Improving Clinical Flow ECHO Collaborative Change Package
|
|
|
- Warren Tucker
- 6 years ago
- Views:
Transcription
1
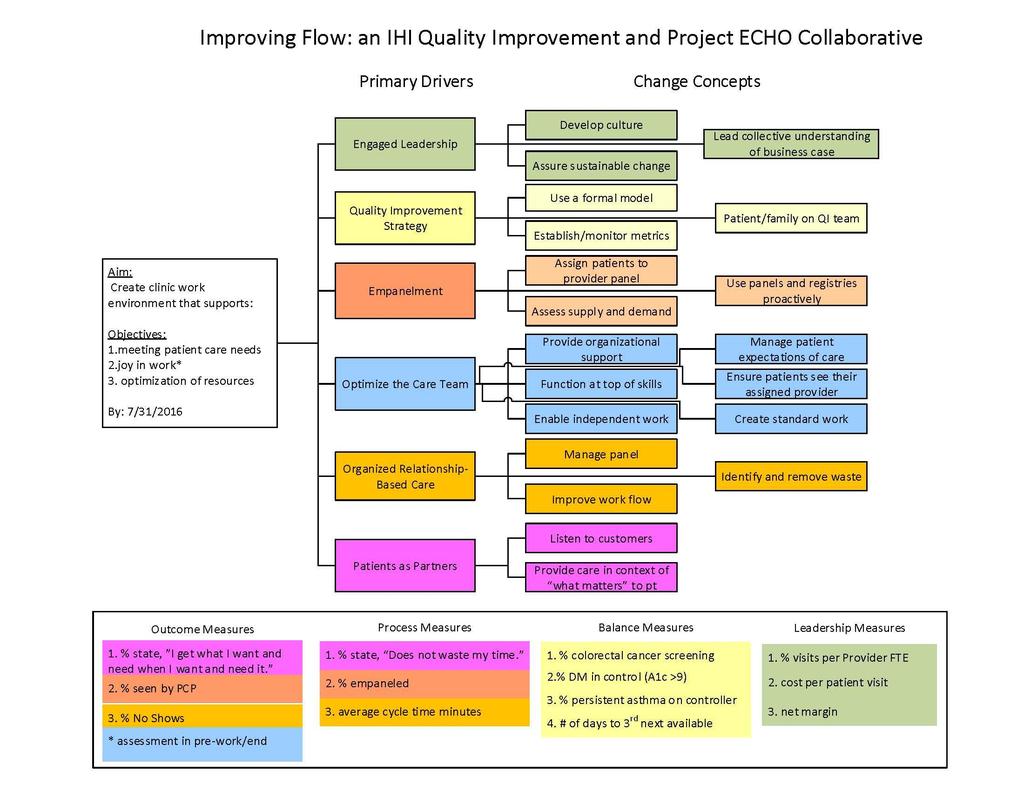
2 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk about the rationale and importance for change Ensure productive dialogue and decision making within team to foster engagement and alignment Build the practice s values on creating a team-based and patient-centered culture into processes for staff hiring and training Explore understanding of a change, importance of a change, and confidence to make the change when working with staff, when making decisions, and when resistance arises Use active listening to gain deeper understanding of the successes, challenges, barriers to change and as a response to resistance Attend team meeting 2x month Do 2 walk-arounds per week asking 5 Brief Questions Schedule protected team time of 1 hour per week for QI Schedule day-to-day leader for 1 hour per day for QI Make Project ECHO aim and team update a 5-minute standing agenda item for every meeting Talk no more than 10% of time in next encounter with staff person Hold discussions among groups within the organization about the changes, surface the successes and challenges Hold monthly review meetings
3 Ensure sustainable change Lead the collective understanding of the business case Ensure key staff have protected time beyond direct patient care to fully participate in transformation activities Clarify the vision, goals, and roles for change Sustain alignment among sponsors up, down, and across the organization through regular meetings about the change Continually review and clarify priorities Maintain ongoing review to ensure progress, sustain engagement and alignment, and address barriers and resource needs Provide clear structure and goals for each stage of improvement: testing, implementation, spread, and sustainability Create transparency around key revenue drivers and expenses Optimize opportunities to reduce expenses and enhance revenue while maintaining service quality Review and ensure the charge master is current Maximize point of service collections Understand the costs of turnover Staff work to the top of their licenses
4 Quality Improvement Strategy Choose and use a formal model for quality improvement (QI) Adopt a QI method and use it consistently to solve operational and clinical problems Create a shared language and culture for quality improvement Link QI training to role in improvement team Set clear improvement goals, expectations, and priorities Use the Model for Improvement for the Improving Clinical Flow ECHO Collaborative during team time and testing of ideas Identify improvement team day-to-day leader, team members, sponsor, and physician champion Compose Collaborative aim for the team Answer What are we trying to accomplish? for every change idea tested using a PDSA cycle Decide how team will know if the test succeeded or failed before the test begins Use clinic data to prioritize initial area of focus Empanelment Providers and care teams see their own patients, patients see their own Establish and monitor metrics to evaluate improvement efforts and outcomes, and ensure all staff members understand the metrics for success Assign all patients to a provider panel Specify which metrics are linked to QI efforts Regularly use data in meetings and communications Use data for improvement, not judgment Periodically review metrics and evaluate trends over time Optimize the use of health information technology for population management, creating huddle summary tools, registry monitoring, etc. Create systematic procedures and timelines for reporting data for use in the Collaborative such as leadership reviews, staff meetings, teleecho clinic Review and update panel assignments on a regular basis Engage providers and support staff in conversations about empanelment Assign a Panel Manager Evaluate panel size based on clinical FTE Create data collection plan for Collaborative data, test plan for ease of collection, and adjust as needed Establish a standing agenda item to review Collaborative data at the beginning of each team meeting, after the review of the Collaborative aim and the PDSAs; check for understanding Display run chart data in common staff areas Test which reports are most useful for patient care and the care teams Use the 4 cut method to empanel most patients Test various staff roles with the Panel Manager tasks Profile the diagnosis codes for a typical panel in your clinic Test processes to monitor patient panels and PCP assignments
5 providers and care teams Assess practice supply and demand, and balance patient load accordingly Use panel data and registries to proactively contact, educate, and track patients by disease status, risk status, selfmanagement status, community and family need Establish standard work for ongoing monitoring and adjustment Evaluate the supply of clinic appointments Evaluate demand for clinical care Manage demand variation proactively Create alternatives to face-to-face care such as or phone care Optimize patient involvement in care Segment patient panels based on needs Develop systems for follow up and support of care plan needs and selfmanagement goals Create actionable data aligned with care team roles and responsibilities to meet patient need Link education and periodic follow-up needs to patient portals as available Test the roles of each care team member in ensuring assignment to a PCP/Care Team Test max-packing a visit, meaning the patient gets all they need in the visit Test alternatives to office visits for tasks that do not need an office visit, such as filling out paperwork Test the RN role in helping to manage the daily care of patients with visits Test strategies to identify individuals with complex and higher needs, run reports on specific panel segments, obtain clinical staff input on patients who need enhanced care Test how to use registries or panel reports in daily huddles Test care team member roles for care plan follow-up, outreach, and care delivery Optimize the Care Team Establish and provide organizational support for care delivery teams accountable for the patient population/panel Commit to provide care in multidisciplinary teams Facilitate and support care team functioning Track and report organizational metrics by team as well as by provider Nurture an organizational culture that supports team-based care Facilitate trust among care team members Create contingency plans for events such as vacations, last minute changes in provider availability, known high or low demand times like flu season or summer Dedicate resources for team-building exercises to help team members develop trust and a coordinated way of working together Establish vacation plans and policies Plan for sudden provider absences Anticipate unexpected increases in demand Develop scripted language for common occurrences such as scheduling challenges, cancellations
6 Develop clear roles and responsibilities for every member of the care team so that they function at the top of their skill sets Periodically assess how staff members spend their time Expand the roles of members to take on tasks previously done by providers or not done at all Evaluate phone activity and subsequent workflows, patient flow, and information flow Redesign workflow processes and document the tasks, workflow, care team member role, materials, training, and support needed to create standard work Leverage messaging and tasking in the electronic health record (EHR) Test MA delivering preventive care per protocol (e.g. immunizations, ordering cancer screening, assessments such as monofilament Research state policies regarding licensure and scope of practice for various roles Test having administrative/front desk staff triage incoming calls, make appointments, fill out forms as much as possible Test using LPNs (as nursing scope allows) to triage patient phone calls or s and only refer to RNs or providers those patients requiring clinical assessment or decision making Test having medical records staff extract external data (lab, referrals) and enter into the electronic health record Test having centralized staff review registries and send exception reports to practice teams Test having front office, MAs, and nurses review registries (or exception reports) to identify patients needing services and call them. Train staff to conduct motivational interviewing, brief action planning, etc. For additional information and resources on this topic, visit: Encourage and enable staff to work independently Develop standard work processes for the delivery of common services and incorporate them into practice workflows and into the electronic health record Maximize the use of standing orders, which enable staff to independently perform key clinical tasks without having to involve the provider Test and refine standard work to reach the right protocol Review the board requirements for licensed positions Include when to ask for help Use daily or frequent huddles with all care team members (for resources on huddles, see les&=search)
7 Locate core team members in close proximity with each other Establish effective communication systems in the care team Use pre-visit planning to ensure all patient needs are identified and all needed information is available at time of visit Communicate among care delivery team throughout the day Use visual flags to smooth flow of the patient visit Establish regular all staff meetings Demonstrate documentation and billing Ensure annual review for all staff Retrain staff after review for additional information and resources on this topic Help patients understand what they can expect in a teambased model of care Ensure that patients are able to see their provider or care team whenever possible Name care teams or designate with a symbol or color Include team care as part of your practice description Co-locate team and the patient care areas for their panel Link patients to a provider and care team so both patients and provider/care team recognize each other as partners in care Train front desk and scheduling personnel regarding importance of provider/care team continuity for patients Provide scripts that promote continuity for staff to use when scheduling appointments Include care team name on business cards for patients Create marketing materials and website design Post pictures of the care teams in patient areas Create a script for staff to use to describe the teambased model with patients Provide a welcome to the practice orientation and information contains resources/tools such as: Patient Partner Packet; Patient Welcome Packet Ensure warm handoffs from Provider to individual care team members and the patient Create letters for new patients to introduce the team Update the practice website with team-based care information Leverage PCP assignment in EHR and test which staff member role is best able to verify PCP on each visit
8 Create standard work for roles, tasks, common processes Provide scripts to help patients understand organizational commitment to continuity Ensure IT systems/ehr have a prominent field to designate PCP and establish processes to ensure this field is filled in Create procedures for common processes Document processes, tasks, and roles in process maps and in a written process Ensure job descriptions, hiring procedures, training, and support are in line with standard work Create processes to update procedures periodically Understand variation in roles and processes and decide what level of variation is needed Organized, Relationship- Based Care This driver encompasses the work that teams do together on behalf of their patients (as opposed to the Manage the panel of patients to efficiently and effectively meet patient care needs Use planned care according to patient need Identify high-risk patients and ensure they are receiving appropriate care and case management services Use point-of-care reminders based on clinical guidelines Understand and manage practice systems external to the visit: calls, refill requests, forms, etc. Plan staff interactions with patients based on their identified needs Use pre-visit planning to ensure all patient needs are identified and all needed information is available at time of visit Test the best use of EHR reminders and staff roles More detailed information about improving workflow and removing waste is available on IHI s website
9 structural work of committing to and establishing strong care teams, which is the focus of the Optimize the Care Team driver) Improve workflow Use automation (e.g., EHR) to prompt for guideline-based care Remove or decrease steps in a process Do tasks in parallel Move steps in the process closer together Find and remove bottlenecks Synchronize patient, provider, and information Standardize rooms, equipment, patient flow, and information flow Ensure that all is ready (e.g., room, equipment, information) for the patient and provider interaction Complete work in real-time Identify and remove Minimize transportation of materials or waste information that is unnecessary Identify process steps that can be eliminated Match inventory to needs; keep stock levels that match actual demand Decrease motion (i.e., wasted time staff or providers spend looking in multiple places for an item or have added steps to accomplish a task Reduce rework due to operational mistakes that occur in the process (such as redrawing blood due to wrong order) Use visual cues such as colored cards for inventory of supplies Place printers and other equipment close to staff who use them regularly Test how to not batch calls for patient requests Ensure supply areas are cleaned and restocked in a standard way Re-supply or staffing is determined according to the actual demand of the patient or staff needs Draw the actual movement of staff and patients (staff and patient flow) in a spaghetti diagram; rearrange clinic and supplies to provide clear linear path Patients as Partners Listen to customers (patients and families) Create strategies to receive patient input on QI team, surveys, focus groups, other Obtain feedback from patients and families about their health care experience and use this information for quality improvement Open each team meeting with a patient story relating to the improvement work and PDSA tests Ask a patient advisor to do a 30-minute observation of the current process Involve a patient in teaching staff a communication technique that is being tested
10 Provide care within the context of what matters to the patient Include patients and families as advisors to or members of the QI team Utilize patient and family input to gain insight into specific areas (e.g., materials, patient care processes) Involve patients in developing their care plans: co-create care plans with patients Clarify which staff role will have standard work expectation to support patientdirected self-management goals Ensure support for diversity and the health literacy needs of patients Respect patient and family values and expressed needs Encourage patients to expand their role in decision making, health-related behaviors, and self-management Establish trusting relationships Communicate with patients in a culturally appropriate manner, in a language and at a level that the patient understands Assess the need for self-management support at every visit Ask a patient advisor to collect data by doing after-visit calls Ask patient advisors to draft 1 st version of a script for staff to use to describe the team-based model Hold focus groups to get input on a change that s being tested (e.g., how to assign the PCP, materials created to message who is on their care team) Begin the patient visit with a question (e.g., What do you need today? ) and listen Test MA role for Brief Action Planning
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Working at Top of License How do you reallocate work among a team? January 28, 2015
 Working at Top of License How do you reallocate work among a team? January 28, 2015 We Want To Hear From You! Type questions into the Questions Pane at any time during this presentation Patient-Centered
Working at Top of License How do you reallocate work among a team? January 28, 2015 We Want To Hear From You! Type questions into the Questions Pane at any time during this presentation Patient-Centered
SAFETY NET MEDICAL HOME INITIATIVE
 SAFETY NET MEDICAL HOME INITIATIVE Key Activities List Background and Description The Safety Net Medical Home Initiative (SNMHI) developed a framework The Change Concepts for Practice Transformation to
SAFETY NET MEDICAL HOME INITIATIVE Key Activities List Background and Description The Safety Net Medical Home Initiative (SNMHI) developed a framework The Change Concepts for Practice Transformation to
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A)
") SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
Productivity: New Care Team Model
 Productivity: New Care Team Model Hudson River HealthCare October 2006 Katherine Brieger, RD,CDE Hudson River HealthCare Hudson River: Harvesting Project Ideas for Spread Beacon 1998: Efficiency Orange
Productivity: New Care Team Model Hudson River HealthCare October 2006 Katherine Brieger, RD,CDE Hudson River HealthCare Hudson River: Harvesting Project Ideas for Spread Beacon 1998: Efficiency Orange
Team Based Care Assessment & Action Plan
 Team Based Care Assessment & Action Plan In the tables below, consider how fully each item has been implemented or functions in your practice. Circle the number that best reflects the completeness of implementation
Team Based Care Assessment & Action Plan In the tables below, consider how fully each item has been implemented or functions in your practice. Circle the number that best reflects the completeness of implementation
Presbyterian Healthcare Services Care Management
 Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
Michigan Primary Care Transformation Project. HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care
 Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Colorado Team-Based Care Initiative Change Package Tool Made possible with funding from the Colorado Health Foundation Contact: Alexia Eslan, JSI,
 Colorado Team-Based Care Initiative Change Package Tool Made possible with funding from the Colorado Health Foundation Contact: Alexia Eslan, JSI, aeslan@jsi.com CO Team-Based Care Initiative Change Package
Colorado Team-Based Care Initiative Change Package Tool Made possible with funding from the Colorado Health Foundation Contact: Alexia Eslan, JSI, aeslan@jsi.com CO Team-Based Care Initiative Change Package
Specialty practices and primary care practices join forces in providing patient centered medical care
 Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
HIT Innovations to Build an Empowering and Learning Culture March 2, 2016
 HIT Innovations to Build an Empowering and Learning Culture March 2, 2016 Jignesh Sheth, MD, Senior Vice President for Clinical Operations Courtney Dempsey, Clinical Innovation Specialist Conflict of Interest
HIT Innovations to Build an Empowering and Learning Culture March 2, 2016 Jignesh Sheth, MD, Senior Vice President for Clinical Operations Courtney Dempsey, Clinical Innovation Specialist Conflict of Interest
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
Joy At Work - BellinHealth and HealthPartners
 Joy At Work - BellinHealth and HealthPartners Restoring Joy in Practice through Team Based Care IHI December 2016 James Jerzak M.D. Kathy Kerscher Bellin Health Green Bay, Wisconsin 1 Agenda Crisis Emerging
Joy At Work - BellinHealth and HealthPartners Restoring Joy in Practice through Team Based Care IHI December 2016 James Jerzak M.D. Kathy Kerscher Bellin Health Green Bay, Wisconsin 1 Agenda Crisis Emerging
Timely and Productive Appointments: Are you Primed?
 The 26 th Annual IHI National Forum on Quality Improvement in Health Care December 7-10, 2014 Orlando Florida Timely and Productive Appointments: Are you Primed? Session D24/E24 HANDOUTS Mina Viscardi
The 26 th Annual IHI National Forum on Quality Improvement in Health Care December 7-10, 2014 Orlando Florida Timely and Productive Appointments: Are you Primed? Session D24/E24 HANDOUTS Mina Viscardi
Instructions for Completing the BHICCI Case Rate Readiness Assessment (CRRA) and Workplan
 and Workplan") Instructions for Completing the BHICCI Case Rate Readiness Assessment (CRRA) and Workplan IEHP intends to sustain integrated complex care through case rate funding to health care organizations/clinics
Instructions for Completing the BHICCI Case Rate Readiness Assessment (CRRA) and Workplan IEHP intends to sustain integrated complex care through case rate funding to health care organizations/clinics
Change is Good: You Go First
 Change is Good: You Go First Judith Schaefer Better Self Management of Diabetes Missouri Foundation for Health St. Louis, Missouri December 2 nd, 2009 Foundation s goals Support organizations that: Strengthen
Change is Good: You Go First Judith Schaefer Better Self Management of Diabetes Missouri Foundation for Health St. Louis, Missouri December 2 nd, 2009 Foundation s goals Support organizations that: Strengthen
Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017
 D21/E21 These presenters have nothing to disclose Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017 Session Objectives P2 Describe how Project ECHO
D21/E21 These presenters have nothing to disclose Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017 Session Objectives P2 Describe how Project ECHO
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
Completing the Specialty Practice Assessment Tool: Guide for Behavioral Health Organizations and Divisions
 Completing the Specialty Practice Assessment Tool: Guide for Behavioral Health Organizations and Divisions Instructions: Please find below guiding questions for behavioral health organizations or divisions
Completing the Specialty Practice Assessment Tool: Guide for Behavioral Health Organizations and Divisions Instructions: Please find below guiding questions for behavioral health organizations or divisions
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Patient Centered Medical Home
 Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
Telecare Services 7/19/2017
 Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Table of Contents for CCC Toolkit
 Section 0.2 Overview Table of Contents for CCC Toolkit This document lists and briefly describes all the tools in the CCC Toolkit in alphabetic order. Time needed: As needed Suggested other tools: How
Section 0.2 Overview Table of Contents for CCC Toolkit This document lists and briefly describes all the tools in the CCC Toolkit in alphabetic order. Time needed: As needed Suggested other tools: How
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, Mike Williams, MPH/HSA The Abaris Group
 NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
POPULATION HEALTH LEARNING NETWORK 1
 In partnership with the California Health Care Foundation (CHCF) and the Blue Shield of California Foundation (BSCF), the Center for Care Innovations (CCI) is launching a Population Heath Learning Network
In partnership with the California Health Care Foundation (CHCF) and the Blue Shield of California Foundation (BSCF), the Center for Care Innovations (CCI) is launching a Population Heath Learning Network
Lean Six Sigma DMAIC Project (Example)
") Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices
 Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Building Coordinated, Patient Centered Care Management Teams
 Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Quality/Performance Improvement Fundamentals
 Quality/Performance Improvement Fundamentals What to do and how to do it Skill Building Session May 29, 2013 Pat Teske, RN,MHA pteske@cynosurehealth.org (661)755-5317 Today Agenda for Today Review ways
Quality/Performance Improvement Fundamentals What to do and how to do it Skill Building Session May 29, 2013 Pat Teske, RN,MHA pteske@cynosurehealth.org (661)755-5317 Today Agenda for Today Review ways
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Select the correct response and jot down your rationale for choosing the answer.
 UNC2 Practice Test 2 Select the correct response and jot down your rationale for choosing the answer. 1. If data are plotted over time, the resulting chart will be a (A) Run chart (B) Histogram (C) Pareto
UNC2 Practice Test 2 Select the correct response and jot down your rationale for choosing the answer. 1. If data are plotted over time, the resulting chart will be a (A) Run chart (B) Histogram (C) Pareto
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
Peer Review Example: Clinician 4 (Meets Expectations)
") Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
HEALTH CARE HOME ASSESSMENT (HCH-A)
") HEALTH CARE HOME ASSESSMENT (HCH-A) To be used by Health Care Homes involved in stage one implementation To asses practice readiness, monitor progress, and for evaluation purposes. Practice name Your name
HEALTH CARE HOME ASSESSMENT (HCH-A) To be used by Health Care Homes involved in stage one implementation To asses practice readiness, monitor progress, and for evaluation purposes. Practice name Your name
A S S E S S M E N T S
 A S S E S S M E N T S Community Design Assessment This process was developed to aid healthcare organizations in taking the pulse of their community prior to the start of capital improvement projects. A
A S S E S S M E N T S Community Design Assessment This process was developed to aid healthcare organizations in taking the pulse of their community prior to the start of capital improvement projects. A
2017 QUALITY PLAN WORK PLAN. Kaiser Permanente of Washington 2017 Quality Work Plan
 Kaiser Permanente of Washington 2017 Quality Work Plan 1 Achieve 2017 Quality Goals: Improve population health, the quality, safety and satisfaction of the customer experience while improving affordability
Kaiser Permanente of Washington 2017 Quality Work Plan 1 Achieve 2017 Quality Goals: Improve population health, the quality, safety and satisfaction of the customer experience while improving affordability
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework
 The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
Patient Centered Medical Home (PCMH)
") Patient Centered Medical Home (PCMH) The PCMH is a model of practice in which a Team of health professionals, guided by a personal physician, provides continuous, comprehensive, and coordinated care in
Patient Centered Medical Home (PCMH) The PCMH is a model of practice in which a Team of health professionals, guided by a personal physician, provides continuous, comprehensive, and coordinated care in
WHITE PAPER. Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice
 WHITE PAPER Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice Maximizing Pay-for-Performance Opportunities In today s
WHITE PAPER Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice Maximizing Pay-for-Performance Opportunities In today s
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Bright Spots in primary care
 Bright Spots in primary care A High- Performing Teaching Practice: Site Visit to Oregon Health & Science University s (OHSU) Family Medicine Clinic at Gabriel Park General information Tom Bodenheimer MD
Bright Spots in primary care A High- Performing Teaching Practice: Site Visit to Oregon Health & Science University s (OHSU) Family Medicine Clinic at Gabriel Park General information Tom Bodenheimer MD
Making the Case for Quality: How to Engage Clinical Staff in QI Activities
 Making the Case for Quality: How to Engage Clinical Staff in QI Activities Kelley Montague, RN Indiana Rural Health Association 2017 Annual Conference June 13-14, 2017 1 Objectives: Understand the importance
Making the Case for Quality: How to Engage Clinical Staff in QI Activities Kelley Montague, RN Indiana Rural Health Association 2017 Annual Conference June 13-14, 2017 1 Objectives: Understand the importance
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Care Management Policies
 POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Hospital Survey on Patient Safety Culture: Debrief and Action Planning
 Hospital Survey on Patient Safety Culture: Debrief and Action Planning August 7, 2018 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association 1 Three
Hospital Survey on Patient Safety Culture: Debrief and Action Planning August 7, 2018 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association 1 Three
Oregon Medical Group Team Medicine 3 April 2014
 Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Indiana Pressure Ulcer Reduction Initiative
 Indiana Pressure Ulcer Reduction Initiative Overview The IHI Breakthrough Series Collaborative is a systematic approach to healthcare quality improvement in which organizations and providers test and measure
Indiana Pressure Ulcer Reduction Initiative Overview The IHI Breakthrough Series Collaborative is a systematic approach to healthcare quality improvement in which organizations and providers test and measure
Primary Care Renewal. Building Successful Practices In The Era Of Accountability Creating Contagious Change
 Primary Care Renewal Building Successful Practices In The Era Of Accountability Creating Contagious Change David Labby, MD PhD Director of Clinical Support and Innovation May 27, 2011 CareOregon Our Vision:
Primary Care Renewal Building Successful Practices In The Era Of Accountability Creating Contagious Change David Labby, MD PhD Director of Clinical Support and Innovation May 27, 2011 CareOregon Our Vision:
Deeper Dive on Team Roles: Part I
 Deeper Dive on Team Roles: Part I Moderator: Diane Altman Dautoff, MSW, EdD, Sr. Consultant, Qualis Health Speakers: Ed Wagner, MD, MPH, Director (Emeritus), MacColl Institute for Healthcare Innovation
Deeper Dive on Team Roles: Part I Moderator: Diane Altman Dautoff, MSW, EdD, Sr. Consultant, Qualis Health Speakers: Ed Wagner, MD, MPH, Director (Emeritus), MacColl Institute for Healthcare Innovation
PCMH 2014 NCQA Standards and Guidelines
 PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Residency PCMH Longitudinal Curriculum Competency Based Goals and Objectives
 PCMH Ambulatory Care Curriculum Goals and Objectives The PCMH Ambulatory Care Curricular Competency Based Goals are: Access to Care Quality Improvement Population Management Team Based Care Integrated
PCMH Ambulatory Care Curriculum Goals and Objectives The PCMH Ambulatory Care Curricular Competency Based Goals are: Access to Care Quality Improvement Population Management Team Based Care Integrated
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Seamless transition from paper to AHS EHR
 Seamless transition from paper to AHS EHR February 15, 2013 Embrace the new world of healthcare Paula D. Peter Galen Certified EHR Consultant 5 yr. AHS and Galen Certified EEHR Consultant Project Manager
Seamless transition from paper to AHS EHR February 15, 2013 Embrace the new world of healthcare Paula D. Peter Galen Certified EHR Consultant 5 yr. AHS and Galen Certified EEHR Consultant Project Manager
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
Presentation Outline
 Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
SMARTCare Site Job Descriptions Site Physician Lead (Champion)
") SMARTCare Site Job Descriptions Site Physician Lead (Champion) Educational Requirements: Local (Site) Physician Champion Cardiovascular Fellow of the American College of Cardiology The Local Physician
SMARTCare Site Job Descriptions Site Physician Lead (Champion) Educational Requirements: Local (Site) Physician Champion Cardiovascular Fellow of the American College of Cardiology The Local Physician
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Appendix 1. Immediate Postpartum Long-Acting Reversible Contraception (LARC)
") Appendix 1. Immediate Postpartum Long-Acting Reversible Contraception (LARC) Program Implementation Guide: Exploration Stage Implementation Guide Overview Each stage of the implementation guide is organized
Appendix 1. Immediate Postpartum Long-Acting Reversible Contraception (LARC) Program Implementation Guide: Exploration Stage Implementation Guide Overview Each stage of the implementation guide is organized
ISAAC. Improving Sickle Cell Care for Adolescents and Adults in Chicago
 ISAAC Improving Sickle Cell Care for Adolescents and Adults in Chicago Improving Sickle Cell Care for Adolescents and Adults in Chicago (ISAAC) nal tools for sickle PROJECT BRIEF: ISAAC is a 6-year NIH/NHLBI-funded
ISAAC Improving Sickle Cell Care for Adolescents and Adults in Chicago Improving Sickle Cell Care for Adolescents and Adults in Chicago (ISAAC) nal tools for sickle PROJECT BRIEF: ISAAC is a 6-year NIH/NHLBI-funded
Patient Centred Medical Home Self-assessment (PCMH-A)
") Centred Medical Home Self-assessment (PCMH-A) Practice name: Your name: Date completed: For more information, contact: Colleen Watkins, NQPHN Chronic Care Team m: 0 0 e: info@nqpcmh.com.au w: nqpcmh.com.au
Centred Medical Home Self-assessment (PCMH-A) Practice name: Your name: Date completed: For more information, contact: Colleen Watkins, NQPHN Chronic Care Team m: 0 0 e: info@nqpcmh.com.au w: nqpcmh.com.au
Klamath Tribal Health & Family Services 3949 South 6 th Street Klamath Falls, OR 97603
 Klamath Tribal Health & Family Services 3949 South 6 th Street Klamath Falls, OR 97603 Phone: (541) 882-1487 or 1-800-552-6290 HR Fax: (541) 273-4564 OPEN 02/03/2017 UNTIL FILLED POSITION: RESPONSIBLE
Klamath Tribal Health & Family Services 3949 South 6 th Street Klamath Falls, OR 97603 Phone: (541) 882-1487 or 1-800-552-6290 HR Fax: (541) 273-4564 OPEN 02/03/2017 UNTIL FILLED POSITION: RESPONSIBLE
Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS) 1,2,3
 1,2,3") Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS),2,3 Individuals interested in using the PCRS in quality improvement work or research are free to do so. We request
Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS),2,3 Individuals interested in using the PCRS in quality improvement work or research are free to do so. We request
University of California, Davis Family Practice Center: Update 2014
 University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
Care Compact Guide Patient-Centered Specialty Care (PCSC) A Component of Medical Neighborhood Initiatives
 A Component of Medical Neighborhood Initiatives") Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
Transformational Patient Care Redesign Project
 Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
The New York State Health Center Controlled Network (NYS-HCCN)
") The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
HealthPartners and the Triple Aim. IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners
 HealthPartners and the Triple Aim IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners HealthPartners Not for profit, consumer governed Integrated care and financing
HealthPartners and the Triple Aim IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners HealthPartners Not for profit, consumer governed Integrated care and financing
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Draft. Public Health Strategic Plan. Douglas County, Oregon
 Public Health Strategic Plan Douglas County, Oregon Douglas County 2014 Letter from the Director Dear Colleagues It is with great enthusiasm that I present the Public Health Strategic Plan for 2014-2015.
Public Health Strategic Plan Douglas County, Oregon Douglas County 2014 Letter from the Director Dear Colleagues It is with great enthusiasm that I present the Public Health Strategic Plan for 2014-2015.
Measurement Strategy Overview
 Mobile Integrated Healthcare Program 911 Nurse Triage Measurement Strategy Overview Aim A clearly articulated goal statement that describes how much improvement by when and links all the specific outcome
Mobile Integrated Healthcare Program 911 Nurse Triage Measurement Strategy Overview Aim A clearly articulated goal statement that describes how much improvement by when and links all the specific outcome
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Practice Facilitators - Catalyst for Medical Home Transformation
 March 27, 2012 Practice Facilitators - Catalyst for Medical Home Transformation Lyndee Knox, PhD, Vanessa Nguyen, MPH, & Diana Traje, MPH Who we are 2 LA Net a Primary Care Practice Based Research & Resource
March 27, 2012 Practice Facilitators - Catalyst for Medical Home Transformation Lyndee Knox, PhD, Vanessa Nguyen, MPH, & Diana Traje, MPH Who we are 2 LA Net a Primary Care Practice Based Research & Resource
Accountable Care Atlas
 Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Revised for SIM Cohort 2, 2017
 Colorado State Innovation Model (SIM) Implementation and Milestone Reporting Summary Guide for Primary Care and Bi-directional Health Home Milestone Activities Revised for SIM Cohort 2, 2017 1 Table of
Colorado State Innovation Model (SIM) Implementation and Milestone Reporting Summary Guide for Primary Care and Bi-directional Health Home Milestone Activities Revised for SIM Cohort 2, 2017 1 Table of
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
PCMH Recognition Redesign: Annual Reporting Requirements to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018
 PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
ACCESS LARC INCREASING ACCESS TO IMMEDIATE POSTPARTUM LONG-ACTING REVERSIBLE CONTRACEPTION
 ACCESS LARC INCREASING ACCESS TO IMMEDIATE POSTPARTUM LONG-ACTING REVERSIBLE CONTRACEPTION Chapter One: Building a Successful Initiative General Quality Improvement Tips It takes a multidisciplinary team
ACCESS LARC INCREASING ACCESS TO IMMEDIATE POSTPARTUM LONG-ACTING REVERSIBLE CONTRACEPTION Chapter One: Building a Successful Initiative General Quality Improvement Tips It takes a multidisciplinary team
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
 Care Model May 12, 2016") update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards: