Hospitals and HealthCare Systems What you were Not taught in PA School
|
|
|
- Ada Burns
- 5 years ago
- Views:
Transcription
1 Hospitals and HealthCare Systems What you were Not taught in PA School Folusho Ogunfiditimi, DM, MPH, PA-C Administrative Director, Adult Clinical Services and Advanced Practice Providers Harper University Hospital/ Hutzel Women s Hospital Detroit Medical Center Tenet Health System fogunfid@dmc.org
2 Objectives Understand the roles of PA s Recruitment and Retention Onboarding and Orientation Clinical Practice Models Compensation Regulatory Standards and Compliance Productivity and Provider Enrollment Team membership/physician Collaboration Quality, Safety and Patient Satisfaction
3 Recruitment and Retention


4 History of Non Traditionally Trained Medical Practitioners.



5 Modern Advanced Practice Providers
6 From Graduation to Hire Average of 90 days Graduation-Board Certification Licensure Interviews Start early PA-Intern / Graduate PA Job Descriptions PA Recruiter PA Leader / Director Shadow opportunities
7 Graduate Physician Assistant is (GPA) is a recently graduated Physician Assistant who has met the academic and State of Michigan practice requirements for certification and Licensure as a Physician Assistant, but who has yet to obtain full organizational credentialing status with the DMC. In accordance with DMC bylaws all licensed physician assistants must undergo organizational credentialing and privileging prior to providing health care services to patients. To this effect the title Physician Assistant - Certified (PA-C) cannot be used until fully credentialed at the DMC and newly graduated PAs, awaiting credentialing will use the title Graduate Physician Assistants.
8 Credentialing Credentialed through Medical Affairs JC requirement Supervising Physician (employed) PA s must have an NPI and DEA License. (NPs as well) Scope of Practice and Core Competencies- Every specialty OPPE and FPPE
9 Job request from Hospital/Offic e Req Approval HR job posting /screening Recruiting NP/PA s Interviews Medical /dept /mlp office Temp Privileges Approval Approval Medical Affairs PA/NP office Exec Dir.- DMC MG notification DMC MG Recruiter Job offer And acceptanc e Approval Start Date HR Process Risk MGT Start NP / PA Training, EMR/CIS Third Party Enrollment and Billing NP/PA orientation Final Credentialin g Approval from Medical Affairs
10 Best Fit and Benefits Salaried vs Hourly Incentives, RVU based, Bonuses CME Sign-on Bonus vs. Retention Bonus Loan Repayment, Immigration Support STD, LTD, Vacation and Sick Leave More rigidity, Less flexibility
11 Onboarding and Orientation
12 Department Dynamics Medicine Medicine Service Medicine Subspecialties Surgery General Surgery Surgery Subspecialties Emergency Medicine Ambulatory Care Centers
13 Team Dynamics PA only NP only PA/NP only PA/NP and Residents PA/NP, Residents, SW, CM, PT/OT, Pharmacy
14 Staffing, Training, Governance Horizontal continuum of care GME, Research, Nursing Model Integrated Health Care Medical and Nursing teams, Advanced Practice Providers, Pharmacy, Administration etc.. Medical Model Human Resources Productivity, Quality, and Compensation Patient
15 Orientation None Formal 1 to 7days System, Hospital, Department, EMR Informal 30 days to Lifetime Checklist
16 Job request from Hospital/Offic e Req Approval HR job posting /screening Recruiting NP/PA s Interviews Medical /dept /mlp office Temp Privileges Approval Approval Medical Affairs PA/NP office Exec Dir.- DMC MG notification DMC MG Recruiter Job offer And acceptanc e Approval Start Date HR Process Risk MGT Start NP / PA Training, EMR/CIS Third Party Enrollment and Billing NP/PA orientation Final Credentialin g Approval from Medical Affairs
17 Medicine Roles Participate in all aspects and stages of care: Front Line: ED, Admissions, Admit H/Ps, Outpt, Inpt and Intra - Op Function in the Middle: keep the dialogue open and process running smoothly: LOS and UR management Inpt setting Follow up visits in outpt settings Patient and family education in person and by phone. Function as Closers : to finish the health care deal ; Transition of care
18 Surgical Role Pre Operative Role Clinical evaluation to include H/P s, Diagnostic evaluation, ancillary study review and medical clearances Operative Role First and Second Assist Robotic assistance Facilitating training and education of residents/students Post Operative Role Discharge management Post operative clinical evaluation, participate in the overall care of patients from presentation onward. Education of patients and families on robotic prostatectomy Develop and maintain social programs
19 Challenges Communication between APPs and MDs Scope of Practice and Supervisory Agreements Employed vs. Non Employed services Diversification of Services Integration with Academic Medicine
20 Opportunities Provision of continuous services to patients for MDs Quality Metrics LOS and Discharge Management Utilization and Resource Management Billing and Reimbursement Core Measures and EMR ICD 10
21 Clinical Practice Models
22 Horizontal Continuum of Care APRNs (NP, CNM CRNA) Education, research, training, care coordination, pt.assessment, evaluation, Dx Tx, Surgical Assist, Anesthesiology, Pre, Ante and Post care. PAs Enhanced Patient Outcomes and Patient Satisfaction
23 Types of Clinical Practice Ambulatory Practice Scribes Shared Side by Side Autonomous Inpatient Practice InterOperative Practice Combined Practice
24 Scribe Practice PATIENT (New and F/U) PA/NP Takes H/P Reports to MD (May or May not dictate) MD repeats all the work of PA/NP and dictates MD Bills at 100%
25 Scribe Practice Pros APP learns clinical practice, dictate etc. Acceptable teaching model for new graduates Cons Physician still has to do full history and exam Double work/single service/ Mild incentive for the MD/poor incentive for the APP Expensive utilization of Providers.
26 Shared Practice Patient (New and F/U) Additional Patients seen by MD PA/NP does complete E/M service, communicates to MD and dictates MD sees patient briefly, and discuses the MDM of the Service. MD bills at 100%
27 Shared Practice Pros Patient seen by two providers. Physician does not have to do full exam, Good incentive for the Physician Billing is done by Physician Meets CMS standards Good teaching and supervisory provisions Cons +/- Access Improvement Poor utilization of resources Low volume days= low productivity from all providers Mild incentive for the APP
28 Side by Side Practice PATIENT (F/U, +/- New) PATIENT (New, +/- F/u) MD may see New patient as a shared visit PA/NP does entire E/M service MD (in the same time) Constant Comm PA/NP bills at 85% if not seen by MD MD bills for his own pt... and may bill for PA/NP pt... if seen, at 100%
29 Side by Side Practice Pros Improved Access MD can see New, APP can see F/U Direct access to MD Easy conversion to Shared Practice CMS compliance with billing and supervisory regulations Good incentive for all providers Cons Not always suitable for New or Consults. Subject to over booking Billing and Reimbursement Limitations: Enrollment, 85% Understanding Legal and Compliance rules. Administrative Impact- Resources and Space
30 Autonomous Practice Pros Best model in ideal setting Improves Access for all patients Good incentive Downstream Feeders Provider is always busy. Safety net for last minute add-ons Productivity justifies administrative Impact. Cons Requires well experienced, confident APP MD may not be present for complex cases Patients may not see MD on 1 st visit Requires trust and good communication between APP and MD
31 Autonomous Practice MD provides indirect supervision and available for consultation if needed. MD free to be in clinic/or/procedure. MD gets downstream opportunities from PA/NP Patients (New and F/U) PA /NP does complete E/M, dictates and bills at 85%
32 Inpatient Utilization Pros Prompt/ Direct/Consistent Pt. access. Autonomous practice MDs gain confidence in APP Good learning opportunities Cons Poor billing / reimbursement Difficult Productivity measurements APPs may be subjected to scut work Requires well experienced, confident APP APP has limited view of Patients
33 Inpatient Utilization PA/NP Rounds alone or with team, writes Progress notes Discharges Pt. MD Rounds In- Patient RVU Formulas Initial Hosp Visit = 5.82/pt. Sub Hosp Visit = 2.07/pt. Inpatient Consult = 3.26/pt. Ave. 6 pt... daily = 22.3 RVU Approx. $550/day
34 OR Utilization and ROI Patient (Operation) Surgeon (MD) First Assist (PA/NP) Surgeon Bills at 100% and PA/NP Bills at 85% of First Assist Fee = 16% of the Surgeons Fee If MD fee for VIP = $12,000 PA/NP fee = $1920
35 Operating Room Utilization Pros Improved Revenue generation: Surgeon fee and First Assistant fee. Develop expertise in OR Comfort and Trust with MD. Standardization of procedures Good quality metrics Cons Can be monotonous Limited view of patient Need experienced provider Specific language is needed in GME programs Competition with GME trainees.
36 Combined Utilization Pros Maximum Utilization Jack of all Trades Experienced flexible provider Develop Trust and Confidence with MD APP. Maximum Access Maximum RVU generation. Cons Potential for APP burn out Master of None Competency measurement is critical Commands higher salary
37 Combined Practice Ambulatory Practice In-Patient Practice OR Practice Experienced PA/NP MD MD MD
38 Recommended Practice Pattern PA/NP New Grad (<1yr of clinical experience) Scribe Practice (not favored) Shared Practice (ideal for this group) Side by Side Practice (ideal for fast learner) Inpatient Utilization (ok for fast learner, but need good orientation), PA/NP (1 3 yrs. of clinical experience) Shared Practice Side by Side Practice Autonomous Practice Inpatient Utilization (Ongoing evaluation needed) OR Utilization (Direct supervision and training required) PA/NP (3-5yrs of clinical experience) All practice patterns, Limited direct supervision in OR PA/NP (>5 yrs. of clinical experience) All practices (Information is based on general limited level 3, 4 and 5 data. Individual providers may exhibit varying degree of competency)
39 Compensation and Provider Enrollment
40 Salary Models Salaried Exempt Employees No overtime Moonlighting Opportunity RVU Based compensation Incentive laden Salaries Productivity and Value provides leverage Market Analysis and Adjustments 92-96% of the percentile Critical to Fill positions
41 Provider Enrollenment Medicare and Medicaid Provider Enrollment Chain and Ownership system (PECOS) internet based CAQH Council for Affordable Quality Healthcare Non profit organization formed by various trade associations Streamline provider credentials with third party billers





42 Provider Enrollenment Third Party Billing Everyone is different
43 Regulatory Standards and Compliance
44 Law vs. Regulation Federal laws Federal agencies and VA Stark Laws Limits on practice delivery models with physicians State Laws vs Organizational Bylaws Be aware of laws affecting similar professions Billing and Reimbursement regulations
45 Physician Certification and 2 Midnight rule ACA Calls for all admissions to be certified by a Physician Verbal tuggle of war between Admitting Physician and Ordering Physician CMS 2 MN rule Observation vs Inpatient Admission
46 Hospital Billing Cost Report Employment relationships No Incident too in hospital based clinics Billing opportunties H/P, daytime and after hours Subsequent hospital care Consults, Procedures Surgery Discharges
47 Section 6407 of the ACA established a face-toface encounter requirement for certain items of DME. The law requires that a physician must document that a physician, nurse practitioner, physician assistant, or clinical nurse specialist has had a face-to-face encounter with the patient. The encounter must occur within the 6 months before the order is written for the DME.
48 Productivity, Value, Billing and Reimbursement
49 ROI- Scribe Practice 50% New (2.22 RVUs) 50% Returns (1.48 RVUs) 440/day rvu/pt. 1 FTE MD@ 1150/day FTE RVU s=27.75/day (approx. $685) Amount is based on Level 3 coding using 2011 Cf of $24.67
50 ROI- Shared Practice FTE 440/day 1.85 rvu/pt. 50% New 50% Returns MD@ 1150/day 1 FTE RVUs=46.25/day Approx.. $1141/day 40% Increase in RVU with 10 additional patients
51 ROI Side by Side Practice rvu/pt. (More Returns, less new) MD may see new pt... as shared MD Available for Direct Consultation rvu/pt. More New, less Return APP maintain individual schedule MD 440/day 1150/day RVU = 55.4/day Approx.. $1366/day 51
52 ROI - Autonomous Practice MD - Run separate clinic, OR, Research, etc. Revenue Generation dependent on daily activities rvu/pt. (New and F/U) 440/day RVU = MD Approx.. $675 +
53 ROI - Combined Practice Ambulatory Practice $625/day In-Patient Practice $550/day OR Practice $1920/day Experienced PA/NP ($440/day) MD MD MD
54 Inpatient Utilization PA/NP Rounds alone or with team, writes Progress notes Discharges Pt. MD Rounds In- Patient RVU Formulas Initial Hosp Visit = 5.82/pt. Sub Hosp Visit = 2.07/pt. Inpatient Consult = 3.26/pt. Ave. 6 pt... daily = 22.3 RVU Approx. $550/day
55 OR Utilization and ROI Patient (Operation) Surgeon (MD) First Assist (PA/NP) Surgeon Bills at 100% and PA/NP Bills at 85% of First Assist Fee = 16% of the Surgeons Fee If MD fee for VIP = $12,000 PA/NP fee = $1920
56 Time and Motion Study Observe and document the time spent by APPs on their daily responsibilities to determine the average amount of time spent on revenue generating and service value added activities. This data will allow the establishment of Service Value Units (SVUs), which will aid in quantifying an APPs productivity.
57 Methodology APPs were randomly selected based on primary location of work. (i.e. Inpatient, Outpatient, Emergency Department and OB) Use of Personal Digital Assistants (PDAs) PDAs were pre-populated with Current Procedure Terminology (CPT) coded defined services (AMA/CPT 2010) APPs recorded their location and main activity on the PDAs randomly every minutes
58 Results Inpatient Study Sample Population: 8 NPs/PAs participated 5 NPs and 3 PAs Departments: Acute Care Surgery (2), General Surgery (1), Hem/Onc (1), Nephrology (1), Neuro Surgery (1), Transplant Surgery (2) Collected 25 days of inpatient MLP activity data 23 weekdays (610 data points) 3 weekend days (119 data points)
59 Collection of Physiological Data 2% Telephone Consultation by NPP 3% Service Value 35.12% Other 3.29% Results Inpatient Study Lunch meeting 0.27% Cafeteria 3% Analysis of Clinical Data 8% Other Revenue Generating Activities 1% Business Meeting 1% Special Reports 3% Team Conferences 16% Procedure Documentation 1% Procedures 3% Charts for each area can be seen in the Appendix Subsequent Hospital Care 34% Discharge Management 16% Admission H/P 4% Post Op Care 3% Other Service Value Activities 3% Revenue Generating 61.59%
60 IP Activities Results Inpatient Study Occurrences Revenue Generating Service Value CPT 2010 Code Subsequent Hospital Care 245 x Discharge Management 116 x Admission H/P 30 x Post Op Care 22 x Based on procedure Procedures 21 x code Based on procedure code Procedure Documentation 6 x Other Revenue Generating Activities 9 x Team Conferences 114 x Analysis of Clinical Data 55 x Telephone Consultation by NPP 25 x Special Reports 24 x Collection of Physiological Data 12 x Business Meeting Council or Committee 7 x N/A Other Service Value Activities 19 x
61 Service Value 38.23% Collection of Physiological Data Team Conference 4% Other 2.73% Results Outpatient Study 1% Telephone Consultation - Patient Follow-Up 4% Other 1% Personal Time 1% Cafeteria 1% Student Precepting 2% Research Visit Documentation 3% Analysis of Clinical Data 18% Other Revenue Generating Activities 0.39% Collection of Physiological Data 1% Procedure 2% Outpatient Visit 32% Procedure Documentation 6% Other Service Value Activities 2% Revenue Generating 59.04% Outpatient Follow- Up 11% General Documentation 8%
62 Statistical Analysis 80.0% 70.0% 60.0% 50.0% 40.0% 30.0% 20.0% 10.0% 0.0% Inpatient Percent of Time Spent on RVU Activities 80.0% 70.0% 60.0% 50.0% 40.0% 30.0% 20.0% 10.0% 0.0% Outpatient Percent of Time Spent on RVU Activities Medicine Department Surgical Department Compared surgical and medicine departments (inpatient and outpatient combined) No difference found between surgical department activities (p = 0.205) Medicine departments are different (p<0.05)
63 Summary of Results Comparison of Activity Categories 70.00% 60.00% 50.00% 40.00% 30.00% 20.00% IP OP ED OB 10.00% 0.00% Revenue Generating Service Value Other
64 Simple Buisness Plan Outpatient 36 hrs. of pt. contact / week. (1 30min slots =14 pts./day, X 5 days = 72 pts. / wk. 5 wks. vacation and 5 days of CME time. 46 wk. /year = 3312 pts. 14pts/day (1.72) (5) (46) = 5538 RVU/yr Or $194,000 60% RVU generation = 3322 RVU/yr. Or $116,000 (approx salary + benefit) 64
65 Employee (PA) Engagement and Physician Collaboration
66 Engagement Opportunties Hospital committee participation From P/T to Medical Executive committee Utilization Resource committee Volunteer opportunities Physician Champion PA s know about PA s.. etc. Be Visible Do not presume that others know
67 Strategic Initiatives PCMH Ambulatory Care centers Centers of Excellence Service Line development Less Inpatient More Outpatient Transition of Care
68 Quality, Safety and Patient Satisfaction
69 Quality and Safety 2015 Reimbursement tied to value not volume (1-2% penalty) Quality Metrics Discharge Management Morbidity and Mortality Core Measures AMI, HF, Pneumonia, Stroke and SCIP
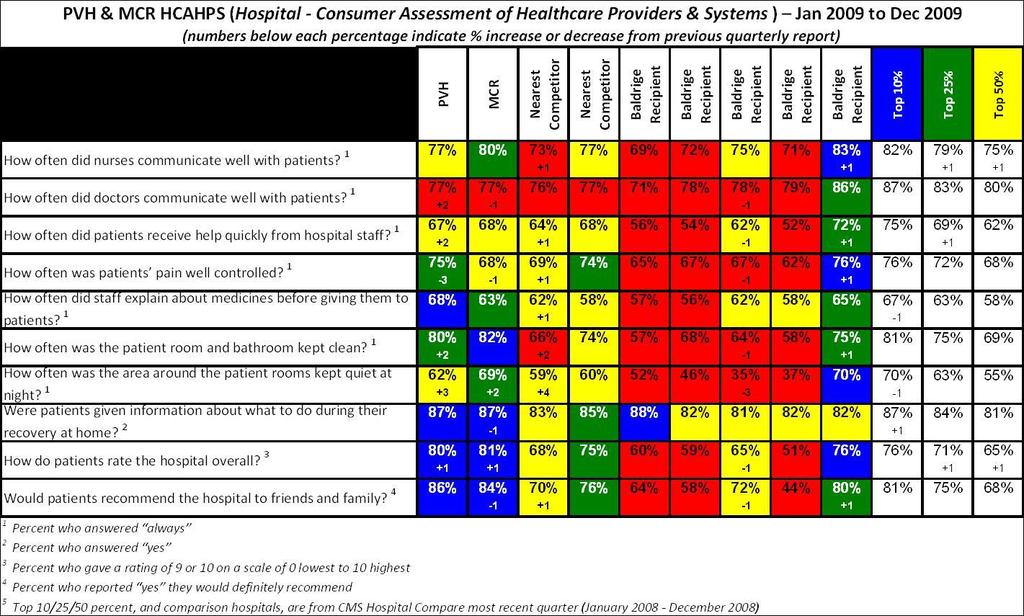
70 Patient Satisfaction HCAPS Hospital Consumer Survey of Healthcare Providers and systems 6 Domains Pain, Communication, Nursing, Hospitals systems 1 domain dedicated to Physicians/Providers NPI used to run reports
71
72 Summary PA s are extremely well positioned Organizational and Patient Throughput Transition of Inpatient care to Acute care Management Transition of Care Productivity tools Advocacy to Improve Laws ACA, Medicaid Expansion Ideas are needed to acieved maximum Patient Access, satisfaction and maintain quality measures
73 Questions
Successful Integration of Advanced Practice Providers into Hospitalist Practice
 Successful Integration of Advanced Practice Providers into Hospitalist Practice Tracy E. Cardin, ACNP, SFHM Population Over Age 65 Doubles by 2030 United States Population Projection Percent Growth from
Successful Integration of Advanced Practice Providers into Hospitalist Practice Tracy E. Cardin, ACNP, SFHM Population Over Age 65 Doubles by 2030 United States Population Projection Percent Growth from
NP or PA as Billing Provider
 NP or PA as Billing Provider Claire Agnew, CPA MBA CHC Vice President of Financial Operations Phoenix Children s Medical Group Phoenix Children s Hospital Arizona s only children s hospital recognized
NP or PA as Billing Provider Claire Agnew, CPA MBA CHC Vice President of Financial Operations Phoenix Children s Medical Group Phoenix Children s Hospital Arizona s only children s hospital recognized
PRACTICE MODELS FOR INPATIENT GI CONSULTATION
 PRACTICE MODELS FOR INPATIENT GI CONSULTATION JAMES S. LEAVITT, MD, FACG PRESIDENT GASTROHEALTH MIAMI, FLORIDA JLEAVITT@GASTROHEALTH.COM An expert is somebody who is more than 50 miles from home, has no
PRACTICE MODELS FOR INPATIENT GI CONSULTATION JAMES S. LEAVITT, MD, FACG PRESIDENT GASTROHEALTH MIAMI, FLORIDA JLEAVITT@GASTROHEALTH.COM An expert is somebody who is more than 50 miles from home, has no
ACADEMIC GROUP PRACTICE AND THE LEADERSHIP OF APRN S
 ACADEMIC GROUP PRACTICE AND THE LEADERSHIP OF APRN S Margaret Head, Chief Operating Officer/Chief Nursing Officer Susan Moseley Gent, Administrative Director Vanderbilt Medical Group March 10, 2012 With
ACADEMIC GROUP PRACTICE AND THE LEADERSHIP OF APRN S Margaret Head, Chief Operating Officer/Chief Nursing Officer Susan Moseley Gent, Administrative Director Vanderbilt Medical Group March 10, 2012 With
Non-Physician i Providers
 Non-Physician i Providers Colleen M. Schmitt, MD, MHS, FACG, FASGE Galen Medical Group Chattanooga, TN cschmitt7@comcast.net 1 To define the steps to develop ancillary infusion and histopathology services
Non-Physician i Providers Colleen M. Schmitt, MD, MHS, FACG, FASGE Galen Medical Group Chattanooga, TN cschmitt7@comcast.net 1 To define the steps to develop ancillary infusion and histopathology services
Aligning Advanced Practice Clinicians with New Care Models
 MGMA 2017 ANNUAL CONFERENCE OCT. 8-11 ANAHEIM, CA Aligning Advanced Practice Clinicians with New Care Models Trish Anen, RN, MBA, NEA-BC Debra Slater Principal, Sullivan, Cotter and Associates Principal,
MGMA 2017 ANNUAL CONFERENCE OCT. 8-11 ANAHEIM, CA Aligning Advanced Practice Clinicians with New Care Models Trish Anen, RN, MBA, NEA-BC Debra Slater Principal, Sullivan, Cotter and Associates Principal,
Are NPs and PAs Right for Your Practice?
 Society of Hospital Medicine Roundtable Are NPs and PAs Right for Your Practice? January 14, 2010 Michael L. Powe, Vice President Health Systems & Reimbursement Policy American Academy of Physician Assistants
Society of Hospital Medicine Roundtable Are NPs and PAs Right for Your Practice? January 14, 2010 Michael L. Powe, Vice President Health Systems & Reimbursement Policy American Academy of Physician Assistants
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
Shared and Incident To Billing of E/M Services in Radiation Oncology Updated November 2017
 ASTRO Guidance on Shared and Incident To Billing of Evaluation and Management Services in Radiation Oncology The Centers for Medicare and Medicaid Services (CMS) establishes Medicare policy for the payment
ASTRO Guidance on Shared and Incident To Billing of Evaluation and Management Services in Radiation Oncology The Centers for Medicare and Medicaid Services (CMS) establishes Medicare policy for the payment
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care
 Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
Embracing Optometry & Vision Plans: Creating a Successful MD/OD Business Model Part I
 Embracing Optometry & Vision Plans: Creating a Successful MD/OD Business Model Part I Disclosure I have no relevant financial relationships with the manufacturers of any commercial products and/or provider
Embracing Optometry & Vision Plans: Creating a Successful MD/OD Business Model Part I Disclosure I have no relevant financial relationships with the manufacturers of any commercial products and/or provider
Building the Eye Care Team: Successfully Integrating an Optometrist to Create a Successful and Ethical MD/OD Practice Model
 Building the Eye Care Team: Successfully Integrating an Optometrist to Create a Successful and Ethical MD/OD Practice Model JILL MAHER, MA, COE MAHER MEDICAL PRACTICE CONSULTING, LLC Disclosure I have
Building the Eye Care Team: Successfully Integrating an Optometrist to Create a Successful and Ethical MD/OD Practice Model JILL MAHER, MA, COE MAHER MEDICAL PRACTICE CONSULTING, LLC Disclosure I have
Introduction. Staffing to demand increases bottom line revenue for the facility through increased volume and throughput and elimination of waste.
 Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Challenges in Faculty Compensation
 Challenges in Faculty Compensation José Biller, MD, FACP, FAAN, FANA, FAHA Professor and Chairman Department of Neurology Loyola University Chicago Stritch School of Medicine Michael Budzynski Executive
Challenges in Faculty Compensation José Biller, MD, FACP, FAAN, FANA, FAHA Professor and Chairman Department of Neurology Loyola University Chicago Stritch School of Medicine Michael Budzynski Executive
Survey of Nurse Employers in California 2014
 Survey of Nurse Employers in California 2014 Conducted by UCSF Philip R. Lee Institute for Health Policy Studies, California Institute for Nursing & Health Care, and the Hospital Association of Southern
Survey of Nurse Employers in California 2014 Conducted by UCSF Philip R. Lee Institute for Health Policy Studies, California Institute for Nursing & Health Care, and the Hospital Association of Southern
Creating a Successful MD/OD Business Model
 Creating a Successful MD/OD Business Model JILL MAHER, MA, COE MAHER MEDICAL PRACTICE CONSULTING, LLC Objectives Challenges faced by Ophthalmology Practices What Can an Optometrist Bring to the Table?
Creating a Successful MD/OD Business Model JILL MAHER, MA, COE MAHER MEDICAL PRACTICE CONSULTING, LLC Objectives Challenges faced by Ophthalmology Practices What Can an Optometrist Bring to the Table?
3. Does the institution have a dedicated hospital-wide committee geared towards the improvement of laboratory test stewardship? a. Yes b.
 Laboratory Stewardship Checklist: Governance Leadership Commitment It is extremely important that the Laboratory Stewardship Committee is sanctioned by the hospital leadership. This may be recognized by
Laboratory Stewardship Checklist: Governance Leadership Commitment It is extremely important that the Laboratory Stewardship Committee is sanctioned by the hospital leadership. This may be recognized by
THE ROLE OF ADVANCED PRACTICE NURSES (APN) IN PROVIDING STROKE CARE IN STROKE BELT. What we know about APNs:
 IN PROVIDING STROKE CARE IN STROKE BELT. What we know about APNs:") THE ROLE OF ADVANCED PRACTICE NURSES (APN) IN PROVIDING STROKE CARE IN STROKE BELT Desiree Metzger-Cihelka, MSN, ARNP-C Cassie Lewis, DNP, ACNP-BC & Pat Lane, MBA, RN What we know about APNs: No shortage
THE ROLE OF ADVANCED PRACTICE NURSES (APN) IN PROVIDING STROKE CARE IN STROKE BELT Desiree Metzger-Cihelka, MSN, ARNP-C Cassie Lewis, DNP, ACNP-BC & Pat Lane, MBA, RN What we know about APNs: No shortage
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
8/31/2015. Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success. Vanderbilt University Medical Center
 Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
ACG GI Practice Toolbox: Adding Advanced Practice Providers to your Practice
 ACG GI Practice Toolbox: Adding Advanced Practice Providers to your Practice AUTHORS: Jaya R. Agrawal, MD, Hampshire Gastroenterology Associates, Florence, MA Wassem Juakiem, MD, Brooke Army Medical Center,
ACG GI Practice Toolbox: Adding Advanced Practice Providers to your Practice AUTHORS: Jaya R. Agrawal, MD, Hampshire Gastroenterology Associates, Florence, MA Wassem Juakiem, MD, Brooke Army Medical Center,
2012 Medical Staff Update 2011 CHALLENGING STANDARDS/NPSGS
 2012 Medical Staff Update Laurel McCourt, M.D. TJC Surveyor: Hospital and Office-Based Surgery Programs, and Special Survey Unit 2011 CHALLENGING STANDARDS/NPSGS 2 Standard/NPSG 2010 Non Compliance 3 2011
2012 Medical Staff Update Laurel McCourt, M.D. TJC Surveyor: Hospital and Office-Based Surgery Programs, and Special Survey Unit 2011 CHALLENGING STANDARDS/NPSGS 2 Standard/NPSG 2010 Non Compliance 3 2011
SCRIBES, SMAS AND INCIDENT T0
 SCRIBES, SMAS AND INCIDENT T0 Andrew R. McCulllough, MD In Transit Objectives Convince you to: Use Scribes Use Shared Medical Appointments Stop using Incident To The Facts of Life as a Physician Burnout
SCRIBES, SMAS AND INCIDENT T0 Andrew R. McCulllough, MD In Transit Objectives Convince you to: Use Scribes Use Shared Medical Appointments Stop using Incident To The Facts of Life as a Physician Burnout
Medical Staff Standards
 Medical Staff Standards CREDENTIALED PROVIDER QUALITY PROFILE Criteria is set by the medical staff at department level and approved by appropriate medical staff committees Monitoring is ongoing at the
Medical Staff Standards CREDENTIALED PROVIDER QUALITY PROFILE Criteria is set by the medical staff at department level and approved by appropriate medical staff committees Monitoring is ongoing at the
Executive Summary. Report. Physician Compensation and Production. Report MGMA Based on 2014 survey data. Medical Group Management Association
 Executive Summary Report MGMA 2015 Physician and Production Report Based on 2014 survey data Medical Group Management Association MGMA 2015 Physician and Production Report Medical Group Management Association
Executive Summary Report MGMA 2015 Physician and Production Report Based on 2014 survey data Medical Group Management Association MGMA 2015 Physician and Production Report Medical Group Management Association
THE ADVANCING ROLE OF ADVANCED PRACTICE CLINICIANS: COMPENSATION, DEVELOPMENT, & LEADERSHIP TRENDS
 THE ADVANCING ROLE OF ADVANCED PRACTICE CLINICIANS: COMPENSATION, DEVELOPMENT, & LEADERSHIP TRENDS INTRODUCTION The demand for Advanced Practice Clinicians (APCs) or Advanced Practice Providers (APPs)
THE ADVANCING ROLE OF ADVANCED PRACTICE CLINICIANS: COMPENSATION, DEVELOPMENT, & LEADERSHIP TRENDS INTRODUCTION The demand for Advanced Practice Clinicians (APCs) or Advanced Practice Providers (APPs)
1:35. NPP April Young Medical Consulting, LLC. Non-Physician Practitioner Coding and Billing. Disclaimer
 Non-Physician Practitioner Coding and Billing Jill Young - CPC, CEDC, CIMC, East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing. The information
Non-Physician Practitioner Coding and Billing Jill Young - CPC, CEDC, CIMC, East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing. The information
EMERGENCY DEPARTMENT CASE MANAGEMENT
 EMERGENCY DEPARTMENT CASE MANAGEMENT By Linda Sallee, Haley Rhodes, Sapna Patel, Cathleen Trespasz Healthcare consumers are becoming more empowered to have healthcare on their terms. With telemedicine,
EMERGENCY DEPARTMENT CASE MANAGEMENT By Linda Sallee, Haley Rhodes, Sapna Patel, Cathleen Trespasz Healthcare consumers are becoming more empowered to have healthcare on their terms. With telemedicine,
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals
 Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals DMC Harper- Hutzel Hospital The DMC is an 8 facility academic medical center Harper-Hutzel is
Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals DMC Harper- Hutzel Hospital The DMC is an 8 facility academic medical center Harper-Hutzel is
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
What is an Inpt & How to get it right. The Challenges of Coverage and Compliance Why is it so hard?
 What is an Inpt & How to get it right The Challenges of Coverage and Compliance Why is it so hard? 1 From the pt: AARP Jan-Feb 2010 issue Hospital Stays are Under Observation Ruth Way fell, was admitted
What is an Inpt & How to get it right The Challenges of Coverage and Compliance Why is it so hard? 1 From the pt: AARP Jan-Feb 2010 issue Hospital Stays are Under Observation Ruth Way fell, was admitted
California Rheumatology Physician Assistant. Located in the Palm Springs Area. Responsibilities include outpatient clinic visits. Monday thru Friday
 California Rheumatology Physician Assistant. Located in the Palm Springs Area. Responsibilities include outpatient clinic visits. Monday thru Friday schedule. Experience in Rheumatology preferred, but
California Rheumatology Physician Assistant. Located in the Palm Springs Area. Responsibilities include outpatient clinic visits. Monday thru Friday schedule. Experience in Rheumatology preferred, but
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment
 Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Northern Illinois Dermatology Physician Assistant Position. Located one hour North of Chicago,. Working with a well established medical/cosmetic
 Northern Illinois Dermatology Physician Assistant Position. Located one hour North of Chicago,. Working with a well established medical/cosmetic dermatology practice.. Responsibilities included clinical
Northern Illinois Dermatology Physician Assistant Position. Located one hour North of Chicago,. Working with a well established medical/cosmetic dermatology practice.. Responsibilities included clinical
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Benchmarking and Key Metrics Utilized by HSCT Administrators. Clint Divine, MBA, MSM Administrative Director, BMT
 Benchmarking and Key Metrics Utilized by HSCT Administrators Clint Divine, MBA, MSM Administrative Director, BMT 1 When you ve seen one HSCT program, you ve seen one HSCT program Although, there are many
Benchmarking and Key Metrics Utilized by HSCT Administrators Clint Divine, MBA, MSM Administrative Director, BMT 1 When you ve seen one HSCT program, you ve seen one HSCT program Although, there are many
Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model. Rome H. Walker MD February 28, 2008
 Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model Rome H. Walker MD February 28, 2008 A Concerted Effort Because the rewards are based on shared performance, the program is intended to create
Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model Rome H. Walker MD February 28, 2008 A Concerted Effort Because the rewards are based on shared performance, the program is intended to create
9/11/15. Reimbursement for Non- Physician Providers Real Life Practice Objectives
 Reimbursement for Non- Physician Providers Real Life Practice 2015 John F. Bishop, PA, CPC, CPMA, CGSC, CPRC AAPA National Chair Reimbursement and ICD-10 Work Groups Principle, John Bishop and Associates,
Reimbursement for Non- Physician Providers Real Life Practice 2015 John F. Bishop, PA, CPC, CPMA, CGSC, CPRC AAPA National Chair Reimbursement and ICD-10 Work Groups Principle, John Bishop and Associates,
Quality, Cost and Business Intelligence in Healthcare
 Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
APNP Hospitalist Program
 APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
2/28/2017 NO DISCLOSURES. K 1/Partner
 NO DISCLOSURES LaMon Norton NP Participant will recognize origin & role of Relative Value Unit (RVU) in coding and reimbursement. Participant will be able to link documentation points to coding and RVU
NO DISCLOSURES LaMon Norton NP Participant will recognize origin & role of Relative Value Unit (RVU) in coding and reimbursement. Participant will be able to link documentation points to coding and RVU
APNP Hospitalist Program Ministry Eagle River Memorial Hospital. Ministry Health Care. Program Objectives. Catholic Health Assembly June 23, 2014
 APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
1998 AAPA Census Report
 Section I. General Information about Respondents Table 1. Distribution of Respondents by Sex Respondents... 15716 100.0% Male... 7413 47.2% Female... 8303 52.8% Table 2. Distribution of Respondents by
Section I. General Information about Respondents Table 1. Distribution of Respondents by Sex Respondents... 15716 100.0% Male... 7413 47.2% Female... 8303 52.8% Table 2. Distribution of Respondents by
2001 AAPA Physician Assistant Census Report 1. Respondents % Male % Female %
 1 Section I. Personal Characteristics of Respondents* Table 1. Distribution of Respondents by Sex Respondents... 19786 100.0% Male... 8603 43.5% Female... 11183 56.5% Table 2. Distribution of Respondents
1 Section I. Personal Characteristics of Respondents* Table 1. Distribution of Respondents by Sex Respondents... 19786 100.0% Male... 8603 43.5% Female... 11183 56.5% Table 2. Distribution of Respondents
Cook County Health & Hospitals System. Special Board Meeting Friday, September 16, 2011
 Cook County Health & Hospitals System Preliminary i FY2012 Budget CCHHS Board of Directors Special Board Meeting Friday, September 16, 2011 Strategic Plan - VISION 2015 Mission To deliver integrated health
Cook County Health & Hospitals System Preliminary i FY2012 Budget CCHHS Board of Directors Special Board Meeting Friday, September 16, 2011 Strategic Plan - VISION 2015 Mission To deliver integrated health
The Healthcare Roundtable
 The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
Outpatient Observation Services
 Outpatient Observation Services Presented by: Gina Hobert, MBA, CHC, CPC-I, CPMA, CEMC, CRC Sr. Manager, Baker Newman Noyes Definition MCR Benefit Policy Manual, CMS 100-02, Chapter 6, 20.6 A. Outpatient
Outpatient Observation Services Presented by: Gina Hobert, MBA, CHC, CPC-I, CPMA, CEMC, CRC Sr. Manager, Baker Newman Noyes Definition MCR Benefit Policy Manual, CMS 100-02, Chapter 6, 20.6 A. Outpatient
Quality and Health Care Reform: How Do We Proceed?
 Quality and Health Care Reform: How Do We Proceed? Susan D. Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Dean of Clinical Affairs Quality and Patient Safety Associate Professor
Quality and Health Care Reform: How Do We Proceed? Susan D. Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Dean of Clinical Affairs Quality and Patient Safety Associate Professor
PHYSICIAN COMPENSATION MODELS IN A CHANGING ENVIRONMENT
 PHYSICIAN COMPENSATION MODELS IN A CHANGING ENVIRONMENT Ralph Llewellyn, CPA, CHFP Partner rllewellyn@eidebailly.com 701-239-8594 Michele Olivier, CPC, CPMA, Consultant molivier@eidebailly.com 303-586-8529
PHYSICIAN COMPENSATION MODELS IN A CHANGING ENVIRONMENT Ralph Llewellyn, CPA, CHFP Partner rllewellyn@eidebailly.com 701-239-8594 Michele Olivier, CPC, CPMA, Consultant molivier@eidebailly.com 303-586-8529
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
2018 MGMA PRACTICE OPERATIONS SURVEY
 (*Asterisks denote required questions) *Note: The Practice Profile must be completed before beginning any of the MGMA Surveys* Note: Multispecialty practices will be asked to break out data for each specialty
(*Asterisks denote required questions) *Note: The Practice Profile must be completed before beginning any of the MGMA Surveys* Note: Multispecialty practices will be asked to break out data for each specialty
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play?
 Programs: What Role Should Compliance Play?") Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
William J. Ennis D.O.,MBA University of Illinois at Chicago Professor Clinical Surgery, Chief Section wound healing and tissue repair
 William J. Ennis D.O.,MBA University of Illinois at Chicago Professor Clinical Surgery, Chief Section wound healing and tissue repair What are the revenue streams What are the expenses How does the hospital
William J. Ennis D.O.,MBA University of Illinois at Chicago Professor Clinical Surgery, Chief Section wound healing and tissue repair What are the revenue streams What are the expenses How does the hospital
Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid
 Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid Information posted on October 8, 2010 Effective for dates of service on or after December 1, 2010, the benefit criteria
Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid Information posted on October 8, 2010 Effective for dates of service on or after December 1, 2010, the benefit criteria
8/28/2014. Compliance and Practical Challenges When Using Scribes: Just What the Doctor Ordered? Objectives of the Presentation
 Compliance and Practical Challenges When Using Scribes: Just What the Doctor Ordered? Jerry Williamson MD. MJ. CHC. LHRM Objectives of the Presentation Definition of a Scribe Duties of a Scribe Regulatory
Compliance and Practical Challenges When Using Scribes: Just What the Doctor Ordered? Jerry Williamson MD. MJ. CHC. LHRM Objectives of the Presentation Definition of a Scribe Duties of a Scribe Regulatory
Provider-Based: What Is It?
 Compliance Risks for Provider-Based and Other Hospital-Based Provider Services 2015 HCCA Compliance Institute Presented by Regan E. Tankersley, Esq. Hall, Render, Killian, Heath & Lyman, P.C. Paul W. Kim,
Compliance Risks for Provider-Based and Other Hospital-Based Provider Services 2015 HCCA Compliance Institute Presented by Regan E. Tankersley, Esq. Hall, Render, Killian, Heath & Lyman, P.C. Paul W. Kim,
RossRichter.com, LLC
 RossRichter.com, LLC 203-461-8043 Specialists in Orthopaedic Recruiting fredperlman@rossrichter.org PLEASE POST FOR PHYSICIAN ASSISTANT STUDENTS: RossRichter.com, LLC was started in 1989 by health care
RossRichter.com, LLC 203-461-8043 Specialists in Orthopaedic Recruiting fredperlman@rossrichter.org PLEASE POST FOR PHYSICIAN ASSISTANT STUDENTS: RossRichter.com, LLC was started in 1989 by health care
5/13/2011. Background. Anesthesia Financials: An Unbalanced Equation. Understanding Anesthesia Financial Drivers
 Understanding Anesthesia Financial Drivers Becker s Hospital Review Annual Meeting, May 2011 Hugh Morgan, CMPE Director, Quality Assurance Background 17+ years healthcare management experience Military,
Understanding Anesthesia Financial Drivers Becker s Hospital Review Annual Meeting, May 2011 Hugh Morgan, CMPE Director, Quality Assurance Background 17+ years healthcare management experience Military,
Drug Medi-Cal Organized Delivery System
 Drug Medi-Cal Organized Delivery System Presented by Elizabeth Stanley-Salazar, MPH CMS Approval of DMC-ODS Waiver under ACA August 13, 2015 Pathway to Parity 2010 President Obama Signs the Affordable
Drug Medi-Cal Organized Delivery System Presented by Elizabeth Stanley-Salazar, MPH CMS Approval of DMC-ODS Waiver under ACA August 13, 2015 Pathway to Parity 2010 President Obama Signs the Affordable
3/28/2016. Evaluation and Management. Evaluation and Management Emerging Trends. Disclosures. Evaluation and Management The History
 Evaluation and Management Emerging Trends Peter Hollmann MD Past CPT Panel Chair Disclosures Ambassador for AMA CPT Member RBRVS Update Committee 2 Evaluation and Management The History Evaluation and
Evaluation and Management Emerging Trends Peter Hollmann MD Past CPT Panel Chair Disclosures Ambassador for AMA CPT Member RBRVS Update Committee 2 Evaluation and Management The History Evaluation and
RossRichter.com, LLC
 identifies opportunities that match your needs. The services we provide are FREE to Physician Assistants. Location ILLINOIS (Chicago Suburbs) Code IL 031618 Title Physician Assistant - Orthopaedics (Sports!)
identifies opportunities that match your needs. The services we provide are FREE to Physician Assistants. Location ILLINOIS (Chicago Suburbs) Code IL 031618 Title Physician Assistant - Orthopaedics (Sports!)
Important Billing Guidelines
 Important Billing Guidelines The guidelines contained herein are meant to assist GHP Family Participating Providers in billing appropriately for medically necessary services rendered to GHP Family Members.
Important Billing Guidelines The guidelines contained herein are meant to assist GHP Family Participating Providers in billing appropriately for medically necessary services rendered to GHP Family Members.
See the Time chapter for complete instructions on how to code using time as the controlling factor when selecting an E/M code.
 2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
ORTHOPEDIC JOINT REPLACEMENT SURGERY: PRESCOTT VALLEY, AZ
 ORTHOPEDIC JOINT REPLACEMENT SURGERY: PRESCOTT VALLEY, AZ Fellowship-trained orthopedic joint replacement doctor is hiring a second Physician Assistant. The position is primarily clinic-based with the
ORTHOPEDIC JOINT REPLACEMENT SURGERY: PRESCOTT VALLEY, AZ Fellowship-trained orthopedic joint replacement doctor is hiring a second Physician Assistant. The position is primarily clinic-based with the
Structural Heart Program Staffing Considerations- Effective Models for Clinic, Procedure and Post Procedure Care
 Structural Heart Program Staffing Considerations- Effective Models for Clinic, Procedure and Post Procedure Care Deborah Campbell Inova Fairfax Medical Campus Edwards Healthcare Leadership Series September
Structural Heart Program Staffing Considerations- Effective Models for Clinic, Procedure and Post Procedure Care Deborah Campbell Inova Fairfax Medical Campus Edwards Healthcare Leadership Series September
Achieving Operational Excellence with an EHR a CIO s Perspective
 Achieving Operational Excellence with an EHR a CIO s Perspective Phyllis Schuck, SPHR CIO of Pinehurst Surgical HIT Session 6.02 Thursday, March 29, 2007 Pinehurst Surgical Organization Overview Founded
Achieving Operational Excellence with an EHR a CIO s Perspective Phyllis Schuck, SPHR CIO of Pinehurst Surgical HIT Session 6.02 Thursday, March 29, 2007 Pinehurst Surgical Organization Overview Founded
Basic Teaching Physician Presence and Documentation
 Basic Teaching Physician Presence and Documentation Welcome to the Children s University Medical Group (CUMG) training on the Teaching Physician Presence and Documentation. The goal of this module is to
Basic Teaching Physician Presence and Documentation Welcome to the Children s University Medical Group (CUMG) training on the Teaching Physician Presence and Documentation. The goal of this module is to
Professional Charges in an Inpatient Setting and Best Practices for Coding Multiple Scenarios. Webinar Subscription Access Expires December 31.
 Professional Charges in an Inpatient Setting and Best Practices for Coding Multiple Scenarios Questions Answers Webinar Subscription Access Expires December 31. How long can I access the on demand version?
Professional Charges in an Inpatient Setting and Best Practices for Coding Multiple Scenarios Questions Answers Webinar Subscription Access Expires December 31. How long can I access the on demand version?
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice
 Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
12/7/2017 OVERVIEW. CPAs & ADVISORS
 CPAs & ADVISORS experience perspective // CY 2018 OPPS/ASC FINAL RULE & OTHER HEALTHCARE REGULATORY UPDATES Michael K. Westerfield, CPA, FHFMA OVERVIEW CY 2018 OPPC/ ASC Final Rule OPPS payment update
CPAs & ADVISORS experience perspective // CY 2018 OPPS/ASC FINAL RULE & OTHER HEALTHCARE REGULATORY UPDATES Michael K. Westerfield, CPA, FHFMA OVERVIEW CY 2018 OPPC/ ASC Final Rule OPPS payment update
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement. Craig J. Wilson
 Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
The Partner of Choice for Leading Health Systems. Learning Objectives. 45+ Health System Partners 750K+ Surgical Procedures $1.
 http://www.advocatehealth.com/images/logo_advocatehealthcare.gif Co-Management: Successfully Improving Care Along the Surgical Continuum Gerald Biala, SCA Senior Vice President of Perioperative Services
http://www.advocatehealth.com/images/logo_advocatehealthcare.gif Co-Management: Successfully Improving Care Along the Surgical Continuum Gerald Biala, SCA Senior Vice President of Perioperative Services
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
Physician Assistant Reimbursement: Hot Topics
 Physician Assistant Reimbursement: Hot Topics 2 Physician Assistant reimbursement: Hot Topics James A. Kilmark, PA-C Physician Assistant in Emergency Medicine Emergency Physicians Medical Group: PA/NP
Physician Assistant Reimbursement: Hot Topics 2 Physician Assistant reimbursement: Hot Topics James A. Kilmark, PA-C Physician Assistant in Emergency Medicine Emergency Physicians Medical Group: PA/NP
Reimbursement Policy. BadgerCare Plus. Subject: Consultations
 Subject: Reimbursement Policy Effective Date: Committee Approval Obtained: Section: Evaluation and 04/20/18 04/20/18 Management *****The most current version of our reimbursement policies can be found
Subject: Reimbursement Policy Effective Date: Committee Approval Obtained: Section: Evaluation and 04/20/18 04/20/18 Management *****The most current version of our reimbursement policies can be found
PPMI in a Community Teaching Hospital
 Presentation Objectives PPMI in a Community Teaching Targeting VBP and ACO metrics Pharmacist Objective: List ACO metrics that pharmacists can share accountability to achieve targets Technician Objective:
Presentation Objectives PPMI in a Community Teaching Targeting VBP and ACO metrics Pharmacist Objective: List ACO metrics that pharmacists can share accountability to achieve targets Technician Objective:
Creating the New Care Design L2. George Kerwin, CEO Patient of Bellin Health Bellin Health Team. Objectives
 Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Getting Paid for What You Do! Coding 2010
 Getting Paid for What You Do! Coding 20 Children s Mercy Health Network 11/17/09 Richard H. Tuck, MD, FAAP Disclosure I have financial relationships or interests with proprietary entities producing health
Getting Paid for What You Do! Coding 20 Children s Mercy Health Network 11/17/09 Richard H. Tuck, MD, FAAP Disclosure I have financial relationships or interests with proprietary entities producing health
Responsibilities of the Urology Physician Assistant/Nurse Practitioner
 Urology Physician Assistant/Nurse Practitioner Oakland, CA Currently seeking an orthopedic Physician Assistant/Nurse Practitioner for an opportunity in the Bay area. Interested candidates should be NCCPA
Urology Physician Assistant/Nurse Practitioner Oakland, CA Currently seeking an orthopedic Physician Assistant/Nurse Practitioner for an opportunity in the Bay area. Interested candidates should be NCCPA
Thinking Outside the Box: Pharmacists Role in Ambulatory Care
 Thinking Outside the Box: Pharmacists Role in Ambulatory Care Tim R. Brown, PharmD, BCACP, FASHP Director, Clinical Pharmacotherapy in Family Medicine Cleveland Clinic Akron General Center for Family Medicine
Thinking Outside the Box: Pharmacists Role in Ambulatory Care Tim R. Brown, PharmD, BCACP, FASHP Director, Clinical Pharmacotherapy in Family Medicine Cleveland Clinic Akron General Center for Family Medicine
Patient Navigator Program
 Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
Deleted Codes. Agenda 1/31/ E/M Codes Deleted Codes New Codes Changed Codes
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February Jean C. Russell, MS, RHIT Richard Cooley, BA, CCS
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
MEDICARE RULE FOR TEACHING PHYSICIANS Effective July 1, 1996.
 MEDICARE RULE F TEACHING PHYSICIANS Effective July 1, 1996. 1.0 GENERAL RULE: If a resident participates in a service provided in a teaching setting, the teaching physician may not bill Medicare for such
MEDICARE RULE F TEACHING PHYSICIANS Effective July 1, 1996. 1.0 GENERAL RULE: If a resident participates in a service provided in a teaching setting, the teaching physician may not bill Medicare for such
Using An APCD to Inform Healthcare Policy, Strategy, and Consumer Choice. Maine s Experience
 Using An APCD to Inform Healthcare Policy, Strategy, and Consumer Choice Maine s Experience What I ll Cover Today Maine s History of Using Health Care Data for Policy and System Change Health Data Agency
Using An APCD to Inform Healthcare Policy, Strategy, and Consumer Choice Maine s Experience What I ll Cover Today Maine s History of Using Health Care Data for Policy and System Change Health Data Agency
2018 MGMA Practice Operations Survey Guide
 2018 MGMA Practice Operations Survey Guide Due Date: April 13, 2018 This document is intended to serve as a guide for completing the 2018 MGMA Practice Operations Survey. An explanation of each survey
2018 MGMA Practice Operations Survey Guide Due Date: April 13, 2018 This document is intended to serve as a guide for completing the 2018 MGMA Practice Operations Survey. An explanation of each survey
Economic Benefits of Less Restrictive Regulation of APRNs in North Carolina:
 Economic Benefits of Less Restrictive Regulation of APRNs in North Carolina: An Analysis of Local and Statewide Effects on Business Activity Christopher J. Conover, PhD Center for Health Policy and Inequalities
Economic Benefits of Less Restrictive Regulation of APRNs in North Carolina: An Analysis of Local and Statewide Effects on Business Activity Christopher J. Conover, PhD Center for Health Policy and Inequalities
Osteopathic Advocacy: Partnering to Advance Sound Health Policy. Nicholas Schilligo, MS Associate Vice President, State Government Affairs
 Osteopathic Advocacy: Partnering to Advance Sound Health Policy Nicholas Schilligo, MS Associate Vice President, State Government Affairs Our Work Work with a variety of stakeholders to promote AOA policies
Osteopathic Advocacy: Partnering to Advance Sound Health Policy Nicholas Schilligo, MS Associate Vice President, State Government Affairs Our Work Work with a variety of stakeholders to promote AOA policies
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital
 Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
Rural Relevance in Oklahoma
 Rural Relevance in Oklahoma OHA Annual Conference 2017 November 1, 2017 Agenda Introductions The Rural Relevance Study Impact of Current and Proposed Health Policies on Rural Providers Oklahoma Rural Hospitals:
Rural Relevance in Oklahoma OHA Annual Conference 2017 November 1, 2017 Agenda Introductions The Rural Relevance Study Impact of Current and Proposed Health Policies on Rural Providers Oklahoma Rural Hospitals:
Bright Spots in primary care
 Bright Spots in primary care A High- Performing Teaching Practice: Site Visit to Oregon Health & Science University s (OHSU) Family Medicine Clinic at Gabriel Park General information Tom Bodenheimer MD
Bright Spots in primary care A High- Performing Teaching Practice: Site Visit to Oregon Health & Science University s (OHSU) Family Medicine Clinic at Gabriel Park General information Tom Bodenheimer MD
Children s Hospital Association Summary of Final Regulation. November 9, 2012
 Medicaid Program; Payment for Services Furnished by Certain Primary Care Physicians and Charges for Vaccine Administration under the Vaccine for Children Program Children s Hospital Association Summary
Medicaid Program; Payment for Services Furnished by Certain Primary Care Physicians and Charges for Vaccine Administration under the Vaccine for Children Program Children s Hospital Association Summary
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
SHAPING THE ED FOR EDUCATION - ALIGNING GOALS
 SHAPING THE ED FOR EDUCATION - ALIGNING GOALS Michael Gibbs, MD Chair, Carolinas Medical Center Megan Fix, MD Associate Program Director, University of Utah Why is this important? History of resident education
SHAPING THE ED FOR EDUCATION - ALIGNING GOALS Michael Gibbs, MD Chair, Carolinas Medical Center Megan Fix, MD Associate Program Director, University of Utah Why is this important? History of resident education
Telemedicine and Health Reform. Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center
 Telemedicine and Health Reform Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center 1 telehealthresourcecenters.org Links to all TRCs National Webinar Series Reimbursement,
Telemedicine and Health Reform Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center 1 telehealthresourcecenters.org Links to all TRCs National Webinar Series Reimbursement,
2013 Physician Inpatient/ Outpatient Revenue Survey
 Physician Inpatient/ Outpatient Revenue Survey A survey showing net annual inpatient and outpatient revenue generated by physicians in various specialties on behalf of their affiliated hospitals Merritt
Physician Inpatient/ Outpatient Revenue Survey A survey showing net annual inpatient and outpatient revenue generated by physicians in various specialties on behalf of their affiliated hospitals Merritt