Office of Billing Compliance Coding, Billing & Documentation Department of Medicine Division of Cardiology
|
|
|
- Susan Quinn
- 6 years ago
- Views:
Transcription
1 Office of Billing Compliance Coding, Billing & Documentation 2016 Department of Medicine Division of Cardiology
2 Why Are We Here? To EDUCATE and PROTECT our providers and organization To provide your department/practice with every tool you need to maximize compliance and get paid what you deserve To update you on the latest CMS/OIG activities related to your specialty To give you confidence in your coding and documentation! 2
3 2016 Code Changes
4 Code Changes For 2016 Cardiovascular System New: CPT 477 replaced Category III code 0262T Transcatheter pulmonary valve implantation, includes procedure, angioplasty and imaging guidance, supervision and interpretation, when performed New: 7211 is for intracranial vessels New: 9401 (Mediastinoscopy with biopsy of mediastinal mass, when performed) and 9402 (Mediastinoscopy with lymph node biopsy, when performed) Revised: 7184, 7185, and 7186 were revised to include description nonintracranial vessels. Fluoroscopy is included. Deleted:
5 Intravascular Ultrasound IVUS codes The IVUS codes, 7250 and the add on code 7251 were deleted and replaced by codes 7252 and the add-on code 725. The biggest change is that the radiological guidance codes, previously separately billable, are now bundled. Additionally, the new codes include transducer placement and manipulation and are also included in IVC filter placement/repositioning/removal. CPT guidelines also state that if lesion extends across the margins of one vessel into another, only a single IVUS code is reported, despite imaging more that open vessel. CPT Code Description Comments 7252 Intravascular ultrasound (noncoronary vessel) during diagnostic evaluation and/or therapeutic intervention, including radiological supervision and interpretation; initial noncoronary vessel Replaces Each additional noncoronary vessel Replaces
6 Prolonged Services: 2016 UPDATE: Prolonged practitioner E/M or psychotherapy service(s) (beyond the typical service time of the primary E/M or psychotherapy service) in the office or other outpatient setting requiring direct patient contact beyond the usual service; first hour (List separately in addition to code for office or other outpatient E/M ( , , , ) or psychotherapy service 9087) Billed by physicians, ARNPs or PAs To bill practitioner prolonged codes must be > than 0 minutes associated with E/M 99415: Prolonged clinical staff service (the service beyond the typical service time) during an E/M service in the office or outpatient setting, direct patient contact with physician supervision; first hour (List separately in addition to code for outpatient E/M service) To bill clinical staff Prolonged codes, time starts at >45 minutes 99416: Prolonged clinical staff service (the service beyond the typical service time) during an E/M service in the office or outpatient setting, direct patient contact with physician supervision; each additional 0 minutes (List separately in addition to code for prolonged service) Do not bill with Do not bill or with NOTE: Document what you did and how long you did it. If you are billing additional procedures, document the time and note that they are excluded from the prolonged service so double-dipping is not questioned. OUTPATIENT ONLY. REGULATIONS PER CMS: The medical record must document by the practitioner to include the dated start and end times of the prolonged service. 6
7 Why Does Documentation Matter? IT S OUR AGREEMENT WITH MEDICARE AND OTHER INSURANCE COMPANIES CORRECT CODING PRACTICE IS PART OF GOOD MEDICAL CARE CIVIL AND CRIMINAL VIOLATIONS ARE HANDED DOWN EACH YEAR FOR CODING ERRORS MILLIONS OF DOLLARS ARE LOST EACH YEAR TO POOR CODING PRACTICES 7

8 Inpatient and Outpatient Evaluation and Management E/M Documentation and Coding 8

9 The Key Documentation Elements History Focus on HPI Physical Exam Medical Decision Making 9
10 Nuts and Bolts of E&M Coding THE THREE KEY DOCUMENTATION ELEMENTS MEDICAL DECISION-MAKING HISTORY PHYSICAL EXAM How does medical necessity fit into these components? Knowing the answer to this question will help you to select E/M codes and reduce audit risk. 10
11 Important! The Nature of the Presenting Problem (NPP) determines the level of documentation necessary for the service The level of care (E/M service) submitted must not exceed the level of care that is medically necessary SO... Medical Decision-Making and Medical Necessity related to the NPP determine the maximum E/M service. The amount of history and exam should NOT generally alone. 11
12 Medical Decision Making (MDM) DOCUMENT EVERYTHING THAT EFFECTS YOUR SERVICE TODAY!! Step 1: Step 2: Number of possible diagnoses and/or management options affecting todays visit. List each separately in A/P and address every diagnosis or management option from visit. Is the diagnosis and/or management options : New self-limiting: After the course of prescribed treatment it is anticipated that the diagnosis will no longer be exist (e.g. otitis, poison ivy, ) New diagnosis with follow-up or no follow-up: Diagnosis will remain next visit Established diagnosis that stable or worse Amount and/or complexity of data reviewed, diagnostic tests, and/or other information that must be obtained, reviewed, and analyzed. Labs, radiology, scans, EKGs etc. reviewed or ordered Review and summarization of old medical records or request old records Independent visualization of image, tracing or specimen itself (not simply review of report) Step : The risk of significant complications, morbidity, and/or mortality with the patient s problem(s), diagnostic procedure(s), and/or possible management options. # of chronic conditions and are the stable or exacerbated (mild or severe) Rxs ordered or renewed. Any Rx toxic with frequent monitoring? Procedures ordered and patient risk for procedure Note: The 2 most complex MDM steps out of the will determine the overall level of MDM 12
13 Medical Decision-Making 1. Number of Diagnoses or Treatment Options One or two stable problems? No further workup required? Improved from last visit? = LOWER COMPLEXITY Multiple active problems? New problem with additional workup? Are problems worse? = HIGHER COMPLEXITY 1
14 Medical Decision-Making 2. Amount/Complexity of Data Were lab/x-ray ordered or reviewed? Were other more detailed studies ordered? (Echo, PFTs, BMD, EMG/NCV, etc.) Did you review old records? Did you view images yourself? Discuss the patient with consultant? 14
15 Medical Decision-Making. Table of Risk Is the presenting problem self-limited? Are procedures required? Is there exacerbation of chronic illness? Is surgery or complicated management indicated? Are prescription medications being managed? 15
16 MDM Step : Risk Presenting Problem Diagnostic Procedure(s) Ordered Management Options Selected Min One self-limited / minor problem Low OP Level IP Sub 1 IP Initial 1 Mod OP Level 4 IP Sub 2 IP Initial 2 High OP Level 5 IP Sub IP Initial 2 or more self-limited/minor problems 1 stable chronic illness (controlled HTN) Acute uncomplicated illness / injury (simple sprain) 1 > chronic illness, mod. Exacerbation, progression or side effects of treatment 2 or more chronic illnesses Undiagnosed new problem w/uncertain prognosis Acute illness w/systemic symptoms (colitis) Acute complicated injury 1 > chronic illness, severe exacerbation, progression or side effects of treatment Acute or chronic illnesses that may pose threat to life or bodily function (acute MI) Abrupt change in neurologic status (TIA, seizure) Labs requiring venipuncture CXR EKG/ECG UA Physiologic tests not under stress (PFT) Non-CV imaging studies Superficial needle biopsies Labs requiring arterial puncture Skin biopsies Physiologic tests under stress (stress test) Diagnostic endoscopies w/out risk factors Deep incisional biopsies CV imaging w/contrast, no risk factors (arteriogram, cardiac cath) Obtain fluid from body cavity (lumbar puncture) CV imaging w/contrast, w/risk factors Cardiac electrophysiological tests Diagnostic endoscopies w/risk factors Rest Elastic bandages Gargles Superficial dressings OTC meds Minor surgery w/no identified risk factors PT, OT IV fluids w/out additives Prescription meds Minor surgery w/identified risk factors Elective major surgery w/out risk factors Therapeutic nuclear medicine IV fluids w/additives Closed treatment, FX / dislocation w/out manipulation Elective major surgery w/risk factors Emergency surgery Parenteral controlled substances Drug therapy monitoring for toxicity DNR
17 Medical Record Documentation CMS: Each medical record shall contain sufficient, accurate information to identify the patient, support the diagnosis, justify the treatment, document the course and results, and promote continuity of care among health care providers. 17
18 Medical Necessity Ignoring how medical decision-making affects E/M leveling can put you at risk. According to the Medicare Claims Processing Manual, chapter 12, section 0.6.1: Medical necessity of a service is the overarching criterion for payment in addition to the individual requirements of a CPT code. It would not be medically necessary or appropriate to bill a higher level of evaluation and management service when a lower level of service is warranted. The volume of documentation should not be the primary influence upon which a specific level of service is billed. Documentation should support the level of service reported. That is, a provider should not perform or order work (or bill a higher level of service) if it s not necessary, based on the nature of the presenting problem. 18
19 Medical Necessity The definitions of medical necessity are important, but it s how they get applied in the claims adjudication process that gives them shape. In other words, when it comes to selecting the appropriate level of care for any encounter, medical necessity trumps everything else, including the documentation of history, physical exam. For physicians this could mean that even bullet-proof documentation of these key components will not ensure protection if auditors find that the medical necessity is lacking. 19
20 Medical Necessity To ensure that the level of care you select matches the intrinsic medical necessity of the encounter, let the key component of medical decision making be your guide. Because it is based on the number and nature of the clinical problems as well as the risk to the patient, the complexity of your medical decision making may be a reliable surrogate for the vaguely defined concept of medical necessity. Practitioners often estimate the medical decision making early in the encounter before they start to document the history and exam. Let the medical decision making point you toward the appropriate code. 20
21 FOUR ELEMENTS of HISTORY Chief Complaint (CC:) History of Present Illness (HPI) location/quality/severity/duration/timing/context/ modifying factors/associated symptoms Review of Systems (ROS) Past/Family/Social History (PFSHx) 21
22 History 1. Chief Complaint Concise statement describing reason for encounter ( stomach pain,, follow-up diabetes ) Can be included in HPI IMPORTANT: The visit is not billable if Chief Complaint is not somewhere in the note Must be follow-up of 22
23 History - HPI 2. The HPI is a chronological description of the patient s illness or condition. The elements to define the HPI are: Location: Right lower quadrant, at the base of the neck, center of lower back Quality: Bright red, sharp stabbing, dull Severity: Worsening, improving, resolving Duration: Since last visit, for the past two months, lasting two hours Timing: Seldom, first thing in the morning, recurrent Context: When walking, fell down the stairs, patient was in an MVA Modifying Factors: Took Tylenol, applied cold compress: with relief/without relief Associated Signs and Symptoms: With nausea and vomiting, hot and flushed, red and itching TWO TYPES: BRIEF EXTENDED 1- elements above or status of 1-2 diagnosis or conditions 4 or > elements above or status of or > diagnosis or conditions 2
24 4. REVIEW OF SYSTEMS History - ROS 14 recognized: Constitutional Psych Eyes Respiratory ENT GI CV GU Skin MSK Neuro Endocrine Heme/Lymph Allergy/Immunology THREE TYPES: PROBLEM PERTINENT EXTENDED COMPLETE (1 SYSTEM) (2-9 SYSTEMS) (10 SYSTEMS) 24
25 History - PFSHx. PAST, FAMILY, AND SOCIAL HISTORY - Patient s previous illnesses, surgeries, and medications - Family history of important illnesses and hereditary conditions - Social history involving work, home issues, tobacco/alcohol/drug use, etc. TWO TYPES: PERTINENT: COMPLETE: 1 area (P, F or S) generally related to HPI All (P, F and S) for New patient and Initial Hospital or 2 of areas (P, F or S) for established pt. 25
26 History PEARLS FOR HISTORY DOCUMENTATION: Must have PAST/FAMILY/SOCIAL history for comprehensive history (ALL THREE) Don t forget 10-system review! You cannot charge higher than a level new or consult visit without COMPREHENSIVE HISTORY 26
27 Physical Examination 4 TYPES OF EXAMS Problem Focused (PF) Expanded Problem Focused (EPF) Detailed (D) Comprehensive (C) 27
28 Coding 1995: Physical Exam BODY AREAS (BA): Head, including face Neck Chest, including breast and axillae Abdomen Genitalia, groin, buttocks Back, including spine Each extremity CODING ORGAN SYSTEMS (OS): Constitutional/General Eyes Ears/Nose/Mouth/Throat Respiratory Cardiac GI GU Musculoskeletal Skin Neuro Psychiatric Hematologic/Lymphatic 28
29 1997 Sub-Specialty Physical Exam Cardiovascular Musculoskeletal Ears, Nose, Mouth and Throat Neurological Eyes Skin Psychiatric Genitourinary (Female) (Male) Respiratory Hematologic / Lymphatic / Immunologic General Multi-system Exam 29
30 Constitutional Eyes ENT & Mouth Neck Respiratory Cardiovascular Gastrointestinal (Abdomen) Musculoskeletal Extremities Skin Neurological/ Psychiatric CARDIOLOGY Examination Measurement of any three of the following seven vital signs: 1) sitting or standing blood pressure, 2) supine blood pressure, ) pulse rate and regularity, 4) respiration, 5) temperature, 6) height, 7) weight (May be measured and recorded by ancillary staff) General appearance of patient (eg, development, nutrition, body habitus, deformities, attention to grooming) Inspection of conjunctivae and lids (eg, xanthelasma) Inspection of teeth, gums and palate Inspection of oral mucosa with notation of presence of pallor or cyanosis Examination of jugular veins (eg, distension; a, v or cannon a waves) Examination of thyroid (eg, enlargement, tenderness, mass) Assessment of respiratory effort (eg, intercostal retractions, use of accessory muscles, diaphragmatic movement) Auscultation of lungs (eg, breath sounds, adventitious sounds, rubs) Palpation of heart (eg, location, size and forcefulness of the point of maximal impact; thrills; lifts; palpable S or S4) Auscultation of heart including sounds, abnormal sounds and murmurs Measurement of blood pressure in two or more extremities when indicated (eg, aortic dissection, coarctation) Examination of: Carotid arteries (eg, waveform, pulse amplitude, bruits, apical-carotid delay) Abdominal aorta (eg, size, bruits) Femoral arteries (eg, pulse amplitude, bruits) Pedal pulses (eg, pulse amplitude) Extremities for peripheral edema and/or varicosities Examination of abdomen with notation of presence of masses or tenderness Examination of liver and spleen Obtain stool sample for occult blood from patients who are being considered for thrombolytic or anticoagulant therapy Examination of the back with notation of kyphosis or scoliosis Examination of gait with notation of ability to undergo exercise testing and/or participation in exercise programs Assessment of muscle strength and tone (eg, flaccid, cog wheel, spastic) with notation of any atrophy and abnormal movements Inspection and palpation of digits and nails (eg, clubbing, cyanosis, inflammation, petechiae, ischemia, infections, Osler s nodes) Inspection and/or palpation of skin and subcutaneous tissue (eg, stasis dermatitis, ulcers, scars, xanthomas) Brief assessment of mental status including Orientation to time, place and person, Mood and affect (eg, depression, anxiety, agitation) 0
31 New Patients Patient not seen by you or your billing group in the past three years (as outpatient or inpatient) 1
32 2
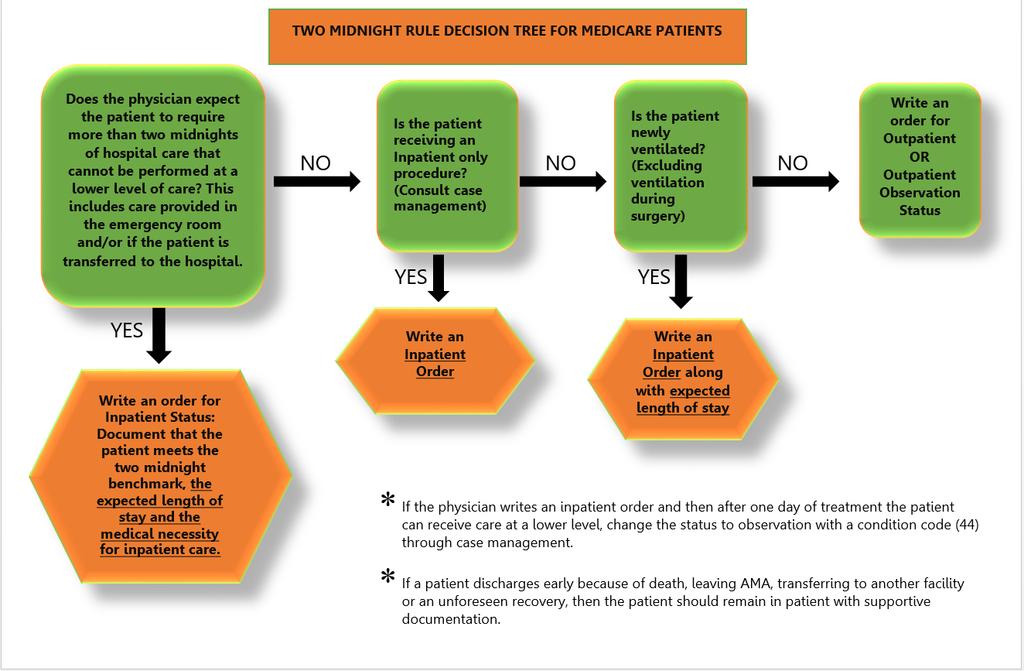
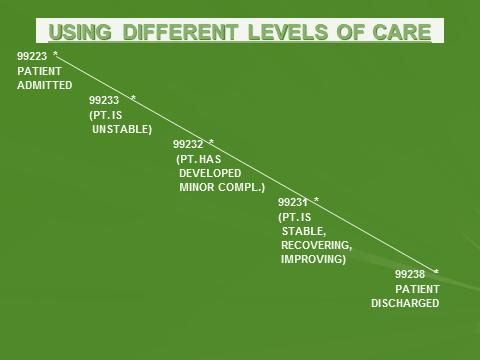
33 Subsequent Hospital Care Inpatient E/M Coding Inpatient Hospital Three levels of service: 9921, 9922, Stable, recovering, improving Problem focused history or exam Not responding, minor complication Expanded problem focused history or exam Very unstable, significant complications Detailed history or exam REMEMBER: What is medically necessary to document for that day?
34 Subsequent Hospital Visits Inpatient Hospital Medical Necessity should drive your documentation for each day s visit: What s wrong with this audit? Day 1: 9922 Day 2: 992 Day : 992 Day 4: 992 Day 5: 992 Day 6: 9929 (discharge to home) 4
35 Hospital Discharge IMPORTANT! Documentation should include: final examination of patient discharge instructions/follow-up preparation of referrals/prescriptions time spent If less than 0 minutes: 9928 If more than 0 minutes: 9929 (TIME must be documented) 5
36 6
37 Hospital Observation Services Admission/Discharge on different days: 99218: Detailed history/exam, low-complexity MDM 99219: Comprehensive history/exam, moderate MDM 99220: Comprehensive history/exam, high MDM 99217: Observation Discharge Admission/Discharge on same day: 9924: Detailed history/exam, low-complexity MDM 9925: Comprehensive history/exam, moderate MDM 9926: Comprehensive history/exam, high MDM Subsequent Observation: 99224, 99225, (New 2011) 7
38 Global Surgical Package Major Surgeries 90 days Miscellaneous Services Preoperative Services Supplies Intraoperative Services Postoperative Pain Management Complications after Surgery Postoperative Visits 8
39 Global Surgical Package NOT INCLUDED: Initial Consultation (57) Services of Other MDs (54, 55) Procedures/Visits Unrelated to Surgical Diagnosis (79, 24) Treatment that is NOT normal part of recovery Diagnostic Tests and Procedures Supplies Postoperative Pain Management Miscellaneous Services Postoperative Visits Preoperative Services Intraoperative Services Complications after Surgery Distinct surgical procedures not due to compx/reoperation (58) Return trip to OR/procedure for complications (78) Failed surgery requiring more extensive procedure Immunosuppressive Rx (24) Critical Care Services 9 (24)
40 Modifiers Indicate that a separate service or procedure has been performed by the same physician on the same day (2 CPT codes submitted) Medicare is monitoring these codes! Recent report from CMS: 5% of claims using modifier -25 did not meet requirements, resulting in $58 million dollars in improper payments You will be audited if you regularly use these codes! Ensure documentation supports the E/M and significant separate procedure. 40
41 Common Modifiers Modifier -25 Signifies visit or consultation for a SIGNIFICANT, SEPARATELY identifiable E/M service on the same day Example - A patient visits a cardiologist complaining of palpitations (Symptoms involving cardiovascular system; palpitations and light-headedness,general symptoms; dizziness and giddiness). The physicians performs a complete cardiac workup (for example, 9924 Office consultation for a new or established patient, which requires these three key components: a detailed history; a detailed examination; and medical decision making of low complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient s and/or family s needs. Usually, the presenting problem(s) are of moderate severity. Physicians typically spend 40 minutes face-to-face with the patient and/or family) and orders a same-day, in-office echocardiogram. You may bill both the echocardiogram and the same-day E/M in this case, using , Echocardiography, transthoracic, real-time with image documentation (2D) with or without M-mode recording; complete and You might also report additional Doppler echocardiography, pulsed wave and/or continuous wave with spectral display; complete (list separately in addition to codes for echocardiographic imaging) or Doppler echocardiography color flow velocity mapping (list separately in addition to codes for echocardiography), depending on the equipment and the images the physician obtained. Only after completing an E/M service would the physician make a decision to perform additional procedures (in this case, the echocardiography). 41
42 Common Modifiers Modifier-24 (Surgery modifier): Unrelated E/M service by the same physician during a post-op period Example: surgeon managing immunosuppression in transplant pt. Example: post-op TURP patient develops chest pain Example: Critical Care services which are UNRELATED to the surgery where a seriously injured or burned patient is critically ill 42
43 Common Modifiers Modifier -57 visit or consult on day of or day before a major surgery (90 days global period) when decision for surgery is made Modifier -59 two services performed at different anatomical sites on the same day on the same patient 4

44 Teaching Physicians (TP) Guidelines Billing Services When Working With Residents Fellows and Interns All Types of Services Involving a resident with a TP Requires Appropriate Attestations In EHR or Paper Charts To Bill 44
45 Evaluation and Management (E/M) E/M IP or OP: TP must personally document by a personally selected macro in the EMR or handwritten at least the following: That s/he was present and performed key portions of the service in the presence of or at a separate time from the resident; AND The participation of the teaching physician in the management of the patient. Initial Visit: I saw and evaluated the patient. I reviewed the resident s note and agree, except that the picture is more consistent with an upper respiratory infection not pneumonia. Will begin treatment with... Initial or Follow-up Visit: I saw and evaluated the patient. Discussed with resident and agree with resident s findings and plan as documented in the resident s note. Follow-up Visit: See resident s note for details. I saw and evaluated the patient and agree with the resident s finding and plans as written. Follow-up Visit: I saw and evaluated the patient. Agree with resident s note, but lower extremities are weaker, now /5; MRI of L/S Spine today. The documentation of the Teaching Physician must be patient specific. 45
46 Unacceptable TP Documentation Assessed and Agree Reviewed and Agree Co-signed Note Patient seen and examined and I agree with the note As documented by resident, I agree with the history, exam and assessment/plan 46
47 Evaluation and Management (E/M) Time Based E/M Services: The TP must be present and document for the period of time for which the claim is made. Examples : Critical Care Hospital Discharge (>0 minutes) or E/M codes where more than 50% of the TP time spent counseling or coordinating care Medical Student documentation for billing only counts for ROS and PFSH. All other contributions by the medical student must be re-performed and documented by a resident or teaching physician. 47
48 Minor (< 5 Minutes): For payment, a minor procedure billed by a TP requires that s/he is physically present during the entire procedure. Example: I was present for the entire procedure. Major (>5 Minutes) TP Guidelines for Procedures SINGLE Procedure / Surgery When the teaching surgeon is present or performs the procedure for a single non-overlapping case involving a resident, he/she or the resident can document the TP s physical presence and participation in the surgery. Example: I was present for the entire procedure (or key and critical portions & description of the key and critical portions of the procedure and immediately available). Endoscopy Procedures (excluding Endoscopic Surgery): TP must be present during the entire viewing for payment. The viewing begins with the insertion and ends with the removal. Viewing of the entire procedure through a monitor in another room does not meet the presence requirement. 48
49 Overlapping Surgeries: CMS Requires 2 Overlapping Surgeries - CMS will pay for two overlapping surgeries, but the teaching surgeon must be present during the critical or key portions of both operations. Consequently, the critical or key portions may not take place at the same time. The teaching surgeon must personally document in the medical record that he/she was physically present during the critical or key portion(s) of both procedures When a TP is not present during non-critical or non-key portions of the procedure and is participating in another surgical procedure, he or she must arrange for another qualified attending surgeon to immediately assist the resident in the other case should the need arise (this cannot be a resident or fellow.) In the case of concurrent surgical procedures, the role of the teaching surgeon in each of the cases is classified as a supervisory service to the hospital rather than a physician service to an individual patient and is not payable under the physician fee schedule. MCM 15505(4)(a)(2) 49
50 High-Risk Procedures & Diagnostic Services 50 Complex or high-risk procedures: Requires personal (in person) supervision of its performance by a TP and is billable only when the TP is present with the resident for the entire procedure. These procedures typically include cardiac and other interventional services. Example: Dr. TP (or I) was present for the entire (identify procedure). Diagnostic services with an interpretation: If documented by a resident to be billed by a TP requires that s/he personally document that s/he personally reviewed the images, tracing, slides etc. and the resident s interpretation and either agrees with it or edits the findings. Example: I personally reviewed the films (and/or slides etc.) and agree with the resident s findings. 50
51 Orders Are Required For Any Diagnostic Procedure With a TC / 26 Modifier The CPT descriptions of documentation requirements for many ophthalmic diagnostic tests include the phrase, "... with interpretation and report." Once the appropriate individual has performed the test, you must document your interpretation of the results somewhere in the medical records. This doesn't have to be anything elaborate. It may merely be a brief phrase indicating if a test is "normal," "stable from a previous test" or "mild superior arcuate defect." 51
52 Critical Care
53 Critical Care: Medical Review Guidelines Providing medical care to a critically ill, injured, or post-operative patient qualifies as a critical care service only if both the illness or injury and the treatment being provided meet the requirements. Clinical Criterion A high probability of sudden, clinically significant or life threatening deterioration of the patient's condition which requires a high level of physician preparedness to intervene urgently Treatment Criterion Life or organ supporting interventions that require frequent assessment and manipulation by the physician. Withdrawal of or failure to initiate these interventions would result in sudden, clinically significant / life-threatening deterioration in the patient s condition. Time spent teaching or by residents may not be used in CC time and NPP time cannot be added to physician time. 5
54 For time based codes, the physician must document the total amount of time spent on any calendar day providing critical care services to a patient. This time may be noncontiguous. Absent exceptional circumstances, generally requiring the skills of different specialty providers, critical care billed by one provider cannot overlap in time with critical care provided by another provider. The time must be spent on the unit. It may include direct bedside care or time spent discussing the case with consultants or reviewing pertinent laboratory or imaging data. 54
55 Time Based CC Codes and Time Codes < 0 min Appropriate E/M code 0-74 min x min x 1 and x min x 1 and x min x1 and x 55
56 Time-Based Critical Care One can also include time spent getting essential information from family members, but should not include minutes just updating the family on the patient s progress. Such conversations can be via telephone, but must be made from the unit in which the patient is cared for. A summary of such interactions should be entered into the medical record to support the total amount of time in critical care should be reported by a provider or subspecialty group only once in a calendar day. Critical care time < 0 min in a single day should be reported using the E/M codes
57 Critical Care Documentation & Criteria MM599 Related Change Request Number: 599 The TP documentation must include: Time the teaching physician spent providing critical care (resident time and time teaching residents does not count toward the 0 minute minimum); That the patient was critically ill during the time the TP saw the patient (met clinical criterion of a high probability of sudden, clinically significant or life threatening deterioration of the patient's condition ); What made the patient critically ill; and The nature of the treatment and management provided by the TP (treatment criterion of Life or organ supporting interventions that require frequent assessment and manipulation by the physician.) Combination of the TP's documentation and the resident s may support CC provided that all requirements for CC services are met. The TP documentation may tie into the resident's documentation. The TP may refer to the resident s documentation for specific patient history, physical findings and medical assessment as long as additional TP documentation is included to support their CC time. 57
58 TP Critical Care Documentation CMS examples of acceptable TP documentation for critical care involving Resident. "Patient developed hypotension and hypoxia; I spent 45 minutes while the patient was in this condition providing fluids, pressor drugs and oxygen. I reviewed the resident's documentation and I agree with the resident's assessment and plan of care." 58
59 TP Critical Care Documentation Patient in CCU Patient Critically Ill (059 min.-74 min.) Patient Critically Ill (75min.- 104min.) Patient Unstable, but not Critically Ill E/M 992 Patient Transferred to Floor 9922 Patient Stable/Recovering E/M 9921 Patient Discharged
60 Top Ten Compliance Issues For Documenting in EMR 60
61 Documentation in EMR CMS IS WATCHING EMR DOCUMENTATION Once you sign your note, YOU ARE RESPONSIBLE FOR ITS CONTENT 61
62 Documentation in EMR Every exam component... Every time you copy forward Family/Social History... Every HPI and ROS item you document means YOU PERFORMED THEM ON THAT VISIT... If you document something you did not do... YOU ARE PUTTING YOURSELF AND THE INSTITUTION AT GREAT RISK! 62
63 Top Ten Compliance Rules for EMR 1. Use Copy Forward with caution Each visit is unique Cloned documentation is very obvious to auditors If you bring a note forward it MUST reflect the activity for the CURRENT VISIT with appropriate editing Strongly advise NOT copying forward HPI, Exam, and complete Assessment/Plan 6
64 NOTE 06/05/12 HPI States: She had a metastatic evaluation on Friday and we will review that together today NOTE 06/26/12 HPI States: She had a metastatic evaluation on Friday and we will review that together today. Here for 2 nd neoadj chemo for bilat breast cancer NOTE 08/06/12 HPI States: She had a metastatic evaluation on Friday and we will review that together today. Here for 4th neoadj chemo for bilat breast cancer 64
 Be judicious with Auto populate Consider Smart Templates")
65 Top Ten Compliance Rules for EMR 2. Don t dump irrelevant information into your note ( the 10-page follow-up note ) Be judicious with Auto populate Consider Smart Templates instead Marking Reviewed for PFSHx or labs is OK from Compliance standpoint (as long as you did it!) 65
66 Top Ten Compliance Rules for EMR. Never copy ANYTHING from one patient s record into another patient s note Self-explanatory 66
67 Top Ten Compliance Rules for EMR 4. Only Past/Family/Social History and Review of Systems may be used from a medical student or nurse s note Student or nurse may start the note Provider (resident or attending) must document HPI, Exam, and Assessment/Plan 67
68 Top Ten Compliance Rules for EMR 5. Never copy documentation from another provider without clearly identifying the original author Can be considered a false claim Not always easy to do better to avoid 68

69 Top Ten Compliance Rules for EMR 6. Utilize Approved Attestations for resident/fellow/mid-level provider notes Important that both providers are identified in the note Auto-Text makes this a 2-click process 69

70 Top Ten Compliance Rules for EMR 7. Be careful with pre-populated No or Negative templates Cautious with ROS and Exam Macros, Check-boxes, or Free Text are safer and more individualized 70
71 Top Ten Compliance Rules for EMR 8. Authenticate all documentation and orders per policy 48 hours for verbal orders 0 days for signed documentation 71
72 Top Ten Compliance Rules for EMR 9. Link diagnosis to each test ordered (lab, imaging, cardiographics, referral) Demonstrates Medical Necessity Know your covered diagnoses for your common labs 72
73 Top Ten Compliance Rules for EMR 10. Individualize every note with a focus on the HPI and Medical Decision Making Results is correct coding with the focus of an E/M selection on medical necessity 7
74 Redemption Tips for Copy and Paste Physicians 74
75 Copy/Paste Philosophy: Your note should reflect the reality of the visit for that day 75
76 Use Specific Dates Don t say Today, Tomorrow, or Yesterday Write specific dates, i.e., ID Consult recommends ceftriaxone through 9/, instead of six more days, which could be carried forward inaccurately Heparin stopped 6/20 due to bleeding will always be better than Heparin stopped yesterday, which can be carried forward in error 76
77 Use Past Tense Neuro status remains stable, will discontinue neuro checks can be copied forward in error Better Neuro checks stopped on 2/24 Added heparin on 4/26 uses past tense and specific date for better accuracy 77
78 Avoid the use of I Unless in Attestation Avoid personal pronouns except attestations I discussed code status with Ms. Smith and she requested to be DNR could be copied forward by someone else Code status discussed with Ms. Smith and she requested to be DNR will always be acceptable and true 78
79 Refresh/Update HPI Everyday Progressive cumulative daily HPIs become unreadable and cumbersome Temptation exists to add no new information If a previous HPI is needed, it is easily found in the EMR on a past note 79
80 Delete the Prior Review of Systems DO NOT COPY FORWARD REVIEW OF SYSTEMS! This leads to contradictions and inconsistency, and danger of documenting something you didn t do HPI Patient reports nausea this morning Templated ROS same day No nausea, no vomiting 80
81 Document the Exam ACTUALLY PERFORMED Always better to document fresh exam every day If copied forward or templated, review the exam closely and make corrections to items you did not perform Credibility is questioned when ear exam is documented every day, or when amputee has 2+ pulses in bilateral lower extremities 81
82 Avoid Routine Daily Labs and Vitals in Each Note These already exist in the EMR Summarize in the Assessment/Plan These can create unnecessary volumes of pages in notes each day Labs and imaging reports are not necessary for billing 82
83 Do Not Use Pending for Consult Requests Instead, put specific date requested: Cardiology consult requested /22 at 4pm This provides a legal safeguard in case of a poor outcome, as well as being accurate Pending can be copied forward for days in error 8
84 Copy / Paste Summary Copy/Paste can be a valuable tool for efficiency when used correctly There are major Compliance risks when used inappropriately, including potential fraud and abuse allegations, denial of hospital days, and adverse patient outcomes Make sure your note reflects the reality and accuracy of the service each day 84

85 Non-Physician Practitioners (NPP s) or Physician Extenders Who is a NPP? Physician Assistant (PA) Nurse Practitioner (NP) 85
86 NPP Agreements & Billing Options Collaborative agreement between the NPP and the group they are working with is required. The agreement extends to all physicians in the group. If the NPP is performing procedures it is recommended a physician confirm their competency with performance of the procedure. NPPs can bill independent under their own NPI # in all places-of-service and any service included in their State Scope of Practice. Supervision is general (available by phone) when billing under their own NPI number. Medicare and many private insurers credential NPPs to bill under their NPI. Some insurers pay 85% of the fee schedule when billing under the NPP and others pay 100% of the fee schedule. Incident-to in the office (POS 11) ONLY Shared visit in the hospital or hospital based clinic (POS 21, 22, 2) 86
87 Shared Visits The shared/split service is usually reported using the physician's NPI. When an E/M service is a shared encounter between a physician and a NPP, the service is considered to have been performed "incident to" if the requirements for "incident to" are met and the patient is an established patient and can be billed under the physician. If "incident to" requirements are not met for the shared/split E/M service, the service must be billed under the non-physician's NPI. Procedures CANNOT be billed shared 87
88 Shared Visits Between NPP and Physician Shared visits may be billed under the physician's name if and only if: 1. The physician provides a medically necessary face-to-face portion of the E/M encounter (even if it is later in the same day as the PA/ARNP's portion); and 2. The physician personally documents in the patient's record the details of their face-to-face portion of the E/M encounter with the patient. If the physician does not personally perform and personally and contemporaneously document their face-to-face portion of the E/M encounter with the patient, then the E/M encounter cannot be billed under the physician's name and must be billed under the NPP. The NPP MUST be an employee (or leased) to bill shared. Documentation from a hospital employed NPP may not be utilized to bill a service under the physician. 88
89 Bill Independently and Not Shared Billing Under The NPP NPI Does not require physician presence. Can evaluate and treat new conditions and new patients. Can perform all services under the state scope-of-practice. Can perform services within the approved collaborative agreement. Recommend physician establish competency criteria and demonstration of performance of procedures within the collaborative agreement between the NPP and physician. 89
90 INCIDENT TO Incident to services must be an integral part of the patient s treatment course Provided under the physician s direct personal supervision (Physician must be present in the office suite and be immediately available to provide assistance and direction throughout the time the services are being performed) Commonly rendered without charge (included in physician s professional services) Commonly furnished in a physician s office (not in a hospital setting) Auxiliary Personnel must be directly employed by the physician, physician group or entity that employs the physician or may be a leased employee 90
91 INCIDENT TO Established Patient Visits: Incident to Billing Requirements Incident-to services are those services commonly furnished in a physician s office that are incident to the professional services of a physician. Physician must personally perform an initial service for each new condition, make an initial diagnosis, and establish a treatment plan. Physician must personally perform subsequent services at a frequency that reflects his/her active participation in and management of the course of the treatment for each medical condition. Services must be performed under a physician s direct personal supervision: (Present in the office suite and immediately available to provide assistance and direction throughout the time the ancillary staff, ARNP, PA is performing the incident to services.) 91
92 Scribed Notes. Record entries made by a "scribe" should be made upon the direction of the physician. A scribe should be merely that, a person who writes what the physician dictates and does. This individual should not act independently or obtain any information independently except to ROS and PFSH. They cannot obtain the HPI, any portion of the PE or MDM. The scribe must note "written by xxxx, acting as scribe for Dr. yyyy." Then, Dr. yyyy indicating that the note accurately reflects work and decisions made by him/her and then authenticate with signature. It is inappropriate for an employee of the physician to round at one time and make entries in the record, and then for the physician to see the patient at a later time and note "agree with above ". AAMC does not support someone dictating as a scribe by an NPP, as scribing is over the shoulder immediate documenter with no services personally performed by the scriber. In this case, the physician should be dictating their own visit. Scribes can do EMRs under their own password. 92
93 Scribed Notes. Individuals can only create a scribe note in an EHR if they have their own password/access to the EHR for the scribe role. Documents scribed in the EHR must clearly identify the scribe s identity and authorship of the document in both the document and the audit trail. Scribes are required to notify the provider of any alerts in the EPIC System. Alerts must be addressed by the provider. Providers and scribes are required to document in compliance with all federal, state, and local laws, as well as with internal policy. Failure to comply with this policy may result in corrective and/or disciplinary action by the hospital and/or department under the University of Miami Medical Group disciplinary policies applicable. Verbal orders may neither be given to nor by scribes. Scribes may pend orders for providers based upon provider instructions. The following attestation must be entered by the scribe: Scribed for [Name of provider] for a visit with [patient name] by [Name of scribe] [date and time of entry]. The following attestation should be entered by provider when closing the encounter: I was present during the time with [patient name] was recorded. I have reviewed and verified the accuracy of the information which was performed by me. [Name of provider][date and time of entry]. 9
94 CASE SAMPLES 94
95 95
96 HIPAA, HITECH, PRIVACY AND SECURITY HIPAA, HITECH, Privacy & Security Health Insurance Portability and Accountability Act HIPAA Protect the privacy of a patient s personal health information Access information for business purposes only and only the records you need to complete your work. Notify Office of HIPAA Privacy and Security at if you become aware of a potential or actual inappropriate use or disclosure of PHI, including the sharing of user names or passwords. PHI is protected even after a patient s death!!! Never share your password with anyone and no one use someone else s password for any reason, ever even if instructed to do so. If asked to share a password, report immediately. If you haven t completed the HIPAA Privacy & Security Awareness on line CBL module, please do so as soon as possible by going to: training_office/learning/ulearn/ 96
97 HIPAA, HITECH, PRIVACY AND SECURITY HIPAA, HITECH, Privacy & Security Several breaches were discovered at the University of Miami, one of which has resulted in a class action suit. As a result, Fair Warning was implemented. What is Fair Warning? Fair Warning is a system that protects patient privacy in the Electronic Health Record by detecting patterns of violations of HIPAA rules, based on pre determined analytics. Fair Warning protects against identity theft, fraud and other crimes that compromise patient confidentiality and protects the institution against legal actions. Fair Warning is an initiative intended to reduce the cost and complexity of HIPAA auditing. UHealth has policies and procedures that serve to protect patient information (PHI) in oral, written, and electronic form. These are available on the Office of HIPAA Privacy & Security website: 97
98 Available Resources at University of Miami, UHealth and the Miller School of Medicine If you have any questions or concern regarding coding, billing, documentation, and regulatory requirements issues, please contact: Gemma Romillo, Assistant Vice President of Clinical Billing Compliance and HIPAA Privacy Officer; or Iliana De La Cruz, RMC, Director Office of Billing Compliance Phone: (05) Also available is The University s fraud and compliance hotline via the web at or toll-free at (24hours a day, seven days a week). Office of billing Compliance website: 98
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation Department of Medicine Division of Endocrinology
 Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016 Department of Medicine Division of Endocrinology Why Are We Here? To EDUCATE and PROTECT our providers and
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016 Department of Medicine Division of Endocrinology Why Are We Here? To EDUCATE and PROTECT our providers and
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation Department of Medicine, Division of Infectious Disease
 Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016 Department of Medicine, Division of Infectious Disease 2016 Code Changes 2 Medicine: Vaccines Deleted: 1 outdated
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016 Department of Medicine, Division of Infectious Disease 2016 Code Changes 2 Medicine: Vaccines Deleted: 1 outdated
Office of Billing Compliance Coding, Billing & Documentation Department of Medicine Division of Nephrology
 Office of Billing Compliance Coding, Billing & Documentation 2016 Department of Medicine Division of Nephrology Why Are We Here? To EDUCATE and PROTECT our providers and organization To provide your department/practice
Office of Billing Compliance Coding, Billing & Documentation 2016 Department of Medicine Division of Nephrology Why Are We Here? To EDUCATE and PROTECT our providers and organization To provide your department/practice
Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program. Medicine Cardiology
 Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program Medicine Cardiology Prepared by: Medical Compliance Services, Miller School of Medicine/University of Miami and
Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program Medicine Cardiology Prepared by: Medical Compliance Services, Miller School of Medicine/University of Miami and
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation Department of Urology
 Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016 Department of Urology 2016 Code Changes 2 Urinary System: Kidney Revised: 5087 deleted transnephric ureteral
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016 Department of Urology 2016 Code Changes 2 Urinary System: Kidney Revised: 5087 deleted transnephric ureteral
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC
 Service in RHC") How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
Evaluation and Management Auditing Back to the Basics. Objectives. Audit Start with the benchmarks CMS MEDPAR by specialty 4/22/2013
 Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Medical Necessity verses Medical Decision Making. Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC
 Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
NEXTGEN E&M CODING DEMONSTRATION
 NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
NEXTGEN E&M CODING DEMONSTRATION
 NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
Anthem Blue Cross and Blue Shield Commercial Professional Reimbursement Policy
 Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
E & M Coding. Welcome To The Digital Learning Center. Today s Presentation. Course Faculty. Beyond the Basics. Presented by
 Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
6/14/2017. Evaluation and Management Coding. Jeffrey D. Lehrman, DPM, FASPS, MAPWCA
 Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Documenting & Coding for Compliance
 Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
Evaluation & Management Documentation Training Tool
 Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table, which
Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table, which
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016
 Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016 Departments of General Internal Medicine, Geriatrics, Community Health Delivery System (CHDS), Kendall & UMHC/PAC
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016 Departments of General Internal Medicine, Geriatrics, Community Health Delivery System (CHDS), Kendall & UMHC/PAC
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation Department of Genetics
 Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2017 Department of Genetics Top Billed Non-E/M Codes CODE PROCEDURES UNITS 9780PR MED NUTR THER, SUBSQ, INDIV, EA
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2017 Department of Genetics Top Billed Non-E/M Codes CODE PROCEDURES UNITS 9780PR MED NUTR THER, SUBSQ, INDIV, EA
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule. Grace Wilson, RHIA
 Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Evaluation & Management Documentation Training Tool
 A MS Medicare Administrative ontractor Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest
A MS Medicare Administrative ontractor Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest
The World of Evaluation and Management Services and Supporting Documentation
 The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
Basic Teaching Physician Presence and Documentation
 Basic Teaching Physician Presence and Documentation Welcome to the Children s University Medical Group (CUMG) training on the Teaching Physician Presence and Documentation. The goal of this module is to
Basic Teaching Physician Presence and Documentation Welcome to the Children s University Medical Group (CUMG) training on the Teaching Physician Presence and Documentation. The goal of this module is to
Start with the Problem
 Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Welcome To The Digital Learning Center. Billing Compliance: Today s Presentation. Course Faculty. Presented by
 Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation Billing liance: Avoiding Fraud & Abuse in Your Medical/Surgical Practice Course
Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation Billing liance: Avoiding Fraud & Abuse in Your Medical/Surgical Practice Course
E/M: Coding Opportunities- Documentation is key
 E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
MEDICARE RULE FOR TEACHING PHYSICIANS Effective July 1, 1996.
 MEDICARE RULE F TEACHING PHYSICIANS Effective July 1, 1996. 1.0 GENERAL RULE: If a resident participates in a service provided in a teaching setting, the teaching physician may not bill Medicare for such
MEDICARE RULE F TEACHING PHYSICIANS Effective July 1, 1996. 1.0 GENERAL RULE: If a resident participates in a service provided in a teaching setting, the teaching physician may not bill Medicare for such
Evaluation and Management
 Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Care Transition Strategies: The 2013 Transition Care Management Codes
 Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
SPECIALTY TIP #13 Evaluation and Management (E&M)
") ICD- 10 SPECIALTY TIPS SPECIALTY TIP #13 Evaluation and Management (E&M) This topic is being addressed in our Specialty Tips series as most providers rate Evaluation and Management as one of the more challenging
ICD- 10 SPECIALTY TIPS SPECIALTY TIP #13 Evaluation and Management (E&M) This topic is being addressed in our Specialty Tips series as most providers rate Evaluation and Management as one of the more challenging
Transition Care Management Update: Practical Applications for 2016
 60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program. Hematology / Oncology
 Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program Hematology / Oncology Prepared by: Medical Compliance Services, Miller School of Medicine/University of Miami and
Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program Hematology / Oncology Prepared by: Medical Compliance Services, Miller School of Medicine/University of Miami and
9/17/2018. Critical to Practices
 Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Presented for the AAPC National Conference April 4, 2011
 Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Evaluation & Management
 Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Office of Billing Compliance 2015 Coding, Billing and Documentation Program. Department of Dermatology
 Office of Billing Compliance 2015 Coding, Billing and Documentation Program Department of Dermatology 2015 Code Changes Dermatology had no specific CPT code additions, revisions or deletions. 2 Documentation
Office of Billing Compliance 2015 Coding, Billing and Documentation Program Department of Dermatology 2015 Code Changes Dermatology had no specific CPT code additions, revisions or deletions. 2 Documentation
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
E/M Auditing: History is the Key
 E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
CODING vs AUDITING Does it all boil down to Medical Necessity?
 PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation
 A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
Office of Billing Compliance 2015 Coding, Billing and Documentation Program. Department of Pediatrics
 Office of Billing Compliance 2015 Coding, Billing and Documentation Program Department of Pediatrics 2015 Code Changes Pediatric Specific CPT Code Changes for 2015 2 New & Revised Codes New 9060 Influenza
Office of Billing Compliance 2015 Coding, Billing and Documentation Program Department of Pediatrics 2015 Code Changes Pediatric Specific CPT Code Changes for 2015 2 New & Revised Codes New 9060 Influenza
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
Medical Decision Making
 Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
Basics of Coding for Compliance. Health Systems Compliance Presented by JoAnn Martinez, CPC Compliance Educator
 Basics of Coding for Compliance Health Systems Compliance Presented by JoAnn Martinez, CPC Compliance Educator Documentation Best Practice Common Themes ICD-10 that support E/M & Procedure Coding Type
Basics of Coding for Compliance Health Systems Compliance Presented by JoAnn Martinez, CPC Compliance Educator Documentation Best Practice Common Themes ICD-10 that support E/M & Procedure Coding Type
Evaluation and Management Services Guide
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide November 2014 / ICN: 006764 PREFACE This guide is offered as a reference tool
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide November 2014 / ICN: 006764 PREFACE This guide is offered as a reference tool
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
Office of Compliance. Complete & Accurate Documentation Core Curriculum for GWU Residents
 Office of Compliance Complete & Accurate Documentation Core Curriculum for GWU Residents December 3, 2014 Medical Record The medical record tells the story of the patient from start to finish. If the story
Office of Compliance Complete & Accurate Documentation Core Curriculum for GWU Residents December 3, 2014 Medical Record The medical record tells the story of the patient from start to finish. If the story
Code Assignment & Validation
 Code Assignment & Validation Evaluation & Management Services Presenter Santa Allaire, RHIT, CCS, CPC, CIRCC, CEMC Disclaimer This presentation is for general education purposes only. The information contained
Code Assignment & Validation Evaluation & Management Services Presenter Santa Allaire, RHIT, CCS, CPC, CIRCC, CEMC Disclaimer This presentation is for general education purposes only. The information contained
POLICY AND PROCEDURE
 AND PROCEDURE NUMBER: 0020 PAGE NUMBER: 1 of 7 I. PURPOSE: To ensure compliance with Federal and State billing and documentation guidelines of all UMMG billing providers. II. SCOPE: University of Miami
AND PROCEDURE NUMBER: 0020 PAGE NUMBER: 1 of 7 I. PURPOSE: To ensure compliance with Federal and State billing and documentation guidelines of all UMMG billing providers. II. SCOPE: University of Miami
E/M Fast Finder. CPT only 2012 American Medical Association. 1 All Rights Reserved.
 E/M Fast Finder The E/M Fast Finder is a carry-along reference to assist in assigning the Evaluation and Management (E/M) codes that are part of the 99000 series of Current Procedural Terminology (CPT
E/M Fast Finder The E/M Fast Finder is a carry-along reference to assist in assigning the Evaluation and Management (E/M) codes that are part of the 99000 series of Current Procedural Terminology (CPT
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation Surgery - Miami Transplant Institute Surgeons
 Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016 Surgery - Miami Transplant Institute Surgeons Why Are We Here? To EDUCATE and PROTECT our providers and organization
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016 Surgery - Miami Transplant Institute Surgeons Why Are We Here? To EDUCATE and PROTECT our providers and organization
Telemedicine Guidance
 Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Advanced Evaluation and. AAPC Regional Conference Chicago 10/27/12
 Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
See the Time chapter for complete instructions on how to code using time as the controlling factor when selecting an E/M code.
 2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation Department of Anesthesiology
 Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016 Department of Anesthesiology Why Are We Here? To EDUCATE and PROTECT our providers and organization To provide
Medical Compliance Services Office of Billing Compliance Coding, Billing & Documentation 2016 Department of Anesthesiology Why Are We Here? To EDUCATE and PROTECT our providers and organization To provide
Office of Billing Compliance 2015 Coding, Billing and Documentation Program. Department of Radiation Oncology
 Office of Billing Compliance 2015 Coding, Billing and Documentation Program Department of Radiation Oncology 2015 Code Changes Radiation Therapy Code Revisions 2 2015 Radiation Therapy Code Revisions Not
Office of Billing Compliance 2015 Coding, Billing and Documentation Program Department of Radiation Oncology 2015 Code Changes Radiation Therapy Code Revisions 2 2015 Radiation Therapy Code Revisions Not
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
Electronic Health Records - Advantages and Pitfalls of Documentation
 Electronic Health Records - Advantages and Pitfalls of Documentation Kansas City, KS HCCA Regional Conference September 25, 2015 1:00 P.M. 2:00 P.M. Presented by: Cynthia A. Swanson, RN, CPC, CEMC, CHC,
Electronic Health Records - Advantages and Pitfalls of Documentation Kansas City, KS HCCA Regional Conference September 25, 2015 1:00 P.M. 2:00 P.M. Presented by: Cynthia A. Swanson, RN, CPC, CEMC, CHC,
Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program
 Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program Dermatology Prepared by: Medical Compliance Services, Miller School of Medicine/University of Miami and Compliance
Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program Dermatology Prepared by: Medical Compliance Services, Miller School of Medicine/University of Miami and Compliance
Compliance Advisory 3 A Challenge for the Electronic Health Record s of Academic Institutions : Purpose Background
 Compliance Advisory 3 A Challenge for the Electronic Health Records of Academic Institutions: Physicians combining documentation or using information documented by others when billing for a professional
Compliance Advisory 3 A Challenge for the Electronic Health Records of Academic Institutions: Physicians combining documentation or using information documented by others when billing for a professional
Evaluation & Management 101 for Clinicians
 Evaluation & Management 101 for Clinicians Kerin Draak, MSN, WHNP BC, CPC, CEMC, COBGC, CPC I System Director of Clinical & Financial Integration Hospital Sisters Health System This is the Full Title of
Evaluation & Management 101 for Clinicians Kerin Draak, MSN, WHNP BC, CPC, CEMC, COBGC, CPC I System Director of Clinical & Financial Integration Hospital Sisters Health System This is the Full Title of
How does one report the performance of both a screening mammogram on the right breast and a diagnostic on the left breast at the same encounter?
 1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
Are they coming to get you! Todd Thomas, CCS-P
 Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
9/17/2018. Place of Service Type of Service Patient Status
 Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
May Non-Physician Practitioner (NPP) Nurse Practitioners and Physician Assistants. Collaborating Together as a Team
 Nurse Practitioners and Physician Assistants. Collaborating Together as a Team") May 2015 Non-Physician Practitioner (NPP) Nurse Practitioners and Physician Assistants Collaborating Together as a Team What is a Non-Physician Practitioner (NPP) or Physician Extender } Physician Assistant
May 2015 Non-Physician Practitioner (NPP) Nurse Practitioners and Physician Assistants Collaborating Together as a Team What is a Non-Physician Practitioner (NPP) or Physician Extender } Physician Assistant
Critical Care What Makes this so Difficult
 Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES. SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION
 NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION Table of Contents GENERAL RULES AND INFORMATION... 3 MMIS MODIFIERS... 13 EVALUATION AND MANAGEMENT
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION Table of Contents GENERAL RULES AND INFORMATION... 3 MMIS MODIFIERS... 13 EVALUATION AND MANAGEMENT
EVALUATION & MANAGEMENT SERVICES CODING. Part I: What is an E&M? Where do you start? Jennifer Jones, CPC, CPC-I
 DOTHAN AL CHAPTER AAPC FALL WORKSHOP Friday November 17, 2017 REGISTRATION BEGINS AT 7:15 am PROGRAM TIME IS 8:00 am 12:30 pm Earn 4 CEU s for a Fee of only $50.00 per attendee (Snacks will be provided
DOTHAN AL CHAPTER AAPC FALL WORKSHOP Friday November 17, 2017 REGISTRATION BEGINS AT 7:15 am PROGRAM TIME IS 8:00 am 12:30 pm Earn 4 CEU s for a Fee of only $50.00 per attendee (Snacks will be provided
Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program. Radiation Oncology
 Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program Radiation Oncology Prepared by: Medical Compliance Services, Miller School of Medicine/University of Miami and Compliance
Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program Radiation Oncology Prepared by: Medical Compliance Services, Miller School of Medicine/University of Miami and Compliance
Office of Billing Compliance 2015 Coding, Billing and Documentation Program. Department of Neurosurgery
 Office of Billing Compliance 2015 Coding, Billing and Documentation Program Department of Neurosurgery 2015 Code Changes 2 New Codes For 2015 6202-05 Myelography via lumbar injection, including radiological
Office of Billing Compliance 2015 Coding, Billing and Documentation Program Department of Neurosurgery 2015 Code Changes 2 New Codes For 2015 6202-05 Myelography via lumbar injection, including radiological
Charting for Midwives. Getting Credit For the Work You Do
 Charting for Midwives Getting Credit For the Work You Do Moving Beyond S.O.A.P. The U.S. health care system is moving past fee-for-service billing. In the future, the providers will be reimbursed based
Charting for Midwives Getting Credit For the Work You Do Moving Beyond S.O.A.P. The U.S. health care system is moving past fee-for-service billing. In the future, the providers will be reimbursed based
Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC Disclaimer
 Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
How to Write a Medical Note for the. Foundations of Doctoring Course and Beyond: Demystifying the Focused (SOAP) Note
 Note") How to Write a Medical Note for the Foundations of Doctoring Course and Beyond: Demystifying the Focused (SOAP) Note and the Comprehensive (H&P) Note by Todd Guth, MD Overview of the Medical Note Medical
How to Write a Medical Note for the Foundations of Doctoring Course and Beyond: Demystifying the Focused (SOAP) Note and the Comprehensive (H&P) Note by Todd Guth, MD Overview of the Medical Note Medical
See the Time chapter for complete instructions regarding how to code using time as the controlling E/M factor.
 2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
Next Gen Training. Why is Next Gen So Important? Step-by-Step Vitals Entry Scenarios and Mock Work-ups
 Next Gen Training Why is Next Gen So Important? Step-by-Step Vitals Entry Scenarios and Mock Work-ups Why is Next Gen So Important? Better for the VFC: All the necessary info can be accessed from any VFC
Next Gen Training Why is Next Gen So Important? Step-by-Step Vitals Entry Scenarios and Mock Work-ups Why is Next Gen So Important? Better for the VFC: All the necessary info can be accessed from any VFC
E&M Coding Pitfalls Jill Young, CPC, CIMC, CEDC. Young Medical Consulting, LLC East Lansing, Michigan
 1 E&M Coding Pitfalls Jill Young, CPC, CIMC, CEDC Young Medical Consulting, LLC East Lansing, Michigan 2 Disclaimer This material is designed to offer basic information for coding and billing. The information
1 E&M Coding Pitfalls Jill Young, CPC, CIMC, CEDC Young Medical Consulting, LLC East Lansing, Michigan 2 Disclaimer This material is designed to offer basic information for coding and billing. The information
RVU KILLERS The Most Common Reimbursement Documentation Errors. Michael Granovsky MD CPC CEDC FACEP President LogixHealth
 RVU KILLERS The Most Common Reimbursement Documentation Errors Michael Granovsky MD CPC CEDC FACEP President LogixHealth Documentation-Why Does It Matter? Must communicate to the payer your concerns and
RVU KILLERS The Most Common Reimbursement Documentation Errors Michael Granovsky MD CPC CEDC FACEP President LogixHealth Documentation-Why Does It Matter? Must communicate to the payer your concerns and
Evaluation and Management Services
 Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice
 Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Modern Optometric Staff BILLING & CODING THE MEDICAL EYE EXAMINATION. I m From The Government. The HIPPA Act of And I m Here To Help
 BILLING & CODING THE MEDICAL EYE EXAMINATION Modern Optometric Staff Ask the right questions, take the right actions Follow HIPPA guidelines Craig Thomas, O.D. 3900 West Wheatland Road Dallas, Texas 75237
BILLING & CODING THE MEDICAL EYE EXAMINATION Modern Optometric Staff Ask the right questions, take the right actions Follow HIPPA guidelines Craig Thomas, O.D. 3900 West Wheatland Road Dallas, Texas 75237
OVERVIEW OF ESSENTIAL CHARTING ELEMENTS FOR THE EMERGENCY DEPARTMENT
 OVERVIEW OF ESSENTIAL CHARTING ELEMENTS FOR THE EMERGENCY DEPARTMENT ALL CHARTING NEEDS TO BE FINISHED AT THE END OF YOUR SHIFT PRIOR TO LEAVING THE ED IF YOU HAVE ANY QUESTIONS, ASK FOR HELP! All of the
OVERVIEW OF ESSENTIAL CHARTING ELEMENTS FOR THE EMERGENCY DEPARTMENT ALL CHARTING NEEDS TO BE FINISHED AT THE END OF YOUR SHIFT PRIOR TO LEAVING THE ED IF YOU HAVE ANY QUESTIONS, ASK FOR HELP! All of the
E-Learning Module M: Assessment Review
 E-Learning Module M: Assessment Review This Module requires the learner to have read Chapter 12 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised: August
E-Learning Module M: Assessment Review This Module requires the learner to have read Chapter 12 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised: August
Efficacy of Tympanostomy Tubes for Children with Recurrent Acute Otitis Media Randomization Phase
 CONSENT FOR A CHILD TO BE A SUBJECT IN MEDICAL RESEARCH AND AUTHORIZATION TO PERMIT THE USE AND SHARING OF IDENTIFIABLE MEDICAL INFORMATION FOR RESEARCH PURPOSES TITLE Efficacy of Tympanostomy Tubes for
CONSENT FOR A CHILD TO BE A SUBJECT IN MEDICAL RESEARCH AND AUTHORIZATION TO PERMIT THE USE AND SHARING OF IDENTIFIABLE MEDICAL INFORMATION FOR RESEARCH PURPOSES TITLE Efficacy of Tympanostomy Tubes for
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Exam. Jen Godreau, BA, CPC, CPEDC. Director of Development & Operations Supercoder.com January 2012
 Exam Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com January 2012 Agenda 1. Embrace the GRAY! 2. Put your clinical savvy to the TEST 3. Make your
Exam Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com January 2012 Agenda 1. Embrace the GRAY! 2. Put your clinical savvy to the TEST 3. Make your
Meet the Presenter. Welcome to PMI s Webinar Presentation. E/M Auditing - Telling an Accurate Patient Story. On the topic:
 Welcome to PMI s Webinar Presentation Brought to you by: Practice Management Institute pmimd.com Meet the Presenter On the topic: Pam Joslin, MM, CMC, CMIS, CMOM E/M Auditing - Telling an Accurate Patient
Welcome to PMI s Webinar Presentation Brought to you by: Practice Management Institute pmimd.com Meet the Presenter On the topic: Pam Joslin, MM, CMC, CMIS, CMOM E/M Auditing - Telling an Accurate Patient
Cloning and Other Compliance Risks in Electronic Medical Records
 Cloning and Other Compliance Risks in Electronic Medical Records Lori Laubach, Partner, Moss Adams LLP Catherine Wakefield, Vice President, Corporate Compliance and Internal Audit, MultiCare 1 AGENDA Basic
Cloning and Other Compliance Risks in Electronic Medical Records Lori Laubach, Partner, Moss Adams LLP Catherine Wakefield, Vice President, Corporate Compliance and Internal Audit, MultiCare 1 AGENDA Basic
Critical Care Services
 Critical Care Services MEHIMA Spring Meeting March 17, 2016 Dianne Rodrigue, PA, MHP, CCDS, CPC Disclaimer This presentation is for general education purposes only. The information contained in these materials
Critical Care Services MEHIMA Spring Meeting March 17, 2016 Dianne Rodrigue, PA, MHP, CCDS, CPC Disclaimer This presentation is for general education purposes only. The information contained in these materials
Office of Billing Compliance 2015 Coding, Billing and Documentation Program. Department of Psychiatry
 Office of Billing Compliance 2015 Coding, Billing and Documentation Program Department of Psychiatry 2015 Code Changes 2 Psychotherapy Services Added to Telehealth Procedure codes added to the list of
Office of Billing Compliance 2015 Coding, Billing and Documentation Program Department of Psychiatry 2015 Code Changes 2 Psychotherapy Services Added to Telehealth Procedure codes added to the list of
PATIENT INFORMATION. Address: Sex: City: State: address: Cell Phone: Home Phone: Work Phone: address: Cell Phone:
 PATIENT INFORMATION Name: _ DOB: _ Age: Address: _Sex: City: _ State: _ Zip: _ Email address: Cell Phone: _ Home Phone: Work Phone: _ Responsible Party (if different from above) Name: DOB: Address: E-mail:
PATIENT INFORMATION Name: _ DOB: _ Age: Address: _Sex: City: _ State: _ Zip: _ Email address: Cell Phone: _ Home Phone: Work Phone: _ Responsible Party (if different from above) Name: DOB: Address: E-mail:
Sec Disconnect Go to End Forward Sec Next Report Go To
 Effective 3/15/04 escription DICTATION SYSTEM FOR INPATIENT HISTORY & PHYSICALS, DISCHARGE SUMMARIES, DELIVERY (NORMAL) NOTES OPERATIVE REPORTS DIAL 3-4000 LISTEN FOR VERBAL PROMPTS. ENTER: First 5 digits
Effective 3/15/04 escription DICTATION SYSTEM FOR INPATIENT HISTORY & PHYSICALS, DISCHARGE SUMMARIES, DELIVERY (NORMAL) NOTES OPERATIVE REPORTS DIAL 3-4000 LISTEN FOR VERBAL PROMPTS. ENTER: First 5 digits
IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY
 Global Surgery Policy Number GLS03272013RP Approved By UnitedHealthcare Medicare Committee Current Approval Date 04/09/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
Global Surgery Policy Number GLS03272013RP Approved By UnitedHealthcare Medicare Committee Current Approval Date 04/09/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
follow-up for pneumonia
 Questions How long can I access the on demand version. Where can I ask questions after the webinar? Can the CC be used as an element of HPI? I have a co-worker who believes it cannot be used at all towards
Questions How long can I access the on demand version. Where can I ask questions after the webinar? Can the CC be used as an element of HPI? I have a co-worker who believes it cannot be used at all towards
Programming a Spinal Cord Neurostimulator
 Programming a Spinal Cord Neurostimulator August 10, 2017 My surgeon wants to bill 95972 for programming along with placement of a spinal neurostimulator. Isn t the programming inclusive to the surgical
Programming a Spinal Cord Neurostimulator August 10, 2017 My surgeon wants to bill 95972 for programming along with placement of a spinal neurostimulator. Isn t the programming inclusive to the surgical
Few non-clinical issues have created as
 from October 2001 How to Get All the 99214s You Deserve It s easier than you might think to get what s coming to you. Emily Hill, PA-C Few non-clinical issues have created as much controversy as the CPT
from October 2001 How to Get All the 99214s You Deserve It s easier than you might think to get what s coming to you. Emily Hill, PA-C Few non-clinical issues have created as much controversy as the CPT
Descriptions: Provider Type and Specialty
 Descriptions: Provider Type and Specialty PROVIDER TYPE/SPECIALTY ADULT PRIMARY CARE Provides care for adults by treating common health problems, performing check-ups and providing prevention services.
Descriptions: Provider Type and Specialty PROVIDER TYPE/SPECIALTY ADULT PRIMARY CARE Provides care for adults by treating common health problems, performing check-ups and providing prevention services.
Global Surgery Fact Sheet
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Global Surgery Fact Sheet Definition of a Global Surgical Package This fact sheet is designed to provide education on the
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Global Surgery Fact Sheet Definition of a Global Surgical Package This fact sheet is designed to provide education on the
Procedure Code Job Aid
 Procedure Code 99211 Job Aid Definition for 99211: Office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician. Usually,
Procedure Code 99211 Job Aid Definition for 99211: Office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician. Usually,
Getting paid properly requires a thorough knowledge of the rules.
 Selecting E/M Codes For Established Patients Getting paid properly requires a thorough knowledge of the rules. Kenneth F. Malkin, D.P.M. Bio: Dr. Malkin is a diplomate of the American Board of Quality
Selecting E/M Codes For Established Patients Getting paid properly requires a thorough knowledge of the rules. Kenneth F. Malkin, D.P.M. Bio: Dr. Malkin is a diplomate of the American Board of Quality