ACA Readiness: Making Change a Reality
|
|
|
- Marshall Farmer
- 6 years ago
- Views:
Transcription

-684-7457 2 A Roadmap for Impactful Change!")


1 ACA Readiness: Making Change a Reality Presented by: MTM Services P. O. Box 1027, Holly Springs, NC Phone: Fax: Scott.Lloyd@mtmservices.org Web Site: wwww.mtmservices.org MTM Publication Ordering Information: or Call (202) A Roadmap for Impactful Change! Operationalizing Health Reform was written by the entire MTM Services Team to be an up to date view of what we have learned working to help hundreds of organizations across the country and abroad make the changes necessary to be successful in today s ever changing environment of health reform. Each of the 14 chapters deal with a specific change focus required to help vision based leaders improve their organization s quality of care, efficiency, and the compliance of their service delivery system! To Order or for more information visit: or If preferred call (202)
2 Experience Improving Quality in the Face of Healthcare Reform MTM Services has delivered consultation to over 700 providers (MH/SA/DD/Residential) in 45 states and 2 foreign countries since MTM Services Access Redesign Experience (Excluding individual clients): 5 National Council Funded Access Redesign grants with 200 organizations across 25 states 6 Statewide efforts with 140 organizations Over 1,500 individualized flow charts created Over $16,000,000 in Annual Savings generated thus far A lot of happy staff and consumers 4 Access Redesign Experience - Improving Quality in the Face of Healthcare Reform David Lloyd, Founder of MTM Services and Senior Consultant for the National Council Scott Lloyd, President of MTM Services and Senior Consultant for the National Council Randy Love, Chief Information Officer for SPQM Data Reporting Services Willa Presmanes, M.Ed., M. A., Medical Necessity/Utilization Management Expert and Co-Author of the DLA-20 (Daily Living Activities) functionality scale Bill Schmelter, Ph.D., Lead Clinical & Collaborative Documentation Consultant for MTM Services and Consultant for the National Council Michael Flora, M.B.A., M.A.Ed., L.P.C.C., L.S.W., Lead Operations Consultant for MTM Services, CEO of the Ben Gordon Center in DeKalb, IL, and Consultant for the National Council David Swann, MA, LCAS, CCS, LPC, NCC M.T.M. Services Senior Integrated Healthcare Consultant, CEO of a public Local Management Entity in North Carolina, and Consultant for the National Council Joy Fruth, M.S.W., Lead Process Change Consultant for M.T.M. Services and Consultant for the National Council Katherine Hirsch, MSW, LCSW, Collaborative Documentation Consultant Specializing in Collaborative Documentation with Children and Consultant for the National Council John Kern, MD - Collaborative Documentation Consultant for M.T.M. Services and Consultant for the National Council Annie Jensen, MSW, LCSW - Process Change Consultant for MTM Services, Vice President of Operations/ Burrell Behavioral Health, and Consultant for the National Council Justin Senechal - Database Developer/Data Analyst for MTM Services Jennifer Senechal Financial Controller and Cost & Revenue Analyst for M.T.M. Services 5 The National Landscape / Today s Reality What can you do about the changes we face Besides Panicking? 6 2

3 The National Landscape So tell me, How bad is it? State Funding Issues Federal Issues: Office of Inspector General Obstacles to Integrated Care Are future rule changes holding you hostage now? Focus on what you can control Agenda Item: It s so awful time Move now, not after the challenges come about. 7 The National Landscape 8 The National Landscape Federal O.I.G. The Office of Inspector General -Do you know about the Exclusion s Database? -Do you know about RAC teams? -A lot of states are the passing the compliance responsibilities to the providers. -Do you know why Money is being taken back? -Increased audits with an emphasis on Medical Necessity Linkage and The Rehabilitation Model. 9 3



4 Quantitative Vs. Qualitative Historically, State MH/DD/SA Departments have focused on quantitative review it is there and is it signed/dated CMS has moved to a qualitative review standard does the documentation quality justify the intensity, duration and frequency of services? Qualitative reviews require demonstration of the Golden Thread. 10 The National Landscape 11 The National Landscape The Compliance Officer is accountable for the organization s compliance program, not the organization s compliance. Everyone is accountable for the latter by either their own conduct or staff or activity overseen. Source: Adam J. Falcone ( 12 4
5 Redesign - Improving Quality in the Face of Healthcare Reform What are your Teams Roadblocks? Team members with differing opinions Teams who setup their systems to the Exceptions. 13 Process Redesign Review Get Past Emotion with the use of Data: Organizations that have continued forward without fully addressing the questions around the creation and use of data reports as part of their decision making process often face some historical management philosophies/challenges that cannot be overcome because they exist in the emotional realm: A lack of data leads to a Retreat Culture Lack of leadership through data opens the door for Passionate Staff 14 Client Definition of Access Client Calls for Help Wait Time # 1 Assessment Appointment Wait Time # 2 Treatment Planning Appointment Wait Time # 3 Client Arrives for an Open Session 15 5
 -The Average Client Time in the process is 3.72 hours, while the Average Staff Time is 4.96.")
6 GAP Results Access is the Key Highlights - -There are 191 Unique Client Entry flows for the 22 organizations represented in the comparison charts. -The Minimum Wait time to Access are is 2.6 days, while the Maximum is 319. (544 is the national high that we have measured if you are curious) -The Average Client Time in the process is 3.72 hours, while the Average Staff Time is GAP Results Access is the Key Access Process - Wait time by Organization and Division 17 GAP Results Access is the Key Access Process - Wait time by Division 18 6



7 GAP Results Access is the Key Access Process - Client time by Organization and Division 19 GAP Results Access is the Key Access Process - Staff time by Organization and Division 20 GAP Results Access is the Key Access Process - Staff vs. Client time by Organization and Division 21 7
8 GAP Results Access is the Key Access Process - Staff vs. Client time by Organization and Division 22 How We Arrived Here 23 No Show/ Cancellation Holiday Sick Leave Vacation Leave Travel Training Typical Center Staff Resource Utilization Billable Service Meetings Paperwork Non-Billable Service 24 8

9 How We Arrived Here Assessment Appointment Wait Time Documentation Concerns Repetitive Data Collection Overly Extensive Narratives Post Session Documentation Time Leads to holding back time Capacity Issues Caseloads Full Staff Short on Direct Service Expectations No Show Issues Leads to double booking Generates Staff Anxiety 25 What we do About it! Collaborative Documentation Same Day Access No Show Management Utilization Review/Utilization Management EOC/LOC 26 Process Redesign Review RESULTS 27 9
 49.25 New Process Averages: 5.04 3.34 2.99 (210.20) 29.31 Savings: 0.66 1.73 0.65 $121.43 19.94 Change %: 12% 34% 18% 37% 40% Avg.")
, Ohio (12), & Wyoming (9).")
10 Process Redesign Review Total Number of Processes Total Staff Time (Hrs) Total Client Time without Wait-time (Hrs) Cost for Process Total Wait-time (Days) Copyright Old Process Averages: (331.63) New Process Averages: (210.20) Savings: $ Change %: 12% 34% 18% 37% 40% Avg. Number of Intakes Per Month Monthly Savings: Annual Savings: 3,843 $466, $5,599, Represented: 28 Organizations of 48 Organizations who started the Access Redesign Grant from Florida (7), Ohio (12), & Wyoming (9). The average annual savings for these 28 organizaitons if $199, per agency. Extrapolating this savings across all organizations who started the pilot would equate to an annual savings of $9,599, Process Redesign Review Total Number of Processes Total Staff Time (Hrs) Total Client Time without Wait-time (Hrs) Cost for Process Total Wait-time (Days) Old Process Averages: (249.38) New Process Averages: (162.19) Copyright Savings: $ Change %: 10% 25% 14% 35% 55% Avg. Number of Intakes Per Month Difference Intake Volume: Intake Volume Change %: Monthly Savings: Annual Savings: 2, % $154,419 $1,853, * Numbers are for 10 Centers from 9 states. Average Savings = $185, per agency. * Take out the 2nd year organizations, Average Savings = $231, per agency. 29 Process Redesign Review 30 10
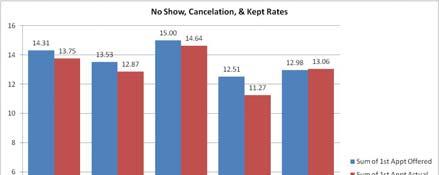
11 The Same Day Access Model; Making it Happen! A Standardized Solution For CBHOs Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC Phone: Fax: Scott.Lloyd@mtmservices.org Web Site: Client Definition of Access Client Calls for Help Wait Time # 1 Assessment Appointment Wait Time # 2 Treatment Planning Appointment Wait Time # 3 Client Arrives for an Open Session 32 Walk In Intake/Assessments a 0% No Show Model Why Same Day Access? It makes Sense! When looking at Access Models, you should first ask yourself, What do I expect when seeking medical care? Client Satisfaction/Engagement Clients who are offered a same day appointment show up 91% of the time, those schedule one day later show up 75% of the time. Teams who move to Same Day Access see a 10% increase in the kept rate of their follow up appointments on average. Reduce System Waste - In several cases, CBHOs have determined that due to the high rate of initial no shows experienced, there would be less clinician time utilized to move to a nonscheduled walk in intake process



12 Assessment Appointment Trends by Days of Wait for all Centers (Over 22,000 Events) Days Wait 34 Assessment Appointment Trends by Days of Wait for all Centers (Over 22,000 Events) Days Wait 35 NCQA Accreditation Standards for Patient- Centered Medical Homes (PCMH) NCQA has published accreditation standards for PCMHs Primary Care Development Corporation has developed a standard version of the Baseline PCMH Self-Assessment Tool that will guide PCMHs in their need to obtain accreditation 36 12





13 Source: Primary Care Corporation PCMH Self- Assessment Tool 37 Walk In Intake/Assessments a 0% No Show Model The Anxiety that can proceed this change is 10 times worse than the change itself! Same Day Access does NOT look like this; as long as you plan it out correctly! Photo Credits: Matador Records & The Simpsons 38 Walk In Intake/Assessments a 0% No Show Model The Set Up Steps for Success! 1. Determine your Organization s Demand and Optimal Hours of Operation 2. Select Your Staffing / Team Model / Back-Up Contingency Staff 3. Set a Plan to handle your Existing Appointments 4. Choreograph your Wait time 5. Communicate and Go! 39 13
14 Walk In Intake/Assessments a 0% No Show Model Set Up Steps: 1. Determine your Organization s Demand and Optimal Hours of Operation Open Access Days (Recommended if demand is sufficient) Full Open Access Hybrid Model Call Ahead Times 40 Walk In Intake/Assessments a 0% No Show Model Set Up Steps: 2. Select Your Staffing / Team Model / Back-Up Contingency Staff Set Team - Intake/Assessment clinicians are assigned full or part time to specifically provide all intake/assessments on a walk in basis. After assessment, consumer is referred to other clinicians for treatment. Negative to this model is that the consumer must tell their story at least two times, UNLESS, the treating clinician will trust and utilized the assessment provided at intake Rotating Team - Regular unit clinicians are scheduled in two-hour blocks beginning each morning and throughout the day (four blocks) to provide intakes. The number of clinicians assigned to each block is based on historical intake calls received and intakes provided. 41 Walk In Intake/Assessments a 0% No Show Model Set Up Steps: 3. Set a Plan to handle your Existing intake / assessment Appointments Smooth Transition Kick-Off Date Existing Appointments End of Transition Walk-In Appointments 42 14
15 Walk In Intake/Assessments a 0% No Show Model Set Up Steps: 4. Choreograph your Wait time Pre-session: What are the pre-session activities that you will utilize? Session goals: Master s Level assessment provided the same day of call or walk in for help (If the consumer calls after 3:00 p.m. they will be asked to come in the next morning unless in crisis or urgent need) Initial diagnosis determined Level of Care and Benefit Design Identified with consumer Initial treatment plan Developed based on Benefit Design Package Follow Up Goals: 2nd clinical appointment for TREATMENT within 8 days of Initial Intake 1st medical appointment within 10 days of Initial Intake 43 Walk In Intake/Assessments a 0% No Show Model Set Up Steps: 5. Communicate and Go! Traditional Script Elements (3-5 min) - Basic Demographics (Name, Phone) Confirm Crisis Status Confirm what services they desire Confirm their funding source - (Script B?) Give them hours of operation & what to bring Ask them what time they plan to come in 44 Open Scheduling Same Day Access Model Consumer Engagement Standards Successfully Running - Now What? 1. Utilize Data to Confirm Planning Assumptions. 2. Monitor and Ensure Sustainability!! Review Capacity and Adjust accordingly 1. No Show Management 2. EOC / LOC Reviews 45 15

, second appointments and noshows.")


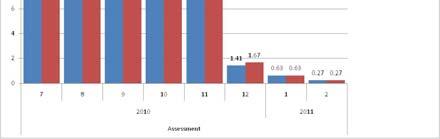
16 Process Redesign Review DATA/ RESULTS 46 Tracking your Transition Our Projections were for a Maximum of 21 Intakes per day, and to achieve an average of 7 Intakes per day with in 16 days. 47 Access to Care Timeliness Case Study Using data that demonstrate the following about the relationship between initial contact for help, Open access (same day assessments), second appointments and noshows. Sample size is 561 new customers who received an intake between January 1, 2009 and May 31, The summary of outcomes identified are outlined below: a. Approximately 95 percent of the customers who have their second appointment scheduled within 12.2 days of their Intake show for that appointment. Therefore the 10 day access standard that is recommended is valid for the second counseling service and medical appointment. b. Approximately 70 percent of customers who have the second appointment scheduled 22 days or more after their intake did not show. c. 100 percent of the customers whose second appointment was canceled by the Center never came back

17 Access to Care Timeliness Case Study 49 Days to Access Services Standard: 10 days from first call/contact to Intake, 1 st Therapy and 1 st Medical Access Redesign Grant Results Assessment Appointment Impacts 51 17


18


19 55 Redesign Results 2 nd Appointment Impact


20 58 Next Steps Questions and Answers? Resources Needed? Thank You 59 20
ACA Readiness: Making Change a Reality
 ACA Readiness: Making Change a Reality Presented by: MTM Services P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-387-9892 Fax: 919-773-8141 E-mail: Scott.Lloyd@mtmservices.org Web Site: wwww.mtmservices.org
ACA Readiness: Making Change a Reality Presented by: MTM Services P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-387-9892 Fax: 919-773-8141 E-mail: Scott.Lloyd@mtmservices.org Web Site: wwww.mtmservices.org
How Easily Can People Access Your Services? Presented by:
 Same Day Access Presented by: ScottLloyd Lloyd, President Audio and Control Panel Opening Your Line 1. Make sure Telephone is the option selected 2. Dial your Access Code 3. Enter your two digit Audio
Same Day Access Presented by: ScottLloyd Lloyd, President Audio and Control Panel Opening Your Line 1. Make sure Telephone is the option selected 2. Dial your Access Code 3. Enter your two digit Audio
Presented by: President M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540
 Presented by Scott C C. Lloyd, oyd, President M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-387-9892 Fax: 919-773-8141 E-mail: Scott.lloyd@mtmservices.org Web Site: wwww.mtmservices.org
Presented by Scott C C. Lloyd, oyd, President M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-387-9892 Fax: 919-773-8141 E-mail: Scott.lloyd@mtmservices.org Web Site: wwww.mtmservices.org
The 5 Steps to Same Day Access
 Joy Fruth, MSW Lead Process Change Consultant MTM Services The 5 Steps to Same Day Access Speaker Name Title Presented Organization By: What is Same Day Access? An engagement strategy whereby organizations
Joy Fruth, MSW Lead Process Change Consultant MTM Services The 5 Steps to Same Day Access Speaker Name Title Presented Organization By: What is Same Day Access? An engagement strategy whereby organizations
VBR - Methodologies of Implementing Costing Measurements
 VBR - Methodologies of Implementing Costing Measurements Presented by: MTM Services P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-387-9892 Fax: 919-773-8141 E-mail: Scott.Lloyd@mtmservices.org Web
VBR - Methodologies of Implementing Costing Measurements Presented by: MTM Services P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-387-9892 Fax: 919-773-8141 E-mail: Scott.Lloyd@mtmservices.org Web
The Care Transitions Network
 Making the move to Value Based Reimbursement/Payment/Purchasing (VBR/P 2 ): Using Data to Improve Care Delivery and Your Organizations Performance The Care Transitions Network Presented by: Scott C. Lloyd,
Making the move to Value Based Reimbursement/Payment/Purchasing (VBR/P 2 ): Using Data to Improve Care Delivery and Your Organizations Performance The Care Transitions Network Presented by: Scott C. Lloyd,
The Care Transitions Network
 Making the move to Value Based Reimbursement/Payment/Purchasing (VBR/P 2 ): Using Data to Improve Care Delivery and Your Organizations Performance The Care Transitions Network Presented by: Scott C. Lloyd,
Making the move to Value Based Reimbursement/Payment/Purchasing (VBR/P 2 ): Using Data to Improve Care Delivery and Your Organizations Performance The Care Transitions Network Presented by: Scott C. Lloyd,
Transforming Healthcare Delivery, the Challenges for Behavioral Health
 Transforming Healthcare Delivery, the Challenges for Behavioral Health Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: mtmserve@aol.com
Transforming Healthcare Delivery, the Challenges for Behavioral Health Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: mtmserve@aol.com
Assessment Overview. David Lloyd, Founder M.T.M. Services
 Integrated Healthcare Readiness Assessment Overview Presented by: M.T.M. Services P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: david.lloyd@mtmservices.org Web Site:
Integrated Healthcare Readiness Assessment Overview Presented by: M.T.M. Services P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: david.lloyd@mtmservices.org Web Site:
Sustaining Open Access. Annie Jensen LCSW Clinical Consultant, MTM Services
 Sustaining Open Access Annie Jensen LCSW Clinical Consultant, MTM Services Annie.Jensen@mtmservices.org Healthcare Reform Context Under an Accountable Care Organization Model the Value of Behavioral Health
Sustaining Open Access Annie Jensen LCSW Clinical Consultant, MTM Services Annie.Jensen@mtmservices.org Healthcare Reform Context Under an Accountable Care Organization Model the Value of Behavioral Health
Enhanced Access: Lessons Learned & Advice for CCBHCs. August 9, 2017
 Enhanced Access: Lessons Learned & Advice for CCBHCs August 9, 2017 Today s Faculty Moderator: Rebecca Farley David VP, Policy and Advocacy at National Council CCBHC Policy Pro 10+ years in health system
Enhanced Access: Lessons Learned & Advice for CCBHCs August 9, 2017 Today s Faculty Moderator: Rebecca Farley David VP, Policy and Advocacy at National Council CCBHC Policy Pro 10+ years in health system
Certified Community Behavioral Health Clinics and Quality It Matters!
 Certified Community Behavioral Health Clinics and Quality It Matters! David R. Swann, MTM Services, LLC Dale Jarvis, Dale Jarvis & Associates Session 4 of the CCBHC Track The CCBHC Roadmap CCBHCs: Quality
Certified Community Behavioral Health Clinics and Quality It Matters! David R. Swann, MTM Services, LLC Dale Jarvis, Dale Jarvis & Associates Session 4 of the CCBHC Track The CCBHC Roadmap CCBHCs: Quality
Alternative Managed Care Reimbursement Models
 Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Collaborative Documentation Will Lower Risk!
 Collaborative Documentation Will Lower Risk! Bill Schmelter PhD Senior Clinical Consultant MTM Services #NatCon14 Ubiquitous Documentation Risk Areas Documentation Linkage Medical Necessity Core elements
Collaborative Documentation Will Lower Risk! Bill Schmelter PhD Senior Clinical Consultant MTM Services #NatCon14 Ubiquitous Documentation Risk Areas Documentation Linkage Medical Necessity Core elements
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
SIGNATURE OF COUNTY ADMINISTRATOR OR CHIEF ADMINISTRATIVE OFFICER
 APPLICATION FORM All applications must include the following information. Separate applications must be submitted for each eligible program. Deadline: June 1, 2016. Please include this application form
APPLICATION FORM All applications must include the following information. Separate applications must be submitted for each eligible program. Deadline: June 1, 2016. Please include this application form
Client Engagement Support Webinar for CCBHCs. December 13, :00pm 3:30pm ET
 Client Engagement Support Webinar for CCBHCs December 13, 2017 2:00pm 3:30pm ET Webinar Login Directions Recommend calling in on your telephone. Enter your unique Audio PIN so we can mute/unmute your line
Client Engagement Support Webinar for CCBHCs December 13, 2017 2:00pm 3:30pm ET Webinar Login Directions Recommend calling in on your telephone. Enter your unique Audio PIN so we can mute/unmute your line
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
The University of Michigan Health System. Geriatrics Clinic Flow Analysis Final Report
 The University of Michigan Health System Geriatrics Clinic Flow Analysis Final Report To: CC: Renea Price, Clinic Manager, East Ann Arbor Geriatrics Center Jocelyn Wiggins, MD, Medical Director, East Ann
The University of Michigan Health System Geriatrics Clinic Flow Analysis Final Report To: CC: Renea Price, Clinic Manager, East Ann Arbor Geriatrics Center Jocelyn Wiggins, MD, Medical Director, East Ann
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Can Improvement Cause Harm: Ethical Issues in QI. William Nelson, PhD Greg Ogrinc, MD, MS Daisy Goodman, CNM. DNP, MPH
 Session Code A4, B4 The presenters have nothing to disclose Can Improvement Cause Harm: Ethical Issues in QI William Nelson, PhD Greg Ogrinc, MD, MS Daisy Goodman, CNM. DNP, MPH December 6, 2016 #IHIFORUM
Session Code A4, B4 The presenters have nothing to disclose Can Improvement Cause Harm: Ethical Issues in QI William Nelson, PhD Greg Ogrinc, MD, MS Daisy Goodman, CNM. DNP, MPH December 6, 2016 #IHIFORUM
Leveraging Shared Decision Making to Manage Population Health Partners HealthCare s Lessons Learned Gloria Stone Plottel, MS, MBA, Founder and CEO,
 Leveraging Shared Decision Making to Manage Population Health Partners HealthCare s Lessons Learned Gloria Stone Plottel, MS, MBA, Founder and CEO, GSPsquared LLC Adam Licurse, MD, MHS, Associate Medical
Leveraging Shared Decision Making to Manage Population Health Partners HealthCare s Lessons Learned Gloria Stone Plottel, MS, MBA, Founder and CEO, GSPsquared LLC Adam Licurse, MD, MHS, Associate Medical
REQUEST FOR LETTERS OF INTEREST:
 REQUEST FOR LETTERS OF INTEREST: Technical Assistance for Implementing Open Access Release Date: January 8, 2018 Letter Due Date: February 15, 2018 Issued by: Behavioral Health System Baltimore, Inc. 100
REQUEST FOR LETTERS OF INTEREST: Technical Assistance for Implementing Open Access Release Date: January 8, 2018 Letter Due Date: February 15, 2018 Issued by: Behavioral Health System Baltimore, Inc. 100
Implementation and Outcomes from Connecticut s Mobile Crisis Intervention Service
 Implementation and Outcomes from Connecticut s Mobile Crisis Intervention Service Jeffrey J. Vanderploeg, Ph.D. Vice President for Mental Health Child Health & Development Institute of Connecticut Tim
Implementation and Outcomes from Connecticut s Mobile Crisis Intervention Service Jeffrey J. Vanderploeg, Ph.D. Vice President for Mental Health Child Health & Development Institute of Connecticut Tim
Medicaid Funded Services Plan
 Clinical Communication Bulletin 007 To: From: All Enrollees, Stakeholders, and Providers Cham Trowell, UM Director Date: May 10, 2016 Subject: Medicaid Funded Services Plan benefit changes, State Funded
Clinical Communication Bulletin 007 To: From: All Enrollees, Stakeholders, and Providers Cham Trowell, UM Director Date: May 10, 2016 Subject: Medicaid Funded Services Plan benefit changes, State Funded
What Did Your PEPPER Tell CMS?
 What Did Your PEPPER Tell CMS? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Matthew P. McGarvey, MBA Director of Business Development Speaker Bio:
What Did Your PEPPER Tell CMS? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Matthew P. McGarvey, MBA Director of Business Development Speaker Bio:
Improved Functioning for Persons with Schizophrenia: DLA-20 and Wellness Tools
 Improved Functioning for Persons with Schizophrenia: DLA-20 and Wellness Tools National Council for Community Behavioral Healthcare Open and close your control panel Join audio: Choose Mic & Speakers to
Improved Functioning for Persons with Schizophrenia: DLA-20 and Wellness Tools National Council for Community Behavioral Healthcare Open and close your control panel Join audio: Choose Mic & Speakers to
The Joint Commission On-Site Survey Process
 The Joint Commission On-Site Survey Process December 7, 2010 Behavioral Health Care Accreditation Team Mary Cesare-Murphy, Ph.D. Executive Director David Wadner, PhD Field Director Peggy Lavin, LCSW Senior
The Joint Commission On-Site Survey Process December 7, 2010 Behavioral Health Care Accreditation Team Mary Cesare-Murphy, Ph.D. Executive Director David Wadner, PhD Field Director Peggy Lavin, LCSW Senior
2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL MEASURES REGISTRY ONLY
 Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL
Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL
Behavioral Health Specialty Services and Integrated Healthcare: Challenges and Opportunities
 Behavioral Health Specialty Services and Integrated Healthcare: Challenges and Opportunities Presented by: David Lloyd, Founder M.T.M. Services P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709
Behavioral Health Specialty Services and Integrated Healthcare: Challenges and Opportunities Presented by: David Lloyd, Founder M.T.M. Services P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709
A SUMMARY OF MEDICAID REQUIREMENTS AND RELATED COA STANDARDS
 A SUMMARY OF MEDICAID REQUIREMENTS AND RELATED COA STANDARDS This tool is intended to provide a broad overview of common Medicaid (MA) requirements in relation to COA s Standards. While there are specific
A SUMMARY OF MEDICAID REQUIREMENTS AND RELATED COA STANDARDS This tool is intended to provide a broad overview of common Medicaid (MA) requirements in relation to COA s Standards. While there are specific
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
Accountable Care Organizations (ACO) Draft 2011 Criteria
 Draft 2011 Criteria") 1 of 11 For Public Comment October 19 November 19, 2010 Comments due 5:00 pm EST Accountable Care Organizations (ACO) Draft 2011 Criteria Overview 2 of 11 Note: This publication is protected by U.S. and
1 of 11 For Public Comment October 19 November 19, 2010 Comments due 5:00 pm EST Accountable Care Organizations (ACO) Draft 2011 Criteria Overview 2 of 11 Note: This publication is protected by U.S. and
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
DRUG MEDI-CAL ORGANIZED DELIVERY SYSTEM (DMC-ODS) PERFORMANCE METRICS. (version 6/23/17)
 PERFORMANCE METRICS. (version 6/23/17)") 1 Access Enrollment information to include the number of DMC-ODS beneficiaries served in the DMC-ODS program Clients Served: 1. Number of DMC-ODS beneficiaries served (admissions) by the DMC- ODS County
1 Access Enrollment information to include the number of DMC-ODS beneficiaries served in the DMC-ODS program Clients Served: 1. Number of DMC-ODS beneficiaries served (admissions) by the DMC- ODS County
A Physician Led Comprehensive Coding Compliance Program: Datamining to Disciplinary Action Plans. Optimizing revenue from a compliance perspective
 A Physician Led Comprehensive Coding Compliance Program: Datamining to Disciplinary Action Plans Keith Ponitz, M.D. October 16,2012 Agenda Background Optimizing revenue from a compliance perspective Mitigate
A Physician Led Comprehensive Coding Compliance Program: Datamining to Disciplinary Action Plans Keith Ponitz, M.D. October 16,2012 Agenda Background Optimizing revenue from a compliance perspective Mitigate
Agenda. National Landscape. Background. Optimizing revenue from a compliance perspective. Mitigate the risk: Data mining and coding audits
 A Physician Led Comprehensive Coding Compliance Program: Datamining to Disciplinary Action Plans Keith Ponitz, M.D. October 16,2012 Agenda Background Optimizing revenue from a compliance perspective Mitigate
A Physician Led Comprehensive Coding Compliance Program: Datamining to Disciplinary Action Plans Keith Ponitz, M.D. October 16,2012 Agenda Background Optimizing revenue from a compliance perspective Mitigate
The North Carolina Mental Health and Substance Abuse Workforce
 The North Carolina Mental Health and Substance Abuse Workforce Erica Richman, PhD, MSW Erin Fraher, PhD, MPP & Katie Gaul, MA Program on Health Workforce Research & Policy Cecil G. Sheps Center for Health
The North Carolina Mental Health and Substance Abuse Workforce Erica Richman, PhD, MSW Erin Fraher, PhD, MPP & Katie Gaul, MA Program on Health Workforce Research & Policy Cecil G. Sheps Center for Health
AOPMHC STRATEGIC PLANNING 2018
 SERVICE AREA AND OVERVIEW EXECUTIVE SUMMARY Anderson-Oconee-Pickens Mental Health Center (AOP), established in 1962, serves the following counties: Anderson, Oconee and Pickens. Its catchment area has
SERVICE AREA AND OVERVIEW EXECUTIVE SUMMARY Anderson-Oconee-Pickens Mental Health Center (AOP), established in 1962, serves the following counties: Anderson, Oconee and Pickens. Its catchment area has
DRUG MEDI-CAL ORGANIZED DELIVERY SYSTEM (DMC-ODS) YEAR 1 PERFORMANCE METRICS (version 10/24/17)
 YEAR 1 PERFORMANCE METRICS (version 10/24/17)") 1 Access Enrollment information to include the number of DMC- ODS beneficiaries served in the DMC-ODS program Clients Served: 1. Number of DMC-ODS beneficiaries served (admissions) by the DMC- ODS County
1 Access Enrollment information to include the number of DMC- ODS beneficiaries served in the DMC-ODS program Clients Served: 1. Number of DMC-ODS beneficiaries served (admissions) by the DMC- ODS County
Patient-centered medical homes (PCMH): Eligible providers.
: Eligible providers.") ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
SALISH BEHAVIORAL HEALTH ORGANIZATION Utilization Management Plan FY
 SALISH BEHAVIORAL HEALTH ORGANIZATION Utilization Management Plan FY 2017-2018 Salish BHO Policies and Procedures The Salish Behavioral Health Organization (SBHO) Utilization Management (UM) Plan summarizes
SALISH BEHAVIORAL HEALTH ORGANIZATION Utilization Management Plan FY 2017-2018 Salish BHO Policies and Procedures The Salish Behavioral Health Organization (SBHO) Utilization Management (UM) Plan summarizes
Provider Frequently Asked Questions
 Provider Frequently Asked Questions Strengthening Clinical Processes Training CASE MANAGEMENT: Q1: Does Optum allow Case Managers to bill for services provided when the Member is not present? A1: Optum
Provider Frequently Asked Questions Strengthening Clinical Processes Training CASE MANAGEMENT: Q1: Does Optum allow Case Managers to bill for services provided when the Member is not present? A1: Optum
Central Ohio Primary Care (COPC) Spotlight on Innovation
 Spotlight on Innovation") Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Building a Smarter Healthcare System The IE s Role. Kristin H. Goin Service Consultant Children s Healthcare of Atlanta
 Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Success Through Synergy
 REGISTRATION FORM NC Council of Community Mental Health, Developmental Disabilities and Substance Abuse Programs 2012 2 June 18-19, 2012 2, Raleigh, NC REGISTRATION CUT OFF DATE IS June 8, 2012 after that
REGISTRATION FORM NC Council of Community Mental Health, Developmental Disabilities and Substance Abuse Programs 2012 2 June 18-19, 2012 2, Raleigh, NC REGISTRATION CUT OFF DATE IS June 8, 2012 after that
Productivity: New Care Team Model
 Productivity: New Care Team Model Hudson River HealthCare October 2006 Katherine Brieger, RD,CDE Hudson River HealthCare Hudson River: Harvesting Project Ideas for Spread Beacon 1998: Efficiency Orange
Productivity: New Care Team Model Hudson River HealthCare October 2006 Katherine Brieger, RD,CDE Hudson River HealthCare Hudson River: Harvesting Project Ideas for Spread Beacon 1998: Efficiency Orange
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
CPT Coding Changes in 2013: Billing, Reimbursement and IT
 CPT Coding Changes in 2013: Billing, Reimbursement and IT Texas Council of Community Centers Presented by: David R. Swann, MA, LCAS, CCS, LPC, NCC Senior Healthcare Integration Consultant Phone: 336-386-9801
CPT Coding Changes in 2013: Billing, Reimbursement and IT Texas Council of Community Centers Presented by: David R. Swann, MA, LCAS, CCS, LPC, NCC Senior Healthcare Integration Consultant Phone: 336-386-9801
Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services HANYS Solutions Patient-Centered Medical
 Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services 2017 HANYS Solutions Patient-Centered Medical Home Advisory Services Overview Current landscape Medical neighborhood Patient-Centered
Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services 2017 HANYS Solutions Patient-Centered Medical Home Advisory Services Overview Current landscape Medical neighborhood Patient-Centered
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
Documentation Training
 Welcome to Documentation Training Please sign in Put cell phones on silence/vibrate Find a seat and buckle up for the ride 1 Documentation Training Quality Improvement Program (408) 793-5894 www.sccmhd.org.
Welcome to Documentation Training Please sign in Put cell phones on silence/vibrate Find a seat and buckle up for the ride 1 Documentation Training Quality Improvement Program (408) 793-5894 www.sccmhd.org.
Peer and Electronic Record Review C 3.12
 WASATCH MENTAL HEALTH SERVICES SPECIAL SERVICE DISTRICT Peer and Electronic Record Review C 3.12 Purpose: The purpose of Wasatch Mental Health s (WMH) peer review program is to ensure the quality and sufficiency
WASATCH MENTAL HEALTH SERVICES SPECIAL SERVICE DISTRICT Peer and Electronic Record Review C 3.12 Purpose: The purpose of Wasatch Mental Health s (WMH) peer review program is to ensure the quality and sufficiency
2) The percentage of discharges for which the patient received follow-up within 7 days after
 The percentage of discharges for which the patient received follow-up within 7 days after") Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
August 8, :00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell
 August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
Medicaid Transformation Overview & Update. Kelly Crosbie, MSW, LCSW Project Lead Quality & Population Health Division of Health Benefits
 Medicaid Transformation Overview & Update Kelly Crosbie, MSW, LCSW Project Lead Quality & Population Health Division of Health Benefits IOM Policy Fellows: February 26, 2018 North Carolina s Vision for
Medicaid Transformation Overview & Update Kelly Crosbie, MSW, LCSW Project Lead Quality & Population Health Division of Health Benefits IOM Policy Fellows: February 26, 2018 North Carolina s Vision for
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Welcome to the Webinar!
 Welcome to the Webinar! We will begin the presentation shortly. Thank you for your patience. Attendees can access the presentation slides now at: http://www.mctac.org/page/events A recording of the event
Welcome to the Webinar! We will begin the presentation shortly. Thank you for your patience. Attendees can access the presentation slides now at: http://www.mctac.org/page/events A recording of the event
Medicaid 101: The Basics for Homeless Advocates
 Medicaid 101: The Basics for Homeless Advocates July 29, 2014 The Source for Housing Solutions Peggy Bailey CSH Senior Policy Advisor Getting Started Things to Remember: Medicaid Agency 1. Medicaid is
Medicaid 101: The Basics for Homeless Advocates July 29, 2014 The Source for Housing Solutions Peggy Bailey CSH Senior Policy Advisor Getting Started Things to Remember: Medicaid Agency 1. Medicaid is
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Medical Home Renovations: A Patient-centered Medical Home Case Study
 Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
THE CONFERENCE WHERE MEDICAL HOME NEIGHBORS TRANSFORM CARE DELIVERY
 THE CONFERENCE WHERE MEDICAL HOME NEIGHBORS TRANSFORM CARE DELIVERY An Official Conference by NCQA PCMH PATIENT-CENTERED MEDICAL HOME CONGRESS October 7-9, 2016 Chicago, IL pcmhcongress.com Developed by
THE CONFERENCE WHERE MEDICAL HOME NEIGHBORS TRANSFORM CARE DELIVERY An Official Conference by NCQA PCMH PATIENT-CENTERED MEDICAL HOME CONGRESS October 7-9, 2016 Chicago, IL pcmhcongress.com Developed by
Medicare Cost Reporting and PPS FFY 2015 Proposed Rule Why it Still Matters. Glenn Grigsby, CPA OACHC 2014 Annual Spring Conference March 11, 2014
 Medicare Cost Reporting and PPS FFY 2015 Proposed Rule Why it Still Matters Glenn Grigsby, CPA OACHC 2014 Annual Spring Conference March 11, 2014 Agenda Medicare cost report myths Common cost reporting
Medicare Cost Reporting and PPS FFY 2015 Proposed Rule Why it Still Matters Glenn Grigsby, CPA OACHC 2014 Annual Spring Conference March 11, 2014 Agenda Medicare cost report myths Common cost reporting
Patient Centered Medical Home Foundation for Accountable Care
 Patient Centered Medical Home Foundation for Accountable Care Outline of Presentation History and tenants of the patient-centered care and PCMH model Defining, measuring, recognizing, and evaluating the
Patient Centered Medical Home Foundation for Accountable Care Outline of Presentation History and tenants of the patient-centered care and PCMH model Defining, measuring, recognizing, and evaluating the
Quality Assurance & Data Quality
 Quality Assurance & Data Quality Barbara Ritter, Michigan Statewide HMIS & Spokane WA. Tom Albanese, Community Shelter Board, Columbus/Franklin County OH. September 14th and 15th, 2004 Chicago, IL Sponsored
Quality Assurance & Data Quality Barbara Ritter, Michigan Statewide HMIS & Spokane WA. Tom Albanese, Community Shelter Board, Columbus/Franklin County OH. September 14th and 15th, 2004 Chicago, IL Sponsored
Quality Management and Improvement 2016 Year-end Report
 Quality Management and Improvement Table of Contents Introduction... 4 Scope of Activities...5 Patient Safety...6 Utilization Management Quality Activities Clinical Activities... 7 Timeliness of Utilization
Quality Management and Improvement Table of Contents Introduction... 4 Scope of Activities...5 Patient Safety...6 Utilization Management Quality Activities Clinical Activities... 7 Timeliness of Utilization
Providing and Documenting Medically Necessary Behavioral Health Services
 Providing and Documenting Medically Necessary Behavioral Health Services Presented by: David Reed, Office Chief, Division of Behavioral Health and Recovery Marc Bollinger, LISCW, CEO, Great Rivers BHO
Providing and Documenting Medically Necessary Behavioral Health Services Presented by: David Reed, Office Chief, Division of Behavioral Health and Recovery Marc Bollinger, LISCW, CEO, Great Rivers BHO
Courtney Reynolds, M.A., M.S.S.A., LSW 1 Minzhi Ye, MA 1 Farida K. Ejaz, Ph.D., LISW-S 1 Raymond Kirsch, B. A. 2 Miriam Rose, M.
 Nothing Beats Good Data: Importance of an Electronic Database to Conduct a Needs Assessment and Track Service Use Among Patients At Risk of Self-Neglect Courtney Reynolds, M.A., M.S.S.A., LSW 1 Minzhi
Nothing Beats Good Data: Importance of an Electronic Database to Conduct a Needs Assessment and Track Service Use Among Patients At Risk of Self-Neglect Courtney Reynolds, M.A., M.S.S.A., LSW 1 Minzhi
a. The financial implications have been estimated in the table below, see Unfunded Mandates.
 BACB code of ethics to which BCBAs must subscribe prevents them from validating or supporting this position in the field. Imagine sending your child to Sent: Friday, August 10, 2018 10:54 AM vg 1 4 2Q18
BACB code of ethics to which BCBAs must subscribe prevents them from validating or supporting this position in the field. Imagine sending your child to Sent: Friday, August 10, 2018 10:54 AM vg 1 4 2Q18
Home Infusion (elective)
") Home Infusion (elective) PGY2 - Health-System Pharmacy Administration (87405) Faculty: Slade, Jamie; Tyler, Linda S. Site: University of Utah Hospitals Clinics Status: Active Not Required Description:
Home Infusion (elective) PGY2 - Health-System Pharmacy Administration (87405) Faculty: Slade, Jamie; Tyler, Linda S. Site: University of Utah Hospitals Clinics Status: Active Not Required Description:
KATHLEEN KEEFE RAFFEL
 KATHLEEN KEEFE RAFFEL kkraffel@usfca.edu KEY KNOWLEDGE AND SKILL AREAS Patient & health education Medical & gerontological social work Staff training & development Curriculum & instructional design Bio-ethics
KATHLEEN KEEFE RAFFEL kkraffel@usfca.edu KEY KNOWLEDGE AND SKILL AREAS Patient & health education Medical & gerontological social work Staff training & development Curriculum & instructional design Bio-ethics
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #51 Navigating Health Care Reform: Creating a Road Map for Success Thursday, August 8 8:15 to 9:45 a.m. Regency
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #51 Navigating Health Care Reform: Creating a Road Map for Success Thursday, August 8 8:15 to 9:45 a.m. Regency
Perfecting Emergency Department Operations
 These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
Critical Access Hospital Quality
 Critical Access Hospital Quality Current Performance and the Development of Relevant Measures Ira Moscovice, PhD Mayo Professor & Head Division of Health Policy & Management School of Public Health, University
Critical Access Hospital Quality Current Performance and the Development of Relevant Measures Ira Moscovice, PhD Mayo Professor & Head Division of Health Policy & Management School of Public Health, University
TYPE OF CALL QUESTION ANSWER. from the CAQH database for the application process?
 Can Sandhills Center pull information from the CAQH database for the application process? This is a brand new credentialing application process, the entire application must be completed. Are there any
Can Sandhills Center pull information from the CAQH database for the application process? This is a brand new credentialing application process, the entire application must be completed. Are there any
IHI Change Conference: Leading at the Edge Informational Call
 September 19, 2017 1:00 PM 2:00 PM ET IHI Change Conference: Leading at the Edge Informational Call Fall 2017 WebEx Quick Reference 2 Please use chat to All Participants for discussion & questions Raise
September 19, 2017 1:00 PM 2:00 PM ET IHI Change Conference: Leading at the Edge Informational Call Fall 2017 WebEx Quick Reference 2 Please use chat to All Participants for discussion & questions Raise
9. Additional Information
 9. Additional Information 9.1 Subcontractors and Participating Practitioners KP defines a subcontractor as an individual participating practitioner, participating practitioner group, or any other entity
9. Additional Information 9.1 Subcontractors and Participating Practitioners KP defines a subcontractor as an individual participating practitioner, participating practitioner group, or any other entity
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Specialty Behavioral Health and Integrated Services
 Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Creating the Collaborative Care Team
 Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS HOME-BASED SERVICES
 NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS HOME-BASED SERVICES Provider will be in compliance with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS HOME-BASED SERVICES Provider will be in compliance with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
Alternative payment model to meet the needs of stakeholders in a community & school-based behavioral health service
 Alternative payment model to meet the needs of stakeholders in a community & school-based behavioral health service September 30, 2016 1:55-2:55 PM Learning Objectives Differentiate among payment models
Alternative payment model to meet the needs of stakeholders in a community & school-based behavioral health service September 30, 2016 1:55-2:55 PM Learning Objectives Differentiate among payment models
Boosting Your Bottom Line
 Boosting Your Bottom Line Making More Money for Clinics Lisa Clark, MBA NYS Office of Mental Health 7/26/16 Partners in CTAC and MCTAC include: Agenda Introduction Review of Revenue Maximization Basics
Boosting Your Bottom Line Making More Money for Clinics Lisa Clark, MBA NYS Office of Mental Health 7/26/16 Partners in CTAC and MCTAC include: Agenda Introduction Review of Revenue Maximization Basics
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT
 NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT Provider will comply with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT Provider will comply with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
Feedback Readiness Index and Fidelity Measure (FRIFM) and Instructions
 and Instructions") Feedback Readiness Index and Fidelity Measure (FRIFM) and Instructions The Scott D. Miller, Co-Founder, ICCE Bob Bertolino and Scott D. Miller, Series Editors for ICCE Manuals The ICCE Manuals on FIT were
Feedback Readiness Index and Fidelity Measure (FRIFM) and Instructions The Scott D. Miller, Co-Founder, ICCE Bob Bertolino and Scott D. Miller, Series Editors for ICCE Manuals The ICCE Manuals on FIT were
NCQA PCMH 2017 Standard Two 4/11/18. 6 PCMH Concepts within the standards
 Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Appendix 6. PCMH 2014 Summary of Changes
 Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Quality Improvement Work Plan
 NEVADA County Behavioral Health Quality Improvement Work Plan Mental Health and Substance Use Disorder Services Fiscal Year 2017-2018 Table of Contents I. Quality Improvement Program Overview...1 A. QI
NEVADA County Behavioral Health Quality Improvement Work Plan Mental Health and Substance Use Disorder Services Fiscal Year 2017-2018 Table of Contents I. Quality Improvement Program Overview...1 A. QI
NCQA PCMH 2017 Standards Intro 3/29/18. 6 PCMH Concepts within the standards
 Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Opportunities for those who stress Compliance at the Start
 Opportunities for those who stress Compliance at the Start Current Medicaid Audit Environment Risk Areas Service Content Medical Necessity Facility designation Documentation Copyright: Mary Thornton &
Opportunities for those who stress Compliance at the Start Current Medicaid Audit Environment Risk Areas Service Content Medical Necessity Facility designation Documentation Copyright: Mary Thornton &
Therapies (e.g., physical, occupational and speech) Medical social worker (MSW) 3328ALL0118-F 1
 Medical social worker (MSW) 3328ALL0118-F 1") 1. Q: Why is Humana implementing this utilization management (UM) program? A: Humana is implementing this program to help coordinate home health care for its Medicare Advantage members in Oklahoma and
1. Q: Why is Humana implementing this utilization management (UM) program? A: Humana is implementing this program to help coordinate home health care for its Medicare Advantage members in Oklahoma and
Outpatient Behavioral Health Basics 1
 6/6/2018 1 Outpatient Behavioral Health Basics 2018 Spring Workshop 1 Description: This class will review the SoonerCare Outpatient Behavioral Health Program. It will include an overview of commonly asked
6/6/2018 1 Outpatient Behavioral Health Basics 2018 Spring Workshop 1 Description: This class will review the SoonerCare Outpatient Behavioral Health Program. It will include an overview of commonly asked
Agenda STATE OF TENNESSEE 12/7/2016
 STATE OF TENNESSEE Tennessee Health Link: Practice Transformation Training 12/14/2016 Agenda Overview of Tennessee Health Link Partnership between HCFA, MCOs, Navigant and Practices Introduction to Navigant
STATE OF TENNESSEE Tennessee Health Link: Practice Transformation Training 12/14/2016 Agenda Overview of Tennessee Health Link Partnership between HCFA, MCOs, Navigant and Practices Introduction to Navigant
Data Shows Rural Hospitals At Risk Without Special Attention from Lawmakers
 Data Shows Rural Hospitals At Risk Without Special Attention from Lawmakers As Affordable Care Act Faces Uncertainty in America s Healthcare Future, Rural Hospitals Barely Hang On Compared to Urban Hospital
Data Shows Rural Hospitals At Risk Without Special Attention from Lawmakers As Affordable Care Act Faces Uncertainty in America s Healthcare Future, Rural Hospitals Barely Hang On Compared to Urban Hospital
Evaluation of Telestroke Services
 Evaluation of Telestroke Services 2013 Telestroke Summit Heart and Stroke Foundation of New Brunswick and the Canadian Stroke Network Dr. Patrice Lindsay Director Best Practices and Performance, Stroke
Evaluation of Telestroke Services 2013 Telestroke Summit Heart and Stroke Foundation of New Brunswick and the Canadian Stroke Network Dr. Patrice Lindsay Director Best Practices and Performance, Stroke
Statewide Behavioral Health and Primary Care Integration Implementation: Challenges and Successes in Missouri
 Session # D5a Statewide Behavioral Health and Primary Care Integration Implementation: Challenges and Successes in Missouri Ronald B. Margolis, PhD, CEO St. Louis Behavioral Medicine Institute Dawn Prentice,
Session # D5a Statewide Behavioral Health and Primary Care Integration Implementation: Challenges and Successes in Missouri Ronald B. Margolis, PhD, CEO St. Louis Behavioral Medicine Institute Dawn Prentice,
Healthcare Effectiveness Data and Information Set (HEDIS)
") Healthcare Effectiveness Data and Information Set (HEDIS) IlliniCare Health is a proud holder of NCQA accreditation as a managed behavioral health organization (MBHO) and prioritizes best in class performance
Healthcare Effectiveness Data and Information Set (HEDIS) IlliniCare Health is a proud holder of NCQA accreditation as a managed behavioral health organization (MBHO) and prioritizes best in class performance
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff {x} Administration { } Community Services {x} Secure Facilities I.
 GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff {x} Administration { } Community Services {x} Secure Facilities Chapter 12: Subject: QUALITY Attachments: A- Corrective Action Plan
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff {x} Administration { } Community Services {x} Secure Facilities Chapter 12: Subject: QUALITY Attachments: A- Corrective Action Plan
Physician/Hospital Integration: Challenges and Opportunities for Small and Rural Hospitals
 Physician/Hospital Integration: Challenges and Opportunities for Small and Rural Hospitals Small and Rural Hospital Conference Charlotte, NC November 12, 2013 Facilitated by: Marc D. Halley, MBA President
Physician/Hospital Integration: Challenges and Opportunities for Small and Rural Hospitals Small and Rural Hospital Conference Charlotte, NC November 12, 2013 Facilitated by: Marc D. Halley, MBA President
West Virginia Department of Health and Human Resources Bureau for Children and Families. Funding Announcement for Functional Family Therapy
 West Virginia Department of Health and Human Resources Bureau for Children and Families Funding Announcement for Functional Family Therapy Functional Family Therapy Funding Announcement Contents I. Introduction...3
West Virginia Department of Health and Human Resources Bureau for Children and Families Funding Announcement for Functional Family Therapy Functional Family Therapy Funding Announcement Contents I. Introduction...3