A Call to Action: Readmission Strategies from the Field
|
|
|
- Gwen Little
- 6 years ago
- Views:
Transcription
1 A Call to Action: Readmission Strategies from the Field Vicky Mahn-DiNicola, RN, MSN,CPHQ VP Research & Market Insights Brenda Pettyjohn, RN, CPHQ Solutions Advisor

2 Tina Esposito Vice President, Center for Health Information Services Advocate Health Care Responsible for system measurement and analytics in support of improved patient outcomes and organizational performance Responsibilities include data warehousing, HIM, and public data. Master in Business Administration Bachelor of Science degree in Health Information Management Certified Six Sigma Black Belt 2


3 Advocate Health Care Corporate offices in Downers Grove, Illinois More than 250 sites offering inpatient, outpatient services, home health services, hospice, counseling, physician services, and health care education programs - 12 hospitals, more than 3,300 beds - 11 acute care hospitals - 1 children s hospital, with 2 campuses The state s largest integrated children s network The region s largest medical group with more than 200 locations across metropolitan Chicago 3

4 Patty Toney RN, MSN Vice President & Chief Nurse Executive CHRISTUS Santa Rosa Health System Vice President and Chief Nurse Executive for a six hospital healthcare system in Santa Rosa, Texas Nursing Degree from Ball State Masters in Nursing Administration Former Chief Nursing Officer for McKenna Hospital in New Braunfels She has been a nurse for over 35 years and has practiced in Critical Care, Labor Delivery and as a House Supervisor for a large 500 bed teaching hospital in New Jersey. 4



5 Christus Health An international Catholic, faith-based, not-for-profit health system comprised of almost 350 services and facilities, including more than 60 hospitals and long-term care facilities, 175 clinics and outpatient centers, and dozens of other health ministries and ventures. CHRISTUS services can be found in over 60 cities in Texas, Arkansas, Iowa, Louisiana, Missouri, Georgia, and New Mexico in the United States, and Mexico. 5











6

7 Pamela Carroll-Solomon, MJ, RHIA, CPHQ, Director, Quality Services, Catholic Health East Trinity Health Director, Quality Services at CHE Trinity Health. Responsible for the MIDAS+ DataVision application since its implementation in Masters of Journalism Bachelors in Health Records Administration from Temple University CPHQ and Lean Six Sigma Black Belt Author of numerous publications on Quality and HIM related topics Member of NQF Readmission Action Team Just celebrated her 16 th year at CHE 7

8 CHE Trinity Health Second-largest Catholic health care delivery system in the nation. Operate in 20 states from coast to coast with 82 hospitals, 88 continuing care facilities and home health and hospice programs that provide more than 2.3 million visits annually. Formed in May 2013, when Trinity Health and Catholic Health East completed their consolidation to strengthen their shared mission, increase excellence in care and advance transformative efforts with their unified voice. 8

9 NQF Readmission Action Team Use of Interact tool Partnering with hospitals to improve care transitions Residents/Family Teaching on resources at facility level CMMI grant on care transitions Front-loading of visits Partnering with other providers to improve care transitions Use of telemedicine 9
10 Advocate Care Model FROM Silo care management Episodes of care Discharges Utilization Management Caring for the sick Production (volume) TO Population/enterprise care management Value-driven coordinated care Transitions Right care at the right place at the right time Improving health status Performance (value/lower cost) 10

11 CHRISTUS Santa Rosa Care Transitions Program Trademarked program designed by Eric Coleman MD, MPH Started in 2009 at St. Michael's in Texarkana and then at SPOHN in Corpus Christi in 2010 Santa Rosa implemented in October 2013 at one of three adult hospitals. Now have CTN in each adult hospital Focus on: AMI, HF and PN Goal: 10% reduction in re-admit by end of Year
12 In a Nutshell. Care Transitions Nurse (CTN) reviews census each morning for AMI, HF or PN diagnosis or related symptoms. Visits patient and family, explains program, obtains consent to enroll. Works w patient and family while in hospital to prepare for discharge Makes 1 home visit within 48 hrs of discharge Makes two F/U telephone calls for total program length of 30 days Hands off patient to primary care provider at end of 30 days 12 12

13 Patient Engagement 13
14 CHE s Approach Readmissions Task Force Use of data to drive improvements Crosscontinuum collaboration Personcentered care Leveraging technology In-depth analysis (DataVision Toolpack) Readmission penalty projection calculations Kept abreast of HEN activities, public release of data Use various MIDAS reports (DV Toolpack, APRDRG reports, new readmission reduction metrics) Inpatient satisfaction with discharge information received SNF Use of Interact tool Partnering with hospitals to improve care transitions Residents/Family Teaching on resources at facility level CMMI grant on care transitions Home Care Front-loading of visits Partnering with other providers to improve care transitions Use of telemedicine Integrate hospitalists and residents into daily operations related to readmissions Importance of palliative care referrals Teach back Partnering with community pharmacies for delivery of home meds prior to discharge Created reports to assist/automate medication reconciliation Monitor recording of discharge instructions Use telemonitoring 14
15 CHE Readmission Penalty Projections FY15 MIDAS data (rate) FY14 QNet data (rate) FY14 CMS Penalt y Factor FY14 Penalty (1- factor) FY15 Estimated Penalty Factor FY15 Estimated Penalty Factor Adjusted DRG Payment FY12 Cost Report DRG Payments Adjusted DRG Payments FY15 Potential Readmission Impact Standard indicators for CMS readmissions reduction program for timeframe of penalty year Calculation: (sum of nums)/ (sum of denoms) * 100 Obtain preview reports, specifically rate data Calculation: (sum of nums)/ (sum of denoms) * 100 From most recent IPPS final rule Calculation: 1 actual penalty factor (from prior year) Calculation: (Projected FY Midas data) x (Prior FY penalty factor)/(prior FY Qnet data) Calculation : 1 FY15 estimated penalty factor From most recent IPPS final rule From most recent IPPS final rule Calculation: (projection FY estimated penalty factor) x (Most current FY cost report DRG payments) Calculation: (Adjusted DRG payments) (Most current FY cost report DRG payments) 15



16 Observational Care Units & Retail Health Clinics 16

17 Leveraging EMR Technology 17

18 Readmission Model Framework Cohort description: 192 K people with hospitals encounters 8 hospitals in Chicago-land area Analyzed observation, medical, and surgical patients Considered all conditions except mental health Please Note: The examples provided are intended to show a representation of the many variables analyzed in the model which is still under development and should not be interpreted as statistically significant predictors for a readmission. 18




19 Readmission Solution Workflow Identify Notify Assess Intervene 19 MPage Discern Alerts PowerForms Readmission Plan of Care 19

20 Discharge Checklist 20

21 How to Manage High-Risk Patients A Qualitative Analysis Example Issue: How to address a highly satisfied patient Response: Aligned with philosophy of doing the right thing for the patient at the right time Worked with patient to assign a primary care team in ED Cut visits from 30 ED visits, 31 admissions, 24 readmits/year to 5 admissions, 1 readmission, no ED visits in next year!! 21
22 CHE Results Vision A.C.T. Applying personcentered interventions leads to less readmissions and better quality of life PfP: 20% Reduction over 3 years Baseline = 1594 per month Saved Year 1 Saved Year 2 AMI, HF, PN, COPD among top 5 diagnoses yearto-year but now seeing rehab Saved Year 3 Exceeded goal of 20% reduction over 3 years actual = 30% 22
23 Outcomes Leading the industry ~ 20% better than industry (Yale, LACE, etc.) Solution purchased by 120 non-advocate Cerner clients Gaining efficiency ~ 3.5 FTE productivity savings across system Automated continuous calculation of risk score in EMR Reducing readmissions 20% reduction in readmission rates (for high risk patients that received interventions) Statistically significant reductions observed for sub-populations (e.g., COPD and HF) 23


24 Dollars (millions) Readmission Rate (%) Readmission Penalty Trend $ $ $1.8 $2.9 $ * $ Lost $ Earned Back $ at Risk Readmission Rate 24
25 CHRISTUS Observations from the field Medication reconciliation and polypharmacy is single biggest problem/challenge Linking patient to pc provider before discharge from hospital is high priority Visit to the home is invaluable for identifying socio-economic issues That said, single biggest reason for refusal to participate is the home visit telemonitoring option needed! CTN works closely with CM to identify potential program candidates 25
26 CHRISTUS Santa Rosa - New Braunfels AMI Readmission Rates FY2014 (Any Payer, Any Diagnosis) New Braunfels Linear (New Braunfels) 19.05% 15.79% 16.67% 10.53% 11.11% 0.00% 0.00% 0.00% 0.00% 0.00% 26
27 CHRISTUS Santa Rosa - New Braunfels Heart Failure Readmission Rates FY2014 (Any Payer, Any Diagnosis) New Braunfels Linear (New Braunfels) 33.33% 18.18% 17.65% 18.18% 20.00% 21.43% 9.09% 10.00% 6.25% 0.00% 27
28 CHRISTUS Santa Rosa - New Braunfels Pneumonia Readmission Rates FY2014 (Any Payer, Any Diagnosis) New Braunfels Linear (New Braunfels) 40.00% 16.67% 12.50% 6.67% 7.69% 7.41% 9.09% 5.88% 0.00% 0.00% 28
29 Next steps at CHRISTUS. Using Midas+ to automate data collection and drill down into demographics, medical history etc. for risk stratification and improved analytics Introduce telemonitoring as an intervention option Create screening criteria for applying right intervention, at the right time, for the best outcome Expand scope of program to include other at risk for re-admit populations such as COPD and diabetes Expand program to include post acute facilities - SNF s, nursing homes, etc. Incorporate Care Transitions program into clinically integrated network of medical homes to build a true coordinated model of care 29
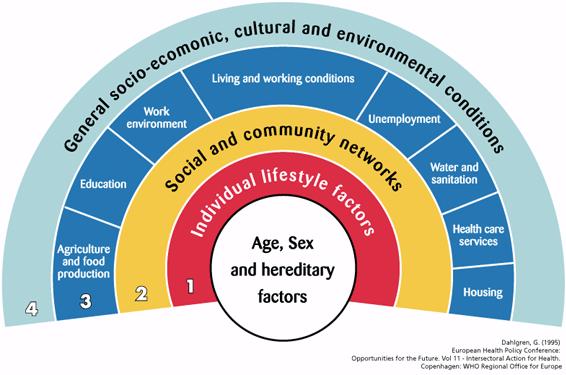
30 Socioeconomic Variables 30


31 Questions and Shared Learning 31


32 We Wish to Thank All Our Midas Clients For Their Support! See You Tonight at the Party!! Vicky Mahn-DiNicola, VP Research & Market Insights, Midas+ Brenda Pettyjohn, Solutions Advisor, Midas+ Tina Esposito, VP Center for Health Information Services, Advocate Health Care
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Program Development. Completion of Gap Analysis. Review of Data. Multi-disciplinary team
 Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Ministries serving as alpha sites committed to
Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Ministries serving as alpha sites committed to
Data-Driven Strategy for New Payment Models. Objectives. Common Acronyms
 Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence
 PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Rachel Brunt, RN, BSN, MBA-HCA, CIC, CPHQ, Director Quality Jessie Hanks, BS, RHIA, Director HIM Lafayette General
PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Rachel Brunt, RN, BSN, MBA-HCA, CIC, CPHQ, Director Quality Jessie Hanks, BS, RHIA, Director HIM Lafayette General
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health
 Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING
 HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Involving Patients and Families to Improve Care Transitions
 Involving Patients and Families to Improve Care Transitions Julius Yang, MD, PhD Director of Inpatient Quality Sarah Moravick, MBA QI Project Manager 1 Overview of Today s Discussion 1. BIDMC s burning
Involving Patients and Families to Improve Care Transitions Julius Yang, MD, PhD Director of Inpatient Quality Sarah Moravick, MBA QI Project Manager 1 Overview of Today s Discussion 1. BIDMC s burning
Redesigning the Role of the RN in Case Management: Impact on HCAHPS and Readmission Rates Session C093. Mercy Health System 09/10/15
 Redesigning the Role of the RN in Case Management: Impact on HCAHPS and Readmission Rates Session C093 2015 ANCC National Magnet Conference Friday October 9th 2015 8:00 a.m. Debra Potempa MSN, RN, NEA
Redesigning the Role of the RN in Case Management: Impact on HCAHPS and Readmission Rates Session C093 2015 ANCC National Magnet Conference Friday October 9th 2015 8:00 a.m. Debra Potempa MSN, RN, NEA
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Quality, Cost and Business Intelligence in Healthcare
 Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
Exploring the Possibilities with MIDAS+ SmartConnect
 June 1 3, 2009 Westin La Paloma Resort Tucson, Arizona Exploring the Possibilities with MIDAS+ SmartConnect Leverage your existing MIDAS+ Care Management tools and consider automating your transition planning
June 1 3, 2009 Westin La Paloma Resort Tucson, Arizona Exploring the Possibilities with MIDAS+ SmartConnect Leverage your existing MIDAS+ Care Management tools and consider automating your transition planning
Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle.
 Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Systems serving as alpha sites committed to implementation
Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Systems serving as alpha sites committed to implementation
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Advocate Medical Group and Advocate BroMenn Medical Center Comprehensive Care Program/ Readmission Risk Program
 Creating Clinically Integrated Health System-Based Medical Groups Collaborative Case Study Advocate Medical Group and Advocate BroMenn Medical Center Comprehensive Care Program/ Readmission Risk Program
Creating Clinically Integrated Health System-Based Medical Groups Collaborative Case Study Advocate Medical Group and Advocate BroMenn Medical Center Comprehensive Care Program/ Readmission Risk Program
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
CAHPS Focus on Improvement The Changing Landscape of Health Care. Ann H. Corba Patient Experience Advisor Press Ganey Associates
 CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Care Transitions The most interesting things happen in doorways --Inferno, Dan Brown. The Triple Aim through the Lens of Care Transitions
 Care Transitions The most interesting things happen in doorways --Inferno, Dan Brown An Under recognized Key to Improving Transitional Care: Feedback Loops Eric A. Coleman, MD, MPH But Dr. Coleman, we
Care Transitions The most interesting things happen in doorways --Inferno, Dan Brown An Under recognized Key to Improving Transitional Care: Feedback Loops Eric A. Coleman, MD, MPH But Dr. Coleman, we
CMS AMI and CABG Bundled Payment Initiative AMGA HF Collaborative December 13, 2016
 CMS AMI and CABG Bundled Payment Initiative AMGA HF Collaborative December 13, 2016 Agenda Collaborative Learnings HF Correlation to AMI and CABG Bundled Payments CMS AMI & CABG Bundled Payment Programs
CMS AMI and CABG Bundled Payment Initiative AMGA HF Collaborative December 13, 2016 Agenda Collaborative Learnings HF Correlation to AMI and CABG Bundled Payments CMS AMI & CABG Bundled Payment Programs
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Public Policy and Health Care Quality. Readmissions: Taking Progress into the Future
 Public Policy and Health Care Quality Readmissions: Taking Progress into the Future Today s Agenda The Current State -- The Hospital Readmissions Reduction Program What Have We Learned? Polish Up the Crystal
Public Policy and Health Care Quality Readmissions: Taking Progress into the Future Today s Agenda The Current State -- The Hospital Readmissions Reduction Program What Have We Learned? Polish Up the Crystal
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Post Acute Care Strategies Do we Own? Buy? Partner? Jan Hamilton-Crawford, FACHE Vice President of Operations
 Post Acute Care Strategies Do we Own? Buy? Partner? Jan Hamilton-Crawford, FACHE Vice President of Operations 3 Shared Definitions Connecting the Dots CHRISTUS Continuing Care CHRISTUS Continuing Care
Post Acute Care Strategies Do we Own? Buy? Partner? Jan Hamilton-Crawford, FACHE Vice President of Operations 3 Shared Definitions Connecting the Dots CHRISTUS Continuing Care CHRISTUS Continuing Care
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives"
 2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Creating a Data-Driven Culture to Right-Size Capacity and Enhance Quality and Safety
 Creating a Data-Driven Culture to Right-Size Capacity and Enhance Quality and Safety MaryPat Sullivan, CNO and Chief Experience Officer, Overlook Medical Center, Atlantic Health System, Summit, NJ Jacalyn
Creating a Data-Driven Culture to Right-Size Capacity and Enhance Quality and Safety MaryPat Sullivan, CNO and Chief Experience Officer, Overlook Medical Center, Atlantic Health System, Summit, NJ Jacalyn
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
A New Clinical Operating Model Transforms Care Delivery and Improves Performance
 A New Clinical Operating Model Transforms Care Delivery and Improves Performance The Unified Clinical Organization (UCO) Paul Conlon, PharmD, JD SVP, Clinical Quality and Patient Safety, Trinity Health
A New Clinical Operating Model Transforms Care Delivery and Improves Performance The Unified Clinical Organization (UCO) Paul Conlon, PharmD, JD SVP, Clinical Quality and Patient Safety, Trinity Health
Improving Care Transitions
 Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Using benchmarking to improve Quality
 Using benchmarking to improve Quality Bent Grubb Laursen, MD, Physician lead, Accenture Denmark @ DocBlogIt DANISH HEALTHCARE SYSTEM IS BETTER THAN THE SWEDISH HEALTHCARE SYSTEM Pride Complacency Insult
Using benchmarking to improve Quality Bent Grubb Laursen, MD, Physician lead, Accenture Denmark @ DocBlogIt DANISH HEALTHCARE SYSTEM IS BETTER THAN THE SWEDISH HEALTHCARE SYSTEM Pride Complacency Insult
Intelligence. Intelligence. Workload forecasting with Cerner Clairvia. Workload forecasting with Cerner Clairvia
 Intelligence Intelligence Workload forecasting with Cerner Clairvia Workload forecasting with Cerner Clairvia Better patient outcomes occur when you have the right care giver, in the right place, at the
Intelligence Intelligence Workload forecasting with Cerner Clairvia Workload forecasting with Cerner Clairvia Better patient outcomes occur when you have the right care giver, in the right place, at the
Nielsen ICD-9. Healthcare Data
 Nielsen ICD-9 Healthcare Data Healthcare Utilization Model The Nielsen healthcare utilization model has three primary components: demographic cohort population counts, cohort-specific healthcare utilization
Nielsen ICD-9 Healthcare Data Healthcare Utilization Model The Nielsen healthcare utilization model has three primary components: demographic cohort population counts, cohort-specific healthcare utilization
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Analytics in Action. Using Data to Improve Care and Reduce Costs CUSTOM MEDIA SPONSORED BY
 Analytics in Action Using Data to Improve Care and Reduce Costs CUSTOM MEDIA SPONSORED BY Imagine an 82-year-old gentleman walks in to your emergency department. He presents with a productive cough and
Analytics in Action Using Data to Improve Care and Reduce Costs CUSTOM MEDIA SPONSORED BY Imagine an 82-year-old gentleman walks in to your emergency department. He presents with a productive cough and
Creating Data-driven Strategies to Improve Hospital Outcomes
 Annual National Institute October 16, 2014 Creating Data-driven Strategies to Improve Hospital Outcomes A Case Manager s Guide Information Data Knowledge 1 2014 Conifer Health Solutions, LLC. All Rights
Annual National Institute October 16, 2014 Creating Data-driven Strategies to Improve Hospital Outcomes A Case Manager s Guide Information Data Knowledge 1 2014 Conifer Health Solutions, LLC. All Rights
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM. CHRISTUS Spohn Hospital Corpus Christi
 TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 CHRISTUS Spohn Hospital Corpus Christi Delivery System Reform Incentive Payment (DSRIP) Projects Category
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 CHRISTUS Spohn Hospital Corpus Christi Delivery System Reform Incentive Payment (DSRIP) Projects Category
Transitions of Care. Scott Clark, President Leading Edge Health Care
 Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
2017/18 Quality Improvement Plan
 2017/18 Improvement Plan Aim Change Enough information at discharge. Readmissio ns CHF Readmissio ns COPD Did you receive enough information from hospital staff about what to do if you were worried about
2017/18 Improvement Plan Aim Change Enough information at discharge. Readmissio ns CHF Readmissio ns COPD Did you receive enough information from hospital staff about what to do if you were worried about
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017
 Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
2017 Quality Improvement Work Plan Summary
 Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Episode Payment Models Final Rule & Analysis
 Episode Payment Models Final Rule & Analysis February 15, 2017 Agenda Overview Changes from Proposed Rule Categorization of Episodes Episode Attribution Reconciliation Quality Performance Cardiac Rehab
Episode Payment Models Final Rule & Analysis February 15, 2017 Agenda Overview Changes from Proposed Rule Categorization of Episodes Episode Attribution Reconciliation Quality Performance Cardiac Rehab
Hendrick Center for Extended Care. Community Health Needs Assessment Implementation Plan
 Hendrick Center for Extended Care Community Health Needs Assessment Implementation Plan - 2014-2016 Overview: Hendrick Center for Extended Care ( HCEC ) is a Long Term Acute Care Hospital, within Hendrick
Hendrick Center for Extended Care Community Health Needs Assessment Implementation Plan - 2014-2016 Overview: Hendrick Center for Extended Care ( HCEC ) is a Long Term Acute Care Hospital, within Hendrick
Driving Business Value for Healthcare Through Unified Communications
 Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
Accountable Care Organizations Creating A Culture Of Engaged Physicians
 Accountable Care Organizations Creating A Culture Of Engaged Physicians Judith Miller, VP Medical Services & CI Advocate Physician Partners August 14, 2014 1 Sites Of Care Advocate Health Care 13 Hospitals
Accountable Care Organizations Creating A Culture Of Engaged Physicians Judith Miller, VP Medical Services & CI Advocate Physician Partners August 14, 2014 1 Sites Of Care Advocate Health Care 13 Hospitals
Central Valley/West Valley Care Coordination Coalitions. Quarterly Community Meeting
 Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting
 Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting Chris Kane SVP, Strategic Business Development WellStar
Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting Chris Kane SVP, Strategic Business Development WellStar
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Value Based Care An ACO Perspective
 Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
How Allina Saved $13 Million By Optimizing Length of Stay
 Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
The Challenges and Opportunities in Using Data Bundled Payment, Care Improvement
 The Challenges and Opportunities in Using Data Bundled Payment, Care Improvement Helen Macfie, Pharm.D., FABC For IHI Leading Population Heath Transformation February, 2017 It started with a project PHYSICIAN
The Challenges and Opportunities in Using Data Bundled Payment, Care Improvement Helen Macfie, Pharm.D., FABC For IHI Leading Population Heath Transformation February, 2017 It started with a project PHYSICIAN
Objectives. Assisted Living. O 2 : Opportunities & Outcomes in Assisted Living. Presented by: Chief Clinical Officer
 O 2 : Opportunities & Outcomes in Assisted Living Presented by: Leigh Ann Frick, PT, MBA Chief Clinical Officer Melissa Moffitt, MS, CCC-SLP Senior Vice President of Senior Living Objectives Identify the
O 2 : Opportunities & Outcomes in Assisted Living Presented by: Leigh Ann Frick, PT, MBA Chief Clinical Officer Melissa Moffitt, MS, CCC-SLP Senior Vice President of Senior Living Objectives Identify the
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Improving the Health of Our Patients and Our Communities:
 Jason Jones, PhD Executive Director Kaiser Permanente, Southern California Patti Harvey, RN, MPH, CPHQ Senior Vice President Kaiser Permanente, Southern California Improving the Health of Our Patients
Jason Jones, PhD Executive Director Kaiser Permanente, Southern California Patti Harvey, RN, MPH, CPHQ Senior Vice President Kaiser Permanente, Southern California Improving the Health of Our Patients
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
Turning Big Data Into Better Care
 Turning Big Data Into Better Care Dickson Advanced Analytics DA 2 Who is CHS and What is DA 2? 2 Who is CHS? Hospitals 42 Employees 62K Care Centers 900+ Physicians 3K Licensed Beds 7,800 Nurses 14K 3
Turning Big Data Into Better Care Dickson Advanced Analytics DA 2 Who is CHS and What is DA 2? 2 Who is CHS? Hospitals 42 Employees 62K Care Centers 900+ Physicians 3K Licensed Beds 7,800 Nurses 14K 3
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM. Jackson Healthcare Center
 TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Jackson Healthcare Center Delivery System Reform Incentive Payment (DSRIP) Projects Category 1 DSRIP
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Jackson Healthcare Center Delivery System Reform Incentive Payment (DSRIP) Projects Category 1 DSRIP
Quality and Health Care Reform: How Do We Proceed?
 Quality and Health Care Reform: How Do We Proceed? Susan D. Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Dean of Clinical Affairs Quality and Patient Safety Associate Professor
Quality and Health Care Reform: How Do We Proceed? Susan D. Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Dean of Clinical Affairs Quality and Patient Safety Associate Professor
Advocate Physician Partners approach to Population Health
 Advocate Physician Partners approach to Population Health Don Calcagno President, Advocate Physician Partners March 9, 2016 Who are Advocate Health Care and Advocate Physician Partners? 1 Advocate Health
Advocate Physician Partners approach to Population Health Don Calcagno President, Advocate Physician Partners March 9, 2016 Who are Advocate Health Care and Advocate Physician Partners? 1 Advocate Health
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE)
") MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.2 November 13, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility,
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.2 November 13, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility,
CKHA Quality Improvement Plan (QIP) Scorecard
 Scorecard") CKHA Quality Improvement Plan () Scorecard 217-18 Quality dimension Performance Indicator 217-18 Performance Goals results where available Current Value Page Safety Medication Reconciliation completed
CKHA Quality Improvement Plan () Scorecard 217-18 Quality dimension Performance Indicator 217-18 Performance Goals results where available Current Value Page Safety Medication Reconciliation completed
Quality Based Impacts to Medicare Inpatient Payments
 Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS 4/19/2016. April 20, 2016
 HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
Hank Fanberg Manager of Research & Development. Dan Castillo, MHA, FACMPE, CHE Program Administrator
 Technology and the Uninsured: Increasing Access and Coordinating Care Doing the Impossible Leveraging Technology to Reduce Costs and Improve the Quality of Care for the Uninsured COUNTY OF ORANGE HEALTH
Technology and the Uninsured: Increasing Access and Coordinating Care Doing the Impossible Leveraging Technology to Reduce Costs and Improve the Quality of Care for the Uninsured COUNTY OF ORANGE HEALTH
& Reward. Opportunity, Risk. HealthPRO Heritage National healthcare solutions firm specializing in Care ReDesign for top of market clients 9/5/2018
 Opportunity, Risk & Reward Care Redesign Cross Continuum Connections Built on a Foundation of Clinical Innovation Elisa Bovee, MS OTR/L, Vice President of Clinical Strategies 2017 LeadingAge New York Annual
Opportunity, Risk & Reward Care Redesign Cross Continuum Connections Built on a Foundation of Clinical Innovation Elisa Bovee, MS OTR/L, Vice President of Clinical Strategies 2017 LeadingAge New York Annual
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE)
") MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.0 October 10, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility, functionality,
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.0 October 10, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility, functionality,
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Post Acute Medical. Debra R Riegel, RN. Presented to: American Hospital Association
 Post Acute Medical Debra R Riegel, RN Presented to: American Hospital Association 1 Introduction Debra R Riegel, RN, CRNP, MSN, CPC- Corporate Director of Appeals Management Post Acute Medical October
Post Acute Medical Debra R Riegel, RN Presented to: American Hospital Association 1 Introduction Debra R Riegel, RN, CRNP, MSN, CPC- Corporate Director of Appeals Management Post Acute Medical October
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution