an inability to source allternative cover contributed to increased pressure onthose on duty. Reprioritisation of work activities and mutual aid from colleages on the other ward on site mitigated risk. There were no patient safety incidents. Additional care worker staff have been used to support close supervision and monitoring of those at risk of falls as well as filling registered nursing gaps when they could not be sourced. Total Cheadle % 98.4% 99.2% 100.6% 1:9 1: % 15% HSCW (10.55%) RN (3.41%) Cottage % 102.9% 95.2% 100.0% 1:8 1: % 5% HSCW (8.31%) RN (5.04%) Safe staffing has been maintained throughout December There were three shifts where proffessional concern was raised (Night shifts) and all of these shifts also had only oneregistered nurse on duty as a result of failure of staff reporting for duty. Staff on the preceding shift offered additional support with key activities, reprioritisation of workload and support from colleagues on site maintained safety. There were no patient safety incidents as a result of staffing reported. Gaps in RN provision have been filled by care workers where registered nurse staff could not be sourced. Additional staff have been used to support close supervision and monitoring of those at risk of falls. Leek Saddler % 101.9% 100.0% 104.5% 1:8 1: % 24% HSCW (0.75%) RN (2.94%) Safe staffing has been maintained throughout December There were two shifts (1 x Early and 1 x Late) where professional concern was raised both of which resulted in only one registered nurse on duty. There was a further shift (Late) where there was only one registered nurse on duty as a result of short notice sickness. Both shifts where concerns were raised related to short notice sickness and high levels of patient dependency, which added additional pressure to those on duty. There were no patient safety incidents resulting from staffing. Gaps in registered nurse provision have been filled by care workers where registered nurse staff could not be sourced. Additional staff have been used to support close supervision and monitoring of those at risk of falls. Total Leek % 102.4% 97.6% 102.6% 1:8 1: % 14% HSCW (4.53%) RN (3.99%) Broadfield % 91.1% 96.7% 111.4% 1:8 1: % 9% HSCW (0.00%) RN (12.02%) Safe staffing has been maintained throughout December There was one shift (Night shift) with only one RN on duty, as the agency member of staff failed to report for duty and no shifts where professional concern was raised. Gaps in nurse staffing have been supported by additional care workers and support has been recieved from the wider MDT working on the ward. Chatterley % 98.8% 96.8% 100.0% 1:8 1: % 27% HSCW (13.14%) RN (6.08%) Safe staffing has been maintained throughout December There were three shifts (2x Night shifts and 1 X Late shift) where professional concern was raised, with both night shifts having only one registered nurse on duty as a result of short notice sickness. Increased patient care needs exceeding staffing capacity prompted professional concerns on the third shift. No safety issues arose as a result of this increase in care needs but the ward staff were under additional pressure to meet patient needs and maintain safety. Additional care workers have been utilised on all late and night shifts to support and monitor those at risk of falls. Haywood Grange % 102.3% 97.8% 107.5% 1:7 1: % 19% HSCW (4.37%) 0 - RN (0.00%) Safe staffing has been maintained throughout December There were no shifts with only one registered nurse on duty and three shifts (2 Night shifts and 1 x Late shift) where professional concern was raised. High patient care needs on these shifts due to deteriorating health problems increased pressure on staff to meet patient needs and maintain safety. There were no patient safety issues arising from staffing. Additional care workers have been utilised on all late and night shifts to support and monitor those at risk of falls. Jackfield % 92.5% 100.0% 94.4% 1:6 1: % 11% HSCW (19.11%) RN (2.26%) Safe staffing has been maintained throughout December There were no shifts with only one registered nurse on duty and two shifts (1 x Late and 1 X Night) where professional concerns was raised. Both shifts experienced increased patient care demands which exceeded capacity placing additional pressure on those on duty. There were no patient safety incidents relating to staffing. Additional care workers have been utilised on all late and night shifts to support and monitor those at risk of falls and those who require the support of more that two members of staff to move safely. Scotia % 96.2% 93.5% 100.0% 1:4 1: % 0% HSCW (12.38%) 0 - RN (0.00%) Safe staffing has been maintained throughout December There were four shifts with only one registered nurse on duty due to sickness absence and due to low patient numbers (4 and 5 patients) a risk review determined it was safe to have one registered nurse on duty. There were no patient safety incidents as a result of staffing. There were no shifts where professional concern was raised. Sneyd % 111.8% 100.0% 131.5% 1:6 1: % 19% HSCW (4.01%) 0 - RN (0.00%) Safe staffing has been maintained throughout December There were no shifts with only one registered nurse on duty or where professional concern was raised.additional care workers have been utilised on all late and night shifts to support and monitor those at risk of falls. Total Haywood % 98.4% 97.5% 108.3% 1:6 1: % 14% HSCW (8.84%) 3 - RN (3.39%) HSCW Overall Total % 99.3% 98.1% 104.0% 1:7 1: % 12% (7.27%) RN (2.82%)

79 Enc 06 REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD TO BE HELD ON: 27 JANUARY 2016 Enclosure: Enc 06 Subject: Quality Scorecard Strategic Goal We will provide high quality and safe services which provide an excellent experience and best possible outcomes We will work with users and carers to deliver integrated services, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Director Lead: Rose Goodwin, Interim Director of Nursing & Quality Recommendation: For Approval & Assurance X For Discussion For Information PURPOSE OF THE REPORT: The report provides the Trust Board with a concise quality scorecard. The scorecard provides the performance, experience, safety, and effectiveness data of service users and carers during November KEY POINTS: Of the 39 indicators with agreed target, there are 7 red rated indicators. Explanation and actions are detailed on the front page of the scorecard. Escalated actions will be developed with operational teams and signed off through Divisional Business Meetings. The Quality Team is coordinating the development of agreed targets and RAG rating thresholds for applicable remaining indicators Further work to develop metrics will be aligned with the development of the Trust Quality Priorities for 2016/17 The Scorecard was received at the Quality Governance Committee on 13 January 2016 INTER DEPENDENCIES: Legal and/or Risk The Quality Scorecard provides the Board with assurance that mechanisms are in place to manage and monitor quality and identify when any concerns may emerge. Clinical All staff have a responsibility for the experience, safety, and quality of the services they provide. Page 1 of 2
80 Financial HR Enc 06 Potential savings linked to better monitoring, reduced risk and prompt action. Training/Development Rolling programme of key governance/quality messages and responsibilities through staff induction. Social Care Social Care data is incorporated in this report for the Trust Service User / Carer Experience work programmes. Patient & Public Involvement Equality Impact Information exempt from Disclosure Requirement for further review User, Carer and Parent feedback along with suggestions of service improvement is included in the User/Carer experience work programmes. A equality impact assessment has been implemented throughout the development of the Quality Framework and associated work programmes. None Monthly RECOMMENDATIONS: The Board is recommended: To discuss and note the quality indicators in the scorecard and the mitigation for November Page 2 of 2

81 Safety Quality Scorecard November 2015 Effectiveness Experience Performance Lead Indicator MONTH TARGET RAG DIRECTION* Exceptions Caroline Llewelly Safety Thermometer - Harm Free Care 84.09% >95% Red n 2014/15 Average EXPLANATION AND ACTIONS Key factor is old harm present on transfer into our care Carrie Felgate Clostridium Difficile Cumulative YTD 14 (YTD) Marie Allen Gary Stubbs Gary Stubbs 10 (annual tolerance) Red Patient feedback on the Quality of Care 85.0% 90% Red D04a: % receiving reablement in the year, where the immediate outcome was no support or low level support D06b: % older people at home and needing no on-going Social Care services 91days following receipt of reablement 2014/15 total % Red 67.3% % Red 54.8% Infection Control team are now reviewing patients daily. New patients with loose stools are screened regardless of risk factors. Infection Control are reviewing lists of patients prior to transfer into the Trust. NB 12 out of 14 cases were deemed unavoidable to the Trust. A variety of actions have been put into place to improve quality in response to the feedback received. Comprehensive Improvement Plan in Place - Owner Ed Finnemore Comprehensive Improvement Plan in Place - Owner Ed Finnemore Gary Stubbs Gary Stubbs i02b(i): The proportion of people using social care who receive direct payments - snapshot J01d: Proportion of clients in receipt of long term support who had a review (rolling 12 months) % Red 24.6% % Red 58.3% Comprehensive Improvement Plan in Place - Owner Ed Finnemore Comprehensive Improvement Plan in Place - Owner Ed Finnemore *Sparklines provide a general direction indicator only, and should be read along with the numerical data Quality Scorecard 18/01/2016 Page 1
82
83 Quality Scorecard November 2015 Safety Lead Indicator MONTH TARGET RAG DIRECTION* 2014/15 Average EXPLANATION AND ACTIONS Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Caroline Llewellyn Caroline Llewellyn Safety Hospitals Safety Thermometer - Harm Free Care 84.09% Hospitals Safety Thermometer - No New Harms 97.73% Caroline Llewellyn Hospitals Key Harms - Pressure Ulcers (All) Caroline Llewellyn Caroline Llewellyn Caroline Llewellyn Hospitals Key Harms - CAUTI (All) Hospitals Key Harms - Falls with harm Hospitals Key Harms - VTE (New) 13.26% 1.89% 1.58% 0.00% >95% Red >95% Green N/A - N/A - N/A - N/A - Key factor is old harm present on transfer into our care 90.92% 92.76% 90.90% 90.86% 89.75% 87.88% 87.75% 84.09% 96.42% 97.70% 96.78% 96.71% 96.62% 97.73% 98.02% 97.73% 9.86% 11.92% 12.29% 10.67% 13.74% 10.23% 10.94% 13.26% 1.30% 0.88% 0.82% 0.92% 1.28% 0.76% 1.58% 1.89% 0.70% 0.32% 1.06% 0.53% 0.88% 1.14% 1.19% 1.58% 0.37% 0.55% 0.24% 0.34% 0.25% 0.00% 0.00% 0.00% Duncan Kett Total incidents reported 1192 >950 Green Quality Priority Duncan Kett Number of 'near misses' reported % Green 6.25 Quality Priority Duncan Kett Total incidents reported applicable to the Partnership Trust Care 822 N/A Duncan Kett Total incidents identified at POA 370 N/A Duncan Kett Number of Serious Incidents (SI's) 18 N/A Duncan Kett Percentage of reported incidents classified as serious incidents 2.19% <3.47% Green 3.47% Quality Priority % 2.38% 3.07% 3.34% 3.69% 1.90% 3.88% 2.19% Duncan Kett Incidents per 1000 community contacts Duncan Kett Incidents per 1000 bed days Duncan Kett Total Falls Incidents 74 N/A Duncan Kett Total Falls Serious Incidents 2 < Duncan Kett Falls per 1000 bed days 9.16 N/A Duncan Kett Number of Never Events 0 0 Green Pressure Ulcers Sue Mason Community Grade 3 & 4 Report Sue Mason Community - Avoidable and Attributable grade 3 & 4 YTD 20 <23 Amber Zero tolerance action plan, including 'react to red' programme with roll-out to community Sue Mason Hospitals - Grade 3 & 4 Report Sue Mason Hospitals - Avoidable and Attributable PUs Pending RCA 0-1 PU reported in October is pending RCA Sue Mason Deep Tissue Sue Mason Grade 1 Report Sue Mason Grade 2 Report Sue Mason Grade 3 Report Sue Mason Grade 4 Report Quality Scorecard 18/01/2016 Page 2
84 Lead Indicator MONTH TARGET RAG DIRECTION* Infection Prevention and Control 2014/15 Average EXPLANATION AND ACTIONS Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Carrie Felgate Clostridium Difficile Cumulative YTD Red 2014/15 total 10 Infection Control team are now reviewing patients daily. New patients with loose stools are screened regardless of risk factors. Infection Control are reviewing lists of patients prior to transfer into the Trust. NB 12 out of 14 cases were deemed unavoidable to the Trust Carrie Felgate Clostridium Difficile per 100k bed days N/A Carrie Felgate Mortality related to CDI (7 days) 0 N/A Carrie Felgate Mortality related to CDI (30 days) 0 N/A Carrie Felgate Mortality related to CDI (90 days) 0 N/A Carrie Felgate E Coli - Number of Incidents 1 N/A - Carrie Felgate Carrie Felgate MRSA Screening on Admission (% screened on elective admission) MRSA Bacteraemia day of admission +1 (Community hospitals) 2014/15 total % 95% Green % 99.00% 99.50% 99.72% % 99.34% 99.76% % 0 0 Green 2014/15 total Carrie Felgate MSSA (number of cases) (Hospital Acquired) 0 N/A *Sparklines provide a general direction indicator only, and should be read along with the numerical data Quality Scorecard 18/01/2016 Page 3
85 Quality Scorecard November 2015 Lead Indicator MONTH TARGET RAG DIRECTION* Corporate Governance Number of Coroners Regulation 28 Elaine received (Previously Coroner Rule Mullington 43's) Third Provider infromation from CDH Robin Medium Sasaru Robin Sasaru Robin Sasaru Robin Sasaru High NICE NICE Guidelines high-risk noncompliance (number of guidance) Effectiveness awaiting SCC data awaiting SCC data 2014/15 Average EXPLANATION AND ACTIONS Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD 0 N/A N/A N/A N/A - - Metric in development NICE Guidelines Compliance 71% N/A - - Metric in development: Currently showing compliance with Previous Years Guidance (April 13 onwards) 55% 58% 64% 64% 66% 70% 71% 71% Audit Julianne National Audit participation Brightman 100% 100% Green 100% 100% 100% 100% 100% 100% 100% 100% 100% Julianne Local Audit projects completed Brightman 8 N/A Quality Visits No visits in Nov 2015 due to the Number of Quality Visits Robin CQC inspection Sasaru Cumulative Assurance Rating Metric in development *Sparklines provide a general direction indicator only, and should be read along with the numerical data Quality Scorecard 18/01/2016 Page 4
86 Quality Scorecard November 2015 Experience Lead Indicator MONTH TARGET RAG DIRECTION* 2014/15 Average EXPLANATION AND ACTIONS Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Wendy Dale Wendy Dale Wendy Dale Wendy Dale Wendy Dale Complaints Number of formal complaints received - Health Number of formal complaints received - Social Care Number of formal complaints received Total Number of compliments received (customer services & ASC only) Complaints Closed within Timescales in Accordance with the National NHS Complaint Regulations 11 N/A - 16 N/A - 27 N/A - 90 N/A - Wendy Dale Complaints referred to the LGO 0 N/A - Wendy Dale Complaints referred to the LGO and Ongoing Wendy Dale Complaints referred to the LGO and Upheld Wendy Dale Complaints referred to the LGO not upheld Wendy Dale Complaints referred to the PHSO and Ongoing Wendy Dale Complaints referred to the PHSO and Upheld Wendy Dale Complaints referred to the PHSO not upheld Wendy Dale Number of complaints reviewed by independent panel 2014/15 total /15 total /15 total /15 total Quality Priority % N/A Green 100% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 3 N/A - 0 N/A - 0 N/A - 4 N/A - 0 N/A - 1 N/A /15 total /15 total /15 total /15 total /15 total /15 total /15 total /15 total Quality Priority Quality Scorecard 18/01/2016 Page 5
87 Lead Indicator MONTH TARGET RAG DIRECTION* 2014/15 Average EXPLANATION AND ACTIONS Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD User and Carer Experience Marie Allen FFT Total captured feedback 3832 N/A Marie Allen Total FFT Sample Green Marie Allen Total FFT Sample Score 98% 90% Green 97% 97% 97% 97% 98% 98% 96% 98% Marie Allen FFT Service User Sample Green 1850 Quality Priority Marie Allen FFT Service User Score 97% 90% Green 97% Quality Priority Marie Allen FFT Carer Sample Green Quality Priority Marie Allen Carer Score 99% 95% Green Quality Priority 2 98% 97% 98% 98% 98% 98% 97% 99% Marie Allen Patient feedback on the Quality of Care 85% 90% Red Continuity of care (no information given on am & pm slot availability is given, and different numbers of staff are providing care on a dayto-day basis) - case mgt has been reviewed, and rotas are being shared with service users. Preferred appt times are allocated where possible, with advanced allocation implemented in Stoke Sexual Health services appointment waiting times for 'clinic in a box' - Service is reviewing appointments to reduce waiting times, and including additional clinics, and developing a service leaflet for waiting times. Community Hospitals- Standards of care - staffing increase on day and night shift. Reminders to staff to ensure that buzzers and personal belongings are kept within reach CYP- Continuity of care for Stoke Children's Continuing Healthcare, (staffing levels, allocated case manager & appointments). New rota with advanced allocations for continuing healthcare in place. North & South have given a rota to service users so they know what staff be seeing them. Quality Priority 2 85% 84% 83% 85% 84% 85% 83% 85% Marie Allen Information 92% 90% Green Quality Priority 2 90% 91% 89% 92% 94% 91% 92% 92% Marie Allen Listened to 95% 90% Green Quality Priority 2 95% 95% 96% 96% 95% 94% 96% 95% Marie Allen Being Involved 96% 90% Green Quality Priority 2 97% 97% 96% 98% 97% 96% 97% 96% *Sparklines provide a general direction indicator only, and should be read along with the numerical data Quality Scorecard 18/01/2016 Page 6
88 Quality Scorecard November 2015 Lead Indicator MONTH TARGET RAG DIRECTION 2014/15 Avg Gary Stubbs Gary Stubbs Gary Stubbs Reablement D04a D06a D06b % receiving reablement in the year, where the immediate outcome was no support or low level support % older people at home 91 days after discharge from hospital into reablement % older people at home and needing no on-going Social Care services 91days following receipt of reablement - 72% Red 67.3% EXPLANATION AND ACTIONS Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Comprehensive Improvement Plan in Place For details please contact Barrie Knox / Ed Finnemore 56.2% 61.4% 60.2% 62.1% 62.9% 62.9% 62.9% 62.4% - 85% Green 87.9% 89.6% 86.2% 86.4% 85.8% 86.0% 86.0% 86.2% 85.4% - 55% Red 54.8% Comprehensive Improvement Plan in Place For details please contact Barrie Knox / Ed Finnemore 56.3% 53.4% 53.0% 51.5% 50.0% 49.6% 50.3% 49.9% Gary Stubbs Timeliness E03 Waiting time from assessment start to assessment completion: percentage completed within 4 weeks - 75% Green 73.3% 75.1% 72.4% 73.6% 73.6% 75.3% 75.7% 76.4% 76.5% Gary Stubbs Carers E11 % carers assessed or reviewed in the year out of the total number of carers 'on the books - 70% Amber 60.7% 86.9% 87.2% 89.8% 88.3% 80.1% 75.1% 70.3% 68.9% Gary Stubbs Safeguarding F05 % cases where the risk of harm has been reduced - 94% Amber 92.1% 92.8% 93.0% 92.9% 92.9% 92.6% 92.7% 92.4% 93.0% Gary Stubbs Personal Budgets i02a(i) % using social care who receive self-directed Increasing - now only 1.2% off 84% - 84% Amber 73.4% support (personal budget or direct payment) - snapshot target 76.0% 79.7% 80.3% 77.3% 75.9% 78.1% 80.8% 82.8% Gary Stubbs Direct Payments i02b(i) The proportion of people using social care who receive direct payments - snapshot Gary Permanent Long Stubbs Stay Residential Gary Admissions Stubbs Social Care ('Fin Yr to Date' unless otherwise stated) % Red 24.6% Comprehensive Improvement Plan in Place For details please contact Barrie Knox / Ed Finnemore 24.3% 24.5% 25.4% 24.3% 24.3% 24.1% 23.9% 24.1% i03a(ii) Younger adults (per 100,000 population) Green i03b(ii) Older people aged 65+ (per 100,000 population) Green Gary Stubbs Reviews J01d Proportion of clients in receipt of long term support who had a review (rolling 12 months) Performance - 70% Red 58.3% Comprehensive Improvement Plan in Place For details please contact Barrie Knox / Ed Finnemore 57.9% 57.5% 57.3% 54.5% 55.5% 55.6% 55.7% 57.7% Referral to Treatment - Long Term Conditions Ian Porter Diabetes Stoke 84.2% 18 weeks % 100.0% 100.0% 100.0% 93.9% 94.9% 100.0% 84.2% Ian Porter Diabetes North Staffs 100.0% 18 weeks % 100.0% 100.0% 100.0% 100.0% 92.9% 100.0% 100.0% Ian Porter Geriatics - Falls 100.0% 18 weeks % 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Ian Porter Geriatics - Parkinsons 95.5% 18 weeks % 100.0% 100.0% 100.0% 100.0% 100.0% 94.1% 95.5% Ian Porter Heart Failure - South 95.2% 18 weeks % 92.1% 96.0% 100.0% 98.5% 98.5% 100.0% 95.2% Referral to Treatment -All Consultant- led Services Ian Porter Non-admitted Completed Pathways 99.5% 95% % 99.6% 99.8% 99.8% 99.8% 99.5% 99.7% 99.5% Ian Porter Admitted Completed Pathways 99.4% 90% % 99.1% 99.4% 99.5% 98.7% 98.5% 98.9% 99.4% Ian Porter Completed Pathways 99.0% 92% % 99.7% 99.7% 99.6% 99.4% 99.3% 99.1% 99.0% Referral to Treatment - Allied Health Professional Ian Porter Cannock Chase CCG 100.0% 95% Green 100.0% 99.0% 100.0% 99.0% 98.0% 99.0% 100.0% 100.0% Ian Porter East Staffordshire CCG 100.0% 95% Green 95.0% 98.0% 100.0% 98.0% 100.0% 100.0% 100.0% 100.0% Ian Porter SES and Seisdon CCG 100.0% 95% Green 99.0% 100.0% 99.0% 99.0% 100.0% 99.0% 100.0% 100.0% Ian Porter Stafford and Surrounds CCG 100.0% 95% Green 100.0% 100.0% 99.0% 100.0% 100.0% 99.0% 100.0% 100.0% Ian Porter North Staffordshire and Stoke on Trent CCG 98.9% 95% Green 99.2% 99.9% 99.7% 99.8% 99.8% 99.8% 99.4% 98.9% *Sparklines provide a general direction indicator only, and should be read along with the numerical data
: Director Lead: We will provide high quality and safe services which provide an excellent experience and best possible outcomes We will work with users and carers to deliver integrated")
89 Enc 07 REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD TO BE HELD ON: 27 JANUARY 2016 Enclosure: 07 Subject: Integrated Performance Report Month 9 Strategic Goal (tick as appropriate): Director Lead: We will provide high quality and safe services which provide an excellent experience and best possible outcomes We will work with users and carers to deliver integrated services, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Jonathan Tringham, Director of Finance and Resources Recommendation: For Approval & Assurance X For Discussion For Information PURPOSE OF THE REPORT: The purpose of this report is to provide a concise integrated view of performance across the organisation for December The report comprises of a summary of integrated performance including Operational, Quality, Finance and Workforce indicators, incorporating trends and benchmarks where appropriate in line with the performance framework that has been adopted by the Partnership Trust. KEY POINTS: Annex 1 - Provides an executive summary and overview of the Partnership Trust s performance. Annex 2 - Details performance against the full suite of the Partnership Trust s Board indicators. Annex 3 - Illustrates the quality assessment of services provided by the Partnership Trust. The selected indicators have been grouped into safety, effectiveness and experience. Annex 4 - Demonstrates the Trust s Board self certification statement response to the TDA for November Annex 5 Detailed analysis by exception. Page 1 of 4

90 Key Performance Messages Enc 07 Overall, of the 59 Partnership Trust s Board performance indicators with targets attached, 37 are green, 7 are amber and 15 are red. The RAG status has changed for 4 indicators in December: 1 indicator improved from Amber to Green 1 indicator improved from Red to Amber 1 indicator dropped from Green to Amber 1 indicator dropped from Amber to red Annex 1 General Updates: This end of quarter report incorporates detailed analysis of underperforming areas. In response to feedback from, FIP and Board, we have introduced the following improvements in the Q3 report: o Included the population size for Operations KPIs in order provide additional context o o Estimated improvement trajectories Assessed in detail data quality drivers for KPIs causing concern (we are currently reviewing DQ % scores methodologies, and these will be added again in the January report). Note that DQ % scores will be lower than the average score of the individual DQ drivers (combined impact of multiple factors). Page 2 of 4
91 Enc 07 Key Areas of Strong Performance Improvement include: The proportion of social care clients receiving self-directed support has followed a steady improvement trend since August (75.9%), and for the first time reached performance levels above target in December (84.9%). This is consistent with the high proportion survey respondents who report feeling that their support is directed by them and responsive to their needs (97%). Key Performance Concerns: The percentage of Harm Free Care in the Safety Thermometer, currently at 91.3% against its 95% target, remains the only area of non-compliance in the Quality Assessment. Social Care indicators remain a source of concern: o Delayed transfers of care attributable to social care (60.0) notably exceed their target (37.5). The delayed days indicator (1,579) is also notably higher than its target (1,015). o The carers assessments indicator has rapidly deteriorated in the year from a peak in June (89.8%) to its current level (66.1%), making it Red for the first time in the year. Detailed analysis and improvement plan are now under development. o Reablement indicators remain below target with no sign of decisive improvement. o The proportion of customers receiving self-directed support through direct payments remains static at 24% below the 27.5% target. o The reviews indicator has started to show signs of improvement, and it currently stands at 63.4% against its 70% target. There will be a huge emphasis on reviews on Q4, as this has been identified as the single most important area of performance by the Commissioner for that period. INTER DEPENDENCIES: Legal and/or Risk Clinical Financial HR Staff and Trade Union involvement actions undertaken/planned Social Care Patient & Public Involvement Equality Impact Information exempt from Disclosure Requirement for The performance information included in the attached report is dependent on the quality of the source data which is taken from a number of information systems. If data consists of poor quality there is a risk that decisions could be made based on flawed performance information, and a risk of adverse audit judgements. It is essential that the performance scorecard continues to include Clinical Quality and Safety related indicators to drive continuous improvement. The financial pressures facing the Partnership Trust over the coming years necessitate the development of further value for money indicators to include in the monthly scorecard. Managing performance outcomes is dependent on its workforce for example training, appraisal and sickness levels. Performance information is shared with staff at all levels of the organisation, and a JSP agreed data input policy requires all staff to input activity within 5 working days. The report includes key Social Care performance indicators. The inclusion of service user feedback in performance reporting is essential for Trust Board assurance. The use of good Data Quality to inform decision making / service delivery is key in ensuring vulnerable groups are not discriminated against. NA Routine reports are provided to the Trust Board, Finance, Investment and Performance Committee and Operational management meetings to Page 3 of 4
92 further review update on performance issues. Enc 07 RECOMMENDATIONS / ACTION REQUIRED: The Trust Board are asked to note the content of the executive summary and performance scorecard. The Committee are asked to approve the Self-Certification Return to the NTDA for November. The Committee is also asked to review the declaration for December against Statements 2 and 5 in light of the warning notice from the CQC and to consider whether it continues to report compliance against Statements 1, 6, 7, and 10. Page 4 of 4
93 ANNEX 2: Section 1 - Quality & Safety - Lead Director - Rose Goodwin - Director of Nursing and Quality - Performance Indicators / December Data - Month 9 Strategic Objective Data Quality Indicator Type Indicator Outturn 2014/15 Target Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Direction of Travel Performance Vs. Benchmark Group L Number of Formal Complaints Received L Health / Social Care L Number of Compliments Received We Will Work with Partners, Users and Carers to Deliver Integrated Services N % of Complaints Acknowledged Within 72 Hours of Receipt 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% N Health / Social Care 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% N Complaints Closed within Timescales in Accordance with the National NHS Complaint Regulations 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% L Social Care Complaints Escalated to the Local Government Ombudsman L L L SC Social Care Complaints Escalated to the Local Government Ombudsman and Upheld ( # awaiting outcome) Health Complaints Escalated to the Parliamentary and Health Service Ombudsman Health Complaints Escalated to the Parliamentary and Health Service Ombudsman and Upheld (# awaiting outcome) Customer Overall Satisfaction (Extremely satisfied at all times) with the Care and Support Experience with Social Care? * 2 # # % 60% 64% 52% 62% 68% 66% 73% 65% 71% SC Sample received - Customer Overall Satisfaction (Extremely satisfied at all times) with the Care and Support Experience with Social Care? * SC Do you feel that you have care and support which is directed by you and responsive to your needs? * 90% 93% 95% 93% 94% 92% 96% 96% 92% 97% SC Sample Received - Do you feel that you have care and support which is directed by you and responsive to your needs? * L L Net Promoter Score (NPS) * 97% 98% 97% 97% 97% 97% 98% 96% 98% 97% 96.1% Net Promoter Score (NPS) Number of people responding * L Number of Serious Incidents L Total Incidents Reported Applicable to the Partnership Trust Care L Percentage of reported incidents classified as serious incidents 3.61% 4.67% 2.32% 3.06% 3.33% 3.67% 1.88% 3.84% 2.19% 2.99% L Number of Total Face to Face Contacts 1,915, , , , , , , , , ,959 1,369,768 TDA Number of Serious Incident Pressure Ulcers Reported (STEIS) TDA TDA TDA Number of Serious Incident Pressure Ulcers Deemed Avoidable Following Root Cause Analysis (RCA) Review Panel ( # awaiting outcome) Number of Serious Incident Pressure Ulcers Deemed Unavoidable Following Root Cause Analysis (RCA) Review Panel ( # awaiting outcome) Serious Incident Falls Reported Through National Reporting System Resulting in Severe Injury or Death # # # # # # # # # # # # TDA Falls per 1000 Inpatient Occupied Bed Days We Will Provide High Quality and Safe Services Which Provide an Excellent Experience and Best Possible Outcomes TDA Outstanding Alerts (more than 3 months old reported through the Central Alerting System) N Mixed Sex Accommodation: Single Sex Number of Breaches N Number of Never Events C Clostridium Difficile - number of avoidable incidents cumulative (INDICATOR AMENDED FROM PREVIOUS MONTHS WHERE INCLUDED UNAVOIDABLE) # awaiting panel 2 <= # 2 C Methicillin-Resistant Staphylococcus Aurous (MRSA) Bacteraemia (number of incidents within 1 month / Hospital associated)
94 C C TDA Methicillin-Resistant Staphylococcus Aurous (MRSA) Screening on Admission (% screened on elective admission) Methicillin-Resistant Staphylococcus Aurous (MRSA) Screening on Admission - No screened on elective admission / No required screening Methicillin-Sensitive Staphylococcus Aureus (MSSA) (No of cases hospital associated) 99.9% 95% 100% 99.0% 99.5% 99.7% 100% 99.3% 99.0% 100% 100% 99.7% 371/ / / / / / / / / TDA Complicated Urinary Tract Infection (CUTI) Percentage 0.57% 0.70% 0.46% 0.34% 0.39% 0.69% 0.48% 0.21% 0.32% 0.27% 0.43% TDA Complicated Urinary Tract Infection (CUTI) - Number with new CUTI / Number of patients 15/ /2170 7/2078 8/ / /2073 4/1916 6/1871 5/1857 TDA E Coli - Number of Incidents SC Compliance with Vulnerable Adults Quality Standards (quarterly) (SC44) 86% 80% 92% 88% 89% 88% SC SC Compliance with Vulnerable Adults Quality Standards (quarterly) (SC44) - Number of people included in the population sample size Compliance with Vulnerable Adults Quality Standards (quarterly) (SC44) Total number of audits due / Total number of audits completed /164 SC Percentage of Cases Where the Risk of Harm has been Reduced (F05) 92.1% 94% Q3 92.8% 93.0% 92.9% 92.9% 92.6% 92.7% 92.4% 93.0% 93.0% 93.0% Percentage of Cases Where the Risk of Harm has been Reduced (F05) - Total Risk / Risks Reduced 688/640 SC Adult Protection Case Closures Open Over 3 Months SC Adult Protection Case Closures Open Over 6 Months L Percentage of Deaths (all inpatient deaths) 7.4% 7.2% 7.3% 8.6% 7.7% 9.0% 12.2% 8.2% 9.3% 7.1% 8.0% L Ordinary Finished Consultant Episodes (FCEs) C Prison Healthcare: Deaths in Custody Indicator Type - N - National L - Local C - Contractual TDA - Trust Development Authority SC - Social Care ACFT - Aspiring Community Foundation * The population size for the Health & Social Care local survey could not be identified To be noted - following feedback from the Trust Board in November 2015 additional metrics have been added to provide context to performance indicators - these metrics have been shaded grey to show for informative purposes only and are not counted towards the overall RAG rated quadrant
95 ANNEX 2: Section 2 Operations - Lead Director - Kieron Murphy - Director of Operations - Performance Indicators / December Data - Month 9 Strategic Objective Data Quality Indicator Type Indicator Outturn 2014/15 Target Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Direction of Travel Performance Vs. Benchmark Group C Delayed Transfers of Care Community Hospitals within the Trust (percentage of occupied bed days) - Overall Trust Percentage 3.4% 3.9% 4.2% 9.4% 10.7% 6.7% 6.4% 6.9% 7.3% 6.4% Delayed Transfers of Care Community Hospitals within the Trust - Overall Trust Patients C Delayed Transfers of Care Community Hospitals within the Trust - Staffs Patients C Delayed Transfers of Care Community Hospitals within the Trust - Stoke on Trent Patients Occupied Bed Days / Beds Available 8800/ / / / / / / / /8649 SC SC Number of Social Care and Joint Delayed Transfers of Care (average no. of people delayed on snapshot dates) (average per month) (E07) Number of Social Care and Joint Delayed Transfers of Care Days (average per month) (E08) L Average Length of Stay (ALOS) (Community Hospitals Mean) C Average Length of Stay (ALOS) (Community Hospitals Median) days N Percentage of Patients Seen Within 4 Hours in MIU/Walk-in Centres 99.8% 95% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% N Number of Patients Seen Within 4 Hours in MIU/Walk-in Centres - Patients Seen / Total Patients 1173/ / / / / / / / /1033 N Percentage of Admitted Patients Meeting the 18 Week Consultant Led Referral to Treatment Target 98.2% 90% 98.4% 99.1% 99.4% 99.5% 98.7% 98.5% 98.9% 99.4% 98.5% 98.9% N Number of Admitted Patients Meeting the 18 Week Consultant Led Referral to Treatment Target - Admitted 18 Week Clock Stops / Total Admitted 18 Week Clock Stops 253/ / / / / / / / /131 N Percentage of Non-Admitted Patients Meeting the 18 Week Consultant Led Referral to Treatment Target 98.8% 95% 99.6% 99.6% 99.8% 99.8% 99.8% 99.5% 99.7% 99.5% 99.6% 99.7% 98.6% ACFT Sep 13 N Number of Non-Admitted Patients Meeting the 18 Week Consultant Led Referral to Treatment Target - Non-admitted 18 Week Clock Stops / Total Non - admitted 18 Week Clock Stops 4890/ / / / / / / / /4541 N Percentage of Patients on Incomplete Consultant-Led Pathways Waiting Less Than 18 Weeks 97.3% 92% 99.4% 99.7% 99.7% 99.6% 99.4% 99.3% 99.1% 99.0% 98.5% 99.3% N Number of Patients on Incomplete Consultant-Led Pathways Waiting Less Than 18 Weeks - 18 Week Incomplete Pathways / Total patients on Pathway 3810/ / / / / / / / /3559 L Number of Consultant-Led Patients Reported as Waiting 26 Weeks or Over (completed pathways) We Will Provide High Quality and Safe Services Which Provide an Excellent Experience and Best Possible Outcomes N C C Number of Consultant-Led Patients Reported as Waiting 52 Weeks or Over (completed pathways) (national target in place 2013/14) Therapies - Percentage of Patients Treated Within 18 Weeks from Referral to Treatment Therapies - Number of Patients Treated Within 18 Weeks from Referral to Treatment - Treatment Within < 18 Weeks / All Therapy Patients with a Clock Stop % 95% 99.5% 99.6% 99.6% 99.8% 99.8% 99.6% 99.6% 99.8% 99.8% 99.7% 8503/' / / / / / / / /8186 C Speech and Language Therapy - First Appointment Within Local Waiting Targets (North only) 92.5% 95% 97.4% 100% 98.5% 100% 100% 100% 100% 100% 100% 99.6% C Speech and Language Therapy - First Appointment (North only) - Patient Seen in Local Timescale / Total Number of Patients 112/ / / / / / / / /108 C Occupational Therapy - First Appointment Within Local Waiting Targets (North only) 97.5% 95% 97.5% 99.0% 99.8% 99.6% 99.8% 100% 100% 99.8% 99.6% 99.3% C Occupational Therapy - First Appointment (North only) - Patient Seen in Local Timescale / Total Number of Patients 867/ / / / / / / / /480 C Physiotherapy - First Appointment Within Local Waiting Targets (North only) 81.2% 90% - Q2 87.7% 85.7% 90.7% 91.0% 80.4% 90.2% 93.3% 93.9% 98.2% 90.6% C Physiotherapy - First Appointment (North only) - Patient Seen in Local Timescale / Total Number of Patients 1818/ / / / / / / / /2130 C Podiatry - First Appointment Within Local Waiting Targets Full Compliance with Routine, Urgent and Intermediate (North only) 90% C Podiatry - First Appointment Full Compliance with Routine, Urgent and Intermediate (North only) - number of Patients seen Percentage of Patients that DNA Their Outpatient/Community Appointment (All Services) % 7.5% 4.5% 4.3% 4.3% 4.6% 4.8% 4.7% 4.6% 4.3% 4.2% 4.4%
96 C Patients that DNA Their Outpatient/Community Appointment (All Services) - Patients that DNA / All Contacts Including DNA 8220/ / / / / / / / /23322 N Percentage Patients Receiving a Diagnostic Scan Within 6 Weeks of Referral 99.2% >99% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% N SC SC SC SC N SC Patients Receiving a Diagnostic Scan Within 6 Weeks of Referral - Scan Within 6 Weeks / Total Number of Scans Waiting time from assessment start to assessment completion: percentage completed within 4 weeks (E03) Waiting time from assessment start to assessment completion Number completed within 4 weeks (E03) - Number of Clients Assessment Completed within 4 weeks / Total number of clients Assessed Proportion of carers assessed or reviewed in the year out of the total number of carers 'on the books (E11) Number of carers assessed or reviewed in the year out of the total number of carers 'on the books (E11) - Year to date average forecast / Total Carers Prison Healthcare Services: Hepatitis B - Percentage vaccinated within 31 days of reception including those already vaccinated (data collected quarterly) Prison Healthcare Services: Hepatitis B Numbers vaccinated within 31 days of reception - Number of patients already vaccinated / Number of patients vaccinated within 31 days / Numbers in prison healthcare Long stay residential care permanent admissions - Younger adults (I03a ii) 235/ / /189 72/72 327/ / / / / % 75% 74.9% 72.8% 73.4% 73.6% 75.1% 75.0% 75.6% 76.5% 76.5% 75.6% 4862/ % 70% 86.9% 87.2% 89.8% 88.3% 80.1% 75.1% 70.3% 68.9% 66.1% 66.1% 4340/ % 80% 79.1% 77.0% 81.8% 76.6% 80.4% 80.1% 85.3% 79.9% 79.9% 180/85/ /102/ /107/ /133/ /97/ /108/ /116/ /107/ SC 34 SC Long stay residential care permanent admissions (ASCOF definition): Older people aged 65+ (I03b ii) SC 1015 Our Organisation Will Develop and Deliver Sustainable, Innovative Services That Support Independence SC SC SC SC SC Percentage of people receiving reablement in the year, where the immediate outcome was no support or low level support (D04a) Number of people receiving reablement in the year, where the immediate outcome was no support or low level support (D04a) - Clients with no needs identified / Total clients Percentage of Older People still at home 91 days after discharge from hospital into reablement (D06a) Number of Older People still at home 91 days after discharge from hospital into reablement (D06a) - Clients at home with no or low services / Total Clients Older people still at home and needing no on-going Social Care services 91days following receipt of reablement services (D06b) 69.1% 72% 56.2% 61.4% 60.2% 62.1% 62.9% 62.9% 62.9% 62.4% 63.0% 63.0% 87.9% 85% 89.6% 86.2% 86.4% 85.8% 86.0% 86.0% 86.2% 85.4% 84.9% 84.9% 54.8% 55% 56.3% 53.4% 53.0% 51.5% 50.0% 49.6% 50.3% 49.9% 49.0% 49.0% 579/ /1040 Eng :74.9% WM: 68.7% Shires: 77.0% Eng: 80.7% WM: 80.0% Shires: 81.3% (unvalidated) SC Older people still at home and needing no on-going Social Care services 91days following receipt of reablement services (D06b) - Clients at home with no services / Total Clients 510/1040 SC The proportion of people using social care who receive self-directed support (personal budget or direct payment) - snapshot (i02ai) 73.4% 84% 76.0% 79.7% 80.3% 77.3% 75.9% 78.1% 80.8% 82.8% 84.9% 84.9% SC The proportion of people using social care who receive self-directed support (personal budget or direct payment) - snapshot (i02ai) - Target Clients / Total Clients 4620/5442 SC The proportion of people using social care who receive direct payments - snapshot (i02bi) 24.6% 27.5% 24.3% 24.5% 25.4% 24.3% 24.3% 24.1% 23.9% 24.1% 24.0% 24.0% SC The proportion of people using social care who receive direct payments - snapshot (i02bi) - Target Clients / Total Clients 1307/5442 We Will Make Excellent Use of Our Resources and Improve Levels of Productivity Across Our Services SC Percentage of clients receiving long-term support at any point in the reporting period who have had any kind of review in the last 12 months (J01d) Percentage of clients receiving long-term support at any point in the reporting period who have had any kind of review in the last 12 months (J01d) - Total Clients with long term support / Total Clients 58.3% 70% 57.9% 57.5% 57.3% 54.5% 55.5% 55.6% 55.7% 57.7% 63.4% 63.4% L Bed Occupancy Inpatients Percentage 93.0% 93.1% 94.0% 94.8% 89.6% 99.4% 97.9% 96.3% 96.5% 98.7% 94.4% 88.1% 7013/11,054
97 ANNEX 2: Children's Services - Lead Director - Kieron Murphy - Director of Children's Services - Performance Indicators / December Submission - Month 9 The RAG ratings have been reviewed with the service for new birth visits and reviews based on performance rates over the past twelve months and in comparison with other NHS Trusts regionally and nationally, where benchmarking information has shown that the Partnership Trust out-performs its peers, and therefore an assessment has been made that an amber rating would provide the appropriate context should performance fall within a 90-94% range Strategic Objective We Will Provide High Quality and Safe Services Which Provide an Excellent Experience and Best Possible Outcomes Data Quality Score Indicator Type C C C C C Indicator Percentage of Births that Receive a Face to Face New Birth Visits within Days by a Health Visitor (data collected quarterly) Data delayed due to changes in national reporting requirements Number of Births that Receive a Face to Face New Birth Visits within Days by a Health Visitor - Total number of face-to-face New Birth Visits (NBV) undertaken between days, by a Health Visitor with mother and father / Total number of population based births, in the geographical area of provider's responsibility Percentage of Children who Received a 12 month review within 15 months (data collected quarterly) Data delayed due to changes in national reporting requirements Number of Children who Received a 12 month review within 15 months - Total number of children who received a review, by the age of 15 months of age, based on the month when the child reached 12 months of age / Total number of children aged 12 months, in the appropriate month Percentage of Children who Received a Year Review (data collected quarterly) Data delayed due to changes in national reporting requirements Outturn 2014/15 Target Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Direction of Travel 90.60% 95% / 98% 93.20% 93.30% 91.20% 93.70% 94.90% 95.50% 94.90% 94.90% 884/ / / / / / / % 95% / 98% 94.80% 93.60% 95.50% 97.10% 96.80% 95.30% 97.00% 97.00% 943/ / / / / / / % 95% / 98% 91.10% 89.60% 91.70% 90.50% 90.50% 92.20% 91.60% 91.60% Latest Performance Vs. Benchmark Group C Number of Children who Received a Year Review - Total number of children who received a review, between the ages of years of age, based on the month when the child reached years of age / Total number of children aged years, in the appropriate month 997/ / / / / / /1040 C C Percentage of Infants for whom Breastfeeding Status is Recorded at the 6-8 Week Check (data collected quarterly) Number of Infants for whom Breastfeeding Status is Recorded at the 6-8 Week Check - Number of infants where feeding status has been recorded at 6-8wk check / Total number of infants receiving 6-8wk check 90.60% 95% / 98% 77.40% 79.80% 79.80% 2225/ /2955 Indicator Type - N - National L - Local C - Contractual TDA - Trust Development Authority SC - Social Care ACFT - Aspiring Community Foundation Trust To be noted - following feedback from the Trust Board in November 2015 additional metrics have been added to provide context to performance indicators - these metrics have been shaded grey to show for informative purposes only and are not counted towards the overall RAG rated quadrant
98 ANNEX 2: Section 3 - Finance - Lead Director - Jonathan Tringham - Director of Finance and Resources - Performance Indicators 2015 / December Data - Month 9 Strategic Objective Data Quality Indicator Type Indicator Outturn 2014/15 Target Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Direction of Travel Performance Vs. Benchmark Group N Financial Performance vs. Planned Performance (favourable performance in brackets) Nil ,012 1, ,320 3,115 L Percentage of Cost Improvement Programme (CIP's) Delivered (Against YTD Plan) 100% 13% 26% 25% 46% 53% 115% 130% 126% 113% 97.2% ACFT Better Payment Practice Code by Volume 95% 90% 89% 91% 87% 87% 86% 86% 86% 87% 90.1% We Will Make Excellent Use of Our Resources and Improve Levels of Productivity Across Our Services ACFT Better Payment Practice Code by Value 95% 93% 94% 95% 87% 86% 87% 87% 86% 90% 85.6% ACFT Liquidity Ratio Days Metric Capital Servicing Capacity Metric ACFT Continuity of Service (CoS) Score ACFT Non-NHS Payables > 90 Days % 5% 10% 10% 18% 25% 18% 15% 20% 13% 17% ACFT Non-NHS Receivables > 90 Days % 5% 17% 14% 24% 31% 33% 29% 35% 34% 33% Indicator Type - N - National L - Local C - Contractual TDA - Trust Development Authority SC - Social Care ACFT - Aspiring Community Foundation Trust
99 ANNEX 2: Section 4 - Workforce - Lead Director - Julie Tanner - Director of Workforce - Performance Indicators / December Data - Month 9 Strategic Objective Data Quality Indicator Type Indicator Outturn 2014/15 Target Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Direction of Travel Performance Vs. Benchmark Group 99% TDA Workforce Sickness Rate Culmative (%) 4.98% 4.67% 4.55% 4.49% 4.44% 4.45% 4.48% 4.45% 4.40% 4.45% 4.46% 4.30% 95% TDA Workforce Sickness Rate (%) - Monthly 4.02% 4.67% 4.55% 4.43% 4.34% 4.49% 4.59% 4.30% 4.07% 4.40% 4.29% Our Workforce Will be Empowered and Supported to Deliver Care in a Way That is Consistent With Our Values 95% ACFT Sickness Absence Rates - Short Term (less than 28 days) 1.58% 1.37% 1.41% 1.17% 1.34% 1.19% 1.35% 1.53% 1.73% 1.36% 95% ACFT Sickness Absence Rates - Long Term (more than 28 days) 3.39% 3.17% 3.02% 3.17% 3.15% 3.40% 2.95% 2.55% 2.67% 2.93% 100% L Percentage of Staff Having 'In-Date' Appraisal 59.08% 95% 62.80% 63.45% 62.48% 59.45% 64.90% 70.18% 73.65% 72.21% 71.50% 77.38% 100% N Statutory & Mandatory Training Compliance 80.52% 90% 79.85% 78.69% 78.80% 77.85% 79.87% 81.43% 83.29% 83.71% 84.39% 87.1% 2.39% March % March % L Staff Turnover Cumulative (excluding bank/fixed term) 9.63% <10% 0.79% 1.74% 2.81% 3.73% 4.74% 5.53% 6.35% 7.28% 8.04% 100% TDA % Registered Nurses 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% Indicator Type - N - National L - Local C - Contractual SHA - Strategic Health Authority SC - Social Care ACFT - Aspiring Community Foundation Trust * Data Completeness included from Month 9
100
101 Annex 3 - Quality Assessment - Lead Director - Rose Goodwin / December Data - Month 9 Domain Indicator Months Performance Target / Tolerance Compliant Percentage of Reported Incidents Classified as Serious Incidents 2.99% Compliance with Vulnerable Adults Quality Standards (Quarter 3) 89% 80% Number of Serious Incident Pressure Ulcers Reported (STEIS) 14 Target in development Number of incidents (causing harm or otherwise) per 1,000 direct / face-toface contacts 5.05 ACFT Benchmark Sep 13 Serious Incident Falls Reported (STEIS) Resulting in Severe Injury or Death 4 Target in development Falls per 1,000 inpatient occupied bed days 7.61 Target in development Safety Safety Thermometer - Percentage of no New Harms (Community Hospitals / Community Services) Safety Thermometer - Percentage of Harm Free Care (Community Hospitals / Community Services) 96.8% > 95% 91.3% > 95% Mixed Sex Accommodation (Single sex number of breaches) 0 0 Clostridium Difficile Number of avoidable incidents cumulative (# awaiting panel) YTD 2 / 2# <=8 Number of Never Events 0 0 MRSA Bacteraemia (Hospital associated) YTD 0 0 MRSA Screening on Admission (% screened on elective admission in month) 100% 95% Venous Thromboembolism (VTE) Screening 100% 100% CQC Compliance with no major impact actions identified Compliant Compliant Number of Coroners Regulation 28 received (Previously Coroner Rule 43's) 0 0 NHS Litigation Authority Failure to maintain, or certify a minimum published CNST level of 1.0 or have in place appropriate alternative arrangements Compliant Compliant WHO Surgical Checklist Compliance Compliant Compliant Effectiveness Certification Against Compliance With Requirements Regarding Access to Healthcare for People With a Learning Disability Compliant Compliant NICE Guidelines Compliance There were 116 new NICE guidelines issued in 2015/16. Since March 2013 there are 31 pieces of guidance that are relevant but partially complaint. A monthly report is sent to the Divisional Business Meetings that details the non-compliance for each Division, the current actions and expected compliance date so it can be monitored at these committees. Participation in National Audit Programme Compliant Compliant SSOTP Re-admission Rates (excluding daycases) 5.3% Net Promoter Score 97% 97% Complaints closed within timescales in accordance with the National NHS Complaint regulations 100% 100% Experience Do you feel that you have care and support which is directed by you and responsive to your needs? 97% 90% Quality Account Maintenance & Development Quality Account Development - The account is available on the Trust's website
102
103 ANNEX 5 - Self Certification Board Statement - Lead Director - Stuart Poynor - Chief Executive - November Submission - Month 8 The Partnership Trust Board is required to submit a self-assessment for each of the below 14 statements to confirm Trust compliance to the TDA on a monthly basis Reference Assessment Full Compliance Comment (Where criteria is not met) For Clinical Quality that: The Board is satisfied that, to the best of its knowledge and using its own processes and having had regard to the TDA s oversight model (supported by Care Quality Commission information, its own information on serious incidents, patterns of complaints, and including any further metrics it chooses to adopt), the trust has, and will keep in place, effective arrangements for the purpose of monitoring and continually improving the quality of healthcare provided to its patients The board is satisfied that plans in place are sufficient to ensure ongoing compliance with the Care Quality Commission s registration requirements. The board is satisfied that processes and procedures are in place to ensure all medical practitioners providing care on behalf of the trust have met the relevant registration and revalidation requirements The board is satisfied that the trust shall at all times remain a going concern, as defined by the most up to date accounting standards in force from time to time. Yes Yes Yes Yes For Governance that: 5 The board will ensure that the trust remains at all times compliant with the NTDA accountability framework and shows regard to the NHS Constitution at all times. Yes 6 All current key risks to compliance with the NTDA's Accountability Framework have been identified (raised either internally or by external audit and assessment bodies) and addressed or there are appropriate action plans in place to address the issues in a timely manner. Yes 7 The board has considered all likely future risks to compliance with the NTDA Accountability Framework and has reviewed appropriate evidence regarding the level of severity, likelihood of a breach occurring and the plans for mitigation of these risks to ensure continued compliance Yes 8 The necessary planning, performance management and corporate and clinical risk management processes and mitigation plans are in place to deliver the annual operating plan, including that all audit committee recommendations accepted by the board are implemented satisfactorily Yes 9 An Annual Governance Statement is in place, and the trust is compliant with the risk management and assurance framework requirements that support the Statement pursuant to the most up to date guidance from HM Treasury ( Yes 10 The Board is satisfied that plans in place are sufficient to ensure ongoing compliance with all existing targets as set out in the NTDA oversight model; and a commitment to comply with all known targets going forward No The Trust is currently in discussion with the TDA to agree a financial outturn that will ensure it is complaint with TDA requirements. 31st March The trust has achieved a minimum of Level 2 performance against the requirements of the Information Governance Toolkit. Yes The board will ensure that the trust will at all times operate effectively. This includes maintaining its register of interests, ensuring that there are no material conflicts of interest in the board of directors; and that all board positions are filled, or plans are in place to fill any vacancies. The board is satisfied that all executive and non-executive directors have the appropriate qualifications, experience and skills to discharge their functions effectively, including setting strategy, monitoring and managing performance and risks, and ensuring management capacity and capability The board is satisfied that: the management team has the capacity, capability and experience necessary to deliver the annual operating plan; and the management structure in place is adequate to deliver the annual operating plan. Yes Yes Yes
104
105 Annex 5 - Detailed analysis by exception 5.1. Delayed Transfers of Care SSOTP Community Hospitals 5.2. Delayed Transfers of Care Social Care 5.3. Reablement Outcomes 5.4. Reviews Weeks Breastfeeding Coverage 5.6. Hepatitis B Vaccination Rates
106 5.1 Delayed Transfers of Care SSOTP Community Hospitals Division Service Service Lead Performance Lead Specialist & Children s Hospitals Sue Pointon Matthew Beardmore Performance Indicator / Issue The percentage of occupied bed days occupied by patients that are a Delayed Transfer of Care (DToC). Background Current Performance RAG Causing Status Concern? Clinical Consequences Reputational R Y Contract ual No contractual target has been agreed for 2015/16. The TDA monitors the Partnership Trust against a Community Trust target of 7.5%. The specialist division monitors against a nominal 5% target. The DToC rate has risen in December. The monthly rate is 7.3% which equates to 622 DToC days (an increase of 10.9% on November s figure of 561 days). Of the 622 days, 385 days related to Stoke-on-Trent patients and 237 days related to Staffordshire patients. Statistical Analysis The following two tables provide detail of the levels of delays caused by the top 4 reasons. The first table splits the current month (December) by Stoke and Staffordshire. The second table provides a three month trend. This demonstrates the increase in delays is due to care packages, completion of assessments and further non acute NHS care. Fig. 1: Top 4 reasons for DToC days (December 2015) SOT Staffs Patient Choice Awaiting Completion of Assessment Awaiting Care Package in Own Home Further non acute NHS care Total Fig. 2: Top 4 reasons for DToC days three month trend Oct-15 Nov-15 Dec-15 Patient Choice Awaiting Completion of Assessment Awaiting Care Package in Own Home Further non acute NHS care Total
107 Fig. 3 provides detail on the attributable agency for all delays in month. Fig. 3: Attributable agency for all DToC days (December 2015) SOT Staffs NHS Social Care Both Total Fig. 4: Delays as a percentage of occupied bed days (chart and table) 12% Delays as a % of OBD's 10% 8% 6% 4% 2% 0% 3.4% 3.9% 4.2% 9.4% 10.7% 6.7% 6.4% 6.9% 7.3% Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar 2015/ /15 Apr May Jun Jul Aug Sep Oct Nov Dec DTOC Days Bed Days
108 Data Quality Assessment Data Quality Data Quality: Overall assessment of data completeness and accuracy based on the data quality drivers below: SD BP UT MC DE Data Quality Assessment (Full) Data Quality Assessment - DTOC.xl QI Key Issues Impacting on Performance Data Quality Drivers Systems Design (SD): The extent to which the system fit for the purpose of the service Business Processes (BP): The extent to which there are robust processes in place to enable data to be recorded accurately and consistently Understanding of requirements by front line staff (UT): The extent to which training is sufficient to ensure staff fully understand the use of and why data is being collected Management checks and feedback as part of episode closure (MC): The extent to which managers quality assure the work of practitioners and feedback to them Data extraction and analysis tools (DE): The extent to which data extraction tools and reports reflect an accurate picture of the information contained in the IT system Quality Indicators (QI): The extent to which the service the indicator relates to has embedded measures of data quality Issues Impact I1: Care package delays During December the number of care package delays has fluctuated but remains high with a peak in the 3 rd and 4 th weeks of the month approaching the Christmas period. These delays did reduce at the end of the month. There were a higher percentage of these delays attributed to Stoke local authority as opposed to County. Some capacity has been made available for Stoke patients with AMG agency to address this issue but this has not been consistently available to reduce community hospital delays and has been limited in capacity. The county authority continues to use their LIS service to support those with long waiting times for care packages or those only requiring simple packages. Both authorities have utilised interim placements for those waiting for care packages where appropriate e.g. Amberley Hs and Brighton House. However availability of these interim placements has also been limited. Prior to Christmas the teams did undertake the empty hospitals exercise to maximise the resources available for discharge prior to the holidays. This involved additional presence on the wards of senior staff from both health and social care. Acuity of the patients in the hospital beds remains high meaning that most care package requests are for complex packages e.g. X4 double care calls. I2: Choice delays The number of choice delays fell during December. The daily patient flow conference calls continue and these call focus on agreeing actions to resolve the choice delays. If these actions do not resolve issues then they are escalated to the Service Managers for support and advice. Service Managers and Social Care Team leaders continue to meet with patients/ families when these delays are escalated to them or when choice letters are issued as per policy. Discharge facilitators and Patient Flow Coordinators support this process. Individual cases are referred to the legal team for their support when required. This has become necessary on occasions when families refuse to look for alternative accommodation when their home of choice has no capacity or when families cannot agree on a home of choice. Court of protection has had to be instigated for 2 cases in order to move forward to discharge; however this is a lengthy process.
109 13: EMI Stay at Home scheme 14: Intermediate care at home I5: Provider availability/ capacity and assessment During the first few weeks of December there was an increase in delays due to capacity within the EMI scheme. In order to reduce these delays patients waiting were considered for interim placement in the EMI assessment beds e.g. Amberley House. However their capacity also diminished during December. There has been and increased demand for this service due to the increase in the number of patients with dementia needs in the community hospitals. During the run up to Christmas there was an increase in delays waiting for Intermediate Care Services in their own home. Capacity within the service was poor at this time. There remain a number of patients in December who have chosen a care home but are on a waiting list for availability in that home of choice. Some patients are on waiting lists for a multiple homes. Both health and social care teams work closely with families to signpost them to homes that have availability. However their capacity can change quickly. Availability of placements is particularly challenging for those with complex needs e.g. EMI nursing. Commissioners did initiate in December a scheme to reward care homes who came to assess and accepted patients into their care within 24 hours of assessment. However there remained some delays waiting for provider assessments. I6: CHC funded patients- In December there remained a number of patients waiting for care home placements or care packages who have full Continuing Healthcare funding in October. These patients are often near the end of life or have complex needs hence the impact of delays is high on both the patient and can be stressful for their families. Families often have a particular care home in mind in these circumstances if capacity is not available this has to be approached sensitively to minimise distress. Care homes with the ability to manage end of life care are also limited. Any patient waiting for a care package at the end of life is treated as a priority for capacity. The care home procurement system (ADAM) for those with CHC funding will be introduced on February 1 st. 17:Awaiting completion of social care assessment There has been an increase in the number of delays attributed to social care assessment during December. There is a high demand for social care assessment in the community hospitals and the capacity to complete these assessments within the 72hrs agreed in the New Care Act is challenging. These issues are escalated to social care team managers daily and resources are re-assigned where appropriate. We have agreed to re- look at our local processes in light of this. I8: Other delays There remain ad-hoc cases of housing or equipment delays. These are monitored closely and issues escalated so that prompt support can be obtained e.g. housing agencies. These delays are usually of short duration.
110 Key Improvement Actions Owner Sue Pointon Actions A1: Escalate care package delay issues to senior managers and commissioners when required to facilitate care agency provision A2: Daily patient flow conference calls to ensure that choice delays are closely monitored and agreed actions allocated to a named individual A3: Service Managers and Social Care Team leaders continue to meet with patients/ families when these delays are escalated to them or when choice letters are issued as per policy A3: Health and Social Care teams work closely with families to signpost them to homes that have availability A4: Proposed introduction of Matrix Dynamic Procurement System for CHC funded patients A5:Review of local processes for referral/notification to social care Issues addres sed I1 Delivery status Issues are raised when required. This process enabled AMG provision to be provided in October which has helped reduce the number of delays Deadline On-going RAG All In place B I2 In place B I3 In place B I4 Delay in implementation of the Matrix system now planned for January 2016.Update - now agreed for implementation on Feb 1 st. System is called ADAM. Training for our staff booked for 28 th January. 17 Earlier identification of the need for social care intervention January16 February 2016 G G R Improvement Trajectory Not applicable. The Partnership Trust remains below the nominal TDA target level of 7.5% Remaining Risks Owner Lisa Hulme Risk Impact Related issues R1: Increasing inability to match capacity of care packages in the community to demand for patients in community hospitals High I1, I4
111 5.2 delayed Transfers of Care Social Care Division Service Service Lead Performance Lead Trust Adult Social Care (ASC) Delayed Transfers of Care (DToC) Area Managers (North & South Divisions) Barrie Knox Performance Indicator / Issue Current Consequences DToC KPIs: E07 - % Number of Social Care and Joint Delayed Transfers of Care EPISODES: Average Per Month E07b - % as E07 Where Reason for Delay Was 'Completion of Assessment' E08 - % Number of Social Care and Joint Delayed Transfers of Care DAYS: Average Per Month E08b - % as E08 Where Reason for Delay Was 'Completion of Assessment' Background Performance Causing Concern? RAG Status Red Red Red Red Clinical Reputational Contract ual Yes Delayed Transfers of Care (DToC) represent a considerable burden on the combined health and social care economies. Patients are unable to be supported in their most suitable care package/environment owing to capacity restraints. The movement is from admitted to community based care. Excess emergency activity within health/social care economies, often experienced during situations of Winter pressures, exacerbate DToC occurrence by creating surges of demand. Statistical Analysis E07 % Number of Social Care and Joint Delayed Transfers of Care EPISODES: Average Per Month E08 - % Number of Social Care and Joint Delayed Transfers of Care DAYS: Average Per Month Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar 0 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Target Actual Performance Desired Improvement Realistic Trajectory Target Actual Performance Desired Improvement Realistic Trajectory E07b - % as E07 Where Reason for Delay Was 'Completion of Assessment' E08b - % as E08 Where Reason for Delay Was 'Completion of Assessment' Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar 0 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Target Actual Performance Desired Improvement Realistic Trajectory Target Actual Performance Desired Improvement Realistic Trajectory
112 Current KPI Performance (as at November 2015 reports are one month in arrears): E07: E07b: Target 37.5 Target 14.0 Actual 64.9 Actual /15 Outturn /15 Outturn 14.8 E08: E08b: Target 1,015 Target 300 Actual 1,691 Actual /15 Outturn 1,311 14/15 Outturn 301 Due to the difficulty in materially impacting performance due to market conditions, the intention is to stabilise performance rather than expect to make significant improvement in the short term across these indicators. Key Issues Impacting on Performance Issues I1 Capacity Restraints within Health & Social Care Provision I2 Care Act Compliant Reporting Impact With growing demand from demographic and acuity factors, the capability to meet demands is stretched over time. Where appropriate provision is unavailable DToCs will occur. The 2012 Health & Social Care Act heralded new standards for reporting DToC. These standards represented a change in reporting for SSoTP. Key Improvement Actions Owner(s) Area Managers Actions Issues addressed Delivery status A1 ASC Reviews Project I1 Reviews audit to ensure alignment of need and provision within ASC. Identified areas for reduced provision will free up capacity for more care packages to be brokered and for LIS team resources to be redirected towards reablement, thus reducing pressure within ASC which will prevent DToCs from taking place. A2 Emergency Planning I1 Substantial work with health and social care commissioners has been undertaken to put in place emergency/winter pressures schemes to provide additional capacity to prevent blockages. Additional funding has been earmarked to support these schemes, though its scale relative to likely demands is limited. A3 Reporting Updates I2 Work has been undertaken internally to update community hospital reporting to be compliant with Care Act requirements. In parallel, SSoTP has been liaising with SCC around data compliance to ensure that Deadline January 2016 March 2016 November 2015 RAG Amber Amber Amber
113 responsibilities and causation for DToCs can be identified. Following preliminary investigations in partnership with SCC, SSOTP is undertaking an extending analysis to standardise implementation to ensure that reporting is accurate and compliant. New date March 2016 Remaining Risks Owner(s) Area Managers Risk Impact Related issues R1 Reviews Project potential for unmet need to be identified rather than Medium I1 streamlining of existing packages thereby generating additional demands within the present funding/capacities. R2 Winter Pressures unusually severe weather patterns will create additional emergency pressures which will overcome planned resources/schemes. Medium I1
114 5.3 Reablement Outcomes Division Service Service Lead Performance Lead Trust Adult Social Care (ASC) Reablement Area Managers (North & South Divisions) Edward Finnemore Performance Indicator / Issue Current Consequences Reablement KPIs D04a - % immediate outcome no/low level support D06b - % at home w/o on-going social care > 91 days Background Performance Causing Concern? RAG Status Red Red Clinical Reputati onal Contract ual Yes The reablement of social care clients is a key deliverable within the Trust s ASC strategy, being the major component to maintain and enhance individual capabilities in meeting their own social care needs. Successful reablement can therefore offset demands for social care provision. KPIs established with Staffordshire County Council (SCC) have sought to measure that success, in the case of D04a and D06b through the rates of clients receiving no/low support following reablement, and the numbers capable of staying at home after three months (91 days). Reablement performance has proved challenging to deliver over many years, and the performance levels for D04a and D06b have both experienced declining trends in recent months within 2015/16. Statistical Analysis
 14/15 Outturn 69.")
115 D04a: Percentage of people receiving reablement in the year, where the immediate outcome was no support or low level support. (ASCOF 2D) Target 72.0% Actual 63.0% (represents 579 service users of a total population of 919) 14/15 Outturn 69.1% D06b: Older people still at home and needing no on-going Social Care services 91 days following receipt of reablement services. Target 55.0% Actual 49.0% (represents 510 service users of a total population of 1,040) 14/15 Outturn 54.8% Data Quality Assessment Systems Design (SD): The extent to which the system fit for the purpose of the service Business Processes (BP): The extent to which there are robust processes in place to enable data to be recorded accurately and consistently Understanding of requirements by front line staff (UT): The extent to which training is sufficient to ensure staff fully understand the use of and why data is being collected Management checks and feedback as part of episode closure (MC): The extent to which managers quality assure the work of practitioners and feedback to them Data extraction and analysis tools (DE): The extent to which data extraction tools and reports reflect an accurate picture of the information contained in the IT system Quality Indicators (QI): The extent the service the indicator relates to has embedded measures of data quality
116 Overall DQ for Social Care Reablement is rated, as of January 2016, at 2.5 (of 5) which gives it an overall amber rating. The attached document provides the underlying assessment for ASC reviews across the six elements contained within the DQ analysis. Social Care Data Quality Assessment - R Key Issues Impacting on Performance Issues I1 Client Scope Impact Efficiency requirements inherent within the ASC contract require greater focus on reablement. More service users will therefore be supported through reablement however there will be an increasing trend for this group to require a level of support (increasing co-morbidities) to enable them to remain at home. Operational response and with reference to the Social Care Act has been to maximise opportunity for service users to undertake reablement program. This has the consequence that more service users will benefit from enablement opportunity however they may have the outcomes of community services at home with reduction on reliance of care placements or the outcome of a care placement. The operational preference to optimise overall outcomes rather than to restrictively pursue indicator performance impacts on performance. I2 Separation Inpatient Enablement Services I3 Internal Service Demarcation Health/Social Care/ Divisional I4 LIS Reablement Focus Issue is to ensure who is included in the cohort sample hospital discharge to enablement program not respite and assessment population. Remaining difficulties across health and ASC teams within the Trust. Specifically accessing therapeutic professional skills (especially physiotherapy). Need to breakdown barriers between Enablement and Intermediate Care teams in order to achieve improved results/sharing professional knowledge. Operational feel that North and South economies operate in parallel rather than concord, with opportunities for shared learning and potential efficiencies lost. 2015/16 operational pressures have resulted in LIS staff supporting maintenance packages rather than focusing purely on reablement. Key Improvement Actions Owner(s) Area Managers
117 Actions Issues addressed Delivery status A1 Hospital Discharge I1, I3 Improvements to discharge information Information being implemented. Impacts on ability to identify most appropriate patients for enablement. Working well with Discharge to Assess (D2A) completing health screen information within CD. Extracted data regarding hospital screening being reviewed for accuracy during January Service user opportunities for Reablement access to be reviewed by management. A2 ASC Reviews Project I1, I4 An analysis of ASC reviews will be undertaken in Autumn 2015 with a view to identifying potential package care provision reductions. Such a reduction will benefit both LIS Teams in being able to refocus back towards reablement, and the wider private marketplace in freeing provision capacity to be made available to other clients. Private sector, Able2, has been brought in to provide reviews capacity need to review quality and impact of the additional resource during Jan-Feb A3 Client Expectation I2 Operational need to continually ensure client expectations upon entering into reablement, to minimise potential for disengagement when exposed to full care clients. Brighton House service user expectation being managed through implementation of new admission information to clarify process and ensure full consent to reablement A4 Staff Communication across Community Services I3 programme. Implementing co-location of Intermediate Care and Enablement staff at Brighton House to bring together staff skills and promote joint working. Scheduled to start October Would benefit from being extended to ILCT/LIS staff, though the Trust estate is a practical restriction on implementation. Deadline March 2016 March 2016 January 2016 November 2015 RAG Amber Amber Completed Completed Remaining Risks Owner(s) Area Managers Risk Impact Related issues R1 Best Practice Learning Across Trust operationally feels as though there Medium I1, I3 are significant gaps between North and South Divisions silo working. Understanding across Areas within Division, but not between Divisions. R2 Continuing Capacity Restraints prevent release of staff to reablement from maintenance packages. Medium I4
118 5.4 Reviews Division Service Service Lead Performance Lead Trust Adult Social Care (ASC) - Reviews Christine Wheeler Edward Finnemore Performance Indicator / Issue Current Performance Consequences ASC Reviews: RAG Status Causing Concern? Clinical Reputational Contract ual J01d Percentage of long-term clients receiving any review (incorporates both J01d(i) community and J01d(ii) residential). Red Yes Background The performance indicators covering Reviews are split as follows: - J01d(i) percentage of long-term community-based clients receiving any review - J01d(ii) percentage of long-term residential-based clients receiving any review J01d represents the Trust s business as usual (BAU) objective for client reviews. Within the Q4 remainder of 2015/16 the Trust has been asked by Staffordshire County Council (SCC) to focus on the priorities of the Reviews Project which is being jointly undertaken between SSoTP and SCC. This focus will be prioritised over its BAU norm at least until March 2016, pending future re-evaluation of ASC review performance within Staffordshire. - Statistical Analysis Client Reviews are currently below target in the Trust for the latter element only and RAG rated as Red: J01d(i) December YTD Trust wide is currently 58.3% (represents 4,854 service users of a 7,446 total population). J01d(ii) December YTD Trust wide is currently 56.4% (represents 2,159 service users of a 3,608 total population). Please see overleaf for latest position shown graphically (December 2015 data). The current trajectory for both elements of Reviews suggest that the Trust will not achieve its target this year. As a result, an action plan has been formulated to ensure that the direction of travel improves to reach the required number of client reviews before the year end as well as contributing to local financial recovery plans. Key contributors to achieving this target include staff within the ILCTs and the CIS. For that reason, both Neighbourhood Managers and ISMs are operationally tasked with driving the required continuing improvements. For example, within the North Division, Newcastle has reorganised its staffing in all teams due to the Care Act and the demands on each team. It became apparent that annual reviews were not being completed in a timely way by the ILCTs and the Community Hospital teams. The reasons for this was due to the ILCTs holding complex cases whereby case work was prioritised based on risk and the pressure the hospital team face to ensure there is patient flow through the system. The other key issue is correct recording within Care Director. For numerous reasons, staff are still not completing this correctly and key areas have been supported by Performance to drill down into the detail to find solutions to this problem.


119 The current Trust Performance for Reviews on a 12 month rolling basis, as of December 2015, measured as per indicator J01d, all long-term clients with any review, is 63.4%. This represents 7,013 reviews within a total service user count of 11,054. The above graph shows the YTD performance which is now starting to move ahead of the established target threshold (70%), however, with SCC s focus on reviews there is now a working target of 100% of clients being reviewed. This is being delivered according to a set of review prioritisation criteria agreed with the Council. Data Quality Assessment Social Care Data Quality Assessment - R Systems Design (SD): The extent to which the system fit for the purpose of the service Business Processes (BP): The extent to which there are robust processes in place to enable data to be recorded accurately and consistently Understanding of requirements by front line staff (UT): The extent to which training is sufficient to ensure staff fully understand the use of and why data is being collected Management checks and feedback as part of episode closure (MC): The extent to which managers quality assure the work of practitioners and feedback to them Data extraction and analysis tools (DE): The extent to which data extraction tools and reports reflect an accurate picture of the information contained in the IT system Quality Indicators (QI): The extent to which the service the indicator relates to has embedded measures of data quality Overall DQ for Social Care Reviews is rated, as of January 2016, at 1.7 (of 5) which gives it an overall red rating. The attached document provides the underlying assessment for ASC reviews across the six elements
120 contained within the DQ analysis. Key Issues Impacting on Performance Issues Impact 1. Demand and Capacity Pressures Current demand exceeds capacity. Although staff have been transferred to the Review team there have been high levels of sickness and, in addition, two of the permanent staff members have been seconded to the Independent Review team. It was originally planned that the Review team would concentrate on the scheduled reviews where the case has been closed with services and the ILCT teams would focus on their key worked cases ensuring these are reviewed. If timely reviews are not held then service users may not be receiving the correct support required to meet their eligible needs. 2. Highly prescriptive recording systems (Care Director) This reduces the reported figures and doesn t reflect the which does not lend itself for staff to correctly and work completed by the teams, which in turn making it intuitively action the right areas, and produces difficult to action areas of poor performance and performance indicators which lack accuracy and recognise good areas for positive outcomes. confidence. Key Improvement Actions Owner Christine Wheeler Actions 1. Ensuring that review performance data on Care Director is captured correctly by all staff within the ILCT and CIS teams. It has become apparent that when completing reviews staff are entering the date into the required field for the next annual review date but are omitting to complete the information screen on Care Director which stipulates when the actual date of the review has occurred. Issues addres sed I2 Delivery status It has been discussed with all staff on the ILCTs that this field must be completed. They have been tasked a deadline date of 9/12/15 to review all of their open cases and ensure that the cases which they have reviewed have the field review date completed. This will increase the number of reviews completed by 130 for the district. Deadline RAG 10/1/2016 A Christine Wheeler is to meet with the Team leaders in CIS to ensure that the staff on their teams also complete this field. Ensuring that the data has been captured will form part of the pre closure checklist send to admin. 2. It has been identified that there are over 250 authorised Service Provisions that do not have a completed review date and a further 23 cases whereby the incorrect field has been completed and not the actual review date. I2 The list of these cases has been obtained and all of the cases will have the correct actual review date inputted on to the information screen on Care Director by the Team Attached Clerk. 20/12/15 A 3. Additional Review Team Recruitment and I1 The Review team have clear Ongoing G
121 Productivity 4. All members of the ILCTs to bring their list of key-worked cases to supervision. They need to demonstrate if the service user has been reviewed that, all of the correct fields have been completed in Care Director. If they have not reviewed the care received, then a plan needs to be agreed with the supervisor as to when they will be completed. This is to be a set agenda item in each person s supervision session. individual targets. A full time staff member should complete 40 reviews per calendar month. This is reviewed in monthly supervision sessions. The Team Attached clerk will record on a dedicated spreadsheet which reviews have been allocated and will update the spreadsheet once the review is completed and correctly recorded in Care Director. I1, I2 Monthly performance meetings are held with the Area Manager, Neighbourhood Managers, Team Leaders and Advanced Practitioners. Clear guidance has been given to all who supervise Social care staff about what is expected from supervision sessions in relation to performance issues. 31/12/15 A 5. Minimum Reviews Staff Target I1, I2 All team members to be allocated five reviews by the Team Attached clerks. These reviews will be kept on a spreadsheet which will be updated once the review has been completed and correctly recorded in Care Director. Target productivity for full time dedicated reviews staff to be 2 reviews per day, or 10 for the whole week. 5. Independent Review Team Monitoring and Engagement I1, I2 Monthly discussions with Wendy Snell to see what is being found in the areas where the pilot is taking place. 6. Monthly Monitoring of all reviews I1 To be on all meetings agenda in each team meeting, locality meeting and supervision sessions 7. Appointing additional Agency resource under Sandra Daniels to carry out targeted reviews between November and March 2016 I1 Project initiation and planning phase 30/01/16 A Ongoing G 31/10/15 G 01/11/15 G Remaining Risks Owner Sandra Daniels Risk Impact Related issues 1. Service users/patients require crisis management rather than a managed review due to lack of capacity. High 1
122 Weeks Breastfeeding Coverage Division Service Service Lead Performance Lead Specialist & Children s Health Visiting Pauline Evans (UNICEF Lead) Matthew Beardmore Performance Indicator / Issue Current Performance Consequences Breastfeeding data coverage 6-8 weeks after birth RAG Causing Clinical Reputational Contract (breastfeeding status of mother to be recorded at 6-8 week visit Status Concern? ual by health visitors). Accurate completion and return of 6-8 week breastfeeding data by health visitors (HV s) to child health to reach minimum target of 95% (NHS England target). Current performance data suggests that no teams within South Staffordshire are achieving this coverage rate, and performance is falling each quarter. Red Background GP s are commissioned to undertake a 6-8 week check of all new born babies, and the recording of the breastfeeding status is one of the questions in this 6-8 week check. The Health Visitor service is commissioned to help maintain the percentage of mums that are fully or partially breastfeeding between the Primary Visit and the 6-8 week check. This is measured by comparing the data at Primary Visit (collected by the Health Visitor) with the data collected by the Health Visitor on behalf of the GP at the 6-8 week check. Historically the 6-8 week data collection has not been formally put into a GP contract so Health Visitors have been tasked with collecting the data and returning to child health. The directive given to Health Visitors across the Partnership Trust is that when they complete height/weight measurements as part of the 6-8 week check, they are also requested to complete the breastfeeding status questions. In the North area (Stoke-on-Trent and North Staffordshire), this information is then directly input onto Trust information systems by Health Visitors. In Southern Staffordshire, the information is removed from the infant s red book and sent to the Health Informatics Service to input onto the Child Health system. 1
123 Statistical Analysis The following chart and table outline current performance for the Partnership Trust as a whole, and then by CCG area (as a proxy for Health Visiting teams). Fig. 1: Breastfeeding Coverage Rate (Summary) 100.0% 80.0% Breastfeeding Coverage Rate by by Quarter (2013/14 and 2014/15 YTD) 60.0% 40.0% 20.0% 91.4% 90.6% 89.5% 88.4% 90.7% 91.8% 89.4% 89.6% 77.4% 79.8% 0.0% Total Target Number of Infants with Breastfeeding Data Recorded Q1 13/14 Q2 13/14 Q3 13/14 Q4 13/14 Q1 14/15 Q2 14/15 Q3 14/15 Q4 14/15 Q1 15/16 Q2 15/16 2,639 2,759 2,749 2,562 2,717 2,761 2,699 2,511 2,225 2,358 Total Infants 2,890 3,048 3,075 2,901 2,996 3,007 3,018 2,802 2,873 2,955 Fig. 2: Breastfeeding coverage rate by CCG (rolling 5 quarters) Q2 2014/15 Q3 2014/15 Q4 2014/15 Q1 2015/16 Q2 2015/16 CCG Cannock Chase 83.1% 87.3% 85.4% 61.9% 64.3% East Staffordshire 84.9% 75.1% 75.4% 58.0% 61.7% North Staffordshire 100.0% 100.0% 100.0% 100.0% 100.0% Seisdon Peninsula 88.8% 87.1% 86.8% 60.3% 71.2% South East Staffs 82.7% 71.1% 74.9% 65.3% 58.7% Stafford and Surrounds 86.7% 87.8% 87.7% 58.9% 68.5% Stoke-on-Trent 100.0% 100.0% 100.0% 100.0% 100.0% Total 91.8% 89.4% 89.6% 77.4% 79.8% Target 95.0% 95.0% 95.0% 95.0% 95.0% 2
124 Data Quality Assessment Data Quality Data Quality: Overall assessment of data completeness and accuracy based on the data quality drivers below: Data Quality Drivers SD BP UT MC DE Data Quality Assessment (Full) Data Quality Assessment - Breastfe QI Key Issues Impacting on Performance Systems Design (SD): The extent to which the system fit for the purpose of the service Business Processes (BP): The extent to which there are robust processes in place to enable data to be recorded accurately and consistently Understanding of requirements by front line staff (UT): The extent to which training is sufficient to ensure staff fully understand the use of and why data is being collected Management checks and feedback as part of episode closure (MC): The extent to which managers quality assure the work of practitioners and feedback to them Data extraction and analysis tools (DE): The extent to which data extraction tools and reports reflect an accurate picture of the information contained in the IT system Quality Indicators (QI): The extent to which the service the indicator relates to has embedded measures of data quality Issues I1: Process for submission and coding of forms not working in South Staffordshire I2: Lack of direct control over data input for Health Visitors I3: Teams do not have staff-level reports to enable any performance issues to be investigated Impact Health Visiting teams are clear that they are sending all their forms through to the Health Informatics Service (HIS) and the HIS are clear that they are coding all forms they receive. However, performance rates suggest that this process is not working Therefore the process for coding needs to be reviewed Health Visiting teams in South Staffordshire are reliant on the HIS to input breastfeeding data on their behalf and therefore have no direct control over the data they collect being recorded on the Child Health system Breastfeeding status reports are set up and available at GP practice level, but do not provide individual staff member detail 3
125 Key Improvement Actions Owner Pauline Evans Actions A1: Assess feasibility of adding SNOMED codes to Lorenzo to enable direct input of breastfeeding data by Health Visitors A2: Assess whether an e-process could be introduced to transfer information A3: Team leaders to check existing breastfeeding status reports and investigate all instances where children do not have their breastfeeding status recorded with individual staff A4: Performance team to assess feasibility of setting up breastfeeding status reports to individual staff member level Issues Delivery addressed status I1, I2 Meeting took place on 5 th October at which this was discussed. This was followed up on 6 th November awaiting confirmation from IM&T of feasibility of SNOMED codes I1, I2 If A1 is deemed not to be feasible, this action will be explored. A similar issue was experienced in the community hospitals, and an e-process introduced, which could be adapted by Health Visitors I3 Reports are in place at GP practice level to enable Team Leaders to do this. Team leaders receive a reminder each month to check their data. I3 We have a current list of staff members aligned to GP practices but due to switch to geographical working awaiting new staff lists to set up reports. If status is directly input onto Child Health system via SNOMED or local codes, reports could be set up this way. Deadline RAG 30/11/2015 A 31/12/2015 (if required) In place 31/12/2015 New date 30/01/2016 A B A 4
126 Improvement Trajectory Based on the actions listed above, the graph below charts progress towards achieving the 95% data coverage target. Taking into account whichever process is used will be introduced during Q4, it is anticipated that it will not be fully embedded until Q2 2016/17, although improvements should be seen during Q4 2015/16 and Q1 2016/17. Fig. 3: Improvement trajectory for Breastfeeding data coverage 100.0% 90.0% 80.0% 70.0% 60.0% Commencement of new process during Q4 2015/16 Process fully embedded by Q2 2016/ % Actual Trajectory Target Remaining Risks Owner Ian Turner Risk Impact Related issues R1: Until a resolution is found, performance will continue to be poor. The Health Visiting service moved from NHS England to Local Authority commissioned in October. High I1, I2 5
127 5.6 Hepatitis B Vaccination Rates Division Service Service Lead Performance Lead Specialist & Children s Offender Healthcare Maggie Whitmore/ Nikki Black Matthew Beardmore Performance Indicator / Issue Current Performance Consequences Percentage of Hepatitis B vaccinations given within 31 days of reception RAG Status Causing Concern? Clinical Reputati onal Contract ual Background A Y The Hepatitis B vaccination rate was slightly below target in November at 79.9%. Had another two patients had a vaccination in-month, the target would have been achieved. This is the first time since July 2015 that the 80% target has not been achieved. The main issues this month have been at Brinsford and Werrington. In the case of the former establishment, there are challenges around the remand environment which means that offenders are not always within prison long enough to have the full course of vaccinations. At Werrington the drop in figures this month relates to a few people declining vaccination, but also a number of patients agreed but were transferred very quickly before injections could be given. Based on performance for the year to date it is anticipated that this is a one-off issue. Vaccination rates continue to be maintained or improve at all other establishments. Drake, Featherstone and Stafford, all achieved 80% or more in-month. The table in fig. 1 outlines the current vaccination rates with the number of patients applicable each month since April Based on overall performance over the past few months, and that all actions at each establishment have been implemented, and all other issues are outside control of the service, it is recommended that this improvement plan is closed. Statistical Analysis Fig. 1: Breakdown of Hep B achievement by month Number of new/transferred prisoners Number of new/transferred prisoners vaccinated with 31 days Number of prisoners already vaccinated Hepatitis B vaccine coverage for all new/transferred prisoners Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov % 77.0% 81.8% 76.6% 80.4% 80.1% 85.3% 79.9%
128 Fig. 2: Breakdown of Hep B achievement by month (April 2014 onwards) 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Overall Target Data Quality Assessment SD BP Data Quality UT MC DE Data Quality Assessment (Full) Data Quality Assessment - Hepatitis QI Data Quality: Overall assessment of data completeness and accuracy based on the data quality drivers below: Data Quality Drivers Systems Design (SD): The extent to which the system fit for the purpose of the service Business Processes (BP): The extent to which there are robust processes in place to enable data to be recorded accurately and consistently Understanding of requirements by front line staff (UT): The extent to which training is sufficient to ensure staff fully understand the use of and why data is being collected Management checks and feedback as part of episode closure (MC): The extent to which managers quality assure the work of practitioners and feedback to them Data extraction and analysis tools (DE): The extent to which data extraction tools and reports reflect an accurate picture of the information contained in the IT system Quality Indicators (QI): The extent to which the service the indicator relates to has embedded measures of data quality
129 Key Issues Impacting on Performance Issues HMP Featherstone I1: Low numbers of permanent staff to carry out Hep B vaccinations I2: Any new staff recruited may require training to carry out vaccinations I3: Training needed for all members of staff in one session to give maximum effect on waiting lists I4: E-training not accessible on Trust website as the site was being updated and therefore not available until September I5: New staff to SSOTP need face to face vaccine training instead of e-training as per infection control policy HMP Brinsford I6: A significant number of patients arriving at HMYOI Brinsford decline Hep B vaccination when offered at secondary screening Impact Recruitment and retention of nurses was very poor over a long period of time therefore agency staff were used in the department to ensure safe staffing levels. Agency staff were not up to date or trained in vaccinating patients so clinic waiting list for Hep B increased Permanent staffing levels increased however new staff did not vaccinate in previous roles therefore needed training in SSOTP vaccination procedures. Clinics had to be cancelled due to only 1 permanent member of staff available to vaccinate patients Experienced permanent staff need mandatory annual updates which they can usually access on-line. As they could not access e-training due to the website being closed for several months, their ability to vaccinate was removed and therefore clinic waiting lists increased as clinics had to be cancelled. As new nurses to SSOTP need to have face to face training instead of e-training, clinics had to be cancelled until face to face training could be arranged. Causes compliance issues as this impacts on the percentage of hep B vaccinations carried out Key Improvement Actions Owner Maggie Whitmore/ Nikki Black Action Issues addres sed Delivery status Deadline HMP Featherstone A1: 6 new staff recruited from May to July I1 Completed 31 st July 2015 A2: Training issues identified I2, I3, I4, I5 Completed 3 rd August 2015 A3: Vaccination trainer identified I3, I4, I5 Completed 3 rd August 2015 A4: Date of training arranged for the 11 th I1, I2, I3 Completed 3 rd August August 2015 A5: All staff advised to come in on days off I3, I5 Completed 3 rd August for training to ensure all staff trained on the 2015 day RAG B B B B B
130 Improvement Trajectory Based on the actions listed above and those from previous iterations of the plan, the graph below charts progress towards achieving the 95% data coverage target: Fig. 3: Improvement trajectory for Hepatitis B vaccination coverage 100.0% 95.0% 90.0% Training issues fully resolved at Featherstone 85.0% 80.0% 75.0% 70.0% 65.0% 60.0% Data recording issues resolved at Werrington Drop in figures at Werrington due to a number of patients being transferred very quickly before injections could be given Actual Trajectory Target Remaining Risks Owner Carol Adams Risk Impact Related issues R1: HMP Brinsford continues to have challenges related to the remand environment which can mean that patients can be transferred from the establishment prior to the full set of vaccinations being given High I2, I3
131 Enc 08 REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST TRUST BOARD MEETING TO BE HELD ON: 27 JANUARY 2016 Enclosure: Enclosure 08 Subject: Finance Report For Period Ending 31 December 2015 (Quarter 3) Strategic Goal: (tick as applicable) We will provide high quality and safe services which provide an excellent experience and best possible outcomes We will work with users and carers to deliver integrated services, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Director Lead: Jonathan Tringham Recommendation: For Approval & Assurance For Discussion For Information PURPOSE OF THE REPORT: The purpose of the report is to present to the Partnership Trust Board the Partnership Trust s financial performance at 31 December 2015 (Quarter 3), and to consider the financial outlook arising from this. KEY POINTS: The Partnership Trust is reporting an actual deficit of 6.651m at the end of Quarter 3, representing an adverse variance of 5.057m against an internal budgeted deficit to date of 1.595m. This compares to the planned financial position submitted to the Trust Development Authority (TDA) of 3.546m deficit at Quarter 3. Following two consecutive months of run-rate deficits in excess of 1m, Month 9 has shown anticipated improvement with an in-month deficit of 0.6m. The latest forecast outturn based upon the performance at Quarter 3, and status of recovery actions, would continue to give rise to a best case outcome of 4.1m, with a most likely scenario in the region of 6.1m. Page 1 of 10
132 Enc 08 The Partnership Trust has now received formal confirmation from the TDA that the capital to revenue funding proposition referred to the Partnership Trust Board last month will be transferred non-recurrently to the Partnership Trust, and will improve the financial position in accordance with discussions with the TDA Business Director. In essence, there will be an expectation that the Partnership Trust now achieves a 0.2m surplus (i.e. the best case 4.1m operating deficit less the 4.3m non-recurrent funding transfer ). It is imperative, therefore, that every opportunity is taken to maximise cost reduction / income maximisation in light of the remaining downward trend required to achieve this target, and contractual risks that may emerge over the final quarter. INTERDEPENDENCIES: Legal and/or Risk Clinical Financial HR Social Care Staff and Trade Union involvement actions undertaken/planned Patient & Public Involvement Equality Impact Information exempt from Disclosure Requirement for further review The key financial risks are identified within the report. The Partnership Trust s budgets need to support the delivery of Clinical Services. Failure to deliver within budget will result in deterioration in the Partnership Trust s financial position and resilience going forwards. The Partnership Trust will need to ensure that all staff with budget responsibility have the relevant training and support to discharge the duties delegated to them. This financial performance covers the whole of the Partnership Trust s activities. This report is for information. The budget supports the delivery of Services provided by the Partnership Trust, and where necessary these plans will have had Patient and Public Involvement. The budget supports the delivery of Services provided by the Partnership Trust, and where necessary these plans will have had an Equality Impact Assessment. This report is for information. Financial performance will be reviewed on a monthly basis. RECOMMENDATIONS: The Partnership Trust Board is asked to consider the financial performance of the Partnership Trust at the end of December 2015 (Quarter 3), the financial prospects for the remainder of the year, and note the approval of the capital to revenue transfer by the TDA. Page 2 of 10
133 Enc 08 POSITION OVERVIEW EBITDA The Partnership Trust's Earnings before Interest, Taxation, Depreciation and Amortisation (EBITDA) for the quarter ending 31 December 2015 shows a deficit of 2.146m (0.8%). This is 3.294m behind the revised plan of 1.148m surplus submitted to the NHS Trust Development Authority (TDA) to take account of the stretch target of 2.015m. INCOME & EXPENDITURE (I&E) POSITION The Partnership Trust's financial position at Quarter 3 is an actual deficit of 6.651m, representing an adverse variance of 5.057m against the internal YTD budget of 1.595m deficit. The Quarter 3 planned deficit submitted to the TDA represented 3.356m. EBITDA Deficit Cash Continuity of Service CIP Delivery Actual vs Plan Forecast vs Plan >5% favourable variance Up to 5% favourable variance On target Up to 5% adverse variance >5% adverse variance CASH The Partnership Trust has a cash balance of 11.5m at the end of December. This is a 4.0m shortfall against the year to date plan of 15.5m. The Partnership Trust is currently scoring a 3 for liquidity as per the Continuity of Services rating. CONTINUITY OF SERVICES RATING The Partnership Trust's overall Continuity of Services rating at Quarter 3 is 2.0, and remains in line with the target set out in the Annual Plan. COST IMPROVEMENT PLAN (CIP) The Partnership Trust has set an internal savings programme for Health services of 13.7m for 2015/16, with a planning estimate of 9.9m represented in the plan submitted to the TDA. The profile of CIP delivery is demonstrated in Appendix 1, and is compared to the TDA plan. The delivery of cash-releasing efficiency, along with the management of demand in Adult Social Care (ASC), have featured as the most critical factors in the financial prospects of the Partnership Trust. The deficit of 6.651m at Quarter 3 is attributable to demand and price pressures in Adult Social Care (ASC) of 3.4m, and a combination of CIP and demand pressures ( 3.3m) manifesting in the Health position, particularly in community hospitals. TEMPORARY STAFFING EXPENDITURE The Partnership Trust has spent m on temporary staff at the end of Quarter 3, comprising m agency staffing, and 2.526m bank staffing. Agency costs peaked between April and August, attributable in the main to the reopening of wards in community hospitals. However temporary staffing costs remain higher than levels experienced last year due to medical demand in Community Hospitals. Page 3 of 10
134 Enc 08 CONTINUITY OF SERVICES RATING METRIC Year to 31 December 2015 Rating Weight Weighted Score Liquidity Ratio Target % 1.5 (Days) Actual % 1.5 n/a (7) Capital Service Target % 0.5 Capacity (Times) Actual % 0.5 >1.25 n/a Risk Rating Target Actual Higher Score Lower Score The weighted score of 2.0 falls in line with the TDA plan score of 2.0, reflecting performance against the capital service capacity rating. ACCOUNTABILITY FRAMEWORK These metrics give an indication of whether there are financial risks within the Partnership Trust. They do not have a bearing on the Continuity of Service rating but are an element of the Partnership Trust's overall RAG rating. At Quarter 3, the Partnership Trust is rated as Red risk overall. The Partnership Trust at Quarter 3 is reporting an actual deficit of 6.651m representing an adverse variance of 3.115m against the TDA planned position of 3.536m deficit. The CIP is ahead of the revised TDA plan at Quarter 3, and accordingly is rating Green in this context. Accountability Framework M07 M08 M09 Forecast Outturn, Compared to Plan Year to Date, Actual compared to Plan Actual Efficiency Year to Date, Compared to Plan Forecast Efficiency, Compared to Plan Forecast Underlying Surplus / (Deficit) Compared to Plan Forecast Year End Charge to Capital Resource Limit Public Dividend Capital Accessed for Liquidity Purposes Forecast Achievement of Stretch Financial Performance Target Page 4 of 10
135 Enc 08 STATEMENT OF COMPREHENSIVE INCOME TO 31 DECEMBER 2015 m Budget Actual Variance Activity Income - Health Adult Social Care (0.6) Other Income Operating Income Pay Expenditure (130.5) (135.7) (5.2) Non-Pay Expenditure (140.6) (145.2) (4.6) Operating Expenditure (271.1) (280.9) (9.8) EBITDA 2.9 (2.1) (5.1) EBITDA % 1.1% (0.8%) Depreciation (2.5) (2.5) 0.0 Interest Received (0.0) Interest Payable (PFI) (1.3) (1.3) 0.0 Dividend (0.7) (0.7) 0.0 Retained Surplus / (Deficit) (1.6) (6.7) (5.1) I&E Surplus / (Deficit) % (0.6%) (2.4%) INCOME Overall, income at Quarter 3 is 4.7m in excess of the Partnership Trust s YTD budget, mostly attributable to short term funding streams in relation to system resilience together with pass through funding. EXPENDITURE Performance against operating budgets demonstrates not only the impact of the factors set out above, but reflects the tangible signs of stress in delivery of efficiency savings, and prevailing demand pressures across the health and social care landscape. I&E POSITION The Partnership Trust's I&E financial position at Quarter 3 shows an actual deficit of 6.651m, representing a 5.057m adverse variance against the YTD internal budget of 1.595m deficit. The position is heavily influenced by performance against the cost improvement plan (CIP), and increasingly as a result of pressures in the Adult Social Care contract and community hospitals particularly. Page 5 of 10
136 Enc 08 YEAR TO DATE SUMMARY This financial year has been difficult for most NHS bodies and local authorities nationally in facing up to public spending constraint and demographic pressures. Locally, it is a very challenging economy. The financial risks for the Partnership Trust, and direction of travel in performance, were highlighted early in the financial cycle, and this has allowed financial recovery action to make a significant improvement in prospects. Following two consecutive months of runrate deficits in excess of 1m, Month 9 has shown anticipated improvement with an in-month deficit of 0.6m. Pay spend has reduced, supported by assertive intervention in the procurement and governance of temporary staffing. In Adult Social Care (ASC), demand and market pressures remain a strong theme, and whilst non-recurrent actions have been developed to recover the position in 2015/16, the underlying run-rate remains a significant forward challenge for the partnership. Elsewhere, financial pressures continue to be characterised by strong demand and cost pressures, hardest felt in community hospitals. STATEMENT OF FINANCIAL POSITION SUMMARY Net assets as at the end of Quarter 3 are 51.1m. EBITDA The Partnership Trust has achieved an EBITDA margin deficit of 0.8% for the period to 31 December 2015 against the TDA planned surplus of 0.4%. FORECAST SUMMARY A review of the position at Quarter 3 has considered the direction of travel in pressures described earlier, progress in the development and delivery of further cash-releasing measures through the Cost Improvement Programme (CIP), financial recovery regime, and Adult Social Care (ASC) services. As highlighted earlier, performance at Quarter 3 has shown some anticipated improvement in recent run-rates with an in-month deficit of 0.6m. Financial prospects are considered more fully in the next section. However, achievement of a 4.1m deficit (prior to the capital to revenue funding now approved by the TDA of 4.3m) remains dependent upon delivery of best case scenarios in relation to financial recovery, and containment of contractual risks and underlying demand pressures, particularly in ASC services and community hospitals. CASH At 31 December 2015 the Partnership Trust had 11.5m of cash. The cash position is 4.0m behind the plan at Quarter 3. This is predominantly due to Creditors which were 5.8m lower than plan, partially offset by Capital Spend 2.5m behind plan, relating to slippage on Project Evolve. Page 6 of 10
137 Enc 08 STATEMENT OF FINANCIAL POSITION AS AT 31 DECEMBER 2015 m 31 December 2015 Land, Buildings and Equipment 87.5 Trade and Other Receivables (>1yr) 0.2 Total Non-Current Assets 87.7 Inventories 0.6 Trade and Other Receivables (<1yr) 17.8 Cash and Cash Equivalents 11.5 Total Current Assets 29.9 Trade and Other Payables (<1yr) (33.2) Provisions (<1yr) (0.1) Borrowings (<1yr) (0.8) Total Current Liabilities (34.2) Creditors (>1yr) 0.0 Provisions (>1yr) 0.0 Borrowings (>1yr) (34.8) Total Non-Current Liabilities (34.8) Net Assets 48.6 Public dividend capital 1.4 Revaluation reserve 17.6 Retained Earnings 29.6 Total Taxpayers' Equity 48.6 CAPITAL PROGRAMME CAPITAL PROGRAMME AS AT 31 DECEMBER 2015 k Plan Actual Variance Estates & Equipping (124) Information Tech 5,348 2,841 (2,507) Total 6,254 3,623 (2,631) Following approval by the Department of Health the Partnership Trust is transferring 4.3m of capital resource to revenue to support the I&E position. The Capital Resource Limit (CRL) for 2015/16 therefore has been reduced by 4.3m to 5.0m. This has been possible due to slippage in both Project Evolve and Estates schemes. The forecast position for Project Evolve accounts is 2.2m, IT Infrastructure 1.9m and Estates 0.9m. Capital spend for the remainder of the year is under close scrutiny to ensure accurate forecasting and delivery of spend in line with our CRL. Due to the change in go-live of Evolve a significant amount of spend has slipped into 2016/17. Page 7 of 10
138 Enc 08 FINANCIAL PROSPECTS A financial risk of up to 8.8m was articulated at Quarter 1, and initiated the development and leadership of a programme of financial recovery and risk containment. Prospects for further improvement from the current trajectory remain dependent upon delivery of best case scenarios in that programme of CIP savings, financial control and governance measures, maximisation of risk-share funding through negotiation, and exploitation of all financial flexibility available. The latest forecast outturn based upon the performance at Quarter 3, and status of recovery actions, would continue to give rise to a best case outcome of 4.1m, with a most likely scenario in the region of 6.1m. To deliver the best case scenario would require a positive outcome in relation to step-up / step-down negotiations with North Staffs commissioners and safeguarding of funding relating to the valuable winter resilience schemes (discharge to assess) approved in 2014/15. The Partnership Trust is clear this represented a recurrent commitment, but CCGs are yet to confirm this in payment and remains subject to their internal investigation. Previous experience tells us that further contractual pressures will inevitably materialise over the final stages of the financial year, and this, together with persistence in demand pressures for ASC and community hospitals, some uncertainty regarding risk-share funding, and the variable impact of financial recovery actions in the ASC area, reflects the spread in the forecast outcome at this stage. The table below provides a high level summary of the challenge. Page 8 of 10
139 Enc 08 SSOTP Financial Prospects - Movement & Analysis of Forecast Best case Forecast 4.1m Most Likely Forecast 6.1m Health ASC Total Health ASC Total m m m m m m Q3 Headline Projection Before Action Financial Recovery:- ASC Efficiency & Risk Share (4.5) (4.5) (3.5) (3.5) CIP Cash-Releasing (0.3) (0.3) (0.3) (0.3) Prescriptive Control of Discretionary Spend (0.3) (0.3) (0.3) (0.3) Agency Workforce Intervention (0.3) (0.3) (0.3) (0.3) Consolidation of Accounting Practice (1.0) (1.0) (1.0) (1.0) Contract Income Pressures:- Contract / Income Pressures NATIONAL CAPITAL TO REVENUE FUNDING OPTION Given the performance nationally, the TDA recently wrote to Trusts with a proposition for transferring any slippage in their capital resource limit (CRL) into revenue funding, on the basis that this would result in a pound for pound improvement in their Income & Expenditure positions. Given the current slippage in the capital programme of the Partnership Trust, this presented an opportunity of just under 4.3m. The Partnership Trust has now received formal confirmation from the TDA that this funding will be transferred non-recurrently to the Partnership Trust, and will improve the financial position in accordance with discussions with the TDA Business Director. In essence, there will be an expectation that the Partnership Trust achieves a 0.2m surplus (i.e. a best case 4.1m operating deficit less the 4.3m non-recurrent transfer. It is imperative that every opportunity is taken to maximise cost reduction / income maximisation in light of the remaining downward trend required, and the contractual risks emerging Page 9 of 10
140 Enc 08 APPENDIX 1: CIP PLAN v ACTUAL 10,000,000 Cumulative CIP Plan Vs Actual CIP Delivery 9,000,000 8,000,000 7,000,000 Amount 000's 6,000,000 5,000,000 4,000,000 Cumulative Actual Original TDA Cumulative Plan Revised TDA Cumulative Plan 3,000,000 2,000,000 1,000,000 - April May June July August September October November December January February March Month Page 10 of 10
141 Enc 09 REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD MEETING TO BE HELD ON: Wednesday 27 th January 2016 Enclosure: Subject: Responsible Officer Report Medical Appraisal Compliance and Revalidation Recommendations Quarter 3 (October December 2015) Strategic Goal (tick as appropriate): Director Lead: We will provide high quality and safe services which provide an excellent experience and best possible outcomes We will work with users and carers to deliver integrated services, simply and effectively Our organisation will develop and deliver sustainable, innovative services that support independence Our workforce will be empowered and supported to deliver care in a way that is consistent with our values We will make excellent use of our resources and improve levels of efficiency across our services Dr James Shipman, Medical Director Recommendation: For Approval & Assurance For Discussion For Information x PURPOSE OF THE REPORT: To provide the Partnership Trust Board with a quarterly update on medical appraisal compliance and Revalidation Recommendations KEY POINTS: This reporting process maintains quarterly communications between Responsible Officers at the local level and their higher-level Responsible Officers (NHS England), to whom they are linked, enabling a picture of high-level indicators (including appraisal rates) to be built up over the year, so that any problems can be identified and resolved at an early stage. The Annual Organisational Audit (AOA) will supersede the need for a quarterly report in the final quarter. Page 1 of 3
142 Enc 09 INTER DEPENDENCIES: Legal and/or Risk Clinical Financial HR Social Care Staff and Trade Union involvement actions undertaken/planned Patient & Public Involvement Equality Impact Information exempt from Disclosure Requirement for further review This is a legal requirement for the Partnership Trust to comply with the Medical Profession (Responsible Officers) Regulations Ensuring that doctors employed by the Trust meet the General Medical Council s fitness to practice standards provides a safe clinical environment within the services of the Partnership Trust. Failure to maintain high professional standards of care may result in significant financial liability to the Partnership Trust in terms of legal claims and settlements. The systems and processes to meet the legal requirements are managed through HR working with the Responsible Officer. No specific inter dependencies No specific involvement No specific involvement No negative impacts identified None Quarterly/Annual reporting RECOMMENDATIONS: The Partnership Trust Board is asked to review and accept the report. Page 2 of 3
143 Enc 09 Staffordshire and Stoke on Trent Partnership NHS Trust Medical Appraisal Compliance and Revalidation Recommendations Quarter 3 October to December 2015 Name of designated body: Staffordshire and Stoke-On-Trent Partnership NHS Trust Responsible Officer: Dr James Shipman, Medical Director No of doctors in the designated body as at 31 December 2015: 46 No of doctors due to hold appraisal meeting: 6 No of doctors who had appraisal meeting: 6 No of doctors who had deferment to next quarter: 0 No of doctors RO accepts postponement is reasonable: 0 No of doctors who had revalidation date due this quarter: 5 No of doctors who had revalidation recommendation: 5 No of doctors who had positive revalidation: 4 No of Doctors who had a recommendation to defer: 1 No of Doctors who had a recommendation of non-engagement: 0 Page 3 of 3
144
145 Evaluation of the Partnership Approach to Leadership Presentation to Trust Board on Wednesday 27 th January
146 Background Newly formed Partnership Trust wanted a bespoke model of leadership development There was requirement to design an approach that aligned to the Partnership Trusts vision, values and behaviours framework Sustainable internal leadership model that supported capacity and capability of all managers Project initiated to develop the leadership approach that the staff wanted Evaluation has been undertaken 12 months on to show what difference it has made
147 The Partnership Approach Implementation Gateway launched April-August managers attended 10 Masterclasses designed developed and delivered by internal staff across the Trust To date 820 staff attended the Gateway Delivery now on a monthly basis Leadership and Management essential 5 day programme 12 Master Classes are now in operation, and over 60 sessions currently scheduled for 2016
148 Level 4 what do staff say? Approximately one year since attending the Gateway, 98% of respondents are still using the models, tools and ideas in practice either some, a little or a lot We have more coaches now, if the environment was not right a good coach or counsellor would recognise that It seems like a long time ago now, but I am now really in a team of one (due to my role). I felt the gateway followed on with what I had done with the king s fund in terms of compassion, it does not always happen due to work pressures but it is what we should be aspiring to. The biggest thing I took from the day was that you have to think about yourself and remember you are the leader but think about yourself (position 1.2.3). We are all stressed and overworked and I do reflect back and think to take a step back, to think about things and to go again. Staff are struggling and you are the one to keep things buoyant.
149 Conclusion The evaluation demonstrates much positive feedback with the majority of colleagues advising that they are utilising the models, tools and ideas learnt on the Gateway. The Gateway gives clear expectations of how the Trust aspires to effective leadership behaviour. It gives a knowledge base to work from, and confirms leaders are managing staff according to the Trust Values. The Focus Group feedback has demonstrated that service users are always at the heart of the services and regardless of how staff may be feeling and they remain professional at all times. The Gateway will be reviewed to ensure it meets the diverse needs of the workforce and addresses the health and social care economy changes.


150 Sustainability The evaluation of the leadership programme has evidenced that we need to continue with a Trust wide programme that embraces current and new managers. The Partnership Initiative our resource centre for Organisational Health, will be the showcase for all Leadership Activity and will allow delivery of all Trust Strategies. All managers who have been recognised as Purple Person in the Talent Management framework, will automatically be put forward for all elements of the leadership Development programme. Operations and Corporate partners as part of Matrix working will be encouraged to support design, development and delivery of Masterclasses, Learn bites, and future leadership development interventions. Every team operations and corporate will be offered a team away day to identify training and development interventions that can support delivery of the business objectives
Trust Board Member Profiles. Non-Executive Directors. David Pearson MBE Chairman
 Trust Board Member Profiles Non-Executive Directors David Pearson MBE Chairman David Pearson was appointed Chairman of Staffordshire and Stoke on Trent Partnership NHS Trust from 6 June 2016. Prior to
Trust Board Member Profiles Non-Executive Directors David Pearson MBE Chairman David Pearson was appointed Chairman of Staffordshire and Stoke on Trent Partnership NHS Trust from 6 June 2016. Prior to
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
NHS England (London) Assurance of the BEH Clinical Strategy
 Assurance of the BEH Clinical Strategy") NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Reducing emergency admissions
 A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
Sponsoring director: Purpose: Decision Assurance For information Disclosable X Non-disclosable
 TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
EAST AND NORTH HERTFORDSHIRE NHS TRUST
 Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Guideline scope Intermediate care - including reablement
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
Inpatient and Community Mental Health Patient Surveys Report written by:
 2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
Job Title: Head of Patient &Public Engagement and Patient Services Directorate: Corporate Affairs Department: Patient and Public Engagement
 Job Description Job Title: Head of Patient &Public Engagement and Patient Services Directorate: Corporate Affairs Department: Patient and Public Engagement Grade 8b Tenure: Permanent Location of Post:
Job Description Job Title: Head of Patient &Public Engagement and Patient Services Directorate: Corporate Affairs Department: Patient and Public Engagement Grade 8b Tenure: Permanent Location of Post:
NHS East and North Hertfordshire Clinical Commissioning Group. Quality Committee. Terms of Reference Version 4.0
 NHS East and North Hertfordshire Clinical Commissioning Group Quality Committee Terms of Reference Version 4.0 1. Introduction 1.1 The Quality Committee (the committee) is established in accordance with
NHS East and North Hertfordshire Clinical Commissioning Group Quality Committee Terms of Reference Version 4.0 1. Introduction 1.1 The Quality Committee (the committee) is established in accordance with
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
Strategic KPI Report Performance to December 2017
 Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
Quality Strategy (Refreshed March 2015)
") Quality Strategy 2012-2017 (Refreshed March 2015) 1 Table of Contents 1. Executive Summary... 3 2. Drivers for improvement... 4 2.1 The Trust s ambition - vision and mission... 4 2.2 Corporate Strategy...
Quality Strategy 2012-2017 (Refreshed March 2015) 1 Table of Contents 1. Executive Summary... 3 2. Drivers for improvement... 4 2.1 The Trust s ambition - vision and mission... 4 2.2 Corporate Strategy...
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TITLE OF REPORT: Looked After Children Annual Report
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 13 Date of Meeting:..27 th October 2017.. TITLE OF REPORT: Looked After Children Annual Report 2016-2017 AUTHOR: Christine Dixon,
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 13 Date of Meeting:..27 th October 2017.. TITLE OF REPORT: Looked After Children Annual Report 2016-2017 AUTHOR: Christine Dixon,
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Improving patient access to general practice
 Report by the Comptroller and Auditor General Department of Health and NHS England Improving patient access to general practice HC 913 SESSION 2016-17 11 JANUARY 2017 4 Key facts Improving patient access
Report by the Comptroller and Auditor General Department of Health and NHS England Improving patient access to general practice HC 913 SESSION 2016-17 11 JANUARY 2017 4 Key facts Improving patient access
Halton. Local system review report Health and Wellbeing Board. Background and scope of the local system review. The review team
 Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
Growth in older people
 Agenda 1. Why create an Integrated Care Organisation (ICO)? 2. NHS vs Local Authority 3. Salford Together 4. Integrated Care Organisation 5. The Financial Negotiation 2 Why integration? -Number of people
Agenda 1. Why create an Integrated Care Organisation (ICO)? 2. NHS vs Local Authority 3. Salford Together 4. Integrated Care Organisation 5. The Financial Negotiation 2 Why integration? -Number of people
Solent. NHS Trust. Patient Experience Strategy Ensuring patients are at the forefront of all we do
 Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
Strategic Risk Report 1 March 2018
 Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Quality & Safety Sub-Committee
 Quality & Safety Sub-Committee Agenda Item QS/029/16 Date: 17/03/2016 Report Title FOIA Exemption Prepared by Presented by Action required Supporting Executive Director Safer Staffing No Exemption Janet
Quality & Safety Sub-Committee Agenda Item QS/029/16 Date: 17/03/2016 Report Title FOIA Exemption Prepared by Presented by Action required Supporting Executive Director Safer Staffing No Exemption Janet
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016
 NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
PATIENT AND SERVICE USER EXPERIENCE STRATEGY
 PATIENT AND SERVICE USER EXPERIENCE STRATEGY APRIL 2017 TO MARCH 2020 Date 24 March 2017 Version Final Version Previously considered by The Patient Experience Group version 0.1 draft The Executive Management
PATIENT AND SERVICE USER EXPERIENCE STRATEGY APRIL 2017 TO MARCH 2020 Date 24 March 2017 Version Final Version Previously considered by The Patient Experience Group version 0.1 draft The Executive Management
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Governance and Quality Committee Review. Wendy Pugh Director of Operations and Nursing. Innovation Tom Jinks - Governance Manager.
 Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY
 Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
102/14(ii) Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review
 Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review") Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Please indicate: For Decision For Information For Discussion X Executive Summary Summary
 Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
WOLVERHAMPTON CCG. Governing Body Meeting 9 th September 2014
 WOLVERHAMPTON CCG Governing Body Meeting 9 th September 2014 ` Agenda item:12 TITLE OF REPORT: REPORT PRESENTED BY: Title of Report: Purpose of Report: Commissioning Committee Summary Kamran Ahmed Update
WOLVERHAMPTON CCG Governing Body Meeting 9 th September 2014 ` Agenda item:12 TITLE OF REPORT: REPORT PRESENTED BY: Title of Report: Purpose of Report: Commissioning Committee Summary Kamran Ahmed Update
Board of Directors. Approval Discussion Information Assurance
 Report Title: Executive/NED Lead: Report author(s): Previously considered by: Board of Directors Tuesday, 31 October 17 Board Assurance Framework & Corporate Risk Register Ann Alderton, Company Secretary
Report Title: Executive/NED Lead: Report author(s): Previously considered by: Board of Directors Tuesday, 31 October 17 Board Assurance Framework & Corporate Risk Register Ann Alderton, Company Secretary
Commissioning and statutory funding arrangements for hospice and palliative care providers in England 2017
 Commissioning and statutory funding arrangements for hospice and palliative care providers in England 2017 Introduction Summary The statutory funding arrangements for adult hospices continue to raise serious
Commissioning and statutory funding arrangements for hospice and palliative care providers in England 2017 Introduction Summary The statutory funding arrangements for adult hospices continue to raise serious
INTEGRATION TRANSFORMATION FUND
 MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
Key facts and trends in acute care
 Factsheet November 2015 Key facts and trends in acute care Introduction Welcome to our factsheet giving an overview of major trends and challenges facing the acute sector. The information has been compiled
Factsheet November 2015 Key facts and trends in acute care Introduction Welcome to our factsheet giving an overview of major trends and challenges facing the acute sector. The information has been compiled
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Shetland NHS Board. Board Paper 2017/28
 Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality and Safety
 Minutes (confirmed) Subject Quality Committee Date 4 April 2017 Time 10.00am 12.30pm Venue Goodwood Room Chair Alison Lewis-Smith Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality
Minutes (confirmed) Subject Quality Committee Date 4 April 2017 Time 10.00am 12.30pm Venue Goodwood Room Chair Alison Lewis-Smith Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality
Primary Care Quality Assurance Framework (Medical Services)
") PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
QUALITY IMPROVEMENT COMMITTEE
 : 2016-002.a QUALITY IMPROVEMENT COMMITTEE Minutes of the meeting held on 11 th February 2016, Conference Room D, 1829 Building Present: Faulkner, Sarah (SF) (Chair) Lay Member, NHS West Cheshire CCG Cavanagh,
: 2016-002.a QUALITY IMPROVEMENT COMMITTEE Minutes of the meeting held on 11 th February 2016, Conference Room D, 1829 Building Present: Faulkner, Sarah (SF) (Chair) Lay Member, NHS West Cheshire CCG Cavanagh,
Thames Ambulance Service Ltd (TASL) Performance Report
 Performance Report") WEST LEICESTERSHIRE CLINICAL COMMISSIONING GROUP BOARD MEETING 8 th of May 2018 Title of the report: Section: Report by: Presented by: Thames Ambulance Service Ltd (TASL) Performance Report Public Joanna
WEST LEICESTERSHIRE CLINICAL COMMISSIONING GROUP BOARD MEETING 8 th of May 2018 Title of the report: Section: Report by: Presented by: Thames Ambulance Service Ltd (TASL) Performance Report Public Joanna
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
TRUST BOARD. Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director. Jo Hunter, Deputy Chief Nurse. Mary Heritage, Assistant Director of Quality
 TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
The Commissioning of Hospice Care in England in 2014/15 July 2014
 The Commissioning of Hospice Care in England in 2014/15 July 2014 Help the Hospices. Company limited by guarantee. Registered in England & Wales No. 2751549. Registered Charity in England and Wales No.
The Commissioning of Hospice Care in England in 2014/15 July 2014 Help the Hospices. Company limited by guarantee. Registered in England & Wales No. 2751549. Registered Charity in England and Wales No.
2020 Objectives July 2016
 ... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Performance Evaluation Report Gwynedd Council Social Services
 Performance Evaluation Report 2013 14 Gwynedd Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Gwynedd Council Social Services for the year
Performance Evaluation Report 2013 14 Gwynedd Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Gwynedd Council Social Services for the year
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST
 EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS DATE: 7 AUGUST 2015 SUBJECT: REPORT FROM: PURPOSE: CHIEF EXECUTIVE S REPORT CHIEF EXECUTIVE Decision CONTEXT / REVIEW HISTORY
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS DATE: 7 AUGUST 2015 SUBJECT: REPORT FROM: PURPOSE: CHIEF EXECUTIVE S REPORT CHIEF EXECUTIVE Decision CONTEXT / REVIEW HISTORY
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
Review of Inpatient Nursing Establishment, Capacity and Capability Review
 Appendix 2 Review of Inpatient Nursing Establishment, Capacity and Capability Review Mental Health Group September 2015 Review March 2016 Author: Heidi Cater, Head of Nursing, Mental Health Page 1 of 15
Appendix 2 Review of Inpatient Nursing Establishment, Capacity and Capability Review Mental Health Group September 2015 Review March 2016 Author: Heidi Cater, Head of Nursing, Mental Health Page 1 of 15
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
Agenda Item number: 9.1. Maggie Bayley, Director of Nursing and Quality
 Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
Report to the Board of Directors 2016/17
 Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
The new CQC approach to hospital inspection. Ann Ford Head of Hospital Inspection (North West) June 2014
 June 2014") The new CQC approach to hospital inspection Ann Ford Head of Hospital Inspection (North West) June 2014 1 Our purpose and role Our purpose We make sure health and social care services provide people with
The new CQC approach to hospital inspection Ann Ford Head of Hospital Inspection (North West) June 2014 1 Our purpose and role Our purpose We make sure health and social care services provide people with
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
Cabinet Member for Education, Children and Families
 Meeting Cabinet Resources Committee Date 24 September 2013 Subject Provision of therapies to Children with Special Educational Needs and placements to children in care Report of Summary Cabinet Member
Meeting Cabinet Resources Committee Date 24 September 2013 Subject Provision of therapies to Children with Special Educational Needs and placements to children in care Report of Summary Cabinet Member
Quality, Safety & Experience (QSE) Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph
 Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph") 1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST. Board Paper - Cover Sheet
 THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST Board Paper - Cover Sheet Date September 2017 Lead Director Report Title Nursing & Midwifery Staffing Three- Monthly Summary Nursing & Patient Services
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST Board Paper - Cover Sheet Date September 2017 Lead Director Report Title Nursing & Midwifery Staffing Three- Monthly Summary Nursing & Patient Services
Improving Mental Health Services in Bath & North East Somerset
 Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Quality Framework Supplemental
 Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Looked After Children Annual Report
 Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
NHS and independent ambulance services
 How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
LEARNING FROM DEATHS (Mortality Policy)
") LEARNING FROM DEATHS () Version: 1.0 Date issued: October 2017 Review date: September 2020 Applies to: All Clinical Staff Groups This document is available in other formats, including easy read summary
LEARNING FROM DEATHS () Version: 1.0 Date issued: October 2017 Review date: September 2020 Applies to: All Clinical Staff Groups This document is available in other formats, including easy read summary
NHS Nursing & Midwifery Strategy
 Colchester Hospital University NHS Foundation Trust NHS Nursing & Midwifery Strategy 2015-2018 Foreword Caring with Pride is our three-year Nursing & Midwifery Strategy for Colchester Hospital University
Colchester Hospital University NHS Foundation Trust NHS Nursing & Midwifery Strategy 2015-2018 Foreword Caring with Pride is our three-year Nursing & Midwifery Strategy for Colchester Hospital University
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
Welcome, Apologies for Absence and Declaration of Board Members Interest
 DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
Quality Assurance Committee Annual Report April 2017 March 2018
 Quality Assurance Committee Annual Report April 2017 March 2018 Quality Assurance Committee Annual Report April 2017 March 2018 1. Introduction The role of the quality assurance committee is to provide
Quality Assurance Committee Annual Report April 2017 March 2018 Quality Assurance Committee Annual Report April 2017 March 2018 1. Introduction The role of the quality assurance committee is to provide
ESHT Our ambition to be outstanding by 2020
 ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
Indicators for the Delivery of Safe, Effective and Compassionate Person Centred Service
 Inspections of Mental Health Hospitals and Mental Health Hospitals for People with a Learning Disability Indicators for the Delivery of Safe, Effective and Compassionate Person Centred Service 1 Our Vision,
Inspections of Mental Health Hospitals and Mental Health Hospitals for People with a Learning Disability Indicators for the Delivery of Safe, Effective and Compassionate Person Centred Service 1 Our Vision,
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
HERTFORDSHIRE COMMUNITY HEALTH SERVICES
 HERTFORDSHIRE COMMUNITY HEALTH SERVICES Minutes of the Hertfordshire Community Health Services Board Meeting Held on Thursday 22 nd July 2010 in the Boardroom, Howard Court Welwyn Garden City. Key Points
HERTFORDSHIRE COMMUNITY HEALTH SERVICES Minutes of the Hertfordshire Community Health Services Board Meeting Held on Thursday 22 nd July 2010 in the Boardroom, Howard Court Welwyn Garden City. Key Points
Health and wellbeing board Date of review: 4 8 September Background and scope of the local system review
 Stoke-on-Trent Local system review report Health and wellbeing board Date of review: 4 8 September 2017 Background and scope of the local system review This review has been carried out following a request
Stoke-on-Trent Local system review report Health and wellbeing board Date of review: 4 8 September 2017 Background and scope of the local system review This review has been carried out following a request
Report to Cabinet. 19 April Day Services for Older People (Key Decision Ref. No. SMBC1621) Social Care
 Social Care") Agenda Item 4 Report to Cabinet 19 April 2017 Subject: Presenting Cabinet Member: Day Services for Older People (Key Decision Ref. No. SMBC1621) Social Care 1. Summary Statement 1.1 On 18 May 2016, Cabinet
Agenda Item 4 Report to Cabinet 19 April 2017 Subject: Presenting Cabinet Member: Day Services for Older People (Key Decision Ref. No. SMBC1621) Social Care 1. Summary Statement 1.1 On 18 May 2016, Cabinet
Seven day hospital services: case study. South Warwickshire NHS Foundation Trust
 Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Clinical Assurance Toolkit (CAT) Strategy
 Strategy") The Newcastle upon Tyne Hospitals NHS Foundation Trust Clinical Assurance Toolkit (CAT) Strategy Effective: January 2014 Review: January 2015 1. Introduction The Trust s Nursing and Midwifery Strategy,
The Newcastle upon Tyne Hospitals NHS Foundation Trust Clinical Assurance Toolkit (CAT) Strategy Effective: January 2014 Review: January 2015 1. Introduction The Trust s Nursing and Midwifery Strategy,
THE SERVICES. A. Service Specifications (B1) Ian Diley (Suffolk County Council)
 Ian Diley (Suffolk County Council)") THE SERVICES A. Service Specifications (B1) Service Specification No. Service Early Supported Discharge for Stroke Patients v5.0 Commissioner Lead Dr Mark Lim, T Woor (Suffolk Stroke Review Project Board)
THE SERVICES A. Service Specifications (B1) Service Specification No. Service Early Supported Discharge for Stroke Patients v5.0 Commissioner Lead Dr Mark Lim, T Woor (Suffolk Stroke Review Project Board)
Best Care Clinical Strategy Principles for the next 10 years of Best Care. Dr Caroline Allum, Executive Medical Director
 Best Care Clinical Strategy 2017 2027 Principles for the next 10 years of Best Care Produced By: Produced For: Dr Caroline Allum, Executive Medical Director NELFT Board Date Produced: 17 th July 2017 Version:
Best Care Clinical Strategy 2017 2027 Principles for the next 10 years of Best Care Produced By: Produced For: Dr Caroline Allum, Executive Medical Director NELFT Board Date Produced: 17 th July 2017 Version:
Summary and Highlights
 Meeting: Trust Board Date: 23 November 2017 Agenda Item: TB/17-18/114 Boardpad ref:14 Agenda item Nursing Strategy Item from Attachments Summary and Highlights Mary Mumvuri Nursing Strategy This agenda
Meeting: Trust Board Date: 23 November 2017 Agenda Item: TB/17-18/114 Boardpad ref:14 Agenda item Nursing Strategy Item from Attachments Summary and Highlights Mary Mumvuri Nursing Strategy This agenda
Safeguarding Vulnerable People Annual Report
 Safeguarding Vulnerable People Annual Report 2014-2015 1. Purpose of report The purpose of this report is to provide assurance that the Trust is fulfilling its responsibilities to promote the safety and
Safeguarding Vulnerable People Annual Report 2014-2015 1. Purpose of report The purpose of this report is to provide assurance that the Trust is fulfilling its responsibilities to promote the safety and
Dudley & Walsall Mental Health Partnership NHS Trust Board
 Dudley & Walsall Mental Health Partnership NHS Trust Board Date of Board Meeting: 29 th July 2 Subject: Performance Corporate Dashboard Month 3 Trust Board Lead: Jacky O Sullivan, Director of Performance
Dudley & Walsall Mental Health Partnership NHS Trust Board Date of Board Meeting: 29 th July 2 Subject: Performance Corporate Dashboard Month 3 Trust Board Lead: Jacky O Sullivan, Director of Performance
OPERATIONAL PERFORMANCE REPORT: March Swindon Community Health Services Overview
 OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
Mental Health Crisis Pathway Analysis
 Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
NHS Trafford Clinical Commissioning Group (CCG) Annual General Meeting(AGM) 26th September
 Annual General Meeting(AGM) 26th September") RIGHT CARE RIGHT TIME RIGHT PLACE NHS Trafford Clinical Commissioning Group (CCG) Annual General Meeting(AGM) 26th September 2017 Introduction Matt Colledge Chair Introduction Trafford Clinical Commissioning
RIGHT CARE RIGHT TIME RIGHT PLACE NHS Trafford Clinical Commissioning Group (CCG) Annual General Meeting(AGM) 26th September 2017 Introduction Matt Colledge Chair Introduction Trafford Clinical Commissioning
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Allied Health Review Background Paper 19 June 2014
 Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY PART 1
 REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY PART 1 Date of Meeting: 24 September 2015 Agenda No: 8.2 Attachment: 14 Title of Document: South West London Collaborative Commissioning programme
REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY PART 1 Date of Meeting: 24 September 2015 Agenda No: 8.2 Attachment: 14 Title of Document: South West London Collaborative Commissioning programme
Calderdale and Huddersfield NHS Foundation Trust End of Life Care Strategy
 Calderdale and Huddersfield NHS Foundation Trust End of Life Care Strategy 2016-2017 Contents Acknowledgements Subject Page Number 1. Introduction 4 2. Vision 5 3. National policy Context 5-6 4. Local
Calderdale and Huddersfield NHS Foundation Trust End of Life Care Strategy 2016-2017 Contents Acknowledgements Subject Page Number 1. Introduction 4 2. Vision 5 3. National policy Context 5-6 4. Local