Chinwe Nwosu, GE/NMF Scholar Supervisor: Dr. Stephen Ttendo, Senior Lecturer/ Head of Department of Anesthesia
|
|
|
- Marilyn Whitehead
- 5 years ago
- Views:
Transcription


1 Chinwe Nwosu, GE/NMF Scholar Supervisor: Dr. Stephen Ttendo, Senior Lecturer/ Head of Department of Anesthesia
2 According to the Uganda Ministry of Health 2010 Clinical Guidelines Read the notes/ medical records of the patient Obtain a standard history and PE Explain the procedure to the patient and ensure understanding Ensure informed consent form is signed Obtain pt weight and baseline vitals Check site and side of the operation Check period of fasting Monitor, record every 5 min. or more frequently, BP, Pulse, Respiration, Colour, oxmetry
3 After anesthesia ensure that the patient recovers from effects of anesthesia Has stable vital signs Is returned to the ward in the fully conscious state, no worse, or if at all possible, even better than before operation.
4 According to the American Society of Anesthesiologists Guidelines Review available medical record, interview and perform focused PE Ensure consent has been obtained Document in the chart that the above has been performed Monitor the patient s oxygenation, ventilation, circulation and temperature at least every 5 minutes for all anesthetics Record the pertinent events of the procedure
5 After anesthesia Conduct a postanesthesia evaluation, assessing patients for sequelae from anesthetic interventions and arranging for appropriate follow-up. Ensure availability of nursing personnel and equipment as required for safe postanesthetic care Ensure transfer of care information pertinent to the patient s specific needs and ensuring a safe transition Remain with the patient as long as medically necessary and until the receiving health care provider has all the information needed to assume care
6 To assess the perioperative care delivered to surgical patients at Mbarara Regional Referral Hospital (MRRH). To explore the opinions of hospital staff on the quality of perioperative care at MRRH To discover the discrepancies between the opinion of staff and the actual care provided to surgical patients at MRRH To determine the barriers to improving certain aspects of perioperative care at MRRH.
7 Patient file review conducted at Mbarara Regional Referral Hospital A sample of surgical cases conducted between the months February, March, and April was provided 78 patient files were randomly selected Data collected using Microsoft Excel
8 Two questionnaires were administered: 1. To anesthesia staff: exploring the staff s assessment of pre- and intraoperative care Questions regarding preoperative assessment, intraoperative monitoring and documentation, barriers to adequate documentation, etc. N = 9 2. To surgical and nursing staff: exploring the hospital staff s assessment of postoperative care Questions regarding postoperative medication delivery and documentation, barriers to proper postoperative care, etc N = 15
9 RESULTS: Component 1

10

11

12
13

14


15 Surgical Pre-Op? Anesthesia Pre-Op?

16 Adequate intraoperative monitors: According to Ministry of Health 2010 Uganda Clinical Guidelines: 0% of cases According to ASA standards: 0% of cases WHO surgical safety checklist utilized: 0% of cases Post-extubation condition documented: 12.8% of cases (n=10)


17 Immediate Post-Op Vitals? Daily Post-Op Vitals?

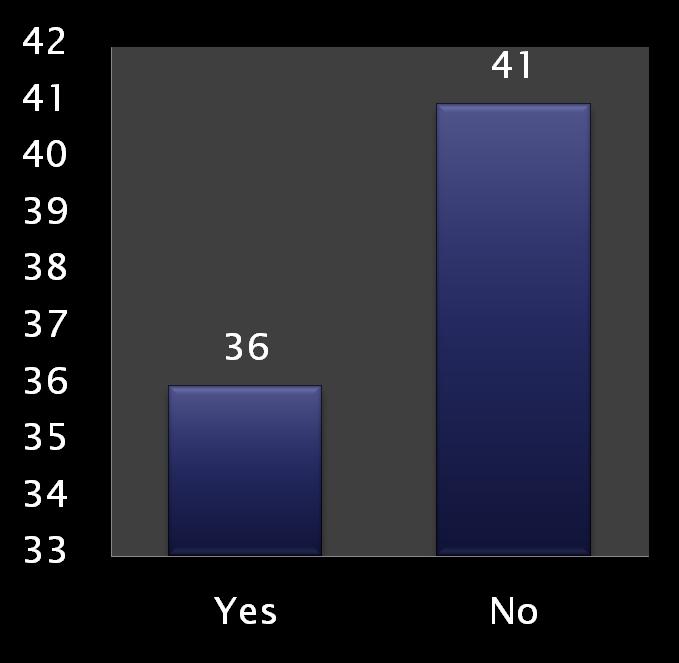
18 Pain medications given as directed? Other medications given as directed?
19 RESULTS: Component 2

20 Are you familiar with the World Health Organization (WHO) surgical safety checklist? Yes 88.9% No 11.1% How often do you think that the WHO surgical safety checklist is used in the MRRH surgical operating theater? In less than 10% of the cases 44.4% 10-25% of the cases 11.1% 26-50% of the cases 22.2% 51-75% of the cases 22.2% In more than 75% of the cases 0%
21 How often do you think that patients preoperative evaluations are documented? In less than 10% of the cases 0% 10-25% of the cases 11.1% 26-50% of the cases 33.3% 51-75% of the cases 33.3% In more than 75% of the cases 22.2%
22 The following are basic standards of monitoring for all patients receiving anesthetics Blood pressure 88.9% Heart rate 100% EKG/ECG 88.9% Temperature 66.7% Inspired/Expired Gases 55.6% SpO 2 100%
23 How often do you think that all necessary parameters are monitored at the MRRH surgical operating theater? In less than 10% of the cases 0% 10-25% of the cases 0% 26-50% of the cases 0% 51-75% of the cases 55.6% In more than 75% of the cases 44.4%
24 What are the barriers to proper intraoperative documentation? Lack of time 22.2% Unfamiliarity with the anesthesia monitoring machine 0% Anesthesia record is difficult to understand 0% Unfamiliarity with the standards of monitoring (i.e. I am not certain which parameters are important to record) 0% Lack of supervision/instruction to staff in training 22.2% Other (please explain):77.8 % none, laziness, underestimation of importance and need for proper documentation, poor attitude of staff, ppl fired/resigned but have no way out, documentation paper out of stock

25 How often do you think that patients vitals are monitored immediately post-operation after returning from the surgical operating theater? In less than 10% of the cases 40% 10-25% of the cases 20% 26-50% of the cases 26.7% 51-75% of the cases 13.3% In more than 75% of the cases 0%
26 How often do you think that patients pain medications are given as directed postoperatively? In less than 10% of the cases 20% 10-25% of the cases 20% 26-50% of the cases 20% 51-75% of the cases 33.3% In more than 75% of the cases 6.7%
27 How often do you think that patients other medications (i.e. antibiotics) are given as directed postoperatively? In less than 10% of the cases 0% 10-25% of the cases 0% 26-50% of the cases 33.3% 51-75% of the cases 60% In more than 75% of the cases 6.7%
28 What are barriers to proper postoperative management and monitoring, including proper medications, vitals monitoring, fluids, etc (circle all that apply)? Lack of supplies 86.7% Which supplies? _Abx, analgesics, preps/dressings, BP cuffs, thermometers, pulse oximeters, IV fluids, oxygen, sundries Lack of properly trained staff 26.7% Lack of time 33.3% Lack of supervision/instruction to staff in training 53.3% Inadequate communication between surgical/anesthesia/nursing staff 53.3% Unfamiliarity with standard postoperative treatment recommendations 73.3% Other (please specify) : 46.7% _understaffing, lack of motivation,/incentive/seriousness, staff over-worked, nurses uncomfortable giving opioids
29 What are barriers to administering medication as prescribed postoperatively (circle all that apply)? Lack of properly trained staff 33.3% Lack of time 33.3% Difficulty locating patient s file 26.7% Inadequate communication between surgical/anesthesia/nursing staff 46.7% Lack of supervision/instruction to staff in training 40% Other (please specify): 40% lack of staff/standards of operating procedure/staff/devotion to job, poor attitude towards pt care
30 What are the barriers to proper medical documentation, including recording patient s vitals, medication charting, etc (circle all that apply)? Lack of properly trained staff 26.7% Lack of time 46.7% Difficulty locating patient s file 26.7% Inadequate communication between surgical/anesthesia/nursing staff 60% Lack of supervision/instruction to staff in training 53.3% Other (please specify): 40% work system, attitude, lack of seriousness/staff/morale, no accountability in case of errors, laziness

31 N % Surgery preoperative assessment completed Anesthesia preoperative assessment completed Adequate intraoperative monitoring 0 0 WHO surgical safety checklist utilized 0 0 Post-extubation status recorded Postoperative vitals recorded Daily vitals recorded 1 1 Pain medicine given as directed Other medications given as directed 36 47
32 Actual Response Pre-Op Evaluation Anesthesia - 65% Surgery- 92 % Avg percentage -78.8% WHO Surgical Checklist Utilized <10% of the cases 0% 10-25% of the cases 11.1% 26-50% of the cases 33.3% 51-75% of the cases 33.3% >75% of the cases-22.2% 0 % <10% of the cases-44.4% 10-25% of the cases 11.1% 26-50% of the cases 22.2% 51-75% of the cases 22.2% >75% of the cases 0%
33 Actual Response Necessary Intraoperative Monitors 0 % <10% of the cases 0% 10-25% of the cases 0% 26-50% of the cases 0% 51-75% of the cases 55.6% In more than 75% of the cases 44.4% Immediate Post-Op Vitals 14% <10% of the cases 40% 10-25% of the cases 20% 26-50% of the cases 26.7% 51-75% of the cases 13.3% > 75% of the cases 0%
34 Actual Response Pain Medications Given 17 % <10% of the cases 20% 10-25% of the cases - 20% 26-50% of the cases 20% 51-75% of the cases 33.3% >75% of the cases 6.7% Other Medications Given 47% <10% of the cases 0% 10-25% of the cases 0% 26-50% of the cases- 33.3% 51-75% of the cases 60% >75% of the cases 6.7%
35 Document everything in ALL surgical and anesthetic procedures Reorganize intraoperative anesthesia record to fit standards recommended by the Uganda Ministry of Health or the ASA Stress the importance of proper documentation to staff at every level of training Improve upon the perioperative communication between surgical, anesthesia, and nursing staff
36 This sample selection contained a significant amount of surgeries from 1 month and could have skewed the results towards either direction Standards of perioperative care adopted at MRRH are not clear, making it difficult to compare the practice at MRRH to standards stated
37 Dr. Stephen Ttendo Manfred Amanya Anesthesia, surgical, and nursing staff at MRRH GE/NMF Program and Faculty Fellow GE/NMF Scholars

38 American Society of Anesthesiologists. Basics of Anesthetic Monitoring October 2010 American Society of Anesthesiologists. Guidelines For Patient Care in Anesthesiology October 2011 Giger, UF, et al. Risk factors for perioperative complications in patients undergoing laparoscopic cholecystectomy: analysis of 22,953 consecutive cases from the Swiss Association of Laparoscopic and Thoracoscopic Surgery database. Journal of the American College of Surgeons, v. 203 issue 5, 2006, p Hollenbeck, BK, Roberts, WW, and Wolf, JS. Importance of perioperative processes of care for length of hospital stay after laparoscopic surgery. Journal of Endourology, v. 20 issue 10, 2006, p Ministry of Health. Uganda Clinical Guidelines. National Guidelines on Management of Common Conditions, January Walder, Bernhard Improvement of perioperative care for better outcomes after surgery European Journal of Anaesthesiology, v. 28 issue 1, 2011 p. 7 9
General OR-Stanford-CA-1 revised: Tuesday, February 02, 2016
 Stanford University Anesthesiology Residency Program Rotation specific goals and objectives for residents Core Curriculum for PGY 1 Surgery Residents on the Anesthesia Rotation Description: The General
Stanford University Anesthesiology Residency Program Rotation specific goals and objectives for residents Core Curriculum for PGY 1 Surgery Residents on the Anesthesia Rotation Description: The General
STATEMENT ON THE ANESTHESIA CARE TEAM
 Committee of Origin: Anesthesia Care Team (Approved by the ASA House of Delegates on October 18, 2006, and last amended on October 21, 2009) Anesthesiology is the practice of medicine including, but not
Committee of Origin: Anesthesia Care Team (Approved by the ASA House of Delegates on October 18, 2006, and last amended on October 21, 2009) Anesthesiology is the practice of medicine including, but not
APPENDIX I QUESTIONNAIRE FOR INTERVIEWING THE ANAESTHESIA PROVIDER
 APPENDIX I QUESTIONNAIRE FOR INTERVIEWING THE ANAESTHESIA PROVIDER We are carrying out a survey to establish the quality of anaesthesia care provided to Obstetric patients in East Africa. We therefore
APPENDIX I QUESTIONNAIRE FOR INTERVIEWING THE ANAESTHESIA PROVIDER We are carrying out a survey to establish the quality of anaesthesia care provided to Obstetric patients in East Africa. We therefore
Beth Israel Deaconess Medical Center Perioperative Services Manual. Guidelines for Perioperative Handoffs from OR to receiving units.
 Beth Israel Deaconess Medical Center Perioperative Services Manual Title: Guidelines for Perioperative Handoffs from OR to receiving units. Policy #: PSM 100-102A Purpose: This guideline provides a standard
Beth Israel Deaconess Medical Center Perioperative Services Manual Title: Guidelines for Perioperative Handoffs from OR to receiving units. Policy #: PSM 100-102A Purpose: This guideline provides a standard
Department of Anesthesiology Anesthesia Curriculum Clinical Base Year
 Anesthesia Curriculum Clinical Base Year Description of Rotation The goal of this month long rotation is to teach the basic skills of anesthesia and to provide a foundation on which to build the initial
Anesthesia Curriculum Clinical Base Year Description of Rotation The goal of this month long rotation is to teach the basic skills of anesthesia and to provide a foundation on which to build the initial
9/29/2017. Enhanced Recovery After Surgery at the University of Virginia Medical Center. Disclosures. Objectives. None
 Enhanced Recovery After Surgery at the University of Virginia Medical Center Bethany Sarosiek, RN, MSN, MPH, CNL University of Virginia Health System Charlottesville, VA ErasRN@virginia.edu Disclosures
Enhanced Recovery After Surgery at the University of Virginia Medical Center Bethany Sarosiek, RN, MSN, MPH, CNL University of Virginia Health System Charlottesville, VA ErasRN@virginia.edu Disclosures
ENVIRONMENT Preoperative evaluation clinic. Preoperative evaluation clinic. Preoperative evaluation clinic. clinic. clinic. Preoperative evaluation
 Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
University of Minnesota Anesthesiology Residency Program PEDIATRIC ANESTHESIA ROTATION GOALS AND OBJECTIVES
 University of Minnesota Anesthesiology Residency Program PEDIATRIC ANESTHESIA ROTATION GOALS AND OBJECTIVES Goals: The overall goal of the rotation is to provide an introduction and understanding of the
University of Minnesota Anesthesiology Residency Program PEDIATRIC ANESTHESIA ROTATION GOALS AND OBJECTIVES Goals: The overall goal of the rotation is to provide an introduction and understanding of the
SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY
 PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
The hospital s anesthesia services must be integrated into the hospital-wide QAPI program.
 A-0416 482.52 Condition of Participation: Anesthesia Services If the hospital furnishes anesthesia services, they must be provided in a well-organized manner under the direction of a qualified doctor of
A-0416 482.52 Condition of Participation: Anesthesia Services If the hospital furnishes anesthesia services, they must be provided in a well-organized manner under the direction of a qualified doctor of
Position Number(s) Community Division/Region(s) Inuvik
 Community Division/Region(s) Inuvik") IDENTIFICATION Department Northwest Territories Health and Social Services Authority Position Title Licensed Practical Nurse Operating Room/PARR Position Number(s) Community Division/Region(s) 47-5892
IDENTIFICATION Department Northwest Territories Health and Social Services Authority Position Title Licensed Practical Nurse Operating Room/PARR Position Number(s) Community Division/Region(s) 47-5892
Management of the Surgical Patient Preoperative, Intraoperative and Postoperative
 NURS 143 Nursing in Health Alterations II Management of the Surgical Patient Preoperative, Intraoperative and Postoperative Upon completion of the O.R., PACU, or SDS experience, the student will be able
NURS 143 Nursing in Health Alterations II Management of the Surgical Patient Preoperative, Intraoperative and Postoperative Upon completion of the O.R., PACU, or SDS experience, the student will be able
Investigation Outline for a Reportable Incident Non-Hospital Surgical Facility
 Investigation Outline for a Reportable Incident Non-Hospital Surgical Facility MANDATORY NOTIFICATION The Medical Director shall notify the College of Physicians & Surgeons of Alberta (Accreditation Department)
Investigation Outline for a Reportable Incident Non-Hospital Surgical Facility MANDATORY NOTIFICATION The Medical Director shall notify the College of Physicians & Surgeons of Alberta (Accreditation Department)
The residents will work at WVU Ruby Memorial under the supervision of departmental faculty.
 CA-2 Intermediate Clinical Training (ICT) Curriculum Department of Anesthesiology Description of Rotation The goal of this multi-month rotation is to build upon the essential skills learned in the BCT
CA-2 Intermediate Clinical Training (ICT) Curriculum Department of Anesthesiology Description of Rotation The goal of this multi-month rotation is to build upon the essential skills learned in the BCT
OSS 654 Anesthesiology Clerkship Syllabus
 OSS 654 Anesthesiology Clerkship Syllabus DEPARTMENT OF OSTEOPATHIC SURGICAL SPECIALTIES SHIRLEY HARDING, D.O. CHAIRPERSON INSTRUCTOR OF RECORD HENRY E. BECKMEYER, D.O. CHIEF, DIVISION OF ANESTHESIOLOGY
OSS 654 Anesthesiology Clerkship Syllabus DEPARTMENT OF OSTEOPATHIC SURGICAL SPECIALTIES SHIRLEY HARDING, D.O. CHAIRPERSON INSTRUCTOR OF RECORD HENRY E. BECKMEYER, D.O. CHIEF, DIVISION OF ANESTHESIOLOGY
ROTATION SUMMARY PEDIATRIC ANESTHESIA ELECTIVE
 ROTATION SUMMARY PEDIATRIC ANESTHESIA ELECTIVE Rotation Contacts and Scheduling Details Rotation Director: Kelly Yeh, MD Director of Pediatric Anesthesia Santa Clara Valley Medical Center kelly.yeh@hhs.sccgov.org.,
ROTATION SUMMARY PEDIATRIC ANESTHESIA ELECTIVE Rotation Contacts and Scheduling Details Rotation Director: Kelly Yeh, MD Director of Pediatric Anesthesia Santa Clara Valley Medical Center kelly.yeh@hhs.sccgov.org.,
Massachusetts Eye and Ear Infirmary CA-3 Rotation in Anesthesiology for Otorhinolaryngologic & Ophthalmolic (ENT) procedures
 procedures") Massachusetts Eye and Ear Infirmary CA-3 Rotation in Anesthesiology for Otorhinolaryngologic & Ophthalmolic (ENT) procedures I. Medical Knowledge A. Cognitive objectives 1. Know age and size appropriate
Massachusetts Eye and Ear Infirmary CA-3 Rotation in Anesthesiology for Otorhinolaryngologic & Ophthalmolic (ENT) procedures I. Medical Knowledge A. Cognitive objectives 1. Know age and size appropriate
CA-3 Curriculum for Cardiac Anesthesia West Virginia University Department of Anesthesiology
 CA-3 Curriculum for Cardiac Anesthesia West Virginia University Department of Anesthesiology Description of Rotation or Educational Experience This rotation is a continuation of the CA-2 Cardiothoracic
CA-3 Curriculum for Cardiac Anesthesia West Virginia University Department of Anesthesiology Description of Rotation or Educational Experience This rotation is a continuation of the CA-2 Cardiothoracic
UNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOL ANESTHESIOLOGY RESIDENCY PROGRAM GOALS AND OBJECTIVES
 UNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOL ANESTHESIOLOGY RESIDENCY PROGRAM GOALS AND OBJECTIVES CA-2/CA-3 REQUIRED ROTATIONS IN PEDIATRIC ANESTHESIOLOGY The Department of Anesthesiology has established
UNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOL ANESTHESIOLOGY RESIDENCY PROGRAM GOALS AND OBJECTIVES CA-2/CA-3 REQUIRED ROTATIONS IN PEDIATRIC ANESTHESIOLOGY The Department of Anesthesiology has established
ENVIRONMENT Preoperative evaluation clinic, Preoperative holding area. Preoperative evaluation clinic, Postoperative care unit, Operating room
 Goals and Objectives, Main Operating Room Anesthesia, VAMC, CA-3 year UCSD DEPARTMENT OF ANESTHESIOLOGY OPERATING ROOM CLINICAL ANESTHESIA AT VAMC GOALS AND OBJECTIVES, CA-3 YEAR PATIENT CARE: To provide
Goals and Objectives, Main Operating Room Anesthesia, VAMC, CA-3 year UCSD DEPARTMENT OF ANESTHESIOLOGY OPERATING ROOM CLINICAL ANESTHESIA AT VAMC GOALS AND OBJECTIVES, CA-3 YEAR PATIENT CARE: To provide
Inguinal hernia repair integrated care pathway (ICP)
") Name Ward Hosp no DOB Affix patient label Inguinal hernia repair integrated care pathway (ICP) Inclusion criteria Patients undergoing inguinal hernia repair aged under 3 months corrected gestational age
Name Ward Hosp no DOB Affix patient label Inguinal hernia repair integrated care pathway (ICP) Inclusion criteria Patients undergoing inguinal hernia repair aged under 3 months corrected gestational age
Position Number(s) Community Division/Region(s) Inuvik
 Community Division/Region(s) Inuvik") IDENTIFICATION Department Northwest Territories Health and Social Services Authority Position Title Charge Nurse Operating Room / PARR Position Number(s) Community Division/Region(s) 47-5668 Inuvik Nursing
IDENTIFICATION Department Northwest Territories Health and Social Services Authority Position Title Charge Nurse Operating Room / PARR Position Number(s) Community Division/Region(s) 47-5668 Inuvik Nursing
WAITING ROOM SIGN IN I. CHIPPER
 www. GoodByeFears.com I. CHIPPER WAITING ROOM SIGN IN On surgery day Chipper's first stop was the Outpatient Surgery waiting room. This is where Chipper signs in. When the nurse calls Chipper s name,
www. GoodByeFears.com I. CHIPPER WAITING ROOM SIGN IN On surgery day Chipper's first stop was the Outpatient Surgery waiting room. This is where Chipper signs in. When the nurse calls Chipper s name,
Preanaesthetic Assessment Clinic
 One-stop Preanaesthetic Assessment Clinic A Kwan, WG Fok, KL Tong, HK Ma Department of Anaesthesiology and Pain Medicine, Operating Room Department and Day Surgery Centre United Christian Hospital 2 Preoperative
One-stop Preanaesthetic Assessment Clinic A Kwan, WG Fok, KL Tong, HK Ma Department of Anaesthesiology and Pain Medicine, Operating Room Department and Day Surgery Centre United Christian Hospital 2 Preoperative
ABO SELF-DIRECTED IMPROVEMENT IN MEDICAL PRACTICE ACTIVITY (CLINICAL)
") ABO SELF-DIRECTED IMPROVEMENT IN MEDICAL PRACTICE ACTIVITY (CLINICAL) Topic Title of Project: Reduction in the Rate of Perioperative Incidents Related to the Intraoperative Time- Out Procedure Project
ABO SELF-DIRECTED IMPROVEMENT IN MEDICAL PRACTICE ACTIVITY (CLINICAL) Topic Title of Project: Reduction in the Rate of Perioperative Incidents Related to the Intraoperative Time- Out Procedure Project
? Prehab, immunonutrition. Safe surgical principles. Optimizing Preoperative Evaluation
 Optimizing Preoperative Evaluation Timothy Geiger, MD, MMHC Associate Professor of Surgery Executive Medical Director, Surgery Patient Care Center Chief, Division of General Surgery Director, Colon and
Optimizing Preoperative Evaluation Timothy Geiger, MD, MMHC Associate Professor of Surgery Executive Medical Director, Surgery Patient Care Center Chief, Division of General Surgery Director, Colon and
Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath
 Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath Up to 25,000 surgical deaths per year 5-10% of surgical cases are high risk 79% of deaths occur in the high risk group Overall
Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath Up to 25,000 surgical deaths per year 5-10% of surgical cases are high risk 79% of deaths occur in the high risk group Overall
ORs in facilities that adopted team training had a lower rate of deaths for
 Patient safety VA study shows fewer patient deaths after OR team training ORs in facilities that adopted team training had a lower rate of deaths for surgical patients than facilities that had not yet
Patient safety VA study shows fewer patient deaths after OR team training ORs in facilities that adopted team training had a lower rate of deaths for surgical patients than facilities that had not yet
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Anesthesiology 302 Introduction to Anesthesia Goals and Objectives
 Anesthesiology 302 Introduction to Anesthesia Goals and Objectives I. The student will be able to perform an appropriate preoperative evaluation, including history, physical exam, and appropriate use of
Anesthesiology 302 Introduction to Anesthesia Goals and Objectives I. The student will be able to perform an appropriate preoperative evaluation, including history, physical exam, and appropriate use of
Quality Improvement Initiative (QII): 2018 Options
: 2018 Options") Quality Improvement Implementation, Option A: Increase Surgeon Engagement Outcome Measure: SSI Summary: Surgeon Engagement is essential for the success of quality improvement programs within hospitals.
Quality Improvement Implementation, Option A: Increase Surgeon Engagement Outcome Measure: SSI Summary: Surgeon Engagement is essential for the success of quality improvement programs within hospitals.
Anesthesia Elective Curriculum Outline
 Department of Internal Medicine Texas Tech University Health Sciences Center Odessa, Texas Anesthesia Elective Curriculum Outline Revision Date: July 10, 2006 Approved by Curriculum Meeting September 19,
Department of Internal Medicine Texas Tech University Health Sciences Center Odessa, Texas Anesthesia Elective Curriculum Outline Revision Date: July 10, 2006 Approved by Curriculum Meeting September 19,
How do we know the surgical checklist is making a meaningful. impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010
 How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #426: Post-Anesthetic Transfer of Care Measure: Procedure Room to a Post Anesthesia Care Unit (PACU) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL
Quality ID #426: Post-Anesthetic Transfer of Care Measure: Procedure Room to a Post Anesthesia Care Unit (PACU) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL
1. Introduction. 1 CMS section
 1. Introduction Anesthesiology is the practice of medicine including, but not limited to, preoperative patient evaluation, anesthetic planning, intraoperative and postoperative care and the management
1. Introduction Anesthesiology is the practice of medicine including, but not limited to, preoperative patient evaluation, anesthetic planning, intraoperative and postoperative care and the management
Enhanced Recovery After Surgery (ERAS) for Elective Colon Resection Surgery at Vancouver General Hospital. What is Possible?
 for Elective Colon Resection Surgery at Vancouver General Hospital. What is Possible?") Enhanced Recovery After Surgery (ERAS) for Elective Colon Resection Surgery at Vancouver General Hospital What is Possible? BC Provincial Collaborative November 25, 2014 Disclosure Statement I do not have
Enhanced Recovery After Surgery (ERAS) for Elective Colon Resection Surgery at Vancouver General Hospital What is Possible? BC Provincial Collaborative November 25, 2014 Disclosure Statement I do not have
Oscar Guillamondegui, MD, MPH, FACS Associate Professor of Surgery Tennessee Surgical Quality Collaborative
 Oscar Guillamondegui, MD, MPH, FACS Associate Professor of Surgery Tennessee Surgical Quality Collaborative NSQIP 2014 A Collaborative that has Reduced Surgical Site Infections Tennessee Surgical Quality
Oscar Guillamondegui, MD, MPH, FACS Associate Professor of Surgery Tennessee Surgical Quality Collaborative NSQIP 2014 A Collaborative that has Reduced Surgical Site Infections Tennessee Surgical Quality
GENERAL PROGRAM GOALS AND OBJECTIVES
 BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
SCIP-Inf-2, SCIP-Inf-3, SCIP-Inf-4, SCIP-Inf- 9, SCIP-Inf-10, SCIP-VTE-1, SCIP-VTE-2 Anesthesia End Time 5
 Release Notes: Alphabetical Data Dictionary Version 3.3 Surgical Care Improvement Project (SCIP) - Data Dictionary The General Abstraction Guidelines explain the different sections of the data element
Release Notes: Alphabetical Data Dictionary Version 3.3 Surgical Care Improvement Project (SCIP) - Data Dictionary The General Abstraction Guidelines explain the different sections of the data element
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
RULES AND REGULATIONS DEPARTMENT OF ANESTHESIOLOGY Revised March 2012
 RULES AND REGULATIONS DEPARTMENT OF ANESTHESIOLOGY Revised March 2012 Section I-Administration Scope of service. 3 Major Diseases/conditions managed 3 Department philosophy and objectives 3 Guidelines
RULES AND REGULATIONS DEPARTMENT OF ANESTHESIOLOGY Revised March 2012 Section I-Administration Scope of service. 3 Major Diseases/conditions managed 3 Department philosophy and objectives 3 Guidelines
CA-2 Curriculum for Obstetric Anesthesia Department of Anesthesiology
 CA-2 Curriculum for Obstetric Anesthesia Department of Anesthesiology Description of Rotation or Educational Experience The goal of the CA-2 rotation in obstetric anesthesia is to enhance the knowledge
CA-2 Curriculum for Obstetric Anesthesia Department of Anesthesiology Description of Rotation or Educational Experience The goal of the CA-2 rotation in obstetric anesthesia is to enhance the knowledge
SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY
 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ANESTHESIA CARE AND INTRAOPERATIVE Job Title of Responsible Owner: EFFECTIVE DATE: REVIEW/REVISED DATE: TYPE: Director of Perioperative
SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ANESTHESIA CARE AND INTRAOPERATIVE Job Title of Responsible Owner: EFFECTIVE DATE: REVIEW/REVISED DATE: TYPE: Director of Perioperative
A Pilot Study in Performance Improvement CME: Using an Electronic Health Record for Guided Self Assessment and Learning
 A Pilot Study in Performance Improvement CME: Using an Electronic Health Record for Guided Self Assessment and Learning Joseph L. Seltzer, MD Jeanne G. Cole, MS Nothing to disclose Timely Administration
A Pilot Study in Performance Improvement CME: Using an Electronic Health Record for Guided Self Assessment and Learning Joseph L. Seltzer, MD Jeanne G. Cole, MS Nothing to disclose Timely Administration
STATEMENT ON GRANTING PRIVILEGES FOR ADMINISTRATION OF MODERATE SEDATION TO PRACTITIONERS WHO ARE NOT ANESTHESIA PROFESSIONALS
 NOT ANESTHESIA PROFESSIONALS (Approved by the ASA House of Delegates on October 25, 2005, and amended on October 18, 2006) Outcome Indicators for Office-Based and Ambulatory Surgery (ASA Committee on Ambulatory
NOT ANESTHESIA PROFESSIONALS (Approved by the ASA House of Delegates on October 25, 2005, and amended on October 18, 2006) Outcome Indicators for Office-Based and Ambulatory Surgery (ASA Committee on Ambulatory
Clinical Fellowship: Cardiac Anesthesia
 Anesthesia and Perioperative Medicine Western University Cardiac Anesthesia Program Director Dr. Anita Cave Please visit the Cardiac Anesthesia Fellowship site for most up-to-date information: http://www.schulich.uwo.ca/anesthesia/education/fellowship/fellowships_offered/cardiac_anesthesia.html
Anesthesia and Perioperative Medicine Western University Cardiac Anesthesia Program Director Dr. Anita Cave Please visit the Cardiac Anesthesia Fellowship site for most up-to-date information: http://www.schulich.uwo.ca/anesthesia/education/fellowship/fellowships_offered/cardiac_anesthesia.html
CA-1 NEUROANESTHESIA ROTATION University of Minnesota Medical Center Rotation Site Director: Dr. Thomas Kozhimannil Rotation Duration: 4 weeks
 CA-1 NEUROANESTHESIA ROTATION Medical Center Rotation Site Director: Dr. Thomas Kozhimannil Rotation Duration: 4 weeks Introduction: The goal of the Neurosurgical Anesthesia Rotation at the is to train
CA-1 NEUROANESTHESIA ROTATION Medical Center Rotation Site Director: Dr. Thomas Kozhimannil Rotation Duration: 4 weeks Introduction: The goal of the Neurosurgical Anesthesia Rotation at the is to train
Peri-operative Pain Management - a multi-disciplinary team-based approach
 Peri-operative Pain Management - a multi-disciplinary team-based approach Dr Steven Wong Chief of Service Department of Anaesthesiology & OT Services Queen Elizabeth Hospital Outline Development of postoperative
Peri-operative Pain Management - a multi-disciplinary team-based approach Dr Steven Wong Chief of Service Department of Anaesthesiology & OT Services Queen Elizabeth Hospital Outline Development of postoperative
Scale is the latter has calculations for a level of risk which L
 The CMUNRO SCALE Education Sheet The CMUNRO SCALE risk assessment mnemonic is the first action in developing a surgical patient's pressure injury prevention plan. The CMUNRO SCALE is an acronym developed
The CMUNRO SCALE Education Sheet The CMUNRO SCALE risk assessment mnemonic is the first action in developing a surgical patient's pressure injury prevention plan. The CMUNRO SCALE is an acronym developed
Principles In developing these recommendations the Consensus Panel first established the following principles for anesthesia outcomes capture:
 Outcomes of Anesthesia: Core Measures The following Core Measures are the consensus recommendations of the Anesthesia Quality Institute (AQI) and the Multicenter Perioperative Outcomes Group (MPOG). They
Outcomes of Anesthesia: Core Measures The following Core Measures are the consensus recommendations of the Anesthesia Quality Institute (AQI) and the Multicenter Perioperative Outcomes Group (MPOG). They
Statement on Safe Use of Propofol (Approved by ASA House of Delegates on October 27, 2004);
;") CREDENTIALING GUIDELINES FOR PRACTITIONERS WHO ARE NOT ANESTHESIA PROFESSIONALS TO ADMINISTER ANESTHETIC DRUGS TO ESTABLISH A LEVEL OF MODERATE SEDATION (Approved by the House of Delegates on October 25,
CREDENTIALING GUIDELINES FOR PRACTITIONERS WHO ARE NOT ANESTHESIA PROFESSIONALS TO ADMINISTER ANESTHETIC DRUGS TO ESTABLISH A LEVEL OF MODERATE SEDATION (Approved by the House of Delegates on October 25,
APPLIES TO: x SummaCare, Inc. x Apex Health Solutions PRODUCT LINE(S): (Check all that apply)
: (Check all that apply)") POLICY NAME: ANESTHESIA PAYMENT POLICY POLICY NUMBER: ISSUING DEPT.: Claims EFFECTIVE DATE: 9/25/2017 APPROVED BY: APPLIES TO: x SummaCare, Inc. x Apex Health Solutions PRODUCT LINE(S): (Check all that
POLICY NAME: ANESTHESIA PAYMENT POLICY POLICY NUMBER: ISSUING DEPT.: Claims EFFECTIVE DATE: 9/25/2017 APPROVED BY: APPLIES TO: x SummaCare, Inc. x Apex Health Solutions PRODUCT LINE(S): (Check all that
HLT07 Health Training Package Learner resource Version 2 Training and Education Support Industry Skills Unit Meadowbank Product Code: 5571
 HLT07 Health Training Package HLTEN512B Implement and monitor nursing care for clients with acute health problems Learner resource Version 2 Training and Education Support Industry Skills Unit Meadowbank
HLT07 Health Training Package HLTEN512B Implement and monitor nursing care for clients with acute health problems Learner resource Version 2 Training and Education Support Industry Skills Unit Meadowbank
Goals and Objectives University of Minnesota Department of Anesthesiology Senior Resident Supervising Rotation
 UM Anesthesiology Page 1 June, 2007 Introduction Goals and Objectives University of Minnesota Department of Anesthesiology Senior Resident Supervising Rotation The ABA defines the attributes of consultant
UM Anesthesiology Page 1 June, 2007 Introduction Goals and Objectives University of Minnesota Department of Anesthesiology Senior Resident Supervising Rotation The ABA defines the attributes of consultant
Goals and Objectives. Assessment Methods/Tools
 CA-2 PEDIATRIC ANESTHESIA ROTATION Minneapolis Children s Hospital and Clinics (MCHC) Rotation Site Director: Dr. Chris Altman Rotation Duration: 6 weeks Introduction: In the CA-2 year residents have the
CA-2 PEDIATRIC ANESTHESIA ROTATION Minneapolis Children s Hospital and Clinics (MCHC) Rotation Site Director: Dr. Chris Altman Rotation Duration: 6 weeks Introduction: In the CA-2 year residents have the
Clinical guideline Published: 23 April 2008 nice.org.uk/guidance/cg65
 Hypothermia: prevention ention and management in adults having surgery Clinical guideline Published: 23 April 2008 nice.org.uk/guidance/cg65 NICE 20. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypothermia: prevention ention and management in adults having surgery Clinical guideline Published: 23 April 2008 nice.org.uk/guidance/cg65 NICE 20. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Chapter 11 Assessment of the Medical Patient DOT Directory
 Chapter 11 Assessment of the Medical Patient U.S. Objectives U.S. Objectives are covered and/or supported by the PowerPoint Slide Program and Notes for Emergency Care, 11th Ed. Please see the Chapter 11
Chapter 11 Assessment of the Medical Patient U.S. Objectives U.S. Objectives are covered and/or supported by the PowerPoint Slide Program and Notes for Emergency Care, 11th Ed. Please see the Chapter 11
Perioperative Surgical Home
 None Disclosures Debnath Chatterjee, M.D. Associate Professor of Anesthesiology CRASH 2015 - Vail, Colorado 2 Learning Objectives What is the PSH model? Describe the concept of the Perioperative Surgical
None Disclosures Debnath Chatterjee, M.D. Associate Professor of Anesthesiology CRASH 2015 - Vail, Colorado 2 Learning Objectives What is the PSH model? Describe the concept of the Perioperative Surgical
Cost Effectiveness of Physician Anesthesia J.P. Abenstein, M.S.E.E., M.D. Mayo Clinic Rochester, MN
 Mayo Clinic Rochester, MN Introduction The question of whether anesthesiologists are cost-effective providers of anesthesia services remains an open question in the minds of some of our medical colleagues,
Mayo Clinic Rochester, MN Introduction The question of whether anesthesiologists are cost-effective providers of anesthesia services remains an open question in the minds of some of our medical colleagues,
Survey on ASA Standards and APSF Recommendations
 Physician-Patient Alliance for Health & Safety Improving Health & Safety Through Innovation and Awareness Survey on ASA Standards and APSF Recommendations Mike Wong Physician-Patient Alliance for Health
Physician-Patient Alliance for Health & Safety Improving Health & Safety Through Innovation and Awareness Survey on ASA Standards and APSF Recommendations Mike Wong Physician-Patient Alliance for Health
Waiting for a family member who is having surgery
 Waiting for a family member who is having surgery UHN Information for families, friends and caregivers in the Surgical Family Waiting Room Your family member, friend or loved one is having surgery. We
Waiting for a family member who is having surgery UHN Information for families, friends and caregivers in the Surgical Family Waiting Room Your family member, friend or loved one is having surgery. We
Review anesthetic human safety hazards annually with all hospital associates. Designate dedicated anesthetic induction and recovery areas.
 Designate dedicated anesthetic induction and recovery areas. Review anesthetic human safety hazards annually with all hospital associates. What are the advantages of having dedicated areas? How would induction
Designate dedicated anesthetic induction and recovery areas. Review anesthetic human safety hazards annually with all hospital associates. What are the advantages of having dedicated areas? How would induction
MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY
 POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
LOUISIANA MEDICAID PROGRAM ISSUED: 02/01/12 REPLACED: 02/01/94 CHAPTER 5: PROFESSIONAL SERVICES SECTION 5.1: COVERED SERVICES PAGE(S) 11
 11") Anesthesia Services Surgical anesthesia services may be provided by anesthesiologists or certified registered nurse anesthetists (CRNAs). Maternity-related anesthesia services may be provided by anesthesiologists,
Anesthesia Services Surgical anesthesia services may be provided by anesthesiologists or certified registered nurse anesthetists (CRNAs). Maternity-related anesthesia services may be provided by anesthesiologists,
DEACONESS HOSPITAL, INC. Evansville, Indiana DEPARTMENT OF ANESTHESIOLOGY RULES & REGULATIONS
 DEACONESS HOSPITAL, INC. Evansville, Indiana DEPARTMENT OF ANESTHESIOLOGY RULES & REGULATIONS I. Department Organization and Direction - The Department of Anesthesiology shall be properly organized, directed
DEACONESS HOSPITAL, INC. Evansville, Indiana DEPARTMENT OF ANESTHESIOLOGY RULES & REGULATIONS I. Department Organization and Direction - The Department of Anesthesiology shall be properly organized, directed
Post Anesthesia Care (PACU) Guidelines
 Guidelines") Post Anesthesia Care (PACU) Guidelines 114 Tiberiu Ezri Introduction Medical errors are difficult to avoid and may increase patient morbidity and mortality rates. The Israeli Ombudsman (The Commissioner
Post Anesthesia Care (PACU) Guidelines 114 Tiberiu Ezri Introduction Medical errors are difficult to avoid and may increase patient morbidity and mortality rates. The Israeli Ombudsman (The Commissioner
Just Culture Toolkit Scenarios
 Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
COMMITTEE ON QUALITY MANAGEMENT AND DEPARTMENTAL ADMINISTRATION AMERICAN SOCIETY OF ANESTHESIOLOGISTS ANESTHESIOLOGY DEPARTMENT QUALITY CHECKLIST
 COMMITTEE ON QUALITY MANAGEMENT AND DEPARTMENTAL ADMINISTRATION AMERICAN SOCIETY OF ANESTHESIOLOGISTS ANESTHESIOLOGY DEPARTMENT QUALITY CHECKLIST The following series of questions has been developed by
COMMITTEE ON QUALITY MANAGEMENT AND DEPARTMENTAL ADMINISTRATION AMERICAN SOCIETY OF ANESTHESIOLOGISTS ANESTHESIOLOGY DEPARTMENT QUALITY CHECKLIST The following series of questions has been developed by
Measure Abbreviation: TEMP 03 (MIPS 424)*
*") Measure Abbreviation: TEMP 03 (MIPS 424)* *TEMP 03 is built to the specification outlined by the Merit Based Incentive Program (MIPS) 424: Perioperative Temperature Management measure. MIPS measure specifications
Measure Abbreviation: TEMP 03 (MIPS 424)* *TEMP 03 is built to the specification outlined by the Merit Based Incentive Program (MIPS) 424: Perioperative Temperature Management measure. MIPS measure specifications
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation
 Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
CRITICAL ACCESS HOSPITALS
 Are anesthesia services and post-anesthesia services medical director(s) qualified in terms of education, experience and competency as determined by the hospital medical staff and appointed by the governing
Are anesthesia services and post-anesthesia services medical director(s) qualified in terms of education, experience and competency as determined by the hospital medical staff and appointed by the governing
SAMPLE Perioperative Self-Assessment Questionnaire
 SAMPLE Perioperative Self-Assessment Questionnaire Hospital Name: Person Completing the Assessment: Date: I. Executive Leadership Yes No 1. Do executive leaders have a defined mode of regular communication
SAMPLE Perioperative Self-Assessment Questionnaire Hospital Name: Person Completing the Assessment: Date: I. Executive Leadership Yes No 1. Do executive leaders have a defined mode of regular communication
PREVENTION OF POSTOPERATIVE PULMONARY COMPLICATIONS: Reducing Postoperative Mechanical Ventilation
 PREVENTION OF POSTOPERATIVE PULMONARY COMPLICATIONS: Reducing Postoperative Mechanical Ventilation Rowena Chona O. Sano, MSN, RN, CNL, CPHQ Memorial Hermann Greater Heights Hospital Houston, TX Nothing
PREVENTION OF POSTOPERATIVE PULMONARY COMPLICATIONS: Reducing Postoperative Mechanical Ventilation Rowena Chona O. Sano, MSN, RN, CNL, CPHQ Memorial Hermann Greater Heights Hospital Houston, TX Nothing
Clinical Fellowship Acute Pain Service
 Anesthesia and Perioperative Medicine Western University Acute Pain Service Program Directors Dr. Kevin Armstrong Dr. Qutaiba Tawfic Please visit the Acute Pain Service Fellowship site for most up-to-date
Anesthesia and Perioperative Medicine Western University Acute Pain Service Program Directors Dr. Kevin Armstrong Dr. Qutaiba Tawfic Please visit the Acute Pain Service Fellowship site for most up-to-date
PRE OPERATIVE MANAGEMENT FOR PEDIATRIC HOSPITALISTS
 Before the Operating Room: PRE OPERATIVE MANAGEMENT FOR PEDIATRIC HOSPITALISTS Presenters: Anjna Melwani, MD Sonaly McClymont, MD David Rappaport, MD Sarah Denniston, MD David Pressel, MD Amy Vinson, MD
Before the Operating Room: PRE OPERATIVE MANAGEMENT FOR PEDIATRIC HOSPITALISTS Presenters: Anjna Melwani, MD Sonaly McClymont, MD David Rappaport, MD Sarah Denniston, MD David Pressel, MD Amy Vinson, MD
KNOW YOUR BATNA: SHARED RISK AND FUTURE PAYMENT SYSTEMS DISCLOSURES OBJECTIVES
 KNOW YOUR BATNA: SHARED RISK AND FUTURE PAYMENT SYSTEMS Stanley W. Stead, M.D., M.B.A. President, Stead Health Group, Inc. Section Chair, ASA Section on Professional Practice AMA Relative Value Update
KNOW YOUR BATNA: SHARED RISK AND FUTURE PAYMENT SYSTEMS Stanley W. Stead, M.D., M.B.A. President, Stead Health Group, Inc. Section Chair, ASA Section on Professional Practice AMA Relative Value Update
ROLE OF THE ANESTHETIST IN ORGANIZING AMBULATORY SURGERY. Dr. Paul Vercruysse M.D. Belgium
 ROLE OF THE ANESTHETIST IN ORGANIZING AMBULATORY SURGERY Dr. Paul Vercruysse M.D. Belgium DISCLOSURES - Conflicts of interest? I am an anesthesiologist... TRADITIONAL ROLE OF THE ANESTHESIOLOGIST EVOLVING
ROLE OF THE ANESTHETIST IN ORGANIZING AMBULATORY SURGERY Dr. Paul Vercruysse M.D. Belgium DISCLOSURES - Conflicts of interest? I am an anesthesiologist... TRADITIONAL ROLE OF THE ANESTHESIOLOGIST EVOLVING
Introduction to Perioperative Nursing
 C H A P T E R 1 Introduction to Perioperative Nursing LEARNER OBJECTIVES 1. Define the three phases of the surgical experience. 2. Describe the scope of perioperative nursing practice. 3. Discuss application
C H A P T E R 1 Introduction to Perioperative Nursing LEARNER OBJECTIVES 1. Define the three phases of the surgical experience. 2. Describe the scope of perioperative nursing practice. 3. Discuss application
JOHNS HOPKINS HEALTHCARE Physician Guidelines
 Page 1 of 7 ACTION New Procedure Amending Procedure Number: Superseding Procedure Number: Repealing Procedure Number: REFERENCES: AMPT Committee ASA Guidelines CMS Guidelines I. GENERAL ANESTHESIA PROCEDURE:
Page 1 of 7 ACTION New Procedure Amending Procedure Number: Superseding Procedure Number: Repealing Procedure Number: REFERENCES: AMPT Committee ASA Guidelines CMS Guidelines I. GENERAL ANESTHESIA PROCEDURE:
Guidelines on Postanaesthetic Recovery Care
 Page 1 of 10 Guidelines on Postanaesthetic Recovery Care Version Effective Date 1 OCT 1992 2 FEB 2002 3 APR 2012 4 JUN 2017 Document No. HKCA P3 v4 Prepared by College Guidelines Committee Endorsed by
Page 1 of 10 Guidelines on Postanaesthetic Recovery Care Version Effective Date 1 OCT 1992 2 FEB 2002 3 APR 2012 4 JUN 2017 Document No. HKCA P3 v4 Prepared by College Guidelines Committee Endorsed by
Sedation/Analgesia by Non-Anesthesiologists. THE UNIVERSITY OF TOLEDO Approving Officer:
 Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Your Anesthesiologist, Anesthesia and Pain Control
 You can reduce your pain level after surgery by planning ahead. For example, if you know that you are going to be getting up to do your exercises with the therapist, ask for pain control medication in
You can reduce your pain level after surgery by planning ahead. For example, if you know that you are going to be getting up to do your exercises with the therapist, ask for pain control medication in
Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition
 Nursing Competency Workbook 6th Edition") Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition The Royal Children's Hospital (RCH) Nursing Competency Workbook is a dynamic document that will
Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition The Royal Children's Hospital (RCH) Nursing Competency Workbook is a dynamic document that will
PREOPERATIVE ASSESSMENT Case Study
 GOALS: The goals of this learning activity seek to establish the need for preoperative nursing assessment, evaluation of chart review and considerations for plan of care and information sharing with surgical
GOALS: The goals of this learning activity seek to establish the need for preoperative nursing assessment, evaluation of chart review and considerations for plan of care and information sharing with surgical
Abdominal Surgery. Beyond Medicine. What to Expect While You Are in the Hospital. ilearning about your health
 ilearning about your health Abdominal Surgery What to Expect While You Are in the Hospital www.cpmc.org/learning Beyond Medicine. Table of Contents On the Day of Your Surgery...3 Your Nursing Care...3
ilearning about your health Abdominal Surgery What to Expect While You Are in the Hospital www.cpmc.org/learning Beyond Medicine. Table of Contents On the Day of Your Surgery...3 Your Nursing Care...3
Having Day Surgery at Toronto Western Hospital (DSU)
") Having Day Surgery at Toronto Western Hospital (DSU) Surgeon: Date of my surgery: Time to arrive at the hospital: Time of my surgery: On the day of your surgery please go to: Preoperative Care Unit (POCU)
Having Day Surgery at Toronto Western Hospital (DSU) Surgeon: Date of my surgery: Time to arrive at the hospital: Time of my surgery: On the day of your surgery please go to: Preoperative Care Unit (POCU)
Measurability of Patient Safety
 Measurability of Patient Safety Marsha Fleischer IMPO Conference, November 17, 2016 External requirements in Germany lead to a higher need for safety and risk management, among others arising from the:
Measurability of Patient Safety Marsha Fleischer IMPO Conference, November 17, 2016 External requirements in Germany lead to a higher need for safety and risk management, among others arising from the:
Class of 2016 DNP Projects. NorthShore University HealthSystem School of Nurse Anesthesia & DePaul University School of Nursing 2016 DNP Projects
 NorthShore University HealthSystem School of Nurse Anesthesia & DePaul University School of Nursing 2016 DNP Projects 1 1. BETTY MESTOUSIS MSN, RN & MINNIE ZHOU BSN, RN Anesthesia Cost Awareness Project:
NorthShore University HealthSystem School of Nurse Anesthesia & DePaul University School of Nursing 2016 DNP Projects 1 1. BETTY MESTOUSIS MSN, RN & MINNIE ZHOU BSN, RN Anesthesia Cost Awareness Project:
Post-operative "Fast-Track" pathways for lung resection. Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic
 Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic
Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic
SURGICAL SAFETY CHECKLIST
 SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
Domain 5 Cardiothoracic Standards RCoA Accreditation 2017
 1 PRIORITY The Care Pathway 5.4.1.1 The process for preoperative assessment presenting for cardiac and thoracic patients (including thoracic aortic) is defined within the patient pathway. 1 A clinical
1 PRIORITY The Care Pathway 5.4.1.1 The process for preoperative assessment presenting for cardiac and thoracic patients (including thoracic aortic) is defined within the patient pathway. 1 A clinical
THE AMERICAN BOARD OF ANESTHESIOLOGY
 THE AMERICAN BOARD OF ANESTHESIOLOGY 4208 Six Forks Road, Suite 1500 Raleigh, NC 27609-5765 Phone: (866) 999-7501 Fax: (866) 999-7503 Website: www.theaba.org MOCA PART 4: IMPROVEMENT IN MEDICAL PRACTICE
THE AMERICAN BOARD OF ANESTHESIOLOGY 4208 Six Forks Road, Suite 1500 Raleigh, NC 27609-5765 Phone: (866) 999-7501 Fax: (866) 999-7503 Website: www.theaba.org MOCA PART 4: IMPROVEMENT IN MEDICAL PRACTICE
Anesthesia Services Policy
 Anesthesia Services Policy Policy Number Annual Approval Date 3/14/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare Medicare
Anesthesia Services Policy Policy Number Annual Approval Date 3/14/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare Medicare
LINEE GUIDA PER INFERMIERI PER LA CHIRURGIA AMBULATORIALE NEGLI STATI UNITI
 LINEE GUIDA PER INFERMIERI PER LA CHIRURGIA AMBULATORIALE NEGLI STATI UNITI MAIMONIDES MEDICAL CENTER DEPARTMENT OF NURSING PERIOPERATIVE SERVICES PRE-ADMISSION TESTING (P.A.T) I. POLICY: To facilitate
LINEE GUIDA PER INFERMIERI PER LA CHIRURGIA AMBULATORIALE NEGLI STATI UNITI MAIMONIDES MEDICAL CENTER DEPARTMENT OF NURSING PERIOPERATIVE SERVICES PRE-ADMISSION TESTING (P.A.T) I. POLICY: To facilitate
Preparing for Thoracic Surgery and Recovery
 Division of Thoracic Surgery Preparing for Thoracic Surgery and Recovery A Guide for Patients and Families Brigham And Women s/faulkner Hospitals Important Phone Numbers Important Phone Numbers BWH NUMBERS
Division of Thoracic Surgery Preparing for Thoracic Surgery and Recovery A Guide for Patients and Families Brigham And Women s/faulkner Hospitals Important Phone Numbers Important Phone Numbers BWH NUMBERS
The Essentials of Maintaining Patient Normothermia
 1 The Essentials of Maintaining Patient Normothermia Copyright 2011 by Virgo Publishing. http://www.infectioncontroltoday.com/ By: Posted on: 02/22/2010 http://www.infectioncontroltoday.com/articles/2010/02/the-essentials-of-maintainingpatient-normothermi.aspx
1 The Essentials of Maintaining Patient Normothermia Copyright 2011 by Virgo Publishing. http://www.infectioncontroltoday.com/ By: Posted on: 02/22/2010 http://www.infectioncontroltoday.com/articles/2010/02/the-essentials-of-maintainingpatient-normothermi.aspx
Norwegian Standard for the Safe Practice of Anaesthesia
 Norwegian Standard for the Safe Practice of Anaesthesia 1. Introduction The Norwegian standard for the safe practice of anaesthesia was first published in 1991. It was then revised in 1994, and subsequently
Norwegian Standard for the Safe Practice of Anaesthesia 1. Introduction The Norwegian standard for the safe practice of anaesthesia was first published in 1991. It was then revised in 1994, and subsequently
AQI48a: Percentage of patients, aged 18 and older, who were surveyed on their patient experience and satisfaction with anesthesia care
 Measure Title AQI48: Patient-Reported Experience with Anesthesia Measure Description Percentage of patients, aged 18 and older, who were surveyed on their patient experience and satisfaction with anesthesia
Measure Title AQI48: Patient-Reported Experience with Anesthesia Measure Description Percentage of patients, aged 18 and older, who were surveyed on their patient experience and satisfaction with anesthesia