INFORMATION ABOUT HEALTH CARE DECISONS. Health Care Proxy MOLST DNR
|
|
|
- Ralf Hamilton
- 5 years ago
- Views:
Transcription

1 INFORMATION ABOUT HEALTH CARE DECISONS Health Care Proxy MOLST DNR February/2017 1
2 Introduction This informational booklet describing different options and procedures for making health care decisions was developed because of a request from a family who found it frustrating to navigate all of the requirements at a time when the family should be spending time with their family member faced with a terminal illness. The different options and many requirements and various forms can be confusing. Much of the information and forms in this booklet can be found in the OPWDD regulations under 14 NYCRR part 633, Section 1750-b of the Surrogate Court Procedure Act, (also called the Health Care Decision Act or HCDA, and guidance from the Department of Health, OPWDD, and other websites. The hope for the development of this booklet is that individuals, family members, legal guardians, doctors, Service Coordinators and staff can review this information and become more familiar with the many requirements for medical decisions under the OPWDD system, before a medical crisis occurs. Some of the required forms have also been included as attachments in this booklet and also can be found on the OPWDD website. The second hope for this booklet is that it will help individuals, families and staff to feel comfortable about beginning a discussion with an individual on what his/her medical wishes are in the event of a serious illness. Making health decisions during a serious illness or at the end of an individual s life can be a very difficult and emotional thing to do. Our hope in developing this booklet is that agencies, individuals, and families communicate and work together to ensure that all the requirements are met and that the individual s wishes are followed. During a medical crisis and when the decision has been made to say goodbye to the individual, the focus should be on families spending time with their loved one, not on trying to decipher laws and requirements. Many of the requirements discussed in this booklet are only applicable to individuals living in an OPWDD certified residential setting (IRA, ICF, Family Care). This booklet begins with an overview of the various healthcare decision options and then has a specific section for each option that provides more detail regarding requirements and procedures. This booklet also includes additional website resources and forms that may be required. Please note: The information summarized in this booklet is for informational purposes only and is not a substitute for legal advice. This booklet reflects the understanding of AccessCNY, which is current as of the date this booklet is published. This information should not be construed as official guidance from any state agency. This booklet is dedicated to Kelly, Richard, Janice, Patricia, Sage, and all of the others who have left us too soon. Your memories will live on in us forever. 2
3 Table of Contents 1. Summary of differences of options pp Health Care Proxy pp Medical decisions for individuals who lack capacity pp MOLST (Medical Orders for Life-Sustaining Treatment) pp Request to Withhold or Withdraw Life-sustaining treatment p Non-Hospital DNR p Additional Resources p Attachments: Health Care Proxy form and directions MOLST form OPWDD Checklist Non-Hospital DNR 3
4 Difference between Living Will, MOLST, Health Care Proxy, Non-hospital DNR A Living Will is a document that is a statement of the individual s medical wishes to be carried out if the individual should become unable to make his/her own decisions. There is no specific form that must be used in NYS for a living will. A Non-Hospital DNR (Do not resuscitate) is a legal document authorized by NYS that an individual can create to direct medical professionals to not perform CPR when the individual s heart stops beating. This document is used after the individual leaves the hospital. This document must be reviewed and signed by the individual s doctor every 90 days. With the creation of the MOLST form, a DNR can be included on the MOLST and a separate form is no longer needed. A Health Care Proxy is a legal document in NYS that allows the individual to appoint another person to make medical decisions for the individual when he/she loses the ability to make his/her own decisions about medical treatment. The individual must be able to understand what the purpose of this document is and name someone as his/her health care agent. The health care agent must follow the individual s wishes about his/her medical care. The Health Care Proxy can include the individual s directions about DNR and other medical treatments. If the Health Care Proxy does not include specific directions about tube and IV feedings for nutrition and fluids, the health care agent is not able to make these decisions for the person. There is a specific Health Care Proxy form that must be used in NYS. The Health Care Proxy only needs to be done once unless the individual wants to change it. The Health Care Proxy must be signed and witnessed and there are specific requirements regarding who can witness and who can be a health care agent for the individual. A MOLST is a legal document that must be signed by a NYS licensed doctor. The MOLST documents the individual s (or legal guardian or involved family member, if the individual has been determined to lack the ability to make medical decisions for him/herself) directions regarding medical treatment including life-sustaining treatments. and must be followed by all NYS doctors. For people receiving OPWDD services, the MOLST is completed by the individual s doctor when the individual has a serious medical condition or end of life. The doctor completes and signs the MOLST after the OPWDD checklist is completed. The OPWDD checklist must be reviewed and signed by a NYS licensed psychologist or another NYS licensed doctor approved by OPWDD. There are certain conditions that must be met under the 1750-b law and specific notifications that must be made when the MOLST is created. The OPWDD checklist ensures that all of the requirements are met. If an individual s condition worsens or will not improve, an individual, legal guardian, or family member can request that the lifesustaining treatment be withheld or withdrawn. To protect the individual, there are additional documentation and notification requirements that need to be made by the doctor to ensure no one objects to the request. If the individual leaves the hospital, the MOLST can still be in effect. 4
5 The individual s doctor must review and sign the MOLST on a regular basis to ensure there are no changes. Non-Hospital DNR, Health Care Proxy and Living Wills are used to document the individual s future wishes about his/her medical treatment. The MOLST is used for immediate decisions about the individual s medical treatment due to a current serious medical or serious chronic condition and applies as soon as the order is signed by the physician. Also, the MOLST includes specific and actionable medical orders that transition with the individual across health care settings. For example, health care proxies and living wills typically contain more general instructions and may not be followed by EMS providers in an emergency Health Care Proxy Person is capable adult HCP created and Health Care agent appointed Copy of HCP kept with individual Health care agent follows HCP after person has been determined that he/she has lost capacity to make decisions Individual Lacks Capacity and does not have a Health Care Proxy Legal Guardian or Surrogate (family member) requests MOLST Doctor completes MOLST after OPWDD checklist has been completed MOLST sent to MHLS and copy kept with individual MOLST reviewed by doctor on a regular basis to ensure no changes Guardian or Surrogate of Individual Without Capacity Request to Withhold or Withdraw Life-Sustaining Treatment (This could be at the same time MOLST is developed) Legal Guardian or Involved family member requests that Life-sustaining treatment be withheld or stopped Doctor completes section on OPWDD checklist and notifies MHLS and agency CEO within 48 hours or ASAP and documents notification If no objections, treatment is withheld or stopped If objection made request suspended until mediation or court decision Non-Hospital DNR Individual has Non-hospital DNR Non-Hospital DNR sent to MHLS and copy kept with individual 5 Document must be reviewed by doctor every 90 days
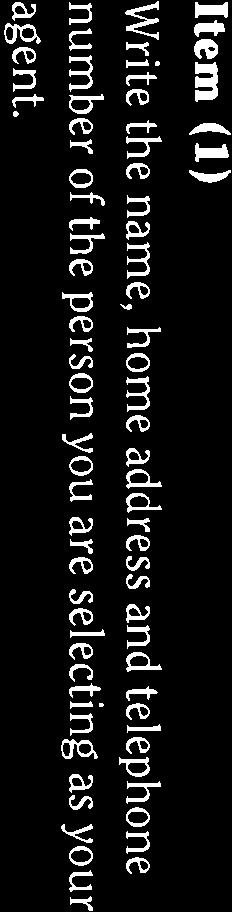
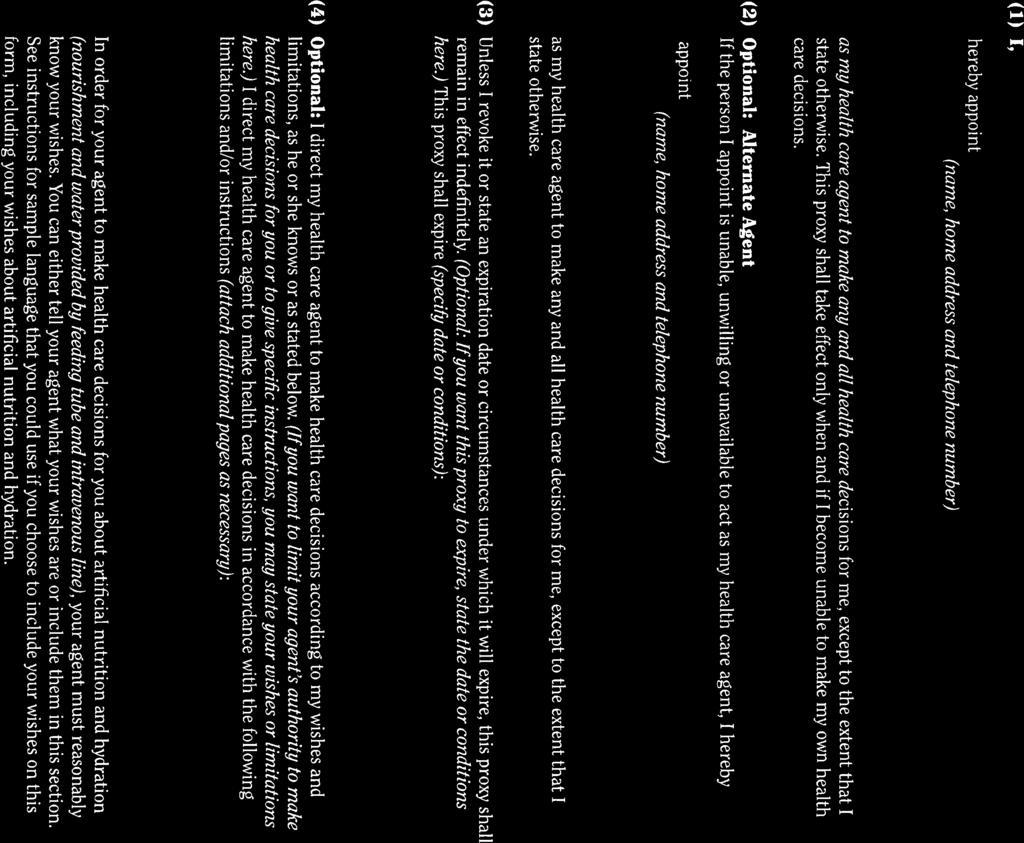
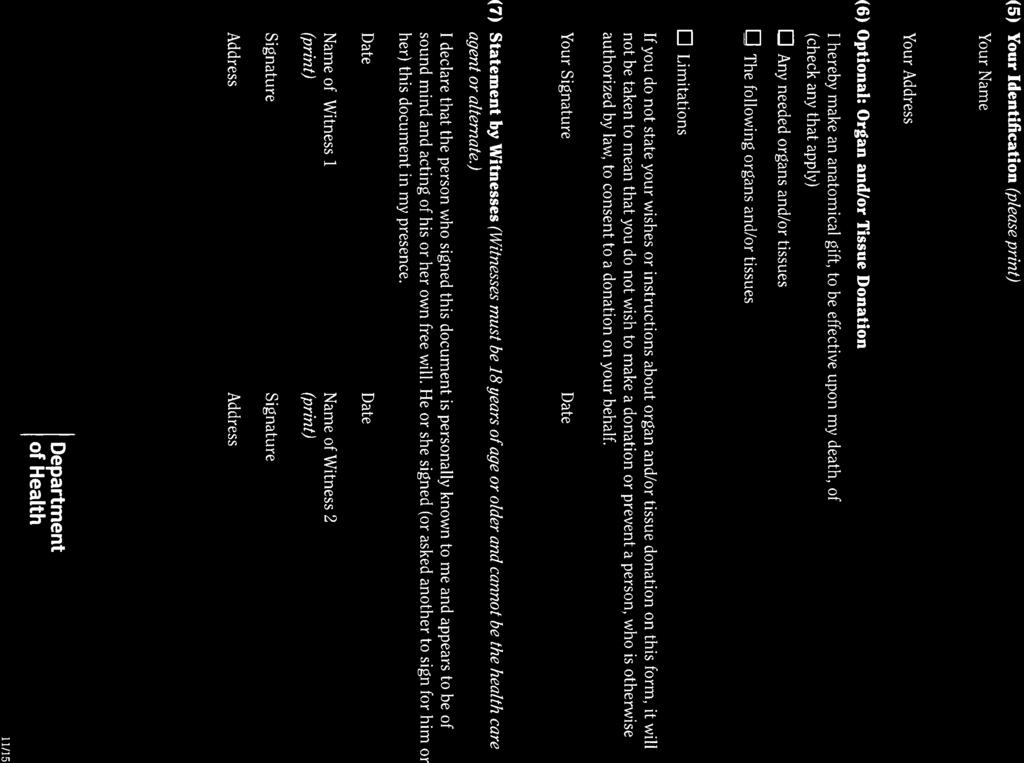
6 Health Care Proxy What is a Health Care Proxy? A health care proxy is a document that is created by an individual which gives another person the authority to make medical decisions for that individual when he/she becomes unable to make the decisions for him/herself. The person delegated (agent) must follow the individual s (principal) directions which are included in the health care proxy. A sample Health Care Proxy form is included in the attachment section of the booklet. Who can create a Health Care Proxy? Any person who is considered a competent adult may create a health care proxy and appoint a health care agent. According to , every adult (individual 18 or older) shall be presumed competent to appoint a health care agent unless the individual: (a) has a legal guardian appointed under article 17-A of the Surrogate s Court Procedure Act (b) has a committee appointed under article 78 of the Mental Hygiene Law (c) has a prior court determination that he or she is not capable of appointing a health care agent (d) is presumed competent but does not understand that he or she is delegating the authority to make decisions about their medical care to another person The determination of an individual s understanding and capacity to appoint a health care agent should be documented in the individual s record. The team (which may include the individual, family members, service coordinator and staff), doctor, or a psychologist can make this determination by asking the individual questions to determine his/her understanding of what a health care proxy is. If an individual has a legal guardian appointed under 17-A Surrogate Court, a health care proxy is not required as the legal guardian has been given the authority to make medical decisions which are in the best interest of the individual. In some cases, the legal guardian may choose to create a health care proxy and appoint another person to be the individual s health care agent, but this is not required. How to create a Health Care Proxy The health care proxy form must be signed and dated by the individual, in the presence of two adult witnesses. Both witnesses must also sign and date the health care proxy form. If the individual is not physically able to sign the health care proxy form, another person may sign and date the form for the individual in the presence of the two witnesses. The witnesses must document that the individual executed the health care proxy willingly. The person appointed as the health care agent cannot sign as one of the witnesses. 6
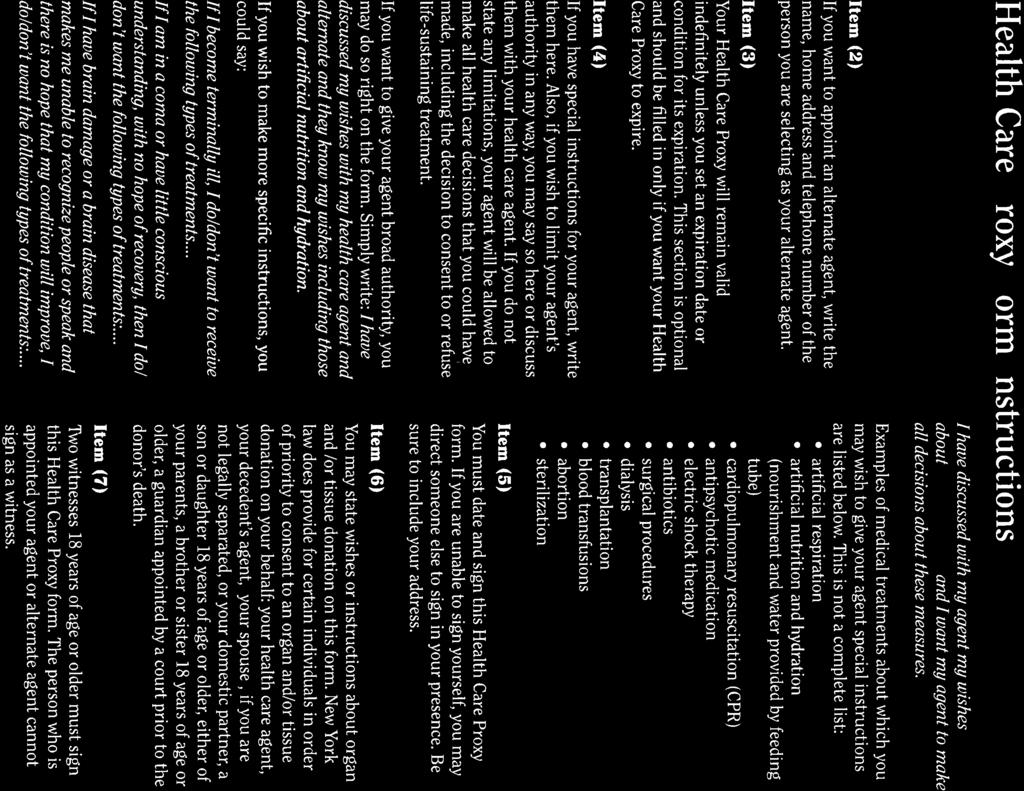
7 Witness Requirements in an OPWDD Certified Residential Setting: (1) at least one witness must be someone who is not affiliated with the residential facility where the individual lives and one witness must be: (a) a NYS licensed physician who is presently employed by the DDSO for at least one year, or (b) a NYS licensed psychologist who is presently employed by the DDSO for at least one year, or (c) the agency s NYS licensed psychologist, who has been working with people with developmental disabilities for at least two years, or (d) a NYS licensed physician who has been approved by OPWDD (some hospitals have doctors who have been approved) Restrictions on who may be the health care agent or alternate agent: (1) for an individual living in an OPWDD certified residential setting such as an IRA the health care agent cannot be any member on the Board, CEO, IRA employee or physician employed with the agency. If any of the individuals listed are related to the individual through blood, marriage or adoption, then they may be appointed as the health care agent (2) the individual s primary physician may not be appointed as the health care agent *If the individual resides in a Family Care setting, the Family Care provider may be appointed as the health care agent The health care proxy must include: (1) the name of the person who the individual has appointed as his/her health care agent (2) a statement confirming that the individual has given the health care agent the authority to make health care decisions on his/her behalf when he/she becomes unable to make the decisions The health care proxy may include: (1) the individual s wishes or instructions about his/her health care decisions. These health care directions may include, but not limited to: (a) administration of artificial nutrition and hydration (feeding tube and IV s) (b) dialysis (c) artificial respiration (d) withholding of life support (e) withdrawal of life support (f) DNR orders (g) Surgical procedures 7
8 (2) limitations to the decisions that the health care agent can make on the individual s behalf (3) that the health care proxy may expire upon a specific date or occurrence of a specific condition. If no specific date or condition is listed, then the health care proxy remains in effect until it is revoked. A health care proxy cannot expire once the individual loses capacity and the agent s authority has been initiated (4) name of the alternate agent if applicable (who will serve in place of the appointed agent when the physician has determined in writing, that the agent is not reasonably available, willing and competent to serve as the agent; or the agent is not expected to become available, willing and competent to make a timely decision regarding the individual s health care needs) When does the Health Care Agent begin making decisions for the individual? The health care agent s ability to make health care decisions for the individual begins when it is determined that the individual lacks capacity to make health care decisions, as a result of the individual s medical condition. The individual s attending physician determines that the individual lacks the capacity to make his/her own health care decisions. When making a determination about the individual s capacity, the attending physician must consult with and receive agreement from a professional who is: (a) a NYS licensed physician presently employed by the DDSO for at least one year, or (b) a NYS licensed psychologist presently employed by the DDSO for at least one year, or (c) the agency s psychologist licensed in NYS, who has been working with people with developmental disabilities for at least two years, or (d) a NYS licensed physician who has been approved by OPWDD (some hospitals have doctors who have been approved) After the consultation regarding the individual s capacity to make health care decisions, the physician must document this determination in the individual s medical record and the following notifications must be made by the attending physician: (a) to the individual, orally and in writing, where there is indication that the individual can understand the notification (b) to the health care agent (c) to the CEO of the agency (if the individual lives in a OPWDD certified residential setting) (d) to the conservator for, or committee or guardian of the individual (if applicable) An individual has the right to object to the determination that he/she lacks the capacity to make health care decisions. 8
9 If an individual has been determined to lose capacity to make health care decisions but then regains his/her ability to make health care decisions, the health care agent s authority will stop at this time. An individual has the right to revoke his/her health care proxy and appoint a new health care proxy. A new health care proxy form should be sent to the individual s physician The health care agent may not make decisions regarding the administration of artificial nutrition and hydration, if the individual has not made his/her wishes known The individual s doctor should keep a copy of the health care proxy in the medical chart. In OPWDD certified residential settings, a copy of the individual s health care proxy should be kept in the individual s record 9
10 Medical Decisions for Individuals Who Lack Capacity Health Care Decisions Act (HCDA) Sometimes an individual lacks the ability to understand medical procedures and is unable to give consent for serious medical treatments, and does not have a legal guardian appointed or a valid Health Care Proxy. It should be documented in the individual s record if, after being assessed by the individual s NYS licensed doctor and a NYS licensed psychologist, that it has been determined that he or she lacks the capacity to make medical decisions for him/herself. If the team is unsure whether the individual has the capacity to make his/her own serious medical decisions, the individual should be assessed by a NYS licensed psychologist and NYS licensed physician (See MOLST section for others who can determine capacity). Who Can Give Consent? For an individual who is 18 years or older and resides in an OPWDD certified residential setting, but lacks capacity to understand the medical treatment, consent must be obtained by one of the surrogates listed below, which are listed in order of priority: 1. a legal guardian with authority to consent to health care 2. an actively involved spouse 3. a parent 4. an actively involved adult child of the individual 5. an actively involved adult sibling 6. an actively involved adult family member (see definition below) 7. the Consumer Advisory Board for Willowbrook Class 8. a surrogate decision-making committee (SDMC) or a court If the individual is under 18 years old, consent must be obtained from one of the surrogates listed below, which are listed in order of priority: 1. a legal guardian with authority to consent to health care 2. an actively involved spouse 3. a parent 4. an actively involved adult sibling 5. an actively involved family member (see definition below) 6. a local commissioner of social services with custody over the minor pursuant to Social Services Law or Family Court Act 7. a surrogate decision-making committee (SDMC) or court If a surrogate is not reasonably available or willing to make a timely decision, and is not expected to become readily available or willing to make a timely decision, the next person on the list, in order listed above, should be contacted. 10
11 Actively involved is defined by the OPWDD regulation (14 NYCRR ) as: Significant and ongoing involvement in a person s life so as to have sufficient knowledge of the person s needs. Family member is defined by the OPWDD regulation (14 NYCRR ) as: Any party related to the individual by blood, marriage or legal adoption. What Medical Decisions Can the Surrogate Make? A surrogate will generally have the authority to make all health care decisions that the individual person could make if he/she had capacity. This includes providing consent for professional medical treatments (see definition below), as well as making decisions to withhold or withdraw life-sustaining treatment. Whenever possible the surrogate and the individual s physician should involve the individual in the discussion about his/her care. Medical decisions made by the authorized surrogate must always be in the best interest of the individual. OPWDD regulation (14 NYCRR part 633) defines professional medical treatment that requires consent as: a medical, dental, surgical or diagnostic intervention or procedure in which a general anesthetic is used or which involves a significant invasion of bodily integrity requiring an incision or producing substantial pain, discomfort, debilitation or having a significant recovery period. In the event of a medical emergency, consent is not required if: the medical, dental, health and hospital services are provided to a person of any age when, in the physician s judgment, an emergency exists creating an immediate need for medical attention. In these medical emergencies, the physician may obtain authorization from the CEO of the agency (if the individual resides in an OPWDD certified setting) if the individual s surrogate is not readily available. Withholding and Withdrawing Life-Sustaining Treatment: The HCDA also grants the Surrogate the authority to make decisions regarding the withholding and withdrawal of life-sustaining treatments for the individual who is experiencing serious and life threatening medical conditions. Life-sustaining treatment includes but is not limited to: artificial nutrition and hydration, CPR, chemotherapy, DNR (Do not resuscitate) order, and DNI (Do not Intubate) order. Unless the individual has a valid health care proxy, a decision to withhold or withdraw life-sustaining treatment must be made in accordance with specific procedures determined by OPWDD. These procedures are discussed in more detail in the MOLST section below. *Sometimes a stand-by guardian is appointed during the 17-A Surrogate court procedure and this person s name is listed in the court papers. A stand by-guardian can immediately take the role of the guardian only when the guardian dies, gives up the role, or the guardian is incapacitated. The stand-by guardian only has 60 days after assuming guardianship to petition the court to become the permanent guardian. 11
12 Medical Orders for Life-Sustaining Treatment (MOLST) What is a MOLST? The MOLST is a form that is completed by the attending physician to document an individual s end of life medical decisions. Many hospitals (especially in the Syracuse area) use the MOLST form. The MOLST allows individuals, legal guardians, involved family members who have been designated as the individual s representative if the individual lacks the ability to make decisions for him/herself, or the Surrogate Decision Making Committee to make decisions regarding life-sustaining treatments for the individual, that are in the best interest of the individual. If an individual, who has been determined to have the capacity to create a health care proxy, has a valid health care proxy and it includes directions about life sustaining treatment, then a MOLST is not required. The MOLST form is used for people with serious health issues or end of life medical conditions. All health care professionals must follow the medical orders, regardless of what setting the individual is in. When an individual resides in an OPWDD certified residential, setting such as an IRA, ICF or Family Care, there are additional requirements put in place to protect the individual s rights. A MOLST must be completed on a standardized form called the DOH-5003 MOLST form and signed by a licensed physician. What is Life-Sustaining Treatment? Life-sustaining treatment is defined as any medical treatment that can sustain life functions and without this treatment the person will most likely die within a relatively short time period. One of the most common examples of life-sustaining treatment is artificial nutrition and hydration through a feeding tube or IV. In June 2010, the law changed and included CPR as a life sustaining treatment; therefore, a DNR (Do not resuscitate) order and a DNI (Do not intubate) order would need to be listed on a MOLST form. What steps are involved in creating a MOLST? For a person living in an OPWDD certified residential setting (IRA, ICF, FC) there is a process that includes the use of a checklist before the physician can sign off on a MOLST form. The required OPWDD checklist ensures that the procedures under the Health Care Decisions Act (HCDA) are followed for decisions to withhold or withdraw life-sustaining treatment for the individual. The physician must document that the individual has a serious illness and meets the requirements of 1750-b of the Surrogate s Court Procedure which includes: 1. Capacity Determination: The physician must confirm to a reasonable degree of medical certainty and document that the individual lacks the capacity to make health care decisions for him/herself. The physician must consult and get agreement with the following health professional: (a) a NYS licensed physician presently employed by the DDSO for at least one year, or (b) a NYS licensed psychologist presently employed by the DDSO for at least one 12
13 year, or (c) the agency s NYS licensed psychologist, who has been working with people with developmental disabilities for at least two years, or (d) a NYS licensed physician who has been approved by OPWDD (some hospitals have doctors who have been approved) 2. Determination of Necessary Medical Criteria: The physician with the agreement of a second physician must determine to a reasonable degree of medical certainty and document that the individual has one of the following medical conditions: (a) a terminal condition; or (b) permanent unconsciousness; or (c) is a medical condition other than the person s DD (developmental disability) which requires life-sustaining treatment, is irreversible and will continue indefinitely AND The life sustaining treatment would cause an extraordinary burden on the individual due to: (a) the individual s medical condition other than DD; and (b) the expected outcome of the life sustaining treatment 3. The physician then completes the OPWDD checklist and signs the checklist with a second witness signature. 4. The physician then completes the MOLST form. The physician and a witness sign the MOLST form. 5. The physician must attach the completed and signed OPWDD checklist to the MOLST and send a copy to MHLS (Mental Hygiene Legal Services). 6. MHLS s primary role is to ensure that the rights of the individual are protected, that the decision is in the best interest of the person and that all required documentation has been completed. MHLS will meet with the individual or may also speak with the legal guardian, family member, doctor or agency provider about the individual s medical condition. 7. If the individual is hospitalized when the MOLST was created and then is released home, the MOLST needs to be reviewed by the individual s doctor on a regular basis to ensure the individual still meets the 1750-b requirements (see above). Although there is no specific frequency written, it is recommended that the individual s doctor reviews the MOLST and signs off that is still applicable every 6 months but minimally every year. 8. For individuals residing in an OPWDD certified setting, a copy of the MOLST and the OPWDD checklist should be kept in the individual s record. 13
14 Withholding or Withdrawing Life-Sustaining Treatment The legal guardian or the individual s authorized representative has the authority to request that additional or current medical life-sustaining treatments be withheld or withdrawn. This is a difficult decision for the guardian and family to make. There are certain criteria under 1750-b and additional notifications that must be made to protect the individual under the law, especially when the individual lives in a certified residential setting (IRA, ICF, FC). 1. If the legal guardian or authorized family member has requested that artificial nutrition or hydration be withdrawn or withheld, the physician must determine and document on the OPWDD checklist form that: (a) there is no reasonable hope of maintaining life; or (b) the artificially provided nutrition or hydration poses an extraordinary burden 2. At least 48 hours prior to the withdrawal or withholding of any life-sustaining treatment (including requesting a DNR), or as soon as possible, the attending physician must notify: (a) the individual with DD, unless therapeutic exception applies; and (b) MHLS and the CEO (Executive Director) of the agency if the person lives in an OPWDD certified residential setting (IRA, ICF, FC); or (c) the Director of the Developmental Disabilities Regional Office (DDRO) ( ) if the individual does not live in a certified residential setting but receives OPWDD services The above parties being notified have the right to object to the decision to withhold or withdraw life-sustaining treatment from the individual. The attending physician will document the notifications on the OPWDD checklist form. If someone objects to the request to withdraw or withhold life-sustaining treatment; the request to withhold or withdraw life-sustaining treatment will be suspended until further mediation or court proceedings determine whether the request will be approved. The attending physician may request the hospital s Ethics Committee review the request if the physician is not in agreement with the request by the legal guardian or authorized family member to withdraw or withhold life-sustaining treatment from the individual. 14
15 Non-Hospital DNR Before the MOLST form was created, an individual, legal guardian or designated surrogate could create a DNR and a non-hospital DNR. A non-hospital DNR is created when the individual leaves the hospital and wants it documented that he/she has a DNR order. A non-hospital DNR is: 1. Created by a physician of a developmental center to be used after the individual leaves the developmental center 2. Created by a physician in a hospital to be used upon release of the individual from the hospital 3. Created by the individual s physician Determination must be made as to whether the individual has the capacity to understand the DNR order and gives consent. If the individual lacks the capacity, the designated surrogate may create the non-hospital DNR on behalf of the individual. (refer to MOLST procedure above for process for determining capacity or surrogate s ability to make decision) The individual has the right to revoke the non-hospital DNR at any time. The individual s doctor must review the non-hospital DNR every 90 days and document this review on the form In an OPWDD certified residential setting (IRA, ICF, FC) a copy of the non-hospital DNR should be kept in the individual s record. 15
16 Additional Resources (Mental Hygiene Legal Services MHLS) (information and forms) 16
17
18
19
20 NEW YORK STATE DEPARTMENT OF HEALTH Medical Orders for Life Sustaining Treatment (MOLST) THE PATIENT KEEPS THE ORIGINAL MOLST FORM DURING TRAVEL TO DIFFERENT CARE SETTINGS. THE PHYSICIAN KEEPS A COPY. LAST NAME/FIRST NAME/MIDDLE INITIAL OF PATIENT ADDRESS CITY/STATE/ZIP DATE OF BIRTH (MM/DD/YYYY) Male Female emolst NUMBER (THIS IS NOT AN emolst FORM) Do Not Resuscitate (DNR) and Other Life Sustaining Treatment (LST) This is a medical order form that tells others the patient s wishes for life sustaining treatment. A health care professional must complete or change the MOLST form, based on the patient s current medical condition, values, wishes and MOLST Instructions. If the patient is unable to make medical decisions, the orders should reflect patient wishes, as best understood by the health care agent or surrogate. A physician must sign the MOLST form. All health care professionals must follow these medical orders as the patient moves from one location to another, unless a physician examines the patient, reviews the orders and changes them. MOLST is generally for patients with serious health conditions. The patient or other decision maker should work with the physician and consider asking the physician to fill out a MOLST form if the patient: Wants to avoid or receive any or all life sustaining treatment. Resides in a long term care facility or requires long term care services. Might die within the next year. If the patient has a developmental disability and does not have ability to decide, the doctor must follow special procedures and attach the appropriate legal requirements checklist. SECTION A Resuscitation Instructions When the Patient Has No Pulse and/or Is Not Breathing Check one: CPR Order: Attempt Cardio Pulmonary Resuscitation CPR involves artificial breathing and forceful pressure on the chest to try to restart the heart. It usually involves electric shock (defibrillation) and a plastic tube down the throat into the windpipe to assist breathing (intubation). It means that all medical treatments will be done to prolong life when the heart stops or breathing stops, including being placed on a breathing machine and being transferred to the hospital. DNR Order: Do Not Attempt Resuscitation (Allow Natural Death) This means do not begin CPR, as defined above, to make the heart or breathing start again if either stops. SECTION B Consent for Resuscitation Instructions (Section A) The patient can make a decision about resuscitation if he or she has the ability to decide about resuscitation. If the patient does NOT have the ability to decide about resuscitation and has a health care proxy, the health care agent makes this decision. If there is no health care proxy, another person will decide, chosen from a list based on NYS law. SIGNATURE Check if verbal consent (Leave signature line blank) DATE/TIME PRINT NAME OF DECISION MAKER PRINT FIRST WITNESS NAME PRINT SECOND WITNESS NAME Who made the decision? Patient Health Care Agent Public Health Law Surrogate Minor s Parent/Guardian 1750 b Surrogate SECTION C Physician Signature for Sections A and B PHYSICIAN SIGNATURE PRINT PHYSICIAN NAME DATE/TIME PHYSICIAN LICENSE NUMBER PHYSICIAN PHONE/PAGER NUMBER SECTION D Advance Directives Check all advance directives known to have been completed: Health Care Proxy Living Will Organ Donation Documentation of Oral Advance Directive DOH 5003 (6/10) Page 1 of 4 HIPAA permits disclosure of MOLST to other health care professionals & electronic registry as necessary for treatment.
21 THE PATIENT KEEPS THE ORIGINAL MOLST FORM DURING TRAVEL TO DIFFERENT CARE SETTINGS. THE PHYSICIAN KEEPS A COPY. LAST NAME/FIRST NAME/MIDDLE INITIAL OF PATIENT DATE OF BIRTH (MM/DD/YYYY) SECTION E Orders For Other Life Sustaining Treatment and Future Hospitalization When the Patient has a Pulse and the Patient is Breathing Life sustaining treatment may be ordered for a trial period to determine if there is benefit to the patient. If a life sustaining treatment is started, but turns out not to be helpful, the treatment can be stopped. Treatment Guidelines No matter what else is chosen, the patient will be treated with dignity and respect, and health care providers will offer comfort measures. Check one: Comfort measures only Comfort measures are medical care and treatment provided with the primary goal of relieving pain and other symptoms and reducing suffering. Reasonable measures will be made to offer food and fluids by mouth. Medication, turning in bed, wound care and other measures will be used to relieve pain and suffering. Oxygen, suctioning and manual treatment of airway obstruction will be used as needed for comfort. Limited medical interventions The patient will receive medication by mouth or through a vein, heart monitoring and all other necessary treatment, based on MOLST orders. No limitations on medical interventions The patient will receive all needed treatments. Instructions for Intubation and Mechanical Ventilation Check one: Do not intubate (DNI) Do not place a tube down the patient s throat or connect to a breathing machine that pumps air into and out of lungs. Treatments are available for symptoms of shortness of breath, such as oxygen and morphine. (This box should not be checked if full CPR is checked in Section A.) A trial period Check one or both: Intubation and mechanical ventilation Noninvasive ventilation (e.g. BIPAP), if the health care professional agrees that it is appropriate Intubation and long term mechanical ventilation, if needed Place a tube down the patient s throat and connect to a breathing machine as long as it is medically needed. Future Hospitalization/Transfer Check one: Do not send to the hospital unless pain or severe symptoms cannot be otherwise controlled. Send to the hospital, if necessary, based on MOLST orders. Artificially Administered Fluids and Nutrition When a patient can no longer eat or drink, liquid food or fluids can be given by a tube inserted in the stomach or fluids can be given by a small plastic tube (catheter) inserted directly into the vein. If a patient chooses not to have either a feeding tube or IV fluids, food and fluids are offered as tolerated using careful hand feeding. Check one each for feeding tube and IV fluids: No feeding tube No IV fluids A trial period of feeding tube A trial period of IV fluids Long term feeding tube, if needed Antibiotics Check one: Do not use antibiotics. Use other comfort measures to relieve symptoms. Determine use or limitation of antibiotics when infection occurs. Use antibiotics to treat infections, if medically indicated. Other Instructions about starting or stopping treatments discussed with the doctor or about other treatments not listed above (dialysis, transfusions, etc.). Consent for Life Sustaining Treatment Orders (Section E) (Same as Section B, which is the consent for Section A) SIGNATURE Check if verbal consent (Leave signature line blank) DATE/TIME PRINT NAME OF DECISION MAKER PRINT FIRST WITNESS NAME PRINT SECOND WITNESS NAME Who made the decision? Patient Health Care Agent Based on clear and convincing evidence of patient s wishes Public Health Law Surrogate Minor s Parent/Guardian 1750 b Surrogate Physician Signature for Section E PHYSICIAN SIGNATURE PRINT PHYSICIAN NAME DATE/TIME DOH 5003 (6/10) Page 2 of 4 This MOLST form has been approved by the NYSDOH for use in all settings.
22 THE PATIENT KEEPS THE ORIGINAL MOLST FORM DURING TRAVEL TO DIFFERENT CARE SETTINGS. THE PHYSICIAN KEEPS A COPY. LAST NAME/FIRST NAME/MIDDLE INITIAL OF PATIENT DATE OF BIRTH (MM/DD/YYYY) SECTION F Review and Renewal of MOLST Orders on This MOLST Form The physician must review the form from time to time as the law requires, and also: If the patient moves from one location to another to receive care; or If the patient has a major change in health status (for better or worse); or If the patient or other decision maker changes his or her mind about treatment. Date/Time Reviewer s Name and Signature Location of Review (e.g., Hospital, NH, Physician s Office) Outcome of Review DOH 5003 (6/10) Page 3 of 4
23 THE PATIENT KEEPS THE ORIGINAL MOLST FORM DURING TRAVEL TO DIFFERENT CARE SETTINGS. THE PHYSICIAN KEEPS A COPY. LAST NAME/FIRST NAME/MIDDLE INITIAL OF PATIENT DATE OF BIRTH (MM/DD/YYYY) SECTION F Review and Renewal of MOLST Orders on This MOLST Form Continued from Page 3 Date/Time Reviewer s Name and Signature Location of Review (e.g., Hospital, NH, Physician s Office) Outcome of Review DOH 5003 (6/10) Page 4 of 4
24 MOLST LEGAL REQUIREMENTS CHECKLIST FOR INDIVIDUALS WITH DEVELOPMENTAL DISABILITIES LAST NAME/FIRST NAME DATE OF BIRTH ADDRESS Note: Actual orders should be placed on the MOLST form with this completed checklist attached. Use of this checklist is required for individuals with developmental disabilities (DD) who lack the capacity to make their own health care decisions and do not have a health care proxy. Medical decisions which involve the withholding or withdrawing of life sustaining treatment (LST) for individuals with DD who lack capacity and do not have a health care proxy must comply with the process set forth in the Health Care Decisions Act for persons with MR (HCDA) [SCPA 1750-b (4)]. Effective June 1, 2010, this includes the issuance of DNR orders. Step 1 Identification of Appropriate 1750-b Surrogate from Prioritized List. Check appropriate category and add name of surrogate. a. 17-A guardian b. actively involved spouse c. actively involved parent d. actively involved adult child e. actively involved adult sibling f. actively involved family member g. Willowbrook CAB (full representation) h. Surrogate Decision Making Committee (MHL Article 80) Step b surrogate has a conversation or a series of conversations with the treating physician regarding possible treatment options and goals for care. Following these discussions, the 1750-b surrogate makes a decision to withhold or withdraw LST, either orally or in writing. Specify the LST that is requested to be withdrawn or withheld: Decision made orally Witness Attending Physician Second Witness Decision made in writing (must be dated, signed by surrogate, signed by 1 witness and given to attending physician). Revised 3/18/2013 Page 1 of 3
25 LAST NAME/FIRST NAME DATE OF BIRTH Step 3 Confirm individual s lack of capacity to make health care decisions. Either the attending physician or the concurring physician or licensed psychologist must: (a) be employed by a DDSO; or (b) have been employed for at least 2 years in a facility or program operated, licensed or authorized by OPWDD; or (c) have been approved by the commissioner of OPWDD as either possessing specialized training or have 3 years experience in providing services to individuals with DD. Attending Physician Concurring Physician or Licensed Psychologist Step 4 Determination of Necessary Medical Criteria. We have determined to a reasonable degree of medical certainty that both of the following conditions are met: (1) the individual has one of the following medical conditions: a. a terminal condition; (briefly describe ); or b. permanent unconsciousness; or c. a medical condition other than DD which requires LST, is irreversible and which will continue indefinitely (briefly describe ) AND (2) the LST would impose an extraordinary burden on the individual in light of: a. the person s medical condition other than DD (briefly explain ) and b. the expected outcome of the LST, notwithstanding the person s DD (briefly explain ) If the 1750-b surrogate has requested that artificially provided nutrition or hydration be withdrawn or withheld, one of the following additional factors must also be met: a. there is no reasonable hope of maintaining life (explain ); or b. the artificially provided nutrition or hydration poses an extraordinary burden (explain ). Attending Physician Concurring Physician Revised 3/18/2013 Page 2 of 3
26 LAST NAME/FIRST NAME DATE OF BIRTH Step 5 Notifications. At least 48 hours prior to the implementation of a decision to withdraw LST, or at the earliest possible time prior to a decision to withhold LST, the attending physician must notify the following parties: the person with DD, unless therapeutic exception applies notified on / / if the person is in or was transferred from an OPWDD residential facility Facility Director notified on / / MHLS notified on / / if the person is not in and was not transferred from an OPWDD residential facility the director of the local DDSO notified on / / Step 6 - I certify that the 1750-b process has been complied with, the appropriate parties have been notified and no objection to the surrogate s decision remains unresolved. Attending Physician Date Note: The MOLST form may ONLY be completed with the 1750-b surrogate after all 6 steps on this checklist have been completed. Revised 3/18/2013 Page 3 of 3
27 State of New York Department of Health Nonhospital Order Not to Resuscitate (DNR Order) Person's Name Date of Birth / / Do not resuscitate the person named above. Physician's Signature Print Name License Number Date / / It is the responsibility of the physician to determine, at least every 90 days, whether this order continues to be appropriate, and to indicate this by a note in the person's medical chart. The issuance of a new form is NOT required, and under the law this order should be considered valid unless it is known that it has been revoked. This order remains valid and must be followed, even if it has not been reviewed within the 90-day period. DOH-3474 (04/09)
 NEW YORK STATE DEPARTMENT OF HEALTH Medical Orders for Life Sustaining Treatment (MOLST) THE PATIENT KEEPS THE ORIGINAL MOLST FORM DURING TRAVEL TO DIFFERENT CARE SETTINGS. THE PHYSICIAN KEEPS A COPY.
NEW YORK STATE DEPARTMENT OF HEALTH Medical Orders for Life Sustaining Treatment (MOLST) THE PATIENT KEEPS THE ORIGINAL MOLST FORM DURING TRAVEL TO DIFFERENT CARE SETTINGS. THE PHYSICIAN KEEPS A COPY.
Deciding About. Health Care A GUIDE FOR PATIENTS AND FAMILIES. New York State Department of Health
 Deciding About Health Care A GUIDE FOR PATIENTS AND FAMILIES New York State Department of Health 2 Introduction Who should read this guide? This guide is for New York State patients and for those who will
Deciding About Health Care A GUIDE FOR PATIENTS AND FAMILIES New York State Department of Health 2 Introduction Who should read this guide? This guide is for New York State patients and for those who will
Supersedes/Updates: 99-10
 No. 08-07 New York State Department of Health Bureau of Emergency Medical Services POLICY STATEMENT Supersedes/Updates: 99-10 November 20, 2008 Re: Medical Orders for Life Sustaining Treatment (MOLST)
No. 08-07 New York State Department of Health Bureau of Emergency Medical Services POLICY STATEMENT Supersedes/Updates: 99-10 November 20, 2008 Re: Medical Orders for Life Sustaining Treatment (MOLST)
Family Health Care Decisions Act (FHCDA)
") Family Health Care Decisions Act (FHCDA) Public Health Law Article 29-CC Added by L. 2010, Ch. 8 Applies to general hospitals and residential health care facilities (nursing homes) Went into effect on
Family Health Care Decisions Act (FHCDA) Public Health Law Article 29-CC Added by L. 2010, Ch. 8 Applies to general hospitals and residential health care facilities (nursing homes) Went into effect on
LOUISIANA ADVANCE DIRECTIVES
 LOUISIANA ADVANCE DIRECTIVES Legal Documents that Ensure that Your Choices for Future Medical Care or the Refusal of Same are Honored and Implemented by Your Health Care Providers Peoples Health is a Medicare
LOUISIANA ADVANCE DIRECTIVES Legal Documents that Ensure that Your Choices for Future Medical Care or the Refusal of Same are Honored and Implemented by Your Health Care Providers Peoples Health is a Medicare
YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE
 YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE Communicating Your Health Care Choices In 1990, Congress passed the Patient Self-Determination Introduction Act. It requires
YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE Communicating Your Health Care Choices In 1990, Congress passed the Patient Self-Determination Introduction Act. It requires
Advance Directives The Patient s Right To Decide CH Oct. 2013
 Advance Directives The Patient s Right To Decide CH80850040 Oct. 2013 Advance Directives Your Right To Make Health Care Decisions Under The Law In Tennessee Tennessee and federal law give every competent
Advance Directives The Patient s Right To Decide CH80850040 Oct. 2013 Advance Directives Your Right To Make Health Care Decisions Under The Law In Tennessee Tennessee and federal law give every competent
MAKING YOUR WISHES KNOWN: Advance Care Planning Guide
 MAKING YOUR WISHES KNOWN: Advance Care Planning Guide ADVANCE CARE PLANNING The process of learning about the type of medical decisions that may need to be made, considering those decisions ahead of time
MAKING YOUR WISHES KNOWN: Advance Care Planning Guide ADVANCE CARE PLANNING The process of learning about the type of medical decisions that may need to be made, considering those decisions ahead of time
What Are Advance Medical Directives?
 What Are Advance Medical Directives? UAMS would like you to know there are ways to let others know what decisions you would want to make about your medical treatments, even when you are unable to speak
What Are Advance Medical Directives? UAMS would like you to know there are ways to let others know what decisions you would want to make about your medical treatments, even when you are unable to speak
My Voice - My Choice
 My Voice - My Choice My Advance Directive Table of Contents Introduction... 2 Words You Need to Know... 3 Legal Document... 4 Helpful Information about your Advance Directive... 10 What makes your life
My Voice - My Choice My Advance Directive Table of Contents Introduction... 2 Words You Need to Know... 3 Legal Document... 4 Helpful Information about your Advance Directive... 10 What makes your life
ADVANCE DIRECTIVE FOR HEALTH CARE
 ADVANCE DIRECTIVE FOR HEALTH CARE This document includes a list of definitions and the two types of Advance Directives (together called a Combined Directive). Some people choose to fill out only one portion.
ADVANCE DIRECTIVE FOR HEALTH CARE This document includes a list of definitions and the two types of Advance Directives (together called a Combined Directive). Some people choose to fill out only one portion.
Your Right to Make Health Care Decisions in Colorado
 Your Right to Make Health Care Decisions in Colorado This e-book informs you about your right to make health care decisions, including the right to accept or refuse medical treatment. It explains the following
Your Right to Make Health Care Decisions in Colorado This e-book informs you about your right to make health care decisions, including the right to accept or refuse medical treatment. It explains the following
TheValues History: A Worksheet for Advance Directives Courtesy of Somerset Hospital s Ethics Committee
 TheValues History: A Worksheet for Advance Directives Courtesy of Somerset Hospital s Ethics Committee Advance Directives Living Wills Power of Attorney The Values History: A Worksheet for Advanced Directives
TheValues History: A Worksheet for Advance Directives Courtesy of Somerset Hospital s Ethics Committee Advance Directives Living Wills Power of Attorney The Values History: A Worksheet for Advanced Directives
ALLINA HOME & COMMUNITY SERVICES ALLINA HEALTH. Advance Care Planning. Discussion guide. Discussion Guide. Advance care planning
 ALLINA HOME & COMMUNITY SERVICES ALLINA HEALTH Advance Care Planning Discussion guide Discussion Guide Advance care planning Advance care planning Any of us could think of a time when we might be too sick
ALLINA HOME & COMMUNITY SERVICES ALLINA HEALTH Advance Care Planning Discussion guide Discussion Guide Advance care planning Advance care planning Any of us could think of a time when we might be too sick
Minnesota Health Care Directive Planning Toolkit
 Minnesota Health Care Directive Planning Toolkit This planning toolkit contains information to help you: Plan Ahead Understand Common Terms Know the Facts Complete a Health Care Directive: Step-by-Step
Minnesota Health Care Directive Planning Toolkit This planning toolkit contains information to help you: Plan Ahead Understand Common Terms Know the Facts Complete a Health Care Directive: Step-by-Step
Advance Care Planning
 Community-wide End-of-life /Palliative Care Initiative Community Conversations on Compassionate Care Advance Care Planning Know your choices, share your wishes: Maintain control, achieve peace of mind,
Community-wide End-of-life /Palliative Care Initiative Community Conversations on Compassionate Care Advance Care Planning Know your choices, share your wishes: Maintain control, achieve peace of mind,
ADVANCE HEALTH CARE DIRECTIVE HEALTH CARE POWER OF ATTORNEY AND LIVING WILL
 ADVANCE HEALTH CARE DIRECTIVE A HEALTH CARE POWER OF ATTORNEY AND LIVING WILL INSIDE: LEGAL DOCUMENTS AND INSTRUCTIONS TO ASSIST YOU WITH IMPORTANT HEALTH CARE DECISIONS Health Care Decision Making Modern
ADVANCE HEALTH CARE DIRECTIVE A HEALTH CARE POWER OF ATTORNEY AND LIVING WILL INSIDE: LEGAL DOCUMENTS AND INSTRUCTIONS TO ASSIST YOU WITH IMPORTANT HEALTH CARE DECISIONS Health Care Decision Making Modern
Living Will Sample Massachusetts (aka "Advanced Medical Directive")
") Living Will Sample Massachusetts (aka "Advanced Medical Directive") Online Living Will Form $8.99 (free trial) click here ADVANCE MEDICAL DIRECTIVE AND HEALTH CARE PROXY GIVEN BY JAMES ROBERT HEDGES THIS
Living Will Sample Massachusetts (aka "Advanced Medical Directive") Online Living Will Form $8.99 (free trial) click here ADVANCE MEDICAL DIRECTIVE AND HEALTH CARE PROXY GIVEN BY JAMES ROBERT HEDGES THIS
WYOMING Advance Directive Planning for Important Healthcare Decisions
 WYOMING Advance Directive Planning for Important Healthcare Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CARING CONNECTIONS Caring Connections,
WYOMING Advance Directive Planning for Important Healthcare Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CARING CONNECTIONS Caring Connections,
ADVANCE DIRECTIVE INFORMATION
 ADVANCE DIRECTIVE INFORMATION NOTE: This Advance Directive Information and the form Living Will and Durable Power of Attorney for Health Care on the Arkansas Bar Association s website are being provided
ADVANCE DIRECTIVE INFORMATION NOTE: This Advance Directive Information and the form Living Will and Durable Power of Attorney for Health Care on the Arkansas Bar Association s website are being provided
Advance Health Care Planning: Making Your Wishes Known. MC rev0813
 Advance Health Care Planning: Making Your Wishes Known MC2107-14rev0813 What s Inside Why Health Care Planning Is Important... 2 What You Can Do... 4 Work through the advance health care planning process...
Advance Health Care Planning: Making Your Wishes Known MC2107-14rev0813 What s Inside Why Health Care Planning Is Important... 2 What You Can Do... 4 Work through the advance health care planning process...
Facing Serious Illness: Make Your Wishes Known to your Health Care Professional
 Facing Serious Illness: Make Your Wishes Known to your Health Care Professional Your Guide to the Oregon POLST Program Physician Orders for Life-Sustaining Treatment Revised: February 19, 2015 This material
Facing Serious Illness: Make Your Wishes Known to your Health Care Professional Your Guide to the Oregon POLST Program Physician Orders for Life-Sustaining Treatment Revised: February 19, 2015 This material
and Affiliates Policy & Procedure Date of Origin: 10/95 Last Reviewed: 12/03 Last Revised: 12/03
 Table of Contents Topic Policy Procedure Page # Page # Purpose and Scope 1 11 Definitions.. 2 - Capacity.. 3 - Who May Consent. 5 - Consent Process. - 13 Levels of Care/Additional Treatment Guidelines
Table of Contents Topic Policy Procedure Page # Page # Purpose and Scope 1 11 Definitions.. 2 - Capacity.. 3 - Who May Consent. 5 - Consent Process. - 13 Levels of Care/Additional Treatment Guidelines
State of Ohio Health Care Power of Attorney of
 Page1 State of Ohio Health Care Power of Attorney of (Print Full Name) (Birth Date) I state that this is my Health Care Power of Attorney and I revoke any prior Health Care Power of Attorney signed by
Page1 State of Ohio Health Care Power of Attorney of (Print Full Name) (Birth Date) I state that this is my Health Care Power of Attorney and I revoke any prior Health Care Power of Attorney signed by
Your Guide to Advance Directives
 Starting Points: Your Guide to Advance Directives Values Statements Healthcare Directives Durable Power of Attorney for Healthcare 1 2 Advances in medicine are helping people to live longer than ever before.
Starting Points: Your Guide to Advance Directives Values Statements Healthcare Directives Durable Power of Attorney for Healthcare 1 2 Advances in medicine are helping people to live longer than ever before.
ADVANCE CARE PLANNING DOCUMENTS
 ADVANCE CARE PLANNING DOCUMENTS Legal Documents to Assure Your Future Health Care Choices Distributed as a Public Service by THE NEVADA CENTER FOR ETHICS & HEALTH POLICY University of Nevada, Reno Revised
ADVANCE CARE PLANNING DOCUMENTS Legal Documents to Assure Your Future Health Care Choices Distributed as a Public Service by THE NEVADA CENTER FOR ETHICS & HEALTH POLICY University of Nevada, Reno Revised
PATIENT INFORMATION ON NEVADA STATE LAW CONCERNING ADVANCE DIRECTIVES TODAY S HEALTHCARE CHOICES
 PATIENT INFORMATION ON NEVADA STATE LAW CONCERNING ADVANCE DIRECTIVES Attachment A TODAY S HEALTHCARE CHOICES Years ago we didn t have the choices in medical care that we have today. Seriously ill people,
PATIENT INFORMATION ON NEVADA STATE LAW CONCERNING ADVANCE DIRECTIVES Attachment A TODAY S HEALTHCARE CHOICES Years ago we didn t have the choices in medical care that we have today. Seriously ill people,
Advance Directive Form
 Advance Directive Form NOTE: This form is being provided to you as a public service. The attached forms are provided as is and are not the substitute for the advice of an attorney. By providing these forms
Advance Directive Form NOTE: This form is being provided to you as a public service. The attached forms are provided as is and are not the substitute for the advice of an attorney. By providing these forms
MY ADVANCE CARE PLANNING GUIDE
 MY DVNCE CRE PLNNING GUIDE Let s TLK! Tell us your values and beliefs about your healthcare. Take time to have the conversation with your physician and your family. lways be open and honest. Leave no doubt
MY DVNCE CRE PLNNING GUIDE Let s TLK! Tell us your values and beliefs about your healthcare. Take time to have the conversation with your physician and your family. lways be open and honest. Leave no doubt
DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Rhode Island Version) You must be at least eighteen (18) years of age.
 You must be at least eighteen (18) years of age.") MASSASOIT INTERNAL MEDICINE (401) 434-2704 massasoitmed.com DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Rhode Island Version) THE DURABLE POWER OF ATTORNEY FOR HEALTH CARE DOCUMENT lets you appoint someone
MASSASOIT INTERNAL MEDICINE (401) 434-2704 massasoitmed.com DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Rhode Island Version) THE DURABLE POWER OF ATTORNEY FOR HEALTH CARE DOCUMENT lets you appoint someone
DURABLE HEALTH CARE POWER OF ATTORNEY AND HEALTH CARE TREATMENT INSTRUCTIONS (LIVING WILL) PART I INTRODUCTORY REMARKS ON HEALTH CARE DECISION MAKING
 PART I INTRODUCTORY REMARKS ON HEALTH CARE DECISION MAKING") DURABLE HEALTH CARE POWER OF ATTORNEY AND HEALTH CARE TREATMENT INSTRUCTIONS (LIVING WILL) PART I INTRODUCTORY REMARKS ON HEALTH CARE DECISION MAKING You have the right to decide the type of health care
DURABLE HEALTH CARE POWER OF ATTORNEY AND HEALTH CARE TREATMENT INSTRUCTIONS (LIVING WILL) PART I INTRODUCTORY REMARKS ON HEALTH CARE DECISION MAKING You have the right to decide the type of health care
Massachusetts Medical Orders for Life Sustaining Treatment (MOLST)
") Massachusetts Medical Orders for Life Sustaining Treatment (MOLST) Prepared by the Center for Developmental Disabilities Evaluation and Research (CDDER) on behalf of the Massachusetts Department of Developmental
Massachusetts Medical Orders for Life Sustaining Treatment (MOLST) Prepared by the Center for Developmental Disabilities Evaluation and Research (CDDER) on behalf of the Massachusetts Department of Developmental
State of Ohio Living Will Declaration with Donor Registry Enrollment Form and State of Ohio Health Care Power of Attorney
 State of Ohio Living Will Declaration with Donor Registry Enrollment Form and State of Ohio Health Care Power of Attorney May 2012 Ohio State Bar Association State of Ohio Living Will Declaration Notice
State of Ohio Living Will Declaration with Donor Registry Enrollment Form and State of Ohio Health Care Power of Attorney May 2012 Ohio State Bar Association State of Ohio Living Will Declaration Notice
NEBRASKA Advance Directive Planning for Important Healthcare Decisions
 NEBRASKA Advance Directive Planning for Important Healthcare Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program of
NEBRASKA Advance Directive Planning for Important Healthcare Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program of
MY ADVANCE CARE PLANNING GUIDE
 MY DVNCE CRE PLNNING GUIDE Let s TLK! Tell us your values and beliefs about your healthcare. Take time to have the conversation with your physician and your family. lways be open and honest. Leave no doubt
MY DVNCE CRE PLNNING GUIDE Let s TLK! Tell us your values and beliefs about your healthcare. Take time to have the conversation with your physician and your family. lways be open and honest. Leave no doubt
Ambulatory Surgery Center Patient Consent to Resuscitative Measures
 Ambulatory Surgery Center Patient Consent to Resuscitative Measures Not a Revocation of Advance Directives or Medical Power Of Attorney All patients have the right to participate in their own health care
Ambulatory Surgery Center Patient Consent to Resuscitative Measures Not a Revocation of Advance Directives or Medical Power Of Attorney All patients have the right to participate in their own health care
Chart Documentation Form
 Chart Documentation Form Aligns with Legal Requirements Checklist #4 Adult hospital or nursing home patients without medical decision-making capacity who do not have a health care proxy and for whom no
Chart Documentation Form Aligns with Legal Requirements Checklist #4 Adult hospital or nursing home patients without medical decision-making capacity who do not have a health care proxy and for whom no
HealthStream Regulatory Script
 HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
ADVANCE DIRECTIVE PACKET Question and Answer Section
 ADVANCE DIRECTIVE PACKET Question and Answer Section Please review the following facts regarding what an Advance Directive is, as well as your right as an adult to create one. If you decide to complete
ADVANCE DIRECTIVE PACKET Question and Answer Section Please review the following facts regarding what an Advance Directive is, as well as your right as an adult to create one. If you decide to complete
LOUISIANA ADVANCE DIRECTIVES
 LOUISIANA ADVANCE DIRECTIVES Legal Documents To Make Sure Your Choices for Future Medical Care or the Refusal of Same are Honored and Implemented by Your Health Care Providers ADVANCE DIRECTIVES INTRODUCTION
LOUISIANA ADVANCE DIRECTIVES Legal Documents To Make Sure Your Choices for Future Medical Care or the Refusal of Same are Honored and Implemented by Your Health Care Providers ADVANCE DIRECTIVES INTRODUCTION
L e g a l I s s u e s i n H e a l t h C a r e
 Page 1 L e g a l I s s u e s i n H e a l t h C a r e Tutorial #6 January 2008 Introduction Patients have the right to accept or refuse health care treatment. For a patient to exercise that right, he or
Page 1 L e g a l I s s u e s i n H e a l t h C a r e Tutorial #6 January 2008 Introduction Patients have the right to accept or refuse health care treatment. For a patient to exercise that right, he or
DOWNLOAD COVERSHEET:
 DOWNLOAD COVERSHEET: This is a standard advance directive for your state, made available to you as a courtesy by Lifecare Directives, LLC. You should be aware that extensive research has demonstrated that
DOWNLOAD COVERSHEET: This is a standard advance directive for your state, made available to you as a courtesy by Lifecare Directives, LLC. You should be aware that extensive research has demonstrated that
Your Right to Make Health Care Decisions
 42 P O Box 10600 Grand Junction, CO 81502-5600 Your Right to Make Health Care Decisions Advance Directives What is an Advance Directive? It is a type of written instruction about your health care to be
42 P O Box 10600 Grand Junction, CO 81502-5600 Your Right to Make Health Care Decisions Advance Directives What is an Advance Directive? It is a type of written instruction about your health care to be
Advance Directive. my wish for: my voice my choice. health care power of attorney and living will
 health care power of attorney and living will print your name date of birth for information contact: patient relations at 910 615-6120 my voice my choice. my wish for: The person I want to make care decisions
health care power of attorney and living will print your name date of birth for information contact: patient relations at 910 615-6120 my voice my choice. my wish for: The person I want to make care decisions
MASSACHUSETTS Advance Directive Planning for Important Healthcare Decisions
 MASSACHUSETTS Advance Directive Planning for Important Healthcare Decisions Caring Connections 1700 Diagonal Road, Suite 625, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a
MASSACHUSETTS Advance Directive Planning for Important Healthcare Decisions Caring Connections 1700 Diagonal Road, Suite 625, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a
Saint Agnes Medical Center. Guidelines for Signers
 597 Saint Agnes Medical Center Page 1 Guidelines for Signers What is an Advance Health Care Directive? An "Advance Health Care Directive" is a document you can use to appoint another person, such as a
597 Saint Agnes Medical Center Page 1 Guidelines for Signers What is an Advance Health Care Directive? An "Advance Health Care Directive" is a document you can use to appoint another person, such as a
Planning in Advance for Your Health Care
 Planning in Advance for Your Health Care This booklet will help you to plan ahead. If you have any questions please call for assistance: NWH Patient Relations Representative 617-243-5052 NWH Pastoral Care:
Planning in Advance for Your Health Care This booklet will help you to plan ahead. If you have any questions please call for assistance: NWH Patient Relations Representative 617-243-5052 NWH Pastoral Care:
Maryland MOLST for the Health Care Practitioner. Maryland MOLST Training Task Force July 2013
 Maryland MOLST for the Health Care Practitioner Maryland MOLST Training Task Force July 2013 What is the Health Care Decisions Act? Health Care Decisions Act Applies in all health care settings and in
Maryland MOLST for the Health Care Practitioner Maryland MOLST Training Task Force July 2013 What is the Health Care Decisions Act? Health Care Decisions Act Applies in all health care settings and in
MY CHOICES. Information on: Advance Care Directive Living Will POLST Orders
 MY CHOICES Information on: Advance Care Directive Living Will POLST Orders My Choices Adults have the right to accept or refuse medical care. As long as you can make health care decisions for yourself,
MY CHOICES Information on: Advance Care Directive Living Will POLST Orders My Choices Adults have the right to accept or refuse medical care. As long as you can make health care decisions for yourself,
Georgia Advance Directive for Healthcare
 Navicent Health Georgia Advance Directive for Healthcare GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE By: Date of Birth: (Print Name) (Month/Day/Year) PART ONE HEALTH CARE AGENT This part allows you to choose
Navicent Health Georgia Advance Directive for Healthcare GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE By: Date of Birth: (Print Name) (Month/Day/Year) PART ONE HEALTH CARE AGENT This part allows you to choose
Advanced Directive For Health Care
 Advanced Directive For Health Care Your Right to Make Your Own Decisions About Medical Care The best source for more information about Advanced Directive is your attorney. Patients of Helen Keller Hospital
Advanced Directive For Health Care Your Right to Make Your Own Decisions About Medical Care The best source for more information about Advanced Directive is your attorney. Patients of Helen Keller Hospital
ABOUT THE ADVANCE DIRECTIVE FOR RECEIVING ORAL FOOD AND FLUIDS IN DEMENTIA. Introduction
 ABOUT THE ADVANCE DIRECTIVE FOR RECEIVING ORAL FOOD AND FLUIDS IN DEMENTIA Introduction There are two purposes to completing an Advance Directive for Receiving Oral Food and Fluids In Dementia. The first
ABOUT THE ADVANCE DIRECTIVE FOR RECEIVING ORAL FOOD AND FLUIDS IN DEMENTIA Introduction There are two purposes to completing an Advance Directive for Receiving Oral Food and Fluids In Dementia. The first
A PERSONAL DECISION
 A PERSONAL DECISION Practical information about determining your future medical care including declaration, powers of attorney for health care and organ donation Determining Your Medical Care is Your
A PERSONAL DECISION Practical information about determining your future medical care including declaration, powers of attorney for health care and organ donation Determining Your Medical Care is Your
SOUTH CAROLINA HEALTH CARE POWER OF ATTORNEY
 SOUTH CAROLINA HEALTH CARE POWER OF ATTORNEY INFORMATION ABOUT THIS DOCUMENT THIS IS AN IMPORTANT LEGAL DOCUMENT. BEFORE SIGNING THIS DOCUMENT, YOU SHOULD KNOW THESE IMPORTANT FACTS: 1. THIS DOCUMENT GIVES
SOUTH CAROLINA HEALTH CARE POWER OF ATTORNEY INFORMATION ABOUT THIS DOCUMENT THIS IS AN IMPORTANT LEGAL DOCUMENT. BEFORE SIGNING THIS DOCUMENT, YOU SHOULD KNOW THESE IMPORTANT FACTS: 1. THIS DOCUMENT GIVES
COLORADO Advance Directive Planning for Important Healthcare Decisions
 COLORADO Advance Directive Planning for Important Healthcare Decisions Caring Connections 1700 Diagonal Road, Suite 625, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
COLORADO Advance Directive Planning for Important Healthcare Decisions Caring Connections 1700 Diagonal Road, Suite 625, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
DIRECTIVE TO PHYSICIANS AND FAMILY OR SURROGATES Advance Directives Act (see , Health and Safety Code) DIRECTIVE
 DIRECTIVE") DIRECTIVE TO PHYSICIANS AND FAMILY OR SURROGATES Advance Directives Act (see 166.033, Health and Safety Code) Instructions for completing this document: This is an important legal document known as an
DIRECTIVE TO PHYSICIANS AND FAMILY OR SURROGATES Advance Directives Act (see 166.033, Health and Safety Code) Instructions for completing this document: This is an important legal document known as an
GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE
 GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE By: Date of Birth: (Print Name) (Month/Day/Year) This advance directive for health care has four parts: PART ONE HEALTH CARE AGENT. This part allows you to choose
GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE By: Date of Birth: (Print Name) (Month/Day/Year) This advance directive for health care has four parts: PART ONE HEALTH CARE AGENT. This part allows you to choose
OREGON Advance Directive Planning for Important Healthcare Decisions
 OREGON Advance Directive Planning for Important Healthcare Decisions Caring Connections 1700 Diagonal Road, Suite 625, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
OREGON Advance Directive Planning for Important Healthcare Decisions Caring Connections 1700 Diagonal Road, Suite 625, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
Advance [Health Care] Directive
![Advance [Health Care] Directive](/thumbs/77/75352901.jpg "Advance [Health Care] Directive") Advance [Health Care] Directive Introduction I have completed this Advance Directive with much thought. This document gives my treatment choices and preferences, and/or appoints a Health Care Agent (also
Advance [Health Care] Directive Introduction I have completed this Advance Directive with much thought. This document gives my treatment choices and preferences, and/or appoints a Health Care Agent (also
MASSACHUSETTS ADVANCE DIRECTIVES
 MASSACHUSETTS ADVANCE DIRECTIVES Advance directives are legal documents that protect your right to refuse medical treatment you do not want, or to request treatment you do want, in the event you lose the
MASSACHUSETTS ADVANCE DIRECTIVES Advance directives are legal documents that protect your right to refuse medical treatment you do not want, or to request treatment you do want, in the event you lose the
GEORGIA S ADVANCE DIRECTIVE FOR HEALTH CARE
 GEORGIA S ADVANCE DIRECTIVE FOR HEALTH CARE The Georgia General Assembly has long recognized the right of individuals to control all aspects of their personal care and medical treatment, including the
GEORGIA S ADVANCE DIRECTIVE FOR HEALTH CARE The Georgia General Assembly has long recognized the right of individuals to control all aspects of their personal care and medical treatment, including the
Patient Self-Determination Act
 Holy Redeemer Hospital Patient Self-Determination Act NOTES:: MAKING YOUR OWN HEALTH CARE DECISIONS: As a competent adult, you have the fundamental right, in collaboration with your health care providers,
Holy Redeemer Hospital Patient Self-Determination Act NOTES:: MAKING YOUR OWN HEALTH CARE DECISIONS: As a competent adult, you have the fundamental right, in collaboration with your health care providers,
PENNSYLVANIA Advance Directive Planning for Important Healthcare Decisions
 PENNSYLVANIA Advance Directive Planning for Important Healthcare Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
PENNSYLVANIA Advance Directive Planning for Important Healthcare Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
Directive To Physicians and Family Or Surrogates (Living Will)
") Directive To Physicians and Family Or Surrogates (Living Will) INSTRUCTIONS FOR COMPLETING THIS DOCUMENT: This is an important legal document known as an Advance Directive. It is designed to help you communicate
Directive To Physicians and Family Or Surrogates (Living Will) INSTRUCTIONS FOR COMPLETING THIS DOCUMENT: This is an important legal document known as an Advance Directive. It is designed to help you communicate
Goals & Objectives 4/17/2014 UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES (AHCD) By Maureen Kroning, EdD, RN. Why would someone need to do this?
 By Maureen Kroning, EdD, RN. Why would someone need to do this?") UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES (AHCD) By Maureen Kroning, EdD, RN Goals & Objectives Participants will increase their knowledge about AHCD Review AHCD documents used at the hospital Role
UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES (AHCD) By Maureen Kroning, EdD, RN Goals & Objectives Participants will increase their knowledge about AHCD Review AHCD documents used at the hospital Role
Health Care Directive
 MINNESOTA PATIENT EDUCATION Health Care Directive Making Your Health Care Choices Known My Health Care Directive My health care directive was created to guide my health care agent and family, friends or
MINNESOTA PATIENT EDUCATION Health Care Directive Making Your Health Care Choices Known My Health Care Directive My health care directive was created to guide my health care agent and family, friends or
Vermont Advance Directive for Health Care
 Vermont Advance Directive for Health Care Prepared by the Vermont Ethics Network Explanation and Instructions You have the right to give instructions about what types of health care you want or do not
Vermont Advance Directive for Health Care Prepared by the Vermont Ethics Network Explanation and Instructions You have the right to give instructions about what types of health care you want or do not
TO HELP EASE DECISION MAKING IN THE FUTURE ADVANCE CARE PLANNING TOOLKIT
 TO HELP EASE DECISION MAKING IN THE FUTURE ADVANCE CARE PLANNING TOOLKIT Advance Care Planning Toolkit Your health care decisions are important. Providing Patient Centered Care is the guiding principle
TO HELP EASE DECISION MAKING IN THE FUTURE ADVANCE CARE PLANNING TOOLKIT Advance Care Planning Toolkit Your health care decisions are important. Providing Patient Centered Care is the guiding principle
OHIO Advance Directive Planning for Important Health Care Decisions
 OHIO Advance Directive Planning for Important Health Care Decisions Caring Info 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Info, a program of the National Organization
OHIO Advance Directive Planning for Important Health Care Decisions Caring Info 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Info, a program of the National Organization
NO TALLAHASSEE, June 30, Mental Health/Substance Abuse
 CFOP 155-52 STATE OF FLORIDA DEPARTMENT OF CF OPERATING PROCEDURE CHILDREN AND FAMILIES NO. 155-52 TALLAHASSEE, June 30, 2017 Mental Health/Substance Abuse USE OF DO NOT RESUSCITATE (DNR) ORDERS IN STATE
CFOP 155-52 STATE OF FLORIDA DEPARTMENT OF CF OPERATING PROCEDURE CHILDREN AND FAMILIES NO. 155-52 TALLAHASSEE, June 30, 2017 Mental Health/Substance Abuse USE OF DO NOT RESUSCITATE (DNR) ORDERS IN STATE
A Personal Decision. Illinois State Medical Society. Practical Information About Determining Your Future Medical Care.
 A Personal Decision 2016 EDITION Practical Information About Determining Your Future Medical Care Living wills Powers of attorney for health care Mental health treatment preference declarations Uniform
A Personal Decision 2016 EDITION Practical Information About Determining Your Future Medical Care Living wills Powers of attorney for health care Mental health treatment preference declarations Uniform
Advance Medical Directives
 Advance Medical Directives What Are Advance Medical Directives? These documents could be a living will or a durable power of attorney for health care (also called a health-care proxy). They allow you to
Advance Medical Directives What Are Advance Medical Directives? These documents could be a living will or a durable power of attorney for health care (also called a health-care proxy). They allow you to
Wyoming Advance Health Care Directive Form for:
 Wyoming Advance Health Care Directive Form for: (print your full name) Please place the completed document on the front of your refrigerator or another location where an emergency responder might easily
Wyoming Advance Health Care Directive Form for: (print your full name) Please place the completed document on the front of your refrigerator or another location where an emergency responder might easily
PHYSICIAN S GUIDELINES FOR WRITING DO NOT RESUSCITATE ORDERS
 PHYSICIAN S GUIDELINES FOR WRITING DO NOT RESUSCITATE ORDERS THE PURPOSE OF CPR IS THE PREVENTION OF SUDDEN UNEXPECTED DEATH. CPR IS NOT INDICATED IN CERTAIN SITUATIONS SUCH AS CASES OF TERMINAL IRREVERSIBLE
PHYSICIAN S GUIDELINES FOR WRITING DO NOT RESUSCITATE ORDERS THE PURPOSE OF CPR IS THE PREVENTION OF SUDDEN UNEXPECTED DEATH. CPR IS NOT INDICATED IN CERTAIN SITUATIONS SUCH AS CASES OF TERMINAL IRREVERSIBLE
LONG TERM SERVICES DIVISION DEPARTMENT OF HEALTH TECHNICAL ASSISTANCE GUIDELINES
 LONG TERM SERVICES DIVISION DEPARTMENT OF HEALTH TECHNICAL ASSISTANCE GUIDELINES TOPIC: GUIDELINES FOR COMMUNITY PROGRAMS, CASE MANAGERS, AND INTERDISCIPLINARY TEAM MEMBERS REGARDING ADVANCE DIRECTIVES
LONG TERM SERVICES DIVISION DEPARTMENT OF HEALTH TECHNICAL ASSISTANCE GUIDELINES TOPIC: GUIDELINES FOR COMMUNITY PROGRAMS, CASE MANAGERS, AND INTERDISCIPLINARY TEAM MEMBERS REGARDING ADVANCE DIRECTIVES
HEALTH CARE DIRECTIVE
 1 HEALTH CARE DIRECTIVE I,, understand this document allows me to do ONE OR BOTH of the following: PART I: Name another person (called the health care agent) to make health care decisions for me if I am
1 HEALTH CARE DIRECTIVE I,, understand this document allows me to do ONE OR BOTH of the following: PART I: Name another person (called the health care agent) to make health care decisions for me if I am
PLANNING YOUR HEALTH CARE IN ADVANCE
 STATE OF NEW YORK OFFICE OF THE ATTORNEY GENERAL PLANNING YOUR HEALTH CARE IN ADVANCE How to Make Your Wishes Known and Honored Attorney General Andrew M. Cuomo Acknowledgments This guide was researched
STATE OF NEW YORK OFFICE OF THE ATTORNEY GENERAL PLANNING YOUR HEALTH CARE IN ADVANCE How to Make Your Wishes Known and Honored Attorney General Andrew M. Cuomo Acknowledgments This guide was researched
PENNSYLVANIA Advance Directive Planning for Important Health Care Decisions
 PENNSYLVANIA Advance Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
PENNSYLVANIA Advance Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee
 Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee What is Advance Care Planning (ACP)? Understanding/clarifying
Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee What is Advance Care Planning (ACP)? Understanding/clarifying
Frequently Asked Questions and Forms
 1-877-209-8086 www.wvendoflife.org Advance Directives for Health Care Decision-Making in West Virginia Frequently Asked Questions and Forms FORMS INSIDE: Living Will - Medical Power of Attorney Combined
1-877-209-8086 www.wvendoflife.org Advance Directives for Health Care Decision-Making in West Virginia Frequently Asked Questions and Forms FORMS INSIDE: Living Will - Medical Power of Attorney Combined
COMMUNICATE YOUR HEALTH CARE WISHES. California Advance Health Care Directive Kit
 COMMUNICATE YOUR HEALTH CARE WISHES. California Advance Health Care Directive Kit CALIFORNIA ADVANCE HEALTH CARE DIRECTIVE Give your loved ones peace of mind; make your wishes known now. This form lets
COMMUNICATE YOUR HEALTH CARE WISHES. California Advance Health Care Directive Kit CALIFORNIA ADVANCE HEALTH CARE DIRECTIVE Give your loved ones peace of mind; make your wishes known now. This form lets
Planning Ahead: How to Make Future Health Care Decisions NOW. Washington
 Washington Planning Ahead: How to Make Future Health Care Decisions NOW Your Questions Answered About Washington Living Wills and Powers of Attorney for Health Care Table of Contents P 1 What You Need
Washington Planning Ahead: How to Make Future Health Care Decisions NOW Your Questions Answered About Washington Living Wills and Powers of Attorney for Health Care Table of Contents P 1 What You Need
Advance Directives. Important information on health care decision-making: You Have the Right to Decide
 Advance Directives Important information on health care decision-making: You Have the Right to Decide The documents provided in this package are being presented to you in accordance with the Federal Patient
Advance Directives Important information on health care decision-making: You Have the Right to Decide The documents provided in this package are being presented to you in accordance with the Federal Patient
Georgia Advance Directive for Health Care
 Georgia Advance Directive for Health Care By: (Print Name) Date of Birth: (Month/Day/Year) This advance directive for health care has four parts: PART ONE PART TWO PART THREE HEALTH CARE AGENT. This part
Georgia Advance Directive for Health Care By: (Print Name) Date of Birth: (Month/Day/Year) This advance directive for health care has four parts: PART ONE PART TWO PART THREE HEALTH CARE AGENT. This part
CHPCA appreciates and thanks our funding partner GlaxoSmithKline for their unrestricted funding support for Advance Care Planning in Canada.
 CHPCA appreciates and thanks our funding partner GlaxoSmithKline for their unrestricted funding support for Advance Care Planning in Canada. For more information about advance care planning, please visit
CHPCA appreciates and thanks our funding partner GlaxoSmithKline for their unrestricted funding support for Advance Care Planning in Canada. For more information about advance care planning, please visit
Advanced Care Planning Guide
 Advanced Care Planning Guide A process to think about, talk about and plan for life-threatening illness or end-of-life care New Hampshire Advance Directives: Durable Power of Attorney for Health Care (DPOAH)
Advanced Care Planning Guide A process to think about, talk about and plan for life-threatening illness or end-of-life care New Hampshire Advance Directives: Durable Power of Attorney for Health Care (DPOAH)
Ethical Issues: advance directives, nutrition and life support
 Ethical Issues: advance directives, nutrition and life support December 12, 2013 2013 LegalHealth Objectives Discuss parameters of consent for medical treatment and legal issues that arise Provide overview
Ethical Issues: advance directives, nutrition and life support December 12, 2013 2013 LegalHealth Objectives Discuss parameters of consent for medical treatment and legal issues that arise Provide overview
North Dakota: Advance Directive
 North Dakota: Advance Directive NOTE: This form is being provided to you as a public service. The attached forms are provided as is and are not the substitute for the advice of an attorney. By providing
North Dakota: Advance Directive NOTE: This form is being provided to you as a public service. The attached forms are provided as is and are not the substitute for the advice of an attorney. By providing
Directive to Physicians and Family or Surrogates
 Directive to Physicians and Family or Surrogates This is an important legal document, known as an Advance Directive. It is designed to help you communicate your wishes about medical treatment at some time
Directive to Physicians and Family or Surrogates This is an important legal document, known as an Advance Directive. It is designed to help you communicate your wishes about medical treatment at some time
MISSOURI HEALTH CARE DIRECTIVE AND DURABLE POWER OF ATTORNEY FOR HEALTH CARE SAMPLE. Jane Doe
 MISSOURI HEALTH CARE DIRECTIVE AND DURABLE POWER OF ATTORNEY FOR HEALTH CARE I. HEALTH CARE DIRECTIVE OF Jane Doe 1. I, Jane Doe, make this HEALTH CARE DIRECTIVE ( Directive ) to exercise my right to determine
MISSOURI HEALTH CARE DIRECTIVE AND DURABLE POWER OF ATTORNEY FOR HEALTH CARE I. HEALTH CARE DIRECTIVE OF Jane Doe 1. I, Jane Doe, make this HEALTH CARE DIRECTIVE ( Directive ) to exercise my right to determine
NEW HAMPSHIRE ADVANCE DIRECTIVE PAGE 4 OF 11 PART I: NEW HAMPSHIRE DURABLE POWER OF ATTORNEY FOR HEALTH CARE. I,, (name)
") NEW HAMPSHIRE ADVANCE DIRECTIVE PAGE 4 OF 11 PART I: NEW HAMPSHIRE DURABLE POWER OF ATTORNEY FOR HEALTH CARE PRINT YOUR NAME PRINT THE NAME AND ADDRESS OF YOUR AGENT I,, (name) hereby appoint (name of
NEW HAMPSHIRE ADVANCE DIRECTIVE PAGE 4 OF 11 PART I: NEW HAMPSHIRE DURABLE POWER OF ATTORNEY FOR HEALTH CARE PRINT YOUR NAME PRINT THE NAME AND ADDRESS OF YOUR AGENT I,, (name) hereby appoint (name of
ADVANCE DIRECTIVE Planning Guide. Information Provided as a Community Service
 ADVANCE DIRECTIVE Planning Guide Information Provided as a Community Service If a medical tragedy strikes, you have the RIGHT TO CHOOSE what medical care you do or do not want. It is best if you make this
ADVANCE DIRECTIVE Planning Guide Information Provided as a Community Service If a medical tragedy strikes, you have the RIGHT TO CHOOSE what medical care you do or do not want. It is best if you make this
Process
 www.theroyl.com Advance Directive And Durable Power Of Attorney Advance Medical Directive State of Virginia The Rest of Your Life recommends that you review completed documents with an attorney, especially
www.theroyl.com Advance Directive And Durable Power Of Attorney Advance Medical Directive State of Virginia The Rest of Your Life recommends that you review completed documents with an attorney, especially
My Wishes for Future Health Care
 My Wishes for Future Health Care Information Package Revised on 26 July 2010 Imagine that, without warning, you have developed a life-threatening illness and are in an intensive care unit of a hospital.
My Wishes for Future Health Care Information Package Revised on 26 July 2010 Imagine that, without warning, you have developed a life-threatening illness and are in an intensive care unit of a hospital.
Advance Directives. Planning Ahead For Your Healthcare
 Advance Directives Planning Ahead For Your Healthcare Core Values Catholic Health Initiatives core values of Reverence, Integrity, Compassion, and Excellence are the guiding principles that provide focus,
Advance Directives Planning Ahead For Your Healthcare Core Values Catholic Health Initiatives core values of Reverence, Integrity, Compassion, and Excellence are the guiding principles that provide focus,
Health Care Directive
 Health Care Directive Overview Adults with decision-making capacity have the right to make choices about their health care. No treatments may be given to someone who does not want them. The attached Durable
Health Care Directive Overview Adults with decision-making capacity have the right to make choices about their health care. No treatments may be given to someone who does not want them. The attached Durable
INSTRUCTION WORKSHEET
 INSTRUCTION WORKSHEET (add or delete as desired) Comfort Care Only means providing relief of pain and suffering in all cases, but not providing machines, devices, or medications that prolong my life in
INSTRUCTION WORKSHEET (add or delete as desired) Comfort Care Only means providing relief of pain and suffering in all cases, but not providing machines, devices, or medications that prolong my life in
HONORING CHOICES MN AND WI HEALTH CARE DIRECTIVE SOMALI
 *1628SO* EMMS Foundation: www.metrodoctors.com 612-362-3704 Revised August 2011 Magac Taariikh 1628 so REV 04/05/12 Advance Directives and Living Will ORIGINAL: Patient PHOTOCOPY: Medical Record Page 1
*1628SO* EMMS Foundation: www.metrodoctors.com 612-362-3704 Revised August 2011 Magac Taariikh 1628 so REV 04/05/12 Advance Directives and Living Will ORIGINAL: Patient PHOTOCOPY: Medical Record Page 1
Adult: Any person eighteen years of age or older, or emancipated minor.
 Advance Directives Policy and Procedure Purpose To provide an atmosphere of respect and caring and to ensure that each patient's ability and right to participate in medical decision making is maximized
Advance Directives Policy and Procedure Purpose To provide an atmosphere of respect and caring and to ensure that each patient's ability and right to participate in medical decision making is maximized
Advance Directives. Making your health care choices known if you can't speak for yourself.
 Advance Directives Making your health care choices known if you can't speak for yourself. ADVANCE DIRECTIVES Making your health care choices known if you can t speak for yourself This booklet contains
Advance Directives Making your health care choices known if you can't speak for yourself. ADVANCE DIRECTIVES Making your health care choices known if you can t speak for yourself This booklet contains