What CAH Board Members Need to Know About Rural Health
|
|
|
- Sabina Mosley
- 5 years ago
- Views:
Transcription
1 What CAH Board Members Need to Know About Rural Health ND Flex Program CAH Board Members August 10, 2012 Presented by: Brad Gibbens, Deputy Director and Assistant Professor Seven Seas Hotel Bismarck, ND Established in 1980, at The University of North Dakota (UND) School of Medicine and Health Sciences in Grand Forks, ND One of the country s most experienced state rural health offices UND Center of Excellence in Research, Scholarship, and CreaPve AcPvity Focus on EducaPng and Informing Policy Research and EvaluaPon Working with CommuniPes American Indians Health Workforce Hospitals and FaciliPes ruralhealth.und.edu 1

2 What is Rural Health? Philosophy: rural people have the same right to expect healthy lives and access to care as do urban people fairness frame Access essential services locally or regionally Access to specialty services through network arrangements Quality of care on par with urban Availability of technology Rural health is very community oriented interdependence frame Integral part of what a community is and how people see themselves More cooperation and collaboration between area providers and systems to increase access and better outcomes for the patient Community Sectors: Economic/business, public/government, education, faith/ church, and health/human services, housing Direct services provided to the public and secondary impact for other sectors Health care is a major employer Community Engagement and Development stronger connections with community 2

3 So Why Is Community Important to Rural Health? Rural culture more interdependence, connectedness, cohesiveness, collaborative, and people identify with institutions and each other Relationships things get done because of people, and sometimes don t get done because of people are the right people at the table? Rural health contributes to the community provision of health services (access), improvement of health, economic contributions, community development, health facilities are a sense of community identity Communities contribute to the rural health system employees, purchase of health services, financing, fund raising, volunteers, ideas and vision 3
4 What are Some Important Rural Health Issues? Access to and availability of care Financial concerns facing rural hospitals and health systems Health workforce Quality of Care Health Information Technology Networks rural hospitals, urban hospitals, clinics, others Emergency Medical Services EMS, ambulance, quick response units Community and Economic Development Health System Reform Sources: 2008 Flex Rural Health Plan, 2009 Environmental Scan, and community presentation feedback surveys Access to and availability of care 4
5 CAHs and Rural Health Issues Overall, CAH administrators in 2011 found issues associated with finance (reimbursement and factors that impact finance including the ability of paoents to pay for services) and health professional workforce were the two most pressing rural health issues Highest rated issue in all 3 surveys was hospital reimbursement from non- Medicare 3 rd Party Payers o About 95% in all 3 years (only issue to do this) Problem, Moderate Problem, and Severe problem Medicare is a concern but not to the same degree mid to high 80% (88% in 2011) ImpacOng the financial picture insurance o Impact of the uninsured 91% o Impact of the underinsured 91% o Increased from about 80% in 2008 Workforce o Physician workforce supply - 91%, increased from 2008 and 2005 o Nursing workforce supply 85%, down slightly from 2008 and up from 2005 o Ancillary workforce supply (lab, X- ray, PT, OT, RT) 73% and down from 2008 and
6 Figure 2. Rural Hospital Issues Comparison of CAH Administrator Surveys 2011, 2008, 2005 Issue Hospital Reimbursement (non-medicare 3rd Party Payer) Health Care Reform Readiness Physician Workforce Supply Impact of Uninsured Impact of Underinsured Hospital Reimbursement - Medicare Nursing Workforce Supply Physical Plant Building Issues Access to Mental Health Services Ancillary Workforce Supply (lab, x-ray, PT, etc.) 2011* * 94% 96% 95% 94% Not Asked Not Asked 91% 82% 72% 91% 79% 96% 91% 75% 95% 88% 86% 84% 85% 89% 81% 79% 64% 88% 79% 79% 73% 73% 86% 88% *Totals represent the combination of problem, moderate problem, and severe problem Financial concerns facing rural hospitals and health systems 6
7 Financial CondiOons ND CAHs higher financial constraints in comparison to naoonal data o ND CAH OperaOng Margins (2009) Ø NaOonal CAH OperaOng Margins Ø MN +3.57, SD +1.72, MT Ø NaOonally about 52% of CAHS have negaove operaong margins; in ND 63% o ND CAH Total Margins (2009) Ø NaOonal CAH Total Margins Ø MN +2.93, SD +1.61, and MT Ø In every year since 2004, ND CAHs averaged negaove total margins but naoonally, posiove Ø NaOonally about 40% of CAHs have negaove total margins; in ND 53% o Some improvement in ND over last year for both total and operaong margins o Cash on hand naoonally (about 66 days); ND (about 37 days) recommended is 60 days Financial CondiOons Local Community Support is CriOcal o 13 CAHs (2011) had local tax support 10 CAHs (2008), 4 CAHs (2005) o A few thousand dollars to 3 CAHs receiving $100,000/year and 2 CAHs $200,000 o 26 CAHs (2011) had a hospital foundaoon 18 (2005) CommuniOes are willing to support their local hospital with their money willing to tax themselves and target donated funds Message conveyed to congressional delegaoon need some level of federal funding for rural health but communioes also willing to support their health systems 7
8 Health Workforce North Dakota Health Workforce o Issues Ø Supply are we producing enough? But the first quesoon is, what is our need? Ø Demand where is the demand located? What types of disciplines? How will demand change over the years? Ø Mal- distribuoon maybe enough but again, where are they going? Ø SoluOons what do we do? And, who is we? 8
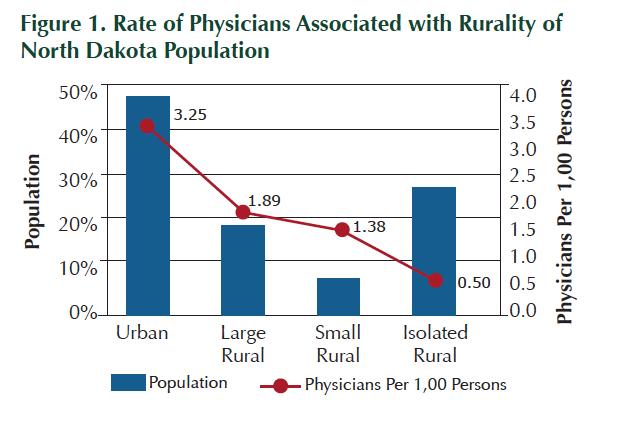
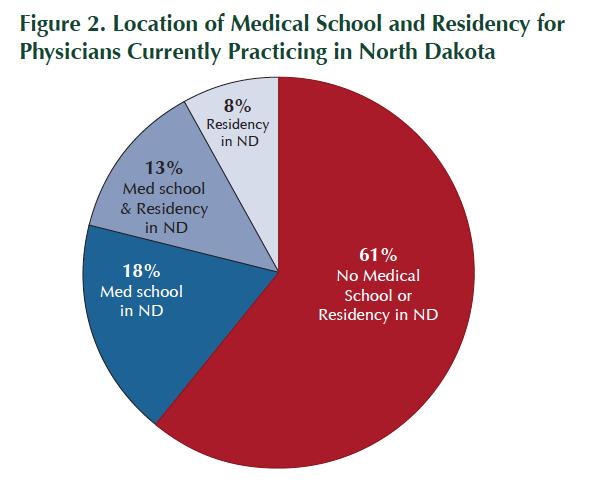
9 9
10 Health Workforce What Can We Do? SoluOons o ACA (naoonal level) has 18 direct focal areas on health workforce NHSC, AHEC, residency training changes, Accountable Care Orgs to rely on PC, etc. o AHEC naoonal funds with state level matching funds o CRH Workforce Development Program state supported to UNDSMHS Ø Workforce specialist R/R assistance, residency fairs, sourcing candidates, work with your recruiter/recruitment firm Ø R COOL- Health Scrub Camps and Scrub Academy o o o o o Ø Workforce research, data analysis, projecoons, and planning GOOD Grow our own Doctors state supported to UNDSMHS Ø Increase number of residency slots, medical students, and health sciences, MPH, Geriatrics Rural Medicine Program state supported tuioon waivers to UNDSMHS ROME rural medical training at 6 sites (3 rd yr med. students) Inter- professional Training UND 1 of only 30 MS out of 126 with this focus Community Level Ø R/R commijees Ø Community Awareness and Involvement Economic Development Ø Networks hospitals working with other hospitals and systems collaboraovely Ø Workforce specialist Quality of Care 10

11 The report finds that several states in the Upper Midwest Iowa, Minnesota, Nebraska, North Dakota, and South Dakota were all providing high quality care at lower cost. Their examples suggest that be3er coordinated care and more efficient use of resources could improve the quality of care people receive while keeping cost in check. Source: Commonwealth Fund Commission on a High Performance Health System's second state scorecard report, October
12 Commonwealth Fund (2009 data, most recent, updated this document July 11, 2012) 9 th overall ranking in health system performance (13 th in previous report) 4 th avoidable hospital use and costs (9 th in previous report) 10 th healthy lives 14 th prevenoon and treatment 13 th equity 10 th for children health system performance (access and affordability ranked 16 th, prevenoon and treatment 23 rd, potenoal to lead healthy lives 11 th, and equity 17 th Source: hcp:// and- Data/State- Data- Center/State- Scorecard/DataByState/State.aspx?state=ND Health InformaOon Technology (HIT) 12
 Hired ND HIT Director - Sheldon Wolf Establish state HIT Office (within ND ND Information Technology Dept.")
13 North Dakota HIT Efforts 2006 First State HIT Summit held ND HIT Steering Committee created 2009-Senate Bill 2332 Established, Governor appointed, Health Information Technology Advisory Committee(HITAC) Hired ND HIT Director - Sheldon Wolf Establish state HIT Office (within ND ND Information Technology Dept.) Established HIT ($5M) Loan Program $8 million for required federal match and operating the HIE State received $5.4 M (five years) federal funds to plan and implement a state Health Information Exchange 2011 State funding to expand HIT Office by 3 FTE Renew ($5 million) State Loan Program Continue ($8 million) for required federal match and operating the HIE 2012 HITAC continues work to implement state Health Information Exchange Electronic Health Record Adoption Significant Changes in North Dakota (2008 to 2012) Adoption and Use of Electronic Health Record(EHR) 20 hospitals have gone live with a certified EHR 17 hospitals have gone live with EHR between 2008 and anticipate they will go live within the next year. Drivers most significant to EHR implementation different from 2008 Medicare/Medicaid incentives and availability of state loan funds Barriers to EHR implementation identified in difficulty in justifying expense or return on investment, development of a sustainable business model and difficulty changing workflow patterns. Infrastructure, Hardware, Software Increase in the number of computers in the rural and urban hospitals with access to the internet. Overall access to high-speed/broadband internet remains high Increase of rural hospital respondents, by 20%, that indicated wireless internet is in place Number of facilities sharing data servers with another rural or tertiary increased. Workforce Decrease in number of rural facilities with no FTE designated to oversee the IT (13 in 2008) by nearly half (7) in Increase in number of facilities that have adequate IT staff 13
14 Networks CAHs and Networks CAHs work within network arrangements to bejer address common issues Use networks to gain greater efficiency and effecoveness, provide cost savings, build capacity, and achieve a higher level of organizaoonal performance CAH survey found that the areas that ND CAHs network around tend to correspond with the areas they expressed concern cost factors, greater efficiency, sharing services, and staff CAHs are responding to key federal health policy focus through networks 14
 and HIT (37 CAHs).")
 How Flex could assist: o Building and facilitaong collaboraoon o Addressing staffing, educaoon, and specialty care o SupporOng technology o Emphasizing")
15 CAHs and Networks CAHs belong to mulople networks 36 CAHs work with 9 hospital networks total of 65 CAH arrangements Network with: Altru, CHI, EssenOa, MedCenter One, Northland Healthcare Alliance, North Region Health Alliance, Sanford, St. Alexius, and Trinity 2 most common funcoons that CAHs address through networks are quality improvement (38 CAH arrangements) and HIT (37 CAHs). Average size of a CAH- based network is 7 CAHs (St. Alexius 11 CAHs, and smallest is EssenOa 1 CAH) How Flex could assist: o Building and facilitaong collaboraoon o Addressing staffing, educaoon, and specialty care o SupporOng technology o Emphasizing quality issues as they relate to credenoaling and peer review o SupporOng primary care o Addressing EMS transport and educaoon CAH/Tertiary Networks Assessment of Characteristics 15
16 Community and Economic Development Community and Economic Development Community PerspecOves on ND Issues Rural Health Issues o Financial issues facing rural hospitals 4.17 o Health system reform 4.12 o Health workforce (physician, nurse, and other health professionals) 4.00 o Access and availability of care (Keeping hospitals and clinics open) 3.96 o EMS 3.90 o Community and economic development 3.85 o Quality of care 3.55 o HIT 3.39 o Networks 3.36 Likert Scale of 1-5 with 1 = no concern and 5 = severe concern Surveys at 7 events 16
17 Community and Economic Development Community PerspecOves on ND Issues Community Factors o Retaining and/or recruipng youth 4.11 o Community growth 3.87 o Local populapon 3.75 o Local economics 3.71 o Available/affordable housing 3.53 o Community leadership 3.50 o Maintaining quality school system 3.47 o Confidence for the town 3.38 o Responsive local government 3.36 o TransportaPon services 3.27 o AcPve faith community 3.12 Likert Scale of 1-5 with 1 = no concern and 5 = severe concern Surveys at 7 events What is the Relationship Between Rural Health and Economic Development? Employment 10 percent of direct employment and 5 percent indirect (15%) Rural hospital first or second largest employer 36 CAHs payroll impact Ø About $215 million impact on rural ND economy Ø About $4-10 million for each CAH, (direct and indirect) CAH average about 220 jobs (about 150 direct and 75 indirect) Statewide CAH s contribute about 8,000 jobs to the rural economy About 40% of CAHs have local tax support and 75% have hospital foundation community support One rural physician can have an impact of $1-1.5 million in a year and generate over 20 additional jobs Statewide 8 of top 10 private employers are health related Statewide health care is 8.5%-9% of GSP ND ranks 6 th for percentage of workers in health care jobs Health jobs rank 2 nd only to business jobs for growth in ND ( ) 17
18 Health System Reform Contact us for more information! Brad Gibbens North Columbia Road, Stop 9037 Grand Forks, North Dakota ruralhealth.und.edu 18
Rural Health: Issues and Solutions for Rural Communities
 Rural Health: Issues and Solutions for Rural Communities Common and Chronic Health Care Management 589 Advanced Nursing Education University of Mary March 26, 2018 Bismarck, ND GoTo Webinar Presented by:
Rural Health: Issues and Solutions for Rural Communities Common and Chronic Health Care Management 589 Advanced Nursing Education University of Mary March 26, 2018 Bismarck, ND GoTo Webinar Presented by:
Rural Health Policy: Issues, Process, and Impact
 Rural Health Policy: Issues, Process, and Impact Social Policy 442 UND Department of Social Work November 6, 2013 Presented by Brad Gibbens, MPA Deputy Director and Assistant Professor Established in 1980,
Rural Health Policy: Issues, Process, and Impact Social Policy 442 UND Department of Social Work November 6, 2013 Presented by Brad Gibbens, MPA Deputy Director and Assistant Professor Established in 1980,
The Opportunity of Rural Health: Challenges and Options for Change
 The Opportunity of Rural Health: Challenges and Options for Change North Dakota Healthcare Financial Management Association (HFMA) November 13, 2014 Minot, ND Presented by: Brad Gibbens, Deputy Director
The Opportunity of Rural Health: Challenges and Options for Change North Dakota Healthcare Financial Management Association (HFMA) November 13, 2014 Minot, ND Presented by: Brad Gibbens, Deputy Director
A Changing Health Care Picture in North Dakota But Community is Still Key
 A Changing Health Care Picture in North Dakota But Community is Still Key Ashley Medical Center Annual Meeting October 18, 2016 Presented by Brad Gibbens, Deputy Director and Assistant Professor Ashley,
A Changing Health Care Picture in North Dakota But Community is Still Key Ashley Medical Center Annual Meeting October 18, 2016 Presented by Brad Gibbens, Deputy Director and Assistant Professor Ashley,
R C H Center for Rural Health
 The Power Potential of Economic Development and dealth lthcare Presented to: Economic Development Association of North Dakota Summer Conference Carrington, ND June 17, 2008 Brad Gibbens, Associate Director
The Power Potential of Economic Development and dealth lthcare Presented to: Economic Development Association of North Dakota Summer Conference Carrington, ND June 17, 2008 Brad Gibbens, Associate Director
Background for Congressman Kevin Cramer s Health Care Reform Roundtable February 22, 2017 Consideration of Rural Health in Health Care Reform
 Background for Congressman Kevin Cramer s Health Care Reform Roundtable February 22, 2017 Consideration of Rural Health in Health Care Reform In rural health, health reform really means maintaining and
Background for Congressman Kevin Cramer s Health Care Reform Roundtable February 22, 2017 Consideration of Rural Health in Health Care Reform In rural health, health reform really means maintaining and
THE CENTER FOR RURAL HEALTH
 P a g e 1 THE CENTER FOR RURAL HEALTH The Center for Rural Health (CRH), established in 198, is one of the nation s most experienced organizations committed to providing leadership in rural health. Their
P a g e 1 THE CENTER FOR RURAL HEALTH The Center for Rural Health (CRH), established in 198, is one of the nation s most experienced organizations committed to providing leadership in rural health. Their
Factors Impacting the Rural Health Delivery System Presented to: OT511 Service Delivery System
 Factors Impacting the Rural Health Delivery System Presented to: OT511 Service Delivery System October 30, 2006 Brad Gibbens Associate Director for Community Development and Policy Center for Rural Health
Factors Impacting the Rural Health Delivery System Presented to: OT511 Service Delivery System October 30, 2006 Brad Gibbens Associate Director for Community Development and Policy Center for Rural Health
Detailed Charts From The North Dakota Hospital Survey Results:
 1/28/1 Detailed Charts From The North Dakota Hospital Survey Results: Workforce Gary Hart, PhD Shawnda Schroeder, PhD September 214 Center for Health School of Medicine and Health Sciences University of
1/28/1 Detailed Charts From The North Dakota Hospital Survey Results: Workforce Gary Hart, PhD Shawnda Schroeder, PhD September 214 Center for Health School of Medicine and Health Sciences University of
UNIVERSITY OF NORTH DAKOTA School of Medicine and Health Sciences Center for Rural Health. NORTH DAKOTA Hospital Association
 UNIVERSITY OF NORTH DAKOTA School of Medicine and Health Sciences Center for Rural Health NORTH DAKOTA Hospital Association NORTH DAKOTA Healthcare Review, Inc. NORTH DAKOTA EMS Association REQUEST FOR
UNIVERSITY OF NORTH DAKOTA School of Medicine and Health Sciences Center for Rural Health NORTH DAKOTA Hospital Association NORTH DAKOTA Healthcare Review, Inc. NORTH DAKOTA EMS Association REQUEST FOR
Center for Rural Health
 Rural Economic Development Believes in Wellness Too Lynette Dickson, MS, LRD Project Director Brad Gibbens, MPA Associate Director Joyce Rice, Project Coordinator Center for Rural Health Established in
Rural Economic Development Believes in Wellness Too Lynette Dickson, MS, LRD Project Director Brad Gibbens, MPA Associate Director Joyce Rice, Project Coordinator Center for Rural Health Established in
Critical Access Hospital and Medicare Rural Hospital Flexibility Program Pre-Conference Workshop. Tuesday, February 18, 2003
 Critical Access Hospital and Medicare Rural Hospital Flexibility Program Pre-Conference Workshop Tuesday, February 18, 2003 Brad Gibbens, MPA, Associate Director bgibbens@medicine.nodak.edu Website: http://medicine.nodak.edu/crh
Critical Access Hospital and Medicare Rural Hospital Flexibility Program Pre-Conference Workshop Tuesday, February 18, 2003 Brad Gibbens, MPA, Associate Director bgibbens@medicine.nodak.edu Website: http://medicine.nodak.edu/crh
A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012
 A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012 Introduction The Computer-Based Record Institute (CPRI) established the
A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012 Introduction The Computer-Based Record Institute (CPRI) established the
American Recovery and Reinvestment Act What s in it for MN Rural Health?
 American Recovery and Reinvestment Act What s in it for MN Rural Health? Rural Health Advisory Committee May 19, 2009 Karen Welle, Asst Director, Office of Rural Health and Primary Care Liz Carpenter,
American Recovery and Reinvestment Act What s in it for MN Rural Health? Rural Health Advisory Committee May 19, 2009 Karen Welle, Asst Director, Office of Rural Health and Primary Care Liz Carpenter,
Strategic Planning. McKenzie County Healthcare Systems, Inc.
 Strategic Planning McKenzie County Healthcare Systems, Inc. Facilitated by Ken Hall, JD Center for Rural Health The University of North Dakota School of Medicine and Health Sciences Funded by The Department
Strategic Planning McKenzie County Healthcare Systems, Inc. Facilitated by Ken Hall, JD Center for Rural Health The University of North Dakota School of Medicine and Health Sciences Funded by The Department
Rural Health A National Prospective. Alan Morgan Chief Executive Officer National Rural Health Association
 Minnesota Rural Health Conference Rural Health A National Prospective Alan Morgan Chief Executive Officer National Rural Health Association NRHA Mission The National Rural Health Association is a national
Minnesota Rural Health Conference Rural Health A National Prospective Alan Morgan Chief Executive Officer National Rural Health Association NRHA Mission The National Rural Health Association is a national
ARRA HITECH Act and Nevada
 ARRA HITECH Act and Nevada Senate Committee on Health & Human Services Nevada Legislature February 17, 2011 Lynn O Mara, MBA State HIT Coordinator Department of Health and Human Services 775.684.7593 lgomara@dhhs.nv.gov
ARRA HITECH Act and Nevada Senate Committee on Health & Human Services Nevada Legislature February 17, 2011 Lynn O Mara, MBA State HIT Coordinator Department of Health and Human Services 775.684.7593 lgomara@dhhs.nv.gov
Case Study. rhrc.umn.edu. November 2013
 Case Study November 2013 Case Studies of Regional Extension Centers Serving Rural Practices: Minnesota & North Dakota Michelle Casey, MS; Ira Moscovice, PhD; and Alex McEllistrem-Evenson, MA In 2010 and
Case Study November 2013 Case Studies of Regional Extension Centers Serving Rural Practices: Minnesota & North Dakota Michelle Casey, MS; Ira Moscovice, PhD; and Alex McEllistrem-Evenson, MA In 2010 and
North Dakota Critical Access Hospital Quality Network Evaluation Executive Summary
 North Dakota Critical Access Hospital Quality Network Evaluation Executive Summary December 2010 Evaluation author: Brad Gibbens, MPA Contributors: Marlene Miller, MSW, LCSW; Jody Ward, RN, BSN; Kristine
North Dakota Critical Access Hospital Quality Network Evaluation Executive Summary December 2010 Evaluation author: Brad Gibbens, MPA Contributors: Marlene Miller, MSW, LCSW; Jody Ward, RN, BSN; Kristine
SMALL HOSPITAL IMPROVEMENT PROGRAM GRANT REPORT
 SMALL HOSPITAL IMPROVEMENT PROGRAM GRANT REPORT Funding period: September 1, 2006-August 31, 2007 Fund number: H3HRH00035-05-02 Facility: Center for Rural Health, University of North Dakota, School of
SMALL HOSPITAL IMPROVEMENT PROGRAM GRANT REPORT Funding period: September 1, 2006-August 31, 2007 Fund number: H3HRH00035-05-02 Facility: Center for Rural Health, University of North Dakota, School of
Health Services for Special Populations: Rural and Community Issues (and Health Reform)
") Health Services for Special Populations: Rural and Community Issues (and Health Reform) MPH 510 Health Care Systems October 15, 2018 UND School of Medicine and Health Sciences Grand Forks, ND Presented
Health Services for Special Populations: Rural and Community Issues (and Health Reform) MPH 510 Health Care Systems October 15, 2018 UND School of Medicine and Health Sciences Grand Forks, ND Presented
SNC BRIEF. Safety Net Clinics of Greater Kansas City EXECUTIVE SUMMARY CHALLENGES FACING SAFETY NET PROVIDERS TOP ISSUES:
 EXECUTIVE SUMMARY The Safety Net is a collection of health care providers and institutes that serve the uninsured and underinsured. Safety Net providers come in a variety of forms, including free health
EXECUTIVE SUMMARY The Safety Net is a collection of health care providers and institutes that serve the uninsured and underinsured. Safety Net providers come in a variety of forms, including free health
McKenzie County Healthcare Systems, Inc.
 Implementation Planning Report McKenzie County Healthcare Systems, Inc. Facilitated by Tim Cox, Tiffany Krinke & Nikhil Kalothia Northland Healthcare Alliance Funded by Northland Healthcare Alliance and
Implementation Planning Report McKenzie County Healthcare Systems, Inc. Facilitated by Tim Cox, Tiffany Krinke & Nikhil Kalothia Northland Healthcare Alliance Funded by Northland Healthcare Alliance and
Rural Health Disparities 5/22/2012. Rural is often defined by what it is not urban. May 3, The Rural Health Landscape
 5/22/2012 May 3, 2012 The Rural Health Landscape Alan Morgan Chief Executive Officer National Rural Health Association National Rural Health Association Membership 2012 NRHA Mission The National Rural
5/22/2012 May 3, 2012 The Rural Health Landscape Alan Morgan Chief Executive Officer National Rural Health Association National Rural Health Association Membership 2012 NRHA Mission The National Rural
Rural Health Grant Opportunities: I Have an Idea But Where s the Money? Wednesday, February 19, 2003
 Rural Health Grant Opportunities: I Have an Idea But Where s the Money? Wednesday, February 19, 2003 Brad Gibbens, MPA, Associate Director bgibbens@medicine.nodak.edu http://medicine.nodak.edu/crh Where:
Rural Health Grant Opportunities: I Have an Idea But Where s the Money? Wednesday, February 19, 2003 Brad Gibbens, MPA, Associate Director bgibbens@medicine.nodak.edu http://medicine.nodak.edu/crh Where:
11/10/2015. Workforce Shortages and Maldistribution. Health Care Workforce Shortages/Maldistribution: Why? Access to Health Care Services
 Workforce Shortages and Maldistribution DEVELOPING NEW STATE LEGISLATIVE HEALTH LEADERS Access to Health Care Services Health Professional Shortage Areas (HPSAs) are geographic areas, or populations within
Workforce Shortages and Maldistribution DEVELOPING NEW STATE LEGISLATIVE HEALTH LEADERS Access to Health Care Services Health Professional Shortage Areas (HPSAs) are geographic areas, or populations within
Recruitment & Financial Benefits of Health Professional Shortage Areas
 Recruitment & Financial Benefits of Health Professional Shortage Areas Bobbi Buckner Bentz, MHA, MPH Primary Care Office Director Iowa Department of Public Health Presentation Goals What is a Health Professional
Recruitment & Financial Benefits of Health Professional Shortage Areas Bobbi Buckner Bentz, MHA, MPH Primary Care Office Director Iowa Department of Public Health Presentation Goals What is a Health Professional
Improving Health in a Climate of Change NACo San Diego, California January 31, 2014
 Improving Health in a Climate of Change NACo San Diego, California January 31, 2014 A. Clinton MacKinney, MD, MS Deputy Director and Assistant Professor University of Iowa College of Public Health 2 Price
Improving Health in a Climate of Change NACo San Diego, California January 31, 2014 A. Clinton MacKinney, MD, MS Deputy Director and Assistant Professor University of Iowa College of Public Health 2 Price
Commission on a High Performance Health System. North Dakota Site Visit - July 18, 2007
 . Commission on a High Performance Health System North Dakota Site Visit - July 18, 2007 Mary Wakefield, Ph.D., R.N. Associate Dean for Rural Health and Director, Center for Rural Health C H R Focus On:
. Commission on a High Performance Health System North Dakota Site Visit - July 18, 2007 Mary Wakefield, Ph.D., R.N. Associate Dean for Rural Health and Director, Center for Rural Health C H R Focus On:
Working Paper Series
 The Financial Benefits of Critical Access Hospital Conversion for FY 1999 and FY 2000 Converters Working Paper Series Jeffrey Stensland, Ph.D. Project HOPE (and currently MedPAC) Gestur Davidson, Ph.D.
The Financial Benefits of Critical Access Hospital Conversion for FY 1999 and FY 2000 Converters Working Paper Series Jeffrey Stensland, Ph.D. Project HOPE (and currently MedPAC) Gestur Davidson, Ph.D.
Illinois Governor s Office of Health Innovation and Transformation
 1 Illinois Governor s Office of Health Innovation and Transformation Medicaid Managed Care Conference October 21, 2014 Michael Gelder, Senior Health Policy Advisor to Governor Pat Quinn Executive Director,
1 Illinois Governor s Office of Health Innovation and Transformation Medicaid Managed Care Conference October 21, 2014 Michael Gelder, Senior Health Policy Advisor to Governor Pat Quinn Executive Director,
NOW, THEREFORE, be it resolved that DHS and HEALTH agree to perform the following in connection with this agreement: Purpose
 COOPERATIVE AGREEMENT between NORTH DAKOTA DEPARTMENT OF HUMAN SERVICES and NORTH DAKOTA DEPARTMENT OF HEALTH and PRIMARY CARE OFFICE/PRIMARY CARE ASSOCIATION This agreement has been made and entered into
COOPERATIVE AGREEMENT between NORTH DAKOTA DEPARTMENT OF HUMAN SERVICES and NORTH DAKOTA DEPARTMENT OF HEALTH and PRIMARY CARE OFFICE/PRIMARY CARE ASSOCIATION This agreement has been made and entered into
HRSA Administrator Describes Role of Family Physicians, PCMH in Health Care System
 Return to Previous Page HRSA Administrator Describes Role of Family Physicians, PCMH in Health Care System By James Arvantes Posted: 10/20/2010, 4:45 p.m. -- The Health Resources and Services Administration,
Return to Previous Page HRSA Administrator Describes Role of Family Physicians, PCMH in Health Care System By James Arvantes Posted: 10/20/2010, 4:45 p.m. -- The Health Resources and Services Administration,
8 / 1 9 / 2. Factors Supporting Critical Access Hospital Turnaround. Muskie School of Public Service
 Factors Supporting Critical Access Hospital Turnaround NOSORH Region C Grantee Meeting Omaha, NE August, Maine Rural Health Research Center Flex Monitoring Team Contact Information John A. Gale Maine Rural
Factors Supporting Critical Access Hospital Turnaround NOSORH Region C Grantee Meeting Omaha, NE August, Maine Rural Health Research Center Flex Monitoring Team Contact Information John A. Gale Maine Rural
Flex Program Overview CAH Administrators. via BTWAN: January 31, :30pm
 Flex Program Overview CAH Administrators via BTWAN: January 31, 2008 2-3:30pm Flex Steering Committee Flex Overview The Medicare Rural Hospital Flexibility Program (Flex Program) was authorized by the
Flex Program Overview CAH Administrators via BTWAN: January 31, 2008 2-3:30pm Flex Steering Committee Flex Overview The Medicare Rural Hospital Flexibility Program (Flex Program) was authorized by the
Health Center Strong:
 Health Center Strong: Developing and Expressing Health Center Value Jonathan Chapman Director, CHC Advisory Services, Capital Link NHCHC National Conference and Policy Symposium May 18, 2018 1 Capital
Health Center Strong: Developing and Expressing Health Center Value Jonathan Chapman Director, CHC Advisory Services, Capital Link NHCHC National Conference and Policy Symposium May 18, 2018 1 Capital
Spring User Conference May Sandestin, FL Detailed Agenda
 Day One: Monday May 16, 2016 3 6 p.m. Conference Registration 5 6 p.m. Customer Welcome and Orientation for First-time Conference Attendees 6 8 p.m. Welcome Reception Day Two: Tuesday May 17, 2016 7 a.m.
Day One: Monday May 16, 2016 3 6 p.m. Conference Registration 5 6 p.m. Customer Welcome and Orientation for First-time Conference Attendees 6 8 p.m. Welcome Reception Day Two: Tuesday May 17, 2016 7 a.m.
Creating Quality Improvement and Incentive Platforms in the Safety Net 2009 Pay for Performance Summit
 Creating Quality Improvement and Incentive Platforms in the Safety Net 2009 Pay for Performance Summit Presented by: Julie Murchinson, Manatt Health Solutions Jonah Frohlich, California HealthCare Foundation
Creating Quality Improvement and Incentive Platforms in the Safety Net 2009 Pay for Performance Summit Presented by: Julie Murchinson, Manatt Health Solutions Jonah Frohlich, California HealthCare Foundation
Making a Difference: Maintaining Access to Quality Healthcare for Rural North Dakotans
 Making a Difference: Maintaining Access to Quality Healthcare for ural North Dakotans Medicare ural Hospital Flexibility Program (Flex) North Dakota Healthcare eview, Inc. North Dakota Communities - Bowman,
Making a Difference: Maintaining Access to Quality Healthcare for ural North Dakotans Medicare ural Hospital Flexibility Program (Flex) North Dakota Healthcare eview, Inc. North Dakota Communities - Bowman,
Minnesota Accountable Health Model Practice Transformation Grant Program
 Amendment to the Request for Proposals Minnesota Accountable Health Model Practice Transformation Grant Program Posted October 20, 2014 Amended November 5, 2014 As of October 23, 2014, the following changes
Amendment to the Request for Proposals Minnesota Accountable Health Model Practice Transformation Grant Program Posted October 20, 2014 Amended November 5, 2014 As of October 23, 2014, the following changes
CAH/FQHC Collaboration
 1 2017 FLEX PROGRAM REVERSE SITE VISIT BETHESDA, MD CAH/FQHC Collaboration A Community s Success Story Coal Country Community Health Center Sakakawea Medical Center 2 Presentation Agenda & Objectives Rural
1 2017 FLEX PROGRAM REVERSE SITE VISIT BETHESDA, MD CAH/FQHC Collaboration A Community s Success Story Coal Country Community Health Center Sakakawea Medical Center 2 Presentation Agenda & Objectives Rural
American Recovery and Reinvestment Act of 2009 Overview
 American Recovery and Reinvestment Act of 2009 Overview Thursday, April 29 th Internet2 Healthcare Conference Crystal City, Virginia Neal Neuberger, Executive Director The Mood in Washington, D.C. - 2009
American Recovery and Reinvestment Act of 2009 Overview Thursday, April 29 th Internet2 Healthcare Conference Crystal City, Virginia Neal Neuberger, Executive Director The Mood in Washington, D.C. - 2009
State Policy and Funding Models for Incumbent Worker Training. Lansing, MI March 29, 2007
 State Policy and Funding Models for Incumbent Worker Training Lansing, MI March 29, 2007 Mission The Workforce Alliance (TWA) is a diverse national coalition of local leaders advocating for federal policies
State Policy and Funding Models for Incumbent Worker Training Lansing, MI March 29, 2007 Mission The Workforce Alliance (TWA) is a diverse national coalition of local leaders advocating for federal policies
DECEMBER Senate Bill 602 sponsored by. Sen. Rockefeller WV
 CENTER FOR RURAL AFFAIRS RURAL ACTION BRIEF VOLUME 1, ISSUE 1 DECEMBER 2004 THE NEW HOMESTEAD ACT WHAT IS IT? The New Homestead Act seeks to attract new residents and businesses to rural areas suffering
CENTER FOR RURAL AFFAIRS RURAL ACTION BRIEF VOLUME 1, ISSUE 1 DECEMBER 2004 THE NEW HOMESTEAD ACT WHAT IS IT? The New Homestead Act seeks to attract new residents and businesses to rural areas suffering
The Minnesota Accountable Health Model SIM Minnesota
 The Minnesota Accountable Health Model SIM Minnesota T E S T I N G A N D I M P L E M E N T I N G T H E M I N N E S O TA A C C O U N TA B L E H E A LT H M O D E L M P H A C O N F E R E N C E J U N E 5,
The Minnesota Accountable Health Model SIM Minnesota T E S T I N G A N D I M P L E M E N T I N G T H E M I N N E S O TA A C C O U N TA B L E H E A LT H M O D E L M P H A C O N F E R E N C E J U N E 5,
North Dakota Health Information Network (NDHIN) April 2015
 April 2015") North Dakota Health Information Network (NDHIN) April 2015 Life begins at the end of your comfort zone. Neale Donald Walsh Governance Health IT Advisory Committee (HITAC) Chair-Lynette Dickson, Associate
North Dakota Health Information Network (NDHIN) April 2015 Life begins at the end of your comfort zone. Neale Donald Walsh Governance Health IT Advisory Committee (HITAC) Chair-Lynette Dickson, Associate
Growing Uninsured. The Nation s Nursing Shortage
 The Health Workforce & New Models of Payment & Delivery of Care: Medical Homes and Accountable Care Organizations, State & National Updates The Nation s Nursing Shortage U.S. will be short 0.25 to 1 million
The Health Workforce & New Models of Payment & Delivery of Care: Medical Homes and Accountable Care Organizations, State & National Updates The Nation s Nursing Shortage U.S. will be short 0.25 to 1 million
National Health Policy Forum December 7, 2012
 Center for Health Innovation National Health Policy Forum December 7, 2012 Integrated Health Services What is CHI? Our Mission Develop and implement strategies and models to improve quality of life and
Center for Health Innovation National Health Policy Forum December 7, 2012 Integrated Health Services What is CHI? Our Mission Develop and implement strategies and models to improve quality of life and
10/21/2012. Healthcare in Very Rural and Frontier Communities: Balancing Equity, Effectiveness and Efficiency.
 www.frontierus.org Healthcare in Very Rural and Frontier Communities: Balancing Equity, Effectiveness and Efficiency Susan Wilger, MPAff National Center for Frontier Communities American Public Health
www.frontierus.org Healthcare in Very Rural and Frontier Communities: Balancing Equity, Effectiveness and Efficiency Susan Wilger, MPAff National Center for Frontier Communities American Public Health
M&M on a 15 Year History of a Merger of Gundersen Clinic and Lutheran Hospital: Struggles and Successes. Jeff Thompson, MD Chief Executive Officer
 M&M on a 15 Year History of a Merger of Gundersen Clinic and Lutheran Hospital: Struggles and Successes Jeff Thompson, MD Chief Executive Officer Who We Are Now Integrated Delivery System Approximately
M&M on a 15 Year History of a Merger of Gundersen Clinic and Lutheran Hospital: Struggles and Successes Jeff Thompson, MD Chief Executive Officer Who We Are Now Integrated Delivery System Approximately
Rural Recruitment for Retention
 Rural Recruitment for Retention Providing Physicians a Road Map for Rural North Dakota Dave Schmitz, MD, FAAFP Stacy Kusler, Center for Rural Health History of Partnerships that work for rural ND: UND
Rural Recruitment for Retention Providing Physicians a Road Map for Rural North Dakota Dave Schmitz, MD, FAAFP Stacy Kusler, Center for Rural Health History of Partnerships that work for rural ND: UND
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model. The New Accountable Care Business Model
 Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
SURVEY OF VIRGINIA S RURAL HEALTH CLINICS
 SURVEY OF VIRGINIA S RURAL HEALTH CLINICS Clinic Data and Needs Assessment Report Fall 2015 Survey conducted by Virginia Rural Health Association in partnership with mjs Consulting, Inc. Funding from Health
SURVEY OF VIRGINIA S RURAL HEALTH CLINICS Clinic Data and Needs Assessment Report Fall 2015 Survey conducted by Virginia Rural Health Association in partnership with mjs Consulting, Inc. Funding from Health
2017 State of Minnesota Rural Health Report to the Minnesota Legislature, Feb. 2017
 2017 State of Minnesota Rural Health Report to the Minnesota Legislature, Feb. 2017 2017 Minnesota Rural Health Association 1 of 22 As rural communities in Minnesota pursue the triple aim of greater access
2017 State of Minnesota Rural Health Report to the Minnesota Legislature, Feb. 2017 2017 Minnesota Rural Health Association 1 of 22 As rural communities in Minnesota pursue the triple aim of greater access
Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it
 Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it CAPT Hernan Reyes, MD Deputy Regional Administrator, HRSA Region 6 July 13, 2016 Objectives Understand the role of HRSA within
Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it CAPT Hernan Reyes, MD Deputy Regional Administrator, HRSA Region 6 July 13, 2016 Objectives Understand the role of HRSA within
Changes in health workforce needs How health workforce planning happens What works and the available policy levers Information needed for health
 August 11, 2015 Bianca Frogner, PhD, Director Center for Health Workforce Studies Sue Skillman, Deputy Director, Center for Health Workforce Studies Associate Director, WWAMI Area Health Education Center
August 11, 2015 Bianca Frogner, PhD, Director Center for Health Workforce Studies Sue Skillman, Deputy Director, Center for Health Workforce Studies Associate Director, WWAMI Area Health Education Center
Minnesota Health Care Home Care Coordination Cost Study
 Minnesota Health Care Home Care Coordination Cost Study Lacey Hartman, Elizabeth Lukanen, and Christina Worrall State Health Access Data Assistance Center (SHADAC) Minnesota Health Care Home Learning Days
Minnesota Health Care Home Care Coordination Cost Study Lacey Hartman, Elizabeth Lukanen, and Christina Worrall State Health Access Data Assistance Center (SHADAC) Minnesota Health Care Home Learning Days
Why SGI Contributes $91.4 billion annually to the state s
 Michigan s Food & Agriculture Industry Strategic Growth Initiative (SGI) Michigan Food and Agriculture Industry Why SGI Contributes $91.4 billion annually to the state s economy. Employs 923,000 Michigan
Michigan s Food & Agriculture Industry Strategic Growth Initiative (SGI) Michigan Food and Agriculture Industry Why SGI Contributes $91.4 billion annually to the state s economy. Employs 923,000 Michigan
Montana Community Health Worker Project Montana Healthcare Foundation Kristin Juliar, Director MT Office of Rural Health/AHEC July 13, 2017
 Montana Community Health Worker Project Montana Healthcare Foundation Kristin Juliar, Director MT Office of Rural Health/AHEC July 13, 2017 History Began exploring interest in CHWs in 2010 Periodic workforce
Montana Community Health Worker Project Montana Healthcare Foundation Kristin Juliar, Director MT Office of Rural Health/AHEC July 13, 2017 History Began exploring interest in CHWs in 2010 Periodic workforce
Mental Health and Primary Care in Rural Minnesota
 Mental Health and Primary Care in Rural Minnesota In 2005, the Rural Health Advisory Committee formed a rural mental health work group to study the delivery of mental health care in rural primary care
Mental Health and Primary Care in Rural Minnesota In 2005, the Rural Health Advisory Committee formed a rural mental health work group to study the delivery of mental health care in rural primary care
The Community Health Needs Assessment Process in North Dakota: The Importance of Community in Community Health
 The Community Health Needs Assessment Process in North Dakota: The Importance of Community in Community Health Brad Gibbens, Deputy Director and Assistant Professor UND Center for Family Medicine Minot,
The Community Health Needs Assessment Process in North Dakota: The Importance of Community in Community Health Brad Gibbens, Deputy Director and Assistant Professor UND Center for Family Medicine Minot,
MEDICAID MEDICAL HOMES PAYING ON A PER MEMBER, PER MONTH BASIS. By: Susan Price, Senior Attorney
 December 8, 2011 2011-R-0394 MEDICAID MEDICAL HOMES PAYING ON A PER MEMBER, PER MONTH BASIS By: Susan Price, Senior Attorney You asked how many state Medicaid programs using a patient-centered medical
December 8, 2011 2011-R-0394 MEDICAID MEDICAL HOMES PAYING ON A PER MEMBER, PER MONTH BASIS By: Susan Price, Senior Attorney You asked how many state Medicaid programs using a patient-centered medical
WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH
 WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH I. CURRENT LEGISLATION AND REGULATIONS Telehealth technology has the potential to improve access to a broader range of health care services in rural and
WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH I. CURRENT LEGISLATION AND REGULATIONS Telehealth technology has the potential to improve access to a broader range of health care services in rural and
California Community Clinics
 California Community Clinics A Financial and Operational Profile, 2008 2011 Prepared by Sponsored by Blue Shield of California Foundation and The California HealthCare Foundation TABLE OF CONTENTS Introduction
California Community Clinics A Financial and Operational Profile, 2008 2011 Prepared by Sponsored by Blue Shield of California Foundation and The California HealthCare Foundation TABLE OF CONTENTS Introduction
California Community Health Centers
 California Community Health Centers Financial & Operational Performance Analysis, 2011-2014 Prepared by Sponsored by Blue Shield of California Foundation Introduction This report, prepared by Capital Link
California Community Health Centers Financial & Operational Performance Analysis, 2011-2014 Prepared by Sponsored by Blue Shield of California Foundation Introduction This report, prepared by Capital Link
North Dakota Nursing Needs Study: Year Four Results and Comparisons
 North Dakota Nursing Needs Study: Year Four Results and Comparisons Patricia Moulton, Ph.D. Presentation for the North Dakota State Board of Nursing July 21, 2006 C H R Overview of the North Dakota Nursing
North Dakota Nursing Needs Study: Year Four Results and Comparisons Patricia Moulton, Ph.D. Presentation for the North Dakota State Board of Nursing July 21, 2006 C H R Overview of the North Dakota Nursing
Georgia Department of Education
 Career, Technical and Agricultural Education FY2016 Budget Guidance for Expending CTAE Grant Funds July 1, 2015 June 30, 2016 TABLE OF CONTENT Pages FY2016 Grant Reporting Date Deadlines... 3 CTAE Function
Career, Technical and Agricultural Education FY2016 Budget Guidance for Expending CTAE Grant Funds July 1, 2015 June 30, 2016 TABLE OF CONTENT Pages FY2016 Grant Reporting Date Deadlines... 3 CTAE Function
In the most recent County Health Rankings & Roadmaps, Red Lake County Ranked 14 th out of 87 Minnesota Counties in overall Health Outcome.
 Red Lake County: County Administration: Agency Name: Red Lake County Social Services Director s Name: Kristi Nelson Address: 125 Edward Ave. PO Box 356 Red Lake Falls, MN 56750 Telephone Number: 218-253-4131
Red Lake County: County Administration: Agency Name: Red Lake County Social Services Director s Name: Kristi Nelson Address: 125 Edward Ave. PO Box 356 Red Lake Falls, MN 56750 Telephone Number: 218-253-4131
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care
 An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
PRIORITY AREA 1: Access to Health Services Across the Lifespan
 PRIORITY AREA 1: Access to Health Services Across the Lifespan GOAL 1: Coordinate health care access strategies that increase the number of knowledgeable residents, promote usage, and establish cost transparency
PRIORITY AREA 1: Access to Health Services Across the Lifespan GOAL 1: Coordinate health care access strategies that increase the number of knowledgeable residents, promote usage, and establish cost transparency
Program of All-inclusive Care for the Elderly (PACE) Summary and Recommendations
 Summary and Recommendations") Program of All-inclusive Care for the Elderly (PACE) PACE Policy Summit Summary and Recommendations PACE Policy Summit On December 6, 2010, the National PACE Association (NPA) convened a policy summit
Program of All-inclusive Care for the Elderly (PACE) PACE Policy Summit Summary and Recommendations PACE Policy Summit On December 6, 2010, the National PACE Association (NPA) convened a policy summit
Driving Change with the Health Care Spending Benchmark
 Driving Change with the Health Care Spending Benchmark Delaware s Road to Value Kara Odom Walker, MD, MPH, MSHS Cabinet Secretary LIFE Conference, January 24, 2018 1 Join us on Twitter: @Delaware_DHSS
Driving Change with the Health Care Spending Benchmark Delaware s Road to Value Kara Odom Walker, MD, MPH, MSHS Cabinet Secretary LIFE Conference, January 24, 2018 1 Join us on Twitter: @Delaware_DHSS
Georgia Department of Education
 Career, Technical and Agricultural Education FY2017 Budget Guidance for Expending CTAE Grant Funds July 1, 2016 June 30, 2017 TABLE OF CONTENT Pages FY2017 Grant Reporting Date Deadlines... 3 CTAE Function
Career, Technical and Agricultural Education FY2017 Budget Guidance for Expending CTAE Grant Funds July 1, 2016 June 30, 2017 TABLE OF CONTENT Pages FY2017 Grant Reporting Date Deadlines... 3 CTAE Function
Expanding Access to Financing & Telehealth for Rural Health Care Providers: Washington State
 Expanding Access to Financing & Telehealth for Rural Health Care Providers: Washington State September 13, 2016 in Olympia, Washington September 15, 2016 in Cheney, Washington Leila Samy, MPH Rural Health
Expanding Access to Financing & Telehealth for Rural Health Care Providers: Washington State September 13, 2016 in Olympia, Washington September 15, 2016 in Cheney, Washington Leila Samy, MPH Rural Health
Creating Philanthropy Initiatives to Enhance Community Vitality
 Winter Fall 2007 2004 Volume 18, 16, Issue 91 Creating Philanthropy Initiatives to Enhance Community Vitality www.iira.org Mark A. Edelman, Ph.D., and Sandra Charvat Burke 1 Many community leaders are
Winter Fall 2007 2004 Volume 18, 16, Issue 91 Creating Philanthropy Initiatives to Enhance Community Vitality www.iira.org Mark A. Edelman, Ph.D., and Sandra Charvat Burke 1 Many community leaders are
Health Reform and The Patient-Centered Medical Home
 THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
NACDD and CDC Health Payer 101 Webinar Series. Webinar #4: Contracting 101
 NACDD and CDC Health Payer 101 Webinar Series Webinar #4: Contracting 101 Jennifer Nolty, Director, Innovative Primary Care National Association of Community Health Centers June 30, 2016 Contracting 101
NACDD and CDC Health Payer 101 Webinar Series Webinar #4: Contracting 101 Jennifer Nolty, Director, Innovative Primary Care National Association of Community Health Centers June 30, 2016 Contracting 101
Georgia Department of Education. Career, Technical and Agricultural Education
 Georgia Department of Education Career, Technical and Agricultural Education Budget Guidance for Expending CTAE Grant Funds in FY2013 TABLE OF CONTENT Pages CTAE Function Codes... 3 Federal Grants Program
Georgia Department of Education Career, Technical and Agricultural Education Budget Guidance for Expending CTAE Grant Funds in FY2013 TABLE OF CONTENT Pages CTAE Function Codes... 3 Federal Grants Program
National Association of Counties. Marcia K. Brand, Ph.D. Deputy Administrator Health Resources and Services Administration March 7, 2011
 National Association of Counties Marcia K. Brand, Ph.D. Deputy Administrator Health Resources and Services Administration March 7, 2011 1 Purpose of This Presentation Overview of the Health Resources and
National Association of Counties Marcia K. Brand, Ph.D. Deputy Administrator Health Resources and Services Administration March 7, 2011 1 Purpose of This Presentation Overview of the Health Resources and
Health Workforce Recruitment and Retention Survey 2014
 Health Workforce Recruitment and Retention Survey 2014 Preliminary Data from the Hospital Survey John Packham, PhD Director of Health Policy Research Office of Statewide Initiatives University of Nevada
Health Workforce Recruitment and Retention Survey 2014 Preliminary Data from the Hospital Survey John Packham, PhD Director of Health Policy Research Office of Statewide Initiatives University of Nevada
Iowa Health Information Technology and Meaningful Use Landscape in 2015
 Health Policy 2-1-2016 Iowa Health Information Technology and Meaningful Use Landscape in 2015 Christopher Carter University of Iowa Peter C. Damiano University of Iowa Xi Zhu University of Iowa Copyright
Health Policy 2-1-2016 Iowa Health Information Technology and Meaningful Use Landscape in 2015 Christopher Carter University of Iowa Peter C. Damiano University of Iowa Xi Zhu University of Iowa Copyright
Primary Care 101: A Glossary for Prevention Practitioners
 PREVENTION COLLABORATION IN ACTION Engaging the Right Partners Primary Care 101: A Glossary for Prevention Practitioners As the U.S. healthcare landscape continues to change under the Affordable Care Act
PREVENTION COLLABORATION IN ACTION Engaging the Right Partners Primary Care 101: A Glossary for Prevention Practitioners As the U.S. healthcare landscape continues to change under the Affordable Care Act
CSOHIMSS Fall Conference Oct 15th, 2010 Healthcare Odyssey Beyond Meaningful Use
 1 CSOHIMSS Fall Conference Oct 15th, 2010 Healthcare Odyssey Beyond Meaningful Use 2 OHIP s Initial Board In September 2009, Governor Strickland designated the Ohio Health Information Partnership (OHIP),
1 CSOHIMSS Fall Conference Oct 15th, 2010 Healthcare Odyssey Beyond Meaningful Use 2 OHIP s Initial Board In September 2009, Governor Strickland designated the Ohio Health Information Partnership (OHIP),
Meeting the Technical Assistance and Training Needs of Iowa Nonprofits
 Meeting the Technical Assistance and Training Needs of Iowa Nonprofits An Evaluation Report for the Larned A. Waterman Iowa Nonprofit Resource Center by Helen A. Schartz, PhD, JD Jill Smith, PhD David
Meeting the Technical Assistance and Training Needs of Iowa Nonprofits An Evaluation Report for the Larned A. Waterman Iowa Nonprofit Resource Center by Helen A. Schartz, PhD, JD Jill Smith, PhD David
Workforce Solutions for Aging Services Careers. Workforce Solutions for Aging Services Careers. Scanning our Environment. LeadingAge Minnesota
 Workforce Solutions for Aging Services Careers Co-sponsored Webinars with Adam Suomala Vice President, Strategic Affiliations Workforce Solutions for Aging Services Careers Scanning our Environment March,
Workforce Solutions for Aging Services Careers Co-sponsored Webinars with Adam Suomala Vice President, Strategic Affiliations Workforce Solutions for Aging Services Careers Scanning our Environment March,
WHITE PAPER. The Shift to Value-Based Care: 9 Steps to Readiness.
 The Shift to Value-Based Care: Table of Contents Overview 1 Value Based Care Is it here to stay? 1 1. Determine your risk tolerance 2 2. Know your cost structure 3 3. Establish your care delivery network
The Shift to Value-Based Care: Table of Contents Overview 1 Value Based Care Is it here to stay? 1 1. Determine your risk tolerance 2 2. Know your cost structure 3 3. Establish your care delivery network
Evaluation of Health Care Homes:
 Division of Health Policy PO Box 64882 St. Paul, MN 55164-0882 651-201-3626 www.health.state.mn.us Evaluation of Health Care Homes: 2010-2012 Minnesota Department of Health Minnesota Department of Human
Division of Health Policy PO Box 64882 St. Paul, MN 55164-0882 651-201-3626 www.health.state.mn.us Evaluation of Health Care Homes: 2010-2012 Minnesota Department of Health Minnesota Department of Human
Frequently Asked Questions
 Frequently Asked Questions What is the Compass Practice Transformation Network (Compass PTN)? The Compass Practice Transformation Network (Compass PTN) was founded by the Iowa Healthcare Collaborative
Frequently Asked Questions What is the Compass Practice Transformation Network (Compass PTN)? The Compass Practice Transformation Network (Compass PTN) was founded by the Iowa Healthcare Collaborative
HRSA & Health Workforce: National Health Service Corps...and so much more
 HRSA & Health Workforce: National Health Service Corps...and so much more U.S. Department of Health and Human Services (HHS) Health Resources and Services Administration (HRSA) Office of Regional Operations
HRSA & Health Workforce: National Health Service Corps...and so much more U.S. Department of Health and Human Services (HHS) Health Resources and Services Administration (HRSA) Office of Regional Operations
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Medicaid EHR Incentive Program Survey of Registrants 2015 Summary of Findings
 Medicaid EHR Incentive Program Survey of Registrants 2015 Summary of Findings INTRODUCTION Beginning in April 2012, providers that registered for the Michigan Department of Health and Human Services (MDHHS)
Medicaid EHR Incentive Program Survey of Registrants 2015 Summary of Findings INTRODUCTION Beginning in April 2012, providers that registered for the Michigan Department of Health and Human Services (MDHHS)
California Program on Access to Care Findings
 C P A C February California Program on Access to Care Findings 2008 Increasing Health Care Access for the Medically Underserved in Four California Counties Annette Gardner, PhD, MPH Some of the most active
C P A C February California Program on Access to Care Findings 2008 Increasing Health Care Access for the Medically Underserved in Four California Counties Annette Gardner, PhD, MPH Some of the most active
How to leverage state funding to bring federal dollars into Nevada
 How to leverage state funding to bring federal dollars into Nevada EXHIBIT F Senate Committee on Health and Human Services Date: 2-12-2013 Page: 1 of 38 FQHC Opportunities for Federal Funding FQHC 101
How to leverage state funding to bring federal dollars into Nevada EXHIBIT F Senate Committee on Health and Human Services Date: 2-12-2013 Page: 1 of 38 FQHC Opportunities for Federal Funding FQHC 101
Before these benefits can be achieved, the Network has three major challenges to overcome:
 April 26, 2011 Dear Colleague: Thank you for your participation in the North Florida Rural Health Workforce Development Leadership Summit that was held on October 14, 2010 at North Florida Community College.
April 26, 2011 Dear Colleague: Thank you for your participation in the North Florida Rural Health Workforce Development Leadership Summit that was held on October 14, 2010 at North Florida Community College.
HITECH Act. Overview and Estimated Timeline
 HITECH Act Overview and Estimated Timeline Key Program, Distribution, Use and Recipients for the HITECH Act* Focused Funds ($2 billion) PROGRAM DISTRIBUTION AGENCY USE OF FUNDS RECIPIENTS HIE Planning
HITECH Act Overview and Estimated Timeline Key Program, Distribution, Use and Recipients for the HITECH Act* Focused Funds ($2 billion) PROGRAM DISTRIBUTION AGENCY USE OF FUNDS RECIPIENTS HIE Planning
TABLE OF CONTENTS. Pages. Federal Grants
 TABLE OF CONTENTS Pages FY2018 Grant Reporting Date Deadlines/Region Coordinator Contact Info... 3 Federal Grants Information..4-5 CTAE Function Codes/Descriptions... 6 Federal Grants Program ID 3315 -Perkins
TABLE OF CONTENTS Pages FY2018 Grant Reporting Date Deadlines/Region Coordinator Contact Info... 3 Federal Grants Information..4-5 CTAE Function Codes/Descriptions... 6 Federal Grants Program ID 3315 -Perkins
Colorado s Health Care Safety Net
 PRIMER Colorado s Health Care Safety Net The same is true for Colorado s health care safety net, the network of clinics and providers that care for the most vulnerable residents. The state s safety net
PRIMER Colorado s Health Care Safety Net The same is true for Colorado s health care safety net, the network of clinics and providers that care for the most vulnerable residents. The state s safety net
Supply and Demand of Health Care Workers in Minnesota. Speaker: Teri Fritsma Wednesday, March 8, :35 3:20 p.m.
 Supply and Demand of Health Care Workers in Minnesota Speaker: Teri Fritsma Wednesday, March 8, 2017 2:35 3:20 p.m. Teri Fritsma Teri Fritsma is a senior research analyst for the Minnesota Department of
Supply and Demand of Health Care Workers in Minnesota Speaker: Teri Fritsma Wednesday, March 8, 2017 2:35 3:20 p.m. Teri Fritsma Teri Fritsma is a senior research analyst for the Minnesota Department of
Writing the Grant: Linking Data Needs and Activities in Rural MA
 Writing the Grant: Linking Data Needs and Activities in Rural MA Ronnie Rom, Massachusetts Rural Hospital Program September 29, 2014, Federal Grant Writing Workshop, Kansas City, MO Outline: Data, Needs,
Writing the Grant: Linking Data Needs and Activities in Rural MA Ronnie Rom, Massachusetts Rural Hospital Program September 29, 2014, Federal Grant Writing Workshop, Kansas City, MO Outline: Data, Needs,