Beyond Implementation: Capturing the Value of Care Coordination
|
|
|
- Frank Harris
- 6 years ago
- Views:
Transcription
1 2015 Webinar Series Pediatric Care Coordination: Beyond Policy, Practice, and Implementation A webinar series brought to you by the National Center for Medical Home Implementation Beyond Implementation: Capturing the Value of Care Coordination May 28, am Noon Central This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number U43MC This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.

2 Beyond Implementation: Capturing the Value of Care Coordination brought to you by the National Center for Medical Home Implementation Moderator: Dian Baker, PhD, RN California State University, Sacramento School of Nursing


3 2015 Webinar Series Pediatric Care Coordination: Beyond Policy, Practice, and Implementation A webinar series brought to you by the National Center for Medical Home Implementation Beyond Policy: Implementing Care Coordination in Practice March 30, 2015 Beyond Practice: Fostering Diverse Partnerships for Successful Care Coordination April 22, 2015 Beyond Implementation: Capturing the Value of Care Coordination May 28, 2015
4 AAP Care Coordination Policy Statement. Policy Statement from the American Academy of Pediatrics Patient- and Family-Centered Care Coordination: A Framework for Integrating Care for Children and Youth Across Multiple Systems Council on Children with Disabilities and Medical Home Implementation Project Advisory Committee Lead Authors: Renee M. Turchi, MD, MPH, FAAP & Richard C. Antonelli, MD, MS, FAAP Pediatrics, May 2014




5 Families are Key Members of the Team!!

6 Care Coordination is Important for ALL these Reasons and More!
7 Objectives for Today s Webinar State the value of measuring and evaluating care coordination activities within the context of improved patient experience, improved health of populations, and decreased cost of health care. Identify tools and strategies to facilitate the measurement of pediatric care coordination activities. Provide examples of how practices are utilizing care coordination performance metrics and methodologies to capture value for patients and families.

8 Beyond Implementation: Capturing the Value of Care Coordination brought to you by the National Center for Medical Home Implementation Richard Antonelli, MD, MS, FAAP Boston Children's Hospital Harvard Medical School National Center for Care Coordination Technical Assistance
9 Disclosures I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this activity. I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.
10 National Center for Care Coordination Technical Assistance (NCCCTA) The mission of the center is to support the promotion, implementation and evaluation of care coordination activities and measures in child health across the United States Contact: Hannah Rosenberg The National Center for Care Coordination Technical Assistance is working in partnership with the National Center for Medical Home Implementation (NCMHI) in the American Academy of Pediatrics. The NCMHI is supported by the Health Resources and Services Administration (HRSA) of the United States Department of Health and Human Services (HHS) grant number U43MC09134.

11 Pediatric Care Coordination Community (RI) States with entities that are in early stages of engagement. Expressed interest in developing care coordination workforce capacity on level of individual institution and/or state-wide program. + *some sites may have implemented since our last communication + + As of May 1, 2015 States with entities that have used the Pediatric Care Coordination Curriculum as a resource to implement care coordination workforce capacity building Across these states, as of May 1, 2015, we are aware of over 20 different institutions using the Pediatric Care Coordination Curriculum as a resource. + States engaged in statewide implementation, some partnering with Title V programs

12 Benefits of Developing a Community Sharing resources Not re-inventing the wheel Learning from others difficulties and successes Potential for collaboration
13 Framework for High Value Care Delivery Model Medical home is an essential component of high performing system, but it needs: Financing Work force development Resources which align with integrated care structures (ie, subspecialties) Technology Collaborative Care Models Integration is essential for success evidence exists!
14 Framework for High Value Care Delivery Model Care Coordination is necessary but not sufficient to achieve integration Care Coordination is the set of activities which occurs in the space between visits, providers, hospital stays, agency contacts Only way to succeed is to engage all stakeholders, including patients and families, as participants and partners

15 Implications for Accountability Measure at all levels of the system Transparency of performance Incentives supporting activities in the space between Education of work force Support for those activities Support for measurement

16 Boston Children s Hospital Integrated Care: Elements Which Support a Network of Care Across the Community Community-based Primary Care Health Centers and Private Practices Primary and Subspecialty Care Accessibility Care Coordination Tracking & Registry Linkage to in-country resources Integration with specialists Elements of Care Integration Inter-Professional Education Communications Portals Warm hand-offs Optimal Models of Care Disease Specific Care Pathways Collaborative Care Models Tele-health Care/ Utilization Management Outcomes / Value Quality Patient/ Family Experience Costs Boston Children s Hospital Centers of Excellence Population Health Integration Collaborator
17 BCH Integrated Care Program Selected Tools and Processes Care Coordination Capacity Building Pediatric Care Coordination Curriculum Care Coordination Measurement Care Coordination Measurement Tool Family Experience Measurement Pediatric Integrated Care Survey Assessing Hospital Discharge Readiness Care Transitions Measure-Pediatric Care Planning Shared Care Planning Approach, Care Coordination Strengths and Needs Assessment
18 How Care Coordination is Financed: Issues & Opportunities Fee-for-Service (FFS) FFS plus per member per month (PMPM) allowance Global Budget Caveats: Know TRUE costs of care Document care coordination activities and outcomes Affordable Care Act: Opportunities in Accountable Arrangements
19 Integrated Care Pilot Project - Neurology Working with strategic partners Enterprise leadership: physician/nursing/social work Family partners: Federation for Children with Special Needs (Mass Family Voices) Developing relationship with business community Payers National Business Group on Health Discussions re: value proposition of care coordination Outcomes tied to triple aim: better outcomes, better experience, reduced cost
20 Creating High Quality Handoffs What is a Handoff? Transfer of pertinent knowledge between members of a patient s care team, often conducted in anticipation of an upcoming patient encounter. What is the Goal of a High Quality Handoff? To enable the care team to maximize the value of every patient interaction by ensuring relevant knowledge learned by one part of a patient s care team is known to other members at the right time and place. 20
21 Creating High Quality Handoffs (cont d) What are the Elements of a High Quality Handoff? Goal of anticipated encounter, from perspective of the family and PCP Relevant clinical information (eg, clinical findings, labs, imaging results) Model of referral relationship (eg, one-time consult, on-going co-management) Time sensitivity of requests and action items in the care plan 21

22 Care Coordination Framework: Key Elements MA Child Health Quality Coalition CC Task Force

23 Beyond Implementation: Capturing the Value of Care Coordination brought to you by the National Center for Medical Home Implementation Hannah Rosenberg, MSc Boston Children s Hospital National Center for Care Coordination Technical Assistance hannah.rosenberg@childrens.harvard.edu
24 Disclosures I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this activity. I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.
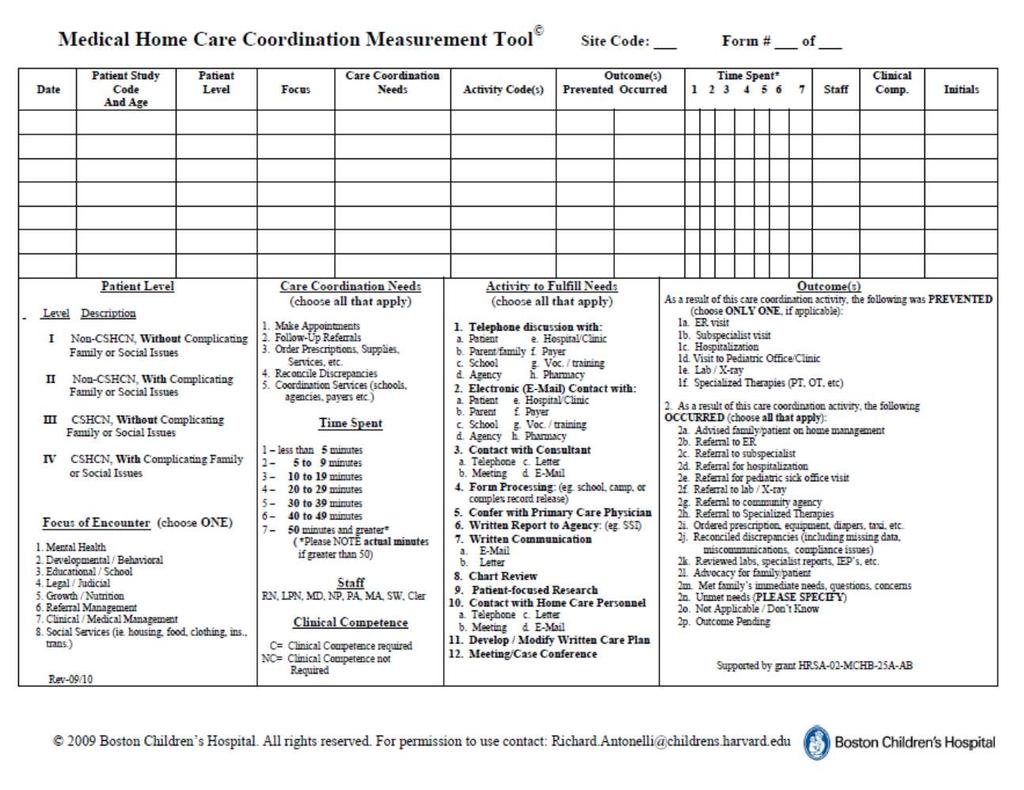
25 Care Coordination Measurement Tool (CCMT) Intended to be adapted to reflect activities and outcomes of teams in diverse settings Tool can be implemented in different ways depending on goal of collecting data for every encounter once a week every quarter, etc Paper version or web-based versions have been used in past In AHRQ Atlas, core tool can be found on BCH website:
26 CCMT Background CCMT is a value capture tool designed to track care coordination activities that are currently being done but not being accounted or reimbursed CCMT works to assign value to care coordination activities and get to a true cost of care Initially developed to be a tool used in pediatric primary care practices as a quality improvement initiative CCMT is intended to be adapted by the user/s CCMT is intended to address quality improvement and finance
27 CCMT Today Available in public domain on BCH website Many institutions are using CCMT to capture value of work that they are doing pediatric primary care adult primary care specialty clinics (inpatient and ambulatory) research settings family-partner organizations
28

29 Adaptation: Questions to Inform Process What is goal of using CCMT to collect data? What will data be used to inform? Who will be completing CCMT? What care coordination tasks do they currently perform? What outcomes occur/are prevented due to these care coordination activities? Does any tool validation need to occur? (further explained later)
30 Implementation: Questions to Inform Process What format will be used to complete CCMT? (Web/paper based?) How often will CCMT be completed? (Think: goal quality improvement/finance)
31 What to Focus on? Quality Improvement If practice/clinic/organization is: Focusing on re-assigning responsibilities/accountability, making sure everyone is working at top of their license In space where already moved from fee-for-service to global budgets Finance If practice/clinic/organization is: In space to inform conversations about financing options Validation (most necessary when addressing finance domain) In past, created vignettes, episode of care Posed to subject matter experts Inter-rater reliability
32 National Study of Care Coordination Measurement in Medical Homes Antonelli, Stille, and Antonelli, 2008 Focus of Encounter: Aggregate Data Primary Focus % Encounters Clinical/Medical Management 67 Referral Management 13 Social Services 7 Education/School 4 Developmental/Behavioral 3 Mental Health 3 Growth/Nutrition 2 Legal/Judicial 1
33 National Study of Care Coordination Measurement in Medical Homes Outcomes Prevented Aggregate Data (32%) of total 3855 CC encounters had something prevented Of the 1232 CC Encounters where prevention was noted as an outcome: Outcome Prevented # Care Coordination Encounters Visit to pediatric office/clinic Emergency department visit Subspecialist visit Percentage
34 National Study of Care Coordination Measurement in Medical Homes 62% of RN CC Encounters prevented something 33% of MD CC Encounters prevented something Non-revenue-generating office nurses drive the most system-level cost savings: avoidance of ED and office visits
 Before actual data is collected, complete trial using a paper version of the tool for staff to get used to using")
35 Suggestions Involve people who will be collecting data in the adaptation process Ensure that everyone using the tool is working from common definitions, terms (tip: vignettes are helpful in this case) Before actual data is collected, complete trial using a paper version of the tool for staff to get used to using tool
36 Steps to Get This Done Decision to Proceed Why? How long to commit? Expected Outcomes Create Episode of Care model Modify CCMT Implement CCMT Incorporate CCMT in electronic format
37 CCMT Use: Boston Children s Hospital Developed REDCap Tool Link available in EMR Spent time usability/feasibility testing Integrated Care Program Martha Eliot Health Center, Behavioral Health Population

38 Beyond Implementation: Capturing the Value of Care Coordination brought to you by the National Center for Medical Home Implementation David K. Urion, MD Boston Children's Hospital Department of Neurology
39 Disclosures I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this activity. I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.
40 40 Baseline Subspecialty Utilization


41 Department of Neurology, Boston Children s Hospital First phase of testing: feasibility/usability of CCMT in clinic
42 Current Quality of Referrals Integration Quality Initial Referrals into Neurology Presence of a referral request: 6.7% Presence of an in-house referral mentioned in a BCH clinical note: 33.3% For patients coming into these pilot sites, little documentation existed regarding source of referral, initial reason for the referral, and expectations of PCP, if any. Integration Quality for Follow-up Visits Follow-up visits generally have no structured mechanism by which the PCP communicates with the subspecialist about new or on-going expectations or needs. Communications are ad hoc or solely dependent on the patient, family, or caregiver to relay to other members of the patient s care team.
43 Closing the Loop Getting Results Where They Need to Be on Time Visits resulting in a lab order 47% Lab order completed 75% Family notified of the test results 77% Referring MD notified of the test results 38% Visits resulting in a consult order 21% Consult order completed 48% Neurologist received consult note 92% Findings based on close the loop measurements conducted for 130 visits across eight clinics in the Department of Neurology from May 2014 to February 2015.
44 Improving Care Transitions Using close the loop measures to confirm improvements in completing lab orders and communicating results in the Rett Clinic: Baseline measurements taken from October 2013 to March Intervention started April 2014 with weekly team conferences to discuss task ownership and order status. Process shifted to an electronic communication process to better fit the team s workflow. * Q data through January and February.


45 Pediatric Integrated Care Survey (PICS) In the Process of Validation Funded by Lucile Packard Foundation Children s Health More than one hundred families of children with complex care needs have responded to a survey designed to capture the family perspective on care integration.

46 Beyond Implementation: Capturing the Value of Care Coordination brought to you by the National Center for Medical Home Implementation Tami Chase, RN Nurse Manager Martha Eliot Health Center
47 Disclosures I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this activity. I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.

48 Martha Eliot puts CCMT into Practice Martha Eliot Health Care urban primary care practice essential part of its community for more than 40 years medical home serving lowincome housing development and greater Boston community 85% Medicaid, the patient population at Martha Eliot is vulnerable, with poor health status; sizeable CYSHCN population. Significant growth in the Mental Health Department is expected in
49 Utilizing the CCMT at Martha Eliot A new position for the Mental Health Department hired August 2014 The role of the RN provides a layer of clinical management, education, inter-visit and care coordination necessary to meet the complex needs of our population The vision of mental health services at Martha Eliot is to be a leader in the provision of community mental health care CCMT is improvised for Mental Health and used in the EHR CCMT captures data for six months

50 Martha Eliot Demonstrates the Use of CCMT 155 encounters were entered by the RN in a 3 month period between 12/11/14-3/11/15. Data demonstrates clinical expertise of a RN needed in the Mental Health Department Improvements were seen in: compliance to patient visits responsiveness to situation of high patient acuity improved rates in medication compliance preventable patient outcomes
51 Martha Eliot Demonstrates the Use of CCMT Example Data Points used: As a result of this care coordination activity, abrupt medication discontinuation by patient/caregiver was prevented 74.2% of the time (115 times) an encounter was recorded As a result of this care coordination activity, medication treatment continuity and compliance occurred 81.3% of the time (126 times) an encounter was recorded In 97.4% of the encounters recorded, clinical competence was required

52 Questions
53 Resources Patient- and Family-Centered Care Coordination: A Framework for Integrating Care for Children and Youth Across Multiple Systems (AAP Policy Statement) Building Your Medical Home: Care Coordination (Resource Guide) Fostering Partnership and Teamwork in the Pediatric Medical Home: A How-To Video Series National Center for Medical Home Implementation: Care Coordination (Additional care coordination resources)
54 And More Resources Pediatric Care Coordination Curriculum Care Coordination Measurement Tool Care Coordination Measures for Primary Care Practice (AHRQ) MA Child Health Quality Coalition National Center for Care Coordination Technical Assistance at Boston Children s Hospital Hannah Rosenberg, Manager: Hannah.Rosenberg@childrens.harvard.edu
55 We re Here to Help You! Have a question about medical home? Contact the National Center for Medical Home Implementation! Medical_home@aap.org Subscribe to our Listserv! 800/ ext 7605
One Family s Care Map.
 Richard C. Antonelli, MD, MS Medical Director of Integrated Care Boston Children s Hospital, Harvard Medical School Director, National Center for Care Coordination Technical Assistance November 20, 2015
Richard C. Antonelli, MD, MS Medical Director of Integrated Care Boston Children s Hospital, Harvard Medical School Director, National Center for Care Coordination Technical Assistance November 20, 2015
National Center for Care Coordination Technical Assistance (NCCCTA) Team
 Team") National Center for Care Coordination Technical Assistance (NCCCTA) Team Richard C Antonelli, MD, MS, FAAP Primary Care Pediatrician Medical Director of Integrated Care Boston Children s Hospital, Harvard
National Center for Care Coordination Technical Assistance (NCCCTA) Team Richard C Antonelli, MD, MS, FAAP Primary Care Pediatrician Medical Director of Integrated Care Boston Children s Hospital, Harvard
Care Coordination Measurement Tool Adaptation and Implementation Guide
 Care Coordination Measurement Tool Adaptation and Implementation Guide The Care Coordination Measurement Tool (CCMT) is of value to all that are attempting to quantitatively describe care coordination
Care Coordination Measurement Tool Adaptation and Implementation Guide The Care Coordination Measurement Tool (CCMT) is of value to all that are attempting to quantitatively describe care coordination
Walking before Running: Developing Care Coordination Capacity to Achieve High Value Outcomes for Patients with Behavioral Health Needs
 Walking before Running: Developing Care Coordination Capacity to Achieve High Value Outcomes for Patients with Behavioral Health Needs Presenter: Richard Antonelli, MD, Medical Director, Integrated Care
Walking before Running: Developing Care Coordination Capacity to Achieve High Value Outcomes for Patients with Behavioral Health Needs Presenter: Richard Antonelli, MD, Medical Director, Integrated Care
Medical Home Network Connect. Implementing PCMH Practices through MHNConnect technology
 Medical Home Network Connect Implementing PCMH Practices through MHNConnect technology Disclosures I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or
Medical Home Network Connect Implementing PCMH Practices through MHNConnect technology Disclosures I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or
Measuring Family Experience of Care Integration to Improve Care Delivery
 Measuring Family Experience of Care Integration to Improve Care Delivery Thursday, June 15, 2017 10-10:30 a.m. PT, 1-1:30 p.m. ET Sponsored by Lucile Packard Foundation for Children's Health Catalyst Center
Measuring Family Experience of Care Integration to Improve Care Delivery Thursday, June 15, 2017 10-10:30 a.m. PT, 1-1:30 p.m. ET Sponsored by Lucile Packard Foundation for Children's Health Catalyst Center
College-wide Patient-Centered Medical Home Program Meharry Medical College
 + The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
+ The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
National Health Policy Forum Richard C. Antonelli, MD, MS Boston Children s Hospital Harvard Medical School November 08, 2013
 National Health Policy Forum Richard C. Antonelli, MD, MS Boston Children s Hospital Harvard Medical School November 08, 2013 Understand the potential strengths of family- and patient-centered Medical
National Health Policy Forum Richard C. Antonelli, MD, MS Boston Children s Hospital Harvard Medical School November 08, 2013 Understand the potential strengths of family- and patient-centered Medical
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
Measure Applications Partnership (MAP)
") Measure Applications Partnership (MAP) Uniform Data System for Medical Rehabilitation Annual Conference Aisha Pittman, MPH Senior Program Director National Quality Forum August 9, 2012 Overview MAP Background
Measure Applications Partnership (MAP) Uniform Data System for Medical Rehabilitation Annual Conference Aisha Pittman, MPH Senior Program Director National Quality Forum August 9, 2012 Overview MAP Background
Issue Brief March 2017
 Issue Brief March 2017 Survey: Quantifying Pediatricians Views on Caring for Children with Special Health Care Needs by Kris Calvin, Megumi Okumura, MD, and Heather Knauer Introduction Children, especially
Issue Brief March 2017 Survey: Quantifying Pediatricians Views on Caring for Children with Special Health Care Needs by Kris Calvin, Megumi Okumura, MD, and Heather Knauer Introduction Children, especially
Brave New World: The Effects of Health Reform Legislation on Hospitals. HFMA Annual National Meeting, Las Vegas, Nevada
 Brave New World: The Effects of Health Reform Legislation on Hospitals HFMA Annual National Meeting, Las Vegas, Nevada Highlights of PPACA Requires most Americans to have health insurance Expands coverage
Brave New World: The Effects of Health Reform Legislation on Hospitals HFMA Annual National Meeting, Las Vegas, Nevada Highlights of PPACA Requires most Americans to have health insurance Expands coverage
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
The Patient Centered Medical Home: 2011 Status and Needs Study
 The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
Blue Cross Blue Shield of Michigan Advancing to the Next Generation of Value Based Pay for Performance
 Blue Cross Blue Shield of Michigan Advancing to the Next Generation of Value Based Pay for Performance Physician Group Incentive Program, Patient Centered Medical Homes, and Moving From Fee for Service
Blue Cross Blue Shield of Michigan Advancing to the Next Generation of Value Based Pay for Performance Physician Group Incentive Program, Patient Centered Medical Homes, and Moving From Fee for Service
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model. The New Accountable Care Business Model
 Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
Sandra Robinson, RN, MSN, ACM, CEN
 Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
DOI: /peds
 Care Coordination for Children and Youth With Special Health Care Needs: A Descriptive, Multisite Study of Activities, Personnel Costs, and Outcomes Richard C. Antonelli, Christopher J. Stille and Donna
Care Coordination for Children and Youth With Special Health Care Needs: A Descriptive, Multisite Study of Activities, Personnel Costs, and Outcomes Richard C. Antonelli, Christopher J. Stille and Donna
A Collection of Strategies Used to Support Innovative and Promising Practices in Pediatric Medical Home Implementation
 A Collection of Strategies Used to Support Innovative and Promising Practices in Pediatric Medical Home Implementation Müge Chavdar, MPH and Joan Jeung, MD, MPH, FAAP This publication of the National Center
A Collection of Strategies Used to Support Innovative and Promising Practices in Pediatric Medical Home Implementation Müge Chavdar, MPH and Joan Jeung, MD, MPH, FAAP This publication of the National Center
The Michigan Primary Care Transformation (MiPCT) Project. PGIP Meeting Update March 09, 2012
 Project. PGIP Meeting Update March 09, 2012") The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
National Center for Medical Home Implementation and National Center for Cultural Competence
 Language Access in Pediatric Primary Care National Center for Medical Home Implementation and National Center for Cultural Competence The National Center for Medical Home Implementation is a cooperative
Language Access in Pediatric Primary Care National Center for Medical Home Implementation and National Center for Cultural Competence The National Center for Medical Home Implementation is a cooperative
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Building a Multi-System Clinically Integrated Network
 Building a Multi-System Clinically Integrated Network 22 nd Annual AHA Leadership Summit July 2014 Valence Health Has Been Helping Provider Organizations Progress Toward Value-Based Care Since 1996 Technology-enabled
Building a Multi-System Clinically Integrated Network 22 nd Annual AHA Leadership Summit July 2014 Valence Health Has Been Helping Provider Organizations Progress Toward Value-Based Care Since 1996 Technology-enabled
Financing and Sustainability Strategies for Behavioral Health Integration Anna Ratzliff, MD, PhD Associate Director for Education AIMS Center
 Financing and Sustainability Strategies for Behavioral Health Integration Anna Ratzliff, MD, PhD Associate Director for Education AIMS Center Advancing Integrated Mental Health Solutions The Healthier
Financing and Sustainability Strategies for Behavioral Health Integration Anna Ratzliff, MD, PhD Associate Director for Education AIMS Center Advancing Integrated Mental Health Solutions The Healthier
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Pediatric Learning Network: Adopting PFE Strategies to Improve Pediatric Asthma Care
 Pediatric Learning Network: Adopting PFE Strategies to Improve Pediatric Asthma Care Lesson 5: Connecting patients/families with appropriate supports and services PCPCC Support and Alignment Network Quality
Pediatric Learning Network: Adopting PFE Strategies to Improve Pediatric Asthma Care Lesson 5: Connecting patients/families with appropriate supports and services PCPCC Support and Alignment Network Quality
The influx of newly insured Californians through
 January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
Roll Out of the HIT Meaningful Use Standards and Certification Criteria
 Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
RPC and OMH Collaborative Care Webinar. February 1, pm
 RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
Red Carpet Care: Intensive Case Management Program for Super-Utilizers
 Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Centers for Medicare & Medicaid Services: Innovation Center New Direction
 Centers for Medicare & Medicaid Services: Innovation Center New Direction I. Background One of the most important goals at CMS is fostering an affordable, accessible healthcare system that puts patients
Centers for Medicare & Medicaid Services: Innovation Center New Direction I. Background One of the most important goals at CMS is fostering an affordable, accessible healthcare system that puts patients
State Title V Health Care Transition Performance Objectives and Strategies: Current Snapshot and Suggestions
 REPORT No.1 F E B R U A R Y 2 0 1 6 State Title V Health Care Transition Performance Objectives and Strategies: Current Snapshot and Suggestions Prepared by Margaret McManus, MHS; Daniel Beck, MA; and
REPORT No.1 F E B R U A R Y 2 0 1 6 State Title V Health Care Transition Performance Objectives and Strategies: Current Snapshot and Suggestions Prepared by Margaret McManus, MHS; Daniel Beck, MA; and
Meaningful Use Stage 2
 Meaningful Use Stage 2 Objectives Gain understanding of the changes Focus on Transitions in Care and Patient Engagement Recognize the increasing HIE role Who Are You? What is YOUR Need Today? A. Office
Meaningful Use Stage 2 Objectives Gain understanding of the changes Focus on Transitions in Care and Patient Engagement Recognize the increasing HIE role Who Are You? What is YOUR Need Today? A. Office
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
TRANSITION PREPARATION
 Health Care Transition & Title V Care Coordination Initiatives: Webinar Series Webinar # 2 March 28, 2018 TRANSITION PREPARATION Michelle Jiggetts, MD, MS, MBA Program Administrator Complex Care Program
Health Care Transition & Title V Care Coordination Initiatives: Webinar Series Webinar # 2 March 28, 2018 TRANSITION PREPARATION Michelle Jiggetts, MD, MS, MBA Program Administrator Complex Care Program
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
SENTINEL METHODS SENTINEL MEDICAL CHART REVIEW GAP ANALYSIS PUBLIC REPORT
 SENTINEL METHODS SENTINEL MEDICAL CHART REVIEW GAP ANALYSIS PUBLIC REPORT Prepared by: Adee Kennedy, MS, MPH, 1 Hana Lipowicz, MPH, 1 Ella Pestine, MPH, 1 Carolyn Balsbaugh, MPH, 1 Meighan Rogers Driscoll,
SENTINEL METHODS SENTINEL MEDICAL CHART REVIEW GAP ANALYSIS PUBLIC REPORT Prepared by: Adee Kennedy, MS, MPH, 1 Hana Lipowicz, MPH, 1 Ella Pestine, MPH, 1 Carolyn Balsbaugh, MPH, 1 Meighan Rogers Driscoll,
Implementing and Improving: Behavioral Health Quality
 Implementing and Improving: Behavioral Health Quality National Collaborative for Innovation in Quality Measurement Sarah Hudson Scholle, MPH, DrPH March 21, 2017 Agenda Alignment of measures and accountability
Implementing and Improving: Behavioral Health Quality National Collaborative for Innovation in Quality Measurement Sarah Hudson Scholle, MPH, DrPH March 21, 2017 Agenda Alignment of measures and accountability
The Pennsylvania Chronic Care Initiative
 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
ACO Model Fits Pediatrics Well
 ACOs and Pediatrics James M. Perrin, MD, FAAP Professor of Pediatrics, Harvard Medical School John C. Robinson Chair of Pediatrics, Associate Chair MassGeneral Hospital for Children Immediate Past President,
ACOs and Pediatrics James M. Perrin, MD, FAAP Professor of Pediatrics, Harvard Medical School John C. Robinson Chair of Pediatrics, Associate Chair MassGeneral Hospital for Children Immediate Past President,
TX Action Learning Collaborative: National Standards for Systems of Care for CYSHCN
 TX Action Learning Collaborative: National Standards for Systems of Care for CYSHCN January 21, 2015. Children s Policy Council 1 http://www.amchp.org/aboutamchp/newsletters/member-briefs/documents/standards%20charts%20final.pdf
TX Action Learning Collaborative: National Standards for Systems of Care for CYSHCN January 21, 2015. Children s Policy Council 1 http://www.amchp.org/aboutamchp/newsletters/member-briefs/documents/standards%20charts%20final.pdf
State Health Department Support for Community Health Worker (CHW) Workforce Development and Engagement
 Workforce Development and Engagement") State Health Department Support for Community Health Worker (CHW) Workforce Development and Engagement Association of State and Territorial Health Officials Technical Assistance August 2017 Guiding principle:
State Health Department Support for Community Health Worker (CHW) Workforce Development and Engagement Association of State and Territorial Health Officials Technical Assistance August 2017 Guiding principle:
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Community Health Worker Integration: Issues and Options for State Health Departments
 Community Health Worker Integration: Issues and Options for State Health Departments ASTHO TECHNICAL ASSISTANCE PRESENTATION MULTI-STATE LEARNING COMMUNITY AUGUST 16, 2017 This webinar is supported by
Community Health Worker Integration: Issues and Options for State Health Departments ASTHO TECHNICAL ASSISTANCE PRESENTATION MULTI-STATE LEARNING COMMUNITY AUGUST 16, 2017 This webinar is supported by
Complex Patient Care Redesign: ThedaCare Innovation. Gregory Long, MD Chief Medical Officer
 Complex Patient Care Redesign: ThedaCare Innovation Gregory Long, MD Chief Medical Officer ThedaCare Northeastern Wisconsin An Integrated Community Health System; >7000 employees Primary service area of
Complex Patient Care Redesign: ThedaCare Innovation Gregory Long, MD Chief Medical Officer ThedaCare Northeastern Wisconsin An Integrated Community Health System; >7000 employees Primary service area of
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In?
 Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Health Information Technology
 ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
Here is what we know. Here is what you can do. Here is what we are doing.
 With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1)
") Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1) Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Professor and Chair Titus Family Department of Clinical
Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1) Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Professor and Chair Titus Family Department of Clinical
Issue Brief. EHR-Based Care Coordination Performance Measures in Ambulatory Care
 November 2011 Issue Brief EHR-Based Care Coordination Performance Measures in Ambulatory Care Kitty S. Chan, Jonathan P. Weiner, Sarah H. Scholle, Jinnet B. Fowles, Jessica Holzer, Lipika Samal, Phillip
November 2011 Issue Brief EHR-Based Care Coordination Performance Measures in Ambulatory Care Kitty S. Chan, Jonathan P. Weiner, Sarah H. Scholle, Jinnet B. Fowles, Jessica Holzer, Lipika Samal, Phillip
Wisconsin State Plan to Serve More Children and Youth within Medical Homes
 Wisconsin State Plan to Serve More Children and Youth within Medical Homes Including those with special health care needs Acknowledgments The Wisconsin Children and Youth with Special Health Care Needs
Wisconsin State Plan to Serve More Children and Youth within Medical Homes Including those with special health care needs Acknowledgments The Wisconsin Children and Youth with Special Health Care Needs
MACRA Frequently Asked Questions
 Following the release of the Quality Payment Program Interim Final Rule, the American Medical Association (AMA) conducted numerous informational and training sessions for physicians and medical societies.
Following the release of the Quality Payment Program Interim Final Rule, the American Medical Association (AMA) conducted numerous informational and training sessions for physicians and medical societies.
Integrated Health System
 Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Community Health Worker Integration: Issues and Options for State Health Departments
 Community Health Worker Integration: Issues and Options for State Health Departments Association of State and Territorial Health Officials Technical Assistance August 2017 Presenters Lucia Colindres-Vasquez,
Community Health Worker Integration: Issues and Options for State Health Departments Association of State and Territorial Health Officials Technical Assistance August 2017 Presenters Lucia Colindres-Vasquez,
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Medical Home Renovations: A Patient-centered Medical Home Case Study
 Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
ACADEMIC GROUP PRACTICE AND THE LEADERSHIP OF APRN S
 ACADEMIC GROUP PRACTICE AND THE LEADERSHIP OF APRN S Margaret Head, Chief Operating Officer/Chief Nursing Officer Susan Moseley Gent, Administrative Director Vanderbilt Medical Group March 10, 2012 With
ACADEMIC GROUP PRACTICE AND THE LEADERSHIP OF APRN S Margaret Head, Chief Operating Officer/Chief Nursing Officer Susan Moseley Gent, Administrative Director Vanderbilt Medical Group March 10, 2012 With
Health Care Transition for Youth with Special Health Care Needs (YSHCN)
") Health Care Transition for Youth with Special Health Care Needs (YSHCN) Stephanie Lawrence, MD Assistant Professor Division of General Internal Medicine Department of Internal Medicine and Pediatrics The
Health Care Transition for Youth with Special Health Care Needs (YSHCN) Stephanie Lawrence, MD Assistant Professor Division of General Internal Medicine Department of Internal Medicine and Pediatrics The
KPMG Digital Health Pulse April 2017
 KPMG Digital Health Pulse 2017 April 2017 Research purpose and design To identify key perceptions about the pace of digital health adoption and key challenges to implementing virtual care programs at hospitals
KPMG Digital Health Pulse 2017 April 2017 Research purpose and design To identify key perceptions about the pace of digital health adoption and key challenges to implementing virtual care programs at hospitals
Payer Perspectives On Value-based Contracting
 Payer Perspectives On Value-based Contracting Miles Snowden, MD, MPH, CEBS Chief Medical Officer 1 A simple goal Making the health system work better for everyone 2 Optum serves 60,000,000+ individuals
Payer Perspectives On Value-based Contracting Miles Snowden, MD, MPH, CEBS Chief Medical Officer 1 A simple goal Making the health system work better for everyone 2 Optum serves 60,000,000+ individuals
Denise Hudson, NR-CMA Health Informatics Specialist Health Services Advisory Group (HSAG) August 10, 2018
 August 10, 2018") Countdown to MIPS* Data Submission Webinar Series Preparing for Fall Without Falling Behind Denise Hudson, NR-CMA Health Informatics Specialist Health Services Advisory Group (HSAG) August 10, 2018 *Merit-based
Countdown to MIPS* Data Submission Webinar Series Preparing for Fall Without Falling Behind Denise Hudson, NR-CMA Health Informatics Specialist Health Services Advisory Group (HSAG) August 10, 2018 *Merit-based
Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP)
 & Patient-Centered Specialty Practice (PCSP)") Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP) Foundation for a Better Health Care System Presenter Jeanette Ikan, M.D., MHAI Objectives: Definition and benefits of PCMH,
Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP) Foundation for a Better Health Care System Presenter Jeanette Ikan, M.D., MHAI Objectives: Definition and benefits of PCMH,
What is a Pathways HUB?
 What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
New York State s Ambitious DSRIP Program
 New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
SAMPLE STRATEGIES AND EVIDENCE-BASED OR -INFORMED STRATEGY MEASURES
 SAMPLE STRATEGIES AND EVIDENCE-BASED OR -INFORMED STRATEGY MEASURES Compiled by the Strengthen the Evidence for Maternal and Child Health Programs Initiative: Strengthen the Evidence is a collaborative
SAMPLE STRATEGIES AND EVIDENCE-BASED OR -INFORMED STRATEGY MEASURES Compiled by the Strengthen the Evidence for Maternal and Child Health Programs Initiative: Strengthen the Evidence is a collaborative
Patient-Centered Medical Homes in Rural and Underserved Areas: A Webinar and Peer Discussion for Primary Care Offices
 Patient-Centered Medical Homes in Rural and Underserved Areas: A Webinar and Peer Discussion for Primary Care Offices Association of State and Territorial Health Officials (ASTHO) August 17, 2016 Dial-In
Patient-Centered Medical Homes in Rural and Underserved Areas: A Webinar and Peer Discussion for Primary Care Offices Association of State and Territorial Health Officials (ASTHO) August 17, 2016 Dial-In
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Transforming Clinical Care: Why Optimization of Clinical Systems Can t Wait
 Transforming Clinical Care: Why Optimization of Clinical Systems Can t Wait A White Paper March 2016 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800-680-7570 Impact-Advisors.com
Transforming Clinical Care: Why Optimization of Clinical Systems Can t Wait A White Paper March 2016 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800-680-7570 Impact-Advisors.com
Clinician Information Packet: Transition from Pediatric to Adult Care
 Clinician Information Packet: Transition from Pediatric to Adult Care 1 This packet contains information about: Processes for planning, transferring and integrating patients into adult care How to incorporate
Clinician Information Packet: Transition from Pediatric to Adult Care 1 This packet contains information about: Processes for planning, transferring and integrating patients into adult care How to incorporate
Primary Care Transformation in the Era of Value
 Primary Care Transformation in the Era of Value CMS Innovation Center & Primary Care Bruce Finke, MD Janel Jin, MSPH Gabrielle Schechter, MPH Center for Medicare & Medicaid Innovation Centers for Medicare
Primary Care Transformation in the Era of Value CMS Innovation Center & Primary Care Bruce Finke, MD Janel Jin, MSPH Gabrielle Schechter, MPH Center for Medicare & Medicaid Innovation Centers for Medicare
Michigan Primary Care Association
 Michigan Primary Care Association Improving Outcomes Finance & Quality through Integrated Information Conference June 2-3, 2016 Shanty Creek Resorts Bellaire, MI Definition and Purpose HRSA s Health Center
Michigan Primary Care Association Improving Outcomes Finance & Quality through Integrated Information Conference June 2-3, 2016 Shanty Creek Resorts Bellaire, MI Definition and Purpose HRSA s Health Center
The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs
 The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs Medical Group Management Association (MGMA ) publications are intended to provide current and accurate information and
The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs Medical Group Management Association (MGMA ) publications are intended to provide current and accurate information and
Serving CYSHCN in Medicaid Managed Care: Contract Language and the Contracting Process
 Serving CYSHCN in Medicaid Managed Care: Contract Language and the Contracting Process November 16, 2017 1:00-2:00 PM, ET For audio: 888-757-2790 Passcode: 105799 Press *6 to mute/unmute your line. Please
Serving CYSHCN in Medicaid Managed Care: Contract Language and the Contracting Process November 16, 2017 1:00-2:00 PM, ET For audio: 888-757-2790 Passcode: 105799 Press *6 to mute/unmute your line. Please
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards
 and the NCQA PCMH 2011 Standards") Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
Anastasia Dodson Associate Director for Policy California Department of Health Care Services 1501 Capitol Avenue Sacramento, CA 95814
 - CALIFORNIA CHILDREN'S HOSPITAL ASSOCIATIO N May 26, 2015 Anastasia Dodson Associate Director for Policy California Department of Health Care Services 1501 Capitol Avenue Sacramento, CA 95814 1215 K STREET
- CALIFORNIA CHILDREN'S HOSPITAL ASSOCIATIO N May 26, 2015 Anastasia Dodson Associate Director for Policy California Department of Health Care Services 1501 Capitol Avenue Sacramento, CA 95814 1215 K STREET
Center for Community Health Navigation at NewYork-Presbyterian Hospital
 Center for Community Health Navigation at NewYork-Presbyterian Hospital CENTER MISSION Mission: To support the health and wellbeing of patients through the delivery of culturallysensitive, peer-based support
Center for Community Health Navigation at NewYork-Presbyterian Hospital CENTER MISSION Mission: To support the health and wellbeing of patients through the delivery of culturallysensitive, peer-based support
Mina Li, MD., PhD., CSM Institute for Disability Studies (IDS) The University of Southern Mississippi
 The University of Southern Mississippi") Mina Li, MD., PhD., CSM Institute for Disability Studies (IDS) The University of Southern Mississippi October 9, 2010 Who are CYSHCN? Children/Youth with Special Health Care Needs (CYSHCN) are those who
Mina Li, MD., PhD., CSM Institute for Disability Studies (IDS) The University of Southern Mississippi October 9, 2010 Who are CYSHCN? Children/Youth with Special Health Care Needs (CYSHCN) are those who
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Strategic Plan. Becoming the Preferred Academic Medical Center of the 21st Century ONEUABMedicine.org/AMC21
 ENGAGEMENT QUALITY FINANCE ADVANCEMENT OF KNOWLEDGE FOUNDATIONS Strategic Plan Becoming the Preferred Academic Medical Center of the 21st Century ONEUABMedicine.org/AMC21 TABLE OF CONTENTS Overview...3
ENGAGEMENT QUALITY FINANCE ADVANCEMENT OF KNOWLEDGE FOUNDATIONS Strategic Plan Becoming the Preferred Academic Medical Center of the 21st Century ONEUABMedicine.org/AMC21 TABLE OF CONTENTS Overview...3
California s Health Homes Program
 California s Health Homes Program HPSM Network Webinar 9/05/18 Goals for Today: Health Homes Program overview CB-CME requirements Program readiness and implementation timeline Gather take-away questions
California s Health Homes Program HPSM Network Webinar 9/05/18 Goals for Today: Health Homes Program overview CB-CME requirements Program readiness and implementation timeline Gather take-away questions
1:00pm EST Webinar will begin shortly.
 Community Health Workers: Part of the Solution for Advancing Health Equity; Perspectives and Initiatives from the New England Regional Health Equity Council 1:00pm EST Webinar will begin shortly. Community
Community Health Workers: Part of the Solution for Advancing Health Equity; Perspectives and Initiatives from the New England Regional Health Equity Council 1:00pm EST Webinar will begin shortly. Community
Alternative Managed Care Reimbursement Models
 Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Developing a Medical-Legal Partnership in Rural Appalachia
 Developing a Medical-Legal Partnership in Rural Appalachia HRSA Disclaimer Community Health Partners for Sustainability, a program of the National Nurse-Led Care Consortium, is supported by the Health
Developing a Medical-Legal Partnership in Rural Appalachia HRSA Disclaimer Community Health Partners for Sustainability, a program of the National Nurse-Led Care Consortium, is supported by the Health
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Improving Diabetes Care in 75 Minutes. Moderator: Jerry Penso, M.D., M.B.A., President & CEO, AMGA
 Improving Diabetes Care in 75 Minutes Moderator: Jerry Penso, M.D., M.B.A., President & CEO, AMGA SESSION OBJECTIVES 1. Identify specific tactics that health care delivery systems can implement to improve
Improving Diabetes Care in 75 Minutes Moderator: Jerry Penso, M.D., M.B.A., President & CEO, AMGA SESSION OBJECTIVES 1. Identify specific tactics that health care delivery systems can implement to improve
Practice Transformation Networks
 Practice Transformation Networks The project described was supported by Funding Opportunity Number CMS-1L1-15-003 from the U. S. Department of Health & Human Services, Centers for Medicare and Medicaid
Practice Transformation Networks The project described was supported by Funding Opportunity Number CMS-1L1-15-003 from the U. S. Department of Health & Human Services, Centers for Medicare and Medicaid
MPA Reference Guide. Millennium Collaborative Care
 Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from