Advance Care Planning: Goals of Care - Calgary Zone
|
|
|
- Lindsey Scarlett Hardy
- 6 years ago
- Views:
Transcription
1 Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST 1
2 Advance Care Planning: Goals of Care Calgary Zone LOOKING BACK OVERVIEW AND HISTORY OF THE ACP/GCD PROGRAM IN THE CALGARY ZONE KEY LEARNINGS RE: POLICY IMPLEMENTATION MOVING FORWARD ACP/GCD RESOURCES GOALS OF THE CURRENT TEAM PROVINCIAL PLANNING CURRENT RESEARCH FINDINGS CHART AUDIT DATA ACCEPT STUDY 2
3 Advance Care Planning: Goals of Care: Calgary Zone The Advance Care Planning: Goals of Care Designation (Adult) (ACP: GCD) policy was launched across all sectors of the former Calgary Health Region on November 25, The Pediatric Policy was implemented in The implementation of these policies were groundbreaking in Alberta and across the country and continues to guide national standards and practice. The development and implementation of these policies was a collaborative effort by many clinicians, program leaders and champions, and was led by the Care at the End of Life Initiative. 3
4 Advance Care Planning: Goals of Care: Calgary Zone The support of ongoing dedicated resources for the integration of this policy has provided the ability to evaluate the progress of implementation and identify outcomes and strategic opportunities for continued growth and improvement The ACP/GCD policy exemplifies the key AHS strategic directions of quality, access and sustainability. The policy implementation activities integrate a quality improvement approach, resulting in ongoing learning to inform related clinical practices. 4
5 Advance Care Planning: Goals of Care: Calgary Zone Access is improved for our patients when there is consensus regarding goals of care. It supports the right care in the right place by being respectful of the patient and family wishes for end of life. The policy supports sustainability as it assists with the elimination of treatments and interventions considered medically inappropriate or those that do not align with an individual s goals for their care. 5
6 Advance Care Planning: Goals of Care: Calgary Zone Pre Change The rationale behind this change: Levels of Care are defined differently within the various adult resuscitation policies in the Region. There was no established process or framework to support individuals in decisionmaking about health care goals. Documentation of decisions regarding health care was inconsistent. Access to documentation of decisions made in other sectors was unpredictable. The Change Provides one policy and framework applicable across the continuum. Replace Levels of Care with Goals of Care Designations throughout the Region. Supports individuals in expressing their wishes and values for health care within the context of medically appropriate treatments. Works to ensures that the outcomes of discussions are documented and available to all health care teams. 6
7 Advance Care Planning: Goals of Care: Calgary Zone Key Features of the Processes & Policy Focus is on the Goals of care A Patient Centric Approach that integrates patient s values, wishes and goals in the context of medically appropriate treatment Ensures infrastructure and processes to support Advance Care Planning. Decisions are honored system wide with a process of documentation and communication to ensure this. Congruent wit the Personal Directives Legislation Provides the framework and tools for clinicians to be able meet the criteria of the policy Provides resources for individuals and families to engage in advance care planning The Goals of care are based on ACP conversations Goals of Care and wishes change over time Provides direction regarding interventions, and location of care. 7
8 Advance Care Planning: Goals of Care: Calgary Zone Adult vs Pediatric Policy Applies only when clinically relevant Respects child/family dynamic Location of care options unique to pediatrics Provision for Mature Minor 8

9 Advance Care Planning: Goals of Care: Calgary Zone Process of arriving at a Goals of Care Order R Medical Care and Interventions including Resuscitation followed by ICU M Medical Care and Interventions, excluding Resuscitation C Medical Care and Interventions, focused on Comfort Diagnosis Prognosis Anticipated Outcomes Wishes and Values Life Support / Life Sustaining Benefits Comfort Measures Resources Cure or control of condition with option for resuscitation Cure or control, no resuscitation Alleviate the symptoms 9

10 Advance Care Planning: Goals of Care: Calgary Zone 10
11 ACP/GCD Calgary Zone Resources Adults: My Voice Planning Ahead Video My Voice Planning Ahead Brochure Understanding Goals of Care Designation Brochure My Voice Workbook Goals of Care Designation Order Form ACP Tracking Record Quick reference pocket cards and posters Pediatrics: Hear My Voice - an activity for families who are coping with a potential illness to encourage them to talk about their values and goals to guide decision making during the illness experience. Hear Our Voice - workbook for parents and guardians to support advance care for children and youth. 11
12 ACP/GCD Calgary Zone Resources Advance Care Planning and Goals of Care training modules for Adults and Pediatrics Adult and Pediatric policies Links to relevant resources and sites 12
13 Key Learning Regarding GCD/ACP Implementation Themes: Leadership & Accountability Education Communication and Engagement Strategies Resources Evaluation and Quality Improvement 13
14 Advance Care Planning: Goals of Care: Calgary Zone MOVING FORWARD 14
15 Advance Care Planning: Goals of Care: Calgary Zone Setting New Vision For the Work The Current Team Continued Integration of the Policy Working with strategies from the chart audit report Engagement with clinicians, patients and public Establishing educational methodologies Reviewing all tools and resources In collaboration with provincial work 15
16 Advance Care Planning: Goals of Care - Calgary Zone Team Roles: Bev Berg, Coordinator Dr. Jessica Simon, Physician Consultant Chandra Vig, Education Consultant Tracy Lynn Wityk Martin, Quality Improvement Specialist Tannis Dorscht, Administrative Support 16
17 Advance Care Planning: Goals of Care Calgary Zone Advance Care Planning is a Process that involves 1. Thinking about values and wishes regarding future health care choices. 2. Learning about medical information that is relevant to their health concerns 3. Choosing an agent and Communicating wishes and values to a designated agent, loved ones and health care providers. 4. Documenting choices, wishes and values. the designated agent(s), loved ones and health care provider 17
18 An Advance Care Plan Advance care plans are verbal or written instructions, made while the individual is still capable, describing what kind of care they would want (or not want) if they become incapable of communicating to others. These plans are made by the individual. No one can make an advance care plan for another person. To be eligible to make an advance care plan in Alberta an individual must be at least 18 years old and be capable of understanding the nature of consequences of their health care choices. Advance care plans communicate when the individual is not able to. The plan, whether verbal or written, becomes their voice. As long as a person is able to understand their health care providers, and can communicate for themselves, doctors, nurses and other health care providers will talk to them about their preferences for health care. A Personal Directive is a written document that enables individuals to give direction and clarification to health professionals and other service providers in accordance with the Personal Directives Act (Alberta). A Personal Directive is effective legally only when the maker of the Personal Directive lacks capacity. While a Personal Directive from another Province or Country may not be valid in Alberta, the document may serve as a guide to help decision-making. 18
19 Advance Care Planning: Goals of Care: Calgary Zone This work continues to be relevant for a number of critical reasons: According to Statistics Canada: 248,000 Canadians die each year In 2020 this number will have increased to 330,000 According to the 2009 CHPCA roundtable on Advance Care Planning: Up to 50% of persons cannot make their own decisions at the end of life (CHPCA) Health professionals typically treat when uncertain of treatment wishes Hospitals remain the major provider of EOL care as 70% of Canadians die in a hospital with one in five of these hospitalized deaths occurring in an ICU Loved ones have a significant chance of not knowing a person s view without discussion 19
20 Advance Care Planning: Goals of Care: Calgary Zone Current Research demonstrates: The absence of Advance Care planning is associated with worse patient and family ratings of quality of life in the terminal phase of illness Those who have end of life conversations with loved ones and health care professionals: Require fewer aggressive medical interventions at the end of life Are more likely to take advantage of relevant resources at end of life Surviving family feel less of a burden with decision making and have reduced suffering/distress in times of bereavement. 20
21 Advance Care Planning: Goals of Care: Calgary Zone Advance Care Planning is a personal issue for everyone. None of us know when we might be involved in an accident or have a physical event that makes it impossible for us to communicate our preferences for medical care. We can all become seriously ill, incapacitated, or be diagnosed with a medical condition that may slowly take away our ability to communicate. Planning ahead helps those we are close to, and health care agents, know and understand our wishes to guide health care decision making. What we ask of others we should consider for ourselves. 21

22 Advance Care Planning: Goals of Care: Calgary Zone Karen Ann Quinlan 1975 age 21 Nancy Cruzan 1983 age 25 Terri Schaivo 1990 age 26 22
23 Advance Care Planning: Goals of Care: Calgary Zone Engage With Grace - The One Slide Project 23
24 Advance Care Planning: Goals of Care Calgary Zone The relevance of ACP/GCD varies according to health conditions and needs. Many chronic conditions have an illness trajectory that can be predicted. Advance care planning enables individuals to investigate treatments as their condition progresses, including the option to trial specific interventions. Calgary Zone story. Seniors live with an awareness that they are nearing the end of their lives and often worry about being a burden to their families. They have experienced the death of friends which may encourage them to plan for their own end of life. ACP research is more prevalent in the last ten years and often focuses on these populations. 24
25 Advance Care Planning: Goals of Care: Calgary Zone Common Barriers and Facilitators for engaging in ACP are: Patient Barriers Perceiving ACP as irrelevant Relationship concerns worried about discussing this with loved ones Need for more information Time constraints in medical encounters The Fear of having discussions regarding end of life care Patient Facilitators More willingness to engage in ACP with individuals who have experienced or witnessed end of life care in loved ones Not wanting to be a burden on loved ones Understanding of life support/ sustaining interventions and the benefits of treatment Compassionate conversations about end of life care 25
26 Advance Care Planning: Goals of Care: Calgary Zone HCP Barriers: Lack of confidence and skills in engaging in the conversation Time constraints The nature of the dialogue Fear of taking away hope HCP Facilitators Skills and confidence in engaging in conversations Patient experiences Personal Experiences 26
27 Current Research In a study conducted by Detering et al,(2010) in Australia 309 medical inpatients aged 80+ were followed for six months or until death. Randomized to two groups usual care and usual care with advance care planning Of the group randomized to ACP 84% expressed wishes or appointed a surrogate, or both Of the 56 patients, of the total study, who died by six months end of life wishes were more likely to be known and followed in the intervention group than the control group, family members had significantly less stress, anxiety and depression and patient and family satisfaction was higher. These authors identify that without the documentation of patient wishes patients may be cared for in a way they would not have chosen at the end of their life. The process of advance care planning informs and empowers patients to have a say about their current and future treatment. P,1. 27
28 Current Research Silveira et al ( 2010) reported the results of an observational, longitudinal study of 3756 elderly Americans and found that the majority need decision-making at the end of life at a time when they lacked the capacity to make decisions Patients who had prepared advance directives received care that was strongly associated with their preferences and the majority preferred limited care or comfort care (only 1.9% wanted all care possible). 28
29 Current Research In another observational study of terminal cancer patients conducted by Wright et al., 2008, the absence of ACP in any of its forms was associated with worse patient ratings of quality of life in the terminal phase of the illness, worse ratings of satisfaction by the family during the terminal illness, and increased family ratings of anxiety and depression. In contrast, when physicians and patients/families engage in ACP, there is less intensification of care (use of intensive care units, lifesustaining technologies, or feeding tube insertions) and more usage of hospice services. Surviving caregivers experienced less regret and showed overall improvements in quality of life during the bereavement period. 29
30 Patient Education Videos Current Research ACP Patient Education Videos have been developed by the Nous Foundation in the USA to help patients make informed decisions. It is a patient-centered supplemental tool to reinforce information introduced by the clinician that empowers patients and their families to make informed decisions consistent with their values. The use and development of video aids is capturing great attention regarding a more informed method of ACP and determining goals of care. 30
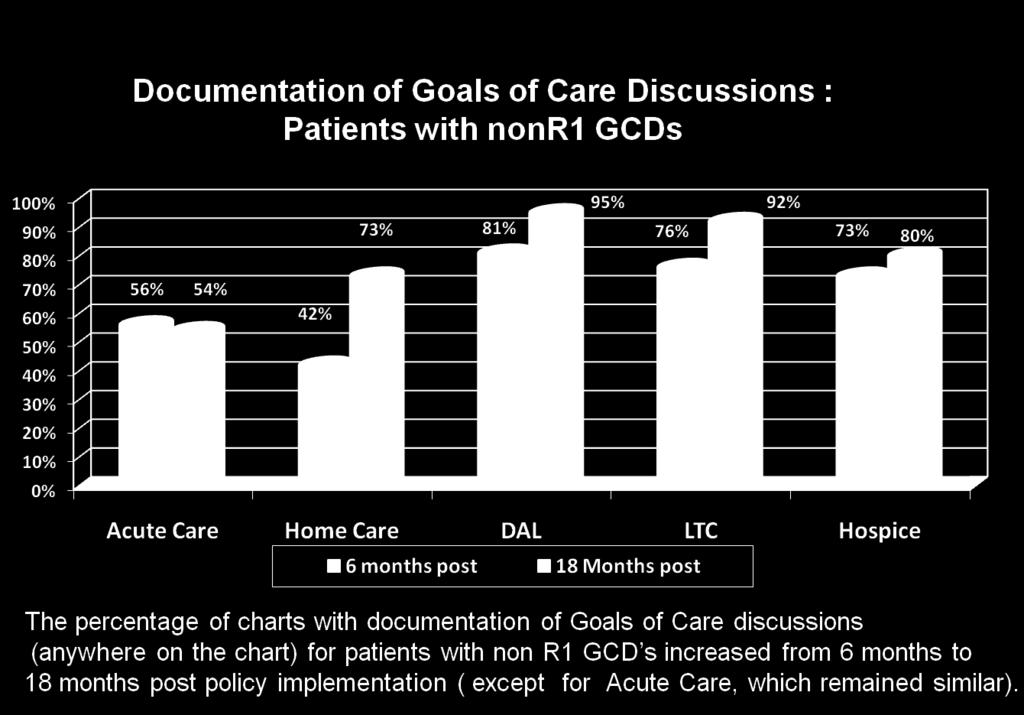
31 Volandes et a., 2011) Conducted a randomized controlled trial of a video decision aid of the goals of care In advanced-dementia among a diverse group of elderly patents in a rural community. 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 72% 16% 12% VERBAL 91% 9% VIDEO Comfort Limited Life Prolonging 31
32 Current Research El-jawalri, et al. ( 2010) conducted a study to determine if a a goals of care video to supplement a verbal description improved end of life decision making for patients with cancer. Participants who viewed the video were more likely to prefer comfort care and void CPR. In both studies the majority of patients: Felt comfortable watching the video Would recommend it for other patients to view Felt that it improved their understanding of levels of care and interventions main shtml 32
33 Advance Care Planning: Goals of Care Calgary Zone Three chart audits have been conducted to measure the success and guide the continued integration of the policy across all adult health care sectors in the Calgary Zone. These audits occurred at baseline (before implementation), and at 6 months and 18 months post implementation. 33
34 Advance Care Planning: Goals of Care Calgary Zone A total of 947 charts were reviewed in Summer/Fall 2010 across all sectors: Acute Care (3 urban sites (9 units), 2 rural sites) Home Care (Palliative and Seniors Teams) Designated Assisted Living (2 DAL sites) Long Term Care (LTC; 4 urban, 1 rural) Hospices (3 sites) 34
35 Advance Care Planning: Goals of Care Calgary Zone Charts were randomly selected from those that focused on patients that would be most likely to require a Goals of Care Designation (GCD) and to benefit from Advance Care Planning (ACP) (including 50 years of age and older and targeted units/teams). The results may not be generalizable to the overall patient/client population served in these sectors. All charts reviewed in this third phase of the chart audit were of current patients. 35
36 Outcomes Outcome 1: Advance Care Planning: Goals of Care Designation (Adult) policy has been successfully implemented across AHS, Calgary Zone - Achieved Outcome 2: Information related to future health care decisions transferred across the service streams - Achieved Outcome 3: Patients' preferences as identified in their medical charts and/or advance directives are followed as they receive medically appropriate end of life care - Achieved 36


37 Presence of Goals of Care Designation (GCD) Order 37

38 Distribution of GCDs 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Acute Care 6 mos. Acute Care 18 mos. Home Care 6 mos. Home Care 18 mos. DAL 6 mos. DAL 18 mos. LTC 6 mos. LTC 18 mos. Hospice 6 mos. Hospice 18 mos. C2 C1 M2 M1 R3 R2 R1 Distributions of GCDs varied by sector and appeared to reflect the general acuity and goals of care for the various populations served. 38
 18 months post-documented discussions (any location) 18 months")

39 Documentation of ACP Discussion (patients with a GCD) 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 85% 89% 89% 89% 88% 77% 73% 80% 69% 69% 33% 41% 38% 21% Acute Care Home Care DAL LTC Hospice 6 months post-documented discussions (any location) 18 months post-documented discussions (any location) 18 months post-documented discussions on ACP Tracking Record 40% Every sector increased the percentage of charts that had any Documentation of Advance Care Planning/Goals of Care discussions from baseline to 6 months to 18 months post policy implementation ( except for DAL, which maintained its 6 month post policy rate). 39
40 40


41 Transfer of Information between LTC/DAL and ED/Acute Care 41

42 Preferences Followed at End of Life Across all sectors, patient preferences for future health care decisions as documented in their medical charts were followed almost 100% of the time. 42

43 Resource utilization of Deceased Patients by GCD 43
44 Advance Care Planning: Goals of Care Calgary Zone Areas for Quality Improvement : Next Steps 1. Enhance the use and transfer of the ACP Tracking Record 2. Education and Quality Improvement activities regarding the transfer of information between service streams 3. Advance Care Planning discussions enhance clinician comfort, skill, and documentation 4. Engaging physicians in the community regarding completing GCD Orders 5. Additional public education to increase comfort with ACP/GCD discussions and process 6. Conduct research regarding the patient/family s experience and perspective of ACP/GCD - The ACCEPT Study 44
ADVANCE CARE PLANNING CONVERSATIONS MATTER GOALS OF CARE DESIGNATIONS
 ADVANCE CARE PLANNING CONVERSATIONS MATTER GOALS OF CARE DESIGNATIONS 1 Objectives Advance Care Planning (ACP) What is it? Why? For Who? Personal directives Advance Care Planning in the healthcare system
ADVANCE CARE PLANNING CONVERSATIONS MATTER GOALS OF CARE DESIGNATIONS 1 Objectives Advance Care Planning (ACP) What is it? Why? For Who? Personal directives Advance Care Planning in the healthcare system
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE ADVANCE CARE PLANNING AND GOALS OF CARE DESIGNATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Seniors Health PARENT DOCUMENT TITLE, TYPE AND NUMBER Not Applicable
TITLE ADVANCE CARE PLANNING AND GOALS OF CARE DESIGNATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Seniors Health PARENT DOCUMENT TITLE, TYPE AND NUMBER Not Applicable
Cancer and Advance Care Planning. Tips for Oncology Professionals
 Cancer and Advance Care Planning Tips for Oncology Professionals Each year, more than 74,000 Canadians die with cancer. When To Have the Discussion...5 Questions to Ask...6 Steps in Initiating and Having
Cancer and Advance Care Planning Tips for Oncology Professionals Each year, more than 74,000 Canadians die with cancer. When To Have the Discussion...5 Questions to Ask...6 Steps in Initiating and Having
Advanced Care Planning and Advanced Directives: Our Roles March 27, 2017
 Advanced Care Planning and Advanced Directives: Our Roles March 27, 2017 2017 NPSS Asheville, NC Overview History of Advanced Directives Importance of Advanced Care Planning for Quality care Our Role in
Advanced Care Planning and Advanced Directives: Our Roles March 27, 2017 2017 NPSS Asheville, NC Overview History of Advanced Directives Importance of Advanced Care Planning for Quality care Our Role in
Quality of Life Conversation On Advance Care Planning
 Quality of Life Conversation On Advance Care Planning Information Packet Page 1 About the Integrated Healthcare Association The nonprofit Integrated Healthcare Association (IHA) convenes diverse stakeholders,
Quality of Life Conversation On Advance Care Planning Information Packet Page 1 About the Integrated Healthcare Association The nonprofit Integrated Healthcare Association (IHA) convenes diverse stakeholders,
Advance Care Planning: Backgrounder. OMA s End-of-Life Care Strategy April 2014
 Advance Care Planning: Backgrounder OMA s End-of-Life Care Strategy April 2014 Definition/Legal Foundation Advance care planning (ACP) is a process of considering, discussing and planning for future health
Advance Care Planning: Backgrounder OMA s End-of-Life Care Strategy April 2014 Definition/Legal Foundation Advance care planning (ACP) is a process of considering, discussing and planning for future health
Advance Care Planning: the Clients Perspectives
 Dr. Yvonne Yi-wood Mak; Bradbury Hospice / Pamela Youde Nethersole Eastern Hospital Correspondence: fangmyw@yahoo.co.uk Definition Advance care planning [ACP] is a process of discussion among the patient,
Dr. Yvonne Yi-wood Mak; Bradbury Hospice / Pamela Youde Nethersole Eastern Hospital Correspondence: fangmyw@yahoo.co.uk Definition Advance care planning [ACP] is a process of discussion among the patient,
CHPCA appreciates and thanks our funding partner GlaxoSmithKline for their unrestricted funding support for Advance Care Planning in Canada.
 CHPCA appreciates and thanks our funding partner GlaxoSmithKline for their unrestricted funding support for Advance Care Planning in Canada. For more information about advance care planning, please visit
CHPCA appreciates and thanks our funding partner GlaxoSmithKline for their unrestricted funding support for Advance Care Planning in Canada. For more information about advance care planning, please visit
MY VOICE (STANDARD FORM)
") MY VOICE (STANDARD FORM) a workbook and personal directive for advance care planning WHAT IS ADVANCE CARE PLANNING? Advance care planning is a process for you to: think about what is important to you when
MY VOICE (STANDARD FORM) a workbook and personal directive for advance care planning WHAT IS ADVANCE CARE PLANNING? Advance care planning is a process for you to: think about what is important to you when
Advance Care Planning: Whose Conversation is it Anyway?
 CNA Webinar Series: Progress in Practice Advance Care Planning: Whose Conversation is it Anyway? Louise Hanvey Registered nurse, project director, advance care planning expert, content strategist May 24,
CNA Webinar Series: Progress in Practice Advance Care Planning: Whose Conversation is it Anyway? Louise Hanvey Registered nurse, project director, advance care planning expert, content strategist May 24,
RIGHTS OF PASSAGE A NEW APPROACH TO PALLIATIVE CARE. INSIDE Expert advice on HIV disclosure. The end of an era in Afghanistan
 Publications Mail Agreement Number 40062599 NOVEMBER 2013 VOLUME 109 NUMBER 9 RIGHTS OF PASSAGE A NEW APPROACH TO PALLIATIVE CARE INSIDE Expert advice on HIV disclosure The end of an era in Afghanistan
Publications Mail Agreement Number 40062599 NOVEMBER 2013 VOLUME 109 NUMBER 9 RIGHTS OF PASSAGE A NEW APPROACH TO PALLIATIVE CARE INSIDE Expert advice on HIV disclosure The end of an era in Afghanistan
DNR Orders: The Demise of a Dinosaur?
 Pediatric Goals of Care: Transitioning Into a New Pediatric Advance Care Planning Policy in Calgary April 29, 2009 Anna C. Zadunayski, LL.B, MSc (Student) Sharron Spicer, B.Sc., MD, FRCPC, Division Chief,
Pediatric Goals of Care: Transitioning Into a New Pediatric Advance Care Planning Policy in Calgary April 29, 2009 Anna C. Zadunayski, LL.B, MSc (Student) Sharron Spicer, B.Sc., MD, FRCPC, Division Chief,
PATIENT RIGHTS, PRIVACY, AND PROTECTION
 REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
Advance Care Planning: Goals of Care Designation
 Advance Care Planning: Goals of Care Designation Approved by: Vice President and Chief Medical Officer; and Vice President, Mission, Ethics & Spirituality Corporate Policy & Procedures Manual Number: Date
Advance Care Planning: Goals of Care Designation Approved by: Vice President and Chief Medical Officer; and Vice President, Mission, Ethics & Spirituality Corporate Policy & Procedures Manual Number: Date
Advance Care Planning. Ken Brummel-Smith, MD Charlotte Edwards Maguire Professor of Geriatrics FSU College of Medicine
 Advance Care Planning Ken Brummel-Smith, MD Charlotte Edwards Maguire Professor of Geriatrics FSU College of Medicine 1 Principles of Ethics Autonomy/Respect for Persons Beneficence Non- maleficence Justice
Advance Care Planning Ken Brummel-Smith, MD Charlotte Edwards Maguire Professor of Geriatrics FSU College of Medicine 1 Principles of Ethics Autonomy/Respect for Persons Beneficence Non- maleficence Justice
End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces.
 End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces. Terms Definitions End of Life Care To assist persons who
End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces. Terms Definitions End of Life Care To assist persons who
Advance Care Planning (and more)
") Advance Care Planning (and more) Tessa & Josie Karl Steinberg, MD, CMD,HMDC @karlsteinberg, karlsteinberg@mail.com WWW.COALITIONCCC.ORG Advance Care Planning ACP is a process that unfolds over a life span
Advance Care Planning (and more) Tessa & Josie Karl Steinberg, MD, CMD,HMDC @karlsteinberg, karlsteinberg@mail.com WWW.COALITIONCCC.ORG Advance Care Planning ACP is a process that unfolds over a life span
Palliative and End-of-Life Care
 Position Statement Palliative and End-of-Life Care A Position Statement Month Year PALLIATIVE AND END-OF-LIFE CARE MONTH YEAR i Approved by the College and Association of Registered Nurses of Alberta ()
Position Statement Palliative and End-of-Life Care A Position Statement Month Year PALLIATIVE AND END-OF-LIFE CARE MONTH YEAR i Approved by the College and Association of Registered Nurses of Alberta ()
Advance Directives The Missing Conversation Why Our Patients Children Are Left Holding The Bag. End of Life Planning Barriers 10/7/2014
 Advance Directives The Missing Conversation Why Our Patients Children Are Left Holding The Bag SC Chapter American College of Physicians October 29, 2014 Sewell I. Kahn, MD FACP End of Life Planning Barriers
Advance Directives The Missing Conversation Why Our Patients Children Are Left Holding The Bag SC Chapter American College of Physicians October 29, 2014 Sewell I. Kahn, MD FACP End of Life Planning Barriers
HealthStream Regulatory Script
 HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
Palliative Care. Care for Adults With a Progressive, Life-Limiting Illness
 Palliative Care Care for Adults With a Progressive, Life-Limiting Illness Summary This quality standard addresses palliative care for people who are living with a serious, life-limiting illness, and for
Palliative Care Care for Adults With a Progressive, Life-Limiting Illness Summary This quality standard addresses palliative care for people who are living with a serious, life-limiting illness, and for
POLST Discussions Doing it Better. Clinical Update in Geriatric Medicine. Judith S. Black, MD, MHA. POLST Overview. Faculty Disclosure PART I
 Faculty Disclosure POLST Discussions Doing it Better Clinical Update in Geriatric Medicine Dr. Black discloses that she is employed by Allegheny Health Network and is an executive committee member of the
Faculty Disclosure POLST Discussions Doing it Better Clinical Update in Geriatric Medicine Dr. Black discloses that she is employed by Allegheny Health Network and is an executive committee member of the
Communication with Surrogate Decision Makers. Shannon S. Carson, MD Associate Professor University of North Carolina
 Communication with Surrogate Decision Makers Shannon S. Carson, MD Associate Professor University of North Carolina Role of Communication with Families in the ICU Sharing information about illness and
Communication with Surrogate Decision Makers Shannon S. Carson, MD Associate Professor University of North Carolina Role of Communication with Families in the ICU Sharing information about illness and
Hospice Palliative Care
 Position Statement Hospice Palliative Care A Position Statement September 2011 HOSPICE PALLIATIVE CARE: A SEPTEMBER 2011 i Approved by the College and Association of Registered Nurses of Alberta () Provincial
Position Statement Hospice Palliative Care A Position Statement September 2011 HOSPICE PALLIATIVE CARE: A SEPTEMBER 2011 i Approved by the College and Association of Registered Nurses of Alberta () Provincial
DIRECTIVE TO PHYSICIANS AND FAMILY OR SURROGATES Advance Directives Act (see , Health and Safety Code) DIRECTIVE
 DIRECTIVE") DIRECTIVE TO PHYSICIANS AND FAMILY OR SURROGATES Advance Directives Act (see 166.033, Health and Safety Code) Instructions for completing this document: This is an important legal document known as an
DIRECTIVE TO PHYSICIANS AND FAMILY OR SURROGATES Advance Directives Act (see 166.033, Health and Safety Code) Instructions for completing this document: This is an important legal document known as an
ABOUT THE ADVANCE DIRECTIVE FOR RECEIVING ORAL FOOD AND FLUIDS IN DEMENTIA. Introduction
 ABOUT THE ADVANCE DIRECTIVE FOR RECEIVING ORAL FOOD AND FLUIDS IN DEMENTIA Introduction There are two purposes to completing an Advance Directive for Receiving Oral Food and Fluids In Dementia. The first
ABOUT THE ADVANCE DIRECTIVE FOR RECEIVING ORAL FOOD AND FLUIDS IN DEMENTIA Introduction There are two purposes to completing an Advance Directive for Receiving Oral Food and Fluids In Dementia. The first
ADVANCE CARE PLANNING GOALS OF CARE CONVERSATIONS MATTER A GUIDE FOR MAKING HEALTHCARE DECISIONS
 ADVANCE CARE PLANNING GOALS OF CARE CONVERSATIONS MATTER A GUIDE FOR MAKING HEALTHCARE DECISIONS What is Advance Care Planning? Advance Care Planning is a way to help you think about, talk about and document
ADVANCE CARE PLANNING GOALS OF CARE CONVERSATIONS MATTER A GUIDE FOR MAKING HEALTHCARE DECISIONS What is Advance Care Planning? Advance Care Planning is a way to help you think about, talk about and document
Advance Care Planning in Canada: Synthesis of Tools. March 22, 2010
 Advance Care Planning in Canada: Synthesis of Tools March 22, 2010 Acknowledgements: This document was prepared to support Advance Care Planning in Canada: National Framework Meeting 2010. The meeting
Advance Care Planning in Canada: Synthesis of Tools March 22, 2010 Acknowledgements: This document was prepared to support Advance Care Planning in Canada: National Framework Meeting 2010. The meeting
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Wow ADVANCE CARE PLANNING The continued Frontier. Kathryn Borgenicht, M.D. Linda Bierbach, CNP
 Wow ADVANCE CARE PLANNING The continued Frontier Kathryn Borgenicht, M.D. Linda Bierbach, CNP Objectives what we want to accomplish Describe the history of advance care planning Discuss what patients/families
Wow ADVANCE CARE PLANNING The continued Frontier Kathryn Borgenicht, M.D. Linda Bierbach, CNP Objectives what we want to accomplish Describe the history of advance care planning Discuss what patients/families
Objectives. Integrating Palliative Care Principles into Critical Care Nursing
 1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
Advance Care Planning Communication Guide: Overview
 Advance Care Planning Communication Guide: Overview The INTERACT Advance Care Planning Communication Guide is designed to assist health professionals who work in Nursing Facilities to initiate and carry
Advance Care Planning Communication Guide: Overview The INTERACT Advance Care Planning Communication Guide is designed to assist health professionals who work in Nursing Facilities to initiate and carry
Your Guide to Advance Directives
 Starting Points: Your Guide to Advance Directives Values Statements Healthcare Directives Durable Power of Attorney for Healthcare 1 2 Advances in medicine are helping people to live longer than ever before.
Starting Points: Your Guide to Advance Directives Values Statements Healthcare Directives Durable Power of Attorney for Healthcare 1 2 Advances in medicine are helping people to live longer than ever before.
Thank you for your interest in completing an Advance Directive.
 Advance Directives Thank you for your interest in completing an Advance Directive. Writing an Advance Directive is an opportunity to direct your future health needs in advance of an illness or crisis.
Advance Directives Thank you for your interest in completing an Advance Directive. Writing an Advance Directive is an opportunity to direct your future health needs in advance of an illness or crisis.
Advance Care Planning Conversations and Goals of Care Discussions: Understanding the Difference
 March 16, 2017 Advance Care Planning Conversations and Goals of Care Discussions: Understanding the Difference Jeff Myers MD, MSEd, CCFP(PC) Nadia Incardona MD, MHSc, CCFP(EM) WHY this is timely JAMA,
March 16, 2017 Advance Care Planning Conversations and Goals of Care Discussions: Understanding the Difference Jeff Myers MD, MSEd, CCFP(PC) Nadia Incardona MD, MHSc, CCFP(EM) WHY this is timely JAMA,
Advance Care Planning and Goals of Care
 Advance Care Planning and Goals of Care A Guide For Patients with A Serious Illness and Their Families Nova Scotia Edition www.nshpca.ca Receiving a diagnosis of a serious illness can be life altering.
Advance Care Planning and Goals of Care A Guide For Patients with A Serious Illness and Their Families Nova Scotia Edition www.nshpca.ca Receiving a diagnosis of a serious illness can be life altering.
Better Ending. A Guide. for a A SSURE Y OUR F INAL W ISHES. Conversations Before the Crisis
 A Guide for a Better Ending A SSURE Y OUR F INAL W ISHES Conversations Before the Crisis Information on Advance Care Planning and Documentation from Better Ending, a Program of the Central Massachusetts
A Guide for a Better Ending A SSURE Y OUR F INAL W ISHES Conversations Before the Crisis Information on Advance Care Planning and Documentation from Better Ending, a Program of the Central Massachusetts
vv POLST for Hospice Providers
 vv. 2.2.17 POLST for Hospice Providers Permission to Use This slide presentation may be used without permission. To promote consistency across the state, the slides may not be altered. You may freely take
vv. 2.2.17 POLST for Hospice Providers Permission to Use This slide presentation may be used without permission. To promote consistency across the state, the slides may not be altered. You may freely take
Conducting Family Conferences at End of Life
 COVENANT HEALTH ETHICS CONFERENCE 2013 Conducting Family Conferences at End of Life Meg Hagerty Social Worker, Mel Miller Hospice, Edmonton General Ingrid de Kock Palliative Care Physician, Palliative
COVENANT HEALTH ETHICS CONFERENCE 2013 Conducting Family Conferences at End of Life Meg Hagerty Social Worker, Mel Miller Hospice, Edmonton General Ingrid de Kock Palliative Care Physician, Palliative
Directive To Physicians and Family Or Surrogates (Living Will)
") Directive To Physicians and Family Or Surrogates (Living Will) INSTRUCTIONS FOR COMPLETING THIS DOCUMENT: This is an important legal document known as an Advance Directive. It is designed to help you communicate
Directive To Physicians and Family Or Surrogates (Living Will) INSTRUCTIONS FOR COMPLETING THIS DOCUMENT: This is an important legal document known as an Advance Directive. It is designed to help you communicate
Did You Know? The Strategic and Compassionate Employer: How Compassionate Care Leave Policies can Improve Employee Retention and Engagement
 The Strategic and Compassionate Employer: How Compassionate Care Leave Policies can Improve Employee Retention and Engagement PRESENTATION TO THE HRPA 2015 CONFERENCE SHARON BAXTER, EXECUTIVE DIRECTOR,
The Strategic and Compassionate Employer: How Compassionate Care Leave Policies can Improve Employee Retention and Engagement PRESENTATION TO THE HRPA 2015 CONFERENCE SHARON BAXTER, EXECUTIVE DIRECTOR,
TSE Chun Yan Chairman, HA Clinical Ethics Committee
 TSE Chun Yan Chairman, HA Clinical Ethics Committee Framework of my talk Brief description on the development of AD in Hong Kong. Three issues for discussion: Whether HK should enact specific legislation
TSE Chun Yan Chairman, HA Clinical Ethics Committee Framework of my talk Brief description on the development of AD in Hong Kong. Three issues for discussion: Whether HK should enact specific legislation
RESOURCES FREQUENTLY ASKED CLINICAL QUESTIONS FOR PROVIDERS
 RESOURCES FREQUENTLY ASKED CLINICAL QUESTIONS FOR PROVIDERS Section 1: General Questions Why is it important that I help patients complete a POLST form? Does the POLST form replace traditional Advance
RESOURCES FREQUENTLY ASKED CLINICAL QUESTIONS FOR PROVIDERS Section 1: General Questions Why is it important that I help patients complete a POLST form? Does the POLST form replace traditional Advance
Sample MOLST Policy for Home Health Care or Hospice
 TOOL 2-7A Sample MOLST Policy for Home Health Care or Hospice SAMPLE/DRAFT MOLST POLICY and PROCEDURE Home Health Care or Hospice Agencies CAUTION: This sample policy should not be accepted as MOLST policy
TOOL 2-7A Sample MOLST Policy for Home Health Care or Hospice SAMPLE/DRAFT MOLST POLICY and PROCEDURE Home Health Care or Hospice Agencies CAUTION: This sample policy should not be accepted as MOLST policy
Improving Use of Advance Directives
 Improving Use of Advance Directives Douglas B. White, MD, MAS Associate Professor of Critical Care Medicine and Medicine Director, Program on Ethics and Decision Making in Critical Illness The CRISMA Center
Improving Use of Advance Directives Douglas B. White, MD, MAS Associate Professor of Critical Care Medicine and Medicine Director, Program on Ethics and Decision Making in Critical Illness The CRISMA Center
Clinical In-Service Goals of Care. Josh Stachniak
 Clinical In-Service Goals of Care Josh Stachniak Agenda 1. Purpose of Today s Presentation 2. Overview of Goals of Care 3. Consent and Goals of Care 4. Dispute Resolution and Goals of Care 5. Advanced
Clinical In-Service Goals of Care Josh Stachniak Agenda 1. Purpose of Today s Presentation 2. Overview of Goals of Care 3. Consent and Goals of Care 4. Dispute Resolution and Goals of Care 5. Advanced
GP SERVICES COMMITTEE Palliative Care INCENTIVES. Revised January 2018
 GP SERVICES COMMITTEE Palliative Care INCENTIVES Revised January 2018 GPSC Palliative Care Planning and Management Fees The following incentive payments are available to B.C. s eligible family physicians.
GP SERVICES COMMITTEE Palliative Care INCENTIVES Revised January 2018 GPSC Palliative Care Planning and Management Fees The following incentive payments are available to B.C. s eligible family physicians.
HPNA Position Statement The Nurse s Role in Advance Care Planning
 HPNA Position Statement The Nurse s Role in Advance Care Planning Background Advances in medical technology have empowered healthcare providers across settings with the means to prolong life. Tied to this
HPNA Position Statement The Nurse s Role in Advance Care Planning Background Advances in medical technology have empowered healthcare providers across settings with the means to prolong life. Tied to this
Building a Person-Centered ADVANCE CARE Planning Program. Barbara J. Smith, LBSW, MS, CHC, NHA Carolyn Stramecki, MHSA, CPHQ
 Building a Person-Centered ADVANCE CARE Planning Program Barbara J. Smith, LBSW, MS, CHC, NHA Carolyn Stramecki, MHSA, CPHQ Objectives Describe components of an advance directive document required to meet
Building a Person-Centered ADVANCE CARE Planning Program Barbara J. Smith, LBSW, MS, CHC, NHA Carolyn Stramecki, MHSA, CPHQ Objectives Describe components of an advance directive document required to meet
Discussing Goals of Care
 Discussing Goals of Care Sarah Beth Harrington, MD UAMS Assistant Professor of Medicine Central Arkansas Veterans Healthcare System Chief of Palliative Care Objectives Understand the importance of discussing
Discussing Goals of Care Sarah Beth Harrington, MD UAMS Assistant Professor of Medicine Central Arkansas Veterans Healthcare System Chief of Palliative Care Objectives Understand the importance of discussing
Advance Care Planning Exploratory Project. Rhonda Wiering, MSN, RN,BC, LNHA Regional Director, Quality Initiatives Avera Health October 18, 2012
 Advance Care Planning Exploratory Project Rhonda Wiering, MSN, RN,BC, LNHA Regional Director, Quality Initiatives Avera Health October 18, 2012 Agenda Overview of the Advance Care Planning Exploration
Advance Care Planning Exploratory Project Rhonda Wiering, MSN, RN,BC, LNHA Regional Director, Quality Initiatives Avera Health October 18, 2012 Agenda Overview of the Advance Care Planning Exploration
Advance Care Planning
 Advance Care Planning Joan M. Teno, MD, MS Professor of Community Health Warrant Alpert School of Medicine at Brown University VJ Periyakoil, MD Course Director & Producer At the end of this session You
Advance Care Planning Joan M. Teno, MD, MS Professor of Community Health Warrant Alpert School of Medicine at Brown University VJ Periyakoil, MD Course Director & Producer At the end of this session You
YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE
 YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE Communicating Your Health Care Choices In 1990, Congress passed the Patient Self-Determination Introduction Act. It requires
YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE Communicating Your Health Care Choices In 1990, Congress passed the Patient Self-Determination Introduction Act. It requires
Advance Care Planning in Ontario A Quality Improvement Toolkit
 Advance Care Planning in Ontario A Quality Improvement Toolkit Introduction What is the Advance Care Planning (ACP) Quality Improvement Toolkit? In January 2013, the Ministry of Health and Long Term Care
Advance Care Planning in Ontario A Quality Improvement Toolkit Introduction What is the Advance Care Planning (ACP) Quality Improvement Toolkit? In January 2013, the Ministry of Health and Long Term Care
MAKING YOUR WISHES KNOWN: Advance Care Planning Guide
 MAKING YOUR WISHES KNOWN: Advance Care Planning Guide ADVANCE CARE PLANNING The process of learning about the type of medical decisions that may need to be made, considering those decisions ahead of time
MAKING YOUR WISHES KNOWN: Advance Care Planning Guide ADVANCE CARE PLANNING The process of learning about the type of medical decisions that may need to be made, considering those decisions ahead of time
Deciding About. Health Care A GUIDE FOR PATIENTS AND FAMILIES. New York State Department of Health
 Deciding About Health Care A GUIDE FOR PATIENTS AND FAMILIES New York State Department of Health 2 Introduction Who should read this guide? This guide is for New York State patients and for those who will
Deciding About Health Care A GUIDE FOR PATIENTS AND FAMILIES New York State Department of Health 2 Introduction Who should read this guide? This guide is for New York State patients and for those who will
ALLINA HOME & COMMUNITY SERVICES ALLINA HEALTH. Advance Care Planning. Discussion guide. Discussion Guide. Advance care planning
 ALLINA HOME & COMMUNITY SERVICES ALLINA HEALTH Advance Care Planning Discussion guide Discussion Guide Advance care planning Advance care planning Any of us could think of a time when we might be too sick
ALLINA HOME & COMMUNITY SERVICES ALLINA HEALTH Advance Care Planning Discussion guide Discussion Guide Advance care planning Advance care planning Any of us could think of a time when we might be too sick
Designing an Advance Care Planning System that Shapes Hospital Utilization
 Designing an Advance Care Planning System that Shapes Hospital Utilization This slide presentation is a copyright of Gundersen Lutheran Medical Foundation, Inc., 2014 2016. All Rights Reserved v4.16 1
Designing an Advance Care Planning System that Shapes Hospital Utilization This slide presentation is a copyright of Gundersen Lutheran Medical Foundation, Inc., 2014 2016. All Rights Reserved v4.16 1
PSYCHOSOCIAL ASPECTS OF PALLIATIVE CARE IN MENTAL HEALTH SETTINGS. Dawn Chaitram BSW, RSW, MA Psychosocial Specialist
 PSYCHOSOCIAL ASPECTS OF PALLIATIVE CARE IN MENTAL HEALTH SETTINGS Dawn Chaitram BSW, RSW, MA Psychosocial Specialist WRHA Palliative Care Program April 19, 2017 OUTLINE Vulnerability and Compassion Addressing
PSYCHOSOCIAL ASPECTS OF PALLIATIVE CARE IN MENTAL HEALTH SETTINGS Dawn Chaitram BSW, RSW, MA Psychosocial Specialist WRHA Palliative Care Program April 19, 2017 OUTLINE Vulnerability and Compassion Addressing
End-of-Life Care Action Plan
 The Provincial End-of-Life Care Action Plan for British Columbia Priorities and Actions for Health System and Service Redesign Ministry of Health March 2013 ii The Provincial End-of-Life Care Action Plan
The Provincial End-of-Life Care Action Plan for British Columbia Priorities and Actions for Health System and Service Redesign Ministry of Health March 2013 ii The Provincial End-of-Life Care Action Plan
ADVANCE DIRECTIVE INFORMATION
 ADVANCE DIRECTIVE INFORMATION NOTE: This Advance Directive Information and the form Living Will and Durable Power of Attorney for Health Care on the Arkansas Bar Association s website are being provided
ADVANCE DIRECTIVE INFORMATION NOTE: This Advance Directive Information and the form Living Will and Durable Power of Attorney for Health Care on the Arkansas Bar Association s website are being provided
Improving End of Life Care in Long Term Care Facilities: Perspectives of Healthcare Providers
 Improving End of Life Care in Long Term Care Facilities: Perspectives of Healthcare Providers Christine Beck, MD CCFP MSc Department of Family Medicine Dalhousie University January 15, 2010 NELS Work In
Improving End of Life Care in Long Term Care Facilities: Perspectives of Healthcare Providers Christine Beck, MD CCFP MSc Department of Family Medicine Dalhousie University January 15, 2010 NELS Work In
Health Care Consent & Advance Care Planning in Ontario. What You Need to Know. Health Care Consent Advance Care Planning Community of Practice
 Health Care Consent & Advance Care Planning in Ontario What You Need to Know Health Care Consent Advance Care Planning Community of Practice Welcome Introductions Webinar Instructions If you have a mute
Health Care Consent & Advance Care Planning in Ontario What You Need to Know Health Care Consent Advance Care Planning Community of Practice Welcome Introductions Webinar Instructions If you have a mute
What is POLST Physician Orders For Life
 POLST in ND Physician Orders for Life Sustaining Treatment 2017 Dakota Conference Nancy Joyner, MS, APRN-CNS, ACHPN Palliative Care Clinical Nurse Specialist HCND s POLST Coordinator Objectives 1. Define
POLST in ND Physician Orders for Life Sustaining Treatment 2017 Dakota Conference Nancy Joyner, MS, APRN-CNS, ACHPN Palliative Care Clinical Nurse Specialist HCND s POLST Coordinator Objectives 1. Define
The POLST Conversation POLST Script
 The POLST Conversation POLST Script The POLST Script provides detailed information in order to develop comfort and competence when facilitating a POLST conversation. The POLST conversation utilizes realistic
The POLST Conversation POLST Script The POLST Script provides detailed information in order to develop comfort and competence when facilitating a POLST conversation. The POLST conversation utilizes realistic
Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee
 Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee What is Advance Care Planning (ACP)? Understanding/clarifying
Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee What is Advance Care Planning (ACP)? Understanding/clarifying
Supporting family caregivers of seniors: improving care and caregiver outcomes in End-of-life care.
 Supporting family caregivers of seniors: improving care and caregiver outcomes in End-of-life care. Dr. Jasneet Parmar, Dr. Suzette Bremault-Phillips, Ms. Melissa Johnson Covenant Health s 25 th Annual
Supporting family caregivers of seniors: improving care and caregiver outcomes in End-of-life care. Dr. Jasneet Parmar, Dr. Suzette Bremault-Phillips, Ms. Melissa Johnson Covenant Health s 25 th Annual
Revised 2/27/17. POLST For General Providers
 Revised 2/27/17 POLST For General Providers Permission to Use This slide presentation may be used without permission. To promote consistency across the state, the slides may not be altered. You may freely
Revised 2/27/17 POLST For General Providers Permission to Use This slide presentation may be used without permission. To promote consistency across the state, the slides may not be altered. You may freely
Improving End-of-life Care: A Community Approach Patricia Bomba, MD, MACP VP & Medical Director, Geriatrics, Excellus BlueCross Blue Shield
 Session Code D20 & E20 This presenter has nothing to disclose Improving End-of-life Care: A Community Approach Patricia Bomba, MD, MACP VP & Medical Director, Geriatrics, Excellus BlueCross Blue Shield
Session Code D20 & E20 This presenter has nothing to disclose Improving End-of-life Care: A Community Approach Patricia Bomba, MD, MACP VP & Medical Director, Geriatrics, Excellus BlueCross Blue Shield
Digital Transformation of MOLST: Getting Started and Ensuring Sustainability
 Digital Transformation of MOLST: Getting Started and Ensuring Sustainability Speakers Patricia Bomba, MD, MACP Vice President and Medical Director, Geriatrics, Excellus BlueCross BlueShield Chair, MOLST
Digital Transformation of MOLST: Getting Started and Ensuring Sustainability Speakers Patricia Bomba, MD, MACP Vice President and Medical Director, Geriatrics, Excellus BlueCross BlueShield Chair, MOLST
What would you like to accomplish in the process of advance care planning and/or in completing a health care directive?
 Completing a health care directive is an important step in making sure your loved ones and health care providers understand your values and choices for health care treatment if you are not able to speak
Completing a health care directive is an important step in making sure your loved ones and health care providers understand your values and choices for health care treatment if you are not able to speak
Advance Care Planning Workbook Ontario Edition
 Advance Care Planning Workbook Ontario Edition Speak Up Ontario c/o Hospice Palliative Care Ontario, 2 Carlton Street, Suite 808, Toronto, Ontario M5B 1J3 Who will speak for you? Start the conversation.
Advance Care Planning Workbook Ontario Edition Speak Up Ontario c/o Hospice Palliative Care Ontario, 2 Carlton Street, Suite 808, Toronto, Ontario M5B 1J3 Who will speak for you? Start the conversation.
Psychological issues in nutrition and hydration towards End of Life
 Psychological issues in nutrition and hydration towards End of Life Dr Sylvia Puchalska, Clinical Psychologist Raisin exercise Why do people eat and drink? What does it MEAN to them? What are some of the
Psychological issues in nutrition and hydration towards End of Life Dr Sylvia Puchalska, Clinical Psychologist Raisin exercise Why do people eat and drink? What does it MEAN to them? What are some of the
Goals of Care. Cancer Education Day. January 13, Wally Liang MD, CCFP(COE), JD, MHSc
, JD, MHSc") Goals of Care Cancer Education Day January 13, 2017 Wally Liang MD, CCFP(COE), JD, MHSc none Conflict of Interest Goals of Advance Directives Promote patient autonomy Prevent interventions that are not
Goals of Care Cancer Education Day January 13, 2017 Wally Liang MD, CCFP(COE), JD, MHSc none Conflict of Interest Goals of Advance Directives Promote patient autonomy Prevent interventions that are not
DNACPR. Maire O Riordan 14 th January 2015
 DNACPR Maire O Riordan 14 th January 2015 Objectives NHS Scotland DNACPR policy Decision making framework and the forms DNACPR within ACP context Communicationwith patients, relatives and colleagues Background
DNACPR Maire O Riordan 14 th January 2015 Objectives NHS Scotland DNACPR policy Decision making framework and the forms DNACPR within ACP context Communicationwith patients, relatives and colleagues Background
TOOL 2-6 Sample MOLST Policy for Acute Care Hospitals 1
 TOOL 2-6 Sample MOLST Policy for Acute Care Hospitals 1 Caution It is not advisable to use MOLST policy written for other institutions, especially policies from out of state. Each institution needs to
TOOL 2-6 Sample MOLST Policy for Acute Care Hospitals 1 Caution It is not advisable to use MOLST policy written for other institutions, especially policies from out of state. Each institution needs to
Social workers involvement in advance care planning: a systematic narrative review
 Wang et al. BMC Palliative Care (2018) 17:5 DOI 10.1186/s12904-017-0218-8 RESEARCH ARTICLE Open Access Social workers involvement in advance care planning: a systematic narrative review Chong-Wen Wang
Wang et al. BMC Palliative Care (2018) 17:5 DOI 10.1186/s12904-017-0218-8 RESEARCH ARTICLE Open Access Social workers involvement in advance care planning: a systematic narrative review Chong-Wen Wang
Honoring Patient Wishes
 Honoring Patient Wishes Nurses communication skills key to helping patients achieve end-of-life goals by Anna Mariani Reseigh Hearing the voice of the customer (VOC) is a goal for many industries. For
Honoring Patient Wishes Nurses communication skills key to helping patients achieve end-of-life goals by Anna Mariani Reseigh Hearing the voice of the customer (VOC) is a goal for many industries. For
Health Care Directive
 MINNESOTA PATIENT EDUCATION Health Care Directive Making Your Health Care Choices Known My Health Care Directive My health care directive was created to guide my health care agent and family, friends or
MINNESOTA PATIENT EDUCATION Health Care Directive Making Your Health Care Choices Known My Health Care Directive My health care directive was created to guide my health care agent and family, friends or
Advance Directive for Health Care
 Advance Directive for Health Care respecting your right to: Choose Your Healthcare Agent Choose the Authority Given to Your Healthcare Agent Choose Your Preferences Related to Treatment & Care Printed
Advance Directive for Health Care respecting your right to: Choose Your Healthcare Agent Choose the Authority Given to Your Healthcare Agent Choose Your Preferences Related to Treatment & Care Printed
Directive to Physicians and Family or Surrogates
 Directive to Physicians and Family or Surrogates This is an important legal document, known as an Advance Directive. It is designed to help you communicate your wishes about medical treatment at some time
Directive to Physicians and Family or Surrogates This is an important legal document, known as an Advance Directive. It is designed to help you communicate your wishes about medical treatment at some time
POLST Cue Card. If you die a natural death, would you want us to try CPR? If yes Requires Full Treatment in Section B. (Ask about Ventilator Trial)
") POLST Cue Card It s important to talk about your health and your wishes for medical care if you got really sick. We talk about this with everyone with serious illness. Your doctor will review what we talk
POLST Cue Card It s important to talk about your health and your wishes for medical care if you got really sick. We talk about this with everyone with serious illness. Your doctor will review what we talk
What is POLST? Physician Orders for Life Sustaining Treatment
 What is POLST? Physician Orders for Life Sustaining Treatment Why POLST? 1. Patient wishes often are not known. The Advance Healthcare Directive (AHCD) may not be accessible. Wishes may not be clearly
What is POLST? Physician Orders for Life Sustaining Treatment Why POLST? 1. Patient wishes often are not known. The Advance Healthcare Directive (AHCD) may not be accessible. Wishes may not be clearly
QUALITY MEASURES WHAT S ON THE HORIZON
 QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
ILLINOIS Advance Directive Planning for Important Health Care Decisions
 ILLINOIS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
ILLINOIS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
Perceptions of Family Cancer Caregivers in Tanzania: A Qualitative Study. Allison Walker
 Perceptions of Family Cancer Caregivers in Tanzania: A Qualitative Study Allison Walker Motivation Upward trend in cancer cases in developing countries Lack of institutional facilities and specialists
Perceptions of Family Cancer Caregivers in Tanzania: A Qualitative Study Allison Walker Motivation Upward trend in cancer cases in developing countries Lack of institutional facilities and specialists
What is palliative care?
 What is palliative care? Hamilton Health Sciences and surrounding communities Palliative care is a way of providing health care that focuses on improving the quality of life for you and your family when
What is palliative care? Hamilton Health Sciences and surrounding communities Palliative care is a way of providing health care that focuses on improving the quality of life for you and your family when
Central Zone Healthcare Plan. For Placement Only. Strategy Overview
 Alberta Health Services Central Zone Healthcare Plan For Placement Only Strategy Overview A plan for us Alberta Health Services (AHS) recognizes every community in Alberta is unique. That s why health
Alberta Health Services Central Zone Healthcare Plan For Placement Only Strategy Overview A plan for us Alberta Health Services (AHS) recognizes every community in Alberta is unique. That s why health
Kay de Vries. Graduate School of Nursing, Midwifery and Health Victoria University Wellington
 Kay de Vries Graduate School of Nursing, Midwifery and Health Victoria University Wellington History/definitions USA/UK/NZ. Capacity & surrogates Barriers to completing ACP Complexity of ACP settings,
Kay de Vries Graduate School of Nursing, Midwifery and Health Victoria University Wellington History/definitions USA/UK/NZ. Capacity & surrogates Barriers to completing ACP Complexity of ACP settings,
PAHT strategy for End of Life Care for adults
 PAHT strategy for End of Life Care for adults 2017-2020 End of Life Care encompasses all care given to patients who are approaching the end of their life and following death, and may be delivered on any
PAHT strategy for End of Life Care for adults 2017-2020 End of Life Care encompasses all care given to patients who are approaching the end of their life and following death, and may be delivered on any
Dementia and End-of-Life Care
 Dementia and End-of-Life Care Part IV: What practical information should I know? About this resource The needs of people with dementia at the end of life* are unique and require special considerations.
Dementia and End-of-Life Care Part IV: What practical information should I know? About this resource The needs of people with dementia at the end of life* are unique and require special considerations.
Environmental Scan for Strengthening End-of-Life Care Across the Continuum. Evidence and Practice
 Environmental Scan for Strengthening End-of-Life Care Across the Continuum Evidence and Practice Report of the Residential Hospice Working Group January 2015 Table of Contents PART I: POLICY ENVIRONMENT...
Environmental Scan for Strengthening End-of-Life Care Across the Continuum Evidence and Practice Report of the Residential Hospice Working Group January 2015 Table of Contents PART I: POLICY ENVIRONMENT...
S A M P L E. About CPR. Hard Choices. Logo A GUIDE FOR PATIENTS AND FAMILIES
 Hard Choices About CPR A GUIDE FOR PATIENTS AND FAMILIES Logo 2016 by Quality of Life Publishing Co. Hard Choices About CPR: A Guide for Patients and Families adapted with permission from: Dunn, Hank.
Hard Choices About CPR A GUIDE FOR PATIENTS AND FAMILIES Logo 2016 by Quality of Life Publishing Co. Hard Choices About CPR: A Guide for Patients and Families adapted with permission from: Dunn, Hank.
HealthStream Regulatory Script
 HealthStream Regulatory Script Advance Directives Release Date: August 2008 HLC Version: 602 Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney
HealthStream Regulatory Script Advance Directives Release Date: August 2008 HLC Version: 602 Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney
Talking to Your Doctor About Hospice Care
 Talking to Your Doctor About Hospice Care Death and dying subjects that were once taboo in our culture are becoming increasingly relevant as more Americans care for their aging parents and consider what
Talking to Your Doctor About Hospice Care Death and dying subjects that were once taboo in our culture are becoming increasingly relevant as more Americans care for their aging parents and consider what
The Impact of Resident Education on Advance Directive Documentation and Resident Knowledge of Advanced Care Planning
 The Impact of Resident Education on Advance Directive Documentation and Resident Knowledge of Advanced Care Planning A. Study Purpose and Rationale Ever since the Patient Self-Determination Act of 1990
The Impact of Resident Education on Advance Directive Documentation and Resident Knowledge of Advanced Care Planning A. Study Purpose and Rationale Ever since the Patient Self-Determination Act of 1990
Table S1 KEYWORDS USED TO SEARCH THE LITERATURE
 Table S1 KEYWORDS USED TO SEARCH THE LITERATURE COPD, CHRONIC OBSTRUCTIVE PULMONARY DIS*", CHRONIC OBSTRUCTIVE AIRWAY DIS*, CHRONIC LUNG DIS*, CHRONIC LUNG ILLNESS, CHRONIC PULMONARY ILLNESS, CHRONIC PULMONARY
Table S1 KEYWORDS USED TO SEARCH THE LITERATURE COPD, CHRONIC OBSTRUCTIVE PULMONARY DIS*", CHRONIC OBSTRUCTIVE AIRWAY DIS*, CHRONIC LUNG DIS*, CHRONIC LUNG ILLNESS, CHRONIC PULMONARY ILLNESS, CHRONIC PULMONARY
Common Questions Asked by Patients Seeking Hospice Care
 Common Questions Asked by Patients Seeking Hospice Care C o m i n g t o t e r m s w i t h the fact that a loved one may need hospice care to manage his or her pain and get additional social and psychological
Common Questions Asked by Patients Seeking Hospice Care C o m i n g t o t e r m s w i t h the fact that a loved one may need hospice care to manage his or her pain and get additional social and psychological
Improving Transitions from Child to Adult Care
 Improving Transitions from Child to Adult Care October 19, 2016 @cfhi_fcass Please introduce yourself and your organization name 4 Let s Tweet Together: Join the conversation on Twitter! @CFHI_FCASS @CAPHC
Improving Transitions from Child to Adult Care October 19, 2016 @cfhi_fcass Please introduce yourself and your organization name 4 Let s Tweet Together: Join the conversation on Twitter! @CFHI_FCASS @CAPHC
Advance Care Planning in Canada: National Framework. for Consultation November, 2010
 Advance Care Planning in Canada: National Framework for Consultation November, 2010 Advance Care Planning in Canada: National Framework ii This Advance Care Planning in Canada: National Framework and Implementation
Advance Care Planning in Canada: National Framework for Consultation November, 2010 Advance Care Planning in Canada: National Framework ii This Advance Care Planning in Canada: National Framework and Implementation