Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
|
|
|
- Barnard McCormick
- 6 years ago
- Views:
Transcription
1 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor
2 What does Transitional Care Include? Transitional Care is the smooth conversion of a patient from one care setting to another setting or to home. It involves patients moving from: Emergency Room to Hospital Observation Emergency Room to Hospital Inpatient Hospital Observation to Inpatient Inpatient to Skilled Care Inpatient to Sub-Acute Care Inpatient to Home Health Inpatient to Home Skilled Care to Acute Care Hospital Sub-Acute Care to Acute Care Sub-Acute Care to Home Skilled Care to Home
3 What is the impetus to do this right? Improved patient outcomes Appropriate patient placement Reduced length of stay Improved patient satisfaction Improved information flow between providers Financial dis-incentives Incomplete hand-offs of care are a patient safety issue
4 What needs to be done? Assure patients are in an appropriate level of care Identify high-risk patients on admission and target risk-specific interventions Assess patients ability to provide self-care post discharge Educate patients and families on post-acute care Coordinate post-discharge care Follow up on at-risk patients Communicate with post-discharge providers
5 Current Models BOOST - Better Outcomes for Older Adults through Safe Transitions Care Transitions Model Society for Hospital Medicine Care Transitions 4 Pillars Coleman Method STAAR - State Action on Avoidable Rehospitalizations IHI AHRQ Care Coordination Model - IHI CGH2H -Common Ground Hospital to Home SMART Signs, Medications, Appointments, Results, Talk Transitional Care Model (TCM) - Mary Naylor University of Pennsylvania GRACE Geriatric Resources for Assessment and Care of Elders Indiana University for Aging Research Guided Care Johns Hopkins University Bridge Program Illinois Transitional Care Consortium COMPASS Organized Medicine Provided Across a Seamless System

6 Midas+ Facets Preadmission Interventions Pre-discharge Interventions Post-discharge Interventions Outcome metrics
7 Pre-Admission Interventions Use of Midas+ Care Management in the Emergency Department
8 Reason for ED Case Management Emergency Department as primary care source Appropriate patient placement Identification of social issues that lead to overuse of the ED Lack of coordination with outpatient providers Providing alternatives to hospitalization
9 Identifying Frequent Users of Emergency Department Services Use Patient Explorer Patients with no identified PCP Patients with chronic Illness Patients with chronic pain Patients with drug-seeking behavior Patients with no insurance Patients with poor social support networks


10 Use a Midas+ Tracking File to track and plan for frequent ED users

11 Build a Worklist Rule to Notify ED Case Management of the Arrival of a Frequent Flier

12 Use a Midas+ Patient-level Focus Study to create a plan track for these frequent fliers.


13 Using Concurrent Review Concurrent Reviews can be done for ED patients for whom admission/observation is being considered.

14 Adding an HCM Review for patients who will not be admitted

15 Adding an HCM Review for Patients who will be admitted

16 Using Screening Criteria - Milliman
17 Using Screening Criteria - Milliman
18 Using Screening Criteria - Milliman

19 Using Screening Criteria - CERME

20 Use Criteria to assist with determining Observation vs. Acute Care Admissions

21 Using Screening Criteria - CERME
22 Tracking Actions and Alternatives to Hospital Admission Referral to Chronic Care Manager Referral to Primary Care Source Internal Clinics Community Clinics Homeless Shelters Prescriptions Transportation Home Health

23 Using the Emergency Department Module

24 Create User Fields for the ED Module
25 Pre-Discharge Interventions Use of Midas+ Hospital Case Management
26 General Goals for Hospital Case Management Reduction in LOS Reduction in readmissions Prevention of additional complications Patient transfer to an appropriate level of post-discharge care Increased patient satisfaction Increased patient/caregiver understanding and competence managing disease Prevention of post-discharge adverse outcomes Improvement in patient safety Improved communication between hospital and postdischarge providers
27 Specific Pre-discharge Strategies Assessment of patient for discharge risk Patient/family involvement care during stay Creation of an individualized discharge plan Teach-back Techniques Medication Reconciliation Discharge Case Manager/Planner Communication with post-discharge providers
28 Focus on Patients With chronic illnesses (physical and mental) With no PCP or Medical Home With no primary caregivers/complex social needs With limited cognitive abilities With targeted/high-risk conditions Acute Myocardial Infarction Pneumonia Congestive Heart Failure COPD Total Hip Replacement Total Knee Replacement
29 Midas+ Modules to Assist with Pre-discharge Assessments Hospital Case Management Concurrent Review Support Services Discharge Planning Encounter Subsystem Observation Module Registration Subsystem Medical History Medical History Problem List

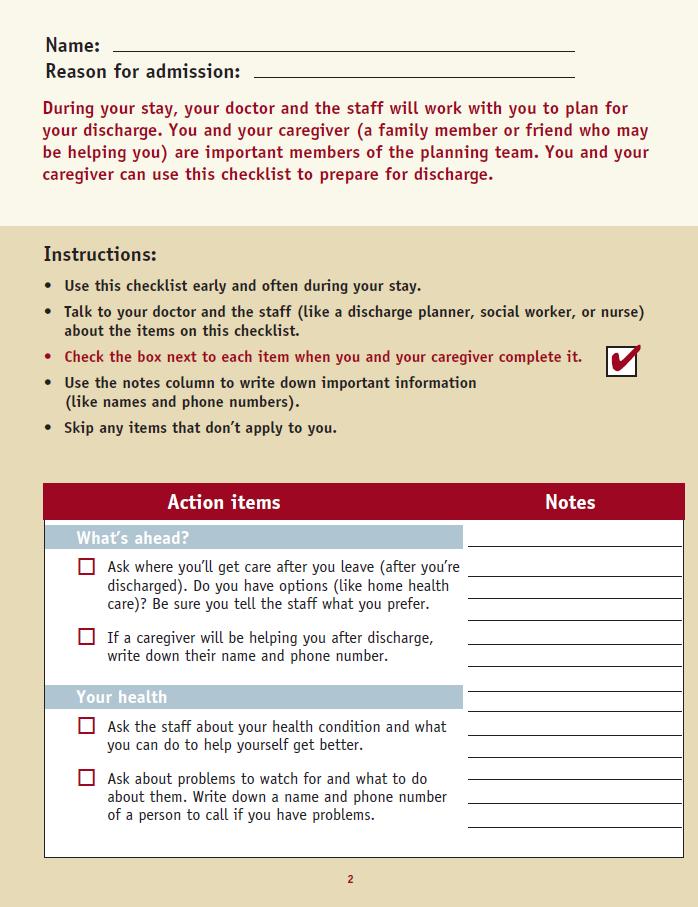
30 Patient Handout

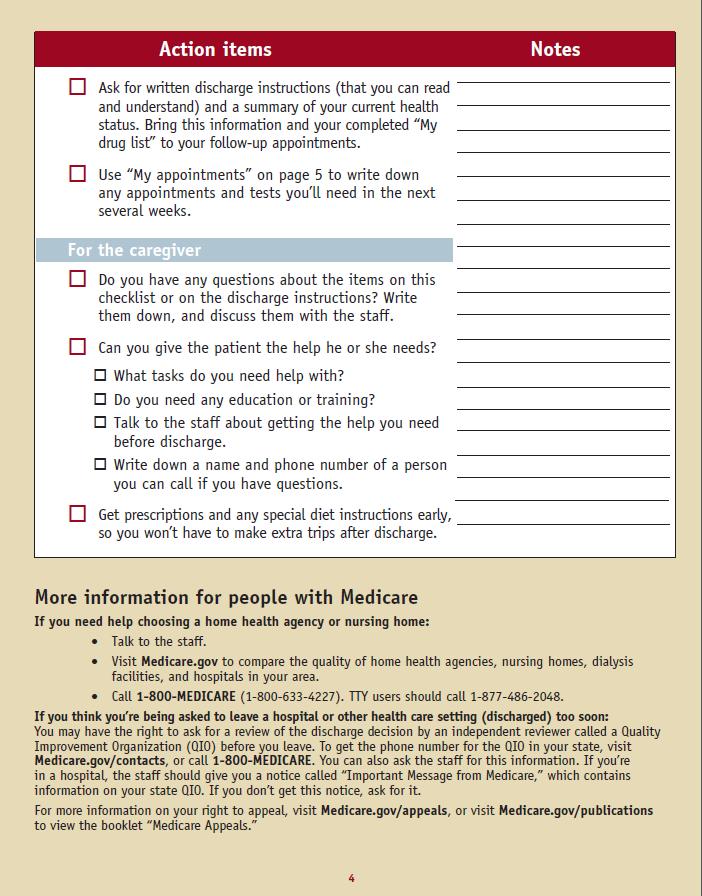
31 Patient Handout

32 Universal Patient Discharge Checklist
33 Coleman Model Four Pillars 1. Medication Self-management 2. Patient uses a Personal Health Record to facilitate communication and ensure continuity across providers and setting 3. Follow Up: Patient schedules and completes follow-up visit with PCP 4. Patient recognizes red flags about worsening conditions and understands how to respond



34 Proven Successes: Teach-back Technique

35 Teach-back Techniques
36 Patient Pass (BOOST)

37 BOOST Patient Pass
38 BOOST Patient Pass as ReporTrack Document
39 Referrals HCM to a Transitional Care Coach FROM: Concurrent Review Support Services Discharge Planning Medical History

40 Referrals to TCC: Concurrent Review Use Concurrent Review to Identify Targeted Readmission Diagnoses

41 Using Support Services to Generate Follow-up

42 Using Discharge Planning to Generate Follow-up with Transitional Care Manager
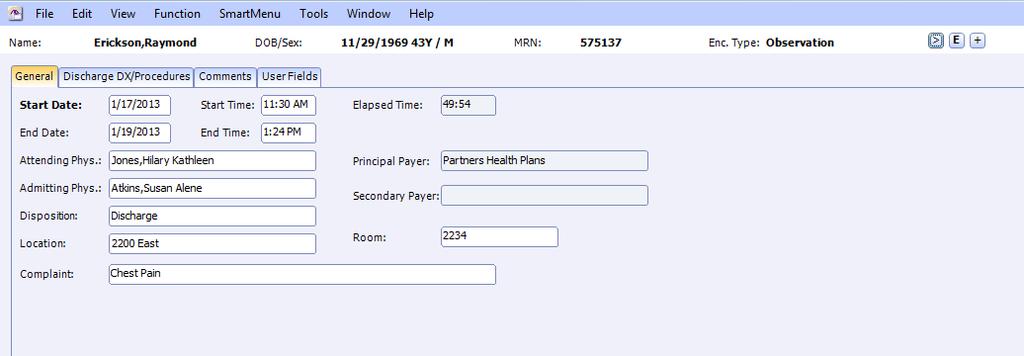
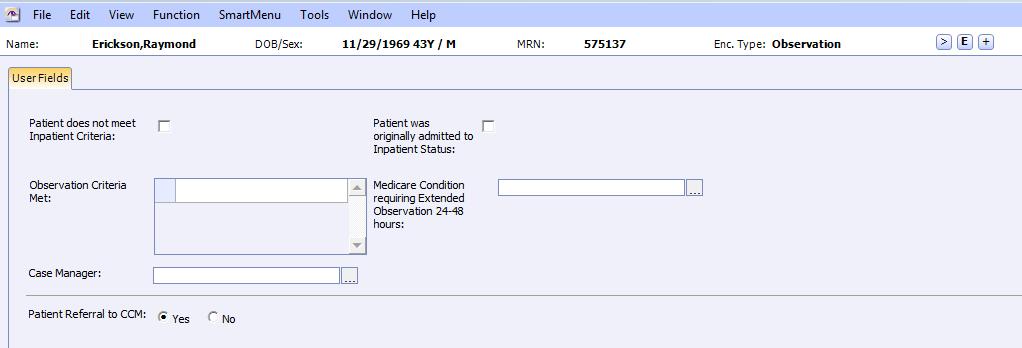
43 Observation Module

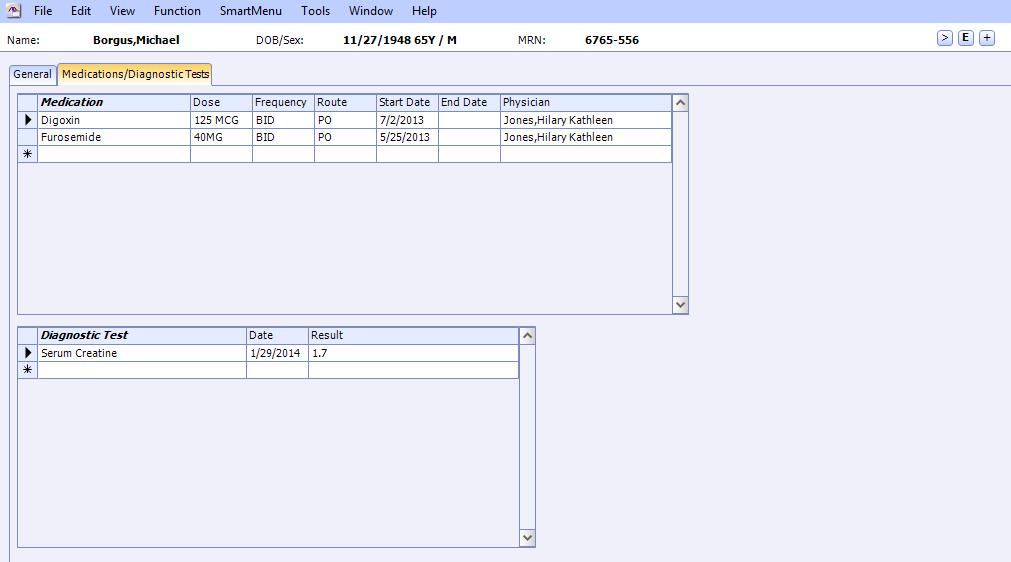
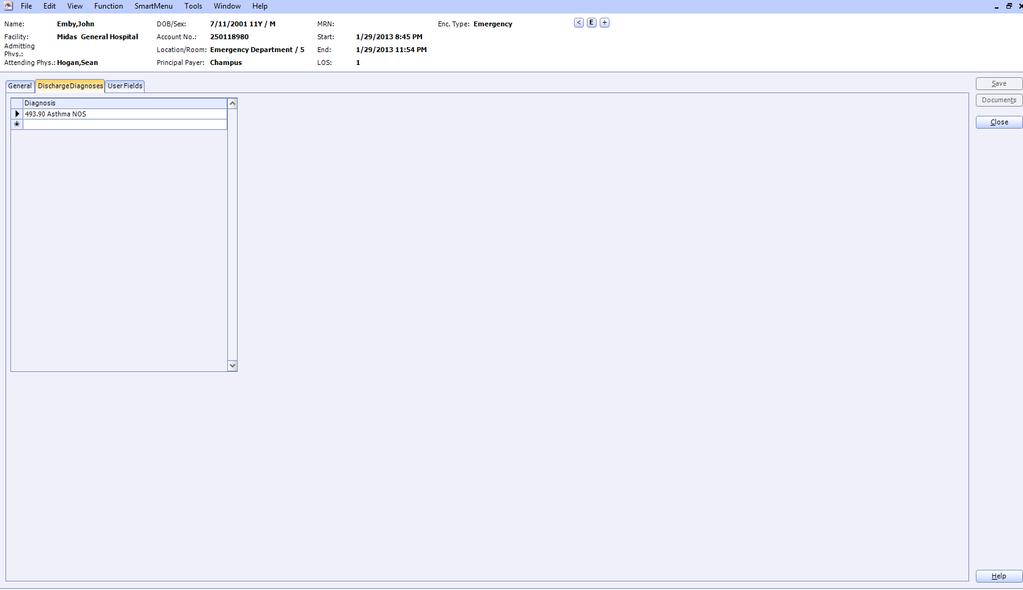
44 Medical History

45 Medical History Problem List

46 Medical History User Fields
47 Coordination with Postdischarge Providers



48 Four Launch Points from Midas+ Concurrent Review Certification Entry Discharge Planning Support Services
49 Curaspan

50 Curaspan and Midas+ Leading provider of patient transition solutions Leading provider of care performance software 10+ year partnership Nearly 350 shared customers



51 Curaspan Powers Care Transitions Care Transition: The movement of a patient from one setting of care to another. 15 years leading the industry Post-Acute Providers 15% of all acute discharge in the US move across our network Patients Discharged Home Transport Agencies 6 million discharges per year Physicians Payers
52 Automate. Collaborate. Optimize. EMR DischargeCentral ReferralCentral Clinical Info Case Manager Referral Packet Intake Coordinator Streamline and automate manual, administrative tasks Easily identify qualified post-acute care providers Securely share clinical information in real-time Gather key metrics on internal hospital processes and external provider performances

53 Save Time with Pre-populated Forms
54 Search for Available and Qualified Providers

55 Share Detailed Provider Profiles

56 Send Referral Packets to Multiple Providers Simultaneously
57 View All Referral Activity in One Place

58 Communicate with Providers Securely
59 Notify All Providers When Referral is Booked


60 Involve Other Members of the Care Continuum

61 Automate. Collaborate. Optimize. EMR ReviewCentral Payer Nurse Clinical Info Utilization Manager Review Reviewer Standardized workflow Secure, time-and-date-stamped communications Real-time workflow reminders Comprehensive reporting Improve internal communication with internal notebook and work lists

62 View All Relevant Patient Information in a Single Place

63 Create and Submit All Forms and Documents Electronically

64 Monitor Submission Status

65 Document and Track Approvals and Denials

66 Track Approved Days

67 Access Robust Transaction Audit Trail

68 Store and Access Documentation of Successful Communication

69 Organize and Prioritize Cases

70 Integration Overview The following data elements would be available for reporting: Referral Data & Time Provider(s) Referral Referral Type Referrer Case Worker Referral Status Provider Status Level of Care & Service Bed Type Anticipated Start Date Actual Start Date Discharge Status Booked provider Discharge Delay Reason Payer Authorization Numbers Number of Days Authorized Share information with clinical and utilization review team members in real time Reduce redundant tasks and eliminate duplicate documentation Access shared data for more complete reporting
71 Reporting Executive Leadership Reports LOS Savings LOS Comparison Days Saved for Facility Placements Provider Scorecard (summary) Referrals In/Out of Network (summary) Compliance Reports Home Care Start of Care Discharge Disposition Discrepancies Early Warning - Referral- Pattern Changes Post-Discharge Release of Information PASRR Completion Care Management Reports Readmissions by: Placement Diagnosis Provider Physician New Placement vs. Returns Referral Process Timeline Barrier Days Case Manager Referrals Decline Reasons Delay Reasons Payer Bookings Operations Reports Placement Cycle Times Referrals In/Out Network (detail) Total Discharges LOS Variance LOS Quarterly Comparison Provider Scorecard (detailed) Unit Statistics Inpatient Length of Stay One-Day Stay



72 Readmission Dashboard Pivot By Provider Date Range Patient Age Diagnosis Payer Physician Provider Patient Age Physician Diagnosis Payer Date Range

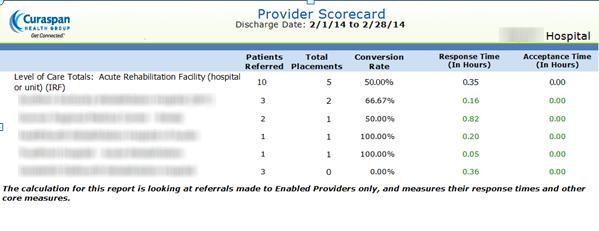
73 Insight Into Provider Performance


74 Insight Into Internal Processes

75 Information At-a-Glance

76 Services Before Implementation Consultative sales process Cross-departmental interviews Access to dedicated clinical, technical and security subject matter experts at Curaspan Sharing of best practices During Implementation Clinical workflow analysis and redesign Project management Manage implementation schedule Identify and overcome roadblocks Oversee technology On-site training Network Development Identify top providers in community Educate providers on new workflows Update provider service profiles After Implementation Regular account check-ins Data analysis Best practices Utilization review Ongoing monitoring of provider utilization Training & Education Computer-based training Regularly scheduled webinars Monthly product and regulatory updates Customer Support Representatives available via phone &
77 Post-discharge Interventions

78 Referrals from Inpatient Discharges Based on the Midas+ modules used from Hospital Case Management, worklist referral to any post-discharge Transitional Care Manager should be set up to be automatic. Referral from Support Services Referral from Concurrent Review Referral from DCP User Fields
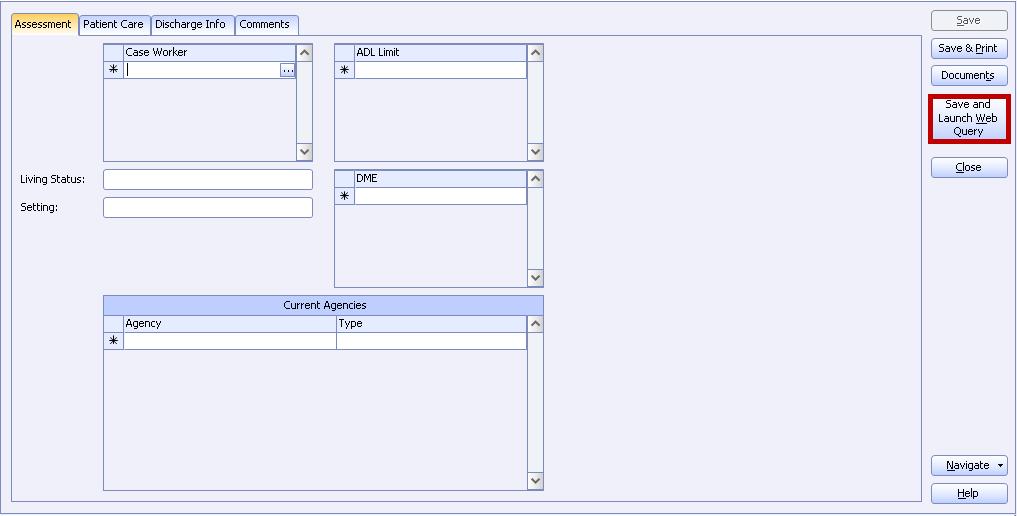
79 Information Flow from Discharge Planning to CCM Episode Site Parameter Transfers data from HCM Discharge Planning Assessment Tab DME Tab Patient Care Tab

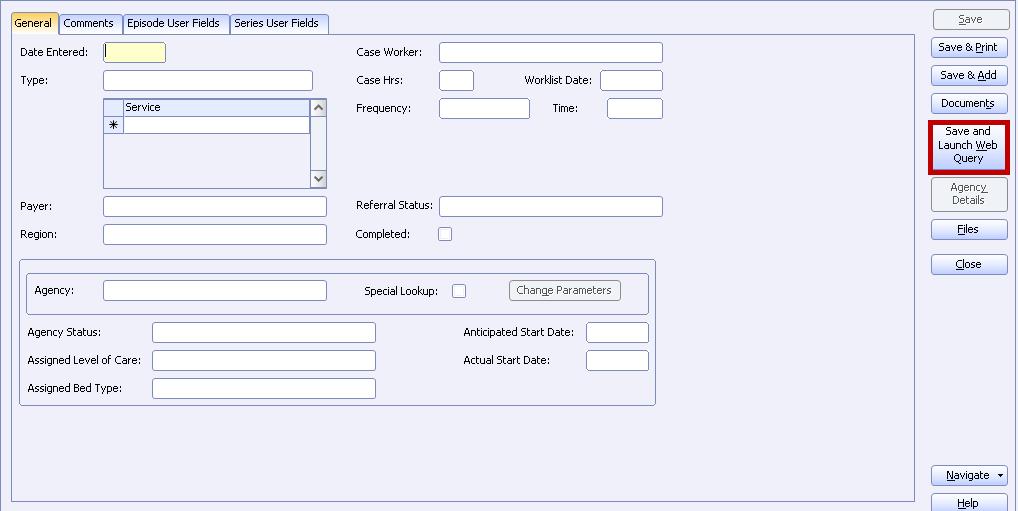
80 Using CCM to Continue Postdischarge Follow-up: Episode Entry

81 Using CCM to Continue Postdischarge Follow-up: Assessments

82 Using CCM to Continue Postdischarge Follow-up: Problem List

83 Using CCM to Continue Post-discharge Follow-up: Referrals and Interventions
84 Evidence-based Models of Transitional Care Care Transitions Intervention (CTI) Transitional Care Model (TCM) Better Outcomes for Older Adults through Safe Transitions (BOOST) The Bridge Model Guided Care Geriatric Resources for Assessment and Care of Elders (GRACE) Project RED (Re-Engineered Discharge) Joint Commission Hot Topics in Health Care: Transitions of Care June 2012
85 Common Elements of Transitional Care Models Multidisciplinary communication, collaboration, and coordination from admission through transition Must include patient and caregivers Care Team includes physician, nurse, pharmacist, social worker Includes active daily patient teaching Includes self-management of medications Joint Commission Hot Topics in Health Care: Transitions of Care June 2012
86 Common Elements of Transitional Care Models Clinician involvement and shared accountability during all points of transition Includes both sending and receiving clinicians Care Coordinator is identified There is a written exchange of information as well as verbal Joint Commission Hot Topics in Health Care: Transitions of Care June 2012
87 Common Elements of Transitional Care Models There is comprehensive planning and risk assessment throughout the hospital stay Discharge Planning begins at admission Patients are assessed during their stay for risk factors that limit self care including: Low literacy Multiple Chronic Conditions Poly-pharmacy Poor self-health ratings Joint Commission Hot Topics in Health Care: Transitions of Care June 2012
88 Common Elements of Transitional Care Models Standardized transition plans, procedures, and forms Written plans and Discharge Summaries include: Active Issues Diagnoses Medications Needed Services Warning signs of worsening condition Whom to contact 24/7 in case of emergency Joint Commission Hot Topics in Health Care: Transitions of Care June 2012
89 Common Elements of Transitional Care Models Timely follow-up, support, and coordination Telephone or in-person follow-up, support, and coordination Performed by Case Manager, Social Worker, nurse, or other health care provider Provided within 48 hours after discharge Patients have a 24/7 number to call for information, reassurance, and advice Joint Commission Hot Topics in Health Care: Transitions of Care June 2012

90 Community Coordination
91 Community Coordination Center For Pathways Community Care Coordination Rockville Institute for the Advancement of Social Science (transitioned from AHRQ) Community care coordination is the process of Identifying and engaging individuals within their community home setting Assessing their health and social needs Connecting them to the health and/or social services they need
92 Outcome Metrics
93 Outcome Metrics LOS RSRRs HWRR Returns to ED % ED patients admitted % Total Inpatients admitted via ED Tracking Readmissions from sub-acute providers Assessing Quality of Interventions outcomes Discharged pts. with ED visit within 10 days
94 Outcome Metrics Available in DataVision HCAPS CDBR:1251 HBIPS Readmission measures CMS Readmissions Reduction Program Indicators Facility Profile Readmission Measures

95 Outcome Metrics
96 References Joint Commission Hot Topics in Health Care: Transitions of Care June 2012 Rockville Institute for the Advancement of Social Science Center for Pathways Community Care Coordination Decreasing Avoidable Hospital Admissions With the Implementation of an Emergency Department Case Management Program Ghazala Q. Sharieff, MD, MBA, et al; American Journal of Medical Quality XX(X) by the American College of Medical Quality Best Practices: Case Management in the Emergency Department; Washington State Hospital Association; June 2012 Hospital-Initiated Transitional Care Interventions as a Patient Safety Strategy: A Systematic Review: Stephanie Rennke, MD, et al Ann Intern Med. 2013;158(5_Part_2): BOOSTing Care Transitions; Society for hospital Medicine; project_boost_background.cfm
97 Thanks for attending. Are there any questions? Barb Craig, Midas+ SaaS Advisor
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Exploring the Possibilities with MIDAS+ SmartConnect
 June 1 3, 2009 Westin La Paloma Resort Tucson, Arizona Exploring the Possibilities with MIDAS+ SmartConnect Leverage your existing MIDAS+ Care Management tools and consider automating your transition planning
June 1 3, 2009 Westin La Paloma Resort Tucson, Arizona Exploring the Possibilities with MIDAS+ SmartConnect Leverage your existing MIDAS+ Care Management tools and consider automating your transition planning
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Connecting Care Across the Continuum
 Connecting Care Across the Continuum A Guide for Providers > Discharging patients should be quick, easy, and painless for everyone including patients, families and the hospital. That s why a hospital that
Connecting Care Across the Continuum A Guide for Providers > Discharging patients should be quick, easy, and painless for everyone including patients, families and the hospital. That s why a hospital that
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014
 USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: High utilizer patients often get a full work-up every time
USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: High utilizer patients often get a full work-up every time
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Best Practices: Access Case Management
 Best Practices: Access Case Management Sarah M. Clark, RN-BC, BSN, MHA/INF, CCM Manager, Care Coordination Education Sentara Healthcare August 15, 2013 1 Objectives Identify key components of an effective
Best Practices: Access Case Management Sarah M. Clark, RN-BC, BSN, MHA/INF, CCM Manager, Care Coordination Education Sentara Healthcare August 15, 2013 1 Objectives Identify key components of an effective
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Park at Allens Creek Suite Allens Creek Road Rochester, NY 14618
 The Park at Allens Creek Suite 100 132 Allens Creek Road Rochester, NY 14618 Phone: (585) 473-7573 Fax: (585) 473-7641 www.mcms.org mcms@mcms.org Monroe County Medical Society Quality Collaborative Community
The Park at Allens Creek Suite 100 132 Allens Creek Road Rochester, NY 14618 Phone: (585) 473-7573 Fax: (585) 473-7641 www.mcms.org mcms@mcms.org Monroe County Medical Society Quality Collaborative Community
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Creating Care Pathways Committees
 Presentation Creating Care Title Pathways Committees December 12, 2012 December 12, 2012 Creating Care Pathways Committees LeadingAge Indiana Integrated Care & Payment Executive Series 1 2012 Health Dimensions
Presentation Creating Care Title Pathways Committees December 12, 2012 December 12, 2012 Creating Care Pathways Committees LeadingAge Indiana Integrated Care & Payment Executive Series 1 2012 Health Dimensions
Safe Transitions: From Patient Centered Care to Patient Directed Care
 Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Transition from Hospital to Home: Importance of Medication Education and Reconciliation
 Transition from Hospital to Home: Importance of Medication Education and Reconciliation Julie Baron, PharmD, CGP, BCACP/Clinical Pharmacy Specialist/Kaiser Permanente Lindsay Salsburg, PharmD, BCACP/Clinical
Transition from Hospital to Home: Importance of Medication Education and Reconciliation Julie Baron, PharmD, CGP, BCACP/Clinical Pharmacy Specialist/Kaiser Permanente Lindsay Salsburg, PharmD, BCACP/Clinical
improvement program to Electronic Health variety of reasons, experts suggest that up to
 Reducing Hospital Readmissions March/2017 The readmission rate for patients discharged to a skilled nursing facility is 25% within 30 days1. What can senior care providers do to reduce these hospital readmissions?
Reducing Hospital Readmissions March/2017 The readmission rate for patients discharged to a skilled nursing facility is 25% within 30 days1. What can senior care providers do to reduce these hospital readmissions?
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Patient Activation Using Technology- Supported Navigators
 Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Medication Reconciliation: Looking Forward
 Medication Reconciliation: Looking Forward Bruce Lambert, Ph.D. Associate Professor Department of Pharmacy Administration University of Illinois at Chicago 833 S. Wood St. (MC 871) Chicago, IL 60612-7231
Medication Reconciliation: Looking Forward Bruce Lambert, Ph.D. Associate Professor Department of Pharmacy Administration University of Illinois at Chicago 833 S. Wood St. (MC 871) Chicago, IL 60612-7231
IMPROVING MEDICATION RECONCILIATION WITH STANDARDS
 Presented by NCPDP and HIMSS for the Pharmacy Informatics Community IMPROVING MEDICATION RECONCILIATION WITH STANDARDS December 13, 2012 Keith Shuster, Manager, Acute Pharmacy Services, Norwalk Hospital
Presented by NCPDP and HIMSS for the Pharmacy Informatics Community IMPROVING MEDICATION RECONCILIATION WITH STANDARDS December 13, 2012 Keith Shuster, Manager, Acute Pharmacy Services, Norwalk Hospital
Get A Seat at the Table
 Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Learning Objectives. Federal Regulations. Upcoming Concerns. Discharge Planning & Follow up with Residents, Family, Team and Community Providers
 Discharge Planning & Follow up with Residents, Family, Team and Community Providers Elise Beaulieu, MSW, LICSW April 17, 2013 Learning Objectives O Understand the overall concepts of discharge planning
Discharge Planning & Follow up with Residents, Family, Team and Community Providers Elise Beaulieu, MSW, LICSW April 17, 2013 Learning Objectives O Understand the overall concepts of discharge planning
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
2017 Edition. MIPS Guide. The rule is in and Medicare physician payments are changing. What does that mean for you?
 2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
EMERGENCY DEPARTMENT CASE MANAGEMENT
 EMERGENCY DEPARTMENT CASE MANAGEMENT By Linda Sallee, Haley Rhodes, Sapna Patel, Cathleen Trespasz Healthcare consumers are becoming more empowered to have healthcare on their terms. With telemedicine,
EMERGENCY DEPARTMENT CASE MANAGEMENT By Linda Sallee, Haley Rhodes, Sapna Patel, Cathleen Trespasz Healthcare consumers are becoming more empowered to have healthcare on their terms. With telemedicine,
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Accountable Care Atlas
 Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
The Changing Landscape: A Confluence of National Attention. Eric A. Coleman, MD, MPH
 Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
PASRR: Partnering with Hospitals in Meeting Patient s Needs
 PASRR: Partnering with Hospitals in Meeting Patient s Needs PASRR Technical Assistance Center February 14, 2012 90 minutes Presenter: Jackie Birmingham, RN, BSN, MS, CMAC Agenda Introduction why PASRR
PASRR: Partnering with Hospitals in Meeting Patient s Needs PASRR Technical Assistance Center February 14, 2012 90 minutes Presenter: Jackie Birmingham, RN, BSN, MS, CMAC Agenda Introduction why PASRR
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Quality, Cost and Business Intelligence in Healthcare
 Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Karen Stasium, BS, MPT, COS C, HCS D
 Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
CHRONIC CARE MANAGEMENT. A Guide to Medicare s New Move Toward Patient-Centric Care
 CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Priceless Partners: Common Patients, Common Goals
 Priceless Partners: Common Patients, Common Goals Erin Hodson, RN, BSN, ACM Senior Director Case Management Inova Fairfax Hospital Pamela Andrews, RN, MSW, MBA, CCM, ACM Director Medical Management INTotal
Priceless Partners: Common Patients, Common Goals Erin Hodson, RN, BSN, ACM Senior Director Case Management Inova Fairfax Hospital Pamela Andrews, RN, MSW, MBA, CCM, ACM Director Medical Management INTotal
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
Involving Patients and Families to Improve Care Transitions
 Involving Patients and Families to Improve Care Transitions Julius Yang, MD, PhD Director of Inpatient Quality Sarah Moravick, MBA QI Project Manager 1 Overview of Today s Discussion 1. BIDMC s burning
Involving Patients and Families to Improve Care Transitions Julius Yang, MD, PhD Director of Inpatient Quality Sarah Moravick, MBA QI Project Manager 1 Overview of Today s Discussion 1. BIDMC s burning
Solution Title: Meeting the Challenge of Health Care Change
 Organization: Western Maryland Health System Solution Title: Meeting the Challenge of Health Care Change Program/Project Description, including Goals: What was the problem to be solved? How was it identified?
Organization: Western Maryland Health System Solution Title: Meeting the Challenge of Health Care Change Program/Project Description, including Goals: What was the problem to be solved? How was it identified?
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Medical Home as a Platform for Population Health
 Medical Home as a Platform for Population Health Population Health Colloquium March 8, 2016 Emily Brower Vice President, Population Health Atrius Health Emily_Brower@atriushealth.org 2016 Atrius Health,
Medical Home as a Platform for Population Health Population Health Colloquium March 8, 2016 Emily Brower Vice President, Population Health Atrius Health Emily_Brower@atriushealth.org 2016 Atrius Health,
Home Assessments Resulting in a Positive Effect on Outcome Score Cards
 Home Assessments Resulting in a Positive Effect on Outcome Score Cards Presented by: Angela Benson, OTR/L, Clinical Specialist *graduated from Mount Aloysius College, Cresson, PA *9 years of experience
Home Assessments Resulting in a Positive Effect on Outcome Score Cards Presented by: Angela Benson, OTR/L, Clinical Specialist *graduated from Mount Aloysius College, Cresson, PA *9 years of experience
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Care Transitions Partnerships that Work for Patients
 Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Telecare Services 7/19/2017
 Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
Project Description: Page Memorial Hospital (PMH) identified a need for patient care coordination and continuity for post discharge care.
 identified a need for patient care coordination and continuity for post discharge care.") Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016
 Narrative for Health Care Organizations in Ontario 3/15/2016") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions
Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions