Improving Patient Safety Across Michigan and Illinois
|
|
|
- Malcolm Newton
- 5 years ago
- Views:
Transcription
1 Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016
2 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions Approach Covenant HealthCare Vignette Franklin Hospital Vignette Q/A 2

3 Peer to Peer Learning Network Share Resources Request Resources Step up to be a Mentor N/Resources/PeerToPeerLearningNet work.aspx 3 3

4 IHA Advocacy Day Improvement Poster Posters turned into IHA by this Spring will be printed and showcased at the State Capitol Building on Thursday, April 14 th. Posters due February 24th We will be accepting posters in 5 different categories 1. Care Coordination 2. Patient Safety 3. Integrated Behavioral Health 4. Medication Safety 5. Population Health 4


5 Designing Your Readmission Reduction Approach Pat Teske, RN, MHA

6 Plan for today Share learnings from skill building exercise Compare and contrast leading evidence based models Creating your own evidence Using an outsourced approach Bringing it all together to Adopt successful approaches from other organizations Adapt these approaches for your organization Abandon approaches that are not a good fit and or do not work in your organization

7 What did you learn? From your skill building analysis of: Data Patient Interviews Provider Interviews Record Review Process Review What surprised you? What was confirmed?
8 Evidence-based models

9 Eric Coleman, MD
10 Key Elements of The Care Transitions Intervention TM Low-cost, low-intensity, adapt to different settings One home visit, three phone calls over 30 days Transition Coach is the vehicle to build skills, confidence and provide tools to support self-care Model behavior for how to handle common problems Practice or role-play next encounter or visit Elicit patient s health related goal Create a gold standard medication list (c) Eric A. Coleman, MD, MPH
 Eric A.")
11 Four Pillars Medication self-management Follow-up with PCP/Specialist Knowledge of red flags or warning signs/symptoms and how to respond Patient-centered record (c) Eric A. Coleman, MD, MPH
12 Personal Health Record Remember to take this Record with you to all of your doctor visits (c) Eric A. Coleman, MD, MPH
13 Hospital Visit Introduce the Program and explain how it will feel different Introduce the Personal Health Record Schedule home visit (with family caregiver) (c) Eric A. Coleman, MD, MPH
14 Home Visit Patient identifies a 30-day health related goal Patient asked: Show me what medications you take and how you take them Transition Coach models the behavior for how to resolve discrepancies, respond to red flags, and obtain a timely follow up appointment Patient and Transition Coach practice or role play next encounter(s) Patient identifies 2-3 questions for next encounter (c) Eric A. Coleman, MD, MPH
15 Three Phone Calls Follow-up on active coaching issues Review the Four Pillars Estimate progress made in activation Ensure that patients needs are being met (c) Eric A. Coleman, MD, MPH
16 Care Transitions Intervention (CTI) Summary of Key Findings Significant reduction in 30-day hospital readmits (time period in which Transition Coach involved) Significant reduction in 90-day and 180-day readmits (sustained effect of coaching) Net cost savings of $300,000 for 350 pts/12 mo ($8,571/pt) Widely adopted by leading health care organizations nationwide (c) Eric A. Coleman, MD, MPH
17 N= day readmits Care Transitions Intervention Control 30-day readmits 60-day readmits 8% 13% 15% 17% 20% 29% P-value Eric A. Coleman, MD, MPH
18 Brian Jack, MD
19 RED Checklist Adopted by National Quality Forum as Safe Practice Ascertain need for and obtain language assistance. 2. Make appointments for follow-up medical appointments and post discharge tests/labs. 3. Plan for the follow-up of results from lab tests or studies that are pending at discharge. 4. Organize post-discharge outpatient services and medical equipment. 5. Identify the correct medicines and a plan for the patient to obtain and take them. 6. Reconcile discharge plan with national guidelines. 7. Teach a written discharge plan the patient can understand. 8. Educate the patient about his/her diagnosis. 9. Assess the degree of the patient s understanding of this plan. 10. Review with the patient what to do if a problem arises. 11. Expedite transmission of the discharge summary to clinicians accepting care of the patient. 12. Provide telephone reinforcement of the Discharge Plan.

20 Operationalizing RED After Hospital Care Plan Discharge Advocate Follow-up phone call
21 Components of RED Intervention In Hospital Nurse Discharge Advocate (DA) Interacts with care team: medication reconciliation, appointments, and national guidelines Prepares and teaches After Hospital Care Plan (AHCP) Post Discharge Clinical Pharmacist Calls for 72 hours post-dc Reinforces dc plan and review medications

22 COVER PAGE

23 MEDICATION PAGE (1 of 3)

24 PATIENT ACTIVATION PAGE
25 Components of RED Intervention In Hospital Nurse Discharge Advocate (DA) Interacts with care team: medication reconciliation, appointments, and national guidelines Prepares and teaches After Hospital Care Plan (AHCP) Post Discharge Clinical Pharmacist Calls for 72 hours post-dc Reinforces dc plan and review medications
26 Randomized Controlled Trial Enrollment N=749 Randomization RED Intervention N=374 Usual Care N= day Outcome Data Telephone Call EMR Review Enrollment Criteria: English speaking Have telephone Able to independently consent Not admitted from institutionalized setting Adult medical patients admitted to Boston Medical Center (urban academic safety-net hospital)
27 Primary Outcome: Hospital Utilization within 30d after dc Hospital Utilizations * Total # of visits Rate (visits/patient/month) ED Visits Total # of visits Rate (visits/patient/month) Readmissions Total # of visits Rate (visits/patient/month) Usual Care (n=368) Intervention (n=370) P-value * Hospital utilization refers to ED + Readmissions
28 Outcome Cost Analysis Cost (dollars) Usual Care (n=368) Intervention (n=370) Difference Hospital visits 412, , ,602 ED visits 21,389 11, ,104 PCP visits 8,906 12,617-3,711 Total cost/group 442, , ,995 Total cost/subject 1, We saved $412 in outcome costs for each patient given RED
29 Mark Williams, MD
30
31
32
33
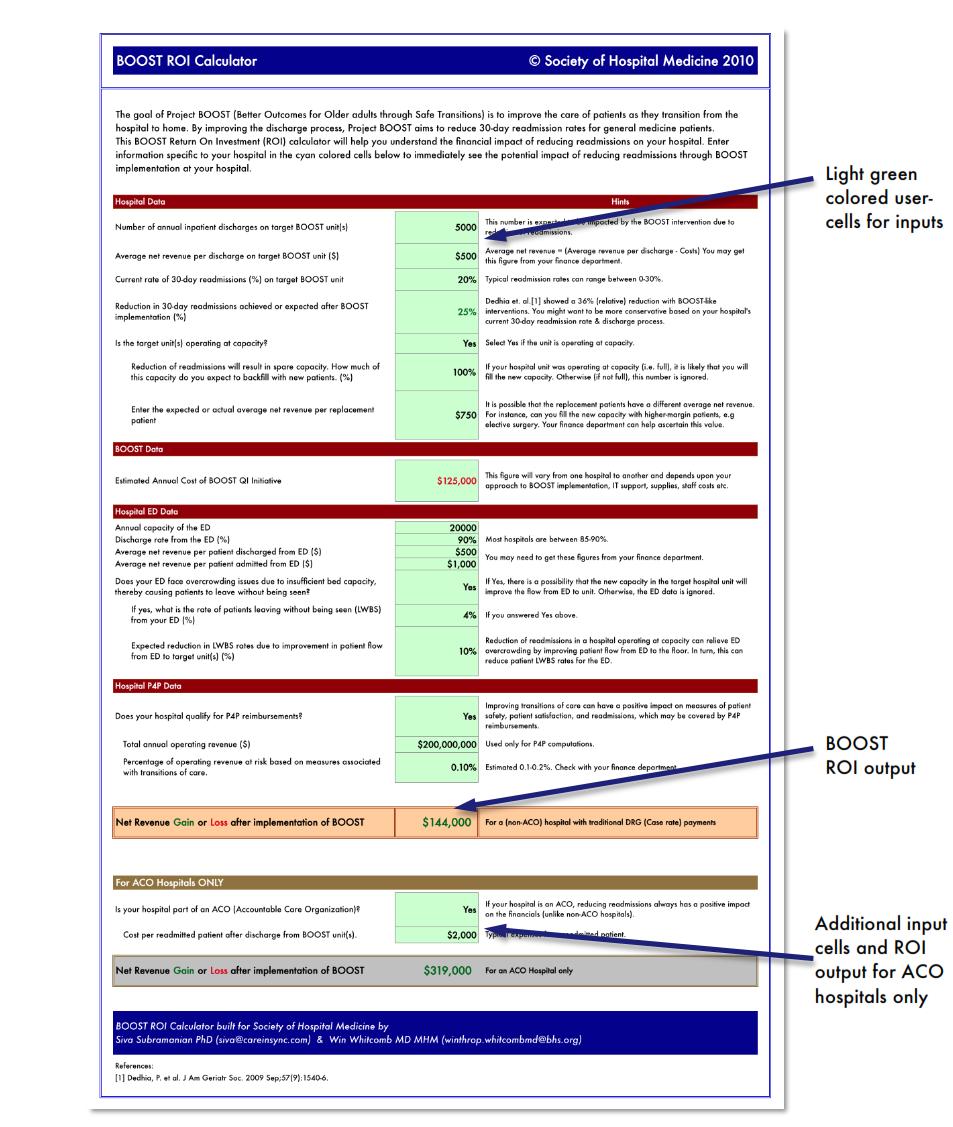
, reflecting an absolute reduction of 2% and a relative reduction of 13.6%. Rehospitalization rates for matched control units were 14.0% in the preintervention period and 14.")
34 Results The average rate of 30-day rehospitalization in BOOST units was 14.7% prior to implementation and 12.7% 12 months later (P = 0.010), reflecting an absolute reduction of 2% and a relative reduction of 13.6%. Rehospitalization rates for matched control units were 14.0% in the preintervention period and 14.1% in the postintervention period (P = 0.831). The mean absolute reduction in readmission rates in BOOST units compared to control units was 2.0% (P = for signed rank test comparing differences in readmission rate reduction in BOOST units compared to sitematched control units). Journal of Hospital Medicine 2013;8: Society of Hospital Medicine
35
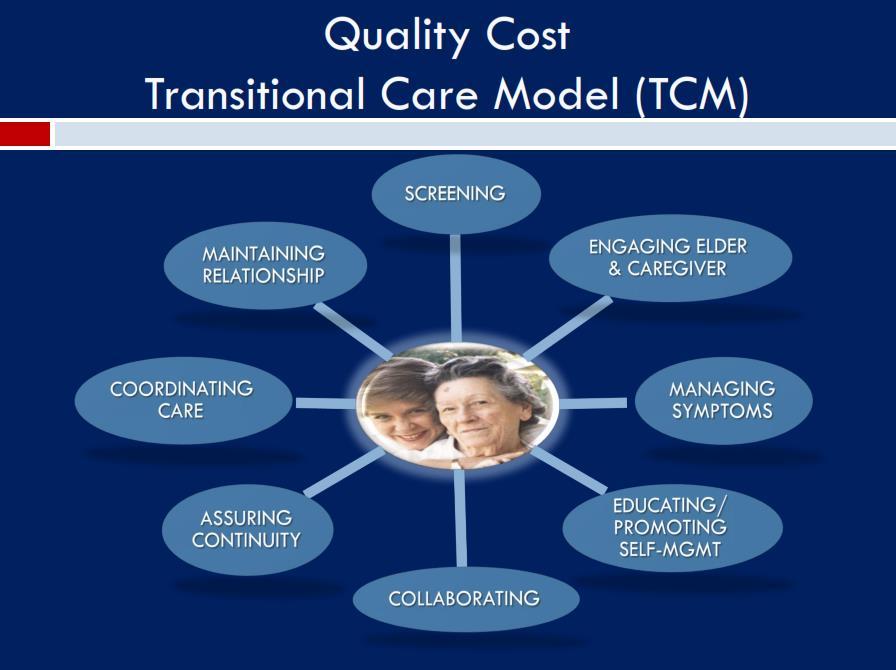
36 Mary Naylor, PhD, RN
37
38
39
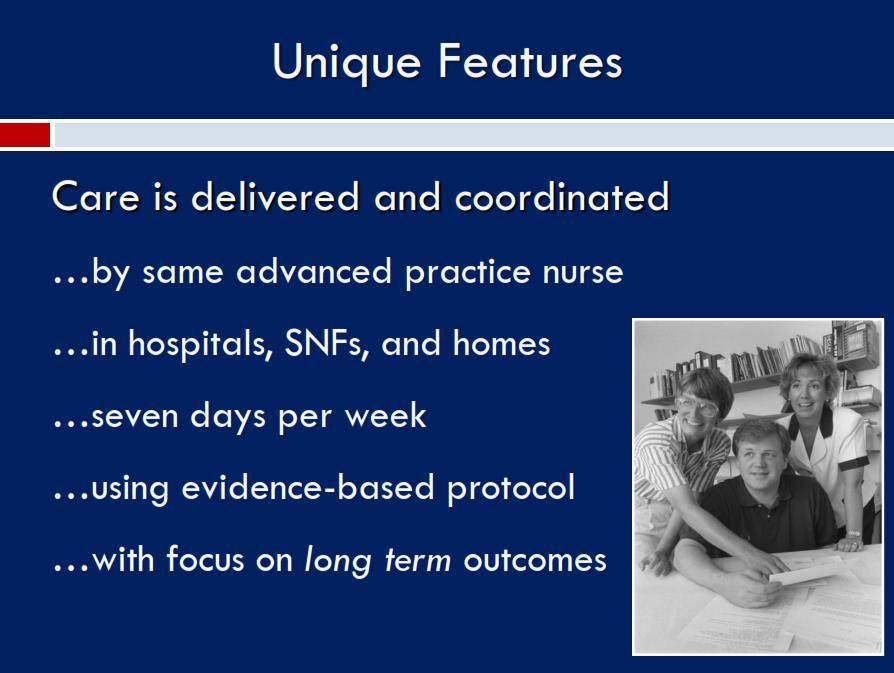
40
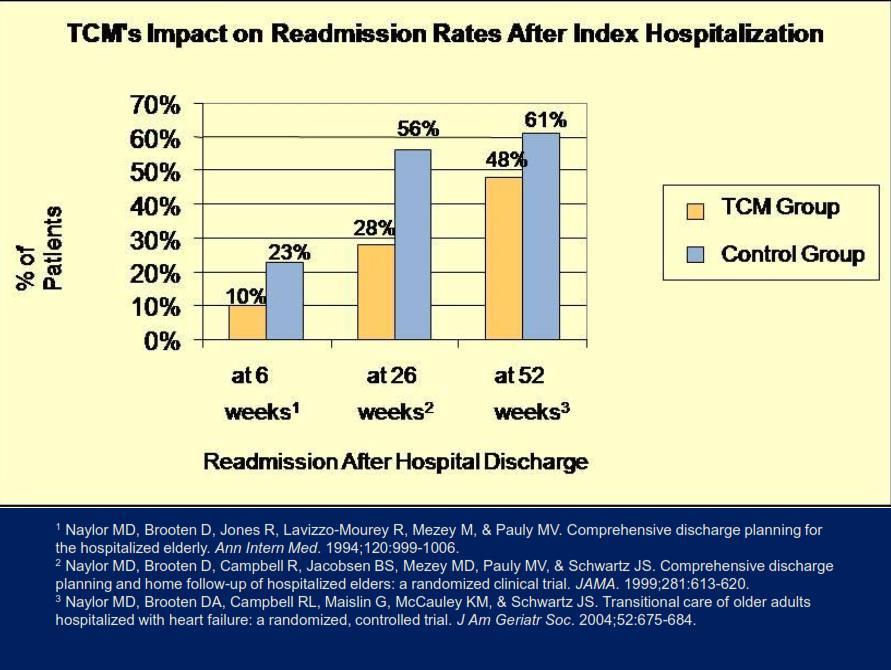
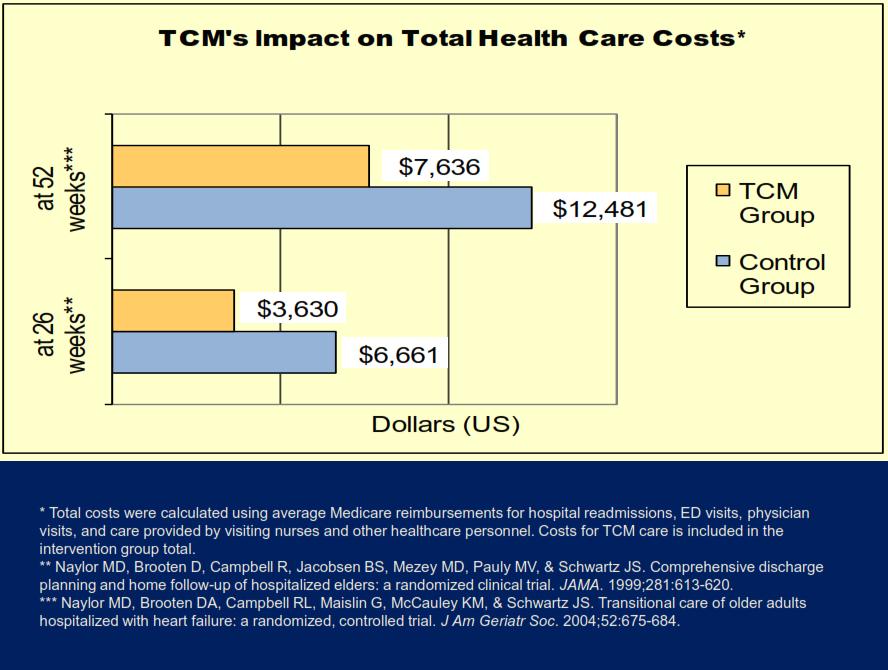
41
42 Models At-A-Glance CTI RED TCM BOOST Staff Coaches (RN) Discharge Advocates (RN) Pharmacists Advance Practice Nurses Unspecified Setting Primarily post discharge Primarily in hospital Primarily post discharge Primarily in hospital Duration post discharge 30 days 72 hours Approx. 8 weeks 72 hours

43 Different Models, Common Themes

44 There s a plan

45 Patient Centered

46 Medications

47 Self Management Knowledge

48 Connections

49 Reinforcement

50 Get into the weeds

51 Select your model
52 Approaches to Reducing Cardiac Readmissions Karen S. Bush, MSN, FNP, BC, NCRP Transition Coach Nurse Practitioner Covenant HealthCare
53 Disclosure Statement I work for Covenant HealthCare I am the President of Selfcare Solutions LLC I own the patents related to this project Covenant HealthCare owns copyrights related to this project


54 Covenant Healthcare Transitions Addressing the Needs of all patients Primary Care and Community Resources Boost Initiatives F/U Appt. Scheduled, Timely D/C summaries, Teach Back, Med. Rec. Case Resource Management Transition Coach

55 What s a Transition Coach?

56 Transition Coach A transition coach is someone who coaches patients in their own health so that they can safely transition from the hospital to the home setting. Typically they start working with patients in the hospital and then follow them post discharge either telephonically or with in home visits. Target is to enhance the safety of the patient s transition which results in a reduction of readmissions
57 Why is a Safe Transition (discharge) Important? It impacts patient s health and well being Physical, emotional as well as financial It impacts family and caregiver burden Physical, emotional as well as financial It impacts how people view care provided at your institution Now with payment reform it impacts reimbursement


58 Where was Covenant? According to the most recently published hospital compare data the U.S. national rate of readmission for heart failure patients was 23% The rate of readmission for Covenant Healthcare during the same time using the same criteria was 26.6% Hospital Compare Quality of Care Profile Page Accessed 2014
59 Everyone has an Opinion How hard can it be to keep people from coming back to the hospital for 30 days? It s just those 4-5 people This research study says to This hospital is doing this We should to this Look at the research and the data Decide what will work and STAY THE COURSE!!!
60 How Patients Feel Patients may have negative feelings and emotions related to their limited reading ability or limited understanding Institute of Medicine, 2004 The health care environment can make it hard for patients to tell us they don t read well or do not understand They hide this with a variety of coping techniques Parikh N Pt Educ and Counseling, 1996


61
 Nearly half of the information that patients retain is incorrect.")
62 The Challenge Studies demonstrate that 40-80% of the medical information patients receive is forgotten immediately. Kessels, RP (2003) Nearly half of the information that patients retain is incorrect. Anderson JL et al (1979) Patients remember and understand less than half of what clinicians explain to them Ley, (1988)




63 Necessary Knowledge for a Heart failure patient The Heart Failure Society of America and the American College of Cardiology identify 6 areas for essential education of the hospitalized patient prior to discharge Recommended activity level Diet (Sodium and Fluid Restriction where appropriate) Discharge Medications Follow up appointment Weight Monitoring What to do if signs or symptoms worsen

64 Current Research is great, but you need to go to the source. Go to the front line Talk to people on the front line Interview, survey, interact Worked with patients Talked to staff


65 I went to the front line I have heart failure??? I just watch what I drink I don t add any salt to my food. Well I wasn t feeling good so I was eating chicken soup and my kids thought I should have gator-aid. They don t weigh me here so why do I have to weigh myself at home
 414 Balancing Beads Patent Selfcare Solutions LLC July 2015 Education that flows across the continuum of care Address symptoms of fluid overload, but also")
66 Balancing your Daily Fluid An interactive tool Covenant HealthCare All rights reserved. Bus Dev (AQ/PK ) 414 Balancing Beads Patent Selfcare Solutions LLC July 2015 Education that flows across the continuum of care Address symptoms of fluid overload, but also address the potential for dehydration and acute kidney injury Involvement of caregivers and family
67
68 Research Study Pretest-Intervention-Posttest-30 day Posttest Primary goal was to improve Heart Failure Maintenance, Management, and Confidence with the use of Diagnosis Specific Toolkit. Pretest for baseline prior to introduction of toolkit Posttest was completed post intervention Posttest 30 days after discharge from the hospital to determine sustainability of change Secondary aim was to reduce 30 day readmission rates
69 Why not just look at readmission rates if that is the goal?
70 Subjects Identified for Study Targeting hospitalized heart failure patients with working DRG of 291, 292, 293 Primary exclusion criteria Discharge disposition other than home Renal Failure on Renal Replacement Therapy Co-morbid COPD with active treatment Kidney or heart transplant patients
71 Study Population: Target 50 patients 6 patients were lost to study 41 patients completed all 3 surveys Return rate of 93% 34.1% female and 65.9% male 29.5% disposition home alone and 70.5% home with family 36.4% received education with a caregiver & 63.6% received education alone
72 Clinical Implications 70 or greater mean=self care adequacy More than ½ of a standard deviation improvement is considered clinically relevant 50 th percentile-marked reductions in the odds of having episodes of hemodynamic congestion and risk of death or hospitalization 75 th percentile=direct inpatient cost savings are seen. Reigel, B et al (2009)
73 Impact of Toolkit on HF Maintenance, Management and Confidence Maintenance Management Confidence Pre Test Immediate Post Test 30 Day Post Test
74 Section/Time Number Mean Std. Deviation Results P Value Pre Test HF Maintenance <0.05 Immediate Post Maintenance < day Post Maintenance <0.05 Pre Test HF Management <0.05 Immediate Post Management < day Post Management <0.05 Pre Test HF Confidence <0.05 Immediate Post Confidence < day Post Confidence <0.05
75 Patient Feedback I used it every day I thought it was an excellent idea and very helpful Because we were at Ludington for several days with our families over Thanksgiving I let my guard down and over indulged in fluid and salt. Because of the study and tool kit I realized something wasn t right. Got my act together and got back on schedule which got me back to feeling better! I liked it very much. I would see it and it would remind me to drink more or less. Weighing myself everyday keeps me in the safe zone. I have been in the safe zone since I started the program. I think this program helped me out a lot. Thank-you The tool kit works. Thank-you Very easy to follow and use. Helpful in getting control of the situation. Great as is. Thank you for the opportunity of doing this study. I never before realized that just one little thing could have such a bearing on my every day living. I will continue the program forever. Thank you again s-o-o-o much
76 Readmission Data 44 patients in the study 40 patients successfully stayed out of the hospital 30 days 4 readmitted within the 30 day window Readmission rate of 9% Hospital purchased 100 more kits Used by NP and RN transition coaches 41 patients received kits in January and February 37 patients successfully stayed out of the hospital 30 days 4 patients readmitted within 30 days post discharge Readmission Rate of 9.8% This demonstrated that an RN or an NP could use this kit successfully with patients

77 Something was missing

78 We needed comparison data




79 Admission Source 255 Heart Failure Patients Admission Source 7% 7% 7% 2% Non Health Care Facility=197 Clinic or Physician Office=18 Transfer from another Hospital=17 Transfer from SNF=17 77% Other=6
80 13.7% 19.2% 17.2% 25.7% 43.0% 57.0% Volume of HF Patients Admitted to PCCU and Effect of Toolkit 255 Heart Failure Patients VOLUME OF PATIENTS ADMITTED TO PCCU VS OTHER UNITS AND READMISSION DATA Volume of Total HF Patients Readmit Rate Readmit Rate for these Units with Toolkit PCCU OTHER UNITS
81 Volume of HF Patients Admitted to PCCU and Effect of Toolkit 255 Heart Failure Patients Units # of 255 CHF patients # of CHF patients readmitted # of CHF patients with kit # of patients readmitted with kit on each unit PCCU /146 or 19.1% Other Units /109 or 25.7% 51 7/51 or 13.7% 29 5/29 or 17.2%
82 12.5% 23.5% 23.5% 33.3% 31.4% 45.1% No Intervention vs TC without and with Toolkit 255 Heart Failure Patients TRANSITION COACH DATA Volume of HF Patients Readmission Rate NO INTERVENTION (N=60) TRANSITION COACH ONLY (N=115) TC WITH TOOLKIT (N -80)
83 No Intervention vs TC without and with Toolkit 255 Heart Failure Patients Intervention # of the 255 CHF patients Percentage of total CHF patients # of CHF patients readmitted Readmit Rate No Intervention % % Transition Coach Only Transition Coach with Toolkit % % % % Transition Coach with & without Toolkit % %
84 Casting a Broader Net The hospital purchased 1,000 more kits for this fiscal year Implement the toolkit for high risk patients (LACE score 10 and above 65) with ejection fraction less than 50% and diagnosis of AMI and CHF patients. Implement the toolkit additionally on any other appropriate heart failure patient. A consult to transition coach has been added to our epic system Toolkit is provided with video education and reinforced using teach back with the transition coaches Each patient will receives at least one post discharge call within 72 hours of discharge by the transition team.
85 How are we doing now? July through December 2014 the readmission rate for our Medicare population discharging with heart failure was 24.31% July through December 2015 the readmission rate for our Medicare population discharging with heart failure is 17.33% We began implementation of the broader use of toolkits with a tracking system integrated into EPIC for the months of October and November. We had 48 high risk patients with the diagnosis of AMI or CHF who received toolkits. The readmission rate for this population was 14.58%
86 Final Thought In the space between chaos and shape there was another chance. Jeanette Winterson
87 Karen S. Bush MSN, FNP BC, NCRP



88 16-bed Critical Access Hospital
89 TipOff program - Our goal is to reduce the readmission percentage Issue: COPD readmissions within 30 days for all causes range from 17% to 25% For moderate-to-severe COPD patients Hospitalized within the last 6 months Discharge home with ability to care for their own chronic condition. Patients can self-monitor and alert provider to critical signs and symptoms before they lead to hospital readmissions or ED visit.
90 Why did Franklin Hospital choose to participate in TipOff? Our strategic plan includes population health goals pertinent to our community. COPD is relevant to our southern Illinois community of farmers, coal industry and allergies. Early interventions and tracking of symptoms at home will result in decreased ER visits and hospitalizations for our patient.
91 How it works The Case Manager screens MIP s for COPD Primary or secondary diagnosis. Determine if patient is discharged home and determine ability to manage chronic condition at home. If both criteria are met, the patient is informed about the TipOff program and permission is required to participate before notification of TipOff. If patient agrees, enrollment is completed. The hospitalist signs consent and attending physician practice is notified of patient s participation. DME s are chosen by the patient from area selection and plays no part in the TipOff program. If home health services are needed by the patient, case management offers a choice of area services at discharge.
92 Results Program started late October We have experienced 3 patients that met criteria. No patients declined to participate. None of the three patients have visited the ED or been readmitted through January 31, We are approaching the RHC for interest in this program.
93 Next Steps Identify a Readmissions Model or Best Practice and design your approach: delsandresources.pdf Next month s webinar will be focused on Care Transitions Illinois Hospitals download your Readmissions Activity Profile and Dashboard Reports: 93

94 March 16 th -Care Transitions 94
Roundtable on Health Literacy Institute of Medicine 17 March 2014
 Project RED: Reengineering the Discharge Process Roundtable on Health Literacy Institute of Medicine 17 March 2014 Michael Paasche-Orlow MD, MA, MPH Associate Professor of Medicine Boston University School
Project RED: Reengineering the Discharge Process Roundtable on Health Literacy Institute of Medicine 17 March 2014 Michael Paasche-Orlow MD, MA, MPH Associate Professor of Medicine Boston University School
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Improving Transitions of Care
 Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
The Changing Landscape: A Confluence of National Attention. Eric A. Coleman, MD, MPH
 Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
New SNF Quality Measures
 New SNF Quality Measures Strategies to Boost your Facility Performance Dr. Kathleen Weissberg, OTD, OTR/L Education Director Select Rehabilitation kweissberg@selectrehab.com Objectives Understand the measure
New SNF Quality Measures Strategies to Boost your Facility Performance Dr. Kathleen Weissberg, OTD, OTR/L Education Director Select Rehabilitation kweissberg@selectrehab.com Objectives Understand the measure
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
Thinking Differently about Hospital Readmissions
 Thinking Differently about Hospital Readmissions LaNita Knoke RN, BS, CMCN Healthcare Strategist Senior Care Continuum Each Home Instead Senior Care franchise office is independently owned and operated.
Thinking Differently about Hospital Readmissions LaNita Knoke RN, BS, CMCN Healthcare Strategist Senior Care Continuum Each Home Instead Senior Care franchise office is independently owned and operated.
Care Transitions Partnerships that Work for Patients
 Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Molina Healthcare Michigan Health Care Services Department Phone: (855) Fax: (800)
 Fax: (800)") Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses
 The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses August 5, 2009 Center for Health Care Strategies Webinar Randall Brown,
The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses August 5, 2009 Center for Health Care Strategies Webinar Randall Brown,
Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure
 Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure November 16, 2016 Panelists Corinne Bott-Silverman, M.D., Cardiologist,
Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure November 16, 2016 Panelists Corinne Bott-Silverman, M.D., Cardiologist,
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
CHF Education March Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN
 CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Safe Transitions: From Patient Centered Care to Patient Directed Care
 Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Care Continuum or Unconnected Silos
 Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Chronic Care Management
 Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
A Virtual Ward to prevent readmissions after hospital discharge
 A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives"
 2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
A Care Transitions Project
 Hospital to Home: A Care Transitions Project Ann Roemen, MBA, CMPE Readmissions 1 in 5 elderly patients Resultsin23million 2.3 re-hospitalizations Annual cost to Medicare - $17 billion + Jencks SF,Williams
Hospital to Home: A Care Transitions Project Ann Roemen, MBA, CMPE Readmissions 1 in 5 elderly patients Resultsin23million 2.3 re-hospitalizations Annual cost to Medicare - $17 billion + Jencks SF,Williams
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Hot Spotter Report User Guide
 PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Heart Failure Nurse Practitioner Role Development and Proposal. Anita M. Wilson, BSN, RN. ACNP, DNP Student Creighton University
 1 Heart Failure Nurse Practitioner Role Development and Proposal Anita M. Wilson, BSN, RN ACNP, DNP Student Creighton University PO Box 21 Kingsley, IA 51028 abwilson@frontiernet.net 712-490-8347 Mary
1 Heart Failure Nurse Practitioner Role Development and Proposal Anita M. Wilson, BSN, RN ACNP, DNP Student Creighton University PO Box 21 Kingsley, IA 51028 abwilson@frontiernet.net 712-490-8347 Mary
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate
 TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
A Call to Action: Readmission Strategies from the Field
 A Call to Action: Readmission Strategies from the Field Vicky Mahn-DiNicola, RN, MSN,CPHQ VP Research & Market Insights Brenda Pettyjohn, RN, CPHQ Solutions Advisor Tina Esposito Vice President, Center
A Call to Action: Readmission Strategies from the Field Vicky Mahn-DiNicola, RN, MSN,CPHQ VP Research & Market Insights Brenda Pettyjohn, RN, CPHQ Solutions Advisor Tina Esposito Vice President, Center
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers
 Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of
 2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company
2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Transitional Care in a Rural Setting:
 2017 Rural Healthcare Leadership Conference Transitional Care in a Rural Setting: Redesigning Hospital Discharge to Enhance Patient Care Tuesday, February 7, 2017 Welcome L. Lee Isley, Ph.D, FACHE Chief
2017 Rural Healthcare Leadership Conference Transitional Care in a Rural Setting: Redesigning Hospital Discharge to Enhance Patient Care Tuesday, February 7, 2017 Welcome L. Lee Isley, Ph.D, FACHE Chief
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Reducing Avoidable Readmissions Within 30 Days of Discharge
 Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
04/08/2015. Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists. Pharmacist Objectives. Technician Objectives
 1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
UCSF Transitional Care Program. Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016
 UCSF Transitional Care Program Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016 Session Objectives Describe elements necessary for building a cross continuum
UCSF Transitional Care Program Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016 Session Objectives Describe elements necessary for building a cross continuum
University Cincinnati Medical Center
 University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health
 Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons
 Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Best Practices in Managing Patients with Heart Failure Collaborative
 Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Documentation 101: CDI JULY 19, 2017
 Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Improving Emergency Department Transitions of Care Can It Help with ED Overcrowding? Stephen V. Cantrill, MD, FACEP Denver Health Medical Center
 Improving Emergency Department Transitions of Care Can It Help with ED Overcrowding? Stephen V. Cantrill, MD, FACEP Denver Health Medical Center Improving Emergency Department Transitions of Care: Can
Improving Emergency Department Transitions of Care Can It Help with ED Overcrowding? Stephen V. Cantrill, MD, FACEP Denver Health Medical Center Improving Emergency Department Transitions of Care: Can
Lost in Transition. Definition. Objectives 9/22/2014
 Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions