Digital Transformation of MOLST: Getting Started and Ensuring Sustainability
|
|
|
- Brook Casey
- 6 years ago
- Views:
Transcription
1 Digital Transformation of MOLST: Getting Started and Ensuring Sustainability
2 Speakers Patricia Bomba, MD, MACP Vice President and Medical Director, Geriatrics, Excellus BlueCross BlueShield Chair, MOLST Statewide Implementation Team & emolst Program Director Leader, Community-wide End-of-life/Palliative Care Initiative Chair, National Healthcare Decisions Day New York State Coalition Carolyn Kazdan, MHSA, NHA Quality Improvement Specialist IPRO Project Manager, CMS Special Innovations Project, emolst Member, MOLST Statewide Implementation Team Executive Committee Katie Orem, MPH Geriatrics & Palliative Care Program Manager, Excellus BlueCross BlueShield emolst Administrator Member, MOLST Statewide Implementation Team Executive Committee Nothing to Disclose

3
4
5 Objectives Identify value of early advance care planning, MOLST/eMOLST implementation in Post-Acute, Long Term Care & the long term care continuum List steps and create a work plan that streamlines adoption of new innovative technology & leverage new CPT codes Produce a work plan for implementation and sustainability of MOLST/eMOLST using existing educational & other resources
6 Deaths Among Seniors New York is ranked #1 in hospital deaths among seniors* (worst in the country) Estimates suggest that 35% of all New Yorkers 65+ die in the hospital** Regional Variation, Medicare Data*** *In Sickness and in Health, Where States are No.1 Wall Street Journal, June 9, 2014 **America's Health Rankings ***Dartmouth Atlas
7 What Do Common Ways of Dying Look Like?

8 How Americans Wish to Die
9 Medicare payments in last year of life account for ¼ of all Medicare spending Data from: Riley G, Lubitz J. Long-Term Trends in Medicare Payments in the Last Year of Life. Health Services Research, 2010;

10 30% of health care is unnecessary or harmful How do we shift the cultural mindset from more treatment is better to the right treatment and care, and no more? Triple Aim, IHI Choosing Wisely Campaign
11 Value of MOLST/eMOLST in Healthcare Promoting value in healthcare encourages hospitals and other providers to reduce waste and unnecessary care while maintaining high quality of care. Hospital Compare: individual hospital results for payment and death(mortality) measures together MOLST/eMOLST: reduce unwanted hospitalizations/ed visits

12 Dedicated Physician & System Champions Align with Health Systems Priorities Palliative Care Advance Care Planning Quality, Patient Safety & Risk Management Compliance with NYSPHL Care Transitions Reducing Readmissions Accountable Care Organizations Innovative Payment Models Medicaid Redesign: DSRIP, FIDA, Health Homes State Health Innovation Plan IOM Dying in America Recommendations



13 MOLST/eMOLST: End-of-life Care Transitions Program Hospital LTC Office A Project of the Community-Wide End-of-life/Palliative Care Initiative
14 Released September 17, Report available: IOM Report Dying in America Delivery of person-centered, family-oriented care Clinician-patient communication and advance care planning Professional education and development Policies and payment systems Public education and engagement
15 Palliative Care Interdisciplinary care aims to relieve suffering and improve quality of life for patients with advanced illness and their families offered simultaneously with all other appropriate medical treatment from the time of diagnosis focuses on quality of life and provides an extra layer of support for patients and families Three Key Pillars with Psychosocial & Spiritual Support Advance Care Planning and Goals for Care Step 1: Community Conversations on Compassionate Care* Step 2: Medical Orders for Life-Sustaining Treatment (MOLST)* Pain and Symptom Management Caregiver Support *A Project of the Community-Wide End-of-life/Palliative Care Initiative


: Hospice Advance care planning &")

16 Continuum of Care Model for Patients with Serious Illness Medical Management of Chronic Disease Integrated with Palliative Care Goals for Care shift 12 mo 6mo Diagnosis Death Palliative Care (PC): Hospice Advance care planning & goals for care, pain and symptom control, caregiver support Progression of Serious Illness Bereavement
17 Released September 17, Report available: Key Recommendations Policies and Payment Systems Actions Encourage states to develop and implement a Physician Orders for Life-Sustaining Treatment (POLST) paradigm program in accordance with nationally standardized core requirements
18 Definitions National POLST Paradigm: process of communication & shared decision making results in POLST; has established endorsement requirements POLST: Physician Orders for Life Sustaining Treatment - different states use different names to describe the state POLST program NY MOLST: Medical Orders for Life-Sustaining Treatment

19 TPOPP MOLST LaPOST SMOST POST MOST MI-POST IPOST DMOST WyoPOLST

20 National POLST Paradigm Programs *As of 2006
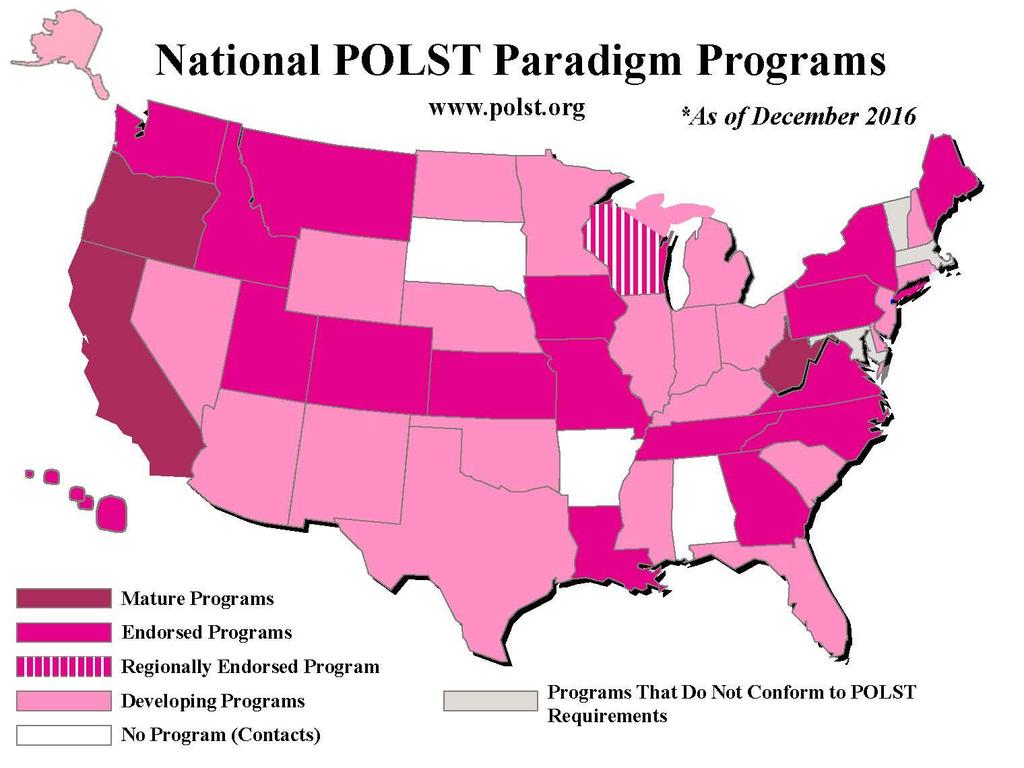
21




22 Standard of Care Advance Directives Medical Orders Health Care Proxy Living Will Organ Donation DNR MOLST



23 Flow of Emergency Care: Standard of Care







24 Flow of Emergency Care: MOLST
25 Bomba PA & Vermilyea Integrating POLST into Palliative Care Guidelines: A Paradigm Shift in Advance Care Planning in Oncology JNCCN 2006; 4(8) (pg 822) Advance Care Planning Compassion, Support and Education along the Health-Illness Continuum Advancing chronic illness Chronic disease or functional decline Multiple comorbidities, with increasing frailty Healthy and independent Maintain & maximize health and independence Death
26 Advance Directives and Actionable Medical Orders Traditional ADs For All Adults Community Conversations on Compassionate Care (CCCC) New York Health Care Proxy Living Will Organ Donation State-specific forms: e.g. Durable POA for Healthcare CompassionAndSupport.org CaringInfo.org Actionable Medical Orders For Those Who Are Seriously Ill or Near the End of Their Lives Medical Orders for Life-Sustaining Treatment (MOLST) Program Do Not Resuscitate (DNR) Order Medical Orders for Life Sustaining Treatment (MOLST) Physician Orders for Life Sustaining Treatment (POLST) Paradigm Programs CompassionAndSupport.org POLST.org Patricia A. Bomba, MD, MACP
27 Bomba PA, Black J. The POLST: An improvement over traditional advance directives. Cleveland Clinic Journal of Medicine. 2012; 79(7): Differences Between POLST/MOLST and Advance Directives Characteristics POLST Advance Directives Population For the seriously ill All adults Timeframe Current care Future care Who completes the form Resulting form Health Care Agent or Surrogate role Health Care Professionals Medical Orders (POLST) Can engage in discussion if patient lacks capacity Patients Advance Directives Cannot complete Portability Provider responsibility Patient/family responsibility Periodic review Provider responsibility Patient/family responsibility
28 Key Recommendations Policies and Payment Systems Actions Require the use of interoperable electronic health records that incorporate advance care planning to improve communication of individuals wishes across time, settings, and providers, documenting: the designation of a surrogate/decision maker patient values and beliefs and goals for care the presence of an advance directive the presence of medical orders for life-sustaining treatment for appropriate populations NY s emolst highlighted in IOM Report Released September 17, Report available:
29 New York emolst An electronic system that guides clinicians and patients through a thoughtful discussion and MOLST process Integrates 8-Step MOLST Protocol & NYSDOH Checklists Allows a team approach within scope of practice Creates MOLST & correct MOLST Chart Documentation Forms emolst ensures MOLST quality, accuracy, accessibility Allows the clinician to print a copy of the emolst form on bright pink paper for the patient Workflow remains the same; EMS needs a copy of emolst Serves as the registry of NY emolst forms to make sure a copy of medical orders & discussion are available in an emergency. emolst is free, available statewide and accessed at NYSeMOLSTregistry.com.
30 8-Step MOLST Protocol 1. Prepare for discussion Understand patient s health status, prognosis & ability to consent Retrieve completed Advance Directives Determine decision-maker and NYSPHL legal requirements, based on who makes decision and setting 2. Determine what the patient and family know re: condition, prognosis 3. Explore goals, hopes and expectations 4. Suggest realistic goals 5. Respond empathetically 6. Use MOLST to guide choices and finalize patient wishes Shared, informed medical decision-making Conflict resolution 7. Complete and sign MOLST Follow NYSPHL and document conversation 8. Review and revise periodically Developed for NYS MOLST, Bomba, 2005; revised 2011
31 AFTER FHCDA: MOLST Instructions and Checklists Ethical Framework/Legal Requirements Checklist #1 - Adult patients with medical decision-making capacity (any setting) Checklist #2 - Adult patients without medical decision-making capacity who have a health care proxy (any setting) Checklist #3 - Adult hospital or nursing home patients without medical decision-making capacity who do not have a health care proxy, and decision-maker is a Public Health Law Surrogate (surrogate selected from the surrogate list) Checklist #4 - Adult hospital or nursing home patients without medical decision-making capacity who do not have a health care proxy or a Public Health Law Surrogate Checklist #5 - Adult patients without medical decision-making capacity who do not have a health care proxy, and the MOLST form is being completed in the community. Checklist for Minor Patients - (any setting) Checklist for Developmentally Disabled who lack capacity (any setting) must travel with the patient s MOLST
32 emolst Produces MOLST and MOLST Chart Documentation Form Align with NYSDOH Checklists
33 emolst and OPWDD MOLST Legal Requirements Checklist for Individuals with DD
34 Research: Site of Death vs. Treatment Requested Death records: 58,000 people who died of natural causes in 2010 and 2011 in OR Nearly 31% of people who died: POLST forms entered in OR's POLST Registry Compared location of death with treatment requested 6.4% of people with POLST forms who selected "comfort measures only" died in hospital 34.2% of people without POLST forms in the registry died in the hospital Fromme, Erik et al (2014). JAGS, on-line June 9, 2014
35 Why emolst: Aligns with New Value-Based, Accountable Care Models Improves quality: discussion of personal-centered values, beliefs and goals for care drives choice of lifesustaining treatment Honors individual preferences: provides MOLST orders and copy of discussion across care transitions Reduces unnecessary and unwanted hospitalizations, ED use, service utilization and expense
36 emolst Case, CNY, 2014: What Can Happen When MOLST is Unavailable but in emolst Elderly gentleman with multiple medical problems, including COPD with recurrent acute respiratory exacerbations & recurrent hospitalizations Has Health Care Proxy, MOLST form Presents to ER with acute respiratory insufficiency; MOLST form left on refrigerator Patient evaluated & treated Plan: intubation & mechanical ventilation and transfer to SUNY Upstate MD in ER signed into emolst goals for care: functionality, remain at home; MOLST: DNR & DNI Patient admitted, treated conservatively, discharged home


37 Why emolst: NYSDOH Attorney, Physician Feedback Quality, Patient Safety and Accessibility CompassionAndSupport YouTube Channel

38 Effective Implementation Requires a Multidimensional Approach *Recommended by the 2014 IOM Dying in America report 1. Culture change* 2. Professional training of physicians, clinicians & other professionals* 3. Public advance care planning education, engagement & empowerment* 4. Thoughtful discussions* 5. Shared, informed medical decision-making* 6. Care planning that supports MOLST 7. System implementation, policies and procedures, workflow 8. Dedicated system and physician champion 9. Leverage existing payment stream (CPT codes and 99498) to encourage upstream shared, informed, decision making* 10. Standardized interoperable online completion and retrieval system available in all care settings to ensure accuracy and accessibility (NYSeMOLSTregistry.com)


39 Culture Change State of New York Department of Health Nonhospital Order Not to Resuscitate (DNR Order) Person's Name: Date of Birth: / / Do not resuscitate the person named above. Physician's Signature Print Name License Number Date / / It is the responsibility of the physician to determine, at least every 90 days, whether this order continues to be appropriate, and to indicate this by a note in the person's medical chart. The issuance of a new form is NOT required, and under the law this order should be considered valid unless it is known that it has been revoked. This order remains valid and must be followed, even if it has not been reviewed within the 90 day period. DOH-3474 (2/92) Thoughtful Discussions Values, Beliefs, Goals Shared Decision Making Preferences Based on Goals Care Plan Based on MOLST










40 Professional Training: Physicians, Health Care Professionals, Others







41 Public Education, Engagement and Empowerment Real Stories








42 Educational Resources MOLST Conferences Community Talks MOLST General Instructions NYSDOH MOLST Checklists CompassionAndSupportYouTubeChannel
43 8-Step MOLST Protocol 1. Prepare for discussion Understand patient s health status, prognosis & ability to consent Retrieve completed Advance Directives Determine decision-maker and NYSPHL legal requirements, based on who makes decision and setting 2. Determine what the patient and family know re: condition, prognosis 3. Explore goals, hopes and expectations 4. Suggest realistic goals 5. Respond empathetically 6. Use MOLST to guide choices and finalize patient wishes Shared, informed medical decision-making Conflict resolution 7. Complete and sign MOLST Follow NYSPHL and document conversation 8. Review and revise periodically Developed for NYS MOLST, Bomba, 2005; revised 2011
44 Care Plan Supports MOLST
45 System Implementation Policies and Procedures Workflow: Current and Future Identification of Patients using a population health approach to screening: Advance care planning for everyone 18 years and older Appropriate for POLST Paradigm Staffing considerations Operational considerations Quality Improvement: Use Plan-Do-Study-Act (PDSA) cycles Develop a work plan, timelines, accountability Plan Execute - Sustain
46 System Implementation Advance Care Planning Clinical Pathway (Work Flow) Life Expectancy of Greater than One Year Start: Physician / Patient Conversation No Does Patient Have Advance Directives? Yes Educate about Importance of Advance Directives Obtain Copy of Completed Advance Directives Provide Information on Advance Directives Elicit Patient's Values and Preferences for End-of-Life Care Assess Barriers to Completing Advance Directives Encourage Patient to Discuss Wishes with Family Are There Barriers to Completing Advance Directives? No Reinforce Need for Updated Advance Directives Assess Appropriateness of Designated Health Care Agent Yes Work to Overcome Barriers No Are the Advance Directives Up-to-Date? Yes Motivate Completion of Advance Directives Inquire about Organ Donation and/or Autopsy Reassess Periodically or as Needs Change Consider Introducing the Palliative Care Team Discuss Palliative Care Options Including Hospice Bomba, JNCCN 4(8),
47 System Implementation Advance Care Planning Clinical Pathway (Work Flow) Life Expectancy of Less than One Year Start: Physician / Patient Conversation No Does Patient Have Advance Directives? Yes For New York State Residents Educate about Importance of Advance Directives Obtain Copy of Completed Advance Directives Provide Information on Advance Directives Elicit Patient's Values and Preferences for End-of-Life Care Assess Barriers to Completing Advance Directives Reinforce Need for Updated Advance Directives Encourage Patient to Discuss Wishes with Family Are There Barriers to Completing Advance Directives? No Assess Appropriateness of Designated Health Care Agent Yes Work to Overcome Barriers No Are the Advance Directives Up-to-Date? Motivate Completion of Advance Directives Complete MOLST Form Yes Complete MOLST Form Reassess Periodically or as Needs Change Consider Introducing the Palliative Care Team Discuss Palliative Care Options Including Hospice Inquire about Organ Donation and/or Autopsy Bomba, JNCCN 4(8),
48 Built-In Quality Measures Completion of ACP process includes properly completed MOLST, as well as documentation of the process MOLST Medical orders properly completed, storage & retrieval Document discussion and process emolst Analytics
49 MOLST Takes Time Person-centered goals for care discussion May require more than 1 session to complete Shared, informed medical decision making process Ethical framework/legal requirements Completion of form Family awareness of person s decision Care Plan to support MOLST Goals for care, preferences and MOLST may change New ACP CPT Codes Overcomes Barrier: Inadequate reimbursement for time spent Consider office workflow transformation
50 Leverage Advance Care Planning CPT Codes and Reimbursement to physicians and qualified health care professionals for providing advance care planning services to Medicare and Medicaid members Time-based 99497: First 30 minutes (16-45 minutes) 99488: Each additional 30 minutes (16-45 additional minutes for a total of minutes) Face-to-face with the patient, family member(s), and/or surrogate No active management of the problem(s) is undertaken during the time period reported. ACP: integral component of the practice of medicine

51 Digital Transformation NYSeMOLSTregistry.com MOLST EMR Toolbar MOLST Chart Documentation Form Align with NYSDOH Checklists
52 Thank You Thank you for your visionary leadership and support of the multiple dimensions needed to ensure proper implementation of Advance Care Planning and the digital transformation of MOLST to emolst. Contact Information: Patricia Bomba, MD, MACP Carolyn Kazdan, MHSA, NHA Katie Orem, MPH
Improving End-of-life Care: A Community Approach Patricia Bomba, MD, MACP VP & Medical Director, Geriatrics, Excellus BlueCross Blue Shield
 Session Code D20 & E20 This presenter has nothing to disclose Improving End-of-life Care: A Community Approach Patricia Bomba, MD, MACP VP & Medical Director, Geriatrics, Excellus BlueCross Blue Shield
Session Code D20 & E20 This presenter has nothing to disclose Improving End-of-life Care: A Community Approach Patricia Bomba, MD, MACP VP & Medical Director, Geriatrics, Excellus BlueCross Blue Shield
emolst: Best Practice for Improving End-of-life Care
 emolst: Best Practice for Improving End-of-life Care Patricia Bomba, MD, MACP Vice President and Medical Director, Geriatrics Chair, MOLST Statewide Implementation Team & emolst Program Director Chair,
emolst: Best Practice for Improving End-of-life Care Patricia Bomba, MD, MACP Vice President and Medical Director, Geriatrics Chair, MOLST Statewide Implementation Team & emolst Program Director Chair,
What is POLST Physician Orders For Life
 POLST in ND Physician Orders for Life Sustaining Treatment 2017 Dakota Conference Nancy Joyner, MS, APRN-CNS, ACHPN Palliative Care Clinical Nurse Specialist HCND s POLST Coordinator Objectives 1. Define
POLST in ND Physician Orders for Life Sustaining Treatment 2017 Dakota Conference Nancy Joyner, MS, APRN-CNS, ACHPN Palliative Care Clinical Nurse Specialist HCND s POLST Coordinator Objectives 1. Define
POLST Discussions Doing it Better. Clinical Update in Geriatric Medicine. Judith S. Black, MD, MHA. POLST Overview. Faculty Disclosure PART I
 Faculty Disclosure POLST Discussions Doing it Better Clinical Update in Geriatric Medicine Dr. Black discloses that she is employed by Allegheny Health Network and is an executive committee member of the
Faculty Disclosure POLST Discussions Doing it Better Clinical Update in Geriatric Medicine Dr. Black discloses that she is employed by Allegheny Health Network and is an executive committee member of the
Advance Care Planning
 Community-wide End-of-life /Palliative Care Initiative Community Conversations on Compassionate Care Advance Care Planning Know your choices, share your wishes: Maintain control, achieve peace of mind,
Community-wide End-of-life /Palliative Care Initiative Community Conversations on Compassionate Care Advance Care Planning Know your choices, share your wishes: Maintain control, achieve peace of mind,
Federal Policy Agenda / 2016 & Beyond
 Federal Policy Agenda / 2016 & Beyond Compassion & Choices is the leading national nonprofit organization dedicated to improving care and expanding choice for people with advanced illness, and nearing
Federal Policy Agenda / 2016 & Beyond Compassion & Choices is the leading national nonprofit organization dedicated to improving care and expanding choice for people with advanced illness, and nearing
POLST: Advance Care Planning for the Seriously Ill
 POLST: Advance Care Planning for the Seriously Ill Advance care planning helps ensure patient treatment preferences are documented, regularly updated, and respected. There are two documents used to record
POLST: Advance Care Planning for the Seriously Ill Advance care planning helps ensure patient treatment preferences are documented, regularly updated, and respected. There are two documents used to record
Advanced Care Planning and Advanced Directives: Our Roles March 27, 2017
 Advanced Care Planning and Advanced Directives: Our Roles March 27, 2017 2017 NPSS Asheville, NC Overview History of Advanced Directives Importance of Advanced Care Planning for Quality care Our Role in
Advanced Care Planning and Advanced Directives: Our Roles March 27, 2017 2017 NPSS Asheville, NC Overview History of Advanced Directives Importance of Advanced Care Planning for Quality care Our Role in
POLST Registry Vendor Webinar. October 8, :00 11:00am
 POLST Registry Vendor Webinar October 8, 2014 10:00 11:00am Agenda Introduction to Project Team Project Background What Is POLST? Technical Requirements RFI and Technology Vendor Process Key Dates Q&A
POLST Registry Vendor Webinar October 8, 2014 10:00 11:00am Agenda Introduction to Project Team Project Background What Is POLST? Technical Requirements RFI and Technology Vendor Process Key Dates Q&A
Advance Care Planning (and more)
") Advance Care Planning (and more) Tessa & Josie Karl Steinberg, MD, CMD,HMDC @karlsteinberg, karlsteinberg@mail.com WWW.COALITIONCCC.ORG Advance Care Planning ACP is a process that unfolds over a life span
Advance Care Planning (and more) Tessa & Josie Karl Steinberg, MD, CMD,HMDC @karlsteinberg, karlsteinberg@mail.com WWW.COALITIONCCC.ORG Advance Care Planning ACP is a process that unfolds over a life span
Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee
 Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee What is Advance Care Planning (ACP)? Understanding/clarifying
Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee What is Advance Care Planning (ACP)? Understanding/clarifying
Revised 2/27/17. POLST For General Providers
 Revised 2/27/17 POLST For General Providers Permission to Use This slide presentation may be used without permission. To promote consistency across the state, the slides may not be altered. You may freely
Revised 2/27/17 POLST For General Providers Permission to Use This slide presentation may be used without permission. To promote consistency across the state, the slides may not be altered. You may freely
 NEW YORK STATE DEPARTMENT OF HEALTH Medical Orders for Life Sustaining Treatment (MOLST) THE PATIENT KEEPS THE ORIGINAL MOLST FORM DURING TRAVEL TO DIFFERENT CARE SETTINGS. THE PHYSICIAN KEEPS A COPY.
NEW YORK STATE DEPARTMENT OF HEALTH Medical Orders for Life Sustaining Treatment (MOLST) THE PATIENT KEEPS THE ORIGINAL MOLST FORM DURING TRAVEL TO DIFFERENT CARE SETTINGS. THE PHYSICIAN KEEPS A COPY.
Sample MOLST Policy for Home Health Care or Hospice
 TOOL 2-7A Sample MOLST Policy for Home Health Care or Hospice SAMPLE/DRAFT MOLST POLICY and PROCEDURE Home Health Care or Hospice Agencies CAUTION: This sample policy should not be accepted as MOLST policy
TOOL 2-7A Sample MOLST Policy for Home Health Care or Hospice SAMPLE/DRAFT MOLST POLICY and PROCEDURE Home Health Care or Hospice Agencies CAUTION: This sample policy should not be accepted as MOLST policy
Disclosure. Objectives. POLST Education for Healthcare Professionals Hospice and Palliative Nurses Association (HPNA) E Learning
 E Learning") POLST (Physicians Orders for Life Sustaining Treatment) Education for Healthcare Professionals Presented by Nancy Joyner, APRN CNS, ACHPN Disclosure Nancy Joyner does not have any financial, professional
POLST (Physicians Orders for Life Sustaining Treatment) Education for Healthcare Professionals Presented by Nancy Joyner, APRN CNS, ACHPN Disclosure Nancy Joyner does not have any financial, professional
Advance Care Planning: Where Does MOLST Fit?
 Advance Care Planning: Where Does MOLST Fit? Patricia Bomba, M.D., F.A.C.P. Vice President and Medical Director, Geriatrics Director, Education for Physicians on End-of-life Care Director, Honoring Patient
Advance Care Planning: Where Does MOLST Fit? Patricia Bomba, M.D., F.A.C.P. Vice President and Medical Director, Geriatrics Director, Education for Physicians on End-of-life Care Director, Honoring Patient
Deciding About. Health Care A GUIDE FOR PATIENTS AND FAMILIES. New York State Department of Health
 Deciding About Health Care A GUIDE FOR PATIENTS AND FAMILIES New York State Department of Health 2 Introduction Who should read this guide? This guide is for New York State patients and for those who will
Deciding About Health Care A GUIDE FOR PATIENTS AND FAMILIES New York State Department of Health 2 Introduction Who should read this guide? This guide is for New York State patients and for those who will
Building a Person-Centered ADVANCE CARE Planning Program. Barbara J. Smith, LBSW, MS, CHC, NHA Carolyn Stramecki, MHSA, CPHQ
 Building a Person-Centered ADVANCE CARE Planning Program Barbara J. Smith, LBSW, MS, CHC, NHA Carolyn Stramecki, MHSA, CPHQ Objectives Describe components of an advance directive document required to meet
Building a Person-Centered ADVANCE CARE Planning Program Barbara J. Smith, LBSW, MS, CHC, NHA Carolyn Stramecki, MHSA, CPHQ Objectives Describe components of an advance directive document required to meet
Supersedes/Updates: 99-10
 No. 08-07 New York State Department of Health Bureau of Emergency Medical Services POLICY STATEMENT Supersedes/Updates: 99-10 November 20, 2008 Re: Medical Orders for Life Sustaining Treatment (MOLST)
No. 08-07 New York State Department of Health Bureau of Emergency Medical Services POLICY STATEMENT Supersedes/Updates: 99-10 November 20, 2008 Re: Medical Orders for Life Sustaining Treatment (MOLST)
Overview 6/25/2014. Advanced Directives. 2. Out of Hospital DNR/DNI 3. University i Hospital DNR/DNI implementation 4. Special circumstances
 Overview 1. Advanced Directives 2. Out of Hospital DNR/DNI 3. University i Hospital DNR/DNI implementation i 4. Special circumstances Advanced Directives A written or oral instruction relating to provision
Overview 1. Advanced Directives 2. Out of Hospital DNR/DNI 3. University i Hospital DNR/DNI implementation i 4. Special circumstances Advanced Directives A written or oral instruction relating to provision
TOOL 2-6 Sample MOLST Policy for Acute Care Hospitals 1
 TOOL 2-6 Sample MOLST Policy for Acute Care Hospitals 1 Caution It is not advisable to use MOLST policy written for other institutions, especially policies from out of state. Each institution needs to
TOOL 2-6 Sample MOLST Policy for Acute Care Hospitals 1 Caution It is not advisable to use MOLST policy written for other institutions, especially policies from out of state. Each institution needs to
Advance Care Planning. Ken Brummel-Smith, MD Charlotte Edwards Maguire Professor of Geriatrics FSU College of Medicine
 Advance Care Planning Ken Brummel-Smith, MD Charlotte Edwards Maguire Professor of Geriatrics FSU College of Medicine 1 Principles of Ethics Autonomy/Respect for Persons Beneficence Non- maleficence Justice
Advance Care Planning Ken Brummel-Smith, MD Charlotte Edwards Maguire Professor of Geriatrics FSU College of Medicine 1 Principles of Ethics Autonomy/Respect for Persons Beneficence Non- maleficence Justice
POLST: What s New and How Can We Do Better? Pam Hiransomboon-Vogel, DNP, FNP-BC, ACHPN
 POLST: What s New and How Can We Do Better? Pam Hiransomboon-Vogel, DNP, FNP-BC, ACHPN The OHSU Center for Ethics in Health Care and POLST Program, have no relevant financial relationships to disclose
POLST: What s New and How Can We Do Better? Pam Hiransomboon-Vogel, DNP, FNP-BC, ACHPN The OHSU Center for Ethics in Health Care and POLST Program, have no relevant financial relationships to disclose
Family Health Care Decisions Act (FHCDA)
") Family Health Care Decisions Act (FHCDA) Public Health Law Article 29-CC Added by L. 2010, Ch. 8 Applies to general hospitals and residential health care facilities (nursing homes) Went into effect on
Family Health Care Decisions Act (FHCDA) Public Health Law Article 29-CC Added by L. 2010, Ch. 8 Applies to general hospitals and residential health care facilities (nursing homes) Went into effect on
Insert State Name Here
 Request for Endorsement of State POLST Program State POLST Program: Insert State Name Here Directions: Please complete the information requested on this form and submit the form and additional information
Request for Endorsement of State POLST Program State POLST Program: Insert State Name Here Directions: Please complete the information requested on this form and submit the form and additional information
INFORMATION ABOUT HEALTH CARE DECISONS. Health Care Proxy MOLST DNR
 INFORMATION ABOUT HEALTH CARE DECISONS Health Care Proxy MOLST DNR February/2017 1 Introduction This informational booklet describing different options and procedures for making health care decisions was
INFORMATION ABOUT HEALTH CARE DECISONS Health Care Proxy MOLST DNR February/2017 1 Introduction This informational booklet describing different options and procedures for making health care decisions was
TO THE PRESENTER: ***
 TO THE PRESENTER: This slideset is shortened from a longer version that is also available on the POLST Illinois website. In this basic presentation, important content from the longer version has been transposed
TO THE PRESENTER: This slideset is shortened from a longer version that is also available on the POLST Illinois website. In this basic presentation, important content from the longer version has been transposed
ADVANCE CARE PLANNING: WHY, HOW, AND IMPACT ON THE TRIPLE AIM
 ADVANCE CARE PLANNING: WHY, HOW, AND IMPACT ON THE TRIPLE AIM John Fox MD, MHA AVP Medical Affairs, Priority Health MCM Board Member Carol Robinson DNP, MS, BSN, RN, CHPN Community Coordinator, MCM OBJECTIVES
ADVANCE CARE PLANNING: WHY, HOW, AND IMPACT ON THE TRIPLE AIM John Fox MD, MHA AVP Medical Affairs, Priority Health MCM Board Member Carol Robinson DNP, MS, BSN, RN, CHPN Community Coordinator, MCM OBJECTIVES
Measure #47 (NQF 0326): Care Plan National Quality Strategy Domain: Communication and Care Coordination
: Care Plan National Quality Strategy Domain: Communication and Care Coordination") Measure #47 (NQF 0326): Care Plan National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Measure #47 (NQF 0326): Care Plan National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
vv POLST for Hospice Providers
 vv. 2.2.17 POLST for Hospice Providers Permission to Use This slide presentation may be used without permission. To promote consistency across the state, the slides may not be altered. You may freely take
vv. 2.2.17 POLST for Hospice Providers Permission to Use This slide presentation may be used without permission. To promote consistency across the state, the slides may not be altered. You may freely take
HealthStream Regulatory Script
 HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
Improving POLST/Advanced Directive Completion in the Primary Care Setting
 University of Portland Pilot Scholars Nursing Graduate Publications and Presentations School of Nursing 2016 Improving POLST/Advanced Directive Completion in the Primary Care Setting Miranda Barlow Anthony
University of Portland Pilot Scholars Nursing Graduate Publications and Presentations School of Nursing 2016 Improving POLST/Advanced Directive Completion in the Primary Care Setting Miranda Barlow Anthony
POLST: An improvement over traditional advance directives
 REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will engage their patients and their families in discussions about their goals and preferences for care at the end of life PATRICIA A. BOMBA, MD, FACP Vice
REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will engage their patients and their families in discussions about their goals and preferences for care at the end of life PATRICIA A. BOMBA, MD, FACP Vice
Palliative Care Competencies for Occupational Therapists
 Principles of Palliative Care Demonstrates an understanding of the philosophy of palliative care Demonstrates an understanding that a palliative approach to care starts early in the trajectory of a progressive
Principles of Palliative Care Demonstrates an understanding of the philosophy of palliative care Demonstrates an understanding that a palliative approach to care starts early in the trajectory of a progressive
Advance Care Planning: Goals of Care - Calgary Zone
 Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST
Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST
Quality of Life Conversation On Advance Care Planning
 Quality of Life Conversation On Advance Care Planning Information Packet Page 1 About the Integrated Healthcare Association The nonprofit Integrated Healthcare Association (IHA) convenes diverse stakeholders,
Quality of Life Conversation On Advance Care Planning Information Packet Page 1 About the Integrated Healthcare Association The nonprofit Integrated Healthcare Association (IHA) convenes diverse stakeholders,
Advance Directive for Health Care
 Advance Directive for Health Care respecting your right to: Choose Your Healthcare Agent Choose the Authority Given to Your Healthcare Agent Choose Your Preferences Related to Treatment & Care Printed
Advance Directive for Health Care respecting your right to: Choose Your Healthcare Agent Choose the Authority Given to Your Healthcare Agent Choose Your Preferences Related to Treatment & Care Printed
FROM THE FIELD. What is POLST?
 Editor s Note: The following Q & A regarding POLST is reformatted from the written testimony ( Renewing the Conversation: Respecting Patients Wishes and Advance Care Planning )by Amy Vandenbroucke, JD,
Editor s Note: The following Q & A regarding POLST is reformatted from the written testimony ( Renewing the Conversation: Respecting Patients Wishes and Advance Care Planning )by Amy Vandenbroucke, JD,
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Oregon POLST Registry FACT SHEET
 FACT SHEET January 2015 OREGON AT A GLANCE ESTABLISHING THE REGISTRY Population (2013) 3.93 million Number of deaths (2013) 33,931 Number of hospitals 58 Number of nursing homes 136* Emergency Medical
FACT SHEET January 2015 OREGON AT A GLANCE ESTABLISHING THE REGISTRY Population (2013) 3.93 million Number of deaths (2013) 33,931 Number of hospitals 58 Number of nursing homes 136* Emergency Medical
Advance Directives The Missing Conversation Why Our Patients Children Are Left Holding The Bag. End of Life Planning Barriers 10/7/2014
 Advance Directives The Missing Conversation Why Our Patients Children Are Left Holding The Bag SC Chapter American College of Physicians October 29, 2014 Sewell I. Kahn, MD FACP End of Life Planning Barriers
Advance Directives The Missing Conversation Why Our Patients Children Are Left Holding The Bag SC Chapter American College of Physicians October 29, 2014 Sewell I. Kahn, MD FACP End of Life Planning Barriers
Massachusetts Medical Orders for Life Sustaining Treatment (MOLST)
") Massachusetts Medical Orders for Life Sustaining Treatment (MOLST) Prepared by the Center for Developmental Disabilities Evaluation and Research (CDDER) on behalf of the Massachusetts Department of Developmental
Massachusetts Medical Orders for Life Sustaining Treatment (MOLST) Prepared by the Center for Developmental Disabilities Evaluation and Research (CDDER) on behalf of the Massachusetts Department of Developmental
End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces.
 End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces. Terms Definitions End of Life Care To assist persons who
End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces. Terms Definitions End of Life Care To assist persons who
Becoming a Conversation Ready Organization
 June 20, 2017 These presenters have nothing to disclose Becoming a Conversation Ready Organization Session 3 Steward: Achieving the reliability of allergy information Lauge Sokol-Hessner, MD Kelly McCutcheon
June 20, 2017 These presenters have nothing to disclose Becoming a Conversation Ready Organization Session 3 Steward: Achieving the reliability of allergy information Lauge Sokol-Hessner, MD Kelly McCutcheon
Plan. Iowa. Nicole Peterson, DNP, ARNP. Jane Dohrmann, MSW, LISW. The POLST Paradigm 4/6/ minute presentation 15 minutes questions/answers
 The POLST Paradigm in Nursing Homes The POLST Paradigm in Nursing Homes Presenters Jane Dohrmann Nicole Peterson Mercedes Bern Klug Hand out of presentation available: http://clas.uiowa.edu/socialwork/nursing
The POLST Paradigm in Nursing Homes The POLST Paradigm in Nursing Homes Presenters Jane Dohrmann Nicole Peterson Mercedes Bern Klug Hand out of presentation available: http://clas.uiowa.edu/socialwork/nursing
Goals & Objectives 4/17/2014 UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES (AHCD) By Maureen Kroning, EdD, RN. Why would someone need to do this?
 By Maureen Kroning, EdD, RN. Why would someone need to do this?") UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES (AHCD) By Maureen Kroning, EdD, RN Goals & Objectives Participants will increase their knowledge about AHCD Review AHCD documents used at the hospital Role
UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES (AHCD) By Maureen Kroning, EdD, RN Goals & Objectives Participants will increase their knowledge about AHCD Review AHCD documents used at the hospital Role
Medical Orders for Life- Sustaining Treatment
 Medical Orders for Life- Sustaining Treatment PILOT PROGRAM CONNECTICUT DEPARTMENT OF PUBLIC HEALTH CONNECTICUT MOLST TASK FORCE OBJECTIVES 1. Define MOLST & historical development in United States and
Medical Orders for Life- Sustaining Treatment PILOT PROGRAM CONNECTICUT DEPARTMENT OF PUBLIC HEALTH CONNECTICUT MOLST TASK FORCE OBJECTIVES 1. Define MOLST & historical development in United States and
Model Policy for HOSPICES Physician Orders for Life Sustaining Treatment (POLST)
") Model Policy for HOSPICES Physician Orders for Life Sustaining Treatment (POLST) September 8, 2009 PURPOSE The purpose of this policy is to define a process for hospice providers to follow when a patient
Model Policy for HOSPICES Physician Orders for Life Sustaining Treatment (POLST) September 8, 2009 PURPOSE The purpose of this policy is to define a process for hospice providers to follow when a patient
Database Profiles for the ACT Index Driving social change and quality improvement
 Database Profiles for the ACT Index Driving social change and quality improvement 2 Name of database Who owns the database? Who publishes the database? Who funds the database? The Dartmouth Atlas of Health
Database Profiles for the ACT Index Driving social change and quality improvement 2 Name of database Who owns the database? Who publishes the database? Who funds the database? The Dartmouth Atlas of Health
Guidance for Oregon s Health Care Professionals
 Guidance for Oregon s Health Care Professionals www.or.polst.org Revised February 19, 2015 Table of Contents Introduction 1 Who Should Have a POLST Form... 2 How Advance Directives and POLST Work Together...
Guidance for Oregon s Health Care Professionals www.or.polst.org Revised February 19, 2015 Table of Contents Introduction 1 Who Should Have a POLST Form... 2 How Advance Directives and POLST Work Together...
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound
 Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Path to Transformation Concept Paper Comments and Recommendations. Palliative Care Community Partners (PCCP)
") Path to Transformation Concept Paper Comments and Recommendations Palliative Care Community Partners (PCCP) c/o Hospice Care of America, Inc., 3815 N Mulford Rd, Rockford, IL / (815)316-2697 As part of
Path to Transformation Concept Paper Comments and Recommendations Palliative Care Community Partners (PCCP) c/o Hospice Care of America, Inc., 3815 N Mulford Rd, Rockford, IL / (815)316-2697 As part of
Model Policy for SKILLED NURSING FACILITIES Physician Orders for Life Sustaining Treatment (POLST)
") Model Policy for SKILLED NURSING FACILITIES Physician Orders for Life Sustaining Treatment (POLST) March 12, 2013 PURPOSE The purpose of this policy is to define a process for skilled nursing facilities
Model Policy for SKILLED NURSING FACILITIES Physician Orders for Life Sustaining Treatment (POLST) March 12, 2013 PURPOSE The purpose of this policy is to define a process for skilled nursing facilities
Outline. I. Overview of QIO Care Transitions. II. Analyses: patient trajectory III. Palliative and end-of-life care
 Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
Chart Documentation Form
 Chart Documentation Form Aligns with Legal Requirements Checklist #4 Adult hospital or nursing home patients without medical decision-making capacity who do not have a health care proxy and for whom no
Chart Documentation Form Aligns with Legal Requirements Checklist #4 Adult hospital or nursing home patients without medical decision-making capacity who do not have a health care proxy and for whom no
South Carolina Coalition for Care of the Seriously Ill (CSI)
") South Carolina Coalition for Care of the Seriously Ill (CSI) Uniform Processes to Improve Consent, Communication, and Decision Making in South Carolina Hospitals Fifth Annual Patient Safety Symposium April
South Carolina Coalition for Care of the Seriously Ill (CSI) Uniform Processes to Improve Consent, Communication, and Decision Making in South Carolina Hospitals Fifth Annual Patient Safety Symposium April
The Evolution of Advance Care Planning and Advance Directives. Charles P. Sabatino, JD ABA Commission on Law and Aging February 23, 2012
 The Evolution of Advance Care Planning and Advance Directives Charles P. Sabatino, JD ABA Commission on Law and Aging February 23, 2012 1 The Crowded Landscape of State Legislation 1. Default Surrogate
The Evolution of Advance Care Planning and Advance Directives Charles P. Sabatino, JD ABA Commission on Law and Aging February 23, 2012 1 The Crowded Landscape of State Legislation 1. Default Surrogate
Health Care Proxy? Do I Need a Living Will? Disty Pearson PA-C Boston Adult Congenital Heart And Pulmonary Vascular Disease Service
 Health Care Proxy? Do I Need a Living Will? Disty Pearson PA-C Boston Adult Congenital Heart And Pulmonary Vascular Disease Service WHY? We need to agree that We are all going to pass Why? If we no longer
Health Care Proxy? Do I Need a Living Will? Disty Pearson PA-C Boston Adult Congenital Heart And Pulmonary Vascular Disease Service WHY? We need to agree that We are all going to pass Why? If we no longer
Model Colorado End-of-Life Options Act Hospice Policy & Procedures
 Model Colorado End-of-Life Options Act Hospice Policy & s [Name of institution] Administrative Policies and Operating s Section: Patient Care Services Policy Title : End-of-Life Care Organization Wide
Model Colorado End-of-Life Options Act Hospice Policy & s [Name of institution] Administrative Policies and Operating s Section: Patient Care Services Policy Title : End-of-Life Care Organization Wide
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
ADVANCE DIRECTIVE INFORMATION
 ADVANCE DIRECTIVE INFORMATION NOTE: This Advance Directive Information and the form Living Will and Durable Power of Attorney for Health Care on the Arkansas Bar Association s website are being provided
ADVANCE DIRECTIVE INFORMATION NOTE: This Advance Directive Information and the form Living Will and Durable Power of Attorney for Health Care on the Arkansas Bar Association s website are being provided
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
Module 6: End-of-Life Care in the Skilled Nursing Center
 Module 6: End-of-Life Care in the Skilled Nursing Center Lesson 2 NE QIN-QIO & Good Shepherd Community Care This material was prepared by the New England Quality Innovation Network-Quality Improvement
Module 6: End-of-Life Care in the Skilled Nursing Center Lesson 2 NE QIN-QIO & Good Shepherd Community Care This material was prepared by the New England Quality Innovation Network-Quality Improvement
Measuring the Quality of Palliative Care in the Intensive Care Unit. Mitchell Levy MD, J. Randall Curtis MD, MPH, John Luce MD, Judith Nelson JD, MD
 ICU Palliative Care Quality Assessment Tool Attending/Housestaff Survey Measuring the Quality of Palliative Care in the Intensive Care Unit Mitchell Levy MD, J. Randall Curtis MD, MPH, John Luce MD, Judith
ICU Palliative Care Quality Assessment Tool Attending/Housestaff Survey Measuring the Quality of Palliative Care in the Intensive Care Unit Mitchell Levy MD, J. Randall Curtis MD, MPH, John Luce MD, Judith
Living Wills and Other Advance Directives
 UW MEDICINE PATIENT EDUCATION Living Wills and Other Advance Directives Writing down your choices for health care for times when you cannot speak for yourself This handout gives basic information about
UW MEDICINE PATIENT EDUCATION Living Wills and Other Advance Directives Writing down your choices for health care for times when you cannot speak for yourself This handout gives basic information about
Adult: Any person eighteen years of age or older, or emancipated minor.
 Advance Directives Policy and Procedure Purpose To provide an atmosphere of respect and caring and to ensure that each patient's ability and right to participate in medical decision making is maximized
Advance Directives Policy and Procedure Purpose To provide an atmosphere of respect and caring and to ensure that each patient's ability and right to participate in medical decision making is maximized
Talking to Your Doctor About Hospice Care
 Talking to Your Doctor About Hospice Care Death and dying subjects that were once taboo in our culture are becoming increasingly relevant as more Americans care for their aging parents and consider what
Talking to Your Doctor About Hospice Care Death and dying subjects that were once taboo in our culture are becoming increasingly relevant as more Americans care for their aging parents and consider what
Preparing for DSRIP: Legal and Strategic Issues for Long-Term Care Providers. LeadingAge New York Webinar
 Preparing for DSRIP: Legal and Strategic Issues for Long-Term Care Providers LeadingAge New York Webinar November 10, 2014 Tracy E. Miller, Esq. Health Care Group Bond, Schoeneck & King, PLLC Delivery
Preparing for DSRIP: Legal and Strategic Issues for Long-Term Care Providers LeadingAge New York Webinar November 10, 2014 Tracy E. Miller, Esq. Health Care Group Bond, Schoeneck & King, PLLC Delivery
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
ILLINOIS Advance Directive Planning for Important Health Care Decisions
 ILLINOIS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
ILLINOIS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
Advance Care Planning Exploratory Project. Rhonda Wiering, MSN, RN,BC, LNHA Regional Director, Quality Initiatives Avera Health October 18, 2012
 Advance Care Planning Exploratory Project Rhonda Wiering, MSN, RN,BC, LNHA Regional Director, Quality Initiatives Avera Health October 18, 2012 Agenda Overview of the Advance Care Planning Exploration
Advance Care Planning Exploratory Project Rhonda Wiering, MSN, RN,BC, LNHA Regional Director, Quality Initiatives Avera Health October 18, 2012 Agenda Overview of the Advance Care Planning Exploration
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Objectives. Integrating Palliative Care Principles into Critical Care Nursing
 1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
Nursing Home Model Policy for West Virginia Physician Orders for Scope of Treatment (POST)
") Nursing Home Model Policy for West Virginia Physician Orders for Scope of Treatment (POST) POLICY STATEMENT: It is the policy of [Name of Facility] to support the rights of residents to make decisions
Nursing Home Model Policy for West Virginia Physician Orders for Scope of Treatment (POST) POLICY STATEMENT: It is the policy of [Name of Facility] to support the rights of residents to make decisions
What is POLST? Physician Orders for Life Sustaining Treatment
 What is POLST? Physician Orders for Life Sustaining Treatment Why POLST? 1. Patient wishes often are not known. The Advance Healthcare Directive (AHCD) may not be accessible. Wishes may not be clearly
What is POLST? Physician Orders for Life Sustaining Treatment Why POLST? 1. Patient wishes often are not known. The Advance Healthcare Directive (AHCD) may not be accessible. Wishes may not be clearly
The California End of Life Option Act (Patient s Request for Medical Aid-in-Dying)
") Office of Origin: I. PURPOSE II. III. A. The California authorizes medical aid in dying and allows an adult patient with capacity, who has been diagnosed with a terminal disease with a life expectancy
Office of Origin: I. PURPOSE II. III. A. The California authorizes medical aid in dying and allows an adult patient with capacity, who has been diagnosed with a terminal disease with a life expectancy
483.10(b)(4) and (8) Rights Regarding Advance Directives, Treatment, and Experimental Research
(4) and (8) Rights Regarding Advance Directives, Treatment, and Experimental Research") 483.10(b)(4) and (8) Rights Regarding Advance Directives, Treatment, and Experimental Research (F155) Surveyor Training of Trainers: Interpretive Guidance Investigative Protocol Federal Regulatory Language
483.10(b)(4) and (8) Rights Regarding Advance Directives, Treatment, and Experimental Research (F155) Surveyor Training of Trainers: Interpretive Guidance Investigative Protocol Federal Regulatory Language
Better Ending. A Guide. for a A SSURE Y OUR F INAL W ISHES. Conversations Before the Crisis
 A Guide for a Better Ending A SSURE Y OUR F INAL W ISHES Conversations Before the Crisis Information on Advance Care Planning and Documentation from Better Ending, a Program of the Central Massachusetts
A Guide for a Better Ending A SSURE Y OUR F INAL W ISHES Conversations Before the Crisis Information on Advance Care Planning and Documentation from Better Ending, a Program of the Central Massachusetts
ADVANCE PLANNING FOR END-OF-LIFE CARE: A PRACTICAL INTRODUCTION
 ADVANCE PLANNING FOR END-OF-LIFE CARE: A PRACTICAL INTRODUCTION WFUBMC Clinical Ethics Committee February 18, 2011 John C. Moskop, Ph.D. Wu Chair in Biomedical Ethics, Professor of Internal Medicine, WFUSOM
ADVANCE PLANNING FOR END-OF-LIFE CARE: A PRACTICAL INTRODUCTION WFUBMC Clinical Ethics Committee February 18, 2011 John C. Moskop, Ph.D. Wu Chair in Biomedical Ethics, Professor of Internal Medicine, WFUSOM
HOSPICE IN MINNESOTA: A RURAL PROFILE
 JUNE 2003 HOSPICE IN MINNESOTA: A RURAL PROFILE Background Numerous national polls have found that when asked, most people would prefer to die in their own homes. 1 Contrary to these wishes, 75 percent
JUNE 2003 HOSPICE IN MINNESOTA: A RURAL PROFILE Background Numerous national polls have found that when asked, most people would prefer to die in their own homes. 1 Contrary to these wishes, 75 percent
ADVANCE CARE PLANNING: REDESIGNING PATIENT-CENTERED CARE
 ADVANCE CARE PLANNING: REDESIGNING PATIENT-CENTERED CARE Christine Wilkins, Ph.D., LCSW March 12, 2018 Why an ACP Program? Despite increased awareness, many do not have advance directives Even when a health
ADVANCE CARE PLANNING: REDESIGNING PATIENT-CENTERED CARE Christine Wilkins, Ph.D., LCSW March 12, 2018 Why an ACP Program? Despite increased awareness, many do not have advance directives Even when a health
and Affiliates Policy & Procedure Date of Origin: 10/95 Last Reviewed: 12/03 Last Revised: 12/03
 Table of Contents Topic Policy Procedure Page # Page # Purpose and Scope 1 11 Definitions.. 2 - Capacity.. 3 - Who May Consent. 5 - Consent Process. - 13 Levels of Care/Additional Treatment Guidelines
Table of Contents Topic Policy Procedure Page # Page # Purpose and Scope 1 11 Definitions.. 2 - Capacity.. 3 - Who May Consent. 5 - Consent Process. - 13 Levels of Care/Additional Treatment Guidelines
Your Guide to Advance Directives
 Starting Points: Your Guide to Advance Directives Values Statements Healthcare Directives Durable Power of Attorney for Healthcare 1 2 Advances in medicine are helping people to live longer than ever before.
Starting Points: Your Guide to Advance Directives Values Statements Healthcare Directives Durable Power of Attorney for Healthcare 1 2 Advances in medicine are helping people to live longer than ever before.
END-OF-LIFE CARE STRATEGIC PLAN FOR NEW JERSEY
 NEW JERSEY HEALTH CARE QUALITY INSTITUTE END-OF-LIFE CARE STRATEGIC PLAN FOR NEW JERSEY New Jersey Health Care Quality Institute End-of-Life Care Strategic Plan for New Jersey 1 Executive Summary At the
NEW JERSEY HEALTH CARE QUALITY INSTITUTE END-OF-LIFE CARE STRATEGIC PLAN FOR NEW JERSEY New Jersey Health Care Quality Institute End-of-Life Care Strategic Plan for New Jersey 1 Executive Summary At the
Administrative Guide. KanCare Program Chapter 11: Hospice. Physician, Health Care Professional, Facility and Ancillary. UHCCommunityPlan.
 KanCare Program Physician, Health Care Professional, Facility and Ancillary Administrative Guide Doc#: PCA-1-003044_06202016 UHCCommunityPlan.com Welcome to UnitedHealthcare This administrative guide is
KanCare Program Physician, Health Care Professional, Facility and Ancillary Administrative Guide Doc#: PCA-1-003044_06202016 UHCCommunityPlan.com Welcome to UnitedHealthcare This administrative guide is
HealthStream Regulatory Script
 HealthStream Regulatory Script Advance Directives Release Date: August 2008 HLC Version: 602 Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney
HealthStream Regulatory Script Advance Directives Release Date: August 2008 HLC Version: 602 Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney
Palliative Care. Care for Adults With a Progressive, Life-Limiting Illness
 Palliative Care Care for Adults With a Progressive, Life-Limiting Illness Summary This quality standard addresses palliative care for people who are living with a serious, life-limiting illness, and for
Palliative Care Care for Adults With a Progressive, Life-Limiting Illness Summary This quality standard addresses palliative care for people who are living with a serious, life-limiting illness, and for
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
OHIO SB 165. Proponents Talking Points & Responses to Talking Points Regarding MOLST
 OHIO SB 165 Proponents Talking Points & Responses to Talking Points Regarding MOLST S.B. 165 would establish procedures for the use of the MOLST form in Ohio. MOLST refers to medical orders for life-sustaining
OHIO SB 165 Proponents Talking Points & Responses to Talking Points Regarding MOLST S.B. 165 would establish procedures for the use of the MOLST form in Ohio. MOLST refers to medical orders for life-sustaining
The District of Columbia Death with Dignity Act (Patient Request for Medical Aid-in-Dying)
") Office of Origin: I. PURPOSE II. A. authorizes medical aid in dying and allows an adult patient with capacity, who has been diagnosed with a terminal disease with a life expectancy of six months or less,
Office of Origin: I. PURPOSE II. A. authorizes medical aid in dying and allows an adult patient with capacity, who has been diagnosed with a terminal disease with a life expectancy of six months or less,
(f) Department means the New Hampshire department of health and human services.
 Department means the New Hampshire department of health and human services.") Adopted Rule 6/16/10. Effective: 7/1/10 1 Adopt He-W 544.01 544.16, cited and to read as follows: CHAPTER He-W 500 MEDICAL ASSISTANCE PART He-W 544 HOSPICE SERVICES He-W 544.01 Definitions. (a) Agent means
Adopted Rule 6/16/10. Effective: 7/1/10 1 Adopt He-W 544.01 544.16, cited and to read as follows: CHAPTER He-W 500 MEDICAL ASSISTANCE PART He-W 544 HOSPICE SERVICES He-W 544.01 Definitions. (a) Agent means
For more information and additional resources go to Name:
 Durable Power of Attorney for Health Care & Health Care Directive Documents are legally valid in Alaska, California, Idaho, Montana, and Washington. What is advance care planning? Advance care planning
Durable Power of Attorney for Health Care & Health Care Directive Documents are legally valid in Alaska, California, Idaho, Montana, and Washington. What is advance care planning? Advance care planning
POLST Cue Card. If you die a natural death, would you want us to try CPR? If yes Requires Full Treatment in Section B. (Ask about Ventilator Trial)
") POLST Cue Card It s important to talk about your health and your wishes for medical care if you got really sick. We talk about this with everyone with serious illness. Your doctor will review what we talk
POLST Cue Card It s important to talk about your health and your wishes for medical care if you got really sick. We talk about this with everyone with serious illness. Your doctor will review what we talk
Having the End of Life Conversation: Practical Concepts for Advocacy Within the Continuum of Care
 Having the End of Life Conversation: Practical Concepts for Advocacy Within the Continuum of Care July 24, 2012 Presented by: Cindy Campbell RN, BSN Associate Director, Operational Consulting Fazzi Associates
Having the End of Life Conversation: Practical Concepts for Advocacy Within the Continuum of Care July 24, 2012 Presented by: Cindy Campbell RN, BSN Associate Director, Operational Consulting Fazzi Associates
POLST Legislative Guide
 POLST Legislative Guide Approved February 28, 2014 National POLST Paradigm Task Force Introduction The development of the Physician Orders for Life-Sustaining Treatment (POLST) Paradigm has generated range
POLST Legislative Guide Approved February 28, 2014 National POLST Paradigm Task Force Introduction The development of the Physician Orders for Life-Sustaining Treatment (POLST) Paradigm has generated range
Facing Serious Illness: Make Your Wishes Known to your Health Care Professional
 Facing Serious Illness: Make Your Wishes Known to your Health Care Professional Your Guide to the Oregon POLST Program Physician Orders for Life-Sustaining Treatment Revised: February 19, 2015 This material
Facing Serious Illness: Make Your Wishes Known to your Health Care Professional Your Guide to the Oregon POLST Program Physician Orders for Life-Sustaining Treatment Revised: February 19, 2015 This material
Five Myths of Advance Care Planning. Charles P. Sabatino, JD, Director ABA Commission on Law and Aging April 13, 2010
 Five Myths of Advance Care Planning Charles P. Sabatino, JD, Director ABA Commission on Law and Aging April 13, 2010 1 Myth 1: People should use their state s official advance directive forms Official
Five Myths of Advance Care Planning Charles P. Sabatino, JD, Director ABA Commission on Law and Aging April 13, 2010 1 Myth 1: People should use their state s official advance directive forms Official
MY CHOICES. Information on: Advance Care Directive Living Will POLST Orders
 MY CHOICES Information on: Advance Care Directive Living Will POLST Orders My Choices Adults have the right to accept or refuse medical care. As long as you can make health care decisions for yourself,
MY CHOICES Information on: Advance Care Directive Living Will POLST Orders My Choices Adults have the right to accept or refuse medical care. As long as you can make health care decisions for yourself,
Maryland MOLST FAQs. Maryland MOLST Training Task Force
 Maryland MOLST FAQs Maryland MOLST Training Task Force October 2017 Frequently Asked Questions About Maryland MOLST What does MOLST stand for? MOLST is an acronym that stands for Medical Orders for Life-Sustaining
Maryland MOLST FAQs Maryland MOLST Training Task Force October 2017 Frequently Asked Questions About Maryland MOLST What does MOLST stand for? MOLST is an acronym that stands for Medical Orders for Life-Sustaining
Wishing Will Not Solve Anything
 Maximizing End-of Life Decisions: at an imperfect time in an imperfect World Nuances, Confusion & Misinformation DNR Family 5 Wishes Guardianship HCP Guilt DNI AND Communication Compassionate Choices Advance
Maximizing End-of Life Decisions: at an imperfect time in an imperfect World Nuances, Confusion & Misinformation DNR Family 5 Wishes Guardianship HCP Guilt DNI AND Communication Compassionate Choices Advance