National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network. Monday, September 12, 2011
|
|
|
- Aubrie Williams
- 6 years ago
- Views:
Transcription

1 National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM 5:15 PM
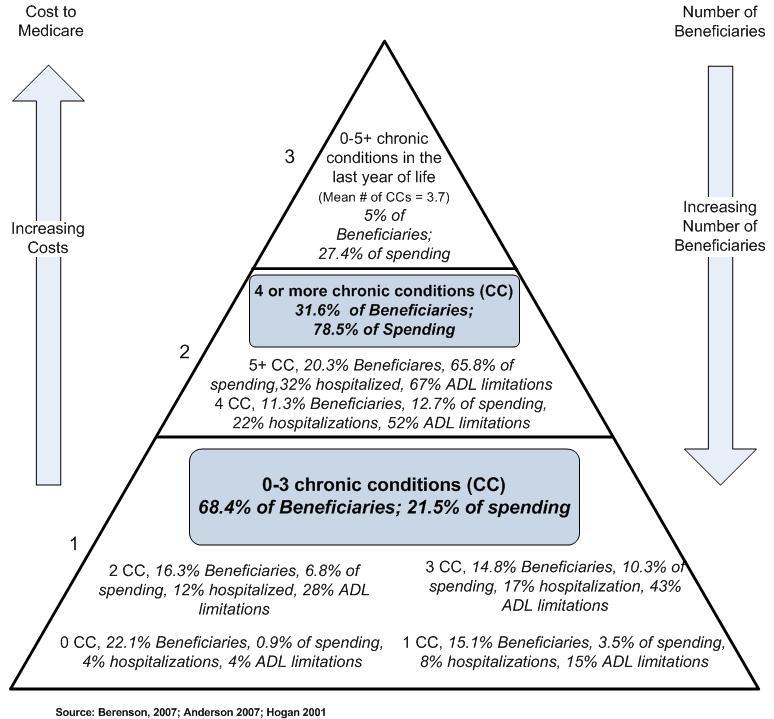
2 Growth in Population of Older Americans & Increase in Chronic Disease The population of older adults is rapidly increasing: By 2030, the number of Americans over 65 is expected to reach 72 million, double the 65+ population of 2003 Older adults are at high risk for chronic conditions including cardiovascular disease, diabetes, and cancer, that require ongoing medical management Chronic conditions result in high health care costs and reduced quality of life
3 Psychosocial Issues also Common A significant subset of older adults also face substantial psychosocial issues, including: Depression, limited mobility, and diminishing finances and/or cognitive skills These issues add to service needs, plus Complicate access to and effective utilization of health and medical services
4 Delivery System Problems Health care systems (public and private) need improvement, especially chronic care delivery Barriers to improvements in care for people with chronic conditions include: Fragmented care delivery, Poor transitions across settings, and Poorly aligned payment incentives that fail to recognize the value of better integration of services S Reinhard, PPI, AARP

5
6 Delivery System Problems Medicare is not perfect and needs improvement Care is not well coordinated, particularly for those with chronic conditions Fee-For-Service payments encourage over utilization of services S Reinhard, PPI, AARP
7 The Genesis of the National Coalition on Care Coordination (N3C) The American Society on Aging (ASA), and the New York Academy of Medicine (NYAM), Social Work Leadership Institute (SWLI) convened a distinguished group of thirty experts from health, human services and long-term care prior to the 2008 ASA Annual Conference on Aging to address key issues in care coordination. The meeting resulted in the formal establishment of the National Coalition on Care Coordination (N3C). Today consists of 40 members
8 2011 N3C Membership Steering Committee: American Geriatrics Society National Council on Aging (NCOA) American Society on Aging National PACE Association Consumer Coalition for Quality Health Care New York Academy of Medicine Matz, Blancato & Associates Partners in Care Foundation Medicare Chronic Care Practice Research Network (MCCPRN) Members: American Association of Retired People Long Term Care Educational Foundation, Area Agency on Aging (Mid-Columbia) George Mason University American College of Physicians National Academy of Certified Care Managers American Medical Association National Alliance for Caregiving Benjamin Rose Institute National Association of Professional Geriatric Care Managers Case Management Society of America National Association of Area Agencies on Aging (n4a) Center for Health Care Strategies National Association of States United for Aging Center for Medicare Advocacy, Inc. and Disabilities (NASUAD) Connecticut Community Care, Inc. National Transitions of Care Coalition COPE Health Care Strategies Paraprofessional Healthcare Institute (PHI) Family Caregiver Alliance Rush University Medical Center Gerontological Society of America SCAN Health Plan Hudson Health Plan SeniorBridge Health and Medicine Policy Research Group Society of Hospital Medicine Illinois Coalition on Aging University of Illinois College of Nursing LeadingAge (formerly American Association of University of Pennsylvania School of Nursing Homes and Services for the Aging) Urban Institute
9 N3C Accomplishments Over its history has convened major sessions at the 2009, 2010 and 2011 American Society on Aging conferences Convened additional meetings with stakeholders in Washington D.C. Commissioned papers discussing current models of care coordination Maintained a visible presence working with relevant individuals in Congress and the Administration in the following areas:
10 N3C Accomplishments cont d During development of language in the Affordable Care Act Implementation of the ACA including filing comments on proposed rules including and meetings with offices such as CMMI Meeting with Administration officials and appropriate Congressional staff on the upcoming reauthorization of the OAA
11 N3C Mission and Goals Improve the quality of life for vulnerable older adults by promoting care coordination as an essential part of health care reform. Convene experts from health, long term care, aging and public policy to develop consensus on effective models of care coordination and build evidence for the effectiveness of care coordination. Understand how expertise of coalition members can be most effectively utilized. Identify opportunities to work with coalition members as allies, thought partners, and policy advocates.
12 N3C Mission and Goals, cont d Develop evidence based specifics about Care Coordination, its benefits, and personnel qualifications. Educate federal and state policy makers on care coordination. Provide interested parties with specifics about the role and benefits of care coordination as part of health care reform.
13 N3C Definition of Care Coordination Care coordination is a person and family-centered, assessment-based, interdisciplinary approach to integrating health care and social support services in a cost-effective manner in which an individual s needs and preferences are assessed, a comprehensive care plan is developed, and services are managed and monitored by an evidence-based process which typically involves a designated lead care coordinator.

14 N3C research/ SWLI review of current programs The majority of programs described in the literature originate in the health care system: Created and implemented either by an insurer or a health provider system Programs implemented by community based organizations appear to be under-represented in the literature We know there are a lot of them; they are not being evaluated and reported on as frequently as medicalbased programs
15 Population Served Programs included serve a diverse population of older adults with respect to: Physical health Mental health and cognitive function Available social support Location (e.g. rural/urban)
16 Setting for Service Delivery Includes:* Clinics Home Adult Day Centers Senior Centers VA Medical Centers Phone * SWLI review focused on community and home-based programs. Hospital-based and residential care programs were excluded by search criteria
17 Program Staffing Commonly nurse lead, with an interdisciplinary team that may include MDs, pharmacist, OT/PT, dietician, social worker community liaison, psychiatrist, psychologist Care manager often works in conjunction with or maintains communication with primary care provider
18 Program Services Baseline and ongoing assessment* Development of individualized care plan* Care management* Communication with PCP* Referrals to medical and supportive services* Medication management Health education Mental health services Communication/advocacy with health care provider Discharge planning Caregiver support * Most commonly included in reviewed programs
19 Care Coordination Program Objectives Improved service utilization Increased use of social and community supportive services and outpatient services Less ER use Fewer and shorter hospital and nursing home stays Improved (or sustained) health, functioning, mental health, and quality of life for care recipients Reduced caregiver burden Improved knowledge and behaviors, including chronic disease self management Reduced health care costs Satisfaction with services
20 Program Outcomes Outcomes measured vary widely between articles Most common positive outcomes include improved service utilization, functioning, mental health, quality of life, satisfaction with services, and reduced caregiver burden Among articles reporting cost outcomes, program costs may be offset by reductions in the cost of institutional services
21 Effective Practices Analysis is ongoing and difficult due to variability in program structure, services, and outcomes measured Preliminary findings regarding effective practices include Program targeting to identify the population who can most benefit from a given intervention Baseline and ongoing assessment of health and social needs Interdisciplinary approach to allow providers to address a spectrum of health and social service needs Enhanced communication among providers, frequently including the primary care physician Flexible provision of services and service intensity Connection to existing community health and supportive services
22 Effective Practices (continued) Although less frequently reported on, literature also highlights the importance of: Shared electronic health record Evidence-based protocols to assess health and social condition and develop care plan Technology-assisted, in-home monitoring (by telephone or remote health monitoring systems) to enhance communication between community-dwelling older adults and providers, especially in rural areas
23 Promising models include: Geriatric Resources for Assessment and Care of Elders (GRACE) After Discharge Care Management of Low Income Frail Elderly (AD-LIFE) Both models improve the quality of care for low income seniors by the longitudinal integration of geriatric and primary care services across the continuity of care Integration with affiliated pharmacy, mental health, hospital, home health, and community-based services
24 Where N3C Advocacy for Care Coordination and Support for New and Existing Models of Care Has Succeeded Advocated Care Coordination as central focus of provisions in PPACA targeting older adults o Center for Medicare Innovation o Support for new and existing models of care coordination (PCMH, Independence at Home and others) Focused on evidence in support of care coordination o Center for Medicare and Medicaid Innovation focus on best practices and evidence-based measures Focused attention on the challenges for the reimbursement mechanisms that support care coordination o Bundled payments and value based purchasing (Medicare Accountable Care Organizations and shared savings)
25 Where N3C Succeeded, Cont d Focused on vulnerable populations and integration of health and long term care o Care coordination models for dual eligibles focus on integration of health and long term care Long-term care measures o Class Independence Benefit Plan o Continued support for Aging and Disability Resource Centers Support for home and community based services o Community based health teams in Patient Centered Medical Homes (PCMH), Community-Based Care Transitions Program, ADRC Support

26 Federal Initiatives to Support State/Community-Based Approaches to Coordinated Care
27 The Aging Network _Structure_Program.pdf

28 Wagner s Chronic Illness Model Change that Works Self- Management Support Health System Organization of Health Care Decision Delivery Support System Design Clinical Information Systems Informed, Activated Patient Productive Interaction s Prepared, Proactive Practice Team Improved Functional and Clinical Outcomes
29 Overview Alignment through implementation of the Affordable Care Act Strategic Framework on Multiple Chronic Conditions National Quality Strategy Federal HIT Strategic Plan Partnership for Patients Themes recurring across multiple initiatives: Importance of care coordination Focus on care transitions Role of community-based services Focus on the patient and family caregivers Triple Aim: Better care, better health, lower cost J Howell, ONC
30 National Quality Strategy Aims Better Care: Improve quality, by making health care more patient-centered, reliable, accessible, and safe Healthy People and Communities: Improve health of population Affordable Care: Reduce cost of quality health care Six Priorities and Goals to help focus public and private efforts: Safer Care: eliminate preventable health care-acquired conditions Effective Care Coordination Person- and Family-Centered Care Prevention and Treatment of Leading Causes of Mortality: prevent and reduce harm caused by cardiovascular disease Support Better Health in Communities Make Care More Affordable National Quality Strategy
31 Partnership for Patients Public-Private Partnership to make care safer, potentially save up to $50 billion Two Goals of the Partnership: Keep hospital patients from getting injured or sicker: decrease preventable hospital-acquired conditions 40% by 2013 cf Up to $500M from CMS Innovation Center Help patients heal without complication: decrease preventable complications during transition from one care setting to another so that hospital readmissions will be reduced 20% by 2013 cf Up to $500M available through Community-Based Care Transitions Program authorized by Section 3026 of ACA J Howell, ONC
32 Partnership for Patients: Community- Based Care Transitions Program 5 years beginning April 12, 2011; rolling application process Program Goals: Improve the quality of care transitions Reduce readmissions for high-risk Medicare beneficiaries Document measureable savings to the Medicare program by reducing unnecessary readmissions Creates source of funding for effectively managing transitions from acute to community-based settings Eligible entities paid on per-discharge basis for Medicare benes at high risk of readmission, including those with multiple chronic conditions, depression, or cognitive impairment. J Howell, ONC

33 Community-Based Care Transitions Program: Selection Criteria Preference given to Administration on Aging grantees that Provide care transition interventions in conjunction with multiple hospitals and practitioners Provide services to medically-underserved populations, small communities, and rural areas Applicants must Identify root causes of readmissions and define target population and strategies for identifying high-risk patients Specify transition interventions, including improving provider communications and patient activation Indicate how community and social supports and resources will be incorporated to enhance beneficiary post-hospitalization management outcomes J Howell, ONC
34 State Demonstrations to Integrate Care for Dual Eligible Individuals Partnership between Federal Office of Integrated Care and the Innovation Center Testing delivery system and payment reform that improves the quality, coordination, and cost-effectiveness of care for dual eligible individuals. On April 14, 2011, 15 states awarded contracts for up to $1million to design new models for serving dual eligibles: West: California, Colorado, Oregon, Washington Midwest: Oklahoma, Michigan, Minnesota, Wisconsin South: North Carolina, South Carolina, Tennessee East : Connecticut, New York, Massachusetts, Vermont Models will be person-centered and fully coordinate primary, acute, behavioral and long-term supports and services. J Howell, ONC
35 CLASS ACT CLASS ACT and care coordination: Based on the model in the Federal Long Term Care Insurance, N3C will work to have care coordination as a benefit in the LTSS package.
36 Bundled Payment Described as the health care reimbursement middle ground between fee-for-service and a capitated payment system. CMS introduced the Bundled Payment for Care Improvement initiative and is seeking applications for different models of bundled care Participants in models would set a target for reimbursement, test new models of care, receive payment for services under the traditional fee-forservice system, and at the conclusion of an episode share in the savings compared to the target price. Letters of intent due Sept. 22
37 CARE COORDINATION AND THE OLDER AMERICANS ACT N3C has recognized the reauthorization of the Older Americans Act is an ideal opportunity to strengthen links between health and long term care and the medical and social models of care. The OAA, through the Aging Network, is a pioneer in development of coordinated services for older adults. Through State Units on Aging, Area Agencies on Aging, service providers, and Aging and Disability Resource Centers

38 Care Coordination and the OAA Reauthorization In anticipation of reauthorization, N3C submitted a paper to Administration on Aging proposing changes to OAA to strengthen care coordination: N3C s recommendations are based on the principle that care coordination must: be assessment driven, include a comprehensive care plan, require ongoing evaluation, and utilize a qualified care coordinator
39 Care Coordination and the OAA Definition: The OAA should include care coordination within its definitions of its programs and services. In particular ADRC s. Integration: The OAA should encourage SUA s and AAA s to integrate care coordination into their plans. The care coordinator should be widely accessible The care plan should be client centered
40 Care Coordination and the OAA Administration: The Assistant Secretary should work with the Administrator of CMS to coordinate efforts and develop ways to ensure that older adults with multiple chronic illnesses receive coordinated care. This can include sharing best practices and disseminating information to the network and health care providers. AOA should ensure a standardized process that the aging network uses to build and Improve linkage between social and medical/health services.
41 Care Coordination and the OAA Title III: Support improved outreach by area agencies with health and medical care entities around care coordination Title IV: N3C supports testing of care coordination models under Title IV subject to funding as well as develop appropriate training curriculums.
42 OAA Reauthorization U.S. Senate Subcommittee on Primary Health and Aging in the Health, Education, Labor and Pensions committee held listening sessions on the Older Americans Act Brian Lindberg presented N3C s care coordination recommendations on August 23 Status of OAA reauthorization remains unclear.
43 Further Information Websites: General Innovation Center SWLI/N3C For Questions:
National Coalition on Care Coordination (N3C)
") National Coalition on Care Coordination (N3C) Origin: partnership between the New York Academy of Medicine and the American Society on Aging Outgrowth of a stakeholder conference in March 2008 Members
National Coalition on Care Coordination (N3C) Origin: partnership between the New York Academy of Medicine and the American Society on Aging Outgrowth of a stakeholder conference in March 2008 Members
Strengthening Services for Older Adults through Changes to the Older Americans Act
 Strengthening Services for Older Adults through Changes to the Older Americans Act RECOMMENDATIONS FOR THE REAUTHORIZATION OF OAA 2011 A REPORT FOR THE ADMINISTRATION ON AGING (AoA) Prepared by The Social
Strengthening Services for Older Adults through Changes to the Older Americans Act RECOMMENDATIONS FOR THE REAUTHORIZATION OF OAA 2011 A REPORT FOR THE ADMINISTRATION ON AGING (AoA) Prepared by The Social
Program of All-inclusive Care for the Elderly (PACE) Summary and Recommendations
 Summary and Recommendations") Program of All-inclusive Care for the Elderly (PACE) PACE Policy Summit Summary and Recommendations PACE Policy Summit On December 6, 2010, the National PACE Association (NPA) convened a policy summit
Program of All-inclusive Care for the Elderly (PACE) PACE Policy Summit Summary and Recommendations PACE Policy Summit On December 6, 2010, the National PACE Association (NPA) convened a policy summit
Healthcare Service Delivery and Purchasing Reform in Connecticut
 Healthcare Service Delivery and Purchasing Reform in Connecticut Presentation to National Association of Medicaid Directors November 9, 2011 Mark Schaefer Director, Medical Care Administration Health Purchasing
Healthcare Service Delivery and Purchasing Reform in Connecticut Presentation to National Association of Medicaid Directors November 9, 2011 Mark Schaefer Director, Medical Care Administration Health Purchasing
Medicare: 2018 Model of Care Training
 Medicare: 2018 Model of Care Training Training Objectives This course will describe how Centene and its contracted providers work together to successfully deliver the duals Model of Care (MOC) program.
Medicare: 2018 Model of Care Training Training Objectives This course will describe how Centene and its contracted providers work together to successfully deliver the duals Model of Care (MOC) program.
Special Needs Plan Model of Care Chinese Community Health Plan
 Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Report from the National Quality Forum: National Priorities Partnership Quarterly Synthesis of Action In Support of the Partnership for Patients
 Report from the National Quality Forum: National Priorities Partnership Quarterly Synthesis of Action In Support of the Partnership for Patients November 30, 2012 Quarterly Update at a Glance Since the
Report from the National Quality Forum: National Priorities Partnership Quarterly Synthesis of Action In Support of the Partnership for Patients November 30, 2012 Quarterly Update at a Glance Since the
Improving the Continuum of Care: Progress on Selected Provisions of the Affordable Care Act One Year Post-Passage
 Improving the Continuum of Care: Progress on Selected Provisions of the Affordable Care Act One Year Post-Passage March 23, 2011 marks the oneyear anniversary of the signing of the Patient Protection and
Improving the Continuum of Care: Progress on Selected Provisions of the Affordable Care Act One Year Post-Passage March 23, 2011 marks the oneyear anniversary of the signing of the Patient Protection and
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Going The Distance To Improve The Care Span: The Duel Over The Dual Eligibles And The Implications For Health Reform
 + Going The Distance To Improve The Care Span: The Duel Over The Dual Eligibles And The Implications For Health Reform By Susan Dentzer Editor in Chief, Health Affairs Presentation to the First National
+ Going The Distance To Improve The Care Span: The Duel Over The Dual Eligibles And The Implications For Health Reform By Susan Dentzer Editor in Chief, Health Affairs Presentation to the First National
Molina Medicare Model of Care
 Molina Medicare Model of Care Provider Network Molina Healthcare 2018 1 Molina s Mission and Vision Our Vision: We envision a future where everyone receives quality health care Our Mission: To provide
Molina Medicare Model of Care Provider Network Molina Healthcare 2018 1 Molina s Mission and Vision Our Vision: We envision a future where everyone receives quality health care Our Mission: To provide
ACCESS TO MENTAL HEALTH CARE IN RURAL AMERICA: A CRISIS IN THE MAKING FOR SENIORS AND PEOPLE WITH DISABILITIES
 ACCESS TO MENTAL HEALTH CARE IN RURAL AMERICA: A CRISIS IN THE MAKING FOR SENIORS AND PEOPLE WITH DISABILITIES A Capitol Hill Briefing Sponsored by the: AMERICAN MENTAL HEALTH COUNSELORS ASSOCIATION (AMHCA)
ACCESS TO MENTAL HEALTH CARE IN RURAL AMERICA: A CRISIS IN THE MAKING FOR SENIORS AND PEOPLE WITH DISABILITIES A Capitol Hill Briefing Sponsored by the: AMERICAN MENTAL HEALTH COUNSELORS ASSOCIATION (AMHCA)
Care Integration and Network Models: How to Become a Player
 Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
The Medical Home Model: What Is It And How Do Social Workers Fit In?
 I S S U E 10 A P R I L 2 0 1 1 PracticePerspectives The National Association of Social Workers 750 First Street NE Suite 700 Stacy Collins, MSW Senior Practice Associate scollins@naswdc.org Washington,
I S S U E 10 A P R I L 2 0 1 1 PracticePerspectives The National Association of Social Workers 750 First Street NE Suite 700 Stacy Collins, MSW Senior Practice Associate scollins@naswdc.org Washington,
Medicare: 2017 Model of Care Training 4/13/2017
 Medicare: 2017 Model of Care Training Training Objectives This course will describe how MHS Health Wisconsin Medicare Advantage and its contracted providers work together to successfully deliver the Model
Medicare: 2017 Model of Care Training Training Objectives This course will describe how MHS Health Wisconsin Medicare Advantage and its contracted providers work together to successfully deliver the Model
Measure Applications Partnership (MAP)
") Measure Applications Partnership (MAP) Uniform Data System for Medical Rehabilitation Annual Conference Aisha Pittman, MPH Senior Program Director National Quality Forum August 9, 2012 Overview MAP Background
Measure Applications Partnership (MAP) Uniform Data System for Medical Rehabilitation Annual Conference Aisha Pittman, MPH Senior Program Director National Quality Forum August 9, 2012 Overview MAP Background
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum. May 2015 avalere.com
 Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Accountable Care in Infusion Nursing. Hudson Health Plan. Mission Statement. for all people. INS National Academy of Infusion Therapy
 Accountable Care in Infusion Nursing INS National Academy of Infusion Therapy November 14 16, 2014 Atlanta, GA Margaret (Peggy) Leonard, MS, RN-BC, FNP Senior Vice President Clinical Services Hudson Health
Accountable Care in Infusion Nursing INS National Academy of Infusion Therapy November 14 16, 2014 Atlanta, GA Margaret (Peggy) Leonard, MS, RN-BC, FNP Senior Vice President Clinical Services Hudson Health
Coordinated Care: Key to Successful Outcomes
 Coordinated Care: Key to Successful Outcomes Best practices in care coordination improve health, lower costs and increase patient satisfaction 402 Lippincott Drive Marlton, NJ 08053 856.782.3300 www.continuumhealth.net
Coordinated Care: Key to Successful Outcomes Best practices in care coordination improve health, lower costs and increase patient satisfaction 402 Lippincott Drive Marlton, NJ 08053 856.782.3300 www.continuumhealth.net
The benefits of the Affordable Care Act for persons with Developmental Disabilities
 Tuesday, 2:30 2:00, B5 The benefits of the Affordable Care Act for persons with Developmental Disabilities Objectives: Notes: Audrey E. Smith, MPH 33-402-9608 Asmith2@waynecounty.com. Identify effective
Tuesday, 2:30 2:00, B5 The benefits of the Affordable Care Act for persons with Developmental Disabilities Objectives: Notes: Audrey E. Smith, MPH 33-402-9608 Asmith2@waynecounty.com. Identify effective
dual-eligible reform a step toward population health management
 FEATURE STORY REPRINT APRIL 2013 Bill Eggbeer Krista Bowers Dudley Morris healthcare financial management association hfma.org dual-eligible reform a step toward population health management By improving
FEATURE STORY REPRINT APRIL 2013 Bill Eggbeer Krista Bowers Dudley Morris healthcare financial management association hfma.org dual-eligible reform a step toward population health management By improving
Community Health Workers: Supporting Diabetes Prevention in Michigan
 Community Health Workers: Supporting Diabetes Prevention in Michigan MICHIGAN DIABETES PREVENTION NETWORK Katie Mitchell, LMSW Project Director, MiCHWA March 31, 2016 Okemos, Michigan MiCHWA is supported
Community Health Workers: Supporting Diabetes Prevention in Michigan MICHIGAN DIABETES PREVENTION NETWORK Katie Mitchell, LMSW Project Director, MiCHWA March 31, 2016 Okemos, Michigan MiCHWA is supported
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015
 MODEL OF CARE TRAINING 2015") SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill
 Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Options for Integrating Care for Dual Eligible Beneficiaries
 CHCS Center for Health Care Strategies, Inc. Technical Assistance Brief Options for Integrating Care for Dual Eligible Beneficiaries By Melanie Bella and Lindsay Palmer-Barnette, Center for Health Care
CHCS Center for Health Care Strategies, Inc. Technical Assistance Brief Options for Integrating Care for Dual Eligible Beneficiaries By Melanie Bella and Lindsay Palmer-Barnette, Center for Health Care
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
The Patient Protection and Affordable Care Act (Public Law )
") Policy Brief No. 2 March 2010 A Summary of the Patient Protection and Affordable Care Act (P.L. 111-148) and Modifications by the On March 23, 2010, President Obama signed into law the Patient Protection
Policy Brief No. 2 March 2010 A Summary of the Patient Protection and Affordable Care Act (P.L. 111-148) and Modifications by the On March 23, 2010, President Obama signed into law the Patient Protection
Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States
: Reform Strategies for States") Advancing innovations in health care delivery for low-income Americans Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States March 6, 2018 Michelle Herman Soper and Alexandra
Advancing innovations in health care delivery for low-income Americans Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States March 6, 2018 Michelle Herman Soper and Alexandra
OneCare Model of Care
 OneCare Model of Care Note: Content of this course was current at the time it was published. As Medicare policy changes frequently, check with your immediate supervisor regarding recent updates. 2018 Learning
OneCare Model of Care Note: Content of this course was current at the time it was published. As Medicare policy changes frequently, check with your immediate supervisor regarding recent updates. 2018 Learning
Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees
 TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
Forces of Change- Seeing Stepping Stones Not Potholes
 May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
States Roles in Rebalancing Long-Term Care: Findings from the Aging Strategic Alignment Project
 States Roles in Rebalancing Long-Term Care: Findings from the Aging Strategic Alignment Project Linda S. Noelker, PhD Katz Policy Institute Benjamin Rose Institute on Aging 11900 Fairhill Road, Suite 300
States Roles in Rebalancing Long-Term Care: Findings from the Aging Strategic Alignment Project Linda S. Noelker, PhD Katz Policy Institute Benjamin Rose Institute on Aging 11900 Fairhill Road, Suite 300
Supporting MLTSS Consumers through Problem Resolution and Advocacy
 Supporting MLTSS Consumers through Problem Resolution and Advocacy James David Toews, Becky A. Kurtz, Eliza Bangit September 11, 2013 Risks of Managed Long-Term Services and Supports (MLTSS) Many managed
Supporting MLTSS Consumers through Problem Resolution and Advocacy James David Toews, Becky A. Kurtz, Eliza Bangit September 11, 2013 Risks of Managed Long-Term Services and Supports (MLTSS) Many managed
CareMore Special Needs Plans Model of Care. Annual Evaluation 2015 Performance
 CareMore Special Needs Plans Model of Care Annual Evaluation 2015 Performance The Special Needs Plans (SNPs) Medicare SNPs are a type of Medicare Advantage Plan (like an HMO or PPO). Medicare SNPs limit
CareMore Special Needs Plans Model of Care Annual Evaluation 2015 Performance The Special Needs Plans (SNPs) Medicare SNPs are a type of Medicare Advantage Plan (like an HMO or PPO). Medicare SNPs limit
Illinois Governor s Office of Health Innovation and Transformation
 1 Illinois Governor s Office of Health Innovation and Transformation Medicaid Managed Care Conference October 21, 2014 Michael Gelder, Senior Health Policy Advisor to Governor Pat Quinn Executive Director,
1 Illinois Governor s Office of Health Innovation and Transformation Medicaid Managed Care Conference October 21, 2014 Michael Gelder, Senior Health Policy Advisor to Governor Pat Quinn Executive Director,
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Best Practices. SNP Alliance. October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees
 SNP Alliance Best Practices October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees Commonwealth Care Alliance is a Massachusetts-based non-profit,
SNP Alliance Best Practices October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees Commonwealth Care Alliance is a Massachusetts-based non-profit,
Community Health Workers: ACA and Redesign Funding Opportunities
 Community Health Workers: ACA and Redesign Funding Opportunities What are the Goals of the Affordable Care Act and Redesign? Increased Coverage Better Population Health Higher Quality, More-Patient Centered
Community Health Workers: ACA and Redesign Funding Opportunities What are the Goals of the Affordable Care Act and Redesign? Increased Coverage Better Population Health Higher Quality, More-Patient Centered
Molina Medicare Model of Care. Healthcare Services Molina Healthcare 2016
 Molina Medicare Model of Care Healthcare Services Molina Healthcare 2016 MHTPS_MOCTRN_062016 1 Molina s Mission Our mission is to provide quality health services to financially vulnerable families and
Molina Medicare Model of Care Healthcare Services Molina Healthcare 2016 MHTPS_MOCTRN_062016 1 Molina s Mission Our mission is to provide quality health services to financially vulnerable families and
Jeffrey B. Klein, FACHE President & CEO
 Jeffrey B. Klein, FACHE President & CEO THE ROAD TO REVOLUTION How serious will the trajectory of demographic shifts and the effects of the health care delivery system change be on America s most vulnerable
Jeffrey B. Klein, FACHE President & CEO THE ROAD TO REVOLUTION How serious will the trajectory of demographic shifts and the effects of the health care delivery system change be on America s most vulnerable
From Fragmentation to Integration: Bringing Medical Care and HCBS Together. Jessica Briefer French Senior Research Scientist
 From Fragmentation to Integration: Bringing Medical Care and HCBS Together Jessica Briefer French Senior Research Scientist 1 Integration: The Holy Grail? An act or instance of combining into an integral
From Fragmentation to Integration: Bringing Medical Care and HCBS Together Jessica Briefer French Senior Research Scientist 1 Integration: The Holy Grail? An act or instance of combining into an integral
Dual Eligibles: Integrating Medicare and Medicaid A Briefing Paper
 Dual Eligibles: Integrating Medicare and Medicaid A Briefing Paper Although almost all older Americans are covered through Medicare, forty-five percent of Medicare beneficiaries (16 million) are poor or
Dual Eligibles: Integrating Medicare and Medicaid A Briefing Paper Although almost all older Americans are covered through Medicare, forty-five percent of Medicare beneficiaries (16 million) are poor or
2014 Model of Care. Provider Training. Molina Medicare _rev_8-14_cab
 2014 Model of Care Provider Training Molina Medicare 2014 5-2013_rev_8-14_cab Course Overview The Model of Care (MOC) is Molina Healthcare s documentation of the CMS directed plan for delivering coordinated
2014 Model of Care Provider Training Molina Medicare 2014 5-2013_rev_8-14_cab Course Overview The Model of Care (MOC) is Molina Healthcare s documentation of the CMS directed plan for delivering coordinated
Response to ODJFS RFI: Ohio Association of Area Agencies on Aging
 Response to ODJFS RFI: Ohio Association of Area Agencies on Aging Creation of an Integrated healthcare Delivery System for Medicare and Medicaid Eligible Beneficiaries: Addressing the needs of Ohio s Older
Response to ODJFS RFI: Ohio Association of Area Agencies on Aging Creation of an Integrated healthcare Delivery System for Medicare and Medicaid Eligible Beneficiaries: Addressing the needs of Ohio s Older
Medicaid and CHIP Payment and Access Commission (MACPAC) February 2013 Meeting Summary
 February 2013 Meeting Summary") Medicaid and CHIP Payment and Access Commission (MACPAC) February 2013 Meeting Summary The Medicaid and CHIP Payment and Access Commission (MACPAC) was established in the Children's Health Insurance Program
Medicaid and CHIP Payment and Access Commission (MACPAC) February 2013 Meeting Summary The Medicaid and CHIP Payment and Access Commission (MACPAC) was established in the Children's Health Insurance Program
Transitions and Long-Term Care: The Minimum Data Set 3.0 Section Q and Money Follows the Person
 Transitions and Long-Term Care: The Minimum Data Set 3.0 Section Q and Money Follows the Person 2 Agenda Housekeeping/Introductions An overview of the Minimum Data Set (MDS) 3.0 Section Q An overview of
Transitions and Long-Term Care: The Minimum Data Set 3.0 Section Q and Money Follows the Person 2 Agenda Housekeeping/Introductions An overview of the Minimum Data Set (MDS) 3.0 Section Q An overview of
Ombudsman Programs: Advocacy in Board & Care Present. Louise Ryan, MPA Ombudsman Program Specialist, ACL/AoA October 26, 2013
 Ombudsman Programs: Advocacy in Board & Care 1981- Present Louise Ryan, MPA Ombudsman Program Specialist, ACL/AoA October 26, 2013 A quick journey of 32 years.. Review history and evolution of board and
Ombudsman Programs: Advocacy in Board & Care 1981- Present Louise Ryan, MPA Ombudsman Program Specialist, ACL/AoA October 26, 2013 A quick journey of 32 years.. Review history and evolution of board and
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Health Plans and LTSS. NASUAD April 20,2011 Mary Kennedy, ACAP Medicare Vice President 1
 Health Plans and LTSS NASUAD April 20,2011 Mary Kennedy, ACAP Medicare Vice President 1 Agenda ACAP Background Health Plan Interest in LTSS Developing Plan Capacity Relationship Building What should states
Health Plans and LTSS NASUAD April 20,2011 Mary Kennedy, ACAP Medicare Vice President 1 Agenda ACAP Background Health Plan Interest in LTSS Developing Plan Capacity Relationship Building What should states
Lessons Learned from the Dual Eligibles Demonstrations. Real-Life Takeaways from California and Other States
 Lessons Learned from the Dual Eligibles Demonstrations 1 May 28, 2015 Real-Life Takeaways from California and Other States Introductions Toby Douglas Consultant, MAXIMUS Former Director of California Department
Lessons Learned from the Dual Eligibles Demonstrations 1 May 28, 2015 Real-Life Takeaways from California and Other States Introductions Toby Douglas Consultant, MAXIMUS Former Director of California Department
Medicare: 2017 Model of Care Training 12/14/201 7
 Medicare: 2017 Model of Care Training 12/14/201 7 What is the Model of Care? The Model of Care (MOC) is Allwell s plan for delivering our integrated care management program for members with special needs.
Medicare: 2017 Model of Care Training 12/14/201 7 What is the Model of Care? The Model of Care (MOC) is Allwell s plan for delivering our integrated care management program for members with special needs.
Community Health Workers & Rural Health: Increasing Access, Improving Care Minnesota Rural Health Conference June 26, 2012
 Community Health Workers & Rural Health: Increasing Access, Improving Care Minnesota Rural Health Conference June 26, 2012 Joan Cleary, Interim Executive Director Minnesota Community Health Worker Alliance
Community Health Workers & Rural Health: Increasing Access, Improving Care Minnesota Rural Health Conference June 26, 2012 Joan Cleary, Interim Executive Director Minnesota Community Health Worker Alliance
LEGISLATIVE REPORT NORTH CAROLINA HEALTH TRANSFORMATION CENTER (TRANSFORMATION INNOVATIONS CENTER) PROGRAM DESIGN AND BUDGET PROPOSAL
 PROGRAM DESIGN AND BUDGET PROPOSAL") LEGISLATIVE REPORT NORTH CAROLINA HEALTH TRANSFORMATION CENTER (TRANSFORMATION INNOVATIONS CENTER) PROGRAM DESIGN AND BUDGET PROPOSAL SESSION LAW 2015-245, SECTION 8 FINAL REPORT State of North Carolina
LEGISLATIVE REPORT NORTH CAROLINA HEALTH TRANSFORMATION CENTER (TRANSFORMATION INNOVATIONS CENTER) PROGRAM DESIGN AND BUDGET PROPOSAL SESSION LAW 2015-245, SECTION 8 FINAL REPORT State of North Carolina
New Opportunities for Case Management Leadership in our Changing Environment
 New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
Report from the National Quality Forum: National Priorities Partnership Quarterly Synthesis of Action In Support of the Partnership for Patients
 Report from the National Quality Forum: National Priorities Partnership Quarterly Synthesis of Action In Support of the Partnership for Patients August 2012 Supporting Patient Safety through the National
Report from the National Quality Forum: National Priorities Partnership Quarterly Synthesis of Action In Support of the Partnership for Patients August 2012 Supporting Patient Safety through the National
Moving the Dial on Quality
 Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Long-Term Care Improvements under the Affordable Care Act (ACA)
") Long-Term Care Improvements under the Affordable Care Act (ACA) South Carolina Health Care Implementation Coalition September 17, 2010 JoAnn Lamphere, DrPH Director, State Government Relations Health &
Long-Term Care Improvements under the Affordable Care Act (ACA) South Carolina Health Care Implementation Coalition September 17, 2010 JoAnn Lamphere, DrPH Director, State Government Relations Health &
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Trends in State Medicaid Programs: Emerging Models and Innovations
 Trends in State Medicaid Programs: Emerging Models and Innovations Speakers: Barbara Edwards, Principal, Steve Fitton, Principal, Tina Edlund, Managing Principal, Moderator: Annie Melia, Information Services
Trends in State Medicaid Programs: Emerging Models and Innovations Speakers: Barbara Edwards, Principal, Steve Fitton, Principal, Tina Edlund, Managing Principal, Moderator: Annie Melia, Information Services
HIT Glossary and Acronym List
 HIT Glossary and Acronym List November 2011 FACT SHEET ACA Patient Protection and Affordable Care Act (see PPACA). ACO Accountable Care Organization: A group of health care providers (e.g. primary care,
HIT Glossary and Acronym List November 2011 FACT SHEET ACA Patient Protection and Affordable Care Act (see PPACA). ACO Accountable Care Organization: A group of health care providers (e.g. primary care,
Introducing AmeriHealth Caritas Iowa
 Introducing AmeriHealth Caritas Iowa A presentation for Iowa providers. CPC; Q215 Iowa V1 Who We Are Who We Serve Agenda Our Mission AmeriHealth Caritas Iowa Why Partner With Us? Questions 2 2 Who We Are
Introducing AmeriHealth Caritas Iowa A presentation for Iowa providers. CPC; Q215 Iowa V1 Who We Are Who We Serve Agenda Our Mission AmeriHealth Caritas Iowa Why Partner With Us? Questions 2 2 Who We Are
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
The Commission on Long-Term Care: Background Behind the Mission
 THE BASICS The Commission on Long-Term Care: Background Behind the Mission As part of the American Taxpayer Relief Act of 2012 (ATRA, P.L. 112-240), Congress created a Commission on Long-Term Care 1 that
THE BASICS The Commission on Long-Term Care: Background Behind the Mission As part of the American Taxpayer Relief Act of 2012 (ATRA, P.L. 112-240), Congress created a Commission on Long-Term Care 1 that
Medical Care Meets Long-Term Services and Supports (LTSS)
") Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
The Long-Term Care Ombudsman Program: What Residents Who Want to Transition Can Expect from Their Advocates
 The Long-Term Care Ombudsman Program: What Residents Who Want to Transition Can Expect from Their Advocates Becky A. Kurtz Director, Office of Long-Term Care Ombudsman Programs MDS 3.0 Section Q National
The Long-Term Care Ombudsman Program: What Residents Who Want to Transition Can Expect from Their Advocates Becky A. Kurtz Director, Office of Long-Term Care Ombudsman Programs MDS 3.0 Section Q National
Quality Measurement at the Interface of Health Care and Population Health
 1 Institute of Medicine Committee on Quality Measures Healthy People Leading Health Indicators December 10, 2012 Quality Measurement at the Interface of Health Care and Population Health Shari M. Ling,
1 Institute of Medicine Committee on Quality Measures Healthy People Leading Health Indicators December 10, 2012 Quality Measurement at the Interface of Health Care and Population Health Shari M. Ling,
Opportunities to Advance Lifespan Respite: Managed Long-Term Services and Supports and Affordable Care Act Options
 Opportunities to Advance Lifespan Respite: Managed Long-Term Services and Supports and Affordable Care Act Options October 18, 2013 Joe Caldwell Director of Long-Term Services and Supports Policy 1 Overview
Opportunities to Advance Lifespan Respite: Managed Long-Term Services and Supports and Affordable Care Act Options October 18, 2013 Joe Caldwell Director of Long-Term Services and Supports Policy 1 Overview
Quality Measures and Federal Policy: Increasingly Important and A Work in Progress. American Health Quality Association Policy Forum Washington, D.C.
 Quality Measures and Federal Policy: Increasingly Important and A Work in Progress American Health Quality Association Policy Forum Washington, D.C. February 9, 2016 Quality Journey NCQA Develops Health
Quality Measures and Federal Policy: Increasingly Important and A Work in Progress American Health Quality Association Policy Forum Washington, D.C. February 9, 2016 Quality Journey NCQA Develops Health
Medicaid Efficiency and Cost-Containment Strategies
 Medicaid Efficiency and Cost-Containment Strategies Medicaid provides comprehensive health services to approximately 2 million Ohioans, including low-income children and their parents, as well as frail
Medicaid Efficiency and Cost-Containment Strategies Medicaid provides comprehensive health services to approximately 2 million Ohioans, including low-income children and their parents, as well as frail
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Medicaid and Medicare Resource Use For Dual Eligibles in Maryland
 Medicaid and Medicare Resource Use For Dual Eligibles in Maryland November 9, 2011 Charles Milligan NAMD Conference The Hilltop Institute at UMBC conducted research on Medicare-Medicaid cross-payer effects
Medicaid and Medicare Resource Use For Dual Eligibles in Maryland November 9, 2011 Charles Milligan NAMD Conference The Hilltop Institute at UMBC conducted research on Medicare-Medicaid cross-payer effects
As part of the Patient Protection and Affordable Care Act
 CENTER FOR HEALTHCARE RESEARCH & TRANSFORMATION Issue Brief February 2016 Affordable Care Act Funding: An Analysis of Grant Programs under Health Care Reform FY2010-FY2015 Spending Provisions...2 Spending
CENTER FOR HEALTHCARE RESEARCH & TRANSFORMATION Issue Brief February 2016 Affordable Care Act Funding: An Analysis of Grant Programs under Health Care Reform FY2010-FY2015 Spending Provisions...2 Spending
Top Reasons to Become an AmeriHealth Caritas Virginia Provider. amerihealthcaritas.com
 Top Reasons to Become an AmeriHealth Caritas Virginia Provider amerihealthcaritas.com WHO WE ARE About AmeriHealth Caritas AmeriHealth Caritas Family of Companies ( AmeriHealth Caritas ) is a national
Top Reasons to Become an AmeriHealth Caritas Virginia Provider amerihealthcaritas.com WHO WE ARE About AmeriHealth Caritas AmeriHealth Caritas Family of Companies ( AmeriHealth Caritas ) is a national
Comment Template for Care Coordination Standards
 GENERAL COMMENTS Thank you for the opportunity to provide input into these very important standards. We offer the following comments in the spirit of improving clarity, consistency, and ease of reading
GENERAL COMMENTS Thank you for the opportunity to provide input into these very important standards. We offer the following comments in the spirit of improving clarity, consistency, and ease of reading
Comprehensive Primary Care for Older Patients with
 Comprehensive Primary Care for Older Patients with Multiple Chronic Conditions Chad Boult JAMA 2010, Care of the Aging Patient: From Evidence to Action Ms. N 77 year-old widow Retired factory worker Lives
Comprehensive Primary Care for Older Patients with Multiple Chronic Conditions Chad Boult JAMA 2010, Care of the Aging Patient: From Evidence to Action Ms. N 77 year-old widow Retired factory worker Lives
Improving Care and Lowering Costs for Dual Eligible Beneficiaries
 Improving Care and Lowering Costs for Dual Eligible Beneficiaries An Overview of Federal and State Efforts on Duals and Suggested Strategies to Position PACE National PACE Association September 13, 2011
Improving Care and Lowering Costs for Dual Eligible Beneficiaries An Overview of Federal and State Efforts on Duals and Suggested Strategies to Position PACE National PACE Association September 13, 2011
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Executive Summary. Leadership Toolkit for Redefining the H: Engaging Trustees and Communities
 Executive Summary Leadership Toolkit for Redefining the H: Engaging Trustees and Communities Report produced by the AHA Committee on Research and Committee on Performance Improvement 2015 Executive Summary
Executive Summary Leadership Toolkit for Redefining the H: Engaging Trustees and Communities Report produced by the AHA Committee on Research and Committee on Performance Improvement 2015 Executive Summary
Overview and Current Status of Program of All-inclusive Care for the Elderly (PACE) Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways
 Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways") Overview and Current Status of Program of All-inclusive Care for the Elderly (PACE) Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways 1 What is On Lok? Original Vision: Help the low-income
Overview and Current Status of Program of All-inclusive Care for the Elderly (PACE) Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways 1 What is On Lok? Original Vision: Help the low-income
The Community based Care Transitions Program (CCTP)
") The Community-based Care Transitions Program Juliana R. Tiongson, MPH The Innovation Center Centers for Medicare and Medicaid Services 1 The Community based Care Transitions Program (CCTP) The CCTP, created
The Community-based Care Transitions Program Juliana R. Tiongson, MPH The Innovation Center Centers for Medicare and Medicaid Services 1 The Community based Care Transitions Program (CCTP) The CCTP, created
Agenda. ACMA A Strong Base
 New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
Issue Brief February 2015 Affordable Care Act Funding:
 CENTER FOR HEALTHCARE RESEARCH & TRANSFORMATION Issue Brief February 2015 Affordable Care Act Funding: An Analysis of Grant Programs under Health Care Reform FY2010- The Patient Protection and Affordable
CENTER FOR HEALTHCARE RESEARCH & TRANSFORMATION Issue Brief February 2015 Affordable Care Act Funding: An Analysis of Grant Programs under Health Care Reform FY2010- The Patient Protection and Affordable
Breaking Down the Silos of Patient Care: Integration of Social Support Services into Health Care Delivery
 Breaking Down the Silos of Patient Care: Integration of Social Support Services into Health Care Delivery Robyn Golden, LCSW Director of Health and Aging Rush University Medical Center National Health
Breaking Down the Silos of Patient Care: Integration of Social Support Services into Health Care Delivery Robyn Golden, LCSW Director of Health and Aging Rush University Medical Center National Health
Patient-Centered Medical Home Best Practices: Case Study Examples
 Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Accountable Care Organizations
 Accountable Care Organizations Randy Wexler, MD, MPH, FAAFP Associate Professor Vice Chair, Clinical Services Department of Family Medicine The Ohio State University Wexner Medical Center Objectives To
Accountable Care Organizations Randy Wexler, MD, MPH, FAAFP Associate Professor Vice Chair, Clinical Services Department of Family Medicine The Ohio State University Wexner Medical Center Objectives To
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Transforming Clinical Practice Initiative Awards
 Transforming Clinical Practice Initiative Awards Americans expect a health care system that delivers the right care, at the right time, and at a cost that is reasonable and easy to understand. Such a system
Transforming Clinical Practice Initiative Awards Americans expect a health care system that delivers the right care, at the right time, and at a cost that is reasonable and easy to understand. Such a system
Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10
 Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10 On March 23, 2010, President Obama signed a comprehensive health care reform bill (H.R. 3590) into law. On March
Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10 On March 23, 2010, President Obama signed a comprehensive health care reform bill (H.R. 3590) into law. On March
Community Mental Health and Care integration. Zandrea Ware and Ricardo Fraga
 Community Mental Health and Care integration Zandrea Ware and Ricardo Fraga One in Five Approximately 1 in 5 adults in the U.S. 43.8 million, or 18.5% experiences mental illness in their lifetime. Community
Community Mental Health and Care integration Zandrea Ware and Ricardo Fraga One in Five Approximately 1 in 5 adults in the U.S. 43.8 million, or 18.5% experiences mental illness in their lifetime. Community
HEALTH PROFESSIONAL WORKFORCE
 HEALTH PROFESSIONAL WORKFORCE (SECTION-BY-SECTION ANALYSIS) (Information compiled from the Democratic Policy Committee (DPC) Report on The Patient Protection and Affordable Care Act and the Health Care
HEALTH PROFESSIONAL WORKFORCE (SECTION-BY-SECTION ANALYSIS) (Information compiled from the Democratic Policy Committee (DPC) Report on The Patient Protection and Affordable Care Act and the Health Care
HEALTH CARE REFORM IN THE U.S.
 HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care
 An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships
 States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
Accountable Care and Governance Challenges Under the Affordable Care Act
 Accountable Care and Governance Challenges Under the Affordable Care Act The First National Congress on Healthcare Clinical Innovations, Quality Improvement and Cost Containment October 26, 2011 Doug Hastings
Accountable Care and Governance Challenges Under the Affordable Care Act The First National Congress on Healthcare Clinical Innovations, Quality Improvement and Cost Containment October 26, 2011 Doug Hastings
Friday Health Plans of Colorado
 QUALITY OVERVIEW Health Plans of Colorado (formerly Colorado Choice Health Plans) Serving Colorado for over 4 years, Health Plans utilizes a community-focused model. We work hand in hand with local providers
QUALITY OVERVIEW Health Plans of Colorado (formerly Colorado Choice Health Plans) Serving Colorado for over 4 years, Health Plans utilizes a community-focused model. We work hand in hand with local providers
Certified Community Behavioral Health Clinic (CCHBC) 101
 101") Certified Community Behavioral Health Clinic (CCHBC) 101 On April 1, 2014, the President signed the Protecting Access to Medicare Act (PAMA) into law, which included a provision authorizing a two part
Certified Community Behavioral Health Clinic (CCHBC) 101 On April 1, 2014, the President signed the Protecting Access to Medicare Act (PAMA) into law, which included a provision authorizing a two part
Integrated Care Management in Rural Communities
 University of Southern Maine USM Digital Commons Behavioral Health Maine Rural Health Research Center (MRHRC) 5-1-2014 Integrated Care Management in Rural Communities Eileen Griffin JD University of Southern
University of Southern Maine USM Digital Commons Behavioral Health Maine Rural Health Research Center (MRHRC) 5-1-2014 Integrated Care Management in Rural Communities Eileen Griffin JD University of Southern
The Center for Medicare & Medicaid Innovations: Programs & Initiatives
 The Center for Medicare & Medicaid Innovations: Programs & Initiatives Rob Stone, Esq. American Health Lawyers Association Institute on Medicare & Medicaid Payment Issues March 30-April 1, 2012 CMMI Mission
The Center for Medicare & Medicaid Innovations: Programs & Initiatives Rob Stone, Esq. American Health Lawyers Association Institute on Medicare & Medicaid Payment Issues March 30-April 1, 2012 CMMI Mission
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology
 Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information