E&M Coding Pitfalls Jill Young, CPC, CIMC, CEDC. Young Medical Consulting, LLC East Lansing, Michigan
|
|
|
- Garey Valentine Johnston
- 5 years ago
- Views:
Transcription
1 1


2 E&M Coding Pitfalls Jill Young, CPC, CIMC, CEDC Young Medical Consulting, LLC East Lansing, Michigan 2
3 Disclaimer This material is designed to offer basic information for coding and billing. The information presented here is based on the experience, training, and interpretation of the author. Although the information has been carefully researched and checked for accuracy and completeness, the instructor does not accept any responsibility or liability with regard to errors, omissions, misuse, or misinterpretation. This handout is intended as an educational a guide and should not be considered a legal/consulting opinion 3

4 PitFall A hidden or unsuspected danger or difficulty Synonyms: Hazard Danger Risk Peril Difficulty 4
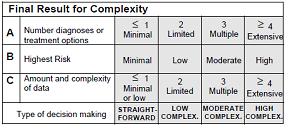
5 New Patient Office Level 4 and Level 5 Comprehensive History Comprehensive Exam Hospital Level 1 and Level 2 and Level 3 Comprehensive History Comprehensive Exam Medical Decision Making Determines the Level of Service 5
6 Comprehensive History History Of Present Illness (HPI) 4 items Since the onset of symptoms what has been going on What s wrong with the patient How bad? How long? What makes it better/worse? 1 other 6
7 Patient #1 A week ago, pt had a loss of consciousness while at home. He was taken to the hospital, diagnosed with a seizure disorder, presumably due to his previous MVA. He has been taking seizure medicine twice per day, but does not know the name of the med. He has not been driving, he has a follow up with neurology. 7
8 Patient #2 Pt presents for management of chronic/new conditions. She is doing well, denies chest pain shortness of breath, palpitations, dizziness/headaches or syncope. Exercising 3x per week for 30 minutes. Feels she eats healthy. In August she had a sore throat for quite a while. When she examined her throat she saw nodules on the tonsils. After a week they were not gone so she saw an ENT. ENT did a biopsy that came back lymphangioma. She obtained a second opinion from U of M and pathology came back the same. She needed no further treatment. 8
9 Comprehensive History Review Of Systems (ROS) 9+ items A complete ROS inquires about the system(s) directly related to the problem(s) identified in the HPI plus all additional body systems.!dg: At least ten organ systems must be reviewed. Those systems with positive or pertinent negative responses must be individually documented. For the remaining systems, a notation indicating all other systems are negative is permissible. In the absence of such a notation, at least ten systems must be individually documented. 9
10 Review of Systems (ROS) A problem pertinent ROS inquires about the system directly related to the problem(s) identified in the HPI.!DG: The patient's positive responses and pertinent negatives for the system related to the problem should be documented. (1 system) An extended ROS inquires about the system directly related to the problem(s) identified in the HPI and a limited number of additional systems.!dg: The patient's positive responses and pertinent negatives for two to nine systems should be documented. 10
11 Patient #1 ROS: Neurologic, cardiopulmonary, constitutional, urologic, gastrointestinal, infectious, negative except as in history of present illness. What was in the HPI? HPI: Patient complains of SOB for 2 days 11

12 Patient #2 ROS: Constitutional, ENT, endocrine cardiac, pulmonary, GI, musculoskeletal, neurologic, hematologic, dermatologic, negative except as in HPI 12
13 Comprehensive History Past, Family, Social History (PFSH) 1 element of each of 3 areas Family history frequently the one missed Non-contributory None on file 13
14 Past Family Social History Don t forget Family History If it is missing, encounter may downcode to subsequent care day. Watch the not specific phrases considered unacceptable Non contributory Not on file Mother Alive 14


15 History Un-obtainable What do you document to get credit? Document your efforts Maybe, document that without a patient s history, the MDM will be at high level. 15
16 History A Narrative When writing a narrative history of the patient to be carried forward for the next physician Do NOT put under HPI make a separate heading May be confused with HPI May appear cloned as an HPI which is problematic 16
17 Interval History Used for categories of: Subsequent hospital care Follow-up inpatient consultations Subsequent nursing facility Not necessary to record information on Past, Family and Social history. 17
18 EXAM (1995 E&M Guidelines) The extent of examinations performed and documented is dependent upon clinical judgement and the nature of the presenting problem(s). They range from limited examinations of single body areas to general multi-system or complete single organ system examinations.!dg: Specific abnormal and relevant negative findings of the examination of the affected or symptomatic body area(s) or organ system(s) should be documented. A notation of "abnormal" without elaboration is insufficient. 18
19 EXAM (1995 E&M Guidelines)!DG: Abnormal or unexpected findings of the examination of the unaffected or asymptomatic body area(s) or organ system(s) should be described.!dg: A brief statement or notation indicating "negative" or "normal" is sufficient to document normal findings related to unaffected area(s) or asymptomatic organ system(s).!dg: The medical record for a general multi-system examination should include findings about 8 or more of the 12 organ systems. 19
 20")
20 (2-4) (5-7) 20
21 EXAM (1995 E&M Guidelines) Detailed -- an extended examination of the affected body area(s) and other symptomatic or related organ system(s). 5-7 body areas or organ systems Patient #1 RRR, CTA, PERRLA, Throat Clear, No hepatosplenlmegaly 21
22 EXAM (1995 E&M Guidelines) Comprehensive -- a general multi-system examination or complete examination of a single organ system. Patient #2 General well developed female, PERRLA, throat clear, cranial nerves intact, heart: RRR; Lungs CTS; Abdomen soft, no hepatosplenomegaly 22
23 Medical Decision Making (MDM) Patient here for check of headaches. Several years ago when she was menopausal she had frequent migraines that were treated with Imitrex. ROS negative except HPI Exam: Well nourished female, in no distress, Heart RRR n1, s1,s2, no murmurs, no s3,s4,nl PMI, pulses intact, no thrills, no bruits Lungs: Clear to auscultation and percussion Skeletal: Normal ROM Abdominal: BS soft, non tender, no hepatosplenomegaly, no pulsations, no bruits, no masses, no hernias 23
 that the patient s problem is new?")
24 DG: Comorbidities/underlying diseases or other factors that increase the complexity of medical decision making by increasing the risk of complications, morbidity, and/or mortality should be documented. Is it obvious (stated) that the patient s problem is new? List diagnoses that are diagnosed, treated, addressed or affect the providers medical decision making Make note of problems that are not stable i.e. worsening, not responding as expected 24

25 Just because a report has been pulled into your progress note does not mean you get credit for it. Must be mentioned or addressed in your note Independent visualization of films can hold extra credit Personally visualized 25
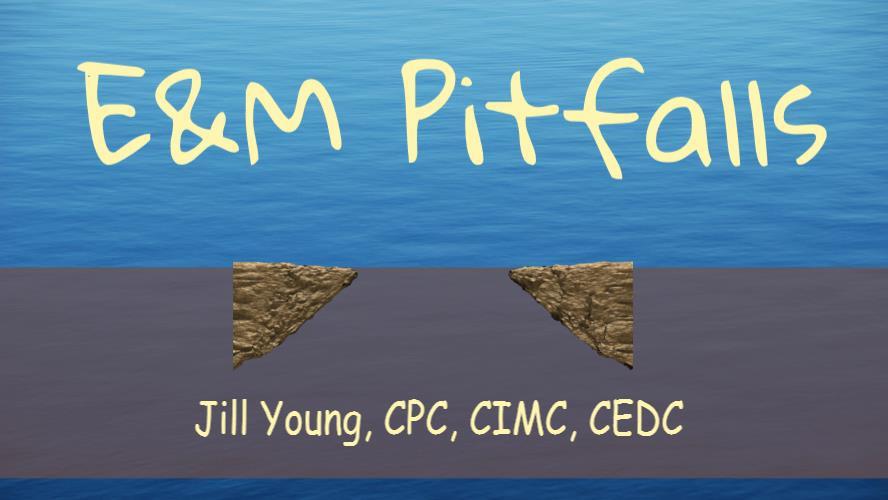
26 26
27 27
28 28
29 With Risk Factors Risk above and beyond the normal risk Patient with kidney issues having a CT scan with contrast State in the record that the patient is at risk Perhaps list why at risk (if not inherently obvious ) 29
30 Drug Therapeutic Requiring Intensive Monitoring for Toxicity Monitor labs Does not tell the untrained auditor that they are being monitored because of toxicity Change to Monitor Labs for toxicity 30
31 Diagnoses Chart documentation In order of severity List in chart must match claim form In order In severity Don t list the Problem List What are YOU taking care of today? 31

32 Patient #1 Patient Active Problem List Pulmonary embolism Colon polyp Nephrolithiasis Erectile dysfunction BPH Closed head injury Essential hypertension Impaired fasting glucose Chronic renal impairment, stage 3 Seizure 32
33 Diagnosis Why is test being ordered? EHR may require match up Signs and Symptoms Negative test 33

34 Diagnosis Diagnostic Match Up Ordering Tests or Preforming services Match the proper diagnosis to the procedure #1 and #1 or A and A Do not rely on front desk to know They cannot change without specific instruction from the provider Encounter that has diagnoses circled Need to also be ordered Not listed alphabetically 34
35 Diagnosis Pt seen for follow up of Sleep Apnea. Pt also complains of asthma flare. SOB, can t sleep Doctor prescribes shot of antibiotic and of steroids Depo-medrol - Sleep Apnea Rocephin Sleep Apnea Office Visit Sleep apnea - Asthma Patient seen for follow up of dislocated finger Patient also has been coughing productively and wheezing Chest x-ray was taken in the office Chest X-ray Dislocated Finger Office Visit pneumonia, unsp -- dislocated finger 35
36 Minor Surgical Procedures - PATH Procedures that take only a few minutes (5 minutes or less) to complete (e.g. simple suture) The teaching physician must be present for the entire procedure Teaching physician or resident may document the teaching physician s presence for the entire procedure 36
37 ENDOSCOPY - PATH Teaching physician must be present during the entire viewing Viewing starts at the time of insertion of the endoscope and ends at the time of removal of the endoscope Viewing the entire procedure through a monitor in another room Does not qualify Teaching physician or resident may document the teaching physician s presence for the entire procedure 37
38 38
39 Prolonged Care & Counseling and Coordination of Care Medical Necessity still must be met Documentation of time Start and stop Plus how much spent in C&C Note must reflect discussion for C&C Note must reflect why extra time was needed for Prolonged Do not put C&C time information at the end of every visit just in case 39
40 Cloned Cloned documentation does not meet medical necessity requirements for coverage of services Lack of specific, individual information Documentation must be specific to the patient and her/his situation at the time of the encounter Cloning of documentation is considered a misrepresentation of the medical necessity requirement for coverage of services. Falsification of medical record Do not pertain to specific visit to which they are added Priority Health 40
41 Medicare Contractors Cloned documentation will be considered misrepresentation of the medical necessity requirement for coverage of services due to the lack of specific individual information for each unique patient. Identification of this type of documentation will lead to denial of services. They warned doctors that it would refuse to pay them if they submitted cloned documentation. NGS 41
42 42
43 Clinical Plagiarism One journal article on EMR cloning went so far as to declare that physicians who copy and paste text from other physicians notes may be committing clinical plagiarism since they are documenting work that they did not perform. The article points out that, from an auditor s standpoint, you don t know how much work was actually done. Reed Gelzer, MD, MPH, co-founder of the Advocates for Documentation Integrity and Compliance Overwriting (cloning) misrepresents who provided the service, which could alter the amount billed. In addition, by submitting cloned documents for billing you are committing (insurance) fraud. 43
44 Provider Attitude Toward Cut & Paste Cross sectional survey Resident and faculty physicians at two academic medical centers 90% of physicians who wrote inpatient notes electronically used copy and paste functionality 70% used it almost always Inconsistencies and outdated information were common (71%) in notes containing copy and paste text. 80% wanted to continue to use copy and paste functionality. (J. Gen Intern Med January; 24(1):63-68) 44
45 45
46 46
47 47
48 Details Questions Type of Service Office New patient Established patient Hospital Admissions Initial Encounters Previously called Consults Subsequent care Location 48
49 Evaluation and Management (E/M) Services (Rev. 3971, Issued: , Effective: , Implementation: ) B. E/M Service Documentation Provided By Students Any contribution and participation of a student to the performance of a billable service (other than the review of systems and/or past family/social history which are not separately billable, but are taken as part of an E/M service) must be performed in the physical presence of a teaching physician or physical presence of a resident in a service meeting the requirements set forth in this section for teaching physician billing. 49
50 Physically Present The teaching physician is located in the same room (or partitioned or curtained area, if the room is subdivided to accommodate multiple patients) as the patient and/or performs a face-to-face service. MCM Chapter 12: Sec 100 Documentation by the resident of the presence and participation of the teaching physician is not sufficient to establish the presence and participation of the teaching physician. MCM Chapter 12: Section
51 Evaluation and Management (E/M) Services (Rev. 3971, Issued: , Effective: , Implementation: ) B. E/M Service Documentation Provided By Students Students may document services in the medical record. However, the teaching physician must verify in the medical record all student documentation or findings, including history, physical exam and/or medical decision making. The teaching physician must personally perform (or re-perform) the physical exam and medical decision making activities of the E/M service being billed, but may verify any student documentation of them in the medical record, rather than re-documenting this work. 51
52 Teaching Physician MUST Verify All student documentation or findings Including history, physical exam and/or medical decision making. Personally perform (or re-perform) Physical exam Medical decision making activities of the E/M May verify student documentation of them rather than redocumenting this work 52
53 J8 Part B Provider Outreach and Education Advisory Group (POE AG) Meeting All other policies of the Teaching Physicians Section remain in place Verified by other POE AG groups, meetings CMS No comment Look to MAC for further comment 53
54 100. Teaching Physician Services- MCM Ch 12 Documentation must be dated and include a legible signature or identity. Pursuant to 42 CFR (b), documentation must identify, at a minimum, the service furnished, the participation of the teaching physician in providing the service, and whether the teaching physician was physically present. 54
55 100. Teaching Physician Services- MCM Ch 12 In the context of an electronic medical record, the term 'macro' means a command in a computer or dictation application that automatically generates predetermined text that is not edited by the user. When using an electronic medical record, it is acceptable for the teaching physician to use a macro as the required personal documentation if the teaching physician adds it personally in a secured (password protected) system. 55
56 100. Teaching Physician Services- MCM Ch 12 In addition to the teaching physician s macro, either the resident or the teaching physician must provide customized information that is sufficient to support a medical necessity determination. The note in the electronic medical record must sufficiently describe the specific services furnished to the specific patient on the specific date. It is insufficient documentation if both the resident and the teaching physician use macros only. 56
57 Scenario 2: The resident performs the elements required for an E/M service in the presence of, or jointly with, the teaching physician and the resident documents the service In this case, the teaching physician must document that he/she was present during the performance of the critical or key portion(s) of the service and that he/she was directly involved in the management of the patient. The teaching physician s note should reference the resident s note. For payment, the composite of the teaching physician s entry and the resident s entry together must support the medical necessity and the level of the service billed by the teaching physician. Chapter 12: Sec:
58 Scenario 2 Minimally acceptable documentation for scenario: I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident s note. Chapter 12: Sec:
59 Scenario 4 - Medical resident admits a patient to a hospital late at night and the teaching physician does not see the patient until later, including the next calendar day: The teaching physician must document that he/she personally saw the patient and participated in the management of the patient. The teaching physician may reference the resident's note in lieu of redocumenting the history of present illness, exam, medical decision-making, review of systems and/or past family/social history provided that the patient's condition has not changed, and the teaching physician agrees with the resident's note. The teaching physician's note must reflect changes in the patient's condition and clinical course that require that the resident's note be amended with further information to address the patient s condition and course at the time the patient is seen personally by the teaching physician. Chapter 12: Sec:
60 Scenario 4 - Medical resident admits a patient to a hospital late at night and the teaching physician does not see the patient until later, including the next calendar day: The teaching physician s bill must reflect the date of service he/she saw the patient and his/her personal work of obtaining a history, performing a physical, and participating in medical decision-making regardless of whether the combination of the teaching physician s and resident s documentation satisfies criteria for a higher level of service. For payment, the composite of the teaching physician s entry and the resident s entry together must support the medical necessity of the billed service and the level of the service billed by the teaching Chapter 12: Sec:
61 Scenario 4 Minimally acceptable documentation for the scenario: I saw and evaluated the patient. I reviewed the resident s note and agree, except that picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs. I saw and evaluated the patient. Discussed with resident and agree with resident s findings and plan as documented in the resident s note. See resident s note for details. I saw and evaluated the patient and agree with the resident s finding and plans as written. I saw and evaluated the patient. Agree with resident s note but lower extremities are weaker, now 3/5; MRI of L/S Spine today. Chapter 12: Sec:
62 Evaluation and Management (E/M) Services Following are examples of unacceptable documentation: Agree with above., followed by legible countersignature or identity; Rounded, Reviewed, Agree., followed by legible countersignature or identity; Discussed with resident. Agree., followed by legible countersignature or identity; Seen and agree., followed by legible countersignature or identity; Patient seen and evaluated., followed by legible countersignature or identity; and A legible countersignature or identity alone. 62
63 Evaluation and Management (E/M) Services Such documentation is not acceptable, because the documentation does not make it possible to determine whether the teaching physician was present, evaluated the patient, and/or had any involvement with the plan of care. 63
64 Evaluation and Management (E/M) Services For purposes of payment, E/M services billed by teaching physicians require that they personally document at least the following: That they performed the service or were physically present during the key or critical portions of the service when performed by the resident; and The participation of the teaching physician in the management of the patient. When assigning codes to services billed by teaching physicians, reviewers will combine the documentation of both the resident and the teaching physician. USE OF GC MODIFIER** 64

65 65
Texas Tech University Health Sciences Center El Paso Billing Compliance Policy
 Teaching Physician Requirements for Evaluation & Management Services, Including Time - Based Codes Approved Date: October 21, 2010 Effective Date: October 21, 2010 TTUHSC El Paso Billing Compliance Website:
Teaching Physician Requirements for Evaluation & Management Services, Including Time - Based Codes Approved Date: October 21, 2010 Effective Date: October 21, 2010 TTUHSC El Paso Billing Compliance Website:
Basic Teaching Physician Presence and Documentation
 Basic Teaching Physician Presence and Documentation Welcome to the Children s University Medical Group (CUMG) training on the Teaching Physician Presence and Documentation. The goal of this module is to
Basic Teaching Physician Presence and Documentation Welcome to the Children s University Medical Group (CUMG) training on the Teaching Physician Presence and Documentation. The goal of this module is to
Jill M. Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, MI 4883
 Jill M. Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, MI 4883 This material is designed to offer basic information for coding and billing. The information presented here is based on
Jill M. Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, MI 4883 This material is designed to offer basic information for coding and billing. The information presented here is based on
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Evaluation and Management Auditing Back to the Basics. Objectives. Audit Start with the benchmarks CMS MEDPAR by specialty 4/22/2013
 Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
The World of Evaluation and Management Services and Supporting Documentation
 The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
Advanced Evaluation and. AAPC Regional Conference Chicago 10/27/12
 Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
MEDICARE RULE FOR TEACHING PHYSICIANS Effective July 1, 1996.
 MEDICARE RULE F TEACHING PHYSICIANS Effective July 1, 1996. 1.0 GENERAL RULE: If a resident participates in a service provided in a teaching setting, the teaching physician may not bill Medicare for such
MEDICARE RULE F TEACHING PHYSICIANS Effective July 1, 1996. 1.0 GENERAL RULE: If a resident participates in a service provided in a teaching setting, the teaching physician may not bill Medicare for such
Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC Disclaimer
 Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
Coding Complexities of Critical Care
 Coding Complexities of Critical Care Jill Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing.
Coding Complexities of Critical Care Jill Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing.
Cloning and Other Compliance Risks in Electronic Medical Records
 Cloning and Other Compliance Risks in Electronic Medical Records Lori Laubach, Partner, Moss Adams LLP Catherine Wakefield, Vice President, Corporate Compliance and Internal Audit, MultiCare 1 AGENDA Basic
Cloning and Other Compliance Risks in Electronic Medical Records Lori Laubach, Partner, Moss Adams LLP Catherine Wakefield, Vice President, Corporate Compliance and Internal Audit, MultiCare 1 AGENDA Basic
Documenting & Coding for Compliance
 Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
Supervising Residents: A Primer for Community Preceptors
 Supervising Residents: A Primer for Community Preceptors This document, along with the Resident Supervision ESSENTIALS For Community Preceptors handout grew from a need identified by the Credentialing
Supervising Residents: A Primer for Community Preceptors This document, along with the Resident Supervision ESSENTIALS For Community Preceptors handout grew from a need identified by the Credentialing
Presented for the AAPC National Conference April 4, 2011
 Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Supervising Residents: A Primer for Community Preceptors
 Supervising Residents: A Primer for Community Preceptors This document, along with the Resident Supervision ESSENTIALS For Community Preceptors handout grew from a need identified by the Credentialing
Supervising Residents: A Primer for Community Preceptors This document, along with the Resident Supervision ESSENTIALS For Community Preceptors handout grew from a need identified by the Credentialing
9/17/2018. Critical to Practices
 Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Start with the Problem
 Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
1:35. NPP April Young Medical Consulting, LLC. Non-Physician Practitioner Coding and Billing. Disclaimer
 Non-Physician Practitioner Coding and Billing Jill Young - CPC, CEDC, CIMC, East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing. The information
Non-Physician Practitioner Coding and Billing Jill Young - CPC, CEDC, CIMC, East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing. The information
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule. Grace Wilson, RHIA
 Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Electronic Health Records - Advantages and Pitfalls of Documentation
 Electronic Health Records - Advantages and Pitfalls of Documentation Kansas City, KS HCCA Regional Conference September 25, 2015 1:00 P.M. 2:00 P.M. Presented by: Cynthia A. Swanson, RN, CPC, CEMC, CHC,
Electronic Health Records - Advantages and Pitfalls of Documentation Kansas City, KS HCCA Regional Conference September 25, 2015 1:00 P.M. 2:00 P.M. Presented by: Cynthia A. Swanson, RN, CPC, CEMC, CHC,
Advanced E/M Auditing: Secrets to Success
 Advanced E/M Auditing: Secrets to Success Presented by Carrie Severson CPC, CPC-H, CPMA, CPC-I Senior Auditor, AAPC Client Services Why We Are Here OIG Report (OEI-04-10-00180) Coding Trends of Medicare
Advanced E/M Auditing: Secrets to Success Presented by Carrie Severson CPC, CPC-H, CPMA, CPC-I Senior Auditor, AAPC Client Services Why We Are Here OIG Report (OEI-04-10-00180) Coding Trends of Medicare
E/M Auditing: History is the Key
 E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
CODING vs AUDITING Does it all boil down to Medical Necessity?
 PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC
 Service in RHC") How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
Evaluation and Management Services
 Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
History of CPT. History of CPT. History of CPT. History of CPT. History of E&M. Workshop Evaluation and Management Coding on the River 2010
 Workshop Evaluation and Management Coding on the River 2010 Presented By: Freda Brinson, CPC, CPC-H, CEMC Freda.brinson@aapcca.org or brinsonfr@sjchs.org Faye Grile, CPC, CPMA, CEMC grilefa1@memorialhealth.com
Workshop Evaluation and Management Coding on the River 2010 Presented By: Freda Brinson, CPC, CPC-H, CEMC Freda.brinson@aapcca.org or brinsonfr@sjchs.org Faye Grile, CPC, CPMA, CEMC grilefa1@memorialhealth.com
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation
 A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
Medical Necessity verses Medical Decision Making. Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC
 Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Anthem Blue Cross and Blue Shield Commercial Professional Reimbursement Policy
 Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
601-Audit Plan for Medicare s Shared Visit Rule
 601-Audit Plan for Medicare s Shared Visit Rule Elin Baklid-Kunz, MBA, CPC, CCS Health Care Compliance Association 6500 Barrie Road, Suite 250, Minneapolis, MN 55435 888-580-8373 www.hcca-info.org Presentation
601-Audit Plan for Medicare s Shared Visit Rule Elin Baklid-Kunz, MBA, CPC, CCS Health Care Compliance Association 6500 Barrie Road, Suite 250, Minneapolis, MN 55435 888-580-8373 www.hcca-info.org Presentation
Evaluation and Management
 Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Shared and Incident To Billing of E/M Services in Radiation Oncology Updated November 2017
 ASTRO Guidance on Shared and Incident To Billing of Evaluation and Management Services in Radiation Oncology The Centers for Medicare and Medicaid Services (CMS) establishes Medicare policy for the payment
ASTRO Guidance on Shared and Incident To Billing of Evaluation and Management Services in Radiation Oncology The Centers for Medicare and Medicaid Services (CMS) establishes Medicare policy for the payment
Are they coming to get you! Todd Thomas, CCS-P
 Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
E & M Coding. Welcome To The Digital Learning Center. Today s Presentation. Course Faculty. Beyond the Basics. Presented by
 Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
ICD-9 (Diagnosis) Coding
 Coding") 1 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University.
1 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University.
Charting for Midwives. Getting Credit For the Work You Do
 Charting for Midwives Getting Credit For the Work You Do Moving Beyond S.O.A.P. The U.S. health care system is moving past fee-for-service billing. In the future, the providers will be reimbursed based
Charting for Midwives Getting Credit For the Work You Do Moving Beyond S.O.A.P. The U.S. health care system is moving past fee-for-service billing. In the future, the providers will be reimbursed based
Evaluation & Management
 Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
9/17/2018. Place of Service Type of Service Patient Status
 Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL
 Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
The Electronic Medical Record: Auditing the Copy and Paste Function
 The Electronic Medical Record: Auditing the Copy and Paste Function Presented by: Kathleen Enniss CPC CHC Compliance Analyst UW Medicine Compliance University of Washington kenniss@uw.edu The EMR: Positive
The Electronic Medical Record: Auditing the Copy and Paste Function Presented by: Kathleen Enniss CPC CHC Compliance Analyst UW Medicine Compliance University of Washington kenniss@uw.edu The EMR: Positive
Evaluation and Management Services Guide
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide November 2014 / ICN: 006764 PREFACE This guide is offered as a reference tool
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide November 2014 / ICN: 006764 PREFACE This guide is offered as a reference tool
The EHR says it s a 99215
 The EHR says it s a 99215 Angela Jordan, CPC, COBGC, AAPC Fellow Senior Managing Consultant AAPC National Advisory Board, Southwest AAPCCA BOD Chair 2012-2013 Leveling E/M services in an EHR can be perilous.
The EHR says it s a 99215 Angela Jordan, CPC, COBGC, AAPC Fellow Senior Managing Consultant AAPC National Advisory Board, Southwest AAPCCA BOD Chair 2012-2013 Leveling E/M services in an EHR can be perilous.
Medical Necessity: Not just LCD. Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC
 Medical Necessity: Not just LCD Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC Medical Necessity In The Law Social Security Act, Title XVIII Section 1862 (a) (1)
Medical Necessity: Not just LCD Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC Medical Necessity In The Law Social Security Act, Title XVIII Section 1862 (a) (1)
Lessons Learned in the EHR
 Lessons Learned in the EHR Lori Laubach, Partner Health Care Consulting Group 1 The material appearing in this presentation is for informational purposes only and is not legal or accounting advice. Communication
Lessons Learned in the EHR Lori Laubach, Partner Health Care Consulting Group 1 The material appearing in this presentation is for informational purposes only and is not legal or accounting advice. Communication
6/14/2017. Evaluation and Management Coding. Jeffrey D. Lehrman, DPM, FASPS, MAPWCA
 Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
E/M: Coding Opportunities- Documentation is key
 E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
1/21/2011. Cindy C. Parman, CPC, CPC H Coding Strategies, Inc.
 Cindy C. Parman, CPC, CPC H Coding Strategies, Inc. www.codingstrategies.com The format and/or content of this presentation is copyright 2011 by Coding Strategies, Inc. (CSI), Powder Springs, GA. This
Cindy C. Parman, CPC, CPC H Coding Strategies, Inc. www.codingstrategies.com The format and/or content of this presentation is copyright 2011 by Coding Strategies, Inc. (CSI), Powder Springs, GA. This
How does one report the performance of both a screening mammogram on the right breast and a diagnostic on the left breast at the same encounter?
 1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
Medical Decision Making
 Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
follow-up for pneumonia
 Questions How long can I access the on demand version. Where can I ask questions after the webinar? Can the CC be used as an element of HPI? I have a co-worker who believes it cannot be used at all towards
Questions How long can I access the on demand version. Where can I ask questions after the webinar? Can the CC be used as an element of HPI? I have a co-worker who believes it cannot be used at all towards
Addressing Documentation Insufficiencies
 Objectives Addressing Documentation Insufficiencies ICAHN June 9,2015 Glenn Krauss, BBA, RHIA, CCS, FCS, PCS,CCS-P, CPUR, C-CDI, CCDS, C- DAM Understand and appreciate physician frustrations with the EHR
Objectives Addressing Documentation Insufficiencies ICAHN June 9,2015 Glenn Krauss, BBA, RHIA, CCS, FCS, PCS,CCS-P, CPUR, C-CDI, CCDS, C- DAM Understand and appreciate physician frustrations with the EHR
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
See the Time chapter for complete instructions regarding how to code using time as the controlling E/M factor.
 2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
Compliant RA Coding and the EHR
 Compliant RA Coding and the EHR Sheri Poe Bernard, CCS-P, CPC, COC, CPC-I Today s goals Consider factors that brought us to the EHRs we are coding from today, and what a compliant EHR is Explore benefits
Compliant RA Coding and the EHR Sheri Poe Bernard, CCS-P, CPC, COC, CPC-I Today s goals Consider factors that brought us to the EHRs we are coding from today, and what a compliant EHR is Explore benefits
May Non-Physician Practitioner (NPP) Nurse Practitioners and Physician Assistants. Collaborating Together as a Team
 Nurse Practitioners and Physician Assistants. Collaborating Together as a Team") May 2015 Non-Physician Practitioner (NPP) Nurse Practitioners and Physician Assistants Collaborating Together as a Team What is a Non-Physician Practitioner (NPP) or Physician Extender } Physician Assistant
May 2015 Non-Physician Practitioner (NPP) Nurse Practitioners and Physician Assistants Collaborating Together as a Team What is a Non-Physician Practitioner (NPP) or Physician Extender } Physician Assistant
EMERGENCY MEDICINE CLINICAL ROTATION COMPETENCY BASED CURRICULUM
 CLINICAL ROTATION COMPETENCY BASED CURRICULUM EMERGENCY MEDICINE During the third year of the curriculum, students expand their knowledge of emergent conditions and gain the ability to apply the knowledge
CLINICAL ROTATION COMPETENCY BASED CURRICULUM EMERGENCY MEDICINE During the third year of the curriculum, students expand their knowledge of emergent conditions and gain the ability to apply the knowledge
Texas Tech University Health Sciences Center Billing Compliance Program Policy and Procedure
 4.2 Teaching Physician Requirements for Evaluation & Management Services Provided under Medicare s Primary Care Exception (PCE) Rule Approved: May 5, 2011 Effective Date: May 5, 2011 Latest Revision: June
4.2 Teaching Physician Requirements for Evaluation & Management Services Provided under Medicare s Primary Care Exception (PCE) Rule Approved: May 5, 2011 Effective Date: May 5, 2011 Latest Revision: June
Personally Providing Services Primary Care Exception Physicians AT Teaching Hospital
 Personally Providing Services Primary Care Exception Physicians AT Teaching Hospital Agenda Services Primary Care Exception (PCE) Physicians AT Teaching Hospital (PATH) 2 Personally Provided Services 3
Personally Providing Services Primary Care Exception Physicians AT Teaching Hospital Agenda Services Primary Care Exception (PCE) Physicians AT Teaching Hospital (PATH) 2 Personally Provided Services 3
2019 Evaluation and Management Coding Advisor. Advanced guidance on E/M code selection for traditional documentation systems
 2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
2018 No. 7: Radiology and Pathology/Laboratory Services
 2018 No. 7: Radiology and Pathology/Laboratory Services POLICIES AND PROCEDURES Page 2 Table of Contents I. Diagnostic Radiology Policy... 3 II. Therapeutic Radiology Policy... 4 III. Pathology... 5 Page
2018 No. 7: Radiology and Pathology/Laboratory Services POLICIES AND PROCEDURES Page 2 Table of Contents I. Diagnostic Radiology Policy... 3 II. Therapeutic Radiology Policy... 4 III. Pathology... 5 Page
Few non-clinical issues have created as
 from October 2001 How to Get All the 99214s You Deserve It s easier than you might think to get what s coming to you. Emily Hill, PA-C Few non-clinical issues have created as much controversy as the CPT
from October 2001 How to Get All the 99214s You Deserve It s easier than you might think to get what s coming to you. Emily Hill, PA-C Few non-clinical issues have created as much controversy as the CPT
Policy No: Page Number: 1 of 5 Effective Date: 08/12/15 ATTACHMENT II
 Page Number: 1 of 5 ATTACHMENT II TITLE: PURPOSE: USE OF CLONED DOCUMENTATION IN THE ELECTRONIC HEALTH RECORD The purpose of the health record is to provide a basis for planning patient care and for the
Page Number: 1 of 5 ATTACHMENT II TITLE: PURPOSE: USE OF CLONED DOCUMENTATION IN THE ELECTRONIC HEALTH RECORD The purpose of the health record is to provide a basis for planning patient care and for the
Critical Care What Makes this so Difficult
 Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
SPECIALTY TIP #13 Evaluation and Management (E&M)
") ICD- 10 SPECIALTY TIPS SPECIALTY TIP #13 Evaluation and Management (E&M) This topic is being addressed in our Specialty Tips series as most providers rate Evaluation and Management as one of the more challenging
ICD- 10 SPECIALTY TIPS SPECIALTY TIP #13 Evaluation and Management (E&M) This topic is being addressed in our Specialty Tips series as most providers rate Evaluation and Management as one of the more challenging
Guidelines for the Oral Presentation
 Guidelines for the Oral Presentation Nersi Nikakhtar, M.D. University of Minnesota Medical School 1 Table of Contents The Oral Presentation: An Introduction... 3 Why Worry About the Oral Presentation?...
Guidelines for the Oral Presentation Nersi Nikakhtar, M.D. University of Minnesota Medical School 1 Table of Contents The Oral Presentation: An Introduction... 3 Why Worry About the Oral Presentation?...
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
Programming a Spinal Cord Neurostimulator
 Programming a Spinal Cord Neurostimulator August 10, 2017 My surgeon wants to bill 95972 for programming along with placement of a spinal neurostimulator. Isn t the programming inclusive to the surgical
Programming a Spinal Cord Neurostimulator August 10, 2017 My surgeon wants to bill 95972 for programming along with placement of a spinal neurostimulator. Isn t the programming inclusive to the surgical
Preventive and Sick Visits Same Day. Objectives
 Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
Demonstrating the Chain of Medical Necessity. Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President
 Demonstrating the Chain of Medical Necessity Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science,
Demonstrating the Chain of Medical Necessity Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science,
BEFORE THE ALASKA OFFICE OF ADMINISTRATIVE HEARINGS ON REFERRAL FROM THE COMMISSIONER OF HEALTH AND SOCIAL SERVICES
 BEFORE THE ALASKA OFFICE OF ADMINISTRATIVE HEARINGS ON REFERRAL FROM THE COMMISSIONER OF HEALTH AND SOCIAL SERVICES In the Matter of: ) ) FAMILY MEDICAL CLINIC ) OAH No. 10-0095-DHS ) DECISION I. INTRODUCTION
BEFORE THE ALASKA OFFICE OF ADMINISTRATIVE HEARINGS ON REFERRAL FROM THE COMMISSIONER OF HEALTH AND SOCIAL SERVICES In the Matter of: ) ) FAMILY MEDICAL CLINIC ) OAH No. 10-0095-DHS ) DECISION I. INTRODUCTION
Chiropractic Record Keeping
 Chiropractic Record Keeping (DeskBook Chapter 4.1) Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science, Accounting
Chiropractic Record Keeping (DeskBook Chapter 4.1) Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science, Accounting
Code Assignment & Validation
 Code Assignment & Validation Evaluation & Management Services Presenter Santa Allaire, RHIT, CCS, CPC, CIRCC, CEMC Disclaimer This presentation is for general education purposes only. The information contained
Code Assignment & Validation Evaluation & Management Services Presenter Santa Allaire, RHIT, CCS, CPC, CIRCC, CEMC Disclaimer This presentation is for general education purposes only. The information contained
Physician Providers include any attending physicians (MD, DO, DPM or dentists).
.") TITLE: ELECTRONIC HEALTH RECORD (EHR) DOCUMENTATION STANDARDS AND GUIDELINES MANUAL: MEDICAL STAFF POLICIES AND PROCEDURES Page 1 of 5 Effective Date: 6/28/2016 Reviewed/Revised: Approval /s/ Jeannette
TITLE: ELECTRONIC HEALTH RECORD (EHR) DOCUMENTATION STANDARDS AND GUIDELINES MANUAL: MEDICAL STAFF POLICIES AND PROCEDURES Page 1 of 5 Effective Date: 6/28/2016 Reviewed/Revised: Approval /s/ Jeannette
Guide to Documentation and Medical Coding 2017
 Guide to Documentation and Medical Coding 2017 Office of Compliance 933 Bradbury SE, Suite 3053 Albuquerque, NM 87106 Phone: 505-925-6053 Fax: 505-925-0934 i ii Table of Contents INTRODUCTION... V CHAPTER
Guide to Documentation and Medical Coding 2017 Office of Compliance 933 Bradbury SE, Suite 3053 Albuquerque, NM 87106 Phone: 505-925-6053 Fax: 505-925-0934 i ii Table of Contents INTRODUCTION... V CHAPTER
2011 Melanoma Physician Quality Reporting (PQRS): FREQUENTLY ASKED QUESTIONS
: FREQUENTLY ASKED QUESTIONS") Q: What is the Physician Quality Reporting System? A: The Physician Quality Reporting System, formerly known as PQRI, is a program developed by the Centers for Medicare and Medicaid Services (CMS) to provide
Q: What is the Physician Quality Reporting System? A: The Physician Quality Reporting System, formerly known as PQRI, is a program developed by the Centers for Medicare and Medicaid Services (CMS) to provide
MED VI MEDICAL INTENSIVE CARE (MICU) GOALS AND OBJECTIVES Internal Medicine University of Toledo
 GOALS AND OBJECTIVES Internal Medicine University of Toledo") MED VI MEDICAL INTENSIVE CARE (MICU) GOALS AND OBJECTIVES Internal Medicine University of Toledo Educational Goals and Objectives: The purpose of this rotation is to provide the residents with the knowledge
MED VI MEDICAL INTENSIVE CARE (MICU) GOALS AND OBJECTIVES Internal Medicine University of Toledo Educational Goals and Objectives: The purpose of this rotation is to provide the residents with the knowledge
RVU KILLERS The Most Common Reimbursement Documentation Errors. Michael Granovsky MD CPC CEDC FACEP President LogixHealth
 RVU KILLERS The Most Common Reimbursement Documentation Errors Michael Granovsky MD CPC CEDC FACEP President LogixHealth Documentation-Why Does It Matter? Must communicate to the payer your concerns and
RVU KILLERS The Most Common Reimbursement Documentation Errors Michael Granovsky MD CPC CEDC FACEP President LogixHealth Documentation-Why Does It Matter? Must communicate to the payer your concerns and
Caldwell Medical Center Departments
 Caldwell Medical Center Departments Surgery Medical / Surgery Same Day Surgery Lab Education Administration Special Care Unit Women s Center Admission Emergency Services Radiology Cardiac Rehab Admission
Caldwell Medical Center Departments Surgery Medical / Surgery Same Day Surgery Lab Education Administration Special Care Unit Women s Center Admission Emergency Services Radiology Cardiac Rehab Admission
Message Response Message
 Message If established pt wouldn't 2 out of 3 still require the level for slide 5? Response Message Can you re-state your question? I am unclear on what you are asking. Thanks You stated that even when
Message If established pt wouldn't 2 out of 3 still require the level for slide 5? Response Message Can you re-state your question? I am unclear on what you are asking. Thanks You stated that even when
Evaluation & Management 101 for Clinicians
 Evaluation & Management 101 for Clinicians Kerin Draak, MSN, WHNP BC, CPC, CEMC, COBGC, CPC I System Director of Clinical & Financial Integration Hospital Sisters Health System This is the Full Title of
Evaluation & Management 101 for Clinicians Kerin Draak, MSN, WHNP BC, CPC, CEMC, COBGC, CPC I System Director of Clinical & Financial Integration Hospital Sisters Health System This is the Full Title of
Hospitalist Coding Compliance sponsored by CHMB
 Hospitalist Coding Compliance sponsored by CHMB CHMB Corporate Overview Founded in 1995 o Privately Held, Profitable and P.E. Funded for Rapid Growth o Inc. 5000 Fastest Growing Private Companies 2008-2012
Hospitalist Coding Compliance sponsored by CHMB CHMB Corporate Overview Founded in 1995 o Privately Held, Profitable and P.E. Funded for Rapid Growth o Inc. 5000 Fastest Growing Private Companies 2008-2012
2/28/2017 NO DISCLOSURES. K 1/Partner
 NO DISCLOSURES LaMon Norton NP Participant will recognize origin & role of Relative Value Unit (RVU) in coding and reimbursement. Participant will be able to link documentation points to coding and RVU
NO DISCLOSURES LaMon Norton NP Participant will recognize origin & role of Relative Value Unit (RVU) in coding and reimbursement. Participant will be able to link documentation points to coding and RVU
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
CREATING AN AUDIT PLAN FOR PHYSICIAN OFFICES. Katherine Abel, CPC, CPB, CPMA, CPPM, CPC-I, AAPC Fellow Director of Curriculum AAPC
 CREATING AN AUDIT PLAN FOR PHYSICIAN OFFICES Katherine Abel, CPC, CPB, CPMA, CPPM, CPC-I, AAPC Fellow Director of Curriculum AAPC OIG Compliance Guidance Implementing written policies, procedures and standards
CREATING AN AUDIT PLAN FOR PHYSICIAN OFFICES Katherine Abel, CPC, CPB, CPMA, CPPM, CPC-I, AAPC Fellow Director of Curriculum AAPC OIG Compliance Guidance Implementing written policies, procedures and standards
The Slippery Slope of Electronic Health Record Systems. Presented by: Maryann C. Palmeter, CPC, CENTC. Learning Objectives
 The Slippery Slope of Electronic Health Record Systems Presented by: Maryann C. Palmeter, CPC, CENTC Learning Objectives Identify key benefits of an electronic health record system (EHR) Define note cloning,
The Slippery Slope of Electronic Health Record Systems Presented by: Maryann C. Palmeter, CPC, CENTC Learning Objectives Identify key benefits of an electronic health record system (EHR) Define note cloning,
Post-Op hemorrhage repair. Is it billable?
 Post-Op hemorrhage repair. Is it billable? August 10, 2017 Can I bill for taking the patient back to the OR to explore and repair post-op hemorrhage on day post-op? I heard that all complications are included
Post-Op hemorrhage repair. Is it billable? August 10, 2017 Can I bill for taking the patient back to the OR to explore and repair post-op hemorrhage on day post-op? I heard that all complications are included
Social Security Number: Employment Status: Employed Unemployed Address: Student Retired
 Please complete all forms fully and to the best of your ability. If something does not apply to you please write N/A in the field. Patient Demographics: Name: Sex: Male Female Address: Apt: City: Marital
Please complete all forms fully and to the best of your ability. If something does not apply to you please write N/A in the field. Patient Demographics: Name: Sex: Male Female Address: Apt: City: Marital
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
May Family Chiropractic Health Information and Health History Patient Name: Gender: Male Female
 1 Health Information and Health History Patient Name: Gender: Male Female Marital Status: (Circle one) M S D W Other: Date of Birth / / Spouse Name: How many children: Patient Social Security Number: -
1 Health Information and Health History Patient Name: Gender: Male Female Marital Status: (Circle one) M S D W Other: Date of Birth / / Spouse Name: How many children: Patient Social Security Number: -
Transition Care Management Update: Practical Applications for 2016
 60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
Office of Compliance. Complete & Accurate Documentation Core Curriculum for GWU Residents
 Office of Compliance Complete & Accurate Documentation Core Curriculum for GWU Residents December 3, 2014 Medical Record The medical record tells the story of the patient from start to finish. If the story
Office of Compliance Complete & Accurate Documentation Core Curriculum for GWU Residents December 3, 2014 Medical Record The medical record tells the story of the patient from start to finish. If the story
LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN
 LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN Created on 6/2/2014 DISCLAIMER DISCLAIMER: WPS Medicare has produced this material as an informational reference. Every reasonable
LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN Created on 6/2/2014 DISCLAIMER DISCLAIMER: WPS Medicare has produced this material as an informational reference. Every reasonable
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice
 Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Getting paid properly requires a thorough knowledge of the rules.
 Selecting E/M Codes For Established Patients Getting paid properly requires a thorough knowledge of the rules. Kenneth F. Malkin, D.P.M. Bio: Dr. Malkin is a diplomate of the American Board of Quality
Selecting E/M Codes For Established Patients Getting paid properly requires a thorough knowledge of the rules. Kenneth F. Malkin, D.P.M. Bio: Dr. Malkin is a diplomate of the American Board of Quality
UWSMPH Clerkship Experience Requirements
 2016-2017 UWSMPH Clerkship Experience Requirements Students will use OASIS to check off each Clerkship Experience Requirement. The following conditions, procedures and learning activities must all be completed
2016-2017 UWSMPH Clerkship Experience Requirements Students will use OASIS to check off each Clerkship Experience Requirement. The following conditions, procedures and learning activities must all be completed
As you write your progress notes,
 Brenda Edwards, CPC, CPC-I, CPMA, CEMC, CPB Do You Know What Is (or Isn t) in Your Documentation? Leaving out key information in patient documentation can compromise quality and cost you money. As you
Brenda Edwards, CPC, CPC-I, CPMA, CEMC, CPB Do You Know What Is (or Isn t) in Your Documentation? Leaving out key information in patient documentation can compromise quality and cost you money. As you