Application for the Medical Venturing Program
|
|
|
- Collin Cook
- 6 years ago
- Views:
Transcription





1 Huntsville Hospital Corporate University Phone Fax Application for the Medical Venturing Program Medical Venturing Paperwork Required for Processing: Completed Application, which includes the following forms: Application/ Badge Form Completed HIPAA Test Affirmation Statement Form Hold Harmless Form Dress & Appearance Policy Form Medical Test Required: Current TB Skin Test (less than one year old) Note: It takes 48 hours to complete this test, see page 2 of the application for more details Photography Release Form May 2017 Page 1 of 11
2 Dear Participant, Thank you for sharing your interest in Huntsville Hospital s Medical Venturing Program through Corporate University. Medical Venturing provides students with opportunities to experience guest speakers, discussion groups, tours, and demonstrations from professionals serving in various healthcare fields. Huntsville Hospital s Post 630 is a partnership with Boy Scouts of America and membership includes both young men and women. Post 630 is the only Venturing Post in the region focusing on hospital-based healthcare. Participants do not to take part in hands-on patient care. There are a few key facts about the Medical Venturing Program that you need to know: 1. Eligibility Participants must be, at a minimum, High School juniors or seniors in order to be eligible to participate. The minimum age to participate in the program is 15 years of age. 2. Pre-requisites for Participation in the Program Prior to beginning the Medical Venturing experience applicants must provide the following to Corporate University: A completed Medical Venturing Application. The application form includes several sections that must be complete and signed. If a student has previously participated in Medical Venturing, a new application and dues payment is required each year. Boy Scouts of America Application A HIPAA (Health Insurance Portability and Accountability Act) Test An Affirmation Statement A Hold Harmless Form A Dress and Appearance Policy Form A Current, Negative Tuberculin (TB) skin test from your doctor or student health center is also required. The test should be read within a year to be valid. Please note, the TB Skin test process takes 48 hours between the TB injection and the reading by a physician. Include the certificate of results from your family physician or other primary care provider. For a $20 fee, the Occupational Health Group is another local resource for TB skin testing (located inside the Medical Mall at Governors Drive). Submit dues of $35 by cash or personal check made payable to: Huntsville Hospital Corporate University Photography Release Form 3. Meetings Youth participating in Medical Venturing meetings will have completed the Pre-requisites listed above. Medical Venturers meet once per month, from September to May, from 6-7:30pm. Venturing resembles a club where members are not only learning about healthcare careers, they are cultivating a network of friends from other high schools and home schools. Participants should plan to attend six (6) of the nine (9) meetings scheduled in order to receive a certificate of participation. Meetings begin promptly at 6:00 p.m. Plan to arrive on time so speakers and/or tours will have sufficient time to cover all that is planned. Meetings end at 7:30p.m. Two adult advisors will be present during each meeting, along with the scheduled speaker. Parents/guardians providing transportation are asked to pick-up Venturers, from The Dowdle Center lobby, at 7:30 pm Parking is located off Longwood Drive, behind the Governors Medical Tower-Spine & Neurosurgery Center. Applicants need to submit their completed Medical Venturing Application, completed Boy Scouts of American Application, current TB Skin Test, and $35 dues to Corporate University s Medical Venturing Program contact, Rosita Karigan. Once we receive your completed paperwork you will be notified by of your first meeting and topic. Packets can be dropped-off at the Dowdle Center, 109 Governor's Drive, faxed to (256) , or mailed to our office at the following address: Attention: Rosita Karigan Huntsville Hospital s Corporate University P.O. Box 1167; Huntsville, AL If you have any questions contact us by phone at (256) or at rosita.karigan@hhsys.org. We look forward to helping you explore your career options in healthcare, and hope your experience will be rewarding. Regards, Rosita Karigan May 2017 Page 2 of 11
3 Medical Venturing Application Deliver to Corporate University located in the Dowdle Center at 109 Governors Drive or return by fax: (256) Name (Please print clearly): (Minimum Age to participate is 15) How Old Are You? Birth date: / / Day Month Year Name of High School (or Home School): Check your class year Sophomore Junior Senior Graduation Year: 20 If Applicant is under the age of 18, Office Use: Completed Requirements: Affirmation Statement TB Skin Test Application Form Boy Scout Application HIPAA Test Photo Release TB Skin Test Expires: / / Receipt Sent Entered in Spreadsheet Scanned Immunizations; in the last year I have: Had a flu shot; Date / / Have not gotten a flu shot Home Address: City: State: Zip Code: Preferred Phone#: ( ) address: Name of Parent/Guardian & Relationship: Cell Phone # of Parent/Guardian: Parent/Guardian s address: Name the Health Care profession(s) you are interested in learning about during your Medical Venturing experience: Choice 1.) Choice 2.) Choice 3.) Medical Venturing meetings are held Tuesday nights, once a month, during the months of September through May. Youth are asked to attend six (6) meetings out of the nine (9) meetings scheduled Meeting Dates: 2018 Meeting Dates: September 19 October 17 November 21 January 16 February 20 March 20 December 19 April 17 (Please check all the months available) May 15 (Please check all the months available) Badge: Students will be assigned a badge to wear during Medical Venturing meetings. The badge is only valid during meetings and should be turned in once the meeting has ended. Medical Venturers will be escorted and wear their badge at all times on campus I have read and understand the cover letter & application information. Parking: If you are a participant on the Huntsville Hospital campus, the designated parking surface lot is west of the Governors Medical Tower, located off of Governor s Drive. If a participant fails to follow the parking guidelines, and does not park in the designated lot, fines are $50.00 for 1 st offense and $ for 2 nd offense. Candidate Signature: Date Submitted: (Signature verifies that the participant has read the above statement & understands the guidelines for Medical Venturing Program.) May 2017 Page 3 of 11
4 Youth Membership Form This form is read by machine. Please print the numbers and letters as shown in the sample application. Unit type: Cub Scout Boy Scout Varsity Scout Venturing Sea Scout (Fill in the circle.) Pack Troop Team Crew Ship Lone Cub Scout Lone Boy Scout YOUTH For pack registration select one: Tiger Club Cub Scout Webelos Scout Arrow of light earned MEMBERSHIP Mark here if new to Scouting. Former Scout Former Venturer Former Sea Scout If applicant has an unexpired membership certificate, registration may be accomplished in this unit by paying $1 for processing the transfer. Mark and attach certificate. It will be returned by the council. Transfer application Unit Number: Transfer from council number: Unit Type: Pack Troop Team Crew Ship Unit Number: Enter membership number from unexpired certificate: Name and address information (Please print one letter in each space.) First name (No initials or nicknames) Middle Name Last name Suffix Mailing Address City State Zip code Home Phone Date of birth (mm/dd/yyyy) Grade - - / / Ethnic background: School African American Native American Alaska Native Asian Caucasian/White Hispanic/Latino Pacific Islander Other Gender: Male Female Boys Life Subscription Parent/guardian information Mark here if address is the same as above. I commit to be an active ScoutParent. Mark here if you are the Tiger Cub adult partner. Mark here if the adult partner/scoutparent is not living at the same address; complete and attach an adult application. Select relationship: Parent Guardian Grandparent Other (specify) First name (No initials or nicknames) Middle Name Last name Suffix Mailing Address City State Zip code Home Phone Date of birth (mm/dd/yyyy) Occupation Employer Gender: - - / / M F Business Phone Ext. Previous Scouting experience Cell phone Parent/guardian address I have read the attached information sheet and approve the application (signature of parent/guardian required if applicant is under 18 years of age). Signature of Parent/Guardian / / Signature of unit leader (or designee) Date Signature of Venturer Registration fee $. Boys Life fee $. May 2017 Page 4 of 11
5 HIPAA Fundamentals Training Introduction - At Huntsville Hospital, privacy of patient information has always been considered a basic right. - What can happen when protected health information is inadvertently exposed? Personal harm to individuals, embarrassment, community mistrust, lawsuits, etc What is HIPAA - HIPAA stands for Health Insurance Portability and Accountability Act. HIPAA is a relatively new federal law that protects Protected Health Information, or PHI. - The law allows for penalties such as fines and/or prison for people caught violating patient privacy. - HIPAA Privacy Regulations became effective in April 2003 and the Security Regulation in April Part of our compliance with the HIPAA law is to provide the required awareness training for employees and workforce members. Protected Health Information - Protected Health Information (PHI) is about patient information whether it is spoken, written, or on the computer. It includes health information about our patients. It can be information as simple as their name. - Certainly we can share PHI when it is part of our job to do so, but beyond that you may have broken the law if you share patient information. Need to Know - A good way to determine if you should share patient data is to ask yourself Do I or others need this information to do the job? Use this little test before you look at patient information or share it with others. - Sometimes you may inadvertently hear or see information that you don t need to know. If so, just keep it to yourself. Dispose of PHI Properly - Trash and garbage bins are another place that might contain PHI. Be sure to dispose of patient lists and other documents that contain PHI in non-public areas. - If you see PHI in the trash in public areas, notify the supervisor immediately. - If you transport PHI, make sure it is secure when not in your sight, such as a locked vehicle. The Privacy Officer - At HH we have a person responsible for insuring that privacy is maintained The Privacy Officer. However, no one person can know if we have a possible threat in every area of such a large organization. - Each of us must do our part to protect patient information. You should always report possible privacy problems to the manager in your area or to the Privacy Officer. Co-Workers, Friends, and Family Situation: You hear about a friend that has had surgery, so you call a nurse on that floor to find out the details. - Friends and co-workers deserve the right to privacy just like any other patient. You cannot seek or share patient information for personal reasons. You may only obtain/share information that you need to know to do your job. - You may personally ask the individual you know about their condition, and it is their choice what to share with you. - You may also ask their permission to share their information with a common friend, but you should never do this without their permission. Don t be Curious Situation: You like to look at the patient directory or surgery schedule daily to see if you know anyone. - This is not within the scope of your job at this hospital. - You are in violation of HIPAA laws and Huntsville Hospital policies. Respect the Privacy of Patients Situation: You are working in an area where caregivers are discussing health information with a patient, a family member, or another caregiver. - You can ask if you need to leave the area. - You may quickly finish your task and leave. - You must keep any health information you overhear to yourself. Protect information in your Possession Situation: In the process of doing your job, you use a list that contains patient names and possibly other patient information. - You should keep the information in your possession at all times. - You should make sure that it is protected from others who would not need the information. - You can turn it over so the information can t be viewed. - You should make sure when you are finished with the information that you have disposed of it properly. - Your supervisor may give you instructions for disposal of PHI. HIPAA Fundamentals Test This completes the fundamental overview of the HIPAA regulations. You now know and are responsible for what is required of you as an employee of Huntsville Hospital. - HIPAA laws also require that we keep a record to show that you have been trained in patient privacy. You should now take the HIPAA FUNDAMENTALS TEST. May 2017 Page 5 of 11
6 Medical Venturing Program HIPAA Fundamentals Test Name 1. HIPAA stands for: a. Health Information Protection Agency Association b. Human Instinct Protection Association Awareness c. Health Insurance Portability and Accountability Act 2. PHI stands for: a. Patient Health Initiatives b. Personal Health Institute c. Protected Health Information 3. The Privacy HIPAA law became effective: a. As soon as everyone in our hospital is trained b. April 2002 c. April 2003 d. December Patient Information is protected when it is: a. Spoken b. Written c. On the computer d. All of the above 5. If you are in a public area and you see PHI in the trash, you should: a. Report this to a supervisor b. Dispose of it properly c. Show it to a friend d. Both a. & b. Date 6. The Privacy Officer is responsible for: a. Checking the trash b. Pulling medical records of patients c. Making sure Huntsville Hospital protects patient information 7. You should ask yourself before you view or share patient information: a. Is this a personal friend or a relative not under my care? b. Will anyone see me reading this? c. Do I need this to do my job at Huntsville Hospital? 8. Patient information that I use for my job: a. Isn t important to anyone else b. Should be protected until I have disposed of it properly c. Is the responsibility of my manager 9. If I want to know about a friend that I see in the hospital, I should: a. Look at their medical record b. Ask the nurse c. Ask the individual 10. If you see another person violating the HIPAA Privacy Laws or the HH Policies: a. You should ask them to stop b. Ignore it and mind your own business c. Report it to your manager or the privacy office ( ) May 2017 Page 6 of 11
7 Medical Venturing Program Affirmation Statement on Security & Privacy of Information HIPAA Fundamentals HIPAA stands for Health Insurance Portability and Accountability Act. HIPAA is a federal law that was enacted in 2003, which protects Protected Health Information or PHI for patients. The law allows for penalties such as fines and/or prison for people caught violating patient privacy. Protected Health Information, or PHI, is any patient information whether it is spoken, written, or on the computer. PHI includes health information about patients in the hospital, and it can be as simple as their name. PHI cannot be shared outside of the hospital, even if you see the information in a public area like the trash. If witness PHI being shared, it needs to be reported to Huntsville Hospital s Privacy Officer at Affirmation Statement I, the undersigned, have read and understand the Huntsville Hospital policy on confidentiality of protected health information as described in the HIPAA Fundamentals Policy, which is in accordance with applicable state or federal law. I also acknowledge that I am aware of and understand the policies of Huntsville Hospital regarding the security of protected health information including the policies relating to the use, collection, disclosure, storage and destruction of protected health information. This protection includes proprietary information. In consideration of my employment or association with Huntsville Hospital, and as an integral part of the terms and conditions of my employment or association, I hereby agree, pledge and undertake that I will not at any time, during my employment or association with Huntsville Hospital, or after my employment or association ends, access or use protected health information, or reveal or disclose to any persons within or outside Huntsville Hospital, any protected health information except as may be required in the course of my duties and responsibilities and in accordance with applicable legislation and policies governing proper release of information. I understand that user identification codes and passwords are not to be disclosed (or shared), nor should any attempt be made to learn or use another employee s code. If I am an instructor, I understand that I assume responsibility for the actions of the students under my supervision to comply with the Security and Privacy of Information Policy. If I am an employer, I understand that I assume responsibility for the actions of my employees to comply with the Security and Privacy of Information Policy. Training: Members of the workforce receive required education concerning security and privacy during new Employee Orientation and during annual required training or upon commencement of the association. Any updates or changes to policies will be communicated via staff meetings, intranet and/or mandatory requirements tests. Corporate Compliance: It is the responsibility of all employees and those associated with Huntsville Hospital to uphold all applicable laws and regulations. All employees must develop an awareness of the legal requirements and restrictions applicable to their respective positions and duties. The hospital has a corporate compliance program to further such awareness and to monitor and promote compliance with such laws and regulations. I am not aware of any violations of applicable laws or regulations and agree to report any violations to the Corporate Compliance Officer. Any questions about the legality or propriety of actions undertaken on or behalf of the Hospital should be referred immediately to the appropriate supervisory personnel, or to the Corporate Compliance Officer. Excluded Party Status: I affirm that I am not an excluded party from participating in Federal health programs, nor am I under investigation which may lead to such sanctions. Computer Applications: I further understand that I may be provided access to certain hardware and software applications, some of which may be proprietary to their respective vendors. I agree to keep the hardware and software applications confidential, to not disclose to third parties, and to use such hardware and software applications only for the benefit of Huntsville Hospital. I understand that violation of this affirmation statement could result in me not being able to participate in Medical Venturing. PRINT NAME: School or Organization Name (if applicable): SIGNATURE: X DATE: WITNESS SIGNATURE: X DATE: 04/2002, 12/2004, 1/2010 May 2017 Page 7 of 11
8 The Healthcare Authority of the City of Huntsville d/b/a Huntsville Hospital WAIVER OF LIABILITY AND HOLD HARMLESS AGREEMENT 1. In consideration for receiving permission to participate in Huntsville Hospital s Job Shadowing, Medical Venturing, or Internship or other Healthcare Observation Program (hereafter referred to as the Program ), I hereby release, waive, discharge and covenant not to sue Huntsville Hospital, its officers, servants, agents and employees (hereinafter referred to as "releasees") from any and all liability, claims, demands, actions and causes of action whatsoever arising out of or relating to any loss, damage or injury, including death, that may be sustained by me, or to any property belonging to me, whether caused by the negligence of the releasees, or otherwise, while participating in the Program, or while in, on or upon the premises where the Program is being conducted, while in transit to or from the premises, or in any place or places connected with the Program. 2. I am fully aware of risks and hazards connected with being on the premises and participating in the Program, and I am fully aware that there may be risks and hazards unknown to me connected with being on the premises and participating in the Program, and I hereby elect to voluntarily participate in the Program, to enter upon the above named premises and engage in activities knowing that conditions may be hazardous, or may become hazardous or dangerous to me and my property. I voluntarily assume full responsibility for any risks of loss, property damage or personal injury, including death, that may be sustained by me, or any loss or damage to property owned by me, as a result of my being a participant in the Program, whether caused by the negligence of releasees or otherwise. 3. I further hereby agree to indemnify and save and hold harmless the releasees and each of them, from any loss, liability, damage or costs they may incur due to my participation in the Program, whether caused by the negligence of any or all of the releasees, or otherwise. 4. It is my express intent that this Release shall bind the members of my family and spouse, if I am alive, and my heirs, assigns and personal representative, if I am deceased, and shall be deemed as a Release, Waiver, Discharge and Covenant Not to Sue the above named releasees. In signing this release, I acknowledge and represent that: A. I have read the foregoing release, understand it, and sign it voluntarily as my own free act and deed; B. No oral representation, statements or inducements, apart from the foregoing written agreement, have been made; C. I, my parent or guardian is at least eighteen (18) years of age and fully competent; D. I execute this Release for full, adequate and complete consideration fully intending to be bound by same. In witness whereof, I have hereunto set my hand and seal this day of, Participant Signature: Name Printed: Parent or Guardian Signature (if participant is under 18 years of age): Name Printed: Witness: Witness Name Printed: May 2017 Page 8 of 11
9 Medical Venturing Program Dress and Appearance Policy Huntsville Hospital s Medical Venturing participants have a responsibility to adhere to the Hospital s dress policy. Therefore, your attire, grooming, and personal hygiene are critically important. We require that you observe the following specific standards regarding personal appearance and neatness while shadowing/observing in the hospital: Clothing/ Attire - Shirts, Blouses, Dresses & Skirts Students should wear shirts, blouses or dresses with sleeves. Sleeves may be short (to the midbicep) or long sleeved. No sheer or sleeveless tops are permitted and no plunging necklines or cleavage should be showing. Lengths of dresses and skirts cannot be shorter than three inches above the knee. Dresses or skirts should not be clinging or tight. - Undergarments Lingerie, t-shirts or briefs should be covered by clothing. - Pants No shorts, blue jeans or work-out/sports clothing. Pants and tops should not reveal the midriff or back area. - Hair is to be clean, well groomed, and a natural color (i.e. no pink, orange, blue). No distracting extremes in hair styling, dyeing, bleaching, or coloring is permitted. Shaving designs into the hair and Mohawks are not permitted. Hair and hair accessories must not be distracting or extreme. Hair below shoulder length should be confined if it falls forward over the face. - Hosiery Students should wear complementary socks or hosiery. - Shoes Clean, closed-toe shoes should be worn with the heel not exceeding 3 high. - Scrubs Some locations may require participants to wear scrubs. Participants will be informed if scrubs are required for their area. Jewelry/ Adornment - Fingernails - Students should not have artificial nails (which include acrylic/gel overlays, acrylic/gel nails, wraps, tips, and nail strengthener or hardener that is not removable by acetone. Fingernails should not exceed ¼ inch from the tip of their finger or have extreme nail art, or colors like black or orange. - Earrings - No more than two earrings per earlobe are allowed. Earrings must not be larger than a quarter and are not permitted on the top of the ear or in the cartilage above the earlobe. - Rings - No more than two rings per hand are allowed. - Bracelets and Necklaces - Two necklaces and two bracelets are permitted. - Body Piercing - Visible body piercing other than earrings is not permitted; this includes tongue piercing and forking, eyebrow piercing, and nose rings. - Tattoos - Applicant should wear clothing that covers tattoos. Hygiene - Personal Hygiene is considered very important. Showering and the use of antiperspirant/ deodorant is required. - Strong perfume or fragrances of any kind are not permitted. All fragrances are discouraged. - Smoking is not permitted on the Hospital campus. Those using tobacco products must take measures to eliminate smoke odor from clothing, skin, and breath. The Dress and Appearance Policy applies to Medical Venturing participants who are wearing a Hospital badge. I have read and understand the Dress and Appearance policy. I understand that if I come to a Medical Venturing Program meeting in violation of this policy, I will not be allowed to remain for the program, and will not receive credit for attendance. Print Name: Signature: Date: / / May 2017 Page 9 of 11
10 CONSENT TO PHOTOGRAPH Marketing & Public Relations Authorization for Filming or Recording Release Form I authorize the release of the initialed item below to be disclosed in the manner described: I agree to grant an interview with, and/or to be photographed, videotaped, or recorded by a representative of print or broadcast media, and I understand that my information, image and/or voice may appear in print or broadcast media. I agree to grant an interview with, and/or to be photographed, videotaped, or recorded representative of Huntsville Hospital and I understand that my information, image and/or voice may appear in Huntsville Hospital promotional or educational material (advertisement, publication, video, web site, etc.). PHOTOGRAPHED EVENT: I agree to grant an interview and/or to be photographed, videotaped, recorded by a representative of law enforcement, public health or social service agency. I understand that I (will, will not) be identified by name and that protected health information (will, will not) be shared with the person performing filming or recording. The purpose for the use/disclosure of this information is: Cooperation with request from media Education of health care professionals Hospital publicity or public education Investigation of a possible crime Other I understand that I have the right to revoke this authorization at any time. I understand that if I revoke this authorization, I must do so in writing and present my written revocation to Huntsville Hospital Marketing Department. I understand that revocation will not apply to information that has already been released in response to this authorization. I also understand that authorizing the disclosure of this information is voluntary. I can refuse to sign this authorization. I need not sign this authorization in order to assure treatment. I understand that I may inspect or obtain a copy of the information to be used or disclosed. I understand that any disclosure of information carries with it the potential for an unauthorized re-disclosure and the information may not be protected by federal confidentiality rules. PRINT NAME Day Time Phone Number Signature (or Legal Representative) of individual being photographed, etc. Legal Representative s Relationship to Patient Physical Description Consenter Witness DATE: Date Department (if HH Employee) Employee ID# (if HH Employee) Identification of Personal Representative if the patient is unable to authorize: Driver s License Work photo badge Other photo ID Power of attorney documentation The original of this document is to be placed in the patient s medical chart and a copy to be maintained n Marketing & Public Relations (Fax ) May 2017 Page 10 of 11



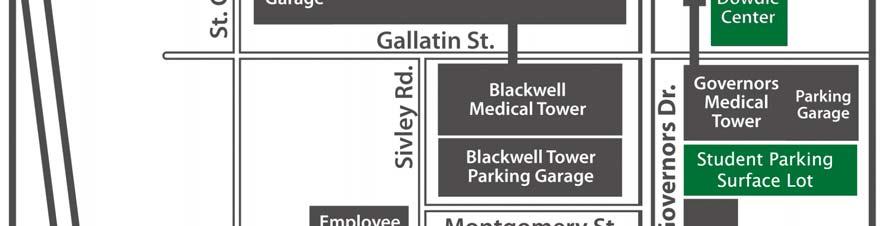
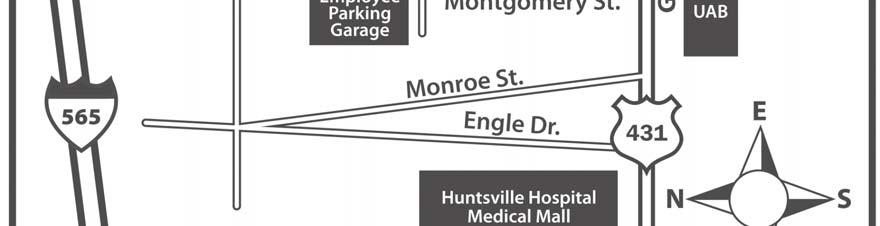
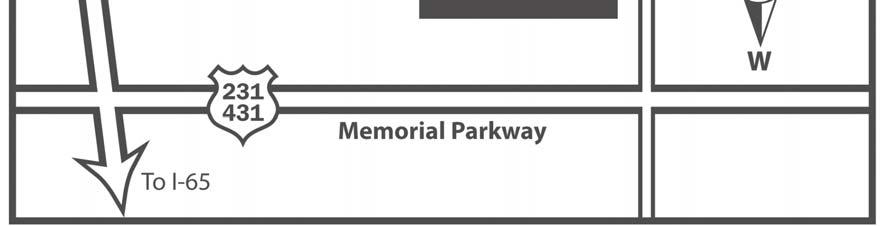
11 Medical Venturing Program Campus Map May 2017 Page 11 of 11
Application for the Job Shadowing/Observation Program
 Huntsville Hospital Corporate University Phone 256-265-8025 Fax 256-265-9417 www.huntsvillehospital.org Application for the Job Shadowing/Observation Program Shadowing Paperwork Submission: Completed Job
Huntsville Hospital Corporate University Phone 256-265-8025 Fax 256-265-9417 www.huntsvillehospital.org Application for the Job Shadowing/Observation Program Shadowing Paperwork Submission: Completed Job
Angelica Srivoraphan Business Development Coordinator Volunteer Services Leader Carolinas Rehabilitation Carolinas HealthCare System
 2015 Dear Shadow Applicant: Thank you for your interest in the shadow program at Carolinas Rehabilitation. The shadow program will be a richly rewarding experience for you and I hope that you will find
2015 Dear Shadow Applicant: Thank you for your interest in the shadow program at Carolinas Rehabilitation. The shadow program will be a richly rewarding experience for you and I hope that you will find
JUNIOR VOLUNTEER SERVICE
 Application is due by April 30 th. Interviews conclude May 18 th Selections made May 31 st Program begins June 4 th Program concludes July 31 st JUNIOR VOLUNTEER SERVICE Thank you for inquiring about the
Application is due by April 30 th. Interviews conclude May 18 th Selections made May 31 st Program begins June 4 th Program concludes July 31 st JUNIOR VOLUNTEER SERVICE Thank you for inquiring about the
Guest Relations for Students
 Guest Relations for Students Guest Relations Tift Regional Health System s (TRHS) culture as an organization and the principles of human relationships by which we operate are reviewed in this program.
Guest Relations for Students Guest Relations Tift Regional Health System s (TRHS) culture as an organization and the principles of human relationships by which we operate are reviewed in this program.
U.S. Army Aeromedical Research Laboratory Gains in the Education of Mathematics and Science Program PARTICIPANT APPLICATION
 To be considered for acceptance into the 2013 GEMS program, submit the following: 1. The Participant Application 2. The Participant Essay 3. The Participant Release Form 4. Participant Safety Information
To be considered for acceptance into the 2013 GEMS program, submit the following: 1. The Participant Application 2. The Participant Essay 3. The Participant Release Form 4. Participant Safety Information
Applicant must have taken the ACT/SAT Test at least once and submit their scores.
 HENDERSON STATE UNIVERSITY SUMMER INSTITUTE STUDENT INFORMATION SHEET Sunday, July 8-Thursday, July 12, 2018 Application deadline for ALL applications is Friday, June 4, 2018 ELIGIBILITY CRITERIA Applicant
HENDERSON STATE UNIVERSITY SUMMER INSTITUTE STUDENT INFORMATION SHEET Sunday, July 8-Thursday, July 12, 2018 Application deadline for ALL applications is Friday, June 4, 2018 ELIGIBILITY CRITERIA Applicant
ADULT APPLICATION IF YOU WOULD LIKE A COPY OF YOUR CRIMINAL BACKGROUND REPORT, PLEASE CONTACT YOUR LOCAL COUNCIL OFFICE.
 ADULT APPLICATION The mission of the Boy Scouts of America is to prepare young people to make ethical and moral choices over their lifetimes by instilling in them the values of the Scout Oath and Law.
ADULT APPLICATION The mission of the Boy Scouts of America is to prepare young people to make ethical and moral choices over their lifetimes by instilling in them the values of the Scout Oath and Law.
REGISTRATION DEADLINE: Feb. 9, 2018
 Richland High School Feb. 17, 2018 REGISTRATION DEADLINE: Feb. 9, 2018 Student Name: Home Address: City: State: Zip: Phone: Email: Date of Birth: Gender: Male Female T-shirt size: Ethnicity (optional):
Richland High School Feb. 17, 2018 REGISTRATION DEADLINE: Feb. 9, 2018 Student Name: Home Address: City: State: Zip: Phone: Email: Date of Birth: Gender: Male Female T-shirt size: Ethnicity (optional):
The Alaska Youth Academy Application
 The Alaska Youth Academy Application Email to katina.charles@tananachiefs.org by June 30 th, 2016 Personal Information Please write in or circle your answer. Name: (First) (Middle) (Last ) Date of Birth
The Alaska Youth Academy Application Email to katina.charles@tananachiefs.org by June 30 th, 2016 Personal Information Please write in or circle your answer. Name: (First) (Middle) (Last ) Date of Birth
PURPOSE: To ensure that all LifeBridge Health employees project a professional image to patients, visitors and guests.
 Policy Title: Facility: Dress Code - LifeBridge LifeBridge Health Effective Date: 7/1/2017 SUMMARY: All LifeBridge Health staff, including residents, staff physicians, volunteers, temporary/agency employees
Policy Title: Facility: Dress Code - LifeBridge LifeBridge Health Effective Date: 7/1/2017 SUMMARY: All LifeBridge Health staff, including residents, staff physicians, volunteers, temporary/agency employees
Junior/Teen Volunteer Program
 Junior/Teen Volunteer Program Dear Prospective Junior/Teen Volunteer: Enclosed you will find information and forms to complete to become a Junior/Teen Volunteer. The Junior/Teen Volunteer Program is a
Junior/Teen Volunteer Program Dear Prospective Junior/Teen Volunteer: Enclosed you will find information and forms to complete to become a Junior/Teen Volunteer. The Junior/Teen Volunteer Program is a
June 22-26, 2015 AIMS Summer Workshop for High School Students
 ADVENTURES IN MEDICINE AND SCIENCE (AIMS) PRACTICAL ANATOMY & SURGICAL EDUCATION (PASE) SAINT LOUIS UNIVERSITY SCHOOL OF MEDICINE (SLU SOM) AIMS Summer Workshop for High School Students hank you for your
ADVENTURES IN MEDICINE AND SCIENCE (AIMS) PRACTICAL ANATOMY & SURGICAL EDUCATION (PASE) SAINT LOUIS UNIVERSITY SCHOOL OF MEDICINE (SLU SOM) AIMS Summer Workshop for High School Students hank you for your
Applicant Name: First Middle Last. Age: Birth Date: Applicant Cell Phone: Address Phone: Number & Street Name City Zip Code
 PLEASE PRINT : Applicant Name: First Middle Last Age: Birth : Applicant Cell Phone: Address Phone: Number & Street Name City Zip Code (Applicant s) E-mail address: / Applicant s Parent s Legal Guardian/Mother/Father
PLEASE PRINT : Applicant Name: First Middle Last Age: Birth : Applicant Cell Phone: Address Phone: Number & Street Name City Zip Code (Applicant s) E-mail address: / Applicant s Parent s Legal Guardian/Mother/Father
The Alaska Youth Academy Application
 The Alaska Youth Academy Application Email to katina.charles@tananachiefs.org by June 26 th, 2015 Personal Information Please write in or circle your answer. Name: (First) (Middle) (Last ) Date of Birth
The Alaska Youth Academy Application Email to katina.charles@tananachiefs.org by June 26 th, 2015 Personal Information Please write in or circle your answer. Name: (First) (Middle) (Last ) Date of Birth
Standards of Professional Attire and Classroom Behavior*
 Standards of Professional Attire and Classroom Behavior* Upon acceptance and entry into the University of Missouri-Kansas City (UMKC) School of Pharmacy (SOP) or Nursing and Health Sciences (SONHS), students
Standards of Professional Attire and Classroom Behavior* Upon acceptance and entry into the University of Missouri-Kansas City (UMKC) School of Pharmacy (SOP) or Nursing and Health Sciences (SONHS), students
Georgetown Police Department 2018 Junior Police Academy Application
 Georgetown Police Department Application Application Deadline: Friday, April 27, 2018 by 5:00pm. There are 25 slots available for each camp, so don t delay in turning in your application. Applications
Georgetown Police Department Application Application Deadline: Friday, April 27, 2018 by 5:00pm. There are 25 slots available for each camp, so don t delay in turning in your application. Applications
Committee/Dept. Approval & Date: Aspirus-wide HRP 10/24/07; AVNA Senior Leadership 11/12/07; ACI Executive Team 11/20/07; WH HRP 11/15/07.
 ASPIRUS, INC. Passion for excellence. Compassion for people. FINAL Policy ID: 10091 Replaces: 07-04-240 (9/15/05); 07-41-107 (6/1/07); 07-68-227 (11/21/06); 07-92-402 (6/15/02) Effective Date: 11/20/07
ASPIRUS, INC. Passion for excellence. Compassion for people. FINAL Policy ID: 10091 Replaces: 07-04-240 (9/15/05); 07-41-107 (6/1/07); 07-68-227 (11/21/06); 07-92-402 (6/15/02) Effective Date: 11/20/07
Returning Volunteer Application
 Returning Volunteer Application Office Use Only Application Received Brenda LeBlanc, Volunteer Coordinator 978-683-4000 x2645 Brenda.leblanc@lawrencegeneral.org Welcome! Returning Volunteers, Before returning,
Returning Volunteer Application Office Use Only Application Received Brenda LeBlanc, Volunteer Coordinator 978-683-4000 x2645 Brenda.leblanc@lawrencegeneral.org Welcome! Returning Volunteers, Before returning,
Hands that serve.hearts that care.
 Hands that serve.hearts that care. Dear Applicant, We are excited that you are interested in volunteering at The University of Mississippi Medical Center (UMMC) and we want to make your volunteering experience
Hands that serve.hearts that care. Dear Applicant, We are excited that you are interested in volunteering at The University of Mississippi Medical Center (UMMC) and we want to make your volunteering experience
Study Abroad Checklist
 Study Abroad Checklist Name: Cell: Email: Semester/Year of Interest: _ Host Program: _ Major: Home Phone: Year in College (circle): FR SO JR SR Academic Advisor: Host Country and City: 1. 2. 3. Meet with
Study Abroad Checklist Name: Cell: Email: Semester/Year of Interest: _ Host Program: _ Major: Home Phone: Year in College (circle): FR SO JR SR Academic Advisor: Host Country and City: 1. 2. 3. Meet with
Student Name: Home Address: Street. City State Zip County of Residence. Student HS Graduation Year: Name of High School: GPA:
 Page 1 of 8 Participant Application SCRUBS CAMP: Hands on Adventures in Health-Care 3 Day Summer Camp (9am - 4pm) Tuesday, June 12 th Thursday June 14 th, 2018 OR Tuesday, July 17 th - Thursday, July 19
Page 1 of 8 Participant Application SCRUBS CAMP: Hands on Adventures in Health-Care 3 Day Summer Camp (9am - 4pm) Tuesday, June 12 th Thursday June 14 th, 2018 OR Tuesday, July 17 th - Thursday, July 19
VOLUNTEER APPLICATION
 VOLUNTEER APPLICATION Name: Age: Date of Birth: Social Security : Address: City: State: Zip Phone: Work: Cell: Email Address: How can we reach you? Home phone Cell phone Text Email Work phone Employer/School:
VOLUNTEER APPLICATION Name: Age: Date of Birth: Social Security : Address: City: State: Zip Phone: Work: Cell: Email Address: How can we reach you? Home phone Cell phone Text Email Work phone Employer/School:
Policy. 3. APPLICABILITY UNM Hospitals and Clinics. 4. POLICY AUTHORITY UNM Hospitals CEO and Administrator of Human Resources authorize this policy.
 Applies To: UNMH Responsible Department: Human Resources Revised: 1/2016 Policy Patient Age Group: (X ) N/A ( ) All Ages ( ) Newborns ( ) Pediatric ( ) Adult 1. POLICY STATEMENT The UNM Hospitals image
Applies To: UNMH Responsible Department: Human Resources Revised: 1/2016 Policy Patient Age Group: (X ) N/A ( ) All Ages ( ) Newborns ( ) Pediatric ( ) Adult 1. POLICY STATEMENT The UNM Hospitals image
APPLICATION
 MAYOR THOMAS C. HENRY CITY OF FORT WAYNE MAYOR S YOUTH ENGAGEMENT COUNCIL 2017-2018 APPLICATION Please mail, deliver or fax completed applications to: MAYOR S OFFICE, ATTN: KAREN L. RICHARDS 200 E. BERRY
MAYOR THOMAS C. HENRY CITY OF FORT WAYNE MAYOR S YOUTH ENGAGEMENT COUNCIL 2017-2018 APPLICATION Please mail, deliver or fax completed applications to: MAYOR S OFFICE, ATTN: KAREN L. RICHARDS 200 E. BERRY
Career. Exploration Program
 Career Exploration Program St. Elizabeth Healthcare is proud to offer a Career Exploration Program to provide realistic experiences and learning opportunities to individuals interested in pursuing a career
Career Exploration Program St. Elizabeth Healthcare is proud to offer a Career Exploration Program to provide realistic experiences and learning opportunities to individuals interested in pursuing a career
Boy Scouts of America
 Boy Scouts of America ADULT APPLICATION The mission of the Boy Scouts of America is to prepare young people to make ethical and moral choices over their lifetimes by instilling in them the values of the
Boy Scouts of America ADULT APPLICATION The mission of the Boy Scouts of America is to prepare young people to make ethical and moral choices over their lifetimes by instilling in them the values of the
Internship Application x2645
 Internship Application 978-683-4000 x2645 Office Use Only Application Received Interview Orientation CORI TB1 TB2 Pin # Entered in Volgistics FLU PERSONAL INFORMATION First Name Last Name Street Address
Internship Application 978-683-4000 x2645 Office Use Only Application Received Interview Orientation CORI TB1 TB2 Pin # Entered in Volgistics FLU PERSONAL INFORMATION First Name Last Name Street Address
If you are currently a High School Senior. you will complete a general volunteer application, not this one.
 2018 North Cypress Medical Center Junior Volunteer Packet Must be a Current High School Sophomore or Junior If you are currently a High School Senior you will complete a general volunteer application,
2018 North Cypress Medical Center Junior Volunteer Packet Must be a Current High School Sophomore or Junior If you are currently a High School Senior you will complete a general volunteer application,
HUMAN RESOURCES POLICY
 HUMAN RESOURCES POLICY Subject EMPLOYEE RELATIONS Title 1 of 5 Revision of 03/01/2010 Effective Date 01/14/2014 Removal Date: I. PURPOSE: Northwestern Memorial s mission of Patients First supports the
HUMAN RESOURCES POLICY Subject EMPLOYEE RELATIONS Title 1 of 5 Revision of 03/01/2010 Effective Date 01/14/2014 Removal Date: I. PURPOSE: Northwestern Memorial s mission of Patients First supports the
WEST VIRGINIA UNIVERSITY SCHOOL OF DENTISTRY POLICY ON PROFESSIONAL APPEARANCE AND ATTIRE
 WEST VIRGINIA UNIVERSITY SCHOOL OF DENTISTRY POLICY ON PROFESSIONAL APPEARANCE AND ATTIRE Revised August 2009 Revised December 2011 Revised January 2013 Revised August 2015 Revised September 2016 WVU SCHOOL
WEST VIRGINIA UNIVERSITY SCHOOL OF DENTISTRY POLICY ON PROFESSIONAL APPEARANCE AND ATTIRE Revised August 2009 Revised December 2011 Revised January 2013 Revised August 2015 Revised September 2016 WVU SCHOOL
Rotation Expectations: Surgery-Ortho Clerkship. Students are required to read ALL expectations prior to orientation.
 Rotation Expectations: Surgery-Ortho Clerkship Students are required to read ALL expectations prior to orientation. Orientation: On the first day of orientation, students will have the opportunity to ask
Rotation Expectations: Surgery-Ortho Clerkship Students are required to read ALL expectations prior to orientation. Orientation: On the first day of orientation, students will have the opportunity to ask
THIS AGREEMENT made effective this day of, 20. BETWEEN: NOVA SCOTIA HEALTH AUTHORITY ("NSHA") AND X. (Hereinafter referred to as the Agency )
 AND X. (Hereinafter referred to as the Agency )") THIS AGREEMENT made effective this day of, 20. BETWEEN: NOVA SCOTIA HEALTH AUTHORITY ("NSHA") AND X (Hereinafter referred to as the Agency ) It is agreed by the parties that NSHA will participate in the
THIS AGREEMENT made effective this day of, 20. BETWEEN: NOVA SCOTIA HEALTH AUTHORITY ("NSHA") AND X (Hereinafter referred to as the Agency ) It is agreed by the parties that NSHA will participate in the
Kennedy King College-Minority Science and Engineering Improvement Program 2013
 Dear Student & Parent/Guardian: This is the Application Packet for the Minority Science and Engineering Improvement Program at Kennedy King College. All documents within this packet must be completed and
Dear Student & Parent/Guardian: This is the Application Packet for the Minority Science and Engineering Improvement Program at Kennedy King College. All documents within this packet must be completed and
2018 MARSHALL COUNTY LAW ENFORCEMENT YOUTH CAMP APPLICATION
 2018 MARSHALL COUNTY LAW ENFORCEMENT YOUTH CAMP APPLICATION Law Enforcement agencies from across Marshall County will sponsor and provide a Law Enforcement Youth Camp for students this year on the dates
2018 MARSHALL COUNTY LAW ENFORCEMENT YOUTH CAMP APPLICATION Law Enforcement agencies from across Marshall County will sponsor and provide a Law Enforcement Youth Camp for students this year on the dates
MEDEX ACADEMY Undergraduate Application
 Undergraduate Application Personal Information: Name: (Last) (First) (Middle) Preferred Name: Address: (Street) (Apt. Number) (City) (State) (Zip Code) Telephone: (Home) (Cell) (Other) E-mail: Date of
Undergraduate Application Personal Information: Name: (Last) (First) (Middle) Preferred Name: Address: (Street) (Apt. Number) (City) (State) (Zip Code) Telephone: (Home) (Cell) (Other) E-mail: Date of
Job Shadow Program Guidelines
 Job Shadow Program Guidelines The Job Shadow Program is intended for those who have an interest in learning more about health care professions. Shadowing allows the participant to follow and observe a
Job Shadow Program Guidelines The Job Shadow Program is intended for those who have an interest in learning more about health care professions. Shadowing allows the participant to follow and observe a
COMMUNITY, COUNSELING & CORRECTIONAL SERVICES, INC. Gallatin County Re-Entry Program SPONSOR FORM
 COMMUNITY, COUNSELING & CORRECTIONAL SERVICES, INC. Gallatin County Re-Entry Program SPONSOR FORM Name of Resident Being Sponsored: Name of Sponsor Applicant: Community passes are one of the most important
COMMUNITY, COUNSELING & CORRECTIONAL SERVICES, INC. Gallatin County Re-Entry Program SPONSOR FORM Name of Resident Being Sponsored: Name of Sponsor Applicant: Community passes are one of the most important
Georgia CTI. Fall Leadership Conference (FLC)
") Georgia CTI Fall Leadership Conference (FLC) Evergreen Marriott Resort November 14-15, 2013 4021 Lakeview Drive Stone Mountain, GA 30083-3099 (770) 879-9900 Hotel Reservation Deadline: October 24 Online
Georgia CTI Fall Leadership Conference (FLC) Evergreen Marriott Resort November 14-15, 2013 4021 Lakeview Drive Stone Mountain, GA 30083-3099 (770) 879-9900 Hotel Reservation Deadline: October 24 Online
Children s Hospital Los Angeles Application for Summer Junior Volunteer Program 2018 (15-17 years of age)
") Children s Hospital Los Angeles Application for Summer Junior Volunteer Program 2018 (15-17 years of age) Dear Volunteer Applicant: Thank you for your interest in becoming a Junior Volunteer at Children
Children s Hospital Los Angeles Application for Summer Junior Volunteer Program 2018 (15-17 years of age) Dear Volunteer Applicant: Thank you for your interest in becoming a Junior Volunteer at Children
Court Referral Program YDAD REGISTRATION
 Court Referral Program YDAD REGISTRATION Case Number# : Name: (First) (Middle Name) (Last Name) Address: City: State: Zip: Home Phone: ( ) Cell: ( ) Work Phone: ( ) Fax #: ( ) Email Address: @. Social
Court Referral Program YDAD REGISTRATION Case Number# : Name: (First) (Middle Name) (Last Name) Address: City: State: Zip: Home Phone: ( ) Cell: ( ) Work Phone: ( ) Fax #: ( ) Email Address: @. Social
2016 Multi-Jurisdictional Law Enforcement Explorer Academy
 2016 Multi-Jurisdictional Law Enforcement Explorer Academy All questions must be answered. If something does not apply please indicate N/A. Note: If there are any un-answered questions on this application
2016 Multi-Jurisdictional Law Enforcement Explorer Academy All questions must be answered. If something does not apply please indicate N/A. Note: If there are any un-answered questions on this application
CAVIT Nursing Assistant Program Handbook
 2015-2016 CAVIT Nursing Assistant Program Handbook PROGRAM PURPOSE The purpose of the CAVIT Nursing Assistant Program is to prepare students for a career in the healthcare industry. Through an integrated
2015-2016 CAVIT Nursing Assistant Program Handbook PROGRAM PURPOSE The purpose of the CAVIT Nursing Assistant Program is to prepare students for a career in the healthcare industry. Through an integrated
THE METROHEALTH SYSTEM POLICIES. POLICY No: II -71(p) Surgical Attire for Operating Rooms and Procedural Areas Originated By: Perioperative Services
 Surgical Attire for Operating Rooms and Procedural Areas Originated By: Perioperative Services") Surgical Attire for Operating Rooms and Procedural Areas Originated By: Perioperative Services Converted from Perioperative Service and name changed from Attire for Operating Room Personnel Policy *12/2013
Surgical Attire for Operating Rooms and Procedural Areas Originated By: Perioperative Services Converted from Perioperative Service and name changed from Attire for Operating Room Personnel Policy *12/2013
*MAMC Regulation DEPARTMENT OF THE ARMY MADIGAN ARMY MEDICAL CENTER Tacoma, Washington MAMC Regulation Number October 2007
 *MAMC Regulation 690-1 DEPARTMENT OF THE ARMY MADIGAN ARMY MEDICAL CENTER Tacoma, Washington 98431-1100 MAMC Regulation Number 690-1 23 October 2007 Civilian Personnel STANDARDS OF DRESS AND APPEARANCE
*MAMC Regulation 690-1 DEPARTMENT OF THE ARMY MADIGAN ARMY MEDICAL CENTER Tacoma, Washington 98431-1100 MAMC Regulation Number 690-1 23 October 2007 Civilian Personnel STANDARDS OF DRESS AND APPEARANCE
WEST VIRGINIA UNIVERSITY SCHOOL OF DENTISTRY POLICY ON PROFESSIONAL APPEARANCE AND ATTIRE
 WEST VIRGINIA UNIVERSITY SCHOOL OF DENTISTRY POLICY ON PROFESSIONAL APPEARANCE AND ATTIRE Revised August 2009 Revised December 2011 Revised January 2013 Revised August 2015 Revised September 2016 Revised
WEST VIRGINIA UNIVERSITY SCHOOL OF DENTISTRY POLICY ON PROFESSIONAL APPEARANCE AND ATTIRE Revised August 2009 Revised December 2011 Revised January 2013 Revised August 2015 Revised September 2016 Revised
After School Program ABBOT DOWNING SCHOOL BEAVER MEADOW SCHOOL
 @ Y 21C Y@21C is a partnership between the 21st Century Community Learning Centers and the Concord Family YMCA. PLEASE NOTE: registration must be confirmed by the YMCA before your child can attend program.
@ Y 21C Y@21C is a partnership between the 21st Century Community Learning Centers and the Concord Family YMCA. PLEASE NOTE: registration must be confirmed by the YMCA before your child can attend program.
Individual Volunteer Application
 Individual Volunteer Application This application is for individuals only. Once you submit this application, the Director of Volunteer Services and Community Outreach will contact you regarding your approval
Individual Volunteer Application This application is for individuals only. Once you submit this application, the Director of Volunteer Services and Community Outreach will contact you regarding your approval
Parent/Guardian Names: Cell Phone: School: Parent/Guardian Signature: Date:
 SPIRIT OF AMERICA BOATING SAFETY PROGRAM Offered by Sailing Center Chesapeake & St. Mary s College of Maryland Open to students who have completed 6 th, 7 th, or 8 th grades in 2017. Summer 2017 Student
SPIRIT OF AMERICA BOATING SAFETY PROGRAM Offered by Sailing Center Chesapeake & St. Mary s College of Maryland Open to students who have completed 6 th, 7 th, or 8 th grades in 2017. Summer 2017 Student
Summer Engineering Academy
 TM February 5, 2018 Aloha, Honolulu Community College is once again pleased to announce its upcoming Summer Engineering Academy. Space will be limited, so please apply as soon as possible. Only 60 students
TM February 5, 2018 Aloha, Honolulu Community College is once again pleased to announce its upcoming Summer Engineering Academy. Space will be limited, so please apply as soon as possible. Only 60 students
Glastonbury Family YMCA. CAMP GLAWACKUS, CAMP LIGER and SPECIALTY CAMPS REGISTRATION PACKET
 2018 Glastonbury Family YMCA CAMP GLAWACKUS, CAMP LIGER and SPECIALTY CAMPS REGISTRATION PACKET CAMP LOCATION 30 High Street South Glastonbury, CT 06073 860-541-1812 STEP STEP one REGISTRATION Done online,
2018 Glastonbury Family YMCA CAMP GLAWACKUS, CAMP LIGER and SPECIALTY CAMPS REGISTRATION PACKET CAMP LOCATION 30 High Street South Glastonbury, CT 06073 860-541-1812 STEP STEP one REGISTRATION Done online,
MESA COMMUNITY COLLEGE. Information Packet 2018 YOUTH COLLEGE. Workshop I & II - Please fill out the following forms and bring to your Audition Time:
 MESA COMMUNITY COLLEGE Information Packet 2018 YOUTH COLLEGE Workshop I & II - Please fill out the following forms and bring to your Audition Time: o 14 years and older Need to provide picture ID for Student
MESA COMMUNITY COLLEGE Information Packet 2018 YOUTH COLLEGE Workshop I & II - Please fill out the following forms and bring to your Audition Time: o 14 years and older Need to provide picture ID for Student
PATIENT INFORMATION Please Print
 PATIENT INFORMATION Please Print DATE Patient s Last Name First Name Middle Name Suffix Gender: q Male q Female Social Security Number of Birth Race Ethnic Group: q Hispanic q Non-Hispanic q Unknown Preferred
PATIENT INFORMATION Please Print DATE Patient s Last Name First Name Middle Name Suffix Gender: q Male q Female Social Security Number of Birth Race Ethnic Group: q Hispanic q Non-Hispanic q Unknown Preferred
Heading. Second Level. Student Orientation
 Heading Second Level Student Orientation Spring 2012 We re proud of our history of serving the health care needs of the residents of McKinney and surrounding areas for more than 80 years. Change and innovation
Heading Second Level Student Orientation Spring 2012 We re proud of our history of serving the health care needs of the residents of McKinney and surrounding areas for more than 80 years. Change and innovation
Effective Date: 08/30/2012. Revised Date: To ensure that all members of VCES are in proper uniform and appearance.
 Scope: All Career Members of Valencia County Emergency Services. Purpose To ensure that all members of VCES are in proper uniform and appearance. 1. General Requirements: a. All Personnel. i. Members shall
Scope: All Career Members of Valencia County Emergency Services. Purpose To ensure that all members of VCES are in proper uniform and appearance. 1. General Requirements: a. All Personnel. i. Members shall
Ambassador Program Application Packet
 Ambassador Program Application Packet Thank you for your interest in becoming an Ambassador at Centinela Hospital Medical Center. Please complete the attached forms and then contact the Centinela Hospital
Ambassador Program Application Packet Thank you for your interest in becoming an Ambassador at Centinela Hospital Medical Center. Please complete the attached forms and then contact the Centinela Hospital
Rhode Island College Club Sports Emergency Information Form
 Rhode Island College Club Sports Emergency Information Form Contact Information Name: Email: Phone Number: Club Sport: Student ID #: Year in School: Local Address: (Street) (City) (State) (Zip) Person
Rhode Island College Club Sports Emergency Information Form Contact Information Name: Email: Phone Number: Club Sport: Student ID #: Year in School: Local Address: (Street) (City) (State) (Zip) Person
Adult Volunteer Application
 Adult Volunteer Application Dear Community Friend: Thank you for your interest in volunteering at Slidell Memorial Hospital (SMH). Volunteering can be quite rewarding and, of course, is a great help to
Adult Volunteer Application Dear Community Friend: Thank you for your interest in volunteering at Slidell Memorial Hospital (SMH). Volunteering can be quite rewarding and, of course, is a great help to
SECTION: EMPLOYEE RELATIONS PAGE: 1 of 6
 MEMORIAL MEDICAL CENTER HUMAN RESOURCES POLICY MANUAL Policy No. 5-7 SECTION: EMPLOYEE RELATIONS PAGE: 1 of 6 SUBJECT: MMC IMAGE DATE: 08/27/98; 11/1/00; 7/26/02; 7/01/03; 5/01/04; 9/01/04; 4/01/06; 9/01/06;
MEMORIAL MEDICAL CENTER HUMAN RESOURCES POLICY MANUAL Policy No. 5-7 SECTION: EMPLOYEE RELATIONS PAGE: 1 of 6 SUBJECT: MMC IMAGE DATE: 08/27/98; 11/1/00; 7/26/02; 7/01/03; 5/01/04; 9/01/04; 4/01/06; 9/01/06;
Clinical Education Policies
 1 Clinical Education Policies Table of Contents Assignment of Students Page 1 Student Information Page 1 Student Information Form Page 2 Reasonable Accommodations Request Student Health Form Pages 3-5
1 Clinical Education Policies Table of Contents Assignment of Students Page 1 Student Information Page 1 Student Information Form Page 2 Reasonable Accommodations Request Student Health Form Pages 3-5
2014 MASH CAMP. June 9-12 Basic (15 student limit) Grades 9-12 June Advanced (15 student limit) Juniors/Seniors ONLY
 Grades 9-12 June Advanced (15 student limit) Juniors/Seniors ONLY") MEDICAL CAMP 2014 MASH CAMP Medical Avenues to Services in Health (M*A*S*H) programs are designed to educate High School students about the possibility of pursuing a career in the health service field
MEDICAL CAMP 2014 MASH CAMP Medical Avenues to Services in Health (M*A*S*H) programs are designed to educate High School students about the possibility of pursuing a career in the health service field
CAMP KEOLA 4-H CAMP June 19-23, 2018 CAMPER REGISTRATION NAME AGE GENDER GRADE MAILING ADDRESS CITY ZIP
 COMPLETE 1 PER CAMPER CAMP KEOLA 4-H CAMP June 19-23, 2018 CAMPER REGISTRATION Camp Fee Date Received Check Number For Office Use Only WHO MAY ATTEND: Fresno County 4-H members who are 9 years old or in
COMPLETE 1 PER CAMPER CAMP KEOLA 4-H CAMP June 19-23, 2018 CAMPER REGISTRATION Camp Fee Date Received Check Number For Office Use Only WHO MAY ATTEND: Fresno County 4-H members who are 9 years old or in
2013 Teen Volunteer Program
 2013 Teen Volunteer Program Volunteer Services Office Dear Teen, Thank you for your interest in volunteering at. Students chosen to serve in our hospital will be those who can best represent our hospital
2013 Teen Volunteer Program Volunteer Services Office Dear Teen, Thank you for your interest in volunteering at. Students chosen to serve in our hospital will be those who can best represent our hospital
CADET TRAINING RECORD INFORMATION SHEET
 CADET TRAINING RECORD INFORMATION SHEET LAST NAME FIRST NAME MIDDLE NAME ADDRESS CITY STATE ZIP CODE HOME PHONE NUMBER PLACE OF BIRTH (City/State) MIDDLE SCHOOL ATTENDED DATE OF BIRTH (mm/dd/yyyy) CITIZENSHIP
CADET TRAINING RECORD INFORMATION SHEET LAST NAME FIRST NAME MIDDLE NAME ADDRESS CITY STATE ZIP CODE HOME PHONE NUMBER PLACE OF BIRTH (City/State) MIDDLE SCHOOL ATTENDED DATE OF BIRTH (mm/dd/yyyy) CITIZENSHIP
HCC EMS Code of Conduct
 HCC EMS Code of Conduct Attendance and Tardiness Attendance at all classroom, skill sessions, and hands on training is mandatory. Tardiness will not be tolerated. This will include when reporting to any
HCC EMS Code of Conduct Attendance and Tardiness Attendance at all classroom, skill sessions, and hands on training is mandatory. Tardiness will not be tolerated. This will include when reporting to any
ADULT APPLICATION. For Learning for Life district and council committee participants and Exploring or Explorer Club adult leaders.
 ADULT APPLICATION For Learning for Life district and council committee participants and Exploring or Explorer Club adult leaders. Mission: To develop and deliver engaging, research-based academic, character,
ADULT APPLICATION For Learning for Life district and council committee participants and Exploring or Explorer Club adult leaders. Mission: To develop and deliver engaging, research-based academic, character,
Beo Nurse Aide Training Program
 Policy for Admission to Program Beo Nurse Aide Training Program 1. Applicants to BEO Nurse Aide Training program must be 18 years of age, enrolled in High School at the Senior level or have a GED. 2. Admission
Policy for Admission to Program Beo Nurse Aide Training Program 1. Applicants to BEO Nurse Aide Training program must be 18 years of age, enrolled in High School at the Senior level or have a GED. 2. Admission
Hats and sun visors are not permitted unless they are issued by HH Health System, face forward, and are in good condition
 Organizational Policies and Procedures Policy Title: Employee Dress, Uniform, and Appearance Policy Department: Human Resources Area: Employee Relations & Practices Effective Date: February, 2016 Pages:
Organizational Policies and Procedures Policy Title: Employee Dress, Uniform, and Appearance Policy Department: Human Resources Area: Employee Relations & Practices Effective Date: February, 2016 Pages:
UNITED STATES MARINE CORPS RECRUITING STATION COLUMBIA 9600 TWO NOTCH RD, SUITE 17 COLUMBIA, SOUTH CAROLINA 29223
 UNITED STATES MARINE CORPS RECRUITING STATION COLUMBIA 9600 TWO NOTCH RD, SUITE 17 COLUMBIA, SOUTH CAROLINA 29223 6 Aug 15 Dear Sir or Ma am, On behalf of the United States Marine Corps, I would like to
UNITED STATES MARINE CORPS RECRUITING STATION COLUMBIA 9600 TWO NOTCH RD, SUITE 17 COLUMBIA, SOUTH CAROLINA 29223 6 Aug 15 Dear Sir or Ma am, On behalf of the United States Marine Corps, I would like to
Please return the completed application to me at the address shown below or .
 Dear Student, Thank you for your interest in becoming a volunteer at Concord Hospital. We believe we can offer you a meaningful experience you will find personally rewarding, while contributing to your
Dear Student, Thank you for your interest in becoming a volunteer at Concord Hospital. We believe we can offer you a meaningful experience you will find personally rewarding, while contributing to your
Student Handbook
 2016-2017 2017 CAVIT Nursing Program Year Two Student Handbook . 2016-2017 NURSING ASSISTANT YEAR TWO PROGRAM GUIDE PROGRAM PURPOSE The purpose of the CAVIT Nursing Assistant Program is to prepare students
2016-2017 2017 CAVIT Nursing Program Year Two Student Handbook . 2016-2017 NURSING ASSISTANT YEAR TWO PROGRAM GUIDE PROGRAM PURPOSE The purpose of the CAVIT Nursing Assistant Program is to prepare students
Department of Physical Therapy DATE: 8/2017 College of Applied Health Sciences University Of Illinois At Chicago PHYSICAL THERAPY POLICY AND PROCEDURE
 TABLE OF CONTENTS Attendance and Tardiness Policies 2 Student Attire and Appearance.6 Use of Electronic Devices..12 1 SUBJECT: Classroom, Laboratory, Clinic, and Assessment Attendance and Tardiness Policies
TABLE OF CONTENTS Attendance and Tardiness Policies 2 Student Attire and Appearance.6 Use of Electronic Devices..12 1 SUBJECT: Classroom, Laboratory, Clinic, and Assessment Attendance and Tardiness Policies
Return Completed Application To: ARISE & Ski, 635 James Street, Syracuse, NY 13203
 ARISE & Ski Volunteer Application We consider applicants for all positions without regard to race, religion, creed, gender, age, disability, marital or veteran status, sexual orientation or any other legally
ARISE & Ski Volunteer Application We consider applicants for all positions without regard to race, religion, creed, gender, age, disability, marital or veteran status, sexual orientation or any other legally
Southlake Regional Health Centre - Dress Code
 Page 1 of 6 Home > Policies & Procedures > Administrative Documents > Administration Manual > Dress Code Disclaimer: the information contained in this document is for educational purposes only. Any PRINTED
Page 1 of 6 Home > Policies & Procedures > Administrative Documents > Administration Manual > Dress Code Disclaimer: the information contained in this document is for educational purposes only. Any PRINTED
Rome Memorial Hospital has openings for a limited number of student volunteers. If you are at least 15 years old and are interested, please:
 1500 North James Street Rome, New York 13440 (315) 338-7000 Dear Student Volunteer Applicant: Rome Memorial Hospital has openings for a limited number of student volunteers. If you are at least 15 years
1500 North James Street Rome, New York 13440 (315) 338-7000 Dear Student Volunteer Applicant: Rome Memorial Hospital has openings for a limited number of student volunteers. If you are at least 15 years
ADULT APPLICATION This application is also available in Spanish. Esta solicitud también está disponible en español.
 BOY SCOUTS OF AMERICA ADULT APPLICATION This application is also available in Spanish. Esta solicitud también está disponible en español. The mission of the Boy Scouts of America is to prepare young people
BOY SCOUTS OF AMERICA ADULT APPLICATION This application is also available in Spanish. Esta solicitud también está disponible en español. The mission of the Boy Scouts of America is to prepare young people
THE 2014 AMERICAN RED CROSS SUMMER YOUTH VOLUNTEER PROGRAM AT THE EVANS ARMY COMMUNITY HOSPITAL FORT CARSON, COLORADO May 27 July 25
 THE 2014 AMERICAN RED CROSS SUMMER YOUTH VOLUNTEER PROGRAM AT THE EVANS ARMY COMMUNITY HOSPITAL FORT CARSON, COLORADO May 27 July 25 The American Red Cross (ARC) at Fort Carson s Evans Army Community Hospital
THE 2014 AMERICAN RED CROSS SUMMER YOUTH VOLUNTEER PROGRAM AT THE EVANS ARMY COMMUNITY HOSPITAL FORT CARSON, COLORADO May 27 July 25 The American Red Cross (ARC) at Fort Carson s Evans Army Community Hospital
NORTH CAROLINA 4-H VOLUNTEER APPLICATION
 NORTH CAROLINA 4-H VOLUNTEER APPLICATION PERSONAL INFORMATION First Name: Middle Name: Last Name: Suffix: Preferred Name: Mailing Address: Mailing Address 2: City: State: Zip: Gender: Male Years in 4-H:
NORTH CAROLINA 4-H VOLUNTEER APPLICATION PERSONAL INFORMATION First Name: Middle Name: Last Name: Suffix: Preferred Name: Mailing Address: Mailing Address 2: City: State: Zip: Gender: Male Years in 4-H:
Date Reviewed: Date Revised: Implementation: CPIC Approved: Board Approved: Feb Responsible Party: HR
 POLICY & PROCEDURE TITLE: Professional Appearance and Dress Code Scope/Purpose: To promote a safe environment and professional atmosphere at all times for employees, patients and visitors through the proper
POLICY & PROCEDURE TITLE: Professional Appearance and Dress Code Scope/Purpose: To promote a safe environment and professional atmosphere at all times for employees, patients and visitors through the proper
Proposed Changes Provided to ONA by CMH. SCOPE: Added Locums/Agency Staff and other contracted individuals that regularly perform work at the hospital
 Proposed Changes Provided to ONA by CMH SCOPE: Added Locums/Agency Staff and other contracted individuals that regularly perform work at the hospital GENERAL POLICY STATEMENT: Employee appearance reflects
Proposed Changes Provided to ONA by CMH SCOPE: Added Locums/Agency Staff and other contracted individuals that regularly perform work at the hospital GENERAL POLICY STATEMENT: Employee appearance reflects
HIPAA PRIVACY TRAINING
 HIPAA PRIVACY TRAINING HIPAA Privacy Training Objective Present a general overview of HIPAA and define important terms Understand the purpose of HIPAA and the Privacy Rule Understand the term Protected
HIPAA PRIVACY TRAINING HIPAA Privacy Training Objective Present a general overview of HIPAA and define important terms Understand the purpose of HIPAA and the Privacy Rule Understand the term Protected
SAISD Volunteer Information Packet
 SAISD Volunteer Information Packet Thank you for choosing to volunteer in the San Antonio Independent School District. We hope that the time that you spend volunteering at SAISD is both fun and rewarding.
SAISD Volunteer Information Packet Thank you for choosing to volunteer in the San Antonio Independent School District. We hope that the time that you spend volunteering at SAISD is both fun and rewarding.
Glastonbury YMCA 29 Welles Street, Glastonbury CT Dear YMCA Family,
 s Dear YMCA Family, Thank you for choosing the Glastonbury Family YMCA Preschool for your early childhood child care needs. We are excited to welcome you and your family to our program! The Y s focus is
s Dear YMCA Family, Thank you for choosing the Glastonbury Family YMCA Preschool for your early childhood child care needs. We are excited to welcome you and your family to our program! The Y s focus is
POLICY NO Volunteer Policy (Replaces Policy Adopted 1/26/1998)
") POLICY NO. 28-01 Volunteer Policy (Replaces Policy Adopted 1/26/1998) Policy Statement Hernando County recognizes that volunteers are essential to the productivity, efficiency and cost effectiveness of
POLICY NO. 28-01 Volunteer Policy (Replaces Policy Adopted 1/26/1998) Policy Statement Hernando County recognizes that volunteers are essential to the productivity, efficiency and cost effectiveness of
Guidelines for All Team Members
 Our patients and their families expect and deserve the assurance that they have made the right choice by entrusting IU Health with their care. We provide this assurance though our unparalleled expertise,
Our patients and their families expect and deserve the assurance that they have made the right choice by entrusting IU Health with their care. We provide this assurance though our unparalleled expertise,
Dear Zoo Crew Applicant,
 Dear Zoo Crew Applicant, Thank you for your interest in Zoo Crew, the Children s Zoo teen volunteer program! For a complete list of program benefits visit our website at www.saginawzoo.com. Please read
Dear Zoo Crew Applicant, Thank you for your interest in Zoo Crew, the Children s Zoo teen volunteer program! For a complete list of program benefits visit our website at www.saginawzoo.com. Please read
DEANS OFFICE USE ONLY (Signature required BEFORE turning in to Activities by February 16, 2016 at 3pm) DEANS APPROVAL DATE
 DEANS APPROVAL DATE") DEANS OFFICE USE ONLY (Signature required BEFORE turning in to Activities by February 16, 2016 at 3pm) DEANS APPROVAL DATE GUEST SMCHS WINTER FORMAL CONTRACT 2016 **This contract must be turned in with
DEANS OFFICE USE ONLY (Signature required BEFORE turning in to Activities by February 16, 2016 at 3pm) DEANS APPROVAL DATE GUEST SMCHS WINTER FORMAL CONTRACT 2016 **This contract must be turned in with
GROUP VOLUNTEER APPLICATION
 Contact Information: Please print clearly GROUP VOLUNTEER APPLICATION Organization Name: Primary Contact Name: Address: Phone: Email: Availability (Check and circle all that apply): Monday Tuesday Wednesday
Contact Information: Please print clearly GROUP VOLUNTEER APPLICATION Organization Name: Primary Contact Name: Address: Phone: Email: Availability (Check and circle all that apply): Monday Tuesday Wednesday
Camp TOV Medical Form
 Mail: Fax: Please send these forms to us by either: Jewish United Fund/Jewish Federation of Metropolitan Chicago Attn: Camp TOV 30 South Wells Street, Room 5034 Chicago, IL 60606 Attn: Camp TOV 312-444-2086
Mail: Fax: Please send these forms to us by either: Jewish United Fund/Jewish Federation of Metropolitan Chicago Attn: Camp TOV 30 South Wells Street, Room 5034 Chicago, IL 60606 Attn: Camp TOV 312-444-2086
POLICY NO Volunteer Policy (Replaces Policy Adopted 12/13/2011)
") POLICY NO. 28-01 Volunteer Policy (Replaces Policy Adopted 12/13/2011) Policy Statement Hernando County recognizes that volunteers are essential to the productivity, efficiency and cost effectiveness of
POLICY NO. 28-01 Volunteer Policy (Replaces Policy Adopted 12/13/2011) Policy Statement Hernando County recognizes that volunteers are essential to the productivity, efficiency and cost effectiveness of
NA APPLICATION FOR ADMISSION
 NA APPLICATION FOR ADMISSION FIRST 2 PAGES OF THIS APPLICATION PACKAGE MUST BE FILLED OUT COMPLETELY AND TURNED IN DURING THE APPLICATION ACCEPTANCE PERIOD. PLEASE PRINT NAME: Last First Initial ADDRESS:
NA APPLICATION FOR ADMISSION FIRST 2 PAGES OF THIS APPLICATION PACKAGE MUST BE FILLED OUT COMPLETELY AND TURNED IN DURING THE APPLICATION ACCEPTANCE PERIOD. PLEASE PRINT NAME: Last First Initial ADDRESS:
CRANFORD POLICE DEPARTMENT YOUTH POLICE ACADEMY
 YOUTH POLICE ACADEMY June 25-29, 2018 8:00 AM 3:00 PM Available to Cranford students graduating 6 th, 7 th, and 8 th grades Learn about the Cranford Police Department and other local, state, and federal
YOUTH POLICE ACADEMY June 25-29, 2018 8:00 AM 3:00 PM Available to Cranford students graduating 6 th, 7 th, and 8 th grades Learn about the Cranford Police Department and other local, state, and federal
Volunteer Application
 Volunteer Application I. CONTACT INFORMATION Mr. Mrs. Name (first): (middle): (last): Ms. Home Address: City: State: Zip: Phone (home): E-mail Address: (business): (cell): Birth Date: Employer/School:
Volunteer Application I. CONTACT INFORMATION Mr. Mrs. Name (first): (middle): (last): Ms. Home Address: City: State: Zip: Phone (home): E-mail Address: (business): (cell): Birth Date: Employer/School:
General Information & Preparation
 Ponderosa Retreat Parent Information Please Keep This Information Paper for your Reference All Other Forms, with $50 Payment, Turn-in by Friday, August 17 All Other Forms Must be Signed to be Valid General
Ponderosa Retreat Parent Information Please Keep This Information Paper for your Reference All Other Forms, with $50 Payment, Turn-in by Friday, August 17 All Other Forms Must be Signed to be Valid General
Parent or Guardian Release and Indemnity Agreement
 Parent or Guardian Release and Indemnity Agreement I hereby request that you accept this application for the enrollment of in the Bellin College Medical Imaging Camp. I hereby release Bellin College and
Parent or Guardian Release and Indemnity Agreement I hereby request that you accept this application for the enrollment of in the Bellin College Medical Imaging Camp. I hereby release Bellin College and
Volunteer/Observation Handbook
 Volunteer/Observation Handbook WELCOME TO BENCHMARK: ABOUT US page 3 MISSION, VISION & VALUES page 4 HIPAA CONFIDENTIALITY AGREEMENT page 5 PROFESSIONAL ATTIRE page 6 RULES OF CONDUCT page 7 HOST & VOLUNTEER
Volunteer/Observation Handbook WELCOME TO BENCHMARK: ABOUT US page 3 MISSION, VISION & VALUES page 4 HIPAA CONFIDENTIALITY AGREEMENT page 5 PROFESSIONAL ATTIRE page 6 RULES OF CONDUCT page 7 HOST & VOLUNTEER
Falls Creek 2016 Registration
 , Falls Creek 2016 Registration Page 1 of 4 Falls Creek 2016 Registration Statement for Participation in Falls Creek Youth Camp Falls Creek Youth Encampment is the largest Christian Youth Camp in America.
, Falls Creek 2016 Registration Page 1 of 4 Falls Creek 2016 Registration Statement for Participation in Falls Creek Youth Camp Falls Creek Youth Encampment is the largest Christian Youth Camp in America.
East Baton Rouge Parish Junior Deputy
 East Baton Rouge Parish Junior Deputy 2018 Application Packet Sheriff Sid J. Gautreaux, III Captain Randy M. Aguillard Program Director raguillard@ebrso.org Junior Deputy Membership Rules All members of
East Baton Rouge Parish Junior Deputy 2018 Application Packet Sheriff Sid J. Gautreaux, III Captain Randy M. Aguillard Program Director raguillard@ebrso.org Junior Deputy Membership Rules All members of
1) INFORMATION ABOUT THE PARTICIPANT AND ACTIVITY
 INFORMATION ABOUT THE PARTICIPANT AND ACTIVITY") 2016-17 South Carolina 4-H Membership and Event Permission Form for Youth (Updated 08.01.16) ALL elements of this form must be completed by youth participating in clubs, field trips, events requiring group
2016-17 South Carolina 4-H Membership and Event Permission Form for Youth (Updated 08.01.16) ALL elements of this form must be completed by youth participating in clubs, field trips, events requiring group
Project Aerospace ACE Academy Application
 Project Aerospace ACE Academy Application Location: (s): The OBAP Aviation Career Education (ACE) Academy is designed to provide a more in-depth look at the aviation industry for students who truly want
Project Aerospace ACE Academy Application Location: (s): The OBAP Aviation Career Education (ACE) Academy is designed to provide a more in-depth look at the aviation industry for students who truly want
Dear Volunteen Applicant:
 Dear Volunteen Applicant: Thank you for your interest in volunteering at Marian Regional Medical Center. Our Volunteen Program is for current high school students who are at least 14 years old. Please
Dear Volunteen Applicant: Thank you for your interest in volunteering at Marian Regional Medical Center. Our Volunteen Program is for current high school students who are at least 14 years old. Please