Surgical Legacies of Modern Combat: Translating Battlefield Medical Practices into Civilian Trauma Care
|
|
|
- Louisa Doyle
- 6 years ago
- Views:
Transcription


1 American College of Surgeons All rights reserved Worldwide. Surgical Legacies of Modern Combat: Translating Battlefield Medical Practices into Civilian Trauma Care Achieving Zero Preventa bl e Deaths Conferenc e April 18-19, 2017 B r i a n E a s t r i d g e, M D, F A C S C O L, M C, U S A R P r o f e s s o r o f S u r g e r y U n i v e r s i t y o f T e x a s H e a l t h S a n A n t o n i o
2 Disclosures None Disclaimer The opinions or assertions contained herein are the private views of the author and are not to be construed as official or as reflecting the views of the Department of the Army or the Department of Defense.
3 War s Role as a Teacher For Antiquity He who would become a surgeon should join an army and follow it for war is the only proper school for a surgeon..
4 World War I IV fluids Blood transfusions Motorized ambulances Topical antisepsis History of Battlefield Medical Lessons Korean Conflict Improved fluid resuscitation Forward availability of definitive surgery Helicopters for patient evac/transport Primary repair/grafts for vascular injury World War II Whole blood/plasma available Specialty-specific surgical groups Antibiotics Fixed wing aero-medical evacuation Desert Shield/Storm Burn team augmentation of evacuation hospitals to provide theater-wide burn care Intercontinental aeromedical Vietnam transport of burn patients Improved use of helicopters Improved laboratory support Portable radiology equipment Mechanical ventilators in theater
5 Contemporary Battlefield Lessons Learned Joint Trauma System Focused empiricism / timely dissemination of knowledge Performance Improvement / generation of best practices Epidemiology of injury death Tactical Combat Casualty Care Acute surgical care Damage control resuscitation Forward surgical elements Serial damage control surgery
6 Genesis of the Military Trauma System Effort Review of Battlefield Medical Care Army Trauma Consultant 2003 Unorganized delivery of trauma care on the battlefield Casualties going to the wrong location Suboptimal staffing and placement of surgical assets Medical records are not reliably being delivered with casualties at each level (<40%) Impact on clinical care Documentation directive No trauma registry driven by medical input that allows accurate description of injuries or deaths Unable to reliably answer questions and improve outcomes Survivable Injuries and/or deaths Lack of performance improvement measures / research
7 American College of Surgeons All rights reserved Worldwide. Battlefield Lesson Learning Healthcare System

8 Joint Trauma System Operational Cycle TRAUMA CARE DELIVERY PERFORMANCE IMPROVEMENT DATA ANALYSIS DOD TRAUMA REGISTRY FIGURE 4-3 Joint Trauma System operational cycle and links to the U.S. Department of Defense s Combat Casualty Care Research Program. NOTE: DoD = U.S. Department of Defense; PI = performance improvement. SOURCE: Haut et al., 2016.






9 JTS Directorate Functions and Services Performance Improvement Reports Clinical Practice Guidelines Concurrent Reports Special Projects

10 Clinical Practice Guidelines Evidence-based Best clinical practice Tailored to operational battlefield environment Open access Resource for deploying surgeons and medical providers
11 Focused Epiricism Pragmatic approach to process improvement Urgency to improve outcomes because of high morbidity and mortality rates High-quality data are not available to inform clinical practice changes Data collection is possible. Principle of focused empiricism is using the best data available in combination with clinical experience to develop clinical practice guidelines through an iterative process Successes Damage control resuscitation Whole blood for massive transfusion Tranexamic acid Failures Factor VIIa
12 Avg Number of Units Average Component Units per Massive Transfusion Deployment of 1st JTTS trauma team Aug 2004 Official Massive Transfusion CPG issued Dec PRBC FFP 10 Whole Blood Platelets Year
13 Damage Control Resuscitation Compliance 70.0% 60.0% IRAQ AFGHANISTAN 50.0% 40.0% 30.0% Crude Adherence Rate Death Rate 20.0% 10.0% 0.0%
14 American College of Surgeons All rights reserved Worldwide. Battlefield Lesson Epidemiology of Prehospital Trauma Mortality
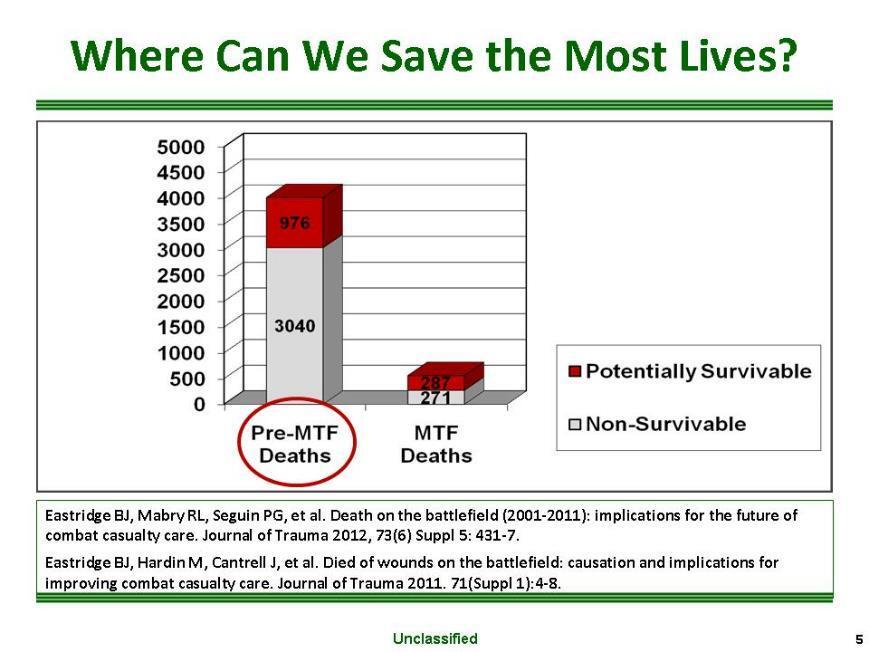
15 DOW KIA
16
 13.")



")
 64%")
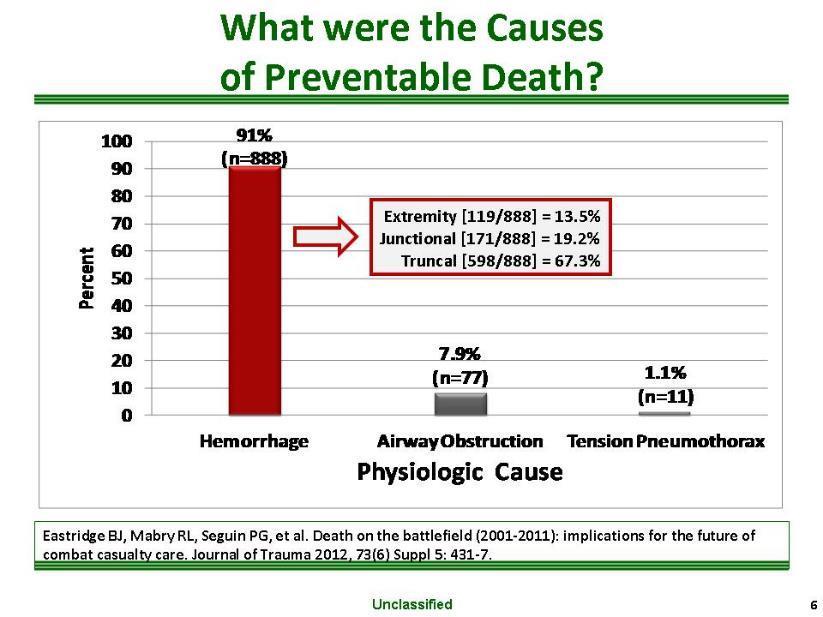
17 Hemorrhage Focus (n=888) 13.5% n=119 Truncal Junctional 19.2% n= % n=598 Extremity 39% Cervical (max AIS 1) 61% Axilla and Groin (max AIS 5) 36% Thoracic (max AIS 3) 64% Abdominopelvic (max AIS 4/5)

18 Eliminating Preventable Death on the Battlefield US Military Preventable Prehospital Deaths = 25% US Rangers Preventable Deaths = 3% Ranger success attribution: Leadership Command-directed casualty response program Training All Rangers and Docs trained in TCCC Kotwal RS, Montgomery HR, Kotwal BM, et al. Eliminating preventable death on the battlefield. Arch Surg 2011.
19 Multi-Disciplinary Multi-Institutional Mortality Investigation in the Civilian Prehospital Environment (MIMIC) Develop a methodology for evaluating the causes and pathophysiology of pre-hospital deaths (optimal & in context) Network of experts to apply the methodology to identify the causes of pre-hospital deaths due to trauma and estimate the potential for survivability. Trauma surgery Neurosurgery Orthopedic surgery Forensic pathology Emergency medicine Emergency medical services
20 Multi-Disciplinary Multi-Institutional Mortality Investigation in the Civilian Prehospital Environment (MIMIC) Define the causes and pathophysiologic mechanisms of 3,000 pre-hospital deaths occurring in six regions of the country representative of the population. Describe the epidemiology of pre-hospital mortality in the context of trauma system development and estimate human and fiscal impact on society. Develop a blueprint for a sustained public health / injury mitigation strategies in the pre-hospital environment, identifying high priority areas for trauma systems performance improvement
21 American College of Surgeons All rights reserved Worldwide. Battlefield Lesson Pre-Hospital Care



22 Tactical Combat Casualty Care Tactical Combat Casualty Care Set of trauma management guidelines customized for the battlefield that focus on the most common causes of preventable deaths on the battlefield: Hemorrhage Noncompressible Junctional Peripheral Airway obstruction Tension pneumothorax Butler FK, Hagmann J, Butler EG. Tactical combat casualty care in special operations. Military Medicine 1996;161(Suppl.):3-16.



23 Pre-Hospital Translation of Lessons Learned Tactical Combat Casualty Care Hartford Consensus Threat suppression Hemorrhage control Rapid Extrication to safety Assessment by medical providers Transport to definitive care Need integrated response Fire, EMS, Law Enforcement, Medical
24 The Hartford Consensus American College of Surgeons FBI White House Medical Policy White House Medical Asst Secretary of Defense - Health Affairs Asst Secretary of Homeland Security Health Affairs Medical Section Major Chiefs of Police ACS Committee on Trauma DoD Committee on TCCC Improving Survival from Active Shooter Events: The Hartford Consensus Active Shooter and Intentional Mass-Casualty Events: The Hartford Consensus II The Hartford Consensus III: Implementation of Bleeding Control The Hartford Consensus IV: A Call for Increased National Resilience 24


25 Pre-Hospital Translation Initiatives LEFR-TCC Law Enforcement First Responder Tactical Casualty Care NAEMT

26 Hemorrhage Control: Tourniquets Kragh, et al Tourniquet Study Ibn Sina Hospital, Baghdad, 2006 Tourniquets are saving lives on the battlefield 31 lives saved in 6 months by use of prehospital tourniquets Kragh JF, Walters TJ, Baer DG, et al. Survival with emergency tourniquet use to stop bleeding in major limb trauma. Annals of Surgery, (1):1-7.
 Transi on (2006-2007)")

27 Impact of Tourniquets on the Battlefield Isolated Extremity Deaths / Year Pre- Tourniquet (Pre 2006) Transi on ( ) Post-Tourniquet (Post 2007) TCCC Interven on Eastridge et al: Death on the Battlefield: Implications for the Future of Combat Casualty Care. J Trauma 2012


28 Civilian Tourniquet Consensus Data strongly suggests that tourniquet use saves lives. Adverse side effects associated with tourniquets appear to be manageable and do not appear to outweigh the benefits of tourniquet use.
29 American College of Surgeons All rights reserved Worldwide. Battlefield Lesson Resuscitation

30 Hemostatic Resuscitation

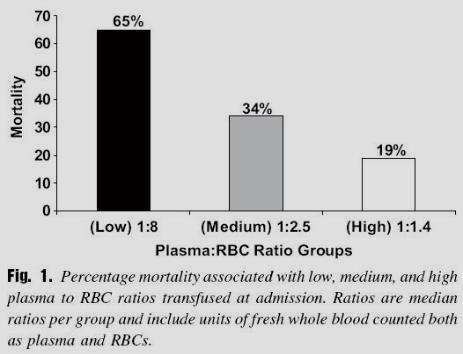
 Holcomb et al JAMA")
31 Civilian Trial Pragmatic Randomized Optimal Platelet and Plasma Ratio Trial (PROPPR) Holcomb et al JAMA 2015;313:

32 Whole Blood Resuscitation in Combat Fresh whole blood use by forward surgical teams in Afghanistan is associated with improved survival compared to component therapy without platelets Transfusion 2013 Shawn C. Nessen, Brian J. Eastridge, Daniel Cronk, Robert M. Craig, Olle Berséus, Richard Ellison, Kyle Remick, Jason Seery, Avani Shah, and Philip C. Spinella FWB in austere combat environments safe and independently associated with improved survival when compared with resuscitation with RBCs and FFP alone.
33 Whole Blood: Back to the Future Whole blood historically primary resuscitative solution for hemorrhagic shock. Transition to using component therapy occurred without evidence superior efficacy or safety. Misconceptions Whole blood must be ABO specific (O low titer 1:256) Whole blood cannot be leukoreduced Cold storage causes loss of platelet function Cold whole blood stored for up to 21 days has greater hemostatic capacity than blood components transfused in a 1 : 1 : 1 (in vitro) Spinella, Cap: Curr Opin Hematol 2016, 23
34 Battlefield Lesson Forward Transitioning Damage Control Philosophy American College of Surgeons All rights reserved Worldwide.


35 Pre-Hospital DCR Concepts Stop obvious hemorrhage Hemostatic adjuncts Correction of coagulopathy Judicious fluid management (permissive hypotension) Thermoregulation Minimize pre-hospital time ( Golden Hour is relative)


36 Golden Hour and the Gates Effect

37 Prehospital Time Noncompressible Torso Hemorrhage (GSW) Critical nature of prehospital time in patients with non-compressible torso hemorrhage. Evacuation times < 30 minutes not realistic, particularly in rural or austere environments. Emphasizes need to develop therapies to increase the window of survival in the prehospital environment. Alarhayem, Eastridge, et al: Mortality in Trauma Patients with Hemorrhage from Alarhayem, Torso Injury Eastridge: Occurs Time Long is Before the Enemy. the Am Golden J Surg 2016 Hour Presented at Southwestern Surgical Congress April 2016

38 Military Tactical DCR Forward FWB is the best prehospital resuscitation fluid 75 th Ranger Regiment program Type O Low Titer Anti-A, Anti-B abs Donors pre-screened for typing, titers, and infectious diseases Use donor pool to transfuse casualties in shock

39 Civilian DCR Forward

40 Prehospital Plasma PAMPer Trial
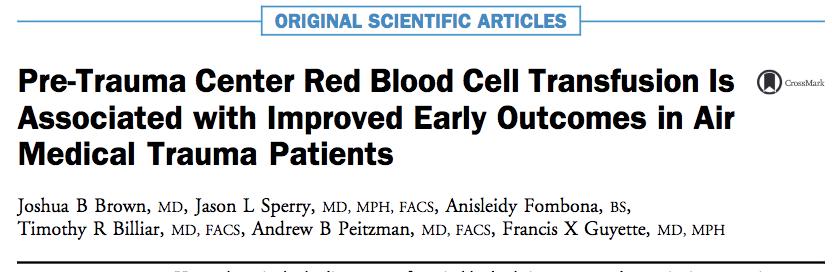

41 Prehospital Blood Outcomes
42 Prehospital Whole Blood Program development /proof of concept in process at several institutions Mayo Clinic University of Pittsburgh University of Texas Health San Antonio / San Antonio Military Medical Center


43 DCR Forward Versus Scoop and Run or Stay and Play? Advanced providers? Critical care capabilities Blood products Surgical capability enroute
44 UK MERT ISS 1-9 ISS ISS > 20 Observed Mortality Expected Mortality Apodaca et al: Performance improvement evaluation of forward aeromedical evacuation platforms in Operation Enduring Freedom.

45 Battlefield Continuum of Care Proof of Concept Forward Surgery Route from Injury to Definitive Care BAS Level 1 CASEVAC 1 Hour Forward Surgical teams Level 2 Surgical Capability TACTICAL EVAC 24 Hours Combat Support Hospital, EMEDS, Fleet Hospital Level 3 STRATEGIC EVAC Hours Definitive Care Level 4
46 Bidirectional
Trauma and Injury Subcommittee: Battlefield Research, Development, Test and Evaluation Priorities. Norman McSwain, MD Subcommittee Member
 Trauma and Injury Subcommittee: Battlefield Research, Development, Test and Evaluation Priorities Norman McSwain, MD Subcommittee Member Defense Health Board November 27, 2012 1 Trauma and Injury Subcommittee
Trauma and Injury Subcommittee: Battlefield Research, Development, Test and Evaluation Priorities Norman McSwain, MD Subcommittee Member Defense Health Board November 27, 2012 1 Trauma and Injury Subcommittee
of Trauma Assembly 28 th Page 1
 Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 11 Preparing for the Next War: Pivotal Military Civilian Relationships January 16, 2015 Disney s Contemporary
Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 11 Preparing for the Next War: Pivotal Military Civilian Relationships January 16, 2015 Disney s Contemporary
Tactical Combat Casualty Care: Transitioning Battlefield Lessons Learned to other Austere Environments
 Tactical Combat Casualty Care: Transitioning Battlefield Lessons Learned to other Austere Environments CAPT (Ret.) Brad Bennett PhD, NREMT-P, FAWM - Chair/Moderator COL Ian Wedmore MD - Co-Chair CAPT (Ret.)
Tactical Combat Casualty Care: Transitioning Battlefield Lessons Learned to other Austere Environments CAPT (Ret.) Brad Bennett PhD, NREMT-P, FAWM - Chair/Moderator COL Ian Wedmore MD - Co-Chair CAPT (Ret.)
JOINT COMMITTEE TO CREATE A NATIONAL POLICY TO ENHANCE SURVIVABILITY FROM MASS CASUALTY SHOOTING EVENTS HARTFORD CONSENSUS II
 July 11, 2013 JOINT COMMITTEE TO CREATE A NATIONAL POLICY TO ENHANCE SURVIVABILITY FROM MASS CASUALTY SHOOTING EVENTS HARTFORD CONSENSUS II Concept to Action On April 2, 2013, representatives from a select
July 11, 2013 JOINT COMMITTEE TO CREATE A NATIONAL POLICY TO ENHANCE SURVIVABILITY FROM MASS CASUALTY SHOOTING EVENTS HARTFORD CONSENSUS II Concept to Action On April 2, 2013, representatives from a select
1/7/2014. Dispatch for fire at Rosslyn, VA metro station Initial dispatch as Box Alarm
 1 Dispatch for fire at Rosslyn, VA metro station Initial dispatch as Box Alarm 4 engines, 2 trucks, 1 rescue, 1 medic unit, 2 battalion chiefs, 1 EMS supervisor, 1 battalion aide First arriving units report
1 Dispatch for fire at Rosslyn, VA metro station Initial dispatch as Box Alarm 4 engines, 2 trucks, 1 rescue, 1 medic unit, 2 battalion chiefs, 1 EMS supervisor, 1 battalion aide First arriving units report
Review of the Defense Health Board s Combat Trauma Lessons Learned from Military Operations of Report. August 9, 2016
 Review of the Defense Health Board s Combat Trauma Lessons Learned from Military Operations of 2001-2013 Report August 9, 2016 1 Problem Statement The survival rate of Service members injured in combat
Review of the Defense Health Board s Combat Trauma Lessons Learned from Military Operations of 2001-2013 Report August 9, 2016 1 Problem Statement The survival rate of Service members injured in combat
Tactical Combat Casualty Care for All Combatants August (Based on TCCC-MP Guidelines ) Introduction to TCCC
 Introduction to TCCC") Tactical Combat Casualty Care for All Combatants August 2017 (Based on TCCC-MP Guidelines 170131) Introduction to TCCC Pretest Pre-Test TCCC Web Link to Video What is TCCC and Why Do I Need to Learn About
Tactical Combat Casualty Care for All Combatants August 2017 (Based on TCCC-MP Guidelines 170131) Introduction to TCCC Pretest Pre-Test TCCC Web Link to Video What is TCCC and Why Do I Need to Learn About
Trauma remains the leading cause of death in adults
 TCCC Standardization The Time Is Now Carl W. Goforth, PhD, RN, CCRN; David Antico, MSN, RN, FNP-BC Trauma remains the leading cause of death in adults worldwide, 1 and a significant portion of those deaths
TCCC Standardization The Time Is Now Carl W. Goforth, PhD, RN, CCRN; David Antico, MSN, RN, FNP-BC Trauma remains the leading cause of death in adults worldwide, 1 and a significant portion of those deaths
Law Enforcement and Public Safety. Medical Response to Trauma: The Hartford Consensus. This module uses information from: Objectives 9/25/2014
 Law Enforcement and Public Safety Medical Response to Trauma: The Hartford Consensus This module uses information from: Improving Survival from Active Shooter Events: The Hartford Consensus Pre-Hospital
Law Enforcement and Public Safety Medical Response to Trauma: The Hartford Consensus This module uses information from: Improving Survival from Active Shooter Events: The Hartford Consensus Pre-Hospital
Law Enforcement and Public Safety. Medical Response to Trauma: The Hartford Consensus
 Law Enforcement and Public Safety Medical Response to Trauma: The Hartford Consensus This module uses information from: Improving Survival from Active Shooter Events: The Hartford Consensus Pre-Hospital
Law Enforcement and Public Safety Medical Response to Trauma: The Hartford Consensus This module uses information from: Improving Survival from Active Shooter Events: The Hartford Consensus Pre-Hospital
of Trauma Assembly 28 th Page 1
 Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 11 Preparing for the Next War: Pivotal Military Civilian Relationships January 16, 215 Disney s Contemporary
Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 11 Preparing for the Next War: Pivotal Military Civilian Relationships January 16, 215 Disney s Contemporary
TCCC for All Combatants 1708 Introduction to TCCC Instructor Guide 1
 TCCC for All Combatants 1708 Introduction to TCCC Instructor Guide 1 1. Tactical Combat Casualty Care for All Combatants August 2017 Introduction to TCCC Tactical Combat Casualty Care is the standard of
TCCC for All Combatants 1708 Introduction to TCCC Instructor Guide 1 1. Tactical Combat Casualty Care for All Combatants August 2017 Introduction to TCCC Tactical Combat Casualty Care is the standard of
Medical Training for U.S. Armed Services Medical Personnel and All Other Combatants
 Medical Training for U.S. Armed Services Medical Personnel and All Other Combatants Military Trauma Care s Learning Health System & its Translation to the Civilian Sector National Association of Emergency
Medical Training for U.S. Armed Services Medical Personnel and All Other Combatants Military Trauma Care s Learning Health System & its Translation to the Civilian Sector National Association of Emergency
Deployment Medicine Operators Course (DMOC)
") Deployment Medicine Operators Course (DMOC) The need has never been more critical to equip those who will first contact the battlefield casualty with lifesaving knowledge to improve survivability. Course
Deployment Medicine Operators Course (DMOC) The need has never been more critical to equip those who will first contact the battlefield casualty with lifesaving knowledge to improve survivability. Course
Battlefield Trauma Systems
 Battlefield Trauma Systems Chapter 35 Battlefield Trauma Systems Introduction A trauma system is an organized, coordinated effort in a defined geographic area that delivers the full range of care to all
Battlefield Trauma Systems Chapter 35 Battlefield Trauma Systems Introduction A trauma system is an organized, coordinated effort in a defined geographic area that delivers the full range of care to all
INSTRUCTOR GUIDE FOR INTRODUCTION TO TCCC-MP
 INSTRUCTOR GUIDE FOR INTRODUCTION TO TCCC-MP 160603 1 1. Introduction to Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Combat Casualty Care is the new standard of care in prehospital
INSTRUCTOR GUIDE FOR INTRODUCTION TO TCCC-MP 160603 1 1. Introduction to Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Combat Casualty Care is the new standard of care in prehospital
High Threat Mass Casualty 1/7/2014. Game changer..
 Changing the Paradigm: Guidelines for High Risk Scenarios E. Reed Smith, MD, FACEP Committee for Tactical Emergency Casualty Care 1 Game changer.. 2 High Threat Mass Casualty What is the traditional teaching
Changing the Paradigm: Guidelines for High Risk Scenarios E. Reed Smith, MD, FACEP Committee for Tactical Emergency Casualty Care 1 Game changer.. 2 High Threat Mass Casualty What is the traditional teaching
Update on War Zone Injuries Stan Breuer, OTD, OTR/L, CHT Colonel, United States Army
 Update on War Zone Injuries Stan Breuer, OTD, OTR/L, CHT Colonel, United States Army Disclaimer: The opinions or assertions contained herein are the private view of the author and are not to be construed
Update on War Zone Injuries Stan Breuer, OTD, OTR/L, CHT Colonel, United States Army Disclaimer: The opinions or assertions contained herein are the private view of the author and are not to be construed
Trauma and Injury Subcommittee
 Trauma and Injury Subcommittee Decision Brief: Combat Trauma Lessons Learned from Military Operations of 2001-2013 Col (Ret) Donald Jenkins, MD, FACS, DMCC Defense Health Board November 6, 2014 1 Overview
Trauma and Injury Subcommittee Decision Brief: Combat Trauma Lessons Learned from Military Operations of 2001-2013 Col (Ret) Donald Jenkins, MD, FACS, DMCC Defense Health Board November 6, 2014 1 Overview
Trauma and Injury Subcommittee: Lessons Learned in Theater Trauma Care in Afghanistan & Iraq. Donald Jenkins, MD Norman McSwain, MD
 Trauma and Injury Subcommittee: Lessons Learned in Theater Trauma Care in Afghanistan & Iraq Donald Jenkins, MD Norman McSwain, MD Defense Health Board November 27, 2012 1 Trauma and Injury Subcommittee
Trauma and Injury Subcommittee: Lessons Learned in Theater Trauma Care in Afghanistan & Iraq Donald Jenkins, MD Norman McSwain, MD Defense Health Board November 27, 2012 1 Trauma and Injury Subcommittee
U.S. ARMY MEDICAL SUPPORT
 U.S. ARMY MEDICAL SUPPORT BY SGT FREDERICK, EVELYN CIVIL AFFAIRS TEAM 8041 MEDIC AGENDA HOSPITAL LEVELS OF CARE TRAINING FOR ALL SOLDIERS: SELF AID, Tactical Combat Casualty Care (TCCC) MEDICS: REGULAR,
U.S. ARMY MEDICAL SUPPORT BY SGT FREDERICK, EVELYN CIVIL AFFAIRS TEAM 8041 MEDIC AGENDA HOSPITAL LEVELS OF CARE TRAINING FOR ALL SOLDIERS: SELF AID, Tactical Combat Casualty Care (TCCC) MEDICS: REGULAR,
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 401 Introduction to Tactical Combat Casualty Care TERMINAL LEARNING OBJECTIVE 1. Given a casualty in a tactical
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 401 Introduction to Tactical Combat Casualty Care TERMINAL LEARNING OBJECTIVE 1. Given a casualty in a tactical
EMS Subspecialty Certification Review Course. Learning Objectives. Scope of Practice
 EMS Subspecialty Certification Review Course 2.3.1 Scope of Practice Models 2.3.1.1 Military/federal government medical personnel 2.3.1.2 State vs. national scope of practice model 2.3.1.2.1 Levels of
EMS Subspecialty Certification Review Course 2.3.1 Scope of Practice Models 2.3.1.1 Military/federal government medical personnel 2.3.1.2 State vs. national scope of practice model 2.3.1.2.1 Levels of
Bringing Combat Medicine to the Streets of EMS. MAJ Will Smith MD, EMT-P US Army
 Bringing Combat Medicine to the Streets of EMS MAJ Will Smith MD, EMT-P US Army Disclaimers No financial or other conflicts to disclose This presentation is NOT an official position or endorsement from
Bringing Combat Medicine to the Streets of EMS MAJ Will Smith MD, EMT-P US Army Disclaimers No financial or other conflicts to disclose This presentation is NOT an official position or endorsement from
Department of Defense Trauma Registry
 Appendix Appendix 3 Department of Defense Trauma Registry General Evidence-based medicine allows for identification of best practices and the timely formulation of clinical practice guidelines. Unfortunately,
Appendix Appendix 3 Department of Defense Trauma Registry General Evidence-based medicine allows for identification of best practices and the timely formulation of clinical practice guidelines. Unfortunately,
Tactical & Hunter First Aid Workshop
 Jackson Hole Gun Club Jackson, WY July 15, 2013 Tactical & Hunter First Aid Workshop LTC Will Smith MD, Paramedic www.wildernessdoc.com Disclaimers No financial conflicts to disclose Board of Advisors
Jackson Hole Gun Club Jackson, WY July 15, 2013 Tactical & Hunter First Aid Workshop LTC Will Smith MD, Paramedic www.wildernessdoc.com Disclaimers No financial conflicts to disclose Board of Advisors
Tactical Combat Casualty Care: Top Lessons for Civilian EMS Systems from 14 Years of War
 Tactical Combat Casualty Care: Top Lessons for Civilian EMS Systems from 14 Years of War Dr. Frank Butler 16 May 2016 Disclaimers The opinions or assertions contained herein are the private views of the
Tactical Combat Casualty Care: Top Lessons for Civilian EMS Systems from 14 Years of War Dr. Frank Butler 16 May 2016 Disclaimers The opinions or assertions contained herein are the private views of the
Answering the Call: Combat Casualty Care Research
 Answering the Call: Combat Casualty Care Research Joint Program Committee on Combat Casualty Care Defense Health Agency Professor of Surgery Uniformed Services University Moral Test Moral test of a nation
Answering the Call: Combat Casualty Care Research Joint Program Committee on Combat Casualty Care Defense Health Agency Professor of Surgery Uniformed Services University Moral Test Moral test of a nation
The Evolution of Battlefield Surgery Post Damage Control Surgery
 The Evolution of Battlefield Surgery Post- 9-11 & Damage Control Surgery LTC DUANE DUKE MD FACS Division Chief of Pediatric Surgery USU Walter Reed Surgery 19OCT2016 Disclosure I have no personal or professional
The Evolution of Battlefield Surgery Post- 9-11 & Damage Control Surgery LTC DUANE DUKE MD FACS Division Chief of Pediatric Surgery USU Walter Reed Surgery 19OCT2016 Disclosure I have no personal or professional
D12/E12: Lessons from a Learning System for Trauma Care
 D12/E12: Lessons from a Learning System for Trauma Care Don Berwick, MD, MPP and John Holcomb, MD December 13, 2017 Committee on Military Trauma Care s Learning Health System and Its Translation to the
D12/E12: Lessons from a Learning System for Trauma Care Don Berwick, MD, MPP and John Holcomb, MD December 13, 2017 Committee on Military Trauma Care s Learning Health System and Its Translation to the
D ebakey1 observed that, Had certain problems in World
 SPECIAL REPORT Implementing and preserving the advances in combat casualty care from Iraq and Afghanistan throughout the US Military Frank K. Butler, MD, David J. Smith, MD, and Richard H. Carmona, MD,
SPECIAL REPORT Implementing and preserving the advances in combat casualty care from Iraq and Afghanistan throughout the US Military Frank K. Butler, MD, David J. Smith, MD, and Richard H. Carmona, MD,
Comparison: ITLS Provider and Trauma Nursing Core Course (TNCC)
") Overview International Trauma Life Support (ITLS) is a global organization dedicated to preventing death and disability from trauma through education and emergency care. ITLS educates emergency personnel
Overview International Trauma Life Support (ITLS) is a global organization dedicated to preventing death and disability from trauma through education and emergency care. ITLS educates emergency personnel
STOP THE BLEED. InfoBrief. International Public Safety Association. March 2018
 1 STOP THE BLEED InfoBrief International Public Safety Association March 2018 2 About This International Public Safety Association InfoBrief discusses how and why the Stop the Bleed program was developed
1 STOP THE BLEED InfoBrief International Public Safety Association March 2018 2 About This International Public Safety Association InfoBrief discusses how and why the Stop the Bleed program was developed
TCCC for Medical Personnel Curriculum 1708
 TCCC for Medical Personnel Curriculum 1708 TCCC-MP Guidelines TCCC Guidelines for Medical Personnel 170131 TCCC Quick Reference Guide Link to TCCC Quick Reference Guide PowerPoint Presentations Intro to
TCCC for Medical Personnel Curriculum 1708 TCCC-MP Guidelines TCCC Guidelines for Medical Personnel 170131 TCCC Quick Reference Guide Link to TCCC Quick Reference Guide PowerPoint Presentations Intro to
Joint Theater Trauma System Clinical Practice Guideline
 HYPOTHERMIA PREVENTION, MONITORING, AND MANAGEMENT Original Release/Approval 2 Oct 2006 Note: This CPG requires an annual review. Reviewed: Sep 2012 Approved: 18 Sep 2012 Supersedes: Hypothermia Prevention,
HYPOTHERMIA PREVENTION, MONITORING, AND MANAGEMENT Original Release/Approval 2 Oct 2006 Note: This CPG requires an annual review. Reviewed: Sep 2012 Approved: 18 Sep 2012 Supersedes: Hypothermia Prevention,
Roles of Medical Care (United States)
") Roles of Medical Care (United States) Chapter 2 Roles of Medical Care (United States) Introduction Military doctrine supports an integrated health services support system to triage, treat, evacuate, and
Roles of Medical Care (United States) Chapter 2 Roles of Medical Care (United States) Introduction Military doctrine supports an integrated health services support system to triage, treat, evacuate, and
The military trauma system has evolved and matured very
 ORIGINAL ARTICLE Evaluation of military trauma system practices related to damage-control resuscitation Keith Palm, RN, Amy Apodaca, PhD, Debra Spencer, RN, George Costanzo, MD, Jeffrey Bailey, MD, Lorne
ORIGINAL ARTICLE Evaluation of military trauma system practices related to damage-control resuscitation Keith Palm, RN, Amy Apodaca, PhD, Debra Spencer, RN, George Costanzo, MD, Jeffrey Bailey, MD, Lorne
PHYSICIAN ASSISTANTS IN TACTICAL MEDICINE TRAINING PROGRAMS
 Physician Assistants in Tactical Medicine Training Programs Chapter 21 PHYSICIAN ASSISTANTS IN TACTICAL MEDICINE TRAINING PROGRAMS Felipe Galvan, PA-C, MPAS; Todd P. Kielman, PA-C, MPAS; Robert M. Levesque,
Physician Assistants in Tactical Medicine Training Programs Chapter 21 PHYSICIAN ASSISTANTS IN TACTICAL MEDICINE TRAINING PROGRAMS Felipe Galvan, PA-C, MPAS; Todd P. Kielman, PA-C, MPAS; Robert M. Levesque,
COMBAT Research Study
 COMBAT Research Study Questions & Answers What is the title of this research study? The Control Of Massive Bleeding After Trauma (COMBAT): A prospective, randomized comparison of early fresh frozen plasma
COMBAT Research Study Questions & Answers What is the title of this research study? The Control Of Massive Bleeding After Trauma (COMBAT): A prospective, randomized comparison of early fresh frozen plasma
Study Title: Optimal resuscitation in pediatric trauma an EAST multicenter study
 Study Title: Optimal resuscitation in pediatric trauma an EAST multicenter study PI/senior researcher: Richard Falcone Jr. MD, MPH Co-primary investigator: Stephanie Polites MD, MPH; Juan Gurria MD My
Study Title: Optimal resuscitation in pediatric trauma an EAST multicenter study PI/senior researcher: Richard Falcone Jr. MD, MPH Co-primary investigator: Stephanie Polites MD, MPH; Juan Gurria MD My
Course: Acute Trauma Care Course Number SUR 1905 (1615)
") Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
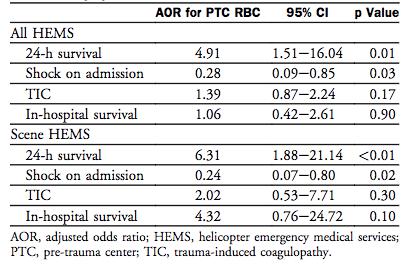
A NATIONAL TRAUMA CARE SYSTEM
 A NATIONAL TRAUMA CARE SYSTEM Integrating Military and Civilian Trauma Care Systems to Achieve Zero Preventable Deaths After Injury Committee on Military Trauma Care s Learning Health System and Its Translation
A NATIONAL TRAUMA CARE SYSTEM Integrating Military and Civilian Trauma Care Systems to Achieve Zero Preventable Deaths After Injury Committee on Military Trauma Care s Learning Health System and Its Translation
UPMC Trauma Care System
 A Western PA Initiative 1 UPMC Trauma Care System Altoona (Level II Adult) Children s Hospital (Level I Pediatric) Hamot (Level II Adult) 2 Mercy (Level I Adult, Burn Center) Presbyterian (Level I Adult)
A Western PA Initiative 1 UPMC Trauma Care System Altoona (Level II Adult) Children s Hospital (Level I Pediatric) Hamot (Level II Adult) 2 Mercy (Level I Adult, Burn Center) Presbyterian (Level I Adult)
ORIGINAL ARTICLE. Eliminating Preventable Death on the Battlefield
 ONLINE FIRST ORIGINAL ARTICLE Eliminating Preventable Death on the Battlefield Russ S. Kotwal, MD, MPH; Harold R. Montgomery, NREMT; Bari M. Kotwal, MS; Howard R. Champion, FRCS; Frank K. Butler Jr, MD;
ONLINE FIRST ORIGINAL ARTICLE Eliminating Preventable Death on the Battlefield Russ S. Kotwal, MD, MPH; Harold R. Montgomery, NREMT; Bari M. Kotwal, MS; Howard R. Champion, FRCS; Frank K. Butler Jr, MD;
DEFENSE HEAL TH BOARD FIVE SKYLINE PLACE, SUITE LEESBURG PIKE FALLS CHURCH, VA
 DEFENSE HEAL TH BOARD FIVE SKYLINE PLACE, SUITE 810 5111 LEESBURG PIKE FALLS CHURCH, VA 22041-3206 JUN 14 2011 FOR: JONATHAN WOODSON, M.D., ASSISTANT SECRETARY OF DEFENSE (HEALTH AFFAIRS) SUBJECT: Tactical
DEFENSE HEAL TH BOARD FIVE SKYLINE PLACE, SUITE 810 5111 LEESBURG PIKE FALLS CHURCH, VA 22041-3206 JUN 14 2011 FOR: JONATHAN WOODSON, M.D., ASSISTANT SECRETARY OF DEFENSE (HEALTH AFFAIRS) SUBJECT: Tactical
Hemorrhage Control by Law Enforcement Personnel: A Survey of Knowledge Translation From the Military Combat Experience
 MILITARY MEDICINE, 180, 6:615, 2015 Hemorrhage Control by Law Enforcement Personnel: A Survey of Knowledge Translation From the Military Combat Experience Sara J. Aberle, MD*; Andrew J. Dennis, DO, FACOS
MILITARY MEDICINE, 180, 6:615, 2015 Hemorrhage Control by Law Enforcement Personnel: A Survey of Knowledge Translation From the Military Combat Experience Sara J. Aberle, MD*; Andrew J. Dennis, DO, FACOS
TCCC Proposed Changes:
 Operationalizing Advanced Resuscitative Care: The experience of the Special Operations Resuscitation Team (SORT) Special Operations Medical Association Scientific Assembly (SOMSA) 16 MAY 2018 COL Jay Baker,
Operationalizing Advanced Resuscitative Care: The experience of the Special Operations Resuscitation Team (SORT) Special Operations Medical Association Scientific Assembly (SOMSA) 16 MAY 2018 COL Jay Baker,
ORIGINAL ARTICLE. Eliminating Preventable Death on the Battlefield
 ONLINE FIRST ORIGINAL ARTICLE Eliminating Preventable Death on the Battlefield Russ S. Kotwal, MD, MPH; Harold R. Montgomery, NREMT; Bari M. Kotwal, MS; Howard R. Champion, FRCS; Frank K. Butler Jr, MD;
ONLINE FIRST ORIGINAL ARTICLE Eliminating Preventable Death on the Battlefield Russ S. Kotwal, MD, MPH; Harold R. Montgomery, NREMT; Bari M. Kotwal, MS; Howard R. Champion, FRCS; Frank K. Butler Jr, MD;
Tactical Combat Casualty Care. CAPT Peter Rhee, MC, USN MD, MPH, DMCC, FACS, FCCM Professor of Surgery / Molecular Cellular Biology
 Tactical Combat Casualty Care CAPT Peter Rhee, MC, USN MD, MPH, DMCC, FACS, FCCM Professor of Surgery / Molecular Cellular Biology Good medicine in bad places Tactical Care 24 man team raid Building
Tactical Combat Casualty Care CAPT Peter Rhee, MC, USN MD, MPH, DMCC, FACS, FCCM Professor of Surgery / Molecular Cellular Biology Good medicine in bad places Tactical Care 24 man team raid Building
Prehospital Blood Product Transfusion by U.S. Army MEDEVAC During Combat Operations in Afghanistan: A Process Improvement Initiative
 MILITARY MEDICINE, 178, 7:785, 2013 Prehospital Blood Product Transfusion by U.S. Army MEDEVAC During Combat Operations in Afghanistan: A Process Improvement Initiative LTC Robert F. Malsby III, MC USA*;
MILITARY MEDICINE, 178, 7:785, 2013 Prehospital Blood Product Transfusion by U.S. Army MEDEVAC During Combat Operations in Afghanistan: A Process Improvement Initiative LTC Robert F. Malsby III, MC USA*;
American College of Surgeons Bleeding Control Legislative Toolkit
 American College of Surgeons Bleeding Control Legislative Toolkit This document is a resource for ACS Chapters, Fellows, and Committee on Trauma (COT) advocates to promote the Stop the Bleed program and
American College of Surgeons Bleeding Control Legislative Toolkit This document is a resource for ACS Chapters, Fellows, and Committee on Trauma (COT) advocates to promote the Stop the Bleed program and
The Journal of TRAUMA Injury, Infection, and Critical Care
 Injury Severity and Causes of Death From Operation Iraqi Freedom and Operation Enduring Freedom: 2003 2004 Versus 2006 Joseph F. Kelly, MD, Amber E. Ritenour, MD, Daniel F. McLaughlin, MD, Karen A. Bagg,
Injury Severity and Causes of Death From Operation Iraqi Freedom and Operation Enduring Freedom: 2003 2004 Versus 2006 Joseph F. Kelly, MD, Amber E. Ritenour, MD, Daniel F. McLaughlin, MD, Karen A. Bagg,
ESCAMBIA COUNTY FIRE-RESCUE
 Patrick T Grace, Fire Chief Page 1 of 7 PURPOSE: To create a standard of operation to which all members of Escambia County Public Safety will operate at the scene of incidents involving a mass shooting
Patrick T Grace, Fire Chief Page 1 of 7 PURPOSE: To create a standard of operation to which all members of Escambia County Public Safety will operate at the scene of incidents involving a mass shooting
DOD INSTRUCTION JOINT TRAUMA SYSTEM (JTS)
") DOD INSTRUCTION 6040.47 JOINT TRAUMA SYSTEM (JTS) Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: September 28, 2016 Releasability: Approved by: Cleared
DOD INSTRUCTION 6040.47 JOINT TRAUMA SYSTEM (JTS) Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: September 28, 2016 Releasability: Approved by: Cleared
MAssive Transfusion In Children (MATIC) Study - Update
 Study - Update") MAssive Transfusion In Children (MATIC) Study - Update Disclosures Consultant US Army Blood Research Program Norwegian Navy Blood Research Program TerumoBCT, Entegrion, Vascular Solutions Octapharma, New
MAssive Transfusion In Children (MATIC) Study - Update Disclosures Consultant US Army Blood Research Program Norwegian Navy Blood Research Program TerumoBCT, Entegrion, Vascular Solutions Octapharma, New
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC CONDUCT TRIAGE
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC 28542-0042 FMSO 107 CONDUCT TRIAGE TERMINAL LEARNING OBJECTIVE (1) Given multiple simulated casualties in a simulated operational
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC 28542-0042 FMSO 107 CONDUCT TRIAGE TERMINAL LEARNING OBJECTIVE (1) Given multiple simulated casualties in a simulated operational
DOD INSTRUCTION MEDICAL READINESS TRAINING (MRT)
") DOD INSTRUCTION 1322.24 MEDICAL READINESS TRAINING (MRT) Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: March 16, 2018 Releasability: Cleared for
DOD INSTRUCTION 1322.24 MEDICAL READINESS TRAINING (MRT) Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: March 16, 2018 Releasability: Cleared for
Defense Health Agency PROCEDURAL INSTRUCTION
 Defense Health Agency PROCEDURAL INSTRUCTION SUBJECT: Implementation Guidance for the Utilization of DD Form 1380, Tactical Combat Casualty Care (TCCC) Card, June 2014 References: See Enclosure 1 NUMBER
Defense Health Agency PROCEDURAL INSTRUCTION SUBJECT: Implementation Guidance for the Utilization of DD Form 1380, Tactical Combat Casualty Care (TCCC) Card, June 2014 References: See Enclosure 1 NUMBER
Dear Chairman Alexander and Ranking Member Murray:
 May 4, 2018 The Honorable Lamar Alexander Chairman Senate Committee on Health, Education, Labor and Pensions United States Senate 428 Dirksen Senate Office Building Washington, DC20510 The Honorable Patty
May 4, 2018 The Honorable Lamar Alexander Chairman Senate Committee on Health, Education, Labor and Pensions United States Senate 428 Dirksen Senate Office Building Washington, DC20510 The Honorable Patty
AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria)
") AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria) Note: In the table below, (E) represents essential while (D) represents desirable criteria. INSTITUTIONAL ORGANIZATION
AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria) Note: In the table below, (E) represents essential while (D) represents desirable criteria. INSTITUTIONAL ORGANIZATION
Sunrise Hospital & Medical Center Response to October 1 Mass Casualty Event. Kimberly Hatchel, DNP, MHA, RN, CENP. #VegasSTRONG
 Sunrise Hospital & Medical Center Response to October 1 Mass Casualty Event Kimberly Hatchel, DNP, MHA, RN, CENP #VegasSTRONG Level II Trauma Center About Sunrise Hospital & Medical Center 692-bed adult
Sunrise Hospital & Medical Center Response to October 1 Mass Casualty Event Kimberly Hatchel, DNP, MHA, RN, CENP #VegasSTRONG Level II Trauma Center About Sunrise Hospital & Medical Center 692-bed adult
Infections Complicating the Care of Combat Casualties during Operations Iraqi Freedom and Enduring Freedom
 2011 Military Health System Conference Infections Complicating the Care of Combat Casualties during Operations Iraqi Freedom and Enduring Freedom The Quadruple Aim: Working Together, Achieving Success
2011 Military Health System Conference Infections Complicating the Care of Combat Casualties during Operations Iraqi Freedom and Enduring Freedom The Quadruple Aim: Working Together, Achieving Success
Trauma Center Pre-Review Questionnaire Notes Title 22
 This Pre-Review Questionnaire is designed to accompany the spread sheet appropriate for the Trauma Center being reviewed For use with review of Level III Trauma Center with American College of Surgeons'
This Pre-Review Questionnaire is designed to accompany the spread sheet appropriate for the Trauma Center being reviewed For use with review of Level III Trauma Center with American College of Surgeons'
Best Medicine, Worst Places: Tactical Medicine in an Urban Environment
 Best Medicine, Worst Places: Tactical Medicine in an Urban Environment Alexander Eastman, MD, MPH, FACS Interim Medical Director The Trauma Center at Parkland UW Medicine EMS & Trauma Conference September
Best Medicine, Worst Places: Tactical Medicine in an Urban Environment Alexander Eastman, MD, MPH, FACS Interim Medical Director The Trauma Center at Parkland UW Medicine EMS & Trauma Conference September
TRAUMA CENTER REQUIREMENTS
 California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
A New Approach to Organization and Implementation of Military Medical Treatment in Response to Military Reform and Modern Warfare in the Chinese Army
 MILITARY MEDICINE, 182, 11/12:e1819, 2017 A New Approach to Organization and Implementation of Military Medical Treatment in Response to Military Reform and Modern Warfare in the Chinese Army Yang Pei,
MILITARY MEDICINE, 182, 11/12:e1819, 2017 A New Approach to Organization and Implementation of Military Medical Treatment in Response to Military Reform and Modern Warfare in the Chinese Army Yang Pei,
NEW TRAUMA CARE SYSTEM. DOD Should Fully Incorporate Leading Practices into Its Planning for Effective Implementation
 United States Government Accountability Office Report to Congressional Committees March 2018 NEW TRAUMA CARE SYSTEM DOD Should Fully Incorporate Leading Practices into Its Planning for Effective Implementation
United States Government Accountability Office Report to Congressional Committees March 2018 NEW TRAUMA CARE SYSTEM DOD Should Fully Incorporate Leading Practices into Its Planning for Effective Implementation
The combat environment in Afghanistan presents unique
 The Journal of TRAUMA Injury, Infection, and Critical Care US Army Two-Surgeon Teams Operating in Remote Afghanistan An Evaluation of Split-Based Forward Surgical Team Operations Shawn C. Nessen, DO, FACS,
The Journal of TRAUMA Injury, Infection, and Critical Care US Army Two-Surgeon Teams Operating in Remote Afghanistan An Evaluation of Split-Based Forward Surgical Team Operations Shawn C. Nessen, DO, FACS,
The following policy was adopted by the San Luis Obispo County EMS Agency and will become effective March 1, 2012 at 0800 hours.
 SLO County Emergency Medical Services Agency Bulletin 2012-02 PLEASE POST New Trauma System Policies and Procedures February 9, 2012 To All SLO County EMS Providers and Training Institutions: The following
SLO County Emergency Medical Services Agency Bulletin 2012-02 PLEASE POST New Trauma System Policies and Procedures February 9, 2012 To All SLO County EMS Providers and Training Institutions: The following
photo ChrisDownie istockphoto.com
 photo ChrisDownie istockphoto.com 48 JEMS DECEMBER 2009 >> By E. Reed Smith, MD; Blake Iselin, FF/EMT-III; & W. Scott McKay Arlington County, Va., Rescue Task Force represents a new medical response model
photo ChrisDownie istockphoto.com 48 JEMS DECEMBER 2009 >> By E. Reed Smith, MD; Blake Iselin, FF/EMT-III; & W. Scott McKay Arlington County, Va., Rescue Task Force represents a new medical response model
History of Trauma Surgery
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-disaster-medicine-and-preparedness/history-of-traumasurgery/1500/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-disaster-medicine-and-preparedness/history-of-traumasurgery/1500/
Bringing Medical Education, Training and Health Care Delivery into the Twenty-first Century
 white paper Bringing Medical Education, Training and Health Care Delivery into the Twenty-first Century By Deborah N. Burgess, M.D., F.A.C.P, Senior Vice President Abstract The aviation industry has been
white paper Bringing Medical Education, Training and Health Care Delivery into the Twenty-first Century By Deborah N. Burgess, M.D., F.A.C.P, Senior Vice President Abstract The aviation industry has been
Chapter 1. Learning Objectives. Learning Objectives 9/11/2012. Introduction to EMS Systems
 Chapter 1 Introduction to EMS Systems Learning Objectives Define the attributes of emergency medical services (EMS) systems List 14 attributes of a functioning EMS system Differentiate the roles and responsibilities
Chapter 1 Introduction to EMS Systems Learning Objectives Define the attributes of emergency medical services (EMS) systems List 14 attributes of a functioning EMS system Differentiate the roles and responsibilities
AAST Senior Visiting Surgeon Program
 AAST Senior Visiting Surgeon Program Landstuhl Medical Center Mary C. McCarthy, MD Professor of Surgery Wright State University School of Medicine 2007 McCarthy Objectives After participating in this activity,
AAST Senior Visiting Surgeon Program Landstuhl Medical Center Mary C. McCarthy, MD Professor of Surgery Wright State University School of Medicine 2007 McCarthy Objectives After participating in this activity,
The Royal College of Surgeons of England
 The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
The U.S. Navy s Forward Resuscitative Surgery System during Operation Iraqi Freedom
 MILITARY MEDICINE, 170, 4:297, 2005 The U.S. Navy s Forward Resuscitative Surgery System during Operation Iraqi Freedom Guarantor: CAPT Rom A. Stevens, MC USNR Contributors: CAPT Harold R. Bohman, MC USN*;
MILITARY MEDICINE, 170, 4:297, 2005 The U.S. Navy s Forward Resuscitative Surgery System during Operation Iraqi Freedom Guarantor: CAPT Rom A. Stevens, MC USNR Contributors: CAPT Harold R. Bohman, MC USN*;
Resuscitative Endovascular Occlusion of the Aorta (REBOA): Challenges of Launching a City Wide Program
: Challenges of Launching a City Wide Program") Resuscitative Endovascular Occlusion of the Aorta (REBOA): Challenges of Launching a City Wide Program Gerald Fortuna, MD Col, USAF, MC, SFS Director, C-STARS St Louis Assistant Professor Sections of Vascular
Resuscitative Endovascular Occlusion of the Aorta (REBOA): Challenges of Launching a City Wide Program Gerald Fortuna, MD Col, USAF, MC, SFS Director, C-STARS St Louis Assistant Professor Sections of Vascular
In an effort to describe periods of profound change in military
 REVIEW ARTICLE Military medical revolution: Prehospital combat casualty care Lorne H. Blackbourne, MD, David G. Baer, PhD, Brian J. Eastridge, MD, Bijan Kheirabadi, PhD, John F. Kragh, Jr., MD, Andrew
REVIEW ARTICLE Military medical revolution: Prehospital combat casualty care Lorne H. Blackbourne, MD, David G. Baer, PhD, Brian J. Eastridge, MD, Bijan Kheirabadi, PhD, John F. Kragh, Jr., MD, Andrew
The 2013 Boston Marathon Bombings
 The 2013 Boston Marathon Bombings Lessons Learned from a Resource-Rich Urban Battlefield Presented at the 41 st Convention of the American Society of Plastic Surgical Nurses Boston, Massachusetts October
The 2013 Boston Marathon Bombings Lessons Learned from a Resource-Rich Urban Battlefield Presented at the 41 st Convention of the American Society of Plastic Surgical Nurses Boston, Massachusetts October
Active Violence and Mass Casualty Terrorist Incidents
 Position Statement Active Violence and Mass Casualty Terrorist Incidents The threat of terrorism, specifically active shooter and complex coordinated attacks, is a concern for the fire and emergency service.
Position Statement Active Violence and Mass Casualty Terrorist Incidents The threat of terrorism, specifically active shooter and complex coordinated attacks, is a concern for the fire and emergency service.
Chapter 1, Part 2 EMS SYSTEMS EMS System A comprehensive network of personnel, equipment, and established to deliver aid and emergency medical care
 1 3 4 5 6 7 8 9 10 11 1 Chapter 1, Part EMS SYSTEMS EMS System A comprehensive network of personnel, equipment, and established to deliver aid and emergency medical care to the community. IN-HOSPITAL COMPONENTS
1 3 4 5 6 7 8 9 10 11 1 Chapter 1, Part EMS SYSTEMS EMS System A comprehensive network of personnel, equipment, and established to deliver aid and emergency medical care to the community. IN-HOSPITAL COMPONENTS
San Diego Operational Area. Policy # 9A Effective Date: 9/1/14 Pages 8. Active Shooter / MCI (AS/MCI) PURPOSE
 PURPOSE") PURPOSE The intent of this Policy is to provide direction for performance of the correct intervention, at the correct time, in order to stabilize and prevent death from readily treatable injuries in the
PURPOSE The intent of this Policy is to provide direction for performance of the correct intervention, at the correct time, in order to stabilize and prevent death from readily treatable injuries in the
among TEMS providers:
 The need for standardization among TEMS providers: Training, credentialing and roles By Scott Warner, MD, EMT Tactical teams which have integrated tactical medics and physicians into their law enforcement
The need for standardization among TEMS providers: Training, credentialing and roles By Scott Warner, MD, EMT Tactical teams which have integrated tactical medics and physicians into their law enforcement
Integration of Tactical Emergency Casualty Care Into the National Tactical Emergency Medical Support Competency Domains
 Integration of Tactical Emergency Casualty Care Into the National Tactical Emergency Medical Support Competency Domains Andre M. Pennardt, MD, FACEP; David W. Callaway, MD, MPA, FACEP; Richard Kamin, MD,
Integration of Tactical Emergency Casualty Care Into the National Tactical Emergency Medical Support Competency Domains Andre M. Pennardt, MD, FACEP; David W. Callaway, MD, MPA, FACEP; Richard Kamin, MD,
THE MEDICAL COMPANY FM (FM ) AUGUST 2002 TACTICS, TECHNIQUES, AND PROCEDURES HEADQUARTERS, DEPARTMENT OF THE ARMY
 AUGUST 2002 TACTICS, TECHNIQUES, AND PROCEDURES HEADQUARTERS, DEPARTMENT OF THE ARMY") (FM 8-10-1) THE MEDICAL COMPANY TACTICS, TECHNIQUES, AND PROCEDURES AUGUST 2002 HEADQUARTERS, DEPARTMENT OF THE ARMY DISTRIBUTION RESTRICTION: Approved for public release; distribution is unlimited. *FM
(FM 8-10-1) THE MEDICAL COMPANY TACTICS, TECHNIQUES, AND PROCEDURES AUGUST 2002 HEADQUARTERS, DEPARTMENT OF THE ARMY DISTRIBUTION RESTRICTION: Approved for public release; distribution is unlimited. *FM
San Joaquin County Emergency Medical Services Agency. Active Threat Plan
 San Joaquin County Emergency Medical Services Agency Active Threat Plan An Integrated Response for Law Enforcement and Multi-Casualty Branch Operations Page 1 of 13 Acknowledgments This plan is based on
San Joaquin County Emergency Medical Services Agency Active Threat Plan An Integrated Response for Law Enforcement and Multi-Casualty Branch Operations Page 1 of 13 Acknowledgments This plan is based on
Police Tactical Teams
 AOHC April 2012 Medical Support of SWAT Teams Fabrice Czarnecki, M.D., M.A., M.P.H., FACOEM I have no disclosures to make. Police Tactical Teams History of SWAT Watts riots 1965 University of Texas tower
AOHC April 2012 Medical Support of SWAT Teams Fabrice Czarnecki, M.D., M.A., M.P.H., FACOEM I have no disclosures to make. Police Tactical Teams History of SWAT Watts riots 1965 University of Texas tower
EMS Medicine Live! Welcome. Seventh EMS Webinar
 EMS Medicine Live! Welcome Seventh EMS Webinar EMS Medicine Live! EML s Mission Community & Academic EMS Physician Education Information Sharing Board Preparation Group involvement See and meet your peers
EMS Medicine Live! Welcome Seventh EMS Webinar EMS Medicine Live! EML s Mission Community & Academic EMS Physician Education Information Sharing Board Preparation Group involvement See and meet your peers
Major Trauma Dashboard Measures. SUPPORT DOCUMENT September 2018 TO BE READ IN CONJUNCTION WITH THE CHILDREN'S MT DASHBOARD
 Major Trauma Dashboard Measures SUPPORT DOCUMENT September 2018 TO BE READ IN CONJUNCTION WITH THE CHILDREN'S MT DASHBOARD Introduction This document addresses key questions relevant to the Children s
Major Trauma Dashboard Measures SUPPORT DOCUMENT September 2018 TO BE READ IN CONJUNCTION WITH THE CHILDREN'S MT DASHBOARD Introduction This document addresses key questions relevant to the Children s
Penn State Milton S. Hershey Medical Center. Division of Trauma, Acute Care & Critical Care Surgery
 Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Summary of the Military Health System Research Symposium (MHSRS) 2018
 2018") Summary of the Military Health System Research Symposium (MHSRS) 2018 Below is an overview of MHSRS and key takeaways from this year s conference in Orlando, Florida on August 19-23 rd. It includes a summary
Summary of the Military Health System Research Symposium (MHSRS) 2018 Below is an overview of MHSRS and key takeaways from this year s conference in Orlando, Florida on August 19-23 rd. It includes a summary
MEMORANDUM FOR MTN PALS PROGRAM DIRECTORS/ADMINISTRATORS. SUBJECT: Hostile Environments Life-Saving Pediatrics (HELP)
") UNIFORMED SERVICES UNIVERSITY OF THE HEALTH SCIENCES 4301 JONES BRIDGE ROAD BETHESDA, MARYLAND 20814-4799 www.usuhs.mil MEMORANDUM FOR MTN PALS PROGRAM DIRECTORS/ADMINISTRATORS SUBJECT: Hostile Environments
UNIFORMED SERVICES UNIVERSITY OF THE HEALTH SCIENCES 4301 JONES BRIDGE ROAD BETHESDA, MARYLAND 20814-4799 www.usuhs.mil MEMORANDUM FOR MTN PALS PROGRAM DIRECTORS/ADMINISTRATORS SUBJECT: Hostile Environments
Pulse Nightclub: Deadliest Mass Shooting In U.S. History William Havron III MD FACS General Surgery Program Director - ORMC
 Pulse Nightclub: Deadliest Mass Shooting In U.S. History William Havron III MD FACS General Surgery Program Director - ORMC Pulse Nightclub Tragedy Pulse Nightclub Tragedy Pulse Nightclub Tragedy Orlando
Pulse Nightclub: Deadliest Mass Shooting In U.S. History William Havron III MD FACS General Surgery Program Director - ORMC Pulse Nightclub Tragedy Pulse Nightclub Tragedy Pulse Nightclub Tragedy Orlando
Title: Massive Transfusion Event Protocol Policy: Clinical Manual/General Clinical
 Title: Massive Transfusion Event Protocol Policy: Manual/General I. POLICY: Massive Transfusion Event (MTE) Protocol: The MTE Protocol is initiated at the request of the anesthesiologist, surgeon or physician
Title: Massive Transfusion Event Protocol Policy: Manual/General I. POLICY: Massive Transfusion Event (MTE) Protocol: The MTE Protocol is initiated at the request of the anesthesiologist, surgeon or physician
Contents. The Event 12/29/2016. The Event The Aftershock The Recovery Lessons Learned Discussion Summary
 #OrlandoUnited: Coordinating the medical response to the Pulse nightclub shooting Christopher Hunter, M.D., Ph.D. Director, Orange County Health Services Department Associate Medical Director, Orange County
#OrlandoUnited: Coordinating the medical response to the Pulse nightclub shooting Christopher Hunter, M.D., Ph.D. Director, Orange County Health Services Department Associate Medical Director, Orange County
Understand the history of school shootings Understand the motivation and similarities regarding school shootings Improve understanding of the
 April, 2015 Understand the history of school shootings Understand the motivation and similarities regarding school shootings Improve understanding of the planning, training, and equipment required to manage
April, 2015 Understand the history of school shootings Understand the motivation and similarities regarding school shootings Improve understanding of the planning, training, and equipment required to manage
UNCLASSIFIED FY 2009 RDT&E,N BUDGET ITEM JUSTIFICATION SHEET DATE: February 2008 Exhibit R-2
 Exhibit R-2 PROGRAM ELEMENT: 0603729N PROGRAM ELEMENT TITLE: WARFIGHTER PROTECTION ADVANCED TECHNOLOGY COST: (Dollars in Thousands) Project Number & Title FY 2007 Actual FY 2008 FY 2009 FY 2010 FY 2011
Exhibit R-2 PROGRAM ELEMENT: 0603729N PROGRAM ELEMENT TITLE: WARFIGHTER PROTECTION ADVANCED TECHNOLOGY COST: (Dollars in Thousands) Project Number & Title FY 2007 Actual FY 2008 FY 2009 FY 2010 FY 2011
Department of Defense INSTRUCTION
 Department of Defense INSTRUCTION NUMBER 6490.3 August 7, 1997 SUBJECT: Implementation and Application of Joint Medical Surveillance for Deployments USD(P&R) References: (a) DoD Directive 6490.2, "Joint
Department of Defense INSTRUCTION NUMBER 6490.3 August 7, 1997 SUBJECT: Implementation and Application of Joint Medical Surveillance for Deployments USD(P&R) References: (a) DoD Directive 6490.2, "Joint
South Central Region EMS & Trauma Care Council Patient Care Procedures
 South Central Region EMS & Trauma Care Council Patient Care s Table of Contents PCP #1 Dispatch PCP #2 Response Times PCP #3 Triage and Transport PCP #4 Inter-Facility Transfer PCP #5 Medical Command at
South Central Region EMS & Trauma Care Council Patient Care s Table of Contents PCP #1 Dispatch PCP #2 Response Times PCP #3 Triage and Transport PCP #4 Inter-Facility Transfer PCP #5 Medical Command at
RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT
 CALIFORNIA TRAUMA REGULATIONS (Title 22) versus ACS RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT 2006 (Green Book) (Level I/II Trauma Centers Only) Requirement TITLE 22 ACS GREEN BOOK Trauma Medical
CALIFORNIA TRAUMA REGULATIONS (Title 22) versus ACS RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT 2006 (Green Book) (Level I/II Trauma Centers Only) Requirement TITLE 22 ACS GREEN BOOK Trauma Medical