Usfbunfou!pg!! Xbs!Dbtvbmujft
|
|
|
- Bennett Marsh
- 5 years ago
- Views:
Transcription
1
2 Usfbunfou!pg!! Xbs!Dbtvbmujft B! D P QB S J T P O! C F U X F FO! W J F U O B! B OE! U IF! Q S F T FO U C h a r l e s J M i d d l e t o n, m d, fa c s Author s ote: The purpose of this brief article is to compare treatment of war casualties in Vietnam, circa 1971, with the treatment being administered today in Iraq and Afghanistan. I will present some statistics, describe changes in care units, evacuation of the wounded, equipment and training of personnel. I will also describe differences in injuries based on weaponry.!j am a board-certified general surgeon and have been in practice since I had the privilege of serving in the US Army in Vietnam in 1971 after completing a five-year surgical residency at Hartford Hospital in Hartford, Connecticut, in During my residency, I saw a moderate amount of blunt trauma, low-velocity gunshot wounds, stab wounds and burns. However, my excellent training did not prepare me for high-velocity gunshot wounds and mine injuries. And I would say that probably pertained to all of the younger general surgeons, including those who were trained at inner-city hospitals, where the number of trauma cases was higher. We learned our lessons largely from those who were there before us on-the-job training, so to speak. L E A R I G O B J E C T I V E S Compare the treatment provided in Vietnam and Iraq. Evaluate how the Forward Surgical Team has contributed to survival rates. Compare the wounds experienced in Vietnam and Iraq. Explain the mechanisms of injury of a landmine vs roadside bomb. Assess the effectiveness of tourniquets. AUGUST 2008 The Surgical Technologist 349


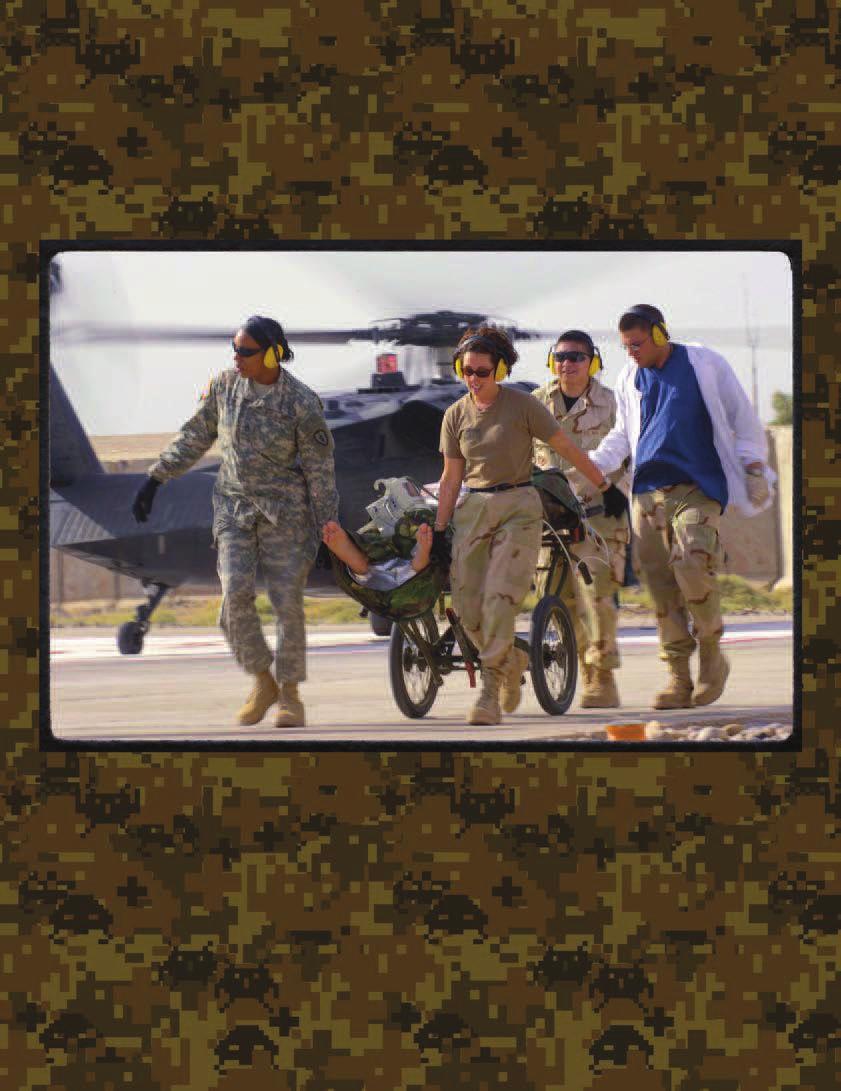
3 296 AUGUST CE CREDIT We cared for GIs, Vietnamese civilians, Korean and Thai allies, orth Vietnamese and even a Polish sailor who was injured on a ship off the coast. My first patient was Viet Cong. Our patients arrived by ambulance, truck and out of the field by helicopter. The injured GI was usually seen first by a medic at a battalion aid station. Heroic DUSTOFF * at i ona l Arch i ve at iona l Arch ive helicopter crews flew to the aid stations and sometimes to crude landing zones in the middle of fire fights to deliver the wounded to the 24th Evacuation Hospital in Long Binh, where we had the expertise and equipment to perform every surgery but cardiac. Those patients, if they survived long enough, were brought to the 3rd Field Hospital in Saigon. I began my tour of duty in Vietnam with a two-week orientation phase, where I worked alongside general surgeons who had been incountry for a longer period of time and with orthopedic surgeons who taught me Whole blood is administered to an the critical lessons of adequate debridement of airborne casualty, extremity wounds, including frequent returns to enclosed in a metal the operating room for additional debridement capsule attached and irrigation, and keeping wounds open until it to the side of an Air Rescue helicopter was safe to close them. about to land at an The general surgeons also acted as the Surgiadvanced air station cal Offcer of the Day (SOD) and were in charge in Korea. A medical of triage, ordering laboratory studies and X-rays technician holds a (we had no ultrasound, CT scan or MRI), calllife-giving bottle ing of appropriate teams and determining the over the wounded order of cases for surgery, but not performing man during the surgery themselves, while acting as SOD. Triage 4-minute flight from the front lines. is the determination among the injured of those 12/31/192 requiring immediate surgery, those whose surgery can be delayed, those requiring minimal surgical care and those in expectant status, who are not likely to live even with surgery. Survival rate statistics from war to war and generation to generation are illuminating. In World War II, the survival rate of GIs reaching hospitals was 69.7 percent. In Korea, that number improved to 7.4 percent. Vietnam saw another small increase with a 76.4 percent survival rate. Today, 90. percent of GIs reaching a field hospital survive the ordeal. 1 During the Vietnam War, the average length of time from initial treatment to transfer to the continental United States (COUS) was 4 days. This would involve initial surgery at a surgical or evacuation hospital, followed by a transfer to Yakota Air Force Base in Japan, or Clark Air Force Base in the Philippines, for possible additional surgery and transfer back to the United States. In Iraq, a wounded soldier is quickly stabilized, including damage-control surgery when necessary. The time from initial treatment in the field until the time of arrival in Landstuhl, Germany, a Level II trauma facility, might be 12 hours. More surgery could be completed in Germany before the patient is flown to COUS, all within three days of the time of initial treatment. Combat units in the field in Vietnam were manned by medics who basically delivered first aid. In today s combat units in Iraq and Afghanistan, Marine and Army infantrymen are all trained in advanced first aid and are taught the ABCs of resuscitation. Every soldier carries two single-handed tourniquet devices they can use on a buddy or on themselves. Since percent of wounds are musculoskeletal, and the major cause of death is still exsanguination, surgeons say the tourniquets are the single greatest life-saving advancement to emerge from the Iraq conflict. They are now being used in ambulances in the United States. 2 Special forces combat medics have more than one year of training and are certified EMTs. In addition, they undergo an extra six months of training, when they learn to resuscitate, place chest tubes, stabilize fractures and perform some amputations and basic surgery. At battalion aid stations, there are physician assistants (PAs) who are also trained in resuscitation and stabilization and are qualified in Advanced Trauma Life * DUSTOFF stands for Devoted Unswerving Service To Our Fighting Forces. 30 The Surgical Technologist AUGUST 2008

4 Support (ATLS). Along with partially-trained surgeons, they start IVs, place chest tubes, stabilize fractures and prepare patients for transfer for additional treatment. 3 Generally, the distance traveled for care after initial treatment at an aid station was not far in Vietnam. Surgical and evacuation hospitals were well-established, permanent facilities with relatively large numbers of surgical and medical specialists, nurses, beds and ancillary personnel, such as lab and X-ray technicians. We had a radiologist and a pathologist as well. In Iraq, because of the long distances traveled for care in a large country, the concept of the Forward Surgical Team was developed after the first Gulf War. This is a mobile unit usually comprised of one surgeon, a nurse anesthetist and a medic. Intravenous treatment begins with procoagulants and whole blood, type O, followed by fresh whole blood with thawed plasma instead of crystalloids. High doses of Factor VII are also used to stop bleeding. Surgeons are using temporary intravascular shunts rather than attempting vascular repair at this point. These have not been found to adversely affect subsequent definitive repair. Patients are then transported to one of two combat surgical hospitals (CSH), where there are two operating rooms, an ICU, and various surgical specialists and a larger staff of nurses and enlisted, noncommissioned offcers (COs). After reevaluation and possible surgery, the patient is prepared for transfer to Landstuhl by Critical Care Aeromedical Transport Teams (CCATT) developed by the Air Force. Continuous intensive care can be given enroute without a 24-hour delay to assure stability. In Vietnam, I accompanied soldiers to Japan and Thailand in C-141s that contained ICUs, but all patients were stable at the time of transfer and no intense active care was given. At Landstuhl, the surgical teams are primarily military. They are also comprised of visiting senior surgeons from the United States, who are invited via a senior visiting surgeon program sponsored by the military. The visiting surgeons add their expertise to surgical care and take back the knowledge they have absorbed in order to enrich the teaching programs at their institutions. 2 In Vietnam, telecommunication technology was relatively primitive. It usually took weeks for families to learn the whereabouts of their loved ones in a war zone. ow, contact is made from Landstuhl to hospitals like Walter Reed, Brooke and Bethesda aval, which will be receiving the injured for further definitive and reconstructive surgery, and reuniting them with their families within hours. Communications can also take place between Landstuhl and forward surgical teams on the ground in Iraq, which allows the hospital an extra window of time to prepare for the arrival of incoming casualties. Most combat casualties in Vietnam were caused by the high-velocity AK-47 assault rifle, artillery or land mines. The AK-47 is still the small-arms weapon of choice for the adversary in Iraq and Afghanistan, but.0 caliber rifles and mortars are also used. Fighting in Iraq has seen changes in style and the degree of devastation, compared to Vietnam. The primary cause of injury in Iraq is the 1mm howitzer shell, which can be hidden under asphalt and detonated from a distance, often with a cell phone. Added shrapnel in the form of nails, screws and nuts covered with feces adds to the lethality of this terrible weapon. Other improvised explosive devices (IEDs) are vehicle-borne and may be accompanied by tanks of propane or other inflammable material adding to the burn effect. Daniel Love/US Army A special forces team medic assigned to the Combined Joint Special Operations Task Force- Afghanistan treats another US Army soldier for shrapnel wounds from a rocket-propelled grenade explosion while battling Taliban fighters in the Sangin District area of Helmand Province, Afghanistan, April 10, AUGUST 2008 The Surgical Technologist 31
 and the 122mm rockets are also used.")
5 Medical evacuation patients on the deck of the amphibious assault ship USS Tripoli (LPH-10) await transfer to the 22nd Casualty Station in Danang, from which they will be sent to COUS. July 1967 Rocket-propelled grenades (RPGs) and the 122mm rockets are also used. 1 Since injuries to the head and chest are often fatal, improved helmets and body armor have helped reduce deaths from these injuries. With the preponderance of wounds to the extremities, as in Vietnam, aggressive and repeated debridement and irrigation are of paramount importance to prevent death from overwhelming infection and to preserve limbs. at i ona l Arch i ve Since the primary cause of injury to coalition forces in Iraq is the roadside bomb, it is worthwhile to describe its mechanisms of injury. The injuries are significantly different from those administered by land mines in Vietnam. The explosion is caused by rapid chemical conversion of a solid or liquid to a gas, accompanied by an enormous release of energy. High-order explosives detonate quickly, generating heat, noise and high-pressure gasses in 1/1,000th of a second, forming a supersonic overpressure shock wave. This blast wave moves in all directions and can exert up to 700 tons of pressure. It creates high-velocity fragmentation of its contents and its container, a blast wind that can reach hurricane strength, structural collapse, burns and toxic inhalants. Secondary-blast pressure effects are caused by reflection off other surfaces, which magnifies the effect particularly in enclosed spaces, where structural collapse increases mortality. Primary blast injuries are the result of overpressurization, which causes damage mainly to gas-filled structures, such as eardrums, lungs and intestines. Secondary blast injuries result from fragmentation, producing both penetrating and blunt-force injuries. Tertiary blast effects result from bodies being thrown by a blast wind, flying through the air or tumbling and striking other objects with additional penetrating or bluntforce injuries. Quaternary blast injuries might include burns or inhalation injury due to temperatures from the explosion reaching as high as 3,000 degrees centigrade. Sutphen has given an excellent description of types of injuries and their evaluation and treatment and gives credit to the Israelis and others for what we have learned. 4 In summary, this article has been written to describe changes that have improved the surgical care of those injured in war since Vietnam. The basic principles remain the same, but changes in training, hospital logistics, equipment and evacuation have resulted in significantly better survival rates. What has not changed since Vietnam is the intensity, courage and dedication of doctors, nurses and surgical technologists who have served in active war zones, sometimes under fire themselves, as they perform their duties. It was an honor for me to have worked alongside them in Vietnam and it provided experiences and memories that I will never forget. A B O U T T H E A U T H O R Charles J Middleton received his BA from Trinity College and his MD from Downstate Medical Center at the State University of ew York in Brooklyn, Y. He previously served as chief of surgery at Berrien County Hospital in ashville, Georgia, from September 2002-September He is currently a general surgeon at the Tarboro Clinic in Tarboro, orth Carolina. References 1. Hyer. Extremity War Injuries: State of the Art and Future Directions. http//:w ww.medscape.com/viewar ticle / Accessed February 1, Frangou C. Controversies in Surgery. surgerynews.com 3. Barclay L. Combat Medicine in Iraq, Part I. medscape.com/viewar ticle/ Accessed February 1, Sutphen SF. Blast Injuries: A Review. com/viewprogram/4714. Accessed February 1, The Surgical Technologist AUGUST 2008

 commissioned a study to improve tourniquet use doctrine and training to maximize the potential life-saving benefits of tourniquet use,")
6 Military technology with civilian application: Most effective tourniquets available today Uncontrollable hemorrhage accounts for almost 0 percent of combat fatalities and up to 80 percent of civilian trauma fatalities in the United 1 States. One of the best methods of combating exsanguination in critical circumstances is the use of a tourniquet. According to some studies, it has been estimated that seven out of 100 battlefield deaths could have been prevented with a properly-applied tourniquet. 2,3 In 200, the US Army Institute of Surgical Research (USAISR) commissioned a study to improve tourniquet use doctrine and training to maximize the potential life-saving benefits of tourniquet use, especially during active combat; and identify an effective, commercially available, simple-to-use, field-compatible 4 tourniquet for issue to all soldiers. Based on an informal internet search for trauma tourniquets, as well as reports from military medical personnel involved in the Iraq conflict regarding functional parameters, USAISR selected seven models for its evaluation. The evaluation process consisted of two experiments. In Experiment I, each model was tested for efficacy (elimination of distal Doppler sound) in volunteer human subjects legs. Those found to be effective in 80 percent or more subjects were then subjected to Experiment II, which tested effectiveness in the sub- jects arms. In both experiments, the subjects were required to apply the device to themselves without any external assistance. The results of the study yielded positive options for both military and civilian application. Of the seven models tested, only three were 100 percent effective in occluding distal arterial Doppler sound in both the arm and leg when self-applied by the volunteer human subjects: the Emergency & Military Tourniquet (EMT), Combat Application Tourniquet (CAT) and Special Operations Force Tactical Tourniquet (SOFTT). Reasons for failure among the other models included mechanical limitations (design or construction), circumferential pain and/or skin-pinching pain. The mechanical augmentation of both the CAT and SOFTT is the windlass, essentially a tension strap that is twisted to compress the wound. The EMT employs a pneumatic system, similar to that of a blood-pressure cuff. For military purposes, the CAT and the SOFTT are advantageous for their lighter weight and affordability, an edge that offers a practical application in the field. In the civilian quarter, however, the EMT is the clear winner. According to the Army s tests, the EMT resulted in significantly less circumferential pain than the other effect ve tourniquets. i An additional advantage to the EMT is its design. While heavier (21g to the CAT s 9g), it boasts a strap width that is nearly twice that of either the CAT or the SOFTT. Studies have shown that a wider tourniquet allows for occlu of blood flow at lower pressure, thus help sion ing to minimize the potential for damage to the underlying tissues. These distinct advantages present the EMT as an excellent option for application in the civilian trauma field in the United States. References 1. Moore Sauaia A; Moore EE et al. Epidemiology of Trauma Deaths: A Reassessment. J Trauma Mabry RL; Holcomb JB; Baker AM; et al. United States Army Rangers in Somalia: An Analysis of Combat Casualties on an Urban Battlefield. J Trauma Bellamy RF; Hagmann JH; Richards DT. Tactical Management of Urban Warfare Casualties in Special Operations. Mil Med Baer David G; Holcomb John B; Kauvar David S; Walters Thomas J. Battlefield Tourniquets: Modern Combat Lifesavers. US Army Med Dept J. April-June WaltersThomas J. Laboratory Evaluation of Battlefield Tourniquets in Human Volunteers. US Army Med Dept J. April-June ticles. com/p/articles/mi_m0vvy/is_200_april-june/ ai_n Accessed June 26, Special Operations Force Tactical Tourniquet (SOFTT). Tact i ca l Med i ca l So l ut i ons LLC Emergency & Military Tourniquet (EMT) De lfi Med i ca l I nnovat i ons, I nc. AUGUST 2008 The Surgical Technologist 33
Update on War Zone Injuries Stan Breuer, OTD, OTR/L, CHT Colonel, United States Army
 Update on War Zone Injuries Stan Breuer, OTD, OTR/L, CHT Colonel, United States Army Disclaimer: The opinions or assertions contained herein are the private view of the author and are not to be construed
Update on War Zone Injuries Stan Breuer, OTD, OTR/L, CHT Colonel, United States Army Disclaimer: The opinions or assertions contained herein are the private view of the author and are not to be construed
TCCC for All Combatants 1708 Introduction to TCCC Instructor Guide 1
 TCCC for All Combatants 1708 Introduction to TCCC Instructor Guide 1 1. Tactical Combat Casualty Care for All Combatants August 2017 Introduction to TCCC Tactical Combat Casualty Care is the standard of
TCCC for All Combatants 1708 Introduction to TCCC Instructor Guide 1 1. Tactical Combat Casualty Care for All Combatants August 2017 Introduction to TCCC Tactical Combat Casualty Care is the standard of
Tactical Combat Casualty Care for All Combatants August (Based on TCCC-MP Guidelines ) Introduction to TCCC
 Introduction to TCCC") Tactical Combat Casualty Care for All Combatants August 2017 (Based on TCCC-MP Guidelines 170131) Introduction to TCCC Pretest Pre-Test TCCC Web Link to Video What is TCCC and Why Do I Need to Learn About
Tactical Combat Casualty Care for All Combatants August 2017 (Based on TCCC-MP Guidelines 170131) Introduction to TCCC Pretest Pre-Test TCCC Web Link to Video What is TCCC and Why Do I Need to Learn About
1/7/2014. Dispatch for fire at Rosslyn, VA metro station Initial dispatch as Box Alarm
 1 Dispatch for fire at Rosslyn, VA metro station Initial dispatch as Box Alarm 4 engines, 2 trucks, 1 rescue, 1 medic unit, 2 battalion chiefs, 1 EMS supervisor, 1 battalion aide First arriving units report
1 Dispatch for fire at Rosslyn, VA metro station Initial dispatch as Box Alarm 4 engines, 2 trucks, 1 rescue, 1 medic unit, 2 battalion chiefs, 1 EMS supervisor, 1 battalion aide First arriving units report
U.S. ARMY MEDICAL SUPPORT
 U.S. ARMY MEDICAL SUPPORT BY SGT FREDERICK, EVELYN CIVIL AFFAIRS TEAM 8041 MEDIC AGENDA HOSPITAL LEVELS OF CARE TRAINING FOR ALL SOLDIERS: SELF AID, Tactical Combat Casualty Care (TCCC) MEDICS: REGULAR,
U.S. ARMY MEDICAL SUPPORT BY SGT FREDERICK, EVELYN CIVIL AFFAIRS TEAM 8041 MEDIC AGENDA HOSPITAL LEVELS OF CARE TRAINING FOR ALL SOLDIERS: SELF AID, Tactical Combat Casualty Care (TCCC) MEDICS: REGULAR,
High Threat Mass Casualty 1/7/2014. Game changer..
 Changing the Paradigm: Guidelines for High Risk Scenarios E. Reed Smith, MD, FACEP Committee for Tactical Emergency Casualty Care 1 Game changer.. 2 High Threat Mass Casualty What is the traditional teaching
Changing the Paradigm: Guidelines for High Risk Scenarios E. Reed Smith, MD, FACEP Committee for Tactical Emergency Casualty Care 1 Game changer.. 2 High Threat Mass Casualty What is the traditional teaching
The 2013 Boston Marathon Bombings
 The 2013 Boston Marathon Bombings Lessons Learned from a Resource-Rich Urban Battlefield Presented at the 41 st Convention of the American Society of Plastic Surgical Nurses Boston, Massachusetts October
The 2013 Boston Marathon Bombings Lessons Learned from a Resource-Rich Urban Battlefield Presented at the 41 st Convention of the American Society of Plastic Surgical Nurses Boston, Massachusetts October
Wounding Patterns for U.S. Marines and Sailors during Operation Iraqi Freedom, Major Combat Phase
 MILITARY MEDICINE, 171, 3:246, 2006 Wounding Patterns for U.S. Marines and Sailors during Operation Iraqi Freedom, Major Combat Phase Guarantor: James M. Zouris, BS Contributors: James M. Zouris, BS*;
MILITARY MEDICINE, 171, 3:246, 2006 Wounding Patterns for U.S. Marines and Sailors during Operation Iraqi Freedom, Major Combat Phase Guarantor: James M. Zouris, BS Contributors: James M. Zouris, BS*;
Roles of Medical Care (United States)
") Roles of Medical Care (United States) Chapter 2 Roles of Medical Care (United States) Introduction Military doctrine supports an integrated health services support system to triage, treat, evacuate, and
Roles of Medical Care (United States) Chapter 2 Roles of Medical Care (United States) Introduction Military doctrine supports an integrated health services support system to triage, treat, evacuate, and
Deployment Medicine Operators Course (DMOC)
") Deployment Medicine Operators Course (DMOC) The need has never been more critical to equip those who will first contact the battlefield casualty with lifesaving knowledge to improve survivability. Course
Deployment Medicine Operators Course (DMOC) The need has never been more critical to equip those who will first contact the battlefield casualty with lifesaving knowledge to improve survivability. Course
AAST Senior Visiting Surgeon Program
 AAST Senior Visiting Surgeon Program Landstuhl Medical Center Mary C. McCarthy, MD Professor of Surgery Wright State University School of Medicine 2007 McCarthy Objectives After participating in this activity,
AAST Senior Visiting Surgeon Program Landstuhl Medical Center Mary C. McCarthy, MD Professor of Surgery Wright State University School of Medicine 2007 McCarthy Objectives After participating in this activity,
INSTRUCTOR GUIDE FOR INTRODUCTION TO TCCC-MP
 INSTRUCTOR GUIDE FOR INTRODUCTION TO TCCC-MP 160603 1 1. Introduction to Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Combat Casualty Care is the new standard of care in prehospital
INSTRUCTOR GUIDE FOR INTRODUCTION TO TCCC-MP 160603 1 1. Introduction to Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Combat Casualty Care is the new standard of care in prehospital
of Trauma Assembly 28 th Page 1
 Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 11 Preparing for the Next War: Pivotal Military Civilian Relationships January 16, 2015 Disney s Contemporary
Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 11 Preparing for the Next War: Pivotal Military Civilian Relationships January 16, 2015 Disney s Contemporary
Bringing Combat Medicine to the Streets of EMS. MAJ Will Smith MD, EMT-P US Army
 Bringing Combat Medicine to the Streets of EMS MAJ Will Smith MD, EMT-P US Army Disclaimers No financial or other conflicts to disclose This presentation is NOT an official position or endorsement from
Bringing Combat Medicine to the Streets of EMS MAJ Will Smith MD, EMT-P US Army Disclaimers No financial or other conflicts to disclose This presentation is NOT an official position or endorsement from
of Trauma Assembly 28 th Page 1
 Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 11 Preparing for the Next War: Pivotal Military Civilian Relationships January 16, 215 Disney s Contemporary
Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 11 Preparing for the Next War: Pivotal Military Civilian Relationships January 16, 215 Disney s Contemporary
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC CONDUCT TRIAGE
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC 28542-0042 FMSO 107 CONDUCT TRIAGE TERMINAL LEARNING OBJECTIVE (1) Given multiple simulated casualties in a simulated operational
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC 28542-0042 FMSO 107 CONDUCT TRIAGE TERMINAL LEARNING OBJECTIVE (1) Given multiple simulated casualties in a simulated operational
UPMC Trauma Care System
 A Western PA Initiative 1 UPMC Trauma Care System Altoona (Level II Adult) Children s Hospital (Level I Pediatric) Hamot (Level II Adult) 2 Mercy (Level I Adult, Burn Center) Presbyterian (Level I Adult)
A Western PA Initiative 1 UPMC Trauma Care System Altoona (Level II Adult) Children s Hospital (Level I Pediatric) Hamot (Level II Adult) 2 Mercy (Level I Adult, Burn Center) Presbyterian (Level I Adult)
Tactical & Hunter First Aid Workshop
 Jackson Hole Gun Club Jackson, WY July 15, 2013 Tactical & Hunter First Aid Workshop LTC Will Smith MD, Paramedic www.wildernessdoc.com Disclaimers No financial conflicts to disclose Board of Advisors
Jackson Hole Gun Club Jackson, WY July 15, 2013 Tactical & Hunter First Aid Workshop LTC Will Smith MD, Paramedic www.wildernessdoc.com Disclaimers No financial conflicts to disclose Board of Advisors
A New Approach to Organization and Implementation of Military Medical Treatment in Response to Military Reform and Modern Warfare in the Chinese Army
 MILITARY MEDICINE, 182, 11/12:e1819, 2017 A New Approach to Organization and Implementation of Military Medical Treatment in Response to Military Reform and Modern Warfare in the Chinese Army Yang Pei,
MILITARY MEDICINE, 182, 11/12:e1819, 2017 A New Approach to Organization and Implementation of Military Medical Treatment in Response to Military Reform and Modern Warfare in the Chinese Army Yang Pei,
Active Violence and Mass Casualty Terrorist Incidents
 Position Statement Active Violence and Mass Casualty Terrorist Incidents The threat of terrorism, specifically active shooter and complex coordinated attacks, is a concern for the fire and emergency service.
Position Statement Active Violence and Mass Casualty Terrorist Incidents The threat of terrorism, specifically active shooter and complex coordinated attacks, is a concern for the fire and emergency service.
JOINT COMMITTEE TO CREATE A NATIONAL POLICY TO ENHANCE SURVIVABILITY FROM MASS CASUALTY SHOOTING EVENTS HARTFORD CONSENSUS II
 July 11, 2013 JOINT COMMITTEE TO CREATE A NATIONAL POLICY TO ENHANCE SURVIVABILITY FROM MASS CASUALTY SHOOTING EVENTS HARTFORD CONSENSUS II Concept to Action On April 2, 2013, representatives from a select
July 11, 2013 JOINT COMMITTEE TO CREATE A NATIONAL POLICY TO ENHANCE SURVIVABILITY FROM MASS CASUALTY SHOOTING EVENTS HARTFORD CONSENSUS II Concept to Action On April 2, 2013, representatives from a select
The U.S. Navy s Forward Resuscitative Surgery System during Operation Iraqi Freedom
 MILITARY MEDICINE, 170, 4:297, 2005 The U.S. Navy s Forward Resuscitative Surgery System during Operation Iraqi Freedom Guarantor: CAPT Rom A. Stevens, MC USNR Contributors: CAPT Harold R. Bohman, MC USN*;
MILITARY MEDICINE, 170, 4:297, 2005 The U.S. Navy s Forward Resuscitative Surgery System during Operation Iraqi Freedom Guarantor: CAPT Rom A. Stevens, MC USNR Contributors: CAPT Harold R. Bohman, MC USN*;
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 401 Introduction to Tactical Combat Casualty Care TERMINAL LEARNING OBJECTIVE 1. Given a casualty in a tactical
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 401 Introduction to Tactical Combat Casualty Care TERMINAL LEARNING OBJECTIVE 1. Given a casualty in a tactical
INTRODUCTION. Section I. SUPPORTING THE BATTLE
 CHAPTER 1 INTRODUCTION Section I. SUPPORTING THE BATTLE 1-1. General a. Warfare has changed significantly since World War II (WW II). The range, accuracy, and lethality of the modern tank gun makes it
CHAPTER 1 INTRODUCTION Section I. SUPPORTING THE BATTLE 1-1. General a. Warfare has changed significantly since World War II (WW II). The range, accuracy, and lethality of the modern tank gun makes it
EMS Subspecialty Certification Review Course. Learning Objectives. Scope of Practice
 EMS Subspecialty Certification Review Course 2.3.1 Scope of Practice Models 2.3.1.1 Military/federal government medical personnel 2.3.1.2 State vs. national scope of practice model 2.3.1.2.1 Levels of
EMS Subspecialty Certification Review Course 2.3.1 Scope of Practice Models 2.3.1.1 Military/federal government medical personnel 2.3.1.2 State vs. national scope of practice model 2.3.1.2.1 Levels of
Chapter I SUBMUNITION UNEXPLODED ORDNANCE (UXO) HAZARDS
 HAZARDS") Chapter I SUBMUNITION UNEXPLODED ORDNANCE (UXO) HAZARDS 1. Background a. Saturation of unexploded submunitions has become a characteristic of the modern battlefield. The potential for fratricide from UXO
Chapter I SUBMUNITION UNEXPLODED ORDNANCE (UXO) HAZARDS 1. Background a. Saturation of unexploded submunitions has become a characteristic of the modern battlefield. The potential for fratricide from UXO
APRIL Soldier Protection Today. By Lauren Fish and Paul Scharre
 APRIL 2018 Soldier Protection Today By Lauren Fish and Paul Scharre 1 ABOUT THE AUTHORS Lauren Fish is a Research Associate with the Defense Strategies and Assessments Program at CNAS. Paul Scharre is
APRIL 2018 Soldier Protection Today By Lauren Fish and Paul Scharre 1 ABOUT THE AUTHORS Lauren Fish is a Research Associate with the Defense Strategies and Assessments Program at CNAS. Paul Scharre is
The Evolution of Battlefield Surgery Post Damage Control Surgery
 The Evolution of Battlefield Surgery Post- 9-11 & Damage Control Surgery LTC DUANE DUKE MD FACS Division Chief of Pediatric Surgery USU Walter Reed Surgery 19OCT2016 Disclosure I have no personal or professional
The Evolution of Battlefield Surgery Post- 9-11 & Damage Control Surgery LTC DUANE DUKE MD FACS Division Chief of Pediatric Surgery USU Walter Reed Surgery 19OCT2016 Disclosure I have no personal or professional
HOSPITALS TO ENTER PATIENTS INTO THE
 PATIENT CRITERIA FOR HOSPITALS TO ENTER PATIENTS INTO THE TRAUMA SYSTEM 1 THE ALABAMA TRAUMA SYSTEM IS UNIQUE NOT ONLY ARE THE TRAUMA HOSPITALS INSPECTED AND CERTIFIED BUT ALSO THEIR CRITICAL RESOURCES
PATIENT CRITERIA FOR HOSPITALS TO ENTER PATIENTS INTO THE TRAUMA SYSTEM 1 THE ALABAMA TRAUMA SYSTEM IS UNIQUE NOT ONLY ARE THE TRAUMA HOSPITALS INSPECTED AND CERTIFIED BUT ALSO THEIR CRITICAL RESOURCES
Medical Advances as a Result of War
 trauma medical director Michael Iwanicki, DO trauma surgeons James P. Cole, Jr., DO, FACS Vijay Nair, MD, FRCS Jeffrey Rosen, MD, FACS director, emergency, emss & trauma division Ginger Diven, RN trauma/emss
trauma medical director Michael Iwanicki, DO trauma surgeons James P. Cole, Jr., DO, FACS Vijay Nair, MD, FRCS Jeffrey Rosen, MD, FACS director, emergency, emss & trauma division Ginger Diven, RN trauma/emss
Trauma Rotation UMASS Memorial University Campus
 Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
OUT-TAKES FROM VIETNAM
 OUT-TAKES FROM VIETNAM TABLE OF CONTENTS I. Introduction II. Film Outline III. Quiz IV. Lesson #26: Introduction to the Vietnam War V. Lesson #27: Vietnam Veterans VI. Lesson #28: Vietnam Refugees VII.
OUT-TAKES FROM VIETNAM TABLE OF CONTENTS I. Introduction II. Film Outline III. Quiz IV. Lesson #26: Introduction to the Vietnam War V. Lesson #27: Vietnam Veterans VI. Lesson #28: Vietnam Refugees VII.
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 506 Perform Aid Station Procedures TERMINAL LEARNING OBJECTIVES 1. In various environments, given standard field
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 506 Perform Aid Station Procedures TERMINAL LEARNING OBJECTIVES 1. In various environments, given standard field
Trauma and Injury Subcommittee: Battlefield Research, Development, Test and Evaluation Priorities. Norman McSwain, MD Subcommittee Member
 Trauma and Injury Subcommittee: Battlefield Research, Development, Test and Evaluation Priorities Norman McSwain, MD Subcommittee Member Defense Health Board November 27, 2012 1 Trauma and Injury Subcommittee
Trauma and Injury Subcommittee: Battlefield Research, Development, Test and Evaluation Priorities Norman McSwain, MD Subcommittee Member Defense Health Board November 27, 2012 1 Trauma and Injury Subcommittee
Disaster Preparedness for
 Disaster Preparedness for Surgeons Charles M. Little, DO FACEP Associate Professor Division of Emergency Medicine University i of Colorado Denver School of Medicine Charles.Little@ucdenver.edu Today s
Disaster Preparedness for Surgeons Charles M. Little, DO FACEP Associate Professor Division of Emergency Medicine University i of Colorado Denver School of Medicine Charles.Little@ucdenver.edu Today s
1. Receives report from EMS and/or outlying facility. 5. Adheres to safety and universal precaution guidelines.
 Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Objectives. Emergency Medicine Risk Factors
 The Uniqueness of Emergency Medicine Risk Management W. Peter Vellman, MD, FACEP Serio Physician Management, LLC Littleton, CO Objectives Recognize key areas impacting the provision of emergency medical
The Uniqueness of Emergency Medicine Risk Management W. Peter Vellman, MD, FACEP Serio Physician Management, LLC Littleton, CO Objectives Recognize key areas impacting the provision of emergency medical
Surgical Legacies of Modern Combat: Translating Battlefield Medical Practices into Civilian Trauma Care
 American College of Surgeons 2017. All rights reserved Worldwide. Surgical Legacies of Modern Combat: Translating Battlefield Medical Practices into Civilian Trauma Care Achieving Zero Preventa bl e Deaths
American College of Surgeons 2017. All rights reserved Worldwide. Surgical Legacies of Modern Combat: Translating Battlefield Medical Practices into Civilian Trauma Care Achieving Zero Preventa bl e Deaths
The Golden Hour: American Battlefield Medicine in World War I
 The Golden Hour: American Battlefield Medicine in World War I George Thompson The University of Kansas Medical Center Zone of the Armies Battlefield Medicine is: Care Under Fire Tactical Field Care
The Golden Hour: American Battlefield Medicine in World War I George Thompson The University of Kansas Medical Center Zone of the Armies Battlefield Medicine is: Care Under Fire Tactical Field Care
Trauma. Level 2. This resident can lead a to recognize common. This resident can. accurately diagnose. team that cares for traumatic conditions and
 Page 1 of 7 Trauma Subject Name Status Employer Program Rotation Evaluation Dates Evaluated by: Evaluator Name Status Employer Program 1 (Trauma) Patient Care: Ward Care This resident is not able lead
Page 1 of 7 Trauma Subject Name Status Employer Program Rotation Evaluation Dates Evaluated by: Evaluator Name Status Employer Program 1 (Trauma) Patient Care: Ward Care This resident is not able lead
Defense Health Agency PROCEDURAL INSTRUCTION
 Defense Health Agency PROCEDURAL INSTRUCTION SUBJECT: Implementation Guidance for the Utilization of DD Form 1380, Tactical Combat Casualty Care (TCCC) Card, June 2014 References: See Enclosure 1 NUMBER
Defense Health Agency PROCEDURAL INSTRUCTION SUBJECT: Implementation Guidance for the Utilization of DD Form 1380, Tactical Combat Casualty Care (TCCC) Card, June 2014 References: See Enclosure 1 NUMBER
SITUATION REPORT occupied Palestinian territory, Gaza 30 May - 3 June 2018
 TYPE OF CASUALTIES TOTAL (353) SITUATION REPORT occupied Palestinian territory, Gaza 30 May - 3 June 2018 OCCUPIED PALESTINIAN TERRITORY 3 KILLED 525 INJURED 10 TRAUMA STABILISATION POINTS 253 ESSENTIAL
TYPE OF CASUALTIES TOTAL (353) SITUATION REPORT occupied Palestinian territory, Gaza 30 May - 3 June 2018 OCCUPIED PALESTINIAN TERRITORY 3 KILLED 525 INJURED 10 TRAUMA STABILISATION POINTS 253 ESSENTIAL
Trauma and Injury Subcommittee: Lessons Learned in Theater Trauma Care in Afghanistan & Iraq. Donald Jenkins, MD Norman McSwain, MD
 Trauma and Injury Subcommittee: Lessons Learned in Theater Trauma Care in Afghanistan & Iraq Donald Jenkins, MD Norman McSwain, MD Defense Health Board November 27, 2012 1 Trauma and Injury Subcommittee
Trauma and Injury Subcommittee: Lessons Learned in Theater Trauma Care in Afghanistan & Iraq Donald Jenkins, MD Norman McSwain, MD Defense Health Board November 27, 2012 1 Trauma and Injury Subcommittee
Chapter 1. Learning Objectives. Learning Objectives 9/11/2012. Introduction to EMS Systems
 Chapter 1 Introduction to EMS Systems Learning Objectives Define the attributes of emergency medical services (EMS) systems List 14 attributes of a functioning EMS system Differentiate the roles and responsibilities
Chapter 1 Introduction to EMS Systems Learning Objectives Define the attributes of emergency medical services (EMS) systems List 14 attributes of a functioning EMS system Differentiate the roles and responsibilities
Medical Operations in Counterinsurgency
 Medical Operations in Counterinsurgency Joining the Fight Maj. David S. Kauvar, M.D., U.S. Army; Maj. Tucker A. Drury, M.D., U.S. Air Force COUNTERINSURGENCY (COIN) CAMPAIGNS generally emphasize nonlethal
Medical Operations in Counterinsurgency Joining the Fight Maj. David S. Kauvar, M.D., U.S. Army; Maj. Tucker A. Drury, M.D., U.S. Air Force COUNTERINSURGENCY (COIN) CAMPAIGNS generally emphasize nonlethal
Tactical Combat Casualty Care. CAPT Peter Rhee, MC, USN MD, MPH, DMCC, FACS, FCCM Professor of Surgery / Molecular Cellular Biology
 Tactical Combat Casualty Care CAPT Peter Rhee, MC, USN MD, MPH, DMCC, FACS, FCCM Professor of Surgery / Molecular Cellular Biology Good medicine in bad places Tactical Care 24 man team raid Building
Tactical Combat Casualty Care CAPT Peter Rhee, MC, USN MD, MPH, DMCC, FACS, FCCM Professor of Surgery / Molecular Cellular Biology Good medicine in bad places Tactical Care 24 man team raid Building
Percent Solution. Because of advances in aeromedical evacuation, most American troops now survive their combat wounds.
 USAF photo by SrA. Brian Ferguson Because of advances in aeromedical evacuation, most American troops now survive their combat wounds. The 90 Percent Solution By Bruce D. Callander and Adam J. Hebert,
USAF photo by SrA. Brian Ferguson Because of advances in aeromedical evacuation, most American troops now survive their combat wounds. The 90 Percent Solution By Bruce D. Callander and Adam J. Hebert,
The Israeli Experience
 E.M.S Response To Terrorism The Israeli Experience GUY CASPI Chief MCI Instructor and Director of Exercises and Operational Training MAGEN DAVID ADOM IN ISRAEL Israel National EMS and Blood Services guyc@mda.org.il
E.M.S Response To Terrorism The Israeli Experience GUY CASPI Chief MCI Instructor and Director of Exercises and Operational Training MAGEN DAVID ADOM IN ISRAEL Israel National EMS and Blood Services guyc@mda.org.il
THE ARMS TRADE TREATY REPORTING TEMPLATE
 THE ARMS TRADE TREATY REPORTING TEMPLATE ANNUAL REPORT IN ACCORDANCE WITH ARTICLE 13(3) - EXPORTS AND IMPORTS OF CONVENTIONAL ARMS COVERED UNDER ARTICLE 2 (1) This provisional template is intended for
THE ARMS TRADE TREATY REPORTING TEMPLATE ANNUAL REPORT IN ACCORDANCE WITH ARTICLE 13(3) - EXPORTS AND IMPORTS OF CONVENTIONAL ARMS COVERED UNDER ARTICLE 2 (1) This provisional template is intended for
PHYSICIAN ASSISTANTS IN TACTICAL MEDICINE TRAINING PROGRAMS
 Physician Assistants in Tactical Medicine Training Programs Chapter 21 PHYSICIAN ASSISTANTS IN TACTICAL MEDICINE TRAINING PROGRAMS Felipe Galvan, PA-C, MPAS; Todd P. Kielman, PA-C, MPAS; Robert M. Levesque,
Physician Assistants in Tactical Medicine Training Programs Chapter 21 PHYSICIAN ASSISTANTS IN TACTICAL MEDICINE TRAINING PROGRAMS Felipe Galvan, PA-C, MPAS; Todd P. Kielman, PA-C, MPAS; Robert M. Levesque,
ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221. I. Title Trauma team Activation Protocol/Roles & Responsibilities of the Trauma Team
 Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221 Subject: Trauma Team Activation Protocol/Roles & Responsibilities of the Trauma Team Trauma Coordinator UTMB respects the diverse culture
Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221 Subject: Trauma Team Activation Protocol/Roles & Responsibilities of the Trauma Team Trauma Coordinator UTMB respects the diverse culture
STAG TRAUMA. Quality Indicators
 STAG TRAUMA Quality Indicators Document Control Document Control Version Quality Indicators V3.3.doc Date Issued 03-09-2013 Author(s) Kirsty Ward Other Related Documents Comments to Angela Khan Document
STAG TRAUMA Quality Indicators Document Control Document Control Version Quality Indicators V3.3.doc Date Issued 03-09-2013 Author(s) Kirsty Ward Other Related Documents Comments to Angela Khan Document
How Battle Field Experience Leads to Improvement in Orthopaedic Care BRETT COURTENAY RAAMC
 How Battle Field Experience Leads to Improvement in Orthopaedic Care BRETT COURTENAY RAAMC Outline Winners from War Medical and Munitions Technology Insurgency Warfare Medical Challenges and Solutions
How Battle Field Experience Leads to Improvement in Orthopaedic Care BRETT COURTENAY RAAMC Outline Winners from War Medical and Munitions Technology Insurgency Warfare Medical Challenges and Solutions
"We were wrong, terribly wrong. We owe it to future generations to explain why." McNamara, writing in his 1995 memoir, In Retrospect, on the
 TLW Objectives 1. Explain the reasons for the escalation of the Vietnam War. 2. Explain the draft policies that led to the Vietnam War becoming a working-class war. 3. Describe the military tactics and
TLW Objectives 1. Explain the reasons for the escalation of the Vietnam War. 2. Explain the draft policies that led to the Vietnam War becoming a working-class war. 3. Describe the military tactics and
Joint Theater Trauma System Clinical Practice Guideline
 BATTLE AND NON-BATTLE INJURY DOCUMENTATION: THE RESUSCITATION RECORD Original Release/Approval 1 Jun 2008 Note: This CPG requires an annual review. Reviewed: Sep 2012 Approved: 18 Sep 2012 Supersedes:
BATTLE AND NON-BATTLE INJURY DOCUMENTATION: THE RESUSCITATION RECORD Original Release/Approval 1 Jun 2008 Note: This CPG requires an annual review. Reviewed: Sep 2012 Approved: 18 Sep 2012 Supersedes:
9/5/2017. Pulse Nightclub Tragedy. Pulse Nightclub Tragedy. Pulse Nightclub: Deadliest Mass Shooting In U.S. History
 Pulse Nightclub: Deadliest Mass Shooting In U.S. History Joseph A. Ibrahim, MD FACS Michael L. Cheatham, MD FACS Pulse Nightclub Tragedy Pulse Nightclub Tragedy 1 Pulse Nightclub Tragedy Orlando Regional
Pulse Nightclub: Deadliest Mass Shooting In U.S. History Joseph A. Ibrahim, MD FACS Michael L. Cheatham, MD FACS Pulse Nightclub Tragedy Pulse Nightclub Tragedy 1 Pulse Nightclub Tragedy Orlando Regional
Government of Azerbaijan
 15. EXPLOSIVE ORDNANCE DISPOSAL (EOD) 1. General Explosive Ordnance Disposal (EOD) is the detection, identification, rendering safe, recovery and final disposal of Unexploded Ordnance (UXO), which has
15. EXPLOSIVE ORDNANCE DISPOSAL (EOD) 1. General Explosive Ordnance Disposal (EOD) is the detection, identification, rendering safe, recovery and final disposal of Unexploded Ordnance (UXO), which has
Navy Medicine. Commander s Guidance
 Navy Medicine Commander s Guidance For over 240 years, our Navy and Marine Corps has been the cornerstone of American security and prosperity. Navy Medicine has been there every day as an integral part
Navy Medicine Commander s Guidance For over 240 years, our Navy and Marine Corps has been the cornerstone of American security and prosperity. Navy Medicine has been there every day as an integral part
Air Force MEDEVAC Kvoup!Foufsubjonfou 6112!Xjmtijsf!Cmwe-!Tuf!223 Mpt!Bohfmft-!DB!: gby xxx/kvoupfou/dpn
 Air Force MEDEVAC Since 2004, over 56,000 Soldiers, Marines and Sailors have been aeromedically evacuated from Iraq and Afghanistan. The process of saving lives and then safely transporting critically
Air Force MEDEVAC Since 2004, over 56,000 Soldiers, Marines and Sailors have been aeromedically evacuated from Iraq and Afghanistan. The process of saving lives and then safely transporting critically
Memoria. deeply. laid. of those. edge any. I would like. us who. among. have. console. adequately. today. danger. It is the. who.
 2017 remarks for DAV representatives at Memoria al Day events SPEECH (Acknowledgement of introduction, distinguished guests, officers and members of the DAV and Auxiliary, and others who are present) Thank
2017 remarks for DAV representatives at Memoria al Day events SPEECH (Acknowledgement of introduction, distinguished guests, officers and members of the DAV and Auxiliary, and others who are present) Thank
THE ARMS TRADE TREATY REPORTING TEMPLATE
 THE ARMS TRADE TREATY REPORTING TEMPLATE ANNUAL REPORT IN ACCORDANCE WITH ARTICLE 13(3) - EXPORTS AND IMPORTS OF CONVENTIONAL ARMS COVERED UNDER ARTICLE 2 (1) This provisional template is intended for
THE ARMS TRADE TREATY REPORTING TEMPLATE ANNUAL REPORT IN ACCORDANCE WITH ARTICLE 13(3) - EXPORTS AND IMPORTS OF CONVENTIONAL ARMS COVERED UNDER ARTICLE 2 (1) This provisional template is intended for
ARLINGTON COUNTY FIRE DEPARTMENT STANDARD OPERATING PROCEDURES
 R SUBJECT: ARLINGTON COUNTY FIRE DEPARTMENT STANDARD OPERATING PROCEDURES Rescue Task Force Response SOP# A.* * /Cat * Initiated APPROVED: James Schw artz Fire Chief Revised A. PURPOSE To establish policies
R SUBJECT: ARLINGTON COUNTY FIRE DEPARTMENT STANDARD OPERATING PROCEDURES Rescue Task Force Response SOP# A.* * /Cat * Initiated APPROVED: James Schw artz Fire Chief Revised A. PURPOSE To establish policies
Pulse Nightclub: Deadliest Mass Shooting In U.S. History William Havron III MD FACS General Surgery Program Director - ORMC
 Pulse Nightclub: Deadliest Mass Shooting In U.S. History William Havron III MD FACS General Surgery Program Director - ORMC Pulse Nightclub Tragedy Pulse Nightclub Tragedy Pulse Nightclub Tragedy Orlando
Pulse Nightclub: Deadliest Mass Shooting In U.S. History William Havron III MD FACS General Surgery Program Director - ORMC Pulse Nightclub Tragedy Pulse Nightclub Tragedy Pulse Nightclub Tragedy Orlando
Global Vigilance, Global Reach, Global Power for America
 Global Vigilance, Global Reach, Global Power for America The World s Greatest Air Force Powered by Airmen, Fueled by Innovation Gen Mark A. Welsh III, USAF The Air Force has been certainly among the most
Global Vigilance, Global Reach, Global Power for America The World s Greatest Air Force Powered by Airmen, Fueled by Innovation Gen Mark A. Welsh III, USAF The Air Force has been certainly among the most
The Royal College of Surgeons of England
 The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
Hemorrhage Control by Law Enforcement Personnel: A Survey of Knowledge Translation From the Military Combat Experience
 MILITARY MEDICINE, 180, 6:615, 2015 Hemorrhage Control by Law Enforcement Personnel: A Survey of Knowledge Translation From the Military Combat Experience Sara J. Aberle, MD*; Andrew J. Dennis, DO, FACOS
MILITARY MEDICINE, 180, 6:615, 2015 Hemorrhage Control by Law Enforcement Personnel: A Survey of Knowledge Translation From the Military Combat Experience Sara J. Aberle, MD*; Andrew J. Dennis, DO, FACOS
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems NPSS Asheville, NC
 Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
MRI Patient Screening and History
 Griffin Imaging, LLC 220 Rock Street Griffin, GA 30224 (770) 229-4660 Fax:: (770) 229-4632 Specializing In Open MRI, CT & Ultrasound MRI Patient Screening and History Patient Information Sheet PATIENT
Griffin Imaging, LLC 220 Rock Street Griffin, GA 30224 (770) 229-4660 Fax:: (770) 229-4632 Specializing In Open MRI, CT & Ultrasound MRI Patient Screening and History Patient Information Sheet PATIENT
CHAPTER 2 THE ARMORED CAVALRY
 CHAPTER 2 THE ARMORED CAVALRY Section I. ARMORED CAVALRY REGIMENT 2-1. Organization The armored cavalry regiment (ACR) is used by the corps commander as a reconnaissance and security force; it is strong
CHAPTER 2 THE ARMORED CAVALRY Section I. ARMORED CAVALRY REGIMENT 2-1. Organization The armored cavalry regiment (ACR) is used by the corps commander as a reconnaissance and security force; it is strong
SITUATION REPORT occupied Palestinian territory, Gaza 4-11 June 2018
 SITUATION REPORT occupied Palestinian territory, Gaza 4-11 June 2018 OCCUPIED PALESTINIAN TERRITORY 4 KILLED 701 INJURED 10 TRAUMA STABILISATION POINTS 253 ESSENTIAL DRUGS IMMEDIATELY NEEDED 243 ESSENTIAL
SITUATION REPORT occupied Palestinian territory, Gaza 4-11 June 2018 OCCUPIED PALESTINIAN TERRITORY 4 KILLED 701 INJURED 10 TRAUMA STABILISATION POINTS 253 ESSENTIAL DRUGS IMMEDIATELY NEEDED 243 ESSENTIAL
THE ARMS TRADE TREATY REPORTING TEMPLATE
 THE ARMS TRADE TREATY REPORTING TEMPLATE ANNUAL REPORT IN ACCORDANCE WITH ARTICLE 13(3) - EXPORTS AND IMPORTS OF CONVENTIONAL ARMS COVERED UNDER ARTICLE 2 (1) This provisional template is intended for
THE ARMS TRADE TREATY REPORTING TEMPLATE ANNUAL REPORT IN ACCORDANCE WITH ARTICLE 13(3) - EXPORTS AND IMPORTS OF CONVENTIONAL ARMS COVERED UNDER ARTICLE 2 (1) This provisional template is intended for
Contents. The Event 12/29/2016. The Event The Aftershock The Recovery Lessons Learned Discussion Summary
 #OrlandoUnited: Coordinating the medical response to the Pulse nightclub shooting Christopher Hunter, M.D., Ph.D. Director, Orange County Health Services Department Associate Medical Director, Orange County
#OrlandoUnited: Coordinating the medical response to the Pulse nightclub shooting Christopher Hunter, M.D., Ph.D. Director, Orange County Health Services Department Associate Medical Director, Orange County
Resource classification Personnel. 6 NIMS (3 of 3) Major NIMS components: Command and management
 Major NIMS components: Command and management") 1 Chapter 38 Incident Management and Triage 2 Incident Command System (1 of 2) ICS=An organized approach for dealing with operations. ICS is used to help control, direct, and coordinate resources. It ensures
1 Chapter 38 Incident Management and Triage 2 Incident Command System (1 of 2) ICS=An organized approach for dealing with operations. ICS is used to help control, direct, and coordinate resources. It ensures
Women who ve paid the cost of war
 Women who ve paid the cost of war Women throughout history who have sacrificed everything for their country are not forgotten but thanked this Women s History Month By signing up for newly opened combat
Women who ve paid the cost of war Women throughout history who have sacrificed everything for their country are not forgotten but thanked this Women s History Month By signing up for newly opened combat
people can remember our breed of men and
 Memorial Day 2012 Fallen, Never Forgotten It is a tremendo ous honor to
Memorial Day 2012 Fallen, Never Forgotten It is a tremendo ous honor to
THE ARMS TRADE TREATY PROVISIONAL TEMPLATE
 27 August 2015 Submitted by: Facilitator on Reporting, Sweden Original: English Arms Trade Treaty First Conference of States Parties Cancun, Mexico, 24-27 August, 2015 THE ARMS TRADE TREATY PROVISIONAL
27 August 2015 Submitted by: Facilitator on Reporting, Sweden Original: English Arms Trade Treaty First Conference of States Parties Cancun, Mexico, 24-27 August, 2015 THE ARMS TRADE TREATY PROVISIONAL
MASS CASUALTY SITUATIONS
 APPENDIX J MASS CASUALTY SITUATIONS J-1. General Mass casualty situations occur when the number of casualties exceeds the available medical capability to rapidly treat and evacuate them. In disaster relief
APPENDIX J MASS CASUALTY SITUATIONS J-1. General Mass casualty situations occur when the number of casualties exceeds the available medical capability to rapidly treat and evacuate them. In disaster relief
3/15/12. Chris attended St. Mary s Catholic School and Clarksville High School. As a senior in high school he decided he would join the army.
 Benjamin F. & Raiford T. Ammons circa 1862. Christopher D. Ammons was born in Norfolk, Virginia on April 18, 1948, the son of Benjamin Troy Ammons and Ester Magna Randolph Ammons of Jackson, TN. The Ammons
Benjamin F. & Raiford T. Ammons circa 1862. Christopher D. Ammons was born in Norfolk, Virginia on April 18, 1948, the son of Benjamin Troy Ammons and Ester Magna Randolph Ammons of Jackson, TN. The Ammons
25 February. Prepared for: National Collegiate Emergency Medical Services Foundation. Conference 2006 Boston, Massachusetts
 25 February Prepared for: National Collegiate Emergency Medical Services Foundation Conference 2006 Boston, Massachusetts What Is Lessons Learned Information Sharing? Online since April 19, 2004 Over 20,000
25 February Prepared for: National Collegiate Emergency Medical Services Foundation Conference 2006 Boston, Massachusetts What Is Lessons Learned Information Sharing? Online since April 19, 2004 Over 20,000
Development of Emergency Medicine in the Far East. Prof V. Anantharaman Department of Emergency Medicine Singapore General Hospital
 Development of Emergency Medicine in the Far East Prof V. Anantharaman Department of Emergency Medicine Singapore General Hospital Prof V. Anantharaman MBBS (S pore), FRCP (Edin), FRCS Ed (A&E), FAMS,
Development of Emergency Medicine in the Far East Prof V. Anantharaman Department of Emergency Medicine Singapore General Hospital Prof V. Anantharaman MBBS (S pore), FRCP (Edin), FRCS Ed (A&E), FAMS,
2nd Lt. Elizabeth Ann Jones Sept. 12, 1943 Feb. 18, 1966 Even as a little girl growing up in South Carolina,
 (8) Nurses The Angels of Vietnam 2nd Lt. Carol Ann Elizabeth Drazba Dec. 11, 1943 Feb. 18, 1966 Carol Ann Drazba was one of the first two women to die in Vietnam. Described by family and friends as always
(8) Nurses The Angels of Vietnam 2nd Lt. Carol Ann Elizabeth Drazba Dec. 11, 1943 Feb. 18, 1966 Carol Ann Drazba was one of the first two women to die in Vietnam. Described by family and friends as always
Patterns of Injury in Hospitalized Terrorist Victims
 Patterns of Injury in Hospitalized Terrorist Victims KOBI PELEG, PHD, MPH,* LIMOR AHARONSON-DANIEL, PHD,* MICHAEL MICHAEL, MD, S.C. SHAPIRA, MD, MPH, AND THE ISRAEL TRAUMA GROUP Acts of terror increase
Patterns of Injury in Hospitalized Terrorist Victims KOBI PELEG, PHD, MPH,* LIMOR AHARONSON-DANIEL, PHD,* MICHAEL MICHAEL, MD, S.C. SHAPIRA, MD, MPH, AND THE ISRAEL TRAUMA GROUP Acts of terror increase
FOR OFFICIAL USE ONLY UNTIL RELEASED BY THE SENATE ARMED SERVICES COMMITTEE STATEMENT OF COLONEL STEPHEN L. JONES, UNITED STATES ARMY COMMAND SURGEON
 FOR OFFICIAL USE ONLY UNTIL RELEASED BY THE SENATE ARMED SERVICES COMMITTEE STATEMENT OF COLONEL STEPHEN L. JONES, UNITED STATES ARMY COMMAND SURGEON UNITED STATES SOUTHERN COMMAND BEFORE THE 107 TH CONGRESS
FOR OFFICIAL USE ONLY UNTIL RELEASED BY THE SENATE ARMED SERVICES COMMITTEE STATEMENT OF COLONEL STEPHEN L. JONES, UNITED STATES ARMY COMMAND SURGEON UNITED STATES SOUTHERN COMMAND BEFORE THE 107 TH CONGRESS
Pediatric Disaster Management and the School System
 Pediatric Disaster Management and the School System Greg Pereira, MBA, RN, CPEN Director of Trauma And Transport Objectives Discuss relationship between Emergency Preparedness and the Community in relation
Pediatric Disaster Management and the School System Greg Pereira, MBA, RN, CPEN Director of Trauma And Transport Objectives Discuss relationship between Emergency Preparedness and the Community in relation
THE ARMS TRADE TREATY REPORTING TEMPLATE
 THE ARMS TRADE TREATY REPORTING TEMPLATE ANNUAL REPORT IN ACCORDANCE WITH ARTICLE 13(3) - EXPORTS AND IMPORTS OF CONVENTIONAL ARMS COVERED UNDER ARTICLE 2 (1) This provisional template is intended for
THE ARMS TRADE TREATY REPORTING TEMPLATE ANNUAL REPORT IN ACCORDANCE WITH ARTICLE 13(3) - EXPORTS AND IMPORTS OF CONVENTIONAL ARMS COVERED UNDER ARTICLE 2 (1) This provisional template is intended for
Effective Date: 7/2004
 MEDICAL STAFF POLICY & PROCEDURE Page 1 of 6 Effective Date: 7/2004 Review/Revised: 9/1/2011 Policy No. MSP 003 Purpose: To assure that physicians at all levels are familiar with their roles during the
MEDICAL STAFF POLICY & PROCEDURE Page 1 of 6 Effective Date: 7/2004 Review/Revised: 9/1/2011 Policy No. MSP 003 Purpose: To assure that physicians at all levels are familiar with their roles during the
THE ARMS TRADE TREATY REPORTING TEMPLATE
 ANNEX 2 ANNUAL REPORTING TEMPLATE THE ARMS TRADE TREATY REPORTING TEMPLATE ANNUAL REPORT IN ACCORDANCE WITH ARTICLE 13(3) - EXPORTS AND IMPORTS OF CONVENTIONAL ARMS COVERED UNDER ARTICLE 2 (1) This provisional
ANNEX 2 ANNUAL REPORTING TEMPLATE THE ARMS TRADE TREATY REPORTING TEMPLATE ANNUAL REPORT IN ACCORDANCE WITH ARTICLE 13(3) - EXPORTS AND IMPORTS OF CONVENTIONAL ARMS COVERED UNDER ARTICLE 2 (1) This provisional
Military Radar Applications
 Military Radar Applications The Concept of the Operational Military Radar The need arises during the times of the hostilities on the tactical, operational and strategic levels. General importance defensive
Military Radar Applications The Concept of the Operational Military Radar The need arises during the times of the hostilities on the tactical, operational and strategic levels. General importance defensive
N: Emergency Nursing. Alberta Licensed Practical Nurses Competency Profile 135
 N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
THE ARMS TRADE TREATY REPORTING TEMPLATE
 THE ARMS TRADE TREATY REPORTING TEMPLATE ANNUAL REPORT IN ACCORDANCE WITH ARTICLE 13(3) - EXPORTS AND IMPORTS OF CONVENTIONAL ARMS COVERED UNDER ARTICLE 2 (1) This provisional template is intended for
THE ARMS TRADE TREATY REPORTING TEMPLATE ANNUAL REPORT IN ACCORDANCE WITH ARTICLE 13(3) - EXPORTS AND IMPORTS OF CONVENTIONAL ARMS COVERED UNDER ARTICLE 2 (1) This provisional template is intended for
After action report Musings From Landstuhl Regional Medical Center July 8-30, Norman McSwain, Jr MD, FAC S
 After action report Musings From Landstuhl Regional Medical Center July 8-30, 20007 Norman McSwain, Jr MD, FAC S This was the most enjoyable, educational and, yes, awesome 3 weeks of my life. Why? Two
After action report Musings From Landstuhl Regional Medical Center July 8-30, 20007 Norman McSwain, Jr MD, FAC S This was the most enjoyable, educational and, yes, awesome 3 weeks of my life. Why? Two
Active Shooter Guideline
 1. Purpose: This procedure establishes guidelines for Monterey County Public Safety Personnel who respond to Active Shooter Incidents (ASI). The goal is to provide effective rescue and treatment procedures,
1. Purpose: This procedure establishes guidelines for Monterey County Public Safety Personnel who respond to Active Shooter Incidents (ASI). The goal is to provide effective rescue and treatment procedures,
History of Trauma Surgery
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-disaster-medicine-and-preparedness/history-of-traumasurgery/1500/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-disaster-medicine-and-preparedness/history-of-traumasurgery/1500/
Incident title: Prison fire
 Incident title: Prison fire Reporter Incident location Dr. Patricio Cortés Picazo Director EMS SAMU Metropolitano Santiago de Chile 2010-2013 Emergency Medical Services SAMU Metropolitano Santiago de Chile
Incident title: Prison fire Reporter Incident location Dr. Patricio Cortés Picazo Director EMS SAMU Metropolitano Santiago de Chile 2010-2013 Emergency Medical Services SAMU Metropolitano Santiago de Chile
Descriptive Summary of Patients Seen at The Surgical Companies During Operation Iraqi Freedom-1
 NAVAL HEALTH RESEARCH CENTER Descriptive Summary of Patients Seen at The Surgical Companies During Operation Iraqi Freedom-1 G. J. Walker J. Zouris M. F. Galarneau J. Dye Report No. 04-39 Approved for
NAVAL HEALTH RESEARCH CENTER Descriptive Summary of Patients Seen at The Surgical Companies During Operation Iraqi Freedom-1 G. J. Walker J. Zouris M. F. Galarneau J. Dye Report No. 04-39 Approved for
The US military is currently engaged in prolonged conflicts
 The Journal of TRAUMA Injury, Infection, and Critical Care Combat Wounds in Operation Iraqi Freedom and Operation Enduring Freedom Brett D. Owens, MD, John F. Kragh, Jr, MD, Joseph C. Wenke, PhD, Joseph
The Journal of TRAUMA Injury, Infection, and Critical Care Combat Wounds in Operation Iraqi Freedom and Operation Enduring Freedom Brett D. Owens, MD, John F. Kragh, Jr, MD, Joseph C. Wenke, PhD, Joseph
FOR IMMEDIATE RELEASE No June 27, 2001 THE ARMY BUDGET FISCAL YEAR 2002
 FOR IMMEDIATE RELEASE No. 01-153 June 27, 2001 THE ARMY BUDGET FISCAL YEAR 2002 Today, the Army announced details of its budget for Fiscal Year 2002, which runs from October 1, 2001 through September 30,
FOR IMMEDIATE RELEASE No. 01-153 June 27, 2001 THE ARMY BUDGET FISCAL YEAR 2002 Today, the Army announced details of its budget for Fiscal Year 2002, which runs from October 1, 2001 through September 30,
"We were wrong, terribly wrong. We owe it to future generations to explain why." McNamara, writing in his 1995 memoir, In Retrospect, on the
 "We were wrong, terribly wrong. We owe it to future generations to explain why." McNamara, writing in his 1995 memoir, In Retrospect, on the management of the Vietnam War. 3 Major Mistakes Made In Vietnam:
"We were wrong, terribly wrong. We owe it to future generations to explain why." McNamara, writing in his 1995 memoir, In Retrospect, on the management of the Vietnam War. 3 Major Mistakes Made In Vietnam:
Combat orthopedic trauma
 Combat orthopedic trauma Przemysław Guła 1, Tomasz Wiśniewski 2, Kimberly Broughton 3, Robert Brzozowski 1 Original article/artykuł oryginalny J ORTHOP TRAUMA SURG REL RES 1 (34-35) 2014 1 Military Institute
Combat orthopedic trauma Przemysław Guła 1, Tomasz Wiśniewski 2, Kimberly Broughton 3, Robert Brzozowski 1 Original article/artykuł oryginalny J ORTHOP TRAUMA SURG REL RES 1 (34-35) 2014 1 Military Institute
Title: ED Management of Trauma Patient Protocol
 Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review: