WISCONSIN OMBUDSMAN PROGRAMS FOR MLTSS
|
|
|
- Sabina Brooks
- 6 years ago
- Views:
Transcription
1 WISCONSIN OMBUDSMAN PROGRAMS FOR MLTSS September 9, 2013 Kim Marheine Ombudsman Services Supervisor State of Wisconsin Board on Aging and Long Term Care Lea Kitz Program Manager Family Care & IRIS Ombudsman Program Disability Rights Wisconsin 1
2 ADULT LTC SYSTEM OVERVIEW Target Groups: Adults with Physical Disabilities Adults with Developmental Disabilities Frail Elderly 2
3 GOALS OF WISCONSIN S FAMILY CARE PROGRAM Family Care is a comprehensive and flexible long-term care service system, which strives to foster people s independence and quality of life, while recognizing the need for interdependence and support. Goals of the Family Care Initiative Choice Give people better choices about the services and supports available to meet their needs Access Improve people s access to services Quality Improve the overall quality of the long-term care system by focusing on achieving people s health and social outcomes Cost-Effectiveness Create a cost-effective long-term care system for the future. 3
4 ADULT LTC SYSTEM OVERVIEW Entry Point: Aging and Disability Resource Center Determines functional eligibility (and facilitates financial eligibility determination with Income Maintenance Consortium) If eligible, neutral Options Counseling is provided 4
5 ADULT LTC SYSTEM OVERVIEW Adult LTC Options FAMILY CARE Managed Care Organization (includes Family Care, Partnership or PACE) MCO receives same capitated rate for each member MCO uses capitated rate to cover all administrative and service costs MCO develops provider network and contracts with providers MCO care team develops and manages Supports/Services plan Include, Respect, I Self-direct (IRIS) Self-Directed Services Fee for Service MA Participant is given allocation Ppt develops Supports/Services plan that meets waiver definitions and keeps budget within allocation Ppt negotiates with providers or hires workers Ppt receives help from a Financial Services Agency and an IRIS Consultant Services Agency 5
, which manages and enforces the contract.")
6 Managed Care Organizations: MCOs in Wisconsin are locally grown each covers multiple counties, and in some counties, members have a choice of MCOs. Currently, MCOs are either private, nonprofit or quasi-governmental LTC districts. All MCOs contract with the Dept. of Health Services (DHS), which manages and enforces the contract. Procurement is every 5 years; 57 of 72 counties have Family Care & IRIS. Financials and risk are regulated by the state Office of the Commissioner on Insurance (OCI). 40,367 members in Family Care, Partnership and PACE currently 6
, which helps participants in their roles of employer authority and budget authority ; and the IRIS Consultant Agency")
7 IRIS: IRIS is offered wherever Family Care is offered. IRIS is administered by the Dept. of Health Services and 2 statewide contractors the Financial Services Agency (FSA), which helps participants in their roles of employer authority and budget authority ; and the IRIS Consultant Agency (ICA), which helps participants understand the program, and helps with plan development. Nearly 9,000 participants in IRIS currently. 7
8 OVERVIEW OF WISCONSIN OMBUDSMAN SERVICES FOR ADULTS IN MLTSS & IRIS BOALTC: Serves members in Family Care aged 60 or more Program added to existing LTC Ombudsman Program Independent state agency FCIOP: Serves members of Family Care or IRIS with PD and DD aged Program developed to provide this service State DHS contracts with P&A 8
9 WISCONSIN S MLTSS OMBUDSMAN PROGRAMS Types of Individual Assistance o Information and Education o Investigation and informal negotiation with Managed Care Organizations (MCOs), the IRIS Program, and Aging and Disability Resource Centers (ADRCs) o Technical Assistance to prepare for appeals hearings or representation All services are free Services can be requested at any point 9
10 WISCONSIN S MLTSS OMBUDSMAN PROGRAMS Systems work o Identify trends and patterns o Provide red flag of emerging issues to Dept. of Health Services o Provide feedback during policy development or changes in program Maintain positive working relationships with MCOs, ADRCs, IRIS contractors, & DHS BOALTC and FCIOP work together to address due process or member rights issues 10
11 BOALTC S FAMILY CARE OMBUDSMAN PROGRAM Functions as a state agency, independent of DHS, regulation and licensing Ombudsman program for people in managed care was added to existing LTC ombudsman services during pilot phase, then de-funded. Re-established by legislative rule 6 years later. Currently 15 regional ombudsmen; supported by a program supervisor, and complemented by a relocation specialist, intake specialist and legal counsel. Case ratio of ~1 : 6,500 11
12 BOALTC S FAMILY CARE OMBUDSMAN PROGRAM Not just typical ombudsman work o In 2008 added one FTE to be designated to Family Care. Immediately cross-trained all ombudsmen due to increase in casework o Made intentional outreach to all MCO s and ADRC s to inform of function of the ombudsman program. DHS issued a memo outlining an expectation for collaboration with advocates. 12
13 BOALTC S FAMILY CARE OMBUDSMAN PROGRAM Not just typical ombudsman work o Initially relationships with MCO s appeared to be more adversarial than collaborative culture misalignment between ombudsmen accustomed to a person-centered framework and MCOs seemingly with a contract-centered framework o Ombudsmen doing typical LTC work prioritize own responsibilities, based on needs of callers. In MLTSS, ombudsman work is often prioritized by the appeal process (members not always timely when requesting advocacy). FC cases often take priority to avoid loss of services or appeal rights. 13
14 BOALTC S FAMILY CARE OMBUDSMAN PROGRAM Comparing Typical LTC Advocacy to MLTSS Advocacy Facility-Based LTC Advocacy: Facilities call for consults, problem-resolution in advance of action Relationships largely collaborative, residentfocused and centered on improving quality of care Ability to collaborate on interpretation of some regulatory guidance MLTSS-Based Advocacy: After advocacy is requested by member, attempt to informally resolve issue Relationships seemingly centered on contract compliance; some MCOs collaborate more easily than others Contract focus very black and white. Best resolution when able to problem-solve informally before decision 14
15 BOALTC S FAMILY CARE OMBUDSMAN PROGRAM Comparing Typical LTC Advocacy to MLTSS Advocacy Facility-Based LTC Advocacy: Complaint resolution by mediation, negotiation, collaboration Easy and immediate access to residents, records, personnel; complaints resolve in days or weeks Residents in facilities have constants: caregivers, medical and social services, equipment, supports, access to community MLTSS-Based Advocacy: Complaint resolution NOAbased, formal appeals & grievance structure Access to records and personnel can be challenging and timeconsuming; complaints resolve most often in several months FC members seem to have few constants, and all changeable dependent on annual contract changes, re-screens, new tools, sustainability measures 15
16 BOALTC S FAMILY CARE OMBUDSMAN PROGRAM Comparing Typical LTC Advocacy to MLTSS Advocacy Facility-Based LTC Advocacy: Care & treatment issues (med management, misappropriation, failure to follow care plan, etc.) trigger regulatory action Retaliation less probable due to constant supports staff, room-mates, volunteers Efforts at promoting selfadvocacy occur over time, during repeated facility visits MLTSS-Based Advocacy: Care and treatment issues of contracted care management units, providers addressed by MCO Retaliation a great concern, as fewer persons in and out of member s home Efforts at promoting selfadvocacy are very focused, with little opportunity for status checks 16
17 DRW S FAMILY CARE & IRIS OMBUDSMAN PROGRAM (FCIOP) FCIOP is a program authorized by state statute and funded through (DHS) After a competitive procurement process, contract was awarded to Disability Rights Wisconsin (DRW) in 2009; contract is administered by DHS Currently 8 ombudsmen working out of 3 offices across the state; supported by a program attorney and a program manager. Case ratio of ~1 : 3,500 17
18 DRW S FAMILY CARE & IRIS OMBUDSMAN PROGRAM (FCIOP) Ombudsmen o Case Management Open cases after referred by DRW Intake Specialist Investigate get signatures and collect records Help client frame the issue and develop support materials Set advocacy strategy and adjust as needed Proceed with goal of resolving issue; informal negotiation preferred, but state fair hearing is often requested o Representation Ombudsmen may represent client at state fair hearing or provide extensive technical assistance 18
19 DRW S FAMILY CARE & IRIS OMBUDSMAN PROGRAM (FCIOP) Program Attorney o Provides regular case check-in s with each ombudsman on each case to ensure: Appropriate advocacy strategy Ensure cases are making progress Provide legal support and advice, including technical assistance for clients preparing for appeals hearings o Advises Program Manager of trends/patterns that should be addressed o Represents or provides representation support for ombudsmen at state fair hearing 19
20 DRW S FAMILY CARE & IRIS OMBUDSMAN PROGRAM (FCIOP) Program Manager o Provides overall case supervision o Works directly with DHS officials on systems issues o Gets directly involved with particularly complex cases or those that may need state intervention o Responsible for outreach o Manages all program personnel, including recruitment, training and ongoing development 20
21 DRW S FAMILY CARE & IRIS OMBUDSMAN PROGRAM (FCIOP) FCIOP is a program within the Protection & Advocacy agency, DRW, but has a firewall that prevents sharing of client services FCIOP is, however, able to use the P&A expertise on Medicaid and Medicare issues, especially in the areas of due process 21
22 SOME DIFFERENCES IN WHAT THE 2 PROGRAMS HANDLE Facilities Complaints Rate Disputes or Contract Issues Ongoing Case Management Caller for Assistance is Someone Besides Member or Member Representative BOALTC Yes No No Yes FCIOP No No No No 22
23 APPEALS, GRIEVANCES AND FAIR HEARINGS Member makes request for new or changed services to MCO; requests are either supported or denied. If denied, member receives written notice of agency decision called a Notice of Action (NOA) o Details the reason for the denial o Provides information about rights to appeal and appropriate timelines o Provides ombudsman contact information 23
24 APPEALS, GRIEVANCES AND FAIR HEARINGS Ombudsman program must rapidly respond to requests for help o Timelines for filing are tight o Closely mirror Medicare/Medicaid rules Family Care has 2 options for appeal o Internal MCO Appeal by committee formed by MCO o State Fair Hearing 24
25 APPEALS, GRIEVANCES AND FAIR HEARINGS Appeal rights under IRIS have been in flux and are currently under redevelopment o State Fair Hearing is available o Requests for reconsideration can be made Nonbinding DHS Review available under both Family Care and IRIS o Provides consultative support only and makes recommendations o Cannot compel MCO/IRIS to take certain actions, but can communicate contractual violations to DHS 25
26 APPEALS, GRIEVANCES AND FAIR HEARINGS Continuing benefits during appeal o Short, strict timeline to make request o Member could be held liable for cost of services provided during the appeal process IF the member loses the appeal 26
27 APPEALS PROCESSES FOR OTHER ISSUES Decisions made by Income Maintenance agencies o Financial eligibility o Cost share amounts Finding of noneligibility or loss of functional eligibility (loss of nursing home level of care ) o If it is an ADRC initial screen or an MCO or IRIS annual rescreen, increased denial of re-evaluating screen unless significant change in condition, sometimes with physician verification. No acknowledgement that there could be a screen error 27
28 WORKING WITH MCO S & IRIS Member Rights Specialists (MCO) or Participant Services Specialists (IRIS) o Assist members with problem-solving, attempt to resolve concerns and conflicts, suggest alternatives to member requests if not part of benefit package o Can assist with appeal process to the extent of filing notices, obtaining records o Is NOT the member s advocate o Does not assist with gathering evidence to support a member s case o Does not represent or speak on behalf of member 28
29 WORKING WITH MCO S: DHS LIAISONS Member Care Quality Specialist (MCQS) o Is liaison between advocates and MCO s for issues related to member quality, rights challenges, concerns about MCO staff attitudes or messaging o Is DHS staff, assigned to a specific MCO Contract Specialist o Is liaison between advocates and MCO s for issues related to contract and/or procedural concerns, such as whether the proper authorization model was followed in responding to members requests o Is DHS staff, assigned to a specific MCO 29
30 OMBUDSMAN QUALIFICATIONS & TRAINING What Attributes We Look for Experience with adult LTC systems, especially with MCOs, IRIS, MA programs Understanding of issues faced by program members and their families different issues and experiences for all 3 populations Able to use sound judgment and a professional approach 30
31 OMBUDSMAN QUALIFICATIONS & TRAINING What Attributes We Look for Confident but not overpowering personality; collaborative; personable Value of social justice and human rights; nonjudgmental Highly organized and able to keep things moving; detail-oriented Able to re-prioritize work as clients needs change 31
32 OMBUDSMAN QUALIFICATIONS, TRAINING & SUPERVISION Staff Development Thorough orientation o Overview and history of MLTSS programs o Expectations in ombudsman role o Relevant statutes, regulations, contracts; tools used by MCOs or IRIS to make authorization decisions o Introductions to the players o Job shadow and mentoring 32
33 OMBUDSMAN QUALIFICATIONS, TRAINING & SUPERVISION Staff Development Ongoing development o Updates on changes in policy or structure o Continued/updated training on all aspects of the job o Training about target group issues and diversity Management of Cases o Communication with clients must be regular o Case notes must be regular and detailed o Need easy access to supervisors for advisement 33
34 MOST COMMON COMPLAINTS Residential Issues o Discharge due to rate dispute between MCO and provider o Slow or no progress of MCO to relocate someone to community setting o Inadequate planning or sudden action when a move is needed; insufficient community supports Decreases/Denials in Services/Supports o Supportive Home Care and Personal Care o Denials of durable medical equipment 34
35 MOST COMMON COMPLAINTS Choice of Provider o Usually seen with employment, day services, residential setting Paternalistic Attitude o Not listening or valuing what member is saying o Taking questioning or challenging by the member personally, rather than professionally Scope of Services Issues o Provider (usually residential) has additional expectations (transportation, activities, meals) in contract with MCO and isn t providing them 35
36 SOME ISSUES EXPERIENCED WITH MLTSS IN WISCONSIN Locally developed MCOs had learning curve Struggles between appropriate levels of service and cost savings continue Driving down of costs takes approximately 5 years from start date of expansion of Family Care into new counties; this period of time requires lots of outreach MLTSS is entitlement; therefore, no wait lists but also causes increase in enrollment from those not on the wait list cost pressures 36
37 SOME ISSUES EXPERIENCED WITH MLTSS IN WISCONSIN Ombudsman programs must watch for situations where cost savings are harmful to individuals or groups of individuals Sustainability measures are being implemented by DHS to provide further cost savings, aimed at increased community and natural supports Relationships with MLTSS contractors can be prickly; important to find a balance between challenging decisions or processes and working together to solve issues 37
38 Questions? Kim Marheine Ombudsman Services Supervisor State of Wisconsin Board on Aging and Long Term Care Lea Kitz Program Manager Family Care & IRIS Ombudsman Program Disability Rights Wisconsin

39 National HCBS Conference September 9, 2013 LEVEL OF CARE EVALUATION IN MLTSS PAUL SAUCIER, TRUVEN HEALTH 2012 Truven Health Analytics Inc.
40 LEVEL OF CARE EVALUATION Criteria and methods for determining need for institutional level of care Required to qualify for Medicaid NF or waiver services At least annual reevaluation or whenever needs change Medical, functional, social Criteria, tools and degree of evaluator discretion vary across states Typical evaluator agencies in FFS: County human services department Area Agency on Aging or Center for Independent Living State Medicaid agency staff Private contractor Sometimes accompanied by options counseling 2012 Truven Health Analytics Inc. 2
41 OPTIONS COUNSELING Support for the individual and family/friends to make informed decisions about LTSS that reflect the individual s values, preferences and needs Typically includes discussion of: Available services to meet individual needs Financing options, including private pay, Medicare, Medicaid 2012 Truven Health Analytics Inc. 3
42 LEVEL OF CARE IN MLTSS How is Level of Care conducted in MLTSS? Does the role of traditional agencies change? Implications 2012 Truven Health Analytics Inc. 4
43 MINNESOTA Function Before MSHO Now Initial LOC for persons new to Medicaid Initial LOC for persons with Medicaid County County County Existing MCO submits to State Re-evaluation County Existing MCO submits to State Options Counseling County for Medicaid options Senior LinkAge Line (MN Board of Aging) for public and private options; or MCO for existing members 2012 Truven Health Analytics Inc. 5
44 TENNESSEE Function Before CHOICES Now Initial LOC for persons new to Medicaid Initial LOC for persons with Medicaid Re-evaluation Options Counseling Area Agency on Aging and Disability (AAAD) for HCBS, or facility for NF AAAD for HCBS, or facility for NF AAAD for HCBS, facility for NF AAAD for HCBS Area Agency on Aging and Disability (AAAD) for HCBS and NF, or facility for NF Existing MCO submits to State for HCBS and NF Existing MCO submits to State AAAD for HCBS and NF; or MCO for existing members 2012 Truven Health Analytics Inc. 6
45 WISCONSIN Function Before Family Care Now Initial LOC for persons new to Medicaid Initial LOC for persons with Medicaid County County ADRC (most run by counties) ADRC Re-evaluation County Existing MCO submits to State Options Counseling County for Medicaid options ADRC for public and private options; or existing MCO for options within plan 2012 Truven Health Analytics Inc. 7
46 IMPLICATIONS FOR TRADITIONAL AGENCIES Challenges Role likely to change, at least incrementally Loss of re-evaluation function Broader scope of counseling (if applicable) requires new knowledge and culture change Opportunities More people being evaluated Ability to evaluate for both HCBS and NF Expanded scope of counseling in some cases 2012 Truven 2012 Health Truven Analytics Health Analytics June 2012 Inc. 8

47 IMPLICATIONS FOR POLICY MAKERS Capacity of traditional agencies to expand or modify role Access to timely evaluations Reliability of evaluations Aligning stakeholder interests toward HCBS expansion Mitigating conflict and maximizing confluence of interest 2012 Truven Health Analytics Inc. 9
48

49 This image cannot currently be displayed. Kansas Association of Area Agencies on k4ad Aging & Disabilities National HCBS Pre-Conference Intensive September 9, 2013 AAAs and Aging and Disability Resource Centers (ADRCs) Janis DeBoer, k4ad Executive Director and ADRC Administrator
50 History: Area Agencies on Aging (AAAs) Eleven AAAs operate across the State of Kansas. The Older Americans Act (OAA) was signed into law by President Lyndon B. Johnson in k4ad

51 History: AAAs and the Older Americans Act Sixty Plus? Call us For information, referral, assistance, meals, in-home services, legal assistance and more 3 k4ad
52 History: AAAs and Community Based Services In 1994, the AAAs contracted with the State agency to provide information and assessments to Kansans regarding community based services through the NF CARE program. PASRR screens were/are also a component of the CARE program. State General Funds were also available to provide case management and coordinate community based services. 4 k4ad
53 History: AAAs and Case Management In 1997, the AAAs became the single point of entry for services to seniors in Kansas, statewide. Funding sources included State General Funds, Older Americans Act and Medicaid. All 11 AAAs contracted with the State of Kansas to become direct service providers of Targeted Case Managers for Medicaid home and community based services (Frail Elderly 1915(c) waiver). The AAAs focus on community based services was measurably strengthened. 5 k4ad

54 History: AAAs and Older Americans Act C a r e g i v e r s 6 k4ad
 Sponsoring Organizations, to assist seniors and their caregivers with enrollment in Medicare prescription drug plans.")
55 History: AAAs and SHIP (CMS-State Health Insurance & Assistance Program) With the implementation of Medicare Part D, the AAAs significantly increased their role, as SHICK (Kansas SHIP) Sponsoring Organizations, to assist seniors and their caregivers with enrollment in Medicare prescription drug plans. 7 k4ad
56 Current: Medicaid Managed Care in Kansas All of the above community based activities occurred prior to Medicaid Managed Care. KanCare in Kansas became effective January 1, Three Medicaid Managed Care Organizations (MCOs) operate in Kansas. PACE is a fourth option. The CARE/PASRR contracts with the AAAs terminated, as of December 31, The Medicaid TCM contracts with the AAAs terminated, as of December 31, k4ad
57 Current: AAAs and ADRCs A lot happened in 2012 On February 27, 2012, a procurement process began to secure a contract for a single ADRC in Kansas. On September 10, 2012, the State of Kansas awarded a single ADRC contract to the Southwest Kansas Area Agency on Aging (SWKAAA). SWKAAA subcontracted with the other 10 AAAs to provide a statewide ADRC. Kansas ADRC includes a call center and 11 walk-in centers, effective November 1, k4ad

58 Current: ADRC Call Center and 11 Walk-In Centers ADRC (2372) 10
59 Current: ADRCs Collectively Cover all 105 Counties ADRCs are a process more than an entity, according to two federal agencies (CMS and ACL). ADRCs provide unbiased, reliable information and counseling to individuals of all ages with all levels of income. ADRCs are a visible and trusted place where people can turn for information, assistance and a single point of entry to public and private long-term supports and services. 11 k4ad
60 Current: AAAs and ADRCs The AAAs/ADRCs customer base grew from: 524,851 Kansans age 60+ To 2,206,600 Kansans age k4ad
61 Current: What is a fully functioning ADRC? A fully functioning ADRC includes six criteria: 1. Information, referral and assistance 2. Options counseling and assistance 3. Streamlined eligibility determination for public programs 4. Person centered transition support 5. Consumer populations, partnerships, and stakeholder involvement 6. Quality assurance and continuous improvement 13 k4ad
62 Current: Kansas ADRC Three Deliverables Services 1. Information, Referral and Assistance 70,857 contacts (estimate 8 months) Population Intended to serve the general population all ages, all income levels (not limited to Medicaid) 2. Options Counseling 8,658 (actual 8 months) 3. Functional Assessments for KanCare/PACE 12,314 assessments (actual 6 months) Intended to serve the general population All ages, All income levels (not limited to Medicaid) Serves the Frail Elderly, Physically Disabled, Traumatic Brain Injury waivers, PACE, NF admissions, MFP (Six Assessment Types) 14
63 Current: KANSAS Function Before KanCare Now Initial LOC for persons new to Medicaid Area Agencies on Aging for CARE/PASRR (in addition to hospitals). For Medicaid waivers, AAAs, Centers for Independent Living, Private CM Orgs. State Staff for PACE. ADRC for Frail Elderly, Physically Disabled and TBI waivers, NF Admissions, PACE, MFP. LOC for persons with Medicaid Same as above Same as above Options Counseling New service since KanCare New service since KanCare 15
64 Current: Level of Care Functional Assessments The ADRCs conduct functional assessments for multiple programs, including Medicaid and PACE. Approximately, 30,000 assessments are projected annually. The extensive experience of the AAAs as assessors and case managers for the past nineteen years greatly enhanced the successful implementation of the ADRC and particularly the functional assessment deliverable. 16 k4ad
65 Current: Options Counseling Forward-thinking service for Medicaid and private pay individuals Critical to Medicaid Managed Care States 17 k4ad
66 Current: Opportunities and Challenges There have been many. 18 k4ad
67 Source/Contact information Data/information source: Aging and Disability Resource Center Successes, October 2010, ADRC Technical Assistance Exchange, U.S. Census Bureau report QT-P1 Age Groups and Sex: 2010 KDADS ADRC website: Janis DeBoer, k4ad, Executive Director and ADRC Administrator, 2910 SW Topeka Blvd., Topeka, KS 66611, k4ad


68 Minnesota Ombudsman for State Managed Health Care Programs National Home & Community Based Services Conference, Pre-Conference Intensives September 9, 2013
69 History with Managed Care 1965 Medicaid program was established 1966 Minnesota joined the Medicaid program with the establishment of Medical Assistance 1985 Minnesota - one of first states to receive a waiver and implement a mandatory managed care program for the Medicaid population Managed Care Ombudsman office established From the beginning certain eligible seniors and disabled were enrolled in managed care.
70 History continued 1995 Waiver approved requiring most Medicaid recipients to receive services through managed care 1997 Minnesota Senior Health Options (MSHO) established through waiver 2000 Waiver for county-based purchasing 2001 Waiver approved to extend MSHO provisions to persons with physical disabilities
71 MCO Contracts There are three MCO contracts: Families and Children Special Needs Basic Care (SNBC) Minnesota Senior Health Options (MSHO) and Minnesota Senior Care Plus (MSC+)
72 Managed Care Enrollment ,439 Total 613,524 Total 12,018 MSC+ 36,349 MSHO 10,205 SNBC 13,067 MSC+ 35,474 MSHO 35,199 SNBC
73 Seniors and Disabled in MCOs 90% of seniors (49,000) in managed long-term care plans 43% of people with disabilities (39,500) enrolled in MCOs
74 Land of 10,000 Ombudsman Long-Term Care ombudsman is a program of the Minnesota Board on Aging housed within DHS. Regional ombudsmen and volunteers work to enhance quality of life and services. Ombudsman for Mental Health and Developmental Disabilities is a separate state office. Assists with complaints, medical review and civil commitment
75 Statutory Authority Ombudsperson shall advocate for recipients enrolled in prepaid health plans through complaint and appeal procedures and ensure that necessary medical services are provided either by the prepaid health plan directly or by referral to appropriate social services. (MN Statutes 256B.69, subd. 20).
76 Staff Five full-time state staff Managed care county advocates in 87 counties and one tribe 14,445 calls to the state in calls for seniors 471 calls for persons with disabilities
77 Broad Overview Investigates complaints Assists enrollees in resolving access, billing and service-related problems Provides information and education regarding Enrollee Rights, the MCO Grievance & Appeal process, the State Fair Hearing process Monitors MCO Grievances and Appeals Tracks and monitors managed care State fair hearings Makes recommendations for MCO audits and DHS/MCO contracts Partners with and provides ongoing education and training for managed care county advocates
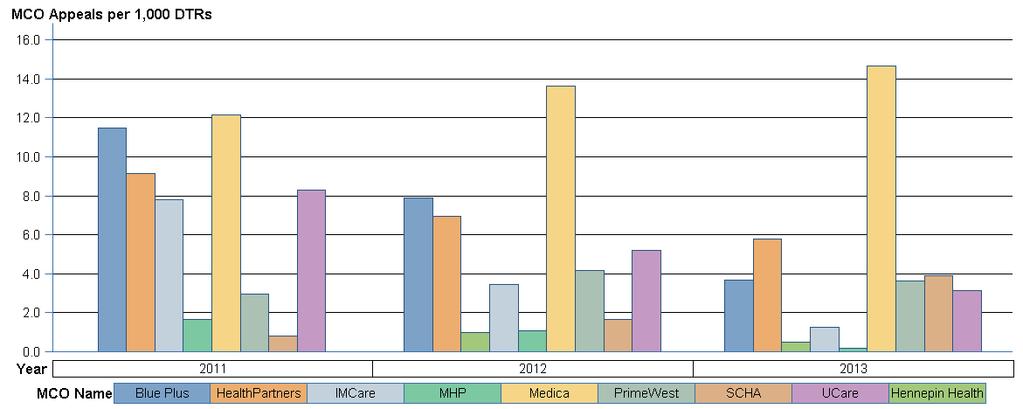
78 Oversight Gathers data to identify and monitor trends DTRs (Denial/Termination/Reduction Notices) Appeals and Grievances State Fair Hearings Spot problems and bring to the Department of Health or to contract management
79

80 Appeals by Service Category For One MCO
81 Oversight Convene MCO appeals and grievances committee Authority over reason and service codes Consulted regarding MCO: Policy & Procedures Notices Member Rights Evidence of Coverage Identify and investigate problem providers
82 Training Quarterly training meetings with County Managed Care Advocates Present at state-wide county conferences On-site visits to MCOs Community outreach to providers and nonprofits
83 Ombudsman in state agency Quicker resolution through access to state data bases Access to enrollment reps and contract managers Input into model contracts At the table with policy experts
84 Ombudsman for State Managed Health Care Programs PO Box St. Paul, MN Margaret Manderfeld (651)
85
86
87
88
89
90
91
92
93
94
95
96
97





98 Managed Long-Term Services & Supports Ombudsman / Patient Advocate Workshop #2 HCBS Pre-Conference Intensives Medicaid Managed Long-Term Care Hawaiʻi September 9, 2013 Leolinda Parlin, Project Director


99 Introductions Leolinda Parlin Project Director, Hilopa a Family To Family Health Information Center Co-Director, Hawaiʻi MCH LEND Program State Coordinator, Family Voices of Hawai i Neutral 3rd Party Secret Agent Mom
100 Outline Provide Historical Convergence of Hawaiʻi Medicaid and the Hilopaʻa F2FHIC Present Overview of the Ombudsman Operation Share Lessons Learned
101 QUEST Q U E S T Quality Care Universal Access Efficient Utilization Stabilizing Costs Transforming the Way Health Care is Provided to QUEST Members
102 Hawaiʻi Medicaid Programs QExA MMC Primary & Acute Limited Chore Cognitive Rehab Long Term Care 65 or over, persons with disabilities QUEST MMC Primary & Acute Everyone else Carve Outs Tranplant SMI Early Intervention IDEA Part C School Based Services DD/MR Waiver Dental Administered by the Med-QUEST Division of Dept. Of Human Services
103 Hawaiʻi Population 2,137 Total Medicaid: 292,581 Total QExA: 16% HCBS: 10% NF: 5% 30, ,806 Population 2010 Census 2013 Medicaid Population % of Population 2013 QExA Population % of Medicaid State of Hawaiʻi 1,360, ,581 22% 45,997 16% Oʻahu 953, ,263 19% 30,342 17% Hawaiʻi 185,079 62,260 34% 6,297 10% Maui 144,444 30,066 21% 3,806 13% Lānaʻi 3, % 73 10% Molokaʻi 7,345 3,305 45% % Kauaʻi County 67,091 16,067 24% 2,137 13% 73 6, Census Data Book Tables; DBEDT QExA Dashboard Report Health Plan Comparison SFY 2013 Monthly Trend Analysis 8/27/2013
104 Little Background on Hilopaʻa F2FHIC Family Opportunity Act 2005, Reauthorized with ACA Established the Family to Family Health Information Centers Ultimate Goal: Families of children with special health care needs (CYSHCN) will partner in decision-making at all levels. Title V MCHB Hilopaʻa to braid firmly sits in the Hawaiʻi Pediatric Association Research & Education Foundation
105 What HRSA & Congress Want Assist families of CSHCN make informed choices about health care Provide information regarding health care needs and resources Identify successful health delivery models Develop with a model for collaboration between families of CSHCN and health professionals Provide training and guidance regarding the care of CSHCN Conduct outreach activities Be staffed by such families who have expertise

106 Our Focus I&R Training Technical Assistance
107 Hilopa a Family to Family Health Information System Telecommunication Schema Hub of virtual phone numbers all call into main phone line (808) Main Phone Line (808) Staff login to get calls Kau i Noe Susan
108 Personal History with Medicaid
109 F2F & DDC Urges Community Advisory for QExA F2F & MCH LEND Convene Focus Groups to Guide QExA Organizational History with Med-QUEST F2F Leads Workgroup and Development of EPSDT Well Child Reporting Forms F2F Conducts Statewide Provider Training on EPDST F2F Supports Training Outreach and Enrollment Counselors and Community Partners F2F Only Qualified and Interested Entity and Appointed to be Ombudsman for QExA (12/1/2009) F2F Contract Expanded to Include ALL Medicaid Programs (7/1/2012) & Reprocured and Awarded (10/1/2013)
110 Ombudsman Provide Information and Referral Phone Fax Text Provide Assistance in Navigating the System Explaining Coaching Representing Interceding Provide Feedback to State & Health Plans



111 Our Role in the Community Somebody
112 Inquiries Distribution of Inquiries Providers 3% Origin of Inquiries Neighbor Islands 29% Oʻahu 71% Beneficiaries 97%
113 Inquiries Continued 90% 80% 70% 60% 50% 68% Distribution by Type of Inquiry 79% 80% 79% 65% 40% 30% 20% 10% 0% 33% 17% 10% 11% 12% 12% 8% 7% Mar-09 Mar-10 Mar-11 Mar-12 Mar-13 General Information, Referral & Navigation 68% 79% 80% 79% 65% Issue Identification 17% 10% 8% 7% 11% Complaints 33% 11% 12% 12% 24% 24% 11%





114 Value Added Personal Experience Training Across Plans & Programs Community Broker & Emissary Focus Groups On-Site Review Team Member Family Voice on DD/MR Utilization Review Committee Rainbow Book Support Beyond Medicaid Connector into Medicaid Sounding Board for the Health Plans

115 What is Right About Hawaiiʻs Program Patti Bazin, Health Care Services Branch Administrator Extremely Accessible State Leadership Equal Partner with the Health Plans Extention of the State Health Plan Monthly Meetings On-site Reviews CAN DO Attitude not a CANNOT Breadth of Total Operation Enhances Ombudsman Services Consumers as Guides Credibility with Providers

116 Moving Forward Continue to guide the community to work with the Health Plans ( that fishing thing) Continue the positive relationship between the Ombudsman and Health Plan leadership Pilot direct referrals to QUEST plans of CSHCN separated from EI/Part C Ramp up for QUEST Integration and implementation of ACA

117 Leolinda Parlin (808)
118 Rosanne J DiStefano, Executive Director Elder Services of the Merrimack Valley, Inc. Sept 9, 2013 Washington, DC
119 AAA (Area Agency on Aging) Private, non-profit 501(c)3 organization serving 23 cities and towns in Northeastern Massachusetts ASAP designated by Massachusetts as Aging Services Access Point Core Functions; over 100 RN s and Social Work staff provide care coordination, care management, screening and assessment for community based care and SNF (skilled nursing facility) approval Manage a network of over 75 vendor contracts for over 120 different community based services Over 30% of staff are bilingual/bicultural


120 In 7 years since the inception of contracts with managed care entities: Agency budget doubled Agency staff doubled Nearly 600% increase in revenue from grants & contracts Federal 11% Client Fees 3% Foundations 0.33% Contributions 2% Grants & Contracts 4.12% Federal, 9.81% Grants & Contracts 23.54% Client Fees 2.05% Contribution s0.85% Foundations 0.28% State 79.90% Revenue FY 2006 $23,777,117 State 63.47% Revenue FY 2013 $47,296,722
121 Transitional Coaching in 6 hospitals (over 12,000 referrals since inception 14 months ago) Transitional Coaching Pilots with 2 managed care providers, one has started, one in negotiations Care Management contract with ACO for large physician group Bridging Care Management & Transitional Coaching for ACO a new model Contracts in place for younger disabled dual eligible population with a managed care provider
122 Self managed teams =empowered staff Empowered clients = activated patients Interdisciplinary service models = products Strategic partnerships and relationships Defined assets = nontraditional role Evidence based approaches = open doors to health care Learning environment = What s a covered life?
123 Interdisciplinary perspective Flexibility Vision Board support Getting past No Innovation and excitement
124 Prevention & chronic disease management Patient activation and education Reduced unnecessary utilization of health care Improved access to care Reduced incidence of avoidable hospitalizations Improved overall patient experience and satisfaction

125 Replicated from Create Supportive Environment Public Health Policy Strengthen Community Action COMMUNITY Self-Management Develop Personal Skills Health Systems Delivery System Design / Re-orient Health Services Information Systems Decision Support Activated Community Informed Activated Patient Prepared Proactive Practice Team Prepared Community Partners Population Health Outcomes/Functional Outcomes
126 Challenges Risks and incentives Goal Alignment ROI Data Analysis Outcomes
127 Massachusetts Health Policy Forum Healthy Aging Communities and Programs Committees Elder Services of the Merrimack Valley Aging Service Network Providers COMMUNITY Care Transitions Healthy Living Center of Excellence Regional Disease Management Coalitions Executive Office of Elder Affairs, Dept of Public Health Medical Care Coordination Hebrew Senior Life Health Systems Health Plans, SCOs, ACOs, PCMH Hospitals, FQHCs, PCP VA, VNA, Home Health Care Activated Community Informed Activated Patient Prepared Proactive Practice Team Prepared Community Partners Population Health Outcomes/Functional Outcomes
128 Define products Know ROI Repackage if necessary Translate labor hours into costs Align goals Create infrastructure Collect and use data
129 and Negotiating Reimbursement Understand Scope of Service desired by Managed Care Organization Negotiate to Broaden (or limit) the Scope of Service based on what you bring Benefits of your enhanced role measureable if possible, suggest targets, use ROI Cost out unit of service estimate time, labor costs, administrative overhead, and investment growth
130 Use as broad a base as possible to arrive at a per enrollee per month (PMPM) rate; not a typical fee for service or unit of service Managed care organizations may have levels of risk be prepared to see different rates and use different products Eventually seek to blend your rates Be open to sharing risk or being paid more for meeting or exceeding standards
131 Agree to evaluate success and reimbursements at a specific date sooner if this is new for one or both parties. Your costs will increase base your rate at labor rates and costs anticipated in the next few years. You may be able to negotiate a start up reimbursement separate from PMPM basis.


132 Timing you and the managed care organization Are financial incentives aligned? Multiple initiatives Outcome and proof of value- getting data No cost pilot with time frame Contract negotiations take time ACO s and corporate buy-in
133

134

135
136 Rosanne J DiStefano, Executive Director Elder Services of the Merrimack Valley, Inc Rdistefano@esmv.org
137 DEVELOPING PRICING STRUCTURES 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
138 OBJECTIVES Participants will have a basic understanding of the various pricing strategies. Participants will understand why price models are important in today s environment Program and fiscal staff will share a common language that translates the work of the organization into the cost of doing business to facilitate managing to outcomes. Participants will understand the basic definitions used in price models Participants will understand how to translate their work into the elements of a price model Participants will understand how price models are used in day to day business operations management 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
139 AGENDA Establishing a Pricing Strategy Rationale for building cost model and developing unit cost pricing How to build the basic model for each type of service Considerations as model is operationalized Example - Carl s Grocery Store Conclude with benefits of developing a pricing model 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
 Copying, reproduction or distribution of these materials without the express written")
140 PRICING STRATEGIES 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
141 WHAT IS A PRICING STRATEGY? Pricing strategy refers to the way in which a company improves or maximizes profits. Strategies typically fall into these catagories: Cut cost Sell more, Find more profit with a better pricing strategy Pricing is a key component of a solid marketing plan Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited



142 ESTABLISHING YOUR PLACE IN THE MARKET Pricing is a key component of a solid marketing plan. Pricing communicates the product/service brand to the customer. Pricing targets your market 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
143 EXAMPLES OF PRICING STRATEGIES Skimming selling a product at a high price, sacrificing high sales to gain a high profit. Often used to recover R&D Loss leader selling a product at a low price (cost) to stimulate other profitable sales. Market-oriented pricing setting a price base on analysis and research compiled from the target market. Penetration pricing low price high market share. Price discrimination different prices for different market segments. Premium pricing Keeping a price high to encourage favorable perceptions among buyers. And, there are many more Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
144 10 QUESTIONS TO ASK What will the customer pay? What kind of customer do I want? How should I react to my competitors pricing? Can I offer different levels of products at different price points? How can I adjust my prices? Have I given the customer a reason to pay more for my product? 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
145 10 QUESTIONS Pricing is a Marketing Function Can I base my price partly on intangible benefits? Should I bundle my products for a single price? Should I discount to get people to buy my product? How does the customer want to buy my product/service 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
146 WHY MODEL? 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

147 WHY MODEL? Our funding streams are changing! Past: We were reimbursed for our costs by Federal, State, and local funders Present: We will be reimbursed per units of service delivered. Future: We will sell our services on a per unit basis to MCOs with a promise to achieve certain outcomes. Using models can answer the what if questions we have to answer when we determine what it will take to achieve promised outcomes for a given price. For example, What if I staff a program with an LSW instead of an RN? What if I increase case load sizes? Create consistency across the AAA Network through the use of standard pricing methodology (note that we are aiming for a standard of practice, not the same prices) Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

148 WHY MODEL? In short, we model to prepare for the future and know: we are able to offer the highest quality services at a competitive price to maintain our market share and profit margin Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
149 BASIC DEFINITIONS IN MODELING 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

150 BASIC DEFINITIONS Cost refers to the amount paid to produce a good or service. The cost represents the sum of the value of the inputs in production - land, labor, capital and enterprise. Price refers to the amount of money that consumers have to give up to acquire a good or service Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited


151 BASIC DEFINITIONS Contingency Used to cover uncertainty. The more conservative (or certain) the model, the less contingency required. May be added into the cost of an item or included as a separate line item. Margin A ratio of profitability calculated as net income divided by revenues, or net profits divided by sales. It measures how much out of every dollar of sales a company actually keeps in earnings. Remember, it s okay. Non profits can earn a profit Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
152 BASIC DEFINITIONS Assumptions Guesses and estimates based on experience and research about how we conduct our business. Assumptions come from how we define our work and are used in what if scenarios. Examples from our work: Caseloads will be 65 to 1. We will hire 1 PSS to support 15 Care managers. We will hire only RNs. We will remain in the same facility. The volume of clients will increase by 5% annually Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

153 FIXED VS. VARIABLE COSTS Fixed Cost do not change as volumes increase. Example from our work: Rent Variable Costs Rise and fall as volume increases or decreases. Example from our work: The number of care managers we hire Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
154 DIRECT VS. INDIRECT COSTS Direct Cost Easily traced to providing the service Example from our work: Variable: Care Manager Salaries Fixed: Care Management Software System Indirect Cost Not easily traced to providing the service. Example from our work: Variable: Cost of providing IT support. Fixed: Rent 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
 Copying, reproduction or distribution of these materials without the express written")
155 BASIC MODEL CONSTRUCTION 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
156 BASIC MODEL CONSTRUCTION A model that is flexible that allows changes assumptions and see what happens. A model that will help develop a menu of services that includes: Standardized definitions for services Cost/price per unit of service Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
157 STEP 1: DEFINE THE SERVICE What services are required to achieve an outcome? What functions required to perform the service? How much time is required to perform the function? What level of staff is required to perform the function at the level required to achieve the outcome? What other resources are required to perform the function to achieve the desired outcome? What will MCOs want that might add cost to providing the service? What is the value added to the MCOs (why will MCOs want it? How will it positively impact their bottom line)? 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
158 Sample Menu of Services The following is for demonstration only and is intended to visualize how the definitions and rates will be used in the marketing of AAA services. Units of service and definitions are made up for the purposes of demonstration. Provider Management Standard Provider Management Package $ ##.## per provider per month The standard package includes: Pre-Certification Review, Compliance Review, Provider Relations Management, Technical Assistance, and Basic Contracting. Premium Provider Management Package $ ##.## per provider per month Includes the standard package plus: Provider Quality Reporting and Selective Contracting. Custom Provider Management Package Rate dependent upon customer requirements Provider management services will be defined by the customer Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

159 STEP 2: DEFINE THE ASSUMPTIONS Fringe Benefit rate of 28% Other direct cost rate of 24% Indirect cost rate of 15% Purchase software at total cost of $500,000. Cost to be recovered in 3 years Lease hold improvement to space $50,000. To be recovered in 8 years. Inflation rate used: 2.8% based on Bureau of Labor Statistics. 5% contingency added to cover risks (e.g., inaccuracy in volume estimates, problems with contractors, etc.) 10% margin Caseload: 75 clients to 1 care manager 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
160 STEP 3: BUILD THE MODEL 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited Positions Salary Ratio Manager $ 75,000 1 Program Assistant $ 35,000 1 Clinical Supervisor $ 40, CMs to 1 Supervisor 1 $ 40, CMs to 1 Care Manager $ 32, clients to 1 Care Manager - Intensive $ 34, clients to 1 Care Manager - RN 1 $ 36, clients to 1 Program Support $ 29, CMs to 1 Turnover Rate Fringe Benefit / Payroll Taxes Rate 28.0% Percentage Other Direct Cost Rate 24.0% Percentage Indirect Cost Rate 15.5% Percentage Contingency Rate 5.0% Percentage Desired Margin 10.0% Percentage Inflation Factor 2.8% Percentage Capital Investment Cost Recovery Period (years) Annual Amount Software 500, ,667 Equipment 100, ,333 Lease Hold Improvements 50, ,250 Total Investment $ 650,000 $ 206,250 For example, look at care management. The salary and caseload may differ by position and type of care manager.
161 STEP 3: BUILD THE MODEL Volume drive your variable costs. It is critical to understand how volume of service impacts your price. Case load Case Load Beginning CeEnrollment rdisenrollment RClient Months Avg Census Community BaseNF Based ratios- Comm. Ratios NF/AL CM FTEs PASSPORT % 2.60% 50,883 4, Assisted Living 395 4% 3% 5, Choices 250 2% 1.50% 3, This model starts with the beginning census (assumption) and projects growth based on enrollment and disenrollment rates (more assumptions). Then, using case load sizes (another assumption), the model determines the number of Care Managers required to serve the population. This model also shows the number of managers and support staff required. Example: If the average census is 4240, then approximately 56 care managers are required.
162 STEP 3: BUILD THE MODEL Example: changing the enrollment rate to 6% increases the number of Care Manager FTEs from 56 to just over 68. Case load Case Load Beginning CeEnrollment rdisenrollment RClient Months Avg Census Community BaseNF Based ratios- Comm. Ratios NF/AL CM FTEs PASSPORT % 2.60% 61,976 5, Assisted Living 395 4% 3% 5, Choices 250 2% 1.50% 3, Example: Changing the caseload from 75 to 85 decreases the number of Care Manager FTEs from 56 to just over 49. Case load Case Load Beginning CeEnrollment rdisenrollment RClient Months Avg Census Community BaseNF Based ratios- Comm. Ratios NF/AL CM FTEs PASSPORT % 2.60% 50,883 4, Assisted Living 395 4% 3% 5, Choices 250 2% 1.50% 3, Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
163 STEP 3: BUILD THE MODEL The final model incorporates all of the assumptions. All of the costs are included: Staff directly involved in providing the service. Other costs such as mileage, supplies, printing, fringe benefits, and so forth. Indirect costs such as rent, overhead, major capital investments. All of the costs are added and divided by the volume of services to get a per unit of service price Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
164 Care Management Total Congratulations! We have a unit price! % Referred for Service 100.0% 100.0% Volume 4,000 4,000 4,000 Labor Cost Position Salaries Number / Ratio FTEs Manager $ 75, ,000 75,000 Program Assistant $ 35, ,000 35,000 Clinical Supervisor $ 40, , ,333 Supervisor 1 $ 40, , ,333 Care Manager $ 32, ,706,667 1,706,667 Program Support $ 25, ,889 88,889 Total Labor 2,332,222 2,332,222 Fringe Benefits 28.0% 653,022 Total Labor Cost 2,985,244 Other Direct Cost 24.0% 716,459 Additional Direct Cost Return on Investment 206,250 Total Direct Cost 3,908,353 Indirect Cost 15.5% 605,795 Sub-total 4,514,148 Inflation Factor 2.8% 252,792 Sub-total 4,766,940 Contingency Rate 5.0% 238,347 Desired Margin 10.0% 476,694 Total Cost 5,481,981 Volume 4,000 Annual Unit Rate $ 1, Monthly Unit Rate 12 $ Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
165 USING MODELS EVERYDAY How can models be used to manage your business? What value do these models add? Does it change the way you think about how we provide services? 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

166 USING MODELS EVERYDAY See what happens when you change how we deliver services Decrease the case load size Increase growth rate Change the average salaries See what happens when you invest in something new Buy new software Remodel your office space So, let s try some! 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
167 Care Management Total What if. I want to buy new software at a cost of $150k for three years? My Return on Investment line will increase to $356,250 and my monthly rate will increase from $114 to over $118 % Referred for Service 100.0% 100.0% Volume 4,000 4,000 4,000 Labor Cost Position Salaries Number / Ratio FTEs Manager $ 75, ,000 75,000 Program Assistant $ 35, ,000 35,000 Clinical Supervisor $ 40, , ,333 Supervisor 1 $ 40, , ,333 Care Manager $ 32, ,706,667 1,706,667 Program Support $ 25, ,889 88,889 Total Labor 2,332,222 2,332,222 Fringe Benefits 28.0% 653,022 Total Labor Cost 2,985,244 Other Direct Cost 24.0% 716,459 Additional Direct Cost Return on Investment 356,250 Total Direct Cost 4,058,353 Indirect Cost 15.5% 629,045 Sub-total 4,687,398 Inflation Factor 2.8% 262,494 Sub-total 4,949,892 Contingency Rate 5.0% 247,495 Desired Margin 10.0% 494,989 Total Cost 5,692,376 Volume 4,000 Annual Unit Rate $ 1, Monthly Unit Rate 12 $ Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
168 Care Management Total What if I want to use RNs to deliver services. Their average salary will be $38,500. My monthly rate will increase from $118 to over $134 % Referred for Service 100.0% 100.0% Volume 4,000 4,000 4,000 Labor Cost Position Salaries Number / Ratio FTEs Manager $ 75, ,000 75,000 Program Assistant $ 35, ,000 35,000 Clinical Supervisor $ 40, , ,333 Supervisor 1 $ 40, , ,333 Care Manager $ 38, ,053,333 2,053,333 Program Support $ 25, ,889 88,889 Total Labor 2,678,889 2,678,889 Fringe Benefits 28.0% 750,089 Total Labor Cost 3,428,978 Other Direct Cost 24.0% 822,955 Additional Direct Cost Return on Investment 356,250 Total Direct Cost 4,608,582 Indirect Cost 15.5% 714,330 Sub-total 5,322,913 Inflation Factor 2.8% 298,083 Sub-total 5,620,996 Contingency Rate 5.0% 281,050 Desired Margin 10.0% 562,100 Total Cost 6,464,145 Volume 4,000 Annual Unit Rate $ 1, Monthly Unit Rate 12 $ Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
 Copying, reproduction or distribution of these materials without the express written")
169 ENOUGH WITH THE WORD PROBLEMS!!! 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
170 WHAT OTHER USES DO MODELS HAVE? Compare prices with competitors See impact of investments on the unit price of services Identify which investments or cuts will have the biggest impact Determine required staffing levels Grant evaluation and preparation Others???? 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
 $ 1,100.00 2.3 Professional Svcs-XYZ Partner $ 25,000.00 52.9 Rent $ 450.00 1.")
171 Care Transitions Program Carl's Grocery Store Model PLAY DATA for Training Purposes FIXED COSTS $ Cost Clients Program Admin Personnel Costs $ 17, Staff members listed here Suzie, Jack, Sam. Telephone & Cell Phones $ Depreciation (QMCO) $ 1, Professional Svcs-XYZ Partner $ 25, Rent $ TOTAL FIXED COSTS $ 44, VARIABLE COSTS Coaching Personnel Costs $ 32, Toni Arquette - Danielle Amrine - Beth Chopra - Vicky DePew - Kieran Fleming - victoria McClain - Cathy VanFossen - Kim W 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
172 SOMETIMES WE JUST NEED TO KNOW WILL IT WORK? 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
173 CULTURAL SHIFT 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
174 CULTURAL SHIFT Standardization across the network Changes the language and creates a bridge between clinical and fiscal teams Examples of success 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

175 EXAMPLES OF SUCCESS

176 QUESTIONS? Sharon Fusco, Director of Business Results and Innovation, Council on Aging of Southwestern Ohio, Cincinnati, OH STILL THE ANSWER Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
177 RETHINKING THE AAA ROLE IN THE MARKETPLACE 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
178 OBJECTIVES Learn to see around the curve? How to evolve in response to shifts in the competitive marketplace. Change the culture to respond to change. What lines of business make sense and who to partner with? 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
179 COUNCIL ON AGING: WHO ARE WE? 41 years of service to older adults, families and caregivers State-designated Area Agency on Aging since Counties in SW Ohio: Butler, Clermont, Clinton, Hamilton and Warren counties One of largest non-profits in our region 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
180 OUR MISSION & VISION Mission: Enhance the lives of adults by assisting them to remain independent at home through a range of quality services Vision: Every senior adult in our region shall have a choice and range of services that will assist them to remain independent in their chosen environment 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
181 COA S CORE FUNCTIONS Administrator Aging & Disability Resource Connections Pre-Admission Review Care Management and Care Coordination Transitional Care Area Agency on Aging 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
182 COA BY THE NUMBERS ,459 clients receiving in-home services Nearly 2 million home-delivered meals (to 10,011homebound older adults) 2.1 million hours of in-home care 280,047 trips to doctors, senior centers 29,322 requests for information about help for seniors 160 education and support sessions with caregivers 102 advocacy meetings with clients and elected officials From 2012 annual report 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
183 BIG PICTURE CHANGES: COA S STORY Moving from: To: 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

184 HOW DO I BEST DESCRIBE OUR CURRENT SITUATION? It feels like this but we aren t standing and waiting. We re more like this just a step ahead of a speeding bullet Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
 Copying, reproduction or distribution of these materials without the express written")
185 COA IN Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
 2013 Council on Aging of Southwestern Ohio, Inc.")
186 THE ENVIRONMENT: READING THE SIGNS In 2006 Managed Care Pilot proposed for PASSPORT in the Cincinnati Region Pressure to reduce Medicaid spending Competition for scarce resources In 2011 Significant budget reductions proposed state and federal State Integrated Care Delivery System is proposed and approved (Duals Demonstration) 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
187 WHY CHANGE?? Bottom line: We could see our funding streams changing and more competitors entering the market. Past: We were reimbursed for our costs from Federal, State and Local entities. Present: Fee for service is here (or almost here) Care Transitions Medicaid waiver services will be provided through a managed care company (MCO). Future: We will sell our services on a per unit basis to MCOs and other payers with a promise to achieve certain outcomes Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

188 WHY CHANGE? In short, we had to prepare for the future and know: we are able to offer the highest quality services at a competitive price to maintain our market share and profit margin Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

189 WAIT A MINUTE Did you say profit margin? Yes. But we are non-profits, isn t that illegal? No. I am still not sure this is right. Non-profits that earn revenue put their revenue back into programs and services to provide Better Service to More Clients. Disclaimer to make the CFO s happy: There is a bit more to it and there are a few rules, but as long as they are followed, it s okay for a nonprofit to bring in more than it costs them to provide services Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

190 BUT WAIT, THERE S MORE We are nonprofits why should we be concerned about being competitive and having a market share? Because: Aging is a hot market high demand + low supply = profit potential Others believe they can do it better. Others can do it at a lower cost. Others can do it and make money at it Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited AND
191 OUR BIGGEST QUESTION: In 2006, Can we compete? We had the history of being a monopoly with state and local funding We get the money without having to compete for it Must rid ourselves of the entitlement mindset In 2011, our questions changed to: Can we compete for business with Managed Care Companies? What are the right products? How should we be positioning our organization for future relevance? 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

192 TO WIN THIS GAME, WE MUST BE ONE STEP AHEAD OF THE MARKET Some people skate to where the puck is. I skate to where the puck is going to be. ~Wayne Gretzky 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

193 WHAT PRODUCTS? AND WHO WILL PURCHASE THEM? We analyzed our current product mix to determine where to invest our time and energy: What products will define our future and are in demand? What products are holding us back? 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
194 WHAT PRODUCTS? AND WHO WILL PURCHASE THEM? We considered several factors: 1. Who will pay for it? Who receives it? 2. Ability to generate revenue (unrestricted funds) 3. Current competitive advantage, strengths, or gaps. We developed short and long term strategies based on our analysis. Question Marks ADRC Provider Management Dogs AAAs Pre-Admission Review Stars Care Transitions Care Coordination Cash Cows Levy Funded Programs Care Management We brought in help external experts who could help us see where the market was going Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited


 Copying,")


195 PLAYING TO WIN MEANS WE CAN CONTINUE TO SERVE OUR CLIENTS! 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
196 BIG PICTURE CHANGES Culture Relationships Strong Market Position Systems People Structure 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

197 STRATEGIES EMPLOYED Structure our organization to compete Build a strong organizational culture. Innovate both in staffing, technology, organizational operations and service package design and delivery. Ensure workforce is aligned with new integration models, technology, and future care delivery system. Ensure composition of the Board of Trustees and Advisory Council reflects expertise needed to provide oversight of execution of strategic plan. Reform provider processes and ensure effectiveness and efficiency of provider contracting, communication and referral process Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited


198 GET THE PEOPLE IN THE RIGHT SEATS ON THE BUS
199 STRUCTURE TO SUPPORT HIGH PERFORMING TEAMS Initiated self directed teams Business Results and Innovation Business Intelligence (analytics) Business Results (quality) Project Management Business Development Innovative Human Resources Executive Level Self Directed Teams Team Educators Creative staffing structures additional duty, contract employees 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
200 PUT SYSTEMS IN PLACE TO SUPPORT THE STRATEGY Built Cost and Pricing Models Bring Program and Finance People Together Know how every position is paid for Relate cost to services sold Train everyone! Pay for Performance Technology Business Intelligence Systems Care Management Systems VPN access for telecommuting 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
201 CREATE THE CULTURE Data Driven Decision Making Focused on Outcomes, Quality and Results Play to Win Use Cost and Price Models to price services, understand the cost of operations, and drive the culture change 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
202 Care Transitions Program Carl's Grocery Store Model For July 2012 $ FIXED COSTS Cost Clients Program Admin Personnel Costs $ 17, Kim Clark - Kim Hotel - Phyllis Clemons - Mary Whipple - Christine Bonner Telephone & Cell Phones $ Depreciation (QMCO) $ 1, Professional Svcs-Health Council $ 27, Rent $ TOTAL FIXED COSTS $ 47, VARIABLE COSTS Coaching Personnel Costs $ 31, Toni Arquette - Danielle Amrine - Beth Chopra - Vicky DePew - Kieran Fleming - victoria McClain - Cathy VanFossen - Kim Wear 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
 Copying, reproduction or distribution of these materials without the express written")
203 BUILDING THE RIGHT PARTNERSHIPS 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
 Copying, reproduction or distribution of these materials without the express written")
204 Future of COA? 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
 Copying, reproduction or distribution of these materials without the express written permission of COA")
205 LOOKING FORWARD TO THE DAY WHERE COA CAN GO FROM Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
206 TO OUR DESTINATION OF CHOICE! It s within our grasp! 2013 Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited

207 QUESTIONS? Sharon Madi Fusco, BSBA, MHR Director of Business Results and Innovation Council on Aging of Southwestern Ohio (513) Direct line THE ANSWER Council on Aging of Southwestern Ohio, Inc. ("COA") Copying, reproduction or distribution of these materials without the express written permission of COA is prohibited
208 Independent Living and Managed Care Kelly Buckland, National Council on Independent Living and Merrill Friedman, WellPoint GBD
209 Overview Experiences included directly from the Centers for Independent Living in WI, CA, KS, AZ, TX and MA Perceptions and Realities Supporting the CILs to thrive in a managed care environment
210 The Good In Wisconsin, the advocates demanded an independent outside grievance resource which has helped to work for consumer directed service in practice as well as in the literature of providers. Managed Care allows for flexible spending of resources that make sense and serve the individuals needs without being restricted by archaic and cumbersome rules and approval processes. For example, they might be able to pay for taking care of a Service Dog while a consumer is in hospital.
211 The Good Good Managed Care Providers can help divert persons to community care rather than nursing homes or other institutions as a cost effective and desirable service. Most MCOs are interested in working in collaboration with ILCs in California. Some MCOs sponsor ILC events and/or programs.
212 The Good The managed Care Provider may pay for assistive technology/equipment that improves the independence of the individual. Where there are good Managed Care Teams, medical and long term care can be successfully managed to the customers benefit. Often the Managed Care providers will support preventative health and wellness programs.
213 The Good Some MCOs are hiring ILC staff to help develop and implement their programs. Some MCOs have significantly improved the accessibility of their facilities, programs and services and they are focusing more attention on the long term transition plans for better access over the long haul.
214 The Good MCOs have collaborated on writing and submitting CMS Innovation Grants. MCOs have signed contracts with ILCs related to Cal-Medi Connect (Duals Demonstration). MCOs have a track record of contracting with ILCs for trainings. MCOs have staff that have joined the board of directors of some ILCs.
215 The Good BCIL has played a major advocacy role and will also be providing services: PAS, core IL services, and what is called IL-LTSS coordination. Regarding the latter, this is a link between the MCO and consumer to ensure adequate provision of LTSS, an IL-LTSS coordinator will sit on the consumer's care team in a role that is part I&R and part advocate. The person works for a community-based disability organization such as an ILC, but the cost is borne by the MCO. Our advocacy efforts have been around establishing consumer protections, and the main ones include:
216 The Good The IL-LTSS coordinator The right to opt-out: enrollment is initially voluntary, then there'll be staggered auto enrollment in some areas, but at all times consumers can opt to not enroll or opt out and go back to fee for service. An independent ombudsperson program. Establishment of the Implementation Council, composed of advocates and consumers on Medicaid (51% of the body). Training programs for the MCOs that include consumers from ILCs and other disability organizations.
217 The Good We also have worked hard to establish relationships with the MCOs, CMS, and state Medicaid. In some sense they are on the other side, but if you do not work collaboratively with them, the consumers will get short changed. These initiatives can be highly complicated and a simple us-them scenario is naïve for the long term. The Mass. Plan proposes to integrate LTSS and primary care for 90,000 people on both Medicare and Medicaid, ages We see this as a great opportunity, a chance for a healthcare program to be built on LTSS over primary care, but are hardly unaware of risks (bad economics for the MCOs leading to reduced services being the primary concern).
218 The Not So Good When the State reimbursement is inadequate or Managed Care providers profit motive is too high, the quality of service suffers. Hours of PAS and Home health services have been cut by 30 to 50 % often without any individual assessments.
219 The Not So Good A bad treatment team at the Managed Care Provider can destroy long term medical and community supports the individual has depended on. As new providers come on the Managed Care scene or old providers move to new area s they often hire staff who do not know the community and are not familiar with the service system.
220 The Not So Good Cash flow for a CIL with a Managed Care Provider can be a financial drain as some MCOs don t pay until 60 to 90 days after the service has been performed and the worker paid. States do not seem to be maintaining their ability to monitor or audit quality after Managed Care has been implemented.
221 The Not So Good Most MCOs have NOT signed contracts with most ILCs. MCOs cite the constantly changing implementations dates as a reason not to sign contracts with ILCs. MCOs also cite the need to understand rate structure before contracting with ILCs.
222 The Not So Good ILCs need to build capacity to meet potential demand but do not have general funds to make this happen. ILCs are not clear about what MCOs are seeking in service provision, mainly because MCOs are unclear about what they need and how much they are willing to pay.
223 The Not So Good There seems to be a mindset that family members and friends should provide PAS for free. This ruins families abilities to earn an income and I think degrades the profession of personal care services. Flip side is that it sets up situations where family income becomes dependent on provision of the PAS. There can be a lowering of quality service to consumers as the person directing the service, the consumer, may have a hard time holding firm against a family member when services aren't up to par.
224 Next Steps Prioritize HCBS in contract development. Engage CILs in negotiations and development early
225 Managed Care Organizations and Area Agency on Aging Working Together
226 Confidentiality The enrollment of any independent contractor or temporary employee in classes or the use of training materials provided by UnitedHealthcare Community & State or its affiliates ( Community & State ) shall not be construed to create a partnership, joint venture or any other relationship between Community & State and such independent contractor or temporary employee. This material, including the trademarks, logos and service marks are the property of Community & State and Community & State Clinical Learning & Development and may not be duplicated or used without the prior written consent of Community & State and Community & State Clinical Learning & Development. 2 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.

227 Objectives Review the role of the Manage Care Organization (MCO) Recall the purpose of the Area Agency on Aging(AAA) Describe the MCO selection process of an AAA organization Recall Quality Metrics the MCO reviews regarding AAA Organization Describe the collaboration between the MCO and AAA s Review MCO Expectations of the AAA 3 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.




228 Snapshot of a Managed Care Organization(MCO) Managed Care Organization Transition al Care Member Care Direction Personal Services Plan of Care Provider Promote Personal Choice Education Communication Accessibility Cost Effective 4 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.

229 Area Agency on Aging(AAA) Established in 1973 under the Older Americans Act Responds to the needs of Americans 60 and over Helps to seniors to identify community based options to remain in a home based setting Located in most local communities throughout Advocates for the elderly Can provide family and caregiver support and may include respite Option Counseling May serve as an ADRC May provide community based services, i.e. personal care, home delivered meals, adult day programs 5 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
230 Selecting a AAA AAA State requirements may determine provider coverage which may be vary upon the size of the area being serviced Physician feedback is key as part of the initial entrance into the market as they maybe able to provide working knowledge of the providers in the area Community resources and agencies may also provide feedback regarding specific providers Once a market is active feedback from members and clinical care coordinators become essential Checklist some key items used when contracting AAA: MCO will ensure policies and procedures are in place MCO ensures disaster plans are available Onsite review tool to be completed by Provider Advocate 6 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.




231 Quality/Reimbursement and the AAA s AAA MCO Quality Review: 8 point check list of activities are completed Website review Monitor timeliness of assessments and member contacts Re-credentialing completed every 2 to 3years dependent upon state requirements Reimbursement: Dependent upon the state requirements State provides rate/codes to be used for services 7 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.



232 MCO Collaboration with AAA Member AAA Collaborate with AAA s to identify community resources available to members Responsive to questions that are poised by AAA s and identified organizations Identify common initiatives in which the MCO and AAA will partner on MCO 8 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
233 Vision/Goals Establish and maintain a collaborative, relationship with the member and family support system Develop cultural awareness and sensitivity to assigned population Establish a working relationship with providers who are involved with member s care Complete all state required and applicable assessments within required timeframes Deliver Care Coordination, i.e. care plan development, coordinate services 9 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
 Ensure timely access to services needed to help each member maintain or improve his/her quality of life Facilitate")
234 Deliver Care Coordination Assess the member s holistically: physical, behavioral, Functional Psychosocial needs Develop a member centered service/care plan(poc) Co-develop POC with member and other representatives or caregivers the member would want to include in the process) Ensure timely access to services needed to help each member maintain or improve his/her quality of life Facilitate access to other social support services and assistance needed in order to promote each member s health, safety and welfare 10 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
235 Communicate Changes Notification to the HP upon changes that may include but are not limited to the following; ER visits, hospital or ambulatory care center admissions; Significant changes in the member s clinical and/or behavioral status that impact the member s service plan. Changes in living arrangements Quality of care concerns Joint operating meetings between lead agency liaison and health plan liaison Coordination with PCP and specialty providers, such as mental health 11 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
236 Education Requirements Case Management: Maintain all necessary certifications, licensures as well as all general state required qualifications, e.g. RN license. Provide staff training related to cultural sensitivity Agree to participate in mutual education and training sessions Knowledge and experience providing case management of the population serviced Community partner and support Caregiver education and training Town Halls 12 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.

237 Identify Quality of Care Issues and Reporting Monitor timeliness of service initiation Report potential Quality of Care Issues and/or Critical Incidents in a timely manner including: member complaints Suspected member abuse, neglect and exploitation Monitor member satisfaction Maintain staffing ratios to ensure proper care of members 13 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.

238 Summary By working together and viewing the member in a holistic manor we can accomplish the following: Provide the member with an improved quality of life Access to critical resources Reduction in hospitalizations Keep the member in their community setting of choice 14 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
Family Care and IRIS Ombudsman Program. Year 3 Annual Report:
 Family Care and IRIS Ombudsman Program For Enrollees Age 18-59 Year 3 Annual Report: July 1, 2010 - June 30, 2011 Report Date: October 1, 2011 MADISON OFFICE 131 W. Wilson St. Suite 700 Madison, WI 53703
Family Care and IRIS Ombudsman Program For Enrollees Age 18-59 Year 3 Annual Report: July 1, 2010 - June 30, 2011 Report Date: October 1, 2011 MADISON OFFICE 131 W. Wilson St. Suite 700 Madison, WI 53703
Family Care and IRIS Ombudsman Program. Year 6 Annual Report:
 Family Care and IRIS Ombudsman Program For Enrollees Age 18-59 Year 6 Annual Report: July 1, 2013 - June 30, 2014 Report Date: October 1, 2014 MADISON OFFICE 131 W. Wilson St. Suite 700 Madison, WI 53703
Family Care and IRIS Ombudsman Program For Enrollees Age 18-59 Year 6 Annual Report: July 1, 2013 - June 30, 2014 Report Date: October 1, 2014 MADISON OFFICE 131 W. Wilson St. Suite 700 Madison, WI 53703
Long-Term Care Improvements under the Affordable Care Act (ACA)
") Long-Term Care Improvements under the Affordable Care Act (ACA) South Carolina Health Care Implementation Coalition September 17, 2010 JoAnn Lamphere, DrPH Director, State Government Relations Health &
Long-Term Care Improvements under the Affordable Care Act (ACA) South Carolina Health Care Implementation Coalition September 17, 2010 JoAnn Lamphere, DrPH Director, State Government Relations Health &
Supporting MLTSS Consumers through Problem Resolution and Advocacy
 Supporting MLTSS Consumers through Problem Resolution and Advocacy James David Toews, Becky A. Kurtz, Eliza Bangit September 11, 2013 Risks of Managed Long-Term Services and Supports (MLTSS) Many managed
Supporting MLTSS Consumers through Problem Resolution and Advocacy James David Toews, Becky A. Kurtz, Eliza Bangit September 11, 2013 Risks of Managed Long-Term Services and Supports (MLTSS) Many managed
Medicaid Managed Care. Long-term Services and Supports Trends
 Medicaid Managed Care Long-term Services and Supports Trends Medicaid Managed Care Statistics As of 2011, 74.2% of Medicaid Enrollees were enrolled in a Medicaid Managed Care system As of 2011, California,
Medicaid Managed Care Long-term Services and Supports Trends Medicaid Managed Care Statistics As of 2011, 74.2% of Medicaid Enrollees were enrolled in a Medicaid Managed Care system As of 2011, California,
STRATEGIES FOR INCORPORATING PACE INTO STATE INTEGRATED CARE INITIATIVES
 NATIONAL PACE ASSOCIATION STRATEGIES FOR INCORPORATING PACE INTO STATE INTEGRATED CARE INITIATIVES A Toolkit for States MARCH, 2014 WWW.NPAONLINE.ORG 703-535-1565 STRATEGIES FOR INCORPORATING PACE INTO
NATIONAL PACE ASSOCIATION STRATEGIES FOR INCORPORATING PACE INTO STATE INTEGRATED CARE INITIATIVES A Toolkit for States MARCH, 2014 WWW.NPAONLINE.ORG 703-535-1565 STRATEGIES FOR INCORPORATING PACE INTO
Managed Long-Term Care in New Jersey
 Managed Long-Term Care in New Jersey April 2009 Jon S. Corzine Governor Heather Howard Commissioner Introduction New Jersey s Fiscal Year 2009 Budget included the following language: On or before April
Managed Long-Term Care in New Jersey April 2009 Jon S. Corzine Governor Heather Howard Commissioner Introduction New Jersey s Fiscal Year 2009 Budget included the following language: On or before April
Sunflower Health Plan
 Key Components for Successful LTSS Integration: Case Studies of Ten Exemplar Programs Sunflower Health Plan Jennifer Windh September 2016 Long- term services and supports (LTSS) integration is the integration
Key Components for Successful LTSS Integration: Case Studies of Ten Exemplar Programs Sunflower Health Plan Jennifer Windh September 2016 Long- term services and supports (LTSS) integration is the integration
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network. Monday, September 12, 2011
 Care Coordination and the Role of the Aging Network. Monday, September 12, 2011") National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
MDS 3.0 Section Q Implementation Questions and Answers from Informing LTC Choice conference and s September 22, 2010
 MDS 3.0 Section Q Implementation Questions and Answers from Informing LTC Choice conference and emails September 22, 2010 DATA USE AGREEMENTS (DUA) 1. Do state agencies need a Data Use Agreement to implement
MDS 3.0 Section Q Implementation Questions and Answers from Informing LTC Choice conference and emails September 22, 2010 DATA USE AGREEMENTS (DUA) 1. Do state agencies need a Data Use Agreement to implement
ABC's of Managed Care and What It Might Mean for Home & Community Based Services
 ABC's of Managed Care and What It Might Mean for Home & Community Based Services This project is supported by a grant from the Pennsylvania Developmental Disabilities Council. David Gates DGates@phlp.org
ABC's of Managed Care and What It Might Mean for Home & Community Based Services This project is supported by a grant from the Pennsylvania Developmental Disabilities Council. David Gates DGates@phlp.org
Options for Integrating Care for Dual Eligible Beneficiaries
 CHCS Center for Health Care Strategies, Inc. Technical Assistance Brief Options for Integrating Care for Dual Eligible Beneficiaries By Melanie Bella and Lindsay Palmer-Barnette, Center for Health Care
CHCS Center for Health Care Strategies, Inc. Technical Assistance Brief Options for Integrating Care for Dual Eligible Beneficiaries By Melanie Bella and Lindsay Palmer-Barnette, Center for Health Care
Transforming Louisiana s Long Term Care Supports and Services System. Initial Program Concept
 Transforming Louisiana s Long Term Care Supports and Services System Initial Program Concept August 30, 2013 Transforming Louisiana s Long Term Care Supports and Services System Our Vision Introduction
Transforming Louisiana s Long Term Care Supports and Services System Initial Program Concept August 30, 2013 Transforming Louisiana s Long Term Care Supports and Services System Our Vision Introduction
COMMUNITY-BASED LONG TERM CARE PROGRAMS IN WISCONSIN. Attorney Mitchell Hagopian Disability Rights Wisconsin July 2013
 COMMUNITY-BASED LONG TERM CARE PROGRAMS IN WISCONSIN I. INTRODUCTION Attorney Mitchell Hagopian Disability Rights Wisconsin July 2013 In 1981, with the creation of the Community Options Program, the state
COMMUNITY-BASED LONG TERM CARE PROGRAMS IN WISCONSIN I. INTRODUCTION Attorney Mitchell Hagopian Disability Rights Wisconsin July 2013 In 1981, with the creation of the Community Options Program, the state
Rate-Setting Strategies to Advance Medicaid Managed Long-Term Services and Supports Goals: State Insights
 Rate-Setting Strategies to Advance Medicaid Managed Long-Term Services and Supports Goals: State Insights Tuesday, August 16, 2016 1:00-2:30 pm ET Made possible by the West Health Policy Center www.chcs.org
Rate-Setting Strategies to Advance Medicaid Managed Long-Term Services and Supports Goals: State Insights Tuesday, August 16, 2016 1:00-2:30 pm ET Made possible by the West Health Policy Center www.chcs.org
Medicaid Transformation
 Medicaid Transformation Debra Farrington Senior Program Manager August 18, 2017 Medicaid Managed Care Already Exists in NC What North Carolina Has Now PRIMARY CARE CASE MANAGEMENT (CCNC) Primary care provider-based
Medicaid Transformation Debra Farrington Senior Program Manager August 18, 2017 Medicaid Managed Care Already Exists in NC What North Carolina Has Now PRIMARY CARE CASE MANAGEMENT (CCNC) Primary care provider-based
The Patient Protection and Affordable Care Act (Public Law )
") Policy Brief No. 2 March 2010 A Summary of the Patient Protection and Affordable Care Act (P.L. 111-148) and Modifications by the On March 23, 2010, President Obama signed into law the Patient Protection
Policy Brief No. 2 March 2010 A Summary of the Patient Protection and Affordable Care Act (P.L. 111-148) and Modifications by the On March 23, 2010, President Obama signed into law the Patient Protection
A Snapshot of Uniform Assessment Practices in Managed Long Term Services and Supports
 A Snapshot of Uniform Assessment Practices in Managed Long Term Services and Supports California Department of Health Care Services, Home and Community Based Services Universal Assessment Workgroup February
A Snapshot of Uniform Assessment Practices in Managed Long Term Services and Supports California Department of Health Care Services, Home and Community Based Services Universal Assessment Workgroup February
A Snapshot of the Connecticut LTSS Rebalancing Agenda
 A Snapshot of the Connecticut LTSS Rebalancing Agenda Agenda Medicaid context and vision State Rebalancing Plan Major elements of rebalancing agenda Money Follows the Person, Nursing Home Rightsizing,
A Snapshot of the Connecticut LTSS Rebalancing Agenda Agenda Medicaid context and vision State Rebalancing Plan Major elements of rebalancing agenda Money Follows the Person, Nursing Home Rightsizing,
The Who, What, When, Where and How of Ombudsman Services for Home Care Consumers
 The Who, What, When, Where and How of Ombudsman Services for Home Care Consumers Becky A. Kurtz, Director, Office of Long-Term Care Ombudsman Programs The Consumer Voice Conference October 25, 2013 1 Brief
The Who, What, When, Where and How of Ombudsman Services for Home Care Consumers Becky A. Kurtz, Director, Office of Long-Term Care Ombudsman Programs The Consumer Voice Conference October 25, 2013 1 Brief
The Commission on Long-Term Care: Background Behind the Mission
 THE BASICS The Commission on Long-Term Care: Background Behind the Mission As part of the American Taxpayer Relief Act of 2012 (ATRA, P.L. 112-240), Congress created a Commission on Long-Term Care 1 that
THE BASICS The Commission on Long-Term Care: Background Behind the Mission As part of the American Taxpayer Relief Act of 2012 (ATRA, P.L. 112-240), Congress created a Commission on Long-Term Care 1 that
California s Coordinated Care Initiative
 California s Coordinated Care Initiative Sarah Arnquist Harbage Consulting Presentation on 4/22/13 2 Overview Federal and State Movement toward Coordinated Care Update on California s Coordinated Care
California s Coordinated Care Initiative Sarah Arnquist Harbage Consulting Presentation on 4/22/13 2 Overview Federal and State Movement toward Coordinated Care Update on California s Coordinated Care
Lessons Learned from MLTSS Implementation in Florida Where Have We Been and Where Are We Going?
 Lessons Learned from MLTSS Implementation in Florida Where Have We Been and Where Are We Going? David Rogers Assistant Deputy Secretary for Medicaid Operations Agency for Health Care Administration 2016
Lessons Learned from MLTSS Implementation in Florida Where Have We Been and Where Are We Going? David Rogers Assistant Deputy Secretary for Medicaid Operations Agency for Health Care Administration 2016
Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10
 Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10 On March 23, 2010, President Obama signed a comprehensive health care reform bill (H.R. 3590) into law. On March
Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10 On March 23, 2010, President Obama signed a comprehensive health care reform bill (H.R. 3590) into law. On March
Medicaid and CHIP Payment and Access Commission (MACPAC) February 2013 Meeting Summary
 February 2013 Meeting Summary") Medicaid and CHIP Payment and Access Commission (MACPAC) February 2013 Meeting Summary The Medicaid and CHIP Payment and Access Commission (MACPAC) was established in the Children's Health Insurance Program
Medicaid and CHIP Payment and Access Commission (MACPAC) February 2013 Meeting Summary The Medicaid and CHIP Payment and Access Commission (MACPAC) was established in the Children's Health Insurance Program
9/10/2013. The Session s Focus. Status of the NYS FIDA Initiative
 Leading Age NY Financial Manager s Conference, September 10-12, 2013 The Otesaga Resort Hotel, Cooperstown NY Paul Tenan VCC, Inc. FIDA: An Overview and Update The Session s Focus Overview of CMS national
Leading Age NY Financial Manager s Conference, September 10-12, 2013 The Otesaga Resort Hotel, Cooperstown NY Paul Tenan VCC, Inc. FIDA: An Overview and Update The Session s Focus Overview of CMS national
kaiser medicaid and the uninsured commission on O L I C Y
 P O L I C Y B R I E F kaiser commission on medicaid and the uninsured 1330 G S T R E E T NW, W A S H I N G T O N, DC 20005 P H O N E: (202) 347-5270, F A X: ( 202) 347-5274 W E B S I T E: W W W. K F F.
P O L I C Y B R I E F kaiser commission on medicaid and the uninsured 1330 G S T R E E T NW, W A S H I N G T O N, DC 20005 P H O N E: (202) 347-5270, F A X: ( 202) 347-5274 W E B S I T E: W W W. K F F.
KanCare and Your Plan of Care: Know Your Rights What you can do when needed services are reduced, eliminated or denied
 KanCare and Your Plan of Care: Know Your Rights What you can do when needed services are reduced, eliminated or denied Kansas Advocates for Better Care 800.525.1782 913 Tennessee, Ste 2, Lawrence, KS 66044
KanCare and Your Plan of Care: Know Your Rights What you can do when needed services are reduced, eliminated or denied Kansas Advocates for Better Care 800.525.1782 913 Tennessee, Ste 2, Lawrence, KS 66044
Medicaid and CHIP Managed Care Final Rule MLTSS
 Medicaid and CHIP Managed Care Final Rule MLTSS John Giles, Technical Director Division of Quality and Health Outcomes Children and Adult Health Programs Group Debbie Anderson, Deputy Director Division
Medicaid and CHIP Managed Care Final Rule MLTSS John Giles, Technical Director Division of Quality and Health Outcomes Children and Adult Health Programs Group Debbie Anderson, Deputy Director Division
Guidance for Monitoring the Toll-Free Helpline and Online Complaint Process. Content
 The State of Wisconsin Board on Aging and Long Term Care A Voice for Long Term Care Consumers Serving Persons Aged 60 and Older Guidance for Monitoring the Toll-Free Helpline and Online Complaint Process
The State of Wisconsin Board on Aging and Long Term Care A Voice for Long Term Care Consumers Serving Persons Aged 60 and Older Guidance for Monitoring the Toll-Free Helpline and Online Complaint Process
Table of Contents Executive Summary... 3 Introduction... 5 Public and Stakeholder Engagement... 5 Ongoing Consumer and Stakeholder Engagement in
 P-01242 (03/2016) 1 Table of Contents Executive Summary... 3 Introduction... 5 Public and Stakeholder Engagement... 5 Ongoing Consumer and Stakeholder Engagement in Family Care/IRIS 2.0... 6 Guiding Principles...
P-01242 (03/2016) 1 Table of Contents Executive Summary... 3 Introduction... 5 Public and Stakeholder Engagement... 5 Ongoing Consumer and Stakeholder Engagement in Family Care/IRIS 2.0... 6 Guiding Principles...
Medicaid Home- and Community-Based Waiver Programs
 INFORMATION BRIEF Research Department Minnesota House of Representatives 600 State Office Building St. Paul, MN 55155 Danyell Punelli, Legislative Analyst 651-296-5058 Updated: October 2016 Medicaid Home-
INFORMATION BRIEF Research Department Minnesota House of Representatives 600 State Office Building St. Paul, MN 55155 Danyell Punelli, Legislative Analyst 651-296-5058 Updated: October 2016 Medicaid Home-
COMMUNITY CLINIC GRANT PROGRAM
 COMMUNITY CLINIC GRANT PROGRAM FINAL GRANT APPLICATION GUIDANCE Grant Project Period: April 1, 2015 March 31, 2016 Application Due: December 22, 2014 MINNESOTA DEPARTMENT OF HEALTH OFFICE OF RURAL HEALTH
COMMUNITY CLINIC GRANT PROGRAM FINAL GRANT APPLICATION GUIDANCE Grant Project Period: April 1, 2015 March 31, 2016 Application Due: December 22, 2014 MINNESOTA DEPARTMENT OF HEALTH OFFICE OF RURAL HEALTH
GAO MEDICARE AND MEDICAID. Consumer Protection Requirements Affecting Dual-Eligible Beneficiaries Vary across Programs, Payment Systems, and States
 GAO United States Government Accountability Office Report to Congressional Requesters December 2012 MEDICARE AND MEDICAID Consumer Protection Requirements Affecting Dual-Eligible Beneficiaries Vary across
GAO United States Government Accountability Office Report to Congressional Requesters December 2012 MEDICARE AND MEDICAID Consumer Protection Requirements Affecting Dual-Eligible Beneficiaries Vary across
Select Topics in Implementing an Integrated Medicaid Managed Long-Term Care Program
 Select Topics in Implementing an Integrated Medicaid Managed Long-Term Care Program TennCare Overview Tennessee s Medicaid Agency Tennessee s Medicaid Program Managed care demonstration implemented in
Select Topics in Implementing an Integrated Medicaid Managed Long-Term Care Program TennCare Overview Tennessee s Medicaid Agency Tennessee s Medicaid Program Managed care demonstration implemented in
Home Care Ombudsman Expansion. Lyle VanDeventer, Deputy State Home Care Ombudsman (v)
") Home Care Ombudsman Expansion Lyle VanDeventer, Deputy State Home Care Ombudsman 217.557.1532 (v) lyle.vandeventer@illinois.gov Service Integration February 22, 2013, the Centers for Medicare and Medicaid
Home Care Ombudsman Expansion Lyle VanDeventer, Deputy State Home Care Ombudsman 217.557.1532 (v) lyle.vandeventer@illinois.gov Service Integration February 22, 2013, the Centers for Medicare and Medicaid
programs and briefly describes North Carolina Medicaid s preliminary
 State Experiences with Managed Long-term Care in Medicaid* Brian Burwell Vice President, Chronic Care and Disability Medstat Abstract: Across the country, state Medicaid programs are expressing renewed
State Experiences with Managed Long-term Care in Medicaid* Brian Burwell Vice President, Chronic Care and Disability Medstat Abstract: Across the country, state Medicaid programs are expressing renewed
Managing Medicaid s Costliest Members
 Managing Medicaid s Costliest Members White Paper January 2018 LTSS / MLTSS / HCBS: Issues & Guiding Principles for State Medicaid Programs Table of Contents Executive Summary... 3 LTSS: The Basics...
Managing Medicaid s Costliest Members White Paper January 2018 LTSS / MLTSS / HCBS: Issues & Guiding Principles for State Medicaid Programs Table of Contents Executive Summary... 3 LTSS: The Basics...
SHARED DECISION-MAKING AND DIGNITY OF RISK
 SHARED DECISION-MAKING AND DIGNITY OF RISK Susan Fisher Wisconsin Guardianship Support Center Managing Attorney Greater Wisconsin Agency on Aging Resources, Inc. & Kim Marheine Ombudsman Services Supervisor
SHARED DECISION-MAKING AND DIGNITY OF RISK Susan Fisher Wisconsin Guardianship Support Center Managing Attorney Greater Wisconsin Agency on Aging Resources, Inc. & Kim Marheine Ombudsman Services Supervisor
MANAGED CARE READINESS
 MANAGED CARE READINESS A SELF-ASSESSMENT TOOL FOR HIV SUPPORT SERVICE AGENCIES U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES HEALTH RESOURCES & SERVICES ADMINISTRATION HIV/AIDS BUREAU MANAGED CARE READINESS
MANAGED CARE READINESS A SELF-ASSESSMENT TOOL FOR HIV SUPPORT SERVICE AGENCIES U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES HEALTH RESOURCES & SERVICES ADMINISTRATION HIV/AIDS BUREAU MANAGED CARE READINESS
MDS 3.0 Section Q Implementation Questions and Answers from Informing LTC Choice conference and s June 7, 2010
 MDS 3.0 Section Q Implementation Questions and Answers from Informing LTC Choice conference and emails June 7, 2010 DATA USE AGREEMENTS (DUA) 1. Do state agencies need a Data Use Agreement to implement
MDS 3.0 Section Q Implementation Questions and Answers from Informing LTC Choice conference and emails June 7, 2010 DATA USE AGREEMENTS (DUA) 1. Do state agencies need a Data Use Agreement to implement
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
From Fragmentation to Integration: Bringing Medical Care and HCBS Together. Jessica Briefer French Senior Research Scientist
 From Fragmentation to Integration: Bringing Medical Care and HCBS Together Jessica Briefer French Senior Research Scientist 1 Integration: The Holy Grail? An act or instance of combining into an integral
From Fragmentation to Integration: Bringing Medical Care and HCBS Together Jessica Briefer French Senior Research Scientist 1 Integration: The Holy Grail? An act or instance of combining into an integral
Medicaid Managed Long Term Care in Florida Issue Brief December 2017 by LuMarie Polivka-West, Sr. Research Associate Volunteer
 Medicaid Managed Long Term Care in Florida Issue Brief December 2017 by LuMarie Polivka-West, Sr. Research Associate Volunteer Henry is a 76 year old, previously self-employed, very frail man with advanced
Medicaid Managed Long Term Care in Florida Issue Brief December 2017 by LuMarie Polivka-West, Sr. Research Associate Volunteer Henry is a 76 year old, previously self-employed, very frail man with advanced
Position Description. Long-Term Care Ombudsman Representatives Program Coordinator
 Hawaii SLTCOP Position Description Long-Term Care Ombudsman Representatives Program Coordinator I IDENTIFYING INFORMATION Position/Pseudo Number: 110939 Department: Health Division: Executive Office on
Hawaii SLTCOP Position Description Long-Term Care Ombudsman Representatives Program Coordinator I IDENTIFYING INFORMATION Position/Pseudo Number: 110939 Department: Health Division: Executive Office on
Virginia s ID/DD Waiver Re-Design Update
 Virginia s ID/DD Waiver Re-Design Update vaaccses Annual Provider Conference June 8, 2015 Connie Cochran, Assistant Commissioner and Dawn Traver, Waiver Operations Director Division of Developmental Services
Virginia s ID/DD Waiver Re-Design Update vaaccses Annual Provider Conference June 8, 2015 Connie Cochran, Assistant Commissioner and Dawn Traver, Waiver Operations Director Division of Developmental Services
Medicaid and You Yesterday and Tomorrow: How Medicaid and Payment Reforms Impact Assisted Living Providers
 Medicaid and You Yesterday and Tomorrow: How Medicaid and Payment Reforms Impact Assisted Living Providers Ohio Assisted Living Association November 5, 2012 Suzanne J. Scrutton Vorys, Sater, Seymour and
Medicaid and You Yesterday and Tomorrow: How Medicaid and Payment Reforms Impact Assisted Living Providers Ohio Assisted Living Association November 5, 2012 Suzanne J. Scrutton Vorys, Sater, Seymour and
1915(i) State Plan Home and Community-Based Services Overview
 State Plan Home and Community-Based Services Overview") GOVERNMENT OF THE DISTRICT OF COLUMBIA Department of Health Care Finance 1915(i) State Plan Home and Community-Based Services Overview Purpose: The Adult Day Health Program- 1915(i) is a new service under
GOVERNMENT OF THE DISTRICT OF COLUMBIA Department of Health Care Finance 1915(i) State Plan Home and Community-Based Services Overview Purpose: The Adult Day Health Program- 1915(i) is a new service under
MEDICAID MANAGED LONG-TERM SERVICES AND SUPPORTS OPPORTUNITIES FOR INNOVATIVE PROGRAM DESIGN
 Louisiana Behavioral Health Partnership MEDICAID MANAGED LONG-TERM SERVICES AND SUPPORTS OPPORTUNITIES FOR INNOVATIVE PROGRAM DESIGN Rosanne Mahaney - Delaware Lou Ann Owen - Louisiana Brenda Jackson,
Louisiana Behavioral Health Partnership MEDICAID MANAGED LONG-TERM SERVICES AND SUPPORTS OPPORTUNITIES FOR INNOVATIVE PROGRAM DESIGN Rosanne Mahaney - Delaware Lou Ann Owen - Louisiana Brenda Jackson,
Disability Rights California
 Disability Rights California California s protection and advocacy system BAY AREA REGIONAL OFFICE 1330 Broadway, Suite 500 Oakland, CA 94612 Tel: (510) 267-1200 TTY: (800) 719-5798 Toll Free: (800) 776-5746
Disability Rights California California s protection and advocacy system BAY AREA REGIONAL OFFICE 1330 Broadway, Suite 500 Oakland, CA 94612 Tel: (510) 267-1200 TTY: (800) 719-5798 Toll Free: (800) 776-5746
Tennessee s Money Follows the Person Demonstration: Supporting Rebalancing in a Managed Long-Term Services and Supports Model
 Tennessee s Money Follows the Person Demonstration: Supporting Rebalancing in a Managed Long-Term Services and Supports Model In 2011, Tennessee was awarded a federal Money Follows the Person (MFP) grant,
Tennessee s Money Follows the Person Demonstration: Supporting Rebalancing in a Managed Long-Term Services and Supports Model In 2011, Tennessee was awarded a federal Money Follows the Person (MFP) grant,
Quality Improvement Program Evaluation
 Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
Better Health Care for all Floridians. July 13, 2012
 RICK SCOTT GOVERNOR Better Health Care for all Floridians ELIZABETH DUDEK SECRETARY July 13, 2012 Prospective Vendor: Subject: Solicitation Number: AHCA ITN 004-12/13 Title: Statewide Medicaid Managed
RICK SCOTT GOVERNOR Better Health Care for all Floridians ELIZABETH DUDEK SECRETARY July 13, 2012 Prospective Vendor: Subject: Solicitation Number: AHCA ITN 004-12/13 Title: Statewide Medicaid Managed
Long-Term Care Glossary
 Long-Term Care Glossary Adjudicated Claim Activities of Daily Living (ADL) A claim that has reached final disposition such that it is either paid or denied. Basic tasks individuals perform in the course
Long-Term Care Glossary Adjudicated Claim Activities of Daily Living (ADL) A claim that has reached final disposition such that it is either paid or denied. Basic tasks individuals perform in the course
Diamond State Health Plan Plus
 I N T E G R A T E D L O N G T E R M Diamond State Health Plan Plus DSHP-Plus C A R E 1115 Demonstration Waiver Diamond State Health Plan (DSHP) Managed Care Delivery System Operational since January 1996
I N T E G R A T E D L O N G T E R M Diamond State Health Plan Plus DSHP-Plus C A R E 1115 Demonstration Waiver Diamond State Health Plan (DSHP) Managed Care Delivery System Operational since January 1996
Washington State LTSS System, History and Vision
 Washington State LTSS System, History and Vision Bea Rector, Director, Home and Services Aging and Long Term Support Administration Washington State Department of Social and Health Services For Northwest
Washington State LTSS System, History and Vision Bea Rector, Director, Home and Services Aging and Long Term Support Administration Washington State Department of Social and Health Services For Northwest
Lessons Learned from the Dual Eligibles Demonstrations. Real-Life Takeaways from California and Other States
 Lessons Learned from the Dual Eligibles Demonstrations 1 May 28, 2015 Real-Life Takeaways from California and Other States Introductions Toby Douglas Consultant, MAXIMUS Former Director of California Department
Lessons Learned from the Dual Eligibles Demonstrations 1 May 28, 2015 Real-Life Takeaways from California and Other States Introductions Toby Douglas Consultant, MAXIMUS Former Director of California Department
The Changing Role of States in Long-Term Services and Supports
 The Changing Role of States in Long-Term Services and Supports TennCare Overview Tennessee s Medicaid Agency Tennessee s Medicaid Program Managed care demonstration implemented in 1994 Operates under the
The Changing Role of States in Long-Term Services and Supports TennCare Overview Tennessee s Medicaid Agency Tennessee s Medicaid Program Managed care demonstration implemented in 1994 Operates under the
Long-Term Services and Supports Study Committee: Person-Centered Medicaid Managed Care
 Long-Term Services and Supports Study Committee: Person-Centered Medicaid Managed Care Barbara R. Sears, Director Ohio Department of Medicaid July 12, 2018 1 Health Care System Choices Fee-for-Service
Long-Term Services and Supports Study Committee: Person-Centered Medicaid Managed Care Barbara R. Sears, Director Ohio Department of Medicaid July 12, 2018 1 Health Care System Choices Fee-for-Service
Strategic Plan SFY
 Strategic Plan SFY 2017-2018 DHS STRATEGY MAP SFY 2017-2018 OUR MISSION We improve the quality of life of vulnerable Oklahomans by increasing people s ability to lead safer, healthier, more independent
Strategic Plan SFY 2017-2018 DHS STRATEGY MAP SFY 2017-2018 OUR MISSION We improve the quality of life of vulnerable Oklahomans by increasing people s ability to lead safer, healthier, more independent
Welcome and Introductions
 Integrating Care for Dual Eligible Beneficiaries National Conference of State Legislatures Fall Forum: Changing Roles of States in Long Term Services and Supports December 3, 2013 Sarah Barth, JD www.chcs.org
Integrating Care for Dual Eligible Beneficiaries National Conference of State Legislatures Fall Forum: Changing Roles of States in Long Term Services and Supports December 3, 2013 Sarah Barth, JD www.chcs.org
Quality Assurance in Minnesota 2007
 Quality Assurance in Minnesota 2007 Findings and Recommendations of the Legislatively- Mandated Quality Assurance Panel Laws of Minnesota 2005, First Special Session, Chapter 4, Article 7, Sec. 57 Final
Quality Assurance in Minnesota 2007 Findings and Recommendations of the Legislatively- Mandated Quality Assurance Panel Laws of Minnesota 2005, First Special Session, Chapter 4, Article 7, Sec. 57 Final
Implementing the Affordable Care Act:
 Implementing the Affordable Care Act: Making it Easier For Individuals to Navigate Their Health and Long Term Care 26 th National Home and Community Based Services Conference Tuesday, September 28, 2010
Implementing the Affordable Care Act: Making it Easier For Individuals to Navigate Their Health and Long Term Care 26 th National Home and Community Based Services Conference Tuesday, September 28, 2010
Options Counseling ADRC Style: Interactive Workshop
 Options Counseling ADRC Style: Interactive Workshop 0 Is Your Organization Ready? What surprised you? Where are your strengths? Where do you need to grow? What other items would you add to this readiness
Options Counseling ADRC Style: Interactive Workshop 0 Is Your Organization Ready? What surprised you? Where are your strengths? Where do you need to grow? What other items would you add to this readiness
SMMC: LTC and MMA. Linda R. Chamberlain, P.A. Member Firm Florida Elder Lawyers PLLC
 SMMC: LTC and MMA Linda R. Chamberlain, P.A. Member Firm Florida Elder Lawyers PLLC 727.443.7898 Why should you care about SMMC Florida has 7M+ people 50 y/o + 4M+ Social Security beneficiaries 3.5M+ Medicare
SMMC: LTC and MMA Linda R. Chamberlain, P.A. Member Firm Florida Elder Lawyers PLLC 727.443.7898 Why should you care about SMMC Florida has 7M+ people 50 y/o + 4M+ Social Security beneficiaries 3.5M+ Medicare
The Long-Term Care Ombudsman Program: What Residents Who Want to Transition Can Expect from Their Advocates
 The Long-Term Care Ombudsman Program: What Residents Who Want to Transition Can Expect from Their Advocates Becky A. Kurtz Director, Office of Long-Term Care Ombudsman Programs MDS 3.0 Section Q National
The Long-Term Care Ombudsman Program: What Residents Who Want to Transition Can Expect from Their Advocates Becky A. Kurtz Director, Office of Long-Term Care Ombudsman Programs MDS 3.0 Section Q National
NEW YORK STATE MEDICAID REDESIGN TEAM AND THE AFFORDABLE CARE ACT (MRT & ACA)
") NEW YORK STATE MEDICAID REDESIGN TEAM AND THE AFFORDABLE CARE ACT (MRT & ACA) The Affordable Care Act (ACA) The Affordable Care Act 3 Officially called the Patient Protection and Affordable Care Act (PPACA)
NEW YORK STATE MEDICAID REDESIGN TEAM AND THE AFFORDABLE CARE ACT (MRT & ACA) The Affordable Care Act (ACA) The Affordable Care Act 3 Officially called the Patient Protection and Affordable Care Act (PPACA)
CAHPS Home and Community- Based Services Survey Tools 2017 HCBS Conference August 31, 2017
 CAHPS Home and Community- Based Services Survey Tools 2017 HCBS Conference August 31, 2017 This document was made possible under Contract HHSM-500-2010-0025I-T006 from the Centers for Medicare & Medicaid
CAHPS Home and Community- Based Services Survey Tools 2017 HCBS Conference August 31, 2017 This document was made possible under Contract HHSM-500-2010-0025I-T006 from the Centers for Medicare & Medicaid
Michigan s Response to CMS Solicitation State Demonstrations to Integrate Care for Dual Eligible Individuals
 Michigan s Response to CMS Solicitation State Demonstrations to Integrate Care for Dual Eligible Individuals Solicitation Number: RFP-CMS-2011-0009 Department of Health and Human Services Centers for Medicare
Michigan s Response to CMS Solicitation State Demonstrations to Integrate Care for Dual Eligible Individuals Solicitation Number: RFP-CMS-2011-0009 Department of Health and Human Services Centers for Medicare
Putting the Pieces Together: Medicaid Redesign and Long Term Care
 Putting the Pieces Together: Medicaid Redesign and Long Term Care Mark Kissinger, Director Division of Long Term Care Office of Health Insurance Programs New York State Department of Health NYAIL September
Putting the Pieces Together: Medicaid Redesign and Long Term Care Mark Kissinger, Director Division of Long Term Care Office of Health Insurance Programs New York State Department of Health NYAIL September
Legislative Report TRANSFORMATION AND REORGANIZATION OF NORTH CAROLINA MEDICAID AND NC HEALTH CHOICE PROGRAMS SESSION LAW
 Legislative Report TRANSFORMATION AND REORGANIZATION OF NORTH CAROLINA MEDICAID AND NC HEALTH CHOICE PROGRAMS SESSION LAW 2016-121 State of North Carolina Department of Health and Human Services Division
Legislative Report TRANSFORMATION AND REORGANIZATION OF NORTH CAROLINA MEDICAID AND NC HEALTH CHOICE PROGRAMS SESSION LAW 2016-121 State of North Carolina Department of Health and Human Services Division
Summary of California s Dual Eligible Demonstration Memorandum of Understanding
 April 2013 Summary of California s Dual Eligible Demonstration Memorandum of Understanding The Nation s Largest, Most Aggressive Plan for Integration On March 27, 2013, the Centers for Medicare and Medicaid
April 2013 Summary of California s Dual Eligible Demonstration Memorandum of Understanding The Nation s Largest, Most Aggressive Plan for Integration On March 27, 2013, the Centers for Medicare and Medicaid
State advocacy roadmap: Medicaid access monitoring review plans
 State advocacy roadmap: Medicaid access monitoring review plans Background Federal Medicaid law requires states to ensure Medicaid beneficiaries are able to access the healthcare providers they need through
State advocacy roadmap: Medicaid access monitoring review plans Background Federal Medicaid law requires states to ensure Medicaid beneficiaries are able to access the healthcare providers they need through
Rate methodology basics
 Outpatient Rates in Medical Assistance 2017 Policy Conference Julie Marquardt Director, Purchasing and Service Delivery 11/14/2017 Minnesota Department of Human Services mn.gov/dhs Rate methodology basics
Outpatient Rates in Medical Assistance 2017 Policy Conference Julie Marquardt Director, Purchasing and Service Delivery 11/14/2017 Minnesota Department of Human Services mn.gov/dhs Rate methodology basics
Volume 24, No. 07 July 2014
 State of New Jersey Department of Human Services Division of Medical Assistance & Health Services Volume 24, No. 07 July 2014 TO: SUBJECT: All Providers For Action For Managed Care Organizations For Information
State of New Jersey Department of Human Services Division of Medical Assistance & Health Services Volume 24, No. 07 July 2014 TO: SUBJECT: All Providers For Action For Managed Care Organizations For Information
Standardizing LTSS Assessments for State Initiatives
 Standardizing LTSS Assessments for State Initiatives Barbara Gage, Ph.D. Elizabeth Blair G. Lawrence Atkins, Ph.D. April 30, 2014 Supported by a grant from The SCAN Foundation advancing a coordinated and
Standardizing LTSS Assessments for State Initiatives Barbara Gage, Ph.D. Elizabeth Blair G. Lawrence Atkins, Ph.D. April 30, 2014 Supported by a grant from The SCAN Foundation advancing a coordinated and
Home and Community-Based Waivers: Opportunities for Community Living for ABI Survivors
 Home and Community-Based Waivers: Opportunities for Community Living for ABI Survivors BIA-MA Brain Injury Conference March 30, 2017 Amy Bernstein Director, Community Based Waivers MassHealth Dorothée
Home and Community-Based Waivers: Opportunities for Community Living for ABI Survivors BIA-MA Brain Injury Conference March 30, 2017 Amy Bernstein Director, Community Based Waivers MassHealth Dorothée
Promising Practices for Diversion and Transition of Persons with Mental Illness Through the PASRR Processes
 Promising Practices for Diversion and Transition of Persons with Mental Illness Through the PASRR Processes Dee O Connor, PhD Jennifer Ingle, MS, CRC Kimberly Wamback, BA University of Massachusetts Medical
Promising Practices for Diversion and Transition of Persons with Mental Illness Through the PASRR Processes Dee O Connor, PhD Jennifer Ingle, MS, CRC Kimberly Wamback, BA University of Massachusetts Medical
Resource Management Policy and Procedure Guidelines for Disability Waivers
 Resource Management Policy and Procedure Guidelines for Disability Waivers Disability waivers Brain Injury (BI) Community Alternative Care (CAC) Community Alternatives for Disabled Individuals (CADI) Developmental
Resource Management Policy and Procedure Guidelines for Disability Waivers Disability waivers Brain Injury (BI) Community Alternative Care (CAC) Community Alternatives for Disabled Individuals (CADI) Developmental
Medicaid 101: The Basics for Homeless Advocates
 Medicaid 101: The Basics for Homeless Advocates July 29, 2014 The Source for Housing Solutions Peggy Bailey CSH Senior Policy Advisor Getting Started Things to Remember: Medicaid Agency 1. Medicaid is
Medicaid 101: The Basics for Homeless Advocates July 29, 2014 The Source for Housing Solutions Peggy Bailey CSH Senior Policy Advisor Getting Started Things to Remember: Medicaid Agency 1. Medicaid is
Colorado Choice Health Plans
 Quality Overview Health Plans Accreditation Exchange Product Accrediting Organization: Accreditation Status: URAC Health Plan Accreditation (Marketplace ) Full Full: Organization demonstrates full compliance
Quality Overview Health Plans Accreditation Exchange Product Accrediting Organization: Accreditation Status: URAC Health Plan Accreditation (Marketplace ) Full Full: Organization demonstrates full compliance
Charting New Territory: Ombudsman Programs and Dual Demonstrations Gabriela Trujillo Williams, Administration for Community Living Francine
 Charting New Territory: Ombudsman Programs and Dual Demonstrations Gabriela Trujillo Williams, Administration for Community Living Francine Chuchanis, Direction Home Akron Canton Area Agency on Aging &
Charting New Territory: Ombudsman Programs and Dual Demonstrations Gabriela Trujillo Williams, Administration for Community Living Francine Chuchanis, Direction Home Akron Canton Area Agency on Aging &
Special Needs BasicCare
 Minnesota Disability Health Options (MnDHO) Special Needs BasicCare (SNBC) Special Needs Purchasing Deb Maruska Program Coordinator Susan Kennedy Project Coordinator Managed Care Programs for People with
Minnesota Disability Health Options (MnDHO) Special Needs BasicCare (SNBC) Special Needs Purchasing Deb Maruska Program Coordinator Susan Kennedy Project Coordinator Managed Care Programs for People with
All related UCare forms can be found, HERE, all DHS forms can be found HERE, all DHS Bulletins can be found HERE.
 Minnesota Senior Health Options (MSHO) Care Coordination (CC) and Minnesota Senior Care Plus (MSC+) Community Case Management (CM) Requirements Updated 1.1.18 All Minnesota Senior Health Options (MSHO)
Minnesota Senior Health Options (MSHO) Care Coordination (CC) and Minnesota Senior Care Plus (MSC+) Community Case Management (CM) Requirements Updated 1.1.18 All Minnesota Senior Health Options (MSHO)
CRSP PACE SOCIAL WORKER SAMPLE JOB DESCRIPTIONS
 SAMPLE JOB DESCRIPTIONS SOCIAL WORKER R 801 North Fairfax Street Suite 309 Alexandria, Virginia 22314 Phone: 703-535-1565 Fax: 703-535-1566 www.npaonline.org SAMPLE A 11/02 Job Code: I. IDENTIFICATION
SAMPLE JOB DESCRIPTIONS SOCIAL WORKER R 801 North Fairfax Street Suite 309 Alexandria, Virginia 22314 Phone: 703-535-1565 Fax: 703-535-1566 www.npaonline.org SAMPLE A 11/02 Job Code: I. IDENTIFICATION
Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States
: Reform Strategies for States") Advancing innovations in health care delivery for low-income Americans Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States March 6, 2018 Michelle Herman Soper and Alexandra
Advancing innovations in health care delivery for low-income Americans Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States March 6, 2018 Michelle Herman Soper and Alexandra
Medicare Medicaid Alignment Initiative (MMAI) November 14, 2014
 November 14, 2014") Medicare Medicaid Alignment Initiative (MMAI) November 14, 2014 MMW work is supported by grants from: The Chicago Community Trust Michael Reese Health Trust The Retirement Research Foundation Who We Are:
Medicare Medicaid Alignment Initiative (MMAI) November 14, 2014 MMW work is supported by grants from: The Chicago Community Trust Michael Reese Health Trust The Retirement Research Foundation Who We Are:
COMMCARE and Independence Waiver Renewals Aging, Attendant Care and OBRA Waiver Amendments Side-by-Side Comparison of Current and Revised Language
 Appendix and Waiver Section Current Language Revised Language Waiver Affected Commenter Name, Date Submitted and Comment Appendix A: Waiver Administration and Operation Appendix A-2-a. Medicaid Director
Appendix and Waiver Section Current Language Revised Language Waiver Affected Commenter Name, Date Submitted and Comment Appendix A: Waiver Administration and Operation Appendix A-2-a. Medicaid Director
Subtitle E New Options for States to Provide Long-Term Services and Supports
 LONG TERM CARE (SECTION-BY-SECTION ANALYSIS) (Information compiled from the Democratic Policy Committee (DPC) Report on The Patient Protection and Affordable Care Act and the Health Care and Education
LONG TERM CARE (SECTION-BY-SECTION ANALYSIS) (Information compiled from the Democratic Policy Committee (DPC) Report on The Patient Protection and Affordable Care Act and the Health Care and Education
National Council on Disability
 An independent federal agency making recommendations to the President and Congress to enhance the quality of life for all Americans with disabilities and their families. Analysis and Recommendations for
An independent federal agency making recommendations to the President and Congress to enhance the quality of life for all Americans with disabilities and their families. Analysis and Recommendations for
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
REPORT OF THE BOARD OF TRUSTEES
 REPORT OF THE BOARD OF TRUSTEES B of T Report 21-A-17 Subject: Presented by: Risk Adjustment Refinement in Accountable Care Organization (ACO) Settings and Medicare Shared Savings Programs (MSSP) Patrice
REPORT OF THE BOARD OF TRUSTEES B of T Report 21-A-17 Subject: Presented by: Risk Adjustment Refinement in Accountable Care Organization (ACO) Settings and Medicare Shared Savings Programs (MSSP) Patrice
VIRGINIA S MEDICARE AND MEDICAID INTEGRATION EXPERIENCE 12/2/2016
 VIRGINIA S MEDICARE AND MEDICAID INTEGRATION EXPERIENCE The Honorable Dr. William Hazel Secretary of Health and Human Resources Commonwealth of Virginia Why Is It Important to Integrate Medicare and Medicaid
VIRGINIA S MEDICARE AND MEDICAID INTEGRATION EXPERIENCE The Honorable Dr. William Hazel Secretary of Health and Human Resources Commonwealth of Virginia Why Is It Important to Integrate Medicare and Medicaid
Managed Long Term Services and Supports (MLTSS) A Forum for Consumers, their Families and Caregivers, Advocates and Community-Based Agencies
 A Forum for Consumers, their Families and Caregivers, Advocates and Community-Based Agencies") Managed Long Term Services and Supports (MLTSS) A Forum for Consumers, their Families and Caregivers, Advocates and Community-Based Agencies 1 Background To give you an update on the implementation of
Managed Long Term Services and Supports (MLTSS) A Forum for Consumers, their Families and Caregivers, Advocates and Community-Based Agencies 1 Background To give you an update on the implementation of
SUPPORTING CONSUMERS WHO TRANSITION OUT OF NURSING HOMES
 SUPPORTING CONSUMERS WHO TRANSITION OUT OF NURSING HOMES What Consumers Say Long-Term Care Ombudsmen: Supporting the Consumer Local LTCO Experience Supporting Consumers Monday, July 14, 2014 WHAT CONSUMERS
SUPPORTING CONSUMERS WHO TRANSITION OUT OF NURSING HOMES What Consumers Say Long-Term Care Ombudsmen: Supporting the Consumer Local LTCO Experience Supporting Consumers Monday, July 14, 2014 WHAT CONSUMERS
Member Services Director
 Central Coast Alliance for Health September 2006 Duty Statement page 1 Member Services Director 1. Responsible for senior management and strategic planning for the Member Services Department, including
Central Coast Alliance for Health September 2006 Duty Statement page 1 Member Services Director 1. Responsible for senior management and strategic planning for the Member Services Department, including
A GUIDE TO HOSPICE SERVICES
 A GUIDE TO HOSPICE SERVICES PURPOSE: Minnesota Rules 4664.0140, subpart 1 states: "Every individual applicant for a license, and every person who provides direct care, supervision of direct care, or management
A GUIDE TO HOSPICE SERVICES PURPOSE: Minnesota Rules 4664.0140, subpart 1 states: "Every individual applicant for a license, and every person who provides direct care, supervision of direct care, or management
Medicaid 101: The Basics
 Medicaid 101: The Basics April 9, 2018 Miranda Motter President and CEO Gretchen Blazer Thompson Director of Govt. Affairs Angela Weaver Director of Regulatory Affairs OAHP Overview Who We Are: The Ohio
Medicaid 101: The Basics April 9, 2018 Miranda Motter President and CEO Gretchen Blazer Thompson Director of Govt. Affairs Angela Weaver Director of Regulatory Affairs OAHP Overview Who We Are: The Ohio
Medicaid Reform: The Opportunities for Home and Community Based Providers. All Rights Reserved
 Medicaid Reform: The Opportunities for Home and Community Based Providers ILS Background & Experience Care Management Company founded in 2001 Focuses on Duals, Medicaid ABD and Managing Medicaid Long term
Medicaid Reform: The Opportunities for Home and Community Based Providers ILS Background & Experience Care Management Company founded in 2001 Focuses on Duals, Medicaid ABD and Managing Medicaid Long term
Program of All-inclusive Care for the Elderly (PACE) Summary and Recommendations
 Summary and Recommendations") Program of All-inclusive Care for the Elderly (PACE) PACE Policy Summit Summary and Recommendations PACE Policy Summit On December 6, 2010, the National PACE Association (NPA) convened a policy summit
Program of All-inclusive Care for the Elderly (PACE) PACE Policy Summit Summary and Recommendations PACE Policy Summit On December 6, 2010, the National PACE Association (NPA) convened a policy summit