Helping Patients Find Their Way. Managing Patient Transitions in the Health Care System
|
|
|
- Stephen Bridges
- 5 years ago
- Views:
Transcription


1 Helping Patients Find Their Way Managing Patient Transitions in the Health Care System
2 Helping Patients Find Their Way Opening Remarks Laurie Zimmer ED/ALC Manager
3 Patient Experience Video Shelley Dobson A Daughter s Experience

4 Helping Patients Find Their Way Panel Discussion #1

5 Helping Patients Find Their Way Keynote Katharine Byrick Partner Health Law Group

6 ESC LHIN Managing Transitions: Legal Framework for Discharge planning and Decision Making Katharine L. Byrick Partner, Health Law Group June 9, 2015
7 Overview Insured Services, when a patient is Ready for Discharge, and Alternative Level of Care Chronic care co-payments and per diem charges for Hospital beds. 7
8 What is an insured service Prescribed services of hospitals and health facilities are insured services. Health Insurance Act, R.S.O. 1993, c. H.6., s.11(2). 8
9 Entitlement to an Insured Service An insured person is not entitled to insured services in a hospital unless the person has been admitted as in-patient on the order of a physician. Regulation 552 to the Health Insurance Act, s.11(1)(a). 9
10 Admission to Hospital A hospital shall accept a person as an in-patient they require the level or type of hospital care provided, and on the order / authority of a physician who is a member of the medical staff at that Hospital. Public Hospitals Act, R.S.O. 1993, c.p.40. s.20. Regulation 965 to the Public Hospitals Act, s.11(1)(2). 10
11 Entitlement to an insured service The in-patient services to which an insured person is entitled without charge include accommodation and meals at the standard or public ward level. Health Insurance Act, s.12. Regulation 552 to the Health Insurance Act, s.7. 11
12 Ready for Discharge If a patient is no longer in need of treatment in the hospital, the attending physician shall make an order that the patient be discharged and shall also communicate the order to the patient. Public Hospitals Act, Hospital Management Regulation, s
13 Ready for Discharge Where an order has been made with respect to the discharge of a patient, the hospital shall discharge the patient and the patient shall leave the hospital on a date set out in the discharge order. Public Hospitals Act, Hospital Management Regulation, s
14 Ready for Discharge The administrator may grant permission for a patient to remain in the hospital for a period of up to twenty-four hours after the date set out in the discharge order. Public Hospitals Act, Hospital Management Regulation, s
15 Patients without a specific destination when ready for discharge A wide range of patients can fall into this category. The options for dealing with these patients will depend to a large degree on the situation of a particular patient. 15
16 Alternative Level of Care When a patient is occupying a bed in a hospital and does not require the intensity of resources/services provided in this care setting (Acute, Complex Continuing Care, Mental Health or Rehabilitation), the patient must be designated Alternate Level of Care (ALC) at that time by the physician or her/his delegate. 16
17 Alternative Level of Care (2) The ALC wait period starts at the time of designation and ends at the time of discharge/transfer to a discharge destination (or when the patient s needs or condition changes and the designation of ALC no longer applies) please see the provincial definition for complete statement, with notes. 17
18 Alternative Level of Care (3) Discharge destinations under the provincial ALC definition include: Home, with or without services Rehabilitation, Complex continuing care, long-term care Transitional care bed, convalescent care bed, palliative care bed Group home, retirement home, shelter, supportive housing 18
19 Alternative Level of Care (4) The definition does not apply to patients: Waiting at home Waiting in an acute care bed for another acute care bed. Waiting in a tertiary care bed for transfer to a non tertiary care bed (repatriation) 19
20 Co-Payments A co-payment for accommodation and meals that are insured services shall be made by or on behalf of an insured person who meets certain criteria. A chronic care co-payment IF the hospital is entitled to charge a copayment. Regulation 552 to the Health Insurance Act, s
21 Co-Payments The criteria: Patients are those who, in the opinion of their attending physician, require chronic care and are more or less permanently resident in a hospital or other institution. Regulation 552 to the Health Insurance Act, s
22 Co-payments v. per diem charges They are not the same! ALC patients may be charged a co-payment. ALC patients who refuse to fully participate in the discharge planning process may be charged a copayment. Per diem charges only apply when specific criteria is met. 22
23 Per Diem charges A Hospital may charge a per diem rate after the effective date of a discharge order, when a patient has refused to leave and/or declined to accept a long-term care bed from one of their facility choices. A discharge planning policy that contemplates a per diem charge should include certain elements. 23
24 Elements for policy of per diem charges 1. The attending physician has: a) discharged the patient, or b) is aware that a patient to be discharged is in receipt of a long-term care bed offer from among his or her facility choices and discharges that patient effective the date that the bed becomes available. 24
25 Elements for policy of per diem charges 2. The per diem rate for uninsured services that will be charged to a patient who remains in the Hospital past his or her discharge date is set out. 3. A rational explanation of the per diem rate for uninsured services is included. 25
26 Elements for policy of per diem charges 4. Any in-patient that is put on long-term care waiting lists shall be immediately notified of the Hospital s policy that s/he will be discharged as of the date that a bed becomes available at any one of his or her facility choices and that s/he will be charged the per diem rate for uninsured services from that date forward. 26
27 Dealing with Difficult Discharge Situations THE KEY IS COMMUNICATION All involved in the discharge planning process, and in the discharge plan, should be working together to form an appropriate plan. First question WHO makes the decision? Second question WHAT to consider in making a decision? 27
28 Capacity - HCCA A two-part test based on s. 4(1) HCCA: a) Is the person able to understand information relevant to making the decision? b) Is the person able to appreciate consequences of a decision or lack of decision? If the answer is yes to both questions: person is capable. Can apply to treatment, admission to a care facility or a personal assistive service. 28
29 Determining Capacity A patient is presumed to be capable The onus is on the evaluator to prove incapacity Evaluator may rely on this presumption unless reasonable grounds to believe otherwise Capacity can change! 29
30 Determining Capacity Test for capacity is objective two parts CCB: there must be cogent and compelling evidence of incapacity It is not enough to disagree with a person s decision to refuse to consent. 30
31 Doubts about capacity? If in doubt, the evaluator proposing a treatment / admission should conduct an evaluation and consider whether: a) The person is able to understand information relevant to making decision; and b) The person is able to appreciate the reasonably foreseeable consequences of treatment or lack of treatment 31
32 Follow up required on finding of incapacity Follow-up to finding of incapacity: a) In accordance with professional guidelines, evaluator must provide to the incapable person information about the consequences of the finding; b) Identify a Substitute Decision Maker (SDM) who may consent on the incapable person s behalf; and c) Document the capacity assessment and consent discussion in the patient s chart 32
33 Substitute Decision Makers (SDMs) and consent More on these in a few minutes!!! 33
34 Role of the Consent and Capacity Board, the CCB The CCB is an independent provincial tribunal that has been established to provide fair and accessible adjudication of consent and capacity issues, balancing the rights of vulnerable individuals with public safety. Consent and Capacity Board Website, online: Ontario Consent and Capacity Board, A Practical Guide to Mental Health and the Law in Ontario, October 2012, page
35 What does the CCB do? The CCB holds hearings under the: Health Care Consent Act Mental Health Act Personal Health Information Protection Act Substitute Decisions Act A complete list of the types of applications that may be made to the CCB can be found in Appendix C in the OHA s A Practical Guide to Mental Health and the Law in Ontario and on the CCB website. 35
36 Who can be a Substitute Decision-Maker? Guardian of the Person, if so authorized: SDA Attorney for Personal Care, is so authorized: SDA CCB appointed representative Spouse or Partner A child or custodial parent or CAS A parent with right of access only A brother or sister Any other relative None of the above: the Public Guardian and Trustee 36
37 SDM the essential ingredients Qualifications Person on the list of potential SDMs: s. 20(1) Capable with respect to the treatment At least 16; unless the parent Not prohibited by court order or separation agreement from having access or giving consent Available Willing to assume responsibility No higher ranking SDM 37
38 Public Guardian and Trustee Where there is no SDM who meets the requirements in s. 20(2), the PGT shall make the decision to give or refuse consent PGT also acts where two equally ranking SDMs are in conflict over a decision Investigations to determine need for guardianship of mentally incapable persons 38
39 Duties of the SDM SDM shall give or refuse consent according to certain principles: Must act in accordance with a prior capable wish, expressed by person > 16 years of age If no known prior, capable wish, must act in accordance with the incapable person s best interests 39
40 What are Best Interests? Values and beliefs held when person was capable; Any wishes expressed that are not P.C.W. ; The following factors: Will improve person s condition or well being Will prevent or reduce the rate of deterioration Will the patient improve, remain the same or deteriorate without Benefits of weighed against risk of harm Comparative benefit of a less restrictive or less intrusive, including no. 40
41 Consent for Admission to Long-Term Care This is often part of the discharge planning process. The definition for capacity with respect to admission to a care facility is the same as for treatment: a) Is the person able to understand information relevant to making the decision? b) Is the person able to appreciate consequences of a decision or lack of decision? 41
42 Consent in Discharge Planning Discharge planning is not limited to admission to a care facility. All aspects of a comprehensive discharge plan should be considered / reviewed in this process. Will likely involve several members of multidisciplinary team. 42
43 Elements of Consent Must relate to the admissions / proposed treatment Must be informed Must be given voluntarily Must not be obtained through fraud or misrepresentation 43
44 Informed Consent - Admission What the admission entails The expected advantages and disadvantages of admission Alternatives to admission The likely consequences of not being admitted 44
45 Informed consent things to remember Ensure that all of the person s questions about the treatment are answered. Following an informed consent discussion, the capable person or SDM is entitled to either consent or refuse to consent to the proposed treatment / admission. Refusal of treatment / admission by a capable person is lawful, even when the refusal jeopardizes life. 45
46 The role of the patient, SDM, family and health care providers What is the proposal for which consent is being sought? Who should be making the decision? What factors should be considered? How quickly should a decision be made? 46
47 Thank you!! 47

48 Helping Patients Find Their Way Keynote Dale Clement Chief Executive Officer Waterloo Wellington CCAC
49 Lunch
50 5-Minute Countdown Video Calendar Girl
51 Patient Experience Video Robert Falconer

52 Helping Patients Find Their Way Presentation Daniel Ball Director of Patient Care & Clinical Analytics Central West CCAC


53 Innovative Health Care Without Boundaries Daniel Ball, June 9 th, 2015 Central West CCAC 53
54 Background Our Team Central West LHIN Is home to over 840 thousand residents living in one of the fastest growing and most culturally diverse regions of Canada 23 Long-Term Care Homes (LTC) providing an estimated 750,000 resident days/year Over 600 Primary Care Physicians 2 hospital corporations (William Osler Health System and Headwaters Health Care Centre), operating 3 hospital sites attending over 70,000 hospital admissions and 233,500 unscheduled ED visits/year 54
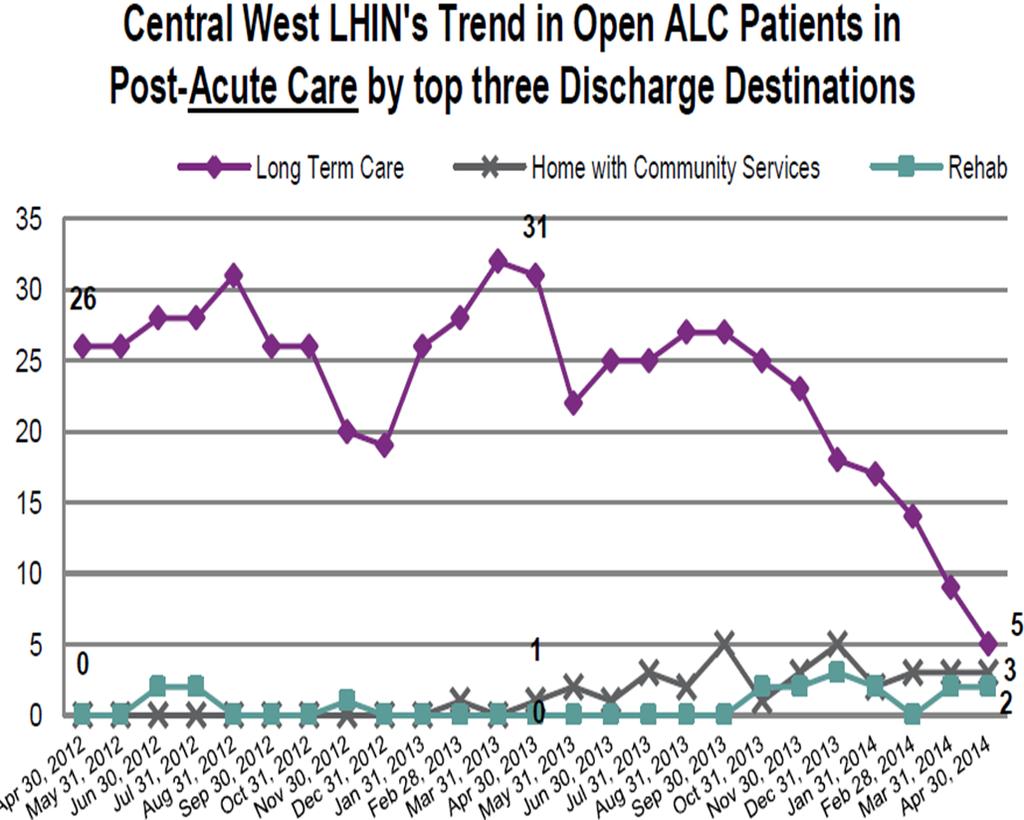
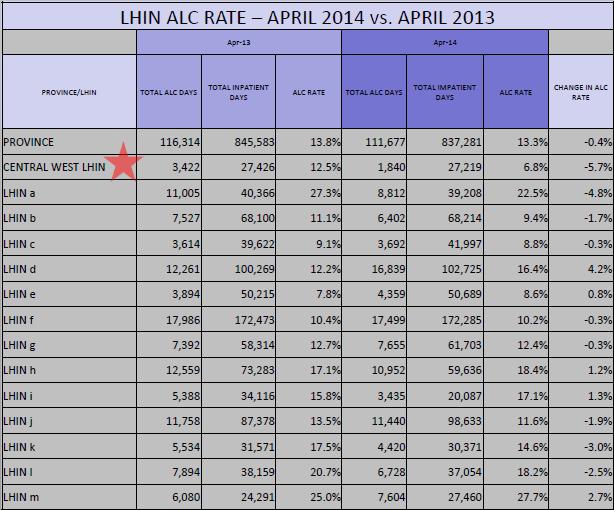
55 Need for Our Team Change In April 2013, 13.3% of Ontario s hospital beds were patients deemed as Alternate Level of Care (ALC) the equivalent to over 116,000 ALC days. In Central West, ALC patients accumulated over 3,400 days (12.5%) which dramatically impacted the efficiency of patient flow. As the majority of these patients were identified as waiting for long-term care (LTC), CW CCAC and WOHS partnered to redesign Home First Strategies. 55

56 56

57 Intro- Home first Redesign Formulating strategy is one thing. Executing Formulating it throughout strategy the entire is one organization thing.... well, that s the really hard well, part. that s Without the effective really hard execution, part. no business strategy can succeed. Executing it throughout the entire organization... Without effective execution, no change strategy can succeed. 57
58 Home First Philosophy The principle of a Home First philosophy is that patients should, where clinically appropriate, return to a home environment in the community following an acute care admission. Home First is not a mandatory program, it is a philosophy intended to promote the Ministry s overarching goal of providing appropriate care in the appropriate setting. There may be some ALC patients for whom a discharge home, even on an interim or transitional basis, is not an appropriate option. 58
59 Patient Flow Objectives Vision Exceptional Patient Experience High Quality Patient Care Smooth Transitions Improved Patient Flow/ Reduced ALC volumes Standardized Processes and Communication Minimize errors in the consent process Integrated Team Optimize roles and minimize duplication 59
60 60
61 61


62 Key Success Our Team Factors Strong Partnerships, Collaboration and Shared Accountabilities to improve the Patient Experience 62
63 Home first Redesign -Approach and Key Success factors- 63


64 System Wide Collaboration and Engagement How can we work together differently? 64
65 System Wide Collaboration and Engagement Hospital Physicians Discharge Care Coordinators CCAC Care Coordinators Professional Practice (Allied Health) Ethicist Legal Counsel LTC Senior Leadership Clinical Management Finance Access & Flow Nursing Community Partners IT/ Decision Support Primary Care 65

66 Review, Identify and Share Performance Our Opportunities Team 66
67 Cause and Effect PEOPLE PROCEDURES Hospital Physicians Allied Discharge Cord CCAC Primary Care Patient/SDM BSO Contracted Service Providers Escalation Med rec Consent Joint Meetings LHIN Boundaries Escalation Team Community Partners Decision Support/IT LTC Health Reports Pathways/Scripts Service bundles ALC Rates Delays Not ordered Hoyer Hospital Bed Not available Consent and Capacity SDM LTC Legislation Hospital Policy/Act EQUIPMENT POLICY Different people own different parts of this problem
68 Cause and Effect PEOPLE PROCEDURES Hospital Physicians Allied Discharge Cord CCAC Primary Care Patient/SDM BSO Contracted Service Providers Escalation Med rec Consent Joint Meetings LHIN Boundaries Escalation Team Community Partners Decision Support/IT LTC Health Reports Pathways/Scripts Service bundles ALC Rates Delays Not ordered Hoyer Hospital Bed Not available Consent and Capacity SDM LTC Legislation Hospital Policy/Act EQUIPMENT We often look for person(s) responsible for the delays rather than looking at the big picture POLICY
 BORROW")
69 Build on Our Best Team Practice Research and consult provincial leaders Evidence based LEND (=give) BORROW (=take) 69
70 Provide Role Clarity: Who is doing what on discharge? Patient Choosing where he/she would like to go after discharge Consenting or withholding consent if something is proposed, and he/she is capable Hospital Team Discharging & developing recommendations to help patient achieve his/her discharge goals The designation of ALC is determined by the physician in collaboration with the interprofessional team CCAC Proposing long term care and/or home care, assisted services Substitute Decision Maker (if required) Providing or withholding consent to what is proposed, in accordance with the principles of substitute decision making from the Health Care Consent Act 70
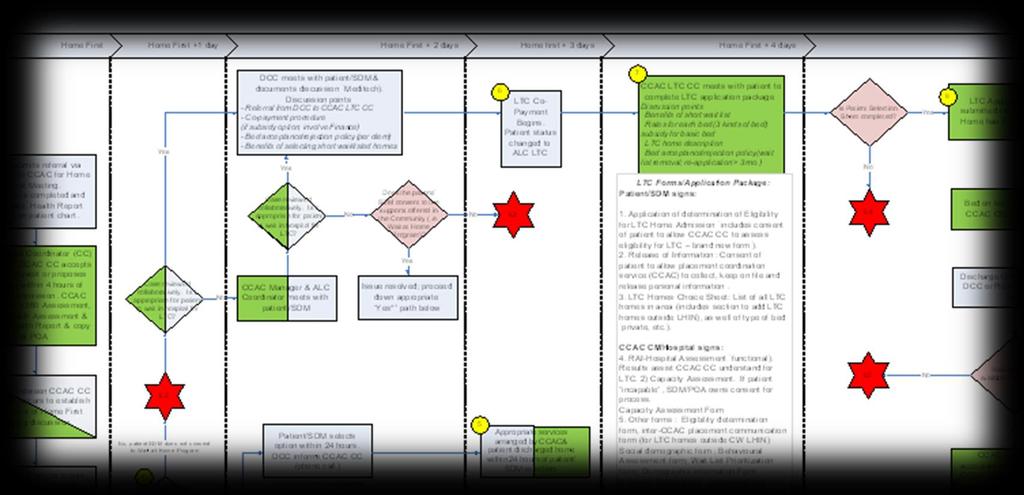

71 Standardized Processes and Pathways 71
72 Optimize Technology Optimize Technology to improve efficiencies Referral Processes Patient lists/census/triage Reporting and monitoring * Optimize roles and minimize duplication 72
73 Documentation Standards Review Documentation Standards Identify and share common errors Create checklists Develop documentation templates 73
 when the patient in incapable 4. not always meet documentation standards to support actions/decisions (i.e. capacity assessments) 5.")
74 Minimize Errors in the Consent Process Health care professionals may: 1. seek consent for decisions that do not require it 2. take direction from a family member when the patient is capable 3. take direction from the wrong substitute decision-maker (SDM) when the patient in incapable 4. not always meet documentation standards to support actions/decisions (i.e. capacity assessments) 5. know of a prior expressed wish but ignore that wish when considering a placement plan 6. wait for an SDM who is not available, willing and capable, instead of proceeding down the hierarchy of decision-makers 7. not use an interpreter when is required 8. identify a POA without seeing/obtaining the POA document 74
75 Consent to Long-Term Care Exploration of patient values, wishes and beliefs around LTC Only CCAC can propose LTC to a capable patient or, in the event of their incapacity, his/her substitute decision-maker (SDM) SDM has legal obligations to: Act on behalf of the patient and not based on his/her own preferences Consent/refuse in accordance with prior expressed, capable wishes Consent/refuse in best interests of patient 75
76 Standardized Communication Scripts developed for staff; Accurate, clear and coordinated communication are key to successful discharge planning. Equips staff with tools to engage in appropriate conversations with patients. Enables staff to meet legal and ethical obligations and avoid common consent errors. Facilitates consistency in messaging and encourages one voice, one team philosophy 76
77 Customized Training and Communication Our Team Customized Training and Communication Hospital CCAC Care Coordinators and Discharge Care Coordinators Allied Professionals Nursing Clinical Managers Hospital Physicians Primary Care LTC Community Support Partners (i.e. assisted living, Retirement Homes) CCAC staff and Contracted Service Providers 77
78 Leadership Create Support Teams Created to support staff (all levels) Meets weekly to review/strategize complex discharges Leadership presence Walk the talk 78

79 Leadership 79
 Meets weekly to")
80 Our Metrics, Team Anyone keeping score? Leadership Support Team Created to support staff (all levels) Meets weekly to review/strategize complex discharges jjjjj jjjjj jjjjj jjjjj jj 80
81 Performance outcomes Home First- Number of Patients Enrolled 2013/ / Readmission Rates 2013/14-14% 2014/15-9 % ALC % % % (February) 81
82 Monitor, Adjust and Sustain 82
83 Performance outcomes Monthly Budget vs Actual 5,300,000 5,100,000 4,900,000 4,700,000 4,500,000 4,300,000 4,100,000 3,900,000 Apr '14 May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Proj'n** Actual Gold and Budget Green Updated Budget Feb '15 In Home excluding PT/E&F Actual Feb 2015 per GL In Home excluding PT/E&F 83
84 Testimonies When staff were asked about the impact of the revised Home First framework on their patients and practice, here s what staff had to say: Having more specific points of contact and knowing exactly who/how I can ask for additional support is a vital component that has improved the process. The new improvements to the Home First process have been beneficial for various reasons such as: -Adding structure to the process making planning and implementation move more smoothly and efficiently. -Allowing Discharge Coordinators to better understand the Home First process through clarification of our role, in addition to the clarification of the roles of other disciplines. We are all talking now from the same book! 84

85 Leading Change 85
86 Our Summary Team Strong Partnerships, collaboration and shared accountabilities to improve the Patient Experience Engage all key Stakeholders Research and consult provincial leaders Identify and share performance opportunities Evidence based Standardize Processes Define Roles & Accountabilities Standardized Communication Staff Training and Resources Minimize errors in the consent process Create Support Teams-Leadership Presence Optimize Technology Monitor, adjust, and sustain 86
87 Take away messages One team, one voice. Build processes around the patient. Don t work patients around the processes. Nothing about me without me- talk with the capable patient Capable patients can choose to live at risk When patients are incapable, ensure the SDM(s) understand their role and that they are making decisions in the best interest of the patient. CCAC s are the placement co-ordinators for admission to long term care homes in Ontario. This role is designated in legislation and cannot be delegated. 87

88 Thank You For your time 88
89 Patient Experience Video Kathryn Brooker

90 Helping Patients Find Their Way Presentation Jane Meadus Barrister & Solicitor Institutional Advocate Advocacy Centre for the Elderly
91 Patient Experience Video Madeline Kerr

92 Helping Patients Find Their Way Panel Discussion #2

93 Helping Patients Find Their Way Closing Remarks Laurie Zimmer ED/ALC Manager


94


95 Questions
96 Thank you
Major Features of the Legislation 3 The Health Care Consent Act, 1996 (HCCA) 3 The Substitute Decisions Act, 1992 (SDA) 4
 3 The Substitute Decisions Act, 1992 (SDA) 4") PRACTICE GUIDELINE Consent Table of Contents Introduction 3 Major Features of the Legislation 3 The Health Care Consent Act, 1996 (HCCA) 3 The Substitute Decisions Act, 1992 (SDA) 4 Definitions 4 Basic
PRACTICE GUIDELINE Consent Table of Contents Introduction 3 Major Features of the Legislation 3 The Health Care Consent Act, 1996 (HCCA) 3 The Substitute Decisions Act, 1992 (SDA) 4 Definitions 4 Basic
CLEONet. for community workers and advocates who work with low income and disadvantaged communities in Ontario.
 This webinar is brought to you by CLEONet www.cleonet.ca ca CLEONet is a web site of legal information for community workers and advocates who work with low income and disadvantaged communities in Ontario.
This webinar is brought to you by CLEONet www.cleonet.ca ca CLEONet is a web site of legal information for community workers and advocates who work with low income and disadvantaged communities in Ontario.
Managing Transitions. A Guidance Document
 Managing Transitions A Guidance Document Disclaimer This resource document was prepared for the ownership and use of the Ontario Hospital Association (OHA) and the Ontario Association of Community Care
Managing Transitions A Guidance Document Disclaimer This resource document was prepared for the ownership and use of the Ontario Hospital Association (OHA) and the Ontario Association of Community Care
Seniors Rights Through the Continuum of Care. Judith Wahl Advocacy Centre for the Elderly
 Seniors Rights Through the Continuum of Care Judith Wahl Advocacy Centre for the Elderly wahlj@lao.on.ca www.acelaw.ca Advocacy Centre for The Elderly 2 Carlton Street, Suite 701 Toronto, Ontario M5B 1J3
Seniors Rights Through the Continuum of Care Judith Wahl Advocacy Centre for the Elderly wahlj@lao.on.ca www.acelaw.ca Advocacy Centre for The Elderly 2 Carlton Street, Suite 701 Toronto, Ontario M5B 1J3
A Guide to Consent and Capacity in Ontario
 A Guide to Consent and Capacity in Ontario Table of Contents Introduction... 1 What Is Informed Consent and Capacity?... 2 Exceptions to Informed Consent and Capacity... 2 Who Determines Capacity?... 4
A Guide to Consent and Capacity in Ontario Table of Contents Introduction... 1 What Is Informed Consent and Capacity?... 2 Exceptions to Informed Consent and Capacity... 2 Who Determines Capacity?... 4
25 COMMON MISCONCEPTIONS ABOUT THE SUBSTITUTE DECISIONS ACT AND HEALTH CARE CONSENT ACT
 25 COMMON MISCONCEPTIONS ABOUT THE SUBSTITUTE DECISIONS ACT AND HEALTH CARE CONSENT ACT INTRODUCTION By: Judith Wahl, LL.B. Executive Director, ACE This paper focuses on common misconceptions or misunderstandings
25 COMMON MISCONCEPTIONS ABOUT THE SUBSTITUTE DECISIONS ACT AND HEALTH CARE CONSENT ACT INTRODUCTION By: Judith Wahl, LL.B. Executive Director, ACE This paper focuses on common misconceptions or misunderstandings
Assessments of Decisional Capacity Who Does an Assessment and How is it to be done. Judith A. Wahl Advocacy Centre for the Elderly
 Assessments of Decisional Capacity Who Does an Assessment and How is it to be done Judith A. Wahl Advocacy Centre for the Elderly Advocacy Centre for The Elderly 2 Carlton Street, Suite 701 Toronto, Ontario
Assessments of Decisional Capacity Who Does an Assessment and How is it to be done Judith A. Wahl Advocacy Centre for the Elderly Advocacy Centre for The Elderly 2 Carlton Street, Suite 701 Toronto, Ontario
CLEONet. for community workers and advocates who work with low income and disadvantaged communities in Ontario.
 This webinar is brought to you by CLEONet www.cleonet.ca ca CLEONet is a web site of legal information for community workers and advocates who work with low income and disadvantaged communities in Ontario.
This webinar is brought to you by CLEONet www.cleonet.ca ca CLEONet is a web site of legal information for community workers and advocates who work with low income and disadvantaged communities in Ontario.
Advance Care Planning Workbook Ontario Edition
 Advance Care Planning Workbook Ontario Edition Speak Up Ontario c/o Hospice Palliative Care Ontario, 2 Carlton Street, Suite 808, Toronto, Ontario M5B 1J3 Who will speak for you? Start the conversation.
Advance Care Planning Workbook Ontario Edition Speak Up Ontario c/o Hospice Palliative Care Ontario, 2 Carlton Street, Suite 808, Toronto, Ontario M5B 1J3 Who will speak for you? Start the conversation.
FIRST AVAILABLE BED POLICIES & DISCHARGE TO A LONG-TERM CARE HOME FROM HOSPITAL
 FIRST AVAILABLE BED POLICIES & DISCHARGE TO A LONG-TERM CARE HOME FROM HOSPITAL Jane E. Meadus Barrister & Solicitor Institutional Advocate Many people end up thinking about long-term care 1 for themselves
FIRST AVAILABLE BED POLICIES & DISCHARGE TO A LONG-TERM CARE HOME FROM HOSPITAL Jane E. Meadus Barrister & Solicitor Institutional Advocate Many people end up thinking about long-term care 1 for themselves
Advance Care Planning In Ontario. Judith Wahl B.A., LL.B. Advocacy Centre for the Elderly 2 Carlton Street, Ste 701 Toronto, Ontario M5B 1J3
 Advance Care Planning In Ontario Judith Wahl B.A., LL.B. Advocacy Centre for the Elderly 2 Carlton Street, Ste 701 Toronto, Ontario M5B 1J3 wahlj@lao.on.ca www.advocacycentreelderly.org What is Advance
Advance Care Planning In Ontario Judith Wahl B.A., LL.B. Advocacy Centre for the Elderly 2 Carlton Street, Ste 701 Toronto, Ontario M5B 1J3 wahlj@lao.on.ca www.advocacycentreelderly.org What is Advance
Transitions in Care. Discharge Planning Pathway & Dashboard
 Transitions in Care Discharge Planning Pathway & Dashboard Scott Jarrett Executive Vice President and Chief of Clinical Programs Humber River Hospital Carol Hatcher Vice President Clinical Programs Humber
Transitions in Care Discharge Planning Pathway & Dashboard Scott Jarrett Executive Vice President and Chief of Clinical Programs Humber River Hospital Carol Hatcher Vice President Clinical Programs Humber
Capability and Consent Tool B.C. Edition
 Capability and Consent Tool B.C. Edition Introduction The Capability and Consent Tool, BC Edition, was developed to assist health care providers to navigate through the complicated system of guardianship
Capability and Consent Tool B.C. Edition Introduction The Capability and Consent Tool, BC Edition, was developed to assist health care providers to navigate through the complicated system of guardianship
Schedule 3. Services Schedule. Social Work
 Schedule 3 Services Schedule Social Work Page 1 of 43 TABLE OF CONTENTS SECTION 1 INTERPRETATION... 4 1.1 Definitions... 4 1.2 Supplementing the General Conditions... 7 SECTION 2 CCAC PLANNING AND REQUESTING
Schedule 3 Services Schedule Social Work Page 1 of 43 TABLE OF CONTENTS SECTION 1 INTERPRETATION... 4 1.1 Definitions... 4 1.2 Supplementing the General Conditions... 7 SECTION 2 CCAC PLANNING AND REQUESTING
The Role of Community Care Access Centres in Admission to Long-Term Care from Hospital
 The Role of Community Care Access Centres in Admission to Long-Term Care from Hospital By: Jane E. Meadus, Institutional Advocate & Staff Lawyer This article was originally published in the Advocacy Centre
The Role of Community Care Access Centres in Admission to Long-Term Care from Hospital By: Jane E. Meadus, Institutional Advocate & Staff Lawyer This article was originally published in the Advocacy Centre
Responsibilities Under Consent Legislation
 JULY 2014 Responsibilities Under Consent Legislation P R O F E S S I O N A L P R A C T I C E G U I D E L I N E COLLEGE OF RESPIRATORY ThERAPISTS OF ONTARIO Professional Practice Guideline CRTO publications
JULY 2014 Responsibilities Under Consent Legislation P R O F E S S I O N A L P R A C T I C E G U I D E L I N E COLLEGE OF RESPIRATORY ThERAPISTS OF ONTARIO Professional Practice Guideline CRTO publications
Advance Care Planning The Legal Issues. Judith Wahl B.A., LL.B. Advocacy Centre for the Elderly 1 2 Carlton Street, Ste 701 Toronto, Ontario M5B 1J3
 Advance Care Planning The Legal Issues Judith Wahl B.A., LL.B. Advocacy Centre for the Elderly 1 2 Carlton Street, Ste 701 Toronto, Ontario M5B 1J3 wahlj@lao.on.ca www.advocacycentreelderly.org What is
Advance Care Planning The Legal Issues Judith Wahl B.A., LL.B. Advocacy Centre for the Elderly 1 2 Carlton Street, Ste 701 Toronto, Ontario M5B 1J3 wahlj@lao.on.ca www.advocacycentreelderly.org What is
Health Care Consent & Advance Care Planning in Ontario. What You Need to Know. Health Care Consent Advance Care Planning Community of Practice
 Health Care Consent & Advance Care Planning in Ontario What You Need to Know Health Care Consent Advance Care Planning Community of Practice Welcome Introductions Webinar Instructions If you have a mute
Health Care Consent & Advance Care Planning in Ontario What You Need to Know Health Care Consent Advance Care Planning Community of Practice Welcome Introductions Webinar Instructions If you have a mute
NAVIGATING AROUND THE ISSUES OF CAPACITY
 NAVIGATING AROUND THE ISSUES OF CAPACITY 14 th ANNUAL ESTATES & TRUSTS SEMINAR presented by: The Hamilton Law Association February 11, 2016 Prepared by: Jane Meadus Advocacy Centre for the Elderly 2 Carlton
NAVIGATING AROUND THE ISSUES OF CAPACITY 14 th ANNUAL ESTATES & TRUSTS SEMINAR presented by: The Hamilton Law Association February 11, 2016 Prepared by: Jane Meadus Advocacy Centre for the Elderly 2 Carlton
Health Care Consent Advance Care Planning Community (HCC ACP CoP) of Practice (HCC ACP CoP) HCC ACP IN ONTARIO SUMMARY OF KEY THEMES AND COMMON ERRORS
 of Practice (HCC ACP CoP) HCC ACP IN ONTARIO SUMMARY OF KEY THEMES AND COMMON ERRORS") Health Care Consent Advance Care Planning Community (HCC ACP CoP) of Practice (HCC ACP CoP) HCC ACP IN ONTARIO SUMMARY OF KEY THEMES AND COMMON ERRORS HCCA Ontario https://www.ontario.ca/laws/statute/96h02
Health Care Consent Advance Care Planning Community (HCC ACP CoP) of Practice (HCC ACP CoP) HCC ACP IN ONTARIO SUMMARY OF KEY THEMES AND COMMON ERRORS HCCA Ontario https://www.ontario.ca/laws/statute/96h02
SDMs and Health Decision Making
 1 SDMs and Health Decision Making Judith Wahl Wahl Elder Law wahlelderlaw@gmail.com 416-209-3407 2 Disclaimer This presentation and any material provided for this presentation is not legal advice but is
1 SDMs and Health Decision Making Judith Wahl Wahl Elder Law wahlelderlaw@gmail.com 416-209-3407 2 Disclaimer This presentation and any material provided for this presentation is not legal advice but is
End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces.
 End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces. Terms Definitions End of Life Care To assist persons who
End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces. Terms Definitions End of Life Care To assist persons who
Health System Performance and Accountability Division MOHLTC. Transitional Care Program Framework
 Transitional Care Program Framework August, 2010 1 Table of Contents 1. Context... 3 2. Transitional Care Program Framework... 4 3. Transitional Care Program in the Hospital Setting... 5 4. Summary of
Transitional Care Program Framework August, 2010 1 Table of Contents 1. Context... 3 2. Transitional Care Program Framework... 4 3. Transitional Care Program in the Hospital Setting... 5 4. Summary of
Quality Management Report 2017 Q2
 Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Making decisions for others Your role as a Substitute Decision Maker
 Making decisions for others Your role as a Substitute Decision Maker Your loved one may not be able to make decisions about his or her health care. This may be a very difficult time for you and your family.
Making decisions for others Your role as a Substitute Decision Maker Your loved one may not be able to make decisions about his or her health care. This may be a very difficult time for you and your family.
9/23/2011. October 2011 Community Treatment Orders and Other Changes to the Mental Health Act
 October 2011 Community Treatment Orders and Other Changes to the Mental Health Act 1 Introduction of Guest Speaker: Gale Melligan, RN, BA, CPMHN(C) CTO Coordinator, St. Joseph s Healthcare Hamilton Mental
October 2011 Community Treatment Orders and Other Changes to the Mental Health Act 1 Introduction of Guest Speaker: Gale Melligan, RN, BA, CPMHN(C) CTO Coordinator, St. Joseph s Healthcare Hamilton Mental
Advance Care Planning in Ontario
 Advance Care Planning in Ontario By Judith A. Wahl B.A., L.L.B. Over the last few years, there has been an increased interest in advance directives from hospitals; long-term care facilities, community-based
Advance Care Planning in Ontario By Judith A. Wahl B.A., L.L.B. Over the last few years, there has been an increased interest in advance directives from hospitals; long-term care facilities, community-based
CHANGES IN ELIGIBILITY CRITERIA IN THE LONG-TERM CARE HOMES ACT, 2007
 CHANGES IN ELIGIBILITY CRITERIA IN THE LONG-TERM CARE HOMES ACT, 2007 By: Jane E. Meadus Institutional Advocate Barrister & Solicitor www.acelaw.ca With the enactment of the Long-Term Care Homes Act (LTCHA)
CHANGES IN ELIGIBILITY CRITERIA IN THE LONG-TERM CARE HOMES ACT, 2007 By: Jane E. Meadus Institutional Advocate Barrister & Solicitor www.acelaw.ca With the enactment of the Long-Term Care Homes Act (LTCHA)
Schedule 3. Services Schedule. Speech-Language Pathology
 Speech-Language Pathology Services Schedule 20112012 Consolidated Services Version Template Document Final February, 2011Version September, 2012 Schedule 3 Services Schedule Speech-Language Pathology Speech-Language
Speech-Language Pathology Services Schedule 20112012 Consolidated Services Version Template Document Final February, 2011Version September, 2012 Schedule 3 Services Schedule Speech-Language Pathology Speech-Language
Advance Care Planning in Ontario A Quality Improvement Toolkit
 Advance Care Planning in Ontario A Quality Improvement Toolkit Introduction What is the Advance Care Planning (ACP) Quality Improvement Toolkit? In January 2013, the Ministry of Health and Long Term Care
Advance Care Planning in Ontario A Quality Improvement Toolkit Introduction What is the Advance Care Planning (ACP) Quality Improvement Toolkit? In January 2013, the Ministry of Health and Long Term Care
Schedule 3. Services Schedule. Occupational Therapy
 Occupational Therapy Services Schedule 2014 Consolidated Services Version Template Final Version September, 2014 Schedule 3 Services Schedule Occupational Therapy Occupational Therapy Services Schedule
Occupational Therapy Services Schedule 2014 Consolidated Services Version Template Final Version September, 2014 Schedule 3 Services Schedule Occupational Therapy Occupational Therapy Services Schedule
GP SERVICES COMMITTEE Palliative Care INCENTIVES. Revised January 2018
 GP SERVICES COMMITTEE Palliative Care INCENTIVES Revised January 2018 GPSC Palliative Care Planning and Management Fees The following incentive payments are available to B.C. s eligible family physicians.
GP SERVICES COMMITTEE Palliative Care INCENTIVES Revised January 2018 GPSC Palliative Care Planning and Management Fees The following incentive payments are available to B.C. s eligible family physicians.
Patient rights and responsibilities
 Patients have rights and responsibilities, and this leaflet will provide you with more information on what you can expect from us, and what we expect of you. Erasmus MC Erasmus MC is a university medical
Patients have rights and responsibilities, and this leaflet will provide you with more information on what you can expect from us, and what we expect of you. Erasmus MC Erasmus MC is a university medical
ISSUES IN LONG-TERM CARE
 ISSUES IN LONG-TERM CARE By Jane E. Meadus Advocacy Centre for the Elderly June 4, 2014 1 ISSUES Admission Home First Philosophy ALC Co-payment Regulated Documents Resident s Rights Reporting in LTC Complaints
ISSUES IN LONG-TERM CARE By Jane E. Meadus Advocacy Centre for the Elderly June 4, 2014 1 ISSUES Admission Home First Philosophy ALC Co-payment Regulated Documents Resident s Rights Reporting in LTC Complaints
Table of Contents 1.0 PURPOSE DEFINITIONS POLICY Requirement for Valid Consent... 3
 AL0100 CONSENT - ADULTS Table of Contents 1.0 PURPOSE... 2 2.0 DEFINITIONS... 2 3.0 POLICY... 3 3.1 Requirement for Valid Consent... 3 3.2 Exceptions from Obtaining Consent... 3 3.3 Responsibility, Hierarchy
AL0100 CONSENT - ADULTS Table of Contents 1.0 PURPOSE... 2 2.0 DEFINITIONS... 2 3.0 POLICY... 3 3.1 Requirement for Valid Consent... 3 3.2 Exceptions from Obtaining Consent... 3 3.3 Responsibility, Hierarchy
Mental Health Services - Delayed Discharges: Update
 NHS Greater Glasgow & Clyde NHS Board Meeting Chief Officer, Glasgow City HSCP and Nurse Director October 20 Paper No: /56 Mental Health Services - Delayed Discharges: Update Recommendation:- The NHS Board
NHS Greater Glasgow & Clyde NHS Board Meeting Chief Officer, Glasgow City HSCP and Nurse Director October 20 Paper No: /56 Mental Health Services - Delayed Discharges: Update Recommendation:- The NHS Board
THE PLAIN LANGUAGE PROVIDER GUIDE TO THE UTAH ADVANCE HEALTH CARE DIRECTIVE ACT
 UTAH COMMISSION ON AGING THE PLAIN LANGUAGE PROVIDER GUIDE TO THE UTAH ADVANCE HEALTH CARE DIRECTIVE ACT Utah Code 75-2a-100 et seq. Decision Making Capacity Definitions "Capacity to appoint an agent"
UTAH COMMISSION ON AGING THE PLAIN LANGUAGE PROVIDER GUIDE TO THE UTAH ADVANCE HEALTH CARE DIRECTIVE ACT Utah Code 75-2a-100 et seq. Decision Making Capacity Definitions "Capacity to appoint an agent"
To ensure clear and consistent communication and processes for levying charges on patients who are:
 TITLE ALTERNATE LEVEL OF CARE ACCOMMODATION CHARGES - PATIENTS WAITING FOR CONTINUING CARE SCOPE Provincial: Finance DOCUMENT # FS-01 APPROVAL LEVEL Executive Leadership Team SPONSOR Finance (Treasurer)
TITLE ALTERNATE LEVEL OF CARE ACCOMMODATION CHARGES - PATIENTS WAITING FOR CONTINUING CARE SCOPE Provincial: Finance DOCUMENT # FS-01 APPROVAL LEVEL Executive Leadership Team SPONSOR Finance (Treasurer)
Palliative Care. Care for Adults With a Progressive, Life-Limiting Illness
 Palliative Care Care for Adults With a Progressive, Life-Limiting Illness Summary This quality standard addresses palliative care for people who are living with a serious, life-limiting illness, and for
Palliative Care Care for Adults With a Progressive, Life-Limiting Illness Summary This quality standard addresses palliative care for people who are living with a serious, life-limiting illness, and for
Guidelines for Issuing a Certificate of Incapability Under the Patients Property Act
 Guidelines for Issuing a Certificate of Incapability Under the Patients Property Act TABLE OF CONTENTS OVERVIEW 3 1 Using These Guidelines 3 1.1 Background 3 1.2 Reason for the Guidelines 3 1.3 Who will
Guidelines for Issuing a Certificate of Incapability Under the Patients Property Act TABLE OF CONTENTS OVERVIEW 3 1 Using These Guidelines 3 1.1 Background 3 1.2 Reason for the Guidelines 3 1.3 Who will
Elder Abuse Response: Things you NEED to know for Effective Intervention
 Elder Abuse Response: Things you NEED to know for Effective Intervention Judith Wahl www.acelaw.ca wahlj@lao.on.ca 2014 1 Focus of Presentation Primarily focused to service providers of any type and friends
Elder Abuse Response: Things you NEED to know for Effective Intervention Judith Wahl www.acelaw.ca wahlj@lao.on.ca 2014 1 Focus of Presentation Primarily focused to service providers of any type and friends
Medical Assistance in Dying
 College of Physicians and Surgeons of Ontario POLICY STATEMENT #4-16 Medical Assistance in Dying APPROVED BY COUNCIL: REVIEWED AND UPDATED: PUBLICATION DATE: KEY WORDS: RELATED TOPICS: LEGISLATIVE REFERENCES:
College of Physicians and Surgeons of Ontario POLICY STATEMENT #4-16 Medical Assistance in Dying APPROVED BY COUNCIL: REVIEWED AND UPDATED: PUBLICATION DATE: KEY WORDS: RELATED TOPICS: LEGISLATIVE REFERENCES:
Legal Issues Advance Care Planning Advance Directives. May 9, 2014
 Legal Issues Advance Care Planning Advance Directives May 9, 2014 Advance Health Care Directives Two types: Instructive Directive Proxy Directive Provides information to health care professionals if a
Legal Issues Advance Care Planning Advance Directives May 9, 2014 Advance Health Care Directives Two types: Instructive Directive Proxy Directive Provides information to health care professionals if a
Specific Decision-making & Emergency Decision-making. Adult Guardianship and Trusteeship Act (AGTA)
") Specific Decision-making & Emergency Decision-making Adult Guardianship and Trusteeship Act (AGTA) 1 How the AGTA was created Extensive community consultation 4330+ Albertans: guardians, trustees, physicians,
Specific Decision-making & Emergency Decision-making Adult Guardianship and Trusteeship Act (AGTA) 1 How the AGTA was created Extensive community consultation 4330+ Albertans: guardians, trustees, physicians,
Getting Ready for Ontario s Privacy Legislation GUIDE. Privacy Requirements and Policies for Health Practitioners
 Getting Ready for Ontario s Privacy Legislation GUIDE Privacy Requirements and Policies for Health Practitioners PUBLISHED BY THE COLLEGE OF DENTAL HYGIENISTS OF ONTARIO SEPTEMBER 2004 2 This booklet is
Getting Ready for Ontario s Privacy Legislation GUIDE Privacy Requirements and Policies for Health Practitioners PUBLISHED BY THE COLLEGE OF DENTAL HYGIENISTS OF ONTARIO SEPTEMBER 2004 2 This booklet is
FAMILY WELLBEING GUIDELINES F18
 FAMILY WELLBEING GUIDELINES F18 Table of Contents 1. About these guidelines... 3 Who are these guidelines for?... 3 What is the purpose of these guidelines?... 3 How should these guidelines be used?...
FAMILY WELLBEING GUIDELINES F18 Table of Contents 1. About these guidelines... 3 Who are these guidelines for?... 3 What is the purpose of these guidelines?... 3 How should these guidelines be used?...
Medical Assistance in Dying
 POLICY STATEMENT #4-16 Medical Assistance in Dying APPROVED BY COUNCIL: REVIEWED AND UPDATED: PUBLICATION DATE: KEY WORDS: RELATED TOPICS: LEGISLATIVE REFERENCES: REFERENCE MATERIALS: OTHER RESOURCES:
POLICY STATEMENT #4-16 Medical Assistance in Dying APPROVED BY COUNCIL: REVIEWED AND UPDATED: PUBLICATION DATE: KEY WORDS: RELATED TOPICS: LEGISLATIVE REFERENCES: REFERENCE MATERIALS: OTHER RESOURCES:
CONSENT POLICY Page 1 of 8 Reviewed: March 2017
 Page 1 of 8 Purpose To ensure all patients at Mercy Hospital are fully informed prior to their operation or procedure. Related Standard Standard 1.8 of the Code of Health & Disability Services Consumers
Page 1 of 8 Purpose To ensure all patients at Mercy Hospital are fully informed prior to their operation or procedure. Related Standard Standard 1.8 of the Code of Health & Disability Services Consumers
A View from a LHIN Breakfast with the Chiefs
 A View from a LHIN Breakfast with the Chiefs Matthew Anderson Chief Executive Officer October 22 nd, 2008 To change the world To change the world To change the world 6 Months of Learning The good news
A View from a LHIN Breakfast with the Chiefs Matthew Anderson Chief Executive Officer October 22 nd, 2008 To change the world To change the world To change the world 6 Months of Learning The good news
Consent to Treatment SEVEN AT A GLANCE SCENARIOS FIGURES NEED TO KNOW. 1. Consent for treatment is always required, except in an emergency.
 SEVEN Consent to Treatment AT A GLANCE Informed Consent to Treatment - 76 l Why Informed Consent is Not Always Obtained - 77 l Elements of Informed Consent - 77 Implied Consent to Treatment - 79 Withdrawal
SEVEN Consent to Treatment AT A GLANCE Informed Consent to Treatment - 76 l Why Informed Consent is Not Always Obtained - 77 l Elements of Informed Consent - 77 Implied Consent to Treatment - 79 Withdrawal
Adult Guardianship and Trusteeship Act: Legislative and Practice Changes
 Adult Guardianship and Trusteeship Act: Legislative and Practice Changes Mareika Purdon, Vice President, Patients as Partners Dr Ty Josdal, Associate Senior Physician Executive Helen Stokes, Executive
Adult Guardianship and Trusteeship Act: Legislative and Practice Changes Mareika Purdon, Vice President, Patients as Partners Dr Ty Josdal, Associate Senior Physician Executive Helen Stokes, Executive
FAMILY WELLBEING GUIDELINES
 FAMILY WELLBEING GUIDELINES 2016 Table of Contents Table of Contents... 1 1. About these guidelines... 2 Who are these guidelines for?... 2 What is the purpose of these guidelines?... 2 How should these
FAMILY WELLBEING GUIDELINES 2016 Table of Contents Table of Contents... 1 1. About these guidelines... 2 Who are these guidelines for?... 2 What is the purpose of these guidelines?... 2 How should these
ASSEMBLY HEALTH AND SENIOR SERVICES COMMITTEE STATEMENT TO. ASSEMBLY, No STATE OF NEW JERSEY DATED: JUNE 13, 2011
 ASSEMBLY HEALTH AND SENIOR SERVICES COMMITTEE STATEMENT TO ASSEMBLY, No. 4098 STATE OF NEW JERSEY DATED: JUNE 13, 2011 The Assembly Health and Senior Services Committee reports favorably Assembly Bill
ASSEMBLY HEALTH AND SENIOR SERVICES COMMITTEE STATEMENT TO ASSEMBLY, No. 4098 STATE OF NEW JERSEY DATED: JUNE 13, 2011 The Assembly Health and Senior Services Committee reports favorably Assembly Bill
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE ADVANCE CARE PLANNING AND GOALS OF CARE DESIGNATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Seniors Health PARENT DOCUMENT TITLE, TYPE AND NUMBER Not Applicable
TITLE ADVANCE CARE PLANNING AND GOALS OF CARE DESIGNATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Seniors Health PARENT DOCUMENT TITLE, TYPE AND NUMBER Not Applicable
Informed consent practice standard
 Informed consent practice standard 14 May 2018 1 Foreword Standards framework The Dental Council (the Council) is legally required to set standards of clinical competence, cultural competence and ethical
Informed consent practice standard 14 May 2018 1 Foreword Standards framework The Dental Council (the Council) is legally required to set standards of clinical competence, cultural competence and ethical
POLICY TITLE Consent for Health Care
 Page 1 of 6 POLICY TITLE 1. PURPOSE To protect the rights of individuals and promote their full participation in making informed decisions with respect to their health care and treatment options. To ensure
Page 1 of 6 POLICY TITLE 1. PURPOSE To protect the rights of individuals and promote their full participation in making informed decisions with respect to their health care and treatment options. To ensure
Mental Health Liaison Workshop
 Mental Health Liaison Workshop UEC Improvement Collaborative Event The Kia Oval, 07 December 2017 Neil Brimblecombe - Chair (co MH Clinical Lead UECC) Barbara Cleaver - Consultant in Emergency Medicine
Mental Health Liaison Workshop UEC Improvement Collaborative Event The Kia Oval, 07 December 2017 Neil Brimblecombe - Chair (co MH Clinical Lead UECC) Barbara Cleaver - Consultant in Emergency Medicine
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Advance Care Planning and Goals of Care
 Advance Care Planning and Goals of Care A Guide For Patients with A Serious Illness and Their Families Nova Scotia Edition www.nshpca.ca Receiving a diagnosis of a serious illness can be life altering.
Advance Care Planning and Goals of Care A Guide For Patients with A Serious Illness and Their Families Nova Scotia Edition www.nshpca.ca Receiving a diagnosis of a serious illness can be life altering.
POLICY TITLE Consent for Health Care
 Page 1 of 6 POLICY TITLE 1. PURPOSE To protect the rights of individuals and promote their full participation in making informed decisions with respect to their health care and treatment options. To ensure
Page 1 of 6 POLICY TITLE 1. PURPOSE To protect the rights of individuals and promote their full participation in making informed decisions with respect to their health care and treatment options. To ensure
Palliative Care Competencies for Occupational Therapists
 Principles of Palliative Care Demonstrates an understanding of the philosophy of palliative care Demonstrates an understanding that a palliative approach to care starts early in the trajectory of a progressive
Principles of Palliative Care Demonstrates an understanding of the philosophy of palliative care Demonstrates an understanding that a palliative approach to care starts early in the trajectory of a progressive
Discharge Planning for Patients Hospitalized for Mental Health Treatment Interpretative Guidelines for Oregon Hospitals
 Discharge Planning for Patients Hospitalized for Mental Health Treatment Interpretative Guidelines for Oregon Hospitals May 2016 1 PURPOSE This document is meant to offer interpretative guidance for Oregon
Discharge Planning for Patients Hospitalized for Mental Health Treatment Interpretative Guidelines for Oregon Hospitals May 2016 1 PURPOSE This document is meant to offer interpretative guidance for Oregon
Erie St. Clair Community Care Access Centre (CCAC) Planning for Long-Term Care When living at home is no longer possible
 Planning for Long-Term Care When living at home is no longer possible") Erie St. Clair Community Care Access Centre (CCAC) Planning for Long-Term Care When living at home is no longer possible www.healthcareathome.ca/eriestclair 310-2222 The Erie St. Clair CCAC Table of Contents
Erie St. Clair Community Care Access Centre (CCAC) Planning for Long-Term Care When living at home is no longer possible www.healthcareathome.ca/eriestclair 310-2222 The Erie St. Clair CCAC Table of Contents
Regional Hospice Palliative Care Model Action Plan
 ITEM 11.1 Regional Hospice Palliative Care Model Action Plan Central LHIN Board of Directors October 28, 2014 1 Agenda Background Declaration A Vision for Palliative Care in Ontario Central LHIN Approach
ITEM 11.1 Regional Hospice Palliative Care Model Action Plan Central LHIN Board of Directors October 28, 2014 1 Agenda Background Declaration A Vision for Palliative Care in Ontario Central LHIN Approach
Patient s Bill of Rights (Revised April 2012)
") Patient s Bill of Rights (Revised April 2012) TIRR Memorial Hermann recognizes the rights of human beings for independence of expression, decision, and action and will protect these rights of all patients,
Patient s Bill of Rights (Revised April 2012) TIRR Memorial Hermann recognizes the rights of human beings for independence of expression, decision, and action and will protect these rights of all patients,
The Newcastle upon Tyne Hospitals NHS Foundation Trust
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Advance Decision to Refuse Treatment Policy (Advanced Refusal of Treatment/ Previously known as Living Wills) Incorporating the Mental Capacity Act
The Newcastle upon Tyne Hospitals NHS Foundation Trust Advance Decision to Refuse Treatment Policy (Advanced Refusal of Treatment/ Previously known as Living Wills) Incorporating the Mental Capacity Act
MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard /10 Q3
 MLAA Performance Assessment Dashboard /10 Q3") MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard - 29/1 Q3 README The 29/1 MLAA Dashboard has been designed to reflect various reporting fiscal periods as well as the
MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard - 29/1 Q3 README The 29/1 MLAA Dashboard has been designed to reflect various reporting fiscal periods as well as the
Chapter 55: Protective Services and Placement
 Chapter 55: Protective Services and Placement Robert Theine Pledl, Attorney Schott, Bublitz & Engel, S.C. Introduction In addition to the procedures for voluntary treatment services and civil commitment
Chapter 55: Protective Services and Placement Robert Theine Pledl, Attorney Schott, Bublitz & Engel, S.C. Introduction In addition to the procedures for voluntary treatment services and civil commitment
STANDARDS AND GUIDELINES TITLE: INFORMED CONSENT STANDARD DOC #: 10 STATUS:
 STANDARDS AND GUIDELINES TITLE: INFORMED CONSENT STANDARD DOC #: 10 STATUS: Approved by Council CIRCULATION DATE: March June 2013 REVISED: June 2013 APPROVAL DATE: July 29, 2013 Note to Readers: In the
STANDARDS AND GUIDELINES TITLE: INFORMED CONSENT STANDARD DOC #: 10 STATUS: Approved by Council CIRCULATION DATE: March June 2013 REVISED: June 2013 APPROVAL DATE: July 29, 2013 Note to Readers: In the
AL0200 CONSENT - PERSONS UNDER 19 YEARS OF AGE. Table of Contents. Administrative Policy Manual Code: AL Legal/Ethical
 Table of Contents 1.0 PURPOSE... 2 2.0 DEFINITIONS... 2 3.0 POLICY... 2 3.1 Consent Requirement... 2 3.2 Exceptions from Obtaining Consent... 3 3.3 Form of Consent... 3 3.4 Age of Consent... 3 3.5 Ability
Table of Contents 1.0 PURPOSE... 2 2.0 DEFINITIONS... 2 3.0 POLICY... 2 3.1 Consent Requirement... 2 3.2 Exceptions from Obtaining Consent... 3 3.3 Form of Consent... 3 3.4 Age of Consent... 3 3.5 Ability
Legally Authorized Representatives in Clinical Trials
 Vol. 7, No. 3, March 2011 Can You Handle the Truth? Legally Authorized Representatives in Clinical Trials By Judy Katzen The sickest patients need the best medical care, which might involve participation
Vol. 7, No. 3, March 2011 Can You Handle the Truth? Legally Authorized Representatives in Clinical Trials By Judy Katzen The sickest patients need the best medical care, which might involve participation
Informed Consent for Treatment/Intervention VHA Clinical Governance in Community Health Discussion Paper March 2009
 Informed Consent for Treatment/Intervention VHA Clinical Governance in Community Health Discussion Paper March 2009 Aim The aim of this paper is to highlight the issues related to informed consent for
Informed Consent for Treatment/Intervention VHA Clinical Governance in Community Health Discussion Paper March 2009 Aim The aim of this paper is to highlight the issues related to informed consent for
Quality Improvement Plans (QIP): Progress Report for 2013/14 QIP
: Progress Report for 2013/14 QIP") Excellent Care for All Quality Improvement Plans (QIP): Report for 201/14 QIP The following template has been provided to assist with completion of reporting on the progress of your organization s QIP.
Excellent Care for All Quality Improvement Plans (QIP): Report for 201/14 QIP The following template has been provided to assist with completion of reporting on the progress of your organization s QIP.
TOOLKIT COORDINATED CARE PLANNING. London Middlesex Health Link
 TOOLKIT COORDINATED CARE PLANNING The toolkit is for any individual/organization who will be participating in the Health Link approach to coordinated care planning September 2016 London Middlesex Health
TOOLKIT COORDINATED CARE PLANNING The toolkit is for any individual/organization who will be participating in the Health Link approach to coordinated care planning September 2016 London Middlesex Health
Choice on Discharge Policy
 Choice on Discharge Policy Reference No: P_CIG_19 Version 1 Ratified by: LCHS Trust Board Date ratified: 13 th September 2016 Name of originator / author: Sarah McKown Name of responsible committee / Individual
Choice on Discharge Policy Reference No: P_CIG_19 Version 1 Ratified by: LCHS Trust Board Date ratified: 13 th September 2016 Name of originator / author: Sarah McKown Name of responsible committee / Individual
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
PROFESSIONAL STANDARDS FOR MIDWIVES
 Appendix A: Professional Standards for Midwives OVERVIEW The Professional Standards for Midwives (Professional Standards ) describes what is expected of all midwives registered with the ( College ). The
Appendix A: Professional Standards for Midwives OVERVIEW The Professional Standards for Midwives (Professional Standards ) describes what is expected of all midwives registered with the ( College ). The
Bayshore Health Care & Kingston Health Sciences Innovative ALC Transitional Care Program
 Innovation Partnership Procurement by Co-Design Bayshore Health Care & Kingston Health Sciences Innovative ALC Transitional Care Program Challenge Brief Contact name Response deadline Anita Fitches October
Innovation Partnership Procurement by Co-Design Bayshore Health Care & Kingston Health Sciences Innovative ALC Transitional Care Program Challenge Brief Contact name Response deadline Anita Fitches October
Guardianship Support Center
 Greater Wisconsin Agency on Aging Resources, Inc. Guardianship Support Center 1414 MacArthur Road, Suite 306; Madison, WI 53714 Hotline: (855) 409-9410 guardian@gwaar.org www.gwaar.org I. Introduction
Greater Wisconsin Agency on Aging Resources, Inc. Guardianship Support Center 1414 MacArthur Road, Suite 306; Madison, WI 53714 Hotline: (855) 409-9410 guardian@gwaar.org www.gwaar.org I. Introduction
COMMITTEE REPORTS TO THE BOARD
 Item # 9 F i COMMITTEE REPORTS TO THE BOARD To From South East LHIN Board Members Quality Committee Reviewed by Quality Committee Committee Members of the Committee were given the opportunity to review
Item # 9 F i COMMITTEE REPORTS TO THE BOARD To From South East LHIN Board Members Quality Committee Reviewed by Quality Committee Committee Members of the Committee were given the opportunity to review
P R O C E D U R E L E V E L 1
 P R O C E D U R E L E V E L 1 TITLE CONSENT TO TREATMENT / PROCEDURE(S) DOCUMENT # PRR-01-01 PARENT DOCUMENT LEVEL LEVEL 1 PARENT DOCUMENT TITLE Consent to Treatment/ Procedure(s) APPROVAL LEVEL Alberta
P R O C E D U R E L E V E L 1 TITLE CONSENT TO TREATMENT / PROCEDURE(S) DOCUMENT # PRR-01-01 PARENT DOCUMENT LEVEL LEVEL 1 PARENT DOCUMENT TITLE Consent to Treatment/ Procedure(s) APPROVAL LEVEL Alberta
Coordinated Care Planning
 Coordinated Care Planning What is a Coordinated Care Plan? A plan for your care that is created with you and your family (as per your direction) and involves all the members of your health care team. What
Coordinated Care Planning What is a Coordinated Care Plan? A plan for your care that is created with you and your family (as per your direction) and involves all the members of your health care team. What
PATIENT RIGHTS, PRIVACY, AND PROTECTION
 REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
Bond University Medical Program. Oncology Rotation Clinician Guide
 Bond University Medical Program Oncology Rotation Clinician Guide YEAR 5 2018 Introduction Students in the final year of the Bond University Medical Program have 6 rotations to train in a broad array of
Bond University Medical Program Oncology Rotation Clinician Guide YEAR 5 2018 Introduction Students in the final year of the Bond University Medical Program have 6 rotations to train in a broad array of
Alberta First Nations Continuing Care Needs Assessment - Health and Home Care Program Staff Survey -
 Alberta First Nations Continuing Care Needs Assessment p. 1 Alberta First Nations Continuing Care Needs Assessment - Health and Home Care Program Staff Survey - Definition of Terms Continuing Care: As
Alberta First Nations Continuing Care Needs Assessment p. 1 Alberta First Nations Continuing Care Needs Assessment - Health and Home Care Program Staff Survey - Definition of Terms Continuing Care: As
Activity Based Cost Accounting and Payment Bundling
 Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
CASLPO Forum. Sudbury Sept 19 th 2017
 CASLPO Forum Sudbury Sept 19 th 2017 1 Carol Bock Deputy Registrar Alexandra Carling Director of Professional Practice and Quality Assurance David Beattie Conseiller orthophonie 2 https://caslpo.adobeconnect.com/caslpoforum/
CASLPO Forum Sudbury Sept 19 th 2017 1 Carol Bock Deputy Registrar Alexandra Carling Director of Professional Practice and Quality Assurance David Beattie Conseiller orthophonie 2 https://caslpo.adobeconnect.com/caslpoforum/
Waterloo Wellington Community Care Access Centre. Community Needs Assessment
 Waterloo Wellington Community Care Access Centre Community Needs Assessment Table of Contents 1. Geography & Demographics 2. Socio-Economic Status & Population Health Community Needs Assessment 3. Community
Waterloo Wellington Community Care Access Centre Community Needs Assessment Table of Contents 1. Geography & Demographics 2. Socio-Economic Status & Population Health Community Needs Assessment 3. Community
Medical Assistance in Dying (Practitioner Administered) Practice Guideline for Pharmacists and Pharmacy Technicians
 Practice Guideline for Pharmacists and Pharmacy Technicians") Medical Assistance in Dying (Practitioner Administered) Practice Guideline for Pharmacists and Pharmacy Technicians 1 BACKGROUND Historically, medical assistance in dying (MAID) has been prohibited in
Medical Assistance in Dying (Practitioner Administered) Practice Guideline for Pharmacists and Pharmacy Technicians 1 BACKGROUND Historically, medical assistance in dying (MAID) has been prohibited in
Expected Death in the Home Protocol EDITH. Guidelines for Implementation
 EDITH Guidelines for Implementation Hospice Palliative Care Teams for Champlain Champlain Community Care Access Centre Centre d accès aux soins communautaires de Champlain Table of Contents 1. Overview...
EDITH Guidelines for Implementation Hospice Palliative Care Teams for Champlain Champlain Community Care Access Centre Centre d accès aux soins communautaires de Champlain Table of Contents 1. Overview...
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS
 ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
ASSESSMENT PROCESS FOR NHS CONTINUING HEALTH CARE OPERATIONAL GUIDANCE FOR PRACTITIONERS
 ASSESSMENT PROCESS FOR NHS CONTINUING HEALTH CARE OPERATIONAL GUIDANCE FOR PRACTITIONERS September 2014 CONTENTS 1. Introduction 2. The National framework for Continuing Healthcare November 2012 (Revised)
ASSESSMENT PROCESS FOR NHS CONTINUING HEALTH CARE OPERATIONAL GUIDANCE FOR PRACTITIONERS September 2014 CONTENTS 1. Introduction 2. The National framework for Continuing Healthcare November 2012 (Revised)
The Special-care Homes Rates Regulations, 2011
 SPECIAL-CARE HOMES RATES, 2011 R-8.2 REG 8 1 The Special-care Homes Rates Regulations, 2011 being Chapter R-8.2 Reg 8 (effective October 1, 2011) as amended by Saskatchewan Regulations 85/2012, 38/2013,
SPECIAL-CARE HOMES RATES, 2011 R-8.2 REG 8 1 The Special-care Homes Rates Regulations, 2011 being Chapter R-8.2 Reg 8 (effective October 1, 2011) as amended by Saskatchewan Regulations 85/2012, 38/2013,
Bond University Medical Program. Haematology Rotation Clinician Guide
 Bond University Medical Program Haematology Rotation Clinician Guide YEAR 5 2018 Introduction Students in the final year of the Bond University Medical Program have 6 rotations to train in a broad array
Bond University Medical Program Haematology Rotation Clinician Guide YEAR 5 2018 Introduction Students in the final year of the Bond University Medical Program have 6 rotations to train in a broad array
AH3600 Repatriation Policy
 1.0 PURPOSE AH3600 Repatriation Policy This policy outlines the standard operating procedure and performance expectations for Patient Repatriation activities originating at Interior Health (IH) acute care
1.0 PURPOSE AH3600 Repatriation Policy This policy outlines the standard operating procedure and performance expectations for Patient Repatriation activities originating at Interior Health (IH) acute care
A checklist to meet ethical and legal obligations to critically ill patients at end of life
 A checklist to meet ethical and legal obligations to critically ill patients at end of life Robert W Sibbald 1,2, Paula Chidwick 3, Mark Handelman, Andrew B Cooper 3,4 1 Department of Family Medicine,
A checklist to meet ethical and legal obligations to critically ill patients at end of life Robert W Sibbald 1,2, Paula Chidwick 3, Mark Handelman, Andrew B Cooper 3,4 1 Department of Family Medicine,
Advance Directives. Advance Care Planning & Required Forms. Person Appointing Patient Advocate: Print name Date of Birth Date signed Phone contact(s)
") Person Appointing Patient Advocate: Print name Date of Birth Date signed Phone contact(s) Advance Directives Advance Care Planning & Required Forms Keep this document for your records and make copies for
Person Appointing Patient Advocate: Print name Date of Birth Date signed Phone contact(s) Advance Directives Advance Care Planning & Required Forms Keep this document for your records and make copies for
Change Management at Orbost Regional Health
 Change Management at Orbost Regional Health Our change management journey 1 Medication Change System Meds at Beds 2 The slightly exaggerated before process 3 Project Goals The purpose of the Meds at Beds
Change Management at Orbost Regional Health Our change management journey 1 Medication Change System Meds at Beds 2 The slightly exaggerated before process 3 Project Goals The purpose of the Meds at Beds
Discharge and Follow-Up Planning. Presented by the Clinical and Quality Team
 Discharge and Follow-Up Planning Presented by the Clinical and Quality Team After today s training you will be able to: Identify and summarize important information about discharge planning Have adequate
Discharge and Follow-Up Planning Presented by the Clinical and Quality Team After today s training you will be able to: Identify and summarize important information about discharge planning Have adequate