BOARD MEETING AGENDA am. Wednesday 01 March Items to be considered in public meeting VENUE
|
|
|
- Laurence Bradford
- 6 years ago
- Views:
Transcription
1 BOARD MEETING Wednesday 01 March am AGENDA Items to be considered in public meeting VENUE Waitemata DHB Boardroom Level 1, 15 Shea Terrace Takapuna 1
2 Karakia E te Kaihanga e te Wahingaro E mihi ana mo te ha o to koutou oranga Kia kotahi ai o matou whakaaro i roto i te tu waatea. Kia U ai matou ki te pono me te tika I runga i to ingoa tapu Kia haumie kia huie Taiki eee. Creator and Spirit of life. To the ancient realms of the Creator Thank you for the life we each breathe to help us be of one mind As we seek to be of service to those in need. Give us the courage to do what is right and help us to always be aware Of the need to be fair and transparent in all we do. We ask this in the name of Creation and the Living Earth. Well Being to All. 2
3 1 MEETING OF THE BOARD 01 March 2017 Venue: Waitemata DHB Boardroom, Level 1, 15 Shea Tce, Takapuna WDHB BOARD MEMBERS Lester Levy - Chair Max Abbott - WDHB Board Member Edward Benson-Cooper WDHB Board Member Kylie Clegg Deputy Chair Sandra Coney - WDHB Board Member Warren Flaunty - WDHB Board Member James Le Fevre - WDHB Board Member Dr Matire Harwood - WDHB Board Member Brian Neeson WDHB Board Member Morris Pita - WDHB Board Member Allison Roe - WDHB Board Member APOLOGIES Time: 09.45am WDHB MANAGEMENT Dale Bramley - Chief Executive Officer Robert Paine - Chief Financial Officer and Head of Corporate Services Andrew Brant - Chief Medical Officer Simon Bowen - Director Health Outcomes Debbie Holdsworth - Director Funding Jocelyn Peach - Director of Nursing and Midwifery Cath Cronin Director of Hospital Services Tamzin Brott Director of Allied Health Fiona McCarthy Director Human Resources Roger Perkins Executive Head Peta Molloy - Board Secretary REGISTER OF INTERESTS Does any member have an interest they have not previously disclosed? Does any member have an interest that may give rise to a conflict of interest with a matter on the agenda? PART 1 Items to be considered in public meeting AGENDA 9.45am 1. AGENDA ORDER AND TIMING 2. BOARD MINUTES 9.50am 2.1 Confirmation of Minutes of the Meeting of the Board (14/12/16) Actions arising from previous meetings 2.2 Confirmation of Minutes of the Executive Committee of the Board (14/2/17) 3. EXECUTIVE REPORTS 9.55am 10.10am 10.20am 3.1 Chief Executive Officer s Report 3.2 Health and Safety Report 3.3 Communications Report 4. PERFORMANCE REPORT 11.00am 4.1 Financial Performance 5. COMMITTEE REPORTS 11.10am 5.1 Minutes of the Hospital Advisory Committee (14/12/16) 5.2 Minutes of the Community and Public Health Advisory Committee Meeting (23/11/16) 6. INFORMATION PAPERS 11.15am 11.20am 11.25am 11.30am 6.1 Statement of Performance Expectation (SPE) Reporting 6.2 Health and Safety Marker Report 6.3 Bowel Screening Pilot Final Evaluation Report 6.4 Privacy Maturity Assessment report 11.35am 7. RESOLUTION TO EXCLUDE THE PUBLIC Waitemata District Health Board, Meeting of the Board 01/03/17 3
4 1 Waitemata District Health Board Board Member Attendance Schedule 2016 NAME FEB APRIL MAY JULY AUG SEPT NOV DEC Dr Lester Levy (Chair) Max Abbott Edward Benson Cooper Appointed on 05 December 2016 Kylie Clegg Sandra Coney * Warren Flaunty James Le Fevre Matire Harwood Appointed on 05 December 2016 Brian Neeson Appointed on 05 December 2016 Morris Pita Christine Rankin * Allison Roe * Gwen Tepania-Palmer Apologies given *Attended part of the meeting only # Absent on Board business ^ Leave of Absence Waitemata District Health Board, Meeting of the Board 01/03/17 4
5 1 Board/Committee Member Lester Levy - Board Chairman Max Abbott REGISTER OF INTERESTS Involvements with other organisations Chair Auckland District Health Board Chair Counties Manukau District Health Board Chair Regional Governance Group, northern region DHBs Chairman Auckland Transport Chairman Health Research Council Independent Chairman Tonkin + Taylor Chief Executive New Zealand Leadership Institute Professor of Leadership University of Auckland Business School Trustee - Well Foundation (ex-officio member) Lead Reviewer - State Services Commission, Performance Improvement Framework (currently undertaking a review of MBIE) Pro Vice-Chancellor (North Shore) and Dean Faculty of Health and Environmental Sciences, Auckland University of Technology Patron Raeburn House Advisor Health Workforce New Zealand Board Member, AUT Millennium Ownership Trust Chair Social Services Online Trust Board member Rotary National Science and Technology Forum Trust Last Updated 05/12/16 19/03/14 Edward Benson-Cooper Chiropractor Milford, Auckland (with private practice commitments) 07/12/16 Kylie Clegg Board Member - Hockey New Zealand 06/12/16 Trustee and Chair - the Hockey Foundation Trustee and Beneficiary - Mickyla Trust Trustee and Beneficiary - M&K Investments Trust (includes a share of less than 1% in Orion Health Group and a shareholding in Nextminute Holdings Ltd) Trustee and Beneficiary - M&K Investments Trust (owns 99% share in MC Capital Ltd and MC Securities Ltd and a minority shareholding in HSCP1 Ltd) Sandra Coney Member Waitakere Ranges Local Board, Auckland Council 15/12/16 Patron Women s Health Action Trust Member Portage Licensing Trust Member West Auckland Trusts Services Warren Flaunty Member Henderson Massey Local Board Auckland Council 06/12/16 Trustee (Vice President) - Waitakere Licensing Trust Shareholder - EBOS Group Shareholder Green Cross Health Director Life Pharmacy Northwest Director Westgate Pharmacy Ltd Chair Three Harbours Health Foundation Director - Trusts Community Foundation Ltd Dr Matire Harwood Senior Lecturer Auckland University 09/12/16 Board Director Health Research Council Director Ngarongoa Limited, which is contractor providing services to National Hauora Coalition. GP at Papakura Marae Health Clinic Advisory Committee Member State Foundation NZ (Maori Health) Member Te Ora, Maori Medical Practitioners James Le Fevre Deputy Chair Auckland District Health Board Emergency Physician Auckland Adults Emergency Department Pre-hospital Physician Auckland HEMS ARHT/Auckland DHB Co-opted Member Whanganui District Health Board Hospital Advisory Committee Trustee Three Harbours Foundation Member Association of Salaried Medical Specialists Member Medical Protection Society Shareholder Pacific Edge Ltd James wife is an employee of the Waitemata DHB, Department of Anaesthesia and Perioperative Medicine and a Medico-Legal Advisor for the Medical Protection Society 14/12/16 Waitemata District Health Board, Meeting of the Board 01/03/17 5
6 1 Board/Committee Member Brian Neeson Allison Roe Morris Pita Involvements with other organisations Member Upper Harbour Local Board Member Human Rights Review Tribunal Member Auckland District Licensing Committee Managing Director BK & VS Neeson Limited Managing Director Apollo Property Investments Limited Property Development Consultant Chairperson Matakana Coast Trail Trust Member - Rodney Local Board, Auckland Council Owner/operator Shea Pita and Associates Limited Shareholder Turuki Pharmacy Limited Member - Eden Park Trust Board Morris wife is member of the Northland District Health Board Shareholder and Director of Healthcare Applications Limited Last Updated 15/12/16 02/11/16 06/12/16 Waitemata District Health Board, Meeting of the Board 01/03/17 6
7 Confirmation of Minutes of the Board meeting held on 14 December 2016 Recommendation: That the Minutes of the Board meeting held on 14 December 2016 be approved. Waitemata District Health Board, Meeting of the Board 01/03/17 7
8 2.1 Minutes of the meeting of the Waitemata District Health Board Wednesday 14 December 2016 held at Waitemata DHB, Boardroom, Level 1, 15 Shea Terrace, Takapuna, commencing at 10.48am (following a Mihi Whakatau for the new Board led by Kaumatua Frank Toa) BOARD MEMBERS PRESENT: Lester Levy (Board chair) Max Abbott Edward Benson-Cooper Kylie Clegg Sandra Coney James Le Fevre Warren Flaunty Matire Harwood Brian Neeson Morris Pita ALSO PRESENT: PART I Items considered in public meeting Dale Bramley (Chief Executive Officer) Robert Paine (Chief Financial Officer and Head of Corporate Services) Debbie Holdsworth (Director Funding) Cath Cronin (Director of Hospital Services) Jocelyn Peach (Director of Nursing and Midwifery) Fiona McCarthy (Director of Human Resources) Tamzin Brott (Director of Allied Health, Scientific and Technical Professions) Peta Molloy (Board Secretary) (Staff members who attended for a particular item are named at the start of the minute for that item) PUBLIC AND MEDIA REPRESENTATIVES: APOLOGIES: WELCOME Annabelle Claridge (University of Auckland and Waitemata DHB employee) (present from p.m.) An apology was received and accepted from Allison Roe. The Board Chair welcomed new and returning Board members and all those present at the meeting. DISCLOSURE OF INTERESTS James Le Fevre advised that he had been appointed as the Auckland DHB Deputy Chair. Waitemata District Health Board, Meeting of the Board 01/03/17 8
9 2.1 Brian Neeson advised that he was a member of the Human Rights Review and a member of the Upper Harbour Local Board. There were no declarations of interest relating to the open section of the agenda. 1 AGENDA ORDER AND TIMING Items were taken in same order as listed in the agenda. 2 RESOLUTION TO EXCLUDE THE PUBLIC (agenda pages 6-7) Resolution (Moved James Le Fevre /Seconded Warren Flaunty) That, in accordance with the provisions of Schedule 3, Sections 32 and 33, of the NZ Public Health and Disability Act 2000: The public now be excluded from the meeting for consideration of the following items, for the reasons and grounds set out below: That, in accordance with the provisions of Schedule 3, Sections 32 and 33, of the NZ Public Health and Disability Act 2000: The public now be excluded from the meeting for consideration of the following items, for the reasons and grounds set out below: General subject of items to be considered 1. Minutes of the Meeting of the Board with Public Excluded 02/11/16 2. Minutes of the Hospital Advisory Committee with Public Excluded 02/11/16 Reason for passing this resolution in relation to each item That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] Ground(s) under Clause 32 for passing this resolution Confirmation of Minutes As per the resolution(s) from the open section of the minutes of the above meeting, in terms of the NZPH&D Act. Confirmation of Minutes As per the resolution(s) from the open section of the minutes of the above meeting, in terms of the NZPH&D Act. Waitemata District Health Board, Meeting of the Board 01/03/17 9
10 2.1 General subject of items to be considered 3.Recommendations of the Audit and Finance Committee with Public Excluded 23/11/16 4. Minutes of the Audit and Finance Committee 05/10/16 5. Minutes of ADHB-WDHB Collaboration Committee Meeting (29/06/16) Reason for passing this resolution in relation to each item That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a) That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] Ground(s) under Clause 32 for passing this resolution Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] Negotiations The disclosure of information would not be in the public interest because of the greater need to enable the board to carry on, without prejudice or disadvantage, negotiations. [Official Information Act 1982 S.9 (2) (j)] Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] Negotiations The disclosure of information would not be in the public interest because of the greater need to enable the board to carry on, without prejudice or disadvantage, negotiations. [Official Information Act 1982 S.9 (2) (j)] Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] Waitemata District Health Board, Meeting of the Board 01/03/17 10
11 2.1 General subject of items to be considered 6. Minutes of the ADHB-WDHB Collaboration Committee Meeting (10/08/16) 6. Tanekaha Unit Business Case 7. CT Scanner Replacement Reason for passing this resolution in relation to each item That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act Ground(s) under Clause 32 for passing this resolution Negotiations The disclosure of information would not be in the public interest because of the greater need to enable the board to carry on, without prejudice or disadvantage, negotiations. [Official Information Act 1982 S.9 (2) (j)] Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] Negotiations The disclosure of information would not be in the public interest because of the greater need to enable the board to carry on, without prejudice or disadvantage, negotiations. [Official Information Act 1982 S.9 (2) (j)] Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] Waitemata District Health Board, Meeting of the Board 01/03/17 11
12 2.1 General subject of items to be considered Reason for passing this resolution in relation to each item [NZPH&D Act 2000 Schedule 3, S.32 (a)] Ground(s) under Clause 32 for passing this resolution Negotiations The disclosure of information would not be in the public interest because of the greater need to enable the board to carry on, without prejudice or disadvantage, negotiations. 8. Electricity Supply Contract(s) That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] [Official Information Act 1982 S.9 (2) (j)] Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] Negotiations The disclosure of information would not be in the public interest because of the greater need to enable the board to carry on, without prejudice or disadvantage, negotiations. 9. Healthcare contract extension That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] [Official Information Act 1982 S.9 (2) (j)] Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] Negotiations The disclosure of information would not be in the public interest because of the greater need to enable the board to carry on, without prejudice or disadvantage, negotiations. [Official Information Act 1982 S.9 (2) (j)] Waitemata District Health Board, Meeting of the Board 01/03/17 12
13 2.1 General subject of items to be considered 10. Radiology Replacement CT Scanner at Waitakere Reason for passing this resolution in relation to each item That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] Ground(s) under Clause 32 for passing this resolution Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] 11.06am to 11.55pm - public excluded session 11.55am to 12.58pm - adjournment 12.58pm - the meeting resumed in open session 3 BOARD MINUTES 3.1 Minutes of the Meeting of the Board - 02/11/16 (agenda pages 11-21) Resolution (Moved Morris Pita/Seconded James Le Fevre) That the Minutes of the Board meeting held on 02 November 2016 be approved. Carried Actions arising from previous meetings (agenda pages 22) The Chief Executive tabled and summarised a memo from the DHB s General Counsel regarding the abdominal aortic aneurysm screening pilot and how the pilot, being offered on the basis of gender and ethnicity, links with the Human Rights Act. The General Counsel has advised that in her view the pilot does not unlawfully discriminate against non-maori men and is not in breach of the Act. 4 EXECUTIVE REPORTS 4.1 Chief Executive s Report (agenda pages 23-49) The Chief Executive introduced and summarised the report. The report was received. 4.2 Health and Safety Performance Report (agenda a pages 50-64) Fiona McCarthy (Director of Human Resources) and Michael Field (General Manager, Occupational Health and Safety) were present for this item. Fiona McCarthy noted that Worksafe New Zealand had provided some new guidance on violence in the workplace and customer areas. She noted that the DHB has since undertaken a review of customer service areas within Mental Health. Waitemata District Health Board, Meeting of the Board 01/03/17 13
14 2.1 Matters covered in discussion and response to questions included: Noting that the DHB is currently undertaking the first round of audits. Noting that with regard to workplace safety and the DHB s policy of staff use of motor vehicles that the DHB has clear guidance for staff when operating a motor vehicle for work purposes. A comprehensive review will be undertaken on the varying types of workplace safety policies. Noting that a gate on the Lake Pupuke jetty will be installed prior to Christmas Noting that in connection with the WINZ decision regarding the Ashburton Case the DHB has already reviewed the Worksafe NZ guidelines and expectations for reception areas. The Board Chair thanked Fiona and Michael and their teams for their work over the past year. The report was received. 4.3 Communications Report (agenda pages 65-72) Matthew Rogers (Director of Communications) introduced and summarised this item. The Board Chair thanked Matthew Rogers and the Communications team for their work over the past year. The report was received. 5 DECISION PAPERS 5.1 Executive Committee of the Board (agenda pages 73-74) The Board Chairman introduced the report. Resolution (Moved James Le Fevre/Seconded Warren Flaunty) a. That the Board approve the establishment of an Executive Committee (under schedule 3 clause 38 of the New Zealand Public Health and Disability Act 2000) to consider any matters that require the urgent attention of the Board during the Christmas/New Year Board recess. b. That membership of the Committee is to comprise the Board Chair, the Deputy Board Chair (Kylie Clegg), Max Abbott, Warren Flaunty and Morris Pita, with a quorum of three members (the Chair or Deputy Chair needs to be one of the three members). c. That the Executive Committee be given delegated authority to make decisions on the Board s behalf relating to the urgent approval of business cases, leases and the awarding of contracts for facilities development, services and supplies and information services and on any other urgent recommendations from a Committee or the Chief Executive (same arrangements as last year). d. That all decisions made by the Executive Committee be reported back to the Board at its meeting on 1 March e. That the Executive Committee be dissolved as at 28 February Carried Waitemata District Health Board, Meeting of the Board 01/03/17 14
15 Hospital Advisory Committee Membership Board Chair verbal report The Board Chairman introduced the report noting that the Board would agree Committee membership at its first meeting in It was noted that all Board members have access to every Committee agenda and that the Chairs of the Committees will provide a detailed update at the Board meetings about Committee meetings held. It was noted that the Deputy Chairs of the metro-auckland DHBs will attend some national meetings of the Board Chairman s behalf. Kylie Clegg noted that attendance at a recent national meeting gave insight into how other DHBs are operating; James Le Fevre also noted that a clear signal expressed was the very real expectation that DHBs work together. Resolution (Moved James Le Fevre/Seconded Warren Flaunty) That the Board: a) Appoints all Board members on an interim basis to the Hospital Advisory Committee. b) Appoints existing co-opted members on an interim basis to the Hospital Advisory Committee. c) Appoints James Le Fevre to Chair the Hospital Advisory Committee on an interim basis. Carried /18 Annual Plan Approach (agenda pages 76-79) Wendy Bennett (Planning and Health Intelligence Manager) introduced this item noting that the Ministry of Health has proposed significant changes to the Annual Plan content and format for 2017/18 as detailed in section 3 of the report (page 77 of the agenda). The Board Chairman noted concern at the removal of the Maori Health Plan and suggested that the DHB continue to provide a Maori Health Plan to ensure service and delivery to Maori continues to be advanced. The Chief Executive also noted that concern at the removal of the Maori Health Plan had been noted at the national Chairs and Chief Executives meeting and was to be reported back to the Ministry of Health. The General Manager, Maori Health (Riki Nia Nia) has also formally written to the Ministry of Health outlining the Waitemata DHB s concerns. Resolution (Moved Matire Harwood/Seconded Kylie Clegg) That the Board: a) Approve the approach to annual planning for 2017/18, including the timetable. b) Note the national planning guidance, including updates and changes. c) Requests that the Maori Health Plan be prepared for Waitemata DHB. Carried Waitemata District Health Board, Meeting of the Board 01/03/17 15
16 Strategic Initiatives - Youth Connections Pledge (agenda pages 80-88) Aroha Haggie (Māori Health Gain Manager, Planning, Funding and Outcomes), Vanessa Duthie (Māori Workforce Development Consultant) and Riki Nia Nia, (General Manager Maori Health) were present for this item. Aroha introduced the report noting the challenge the DHB has regarding youth employment for Maori and Pacific. The Pledge was established with the Council and will allow the DHB to focus on targeting those between 15 and 24 years of age for employment opportunities. Sandra Coney noted that the Auckland Council s Local Board in the area was funding approximately five programmes aimed at assisting Maori and Pacific youth to gain their drivers licence and the like. It was suggested that the DHB connect with the Local Boards on this matter as well. Morris Pita acknowledged the work undertaken by Aroha Haggie and Vanessa Duthie in this area. Resolution (Moved Morris Pita/Seconded Matire Harwood) a) That the Waitemata DHB Board receives the report and recommendation from the Manawa Ora Committee and: b) That the Board endorses the DHB becoming a Youth Employment Pledge Partner with Youth Connections. Carried 6 PERFORMANCE REPORTS 6.1 Financial Performance (agenda pages ) Robert Paine (Chief Financial Officer and Head of Corporate Services) introduced this item. The report was noted. 7 COMMITTEE REPORTS 7.1 Hospital Advisory Committee Meeting - 02/11/16 (agenda pages ) Resolution (Moved Sandra Coney/Seconded Kylie Clegg) That the draft minutes of the Health Advisory Committee meeting held on 02 November 2016 be received. Carried Waitemata District Health Board, Meeting of the Board 01/03/17 16
17 Recommendation from the Auckland DHB and Waitemata DHB Disability Support Advisory Committee Meeting (01/07/16) (agenda page 112) Resolution (Moved Sandra Coney/Seconded Kylie Clegg) That the following recommendation from the Auckland DHB and Waitemata DHB Disability Support Advisory Committee Meeting held on 1 June 2016 be approved: Ref. Item/Recommendation 4.2 Collection of Data for Patients with Disabilities That the Board: 1. Receives the report. 2. Notes that the Auckland Metro DiSAC groups: 2.1. Actively engage with the disability data and evidence working group 2.2. Seek to understand how the need for better disability population data will be reflected in the review of the disability strategy. 3. Notes that that the Auckland Metro DiSAC groups recommend to their Boards that: 3.1. The same method of data collection be employed across the three regional DHBs 3.2. They investigate processes for the collection of the identified data about staff with disabilities A small working party be established representing the three DHBs to establish guidelines relating to the collection of data to support the DHBs to be good employers of people with disabilities. Carried 8 INFORMATION PAPERS 8.1 International Benchmarking of Asian Health Outcomes for Waitemata and Auckland DHB (agenda pages ) Samantha Bennett (Asian, Migrant and Refugee Health Gain Manager) and Dr Lifeng Zhou (Senior Epidemiologist and Asian Health Advisor) were present for this item. The Chief Executive introduced the item and the Board Chair noted that it was a very good review and well presented. Max Abbott also commended all involved and noted it would be important to monitor progress; it was noted that monitoring would occur. The report was noted. Waitemata District Health Board, Meeting of the Board 01/03/17 17
18 /2018 Budget process Delivering Strategic and Financial Outcomes (agenda pages ) Simon Watts (Deputy Chief Financial Officer Provider) and Robert Paine (Chief Financial Officer and Head of Corporate Services) presented this this item. Simon noted that the process is part of a regional initiative. The report was noted. 8.3 Health and Safety Marker Report - Update (agenda pages ) Fiona McCarthy (Director of Human Resources) presented this item noting that the incident investigation had concluded with all others scheduled to be completed by May The report was noted. The Chair thanked those present. The meeting concluded at 2.02 pm SIGNED AS A CORRECT RECORD OF THE MEETING OF THE WAITEMATA DISTRICT HEALTH BOARD - BOARD MEETING HELD ON 14 DECEMBER 2016 CHAIR Waitemata District Health Board, Meeting of the Board 01/03/17 18
19 2.1 Actions Arising and Carried Forward from Previous Board Meetings as at 22 February 2017 (No current items) Waitemata District Health Board, Meeting of the Board 01/03/17 19
20 Confirmation of Minutes of the Executive Committee of the Board meeting held on 14 February 2017 Recommendation: That the Minutes of the Executive Committee of the Board meeting held on 14 February 2017 be approved. Waitemata District Health Board, Meeting of the Board 01/03/17 20
21 2.2 Minutes of the Meeting of the Waitemata DHB Executive Committee Wednesday 14 February 2017 held by teleconference commencing at 12.07p.m. Part 1 - Items considered in public meeting COMMITTEE MEMBERS PRESENT: ALSO PRESENT: Lester Levy (Board Chairman) Morris Pita Kylie Clegg (Deputy Board Chair) Dale Bramley (Chief Executive Officer) Robert Paine (Chief Financial Officer and Head of Corporate Services) Peta Molloy (Board Secretary) PUBLIC AND MEDIA REPRESENTATVES: There were no members of the public or media representatives present. APOLOGIES: Apologies were received and accepted from Max Abbott and Warren Flaunty. DISCLOSURE OF INTERESTS: There were no notifications of additions or amendments to interests that had been previously advised by members. There were no identified conflicts of interests for this agenda. 1 Resolution to Exclude the Public Resolution (Moved Kylie Clegg/Seconded Morris Pita) That, in accordance with the provisions of Schedule 3, Sections 32 and 33, of the NZ Public Health and Disability Act 2000: The public now be excluded from the meeting for consideration of the following items, for the reasons and grounds set out below: Waitemata District Health Board, Meeting of the Board 01/03/17 21
22 2.2 General subject of items to be considered 1. Approval for payments for C Class Shares in health Alliance 2. Crown Debt Equity Swap Approval Report 3. Mental Health Courtyard Reason for passing this resolution in relation to each item That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] Ground(s) under Clause 32 for passing this resolution Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] Negotiations The disclosure of information would not be in the public interest because of the greater need to enable the board to carry on, without prejudice or disadvantage, negotiations. 4. General Ward That the public conduct of the whole or the Bed Replacement relevant part of the proceedings of the Programme meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] [Official Information Act 1982 S.9 (2) (j)] Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S.9 (2) (i)] p.m p.m. - public excluded session The meeting concluded at p.m. SIGNED AS A CORRECT RECORD OF THE EXECUTIVE COMMITTEE MEETING OF THE WAITEMATA DISTRICT HEALTH BOARD HELD ON 14 FEBRUARY 2017 CHAIR Waitemata District Health Board, Meeting of the Board 01/03/17 22
23 3.1 Chief Executive s Report 3.1 Recommendation: That the report be received. Prepared by: Dr Dale Bramley (Chief Executive Officer) Key Points A number of significant events have taken place across the DHB of late including the launch of the International Benchmarking of Asian Health Outcomes Report for Auckland and Waitemata DHBs. The overall finding is that Asian peoples as one group experience excellent health outcomes in Auckland and Waitemata compared with the rest of the country, and when benchmarked internationally. In a recent release of Official Information Act statistics by the State Services Commission, Waitemata was the most compliant of the large metropolitan DHBs and ranked third of 20 DHBs overall. A number of projects under the Leapfrog Programme are well-advanced, with some due for completion shortly, e.g. the Community Allied Health mobile tablet project and a new phase of the Programme is underway for 2017, including a revised Outpatient Follow-up Project. As part of monitoring our performance against DHB priorities, a national inpatient survey was conducted in November 2016 which showed a modest improvement compared with previous results. The Friends and Family Test conducted in November and December 2016 produced a Net Promoter Score of 73 and 74 respectively, well above the DHB target of 65. The Northern Region is working on a Long Term Investment Plan to guide all significant future capital investments in the region. A progress report will be provided in due course. Latest health target results for DHBs shows strong performance by Waitemata. It is leading the country for both the childhood obesity target and the cancer target. Waitemata also performed exceptionally well on the ED target and exceeded expectations on the elective target. Progress continues to be made on the immunisation and smoking targets. 1. News and events summary A number of events of significance took place across the DHB over the past six weeks: At their meeting on 20 January 2017, the Northern Regional Executive Forum agreed in principle for Waitemata DHB to act as the Northern Bowel Screening Regional Centre. Subject to confirmation of funding, the Northern Cancer Network will collaborate and support Waitemata DHB with the development of the Centre. The International Benchmarking of Asian Health Outcomes Report for Waitemata and Auckland DHBs was launched on 9 February in conjunction with the DHB s Asian Health Service's Lunar New Year celebration. The report profiles the health of Waitemata and Auckland DHBs Asian populations in an international context considering Asian health status against life expectancy Waitemata District Health Board, Meeting of the Board 01/03/17 23

24 3.1 and health outcomes. The report details areas of high and low performance, issues and unmet need for Asian subgroups with suggested recommendations highlighted for maintaining, improving or accelerating health status where there are identified health outcome differences. The overall findings highlight that Asian peoples as one group experience excellent health outcomes and health status in Auckland and Waitemata compared to the rest of the New Zealand population, and when benchmarked internationally. The areas benchmarked include high life expectancy at birth, lower rates of infant mortality, and lowest rate of Years of Life Lost (YLL) from CVD and cancer. In the Waitemata district Asian peoples have a life expectancy of 90 years at birth. For the Chinese population in Waitemata, life expectancy is a remarkable 92.9 years. The impact from diabetes for both DHBs was also low when considered internationally. These results are consistent with the well-established phenomenon of the healthy migrant effect. Our challenge is to maintain these excellent results and address areas where issues are emerging for some Asian sub groups. The report identifies specific points of focus and outlines some recommendations that will help us maintain world-class health status for our Asian population. These include the future burden of lifestyle-associated risk factors such as smoking and obesity, the ability of the Asian population to get information on the health and disability system, and access to culturally appropriate health services in a timely manner. We are highly committed to achieving and maintaining equitable health outcomes for the multiple, varied population groups in Auckland and look forward to working with our many partners who are passionate about Asian health and wellbeing. l-r: Chinese cultural performer from Colourful Art Performing Group, Grace Ryu Operations Manager Asian Health Services, Samantha Bennett Manager Asian, Migrant and Refugee Health, Dr Lifeng Zhou - Senior Epidemiologist and Asian Health Advisor, Dr Dale Bramley Chief Executive, Jenny Kim Asian Cultural Support Coordinator. Waitemata District Health Board, Meeting of the Board 01/03/17 24

25 3.1 Ribbon Cutting Ceremony at the report launch - l-r: Jenny Kim, Dr Dale Bramley, Naida Glavish, Samantha Bennett, Grace Ryu, Dr Lifeng Zhou On 2 February, Board Chair Dr Lester Levy announced to all metro Auckland DHB staff that the three DHBs will be working more closely as part of an integrated system. Waitemata DHB welcomed this announcement and is committed to working with Auckland and Counties Manukau DHBs to provide the best possible care for the people of Auckland, an approach we take across many services already. This is a great opportunity to meet the challenges of a growing population with innovation in the way healthcare is delivered. The chance to share and learn from what each DHB does best will significantly benefit our services and the people we care for. On 8 February, the Board Chair, Chief Executive and Chief Medical Officer appeared before the Health Select Committee (HSC). The Committee was interested to hear of the progress Waitemata DHB is making, the HSC expressed strong interest in International Benchmarking of Asian Health Outcomes Report discussed above. The State Services Commissioner published the first set of Official Information Act (OIA) performance statistics covering 110 different government agencies on 31 January. The statistics have been released as part of a wider programme of work to improve compliance to the Official Information Act to build New Zealanders trust and confidence in government agencies. The first publication of statistics details the number of requests each agency received during the 2015/16 financial year (1 July June 2016) and whether they were handled within the timeframe required by the OIA. Over time the information on performance that is gathered and published will increase to provide a more comprehensive picture of compliance with the letter and spirit of the Act. Whilst DHBs were identified as a group needing to improve, Waitemata was the most compliant of the large metropolitan DHBs and third of the 20 DHBs in compliance overall. During the 2015/16 financial year the DHB received 208 requests received of which 97.6% were processed within the timeframe stipulated by the Act. The full report can be found on the State Services Commission website: Considerable progress has been made on the development of Whēnua Pūpuke, the DHB s new Clinical Skills Centre. Situated on the lakefront, it will house many of the academic activities Waitemata District Health Board, Meeting of the Board 01/03/17 25

26 3.1 taking place across the DHB with a 250 seat auditorium as well as clinical and teaching spaces. A clinical skills laboratory will occupy a significant portion of the first floor where an AUT exercise testing laboratory will also be located. The centre will officially open on 6 June with a number of events scheduled to take place during opening week including a public open day on 7 June where staff and visitors will tour the facility and learn more about the DHB and its groundbreaking e-health developments. Various displays are also being planned to highlight the work being done by the Māori, Pacific and Asian health teams and the Well Foundation. Simulation equipment will be exhibited and AUT will have a range of interactive stations set up in its Biomechanics Lab. The programme for the opening will be finalised in the coming weeks. Progress well underway on Whēnua Pūpuke, Waitemata DHB s dedicated Clinical Skills Centre Christmas festivities are a highlight each year across the DHB. Last year was no exception with an extensive programme of activities across hospital and community sites for staff and patients to celebrate the season. Events included services in our hospital chapels for patients, visitors and staff; community choirs caroling in the wards and special visits from Silver Fern Maria Tutaia and Breakers player Tom Abercrombie. The standard of festive decorations among our various teams was truly outstanding. Many staff went to considerable effort to bring Christmas cheer to our patients and their colleagues. I want to thank the teams and individuals for the passion and hard work that went into celebrating the season. We received a record number of entries into the annual Christmas decoration competition and each year the displays are more impressive than the last. The winners were: North Shore Hospital Overall winner: Ward 3 and Ward 6 (joint-winners) Runners-up: Hine Ora and PACU Winner for Community North Shore campus: 3 Mary Poynton Crescent (Asian Health Services, Quality Team, Smokefree Services) Runner-up for Community North Shore campus: 15 Shea Terrace (level 2) Winner for most edible design: 15 Shea Terrace (level 1) Runners-up for most edible design: Clinical Records and Radiology Waitemata District Health Board, Meeting of the Board 01/03/17 26
 Community sites Overall winner: Slark Hyperbaric Unit Overall runners-up:")
27 3.1 Waitakere Hospital campus CEO award for outstanding effort: Ethel Aguirre Henderson - CSS Overall winner: Rangatira and Titirangi (joint-winners) Overall runner-up: Allied Health Winner for most edible design: Allied Health Highly commended: Maternity, Diabetes, Radiology, SCBU, Anawhata CNM office (Donna Riddell) Community sites Overall winner: Slark Hyperbaric Unit Overall runners-up: Mason Clinic prisoner liaison team, Bowel-screening co-ordination centre Highly commended: Wilson Centre, Karaka Allied Health team, Karaka district nursing, CADS, Child, Women and Family Services Taharoto, Corporate offices - 15 Shea Terrace. Stuff.co.nz visited Rangatira Ward at Waitakere Hospital producing a video capturing the spirit of the Christmas competition: Waitakere-Hospital Slark Hyperbaric Unit s award winning decorations Waitemata District Health Board, Meeting of the Board 01/03/17 27

 programme.")
28 3.1 Allied Health teams at Waitakere Hospital getting into the Christmas spirit with their Kiwi bach-themed display On 7 February we welcomed 106 new graduate nurses into our workforce with an event held at Waitakere Hospital s conference room. Senior nurses were among the DHB tangata whenua there to congratulate graduates on the first day of their careers. This is the largest intake of graduate nurses ever at the DHB, with 72 joining our General Health services, 20 joining Primary Health services across the DHB and a further 14 joining our Mental Health services. All graduates will undertake the DHB s Nursing Entry To Practice (NETP/NESP) programme. The intake demonstrates the DHB s commitment to expanding our clinical workforce and fostering the growth and development of our future leaders in nursing. Senior nurses greet new graduates at the welcome event held at Waitakere Hospital Dr Peter van de Weijer, Clinical Director of Obstetrics and Gynaecology and Head of the Division Child and Women and Family Services, officially resigns this month after six years at Waitemata DHB. Peter has been a true champion for empowering women to take ownership of their health. Waitemata District Health Board, Meeting of the Board 01/03/17 28

29 3.1 In 2012 Peter pioneered e-consults, providing the primary caregiver with specialist support and advice on how to manage discomfort and disease in the primary care setting. The programme has allowed patients to access specialist advice and have this incorporated into a management plan by their GP. It has enabled women to make decisions about their health in a setting they are comfortable with, enhancing patient experience and reducing the need for hospital visits. Peter will also be remembered for the guidance and encouragement he has provided for young doctors. I would like to thank Peter for his leadership and considerable contribution to the DHB. Director of Nursing Jocelyn Peach with Dr Peter van de Weijer speaking at his retirement morning tea In 2015/16 the Board supported a business case to greatly increase staffing levels of the Child and Adolescent Mental Health Service through the delivery of a new service based in the north Rodney area. On 12 December, the service was officially opened in Orewa and will shortly house its complete staff quota of nine fulltime clinical staff, including a psychiatrist. The service has been tailored to ensure the right treatment is available in the right place, at the right time with the increase in staffing to greatly enhance access to high quality mental health services for local families and whānau. Staff based in the Orewa facility will have the flexibility to travel to meet demand within the broader north Rodney area. The development reflects the DHB s ongoing commitment to measure demand and provide high quality, accessible child and adolescent mental health services as our population grows. Waitemata District Health Board, Meeting of the Board 01/03/17 29

30 3.1 Mental Health Services staff at the launch of the new north Rodney CAMHS service - l-r: Selena Griffith, Danielle Morrison, Shreya Rao, Michelle Ball, Janette Backhouse, Dr Mirsad Begic, Heloise Pilling, Lorraine Emerson, Rachael Meese The DHB had its Health and Disability Service Standards certification audit for the Ministry of Health in November. This certification audit included site visits to North Shore and Waitakere hospitals, Mason Clinic and Wilson Centre. Positive feedback was received from auditors who made special mention that the DHB had no corrective actions needed around nursing documentation, a rare feat for a DHB to achieve. I would like to congratulate our nursing staff for their efforts. Auditors were also impressed with the link of organisational values to our practice and patient experience stating that the values are embedded in quality programmes across the organisation and are the foundations for decision making, along with clinical engagement and leadership. Whilst the report identifies areas for improvement, I would like to thank all staff and services involved in the auditing process and for showing great commitment to quality improvement for our patients and community. A number of Waitemata DHB initiatives were profiled on national news media over the summer period: Māori Television s Te Kāea news bulletin featured an item on the DHB s screening pilot programme to address Abdominal Aortic Aneurysm (AAA) in Māori on 16 December. The DHB is working to address nationally-recognised inequalities between non-māori and Māori in health outcomes and this is one area where significant, positive inroads are being made. About 220 New Zealand men die of AAA in New Zealand each year and Māori are at a significantly higher risk of dying from AAA than non-māori. Additionally, Māori also appear to develop this condition about eight years earlier than non-māori. Waitemata carried out an AAA pilot screening programme in 2016 across three general practices in the Waitemata district. Preliminary results were so convincing that the pilot programme has now been extended to the Māori population (men aged and women aged 65-74) enrolled with a general practice under Auckland and Waitemata. Screening will take place between January and September Waitemata District Health Board, Meeting of the Board 01/03/17 30
31 3.1 TVNZ 1 featured the DHB s successful e-prescribing roll-out on the 6pm, 22 December bulletin. The implementation of e-prescribing began in a 55-bed ward in November Late last year the roll-out of electronic medication management was completed to all acute beds. It is a significant achievement for the DHB, which now has the largest number of beds implemented of any single DHB in NZ, delivering epa across 970 beds in its North Shore and Waitakere Hospitals, as well as various other major clinical sites. The DHB s work to improve patient sleep in our hospitals was profiled on TV3 s 6pm, 29 December bulletin. The item featured activity undertaken through patient feedback channels to understand factors preventing patients from getting quality sleep in our clinical environments. It highlighted a number of actions undertaken by the DHB to optimise sleep including the introduction of sleep packs as part of a pilot programme in three wards and sleep audits to assess the physical and auditory environment of clinical spaces. Further details can be found in the Patient Experience section of this report. Creating a culture of appreciation A further 27 staff have been recognised in the CEO Awards, launched in mid-2014 to celebrate those staff, nominated by their colleagues and patients, who demonstrate our organisational values through their work. Each staff member whose nomination is considered worthy of acknowledgement receives a personalised letter of thanks, a certificate of appreciation and a small gift. Staff acknowledged with a CEO Award since the last Board meeting include: Michael Parker, Acting Professional and Clinical Leader, Allied Health Prof. Leadership - Allied Health, nominated by Margaret Ross Organised the inaugural MHS OA OT symposium which was held at Waitemata DHB. Tazman Waata, Occupational Therapist, Inpatient North Therapies - Allied Health, nominated by Mosese Rigamoto Petrie Raddock, Physiotherapist, Inpatient North Therapies - Allied Health, nominated by Mosese Rigamoto Tazman and Petrie are two inspirational key workers with client centeredness, respect and compassion who used these traits recently to engage with a client. Josilina Silimaka, Personal Assistant - Pacific Support Services, nominated by Pulotu Bruce Levi Josilina works tirelessly and always cheerfully for the leadership and Tautai Fakataha teams of Pacific Health. David Price, Director - Patient Experience, nominated by Alan Jenner Following a complicated situation, David s repeated and continual involvement went way beyond the call of duty and our expectations, and helped smooth the waters marvellously. Dr Jye Lu, O&G Consultant and Gynae Oncology Lead - Gynaecology Services, nominated by Gwyneth Capes and Nikki Cole Her enthusiasm in this new role has already made a difference to Waitemata patients along their cancer journey and continues to do so. Linda Halfpenny, Vision and Hearing Technician - Child and Family West, nominated by Carole Harkness Upholds values of better, best, brilliant ensuring she consistently screens a high number of children for the B4 School Check Programme. Waitemata District Health Board, Meeting of the Board 01/03/17 31
32 3.1 Maxine Barnard, Administrator - Gateway Assessment Programme and Violence Intervention Programme, nominated by Sarah Watson Maxine is a hard-working, positive person who is always willing to help others and she shows great compassion to her colleagues. Shane Fullam, Information Systems Specialist- Health Information Group, nominated by Jennifer Kyme Shane is a credit to his department and a pleasure to work with. Sara Mellow, House Officer- General Medical, nominated by Lee Roberts - Ward 5 Nothing is too much trouble. She is kind and caring. An asset to Waitemata DHB. Linda Thompson, Registered Nurse - Home Health Support West, nominated by Sarah McKinlay For maintaining her cheerful attitude and entertaining both staff and patients in her daily work. Karen Fresco, Registered Nurse - Home Health Support West, nominated by Sarah McKinlay For her tireless efforts to support the wound care shared care project at Health New Lynn. Kylie Amai, Registered Nurse - Home Health Support West, nominated by Sarah McKinlay Kylie is passionate and dedicated to her role and this shines through when with her patients. Hannah O'Brien, Enrolled Nurse - Home Health Support West, nominated by Sarah McKinlay Hannah is one of our newly qualified enrolled nurses and has grown so much in her abilities in the last year. Denise Huggard, Registered Nurse - Home Health Support West, nominated by Sarah McKinlay Denise has overcome many challenges this year and has maintained her abilities to deliver good care. Trenna Wilkinson, Charge Nurse Manager - Wainamu Ward, nominated by Shelley Vaudrey Trenna is dedicated, professional, hardworking, passionate, and always works with patients and whanau as her main focus. Melanie Shields, Occupational Therapist - MHSOP, nominated by Margaret Ross Karyn Campbell, Occupational Therapist - MHSOP, nominated by Margaret Ross Sandra Tait, Occupational Therapist - MHSOP, nominated by Margaret Ross Helped organise the inaugural MHS OA OT symposium which was held at Waitemata DHB. Sinead O'Malley, Registered Nurse - Emergency Care Centre, nominated by Sue Lamb Judy Vette, Registered Nurse - Emergency Care Centre, nominated by Sue Lamb Diane Bratton, Nurse Educator- Emergency Care Centre, nominated by Sue Lamb For providing support and guidance, over and above the requirements, to staff settling in a new department. Doreen Retimana, Registered Nurse - Rata Unit, nominated by Stuart Dysart Pauline Matthews, Staff Nurse - Rata Unit, nominated by Stuart Dysart For their dedicated hard work, team spirit and contribution to the preparation for the Patient and Whanau centred care standards. Tina Harrison, Clinical Team Leader - CADS West, nominated by Diana Turner Tina has provided outstanding support, understanding to not just myself but other members of our team when unexpected life and family events occur. Janine Hatton, Forensic Prison Team - Mason Clinic, nominated by Shivika Singh For handling issues of all sorts, taking calls throughout the day and much more while being great in every way. Fiona Hollis, Outpatient Receptionist - ICU, nominated by Vicki Hustler For excellent customer service and data quality. Waitemata District Health Board, Meeting of the Board 01/03/17 32
33 2. Upcoming events 3.1 Looking toward the upcoming months, we can expect to see: Progress on construction of the Clinical Skills Centre on the North Shore Hospital campus with the official opening week planned for 6 June. Opening of the Waitakere Hospital gym for staff. Opening of the refurbished Community Building 5 on the North Shore Hospital campus to house outpatient clinics. The building has been gifted the name Kahui Manaaki cluster of kindness by Chief Advisor Tikanga Naida Glavish. Dawn blessing for the opening of Waitakere Hospital Emergency Department s dedicated paediatric zone on 23 February. Full opening of stage 2 of Waitakere Hospital s expanded Emergency Department scheduled for April/May with formal opening date to be advised. Patient Experience Week in April. All-staff survey to enhance understanding and engagement in our workforce. The inaugural Living with Type-1 Diabetes Awards to acknowledge patients who have successfully managed the condition long-term. Commencement of the CEO Lecture Series 3. Future Focus The Leapfrog programme was established as a means to support a focused, intensive burst to take a large leap in moving the DHB from where we are to where we want to be. The programme consists of a small number of strategic organisation-wide projects that are resourced to achieve significant change and impact on health outcomes and patient/family experience. The intended benefits are to move these projects along at a faster pace with top-level support for the significant changes required, giving greater visibility and attention to those projects identified as being important in achieving the DHB s priorities and purpose as well as instilling the culture of improvement and innovation. Under the Mobility Strategy, design is underway of the first Mobile Enterprise Application Platform (MEAP) app MyPatientList. The app will support clinicians in managing their tasks and will integrate with patient information systems. The Community Allied Health mobile tablet project evaluation will be completed this month. Early indications are very positive in terms of time saved, increase in patient visits, and patient ratings of use of the ipads during consultations. eprescribing is currently being implemented in the Intensive Care Unit (ICU) with a number of staff working in innovative ways to resolve issues specific to this clinical environment. The Voice-to-Text project has progressed with the roll-out now on track and authors steadily increasing beyond 80. The latest feedback from Winscribe is that our transcriptionists using the editing functionality from the speech recognition module are 50% faster. They have gone from the base-lined 12 minutes dictation processed per hour to 18 minutes. Put differently, one minute of dictation used to take five minutes to type and now takes three minutes. Waitemata District Health Board, Meeting of the Board 01/03/17 33
34 3.1 The elaboratories team are working on an April go live date for the foundation implementation in Older Adults Services. This has included the internal development of new forms with printed colour-coded tube labels that peel off the back of the form. evitals has rolled out to 764 beds across both hospital sites with the team are now working on maternity and paediatrics systems and nursing assessments. A variation is required adding the Emergency Department (ED) to the scope and extending the timeline by five months to July This will allow the full potential and benefits of the system to be realised, yet remain within the overall approved budget, despite earlier delays in the provisioning of environments. The Patient Experience Reporting System (PERSy) project is in close-out phase. The next phase for this project will involve services collecting patient reported outcomes measures (PROMS), including for the Precision Driven Health funded HOPE research project. The next phase of the Leapfrog Programme is underway for This includes a revised Outpatient Follow-up Project to extend the focus and priority of this area. An options analysis and case for check-in kiosks in the outpatients service is in preparation, and trials of remote consultations using telehealth are planned as part of a healthalliance-led regional process. Data discovery is already underway with the implementation of a Business Intelligence (BI) tool as the first step in developing clinical dashboards. 4. Outcomes discussion This month, I have asked Dr Karen Bartholomew to summarise a Waitemata-DHB led survey of Māori patients and whānau admitted with Ambulatory Sensitive Hospitalisations (ASH). A paper on the survey was authored by Carol Barker, Sue Crengle, Dale Bramley, Karen Bartholomew, Patricia Bolton, Michael Walsh, Jean Wignall and published in the New Zealand Medical Journal, October Ambulatory Sensitive Hospitalisations Survey (ASH) Admissions for ASH conditions represent admissions that are potentially preventable with high quality timely primary care. Although rates for preschool ASH admissions at Waitemata DHB are comparatively low nationally, Māori and Pacific rates are 2-4 times higher than other population groups. The survey examined local pathways to hospitalisation for Māori. The results provide an alternative to the usual narrative surrounding ASH. Participants demonstrated appropriate health seeking behaviour, pertinent use of secondary care services and accurate recall of diagnoses. The survey also found high levels of engagement with primary care with high rates of self-reported enrolment, utilisation and preference for primary care. Issues with access out of hours, transport and same day appointment availability were noted. Preschool ASH is one of the new System Level Measures (SLM) being introduced by the Ministry of Health. The primary care Alliance Leadership Team (ALT) and the DHB have an agreed SLM improvement plan; for ASH these include an initial focus on immunisation, oral health and skin infections. The Māori Health Plan includes further work on asthma readmissions and the development of a process to support primary care enrolment for all Māori patients admitted with ASH, where a GP is not identified. Waitemata District Health Board, Meeting of the Board 01/03/17 34
35 3.1 About the survey: Aim: Ambulatory Sensitive Hospitalisations (ASH) are a group of conditions potentially preventable through interventions delivered in the primary health care setting. ASH rates are consistently higher for Māori compared with non-māori. This study aimed to establish Māori experience of factors driving the use of hospital services for ASH conditions, including barriers to accessing primary care. Method: A telephone questionnaire exploring pathways to ASH was administered to Māori (n=150) admitted to Auckland and Waitemata District Health Board (DHB) hospitals with an ASH condition between January 1 June 30, Results: A cohort of 1,013 participants were identified; 842 (83.1%) were unable to be contacted. Of the 171 people contactable, 150 agreed to participate, giving an overall response rate of 14.8% and response rate of contactable patients of 87.7%. Results demonstrated high rates of self-reported enrolment, utilisation and preference for primary care. Many participants demonstrated appropriate health seeking behaviour and accurate recall of diagnoses. While financial barriers to accessing primary care were reported, non-financial barriers including lack of after-hours provision (12.6% adults, 37.7% children), appointment availability (7.4% adults, 17.0% children) and lack of transport (13.7% adults, 20.8% children) also featured in participant responses. Conclusions: Interventions to reduce Māori ASH include: timely access to primary care through electronic communications, increased appointment availability, extended opening hours, low cost after-hours care and consistent best management of ASH conditions in general practice through clinical pathways. Facilitated enrolment of ASH patients with no general practitioner could also reduce ASH. Research into transport barriers and enablers for Māori accessing primary care is required to support future interventions. A complete copy of the survey can be found as an appendix to this report (Appendix 1). Waitemata District Health Board, Meeting of the Board 01/03/17 35
36 3.1 Waitemata District Health Board, Meeting of the Board 01/03/17 36

37 3.1 Waitemata District Health Board, Meeting of the Board 01/03/17 37

38 3.1 Waitemata District Health Board, Meeting of the Board 01/03/17 38
39 5. Board performance priorities 3.1 The following provides a summary of the work underway to deliver on the DHB s priorities: Relief of suffering Progress: a Patient and Whānau-Centred Care Patient feedback Health Quality and Safety Commission National Inpatient Survey The last National Survey for 2016 was conducted in November. We received responses from 153 people a 38% survey return rate for Waitemata DHB. All domains are up 0.1 point in comparison to last quarter, except for Partnership. Overall, in comparison to 2015 national survey results, an increase of 0.2 points in Communication and Partnership domains, with no change for Coordination and Needs. The results for the four domains: Year & Quarter Total Communication Partnership Coordination Needs Surveys Oct - Dec Jul - Sep Apr - Jun Jan - Mar Overall Overall Other significant results in the National Survey to highlight for the last quarter of 2016: - 59% of survey respondents are aged over 65. These respondents are also most satisfied with their experience compared to other age groups. - Respondents between the ages (23% of respondents) are least satisfied with their experience scoring below 8 in all survey domains. - 70% of respondents were NZ European, 9% other ethnicity, 4% Māori/NZ European and 3% Māori. - Privacy, explanation of surgery, confidence in nursing staff and treated with respect and dignity are the four questions where Waitemata DHB has performed most highly. - Family/whānau inclusion in care, explanation of medication side effects, cleanliness of ward/hospital and enough information to manage condition on discharge are the four questions where improvement is indicated. Friends and Family Test During November and December 2016 we received feedback from 1,957 people through the Friends and Family Test (FFT). The Net Promoter Score (NPS) for November was 73 and for December 74, well above the DHB target of 65. December had the highest recorded NPS for Waitemata District Health Board, Meeting of the Board 01/03/17 39


40 3.1 November results December results Waitemata District Health Board, Meeting of the Board 01/03/17 40
41 3.1 Total Responses to Family and Friends Test across Waitemata DHB Family and Friend Test Comments Even though our visit today was unscheduled everybody in your team was friendly and helpful and showed lots of empathy, thank you. - Orthopaedics Outpatients NSH Such a diverse range of people all work here with one thing in common, they all made me feel welcome, smiled and nothing was a problem. Thanks everyone. Wainamu Ward WTK Didn't have to wait long and saw 2 doctors very quickly who were very friendly and understandable. Outpatients ORL NSH Friendly service and keeping us informed with her progress from the start to finish including diagnosis and medication and all the help you guys have done including options in her health. ICU/HDU NSH I'm extremely grateful to the doctors and nurses who have been so kind and are amazing at their job. I cannot say thank you enough. Every member on the team at SCBU deserves a medal or a large pay rise. They work so hard and take the time. SCBU WTH You have been very patient and given me the assistance I needed. Explained clearly. Nice to have someone sympathetic to talk to. - Allied Health Community Adults Rodney Waitemata District Health Board, Meeting of the Board 01/03/17 41

42 3.1 Happy Or Not Happy or Not machines are placed in specific thoroughfares or service areas were people are asked to press a button to rate how welcoming and friendly we were in relation to their recent visit. Reports are sent daily to each area with a breakdown of times of day, to highlight specific times or days of excellent performance or opportunities for improvement. December results Patient Experience Strategy for The Patient Experience strategy is nearing completion with the following aims underpinning all patient experience work. It will come to the Board for endorsement in April Patient Information Patient Information booklet The North Shore Hospital patient information booklet pilot has been completed. Due to positive feedback from both staff and patients the booklet will be updated and launched across North Shore Hospital for all patients to have access to a variety of information. The information provides great insights into all the various services available to our community and specific functions of the hospital. The Waitakere Hospital information booklet will be piloted within the first half of Thank you to Waitakere Health Link and Health Link North for their ongoing contribution to this project. Waitemata District Health Board, Meeting of the Board 01/03/17 42
43 3.1 Outpatient Letters The Patient Experience Team in partnership with Waitakere Healthlink and Healthlink North is reviewing the more than 700 outpatient letters currently sent by the DHB. The main aim of the review is to reduce the amount of letters, ensure the letters are welcoming and friendly and to meet the health literacy needs of our community. A majority of these letters have now been reviewed. Wayfinding maps and a brochure will be provided to assist patients in preparation for their outpatient visit including suggested questions to ask at the appointment. Patient Experience Activity Sleep Pack Pilot Sleep is one of the top three patient feedback themes reported through Waitemata DHB family and friends tests and the National Patient Experience Survey. The Well Foundation has sponsored the creation of sleep packs that are currently being piloted on Ward 2, Muriwai and Titirangi wards. The sleep packs, which were put together by volunteers, have an eye mask, ear plugs, camomile tea, an education pamphlet on sleep and a Well Foundation information pamphlet. Due to the success of the pilot the packs will be rolled out across the organisation in early Volunteer Recruitment Campaign The volunteer programme has started a recruitment campaign to increase volunteer numbers across the organisation. Articles have been printed in local newspapers celebrating the service many long term volunteers have given, as well as targeted articles on social media for volunteer recruitment. The Volunteer Coordinator has fielded numerous calls from potential volunteers. Patient Experience Week 2017 The dates for Patient Experience week celebrations have been confirmed 24 to 28 April Promotion of Patient Experience initiatives will take centre stage across the organisation during this period. This is in line with the international week of celebrations for Patient Experience. The proposed timetable of events will be available from mid-february, with joint Auckland regional events. Other Patient Experience Activity There are a number of service improvement activities that the Patient Experience team are currently supporting: - Trial of music therapy in North Shore Hospital rehabilitation wards - Orthopaedics outpatient experience - exploring other methodologies to understand the patient experience - Maternity service patient experience survey and phone call interviews - e-learning patient experience training module - Patient story programme review - Exploring the options for improving maternity inpatient food including self-service breakfast - Oncology services patient experience phone call interviews. Waitemata District Health Board, Meeting of the Board 01/03/17 43
44 3.1 Facilities Major capital projects need strong regional support and alignment. The Northern Region is working on a Long Term Investment Plan (LTIP) to guide all significant future capital investments in the region. The Board will be regularly updated on this work going forward. North Shore Hospital Sky Bridge Main project is complete including the bridge lights donated by ECC Limited. North Shore Hospital Community Building 5 Asbestos removal and remediation of structural defects has been concluded and construction will be complete on 15 March This will be followed by final fit-out of furniture, fittings and commissioning. Operational opening is planned for April North Shore Hospital Surgical Pathology Offices Relocation The offices opened in December as planned. Surgical Pathology has moved into the new office. Feedback following the move has been very positive. North Shore Hospital Pupuke Building Services Relocation Pupuke, Marinoto and Te Whiringa are vacated and are being prepared for demolition. QTR and Taharoto South remain occupied pending confirmation of the demolition programme. Tenders for demolition works close mid-february. Tender review, demolition options and recommendations will be prepared for submission for approval by end of March. Waitakere Hospital Emergency Department Redevelopment The facility is operating well. Some small changes to signage, window treatment and sound proofing are required near reception to enhance privacy. Waitakere Hospital additional ED Facility Improvements The multiphase refurbishment of the existing footprint is progressing well and due for completion in April Waitakere Hospital Additional Beds Wainamu and Muriwai Wards RCC healthcare is progressing construction works with anticipated disruptions to the wards generally as planned. To date there have been no major issues and both patients and staff are coping well with the necessary works. Elective Capacity and Inpatient Beds business case to Capital Investment Committee (CIC) The short list of options and Strategic Assessment have been submitted to the CIC for review. Mason Clinic presentation to CIC for refurbishment of Tanekaha Following Board endorsement the Tanekaha indicative business case was submitted to Treasury and CIC in December 2016 for approval. Feedback is awaited from the CIC. Replacement Wards Project Waitemata DHB continues to proceed with planning and development of the Investment Logic Mapping to support the business case. This will ensure that the two items are created in parallel and there are no time delays. The Risk Profile Assessment (RPA) has been submitted to Treasury. Point of Entry document will be submitted following feedback from Treasury on the RPA. Work continues on developing the functional design briefs, models of care and accommodation schedules that will inform design. Waitemata District Health Board, Meeting of the Board 01/03/17 44
45 3.1 Better Outcomes Progress: On track a Achieving the health targets as at December 2016: Shorter waits in Emergency Departments 98% (target 95%) Improved Access to Elective Surgery 105% (target 100%) Increased immunisation 92% (target 95%) Better help for smokers to quit - maternity 78% (target 90%) Raising healthy kids 100% (target 70%) Faster Cancer Treatment (FCT 62 days) 90% (target 85%) Health Quality and Safety Markers December 2016 Falls Falls risk assessment audits that inform the Health Quality and Safety Commission data continue and are conducted monthly. Overall Acute and Emergency Medicine completed 97% of falls risk assessments, Specialist Medicine and Health of Older People completed 100% and S & A completed 93 % on admission. Of those, Acute and Emergency Medicine completed 93%, Specialist Medicine and Health of Older People completed 95 % and S & A completed 70% within eight hours of admission (against a target of 90%) Hand Hygiene Waitemata DHB s Hand Hygiene Audit results for December 2016 are a compliance rate of 85.3% exceeding the national target of 80%. Healthcare-Associated Infections The CLAB insertion bundle was used in ICU on 100% of occasions in December The insertion bundle compliance meets the national target of 90%. Health Quality and Safety Markers - January 2017 Falls Falls risk assessment audits that inform the Health Quality and Safety Commission data continue and are conducted monthly. Overall Acute and Emergency Medicine completed 97% of falls risk assessments, Specialist Medicine and Health of Older People completed 100% and S & A completed 100 % on admission. Of those, Acute and Emergency Medicine completed 89%, Specialist Medicine and Health of Older People completed 89% and S & A completed 81% within eight hours of admission (against a target of 90%) Hand Hygiene Waitemata DHB s Hand Hygiene Audit results for January 2017 are not yet available. Healthcare-Associated Infections The CLAB insertion bundle was used in ICU on 100% of occasions in January The insertion bundle compliance meets the national target of 90%. Elective Surgery Centre (ESC) As at the end of December 2016, the Elective Surgery Centre treated 2,586 patients which is tracking at 99% of Ministry of Health target. The average theatre utilisation during this period sits at 85% which is equal to the same period in Waitemata District Health Board, Meeting of the Board 01/03/17 45
46 3.1 Operationally ESC continues to provide efficient and productive service to its patients and clinicians with patient satisfaction and feedback continuing to be excellent despite increased workload. ESC continues to plan the management of patient volumes directly alongside Surgical and Ambulatory Services to ensure all targets are met regarding ESPI compliance and MOH volumes. In summary, the patient and SMO feedback continues to remain extremely positive, with the processes and facility working very well. An excellent team spirit continues among the staff, who are extremely proud of the service they offer patients. Māori Health Annual Planning Ministry of Health planning expectations have evolved over the last five years. In 2013/14, the planning guidance was updated to include a prescribed template for DHB Māori health plans as a standalone but companion document to the Annual Plan. The purpose of the Annual Māori Health Plans was to accelerate Māori health gain within our respective districts. It provided each District Health Board and their local health services with priority areas for action for the financial year and specified accountabilities for the activities. In 2017/18 the Ministry of Health planning guidance amended this requirement to no longer require a separate District Health Board Māori health plan by integrating Māori health planning into the Annual Plan. However, in December 2016 the Board Chair communicated his intention at the Auckland and Waitemata DHB Board meetings to continue with Māori Health Plans and to align these across the three metro Auckland DHBs in 2017/18. Respective DHB Māori health, planning and funding teams met over December-January to explore opportunities to realise that objective. Through these meetings the Metro Auckland District Health Boards are proposing to our respective Māori Health Gain Advisory Committees that we: Continue with a common flow to the Māori health planning documents. This will make it easier for community, clinical, operational and executive leaders working across the region to review and engage with the respective plans. Adopt a life course approach to the presentation of activities and indicators. This will better reflect the NZ Health Strategy and local DHB strategy focus on health equity and Māori world view of collective wellbeing than the current indicator list method of the current Ministry of Health template. Maintain the nationally determined priority areas and indicators from the 2016/17 Māori Health Plan, with the incorporation of System Level Measure (SLM) actions. Continue to have a limited number of local priorities for each District Health Board to support the needs and opportunities for their respective Māori communities. Provide a list of potential priority areas where regional collaboration could be beneficial. Further discussion will be required to determine which of these are included in the 2017/18 Māori Health Plans as regional priorities. As with previous years, we will continue to consult with the relevant internal and external partners throughout the development of the Māori health plans including our Memorandum of Understanding partners. Waitemata District Health Board, Meeting of the Board 01/03/17 46
47 3.1 Workforce DHB workforce ethnicity data quality has been a focus of the Māori Workforce Development Alliance Leadership Team. A complete District Health Board workforce ethnicity data set to 95% has been achieved. A follow on activity is underway to classify and store all new data in accordance with census standards. Pacific Health Pacific Health Action Plan The Pacific Health Action plan has been reviewed and updated incorporating hospital activities which enable the improvement of patient experience and outcomes for Pacific families. This has been accepted by and discussed with the Pacific Health Action Plan Committee which involves a strong community voice and is chaired by the CPHAC Pacific Representative Rev Dr Featuanai Liuaana. Diabetes DNA rate There will be a focus on improving the attendance rates of Pacific patients at diabetes appointments over the next three months. The Tautai Fakataha DNA (Did Not Attend) lead will prioritise the DNA list for pre appointments for Diabetes for Pacific patients and survey patients over the phone on how to improve appointment attendance. Bariatric surgery patient experience The Bariatric surgery interviews with Pacific patients and their families were completed as part of the service improvement for Bariatric Surgery Services. A report is currently being compiled with the findings. Health Science Academies A variation to extend the contract term to the end of 2017 has been addressed by the Ministry of Health and new contracts have been delivered to the respective schools operating Health Science Academies (Waitakere College and Onehunga High School). Pacific staff wellness Pacific fitness training as part of the Pacific staff wellness programme is facilitated by public health physician Dr Felicity Williamson and the Pacific Health Gains team. All staff are invited to join fitness programme on Thursday mornings at 7.30am in the car park next to the staff gym on Shea Terrace. Cultural competency training The Pacific Best Practice lead facilitator will be attending training in Seattle to externally validate our cultural competency programmes and practices. These programmes have been rolled out to 530 staff to date and will continue to improve engagement with Pacific patients and their families. Waitemata District Health Board, Meeting of the Board 01/03/17 47
48 CEO Scorecard 3.1 Actual Target Trend Patient Experience Actual Target Trend Better help for smokers to quit - maternity 78% 90% q Complaint Average Response Time 13 days <14 days p Better help for smokers to quit - primary care 88% 90% p Net Promoter Score FFT p Improved Access to Elective Surgery - WDHB 105% 100% p Shorter Waits in ED 98% 95% p Quality & Safety Trend Faster cancer treatment (62 days) 90% 85% Older patients assessed for falling risk 98% 90% Increased immunisation (8-month old) 92% 95% q Occasions insertion bundle used 100% 95% Raising Healthy kids 100% 70% p a. Good hand hygiene practice 86% 80% q Pressure injuries grade 3&4 0 0 ICU - CLAB rate per 1000 line days 1 <1 p b. Provider Arm - Service Delivery Antibiotic in the right time 92% 100% Waiting Times Actual Target Trend Improving outcomes ESPI Better help for smokers to quit - hospitalised 99% 95% ESPI 2 - % patients waiting > 4 months for FSA Compliant Population coverage/access Trend ESPI 5 - % patients not treated within 4 months Compliant Cervical Screening 76% 80% Diagnostics Breast screening 67% 70% % of CT scans done within 6 weeks 99% 95% p c. Bowel Screening Participation % of MRI scans done within 6 weeks 95% 85% q - Round 2 55% 60% p Urgent diagnostic colonoscopy (14 days) 98% 85% p - Round 3 52% 60% q Diagnostic colonoscopy (42 days) 77% 70% p Surveillance colonoscopy (84 days) 83% 70% p Treatment d. HSMR (Source: Health Round Tables) 106% <103% p d. Patient Flow Surgical intervention rates (per 10,000 pop) Elective Surgical Discharges (YTD) - Angioplasty p Elective Discharges - Total 10,127 10,074 p - Angiography p Elective Discharges - Provider Arm 7,012 6,805 p - Major joints p Elective Discharges - IDF Outflow 3,115 3,269 p - Cataract p a. Efficiency # NOF patients to theatre (48 hours) 95% 85% p Outpatient DNA rate (FSA + FUs) 9% <10% ST elevation MI receiving PCI (120 mins) 90% 80% p Average Length of Stay - Electives 1.46 days <1.69 days q AT&R referrals assessed (2 working days) 94% 90% q Average Length of Stay - Acutes 2.64 days <2.51 days q Staff Experience Actual Target Trend Major Capital Programmes Time Budget Quality Sick leave rate 3.2% <3.8% Te Atarau car park (mid 2016) - completed Turnover rate 11% 8-12% WTH Emergency Department redevelopment (Apr 2016) Lost time injury rate (per hours worked) 12 <5 Mason clinic - 15 Bed medium secure unit (May 2017) NSH Building 5 Refurbishment (Mar 2017) Financial Result Trend Clinical and Learning Skills Centre (Apr 2017) Net Surplus/Deficit (YTD) 1,483 k 1,405 k Elective Capacity and Inpatient beds (TBC) Bridge ESC to Medical Tower (Sep 16) f. Health Targets Waitemata DHB Monthly Performance Scorecard CEO Scorecard December /17 Managing our Business Best Care How to read Performance indicators: Trend indicators: Achieved/ On track Substantially Achieved but off target p Performance improved compared to previous month Not Achieved but progress made Not Achieved/ Off track q Performance declined compared to previous month Performance was maintained Key notes 1. Most Actuals and targets are reported for the reported month/quarter (see scorecard header). 2. Actuals and targets in grey bold italics are for the most recent reporting period available where data is missing or delayed. 3. Trend lines represent the data available for the latest 12-months period. All trend lines use auto-adjusted scales: the vertical scale is adjusted to the data minimum-maximum range being represented. Small data range may result small variations perceived to be large. a. One month in arrears - as at Nov 2016 b. As at Jun Q4 2015/16 (latest HQSC data available). c. Bowel Screening Round 2 (closed) Jun Q4 2015/16 - Round 3 commenced (participation rate for invites Jan - Sep 2016). d. Reported quarterly - as at Sep Q1 2016/17. e. As at Sep Q1 2016/17. f. New method of calculation and target June Rate per hours worked A question? Contact: Victora Child - Reporting Analyst, Planning & Health Intelligence Team: victoria.child@waitematadhb.govt.nz Planning, Funding and Health Outcomes, Waitemata DHB 48
49 ARTICLE 3.1 Pathways to ambulatory sensitive hospitalisations for Māori in the Auckland and Waitemata regions Carol Barker, Sue Crengle, Dale Bramley, Karen Bartholomew, Patricia Bolton, Michael Walsh, Jean Wignall ABSTRACT AIM: Ambulatory Sensitive Hospitalisations (ASH) are a group of conditions potentially preventable through interventions delivered in the primary health care setting. ASH rates are consistently higher for Māori compared with non-māori. This study aimed to establish Māori experience of factors driving the use of hospital services for ASH conditions, including barriers to accessing primary care. METHOD: A telephone questionnaire exploring pathways to ASH was administered to Māori (n=150) admitted to Auckland and Waitemata District Health Board (DHB) hospitals with an ASH condition between January 1 st June 30 th RESULTS: A cohort of 1,013 participants were identified; 842 (83.1%) were unable to be contacted. Of the 171 people contactable, 150 agreed to participate, giving an overall response rate of 14.8% and response rate of contactable patients of 87.7%. Results demonstrated high rates of self-reported enrolment, utilisation and preference for primary care. Many participants demonstrated appropriate health seeking behaviour and accurate recall of diagnoses. While financial barriers to accessing primary care were reported, non-financial barriers including lack of after-hours provision (12.6% adults, 37.7% children), appointment availability (7.4% adults, 17.0% children) and lack of transport (13.7% adults, 20.8% children) also featured in participant responses. CONCLUSIONS: Interventions to reduce Māori ASH include: timely access to primary care through electronic communications, increased appointment availability, extended opening hours, low cost after-hours care and consistent best management of ASH conditions in general practice through clinical pathways. Facilitated enrolment of ASH patients with no general practitioner could also reduce ASH. Research into transport barriers and enablers for Māori accessing primary care is required to support future interventions. Ambulatory Sensitive Hospitalisations (ASH) is an academic construct of a group of conditions for which hospitalisation is potentially preventable through prophylactic or therapeutic interventions delivered in the primary health care setting. 1 ASH are often categorised as vaccine-preventable, acute or chronic conditions. Key pathways to this categorisation of ASH include inadequate vaccination, lack of early detection and treatment of acute conditions, and inadequate control of chronic conditions. 2 ASH rates for 0 4 year olds have recently been employed as a measure of health care integration and whole system performance in the Ministry of Health s Integrated Performance and Incentives Framework. 3 ASH rates are also employed as an indicator for Māori Health. 4 6 The Ministry of Health have recently undertaken a review of the methodology and definition of ASH. 7 ASH rates are consistently higher for Māori, with rates 1.6 to 2.3 times higher for Māori than non-māori. 4 Multiple factors have been linked to ASH. Health care affordability, accessibility and availability have been shown to reduce ASH, 8 12 as has acceptability of care, quality of care and accommodation of patient preferences. 8,11,13 Access to the socioeconomic determinants of health including income, 9,10,12,14 education, 12,14 transport, 11 quality housing 15 and social supports can also reduce ASH. 13,14,16,17 Other factors that impact upon ASH include Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
50 ARTICLE 3.1 health-seeking behaviour and practitioner factors. 8,11,13 While ASH are considered potentially preventable through interventions delivered in the primary health care setting, the impact of social determinants of health limit the use of ASH to determine preventability within primary care. 8 Overall primary care access with regard to use and availability of services is lower for Māori than non-māori as demonstrated by gaps in enrolment for primary care, 18 well child and oral health services. 19 However, this is variable across age groups and geographical regions, and ethnicity misclassification is likely to account for some of the difference. 20 Māori are more likely to face financial barriers for general practitioner (GP), after-hours and pharmacy services, to experience unmet need for health care due to lack of transport and are less likely to secure an available appointment within 24 hours of enquiry. 4 There is also evidence of poorer quality of primary care for Māori, who may receive shorter consultations, fewer investigations, fewer prescriptions and lower secondary care referral rates than non-māori. 21 As an indicator of health system performance, within the context of known issues of primary care access and quality, high Māori ASH rates may represent an appropriate response of seeking necessary care from the most accessible source. A number of interventions have been identified in the literature as beneficial in reducing ASH. These include condition specific, multidisciplinary, patient centric programmes; increased access to primary care, in particular for children and underserved populations; and managing patients out of hospital through community-based pharmacological and telemedicine interventions. 22 Methods The study used descriptive methodology to report perceptions about health care experience, pathways to admission, attitudes and behaviours. The study was a telephone administered questionnaire (Appendix 1 and 2) developed utilising standard validated questions from the New Zealand Health Survey (NZHS) 23 and Agency for Healthcare Research and Quality Clinician Survey. 24 The population of interest were Māori aged 0 74 admitted to Waitemata DHB (North Shore Hospital or Waitakere Hospital), or Auckland DHB (Auckland City Hospital or Starship Hospital) with a primary diagnosis of an ASH condition from January 1 st June 30 th The Ministry of Health ASH definition at the time of the study was used to determine which conditions were classified as ASH. Usual ASH filters were applied (eg deceased patients, babies <28 days and admissions lasting <3 hours were excluded). 7 Questionnaire surveys were conducted from April 8 th July 2 nd 2015 by culturally appropriate, trained telephone interviewers using an agreed script. Verbal consent to participate was sought from participants or parents/guardians of children (less than 16 years). The survey included multiple choice questions with a number of free text options. Questions explored primary care enrolment and utilisation, history of the ASH condition, health seeking behaviours, health care journey in the week and year prior to admission, and barriers and enablers to accessing primary care. Interviews were between 15 minutes and one hour in duration. Participant responses were matched with hospital data including: demographic data, National Health Index (NHI) number, admitting hospital, deprivation level and whether a named GP was recorded in the hospital records at admission. Ethnicity was prioritised according to standard ethnicity protocols. 25 Deprivation was assigned using the New Zealand Index of Deprivation (NZDep), a small area measure of deprivation derived from census data. 26 NZDep was categorised into quintiles (1 least deprived quintile, 5 most deprived quintile). At the time data were extracted, new domicile codes based on 2013 census area units were yet to be implemented, however, updated 2013 NZDep scores were available. Where a domicile code remained unchanged from 2006, its 2013 NZDep score was used. Where a domicile was no longer in use, the 2006 NZDep score was used as a proxy. Descriptive statistics are presented and qualitative data were analysed using thematic analysis. Statistical analysis was undertaken in Stata 13.0 (StataCorp Stata Statistical Software: Release 13. College Station, TX: StataCorp LP) and Microsoft Excel. Differences in characteristics between participants and non-participants were Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
51 ARTICLE 3.1 assessed using two sample t-tests, Wilcoxon rank-sum test, Pearson s chi-squared and Fisher s Exact test. The survey was considered low risk, not requiring formal approval from the Health and Disability Ethics Committee. DHB localities approval was granted. A $20 supermarket voucher koha was offered to survey participants. Systems were put in place to manage any possible disclosure of information, psychological distress or service complaints. Participants who raised any issues were offered follow up with hospital whānau support services (He Kamaka Waiora). Results A cohort of 1,013 eligible participants were identified from hospital records, 150 participants (97 adults, parents/guardians of 53 children) completed the telephone survey, giving an overall response rate of 14.8% (Figure 1). Of the eligible cohort, 802 (79.2%) were unable to be contacted despite up to three attempts at different times of the day/ week, and 40 (3.9%) were found to have no such telephone number. Of the 171 people that were contactable, 150 agreed to participate (response rate of contactable patients of 87.7%). Survey participants had similar demographic characteristics to non-participants (Table 1). Māori participants admitted with an ASH condition during the study period were more likely to live in the highest deprivation quintile compared with non-māori admitted with an ASH condition (36.0% and 22.6% respectively). Participants were also more likely to live in areas of high deprivation compared with the total Māori population for Auckland and Waitemata DHBs, in which 27% and 14% of Māori live in the most deprived quintile. Leading ASH conditions for adults surveyed were cellulitis, angina and chest pain, pneumonia and kidney/urinary infections. For children surveyed, leading ASH conditions included dental conditions, asthma and cellulitis (Table 1). Non-participants include persons who were non-contactable or who declined to participate. Participants reported high levels of enrolment and utilisation of primary care services. Self-reported enrolment was higher than the percentage of participants who had a GP listed in the hospital data (95.9% versus 85.6% for adults, 100% versus 71.7% for children). Participants reported regular contact with primary care with 84.9% of adults and 90.2% of children being seen two or more times in the 12 months before admission (Table 2). Participants reported a strong preference for seeing a GP first, rather than visiting a hospital or other health provider (74.7% adults and 94.2% children). Thematic analysis demonstrated preference for seeing a GP was due to ease of access and greater convenience of a GP compared with hospital Figure 1: Flow diagram of participants eligible to participate in the pathways to ASH survey. Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
52 ARTICLE 3.1 Table 1: Comparison of characteristics for participants and non-participants. Factor Level Participants (%) Non-participants (%) p-value N Age, mean (SD) 33.4 (23.6) 33.1 (23.3) 0.89 Gender F 72 (48.0) 455 (52.7) 0.29 M 78 (52.0) 408 (47.3) NZDep quintile 1 12 (8.0) 57 (6.7) (16.0) 122 (14.2) 3 27 (18.0) 169 (19.7) 4 33 (22.0) 196 (22.9) 5 54 (36.0) 313 (36.5) GP recorded at admission No 29 (19.3) 194 (22.5) 0.39 Yes 121 (80.7) 669 (77.5) LOS, median (IQR) 1 (0, 3) 1 (1, 3) 0.46 ASH category Cellulitis 23 (15.3) 182 (21.1) Dental conditions 21 (14.0) 112 (13.0) Asthma 19 (12.7) 39 (4.5) Angina and chest pain 12 (8.0) 95 (11.0) Respiratory infections: pneumonia 11 (7.3) 45 (5.2) Kidney/urinary infection 11 (7.3) 59 (6.8) Gastroenteritis/dehydration 9 (6.0) 64 (7.4) Congestive heart failure 6 (4.0) 39 (4.5) Diabetes 6 (4.0) 29 (3.4) Myocardial infarction 5 (3.3) 31 (3.6) Stroke 5 (3.3) 14 (1.6) or other providers. Participants valued the long established relationships and history they shared with their GP. Many participants reported that hospitals were for emergencies and that it was inappropriate to visit a hospital for non-urgent issues. One in four adults preferred to visit a hospital or specialist first if they were unwell, needed a check-up or health advice. Reasons given for this preference included better quality of care, lower costs and lack of available appointments in primary care. High levels of continuity of carer (GP or practice nurse) were demonstrated with the majority of adults (75.3%) and children (70.6%) reporting they would usually see the same GP or practice nurse. Participants reported receiving comprehensible health instructions from primary care staff about taking care of their illness (adults 83.0%, children 96.1%). High levels of concordance were seen between self-identified reason for admission and ASH category coded at discharge. Concordance was particularly high for children (92.5%) (Table 2). Despite high levels of self-reported enrolment, utilisation and preference for general practice, a significant number of participants reported never seeing a health professional for their current ASH condition (22.7% adults, 39.6% children) and had not seen a GP or practice nurse in the week Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
53 ARTICLE 3.1 Table 2: Summary of findings. Findings Adults (%)* Children (%)* Self-reported enrolment with a GP 93/97 (95.9) 53/53 (100) GP details recorded in hospital data 83/97 (85.6) 38/53 (71.7) Two or more GP visits in the 12 months before admission 79/93 (84.9) 46/51 (90.2) Four or more GP visits in the 12 months before admission 65/93 (69.9) 29/51 (56.9) 10 or more GP visits in the 12 months before admission 34/93 (36.6) 3/51 (5.9) Prefer GP as first health contact 71/95 (74.7) 49/52 (94.2) Continuity of carer when seen in primary care 67/89 (75.3) 36/51 (70.6) Received comprehensible health instructions in primary care in the 12 months 73/88 (83.0) 49/51 (96.1) before admission Concordance between ASH coding and self-reported reason for admission 67/97 (69.1) 49/53 (92.5) Did not see a health professional for the ASH condition before admission 22/97 (22.7) 21/53 (39.6) Did not see a GP or Practice nurse in the week before admission ** 39/95 (41.1) 13/34 (38.2) Unwell for less than one week before admission 46/97 (47.4) 22/53 (41.5) Unable to see a GP within 24 hours of request in the 12 months before admission 31/97 (32.0) 5/53 (9.4) Used telephone or to access GP practice in the 12 months before admission 27/97 (27.8) 6/53 (11.3) Readmitted for the same ASH condition 41/96 (42.7) 15/53 (28.3) *Percentages presented use the total number of participants who provided a response to the question as the denominator. Includes visits to a GP and practice nurse. Prefer to visit their GP first rather than visiting a hospital or other health provider if they are unwell, need a check-up or health advice. When seen in primary care, participants would usually see the same GP or GP nurse. Reported always or almost always being given easy-to-understand instructions from their GP or GP nurse about taking care of their illness/child s illness. **Excludes participants with dental conditions. before admission (adults 41.1%, children 38.2%, excludes dental admissions). Many adults (47.4%) and children (41.5%) reported being unwell for less than one week before admission (Table 2). There was evidence of barriers to timely access to a GP with 32% of adults reporting they were unable to see a GP within 24 hours. Lack of available appointments was the main reason given by adults (48.4%) for being unable to access a GP within 24 hours. Telephone and communications were used less often to access GP advice (adults 27.8%, children 11.3%) (Table 2). In the week prior to admission, 41.5% of children and 58.8% of adults reported seeing a GP or practice nurse. Adult readmissions for the ASH condition were seen across the spectrum of ASH conditions, whereas asthma accounted for 73.3% of paediatric ASH readmissions. General practice not being open when needed or lack of after-hours provision were the main reasons given for children delaying or not seeing a GP before going to hospital. Other factors included lack of transport, no available appointment and financial barriers. For adults, financial barriers, including being unable to afford to see the GP, being unable to pay for prescriptions and pre-existing debts with the GP, were the main reason for delaying or not seeing a GP. Other reasons given were general practice not being open or not having after-hours provision, lack of transport and no available appointments. Key enablers, reported by caregivers that would make accessing a GP easier for children, were enhanced affordability and availability of after-hours care. Other facilitators included having transport to see the GP and free or low cost GP care. For adults, reducing financial barriers to both general practice and after-hours care was the most important measure to make seeing a GP easier. Other facilitators included having transport and GPs being open after-hours (Table 3). Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
54 ARTICLE 3.1 Table 3: Summary of barriers and enablers to accessing a GP. Barriers to accessing a GP Adults N=95 (%)* Children N=53(%)* GP not open or it was after-hours 12 (12.6) 20 (37.7) Lack of transport 13 (13.7) 11 (20.8) No appointments available 7 (7.4) 9 (17.0) Unable to afford to see a GP 14 (14.7) 3 (5.7) Unable to afford prescriptions 7 (7.4) 1 (1.9) Owe the GP money 3 (3.2) 4 (7.5) Waiting times too long 3 (3.2) 2 (3.8) Negative experience with a GP in the past 4 (4.2) 4 (7.5) Could not get childcare 1 (1.1) 0 (0.0) Could not get in touch with the doctor 0 (0.0) 2 (3.8) Thought I would not be respected 0 (0.0) 0 (0.0) Thought the GP would not want to help me 0 (0.0) 1 (1.9) Do not trust GPs 0 (0.0) 0 (0.0) Enablers to accessing a GP Adults N=94 (%) Children N=52 (%) Free or low cost after-hours 31 (32.9) 43 (82.7) GP practice open after-hours 27 (28.7) 42 (80.8) Having transport to the GP 30 (31.3) 37 (71.2) Free or low cost GP care 50 (53.1) 34 (65.4) Feeling welcome at GP practice 3 (3.2) 1 (1.9) Feeling that the GP respects me 2 (2.1) 1 (1.9) More appointments 2 (2.1) 0 (0.0) Shorter waiting times 2 (2.1) 0 (0.0) Having childcare 1 (1.1) 0 (0.0) *Percentages presented use the total number of participants who provided a response to the question as the denominator. Could not afford to pay for medication if the GP was to give them a prescription. Sub-analysis of enablers to accessing primary care reported by caregivers demonstrated no significant differences in responses for children aged <6 or 6 reporting that free or low cost GP (<6 years: 18/27, 6 years 16/26, p=0.70) or free or low cost after-hours care (<6 years: 21/27, 6 years 22/26, p=0.53) would make it easier to see a GP. Discussion Māori patient and whānau experience presented in this study provides a counter narrative to the deficit focus often taken in reports on ASH. Many participants demonstrated appropriate health-seeking behaviour, pertinent use of secondary care services and accurate recall of diagnoses. Of interest in this survey was the high proportion of un-contactable patients. This raises concerns regarding the ability of hospital services to contact patients post-discharge and the accuracy of contact details included on discharge summaries. Local work on diabetes clinic Did Not Attend rates has also demonstrated a high proportion of un-contactable patients. The importance of accurate patient contact details has been recognised nationally with the Ministry of Health undertaking a National Enrolment Service (NES). The NES will allow primary care to update the NHI health identity data with contact details; hospital services will then be able to access more accurate data. 27 Introduction of a DHB caller ID to identify incoming calls as being from the DHB could be investigated as a way of improving telephone call pick-up rates and contactability of patients post-discharge. Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
55 ARTICLE 3.1 The study demonstrates several key areas for intervention to reduce high Māori ASH rates. Inconsistencies between self-reported enrolment and presence of a GP recorded in hospital data may reflect incomplete recording of GP details or patients incorrectly assuming they are enrolled. However, the majority of participants had seen their GP in the last 12 months. These inconsistencies raise the possibility that discharge communications for some participants are not reaching their GP which may be contributing to ASH readmissions. Lower rates of Primary Health Organisation (PHO) reported enrolment for Māori are compounded by known ethnicity misclassification, which underestimates PHO enrolment for Māori. 20 Structured discharge planning has been shown to reduce ASH admission. 14,22 Recommendations to improve this include steps to increase Māori enrolment through the Multi-Enrolment Project to enrol newborns into a range of services including primary care and oral health services. Multi-enrolment of newborns has been employed by the Porirua Social Sector Trial, successfully contributing to an increase in children enrolled in oral health services. 28 Other recommended activities include ensuring GP details are checked and updated with each admission and active follow up and facilitated enrolment of ASH patients with no GP identified.despite high levels of utilisation of primary care services in the previous year, many adults and children did not see a GP or practice nurse in the week before admission. Given that 47.4% of adults and 41.5% of children were unwell for less than one week, lack of GP contact in the week prior to admission represents a lost opportunity to prevent an admission. Timely access to a GP and lack of available appointments was a recurrent issue for many adults. Similar findings have been found nationally with 21% of Māori adults and 16% of Māori children being unable to get an appointment at their usual medical centre within 24 hours in the last 12 months. 4 Given the potential to mitigate ASH with primary care interventions, improving timely access to primary care is an important step in reducing ASH. Greater use of electronic communications between patients and primary care through services such as the Electronic Health Record and Patient Portal could improve timely access to GP advice and management for chronic conditions. Telemedicine including regular contact by telephone has been shown to reduce ASH for chronic conditions including heart failure and diabetes. 14 Ensuring that these enhanced systems work for Māori and do not increase ethnic inequities is important. Free or low cost GP care and after-hours care were identified by adults as key enablers for accessing a GP. Having GP practices open after-hours and low cost or free after-hours care were key enablers identified to improve children s access to a GP. Given the acute nature of many paediatric ASH and the strong preference from caregivers to see a GP, steps to extend GP opening hours and free or low cost afterhours care could reduce ASH. At the time of the ASH survey coverage for free afterhours care for children under six years old was 98% and 96% for Auckland and Waitemata DHBs respectively. Extension of free after-hours care to include children aged under thirteen may further reduce financial barriers to after-hours care. While financial barriers to accessing primary care were reported by many participants, non-financial barriers including appointment availability, after-hours care and transport also featured in participant responses. Comparisons between participants and non-participants indicate there were no significant differences with regard to age, gender, deprivation, record of a GP at admission, length of stay and ASH condition. However, the high number of un-contactable people and subsequent low response rate of eligible participants means the study is exploratory and limits generalisability of results. Areas of further research Lack of transport was identified as preventing or delaying adults and children from seeing a GP. Findings from the NZHS support the importance of transport as a barrier to accessing primary care for Māori. 4 The NZHS reported Māori adults and children were more likely to experience unmet need for a GP due to lack of transport than non-māori with rate ratios of two and Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
56 ARTICLE 3.1 three respectively. 4 Lack of transport may be due to lack of access to a car, being unable to drive due to medical or licencing restraints, lack of access to public transport or inability to fund transport. Further research into the nature of transport barriers and enablers for Māori accessing primary care is required to support future interventions. Despite high levels of contact with primary care, participants were still admitted with an ASH condition. This suggests steps to mitigate some ASH admissions were not being fully realised. Ensuring consistent, best practice management of ASH conditions in general practice through clinical pathways could prevent some of these ASH admissions. Admission with an ASH condition despite GP contact in the week prior may reflect referral being necessary at the point of presentation, limiting timely effective intervention in primary care. A more detailed case review would be needed to understand this further. High rates of paediatric asthma readmissions suggest a recurrent failure to mitigate potentially preventable admissions, despite cases being seen repeatedly by primary and secondary care. The underlying cause of these readmissions is unclear and could relate to access and quality of GP services, quality of hospital management, discharge planning, health literacy 29 and environmental factors such as crowded and poor quality housing. 10,15,29 Again, a more detailed case review would be needed to understand this further. Further research to assess the impact on ASH following subsidised GP visits for children aged under six and more recently, children aged under thirteen would further clarify the influence of financial barriers on ASH. Strengths and limitations Strengths of this research include the focus on patient and whānau experience to inform relevant interventions for Māori. The survey was comprehensive in its enquiry across pathways to ASH with questions relating to social determinants of health, access to primary care and quality of care received. Quantitative and qualitative data allowed for both breadth and depth of enquiry. The use of validated questions previously included in the NZHS allowed regional findings to be compared with the national context. Study limitations include the low response rate limiting generalisability of results and potential for selection bias as patients were not randomly selected. However, there were no significant differences between these two groups, suggesting the impact of selection bias is likely to have been low. Recall bias may have arisen due to delay between hospital admission and survey completion which was 2 17 weeks (average 10 weeks) following discharge. Questions relating to events 12 months before admission add to the potential for recall bias. Pathways to dental ASH, a leading ASH condition for children, are likely to be affected by utilisation, access and quality of oral health services which were not specifically covered in this survey. Conclusion This study demonstrated many positive findings including appropriate healthseeking behaviour, accurate recall of diagnoses and high rates of self-reported enrolment, utilisation and preference for primary care. Financial barriers to accessing primary care were reported, as well as non-financial barriers including appointment availability and lack of transport. Measures to reduce the high ASH rates for Māori include: timely access to primary care through electronic communications, increased appointment availability, extended opening hours and low cost or free after-hours care, consistent best management of ASH conditions through clinical pathways and addressing transportation barriers. Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
57 ARTICLE 3.1 Competing interests: Dale Bramley is the CEO of Waitemata DHB. Acknowledgements: Survey participants, Selah Hart, John Patterson He Kamaka Waiora: Hospital Whānau Support Services, Aroha Haggie. Author information: Carol Barker, Department of Planning, Funding and Outcomes, Auckland and Waitemata District Health Boards, Auckland; Sue Crengle, Invercargill Medical Centre, Invercargill; Dale Bramley, Chief Executive Officer, Waitemata District Health Board, Auckland; Karen Bartholomew, Department of Planning, Funding and Outcomes, Auckland and Waitemata District Health Boards, Auckland; Patricia Bolton, Department of Planning, Funding and Outcomes, Auckland and Waitemata District Health Boards, Auckland; Michael Walsh, Department of Planning, Funding and Outcomes, Auckland and Waitemata District Health Boards, Auckland; Jean Wignall, Department of Planning, Funding and Outcomes, Auckland and Waitemata District Health Boards, Auckland. Corresponding author: Carol Barker, Department of Planning, Funding and Outcomes, Auckland and Waitemata District Health Boards, 15 Shea Terrace, Auckland. URL: REFERENCES: 1. Jackson G, Tobias M. Potentially avoidable hospitalisations in New Zealand, Aust N Z J Public Health 2001; 25(3): Page A, Ambrose SJ, Glover JD, et al. Atlas of Avoidable Hospitalisations in Australia: ambulatory care-sensitive conditions. Adelaide: Public Health Information Development Unit University of Adelaide, Health Improvement and Innovation Resource Centre. Integrated Performance and Incentive Framework (IPIF) 2015 [cited 2015 October 19]. Available from: org.nz/section/35484/ integrated-performance-and-incentive-framework/?tab= Ministry of Health. Tatau Kahukura: Māori Health Chart Book 2015 (3rd edition). Wellington: Ministry of Health, Waitemata District Health Board. Maori Health Plan: Auckland: Waitemata District Health Board; Auckland District Health Board. Maori Health Plan: Auckland: Auckland District Health Board; National Service Framework Library. Ambulatory sensitive (avoidable) hospital admissions.: National service Framework Library; 2015 [cited 2015 December 16]. Available from: nsfl.health.govt.nz/ accountability/performance-and-monitoring/ data-quarterly-reports-and-reporting/ambulatory-sensitive. 8. Ansari Z. The concept and usefulness of ambulatory care sensitive conditions as indicators of quality and access to primary health care. Aust J Prim Health 2007; 13(3): Barnett R, Malcolm L. Practice and ethnic variations in avoidable hospital admission rates in Christchurch, New Zealand. Health and Place 2010; 16(2): Craig E, Anderson P, Jackson G, et al. Measuring potentially avoidable and ambulatory care sensitive hospitalisations in New Zealand children using a newly developed tool. N Z Med J 2012; 125(1366): Longman JM, Singer JB, Gao Y, et al. Community based service providers perspectives on frequent and/or avoidable admission of older people with chronic disease in rural NSW: A qualitative study. BMC Health Services Research 2011; 11(1): Ansari Z, Rowe S, Ansari H, et al. Small area analysis of Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
58 ARTICLE 3.1 ambulatory care sensitive conditions in Victoria, Australia. Population Health Management 2013; 16(3): Freund T, Campbell SM, Geissler S. et al. Strategies for reducing potentially avoidable hospitalizations for ambulatory care sensitive conditions. Annals of Family Medicine 2013; 11(4): Purdy S. Avoiding hospital admissions: what does the research evidence say? London: King s Fund, Jackson G, Thornley S, Woolston J, et al. Reduced acute hospitalisation with the healthy housing programme. Journal of epidemiology and community health 2011:jech Butler DC, Thurecht L, Brown L, et al. Social exclusion, deprivation and child health: A spatial analysis of ambulatory care sensitive conditions in children aged 0-4 years in Victoria, Australia. Soc Sci Med 2013; 94: Longman J, Passey M, Singer J, et al. The role of social isolation in frequent and/or avoidable hospitalisation: Rural community-based service providers perspectives. Australian Health Review 2013; 37(2): Ministry of Health. Enrolment in a Primary Health Organisation. Wellington Ministry of Health 2015 [cited 2015 December 15]. Available from: health.govt.nz/our-work/ primary-health-care/about-primary-health-organisations/ enrolment-primary-health-organisation. 19. Ministry of Health. Indicators for the Well child/tamariki Ora Quality Improvement Framework-September Wellington: Ministry of Health, Bramley D, Latimer S. The accuracy of ethnicity data in primary care. N Z Med J 2007; 120(1264). 21. Crengle S, Lay-Yee R, Davis P, et al. A comparison of Māori and non-māori patient visits to doctors: the National Primary Medical Care Survey (NatMedCa): 2001/02. Report 6. Wellington: Ministry of Health Basu A, Brinson D. The effectiveness of interventions for reducing ambulatory sensitive hospitalisation: a systematic review. Christchurch: Health Services Assessment Collaboration (HSAC), Ministry of Health. New Zealand Health Survey: Ministry of Health; 2015 [cited 2015 November 6]. Available from: nz-health-statistics/national-collections-and-surveys/ surveys/current-recent-surveys/ new-zealand-health-survey. 24. Agency for Healthcare Research and Quality. Surveys and guidance: Clinicians and groups: Agency for Healthcare Research and Quality; 2011 [cited 2015 November 6]. Available from: gov/surveys-guidance/ CG/index.html. 25. Ministry of Health. Ethnicity Data Protocols for the Health and Disability Sector. Wellington: Ministry of Health, Atkinson J, Salmond C, Crampton P. NZDep2013 Index of Deprivation. Wellington: Department of Public Health, University of Otago, Ministry of Health. National Enrolment Service. Wellington: Ministry of Health; 2016 [cited 2016 April 4]. Available from: health.govt.nz/our-work/ primary-health-care/ primary-health-caresubsidies-and-services/ national-enrolment-service. 28. Compass Health. Porirua Social Sector Trial Tumai Hauora Ki Porirua Annual Update for July June Wellington: Compass Health 2015 [cited October]. 29. Crengle S, Robinson E, Grant C, et al. Pharmacological management of children s asthma in general practice: findings from a community-based cross-sectional survey in Auckland, New Zealand. NZ Med J 2011; 124: Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
59 ARTICLE 3.1 Appendices Appendix 1: Pathways to Ambulatory Sensitive Hospitalisations: Adult Survey Survey Instructions Answer each question by marking the box to the left of your answer. You are sometimes asked to skip over some questions in this survey. When this happens you will see an arrow with a note that tells you what question to answer next, like this: o Yes g If Yes, go to #1 on page 1 o No Your child s health 1. What illness did you come into hospital for? 7. When was the last time you saw a health professional for the illness you were admitted to hospital with? o Never g If Never, go to #21 on page 5 o The day I went to hospital o 2 days 1 week (7 days) ago o Between 1 week and 1 month ago o Between 1 month and 3 months ago o Between 3 months and 12 months ago o More than 12 months ago o I don t remember 2. How long have you had this illness? o 1 day 1 week (7 days) o Between 1 week and 1 month o Between 1 month and 3 months o Between 3 months and 12 months o More than 12 months o I don t remember 3. Do you need or take medicine prescribed by a doctor for this illness? o Yes o No 4. Have you been admitted to hospital with this illness before? o Yes o No o I don t know/remember 8. What health professional/s did you see for this illness before you went to hospital? o None o GP o GP nurse o Other 9. Was this the health professional/s you usually see if you need a check-up, want advice about a health problem, or get sick or hurt? o Yes o No 10. What care did you receive from the health professional? o Referral to hospital o Advice or instructions o Pamphlet or written information Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
60 ARTICLE 3.1 Your care from health professionals 5. Do you have a GP or a GP practice that you visit if you need a check-up, want advice about a health problem, or get sick or hurt? o Yes o No 6. Are you enrolled with a GP? o Yes o No o I don t know 12. When you went to see a GP or GP nurse, would the same GP or GP practice nurse usually see you? o Yes o No o I don t know 13. In the last 12 months, how often did this GP or GP nurse give you easy to understand instructions about taking care of your illness? o Never o Almost never o Sometimes o Usually o Almost always o Always o Medication script o Medication administered by a GP or nurse o Wound care o I don t know o Other 11. In the last 12 months, how many times did you visit a GP or GP nurse to get care for yourself? o 1 time o 4 o 2 o 5 to 9 o 3 o 10 or more times 16. The last time you couldn t be seen by a GP within 24 hours, why was that? o There weren t any appointments o The time offered didn t suit me o The appointment was with a GP I didn t want to see o I could have seen a nurse but I wanted to see a GP o I don t know o Another reason: Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
61 ARTICLE In the past 12 months, has there been a time when you wanted to see a GP, within the next 24 hours, but they were unable to see you? o Yes o No o I don t know 15. How many times has this happened in the past 12 months? o 1 time o 2 o 3 or more times o I don t know 17. In the past 12 months, did you phone a GP practice with a medical question during regular office hours or the practice with a medical question? A medical question includes test results. o Yes o No o I don t know/remember 18. In the past 12 months, when you phoned the GP practice during normal office hours or ed the GP practice, how often did you get an answer to your medical question the same day? o Always o Usually o Sometimes o Never o I don t know/remember 19. In the last 7 days, how many times did you visit a GP or GP nurse to get care for yourself? o Never g If Never, go to #21 on page 5 o 1 time o 2 o 3 or more times 20. In the last 7 days, how often did this GP or GP nurse give you easy to understand instructions about taking care of your illness? o Never o Almost never o Sometimes o Usually 22. Did any of these reasons about accessing a GP make you choose not to see a GP before going to hospital, or delay you seeing a GP? o My GP wasn t open when I needed to see them, or it was after hours o I couldn t get in touch with the doctor o There were no appointments available Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
62 ARTICLE 3.1 o Almost always o Always 21. Did any of these reasons about a GP s or GP practice s behaviour make you choose not to see a GP before going to hospital or delay you seeing a GP? o I thought I would not be respected o I thought the GP would not want to help me o I do not trust GPs o I have had a negative experience with a GP in the past o I couldn t get transport to see the GP o I couldn t get childcare o I couldn t afford to see the GP o I couldn t afford to pay for medication if the GP was to give me a prescription o I owe the GP money o Other Please tell us more about this: o Other Please tell us more about this: 23. When you need a check-up, want advice about a health problem, or get sick or hurt, where would you prefer to go first? (Choose one only) o GP o Hospital o Other Please tell us more about this: About you 26. What is your age? o 0 4 o o 5 9 o o o o o o o o o o o o Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
63 ARTICLE When you went to the hospital did you think you would be admitted to hospital? o Yes o No 25. What would make it easier for you to see a GP? o Having transport to the GP o Free or low cost GP care o GP practice open after hours o Free or low cost after hours care o Feeling welcome at the GP practice o Feeling that the GP respects me o Other Please tell us more about this: 27. Are you? o Male o Female 28. What is your highest level of education? o Primary school / Kura kaupapa o Secondary school / Kura kaupapa (High School/College) o Tertiary / Wananga (University or Polytechnic) o No formal education 29. What is your hospital number (NHI)? (This might be on your hospital wrist band, or the kaiatawhai may be able to help you find it) Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
64 ARTICLE 3.1 Appendix 2: Pathways to Ambulatory Sensitive Hospitalisations: Child (caregivers) Survey Survey Instructions Answer each question by marking the box to the left of your answer. You are sometimes asked to skip over some questions in this survey. When this happens you will see an arrow with a note that tells you what question to answer next, like this: o Yes g If Yes, go to #1 on page 1 o No Your child s health 1. What illness did your child come into hospital for? 2. How long has your child had this illness? o 1 day 1 week (7 days) o Between 1 week and 1 month o Between 1 month and 3 months o Between 3 months and 12 months o More than 12 months o I don t remember 3. Does your child need or take medicine prescribed by a doctor for this illness? o Yes o No 4. Has your child been admitted to hospital with this illness before? o Yes o No o I don t know/remember 7. When was the last time your child saw a health professional for the illness they were admitted to hospital with? o Never g If Never, go to #21 on page 5 o The day I went to hospital o 2 days 1 week (7 days) ago o Between 1 week and 1 month ago o Between 1 month and 3 months ago o Between 3 months and 12 months ago o More than 12 months ago o I don t remember 8. What health professional/s did your child see for this illness before they went to hospital? o None o GP o GP nurse o Other 9. Was this the health professional/s your child usually sees if they need a check-up, get sick or hurt or you want advice about a health problem? o Yes o No 10. What care did your child receive from the health professional? o Referral to hospital o Advice or instructions o Pamphlet or written information Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
65 ARTICLE 3.1 Your child s care from health professionals 5. Does your child have a GP or a GP practice that you visit if they need a check-up, get sick or hurt or you want advice about a health problem? o Yes o No 6. Is your child enrolled with a GP? o Yes o No o I don t know 12. When you went to see a GP or GP nurse, would the same GP or GP practice nurse usually see your child? o Yes o No o I don t know 13. In the last 12 months, how often did this GP or GP nurse give you easy to understand instructions about taking care of your child s illness? o Never o Almost never o Sometimes o Usually o Almost always o Always o Medication script o Medication administered by a GP or nurse o Wound care o I don t know o Other 11. In the last 12 months, how many times did your child visit a GP or GP nurse to get care? o 1 time o 4 o 2 o 5 to 9 o 3 o 10 or more times 16. The last time your child couldn t be seen by a GP within 24 hours, why was that? o There weren t any appointments o The time offered didn t suit me o The appointment was with a GP I didn t want to see o I could have seen a nurse but I wanted to see a GP o I don t know o Another reason: Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
66 ARTICLE In the past 12 months, has there been a time when you wanted your child to see a GP, within the next 24 hours, but the GP was unable to see them? o Yes o No o I don t know 15. How many times has this happened in the past 12 months? o 1 time o 2 o 3 or more times o I don t know 17. In the past 12 months, did you phone a GP practice with a medical question about your child during regular office hours, or the practice with a medical question about your child? A medical question includes test results. o Yes o No o I don t know/remember 18. In the past 12 months, when you phoned the GP practice during normal office hours or ed the GP practice, how often did you get an answer to your medical question about your child the same day? o Always o Usually o Sometimes o Never o I don t know/remember 19. In the last 7 days, how many times did your child visit a GP or GP nurse to get care? o Never g If Never, go to #21 on page 5 o 1 time o 2 o 3 or more times Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
67 ARTICLE In the last 7 days, how often did this GP or GP nurse give you easy to understand instructions about taking care of your child s illness? o Never o Almost never o Sometimes o Usually o Almost always o Always 21. Did any of these reasons about a GP s or GP practice s behaviour make you choose not to take your child to a GP before going to hospital or delay you in taking your child to see a GP? o I thought I would not be respected o I thought the GP would not want to help me o I do not trust GPs o I have had a negative experience with a GP in the past 22. Did any of these reasons about accessing a GP make you choose not to take your child to a GP before going to hospital, or delay you in taking your child to see a GP? o My GP wasn t open when I needed to see them, or it was after hours o I couldn t get in touch with the doctor o There were no appointments available o I couldn t get transport to see the GP o I couldn t get childcare o I couldn t afford to see the GP o I couldn t afford to pay for medication if the GP was to give my child a prescription o I owe the GP money o Other Please tell us more about this o Other Please tell us more about this Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
68 ARTICLE When your child needs a check-up, gets sick or hurt or you want advice about a health problem, where would you prefer to take your child first? (Choose one only) o GP o Hospital o Other Please tell us more about this About your child 26. What is your child s age? o 0 4 o 5 9 o o Is your child? o Male o Female 24. When you went to the hospital did you think your child would be admitted to hospital? o Yes o No 25. What would make it easier for you to take your child to a GP? o Having transport to the GP o Free or low cost GP care o GP practice open after hours o Free or low cost after hours care o Feeling welcome at the GP przactice o Feeling that the GP respects me 28. What is your highest level of education? (parent or legal guardian) o Primary school/kura kaupapa o Secondary school/kura kaupapa (High School/College) o Tertiary/Wananga (University or Polytechnic) o No formal education 29. What is your child s hospital number (NHI)? (This might be on your hospital wrist band, or the kaiatawhai may be able to help you find it) o Other Please tell us more about this Te Hauora mō ngā Iwi Katoa NZMJ 28 October 2016, Vol 129 No 1444 ISSN NZMA
69 3.2 Health and Safety Performance Report March Recommendation: That this report be received. Prepared by: Michael Field (Group Manager, Occupational Health and Safety) Endorsed by: Fiona McCarthy (Director Human Resources) Glossary CO - Corporate CWF - Child, Women and Family Services ESC - Elective Surgical Centre HO - Hospital Operations MEDHOP - Medical and Health of the Older Persons Service MH - Mental Health and Addictions Services OH&S - Occupational Health and Safety SA - Surgical and ambulatory services 1. Purpose of report The purpose of the Health and Safety (H&S) report is to provide quarterly reporting of health, safety and wellbeing performance including compliance, indicators, issues and risks to the Waitemata District Health Board. 2. Strategic Alignment Community, whanau and patient centred model of care Emphasis and investment on both treatment and keeping people healthy Intelligence and insight Evidence informed decision making and practice Outward focus and flexible, service orientation Operational and financial sustainability This report comments on issues and risks that impact of patient care and organisational culture. This report comments on organisational health information via incidents, health monitoring, and leave information. The report provides information and insight into workplace incidents and what the DHB is doing to respond to these and other workplace risks. The leading and lagging indicator dashboard is based on current best practise indicators and targets. Health, safety and wellbeing risks and programmes are inherently focused on staff, patients, visitors, students and contractors. All strategic and operational work programmers and policy decisions are discussed with relevant services e.g. site visits, approaches to reduce risks (Section 6). As appropriate, programmes of work will outline how services will ensure operational or financial sustainability and how measures of success are set and value and return on investment is monitored. Waitemata District Health Board, Meeting of the Board 01/03/17 69
70 Trend highlights at a glance (rolling 12 months) 3.2 Staff incidents The growth in reported staff incidents is beginning to slow and it is expected that this trend will continue for the next 6 months. Injury claims, frequency and severity are all trending down or are stable. Pre-employment Screening Pre-employment screening prior to commencement remains steady, however this is expected to change when we rollout out compulsory screening process, scheduled for February next year. Process currently in pilot in Mental Health Services. Health and Safety representative vacancies Health and Safety Representative vacancies are decreasing, which is a positive sign as we engage in increased health and safety activity and training. Attendance at Health and Safety Orientation Attendance at the DHB health and safety orientation continues to be high. Number of staff injury claims The number of staff injury claims, although varying to a large degree month on month, remains fairly stable on average. If current trends continue, this will begin to reflect a downward trend over time. Key Increased performance Steady performance Decreased performance Waitemata District Health Board, Meeting of the Board 01/03/17 70
71 Performance Scorecard 3.2 In summary, for January Downward trend in number of staff reported incidents No contractor incidents reported Injury frequency Steady uptake of orientation and health and safety rep training Steady levels of pre-employment screening prior to employment Slight decrease in hand hygiene from last month (85% vs 87%) Waitemata District Health Board, Meeting of the Board 01/03/17 71
72 Key Health and Safety Risks The table below outlines our key health and safety risks together with commentary on the current status/issues related to that risk and any actions to address issues. We have added residual risk (the portion of risk that is left after a risk assessment has been conducted) to this table. The actions reported each month are controls in progress and the residual risks from each of these identified risk areas will vary. The DHB has attempted to note the residual risk in the context of the original risk using a traffic light after each risk below. Risk: Aggression-physical and verbal Previous Report Action Community worker alarm tender evaluations complete and business case being drafted. Complete: 30% Draft police complaints policy has been reviewed and feedback provided to Legal Services to complete policy. Complete: 50% Current Action No change from previous report, due to holiday period. Complete: 30% Awaiting final version from Legal Services. Complete: 50% Red Beach Hazard Review: Recommendations provided following the hazard review are either complete or underway. Complete: 25% He Puna Waiora hazard review complete. Complete: 100% All Mental Health Unit reviews have now been completed and the resulting reports supplied to the service. Many of the immediate actions have already been implemented and it is expected that the majority of the remainder will be complete by early next year. Complete: 75% All actions implemented, awaiting final installation of reception desk bar top and side screens. Complete: 80% All actions now completed. Additional actions requested during follow-up site walkthrough, however not of significant risk. Complete: 95% (in light of new actions) Actions almost completed and prioritisation of remaining actions is underway. Complete: 85% New action: Template for services to review their public reception areas planned and due to roll out March Complete: 0% Residual Risk: As these projects are still underway, the residual risk has not changed. It is envisioned that the residual risk levels will reduce upon project delivery. Original Risk Residual Risk Waitemata District Health Board, Meeting of the Board 01/03/17 72
73 3.2 Risk: Blood and Body Fluid Incidents (BBFA) Previous Report Action Needleless systems: Rollout continues to progress into other areas of Waitemata DHB. Deep dive audit scheduled for April Complete: 65% Residual Risk: Nil change Original Risk Risk: Hazardous Substances (HSNO) Previous Report Action HSNO audits continue to progress on-target, with great progress being made in high use/volume areas that have undergone audit to date. Complete: 15% HSNO inventory is currently being updated to allow for a greater level of automation and for each area to be able to use it to produce local level inventories. Complete: 15% Current Action Needleless systems: No change due to holiday period. Complete: 65% Residual Risk Current Action HSNO audits continue to progress on-target, with great progress being made in high use/volume areas that have undergone audit to date. Audits completed: 18% HSNO inventory work has been completed, including automation for areas to create their own specific registers. Complete: 100% The Waitakere Hospital Hazardous Goods Store is being retendered week commencing , and we are hopeful that we will be able to obtain more competitive pricing. Tender duration is 15 days. Complete: 10% Tender has been extended to end February. Complete: 10% Residual Risk: As this audit project progresses and each area becomes compliant, this residual level of risk will reduce. Original Risk Residual Risk Risk: Contractor and Procurement Management Previous Report Action The Asbestos Management Group is currently investigating options with ADHB to use their asbestos register system. Complete: 40% A meeting has been held with Facilities and Development Trades staff and Project Managers about potential exposure sources and the need for these staff to take all appropriate measures to protect themselves. Complete: 100% A Facilities and Development Health and Safety Manager has been appointed to progress outstanding contractor processes such as review of orientation, shared PCBU responsibilities, and environmental and construction reviews. Complete: 50% Residual Risk: Nil change. Original Risk Current Action Facilities are now working through the process of matching our own registers and information with the fields available within the ADHB Asbestos Register, to ensure compatibility. Complete: 60% No update required (will be removed for next report). Complete: 100% A Facilities and Development Health and Safety Manager has commenced work and OH&SS are collaborating closely with him to fast-track project and system implementation. Complete: 80% Residual Risk Waitemata District Health Board, Meeting of the Board 01/03/17 73
74 3.2 Risk: Manual and Patient Handling Previous Report Action All OH&SS staff are attending manual handling training, to ensure they are able to provide adequate and consistent advice. Complete: 90% Manual handling incidents remain high so an audit has been commissioned via internal audit to review what else we can do to manage these incidents. Complete: 10% Original Risk Current Action All OH&SS staff have now completed the Moving & Handling training. Complete: 100% Manual handling incidents reducing so audit may not be needed, however each incident will continue to be reviewed. Complete: 10% Residual Risk Risk: Health and Wellbeing (stress, fatigue, depression) Previous Report Action Progress continues to be made in the implementation of the strategy; however it is worth noting that this constitutes a 3 year process. Complete: 15% Original Risk Risk: Physical environment (ventilation, lighting, equipment) Previous Report Action A number of issues have been directly addressed relating to heating and/or cooling within areas, with very quick responses from Facilities Maintenance. Complete: 100% Current Action Planning has commenced regarding project prioritisation. Work on the current projects: Well at work expo Summer events Walking challenge Diversity fund Mindfulness and wellbeing sessions Health assessments Complete: 20% Residual Risk Current Action No update required (will be removed for next report) Complete: 100% All recommendations to improve the helipad have been accepted and a project manager is being allocated by Facilities and Development to arrange the required works. Complete: 60% Progress continues to be made. Complete: 65% Loading Docks: This review has been completed and recommended actions provided and approved for implementation. Contact has been made with Facilities and Development for the allocation of a Project Manager to oversee these works. Complete: 40% Loading Docks: Awaiting final costs from facilities Project Manager. Complete: 40% Residual Risk: The residual risk remains the same at present until we complete some environmental projects and get regular environment reviews underway. Original Risk Residual Risk Waitemata District Health Board, Meeting of the Board 01/03/17 74
75 3.2 Risk: Slips trips and Falls Previous Report Action Replacement of non-slip carpet is to be completed this year. Complete: 80% Staff communications: ACC have notified us that their communications will not be ready until midnext year, so we have begun developing our own communications strategy and will engage with Communications to assist us with this. Complete: 60%. Current Action Replacement work continues. Complete: 90% Staff communications: Project has been instigated with communications to progress this work. Complete: 65% Residual Risk: The residual risk has dropped for entryways, however this makes up a small proportion of overall slip, trip and fall events, requiring the residual risk to remain the same. As staff communications are developed and delivered, it is expected that this residual risk will fall. Original Risk Residual Risk 4. Stakeholder feedback 4.1 Funding, Planning and Outcomes Nil to report this period 4.2 Regulatory Bodies WorkSafe NZ has now released a number of guidance documents, each of which is being incorporated into our understanding and processes, where applicable. These guidance documents cover: Reasonably Practicable - a quick guide as to the meaning of the terminology, confirming our existing understanding Violence at work customer service areas - this has provided support for the previously designed template for reception hazard reviews Overlapping duties - this guide covers off overlapping duties where more than one PCBU is involved on a site or in an incident. This document has been shared with Facilities to ensure consistency of understanding, where dealing with contractors Waitemata District Health Board, Meeting of the Board 01/03/17 75




76 5. Staff Reported Incidents 3.2 Rolling year-on-year monthly average comparison: Previous 12 months Current 12 months Current Period: The number of reported incidents by staff during the month of November 2016 was 151, December 2016 was 125 and January 2017 was 97. Rolling 12 month analysis: The number of reported staff incidents has begun to slow and this trend is expected to continue for the next 6 months before finally stabilising. Factors that reassure us the number of incidents themselves are not a concern includes the indicators for claims, injury frequency and injury severity, which are heading down or stable. Waitemata District Health Board, Meeting of the Board 01/03/17 76
77 Notifiable Events The DHB noted 0 notifiable events in November The DHB noted 1 notifiable event in December A staff member was playing table tennis, fell and fractured their ankle and was admitted to hospital for surgery The DHB noted 0 notifiable events in January Waitemata District Health Board, Meeting of the Board 01/03/17 77

78 7. Top Incident types that cause harm 3.2 The main types of incidents that cause harm to our staff and their management are outlined in the following tables. 7.1 Aggression Rolling year-on-year monthly average comparison: Previous 12 months Current 12 months Actions: The DHB is continuing to work on the Security Review Project, which includes the following workstreams: Security policy and procedures (in draft) Risk framework (already in use) Training (draft schedule in discussion) Community worker alarms (in RFP) Emergency department (managing appropriate behaviours) Security alerts (procedure to be developed) Tracking vulnerable patients (in RFP) Rolling 12 month analysis: Our focus remains strongly focussed on public/staff interface points, including reception areas. Trend Analysis: The nature of aggression incidents makes trend analysis between services extremely difficult (i.e. why is MEHOP high one report and MH high the next). Recent incidents in the MEHOP service stem from: 1. Unwell patients with difficult behaviours generating several incidents 2. Patients new to the ward or hospital and settling into or transferring into care Waitemata District Health Board, Meeting of the Board 01/03/17 78





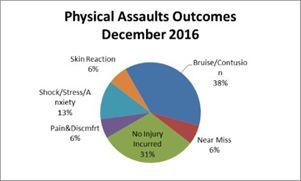
79 3.2 Waitemata District Health Board, Meeting of the Board 01/03/17 79
, inattention (5), obstruction (2) Unsafe/Improper Practice (1) and wet floor (1).")
, wet floor (1), work practice (2), faulty equipment (1), inattention (1), polished/greasy surface (2).")
80 Slips, Trips and Falls Rolling year-on-year monthly average comparison: Previous 12 months Current 12 months Current period: The 17 Slips, trips and falls in November were categorized as being caused by: environment (8), inattention (5), obstruction (2) Unsafe/Improper Practice (1) and wet floor (1). The 13 Slips, trips and falls in December were categorized as being caused by: environment (3) obstruction (2) unsafe/improper practice (1), and wet floor (2), work practice (3), faulty equipment (2). The 11 Slips, trips and falls in January were categorized as being caused by: environment (4), wet floor (1), work practice (2), faulty equipment (1), inattention (1), polished/greasy surface (2). Rolling 12 month analysis: The reported incidents of slips, trips and falls have reduced, in line with the warmer and less wet weather. Trend Analysis: Slips trips and falls are very much driven by changes in weather, with wet period leading to higher incidents. A message for staff not to text and walk has been circulated as inattention is a high factor in falls. Waitemata District Health Board, Meeting of the Board 01/03/17 80

81 Moving and Handling Rolling year-on-year monthly average comparison: Previous 12 months 9.42 Current 12 months 7.17 Current period: Of the 6 incidents recorded in November, 3 were categorized as pain and discomfort, 1 was a sprain/strain, 1 was bruise/contusion, and 1 was no injury incurred. Of the 8 incidents recorded in December, 3 were categorized as pain and discomfort, 3 were sprains/strains, 2 were bruise/contusion. Of the 4 incidents recorded in January, 3 were categorized as strain/sprain, 1 was bruise/contusion. Rolling 12 month analysis: Moving and handling related injuries to staff continues to be of concern, however collaborative work between OH&SS and Moving and Handling seems to be positively impacting on the number of reported incidents. This trend is likely to continue, as more areas undergo Moving and Handling training. Trend Analysis: Moving and Handling incidents tend to fall in line with increases and decreases in patient numbers within the hospital environment, with higher numbers leading to more incidents (i.e. the more patients we are handling, the higher the chance of an incident occurring). Waitemata District Health Board, Meeting of the Board 01/03/17 81
82 8. Health, Safety and Wellbeing Activity Occupational Health Influenza Vaccinations Planning has commenced for the 2017 flu campaign, with over 50 localised vaccinators being trained to administer flu vaccinations in a far more accessible way for staff. We are also looking at running spot clinics during staff handovers and meeting times, in order to maximise the numbers of staff we are able to offer vaccinations to. 8.2 Training Requirements We continue to work with Learning and Development training schedules for all staff. Dates for the Board level Governance training are to be confirmed. Manager training is scheduled to continue throughout Safe Way of Working (SWoW) self-audit tool Development of a new self-audit tool, following the 12 key elements of our Safe Way of Working has now been completed (Appendix 2). This self-audit is designed to allow Waitemata DHB to understand levels of compliance from an individual group level, all the way through to a divisional level. It is also designed as a resource for managers, to assist them in understanding the expectations relating to Health, Safety and Wellbeing. This audit tool is scheduled to be completed by all areas of Waitemata DHB in April of each year, with any areas showing a higher need for improvement undergoing a follow-up audit in the six months following. 8.4 Working with our business partners In recognition that some of our contractors work with us in a far more integrated way, we have designated these contractors as business partners. At this stage, this includes healthalliance and Compass, both of which we have engaged with collaboratively to enable them to integrate with our own Health and Safety systems. We have also set up regular meetings with them and have invited representatives to join our Health, Safety and Wellbeing Committee. 8.5 Health and Safety Resource Recommendations Update Work has progressed regarding the resource recommendations first presented to the Board in August 2016, with each item either completed or underway. The two most notable achievements are the finalisation of the Safe Way of Working Audit, which will increase visibility of compliance and achievements, and the recruitment of a Health and Safety Manager for Facilities. With the new position in place, Facilities are now able to dedicate resource to the area of Health and Safety, strongly supported and working in collaboration with Occupational Health and Safety. An update on the resource recommendations will occur in August Waitemata District Health Board, Meeting of the Board 01/03/17 82
83 Appendix Glossary for Monthly Performance Scorecard and Report Lost time incidents Lost time injury Frequency Rate Injury Severity Rate Lost Time Injury Rate Notifiable Injury/illness Notifiable Incident Notifiable Event Pre- Employment Significant Hazard (Instead of a definition all hazards are risk rated to determine how serious they are in the new legislation) Psychosocial Risk Patients who are away without leave (AWOLs) PCBU Officer Worker Reasonably Practicable Any injury claim resulting in lost time. No of lost time Injuries per million hours worked. Mathematical calculation that describes the number of lost days experienced as compared to the number of incidents experienced. Mathematical calculation that describes the number of lost time injuries per 100 fulltime employees at any given time frame. (a) Amputation of body part, serious head injury, serious eye injury, serious burn, separation of skin from underlying tissue, a spinal injury, loss of bodily function, serious lacerations. (b) any admission to hospital for immediate treatment (c) any injury /illness that requires medical treatment within 48 hours of exposure to a substance (d) any serious infection (including occupational zoonoses) to which carrying out of work is a significant factor, including any infection attributable to carrying out work with micro-organisms, that involves providing treatment or care to a person, that involves contact with human blood or bodily substances, involves contact with animals, that involves handling or contact with fish or marine mammals. (e) any other injury/illness declared by regulations to be notifiable. An unplanned or uncontrolled incident in relation to a workplace that exposes a worker or any other person to a serious risk to that person s health or safety arising from an immediate or imminent exposure to an escape, spillage or leakage of a substance; an implosion explosion or fire; an escape of gas or steam; an escape of a pressurised substance; an electric shock; a fall or release from height of any plant or substance; collapse or partial collapse of a structure; interruption of the main system of ventilation in an underground excavation or tunnel; collision between two vessels or capsize; or any other incident declared by regulations to be a notifiable incident. Death of a person, notifiable injury or illness or a notifiable incident. Health screening for new employees A hazard with the potential to cause serious harm. Might be those aspects of the design and management of work and its social and organisational contexts that have the potential for causing psychological or physical harm. Patients under the Mental Health (compulsory Assessment and Treatment) Act 1992, who leave DHB premises without prescribed or approved leave Person conducting business or undertaking Person occupying the position of a director of a company or includes any other person occupying a position in relation to the business or undertaking that allows the person to exercise significant influence over the management of the business or undertaking. An individual who carries out work in any capacity for the PCBU e.g. employee, contractor or sub-contractor, employee of the sub-contractor, employee of labour hire company, outworker, apprentice or trainee, person gaining work experience, volunteer. Means that which is or was at a particular time reasonably able to be done in relation to ensuring health and safety, taking into account and weighing up all relevant matters.eg the likelihood of the hazard/risk occurring and the degree of harm resulting, what the person knows about hazard/risk and how to eliminate/ minimise the risk and the cost associated with elimination of the hazard/risk. Waitemata District Health Board, Meeting of the Board 01/03/17 83
84 Appendix 2 - Auditing A Safe Way of Working Management System 3.2 Health & Safety Wellbeing Management System Audit Table of Contents 1. Framework Purpose Scope Reference Document Frequency Responsibilities Occupational Health and Safety Service General Manager Manager/Supervisor at Departmental Level Health and Safety Representative Operational Manager/Service Manager (or equivalent) Where Immediate Action is Required Appendix A: SWOW Audit Tool Department Level Brief Input Results A Safe Way of Working Departmental Audit Appendix B: SWOW Audit Tool Operations/Service Level Brief Inputs Example Synthesis and Results A Safe Way of Working Service Audit Element 1: Policy, Objectives & Organisational Responsibility...15 Element 2: Employee Participation...16 Element 3: Design, Construction, Maintenance and Renovation (Contractor Management)...17 Element 4: Emergency Planning and Readiness...18 Element 5: Hazard Management and Risk Assessment...19 Element 6: Hazardous Substance Management...21 Element 7: Health and Wellbeing Management...22 Element 8: Plant, Machinery and Equipment Management...23 Element 9: Procurement and Purchasing Management...24 Element 10: Notifiable Event, Incident and Near Miss Management...25 Element 11: Worker, Patient, Visitor and Public Safety and Security Management...26 Element 12: Work Method and Procedures Management...27 Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 1 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 84
 is part of the Waitemata District Health Board (Waitemata DHB) Quality and Risk Management System (Figure 1). Figure 1.")
85 Appendix 2 - Auditing A Safe Way of Working Management System 3.2 Health & Safety Wellbeing Management System Audit 1. Framework 1.1 Purpose The Safe Way of Working (SWOW) is part of the Waitemata District Health Board (Waitemata DHB) Quality and Risk Management System (Figure 1). Figure 1. Waitemata DHB is committed to promoting & maintaining the health, safety & wellbeing of everyone affected by its activities This document aims to provide a standard audit process to assess and gauge the level of conformance with the established key performance indicators (KPIs) under the SWOW across Waitemata DHB. 1.2 Scope This document applies to all areas of the Waitemata DHB and is relevant to all workers/employees, including volunteers and students. The document describes the process the auditors need to follow when conducting the SWOW audit. The Auditors in this document refer to the following: The Departmental Manager/supervisor who is expected to complete the audit tool in Appendix A. They may find the support of the Health and Safety Representative (H&SR) useful in completing this tool; and, The Waitemata DHB division s Operational Manager/Service Manager who is expected to complete the audit tool in Appendix B. The audit tools in this document cover the KPIs for the twelve (12) elements of the SWOW Health, Safety & Wellbeing system. Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 2 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 85
86 Appendix 2 - Auditing A Safe Way of Working Management System 3.2 Health & Safety Wellbeing Management System Audit 1.3 Reference Document Safe Way of Working, , March Frequency Annually (every 12 months), occurring in April each year. Any audit result that raises concern will be subject to a repeat audit 6 months later (frequency of audit is subject to review). 2. Responsibilities The audit tools have been developed to oversee the implementation and effectiveness of the SWOW management system and to identify opportunities for continual improvement. The Waitemata DHBs Occupational Health and Safety Service will respond where low scores have been identified and support any identified opportunities for continual improvement. Each SWOW element has a set of guide questions to audit and assess the KPI for that element. The auditors will answer the guide questions and confirm that documented evidence of compliance is available. Waitemata DHB s Occupational Health and Safety Service will conduct random internal audits of this documented evidence, so there will be a requirement to produce documented evidence to support the initial audit findings. 2.1 Occupational Health and Safety Service Responsible for the overview of the audit process, both organisationally and by division, with accountability held by the Director of HR. Identifying areas of concern and notifying the area and relevant managers, including General Manager, of 6 month repeat audit requirement, along with details on specific audit items to be improved and actions to be taken. Provide support and assistance to areas undergoing audit. Annually this will be light support, clarifying audit questions etc; however a high level of support will be supplied to areas undergoing a 6 month repeat audit. Provision of reports of audit outcomes, including year-on-year changes, to varying levels of detail, to: o WDHB Board o Health, Safety & Wellbeing Committee o Executive Leadership Team o Senior Management Team o General Managers 2.2 General Manager The General Managers are accountable for ensuring that the plan of actions, arising from each audit, are developed and implemented. The General Managers are responsible for overseeing any required 6 month repeat audit, as advised by the Occupational Health and Safety Service. Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 3 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 86
87 Appendix 2 - Auditing A Safe Way of Working Management System 3.2 Health & Safety Wellbeing Management System Audit 2.3 Manager/Supervisor at Departmental Level To complete audit attached as Appendix A. Ensure responses are based on available documented evidence. Supply completed form to Operational Manager/Service Manager to allow them to compile results with other Departmental audit results and complete form found in Appendix B. Please also copy to the Occupational Health and Safety Service. 2.4 Health and Safety Representative Provide support to the Manager/Supervisor, as necessary. 2.5 Operational Manager/Service Manager (or equivalent) Collect all completed audit forms from Manager/Supervisors at Departmental Level. Complete the form attached as Appendix B based on the data gathered and supply a copy to the Occupational Health and Safety Service. 2.6 Where Immediate Action is Required Where issues are identified that require immediate action, the manager/supervisor of the area is required to take action. Where immediate action is not possible, for whatever reason, including budgetary constraints, insufficient delegated authority etc, the matter must be immediately escalated to the next level of management. This escalation process must continue until action is able to be taken, up to and including seeking approval from the General Manager. Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 4 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 87
88 Appendix 2 - Auditing A Safe Way of Working Management System 3.2 Health & Safety Wellbeing Management System Audit 3. Appendix A: SWOW Audit Tool Department Level 3.1 Brief This audit aims to assess the level of conformance with the established key performance indicators (KPIs) under the 12 Elements of the Safe Way of Working across Waitemata DHB at a Departmental Level. 3.2 Input The guide questions are answerable by Yes, No, or Partial. Acceptable verifications or evidences are provided for each question. If the question merits a partial response, an indication of compliance is recommended to be included on the Notes section of the audit form. Response guideline is summarised in Table A-1. Table A-1. Response guideline for auditors at departmental level. Response Description Yes (Y) A question merits a yes (Y) response if there is documented evidence of full compliance. Note: There may be a requirement to produce evidence to support the findings. Partial (P) No (N) Not Applicable (N/A) A question merits a partial (P) response if there is partial evidence (i.e. not full) to answer the question. It usually prompts the following responses: not all, most of the time, or usually. A question merits a No (N) response if there is no documented evidence or verification to answer the question. A question merits not applicable (N/A) if the question does not apply to the work place. Please ensure this is definitely the case before responding with N/A. 3.3 Results The completed form must be provided to the Operational/Service Manager for completion of the audit tool in Appendix B and a copy sent to the Occupational Health and Safety Service. Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 5 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 88
89 A Safe Way of Working Departmental Audit Auditor: Designation: Date: Department: Question Verifications Result Notes 1 Policy, Objectives & Organisational Responsibility 1.1 Is health, safety and wellbeing (HS&W) a fixed agenda item in team meetings? Meeting minutes Y/N/P 1.2 Are the minutes of the meetings documented and available? Records of minutes Y/N/P 1.3 All staff has undergone local induction? Local induction form Y/N/P 1.4 Does the local induction checklist include HS&W? Local induction form Y/N/P 2 Employee Participation 2.1 Do you have a Health and Safety Representative/s (H&S Rep) in your department or work group/s? H&S Rep name Y/N/P 2.2 Have the H&S Reps attended all required training? Records of training/certificates Y/N/P 2.3 Has the manager attended HS&W training within the last 2 years? Records of training Y/N/P Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 6 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 89
90 Question Verifications Result Notes Have all workers/employees completed their mandatory training? Records of training Y/N/P 2.5 Do the manager and H&S Rep attend divisional meetings? Meeting minutes Y/N/P 2.6 Are HS&W hazards, near misses, or incidents discussed in team meetings? Meeting minutes Y/N/P 3 Design, Construction, Maintenance & Renovation (Contractor Management) 3.1 Are managers aware of contractors in their areas? Department records of notification Y/N/P 3.2 Do contractors undergo local induction in your work area/department? Induction records Y/N/P 3.3 Are workers/staff advised and made aware of the contractors and associated hazards in the work area before contractors start work? 3.4 Are the workers/staff/end users consulted for design input when refurbishment is done in the work area? 4 Emergency Planning and Readiness 4.1 Do you have a documented emergency response procedure in your work area? Correspondence records/notification Procedure for review of associated risks and hazards Correspondence records/meeting minutes Document Y/N/P Y/N/P Y/N/P 4.2 Do you have an emergency response plan displayed in your Signage Y/N/P Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 7 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 90
91 work area? Question Verifications Result Notes Have you had an emergency response practice? Evacuation record/ records of trainings. Designated fire warden 5 Hazard Management and Risk Assessment 5.1 Is the hazard register current and regularly maintained in your work area? Completed hazard register 5.2 Are all hazards adequately investigated and addressed? Completed hazard register Y/N/P Y/N/P Y/N/P 5.3 Are hazards, risks, and corrective/corrected actions communicated and discussed with all staff? Correspondence records Y/N/P 5.4 Are health and safety audit schedules adhered to? Audit forms Y/N/P 5.5 Are hazard reviews of reception areas conducted every six months? 6 Hazardous Substance Management 6.1 Do you have an inventory for all the hazardous substances on your workplace? Audit forms Copy of inventory Y/N/P Y/N/P 6.2 Do you have Safety Data Sheets (SDS) for all hazardous substances in your work place and accessible to staff? Copies of SDS Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 8 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. Y/N/P 91
92 Question Verifications Result Notes Are workers/staff aware of Waitemata DHB s policy and the hazardous substances page on Staffnet? Ask workers/staff and manager Y/N/P 6.4 Are all hazardous substances labelled, stored, and disposed of according to manufacturer s instructions? 6.5 All personal protective equipment (PPE) is available, used, and maintained? 6.6 Are the relevant workers/staff aware of spill procedure and spill kit available, as appropriate? Inspect Inspect Inspect Y/N/P Y/N/P Y/N/P /NA 7 Health & Wellbeing Management 7.1 Does the H&S notice board have current information on: - ACC Partnership Program - Incident reporting - Employee Assistance Program (EAP) - Bullying & harassment contacts - OH&SS - Who the H&S Reps are - Fire Wardens - Latest wellbeing initiatives? 7.2 Have all new workers/employees been screened for fitness of role (i.e., pre-employment screening)? Inspect View records Y/N/P Y/N/P 7.3 Are manager and workers/employees aware of the Minutes of Y/N/P Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 9 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 92
93 Question Verifications Result Notes rehabilitation process and return to work program? rehabilitation meetings Plant, Machinery and Equipment Management 8.1 Do all equipment (e.g., clinical equipment and non-clinical equipment such as heaters, electrical appliances, motor vehicles etc) have maintenance schedule attached (i.e., tagged)? View equipment or tags Confirm with facilities Y/N/P 8.2 Do workers/staff know how to report faulty equipment? Ask staff Y/N/P 8.3 Are workers/staff aware on the need to visually inspect equipment prior to use? Ask staff Y/N/P 8.4 Is Personal Protective Equipment (PPE) used when required? Inspect Y/N/P 8.5 Does all equipment have an asset number? View equipment Y/N/P 9 Procurement & Purchasing Management 9.1 Are area workers/staff consulted prior to purchasing equipment or new products? 9.2 Is there a training programme for new equipment/products prior to their use? View correspondences or documentation View documentation, records, correspondences Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 10 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. Y/N/P Y/N/P 10 Notifiable Event, Incident, and Near Miss Management 10.1 Have manager(s) been trained in incident and accident Training records Y/N/P 93
94 Question Verifications Result Notes investigation (e.g. received training from Quality Service)? Are reports on employee accidents/incidents reported back to workers/staff working in the area or department? 10.3 Are workers/staff aware of correct procedure for reporting an incident at work? 10.4 Do managers investigations include corrective/preventative actions? View documents, reports, or minutes Ask employee Incident reports Trend reporting from health and safety minutes Y/N/P Y/N/P Y/N/P 11 Worker, Patient, Visitor & Public Safety and Security Management 11.1 Are local hazards clearly identifiable to non WDHB employees? View signage Y/N/P 11.2 Are there records kept showing orientation to your department for students, volunteers, other groups? 11.3 Do workers/staff record every incident of verbal and physical aggression? View records Documentation on student competency level View records Y/N/P Y/N/P 12 Work Method and Procedures Management 12.1 Are there safe operating procedures (SOPs) or safe working procedures (SWP) in the work area and are they available to the workers/staff? View documents, signage Clinical notes, Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 11 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. Y/N/P 94
95 Question Verifications Result Notes guidelines, procedures, care plans etc 3.2 Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 12 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 95
96 Management System Auditing A Safe Way of Working (SWoW) 3.2 Health & Safety Wellbeing Management System Audit 5. Appendix B: SWOW Audit Tool Operations/Service Level 5.1 Brief This audit aims to assess the level of conformance with the established key performance indicators (KPIs) under the 12 Elements of the Safe Way of Working across Waitemata DHB at an Operational/Service level. 5.2 Inputs This audit requires the completion of the Departmental audits using the tool in Appendix A. The total number of Yes, No, and Partial responses for each question for all the departments will be tallied for the service. Where a question in a criterion is answered as not applicable, it will not be given a score. It is important to check that the question is genuinely not applicable. The maximum score should be adjusted accordingly. 5.3 Example An example of a completed part of the form is set out below. It is based on the following scenario: A total of 10 departments completed the audit (Appendix A) for a Service; For question 1.1, out of the ten (10) departments, four (4) answered yes, two (2) answered No, and four (4) answered Partial ; and, The example template below has been completed based on the scenario outlined above. Element 1: Policy, Objectives & Organisational Responsibility Guide Questions 1.1 Health, Safety and Well-being (HS&W) is an agenda item at all department meetings? 1.2 Are the minutes of the meetings documented and available? 1.3 All staff have undergone local induction? 1.4 Does the local induction checklist include HS&W? Yes Response No Response Partial Response # of # of # of Yes % % % No Partial 4/10 40% 2/10 20% 4/10 40% 5/10 50% 1/10 10% 4/10 70% 6/10 60% 1/10 10% 3/10 30% 9/10 90% 0/10 0% 1/10 10% Total for the Element 24/40 60% 4/40 10% 12/40 30% Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 13 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 96
97 Management System Auditing A Safe Way of Working (SWoW) 3.2 Health & Safety Wellbeing Management System Audit 5.4 Synthesis and Results The results of this audit are to be collated, packaged, and supplied to the General Manager and a copy provided to the Occupational Health and Safety Service. Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 14 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 97
98 Auditing A Safe Way of Working (SWoW) Management System A Safe Way of Working Service Audit Health & Safety Wellbeing Management System Audit Auditor: Date: Designation: Service: Version: Version 1, September 2016 Division: Element 1: Policy, Objectives & Organisational Responsibility Yes Response No Response Partial Response Guide Questions # of # of Yes % # of No % Partial % 1.1 Health, Safety and Well-being (HS&W) is an agenda item at all / / / department meetings? 1.2 Are the minutes of the meetings documented and available? / / / 1.3 All workers/staff have undergone local induction? / / / 1.4 Does the local induction checklist include HS&W? / / / Total for the Element / / / Notes/Comments: Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 15 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 98
99 Auditing A Safe Way of Working (SWoW) Management System 3.2 Health & Safety Wellbeing Management System Audit Element 2: Employee Participation Yes Response No Response Partial Response Guide Questions # of # of Yes % # of No % Partial % 2.1 Is there a Health and Safety Representative (H&S Rep) in the / / / department/work group? 2.2 Have the H&S Reps attended all required training? / / / 2.3 Have managers for each department undertaken training in / / / HS&W in the last two years? 2.4 Have all workers/employees undertaken required yearly / / / mandatory training? 2.5 Do the managers and H&S Reps attend divisional meetings? / / / 2.6 Are HS&W hazards, near misses, or incidents discussed in team / / / meetings? Total for the Element / / / Notes/Comments: Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 16 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 99
100 Auditing A Safe Way of Working (SWoW) Management System 3.2 Health & Safety Wellbeing Management System Audit Element 3: Design, Construction, Maintenance and Renovation (Contractor Management) Yes Response No Response Partial Response Guide Questions # of # of Yes % # of No % % Partial 3.1 Are managers aware of contractors in their areas? / / / 3.2 Do contractors undergo local induction in your work / / / area/department? 3.3 Are workers/staff advised and made aware of the contractors and / / / associated hazards in the work area before contractors start work? 3.4 Are the workers/staff/end users consulted for design input when / / / refurbishment is done in the work area? Total for the Element / / / Notes/Comments: Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 17 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 100
101 Auditing A Safe Way of Working (SWoW) Management System 3.2 Health & Safety Wellbeing Management System Audit Element 4: Emergency Planning and Readiness Yes Response No Response Partial Response Guide Questions # of # of Yes % # of No % Partial % 4.1 Do you have a documented emergency response procedure in / / / your work area? 4.2 Do you have an emergency response plan displayed in your work / / / area? 4.3 Have you had an emergency response practice? / / / Total for the Element / / / Notes/Comments: Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 18 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 101
102 Auditing A Safe Way of Working (SWoW) Management System 3.2 Health & Safety Wellbeing Management System Audit Element 5: Hazard Management and Risk Assessment Yes Response No Response Partial Response Guide Questions # of # of Yes % # of No % Partial % 5.1 Is the hazard register current and regularly maintained in your / / / work area? 5.2 Are all hazards adequately investigated and addressed? / / / 5.3 Are hazards, risks, and corrective/corrected actions / / / communicated and discussed with all workers/staff? 5.4 Are health and safety audit schedules adhered to? / / / 5.5 Are hazard reviews of reception areas conducted every six months? Total for the Element / / / Notes/Comments: Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 19 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 102
103 Auditing A Safe Way of Working (SWoW) Management System 3.2 Health & Safety Wellbeing Management System Audit Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 20 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 103
104 Auditing A Safe Way of Working (SWoW) Management System 3.2 Health & Safety Wellbeing Management System Audit Element 6: Hazardous Substance Management Yes Response No Response Partial Response Guide Questions # of # of Yes % # of No % Partial % 6.1 Do you have an inventory for all the hazardous substances in your / / / workplace? 6.2 Do you have Safety Data Sheets (SDS) for all hazardous / / / substances in your work place and accessible to workers/staff? 6.3 Are workers/staff aware of Waitemata DHB s policy and the / / / hazardous substances page on Staffnet? 6.4 Are all hazardous substances labelled, stored, and disposed of / / / according to manufacturer s instructions? 6.5 All personal protective equipment (PPE) is available, used, and / / / maintained? 6.6 Are the relevant workers/staff aware of spill procedure and spill / / / kit available, as appropriate? Total for the Element / / / Notes/Comments: Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 21 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 104
105 Auditing A Safe Way of Working (SWoW) Management System 3.2 Health & Safety Wellbeing Management System Audit Guide Questions 7.1 Does the H&S notice board have current information on ACC partnership program, incident reporting, Employee Assistance Program (EAP), bullying & harassment contacts, Occupational Health & Safety Service (OH&SS), H&S Reps, fire wardens, and latest wellbeing initiatives? 7.2 Have all new workers/employees been screened for fitness of role (i.e. pre-employment screening)? 7.3 Are manager and workers/employees aware of the rehabilitation process and return to work program? Element 7: Health and Wellbeing Management Yes Response No Response Partial Response # of Yes % # of No % # of Partial / / / / / / / / / Total for the Element / / / % Notes/Comments: Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 22 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 105
106 Auditing A Safe Way of Working (SWoW) Management System 3.2 Health & Safety Wellbeing Management System Audit Guide Questions 8.1 Does all equipment (e.g., clinical equipment and non-clinical equipment such as heaters, electrical appliances, motor vehicles etc) have maintenance schedule attached (i.e., tagged)? Element 8: Plant, Machinery and Equipment Management Yes Response No Response Partial Response # of Yes % # of No % # of Partial / / / 8.2 Do workers/staff know how to report faulty equipment? / / / 8.3 Are workers/staff aware on the need to visually inspect / / / equipment prior to use? 8.4 Is Personal Protective Equipment (PPE) used when required? / / / 8.5 Does all equipment have an asset number? / / / Total for the Element / / / % Notes/Comments: Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 23 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 106
107 Auditing A Safe Way of Working (SWoW) Management System 3.2 Health & Safety Wellbeing Management System Audit Element 9: Procurement and Purchasing Management Yes Response No Response Partial Response Guide Questions # of # of Yes % # of No % Partial % 9.1 Are area workers/staff consulted prior to purchasing equipment / / / or new products? 9.2 Is there a training programme for new equipment/products prior / / / to their use? Total for the Element / / / Notes/Comments: Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 24 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 107
108 Auditing A Safe Way of Working (SWoW) Management System 3.2 Health & Safety Wellbeing Management System Audit Element 10: Notifiable Event, Incident and Near Miss Management Yes Response No Response Partial Response Guide Questions # of # of Yes % # of No % Partial % 10.1 Have manager(s) been trained in incident and accident / / / investigation (e.g. received training from Quality Service)? 10.2 Are reports on worker/employee accidents/incidents reported / / / back to workers/staff working in the area or department? 10.3 Are workers/staff aware of the correct procedure for reporting an / / / incident at work? 10.4 Do managers investigations include corrective/preventative / / / actions? Total for the Element / / / Notes/Comments: Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 25 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 108
109 Auditing A Safe Way of Working (SWoW) Management System 3.2 Health & Safety Wellbeing Management System Audit Element 11: Worker, Patient, Visitor and Public Safety and Security Management Yes Response No Response Partial Response Guide Questions # of # of Yes % # of No % % Partial 11.1 Are local hazards clearly identifiable to non WDHB employees? / / / 11.2 Are there records kept showing orientation to your department for students, volunteers, other groups? 11.3 Do workers/staff record every incident of verbal and physical aggression? / / / / / / Total for the Element / / / Notes/Comments: Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 26 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 109
110 Auditing A Safe Way of Working (SWoW) Management System 3.2 Health & Safety Wellbeing Management System Audit Guide Questions 12.1 Are there safe operating procedures (SOPs) or safe working procedures (SWP) in the work area and are they available to the workers/staff? Element 12: Work Method and Procedures Management Yes Response No Response Partial Response # of Yes % # of No % # of Partial / / / Total for the Element / / / % Notes/Comments: Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 27 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 110
111 Auditing A Safe Way of Working Management System 3.2 Health & Safety Wellbeing Management System Audit Table B-1. Summary of % compliance for each element. SWOW Element Element 1 - Policy, Objectives & Organisational Responsibility Overall Percentage of Yes Response Element 2 - Employee Participation Element 3 - Design, Construction, Maintenance and Renovation (Contractor Management) Element 4 - Emergency Planning and Readiness Element 5 - Hazard Management and Risk Assessment Element 6 - Hazardous Substance Management Element 7 - Health and Wellbeing Management Element 8 - Plant, Machinery and Equipment Management Element 9 - Procurement and Purchasing Management Element 10 - Notifiable Event, Incident and Near Miss Management Element 11 - Worker, Patient, Visitor and Public Safety and Security Management Element 12 - Work Method and Procedures Management Issued by Group Manager, Occupational Issued Date January 2017 Classification Class # Health & Safety Authorised by Director of Human Resources Review Period 24mnths Page Page 28 of 28 This information is correct at date of issue. Always check on Waitemata DHB Controlled Documents site that this is the most recent version. 111
112 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS * Score : 0 Non No process, system or structure as required to meet the Resource Assessment Criteria 1 Partial Process, system or structure but no supporting documentation as required 2 Partial Documented process, system and structure but no evidence to show implemented 3 Partial Documented process, system or structure implemented but not fully applied 4 Partial Documented and implemented process, system or structure 5 Full Process, system or structure with an internal self-monitoring Process by (I) (A) (A) N/A Not applicable Element 1 : Health and Safety Management Systems Recommendation Proposed Action Who Timeframe 1.1 Health and Develop an Audit Standard / Audit Tool directly from the Agree develop as a leading OH&SS and Safety Policy Health, Safety and Wellbeing Policy so that it can be used to Audit and measure the DHB s Service Area, Department and Workplace location commitment and application indicator Director of HR Sept Health and Safety Management System 1.3 Health and Safety Business Plans After the next annual review of the Safe Way of Working get all the Service Area Managers to sign off to approve their support of the Health and Safety Management System - and - present it to the Executive Management Team for their approval. This approved Health and Safety Management System can then be presented to the Board of Directors as the confirmed Waitemata DHB s Health and Safety Management System It is recommended that each Service Area implement annual Health and Safety Business KPI s for their Service Area to drive and support their commitment of the Health and Safety Policy and the Safe Way of Working Agree but we will co-design SWOW. For review 2017/18 16/17 update for new legislation complete SWOW to be reviewed externally as part of 17/18 review. Agree element KPIs to be part of service H&S meeting GM to sponsor these meetings OH&SS HS&W Committee OH&SS and Director of HR 2017/18 Oct 2016 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page 1 112
113 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Once developed the Service Area Business KPIs can be coordinated and collated to form a Waitemata DHB Health and Safety Business Plan. This collated Waitemata DHB Health and Safety Business Plan could then be assessed for resourcing and submitted to the Board of Directors as the Waitemata DHB s annual Health and Safety Business Plan Occupational Health and Safety Department work with service areas (as is in the past) to help them develop their Health and Safety KPIs and priority areas to be achieved. Occupational Health and Safety Department work with service areas and the Executive Management Team to help them coordinate and develop a Waitemata Health and Safety Business Plan and the priority areas to be achieved. Agree a health and safety strategy is a priority for the Health, Safety and Wellbeing committee Complete for 16/17 in SWOW Work with Service Managers on a system for reporting KPIs (Template) Interim plan complete final to be developed with HS&W committee HS&W Committee Dec 2016 OH&SS and Director of HR Oct 2016 OH&SS and Director of HR Dec Health and Safety Corrective Actions Develop a corrective action/improvement process/noncompliance standard protocol so that regardless of where the corrective action is generated from each correction action receives the same attention until sign off. This standard protocol will ensure a DHB consistency across the Divisions, Service Areas and Workplace locations. Process exists but should be reviewed. Develop a training programme for Managers. This includes investigation training plus changes to Riskpro system to allow data capture and preventions to closing incident until actions complete. Investigation process deep dive planned for 16/17 via Quality/Group Manager OH&SS Dec 2016 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page 2 113
114 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 1.5 Health and Safety Compliance Programme 1.6 Health and Safety Reporting No recommendation It is recommended that Health and Safety Management System reporting be further developed to include detailed Lead Indicator reporting from the Service Areas initially and then collectively to provide detailed Governance Responsibility information to the Board of Directors Internal audit Agreed. To develop a 14 element SWOW lead indicator template starting with HSNO OH&S Group Manager and Director of HR Complete (HSNO) Jun 2017 (SWOW) 1.7 Health and Safety Committees 1.8 Health and Safety Process Methods It is recommended that the Board of Directors consider initiating their own Health and Safety Sub Committee or Health and Safety Governance Committee to address and focus on Waitemata s Health and Safety Management No recommendation Complete We have a Health, Safety & Wellbeing governance committee. A patient harm subcommittee is in place. Board to see all H&S papers. G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page 3 114
115 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 1.9 Process and Procedures include Safe Moving and Handling The following detail may be used to summarise the impact of staff moving and handling injuries, near misses and incidents within the DHB. Information to be considered: Lagging indicators Number and cost of lost time staff injuries related to moving and handling.(m&h) Number of light duty restrictions for staff due to M&H Percentage M&H injuries compared to all other injuries to staff Number and cost of short and long-term disability claims related to M&H Agree review and advise measures for service and Board reporting Moving & Handling Consultant (M&HC) Sep 2016 Patient injury and incidents related to M&H Leading indicators Corrective actions put in place as a result of 1. Incident report investigation 2. Staff requests including educator team 3. Progress in technology and/or education Practice development via professional development and organisational service development G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page 4 115
116 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Attendance of M&H mandatory training within acceptable and documented timeframes 1.10 Health and Safety Document Control Service user feedback both staff and patients Include direct legislation and Ministry of Health minimum standards within the new document template The Occupational Health and Safety Department need to write a brief of their document control process to ensure a consistency is applied and used. Complete Complete Element 1: Health and Safety Systems Element Score 3 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page 5 116
117 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 2 : People Engagement, Development and Leadership 2.1 Training and Training Records (Special Project) 2.2 Health and Safety Training Modules to Complement Responsibilities Recommendation Proposed Action Who Timeframe Conduct a Training Regime Review against the legal 1. Review of all Board, Director of HR and the WDHB assigned Health and Safety SMT and worker Nov 2016 Responsibilities and identify the commensurate training underway with Training Modules required to be presented so that H&S and L&D personnel can fulfil their delegated responsibilities. 2. Review of H&S rep This requires a documented reporting process. training also underway with H&S modules being updated and transition training complete 3. HSNO handler training in place 4. Mandatory H&S orientation n place. 5. Facilities Project manager training for KPIs in place Develop and Present commensurate training that Same as 2.1 OH&SS aligns with assigned health and safety responsibilities Oct 2016 and the Safe Way of Working for Management and Up skilling of Health and Safety Representatives Incident Investigation Training The importance of Incident Reporting Auditor / Assessment Training G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page 6 117
118 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Safety Committee Training Hazardous Substances / Chemical Management Training Hazardous Substances / Chemical Handling Training Contractor Management Training Hazard and Risk Management Training Developing Safe Work Practices Health and Wellbeing Training 2.3 Health and Safety Induction/Orientation (Special Project) It is recommended that the WDHB conduct a review of the current Induction/Orientation Programme standard of content considering what information new and transferring personnel need considering:- WDHB specific information Division specific information Service Area specific information Department specific information Workplace specific information and Job Role / Responsibility specific information Organisational orientation project to be assigned to Occ health Nurse. New on line orientation complete Induction checklist in place. Orientation for student placements will be reviewed as part of the above project with the profession leads and those responsible for all Clinical Training. Director of HR OH&SS scoping underway Jocelyn Peach/Tamzin Brott/Director Clinical Training(Drs) Start in Oct 2016 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page 7 118
119 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Develop a standard of content for Waitemata DHB Inductions and Orientation so that regardless of the Service Area, Department or Workplace location personnel are getting the same message, content and local workplace related information. Induction checklist complete as above we ll review service orientation to enhance organisational orientation processes OH&SS Start in Oct 2016 It is recommended that an Induction / Orientation content review is conducted annually and that Service Areas ensure Inductions standards are maintained and all inductions are recorded Agreed. Recording of orientation to be discussed with L&D Service Managers OH&SS Annual It is recommended that the Induction / Orientation recording is reviewed across the DHB to ensure one standard is applied for recording induction / orientation training and all records are retrievable Agreed see 2.3 OH&SS with Area Managers and Service Managers Start in Oct 2016 Develop a self-managed induction / orientation programme template with sign off for use when inducting Line Management and Senior Management personnel Complete OH&SS Complete G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page 8 119
120 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 2.4 Health and Safety Training It is recommended Service Areas develop and resource a collective annual Health and Safety Training Plan for their collective departments and or workplace location personnel who hold Health and Safety Responsibilities on behalf of the WDHB Agree See 2.1 and 2.2 Service / Departmental Managers Nov 2016 Collate the Service Area Health and Safety Training Plans to develop and resource a Waitemata DHB Health and Safety Training Plan It is recommended that the WDHB initiate a process to provide assurance as an Employer that Employee Induction / Orientation is happening for a new or transferring Employee. The Induction / Orientation should happen at all levels Corporate, Service Area, Department and Workplace location and then recorded upon completion Not agreed as suggested but training action as per 2.1 Agree - See 2.3 Learning & Development/OH&SS Nov WDHB Mandatory Training and Training Records Identify the risk to the DHB for core training competency information not being recorded correctly and available Complete Learning & Development August 2016 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page 9 120
121 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 2.6 Health and Safety Responsibilities Special Note - Pike River Royal Commission finding - Recommendation seven (7) states as follows:- Recommendation 7: Directors should rigorously review and monitor their organisation s compliance with health and safety law and best practice With the proposed Health and Safety Legislation (Reform Bill) it will be important to ensure that Health and Safety Responsibilities are developed for the Board of Directors and the Chief Executive. It will then be important to cascade the Health and Safety responsibilities through the varying levels of management. The responsibilities will also need to consider the health and safety commitment included within the DHB s Health and Safety Policy With the implementation of detailed Health and Safety responsibilities Key Performance Indicators or Key Result Areas can be established as part of the Health and Safety Management System Performance Management Process Board Charter complete Policy notes responsibilities of managers and officers and workers KPIs established for each element and now need to align with Performance Appraisals and position descriptions (latter is complete) Governance audit complete and planned to redo in 17/18 Key Result area have been updated to reflect new legislation and authorised by the Board. Communication complete Service Managers/OH&SS service OH&SS & Director of HR Internal audit HR and OH&SS G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
122 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 2.7 Employee Skill/Competency Matrices I would strongly suggest that Service Areas and Departments assess the potential use of skill matrices per employee to record job related information, instruction, training, competency and skill achievements Develop a Skill / Competency Matrix Framework and introductory programme for use and application across the DHB Service Areas and Departments Not agreed but complete for OH&SS As above Element 2: People Engagement, Development and Leadership Score 3 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
123 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 3 : Hazard and Risk Management Recommendation Proposed Action Who Timeframe 3.1 Safety Critical No recommendation Element Hazard and Risk Management 3.2 Hazard and Risk No recommendation Management jointly managed 3.3 New Hazard and Risk No recommendation Management Process 3.4 Safe Way of Working All related documents for this Element need to be collated Agreed position HR and OH&SS Responsibilities, Key Result Areas and Job, Position Description Correlation to provide an alignment with the Safe Way of Working Element Hazard Management and Risk Management Associated responsibilities, key performance indicators and job position description contents need to be aligned description statement updated. KPIs as per 1.3 and 2.6 Oct Hazard and Risk Management Lead Indicator It is recommended that Hazard and Risk Management be introduced as a Management Lead Indicator within each Service Area. (Lead Indicator reference detail in the Executive Summary of Findings page 8) The Lead Indicator can then be reported on by the Service Areas to the Executive Management Team to review prior to collectively collating them for an overall status report to the Board of Directors. This enables the Executive Management Team and the Board to monitor the lead indicator as part of their Governance responsibility Agreed hazard management will be one of the lead indicators. See actions 1.6. OH&SS and Director HR Complete (HSNO) Jun 2017 (SWOW) G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
124 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 3.6 Hazard and Risk Management Safe Way of Working Audit Develop the Safe Way of Working element audit for Hazard and Risk Management so that it is more definitive in detail so that it actually audits (with verification) the following sub elements:- Procedure - implementation, application and use across the Service Areas, Departments and Workplace locations Training Instruction and Competencies - relevant to the element Responsibilities, Accountabilities and Authorities - relevant to the element Add a column to the Hazard Risk Register to record any related type of incident to the relevant hazard whether Patient related or Staff related to gauge the Hazard Management / Risk controls in place. This also provides a process to cross reference the hazard risk register and potentially identify newly identified hazards from an incident The Service Area Team Management Meetings review and sign off (minimum six monthly) their Service Area and Department Hazard/Risk Registers Develop standard Hazard and Risk Register Review process to ensure a consistency is applied across the DHB. Develop Hazard and Risk Management Training to be an annual and ongoing safety critical programme to ensure consistent application and use across the DHB See actions in 1.6 System not currently able to add new functionality. Future capability being assessed On line register has a 12 month auto review process. Complete survey mgrs. on application, review and follow up to identify issues See 2.1 OH&SS OH&SS and Quality Department/Service Managers/OH&SS Department/Service Mangers /OH&SS OH&SS Complete (HSNO) Jun 2017 (SWOW) 2016/17 Complete Complete Oct 2016 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
125 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Once each Department updates their Hazard/Risk Registers to include residual risk it will be important to re-assess the health and safety checklists to ensure they monitor the hazard and risk registers documented controls NB: Work Fatigue and Stressors were mentioned many times during the Resource Assessment discussions with varying controls and levels of concern This important Area should be assessed DHB wide across all the Service Areas and Workplace locations and a Project approach applied to address this Hazard and its associated risks, controls and residual risk to the DHB. Complete-We have a review process: The electronic hazard management system has a built in review process that turns an overdue task from red to green and managers and H&S representatives get an to tell them that a review is due.. The OH&S system coordinator will get a monthly report from Quality Hub to make sure hazards are being reviewed on time. A work stream in the Healthy Workplaces Strategy will review this concern but in some instances areas will have mitigations as part of the hazard management system. OH&SS Complete Healthy Workplaces Steering Group Element 3: Hazard and Risk Management Score 3 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
126 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 4 : Injury Prevention and Incident Management Recommendation Proposed Action Who Timeframe 4.1 Safety Critical Develop an Audit Standard / Audit Tool directly from the OH&SS Element Injury Prevention and Incident Management Employee Incidents at Work so that it can be used to Audit and measure the DHB Service Areas responsibility for commitment, application and use of the document and provide a Governance Assurance of the process Complete (HSNO) 4.2 Patient and Staff Incidents Develop an Audit Standard / Audit Tool directly from the Reportable Events Management so that it can be used to Audit and measure the DHB Service Areas responsibility for commitment, application and use of the document and provide a Governance Assurance of the process Incident Management Exercise Identify the last 3 months of patient incidents and staff incidents. Select 10 incidents from each (patient incidents and staff incidents) and assess:- Was each incident investigated Were corrective actions initiated from each incidents investigation Were corrective actions followed through to completion and signed off Were the incidents contributing hazards identified Employee work related events are already measured in the Boarded reported scorecard. Other actions as per 1.6 Agree A collaborative process will be formulated. OH&SS will identify one worker incident per week to assess required actions were implemented Quality OH&SS in collaboration with Quality Jun 2017 (SWOW) TBA Dec 2016 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
127 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Were the incidents contributing hazard / risks cross reference with the existing hazard / risk register controls Did the investigation identify process or procedure changes Was the investigation formally signed off / closed out The above will provide assurance that the following has occurred Identify causative hazard Manage the hazard to prevent recurrence Communicate actions to Employee Document actions on current online incident reporting system Develop a stringent staff incident profile and assessment process to measure a reported incident and its potential 4.3 Develop a promotion across the Service Areas, Departments and Workplace locations and through the Safety committees regarding the importance, value and responsibility of reporting all type incidents If the above is carried out this will automatically happen and identify near misses. Complete OH&SS Complete G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
128 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 4.4 Incident Corrective Actions Same as 1.4 Develop a Corrective Action/Improvement Process/Non Compliance standard. Agreed. Standard to be added to SWOW Quality/OH&SS Mar Incident Management Responsibility General Managers of Service Areas need to review the Service Area responsibilities they hold on behalf of the Waitemata DHB for managing and monitoring incidents Develop a formal Incident Investigation Training Module with a process that follows the DHB s Incident Management documents. This should be developed and presented as paramount to personnel with an Incident Management and an Investigation responsibility Agree: KPI to support this and includes the investigation and corrective action monitoring of incidents. Action as per 1.3 and 2.6. Agreed as per 2.1 Department/Service managers Oct 2016 OH&SS/Quality Oct 2016 The DHB should consider developing an internal Safety Alert process whereby any incident that has occurred and has the potential of occurrence within another Service Area are notified Agreed: This already happens as part of the OH&SS review of hazard registered but there needs to be a more formal system to alert other areas of the risk. OH&SS with Quality Dec Facilities and Contractor Reporting Contractor reporting of incidents should be spelled out in the Contracts Health and Safety Service Agreement or the specific Contract Responsibility document linked to all type Contracts Agreed: systems are being upgraded to include capability assessments and preferred contract Facilities/OH&SS Oct 2016 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
129 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 4.7 Detailed Review of Statistical Information Safe Way of 4.8 Working Responsibilities Key Result Areas and Job Position Description Correlation 4.9 Incident Management Lead Indicator No recommendation All related documents for this Element need to be collated to provide an alignment with the Safe Way of Working Element Incident Management Associated responsibilities, key performance indicators and job position description contents need to be aligned It is recommended that Incident Management be introduced as a Management Lead Indicator within each Service Area. (Lead Indicator reference detail in the Executive Summary of Findings page 8) The Lead Indicator can then be reported on by the Service Areas to the Executive Management Team to review prior to collectively collating them for an overall status report to the Board of Directors. This enables the Executive Management Team and the Board to monitor the lead indicator as part of their Governance responsibility providers Agreed position description statement updated. KPIs as per 1.3 and 2.6 Agreed as per 4.1 HR/OH&SS OH&SS Oct 2016 Complete (HSNO) Jun 2017 (SWOW) G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
130 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 4.10 Incident Management Safe Way of Working Audit Develop the Safe Way of Working element audit for Incident Management so that it is more definitive in detail so that it actually audits (with verification) the following sub elements:- As per 2.1 and 4.1 OH&SS Oct Incident Management High Potential Incidents Procedure - implementation, application and use across the Service Areas Departments and Workplace locations Training Instruction and Competencies - relevant to the element Responsibilities, Accountabilities and Authorities - relevant to the element High Potential Incidents for staff and patients be reported to and assessed by the Executive Management Team and then reported to the Board of Directors Complete Complete 4.12 Incident Management Health and Safety Training Incident Investigations outcomes / corrective actions be collectively assessed by the Occupational Health and Safety Department for the development of ongoing Health and Safety Training Complete Complete G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
131 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 4.13 Incident Management Incident Trends Incident Trends be assessed by the Occupational Health and Safety Department to initiate Projects to improve the Health and Safety Management System Complete: The SWOW planning by the OH&S team identifies projects to improve the H&S management system annually and reviewed regularly. Complete Element 4: Injury Prevention and Incident Management Score 3 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
132 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 5 : Emergency Response Planning and Management Recommendation Proposed Action Who Timeframe 5.1 Safety Critical No recommendation Element Emergency Response Planning and Management 5.2 Emergency Response No Recommendation Planning and Training 5.3 Potential Emergency Assessment Complete When the Hazard Risk Registers are populated for the Workplaces, Departments and Service Areas they should be assessed in detail as planned to identify any further potential DHB emergencies Complete OH&SS do this assessment as part of regular hazard register reviews 5.4 Emergency Risk Response Assessment 5.5 Emergency Risk Response 5.6 Emergency Plans Escalation and Communication 5.7 Emergency Response Plan Testing No recommendation No Recommendation No Recommendation Develop from the Waitemata DHB extensive district wide Emergency Response Plans a rolling schedule of specific isolated sites and workplace locations and conduct walk through evacuation exercises Complete-Plans are in place. Complete 5.8 Emergency Response Plan Review No Recommendation G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
133 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 5.9 Emergency Response Equipment Readiness 5.10 Emergency Response First Aid Response 5.11 Safe Way of Working Responsibilities Key Result Areas and Job Position Description Correlation 5.12 Emergency Response Planning and Management Lead Indicator No Recommendation Ensure non inpatient departments and Workplace locations have trained and certified first aiders as well as back up personnel and first aid kits Include in the Safe Way of Working Audit a questioning process to assess and verify Certified First Aid Response Trained personnel and back up and first aid kits available All related documents for this Element need to be collated to provide an alignment with the Safe Way of Working Element Emergency Response Planning and Management Associated responsibilities, key performance indicators and job position description contents need to be aligned It is recommended that Emergency Response Planning and Management be introduced as a Management Lead Indicator within each Service Area. (Lead Indicator reference detail in the Executive Summary of Findings page 8) The Lead Indicator can then be reported on by the Service Areas to the Executive Management Team to review prior to collectively collating them for an overall status report to the Board of Directors. This enables the Executive Management Team and the Board to monitor the lead indicator as part of their Governance responsibility. Partial. All offsite areas are advised re having a First Aider on site. Compliance needs to be captured. Agreed Agreed position description statement updated. KPIs as per 1.3 and 2.6 Agreed Actions as per 1.6 OH&SS as part of system audit. OH&SS Oct 2016 Oct 2016 HR and OH&SS Oct 2016 Jocelyn Peach / OH&SS Complete (HSNO) Jun 2017 (SWOW) G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
134 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 5.13 Emergency Response Planning and Management Safe Way of Working Audit Develop the Safe Way of Working element audit for Emergency Response Planning and Management so that it is more definitive in detail so that it actually audits (with verification) the following sub elements:- Procedure - implementation, application and use across the Service Areas, Departments and Workplace locations Training Instruction and Competencies - relevant to the element Responsibilities, Accountabilities and Authorities - relevant to the element Agree as per 1.6 and 2.1 Jocelyn Peach / OH&SS Dec 2016 Element 5: Emergency Response Planning and Management Score 4 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
135 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 6: Contractors and Suppliers Management Recommendation Proposed Action Who Timeframe 6.1 Safety Critical The New Task Force Report - No Recommendation Element Contractors and Suppliers Management 6.2 Contractor A detailed assessment to identify the many types of Complete involvement at the Waitemata DHB contracts and then associated contractors and subcontractors selected to fulfil the many and diversified WDHB contracts. Complete 6.3 DHB Contractor Management No Recommendation 6.4 Contractor Set Up Waitemata District Health Board requires one Management System that can be used for:- Contractors and all levels of Sub Contractor being involved with Projects Contractors involved with the Servicing of Clinical Equipment Contractors involved with Facilities Maintenance Contractors involved with the Servicing of the DHB s Security System Maintenance The system to include:- Contractor Pre-qualification / Registration / Requalification Contractor Selection Contractor Engagement Contractor Performance Management Agreed to complete one management system for contractors Facilities / OH&SS May 2017 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
136 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 6.5 DHB Contractor Podium Project 6.6 Contractor Capability Assessment Questionnaire Contract and Contractor review at pre-determined intervals during the Contract It is recommended that a step by step start-up process be developed, implemented, applied and used across the DHB Service Areas, Departments and Workplace locations to commence the Management of Contractors. No Recommendation Waitemata DHB should consider developing a Health and Safety Contractor Capability Assessment Questionnaire. A Contractor Capability Assessment Questionnaire requires a Contractor to answer pre-determined Health and Safety Management questions (relevant and contract specific) to sell their capability, to complete the contracts scope of work and at the same time sell their capability to manage any and all associated scope of work Health and Safety As per above Complete Complete The questionnaire should focus initially on the Contractors Management of the 5 safety critical Health and Safety Management Elements namely:- Hazard and Risk Management Incident / Accident Management Emergency Planning and Response Management Sub-Contractor Management of all levels of Sub Contracting Safe Work Practices G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
137 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS In the case of the Hazard and Risk Management safety critical element the Lead Contractor will be required to provide a Hazard and Risk Register for the Project Site that includes the Contracts related scope of work hazards. Currently Facilities are doing this until the system is mature enough for contractors to do their own. Larger contractors e.g. Fletchers already have this in place. Facilities & Development / OH&SS for non- Facilities contractors. Dec 2016 This will be required to be signed by the Contractors CEO and included within the Contractors Tender document so that it can be assessed and verified during the Tender selection process Not agreed. Hazards to be dynamically assessed by the project/works leads. Facilities Dec 2016 As the Contract Progresses the Hazard and Risk Register will progress to align and manage the changing Hazards and Risks on site Waitemata DHB develop a formal Contractor Induction and recording process for all type Contractors used within the Service Areas, Departments and Workplace locations (Facilities have a detailed Induction Programme) Complete Agreed. This project is part of the OH&S SWOW planning process for non- Facilities contractors. Facilities-in process of development. Orientation for Facilities contractors exists OH&SS Facilities and OH&S and Infection Control Nov 2016 Orientation: PowerPoint Aug 2016 On-line 2017 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
138 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 6.7 Contract Health and Safety Audits The WDHB assess Insurance/Liability coverage required from Contractors to cover a Contractors scope of work liabilities The Capability Assessment Questionnaire completed by the Contractor is to be also used for Contract related Audits and Contract / Contractor review meetings This is checked for all Facilities contractors but process with h/alliance still to be checked. A regional project has been started to address this as part of the process of contractor engagement for all DHB s Complete-Internal audits are done randomly by project managers. Complete Regional OH&SS/hAlliance Dec 2016 Complete The Contractors Site Specific Safety Plan must be project specific and must be accompanied with its own Audit Standard / Audit Tool that has been written directly from the plan. Contractor Responsibilities must be defined within the Site Specific Safety Plan Site Specific plans are not done in NZ (Australian) The Contractor will provide (to be mutually agreed) an Audit Calendar/Schedule for the Project that states the frequency of the Safety Plan Audit and who will conduct the Audits (internally and externally) on behalf of the Contractor and confirm that a copy of the full audit, audit report and recommendations will be provided to the Waitemata DHB. G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
139 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Confirmation will also be required from the Contractor that the Waitemata DHB may / will conduct a verification audit at their discretion External audits also being done. 6.8 Contractor Health and Safety Specifications 6.9 Contractor Permit to Work Each Audit conducted by the Contractor will include an Improvement Plan (if deficiencies are detected) and be presented to the DHB on-site Project Meetings for further discussion and the monitoring of the Improvement Plans Review and develop Waitemata DHB Health and Safety specifications for inclusion within Tender Specifications and Contract documents. Contractors who visit DHB sites for contract related works should require a signed Permit to Work prior to the commencement of their job as a result of consultation with the Head of the relevant Department and the person coordinating the Contractors scope of work Audits presently being done by Waitemata DHB Apart from the larger contractors e.g. Fletchers. In the future when the system is more mature all contractors will be guided to do their own audits which Waitemata will oversee. Complete Complete Complete Complete G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
140 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 6.10 Waitemata Property Management Leased Buildings An engagement and consultation of Services (master list) is required for the WDHB refurbishment, refit prior to occupancy for Leased Buildings that considers collaboration involvement This to include for example:- Complete part of refurbishment design and fit out process Compete Infection Control Security Warrant of Fitness Fire Equipment Inspection Emergency Plan Occupational Health Movements and Handling Traffic Fleet and Pedestrian Ergonomics 6.11 Safe Way of Working Responsibilities Key Result Areas and Job Position Description Correlation 6.12 Contractors and Suppliers Management Lead Indicator All related documents for this Element need to be collated to provide an alignment with the Safe Way of Working Element Contractors and Suppliers Management Associated responsibilities, key performance indicators and job position description contents need to be aligned It is recommended that Contractors and Suppliers Management be introduced as a Management Lead Indicator within each Service Area. (Lead Indicator reference detail in the Executive Summary of Findings page 8) Agreed position description statement updated. KPIs as per 1.3 and 2.6 Actions as per 1.6 and 2.1. OH&SS with Facilities and Development OHS&S Oct 2016 Complete (HSNO) Jun 2017 (SWOW) G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
141 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS The Lead Indicator can then be reported on by the Service Areas to the Executive Management Team to review prior to collectively collating them for an overall status report to the Board of Directors. This enables the Executive Management Team and the Board to monitor the lead indicator as part of their Governance responsibility 6.13 Contractors and Suppliers Management Safe Way of Working Audit Develop the Safe Way of Working element audit for Hazard and Risk Management so that it is more definitive in detail so that it actually audits (with verification) the following sub elements:- Procedure - implementation, application and use across the Service Areas, Departments and Workplace locations Training Instruction and Competencies - relevant to the element Responsibilities, Accountabilities and Authorities - relevant to the element Actions as per 6.12 OH&SS with Facilities and Development Mar Contractor Management It is recommended that the DHB conduct a detailed assessment to identify the many types of Contracts and then associated Contractors and Sub Contractor selected to fulfil the many and diversified WDHB Contracts Refer 6.4 OH&SS/Facilities May 2017 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
142 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Assess the WDHB Contactors and Sub Contractors that have been selected and engaged by the DHB that have and have not been subject to the WDHB Contractor Management Process. Agree all contractors on a PO will have general terms and conditions in place. OH&SS/Facilities Nov 2016 Element 6: Contractors and Supply Management Score 2 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
143 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 7: Infection Prevention and Control 7.1 Infection Prevention and Control Service Programme Recommendation Proposed Action Who Timeframe Develop an Audit Standard / Audit Tool directly from the As per 1.6 and 2.1. Infection Prevention and Control related policies so they can Mar 2017 be used to Audit and measure the DHB s Infection Prevention and Control commitment, application and use across identified areas of the WDHB 7.2 Infection Prevention and Control Management System Framework 7.3 Infection Prevention and Control Skill Matrix 7.4 Infection Prevention and Control Hazard and Risk Management Process No Recommendation No Recommendation I would recommend that an extra column be added to the end of the Risk Register that records any related incident per risk. This information can then be used to assess trends and review / assess if the applied treatment actions and control information was applied and used Disagree: This information can be obtained via Medtech currently. Adding another column to the hazard register will be labour intensive and will not add value. Element 7: Infection, Prevention and Control Score 4 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
144 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 8: Hazardous Materials and Substances 8.1 Hazardous Materials and Substances Management 8.2 Hazardous Materials and Substances Management Risk Process Recommendation Proposed Action Who Timeframe No Recommendation Ensure that with the implementation of the Hazardous Substances Process a Service Area, Department and Workplace location consistency is applied and used. Include a maintenance and monitoring process programme to provide a governance assurance responsibility that the consistent approach is continually applied and used across the DHB. This will ensure the process becomes embedded within the Waitemata DHB Health and Safety Management System the Safe Way of Working Complete and being rolled out HSNO Co-ordinator / EPMG Jul 2017 As the project progresses assess the potential staff risk exposures per Service Area, department or workplace location per person considering surveillance monitoring and any additional first aid consumables beyond the standard first aid kit contents from the Safety Data Sheet Agree. The Health Monitoring role will develop this process OH&SS (Special Role) Apr Hazardous Materials and Substances Project Management No Recommendation G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
145 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 8.4 Chemical Procurement / Purchasing Process 8.5 Hazardous Materials and Substances Safe Use Training No Recommendation Develop Hazardous Substances Training and information for this element for personnel who have varied levels of responsibility for this element for example Service Areas Managers, general Staff Inductions, Health and Safety Representatives, Safety Committee Members etc. Complete and see actions as per 2.1 Investigate potential accredited training related to hazardous substances HSNO Co-ordinator / EPMG HSNO Co-ordinator Mar Hazardous Materials and Substances Disposal 8.7 Safe Way of Working Responsibilities Key Result Areas and Job Position Description Correlation No Recommendation All related documents for this Element need to be collated to provide an alignment with the Safe Way of Working Element Hazardous Materials and Substances Associated responsibilities, key performance indicators and job position description contents need to be aligned Agreed position description statement updated. KPIs as per 1.3 and 2.6 HR and OH&SS Oct Hazardous Materials and Substances Lead Indicator It is recommended that Hazardous Materials and Substances be introduced as a Management Lead Indicator within each Service Area. (Lead Indicator reference detail in the Executive Summary of Findings page 8) Agree- actions as per 1.6 and 2.1 OH&SS/EPMG/HSNO Co-ordinator Complete (HSNO) Jun 2017 (SWOW) G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
146 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS The Lead Indicator can then be reported on by the Service Areas to the Executive Management Team to review prior to collectively collating them for an overall status report to the Board of Directors. This enables the Executive Management Team and the Board to monitor the lead indicator as part of their Governance responsibility 8.9 Hazardous Materials and Substances Safe Way of Working Audit Develop the Safe Way of Working element audit for Hazardous Materials and Substances so that it is more definitive in detail so that it actually audits (with verification) the following sub elements:- Procedure - implementation, application and use across the Service Areas, Departments and Workplace locations Training Instruction and Competencies - relevant to the element Responsibilities, Accountabilities and Authorities - relevant to the element Develop a Hazard Substances Risk Register to record any and all Hazardous Substances using the new Hazard and Risk Management template. The Hazardous Substances Management Policy when completed be developed into an Audit Tool/Standard and applied and used as an internal audit process Complete Complete Agree. HSNO Coordinator to develop the internal audit process (class 9 s) Complete Complete HSNO Co-Ordinator / EPMG Complete G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
147 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 8: Hazardous Materials and Substances Management Score 3 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
148 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 9: Safety of Facilities, Equipment and Associated Maintenance Recommendation Proposed Action Who Timeframe 9.1 Safety of Facilities Pre-qualify all Contractors using the Contractor Agree Health and Safety Capability Questionnaire recommended in Element 6. 1) GM Facilities as per 6.14 GM Facilities and Development May ) All other contracts OH&S 9.2 Safety of Clinical Equipment No Recommendation 9.3 Procurement of Safe Plant, Machinery and Clinical Equipment 9.4 Plant and Equipment Maintenance 9.5 Plant and Equipment Fault Reporting 9.6 Facilities and Clinical Engineering Hazard and Risk Register 9.7 Facilities and Clinical Engineering Hazardous Substances Register Develop a Capex assessment content that includes health and safety legislative requirements prior to sign off to complement the existing documented process. No Recommendation No Recommendation No Recommendation Develop a formal ladder register to ensure inspection checks are conducted to a set frequency. Agree. Procurement Form needs to include H&S requirements. Complete OH&SS with Capital Accountant (Chris Watson) Oct 2016 Complete Element 9: Safety of Facilities, Equipment and Associated Maintenance Score 3 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
149 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 10: Health, Security and Wellbeing 10.1 Health and Wellbeing 10.2 Pre-Employment Medical Screening 10.3 Wellbeing Programme Research 10.4 Wellbeing Programme 10.5 Employee Assistance Programme Recommendation Proposed Action Who Timeframe No Recommendation No Recommendation No Recommendation Develop a long term Wellbeing Programme for the DHB with at least a five year strategy. Include all previous one of short term campaigns for example Diet advice, Stop Smoking, and Fitness and the whole process of Medical Screening, Monitoring, Surveillance, Management Referrals and Exit Medicals No Recommendation Agree. Three year Healthy Workplaces Strategy is approved for OH&SS cover medical screening, monitoring & surveillance. HR: Manage Exit Interviews OH&SS/HR G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
150 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 10.6 Psychosocial Hazard Management Within the development of the long term Wellbeing Programme for the DHB include the development of a specific Psychosocial Hazard / Risk Register. The register can be used to identify and list the Psychosocial Hazards and assess their risks to the DHB. It can then be used to define and list the existing controls already in place and identify additional controls that can become part of the wellbeing programmes development. Use of the existing Hazard / Risk Management template will include the process of identifying the Residual Risk (the risk that still needs to be managed) whereby additional controls or secondary controls may need to be considered and developed Psychosocial hazard management needs to be included in the hazard management system across the DHB not just in some areas. Legislation requires these risks to be managed as any other risk. Investigation into how this can be improved across the organisation. OH&SS/All departmental and Service Managers Dec Employee Health Risk Exposure Identify relevant Employee Work Groups that initially may be at risk and conduct a formal Employee Health Hazard and Wellbeing / Risk Exposure Survey / Assessment Health Monitoring will be done with specific at risk workgroups OH&SS Mentoring All related documents for this Element need to be collated to provide an alignment with the Safe Way of Working Element Health and Wellbeing Associated responsibilities, key performance indicators and job position description contents need to be aligned Agreed position description statement updated. KPIs as per 1.3 and 2.6 HR and OH&SS Oct 2016 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
151 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 10.9 Health and Wellbeing Lead Indicator It is recommended that Health and Wellbeing be introduced as a Management Lead Indicator within each Service Area. (Lead Indicator reference detail in the Executive Summary of Findings page 8) The Lead Indicator can then be reported on by the Service Areas to the Executive Management Team to review prior to collectively collating them for an overall status report to the Board of Directors. This enables the Executive Management Team and the Board to monitor the lead indicator as part of their Governance responsibility Agree- actions as per 1.6 and 2.1 OH&SS /Director HR Complete (HSNO) Jun 2017 (SWOW) Health and Wellbeing Safe Way of Working Audit Develop the Safe Way of Working element audit for Health and Wellbeing so that it is more definitive in detail so that it actually audits (with verification) the following sub elements:- As per 10.9 Procedure - implementation, application and use across the Service Areas, Departments and Workplace locations Training Instruction and Competencies - relevant to the element Responsibilities, Accountabilities and Authorities - relevant to the element G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
152 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Security The Waitemata DHB Security Management Review Security Retail Areas and Cash Takings No Recommendation Assess the risk to patient / clients, staff, volunteers, visitors and public regarding cash management for retail cafes and pharmacies on Waitemata premises considering:- Complete new cash management and security processes in place Complete Security of cash on site Transfer of cash from sites Duress support Element 10: Health, Safety and Wellbeing Score 3 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
153 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 11: Inspections, Monitoring Checks and Audits 11.1 Inspections and Audits 11.2 Safe Way of Working Audits Recommendation Proposed Action Who Timeframe No Recommendation Develop the Safe Way of Working Audit per Element that it is more definitive in detail so that it actually audits (with verification) the following sub elements:- Agree- actions as per 1.6 and 2.1 OH&SS Complete (HSNO) Procedure - implementation, application and use across the Service Areas, Departments and Workplace locations Training Instruction and Competencies - relevant to the element Responsibilities, Accountabilities and Authorities - relevant to the element Jun 2017 (SWOW) Develop a DHB Audit Calendar that includes all Service Area Departments and Workplace locations to show the coverage and to record each audits completion. Audit completions could be reported regularly to the Board of Directors as Governance Assurance Agree. Will put in place a SWOW audit calendar OH&SS Dec 2016 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
154 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 11.3 Safe Way of Working Inspections Develop a Standard (Process / Protocol) with a start to finish loop for conducting Health and Safety Inspections across the DHB to ensure a consistency is applied across the Service Areas, Departments and Workplace locations Agree. Also action as per 1.4 OH&SS Mar 2017 When the new specific Workplace, Department and Service Area Hazard / Risk Registers are completed they can be used as the basis for the development of the workplace Self-Monitoring Inspection and Audit Programme. Agree action as per 11.2 and 11.3 OH&SS Mar 2017 This process will ensure the Register is cross referenced during the check and audit thereby providing a tight Layer of Protection. The frequency of checking will be based on a Hazards Residual Risk (the Risk that still need to be managed) Health and Safety Monitoring Checklists and Audits should have Service Area Management sign off or representation sign off to ensure they are completed as a Service Manager responsibility Agree and in conjunction with OH&SS Oct 2016 Element 11: Inspections, Monitoring Checks and Audits Score 3 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
155 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 12: Health and Safety Representatives 12.1 Health and Safety Representative Role Recommendation Proposed Action Who Timeframe No Recommendation 12.2 Health and Safety Representative Training Review the Health and Safety Representative Course Training Calendar so that recently elected or appointed Health and Safety Representatives can commence their training as soon as possible after their election or appointment Complete Complete 12.3 Health and Safety Representative Induction/Orientation Develop a standard (for consistency of use across the DHB) Health and Safety Representative Induction / Orientation Programme that can be used to support the Health and Safety Representative prior to and post training as a resource Agree will be reviewed as part of a special project allocated to the H&S specialised lead OH&SS Oct 2016 Ensure that it includes a self-managed induction process for the Service Area Department that requires involvement commitment and sign off by both Management and the Health and Safety Representative when completed G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
156 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 12.4 Health and Safety Representative Time allocation for the Role Assess the physical work load required of a Health and Safety Representatives to complete their assigned support responsibilities for health and safety in line with Participation Agreement and Waitemata DHB requirements Actions as per 12.3 OH&SS Department /Service Managers Oct 2016 Assess the resources required including the availability of computers and the level of computer skills required for a Health and Safety Representative to fulfil their responsibility role Action as per Health and Safety Representative Future Role (Special Project) Ensure that each Health and Safety Representative has the time available and the required computer skills to do the role of supporting the department Manager to achieve Waitemata s Health and Safety Management It is recommended that the Waitemata DHB conduct an across the board review of the Health and Safety Representative role, responsibility and involvement support to the WDHB Health and Safety Management System the Safe Way of Working. It should consider the DHB role requirements workload efficiencies, participation agreement requirements and the new reform bill requirements - Assess:- Managements responsibility to the Health and Safety Representative The number of Health and Safety Representatives needed across the DHB considering the DHB Health and Safety Management Structure The Health and Safety Representative As above Agree actions as per 12.3 OH&SS Oct 2016 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
157 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS representation / coverage needed for efficiencies to meet legislative and participation agreement requirements consider Service Area and Geographical locations Health and Safety Representative turnover in the last twelve months and reason for the turnover The need for a Health and Safety Representative Induction / Orientation Programme pre and post training The possibility of the Induction / Orientation being partly self-managed with Management and Health and Safety Representative sign off when the induction is completed Training Course frequency to meet the elected Health and Safety Representative needs The allocation of time required for a Health and Safety Representative to fulfil their responsibility and role What duties a Health and Safety Representative must do and may be delegated to do as part of their role and responsibility do they vary across Service Areas and Departments How a Health and Safety Representative handles a health and safety issue from a staff member in their work group The systems and processes that are currently used to and how they might be streamlined The Occupational Health and Safety Departments support role to the Health and Safety G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
158 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Representative and the actual frequency of contact and the type of support to be provided to build the Representative confidence for the role The potential of upskilling a Health and Safety Representative beyond HSR training and the skills and competencies required to assist the DHB considering the Safe Way of Working Elements To show the Waitemata DHB S commitment to the Employee Participation Agreement and to meet future legislative requirements under the new Health and Safety Reform Bill develop a pool of Health and Safety Representatives. The pool of Health and Safety Representatives could be involved in a consultation role within DHB Projects. Once the pool has been developed the DHB could promote their availability. Participation agreement in consultation with regional and union stakeholders. Also complete is the development of a higher level Health and Safety representative who can assist with decision making at the Health, Safety and Wellbeing Committee level. NZQA Training will be offered in house to these reps once all have volunteered to represent all services. Process to be confirmed and agreed in the Employee Participation Agreement. OH&SS Oct 2016 Element 12: Health and Safety Representatives 3 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
159 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Score Element 13: Health and Safety in Construction and Design 13.1 Health and Safety in Construction and Design Guidelines 13.2 Health and Safety in Construction and Design Processes Application and Use Recommendation Proposed Action Who Timeframe No Recommendation Document collaboration guides for Projects. This to include DHB Project Managers, DHB Health and Safety, Project Managers and Lead Contractors so that the Health and Safety Management System to be applied for the Project can be agreed up front prior to the projects commencement All related documents for this Element need to be collated to provide an alignment with the Safe Way of Working Element Health and Safety in Construction and Design Processes Complete Agreed position description statement updated. KPIs as per 1.3 and 2.6 OH&SS Complete Oct Health and Safety in Construction and Design Lead Indicator Associated responsibilities, key performance indicators and job position description contents need to be aligned It is recommended that Health and Safety in Construction and Design be introduced as a Management Lead Indicator within each applicable Service Area. (Lead Indicator reference detail in the Executive Summary of Findings page 8) Agree- actions as per 1.6 and 2.1 OH&SS/Director HR Complete (HSNO) Jun 2017 (SWOW) G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
160 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS 13.4 Health and Safety in Construction and Design Safe Way of Working Audit The Lead Indicator can then be reported on by the applicable Service Areas to the Executive Management Team to review prior to collectively collating them for an overall status report to the Board of Directors. This enables the Executive Management Team and the Board to monitor the lead indicator as part of their Governance responsibility Develop the Safe Way of Working element audit for Health and Safety in Construction and Design so that it is more definitive in detail so that it actually audits (with verification) the following sub elements:- Procedure - implementation, application and use across the Service Areas, Departments and Workplace locations Training Instruction and Competencies - relevant to the element Responsibilities, Accountabilities and Authorities - relevant to the element Agree actions as per 13.3 OH&SS Mar Health and Safety in Construction and Design Resource Requirements The Capital Projects Management Guidelines be developed into an Audit Standard / Audit Tool and used across the Projects to provide a Governance Assurance that the guidelines are being applied and used Agree in progress Facilities & Development Draft guidelines in place Dec ) Follow up June ) Final G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
161 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS follow up Dec 2017 Element 13: Health and Safety in Construction and Design Score 2 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
162 3.2 Waitemata District Health Board Health and Safety Resource Assessment Report RECOMMENDATIONS Element 14: Clinical Leadership of Health and Safety Issues 14.1 Clinical Leadership and the Safe Way of Working 14.2 Infection Prevention and Control 14.3 Governance Components 14.4 External Accountability Element 14: Clinical Leadership of Health and Safety Issues Recommendation Proposed Action Who Timeframe No Recommendation No Recommendation No Recommendation No Recommendation 4 G Drive: Occ health Prepared by Approved by: OHSS Manager Date: Review Date: Form number: Page
163 3.3 Communications Report 3.3 Recommendation: That the report be received. Prepared by: Holly McClune (Deputy Director Communications) Communications support The communications team provided advice and support to the following projects/campaigns/issues/ events over the last ten weeks: Input into front page design and navigation of new intranet site, including survey of satisfaction with the existing Staffnet platform Communications around NZRDA strike activity Coordination of responses to Dear Dale s to the CEO from DHB staff Update of organisational charts Communications support for the Primary Care and Community Services Launch Communications support for AAA screening programme Planning for opening of Waitemata Clinical and Learning Skills Centre Review of General Surgery department communications Communications support for Outpatients move to refurbished Community Health Building Communications support for the lifting of toll bars on DHB phones Communications for primary care to increase non-surgical procedures at ESC Communications support for the Work Expo (March 2017) Communications around the opening of exercise room at Waitakere Hospital Communications support for blessing of new Waitakere ED Paediatric Zone Communications support for Pukekohe Intermediate Dental Clinic Public Health Notice Planning work for inaugural Diabetes Awards (February 2017) Assisting with responses to questions from Parliamentary Select Committee on Health Communications support for Waitemata DHB Christmas activities, including the Staff Christmas decoration competition and BBQ Involvement in the International Benchmarking of Asian Health Outcomes report launch for Waitemata and Auckland DHBs Support for paediatric outpatients relocation to North Shore Hospital tower block Review of data for State Services Commission Publication of OIA compliance results Communications support for hospital Summer Plan Communications support for Waitemata-led cervical self screening study Media relations around Health Targets results Communications support for Primary Care Portal project Communications advice to Traffic Services Communications support for release of National Patient Flow data Drafting material for the 2016/17 Annual Plan Planning for Patient Experience Week Communications around HR-led all staff survey Media relations around DHB sleep strategy and sleep pack pilot Media relations around e-prescribing roll-out Ongoing weekly internal communication via Staffnet and Waitemata Weekly Waitemata District Health Board, Meeting of the Board 01/03/17 163
164 3.3 Liaison with Well Foundation Marketing and Communications Ongoing after-hours and weekend media line cover and senior management communications support Proof-read leaflets, booklets and brochures for various departments Ongoing social media strategy, activity and issues management Event photography Drafting of correspondence from the corporate office Review of copy for DHB website Management of DHB general all-user screen saver content Approval for all-user staff s Weekly Board briefing Publications The communications team published the following during the last six weeks: Certificate Christmas Decorations Document Community Services Plan Healthlines magazine November-December (issue 218) Healthlines magazine January-February (issue 219) Leaflet Metformin in Pregnancy Poster Christmas Decorations Poster Skin-to-Skin Logo StaffNet design Yearbook 2016 Waitemata Weekly, ed to all staff users Fortnightly A Note From the CEO to all staff Weekly National Health Targets updated and communicated Waitemata DHB, Careers and Awhina websites Google Analytics Statistics Waitemata DHB website Number of visits December 2016 January 2017 Total visits to this site 36,063 40,225 New Zealand 34,025 37,750 Australia USA United Kingdom Top areas December 2016 January 2017 Home page 18,429 19,982 Waitemata DHB staff page 12,117 13,922 North Shore Hospital 5,484 6,246 Waitakere Hospital 1,960 2,220 Contact us 1,715 1,884 Traffic sources December 2016 January 2017 Search traffic 72% 73% Direct traffic 23% 22% Referral traffic 5% 5% Waitemata District Health Board, Meeting of the Board 01/03/17 164
165 3.3 Careers website Number of visits December 2016 November 2016 Total visits to this site 11,545 16,146 New Zealand 10,043 13,815 United Kingdom United States Australia India Waitemata District Health Board, Meeting of the Board 01/03/17 165
166 3.3 Awhina Health Campus website Number of visits December 2016 January 2017 Total visits to this site 1, New Zealand Russia 43 - <not set> United States Social media Waitemata DHB Facebook page likes 2328* Waitemata DHB Facebook star rating - 4.3/5 (196 reviews)* Twitter 1765 followers* *As at 10 February 2017 Waitemata District Health Board, Meeting of the Board 01/03/17 166
167 3.3 OIAs received A total of 37 new OIA requests were received between 29 November 2016 and 13 February 2017: A. Leaman (Fairfax Media) - Amount of money spent on treating people who are ineligible for public healthcare from R. Schumann - Copy of financial reports detailing funding provided to residential care/rest homes A. Marett (Labour) - sub-specialties provided by ophthalmology services and patients waiting for follow-up appointments B. Lane (PSA) - Copies and drafts of the He Puna Waiora Risk Assessment Report from 12/9/16 C. Taylor (NZ Doctor) - Primary care after-hours correspondence over last two years L. Hopkins (NZ First) - Number of continence nurses/advisors employed each year since 2008 E. Miles (NZ First) - List of medical professionals in NZ on a 'skilled migrant category resident visa' or 'skill shortage list visa' that have had a complaint laid against them S. Robson (RNZ) - Details on wait times, appointment rates and shortfalls in relation to youth oral health matters raised in CPHAC papers D. Firth - Respite policy for carers of totally disabled patients R. Schumann - Funding to individual rest homes over the last financial year A. Vailahi (NZ First) - Cost of treatment and written-off debts for healthcare to non-new Zealanders K. Dennett (Fairfax Media) - Details of overseas medical staff and recruitment costs R. Karetai (Rainbow Wellington) - Details of policies in place regarding unlawful discrimination against Transgender New Zealanders P. Body (AUT) - Number of psychotherapists and psychologists employed before 2009 and each year from C. Austin (Cancer Society of NZ) - Number of National Travel Assistance Fund applications received, declined, accepted and amount spent since 2005 R. Towner (Bell Gully) - Request for information in relation to an individual staff member R. Towner (Bell Gully) - Second request for information in relation to an individual staff member A. Marett (Labour) - Eligibility and funding information regarding home-based support services B. Doncliff - Information about clinical/professional supervision programmes including departments and staff numbers involved T. Forde (Green Party) - Information regarding any changes made to mental health services in last 12 months A. Vailahi (NZ First) - Information regarding number of motor vehicles owned/leased as at 30/1/17 A. Marett (Labour) - Amount spent on primary mental health since 2012/13 H. Martin (Fairfax) - People under 18 who have accessed CADS either through self-referral or otherwise for the years and breakdown of data A. Vailahi (NZ First) - Request for information on insulation and floor coverings installed in facilities or properties since 1 January 2011 A. Marett (Labour) - Number of self-inflicted deaths by clients while in the care of community mental health broken down by year O. Carville (NZ Herald) - Confirmed suicide attempts / self-inflicted injuries for under-25s in past financial year A. Vailahi (NZ First) - Number of staff employed to develop policy / deliver services to Maori and Pacifica peoples A. Bray (Labour) - Number of coronary bypass operations and angioplasties performed between A. Andrews (FYI website) - Total number of hospital beds at WDHB from Waitemata District Health Board, Meeting of the Board 01/03/17 167
168 3.3 E. Donovan (Radio NZ) - Amount of funding received / put into forensic psychiatry services from M. Prescott - Information / policies about allowing or not allowing support people to stay with mothers who have recently given birth S. Gee (Fairfax Media) - Total cost of treatment for non-new Zealand citizens in the last five years O. Hamed (APEX) - Number of psychologists being supervised and with access to external supervision L. Dalal (FYI website) - Number of PGY1 positions filled by PGY2 or higher appointees A. Bray (Labour) - Amount owed by non-resident New Zealanders for unpaid medical bills from A. Bray (Labour) - Number of people who stopped/quit smoking from A. Marett (Labour) - Costs submitted/amount agreed on with MOH to clear back log in relation to ophthalmology services Media Clippings - 28 November February 2017 Positive + Neutral 0 Negative - Channel, Auckland Well Said + Director takes a bow 0 Dominion Post The shocking truth of ECT - Listener NZ Stroke of good fortune 0 Mahurangi Matters DHB leads country in cancer targets + New study bolsters case for road sealing 0 Quilters spread Christmas cheer + Nor West News Waitemata leads treatment targets + Taking a swing at a second world record 0 North Harbour News Waitemata DHB leads treatment targets + Health staff left concussed and bruised - Junior doctors striking over hours - Waitemata District Health Board, Meeting of the Board 01/03/17 168
169 3.3 North Shore Times Golfers set record + Waitemata DHB leads in two health targets + Bus and van collision proves fatal 0 Crash update 0 What s on health free cervical smear clinic + Hungry kids hiding in leafy suburbs 0 Highlights from the community s year diesel spill on lake - Patient aggression on the rise - Junior doctor strike 0 Hospital greeters + Balloon artist s work reaches new heights 0 NZ Doctor Auckland DHBs circle the wagons on after-hours plan, GPs left in the dark - Mobile phone technology s rapid uptake will tap in the future of healthcare delivery + Auckland GPs criticise mean DHB proposal on methadone funding - Whatever happened to Bowel Screening Pilot 0 Whatever happened to Diesel leak - Double-whammy screening goes across two DHBs targeting Maori and aneurysms + DHBs vigilant for cyber threats 0 GP celebrates breakthrough in wrangle over Auckland methadone funding 0 NZ Herald/Herald on Sunday/NZherald.co.nz/Weekend Herald The perfect little presents 0 Ella leads New Year babies 0 Pool incident 0 Acid drum spill 0 Bowel screening programme: Responding to the critics 0 Hospitals full as three-day strike begins 0 Dental scare - Scared parents fill clinics - Upsetting time as family waits - Rheumatic fever efforts fall short - Otago Daily Times Van driver killed 0 Cxbladder Monitor to be launched stateside 0 Blood tests start after dental scare - Pharmacy Today New free education courses for pharmacy + Switch to electronic records challenging but rewarding + Waitemata District Health Board, Meeting of the Board 01/03/17 169
170 3.3 The Press Christchurch Double standard claim on DHB pay 0 Dental clinic warning - Bowel screening for Canterbury delayed 0 Waikato Times ECT used in 10pc of mental cases - Assaults on health staff rise - Maori health study gets $1m + Check on clinics after scare - Western Leader In brief - Bowel Screening 0 Health visits and Santa + Rescue helicopter 0 Milestones Well Foundation + Volunteers at Waitakere hospital + High praise for 87-year-old hospital helper + Weighing up obesity statistics 0 Parents feel judged 0 Psychologist helps Maori misdiagnosis + Health staff are left concussed, bruised - Junior doctors to strike for safer working hours - Volunteers needed at the hospital + Young start in tofu business 0 TOTAL: Positive + 20 Neutral 0 27 Negative - 19 Total items 66 Waitemata District Health Board, Meeting of the Board 01/03/17 170
171 4.1 Financial Performance Recommendations: 4.1 That the Board: a) Note the content of this report, with particular reference to the relative financial results in the Provider and Funder divisions and the plans to improve financial performance. b) Receive the following reports: 1 Executive Summary and key themes 2 Financial Overview of the 2016/17 result 3 Financial Performance - DHB Arms 4 Financial Performance - Other Indicators / Trends 5 Capital Expenditure 6 Financial Position 7 Cash flow Position 8 Treasury Prepared by: Rosemary Chung (Deputy Chief Financial Officer-Corporate) and Simon Watts (Deputy Chief Financial Officer-Provider) Endorsed by: Robert Paine (Chief Financial Officer and Head of Corporate Services) 1 Executive Summary and key themes The DHB continues to operate within its financial budget and is on track to deliver a better than budget result at year end. The Provider, however, continues to operate in deficit with a year to date unfavourable variance to budget of $4.964m and the Funder is favourable to budget by $5.042m. The key variables affecting the Provider result continues to be high bureau and other outsourced services that are costing more than the savings that are caused by staff vacancies. Efforts to manage high levels of overtime, sick leave and bureau usage have had some success, but cost pressures continue. Clinical supplies, utilities (water and power) and maintenance (including the cost of diesel spill cleanup) continue to challenge the result. In addition, savings targets booked into budgets more than explain year to date variances. The Provider arm has a number of streams of work in progress currently to enable it to obtain financial sustainability. Work streams have been organised as tactical savings opportunities are identified, benefits from procurement supply chain and capital projects are identified to ensure that they are realised, and larger, strategic responses to the Provider arm performance are developed, leveraging off the work of Deloitte. Waitemata District Health Board, Meeting of the Board 01/03/17 171
172 Examples of these streams include: Review of Emergency Department and Assessment and Diagnostic Unit patient hours Review of outpatient clinics and follow-up appointments Review of the Radiology service production plans Centralised roster systems implementation Review of nurse led clinics Co-location of patients during the summer months. 4.1 Within the services management teams are also actively monitoring performance and tight cost controls are in place in all key areas of expenditure that include: Delegation being escalated to General Manager level as required External bureau and all overtime requests being reviewed by the General Manager as required Fortnightly reviews of financial performance against plan by Chief Operating Officer, General Manager, Deputy Chief Financial Officer and Clinical leads Within the Corporate Service, DHB wide initiatives are being agreed, which include: Procurement Savings initiatives Inventory rationalization and process efficiency Utility efficiency programme. 2 Financial Overview of the 2016/17 result For the month of December, the DHB result is a deficit of $301k against a budgeted deficit of $307k and is therefore $6k favourable to budget. For the month, the Provider arm is $791k unfavourable to budget, the Funder Arm is $795k favourable to budget and the Governance and Funding Arm is $1k favourable to budget. Waitemata District Health Board, Meeting of the Board 01/03/17 172
173 The financial result for the month of December 2016 compared to the budget is summarised in the table below: 4.1 WAITEMATA DISTRICT HEALTH BOARD CONSOLIDATED STATEMENT OF FINANCIAL PERFORMANCE Reporting Date 31 December 2016 ($000's) MONTH YEAR TO DATE FULL YEAR Actual Budget Variance Actual Budget Variance Forecast Budget Variance REVENUE Crown 134, ,384 1, , ,183 2,206 1,600,414 1,600,414 0 Other 3,128 3,237 (109) 17,419 19,703 (2,285) 39,611 39, , ,621 1, , ,887 (78) 1,640,025 1,640,025 0 EXPENDITURE Personnel - Medical 15,403 14,763 (639) 84,802 86,685 1, , , Nursing 19,724 20, , , , , Allied Health 8,914 9, ,820 54, , , Support 1,455 1, ,785 9, ,548 18, Management / Administration 5,764 6, ,193 36, ,480 73,480 0 Total Personnel 51,259 51, , ,548 4, , ,361 0 Other Outsourced Services 5,894 5,484 (411) 38,221 33,643 (4,578) 66,590 66,590 0 Clinical Supplies 10,475 8,835 (1,640) 58,089 56,126 (1,962) 110, ,938 0 Infrastructure & Non-Clinical Supplies 9,415 7,407 (2,008) 54,333 47,460 (6,873) 89,228 89,228 0 Funder Provider Payments 60,933 63,284 2, , ,704 8, , , ,717 85,009 (1,708) 521, ,933 (4,580) 1,026,164 1,026,164 0 Total Expenditure 137, ,927 (1,049) 818, , ,635,525 1,635,525 0 NET RESULT (301) (307) 6 1,483 1, ,500 4,500 0 Comment on Major Variances Revenue Revenue is $78k unfavourable to budget year to date. The unfavourable year to date variance includes interest revenue $1.3m less than budget which is reflective of a combination of the cash balance and the continuing low interest rates, drug trial and donation revenue of $1.0m which are expected to be recovered in the latter part of the year. This is offset against by a favourable variance for the Ministry of Health and other DHB funding of $2.2m. Expenditure Overall expenditure was favourable to budget by $157k year to date. The key variances are summarised below. Personnel Costs ($4.737m favourable year to date) A significant contributor to the favourable variance is vacancies due to positions budgeted in the new financial year that have yet to be appointed. Variances in Personnel Cost categories were as follows: Medical staff costs are favourable by $1.883m year to date. This favourable variance is primarily driven by vacancies. Nursing staff costs are favourable by $735k for the year to date. The Provider services have continued to have a strong drive on monitoring overtime hours which has been a positive contributor to the variance. The favourable variance is offset by unfavourable outsourced bureau Waitemata District Health Board, Meeting of the Board 01/03/17 173
174 costs to cover un-recruited vacancies, watch cover and sick leave which is being actively monitored to ensure appropriate deployment 4.1 Allied Health staff costs were year to date favourable to budget by $856k largely due to vacancies in the Sub Speciality and Child Women and Family services. Support staff costs are favourable by $287k year to date. Management and Administration staff costs are favourable by $976k year to date. The favourable variance is offset in part by outsourced costs due to contractors currently in place. The variance also includes un-recruited positions and savings. The replacement of contractors with permanent staff is being actively pursued. Outsourced Services Costs ($4.578m unfavourable for the year to date) The variance relates to positions to be recruited and vacancies which are covered by outsourced resources. This includes nursing bureau costs largely due to the requirement for unplanned watches. The variance also includes savings targets which have been met in other cost lines. Clinical Supplies Costs ($1.962m unfavourable for the year to date) The year to date variance is driven by unfavourable variances in Hospital operations $1m, surgical and ambulatory services $727k and Children Woman and Family $370k. Favourable variances have been incurred by medicine and mental health. The favourable variances are offset against planned savings targets. Infrastructure costs ($6.873m unfavourable for the year to date) The year to date unfavourable variance is largely due to saving targets recorded in infrastructure, where the savings are offset in other expense lines. Funder Provider Payments ($8.833m favourable for the year to date) Funder Provider payments for December are $2.35m favourable for the month and $8.83m favourable for the year to date. Funder Provider payments as reported in the Consolidated Statement of Financial Performance table are for all Funder payments to third party providers and includes payments to NGO Providers as well as payments to other DHBs through Inter District Flow expenditure. It does not include payments made to the Waitemata DHB Provider Arm. Commentary on key drivers of the favourable Funder position are summarised under the Funder Financial Performance section that follows later in the report. 3 Financial Performance - DHB Arms The financial performance for each of the DHB Arms for the month and the year is summarised in the table below, and the detailed Statement of Financial Performance by DHB Arm is attached to this report (Attachment 1). Waitemata District Health Board, Meeting of the Board 01/03/17 174
175 WAITEMATA DISTRICT HEALTH BOARD FINANCIAL PERFORMANCE BY DHB ARM Reporting Date 31 December 2016 ($000's) MONTH YEAR TO DATE FULL YEAR Actual Budget Variance Actual Budget Variance Forecast Budget Variance REVENUE Provider Arm - Clinical Services 4,205 3, ,328 23, ,196 47,196 0 Provider Arm - Corporate & Support Services 70,315 67,986 2, , ,864 3, , ,952 0 Governance & Funding Admin Arm 1,052 1,081 (29) 6,377 6,484 (107) 12,969 12,969 0 Funder 130, ,824 1, , ,944 1, , ,280 0 Elimination (68,107) (65,165) (2,942) (396,045) (390,990) (5,055) Consolidated 137, ,621 1, , ,887 (78) 1,638,397 1,638, EXPENDITURE Provider Arm - Clinical Services 58,773 57,592 (1,181) 317, ,079 (6,366) 633, ,382 0 Provider Arm - Corporate & Support Services 17,219 14,971 (2,249) 123, ,214 (2,449) 229, ,766 0 Governance & Funding Administration 1,051 1, ,346 6, ,969 12,969 0 Funder 129, ,449 (591) 766, ,694 3, , ,780 0 Elimination (68,107) (65,165) 2,942 (396,045) (390,990) 5,055 0 Consolidated 137, ,927 (1,049) 818, , ,633,897 1,633,897 0 NET RESULT Provider Arm - Clinical Services (54,567) (53,697) (871) (293,116) (287,494) (5,622) (586,186) (586,186) 0 Provider Arm - Corporate & Support Services 53,095 53, , , , ,186 0 Governance & Funding Admin Arm Funder 1, ,292 2,250 5,042 4,500 4,500 0 Elimination 0 (0) 0 0 (0) Consolidated (301) (307) 6 1,483 1, ,500 4, Provider Clinical Services The Provider Clinical services result for the month ended 31 December 2016 is $871k unfavourable to budget and year to date is $5,622k unfavourable to budget. The key drivers of the services financial performance are summarised below. Medicine and Health of Older People Acute and Emergency Medicine The division is $1.9m unfavourable for the six months ended 31 December The volume of dedicated patient watches was favourable to budget in the month, however, on a YTD basis patient watches have generated an unfavourable variance in bureau costs of $862k. Nursing costs are unfavourable to budget by $441k YTD with pricing being a significant component. Registrars and House Officers are unfavourable $238k and $332k respectively YTD, with both price and volume driving the adverse position. Sub Specialty Medicine The division is $0.3m favourable for the six months ended 31 December The favourable result is driven predominantly with increased ACC revenue of $125k YTD particularly from the Assessment Treatment and Rehabilitation service and vacancies currently within Allied Health, contributing $275k YTD. Surgical and Ambulatory Services The service is $3.2m unfavourable for the six months ended 31 December This financial position has been adjusted to reflect the financial position taking into account additional costs anticipated in order to achieve the Surgical Health Target. The service has employed tight controls across all key areas of expenditure with all requests for recruitment to be reviewed by the General Managers and all key procurement requests now centralised. Work is ongoing to realise any savings opportunities through procurement arrangements and potential efficiencies in service delivery models. The executive has requested a detailed financial forecast and savings mitigation plan through to the end of the financial year. Waitemata District Health Board, Meeting of the Board 01/03/17 175
176 Elective Service Centre The service is $0.3m unfavourable for the six months ended 31 December This financial position has been adjusted to reflect the financial position taking into account additional costs anticipated in order to achieve the Surgical Health Target. Work is ongoing to investigate any savings opportunities through procurement arrangements and potential efficiencies in service delivery models. In addition to a detailed forecast for the service the executive have initiated a whole of service review of financial and operational performance in order to identify and implement further areas of improvement. 4.1 Child Women and Family Services The service is $0.6m unfavourable for the six months ended 31 December 2016 and reported a $23k favourable financial result for the month of December The result was primarily driven by several factors that include improved Child Rehab Out of Auckland Area bed day revenue and new unbudgeted service level agreements $35k, staffing benefits relating to a higher uptake of annual leave and vacancies that are expected to be filled in the new year $177k. Partially offsetting this overall result were a combination of unmet savings initiatives, cost pressures in cleaning, treatment disposables and repairs and maintenance costs across the dental facilities $190k. Service activity remains positive with Neonatal Inpatients tracking at 91% (December 20 16) 101% (Year to date) of targeted case weighted discharge, Gynecology electives at 116% (December 20 16) and 95% (Year to date) and Gynecology acute 106% (December 2016) and 99% (Year to date) of target, Maternity Inpatient acute 119% and 116% with Pediatric Inpatient acute 86% and 110% respectively. Child, Women and Family Services are expecting to another favourable month in January with the ward closures to match reduced demand over the summer months, and the redeployment of staff into other wards. Maximising staff annual leave without compromising clinical activity remains a key focus. Mental Health Services The service is $264m favourable for the six months ended 31 December This is primarily driven by favorable variances in personnel and other direct costs. The personnel variance of $35k YTD is driven by a large number of vacancies in nursing offset by casual staff and overtime cover. Other direct costs are favourable by $400k YTD driven by clinical supplies and infrastructure. Clinical supply variance is the flexifund account for patient s healthcare and wellbeing in community homes. Other Revenue is $170k unfavourable YTD driven by the new and extended Child and Youth services in Rodney. 3.2 Corporate and Support Services The overall year to date result for Provider Support is $2.150m unfavourable. The Corporate and Support Services includes centrally budgeted savings which is the major contributor to the unfavourable variance. The overall result for Hospital Operations is $459k unfavourable for the year to date to December This is primarily due to unfavourable activity related non-pay costs. This includes the cost of pharmaceuticals and patient meal costs which are unfavourable due to a 1% increase in price for indexation per the terms of the contract plus a further 5.5% uplift in price due to lower than anticipated number of DHBs participating in the national Food Services Agreement. 3.3 Financial Performance Funder The Funder net result for December is $0.79m favourable for the month and $5.04m favourable year to date. The Funder result as reported in the Financial Performance by DHB Arm table represents the totality of the Funder and is inclusive of Funder Provider Arm Services, Funder NGO Services and Waitemata District Health Board, Meeting of the Board 01/03/17 176
177 Funder IDF Services. The Funder favourable net result variance is the net position inclusive of all of Funder divisions. The favourable position is mostly a consequence of upsides within the Funder NGO Services division. It results from a range of contributing factors which includes budgeted service initiatives not yet fully committed. Lower than budget utilisation across the major demand service categories (especially Aged Residential Care) and once off upsides relating to prior year adjustments also contribute to the favourable NGO position. The Funder net position also includes the adverse impact of additional revenue allocations to the Provider Arm. These allocations mostly relate to the over delivery within acute inpatient services based on year to date utilisation against plan and is subject to monthly revision going forwards Financial Performance - Governance and Funding Administration Arm The Governance and Funding Administration (GFA) represents the Waitemata DHB share of the joint Planning Funding and Outcomes Arm and includes the Waitemata DHB share of the Northern Regional Alliance. The GFA Core Net Result is on budget for the month and year to date. 4 Financial Performance Other Indicators/Trends 4.1 Net Result The actual net result performance against the budget for the DHB tracked over time is illustrated in the graph below. The overall DHB result for the six months to 31 December 2016 is a surplus of $1.483m which is $78k favourable to budget. Waitemata District Health Board, Meeting of the Board 01/03/17 177
178 4.2 Savings Targets and Initiatives The Savings Initiatives which have currently been identified are summarised as: 4.1 Savings Category $000s Annual Leave Review and Management 700 Overtime reviews 1,000 Other Personnel Initiatives 2,075 Elective Surgery 400 Elective theatre efficiency 320 Waitemata Central 1,100 Revenue Generation 500 Fleet Strategy 500 Procurement 2,000 Supply Chain 1,000 Other Non-Personnel Initiatives 7,787 To be allocated 4,334 TOTAL 21,716 Predicted savings achieved to 31 December 2016 are estimated at $4.27m. In this report, a summary of the initiatives being undertaken by the Hospital Operations Services is included below. The Hospital Operations Service has made solid progress in achieving efficiency initiatives in 2016/17. The targeted savings for to six months to 31 December 2016 was $654,000 and the service has made $839,000 December year to date. The key drivers of this performance include, firstly, implementing continuous monitoring of existing blood product protocols that has resulted in reduced volumes being required ($125k). Secondly, procurement and purchasing savings for cleaning chemicals and laboratory reagent consumables ($244k) and thirdly, implementing a variety of optimisation projects in the pharmaceutical and laboratory service that have increased revenue and saved costs ($470k). Local Procurement Current projects underway have predicted annualised savings of in excess of $2.0m. Annualised Procurement and Supply Chain savings achieved in the current financial year to the end of January amounts to $786k. There are a large number of procurement initiatives in the pipeline which forecast savings. These activities include: Identifying areas for high spend where contracts are required or require renegotiation: Negative pressure wound therapy is a category where there were two contracts with multiple price structures. We approached a panel supplier and negotiated a favourable rent-to-own model. Clinical trials have commenced and should be completed by mid-march. Provided clinical evaluation is successful the benefit will be $1.42m over 5 years. Waitemata District Health Board, Meeting of the Board 01/03/17 178
179 Mobility Aids Rental Equipment: A working group has been set up to develop more efficient processes and systems regarding the management of mobility aids. Forecast savings already achieved is $100k annualised. 4.1 Proposed Price Increases: There was a price increase proposed by a supplier which we have renegotiated providing an annualised benefit (avoided cost increase) of $100k and have a short term agreement put in place to secure the pricing. Requests for Proposals to Market: The team with the Services are working well with ha FPSC to prepare sourcing briefs to put out into the market. Two of the current projects: Medical Gas RFP. Two suppliers have been appointed to the Panel. Waitemata DHB has reviewed the offers by the two suppliers and have selected a supplier which will result in an inventory management solution and a reduction in stock volume by an estimated 25%. ADRS cleaning contracts: Waitemata DHB currently has a number of expired cleaning contracts. Analysis has been undertaken on the current suppliers to understand time in clinic and effectiveness of the service. An RFP has gone to market and we are due to have responses by the end of February. Pharmac Wound Care Introduction: Pharmac have recently concluded a market share agreement within the Wound care category. The team has implemented the opportunities under the new contract with an expected annualised savings in excess of $100k. 5 Capital Expenditure Capital expenditure planned for the 2016/17 year is $74.926m. The table below summarises performance against the capital expenditure budget for the month and for the year. $'000s Full Year Budget Month (Dec-16) YTD (Dec-16) Actual Budget Variance Actual Budget Variance Land Buildings & Plant 46,133 4,117 3,277 (840) 24,307 24, Clinical Equipment 8, ,158 4,516 1,358 Other Equipment 4, ,638 2,437 Information Technology 6, , ,336 3, Purchase of softw are 7, ,072 2, ,212 3,212 Motor Vehicles 2, , Total Capital Expenditure 74,926 5,192 7,772 2,580 30,631 39,248 8,617 Note: The Full Year Budget is based last filed DAP. As at December 2016, capital expenditure year to date is $8.617m below the plan. The majority of spend has been incurred on four large facilities capital projects. These are the Community Building 5 refurbishment, the Learning Centre, Waitakere Emergency Department and Mason Clinic 15 Medium Secure Units. 6 Financial Position The financial position as at 31 December 2016 is shown below. This indicates a strong balance sheet, with net worth of $ m including $65m in cash and deposits. The detailed Statement of Financial Position for the DHB Parent is provided as Attachment 2. Waitemata District Health Board, Meeting of the Board 01/03/17 179
180 Opening Dec-16 Dec-16 Dec-16 Full Year In $'000s 30 Jun-16 Actual Budget Variance Budget Crown Equity 335, , ,172 (2,287) 342,854 Represented by : Current Assets 137, , ,738 3, ,487 Current Liabilities 268, , ,533 (11,909) 255,459 Net Working Capital (130,721) (143,943) (135,795) (8,148) (154,972) Fixed Assets 748, , ,370 (15,214) 800,229 Term Liabilities 281, , ,403 20, ,403 Total Employment of Capital 335, , ,172 (2,787) 342, Cash flow Position Summary of the cash flow statement as at 31 December 2016 is shown below. The detailed Cash flow statement is provided as Attachment 3. $'000s Month YTD Actual Budget Variance Actual Budget Variance Opening cash 0 66, ,682 Operating 4,245 2,062 2,183 14,186 15,937 (1,751) Investing (5,193) (7,271) 2,078 (12,631) (36,242) 23,611 Financing (1,555) (1,000) (555) Closing cash 0 0 Closing Cash Balance in HBL Sw eep account 55,187 55,187 Deposits 10,000 10,000 Closing Cash + Deposits 65,187 59,369 5,818 65,187 59,371 5,816 The DHB s cash position in the NZHPL sweep as at 31 December 2016 is $55m (Last month $56m). The balance total cash balance including deposits is $65m (last month $66m). The DHB also monitors performance in collecting amounts owed by other organisations; the total amount owed to the DHB as at 31 December 2016 was $14.3m (last month balance owed was $-18.0m). 50% of this is within the 60 days period (41% of this relates to Ministry of Health and 28% to other DHBs). 50% is over 60 days and the majority of this is in the area most difficult to collect, i.e. non-residents income. An Accounts Receivables report and explanation for amounts overdue for more than 60 days is provided as Attachment 4. 8 Treasury 8.1 Financing Activity Term debt drawn and average interest expense and rates are shown in the Tables below. Month Term Debt ($ 000s) CHFA Interest Expense ($ 000s) Jul , Aug , Sep , Oct , Nov , Dec , YTD 276,706 5,250 $ m of Crown debt was fully drawn as at 31 December All loan facilities have been drawn down as at 31 December Waitemata District Health Board, Meeting of the Board 01/03/17 180

181 $ Millions The average interest rates on the loan portfolio are provided in the table below: NZD Available Facilities $000 Drawn Debt Current Drawn Debt Last Month $000 Interest Rate Current Interest Rate Last 4.1 CHFA Fixed $250,996 $250,996 $272, % % CHFA Floating $25,710 $25,710 $3, % % Total Facilities $276,706 $276,706 $276, % % Monthly Weighted Average Interest Cost (Including Hedges & Margin) % % All Crown Debt was converted to Equity on 15 February Treasury Policy All Waitemata DHB debt shall be borrowed on either a fixed interest rate or floating interest rate basis, subject to the requirement that the overall percentage of fixed (fixed/floating master limit) in any time bucket must be in accordance with the following limits: The fixed rate amount at month-end reporting dates must be within the following maturity bands (percentages calculated on the fixed rate amount at month end): The interest rate re-pricing risk profile for the Waitemata DHB Crown debt is shown in the graph below: WAITEMATA DISTRICT HEALTH BOARD Interest Rate Repricing Risk Profile yrs 10% - 70% Interest Rate Re-Pricing 3-5 yrs 10% - 70% 21% 29% yrs 10% - 70% Years Fixed Debt Maturity Floating Waitemata District Health Board, Meeting of the Board 01/03/17 181
182 All Crown Debt was converted to Equity on 15 February Financial Covenants Waitemata DHB s performance against financial covenants (which are currently waived) is summarised below and compliance was achieved. 4.1 Financial Covenants Actual Budget Covenant Met Shareholders Funds (=> $70 million) 337 m 340 m Yes Net Total Debt / (Net Total Debt + SHF) < 65% 48% 49% Yes ANZ Interest Cover EBITDA / Net Interest (> 1.5:1) 9 12 Yes CHFA Interest Cover EBITDA / Net Interest (> 2.5:1) 5 7 Yes Waitemata District Health Board, Meeting of the Board 01/03/17 182
183 ATTACHMENT 1 WAITEMATA DISTRICT HEALTH BOARD STATEMENT OF FINANCIAL PERFORMANCE BY DHB SERVICE GROUP 31 December MONTH Direct Revenue Direct Expenditure Net Result FTE's Head Count ($000's) Actual Budget Variance Actual Budget Variance Actual Budget Variance Actual Budget Variance Actual Provider Medical Services 1, ,762 21, (20,695) (20,948) 253 4,100 3,962 (137) 2,449 Surgical Services ,678 13,266 (1,412) (13,789) (12,623) (1,165) 1,148 1,025 (123) 1,298 ESC (3) 2,259 2,029 (230) (2,216) (1,983) (233) (4) 111 Child, Women & Family Services 1,139 1, ,113 8,100 (13) (6,974) (6,997) ,187 Mental Health 1,068 1,131 (64) 11,961 12, (10,893) (11,145) 252 1,259 1, ,391 Sub Total - Clinical Services 4,205 3, ,773 57,592 (1,181) (54,567) (53,697) (871) 7,486 7,348 (138) 6,436 Director of Hospital Services (67) 2,337 2,104 (233) (1,707) (1,407) (300) Hospital Operations 1, ,482 5,936 (547) (5,285) (5,586) (30) 1,060 Facilities ,749 2,470 (279) (2,379) (2,419) (43) 94 Provider Management 66,232 65,030 1,202 (4,605) (5,996) (1,391) 70,838 71,027 (189) 0 0 Corporate 1,885 1, ,257 10, (8,372) (8,599) Sub Total - Corporate & Support Services 70,315 67,986 2,329 17,219 14,971 (2,249) 53,095 53, ,917 1,911 (5) 1,465 Total Provider 74,520 71,881 2,639 75,992 72,563 (3,430) (1,472) (682) (791) 9,403 9,260 (144) 7,901 Governance & Funding Administration 1,052 1,081 (29) 1,051 1, Funder Arm Funder NGOs 38,644 40,318 (1,674) 37,543 39,943 2,401 1, Funder Inter District Flows 23,459 23, ,390 23,341 (50) Total Funder Arm 62,103 63,659 (1,556) 60,933 63,284 2,351 1, Consolidated 137, ,621 1, , ,927 (1,049) (301) (307) 5 9,487 9,356 (131) 8,000 YEAR TO DATE Direct Revenue Direct Expenditure Net Result FTE's Full Year ($000's) Actual Budget Variance Actual Budget Variance Actual Budget Variance Actual Budget Variance Budget Provider Medical Services 7,001 5,979 1, , ,417 (2,620) (108,036) (106,437) (1,599) 1,972 1, (218,746) Surgical Services 4,237 3, ,803 78,012 (2,791) (76,566) (74,157) (2,410) 1,107 1,067 (40) (154,205) ESC (414) 276 (690) 13,642 13,083 (559) (14,057) (12,808) (1,249) (2) (25,287) Child, Women & Family Services 6,761 6, ,130 44,300 (830) (38,369) (37,740) (629) (74,966) Mental Health 6,744 6,914 (170) 62,832 63, (56,088) (56,352) 264 1,240 1, (112,982) Sub Total - Clinical Services 24,328 23, , ,079 (6,366) (293,116) (287,494) (5,622) 5,310 5, (586,186) Director of Hospital Services 4,780 4, ,742 11,846 (896) (7,962) (7,664) (298) (2,543) Hospital Operations 3,116 2,096 1,019 37,981 36,503 (1,479) (34,866) (34,407) (459) (14) (70,824) Facilities 1, ,192 16,684 15,135 (1,549) (15,188) (14,831) (357) (42) (29,745) Provider Management 394, ,181 4, (6,065) (6,319) 394, ,245 (1,751) ,049 Corporate 6,800 11,101 (4,302) 56,002 63,795 7,793 (49,202) (52,694) 3, (94,751) Sub Total - Corporate & Support Services 410, ,864 3, , ,214 (2,449) 287, , (32) 586,186 Total Provider 435, ,448 3, , ,293 (8,815) (5,841) (845) (4,996) 6,301 6, Governance & Funding Administration 6,377 6,484 (107) 6,346 6, Funder Arm Funder NGOs 237, ,910 (4,008) 230, ,660 9,425 7,667 2,250 5,417 4,500 Funder Inter District Flows 140, , , ,044 (593) (375) (375) Total Funder Arm 378, ,954 (3,791) 370, ,704 8,833 7,292 2,250 5,042 4,500 Consolidated 819, ,887 (79) 818, , ,483 1, ,388 6, ,500 Waitemata District Health Board, Meeting of the Board 01/03/17 183
184 ATTACHMENT 2 Attachment 2 WAITEMATA DISTRICT HEALTH BOARD STATEMENT OF FINANCIAL POSITION ($'000s) Reporting Date 31 December /06/ /06/2017 Actual Actual Budget Budget Crown Equity 103,015 Crown Equity 103, , , ,890 Revaluation Reserve 273, , ,813 (42,785) Retained Earnings - Prior Years (40,936) (38,474) (38,474) 1,849 Retained Earnings /17 1,484 1,818 4, , , , ,854 Represented by : Current Assets 81,631 Bank and Short Term Deposits 65,187 61,808 42,959 47,953 Debtors 47,301 48,200 49,713 1,113 Prepayments 2,260 1,115 1,115 6,614 Inventory 6,752 6,615 6,700 Assets Held for Resale 137, , , ,487 Current Liabilities Bank Overdraft 116,440 Creditors 136, , ,620 46,645 Provisions and Accruals ,898 Staff Related Liabilities - Current 102, , ,170 26,049 Term Debt - Current Portion 25,966 26,049 26, , , , ,459 (130,721) Net Working Capital (143,943) (135,795) (154,972) Fined Assets 612,730 Land, Buildings and Plant (net) 604, , ,877 3,660 Leasehold Building Works (net) 3,478 3,751 3,751 39,963 Equipment (net) 36,105 36,552 33, Information Technology (net) 62 (69) (69) 192 Intangible Software (net) (14) 2,784 Vehicles (net) 2,511 2,289 1,813 50,975 Work in Progress 78,759 86, , , , , ,910 38,089 LT & Investments in Associates 38,089 45,319 45,319 38,089 38,089 45,319 45,319 Term Liabilities 29,825 Staff Related Liabilities- Term 29,927 42,400 42, Trust and Special Funds ,435 10, ,519 Term Debt - Enternal 251, , , , , , , , , , ,854 Waitemata District Health Board, Meeting of the Board 01/03/17 184
185 ATTACHMENT 3 WAITEMATA DISTRICT HEALTH BOARD CASHFLOW STATEMENT ($'000s) Reporting Date 31 December Month YTD Actual Budget Variance Actual Budget Variance Cash flows from operating activities: Inflows Crown 140, ,796 5, , ,809 25,784 Interest Received (383) 2,990 3,006 (16) Other Revenue 3,903 1,328 2,575 22,071 8,089 13,982 Outflows Staff 50,206 51,906 1, , ,138 1,898 Suppliers 21,260 7,234 (14,026) 130, ,608 (18,761) Other Providers 64,758 62,231 (2,527) 405, ,389 (32,283) Capital Charge 10,663 12,264 1,601 10,663 12,264 1,601 Interest Paid ,163 5, GST (net) (7,679) 0 7,679 (5,639) 0 5,639 Net cash from Operations 4,245 2,062 2,183 14,186 15,937 (1,751) Cash flows from investing activities: Inflows Sale of Fixed Assets Associates Outflows Capital Expenditure 5,193 7,271 2,078 30,631 36,242 5,611 Investments (18,000) 0 18,000 Net cash from Investing (5,193) (7,271) 2,078 (12,631) (36,242) 23,611 Cash flows from financing activities: Inflows Equity Injections New Debt Deposits Recovered Outflows Debt Repayments ,000 0 Funds to Deposit (948) ,555 0 (1,555) Net cash from Financing (1,555) (1,000) (1,555) Net increase / (decrease) 0 (5,209) 0 (21,305) Opening cash 0 66, ,682 Closing cash 0 59, ,371 Closing Cash Balance in HBL Sweep account 55,187 55,187 Waitemata District Health Board, Meeting of the Board 01/03/17 185
186 ATTACHMENT 4 WAITEMATA DISTRICT HEALTH BOARD Reporting Date 31 December 2016 STATEMENT OF ACCOUNTS RECEIVABLES Ref As % Total Outstanding Current 1-30 D D D 91 Days + Prior Month ACC 0.6% 80, , , , , , , Accredited Employers 0.0% 1, , Commercial 4.1% 590, , , , , , Crown (excluding MoH) 8.2% 1,162, , , , , , ,281, DHBS' 30.2% 4,308, ,169, , , , ,167, ,313, MOH 35.5% 5,067, ,601, , , , ,303, ,020, Non Residents 21.2% 3,030, , , , , ,245, ,119, Overseas Govt 0.0% Patient 0.2% 22, , , , , Staff 0.0% , WDHB Total 7.00% 14,266, ,848, ,496 1,258,490 1,244,166 5,933,888 17,953, % 7% 9% 9% 42% Total Less Nres 11,235,511 4,834, , ,413 1,021,164 3,688,214 43% 7% 9% 9% 33% Total 30+ 5,666,791 50% REF 1 ACC ACC had the lowest outstanding amount to date due to the lowest billing month in Dec16. The aging amount, $69k under 91 days being 86% of the total amount outstanding. 65% of this is awaiting a credit request. 3 Commercial The $131,612 in the 360+ days catagory owed by Trascirptionz Ltd is being reviewed by deputy CFO and the legal team. $13,275 in the 360+ category is being disputed by Fuji Xerox Ltd. 4 Crown Ministry of Justice has managed to settle $15k of their outstanding debt in the 90+category. Three harbours health found have also settled $164,115 of their outstanding debt in 90+category 5 DHB's For 91+days overdue: CMDHB $344K OPEX cost from which is waiting resolution. ADHB $1.9M for 61+days - escalated unpaid invoices to David Vial to pass along the concerned dept/services 6 MOH 31+ days overdue - $2.1M down by 52% from last month 7 Non Residents $1,507,985 is on a current payment plan. This category of debtors is the most difficult to collection from. Waitemata District Health Board, Meeting of the Board 01/03/17 186
187 5.1 Minutes of the Health Advisory Committee Meeting 14 December Recommendation: That the draft minutes of the Health Advisory Committee meeting held on 14 December 2016 be received. Waitemata District Health Board, Meeting of the Board 01/03/17 187
188 Minutes of the meeting of the Waitemata District Health Board Hospital Advisory Committee Wednesday 14 December held at Waitemata District Health Board Boardroom, Level 1, 15 Shea Terrace, Takapuna, commencing at 2.07pm PART I Items considered in public meeting COMMITTEE MEMBERS PRESENT ALSO PRESENT James Le Fevre (Committee Chair) Lester Levy (Board Chairman) Max Abbott Edward Benson Cooper Kylie Clegg (Board Deputy Chair Sandra Coney (Committee Deputy Chair) (until 2.41pm) Warren Flaunty Brian Neeson Morris Pita Susanna Galea (co-opted member) Donna Riddell (co-opted member) Dale Bramley (Chief Executive Officer) Andrew Brant (Chief Medical Officer) Cath Cronin (Director of Hospital Services) Fiona McCarthy (Director of Human Resources) Andrew Brant Tamzin Brott Jocelyn Peach Emma Farmer (HOD Midwifery, Child, Women and Family Services) Stephanie Doe (Acting General Manager, Child, Women and Family) Jeremy Skipworth (Clinical Director, Forensic Services) Joanne Brown (Funding and Development Manager-Hospitals) David Price (Director of Patient Experience) Helen Wihongi (Acting Chief Advisor Tikanga) Michelle Sunderland (General Manager, Surgical and Ambulatory Services) Mark Watson (General Manager, Elective Surgery Centre) David Grayson (Acting Chief of Surgery) Peta Molloy (Board Secretary) (Staff members who attended for a particular item are named at the start of the minute for that item.) APOLOGIES Resolution (Moved Max Abbott/Seconded Warren Flaunty) Waitemata District Health Board, Meeting of the Board 01/03/17 188
189 Apologies were received and accepted from Allison Roe, Matire Harwood, Willem Landman, David Ryan and for early departure from Sandra Coney. Carried 5.1 WELCOME The Committee Chair welcomed those present. DISCLOSURE OF INTERESTS There were no additions or amendments to the interests register. There were no declarations of interest relating to the open section of the agenda. 1. AGENDA ORDER AND TIMING Items were taken in the same order as listed in the agenda. 2. COMMITTEE MINUTES 2.1 Confirmation of the Minutes of the Hospital Advisory Committee Meeting held on 02 November 2016 (agenda pages 6-13) Resolution (Moved Sandra Coney/Seconded Kylie Clegg) That the Minutes of the Hospital Advisory Committee meeting held on 02 November 2016 be approved. Carried Actions Arising (agenda page 14) No issues were raised. 3. PROVIDER ARM PERFORMANCE REPORT 3.1 Provider Arm Performance Report June 2016 (agenda pages 15-80) Robert Paine (Chief Financial Officer and Head of Corporate Services) and Cath Cronin (Director Hospital Services) introduced the report. Matters highlighted or updated included: Acknowledging the work undertaken towards achieving the Faster Cancer Treatment health target. That the clarification on the median/or mean for the average length of stay graphs will be provided to the Committee at its next meeting. Waitemata District Health Board, Meeting of the Board 01/03/17 189
190 Human Resources Fiona McCarthy (Director, Human Resources) summarised this section of the report. Mental Health and Addiction Susanna Galea (Acting General Manager, Mental Health), Helen Wood (Project Manager, Mental Health) and Alex Craig (Associate Director of Nursing, Mental Health) presented this section of the report. 5.1 Matters highlighted and response to questions included: That an update on codeine addiction will be provided to the Committee at its next meeting. That two more beds were opened in He Puna Waiora with an additional five to open on Friday 16 th December. That the courtyards within the mental health service were opened when appropriate staff support was available. The Committee Chair acknowledged the work of the team during the period when bed closures where necessary. Specialty Medicine and Health of Older Persons Debbie Eastwood (General Manager, Medicine and Health of Older People Services), John Scott (Head of Division, Speciality Medicine and Health of Older People Services) and Dr Gerard de Jong (Head of Division, Acute and Emergency Medicine Division) presented this section of the report. Matters covered in discussion and response to questions included: Noting that there had been a dedicated focus during the past year on the lung cancer pathway. The superb work of the team was acknowledged. Noting that EDARS is a full service and is progressing very well. That with regard to respiratory services and patients that require monitoring overnight are traditionally transferred to North Shore Hospital to stay overnight. Andrew Brant noted that the wider sleep service is to be reviewed with the possibility of providing services across both sites. Child Women and Family Dr Peter van de Weijer (Head of Department Medical), Stephanie Doe (Acting General Manager Child, Women and Family Services) and Emma Farmer (Head of Department, Midwifery) presented this section of the report. Matters covered in discussion and response to questions included: Noting the launch of the mobile health clinic. That one in four women giving birth are Asian and that there is a large number of Chinese midwives with more Chinese and other Asian students training to become midwives. Waitemata District Health Board, Meeting of the Board 01/03/17 190
191 Surgical and Ambulatory Services/Elective Surgical Centre Michelle Sunderland (General Manager, Surgical and Ambulatory Services) and Michael Rodgers (Chief of Surgery) presented this section of the report. 5.1 Matters covered in discussion and response to questions included: Noting that the North Shore Hospital theatre refurbishment is now complete. That following a major recruitment initiative, nursing appointments for ICU had been made. Provider Arm Support Services Cath Cronin summarised this section of the report. Resolution (Moved Warren Flaunty/Seconded Kylie Clegg) That the report be received. Carried 4. CORPORATE REPORTS Clinical Leaders Report (agenda pages 81-90) Tamzin Brott (Director of Allied Health) presented this item. Apologies were noted from Dr Andrew Brant (Chief Medical Officer) and Dr Jocelyn Peach (Director of Nursing and Midwifery; Emergency Systems Planner). Tamzin Brott, in Jocelyn Peach s absence, noted that Jenny Parr (Associate Director of Nursing) had resigned and would be commencing a role at Counties Manukau DHB. Jenny s contribution to her role at Waitemata DHB was acknowledged. Tamzin also noted the launch of the Allied Health scorecard (page 86 of the agenda). She further summarised the Allied Health, Scientific and Technical Staff section of this report. In response to a question about learning from the social work patient experience survey, Tamzin noted that it is a small service and the importance of a personal approach and style was identified. Resolution (Moved Kylie Clegg /Seconded Susanna Galea) That the report be received. Carried 4.2 Human Resources (agenda pages ) Fiona McCarthy (Director of Human Resources) and Vanessa Aplin (Recruitment Manager) were present for this item. Waitemata District Health Board, Meeting of the Board 01/03/17 191
192 Vanessa Aplin gave a PowerPoint presentation on the Waitemata DHB Maps and Acronyms Mobile App. Highlights of the presentation included: Outlining the purpose of the App which will assist staff to find hospital sites from their phone; provide help with definitions of common acronyms; help staff find their way around the Waitemata DHB sites from their phone. What the app looks like Locating the app link for staff, logging on and the home page. The next steps of the app development. 5.1 Resolution (Moved Edward Benson-Cooper/Seconded Susanna Galea) That the report be received. Carried 5. RESOLUTION TO EXCLUDE THE PUBLIC (agenda page 104) Resolution (Moved Brian Neeson/Seconded Warren Flaunty) That, in accordance with the provisions of Schedule 3, Sections 32 and 33, of the NZ Public Health and Disability Act 2000: The public now be excluded from the meeting for consideration of the following items, for the reasons and grounds set out below: General subject of items to be considered 4. Confirmation of Public Excluded Minutes Hospital Advisory Committee Meeting of 02/11/16 Reason for passing this resolution in relation to each item That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] 2. Quality Report That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] Ground(s) under Clause 32 for passing this resolution Confirmation of Minutes As per resolution(s) to exclude the public from the open section of the minutes of the above meeting, in terms of the NZPH&D Act. Privacy The disclosure of information would not be in the public interest because of the greater need to protect the privacy of natural persons, including that of deceased natural persons. [Official Information Act 1982 S.9 (2) (a)] Waitemata District Health Board, Meeting of the Board 01/03/17 192
193 General subject of items to be considered Reason for passing this resolution in relation to each item 3. HR Update Report That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act Education Programme [NZPH&D Act 2000 Schedule 3, S.32 (a)] That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9 (2) (g) (i)) of the Official Information Act [NZPH&D Act 2000 Schedule 3, S.32 (a)] Ground(s) under Clause 32 for passing this resolution Privacy The disclosure of information would not be in the public interest because of the greater need to protect the privacy of natural persons, including that of deceased natural persons. [Official Information Act 1982 S.9 (2) (a)] Negotiations The disclosure of information would not be in the public interest because of the greater need to enable the board to carry on, without prejudice or disadvantage, negotiations. [Official Information Act 1982 S.9 (2) (j)] Privacy The disclosure of information would not be in the public interest because of the greater need to protect the privacy of natural persons, including that of deceased natural persons. [Official Information Act 1982 S.9 (2) (a)] 5.1 Carried The open session of the meeting concluded at 3.16 pm. SIGNED AS A CORRECT RECORD OF THE WAITEMATA DISTRICT HEALTH BOARD HOSPITAL ADVISORY COMMITTEE MEETING OF 14 DECEMBER 2016 COMMITTEE CHAIR Waitemata District Health Board, Meeting of the Board 01/03/17 193
194 5.2 Auckland DHB and Waitemata DHB Community and Public Health Advisory Committees Meeting 23 November Recommendation: That the draft minutes of the Community and Public Health Advisory Committee meeting held on 23 November 2016 be received. Waitemata District Health Board, Meeting of the Board 01/03/17 194
195 Minutes of the meeting of the Auckland DHB and Waitemata DHB Community and Public Health Advisory Committees Wednesday 23 November held at Waitemata DHB Boardroom, Level 1, 15 Shea Terrace, Takapuna, commencing at 2.04 p.m. Part I - Items considered in Public Meeting COMMITTEE MEMBERS: Gwen Tepania-Palmer (Committee Chair) (ADHB and WDHB Board member) Max Abbott (WDHB Board member) (present from 2.10pm) Jo Agnew (ADHB Board member) Peter Aitken (ADHB Board member) Judith Bassett (ADHB Board member) Chris Chambers (ADHB Board member) Sandra Coney (WDHB Board member) Lee Mathias (ADHB Deputy Chair) Christine Rankin (WDHB Board member) (until 3.30pm, Item 4.1) Tim Jelleyman (Co-opted member) ALSO PRESENT: Dale Bramley (WDHB Chief Executive Officer) Ailsa Claire (ADHB Chief Executive) (from 2.08pm) Debbie Holdsworth (ADHB and WDHB, Director Funding) Karen Bartholomew (ADHB and WDHB, Acting Director Health Outcomes) Peta Molloy (WDHB, Board Secretary) (Staff members who attended for a particular item are named at the start of the minute for that item) WELCOME: APOLOGIES: The Committee Chair opened the meeting with reflection and acknowledgement of the recent earthquake in the South Island. The Committee Chair also noted that Simon Bowen (Director of Health Outcomes) had been seconded to work on the Regional Long Term Investment Plan and that Karen Bartholomew was Acting Director of Health Outcomes. The Committee thanked Simon Bowen for his contributions. Resolution (Moved Lee Mathias /Seconded Jo Agnew) That apologies be received and accepted from Lester Levy, Warren Flaunty, Elsie Ho, Rev. Featunai Liuaana, Allison Roe, Robyn Northey and for early departure from Christine Rankin. Carried Waitemata District Health Board, Meeting of the Board 01/03/17 195
196 DISCLOSURE OF INTERESTS Sandra Coney advised that she was now a member of the Portage Licencing Trust. There were no declarations of interests relating to the agenda AGENDA ORDER AND TIMING Items were taken in the same order as listed on the agenda. 2. COMMITTEE MINUTES 2.1 Confirmation of Minutes of the Auckland and Waitemata DHBs Community and Public Health Advisory Committees Meeting held on 12/10/16 (agenda pages 7-13) Resolution (Moved Lee Mathias/Seconded Peter Aitken) That the Minutes of the Auckland and Waitemata District Health Boards Community and Public Health Advisory Committees Meeting held on 12 October 2016 be approved. Carried Matters Arising (agenda pages 14-15) The updates for the matters arising were noted. 3 INFORMATION ITEMS 3.1 Prevalence and management of diabetes (agenda pages 16-24) (Sarah Gray (Public Health Physician), Jagpal Benipal (Senior Programme Manager), Dr Catherine McNamara (Diabetologist) and Dr Allan Moffit (Clinical Director, ProCare Health) were present for this item. Dr Allan Moffit introduced the paper, matters that he highlighted included: That the report provides the Committees with an update on the prevalence and management of diabetes and that although there has been some issues with the accuracy of data collection, it is known that there are approximately 50,000 people with diabetes across the Auckland and Waitemata DHB districts. That it is important to note the disease is highest amongst Maori and Pacific (with Pacific at 15%) and Indian (11%) populations. That there is an increase in diagnoses of approximately 7% per annum That the recording of definitions by PHOs has been revisited and reset to ensure data accuracy; it is anticipated that accurate data reporting will commence in Noting the five work streams identified in the report (pages 21 to 24) being: systems redesign; clinical optimisation including care planning; self-management support and diabetes self-management education; workforce development and Mana Tu. Waitemata District Health Board, Meeting of the Board 01/03/17 196
197 Matters covered in discussion and response to questions included: That the emerging model of care will challenge the status quo; there has been work undertaken by professionals in the co-design space with people who have diabetes and a workshop was also held. Noting that steps are being taken to increase the quality of foot checks undertaken as part of a diabetic annual review within primary care. 5.2 The Committee Chair requested an update on the prevalence and management of diabetes also be provided to the Manawa Ora Committees. Ailsa Claire acknowledged the work of Dr Moffitt and the team. Resolution (Moved Lee Mathias/Seconded Jo Agnew) That the report be received. Carried 3.2 Auckland DHB Integrated Child and Youth Mental Health & Addictions Directions Update (agenda pages 25 to 54) Trish Palmer (Funder Mental health and Addictions and Chair of the Implementation Governance Group) presented this item. Matters covered in discussion and response to questions included: Noting that youth particularly engage with the use of e-tools and that the recent innovation with Spark has had a lot of uptake, but a low completion rate; this has led to an App being developed. That there has bene a small decline in youth suicide rates. That work is being undertaken to look at self-harm data and interventions in place in this area. That with regard to child health, a mental health programme update is in the early stages of development across the sector. Trish Palmer was thanked for this report. Resolution (Moved Tim Jelleyman/Seconded Max Abbott) That the report be received. Carried 3.3 Cervical Screening Update - Primary HPV screening (agenda pages 55 to 61) Dr Karen Bartholomew (Public Health Physician, Health Gain Team) presented this item. Matters covered in discussion and response to questions included: That with regard to rates of immunisation there was a good coverage for Maori and Pacific women with Auckland DHB have the highest rate nationally. Waitemata District Health Board, Meeting of the Board 01/03/17 197
198 Noting that the cervical screening rate as it stands has shown remarkable results, however, there was still an inequity gap. Karen Bartholomew was thanked for this report. 5.2 Resolution (Moved Max Abbott/Seconded Jo Agnew) That the report be received. Carried 4. STANDARD REPORTS 4.1 Planning, Funding and Outcomes Update (agenda pages 62 to 76) Dr Debbie Holdsworth (Director, Funding) and Aroha Haggie (Manager Maori Health Gain) summarised this item. Matters covered in discussion and response to questions included: That a programme of work is underway to determine the reasons for the decline rate for referral as part of the Raising Health Kids target. It was noted that it is a new programme. It was further noted that the importance of bringing awareness to health from preconception and earliest childhood is recognised. That a report will be provided to the Committees in 2017 providing an update and regional status on programmes such as Green Prescription, Active Families, Preschool Active Families and the like. The DHBs are in the process of going to market to retender these contracts. Resolution (Moved Judith Bassett/Seconded Peter Aitken) That the report be received. Carried 4.2 Primary Care Update (agenda pages 77 to 120) Tim Wood (Deputy Director and Funding and Development Manager - Primary Care, Waitemata and Auckland DHB) and Dr Stuart Jenkins (Clinical Director Primary Care) summarised this item. Matters covered in discussion and response to questions included: That with regard to system level measures, there is a baseline for each of the metro- Auckland DHBs. Clarification was sought on whether Auckland DHB separates acute bed days that are tertiary and secondary, this information will be provided by via to Lee Mathias. That with regard to PHO financial incentives, this was agreed when transitioning to system level measures. Waitemata District Health Board, Meeting of the Board 01/03/17 198
199 That with regard to the percentage of government funding for primary care practices, that analysis has been undertaken in the past and that funding amounts vary depending on the practice. Tim Wood and the team involved in this report were thanked. 5.2 Resolution (Moved Peter Aitken/Seconded Lee Mathias) That the report be received. Carried 5. GENERAL BUSINESS In response to a question about Auckland Localities and the ASH rate, Tim Wood noted that an update would be provided to the Committees at its next meeting. Dr Chris Chambers and Peter Aitken noted that this was their final meeting; the Committee Chair thanked them both for their contribution and commitment to the Committee. Sandra Coney also acknowledged the Committee Chair for her work over the past year. The Committee Chair thanked those present for their participation in the meeting. The meeting concluded at 3.42 pm. SIGNED AS A CORRECT RECORD OF A MEETING OF THE AUCKLAND AND WAITEMATA DISTRICT HEALTH BOARDS COMMUNITY AND PUBLIC HEALTH ADVISORY COMMITTEES HELD ON 23 NOVEMBER 2016 CHAIR Waitemata District Health Board, Meeting of the Board 01/03/17 199
200 6.1 Statement of Performance Expectations (SPE) Performance Report: Quarter 2, 2016/17 Recommendation: That the report be received. 6.1 Prepared by: Wendy Bennett (Planning and Health Intelligence Manager, Auckland and Waitemata DHBs) Endorsed by: Karen Bartholemew (Acting Director Health Outcomes, Auckland and Waitemata DHBs) and Simon Bowen (Director Health Outcomes) Glossary ARPHS CEO CVD DHB HAC HT POAC SIR SPE TB WIES YTD - Auckland Regional Public Health Service - Chief Executive Officer - Cardiovascular disease - District Health Board - Hospital Advisory Committee - Health Target - Primary Options for Acute Care - Surgical intervention rate - Statement of Performance Expectations - Tuberculosis - Weighted Inlier Equivalent Separation - Year-to-date 1. Introduction The Board has requested regular reporting of the indicators in the Statement of Performance Expectations (SPE) that makes up a key component of the Annual Plan. Measures within the SPE (Module 3 of the Annual Plan) represent the outputs/activities we deliver to meet our goals and objectives in the first two modules of the Annual Plan, and also provide a reasonable representation of the vast scope of business-as-usual services provided, using a small number of cornerstone indicators. Performance measures are concerned with the quantity, quality and the timeliness of service delivery. Actual performance against these measures is reported in the DHB s Annual Report, and audited at year end by the DHB s auditors, AuditNZ. Many of the indicators included in the SPE are currently reported via other scorecards/reports to Board and Board Committees. Therefore, this report excludes variance reported elsewhere for indicators included in other reports. This report also excludes indicators for which data is only available annually. This report represents the first SPE report to the Board. Auckland DHB has met the majority of SPE indicator targets in Prevention Services (Output Class 1) and Rehabilitation and Support Services (Output Class 4). We continue to focus on our performance in Early Detection and Management (Output Class 2) by working with our Primary Care partners to improve service. In the Intensive Assessment and Treatment (Output Class 3) indicators, we note that all of our quality and patient safety indicators are on track; our key area of focus is orthopaedic waiting times. Waitemata District Health Board, Meeting of the Board 01/03/17 200
201 How to interpret the scorecards Traffic lights For each measure, the traffic light indicates whether the actual performance is on target or not for the reporting period (or previous reporting period if data are not available as indicated by the grey bold italic font). 6.1 Measure description Traffic light Trend indicator Actual Target Trend Better help for smokers to quit - hospitalised 98% 95% The colour of the traffic lights aligns with the Annual Plan: Traffic light Criteria: Relative variance actual vs. target Interpretation On target or better Achieved % achieved 0.1 5% away from target Substantially Achieved % away from target AND Not achieved, but progress %*achieved improvement from last month made % away from target, AND no <94.9% achieved improvement, OR >10% away from target Not Achieved Exception: Cardiac arrest calls is Green if number 1, Blue if =2, Amber if =3 and Red if 4 Trend indicators A trend line and a trend indicator is reported against each measure. Trend lines represent the actual data available for the latest 12-months period. All trend lines use auto-adjusted scales: the vertical scale is adjusted to the data minimum-maximum range being represented. The small data range may result in small variations appearing to be large. Note that YTD measures (e.g., WIES volumes, revenue) are cumulative by definition. As a result their trend line will always show an upward trend that resets at the beginning of the new financial year. The line direction is not necessarily reflective of positive performance. To assess the performance trend, use the trend indicator as described below. The trend indicator criteria and interpretation rules: Trend indicator Rules Interpretation Current > Previous month (or reporting period) performance Improvement Current < Previous month (or reporting period) performance Decline Current = Previous month (or reporting period) performance Stable By default, the performance criteria is the actual:target ratio. However, in some exceptions (e.g., when target is 0 and when performance can be negative (e.g., net result) the performance reflects the actual. Look up for scorecard-specific guidelines are available at the bottom of each scorecard: Key notes 1. Most Actuals and targets are reported for the reported month/quarter (see scorecard header). 2. Actuals and targets in grey bold italics are for the most recent reporting period available where data is missing or delayed. 3. Trend lines represent the data available for the latest 12-months period. All trend lines use auto-adjusted scales: the vertical scale is adjusted to the data minimum-maximum range being represented. Small data range may result small variations perceived to be large. a. ESPI traffic lights follow the MoH criteria for funding penalties: ESPI 2: the traffic light will be green if no patient is waiting, blue if greater than 0 patients and less than or equal to 10 patients or less than 0.39%, and red if 0.4% or higher. ESPI 5: the traffic light will be green if no patient is waiting, blue if greater than 0 patients and less than or equal to 10 patients or less than 0.99% and red if 1% or higher. Waitemata District Health Board, Meeting of the Board 01/03/17 201
202 SPE scorecard: Q2 2016/17 Statement of Performance Expectations Quarter /17 December 2016 Output Class 1: Prevention Services Health Promotion Actual Target Trend Acute services Actual Target Trend Better help for smokers to quit - hospitalised 98% 95% Number of ED attendances (YTD) 58,772 Better help for smokers - Primary Care 89% 90% Total acute WIES (DHB Provider - YTD) 31,104 30,224 Better help for smokers - Maternity 89% 90% Shorter Waits in ED 97% 95% Raising Healthy kids 100% 70% Faster cancer treatment - within 62 days 90% 85% Green Prescriptions - adults 3,593 3,644 % of eligible stroke patients thrombolysed 7% 6% % of stroke patients admitted to stroke unit 83% 80% Health Protection (ARPHS - all northern region DHB results) Coronary angiography in 3 days (ACS patients) 68% 70% Tobacco retailer compliance checks conducted (YTD) % of TB treatments with start date 100% 85% Maternity Number of births in Waitemata DHB hospitals (YTD) 3,690 Population based screening % primiparous vaginal births with 3rd/4th degree tears 3.0% Breast screening coverage 67% 70% Bowel screening - participation (round 3) 54% 60% Elective (inpatient/outpatient) Bowel screening - colonoscopy within 55 days 98% 95% HT: elective surgical discharges 105% 100% Gateway assessments waiting over timeframe 2 0 Surgical intervention rates (SIR) - joints Percentage of B4 School Checks completed (YTD) 47% 45% SIR - cataracts SIR - cardiac Output Class 2: Early Detection and Management SIR - PCR SIR - angiogram % urgent diagnostic colonoscopy in 14 days 98% 85% Primary health care Actual Target Trend % non-urgent diagnostic colonoscopy in 42 days 77% 70% Primary care enrolment 92% 95% % waiting > 4 months for their FSA Compliant POAC Referrals YTD % waiting > 4 months for their treatment Compliant Increased immunisation (8-month old) 92% 95% Cervical Screening 76% 80% Quality and patient safety (HQSC) Diabetes management 68% 69% HSMR (Source: Health Round Tables) CVD on Triple therapy 54% 56% Percentage of opportunities for hand hygiene taken 86% 80% % CVD risk assessed in last 5 years 91% 90% Older patients assessed for risk of falling 98% 90% Hip & Knee operations with prophylactic antibiotic given 92% 95% Community referred testing and diagnostics Staph bacteraemia rate per 1,000 inpatient bed days 0 GP referred radiological tests 18,673 15,438 Net Promoter Score FFT % CTs completed within 6 weeks 99% 95% % of falls risk patients received an individualised care plan 95% 80% % MRIs completed within 6 weeks 95% 85% Rate of falls with major harm 0.1 <2 % of hip & knee procedures given right antibiotic in right dose 100% 95% Output Class 4: Rehabilitation and Support Services Output Class 3: Intensive Assessment and Treatment % hip/knee procedures given appropriate skin preparation 100% 100% Surgical site infections per 100 hip and knee operations 0.00 <1.3 Number of pressure injuries grade 3 & 4 - Provider Arm 0 0 Home-based support Actual Target Trend Number of patients with pressure injuries per 100 patients Average no.hours per month of HBSS for personal care 74,503 Average no.hours per month of HBSS for household mgmt 16,153 Mental health Long term support 65+ who have had interrai 97% 75% Mental health service access % 3.1% % urgent InterRAI assessed in 5 working days 71% Mental health service access % 3.4% % non-urgent InterRAI assessed in 15 working days 30% Mental health service access % 2.1% 0-19 Mental Health waiting within 3 weeks 60% 80% Palliative Care 0-19 Mental Health waiting within 8 weeks 85% 95% Number of contacts (YTD) 7, Addictions waiting within 3 weeks 88% 80% Proportion of hospice patient deaths that occur at home 34% 0-19 Addictions waiting within 8 weeks 97% 95% Proportion of referrals that wait >48 hours for a hospice bed 5% 6.1 Residential Care ARC providers with 4 year audit certification 23% How to read Performance indicators: Trend indicators: Achieved/ On track Substantially Achieved but off target Performance improved compared with previous quarter Not Achieved but progress made Not Achieved/ Off track Performance declined compared with previous quarter Performance was maintained The triple therapy target published in the 2016/17 Annual Plan (55%) has been superceded by the SLM Plan target Key notes A Question? Waitemata District Health Board, Meeting of the Board 01/03/17 202
203 Output Class 1: Prevention Services Scorecard Variance Report Indicator On target Variance commentary Health promotion 1. Better help for smokers to quit In CEO, HAC reports hospitalised 2. Better help for smokers to quit Primary In CEO, Primary Care reports Care 3. Better help for smokers to quit In CEO report maternity 4. Raising Healthy Kids In CEO report 5. Green Prescription adults Health protection (ARPHS all northern region DHB results) 6. Tobacco retailer compliance checks conducted (YTD) 7. % of TB treatments with start date Population-based screening 8. Breast screening coverage In CEO report 9. Bowel screening participation (round In CEO report 3) 10. Bowel screening colonoscopy within 55 days 11. Gateway assessments waiting over In HAC report timeframe 12. % of Before School Checks completed (YTD) 6.1 Output Class 2: Early Detection and Management Scorecard Variance Report Indicator On target Variance commentary Primary health care 13. Primary care enrolment In Primary Care report 14. POAC referrals YTD 15. Increased immunisation (8-month old) In CEO report 16. Cervical screening In CEO report 17. Diabetes management In Primary Care report 18. CVD on triple therapy 19. % CVD risk assessed in the last 5 years Community-referred testing and diagnostics 20. GP-referred radiological tests 21. % CTs completed within 6 weeks In CEO, HAC reports 22. % MRIs completed within 6 weeks In CEO, HAC reports Waitemata District Health Board, Meeting of the Board 01/03/17 203
204 Output Class 3: Intensive Assessment and Treatment Scorecard Variance Report Indicator On target Variance commentary Acute services 23. Number of ED attendances (YTD) No set target 24. Total acute WIES (DHB Provider YTD) In HAC report 25. Shorter Waits in ED In CEO, HAC reports 26. Faster Cancer Treatment within 62 In CEO, HAC reports days 27. % of eligible stroke patients thrombolysed 28. % of stroke patients admitted to stroke unit 29. Coronary angiography in 3 days (ACS patients) Maternity 30. Number of births in Waitemata DHB hospitals (YTD) 31. % primiparous vaginal births with third/fourth degree tears No set target Elective (inpatient/outpatient) 32. HT: elective surgical discharges In CEO, HAC reports 33. Surgical intervention rates (SIR) joints In CEO report 34. SIR cataracts In CEO report 35. SIR cardiac 36. SIR PCR 37. SIR angiogram In CEO report 38. % urgent diagnostic colonoscopy in 14 In CEO, HAC reports days 39. % non-urgent diagnostic colonoscopy in In CEO, HAC reports 42 days 40. % waiting >4 months for their FSA (ESPI In CEO, HAC reports 2) 41. % waiting >4 months for their treatment In CEO, HAC reports (ESPI 5) Quality and patient safety (HQSC) 42. Hospital standardised mortality ratio In CEO report 43. % of opportunities for hand hygiene In HAC report taken 44. Older patients assessed for risk of falling In CEO, HAC reports 45. Hip and knee operations with prophylactic antibiotic given 46. Staph bacteraemia rate per 1,000 inpatient bed days 47. Net Promoter Score FFT In CEO report 48. % of falls risk patients received an individualised care plan 49. Rate of falls with major harm In HAC report 6.1 Waitemata District Health Board, Meeting of the Board 01/03/17 204
205 Indicator On target Variance commentary 50. % of hip and knee procedures given appropriate skin preparation 51. Surgical site infections per 100 hip and knee operations 52. Number of pressure injuries grade 3 and In CEO, HAC reports 4 Provider Arm 53. Number of patients with pressure In Quality report injuries per 100 patients Mental health 54. Mental Health service access 0-19 In HAC report 55. Mental Health service access In HAC report 56. Mental Health services access 65+ This population has increased. We are pursuing additional inpatient beds and developing closer links with Primary Care as outlined in the Our Health in Mind programme Mental Health waiting within 3 In HAC report weeks Mental Health waiting within 8 weeks Addiction waiting within 3 weeks Addiction waiting within 8 weeks Relocation of the North CAMHS affected efficiencies; we anticipate improved performance once full service delivery resumes at the new facility 6.1 Output Class 4: Rehabilitation and Support Services Scorecard Variance Report Indicator On target Variance commentary Home-based support 61. Average number of hours per month of HBSS for personal care No set target 62. Average number of hours per month of HBSS for household management No set target 63. Long-term support 65+ who have had InterRAI 64. % urgent InterRAI assessed in 5 working days 65. % non-urgent InterRAI assessed in 15 working days Waitemata District Health Board, Meeting of the Board 01/03/17 205
206 Indicator On target Variance commentary Palliative care 66. Number of contacts (YTD) No set target 67. Proportion of hospice patient deaths that occur at home 68. Proportion of referrals that wait >48 hours for a hospice bed Residential care 69. ARC providers with 4-year audit certification The 40% baseline (2015/16) was set prior to a definition change, which now excludes patient deaths occurring at high- and lowlevel residential aged care (21% and 0%, respectively, in Q2) 6.1 Waitemata District Health Board, Meeting of the Board 01/03/17 206
207 6.2 Health and Safety Marker Report update March 2017 Recommendation: That the report be received. Prepared by: Fiona McCarthy (Director Human Resources) 6.2 Purpose of report The purpose of this report is to provide an update on progress towards meeting the expectations of the Health and Safety at Work Act 2015, which came into effect on 4 April Executive Summary The new Health and Safety at Work Act 2015 came into force on 4 April The new legislation is the result of work from the health and safety taskforce established in 2012 to evaluate whether the workplace and safety system in New Zealand was fit for purpose, and to recommend practical strategies for reducing the high rate of workplace fatalities and serious injuries by From taskforce recommendations made in 2013, WorkSafe NZ was established with one goal to reduce workplace deaths and injuries by 25% by The DHB has been working on key aspects of the legislation specifically those around employee participation and engagement and work with PCBUs where we share accountability and procurement processes. While updating key policy and work methods, the DHB continues to have an active programme in place to measure and mitigate any resulting or residual risks. To monitor our compliance a number of deep dive audits are scheduled for 2016/17, as well as the roll out of the safe way of working self-audit tool. A summary of our compliance with the Act is outlined below and details are outlined in Appendix 1. Key High complies substantially or fully with Act Good some actions to be completed Low significant or some key actions to be completed Topic Level of Outstanding actions performance 1. Policy High Safe way of working self-audit and internal audits to identify any policy/process actions 2. Worker engagement, participation and representation Good Region work participation agreement still in discussion. Final training framework being finalised. 3. Notifiable events High 4. Health and Safety Committee High 5. Orientation Good Orientation systems for contractors, volunteers and students being updated or reviewed. Waitemata District Health Board, Meeting of the Board 01/03/17 207
208 Topic Level of Outstanding actions performance 6. Risk Management High Investigation processes currently being reviewed. 7. Contractors (Facilities, Health Low Work across a number of topics is underway Alliance and Information Technology) 8. Hazardous substances Low High use areas accounting for 80% of chemicals currently under audit however over 300 sites still to be completed. This is a three year piece of work. 9. Health of workers Low Comprehensive health monitoring plan in development. 10. Equipment and Maintenance To be determined Deep dive audit on essential services and infrastructure maintenance underway. 11. Training Good Health and safety training in place but key components being reviewed. 12. Audits High Safe way of working self-audit currently being rolled out across the DHB. 6.2 Deep dive audits scheduled for 2016/17: Health and safety incident investigation (audit complete) Essential services and maintenance of equipment, machinery and infrastructure (audit underway) Review of approach and controls in relation to the Waitemata DHB high accident types. The high accident types are: o Aggression o Moving and handling o Slips, trips and falls Community services risk and controls 13. Reporting Good A health and safety scorecard to allow access to regular reporting is in development. 14. Resources Good Some roles still in recruitment. Waitemata District Health Board, Meeting of the Board 01/03/17 208
209 2. Glossary PCBU person conducting a building or undertaking, and has a primary duty of care to ensure the health and safety of workers. The DHB is the PCBU. Officers - Includes Board Directors and the Senior Management team who make governance decisions that significantly affect the business. Officers have a duty of due diligence to ensure their business complies with its health and safety obligations. Officers may be found guilty of an offence under the Act, in addition to the PCBU. 6.2 Due Diligence taking steps to acquire and keep up to date knowledge of health and safety matters. Gain an understanding of the business and hazards and risk associated with that business. Ensure PCBU has available and uses appropriate resources and processes to manage risk. Ensure PCBU has appropriate processes for considering incidents, hazard and risks in a timely way. Ensure PCBU implements processes for complying with obligations under the Act, validates the provision and use of resources and processes to comply with obligations under the Act. Workers - Workers have a duty to take reasonable care for their own safety and that their own actions do not adversely affect the safety of others. They need to comply with reasonable health and safety instructions from the PCBU and co-operate with health and safety policies and procedure. Workers are people who work at the DHB and include employees, contractors, sub-contractors or their employees, apprentices, trainees, persons gaining work experience, employees of a labour hire company and volunteers. Other people - People who come to the workplace such as visitors or customers also have duties to comply with health and safety processes. Our patients and visitors are in this group. Notifiable injury or illness an injury or illness that requires immediate treatment (i.e. amputation, serious burn, serious head injury or burn), admission to hospital, serious infection and medical treatment within 48 hours of exposure. All notifiable injuries or illnesses are to be reported to WorkSafe NZ. Notifiable incident - an incident that is an unplanned or uncontrolled incident in a workplace and that exposes a worker or other person to a serious risk to health and safety. Notifiable incidents include events such as: a spillage or leak of a substance; explosion or fire; escape of gas or steam; falls; electric shocks; structural collapses; in rush of water, gas or mud; interruption of underground ventilation. All notifiable instances are to be reported to WorkSafe NZ. Health and Safety Representative - a person elected to represent the workers in relation to health and safety matters. The representative has specific functions and roles under Schedule 2 of the Act. Waitemata District Health Board, Meeting of the Board 01/03/17 209
210 Appendix 1 Progress implementing the Health and Safety at Work Act Policy The DHB policies have been reviewed and are aligned to the new legislation. Changes and updates to policy will occur over the next few years as new regulations, audits and experimental learnings lead to new processes. Significant policy changes will be endorsed by the Board Worker engagement, participation, and representation What the Act says How do we comply? A PCBU must: Initiate election of health and safety representatives on request of workers. Agree the work groups that are represented by a health and safety representative. Consult about matters related to health and safety Provide information as requested with due consideration to the Privacy Act Allow a health and safety representative time to discharge their powers under the act New regulations on worker engagement, participation and representation were introduced in February 2016 and outline the functions, number, training, powers and participation expectations of health and safety representatives. We have 307 health and safety representatives throughout the business, most of whom have baseline health and safety representative training, as endorsed by WorkSafe NZ as well as divisional health and safety committees in place to provide ways to participate in local issues. In addition, the annual update of hazards is reviewed by representatives, and representatives participate in the self-assessed departmental health and safety audit. Representatives also undertake DHB wide health and safety activity such as flushing low use water outlets. Seven health and safety representatives sit on our health, safety and wellbeing committee. Transition training for representatives has been provided and foundation health and safety training is available online. What is outstanding? The regional employee participation agreement between the Northern Region DHBs and unions has not yet been signed by the Unions. We are working with the national bipartite group on an agreed way to include other PCBUs (e.g. compass and health alliance) in the agreement. Ongoing training needs (as part of the new Worker Engagement, Participation and Representation Regulations) are being assessed following the completion of a special project led by Margaret Kamphuis, Specialist Health and Safety Advisor. We are currently working with the metro DHBs to look at region wide representative structures and training. Waitemata District Health Board, Meeting of the Board 01/03/17 210
211 Consequences 3. Notifiable events What the Act says How do we comply? What is outstanding? Consequences Meeting with on-site contractors to establish health and safety representatives and discuss health and safety matters together are commencing. There are fines for not having appropriate employee participation processes in place. A PCBU must Report on notifiable injury, illness and incidents as soon as possible after being made aware of them. Secure a site if a notifiable event has occurred. Keep a record of notifiable events We currently have notifiable event reporting and recording processes in place. There are no outstanding actions, although we note that some of the actions in point 6 will benefit the notifiable event review process. There are fines for not notifying workplace injury or illness as soon as possible after being made aware of them Health and Safety Committee What the Act says How do we comply? What is outstanding? Consequences A PCBU must: Put in place a health and safety committee if requested by a worker. Establish a health and safety committee within two months of this request. Consult about health and safety matters with the committee. Allow time for members to attend and carry out functions as a member of the committee. Provide information to the committee Within a reasonable time, adopt recommendations made by the committee. A PCBU can also establish a Health and Safety Committee on its own initiative. The DHB has an organisation wide Health, Safety and Wellbeing Committee. There are no outstanding actions. There are fines for not setting up a Health and Safety Committee if requested, and if a PCBU does not: allow time for members to attend committee meetings/consider matters raised at the committee; or if a PCBU does not implement recommendations from the committee. 5. Orientation What the Act says How do we comply? Orientation to a workplace is an important part of complying with the duty of care to ensure the provision and maintenance of a workplace that does not give rise to health and safety risks. Pre commencement orientation and a safety first video are now in use for orientation, training and general health and safety messaging. A departmental health and safety induction checklist is sent to recruiting managers. Waitemata District Health Board, Meeting of the Board 01/03/17 211
212 What is outstanding? Consequences 6. Risk Management What the Act says How do we comply? We need to put an Officer orientation programme in place due March. We need to check orientation processes for students and volunteers and a review of DHB health and safety training (inclusive of students and volunteers) is almost complete and orientation needs will be reviewed as part of the current scoping to put DHB orientation resources on line. There are fines and criminal punishments of imprisonment for reckless conduct in respect to duty of care, and fines for failing to comply with risks that expose individuals to death or serious injury/illness. PCBUs have a duty of care to ensure the health and safety of another person is not put at risk from work carried out as part of the conduct of the business or undertaking. Risks must be eliminated or minimised so that a PCBU can, in so far is reasonably practicable: Provide a workplace without risk Provide and maintain safe systems, plant and structures Ensure the safe handling, storage and use of plants, substances and structures Provide training or supervise to protect persons from risk Maintain accommodation so a worker is not exposed to risk We have an online hazard management system where hazards are identified and controls recorded. This is complemented by a corporate risk register where service, division and organisation wide health and safety risks are also recorded, controlled and regularly reviewed. Hazards/Risks are reviewed every 12 months by the divisional lead manager and Health and Safety Representatives. Waitemata 2025 design and works impact meetings are occurring. Processes to monitor and maintain operational compliance are in place, i.e., fire management plan, training, exercises, maintaining clear egress, etc., and are part of a current process improvement review. Entrance ways have signage to indicate they may be slippery when wet. On wet days, additional signage is displayed to alert patients, staff, visitors, contractors to potential slip, trip and fall hazards. This expectation is audited. CCTVs are active in appropriate places on and around our sites. A hazard and security risk assessment tool is being piloted in Community and inpatient Mental Health settings. Asbestos surveys are ongoing. Regular on site campus audit criteria is drafted and in process of being validated. Resource will then be assigned to start the audits. 6.2 Waitemata District Health Board, Meeting of the Board 01/03/17 212
213 What is outstanding? Consequences Confirmation of investigation methodology due December. Following our first deep dive audit on incident investigations, an investigation method, process and training is being developed and is due for release in March. There are fines and punishments of imprisonment for reckless conduct in respect to duty of care, and fines for failing to comply with risks that expose individuals to death or serious injury/illness Contractors (Facilities, Health Alliance and Information Technology) What the Act says How do we comply? The PCBU, as well as ensuring the health and safety of its employees (workers), is also required to ensure the health and safety of other workers, as well as ensuring that plant, fixtures and fittings are without risks to health and safety of any person. There are new asbestos regulations that require a change in how PCBU s currently manage and remove asbestos. Selection of Contractors: The DHB has moved to a process of selecting a panel of preferred contractors who can tender for DHB construction and refurbishment work as it arises. Each main contractor has to first qualify to be a part of the panel by satisfactorily completing contractor health and safety questionnaire which allows the organisation to demonstrate their performance against 12 health and safety criteria. Maintenance contractors do not have a preferred supplier arrangement in place as yet but contracts are in place and current for main contractors. Supplier Contracts and RFP processes: DHB contracts provide a standardised health and safety statement for minor or individual contracts. This clause is confirmed as satisfying the Act. Health Alliance procurement processes: Documentation is not adequate for the new Act. Orientation: Construction contractor induction is in place and completed prior to gaining access to the relevant site. Site access: All building contractors must report to Facilities before commencing their work and all Health Alliance (ha) staff (IT) will report to security. In addition, New projects must be agreed and coordinated with Facilities prior to commencing New contractors must complete induction prior to starting work A contractor carrying out an agreed task e.g. for call out that does not need to be reported to Facilities prior they do need to report to area supervisor prior to and post work. All contractors must have a Waitemata DHB photo ID which will only be issued after completing induction) All healthalliance staff and contractors are required to have healthalliance issued photo identification on them at all times and visible. Usually if they are based on a particular site on a regular basis (i.e. not just visiting) then we will request a security access card with photo ID for that staff member from the site. Facilities: Once inducted, contractors working for Facilities are issued with a Waitemata DHB ID card with a photo. Proof of identification (passport/ drivers licence) is required to obtain this ID. The duration of the ID card can be set to cover the estimated time of the project. Waitemata District Health Board, Meeting of the Board 01/03/17 213
214 What is outstanding? On the job: Toolbox meetings occur on a scheduled basis. There is active management and collaboration with architects and designers to meet design expectations and requirements. Work impact meetings to assess risk occur regularly and ensure contractor health and safety plans are implemented. All Project managers, including the 2025 team are Site Safe certified. Regular meeting with construction contractors are occurring. Asbestos: Asbestos register is in place and is updated as new surveys are completed. Corrective actions are being implemented to mitigate identified hazards. Asbestos management plans are being developed and implemented. This work is being led by the Waitemata DHB Asbestos Management Group. Incidents and Accidents: Reporting of incidents and accidents follow the DHB process. Contractors experiencing any accident or incident are required to notify the DHB, investigate and report back any findings. On site audits: Regular external audits are conducted for construction site work. Project managers also undertake audits of their projects. Orientation: Induction material is in place. On the job: A pre start safety meeting process is in development for all build projects, as well as ensuring work impact meetings occur regularly during the project. Safety in design guidance is in development. Accidents and Incidents: Facilities adopted an ICAM concept of investigation that will identify why things went wrong and what actions are required to ensure compliance and keep workers safe. Records gained through incident reviews, audits and investigations are saved as confirmation of active management by the DHB in its role as the PCBU. Maintenance work review and sign off: For IT project work related to moves and new fit-outs, the desktop team work closely with the Waitemata DHB Project Manager who reviews and signs-off that the work is complete. Building project health and safety management and sign off: A performance review is done mid-way through each major building project. Health and Safety design sign off and pre-occupation processes are complete. The building sign off process follow the relevant policy. Post Implementation Reviews (PIRs): PIRs are done for each facility build project and results provided to the contractor selection panel. Selection of contractors: The DHB is moving to the same preferred supplier process for maintenance contractors as noted above for large construction contractors. This process will be in place by June Waitemata DHB maintenance team requires contractors to provide suitable prequalification material by a certain date. If not met the contractor will be removed from the approved contractor list. health Alliance processes: The DHB is working with health Alliance about site orientation, safety and procurement processes Asbestos: To complete the development of asbestos management plan in line with new regulations. Maintenance work review and sign off: The DHB is currently sharing learning from ADHB on a task planning and sign off process for maintenance work, ensuring competent review and management oversight. Building project health and safety management and sign off: Complete implementation of project sign off documentation. 6.2 Waitemata District Health Board, Meeting of the Board 01/03/17 214
215 Consequences Meetings: Put in place regular meetings with maintenance contractors There are fines and punishments of imprisonment for reckless conduct in respect to duty of care, and fines for failing to comply with risks that expose individuals to death or serious injury/illness. 8. Hazardous substances What the Act says A PCBU has a primary duty of care to provide for staff use, handling and storage of substances. 6.2 How do we comply? The DHB is also required to comply with the Hazardous Substances and New Organisms Act 1996 which requires the DHB to prevent and manage adverse effects of hazardous substances and new organisms. The DHB has focused on the 33 areas with high volume use of hazardous substances, with 340 substances identified and added to the online register of substances available on StaffNet. A new and comprehensive HSNO policy has also been developed and published on the intranet, with a strong focus on roles and responsibilities. The Intranet HSNO site now contains hot links to information covering: Policy document Full HSNO database of all hazardous substances identified, including constituents, product state, UN number, CAS number, identified hazards, exposure limits, HSNO class and PPE specific to each substance. Master Material Safety Data Sheets (MSDS) repository Wastewater Disposal Guidelines Training resources, including introductory PowerPoint List of all Approved Handlers and their locations Emergency response requirements Specific spill kit contents list Managers responsibilities Key contacts for staff Approved handler training has been delivered for high risk areas. What is outstanding? Consequences Work has also concluded with healthalliance, to ensure that Material Safety data Sheets are supplied for all new chemicals being procured. We have another estimated 350 areas to review but a comprehensive audit of the 33 high risk areas are underway. The business case for the construction of a Hazardous Substances Store for Waitakere Hospital is now out for tender. The construction of this store will greatly reduce the risk associated with the bulk storage and disposal of hazardous substances at Waitakere Hospital. There are fines and punishments of imprisonment for reckless conduct in respect to duty of care, and fines for failing to comply with risks that expose individuals to death or serious injury/illness. It is worth noting that hazardous substances are covered under three sets of national legislation, as well as local bylaws (Health and Safety at Work Act 2015, Hazardous Substances and New Organisms (HSNO) Act 1996, Resource Management Act 1991 and Auckland Council s Water Supply and Wastewater Bylaw ), under all of which fines can be payable. Waitemata District Health Board, Meeting of the Board 01/03/17 215
216 9. Health of workers What the Act says How do we comply? A PCBU must ensure that the health of workers and conditions of the workplace are monitored for the purpose of preventing injury or illness. The PCBU must, as far as reasonably practicable, maintain accommodation so that the worker is not exposed to risks to health and safety. The DHB has pre-employment screening in place however a number of staff still commence work pending their results. A pilot is underway to trial a process to ensure that staff cannot start until the health screening process is complete, results known, vaccinations or other actions are complete and the potential employee is fit for work or an offer is withdrawn if they are not fit to work. We undertake occupational health monitoring via our Occupational Physician health clinics and have now extended this to monitoring exposure to noisy areas (facilities), hazardous substances, laser care, and other risk areas. Monitoring for exposure for radiation (Radiology, Cardiac Catheter Lab) occurs externally. We provide free influenza and other vaccinations. A stocktake of issues with workplace heating, ventilation and cooling was completed in May 2015 and is being implemented in priority order. Areas with friable asbestos require additional security clearance to gain access. Containers for sharps, hazardous materials and substances are provided on each site. Staff are provided with personal protective equipment (PPE) to wear. PPE requirements are outlined in various policies including the hazardous substances register, use of lasers, gloves, etc. Infection control processes are in place to manage any disease outbreaks and exposure. Installation of signage close to potential slip, trip and fall hazards has occurred and cleaner are asked to regularly monitor wet areas. Regular communication on hazards is issued. New for March 2017 Influenza planning for 2017 is well underway with vaccine ordered, final vaccinator training being signed off, communications being drafted and patient vaccination protocol being developed. The safe way of working audit tool has completed its pilot at Mason and the audit tool is now being rolled out across the DHB. 6.2 Waitemata District Health Board, Meeting of the Board 01/03/17 216
217 What is outstanding? Consequences Health monitoring programmes should be in place across all relevant risk areas. An audit on use of PPE will be planned as part of the health monitoring programme to validate the application of various policies and risk controls due June There are fines and punishments of imprisonment for reckless conduct in respect to duty of care, and fines for failing to comply with risks that expose individuals to death or serious injury/illness Equipment and Maintenance What the Act says How do we comply? A PCBU must provide and maintain a work environment that is without risk to health and safety. Equipment that is broken is escalated for capital replacement as relevant. A register of capital assets is in place and being added to, to ensure that equipment is budgeted for replacement according to the life span of that equipment. All bio-medical equipment is maintained by the Bio-Engineering team A fast track process is in place to approve maintenance triggered for health and safety reasons. A Board approved funding pool for major Health and Safety purchases has been accrued for activation by the Chief Financial Officer as relevant. What is outstanding? Consequences New for March 2017 Work on updating the helipad area (i.e. safety zone painting, visual and audio alarms and pedestrian crossing) and implementing loading dock safety measures (e.g. safe walkways and barriers) will commence in April on appointment on a project manager. Alert systems for community workers have completed their RFP and applications are being reviewed. There are fines and punishments of imprisonment for reckless conduct in respect to duty of care, and fines for failing to comply with risks that expose individuals to death or serious injury/illness. 11. Training What the Act says How do we comply? A PCBU must provide any information, training, instruction and supervision necessary to protect all persons from risks to health and safety arising from work carried out by the DHB. Orientation training is provided to staff pre commencement and within the first four weeks of their employment. Health and Safety representatives are provided with two days of training (Four half day modules) by the Occupational Health and Safety Service covering an introduction to health and safety management, hazard and emergency management, accidents and occupational rehabilitation, safe working procedure, health and wellbeing and the new legislation. All staff are required to complete the annual health and safety update online. Waitemata District Health Board, Meeting of the Board 01/03/17 217
218 Training is provided on departmental specific instances such as moving and handling in patient areas, crisis intervention in areas where aggressive clients may be experienced, calming and restraint in mental health services, laser care in theatre, handling sharps by infection prevention and control. As already noted, approved handler training is in place for hazardous substances. Training is provided on how to access our incident management, risk register and hazard register systems. 6.2 Training for notifiable events is complete. Emergency Response Training occurs regularly Fire Response and Evacuation Training occurs for all new staff and annually online and face to face in key areas Fire Evacuation Training occurs across all DHB areas six monthly which means each week there are activities in order to cover all areas Warden Training occurs on all sites annually for all wardens and deputy wardens. This is for all areas so requires multiple sessions annually Duty Nurse Manager training occurs for all new staff and three times a year Incident Management Team training occurs quarterly Key staff are required to attend Health CIMS2 training which is available monthly and is done as a regional programme with the other DHBs. This is open to all health settings including PHO s Accident and Medical centres and Residential Aged Care key staff Key staff attend CIMS4 training quarterly The DHB runs particular Health CIMS4 training with a provider twice a year for key areas that have identified a need. Board and Senior Management training on health, safety and wellbeing is due December. New for March 2017 ADHB wide health and safety training stocktake is complete and we are reviewing training gaps for recommendation to the Senior Management team in April What is outstanding? Consequences The first analysis of the security training framework has been reviewed and accepted and a detail business case is currently underway. The training framework for security is currently being reviewed. A DHB wide training framework is being developed to enable officers and workers to increase awareness and knowledge of health and safety systems and processes. There are fines and punishments of imprisonment for reckless conduct in respect to duty of care, and fines for failing to comply with risks that expose individuals to death or serious injury/illness. Waitemata District Health Board, Meeting of the Board 01/03/17 218
219 12. Audits What the Act says How do we comply? What is outstanding? Consequences 13. Reporting What the Act says How do we comply? What is outstanding? Consequences An Officer of a PCBU must verify the provision and use of resources and processes put in place by the DHB. Since early 2015 we have completed a number of readiness audits to access compliance with the new health and safety legislation and to assess new or different resources needed. Going forward the Northern region has agreed to undertake two audits during which includes community workers and contractor management. Regular external audits of contractor sites are in place. A governance audit has just been completed with five corrective actions. An audit programme for 2016/2017 has been agreed with Internal audit and includes deep dive audits on essential service maintenance, investigation processes and feedback loops, contractor management, community safety, governance assurance, efficacy of works to improve our three top accident types, and environmental controls. New for March 2017 The first deep dive for 2016/17 has been completed for incident investigations with 16 corrective actions, some of which are complete and the rest due for completion March June The safe way of working audit tool is currently being rolled out. There are no outstanding actions. There are fines and punishments of imprisonment for reckless conduct in respect to duty of care, and fines for failing to comply with risks that expose individuals to death or serious injury/illness. An Officer of a PCBU must ensure they acquire and keep up to date on health and safety matters. Monthly reports on health and safety matters are provided to the Board meeting and the Audit and Finance Committee meeting. In time reporting will incorporate feedback from the organisational Health, Safety and Wellbeing committee. A new Board Health and Safety Reporting format has been in place since November The DHB will focus on trend drivers in future reporting to give Board members a view on what impacts our health, safety and wellbeing performance. There are fines and punishments of imprisonment for reckless conduct in respect to duty of care, and fines for failing to comply with risks that expose individuals to death or serious injury/illness. 6.2 Waitemata District Health Board, Meeting of the Board 01/03/17 219
220 14. Resources What the Act says How do we comply? What is outstanding? Consequences An Officer of a PCBU must verify the provision and use of resources and processes put in place by the DHB. A resource review was completed last year. Recommended actions were tabled to the Board in August. On review of the report we have already implemented the following new resource: 0.4 training FTE to an existing Health and Safety adviser role Hazardous substances co-coordinator (1 FTE) Health monitoring nurse specialist (1FTE fixed term for two years) Health and Safety advisor (1FTE) so we can spread training across the advisory team and allow advisors to have service portfolios for in service outreach, advice, training and assistance Health and Safety Manager has been employed by Facilities and Development. (1FTE) And the following are due to be recruited Investigator/auditor (1FTE) Analyst and reporting specialist (1FTE) Complete recommendations from the resource review- first progress report due March There are fines and punishments of imprisonment for reckless conduct in respect to duty of care, and fines for failing to comply with risks that expose individuals to death or serious injury/illness. 6.2 Waitemata District Health Board, Meeting of the Board 01/03/17 220
221 6.3 Bowel Screening Pilot Final Evaluation Report Recommendation: That the Bowel Screening Pilot Evaluation Report be received. Prepared by: Dr Debbie Holdsworth (Director Funding) 6.3 Glossary BSP Bowel Screening Pilot, the pilot 1. Strategic Alignment Emphasis and investment on both treatment and keeping people healthy Intelligence and insight Waitemata DHB is pilot site of the National Bowel Screening Pilot. The goal of the pilot is to determine whether organised bowel screening can be introduced in New Zealand in a way that is effective, safe and acceptable for participants, equitable and economically efficient. 2. Summary The Ministry of Health funded Waitemata District Health Board to run a Bowel Screening Pilot from 2012 to 2015, to inform whether a national bowel screening programme should be introduced. The original two screening rounds of the pilot were completed in December Budget 2015 provided funding for the pilot to run for a third two year cycle while the results of the original pilot were evaluated to inform a decision regarding a national roll out. Budget 2016 provided $39.3 million over four years for a progressive national bowel screening programme rollout, starting with Hutt Valley and Wairarapa DHBs in July A substantive update was provided to the Board in June 2016 regarding this announcement. It included its impact on the Waitemata pilot which will now transition into a regular screening programme from January At the June 2016 meeting of the Board, Board members expressed interest in receiving copies of any evaluation undertaken of the pilot once these became publicly available. In February 2017, the Ministry publically released the findings of the final evaluation report and as requested by the Board, this is attached for information. Summary of Final Evaluation Report of the Bowel Screening Pilot: Screening Rounds One and Two The report is the final evaluation report of the Pilot, undertaken by Litmus, the Centre for Public Health Research Massey University, and Sapere Research Group, following the completion of the distribution of invitations for screening Rounds 1 and 2 (January 2012 December 2015). The goal of the evaluation was to determine whether organised bowel screening could be introduced in New Zealand in a way that is effective, safe and acceptable for participants, equitable and economically efficient. A copy of the report is available in the Diligent Boardbooks resource centre or at: Waitemata District Health Board, Meeting of the Board 01/03/17 221
222 The report found that: the pilot has demonstrated that a national bowel screening programme could be safely introduced in New Zealand it is considered highly probable that a well-managed bowel screening programme will reduce deaths from bowel cancer bowel screening is cost saving and brings health benefits participation in the pilot was higher in most groups than the internationally accepted minimum enabling equal participation in a national programme is essential the evaluation noted the challenges to a national programme presented by colonoscopy workforce capacity. 6.3 National Rollout Progress Waitemata DHB is currently supporting the implementation of both the Hutt Valley and Wairarapa sites and has also been endorsed by the North Region Executive Forum to act as the Northern Bowel Screening Regional Centre. In addition, the Ministry have released the RFP for the National Coordination Centre which is due March 17, We will bring a more substantive progress update to the Board in May 2017 when we anticipate the latest Ministry monitoring report will be available. This will include results for the third cycle up to September Waitemata District Health Board, Meeting of the Board 01/03/17 222
223 6.4 Privacy Maturity Assessment 2017 Recommendations: That the Board notes: a) That the attached Privacy Maturity Assessment Report has been submitted to the Government Chief Privacy Officer. b) The achievements against targets set for 2016/17. c) The targets which have been set for improving Waitemata DHB s privacy maturity over the next 12 months. 6.4 Prepared by: Amanda Mark (General Counsel) and Carol Jansen (Privacy Administrator) Endorsed by: Privacy and Security Governance Group, Robert Paine (Chief Financial Officer and Head Corporate Services), Stuart Bloomfield (Chief Information Officer) and Dr Dale Bramley (Chief Executive officer) Glossary DHB - District Health Board GCPO - Government Chief Privacy Officer PMAF - Privacy Maturity Assessment Framework PSGG - Privacy and Security Governance Group (a Waitemata DHB committee) 1. Executive Summary The Government Chief Privacy Officer (GCPO) requires all public sector agencies including DHBs to self-assess their privacy maturity annually against a privacy maturity assessment framework (PMAF) and set goals for improving their privacy maturity for the following 12 months. Waitemata DHB submitted its first annual self-assessment to the GCPO in late March A second self- assessment for the year from 1 April 2016 to 31 March 2017 must be submitted by 31 March 2017 and a draft is attached as Appendix 1 for the Board s information. Good progress has been made this year. Generally we have met and often exceeded the goals we set ourselves for improving our privacy maturity in 2016/17. This is reflected in an increase in our maturity rating from defined (indicating that there is a holistic approach to privacy and widespread awareness of its importance) to embedded (indicating that privacy is embedded into our operations with consistent governance and oversight) in most areas. 2. Introduction/Background The Privacy Maturity Assessment Framework (PMAF) The PMAF assesses privacy management across the whole organisation against nine elements and rates maturity on a five tier scale. The nine elements are: 1. Governance, leadership and accountability 2. Culture 3. Assurance Waitemata District Health Board, Meeting of the Board 01/03/17 223
224 4. Information management 5. Privacy risk assessment 6. Privacy Programme 7. Business processes 8. Implementation of the Information Privacy Principles in the Privacy Act Breach and incident management 6.4 The Maturity Assessment rating scale, from lowest to highest, is: Ad hoc an unstructured approach where policies and processes are not sufficiently defined and privacy management is dependent on individual initiative rather than documented processes Developing privacy management is seen as a compliance exercise and overall approach is reactive with limited central oversight and siloed approaches Defined privacy policies and processes are defined and comprehensive, there is a holistic approach to managing privacy and widespread awareness Embedded privacy management is embedded into the design and functionality of business processes and systems and is consistent across the agency with well-defined governance and oversight structures Optimised privacy management is viewed as a strategic initiative with a clear agency culture of continuous improvement. The agency is viewed by stakeholders and the public as a leader in privacy management and introduces innovative initiatives to address privacy issues. It is important to note that: The maturity levels stated in the report are averages, there is an underlying detailed framework which sets out the attributes for each element. At the attribute level part scores are not possible, all components described in the framework must be fully in place before the maturity level can be achieved. The assessment is of our maturity as a DHB. This does not include completing a formal assessment of our suppliers (e.g. healthalliance processes are not included in this assessment). The impact of our providers on our privacy maturity is however captured by some of the attributes which consider our processes for managing third parties and contractors. 3. Progress/Achievements/Activity Outcome of Privacy Maturity Assessment (PMA) Our maturity across the nine elements as at March 2016 is shown in blue in the diagram (Figure 1) below. The improvement we expected to make last year is shown in yellow and our five year target state is shown in green. Generally we fell within the defined or embedded levels of maturity. The defined rating indicates that we have well defined and comprehensive privacy policies, a holistic approach to managing privacy and wide awareness of privacy. The embedded rating indicates that privacy management is embedded in our business processes and systems consistently across the organisation with welldefined governance and oversight structures. We have made good progress this year. Generally we have met and often exceeded the goals we set ourselves for improving our privacy maturity in 2016/17. This is reflected in an increase in our maturity rating from defined (indicating that there is a holistic approach to privacy and widespread Waitemata District Health Board, Meeting of the Board 01/03/17 224
225 awareness of its importance) to embedded (indicating that privacy is embedded into our operations with consistent governance and oversight) in most areas. 6.4 Figure 1: Overall Rating as at March 2016 Our maturity across the nine elements as at February 2017 is shown in blue in the diagram below (Figure 2). Again the expected improvement over the next year is shown in yellow and the five year target state in green. In most areas our maturity has improved and we now have an embedded level of maturity indicating that privacy management is embedded into the design and functionality of our business processes and systems and is consistent across the DHB with well-defined governance and oversight structures. Figure 2: Overall rating as at February 2017 Waitemata District Health Board, Meeting of the Board 01/03/17 225
226 A comparison of our scores in March 2016 and current scores appears in the table below: Attribute March 2016 Current Governance, leadership and accountability Culture Assurance Information Management Privacy Risk Management Privacy Programme Business Processes Implementation of the Information Privacy Principles in Privacy Act Incident and breach management Key achievements in the last year include: Introduction of a privacy strategy, privacy risk appetite and privacy programme. Appointment of a 0.5 FTE Privacy Administrator to oversee the implementation of privacy measures. The Privacy Administrator reports to the Chief Information Officer. Implementation of formal reporting processes for privacy incidents, privacy risks, and management of access and correction requests as follows: o A register of incidents involving privacy breaches has been established. Incidents are reviewed by the Privacy and Security Governance Group (PSGG) as they occur and recommendations are fed back to services for implementation. PSGG also reviews the incident register every six months to identify and address any trends. o Privacy risks identified in Service risk registers are regularly reported to PSGG by the Compliance and Risk Manager. PSGG reviews these risks as well as risks on the Regional Information Security risk register maintained by Waitemata DHB s shared service agency, healthalliance. o Processes for managing access and correction requests in the Clinical Records Service have been reviewed and documented. A summary is reported to PSGG quarterly. In 2016 we aimed for incremental continuous improvement in all areas and achieved, or in some areas, exceeded this in all but one area. The one area where we fell short was the goal of 90% of new employees completing the privacy e- learning module within six months of starting. We fell well short of this goal with only 43% of new staff completing the module within this timeframe. Overall only 60% of staff have completed the module. This is disappointing as the module is brief and engaging and takes only 10 minutes to complete. In the coming year we will assess the reasons for the low completion rates and what we can do to address them. We have already initiated discussions with Human Resources to see how we can improve completion rates. One possibility is that access to key programmes such as Concerto is made conditional on completion of the privacy module. Completing the privacy module might take place before or after Concerto training. Waitemata District Health Board, Meeting of the Board 01/03/17 226
227 Goals for Next Twelve Months As we did in 2017, we recommend further continuous improvement in all areas as the most efficient use of resources in the next 12 months. This is because: our current maturity is already well developed in a number of areas all the attributes specified by PMAF within each area must be fully achieved before the next maturity rating is reached; and a state of 4-Embedded is a high bar as defined in the maturity framework. 6.4 Priorities will include: Improving staff compliance with privacy training o Devise methods to achieve KPI target (90% of new staff complete Privacy elearning course within the first 6 months). o Improve mechanisms to ensure external contractors/agents complete appropriate privacy training Rolling out a privacy assurance framework and identifying additional assurance activities o work with internal audit to identify appropriate privacy related assurance activities. o monitor trends in both incidents and risks and use this information to inform assurance activities. Reinforcing the risk management framework and improve risk reporting by services o Implement processes to ensure that privacy risk information is analysed to identify trends from historic information and assess effectiveness of controls. o Identify mechanisms by which risks can be linked to the privacy strategy and key performance indicators so that risk information is integrated into reporting of privacy management performance. o Use enhanced risk information to update policies and processes. 4. Conclusion The Privacy Maturity Assessment indicates that there has been good improvement in our privacy maturity with all but one goal achieved and most exceeded and a movement from a defined to an embedded rating in most areas. We expect there to be further steady progress in the coming year. Waitemata District Health Board, Meeting of the Board 01/03/17 227

228 UNCLASSIFIED Appendix 1 Government Chief Privacy Officer 6.4 Annual Agency Self-Assessment Report 2017 Waitemata District Health Board UNCLASSIFIED [Agency to reclassify completed report and update protective markings see content for more guidance] 228
Wednesday 29 th June Note: Public Excluded Session 9.45am to 12.15pm Open meeting from 12.45pm
 BOARD MEETING Wednesday 29 th June 2016 9.45am Note: Public Excluded Session 9.45am to 12.15pm Open meeting from 12.45pm AGENDA Items to be considered in public meeting VENUE Waitemata DHB Boardroom Level
BOARD MEETING Wednesday 29 th June 2016 9.45am Note: Public Excluded Session 9.45am to 12.15pm Open meeting from 12.45pm AGENDA Items to be considered in public meeting VENUE Waitemata DHB Boardroom Level
Wednesday 16 th December Note: Public Excluded Session 10.15am to 12.15pm Open meeting from 12.45pm
 BOARD MEETING Wednesday 16 th December 2015 10.15am Note: Public Excluded Session 10.15am to 12.15pm Open meeting from 12.45pm AGENDA Items to be considered in public meeting VENUE Waitemata DHB Boardroom
BOARD MEETING Wednesday 16 th December 2015 10.15am Note: Public Excluded Session 10.15am to 12.15pm Open meeting from 12.45pm AGENDA Items to be considered in public meeting VENUE Waitemata DHB Boardroom
Wednesday 10 th August Note: Public Excluded Session 11.00am to 12noon Open meeting from 12.45pm
 BOARD MEETING Wednesday 10 th August 2016 11.00am Note: Public Excluded Session 11.00am to 12noon Open meeting from 12.45pm AGENDA Items to be considered in public meeting VENUE Waitemata DHB Boardroom
BOARD MEETING Wednesday 10 th August 2016 11.00am Note: Public Excluded Session 11.00am to 12noon Open meeting from 12.45pm AGENDA Items to be considered in public meeting VENUE Waitemata DHB Boardroom
BOARD MEETING AGENDA. 9.45am. Wednesday 22 August Items to be considered in public meeting VENUE
 BOARD MEETING Wednesday 22 August 2018 9.45am AGENDA Items to be considered in public meeting VENUE Waitemata DHB Boardroom Level 1, 15 Shea Terrace Takapuna 1 Karakia E te Kaihanga e te Wahingaro E mihi
BOARD MEETING Wednesday 22 August 2018 9.45am AGENDA Items to be considered in public meeting VENUE Waitemata DHB Boardroom Level 1, 15 Shea Terrace Takapuna 1 Karakia E te Kaihanga e te Wahingaro E mihi
2.1 Confirmation of Minutes of the Meeting of the Board on 26 January 2011
 2.1 Confirmation of Minutes of the Meeting of the on 26 January 2011 Recommendation: That the Minutes of the Meeting of the held on 26 January 2011 be approved. Waitemata District Health, Meeting of the
2.1 Confirmation of Minutes of the Meeting of the on 26 January 2011 Recommendation: That the Minutes of the Meeting of the held on 26 January 2011 be approved. Waitemata District Health, Meeting of the
Community and Public Health Advisory Committees Meeting. Wednesday 13 September am
 Community and Public Health Advisory Committees Meeting Wednesday 13 September 2017 10.00am Venue Waitemata District Health Board Boardroom Level 1, 15 Shea Tce Takapuna 1 Karakia E te Kaihanga e te Wahingaro
Community and Public Health Advisory Committees Meeting Wednesday 13 September 2017 10.00am Venue Waitemata District Health Board Boardroom Level 1, 15 Shea Tce Takapuna 1 Karakia E te Kaihanga e te Wahingaro
Community and Public Health Advisory Committees Meeting. Wednesday 21 June am
 Community and Public Health Advisory Committees Meeting Wednesday 21 June 2017 10.00am Venue Waitemata District Health Board Boardroom Level 1, 15 Shea Tce Takapuna 1 Karakia E te Kaihanga e te Wahingaro
Community and Public Health Advisory Committees Meeting Wednesday 21 June 2017 10.00am Venue Waitemata District Health Board Boardroom Level 1, 15 Shea Tce Takapuna 1 Karakia E te Kaihanga e te Wahingaro
BOARD MEETING AGENDA. 1pm. Wednesday 27 September Items to be considered in public meeting VENUE
 BOARD MEETING Wednesday 27 September 2017 1pm AGENDA Items to be considered in public meeting VENUE Waitemata DHB Boardroom Level 1, 15 Shea Terrace Takapuna 1 Karakia E te Kaihanga e te Wahingaro E mihi
BOARD MEETING Wednesday 27 September 2017 1pm AGENDA Items to be considered in public meeting VENUE Waitemata DHB Boardroom Level 1, 15 Shea Terrace Takapuna 1 Karakia E te Kaihanga e te Wahingaro E mihi
HOSPITAL ADVISORY COMMITTEE (HAC) MEETING. Wednesday 03 May 2017 A G E N D A
 MEETING. Wednesday 03 May 2017 A G E N D A") HOSPITAL ADVISORY COMMITTEE (HAC) MEETING Wednesday 03 May 2017 1.30pm A G E N D A VENUE Waitemata District Health Board Boardroom Level 1, 15 Shea Tce Takapuna 1 1 HOSPITAL ADVISORY COMMITTEE (HAC) MEETING
HOSPITAL ADVISORY COMMITTEE (HAC) MEETING Wednesday 03 May 2017 1.30pm A G E N D A VENUE Waitemata District Health Board Boardroom Level 1, 15 Shea Tce Takapuna 1 1 HOSPITAL ADVISORY COMMITTEE (HAC) MEETING
HOSPITAL ADVISORY COMMITTEE (HAC) MEETING. Wednesday 14 June 2017 A G E N D A
 MEETING. Wednesday 14 June 2017 A G E N D A") HOSPITAL ADVISORY COMMITTEE (HAC) MEETING Wednesday 14 June 2017 1.00pm A G E N D A VENUE Waitemata District Health Board Boardroom Level 1, 15 Shea Tce Takapuna 1 1 HOSPITAL ADVISORY COMMITTEE (HAC) MEETING
HOSPITAL ADVISORY COMMITTEE (HAC) MEETING Wednesday 14 June 2017 1.00pm A G E N D A VENUE Waitemata District Health Board Boardroom Level 1, 15 Shea Tce Takapuna 1 1 HOSPITAL ADVISORY COMMITTEE (HAC) MEETING
HOSPITAL ADVISORY COMMITTEE (HAC) MEETING. Wednesday 28 March 2018 A G E N D A
 MEETING. Wednesday 28 March 2018 A G E N D A") HOSPITAL ADVISORY COMMITTEE (HAC) MEETING Wednesday 28 March 2018 1.30pm A G E N D A VENUE Waitemata District Health Board Boardroom Level 1, 15 Shea Tce Takapuna 1 HOSPITAL ADVISORY COMMITTEE (HAC) MEETING
HOSPITAL ADVISORY COMMITTEE (HAC) MEETING Wednesday 28 March 2018 1.30pm A G E N D A VENUE Waitemata District Health Board Boardroom Level 1, 15 Shea Tce Takapuna 1 HOSPITAL ADVISORY COMMITTEE (HAC) MEETING
HOSPITAL ADVISORY COMMITTEE (HAC) MEETING. Wednesday 29 November 2017 A G E N D A
 MEETING. Wednesday 29 November 2017 A G E N D A") HOSPITAL ADVISORY COMMITTEE (HAC) MEETING Wednesday 29 November 2017 1.30pm A G E N D A VENUE Waitemata District Health Board Boardroom Level 1, 15 Shea Tce Takapuna 1 1 HOSPITAL ADVISORY COMMITTEE (HAC)
HOSPITAL ADVISORY COMMITTEE (HAC) MEETING Wednesday 29 November 2017 1.30pm A G E N D A VENUE Waitemata District Health Board Boardroom Level 1, 15 Shea Tce Takapuna 1 1 HOSPITAL ADVISORY COMMITTEE (HAC)
Acute Perinatal and Infant Mental Health Workstream Groups. (Metro Auckland) - Terms of Reference
 - Terms of Reference") 1 Purpose & Brief Purpose The Acute Perinatal Infant Mental Health Group ToR is to provide a framework and direction to ensure the timely response to the planning and delivery of the agreed service developments
1 Purpose & Brief Purpose The Acute Perinatal Infant Mental Health Group ToR is to provide a framework and direction to ensure the timely response to the planning and delivery of the agreed service developments
Open Board Meeting. Wednesday, 22 February :00am. A+ Trust Room Clinical Education Centre Level 5 Auckland City Hospital Grafton
 Open Board Meeting Wednesday, 22 February 2017 09:00am Note: Open Meeting from 9:00 am to 11:30am Public Excluded Session 11:30am to 12:30pm A+ Trust Room Clinical Education Centre Level 5 Auckland City
Open Board Meeting Wednesday, 22 February 2017 09:00am Note: Open Meeting from 9:00 am to 11:30am Public Excluded Session 11:30am to 12:30pm A+ Trust Room Clinical Education Centre Level 5 Auckland City
Operations Manager, Asian Health Services
 Date: February 2016 (Review Feb 2017) Job Title : Operations Manager, Asian Health Department : Hospital Location : Waitemata District Health Board Sites including North Shore and Waitakere Hospitals Reporting
Date: February 2016 (Review Feb 2017) Job Title : Operations Manager, Asian Health Department : Hospital Location : Waitemata District Health Board Sites including North Shore and Waitakere Hospitals Reporting
Auckland DHB Strategy to 2020
 Our Vision Healthy communities World-class healthcare Achieved together Kia kotahi te oranga mo te iti me te rahi o te hāpori Our Strategic Themes Community, family/whānau and patientcentric model of healthcare
Our Vision Healthy communities World-class healthcare Achieved together Kia kotahi te oranga mo te iti me te rahi o te hāpori Our Strategic Themes Community, family/whānau and patientcentric model of healthcare
How do we set national health research priorities for New Zealand? Summary of Consultation and Submissions
 How do we set national health research priorities for New Zealand? Summary of Consultation and Submissions Background Information The first ever New Zealand Health Research Strategy 2017 2027 (NZHRS) aims
How do we set national health research priorities for New Zealand? Summary of Consultation and Submissions Background Information The first ever New Zealand Health Research Strategy 2017 2027 (NZHRS) aims
Strategic Plan
 Strategic Plan 2013-2025 Toi Te Ora Public Health Service (Toi Te Ora) is one of 12 public health units funded by the Ministry of Health and is the public health unit for the Bay of Plenty and Lakes District
Strategic Plan 2013-2025 Toi Te Ora Public Health Service (Toi Te Ora) is one of 12 public health units funded by the Ministry of Health and is the public health unit for the Bay of Plenty and Lakes District
Contemporary Art Foundation STATEMENT OF INTENT
 Contemporary Art Foundation STATEMENT OF INTENT 1 July 2014-30 June 2017 Board Approved 9th June 1 Contents 1.0 Introduction 2.0 Trust Objectives 3.0 Governance 4.0 Nature and Scope of Activities 5.0 Accounting
Contemporary Art Foundation STATEMENT OF INTENT 1 July 2014-30 June 2017 Board Approved 9th June 1 Contents 1.0 Introduction 2.0 Trust Objectives 3.0 Governance 4.0 Nature and Scope of Activities 5.0 Accounting
Māori Women s Health Liaison Coordinator
 Date: 26 August 2013 Job Title : Māori Women s Health Liaison Department : Womens Health Services Location : Waitakere and North Shore Hospitals and community Reporting To : Midwife Manager - Community
Date: 26 August 2013 Job Title : Māori Women s Health Liaison Department : Womens Health Services Location : Waitakere and North Shore Hospitals and community Reporting To : Midwife Manager - Community
MIHI WELCOME. Whano! Whano! Haere mai te toki Haumie hui e tāiki e!
 Te Rautaki Māori Better Māori Health Outcomes through Great Primary Care MIHI WELCOME Piki mai, Kaki mai Homai te waiora ki āhau Tiaki wai! Tiaki wai! Tiaki waiora! Ka whakawhitia te awa I pikopiko I whiti
Te Rautaki Māori Better Māori Health Outcomes through Great Primary Care MIHI WELCOME Piki mai, Kaki mai Homai te waiora ki āhau Tiaki wai! Tiaki wai! Tiaki waiora! Ka whakawhitia te awa I pikopiko I whiti
Minutes Public session
 Minutes Public session Meeting of the held in the Board Room, Fourth Floor, Ward/Administration Building Whanganui Hospital, 100 Heads Road, Whanganui on Friday 18 May, commencing at 10.00am Present Mrs
Minutes Public session Meeting of the held in the Board Room, Fourth Floor, Ward/Administration Building Whanganui Hospital, 100 Heads Road, Whanganui on Friday 18 May, commencing at 10.00am Present Mrs
Clinical Director - Primary Care Position Description
 Date: May 2010 Job Title : Clinical Director Primary Care Department : Planning and Funding Location : Funding and Planning team, Shea Tce. North shore Hospital Reporting To : Director Integration and
Date: May 2010 Job Title : Clinical Director Primary Care Department : Planning and Funding Location : Funding and Planning team, Shea Tce. North shore Hospital Reporting To : Director Integration and
Duty Nurse Manager Waitemata Central Position Description
 Date: January 2016 (review January 2017) Job Title : Department : Location : Waitemata DHB (based at NSH and/or WTH) Reporting to Professional Line Operations Manager (NSH and /or WTH) Charge Nurse Manager
Date: January 2016 (review January 2017) Job Title : Department : Location : Waitemata DHB (based at NSH and/or WTH) Reporting to Professional Line Operations Manager (NSH and /or WTH) Charge Nurse Manager
Operations Manager - Outpatients
 Date: July 2017 Job Title : Operations Manager Outpatients Surgical and Ambulatory Services Department : Surgical & Ambulatory Services Location : All WDHB sites, including North Shore and Waitakere Hospitals
Date: July 2017 Job Title : Operations Manager Outpatients Surgical and Ambulatory Services Department : Surgical & Ambulatory Services Location : All WDHB sites, including North Shore and Waitakere Hospitals
Registered Nurse - Quality Improvement Coordinator, West Auckland Locality
 Date: December 2013 Job Title : Registered Nurse Quality Improvement Coordinator West Department Location Reporting To Direct Reports : Primary Health Care Nursing Development Team : Waitemata District
Date: December 2013 Job Title : Registered Nurse Quality Improvement Coordinator West Department Location Reporting To Direct Reports : Primary Health Care Nursing Development Team : Waitemata District
Charge Nurse Manager Adult Mental Health Services Acute Inpatient
 Date: February 2013 DRAFT Job Title : Charge Nurse Manager Department : Waiatarau Acute Unit Location : Waitakere Hospital Reporting To : Operations Manager Adult Mental Health Services for the achievement
Date: February 2013 DRAFT Job Title : Charge Nurse Manager Department : Waiatarau Acute Unit Location : Waitakere Hospital Reporting To : Operations Manager Adult Mental Health Services for the achievement
RUN DESCRIPTION. North Shore Hospice, Shea Terrace, Takapuna, Auckland. Employed by WDHB and on secondment for the duration of the run
 RUN DESCRIPTION POSITION: Palliative Medicine Registrar In Patient DEPARTMENT: North Shore Hospice, Shea Terrace, Takapuna, Auckland PLACE OF WORK: North Shore Hospice RESPONSIBLE TO: Palliative Care Consultants
RUN DESCRIPTION POSITION: Palliative Medicine Registrar In Patient DEPARTMENT: North Shore Hospice, Shea Terrace, Takapuna, Auckland PLACE OF WORK: North Shore Hospice RESPONSIBLE TO: Palliative Care Consultants
REGIONAL ARTS AND CULTURE FUNDING ALLOCATION SUBCOMMITTEE
 NOTICE OF INAUGURAL MEETING REGIONAL ARTS AND CULTURE FUNDING ALLOCATION SUBCOMMITTEE I hereby give notice that an Inaugural Meeting will be held on:- DATE: Monday, 22 April 2002 TIME: 7.00 pm VENUE: Civic
NOTICE OF INAUGURAL MEETING REGIONAL ARTS AND CULTURE FUNDING ALLOCATION SUBCOMMITTEE I hereby give notice that an Inaugural Meeting will be held on:- DATE: Monday, 22 April 2002 TIME: 7.00 pm VENUE: Civic
Operations Manager ORL
 Date: October 2016 Job Title : Operations Manager ORL Surgical and Ambulatory Services Department : Surgical & Ambulatory Services Location : All WDHB sites, including North Shore and Waitakere Hospitals
Date: October 2016 Job Title : Operations Manager ORL Surgical and Ambulatory Services Department : Surgical & Ambulatory Services Location : All WDHB sites, including North Shore and Waitakere Hospitals
POSITION DESCRIPTION
 POSITION DETAILS: POSITION DESCRIPTION TITLE: Public Health Nurse Refugee Health Screening Service REPORTS TO: Programme Supervisor LOCATION: Auckland Regional Public Health Service (ARPHS). Position based
POSITION DETAILS: POSITION DESCRIPTION TITLE: Public Health Nurse Refugee Health Screening Service REPORTS TO: Programme Supervisor LOCATION: Auckland Regional Public Health Service (ARPHS). Position based
MAORI RESPONSIVENESS STRATEGY
 MAORI RESPONSIVENESS STRATEGY July 2002 m FOREWORD E nga rangatira o nga hau e wha, tena koutou katoa. Kei te mihi atu, kei te tangi atu. Kei te tangi atu ki nga mate o nga Marae maha o Aotearoa nei. Ratau
MAORI RESPONSIVENESS STRATEGY July 2002 m FOREWORD E nga rangatira o nga hau e wha, tena koutou katoa. Kei te mihi atu, kei te tangi atu. Kei te tangi atu ki nga mate o nga Marae maha o Aotearoa nei. Ratau
Board Secretary. Position Description
 Date: May 2018 Job Title : Board Secretary Department : Corporate Services Location : Level 2, 15 Shea Terrace, Takapuna Reporting To : Chief Financial Officer and Head of Corporate Services Direct Reports
Date: May 2018 Job Title : Board Secretary Department : Corporate Services Location : Level 2, 15 Shea Terrace, Takapuna Reporting To : Chief Financial Officer and Head of Corporate Services Direct Reports
IQ Action Plan: Supporting the Improving Quality Approach
 IQ Action Plan: Supporting the Improving Quality Approach i ii Citation: Minister of Health. 2003.. Wellington:. Published in September 2003 by the PO Box 5013, Wellington, New Zealand ISBN 0-478-25800-3
IQ Action Plan: Supporting the Improving Quality Approach i ii Citation: Minister of Health. 2003.. Wellington:. Published in September 2003 by the PO Box 5013, Wellington, New Zealand ISBN 0-478-25800-3
GATEWAY ASSESSMENT SERVICE: SERVICE SPECIFICATION
 GATEWAY ASSESSMENT SERVICE: SERVICE SPECIFICATION 2017 GATEWAY ASSESSMENT SERVICE SPECIFICATION 1 Table of Contents 1. About the Service Specification... 4 Purpose... 4 2. Service overview... 5 Brief description
GATEWAY ASSESSMENT SERVICE: SERVICE SPECIFICATION 2017 GATEWAY ASSESSMENT SERVICE SPECIFICATION 1 Table of Contents 1. About the Service Specification... 4 Purpose... 4 2. Service overview... 5 Brief description
Capital & Coast DHB System Level Measures Improvement Plan 2016/17
 Capital & Coast DHB System Level Measures Improvement Plan 2016/17 Written by: Astuti Balram, ICC Programme Manager, on behalf of the CCDHB Integrated Care Collaborative (ICC) Alliance Version 4 Released
Capital & Coast DHB System Level Measures Improvement Plan 2016/17 Written by: Astuti Balram, ICC Programme Manager, on behalf of the CCDHB Integrated Care Collaborative (ICC) Alliance Version 4 Released
Board Meeting. Wednesday, 18 February :30pm. A+ Trust Room Clinical Education Centre Level 5 Auckland City Hospital Grafton
 Board Meeting Wednesday, 18 February 2015 2:30pm A+ Trust Room Clinical Education Centre Level 5 Auckland City Hospital Grafton Published 12 February 2015 1 Agenda Meeting of the Board 18 February 2015
Board Meeting Wednesday, 18 February 2015 2:30pm A+ Trust Room Clinical Education Centre Level 5 Auckland City Hospital Grafton Published 12 February 2015 1 Agenda Meeting of the Board 18 February 2015
BARTS AND THE LONDON NHS TRUST TRUST BOARD MEETING
 BARTS AND THE LONDON NHS TRUST TRUST BOARD MEETING Minutes of the open meeting of the Trust Board held on Wednesday 26 January 2005 at 11.30am in the Old Library, School of Medicine and Dentistry, Turner
BARTS AND THE LONDON NHS TRUST TRUST BOARD MEETING Minutes of the open meeting of the Trust Board held on Wednesday 26 January 2005 at 11.30am in the Old Library, School of Medicine and Dentistry, Turner
Clinical Nurse Specialist / Nurse Practitioner Intern Women s Health
 Date: December 2017 Job Title : Clinical Nurse Specialist / Nurse Practitioner The CNS / NP Intern for Women s Health works in a collaborative environment, to facilitate the development of advanced nursing
Date: December 2017 Job Title : Clinical Nurse Specialist / Nurse Practitioner The CNS / NP Intern for Women s Health works in a collaborative environment, to facilitate the development of advanced nursing
Leeds West CCG Governing Body Meeting
 Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
Position Description
 Date: June 2014 Job Title : Community Mental Health Nurse / Alcohol & Drug Clinician: Older People Department : 65+ team, Community Alcohol & Drug Service (CADS) Location : CADS West, 1 Trading Place,
Date: June 2014 Job Title : Community Mental Health Nurse / Alcohol & Drug Clinician: Older People Department : 65+ team, Community Alcohol & Drug Service (CADS) Location : CADS West, 1 Trading Place,
Hospital Advisory Committee Meeting. Wednesday, 07 June pm. A+ Trust Room Clinical Education Centre Level 5 Auckland City Hospital Grafton
 Hospital Advisory Committee Meeting Wednesday, 07 June 2017 1.30pm A+ Trust Room Clinical Education Centre Level 5 Auckland City Hospital Grafton Healthy communities World-class healthcare Achieved together
Hospital Advisory Committee Meeting Wednesday, 07 June 2017 1.30pm A+ Trust Room Clinical Education Centre Level 5 Auckland City Hospital Grafton Healthy communities World-class healthcare Achieved together
JOB TITLE: Social Worker, Child and Adolescent Mental Health Service (CAMHS)
") JOB TITLE: Social Worker, Child and Adolescent Mental Health Service (CAMHS) 1. PURPOSE OF POSITION To provide a community/outpatient based Mental Health Service to children and youth and their families
JOB TITLE: Social Worker, Child and Adolescent Mental Health Service (CAMHS) 1. PURPOSE OF POSITION To provide a community/outpatient based Mental Health Service to children and youth and their families
Occupational Therapist
 Date: January 2017 Job Title : Occupational Therapist Department : Allied Health - Early Discharge and Rehabilitation Service (EDARS) Location : All Waitemata DHB (North Shore, Rodney and Waitakere) Reporting
Date: January 2017 Job Title : Occupational Therapist Department : Allied Health - Early Discharge and Rehabilitation Service (EDARS) Location : All Waitemata DHB (North Shore, Rodney and Waitakere) Reporting
Cultural Case Worker
 Date: 8 May 2014 Job Title : Cultural Case Worker Department : Child Health Services Location : Child Development (Waitakere base, required to work in multiple locations) Reporting To : Team Leader Child
Date: 8 May 2014 Job Title : Cultural Case Worker Department : Child Health Services Location : Child Development (Waitakere base, required to work in multiple locations) Reporting To : Team Leader Child
Clinical Director. Position Description
 Clinical Director Position Description About Pathways and the Wise Group Pathways At Pathways, we provide community-based mental health, addiction and wellbeing services throughout New Zealand. Every year
Clinical Director Position Description About Pathways and the Wise Group Pathways At Pathways, we provide community-based mental health, addiction and wellbeing services throughout New Zealand. Every year
Position Description
 Position Description Position Title: Reports to: Key Relationships: Direct Reports: Clinical Team Leader Chief Executive Officer/ General Manager Internal: Finance Administrator, Fundraising Manager, Volunteer
Position Description Position Title: Reports to: Key Relationships: Direct Reports: Clinical Team Leader Chief Executive Officer/ General Manager Internal: Finance Administrator, Fundraising Manager, Volunteer
Designated Title: Clinical Nurse Specialist. Position Title: Clinical Nurse Specialist Reconstructive Breast Surgery
 Designated Title: Clinical Nurse Specialist Position Title: Clinical Nurse Specialist Reconstructive Breast Surgery This role is considered a non-core children s worker and will be subject to safety checking
Designated Title: Clinical Nurse Specialist Position Title: Clinical Nurse Specialist Reconstructive Breast Surgery This role is considered a non-core children s worker and will be subject to safety checking
Senior Medical Officer and Clinical Leader Hyperbaric Medicine
 Senior Medical Officer and Clinical Leader Date: August 2017 Job Title : Senior Medical Officer and Clinical Leader Hyperbaric Medicine Department : Medicine and Health of Older People Services, Waitemata
Senior Medical Officer and Clinical Leader Date: August 2017 Job Title : Senior Medical Officer and Clinical Leader Hyperbaric Medicine Department : Medicine and Health of Older People Services, Waitemata
Operations Manager - WDHB ORL and Urology Surgical and Ambulatory Services
 Date: July 2014 Job Title : Operations Manager ORL and Urology Department : Surgical & Ambulatory Services Location : All WDHB sites, including North Shore and Waitakere Hospitals Reports to : GM S&AS
Date: July 2014 Job Title : Operations Manager ORL and Urology Department : Surgical & Ambulatory Services Location : All WDHB sites, including North Shore and Waitakere Hospitals Reports to : GM S&AS
NURSING NURSING NURSING
 NURSING A FUTURE IN NURSING WHAT IS A CAREER IN NURSING LIKE? If doctors are the organs of healthcare, then nurses are the blood they make sure the whole system runs smoothly, performing critical specialist
NURSING A FUTURE IN NURSING WHAT IS A CAREER IN NURSING LIKE? If doctors are the organs of healthcare, then nurses are the blood they make sure the whole system runs smoothly, performing critical specialist
Dietitian - Community
 Dietitian - Community Position Description Date: October 13 Job Title : Dietitian - Community Department Location Reporting To Direct Reports Functional Relationships with : Medicine and Health of Older
Dietitian - Community Position Description Date: October 13 Job Title : Dietitian - Community Department Location Reporting To Direct Reports Functional Relationships with : Medicine and Health of Older
Operations Manager Whitiki Maurea Maori Mental Health and Addiction Service
 Date November 2017 Job Title Role Context Operations Manager/Kaiwhakahaere Hautu The DHB has three levels of Operations Managers. While the accountabilities are the same, the size of each service profile
Date November 2017 Job Title Role Context Operations Manager/Kaiwhakahaere Hautu The DHB has three levels of Operations Managers. While the accountabilities are the same, the size of each service profile
Statement of Strategic Intentions 2017 to 2021 Ministry of Health
 E.10 SOSI (2017/21) Statement of Strategic Intentions 2017 to 2021 Ministry of Health Citation: Ministry of Health. 2017. Statement of Strategic Intentions 2017 to 2021. Wellington: Ministry of Health.
E.10 SOSI (2017/21) Statement of Strategic Intentions 2017 to 2021 Ministry of Health Citation: Ministry of Health. 2017. Statement of Strategic Intentions 2017 to 2021. Wellington: Ministry of Health.
Building a Healthy New Zealand
 Building a Healthy New Zealand Becoming a DHB board member Released August 2013 www.health.govt.nz Citation: Ministry of Health. 2013. Building a Healthy New Zealand: Becoming a DHB board member. Wellington:
Building a Healthy New Zealand Becoming a DHB board member Released August 2013 www.health.govt.nz Citation: Ministry of Health. 2013. Building a Healthy New Zealand: Becoming a DHB board member. Wellington:
Note: Open Meeting from 2:00pm Public Excluded to follow
 Open Board Meeting Wednesday, 2 September 217 2:pm Note: Open Meeting from 2:pm Public Excluded to follow A+ Trust Room Clinical Education Centre Level 5 Auckland City Hospital Grafton Healthy communities
Open Board Meeting Wednesday, 2 September 217 2:pm Note: Open Meeting from 2:pm Public Excluded to follow A+ Trust Room Clinical Education Centre Level 5 Auckland City Hospital Grafton Healthy communities
Auckland DHB and Waitemata DHB Collaboration Maternity Plan. Working together to plan future maternity services to 2025
 Auckland DHB and Waitemata DHB Collaboration Maternity Plan Working together to plan future maternity services to 2025 Auckland DHB and Waitemata DHB Womens Health Collaboration Maternity Plan 2015 Auckland
Auckland DHB and Waitemata DHB Collaboration Maternity Plan Working together to plan future maternity services to 2025 Auckland DHB and Waitemata DHB Womens Health Collaboration Maternity Plan 2015 Auckland
NGO adult mental health and addiction workforce
 more than numbers NGO adult mental health and addiction 2014 survey of Vote Health funded 1 Recommended citation: Te Pou o Te Whakaaro Nui. (2015). NGO adult mental health and addiction : 2014 survey of
more than numbers NGO adult mental health and addiction 2014 survey of Vote Health funded 1 Recommended citation: Te Pou o Te Whakaaro Nui. (2015). NGO adult mental health and addiction : 2014 survey of
Job Title: Social Worker Marinoto CAMHS Position Description
 Date: February 2013 Job Title : Allied Health- Social Worker Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships with : Internal
Date: February 2013 Job Title : Allied Health- Social Worker Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships with : Internal
Quality and Patient Safety Team Leader
 Date : February 2018 Job Title : Quality and Patient Safety Team leader Department : Quality and Risk Location : All Waitemata DHB Sites Reporting To : Quality and Risk Manager Direct Reports : Quality
Date : February 2018 Job Title : Quality and Patient Safety Team leader Department : Quality and Risk Location : All Waitemata DHB Sites Reporting To : Quality and Risk Manager Direct Reports : Quality
NHS GRAMPIAN. Clinical Strategy
 NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
Job Title: Social Worker
 Date: March 2017 Job Title : Allied Health- Social Worker Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships with Guidance
Date: March 2017 Job Title : Allied Health- Social Worker Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships with Guidance
Job Title Occupational Therapist Marinoto CAMHS
 Date: February 2013 Job Title : Allied Health- Occupational Therapist Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships with
Date: February 2013 Job Title : Allied Health- Occupational Therapist Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships with
Hospital Advisory Committee Meeting. Wednesday, 15 March pm. A+ Trust Room Clinical Education Centre Level 5 Auckland City Hospital Grafton
 Hospital Advisory Committee Meeting Wednesday, 15 March 2017 1.30pm A+ Trust Room Clinical Education Centre Level 5 Auckland City Hospital Grafton Healthy communities World-class healthcare Achieved together
Hospital Advisory Committee Meeting Wednesday, 15 March 2017 1.30pm A+ Trust Room Clinical Education Centre Level 5 Auckland City Hospital Grafton Healthy communities World-class healthcare Achieved together
Ontario Quality Standards Committee Draft Terms of Reference
 Ontario Quality Standards Committee Draft Terms of Reference 1. Introduction The Ontario Health Quality Council (Health Quality Ontario) officially commenced operation on April 1st, 2010. Created under
Ontario Quality Standards Committee Draft Terms of Reference 1. Introduction The Ontario Health Quality Council (Health Quality Ontario) officially commenced operation on April 1st, 2010. Created under
Nurse Educator Special Care Baby Unit Position Description
 : November 20142013 Job Title : Nurse Educator Special Care (SCBU) Department : Child Women and Family Service Location : Child Health services including but not limited to North Shore and Waitakere Hospitals
: November 20142013 Job Title : Nurse Educator Special Care (SCBU) Department : Child Women and Family Service Location : Child Health services including but not limited to North Shore and Waitakere Hospitals
HEALTH PROMOTING SCHOOLS ADVISOR/FACILITATOR
 Date: JULY 2017 Job Title : HEALTH PROMOTING SCHOOLS Department : CHILD AND FAMILY SERVICE Location : WAITEMATA DHB sites as required Reporting To : Child and Family Team Leader. Ministry of Health HPS
Date: JULY 2017 Job Title : HEALTH PROMOTING SCHOOLS Department : CHILD AND FAMILY SERVICE Location : WAITEMATA DHB sites as required Reporting To : Child and Family Team Leader. Ministry of Health HPS
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
Perioperative Nurse Coordinator Lead [Surgical]
![Perioperative Nurse Coordinator Lead [Surgical]](/thumbs/80/80543803.jpg "Perioperative Nurse Coordinator Lead [Surgical]") Date : July 2017 Job Title : Perioperative Nurse Coordinator Lead Note: Lead role is equivalent to Associate Clinical Charge Nurse Level [SN 4] Department : Surgical and Ambulatory Services Otorhinolaryngology
Date : July 2017 Job Title : Perioperative Nurse Coordinator Lead Note: Lead role is equivalent to Associate Clinical Charge Nurse Level [SN 4] Department : Surgical and Ambulatory Services Otorhinolaryngology
POSITION DESCRIPTION
 POSITION DESCRIPTION Position details: Title: Reports to: Reports professionally to: Date: Charge Nurse Te Whetu Tawera Nurse Manager Nurse Director Mental Health and Addiction Healthcare Service Group
POSITION DESCRIPTION Position details: Title: Reports to: Reports professionally to: Date: Charge Nurse Te Whetu Tawera Nurse Manager Nurse Director Mental Health and Addiction Healthcare Service Group
Position Description
 Date: Dec 2012 Job Title : Allied health- Psychotherapist/ Child Psychotherapist Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships
Date: Dec 2012 Job Title : Allied health- Psychotherapist/ Child Psychotherapist Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships
Child Health 2020 A Strategic Framework for Children and Young People s Health
 Child Health 2020 A Strategic Framework for Children and Young People s Health Consultation Paper Please Give Us Your Views Consultation: 10 September 2013 21 October 2013 Our Child Health 2020 Vision
Child Health 2020 A Strategic Framework for Children and Young People s Health Consultation Paper Please Give Us Your Views Consultation: 10 September 2013 21 October 2013 Our Child Health 2020 Vision
Unit Manager/Theatre Services NSH and WTH
 Date: April 2013 (review April 2014) Job Title : Unit Manager / Theatre Services NSH/WTH North Shore and WTH Theatres and PACU, Central Sterile Supply Unit Department : Surgical and Ambulatory Services
Date: April 2013 (review April 2014) Job Title : Unit Manager / Theatre Services NSH/WTH North Shore and WTH Theatres and PACU, Central Sterile Supply Unit Department : Surgical and Ambulatory Services
Anaesthesia Fellow. Position Description. Department : Department of Anaesthesia & Perioperative Medicine
 Job Title : Anaesthesia Fellow Department : Department of Anaesthesia & Perioperative Medicine Location : Waitemata District Health Board Reporting To : Clinical Director Anaesthesia Direct Reports : Anaesthesia
Job Title : Anaesthesia Fellow Department : Department of Anaesthesia & Perioperative Medicine Location : Waitemata District Health Board Reporting To : Clinical Director Anaesthesia Direct Reports : Anaesthesia
Promoting Healthy Eating at the Local Government Level
 Evidence Snapshot March 2016 Promoting Healthy Eating at the Local Government Level Case Studies Case Study 1 Establishing a Local Food Policy Council With a collaborative response by both the community
Evidence Snapshot March 2016 Promoting Healthy Eating at the Local Government Level Case Studies Case Study 1 Establishing a Local Food Policy Council With a collaborative response by both the community
YOUR PROPOSED NEW MECA
 NZNO/DHB MECA 2017 Ehara taku toa i te toa takitahi, ēngari he toa taki mano 14 November 2017 YOUR PROPOSED NEW MECA Introduction from your negotiation team Kia ora koutou from your negotiation team. We
NZNO/DHB MECA 2017 Ehara taku toa i te toa takitahi, ēngari he toa taki mano 14 November 2017 YOUR PROPOSED NEW MECA Introduction from your negotiation team Kia ora koutou from your negotiation team. We
WAVE Project Plan
 WAVE Project Plan 2018-19 Project Title WAVE 2018-2019 Short Description Wellbeing and Vitality in Education: supporting our children and young people to learn well and be well. Commencement Date 1 July
WAVE Project Plan 2018-19 Project Title WAVE 2018-2019 Short Description Wellbeing and Vitality in Education: supporting our children and young people to learn well and be well. Commencement Date 1 July
MaORI POLICY DATE ADOPTED: 9 MAY 2017
 MaORI POLICY DATE ADOPTED: 9 MAY 2017 PERSON RESPONSIBLE: Māori Relationships Manager COMMITTEE RESPONSIBLE: Māori Standing Committee CATEGORY: Economic Development & Engagement STATUS: Final DATE REVISED
MaORI POLICY DATE ADOPTED: 9 MAY 2017 PERSON RESPONSIBLE: Māori Relationships Manager COMMITTEE RESPONSIBLE: Māori Standing Committee CATEGORY: Economic Development & Engagement STATUS: Final DATE REVISED
Operations Manager Orthopaedic Surgery
 Date: June 2017 Job Title : Operations Manager Department : Orthopaedic Service Location : All WDHB sites, including North Shore and Waitakere Hospitals Reporting To Clinical/Management Partnership : :
Date: June 2017 Job Title : Operations Manager Department : Orthopaedic Service Location : All WDHB sites, including North Shore and Waitakere Hospitals Reporting To Clinical/Management Partnership : :
POSITION DESCRIPTION
 POSITION DESCRIPTION Position Details: Title: Community Support Worker Department: Manawanui Oranga Hinengaro Kaupapa Maori Service Reports to: Team Leader Location: Whatua Kaimarie Marae Complex (Manawanui)
POSITION DESCRIPTION Position Details: Title: Community Support Worker Department: Manawanui Oranga Hinengaro Kaupapa Maori Service Reports to: Team Leader Location: Whatua Kaimarie Marae Complex (Manawanui)
NESP Nurse Advisor District Mental Health Service
 Date: August 2015 Job Title : NESP Nurse Educator Waitemata District Health Board & University of Auckland. Department : Mental Health Services Group Location : Mental Health Services sites Reporting To
Date: August 2015 Job Title : NESP Nurse Educator Waitemata District Health Board & University of Auckland. Department : Mental Health Services Group Location : Mental Health Services sites Reporting To
Position Description
 Position Description Position Details: Title: Intensivist Department: Critical Care Medicine Reports to: Location: Clinical Director, Department of Critical Care Medicine Auckland City Hospital Date: September
Position Description Position Details: Title: Intensivist Department: Critical Care Medicine Reports to: Location: Clinical Director, Department of Critical Care Medicine Auckland City Hospital Date: September
Operations Director, Specialist Community & Regional Services Clinical Director, Mental Health Director of Nursing
 TO Hospital Advisory Committee FROM Operations Director, Specialist Community & Regional Services Clinical Director, Mental Health Director of Nursing DATE 26 August 2014 SUBJECT Mental Health Review MEMORANDUM
TO Hospital Advisory Committee FROM Operations Director, Specialist Community & Regional Services Clinical Director, Mental Health Director of Nursing DATE 26 August 2014 SUBJECT Mental Health Review MEMORANDUM
Dermatologist. Position Description. Department : Dermatology Service, Medicine & Health of Older People Services
 Date: January 2015 Job Title : Dermatologist Department : Dermatology Service, Medicine & Health of Older People Services Location : Waitemata DHB (North Shore Hospital & Waitakere Hospital Sites) Reporting
Date: January 2015 Job Title : Dermatologist Department : Dermatology Service, Medicine & Health of Older People Services Location : Waitemata DHB (North Shore Hospital & Waitakere Hospital Sites) Reporting
Job Title HEALTH PROMOTING SCHOOLS ADVISOR
 Date: JULY 2014 JOB TITLE: Department: Location: Reporting To: Direct Reports: Functional Relationships with: HEALTH PROMOTING SCHOOLS ADVISOR Child and Family Waitemata DHB sites as required Team Leader
Date: JULY 2014 JOB TITLE: Department: Location: Reporting To: Direct Reports: Functional Relationships with: HEALTH PROMOTING SCHOOLS ADVISOR Child and Family Waitemata DHB sites as required Team Leader
Registered Nurse. Position Description. Location : Puriri Centre, Regional Forensic Psychiatry Services
 Date: January 2016 Job Title : Registered Nurse Department : Forensic Prison Team, Auckland Regional Forensic Psychiatry Services. Location : Puriri Centre, Regional Forensic Psychiatry Services Reporting
Date: January 2016 Job Title : Registered Nurse Department : Forensic Prison Team, Auckland Regional Forensic Psychiatry Services. Location : Puriri Centre, Regional Forensic Psychiatry Services Reporting
POSITION DESCRIPTION. Title: Interventional Radiology Co-ordinator Department: Interventional Radiology
 POSITION DESCRIPTION Position Details: Title: Interventional Radiology Co-ordinator Department: Interventional Radiology Reports: Service Manager Radiology Location: Auckland City Hospital Director Interventional
POSITION DESCRIPTION Position Details: Title: Interventional Radiology Co-ordinator Department: Interventional Radiology Reports: Service Manager Radiology Location: Auckland City Hospital Director Interventional
Bowel Screening Pilot (BSP) Maori Community Coordinator
 Maori Community Coordinator") Date: January 2018 Job Title : National Bowel Screening Programme (NBSP) Maori Health Promoter Department : Surgical and Ambulatory Services Location : Bowel Screening 2 Lake Pupuke Drive, Takapuna FTE
Date: January 2018 Job Title : National Bowel Screening Programme (NBSP) Maori Health Promoter Department : Surgical and Ambulatory Services Location : Bowel Screening 2 Lake Pupuke Drive, Takapuna FTE
Psychologist/Clinical Psychologist Marinoto CAMHS Position Description
 Date: March 2017 Job Title : Allied Health - Psychologist/ Clinical Psychologist Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships
Date: March 2017 Job Title : Allied Health - Psychologist/ Clinical Psychologist Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships
Northern Region Health Plan 2017/18
 Northern Region Health Plan 2017/18 November 2017 Foreword This is our seventh regional plan. Over recent years we have seen demonstrable improvements in our health services. More patients are getting
Northern Region Health Plan 2017/18 November 2017 Foreword This is our seventh regional plan. Over recent years we have seen demonstrable improvements in our health services. More patients are getting
Job Title:Psychotherapist/Child Psychotherapist Marinoto CAMHS Position Description
 Date: February 2013 Job Title : Allied health- Psychotherapist/ Child Psychotherapist Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional
Date: February 2013 Job Title : Allied health- Psychotherapist/ Child Psychotherapist Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional
Complaints and Adverse Events Manager Position Description
 Date : May 2016 Job Title : Complaints and Department : Corporate Quality Location : All Waitemata DHB sites (main office at NSH site) Reporting To : Quality and Risk Manager Direct Reports : Nil Functional
Date : May 2016 Job Title : Complaints and Department : Corporate Quality Location : All Waitemata DHB sites (main office at NSH site) Reporting To : Quality and Risk Manager Direct Reports : Nil Functional
PUBLIC HEALTH SERVICE HEALTH PROMOTION TIER TWO SERVICE SPECIFICATION
 All District Health Boards PUBLIC HEALTH SERVICE HEALTH PROMOTION TIER TWO SERVICE SPECIFICATION Status: Approved for recommended nationwide use for the non-mandatory description of services funded by
All District Health Boards PUBLIC HEALTH SERVICE HEALTH PROMOTION TIER TWO SERVICE SPECIFICATION Status: Approved for recommended nationwide use for the non-mandatory description of services funded by
Psychologist/Clinical Psychologist Position Description
 Date: Dec 2015 Job Title : Allied Health - Psychologist/ Clinical Psychologist Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships
Date: Dec 2015 Job Title : Allied Health - Psychologist/ Clinical Psychologist Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships
ACF(M)15/03 Minutes: GREATER GLASGOW AND CLYDE NHS BOARD
15/03 Minutes: GREATER GLASGOW AND CLYDE NHS BOARD") ACF(M)15/03 Minutes: 22-33 GREATER GLASGOW AND CLYDE NHS BOARD Minutes of a Meeting of the Area Clinical Forum held in Meeting Room A, J B Russell House, Corporate Headquarters, Gartnavel Royal Hospital,
ACF(M)15/03 Minutes: 22-33 GREATER GLASGOW AND CLYDE NHS BOARD Minutes of a Meeting of the Area Clinical Forum held in Meeting Room A, J B Russell House, Corporate Headquarters, Gartnavel Royal Hospital,
Pacific health evidence and outcomes?
 Pacific health evidence and outcomes? Outline Pacific population profile and health indicators Why so little progress? A Pacific family s engagement with primary care Engaging vulnerable consumers to improve
Pacific health evidence and outcomes? Outline Pacific population profile and health indicators Why so little progress? A Pacific family s engagement with primary care Engaging vulnerable consumers to improve
The Care Values Framework
 The Care Values Framework 2017-2020 1 States of Guernsey An electronic version of the framework can be found at gov.gg/carevaluesframework Contents Foreword from the Chief Secretary Page 05 Chief Nurse
The Care Values Framework 2017-2020 1 States of Guernsey An electronic version of the framework can be found at gov.gg/carevaluesframework Contents Foreword from the Chief Secretary Page 05 Chief Nurse
BLACKPOOL COUNCIL (CHILDREN S SERVICES; CHILDREN S CENTRES) And. BLACKPOOL TEACHING HOSPITALS NHS TRUST (Children s Community Health Services) DATED
 And. BLACKPOOL TEACHING HOSPITALS NHS TRUST (Children s Community Health Services) DATED") BLACKPOOL COUNCIL (CHILDREN S SERVICES; CHILDREN S CENTRES) And BLACKPOOL TEACHING HOSPITALS NHS TRUST (Children s Community Health Services) DATED 1 April 2012 31 March 2015 MEMORANDUM OF UNDERSTANDING
BLACKPOOL COUNCIL (CHILDREN S SERVICES; CHILDREN S CENTRES) And BLACKPOOL TEACHING HOSPITALS NHS TRUST (Children s Community Health Services) DATED 1 April 2012 31 March 2015 MEMORANDUM OF UNDERSTANDING
Healthy Skin in Greater Wellington Hui - 26 May 2011 Totara Lodge, Trentham, pm
 Healthy Skin in Greater Wellington Hui - 26 May 2011 Totara Lodge, Trentham, 2.00-4.00 pm Present: Adrian Gilliland (Clinical Advisor Primary and Integrated Care, Capital & Coast DHB) Api Poutasi (Public
Healthy Skin in Greater Wellington Hui - 26 May 2011 Totara Lodge, Trentham, 2.00-4.00 pm Present: Adrian Gilliland (Clinical Advisor Primary and Integrated Care, Capital & Coast DHB) Api Poutasi (Public
Nepean Blue Mountains Primary Health Network GP Advisory Committee TERMS OF REFERENCE
 Nepean Blue Mountains Primary Health Network GP Advisory Committee TERMS OF REFERENCE 1. Accountability 1.1 The GP Advisory Committee is an advisory body to the Board of Wentworth Healthcare Limited (
Nepean Blue Mountains Primary Health Network GP Advisory Committee TERMS OF REFERENCE 1. Accountability 1.1 The GP Advisory Committee is an advisory body to the Board of Wentworth Healthcare Limited (