Meet the Presenter. Welcome to PMI s Webinar Presentation. E/M Auditing - Telling an Accurate Patient Story. On the topic:
|
|
|
- Michael Mervin Webster
- 5 years ago
- Views:
Transcription

1 Welcome to PMI s Webinar Presentation Brought to you by: Practice Management Institute pmimd.com Meet the Presenter On the topic: Pam Joslin, MM, CMC, CMIS, CMOM E/M Auditing - Telling an Accurate Patient Story
2 Welcome to Practice Management Institute s Webinar and Audio Conference Training. We hope that the information contained herein will give you valuable tips that you can use to improve your skills and performance on the job. Each year, more than 40,000 physicians and office staff are trained by Practice Management Institute. For 30 years, physicians have relied on PMI to provide up-to-date coding, reimbursement, compliance and office management training. Instructor-led classes are presented in 400 of the nation s leading hospitals, healthcare systems, colleges and medical societies. PMI provides a number of other training resources for your practice, including national conferences for medical office professionals, self-paced certification preparatory courses, online training, educational audio downloads, and practice reference materials. For more information, visit PMI s web site at Please be advised that all information in this program is provided for informational purposes only. While PMI makes all reasonable efforts to verify the credentials of instructors and the information provided, it is not intended to serve as legal advice. The opinions expressed are those of the individual presenter and do not necessarily reflect the viewpoint of Practice Management Institute. The information provided is general in nature. Depending on the particular facts at issue, it may or may not apply to your situation. Participants requiring specific guidance should contact their legal counsel. CPT is a registered trademark of the American Medical Association. Practice Management Institute 8242 Vicar San Antonio, Texas tel: fax: (210) info@pmimd.com
3 E/M Auditing: Telling an Accurate Patient Story Brought to you by Pam Joslin, MM, CMC, CMIS, CMOM, CMCO, CEMA Practice Management Institute pmimd.com Current Procedural Terminology (CPT ) is copyright 2016 of the American Medical Association. All Rights Reserved. No fee schedules, basic units, relative values, or related listings are included in CPT. The AMA assumes no liability for the data contained herein. Applicable FARS/DFARS restrictions apply to government use Practice Management Institute 2 1
4 Introduction The Medical record is a legal document that serves as a chronological record of pertinent facts and observations about a patient s health. A chart audit is an examination of medical records to determine how well a practice performs. The Office of Inspector General (OIG) has initiated audit initiatives to determine whether Medicare is making erroneous payments. A baseline audit should be conducted to examine the claim development and submission process. 3 What Causes a Carrier Audit? Random audits Complaints from patients and employees Repeated billing problems from carrier Abnormal distribution of E/M levels of care Unusually high numbers of any single code Failure to follow non-par Medicare rules Failure to routinely collect deductibles and co-pays Medical record that does not support the CPT code 4 2
5 Improper Payments for E/M Services Cost Medicare Billions Medicare paid $32.3 billion for E/M services in 2010, representing nearly 30 percent of Part B payments that year. E/M services are divided into broad categories that reflect the type of service, the place of service, and the patient s status. In 2012, OIG reported that from 2001 to 2010, physicians increased their billing of higher level codes for E/M services in all visit types. Additionally, OIG identified 1,669 physicians who consistently billed for the two highest level codes for E/M services in E/M services must be medically reasonable and necessary, in addition to meeting the individual requirements of the CPT code that is used on the claim. According to CMS, [I]t would not be medically necessary or appropriate to bill [for] a higher level of [E/M] service when a lower level of service is warranted. Physicians are responsible for ensuring that the claims they submit to Medicare accurately reflect the E/M services provided and the billing levels corresponding to those services. 6 3
6 Audit Surveillance Increasing The Office of the Inspector General is increasing its audit surveillance. New attention from the OIG, RACs, ZPICs, PSCs are resulting in medical offices losing thousands of dollars annually. 7 Types of Audits There are many types of medical record audits: Internal audits Preliminary audits Comprehensive audits Retrospective audits Pre-payment audits Compliance audits External audits 8 4


7 Percentage of E/M Claims and Type of Error Source: 9 Percentage of Upcoded & Downcoded Claims for E/M 10 5
8 Audit Findings 55% of claims for E/M services were incorrectly coded and/or lacking documentation 26% were upcoded 15% were downcoded 12% were insufficiently documented 7% were undocumented 2% had other coding errors Claims for E/M services billed for by high-coding physicians were more likely to be incorrectly coded or insufficiently documented than those billed for by other physicians. 11 What Can Your Healthcare Organization Do to Avoid Audits? 1. Ensure your practice has a WRITTEN compliance program. 2. Ensure that your practice has a Billing Policy Manual. 3. Ensure that your healthcare organization conducts periodic chart audits internally. 4. Attend education sessions for the entire office on a regular basis. 5. A billing service should be investigated thoroughly prior to hiring. 6. Use only CURRENT ICD-10 and CPT coding books. 7. Develop/Use forms and checklists to eliminate human error. 8. New providers hired should be trained on documentation guidelines. 12 6
9 DOCUMENTATION GUIDELINES FOR EVALUATION AND MANAGEMENT SERVICES 13 General Principles of Medical Record Documentation The principles of documentation listed below are applicable to all types of medical and surgical services in all settings. For Evaluation and Management (E/M) services, the nature and amount of physician work and documentation varies by type of service, place of service and the patient s status. The general principles listed below may be modified to account for these variable circumstances in providing E/M services: 1. The medical record should be complete and legible. 2. The documentation of each patient encounter should include: reason for the encounter and relevant history, physical examination findings and prior diagnostic test results; assessment, clinical impression or diagnosis; plan for care; date and legible identity of the observer. 14 7
10 General Principles of Medical Record Documentation 3. If not documented, the rationale for ordering diagnostic and other ancillary services should be easily inferred. 4. Past and present diagnoses should be accessible to the treating and/or consulting physician. 5. Appropriate health risk factors should be identified. 6. The patient s progress, response to and changes in treatment, as well as revision of diagnosis should be documented. 7. The CPT and ICD-10 codes reported on the health insurance claim form or billing statement should be supported by the documentation in the medical record. 15 Documentation of E/M Services The descriptors for the levels of E/M services recognized seven components that are used in defining the levels of E/M services. These components are: history examination medical decision making counseling coordination of care nature of presenting problem; and time 16 8
11 The first three of these components - history, examination, and medical decision making) - are the key components in selecting the level of E/M services. Because the level of E/M service is dependent on all three key components, performance, and documentation of one component at the highest level does not necessarily mean that the encounter in its entirety qualifies for the highest level of E/M service. These documentation guidelines for E/M services reflect the needs of the typical adult population. 17 Documentation of E/M Services Documentation of History The levels of E/M services are based on four types of history (Problem Focused, Expanded Problem Focused, Detailed, and Comprehensive). Each type of history includes some or all of the following elements: Chief complaint (CC); History of present illness (HPI); Review of systems (ROS); and Past, family and/or social history (PFSH). The extent of history of present illness, review of systems and past, family and/or social history that is obtained and documented is dependent upon clinical judgment and the nature of the presenting problem(s). 18 9
12 Capsulization of History Documentation Requirements Chief Complaint History of Present Illness Review of Systems Past, Family and/or Social History Type of History Brief (1 3) N/A N/A Problem Focused Brief (1 3) Problem Pertinent Extended (4+)* Extended (2 9) Pertinent (1 of 3) Detailed N/A Extended (4+)* Complete (10+) Complete (2 of 3) or (3 of 3)** *Status of 3 chronic of inactive conditions **2 of 3 is for an established patient; 3 of 3 is for a new patient Extended Problem Focused Comprehensive 19 DG: The CC, ROS and PFSH may be listed as separate elements of history, or they may be included in the description of the history of the present illness. DG: A ROS and/or a PFSH obtained during an earlier encounter does not need to be re-recorded if there is evidence that the physician reviewed and updated the previous information. The review and update may be documented by: Describing any new ROS and/or PFSH information or noting there has been no change in the information; and Noting the date and location of the earlier ROS and/or PFSH
13 DG: The ROS and/or PFSH may be recorded by ancillary staff or on a form completed by the patient. There must be a notation supplementing or confirming the information recorded by others. DG: If the physician is unable to obtain a history from the patient or other source, the record should describe the patient s condition or other circumstance which precludes obtaining a history. 21 Chief Complaint Chief complaint (CC) The CC is a concise statement describing the symptom, problem, condition, diagnosis, physician recommended return, or other factor that is the reason for the encounter, usually stated in the patient s words. DG: The medical record should clearly reflect the chief complaint
14 History of Present Illness (HPI) The HPI is a chronological description of the development of the patient's present illness from the first sign and/or symptom or from the previous encounter to the present. It includes the following elements: location, quality, severity, duration, timing, context, modifying factors, and associated signs and symptoms. Brief and extended HPIs are distinguished by the amount of detail needed to accurately characterize the clinical problem(s). 23 A brief HPI consists of one to three elements of the HPI. DG: The medical record should describe one to three elements of the present illness (HPI). An extended HPI consists of at least four elements of the HPI or the status of at least three chronic or inactive conditions. DG: The medical record should describe at least four or more elements of the present illness (HPI) or status of at least three chronic or inactive conditions
15 Review of Systems (ROS) A ROS is an inventory of body systems obtained through a series of questions seeking to identify signs and/or symptoms which the patient may be experiencing or has experienced. For purposes of ROS, the following systems are recognized: Constitutional symptoms (fever, weight loss) Eyes Ears, Nose, Mouth, Throat Cardiovascular Respiratory Gastrointestinal Genitourinary Musculoskeletal Integumentary (skin and/or breast) Neurological Psychiatric Endocrine Hematologic/Lymphatic Allergic/Immunologic 25 Problem Pertinent ROS A problem pertinent ROS inquires about the system directly related to the problem(s) identified in the HPI. DG: The patient s positive responses and pertinent negatives for the system related to the problem should be documented. An extended ROS inquires about the system directly related to the problem(s) identified in the HPI and a limited number of additional systems. DG: The patient's positive responses and pertinent negatives for two to nine systems should be documented
16 Complete ROS A complete ROS inquires about the system(s) directly related to the problem(s) identified in the HPI plus all additional body systems. DG: At least 10 organ systems must be reviewed. Those systems with positive or pertinent negative responses must be individually documented. For the remaining systems, a notation indicating all other systems are negative is permissible. In the absence of such a notation, at least 10 systems must be individually documented. 27 Past, Family and/or Social History (PFSH) The PFSH consists of a review of three areas: past history (the patient s past experiences with illnesses, operations, injuries and treatments); family history (a review of medical events in the patient s family, including diseases which may be hereditary or place the patient at risk); social history (an age-appropriate review of past and current activities)
17 Pertinent PFSH A pertinent PFSH is of a review of the history area(s) directly related to the problem(s) identified in the HPI. DG: At least one specific item from any of the three history areas must be documented for a pertinent PFSH 29 Complete PFSH A complete PFSH is of a review of two or all three of the PFSH history areas, depending on the category of the E/M service. A review of all three history areas is required for services that by their nature include a comprehensive assessment or reassessment of the patient. A review of two of the three history areas is sufficient for other services. DG: At least one specific item from two of the three history areas must be documented for a complete PFSH for the following E/M services: office or other outpatient services, established patient; emergency department; subsequent nursing facility care; domiciliary care, established patient; and home care, established patient
18 Past History A review of the patient's past experiences with illnesses, injuries, and treatments that include significant information about: prior major illnesses and injuries prior operations prior hospitalizations current medications allergies age appropriate immunizations age appropriate feeding/dietary status 31 Family History A review of medical events in the patient's family that includes significant information about: the health status or cause of death of parents, siblings, and children specific diseases related to problems identified in the chief complaint or history of the present illness and/or review of systems diseases of family members which may be hereditary or place the patient at risk 32 16
19 Social History An age-appropriate review of past and current activities which include significant information about: marital status and/or living arrangements current employment occupational history use of drugs, alcohol, and tobacco level of education sexual history other relevant social factors 33 Documentation of Examination The levels of E/M services are based on four types of examination that are defined as follows: Problem Focused -- a limited examination of the affected body area or organ system. Expanded Problem Focused -- a limited examination of the affected body area or organ system and any other symptomatic or related body area(s) or organ system(s). Detailed -- an extended examination of the affected body area(s) or organ system(s) and any other symptomatic or related body area(s) or organ system(s). Comprehensive -- a general multi-system examination or complete examination of a single organ system and other symptomatic or related body area(s) or organ system(s)
20 Types of Examinations These types of examinations have been defined for general multi-system and the following single organ systems: Cardiovascular Ears, Nose, Mouth and Throat Eyes Genitourinary (Female) Genitourinary (Male) Hematologic/Lymphatic/ Immunologic Musculoskeletal Neurological* Psychiatric Respiratory Skin* *dependent on a demonstration that the physician work is equivalent to that of a general multi-system examination 35 General Multi-System Examinations A general multi-system examination or a single organ system examination may be performed by any physician regardless of specialty. To qualify for a given level of multi-system examination, the following content and documentation requirements should be met: Problem Focused Examination should include performance and documentation of one to five elements in one or more organ systems(s) or body area(s). Expanded Problem Focused Examination should include performance and documentation of at least six elements in one or more related body area(s) or organ system(s). Detailed Examination should include at least six organ systems or body areas with a least two elements, for a total of twelve elements. Comprehensive should include at least nine organ system or body areas. For each area/system, documentation of at least two elements
21 General Multi-System Exam Constitutional Eyes Ears, Nose, Mouth, and Throat Neck Respiratory Cardiovascular Chest (Breasts) Gastrointestinal Genitourinary Lymphatic Musculoskeletal Skin Neurologic Psychiatric 37 Content and Documentation Requirements Level of Exam Problem Focused Expanded Problem Focused Detailed Comprehensive Perform and Document One to five elements identified by a bullet. At least six elements identified by a bullet. At least two elements identified by a bullet from each of six areas/systems OR at least twelve elements identified by a bullet in two or more areas/systems. Perform all elements identified by a bullet in at least nine organ systems or body areas and document at least two elements identified by a bullet from each of nine area/systems
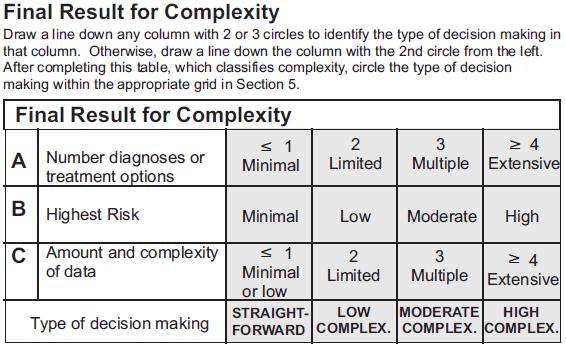
22 Documentation of the Complexity of Medical Decision Making Medical decision making refers to the complexity of establishing a diagnosis and/or selecting a management option as measured by: The number of possible diagnoses and/or the number of management options that must be considered. The amount and/or complexity of medical records, diagnostic tests, and/or other information that must be obtained, reviewed, and analyzed. The risk of significant complications, morbidity, and/or mortality, as well as co-morbidities, associated with the patient s presenting problem(s), the diagnostic procedure(s) and/or the possible management options. 39 Medical Decision-Making Number of Diagnoses or Management Options Minimal Amount and/or Complexity of Data to be Reviewed Minimal or None Risk of Significant Complications, Morbidity, and/or Mortality Minimal Type of Decision Making* Straightforward Limited Limited Low Low Complexity Multiple Moderate Moderate Moderate Complexity Extensive Extensive High High Complexity *NOTE to qualify for a type of medical decision making, 2 of 3 elements must either be met or exceeded
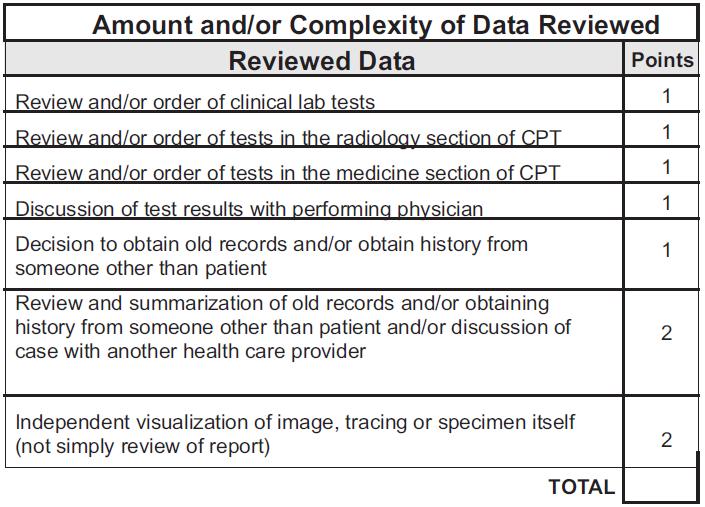
23 Number of Diagnoses or Management Options The number of possible diagnoses and/or the number of management options that must be considered is based on the number and types of problems addressed during the encounter, the complexity of establishing a diagnosis and the management decisions that are made by the physician. DG: For each encounter as assessment, clinical impression, or diagnosis should be documented. DG: The initiation of, or changes in, treatment should be documented. DG: If referrals are made, consultations requested or advice 41 Amount and/or Complexity of Data to be Reviewed Based on the types of diagnostic testing ordered or reviewed. DG: DG: DG: DG: If a diagnostic service is ordered, planned, scheduled, or performed at the time of the E/M encounter, the type of service should be documented. The review of lab, radiology, and/or other diagnostic tests should be documented. A decision to obtain old records or additional history from the family, caretaker, or other source to supplement that obtained from the patient should be documented. Relevant findings from the review of old records, and/or the receipt of additional history of family, caretaker, or other source should be documented
24 Amount and/or Complexity of Data to be Reviewed DG: DG: The results of discussion of laboratory, radiology or other diagnostic tests with the physician who performed or interpreted the study should be documented. The direct visualization and independent interpretation of an image, tracing or specimen previously or subsequently interpreted by another physician should be documented. 43 Risk of Significant Complications, Morbidity, and/or Mortality Based on the risks associated with the presenting problem(s), the diagnostic procedures(s), and the possible management options. DG: DG: DG: Co-morbidities/underlying diseases or other factors that increase the complexity of medical decision making by increasing the risk of complications, morbidity, and/or mortality should be documented. If a surgical or invasive diagnostic procedure is ordered, planned or scheduled at the time of the E/M encounter, the type of procedure should be documented. If a surgical or invasive diagnostic procedure is performed at the time of the E/M encounter, the specific procedure should be documented
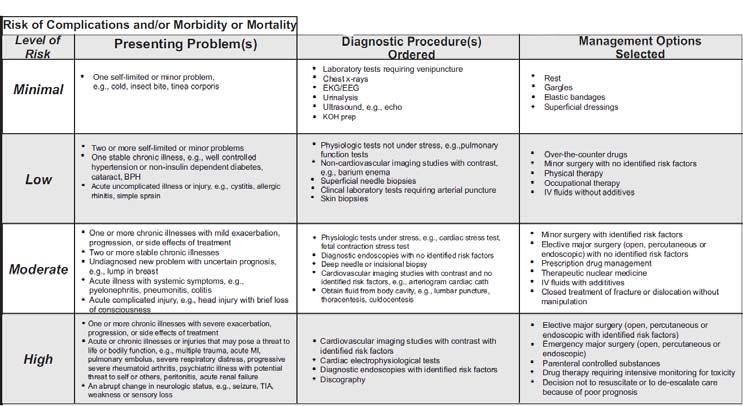
25 Risk of Significant Complications, Morbidity, and/or Mortality DG: The referral for or decision to perform a surgical or invasive diagnostic procedure on an urgent basis should be documented or implied. 45 Table 1 PRESENTING PROBLEMS Minimal Low Moderate High One self limited or minor problem, e.g. cold, insect bite Two or more selflimited or minor problems One stable, e.g. well controlled hypertension or diabetes Acute uncomplicated illness or injury, e.g. cystitis, allergic rhinitis, simple sprain One or more chronic illness with mild exacerbation Two or more stable chronic illnesses Undiagnosed new problem with uncertain prognosis, e.g. lump in breast, rectal bleeding Acute illness with systemic symptoms, e.g. pyelonephritis, pneumonitis, colitis Acute complicated injury, e.g. head injury with brief loss of consciousness One or more chronic illnesses with severe exacerbation Acute or chronic illnesses or injuries that pose a threat to life of bodily function, e.g. multiple trauma, acute MI Severe respiratory distress Progressive, severe rheumatoid arthritis Depression with suicidal ideation 46 23
26 Table 2 DIAGNOSTIC PROCEDURES Minimal Low Moderate High Lab tests requiring venipuncture Chest X-rays EKG EEG Urinalysis Ultrasound, e.g. echocardiography Physiologic tests not under stress, e.g. pulmonary function tests Noncardiovascular imagine studies with contrast e.g. barium enema Superficial needle biopsies Clinical lab tests requiring arterial puncture Physiologic tests under stress, e.g. cardiac stress test Endoscopies with no identified risk factors Deep needle or incisional biopsy Cardiovascular imagining studies with contrast and no identified risk factors; e.g. arteriogram, cardiac catheterization Lumbar puncture Cardiovascular imaging studies with identified risk factors Cardiac electro physiological tests Endoscopies with identified risk factors 47 Table 3 MANAGEMENT OPTIONS Minimal Low Moderate High Rest Gargles Elastic bandages Superficial dressings Over the counter drugs Minor surgery with no identified risk factors Physical Therapy Occupational therapy Minor surgery with identified risk factors Referral for or decision to perform elective major surgery with no identified risk factors Simple prescription drug management Therapeutic nuclear medicine Elective major surgery with identified risk factors Referral for or decision to perform emergency major surgery Parenteral controlled substances Multiple drug therapy requiring intensive monitoring for toxicity 48 24
27 Summary Table 4 In the table below, find the circle(s) farthest to the right. Draw a line down that column to the bottom row and circle to overall risk. Presenting Problem(s) (Table 1) Diagnostic Procedures (Table 2) Management Options (Table 3) Minimal Low Moderate High Minimal Low Moderate High Minimal Low Moderate High Overall Risk 1 Minimal 2 Low 3 Moderate 4 High MEDICAL NECESSITY 50 25
28 Medical Necessity According to Medicare.gov, medically necessary is defined as health-care services or supplies needed to prevent, diagnose, or treat an illness, injury, condition, disease, or its symptoms and that meet accepted standards of medicine. For a service to be considered medically necessary, it must be reasonable and necessary to diagnosis or treat a patient s medical condition. When submitting claims for payment, the diagnosis codes reported with the service tells the payer "why" a service was performed. The diagnosis reported helps support the medical necessity of the procedure. 51 Example For example, a patient presents to the office with chest pain and the physician orders an electrocardiogram (ECG). A 12-lead ECG performed in the office and interpreted by a physician is reported with CPT code The reason the physician orders the ECG is because the patient is complaining of chest pain. The diagnosis code for unspecified chest pain is R
29 In this case, the provider should be queried why the chest X- ray was ordered so the proper diagnosis can be reported. The provider may have wanted a knee X-ray and made a mistake when writing his orders. By asking the provider for clarification, you have prevented the performance of an unnecessary test because the provider really intended to order a knee X-ray. In this case, the knee pain would support the order of the knee X-ray. If the provider intended to order a chest X-ray, by asking for clarification you can report the service with a more appropriate ICD-10-CM code and eliminate a claim denial. 53 The provider must document the diagnosis for all procedures that are performed. The provider also must include the diagnosis for each diagnostic test ordered. A common error seen when reviewing medical documentation is that the provider will document a diagnosis and indicate tests ordered, but it is unclear that all the tests ordered are for the diagnosis documented in the assessment. For example, the patient presents with right knee pain and the physician performs an arthrocentesis. He also orders a chest X-ray. The only diagnosis documented is knee pain. The knee pain supports the medical necessity for performing the arthrocentesis, but it does not support the medical necessity for the chest X-ray
30 Case Study CC: Seeking a new primary physician HPI: The patient is a pleasant 65 year old female who presents to establish care with a local primary physician after moving to this area recently, to be near her daughter. She has a history of hypertension and type II diabetes, both controlled with medications. She also has a history of coronary artery disease, which has been asymptomatic for the last three years following PTCA deploying 2 stents. She has no spontaneous current complaints. ROS: Complete ROS was performed and documented and was positive for intermittent lower extremity edema and easy bruising. For more details, please refer to the ROS questionnaire with today s date located in the chart. Medications: Atenolol 25 mg PO QD. Glyburide 5 mg PO BID. Lisinopril 10 mg PO BID. Atorvastatin 20 mg PO QD. PMH: In addition to the HPI, she has osteoarthritis. SH: The patient has been widowed for 5 years. She denies tobacco or alcohol abuse. 55 Exam: Vitals: 116/70, 80, 97.9 General Appearance: NAD, well conversant Eyes: Anicteric sclerae, moist conjunctiva; no lid-lag; PERRLA. HEENT: AT/NC; oropharynx clear with MMM and no mucosal ulcerations; auditory canals patent with pearly TMs. Normal hard and soft palate. Neck: Trachea midline; FROM, supple, no thyromegaly or lymphadenopathy. Lungs: CTA, with normal respiratory effort and no intercostal retractions. CV: RRR, no MRGs Abdomen: Soft, non-tender; no masses or HSM. Extremities: No peripheral edema or extremity lymphadenopathy. Skin: Normal temperature, turgor and texture; no rash, ulcers or nodules. Psych: Appropriate affect, alert and oriented to person, place and time. Labs: HGBA1c 6.8; BUN 25, creatinine 0.8; LDL 86, HGB

31 Assessment: 1. Well controlled essential hypertension 2. Optimally controlled NIDDM 3. Stable CAD Plan: 1. Continue current medications unchanged 2. Return visit in two months 3. Will repeat HGBA1c, CBC, and renal profile 4. Will repeat LFTs since patient is on statin medication 5. Will re- check microalbumin/creatinine 57 Rationale 58 29

32 Rationale Examination Comprehensive (20 Bullets) Constitutional Bullet #1, Bullet #2 Eyes Bullet #1, Bullet #2 Ears, nose, mouth, & throat Bullet #1, Bullet #6 Neck Bullet #1, Bullet #2 Respiratory Bullet #1, Bullet #4 Cardiovascular Bullet #2, Bullet #7 Gastrointestinal Bullet #1, Bullet #2 Lymphatic Bullet #1, Bullet #4 Skin Bullet #1, Bullet #2 Psychiatric Bullet #2, Bullet #
33 61 Rationale Medical Decision Making Moderate Complexity #Dx Multiple (3 established and stable problems: hypertension, diabetes, and CAD) Data Minimal Risk Moderate 62 31

34
35

36 Tips, Tools & Techniques Have a written compliance plan in place Conduct audits on a regularly scheduled basis and provide feedback Track and train in areas of deficiency to maximize results and be audit-proof 68 34
37 Questions? Thank you for your attendance! Get your questions answered on PMI s Discussion Forum: 35
6/14/2017. Evaluation and Management Coding. Jeffrey D. Lehrman, DPM, FASPS, MAPWCA
 Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Medical Necessity verses Medical Decision Making. Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC
 Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Anthem Blue Cross and Blue Shield Commercial Professional Reimbursement Policy
 Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
Evaluation and Management Auditing Back to the Basics. Objectives. Audit Start with the benchmarks CMS MEDPAR by specialty 4/22/2013
 Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Evaluation & Management Documentation Training Tool
 Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table, which
Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table, which
The World of Evaluation and Management Services and Supporting Documentation
 The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
Evaluation & Management Documentation Training Tool
 A MS Medicare Administrative ontractor Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest
A MS Medicare Administrative ontractor Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest
Evaluation and Management Services Guide
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide November 2014 / ICN: 006764 PREFACE This guide is offered as a reference tool
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide November 2014 / ICN: 006764 PREFACE This guide is offered as a reference tool
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation
 A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule. Grace Wilson, RHIA
 Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC
 Service in RHC") How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
NEXTGEN E&M CODING DEMONSTRATION
 NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
NEXTGEN E&M CODING DEMONSTRATION
 NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
Start with the Problem
 Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
EVALUATION & MANAGEMENT SERVICES CODING. Part I: What is an E&M? Where do you start? Jennifer Jones, CPC, CPC-I
 DOTHAN AL CHAPTER AAPC FALL WORKSHOP Friday November 17, 2017 REGISTRATION BEGINS AT 7:15 am PROGRAM TIME IS 8:00 am 12:30 pm Earn 4 CEU s for a Fee of only $50.00 per attendee (Snacks will be provided
DOTHAN AL CHAPTER AAPC FALL WORKSHOP Friday November 17, 2017 REGISTRATION BEGINS AT 7:15 am PROGRAM TIME IS 8:00 am 12:30 pm Earn 4 CEU s for a Fee of only $50.00 per attendee (Snacks will be provided
Evaluation and Management
 Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Documenting & Coding for Compliance
 Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
E & M Coding. Welcome To The Digital Learning Center. Today s Presentation. Course Faculty. Beyond the Basics. Presented by
 Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Evaluation & Management 101 for Clinicians
 Evaluation & Management 101 for Clinicians Kerin Draak, MSN, WHNP BC, CPC, CEMC, COBGC, CPC I System Director of Clinical & Financial Integration Hospital Sisters Health System This is the Full Title of
Evaluation & Management 101 for Clinicians Kerin Draak, MSN, WHNP BC, CPC, CEMC, COBGC, CPC I System Director of Clinical & Financial Integration Hospital Sisters Health System This is the Full Title of
SPECIALTY TIP #13 Evaluation and Management (E&M)
") ICD- 10 SPECIALTY TIPS SPECIALTY TIP #13 Evaluation and Management (E&M) This topic is being addressed in our Specialty Tips series as most providers rate Evaluation and Management as one of the more challenging
ICD- 10 SPECIALTY TIPS SPECIALTY TIP #13 Evaluation and Management (E&M) This topic is being addressed in our Specialty Tips series as most providers rate Evaluation and Management as one of the more challenging
Evaluation & Management
 Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
Presented for the AAPC National Conference April 4, 2011
 Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
E/M: Coding Opportunities- Documentation is key
 E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL
 Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Medical Decision Making
 Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES. SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION
 NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION Table of Contents GENERAL RULES AND INFORMATION... 3 MMIS MODIFIERS... 13 EVALUATION AND MANAGEMENT
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION Table of Contents GENERAL RULES AND INFORMATION... 3 MMIS MODIFIERS... 13 EVALUATION AND MANAGEMENT
Evaluation and Management Services
 Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Office of Compliance. Complete & Accurate Documentation Core Curriculum for GWU Residents
 Office of Compliance Complete & Accurate Documentation Core Curriculum for GWU Residents December 3, 2014 Medical Record The medical record tells the story of the patient from start to finish. If the story
Office of Compliance Complete & Accurate Documentation Core Curriculum for GWU Residents December 3, 2014 Medical Record The medical record tells the story of the patient from start to finish. If the story
Code Assignment & Validation
 Code Assignment & Validation Evaluation & Management Services Presenter Santa Allaire, RHIT, CCS, CPC, CIRCC, CEMC Disclaimer This presentation is for general education purposes only. The information contained
Code Assignment & Validation Evaluation & Management Services Presenter Santa Allaire, RHIT, CCS, CPC, CIRCC, CEMC Disclaimer This presentation is for general education purposes only. The information contained
E/M Fast Finder. CPT only 2012 American Medical Association. 1 All Rights Reserved.
 E/M Fast Finder The E/M Fast Finder is a carry-along reference to assist in assigning the Evaluation and Management (E/M) codes that are part of the 99000 series of Current Procedural Terminology (CPT
E/M Fast Finder The E/M Fast Finder is a carry-along reference to assist in assigning the Evaluation and Management (E/M) codes that are part of the 99000 series of Current Procedural Terminology (CPT
How does one report the performance of both a screening mammogram on the right breast and a diagnostic on the left breast at the same encounter?
 1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Few non-clinical issues have created as
 from October 2001 How to Get All the 99214s You Deserve It s easier than you might think to get what s coming to you. Emily Hill, PA-C Few non-clinical issues have created as much controversy as the CPT
from October 2001 How to Get All the 99214s You Deserve It s easier than you might think to get what s coming to you. Emily Hill, PA-C Few non-clinical issues have created as much controversy as the CPT
Care Transition Strategies: The 2013 Transition Care Management Codes
 Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
Basics of Coding for Compliance. Health Systems Compliance Presented by JoAnn Martinez, CPC Compliance Educator
 Basics of Coding for Compliance Health Systems Compliance Presented by JoAnn Martinez, CPC Compliance Educator Documentation Best Practice Common Themes ICD-10 that support E/M & Procedure Coding Type
Basics of Coding for Compliance Health Systems Compliance Presented by JoAnn Martinez, CPC Compliance Educator Documentation Best Practice Common Themes ICD-10 that support E/M & Procedure Coding Type
RVU KILLERS The Most Common Reimbursement Documentation Errors. Michael Granovsky MD CPC CEDC FACEP President LogixHealth
 RVU KILLERS The Most Common Reimbursement Documentation Errors Michael Granovsky MD CPC CEDC FACEP President LogixHealth Documentation-Why Does It Matter? Must communicate to the payer your concerns and
RVU KILLERS The Most Common Reimbursement Documentation Errors Michael Granovsky MD CPC CEDC FACEP President LogixHealth Documentation-Why Does It Matter? Must communicate to the payer your concerns and
Rational Physician Coding for Hospital Progress Notes. Redacted Version. Peter R. Jensen, MD, CPC
 Rational Physician Coding for Hospital Progress Notes Peter R. Jensen, MD, CPC www.emuniversity.com Rational Physician Coding for Hospital Progress Notes Peter R. Jensen, MD, CPC For clinically driven
Rational Physician Coding for Hospital Progress Notes Peter R. Jensen, MD, CPC www.emuniversity.com Rational Physician Coding for Hospital Progress Notes Peter R. Jensen, MD, CPC For clinically driven
How to Write a Medical Note for the. Foundations of Doctoring Course and Beyond: Demystifying the Focused (SOAP) Note
 Note") How to Write a Medical Note for the Foundations of Doctoring Course and Beyond: Demystifying the Focused (SOAP) Note and the Comprehensive (H&P) Note by Todd Guth, MD Overview of the Medical Note Medical
How to Write a Medical Note for the Foundations of Doctoring Course and Beyond: Demystifying the Focused (SOAP) Note and the Comprehensive (H&P) Note by Todd Guth, MD Overview of the Medical Note Medical
NEW YORK STATE MEDICAID PROGRAM PODIATRY PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM PODIATRY PROCEDURE CODES Table of Contents GENERAL INFORMATION AND INSTRUCTIONS... 3 MMIS MODIFIERS... 12 LABORATORY SERVICES PERFORMED IN A PODIATRIST'S OFFICE... 13 MEDICAL
NEW YORK STATE MEDICAID PROGRAM PODIATRY PROCEDURE CODES Table of Contents GENERAL INFORMATION AND INSTRUCTIONS... 3 MMIS MODIFIERS... 12 LABORATORY SERVICES PERFORMED IN A PODIATRIST'S OFFICE... 13 MEDICAL
Strategies for Coding, Billing and Getting Paid Appropriately. A Guide for Family Physicians
 2016 Strategies for Coding, Billing and Getting Paid Appropriately A Guide for Family Physicians TABLE OF CONTENTS Chapter One Tools and Resources for Practice Success Chapter Two The Revenue Cycle Management
2016 Strategies for Coding, Billing and Getting Paid Appropriately A Guide for Family Physicians TABLE OF CONTENTS Chapter One Tools and Resources for Practice Success Chapter Two The Revenue Cycle Management
Transition Care Management Update: Practical Applications for 2016
 60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
History of CPT. History of CPT. History of CPT. History of CPT. History of E&M. Workshop Evaluation and Management Coding on the River 2010
 Workshop Evaluation and Management Coding on the River 2010 Presented By: Freda Brinson, CPC, CPC-H, CEMC Freda.brinson@aapcca.org or brinsonfr@sjchs.org Faye Grile, CPC, CPMA, CEMC grilefa1@memorialhealth.com
Workshop Evaluation and Management Coding on the River 2010 Presented By: Freda Brinson, CPC, CPC-H, CEMC Freda.brinson@aapcca.org or brinsonfr@sjchs.org Faye Grile, CPC, CPMA, CEMC grilefa1@memorialhealth.com
CODING vs AUDITING Does it all boil down to Medical Necessity?
 PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
Rational Physician Coding for E/M Consult Services. Redacted Version. Peter R. Jensen, MD, CPC
 Rational Physician Coding for E/M Consult Services Peter R. Jensen, MD, CPC www.emuniversity.com Rational Physician Coding for E/M Consult Services Peter R. Jensen, MD, CPC For clinically driven E/M coding
Rational Physician Coding for E/M Consult Services Peter R. Jensen, MD, CPC www.emuniversity.com Rational Physician Coding for E/M Consult Services Peter R. Jensen, MD, CPC For clinically driven E/M coding
Charting for Midwives. Getting Credit For the Work You Do
 Charting for Midwives Getting Credit For the Work You Do Moving Beyond S.O.A.P. The U.S. health care system is moving past fee-for-service billing. In the future, the providers will be reimbursed based
Charting for Midwives Getting Credit For the Work You Do Moving Beyond S.O.A.P. The U.S. health care system is moving past fee-for-service billing. In the future, the providers will be reimbursed based
Are they coming to get you! Todd Thomas, CCS-P
 Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
2019 Evaluation and Management Coding Advisor. Advanced guidance on E/M code selection for traditional documentation systems
 2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
HEALTH DEPARTMENT BILLING GUIDELINES
 HEALTH DEPARTMENT BILLING GUIDELINES Acknowledgement: Current Procedural Terminology (CPT ) is copyright 2017 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative
HEALTH DEPARTMENT BILLING GUIDELINES Acknowledgement: Current Procedural Terminology (CPT ) is copyright 2017 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative
Implementation Date: January 2018 Clinical Operations
 Magellan Healthcare Clinical guidelines RECORD KEEPING AND DOCUMENTATION STANDARDS Original Date: November 2015 Page 1 of 11 Physical Medicine Clinical Decision Making Last Review Date: June 2017 Guideline
Magellan Healthcare Clinical guidelines RECORD KEEPING AND DOCUMENTATION STANDARDS Original Date: November 2015 Page 1 of 11 Physical Medicine Clinical Decision Making Last Review Date: June 2017 Guideline
IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY
 Global Surgery Policy Number GLS03272013RP Approved By UnitedHealthcare Medicare Committee Current Approval Date 04/09/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
Global Surgery Policy Number GLS03272013RP Approved By UnitedHealthcare Medicare Committee Current Approval Date 04/09/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
Documentation for ED Visits with "Additional Work-Up" Planned. Presented by Rae Jimenez, CPC, CDEO, CPB, CPMA, CPPM, CPC-I, CCS
 Documentation for ED Visits with "Additional Work-Up" Planned Presented by Rae Jimenez, CPC, CDEO, CPB, CPMA, CPPM, CPC-I, CCS Course Objectives Discuss gray areas for E/M selection for the professional
Documentation for ED Visits with "Additional Work-Up" Planned Presented by Rae Jimenez, CPC, CDEO, CPB, CPMA, CPPM, CPC-I, CCS Course Objectives Discuss gray areas for E/M selection for the professional
Message Response Message
 Message If established pt wouldn't 2 out of 3 still require the level for slide 5? Response Message Can you re-state your question? I am unclear on what you are asking. Thanks You stated that even when
Message If established pt wouldn't 2 out of 3 still require the level for slide 5? Response Message Can you re-state your question? I am unclear on what you are asking. Thanks You stated that even when
FQHC Behavioral Health Billing Codes
 FQHC s Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though process clearly reflected in assessment
FQHC s Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though process clearly reflected in assessment
Welcome To The Digital Learning Center. Billing Compliance: Today s Presentation. Course Faculty. Presented by
 Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation Billing liance: Avoiding Fraud & Abuse in Your Medical/Surgical Practice Course
Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation Billing liance: Avoiding Fraud & Abuse in Your Medical/Surgical Practice Course
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
Primary Care Setting Behavioral Health Billing Codes
 Primary Care Setting s Medicaid Medicare Third Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though
Primary Care Setting s Medicaid Medicare Third Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though
The E/M Essentials Pocket Guide
 The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CCS-P, CEMC The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CEMC, CCS-P The E/M Essentials Pocket Guide is published by HCPro, a division
The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CCS-P, CEMC The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CEMC, CCS-P The E/M Essentials Pocket Guide is published by HCPro, a division
Review case problems to differentiate code linkage of diagnosis and procedure.
 South Central College HC 1928 CPT Coding I Course Information Description This course is the introduction of CPTcoding and provides and in-depth review of the coding and reimbursement system used in outpatient
South Central College HC 1928 CPT Coding I Course Information Description This course is the introduction of CPTcoding and provides and in-depth review of the coding and reimbursement system used in outpatient
9/17/2018. Place of Service Type of Service Patient Status
 Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
PREVENTIVE MEDICINE AND SCREENING POLICY
 UnitedHealthcare Oxford Reimbursement Policy PREVENTIVE MEDICINE AND SCREENING POLICY Policy Number: ADMINISTRATIVE 238.19 T0 Effective Date: July 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
UnitedHealthcare Oxford Reimbursement Policy PREVENTIVE MEDICINE AND SCREENING POLICY Policy Number: ADMINISTRATIVE 238.19 T0 Effective Date: July 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
Meet the Presenter. HCPCS Reimbursement Impacts the Bottom Line. Welcome to PMI s Webinar Presentation. On the topic:
 Welcome to PMI s Webinar Presentation Brought to you by: Practice Management Institute pmimd.com Meet the Presenter Rhonda Granja CMC, CMIS, CMOM, CPC, CPM, MCS Faculty Practice Management Institute On
Welcome to PMI s Webinar Presentation Brought to you by: Practice Management Institute pmimd.com Meet the Presenter Rhonda Granja CMC, CMIS, CMOM, CPC, CPM, MCS Faculty Practice Management Institute On
Patient s Full Name DOB Age. Patient s SSN Sex: Male Female Preferred Language. Place of Birth: City State Country
 Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
follow-up for pneumonia
 Questions How long can I access the on demand version. Where can I ask questions after the webinar? Can the CC be used as an element of HPI? I have a co-worker who believes it cannot be used at all towards
Questions How long can I access the on demand version. Where can I ask questions after the webinar? Can the CC be used as an element of HPI? I have a co-worker who believes it cannot be used at all towards
Coding and Billing for Lifestyle Medicine
 Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
MEDICAL POLICY No R2 TELEMEDICINE
 Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
9/17/2018. Critical to Practices
 Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Meet the Presenter. Welcome to PMI s Webinar Presentation. Understanding the Current State of a Patient-Oriented Experience.
 Welcome to PMI s Webinar Presentation Brought to you by: Practice Management Institute pmimd.com Meet the Presenter On the topic: Sherita Sutton, MPH, CMA PMI Corporate Partner Instructor Understanding
Welcome to PMI s Webinar Presentation Brought to you by: Practice Management Institute pmimd.com Meet the Presenter On the topic: Sherita Sutton, MPH, CMA PMI Corporate Partner Instructor Understanding
Getting paid properly requires a thorough knowledge of the rules.
 Selecting E/M Codes For Established Patients Getting paid properly requires a thorough knowledge of the rules. Kenneth F. Malkin, D.P.M. Bio: Dr. Malkin is a diplomate of the American Board of Quality
Selecting E/M Codes For Established Patients Getting paid properly requires a thorough knowledge of the rules. Kenneth F. Malkin, D.P.M. Bio: Dr. Malkin is a diplomate of the American Board of Quality
HC 1930 HC 1930 ICD-9-CM III/CPT Coding II
 South Central College HC 1930 HC 1930 ICD-9-CM III/CPT Coding II Course Information Description Total Credits 4.00 Total Hours 80.00 Types of Instruction This course is a continuation of HC 1920, 1925,
South Central College HC 1930 HC 1930 ICD-9-CM III/CPT Coding II Course Information Description Total Credits 4.00 Total Hours 80.00 Types of Instruction This course is a continuation of HC 1920, 1925,
Modern Optometric Staff BILLING & CODING THE MEDICAL EYE EXAMINATION. I m From The Government. The HIPPA Act of And I m Here To Help
 BILLING & CODING THE MEDICAL EYE EXAMINATION Modern Optometric Staff Ask the right questions, take the right actions Follow HIPPA guidelines Craig Thomas, O.D. 3900 West Wheatland Road Dallas, Texas 75237
BILLING & CODING THE MEDICAL EYE EXAMINATION Modern Optometric Staff Ask the right questions, take the right actions Follow HIPPA guidelines Craig Thomas, O.D. 3900 West Wheatland Road Dallas, Texas 75237
ICD-9 (Diagnosis) Coding
 Coding") 1 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University.
1 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University.
3/16/2016. No Treble. OIG Reports. Highlights OIG Report Coding Trends. Presented by Maggie Mac CPC, CEMC, CHC, CMM, ICCE
 It s All About That E/M No Treble Presented by Maggie Mac CPC, CEMC, CHC, CMM, ICCE OIG Reports Coding Trends of Medicare Evaluation and Management Services ~ May 2012 Improper Payments for Evaluation
It s All About That E/M No Treble Presented by Maggie Mac CPC, CEMC, CHC, CMM, ICCE OIG Reports Coding Trends of Medicare Evaluation and Management Services ~ May 2012 Improper Payments for Evaluation
During the hospital medicine rotation, residents will focus on the following procedures as permitted by case mix:
 Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
E/M Auditing: History is the Key
 E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
See the Time chapter for complete instructions regarding how to code using time as the controlling E/M factor.
 2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
Global Surgery Fact Sheet
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Global Surgery Fact Sheet Definition of a Global Surgical Package This fact sheet is designed to provide education on the
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Global Surgery Fact Sheet Definition of a Global Surgical Package This fact sheet is designed to provide education on the
MEDICAL POLICY No R1 TELEMEDICINE
 Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Coding, Corroboration, and Compliance How to assure the 3 C s are met
 Coding, Corroboration, and Compliance How to assure the 3 C s are met Sue Roehl, RHIT, CCS sroehl@eidebailly.com 701-476-8770 OIG 1996 - $23.2 Billion errors Figure 1 Insufficient/No documentation 46.76%
Coding, Corroboration, and Compliance How to assure the 3 C s are met Sue Roehl, RHIT, CCS sroehl@eidebailly.com 701-476-8770 OIG 1996 - $23.2 Billion errors Figure 1 Insufficient/No documentation 46.76%
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR fax Physician
 Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
Anesthesia Services Policy
 Anesthesia Services Policy Policy Number Annual Approval Date 3/14/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare Medicare
Anesthesia Services Policy Policy Number Annual Approval Date 3/14/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare Medicare
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
Medical Necessity: Not just LCD. Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC
 Medical Necessity: Not just LCD Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC Medical Necessity In The Law Social Security Act, Title XVIII Section 1862 (a) (1)
Medical Necessity: Not just LCD Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC Medical Necessity In The Law Social Security Act, Title XVIII Section 1862 (a) (1)
New Patient Registration Form NJR_NP_F100
 New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Procedure Code Job Aid
 Procedure Code 99211 Job Aid Definition for 99211: Office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician. Usually,
Procedure Code 99211 Job Aid Definition for 99211: Office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician. Usually,
Dear New Patient: Sincerely, The Scheduling Staff
 Dear New Patient: Welcome to Garden State Urology. The physicians in our group are board-certified, fellowship trained urologists who provide stateof-the-art care that rivals the finest academic institutions
Dear New Patient: Welcome to Garden State Urology. The physicians in our group are board-certified, fellowship trained urologists who provide stateof-the-art care that rivals the finest academic institutions
Global Days Policy. Approved By 7/12/2017
 Global Days Policy Policy Number 2018R0005A Annual Approval Date 7/12/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible for submission of accurate
Global Days Policy Policy Number 2018R0005A Annual Approval Date 7/12/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible for submission of accurate
Gynecologic or Annual Women s Exam Visit & Use of Q0091 (Pap, Pelvic, & Breast Visit)
") Manual: Policy Title: Reimbursement Policy Gynecologic or Annual Women s Exam Visit & Use of Q0091 (Pap, Pelvic, & Breast Visit) Section: Evaluation & Management Services Subsection: None Date of Origin:
Manual: Policy Title: Reimbursement Policy Gynecologic or Annual Women s Exam Visit & Use of Q0091 (Pap, Pelvic, & Breast Visit) Section: Evaluation & Management Services Subsection: None Date of Origin:
Preventive and Sick Visits Same Day. Objectives
 Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
Advanced Evaluation and. AAPC Regional Conference Chicago 10/27/12
 Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Coding Companion for Primary Care. A comprehensive illustrated guide to coding and reimbursement
 Coding Companion for Primary Care A comprehensive illustrated guide to coding and reimbursement 2009 Contents Getting Started with Coding Companion... i Integumentary...1 Breast...67 General Musculoskeletal...68
Coding Companion for Primary Care A comprehensive illustrated guide to coding and reimbursement 2009 Contents Getting Started with Coding Companion... i Integumentary...1 Breast...67 General Musculoskeletal...68
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Telemedicine Guidance
 Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
PATIENT INFORMATION. Address: Sex: City: State: address: Cell Phone: Home Phone: Work Phone: address: Cell Phone:
 PATIENT INFORMATION Name: _ DOB: _ Age: Address: _Sex: City: _ State: _ Zip: _ Email address: Cell Phone: _ Home Phone: Work Phone: _ Responsible Party (if different from above) Name: DOB: Address: E-mail:
PATIENT INFORMATION Name: _ DOB: _ Age: Address: _Sex: City: _ State: _ Zip: _ Email address: Cell Phone: _ Home Phone: Work Phone: _ Responsible Party (if different from above) Name: DOB: Address: E-mail:
Health Assessment Student Handbook
 Health Assessment Student Handbook Fall 2017 Your guide to the Shadow Health Digital Clinical Experience UGV.1 Table of Contents WELCOME!... 3 HEALTH HISTORY Instructions... 4 HEENT Instructions... 5 RESPIRATORY
Health Assessment Student Handbook Fall 2017 Your guide to the Shadow Health Digital Clinical Experience UGV.1 Table of Contents WELCOME!... 3 HEALTH HISTORY Instructions... 4 HEENT Instructions... 5 RESPIRATORY