Making the Case and Making It Work: Integrating Behavioral Health into Primary Care
|
|
|
- Carmella Park
- 5 years ago
- Views:
Transcription

1 LEARN MORE ibhpartners.org Making the Case and Making It Work: Integrating Behavioral Health into Primary Care Karen W. Linkins, PhD May 18, 2016
2 What we ll cover today Why Integrated Behavioral Health Changing policy environment Where we are headed: Collective impact and Accountable Communities of Health
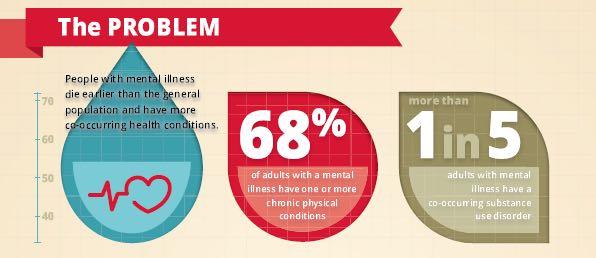
3 The Problem: Fragmentation Clinical delivery Payment /financing Community expectation Fragmentation Training/education
4
5 Quick Review: Case for Integration 5% of the population use 50% of the health care resources (the 5/50 population) 1% use 20% of the health care resources Half of both groups have a behavioral health disorder Primary care is the sole source of MH treatment for 1/3 of patients receiving care for a MH condition Depressed patients are 3 times more likely than nondepressed patient to be non-compliant with treatment recommendations 5
6 Behavioral Health is a Key Concern for Health Care Disparities: Affects low-income populations o Nearly half (49%) of all Medicaid beneficiaries with disabilities have a psychiatric diagnosis o Among Dual eligibles (Medicare/Medicaid), 44 percent have at least one mental health diagnosis Cost driver o Behavioral health disorders are among the five most costly conditions in the U.S. with expenditures of $57 billion o Mood disorders such as depression are third most common cause of hospitalization in the U.S for both youth and adults
7 We only spend 5% of our health dollars to address what causes 60% of our avoidable deaths Causes of avoidable death in the United States 1 United States health expenditures in Social factors Health care Population-wide approaches to health improvement Behavioral health prevention Chemical dependency prevention Maternal and child health programs Public health activities Research School health programs 15% 10% 5% 30% Genetics 40% 95% 5% Behavior Environment Health care 1 McGinnis et al., The case for more active policy attention to health promotion. Health Affairs 2002; 21(2): Centers for Medicare & Medicaid Services, Office of the Actuary. National health expenditures, by source of funds and type of expenditure
8 Economic Impact of Integrated Behavioral Health CMSP: reimbursing primary care clinics for up to 10 mental health visits and 20 substance abuse visits per year resulted in a dramatic 57% drop in psychiatric days by the treated group (vs. a 71% increase in the business-as-usual controls). However, this cost-savings was neutralized by an increase in outpatient expenses. Nonetheless, CMSP has elected to continue the program with the expectation that there will be savings once the program is further underway. Evaluation of the CMSP Behavioral Health Pilot Project, Draft Final Report, prepared for CMSP by the Lewin Group, February, 2011 Depression management for depressed primary care clients resulted in a $980 cost decrease for those who complained of psychological symptoms, but there was a $1,378 cost increase for those who complained of physical symptoms only. Miriam Dickinson et al., RCT of a Care Manager Intervention for Major Depression in Primary Care: 2-Year Costs for Patients With Physical vs Psychological Complaints Annals of Family Medicine, 2005, 3: The impact of psychological interventions on the use of medical services was evaluated by examining the outcome of 91 studies published between 1967 and 1997 using meta-analytic techniques and percentage estimates. Results provided evidence for a medical cost-offset effect, specifically in the domain of behavioral medicine. Average savings resulting from implementing psychological interventions was estimated to be about 20%. About one third of the articles demonstrated that dollar savings continued to be substantial even when the cost of providing the psychological intervention was subtracted from the savings. Jeremy A. Chiles et al. The Impact of Psychological Interventions on Medical Cost Offset: A Meta-analytic Review Clinical Psychology: Science and Practice, June 1999, Vol. 6. Collaborative care, implemented through brief cognitive-behavioral therapy and enhanced patient education in primary care, increased depression treatment costs, but improved the cost-effectiveness of treatment for patients with major depression. A cost offset in specialty mental health costs, but not medical care costs, was observed. Von Korff, Treatment cost offsets and cost-effectiveness of collaborative management of depression, Psychosomatic Medicine, 1998, 60. When clients with diabetes and depression received depression collaborative care (a depression care manager offered education, behavioral activation, and a choice of problem-solving treatment or support of antidepressant management by the primary care physician), an incremental net benefit of $1,129 was found over two years. The study concluded that this intervention is a high-value investment for older adults with diabetes; it is associated with high clinical benefits at no greater cost than usual care. Wayne Katon et al. Cost-Effectiveness and Net Benefit of Enhanced Treatment of Depression for Older Adults with Diabetes and Depression. Diabetes Care 29: , When family physicians worked collaboratively with mental health professionals to treat persons on short-term mental health disability leave, their patients returned to work at higher rates than those treated by physicians alone. The average cost savings to employers was $503 per patient. Carolyn Dewa et al. Cost, Effectiveness and Cost-Effectiveness of a Collaborative Mental Health Care Program for People Receiving Short-Term Disability Benefits for Psychiatric Disorders, Canadian Journal of Psychiatry, 54(6), Over 24 months, clients having both diabetes and depression who were assigned to a stepped-care depression treatment program had outpatient health services costs that averaged $314 less compared to those who received care as usual. The authors conclude that for adults with diabetes, systematic depression treatment appears to have significant economic benefits from the health plan perspective. Gregory Simon et al., Cost-effectiveness of Systematic Depression Treatment Among People With Diabetes Mellitus, Archives of General Psychiatry, January, 2007, Vol. 64, No. 1. A study of Medicaid recipients diagnosed as chemically dependent found that those not using mental health services increased their medical costs by 91% during the study period, compared to decreased costs for recipients of mental health treatment. In the first twelve months after treatment, some interventions produced net decreases of approximately $514 per person. N.,Cummings, et al. The impact of psychological intervention on healthcare utilization and costs. Biodyne Institute, A collaborative care intervention for primary care clients with panic disorder, including systematic patient education and approximately two visits with an on-site consulting psychiatrist, resulted in no significant differences in total outpatient costs, and an analysis suggests a 70% probability that the intervention led to lower costs and greater effectiveness compared with usual care. Wayne J. Katon, Cost-effectiveness and Cost Offset of a Collaborative Care Intervention for Primary Care Patients with Panic Disorder, Arch Gen Psychiatry. 2002; 59. Comprehensive collaborative and structured mental health services provided to high utilizers of mental health services resulted in a 65% reduction in community hospital days. Nancy Anderson, Medical Cost Offsets Associated with Mental Health Care A Brief Review, Washington State Dept. of Social and Health Services, December, Use of managed mental health care (structured, targeted, focused and brief treatment) for Medicaid enrollees reduced medical services costs and utilization by 23 to 40 percent relative to control groups. For enrollees with chronic medical diagnoses, managed treatment reduced medical costs by 28 to 47 percent. For enrollees without chronic medical diagnoses, traditional fee-for-service also reduced medical costs by about 20% but used three times as many outpatient visits. Costs of managed treatment were recovered in 6 to 24 months. The managed mental health group spent fewer days in the hospital and used the emergency room less. MS Pallak et al., Medical costs, Medicaid, and managed mental health treatment: the Hawaii study, Managed Care Q, 1994 Spring; 2 (2). An eight-session mind/body education program for people prone to somatization and an eight session chronic pain management program decreased medical office visits by about 35%. Daniel Bruns et al., The Implementation of Integrated Primary Care at Kaiser Permanente :An Interview with Roger Johnson, Dec., Primary care clients assigned to enhanced care for depression not only experienced significantly more depression-free days compared with usual care clients, but cost the health plan significantly less ($568 vs -$12 in incremental costs; P <.001). Katherine Rost, Cost-Effectiveness of Enhancing Primary Care Depression Management on an Ongoing Basis, 2005, Annals of Family Medicine 3: Johns Hopkins HealthCare examined the first 12 months of claims histories of 603 adult Medicaid enrollees who frequently used medical services and had a recent history of substance abuse. An intervention group of 400 was targeted for management by substance abuse coordinators and nurse care managers who received training in the integration of medical case management and substance abuse services. The training included mock interviews, lectures, and case conferences on substance abuse topics. A comparison group of 203 members received routine care in the form of separate outreach from substance abuse coordinators and care managers. Early results indicate that the intervention group reduced medical costs by $122 per member per month as compared to an increase in the comparison group. The intervention group s cost reductions were realized through a decrease of 288 admissions per 1,000 members as well as a decrease in 92 days admitted per 1,000 members. Moreover, the intervention group experienced increased enrollment in substance abuse treatment and case management, which appropriately offset some of the savings from hospital utilization. In all, the PMPM cost reductions among intervention group members totaled $503,616 through the first year of the program, relative to baseline. see Johns Hopkins Healthcare: Demonstrating a Return on Investment for Integrated Substance Abuse and Treatment Though the a primary care depression management intervention added to the total care costs the first year of operation, these costs were largely off-set by general health care savings during the second year. The intervention produced health and mental health improvements without a significant increase in costs. Wayne Katon et al., Cost-effectiveness of Improving Primary Care Treatment of Late-Life Depression, Archives of General Psychiatry, 2005, 62. Patients participating in the IMPACT program for treating depression in primary care had lower mean total healthcare costs than usual care patients during a four year period. Jurgen Unutzer et al., Long-term Cost Effects of Collaborative Care for Late-life Depression, American Journal of Managed Care, Vol. 14, No. 2, 2008 Patients who receive care for depression in primary care clinics with routine mental health integration teams and care processes were 54% less likely to use higher-order emergency department services. Brenda Reiss- Brennan et al., Cost and Quality Impact of Intermountain s Mental Health Integration Program, Journal of Healthcare Management, 55:2, Primary care patients with diabetes and major depression assigned to an intervention program including education about depression, behavioral activation and and a choice between anti-depressant medication or problem-solving therapy had improved depression outcomes compared to the usual care group with no evidence of greater long-term costs. Wayne Katon et al., Long-Term Effects on Medical Costs of Improving Depression Outcomes in Patients with Depression and Diabetes:, Diabetes Care, Vol. 31, 2008 When comparing clients with the highest risk scores enrolled in patient-centered health homes (PCHM) vs. those not enrolled, the PCMH model was show to have a significant reduction in total costs in the first two years and significantly lower client admissions in the three years studied. Susannah Higgins et al., March, Published on-line


9 The Solution Primary Care 9
10 Integrated Care Definition Integration of behavioral health and physical health care refers to the intentional, ongoing, and committed coordination and collaboration among all providers and the individual in treatment. Providers recognize and appreciate the interdependence they have with each other and the patient/client to positively impact healthcare outcomes. (Agency for Health Care Research and Quality (AHRQ))

11 Different types of models for integrated behavioral health have challenges Referral BH Med Coordination/partnership Colocation BH Medical BH Medical
12 Key Features of Successful Models Communication: Warm handoffs vs. referrals Shift in scope and approach to practice: e.g., Consulting psychiatrist vs. extended evaluation with case load Coordination: e.g., PCP prescribing vs. two prescribers Engagement and Activation: Recovery orientation and patient self management skills Data driven care: e.g., Data and documentation sharing; outcome tracking
13 Two Roles of BH Providers Behavioral Health in Primary Care Food MH/SU Mart Behavioral Health Specialty Centers of Excellence Food MH/SU Mart PC Embedded mental health and substance use services in a primary care clinic with the ability to address needs of persons with mild to moderate behavioral health disorders PC A partner with medical homes, providing high value, whole healthoriented, specialty care to individuals with complex behavioral health conditions 13
14 Integrated Care is Moving in the Right Direction, but has Challenges Lack of knowledge and experience with value based purchasing (rather than volume) and connection to outcomes Disconnect between belief in recovery philosophy and expectations for patient outcomes Perceived and real barriers to data sharing Stigma towards patients with mental illness and addiction persists among medical providers creating barriers to access and treatment follow through 14
15 New Models of Care are Changing Faster than Work Force Supply & Preparedness Most providers receive limited training on working in teams; happens on the job MH provider shortages CA rural counties (OSHPD, 2011) Demand for MH/SU social workers is projected to increase by 22.8 percent and 35.4 percent, respectively, from 2006 to 2016 (California Employment Development Department) Medical and BH fields have distinctly different training programs, professional cultures, and treatment approaches. BH providers lag behind medical providers in their capacity to track treatment outcomes and use data for clinical decision making
16 Consumers feel stigmatized by health providers Orientation of primary care is reactive which deters clients reluctant or unable to seek help Physicians inexperienced in with mental health work may resist getting further involved with a client by not actively asking about symptoms (M. Phelan, 2001) Cramped schedules can limit time physicians have to discuss behavioral health issues with clients Subtle or not so subtle judgments and communication about patients mental health and substance use issues 16
17 17 Why stigma should matter to providers Issues with medication adherence Drop-outs and no shows Access Poor physical health outcomes Patient Experience: Key component and measure in the Triple Aim
18 18 IBH a Key Strategy for Improving Patient Experience Research evidence: IBH is an effective strategy to reduce stigma and improve access to behavioral health services, especially for vulnerable populations A 2005 IOM report concluded that the only way to achieve true quality and equality in the health care system is to integrated primary care with mental health and substance use services *Ivbijaro, G. & Funk, M. (2008.) No mental health without primary care. Mental Health in Family Medicine, 5(3), September, *Kautz C, Mauch D, and Smith S. Reimbursement of Mental health services in primary care settings. Rockville: Center for Mental Health Services, Substance Abuse and Mental Health Services Administration, 2008.
19 Changing Policy Landscape
20
21 Health Reform is Pushing for System Realignment to Reduce Costs Current Resource Allocation All things Inpatient and Institutional $ Prevention, Primary Care, BH Inpatient & Institutional Prevention, Early Intervention, Primary Care, and Behavioral Health $ Needed Resource Allocation 21
22 Examples of Changing Integrated Behavioral Health Policy Landscape Medi-Cal Expansion: Expanded role of MCOs and expanded population ACA Section 2703 Health Home Practice Transformation CA Medi-Cal 1115 Waiver Accountable Communities for Health 22
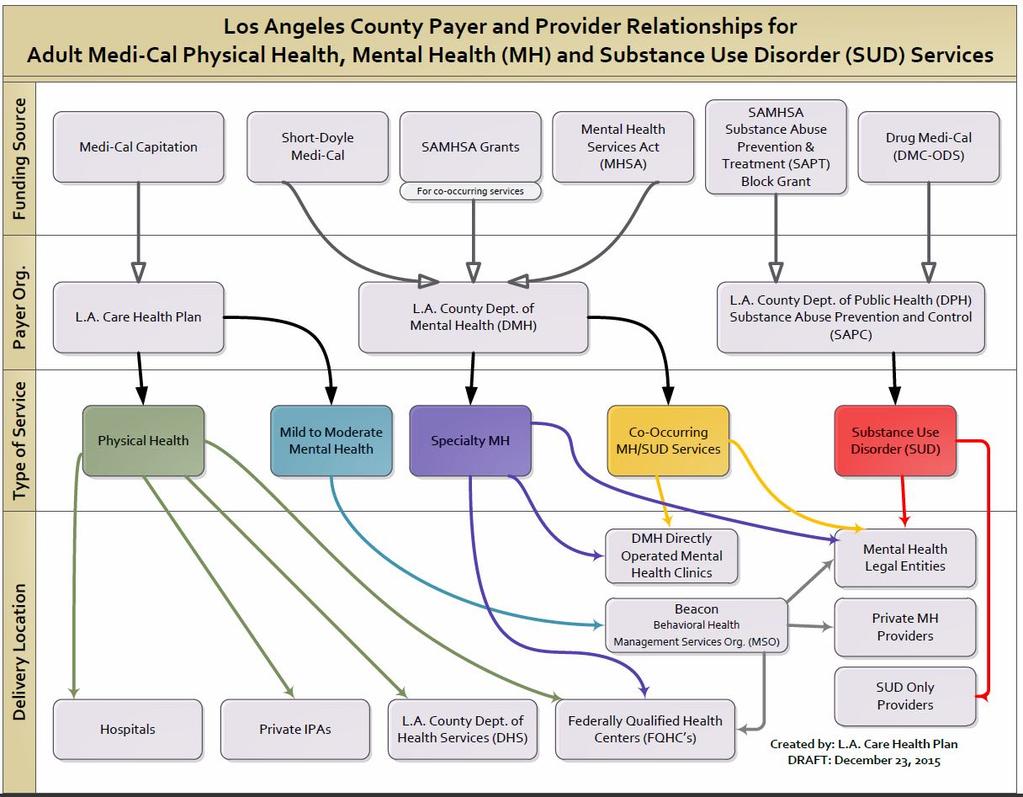
23 Medi-Cal Expansion and Expanded Benefit Started in 2014, but systems are still adjusting New relationships at the county level County Behavioral Health, Health Plans, Managed Behavioral Health Organizations (e.g., Beacon), FQHCs and CHCs Emphasis placed on care transitions and maintaining continuity of care e.g., hospital to community Acceleration of new integrated care delivery models, e.g. team-based care 23
24 ACA à Practice Transformation Integrated, Coordinated Care, e.g. Patient-Centered Medical Home (section 2703) o Growing awareness of the consequences of untreated mental health and SUD needs o Recognition of need for Integration/Person-Centered/Whole Person Care to achieve Triple Aim o Increased recognition of the role of housing; need to develop new partnerships with non-medical providers (Housing First) o Parity Implementation delayed in CA until 2018, but it s still important to invest in capacity and infrastructure 24
25 Medi-Cal 1115 Waiver Components Shift from fee-for-service to Global Payment Program for services to the uninsured in designated public hospital systems Delivery system transformation and alignment incentive program for public and municipal hospitals Whole Person Care Pilots to target more integrated care for high-risk, vulnerable populations 25
26 Challenges in the New Practice Environment Significant progress in practice and system transformation in CA and nationally that provide strong evidence base, BUT there are issues with sustainability and spread Infrastructure and workforce (and practice culture) challenges in achieving: ² Integrated, team based care with all members working to the top of their license, delegating activities to different team members, as appropriate ² Improved population management ² Better implementation and use of HIT, e.g., QI tracking of treatment outcomes ² Payment reform (e.g., value based purchasing) ² Shifting from data collection for compliance to using data for accountability 26
27 Key Reform Ingredient à Outcomes Measurement US behavioral health system is moving from 50 states (50 sets of rules) to a national quality framework for BH BUT there are currently many different quality measures relevant to BH (no clear consensus): o 116 in draft NBHQF o 64 in Meaningful Use set o 44 in the Physician Quality Reporting System o 37 in the SAMHSA State URS set o 28 in the FQHC UDS set 27
28 Changing the Frame: Collective Impact

29 Collective Impact is the commitment of a group of actors from different sectors to a common agenda for solving a specific social problem, using a structured form of collaboration. The Collective Impact Foundation Kania & Kramer, Collective Impact, Stanford Social Innovation Review,


30 Isolated Impact: The Collective Impact Foundation What we know Isolated Impact: o The prevailing model of health and human services in the US. o Historically promoted by payors and funders. o Has resulted in the development of over 1 million US nonprofit organizations devoted to isolated impact. Isolated Impact Definition: Efforts to effectively address a health or social problem by contracting with organizations thatspecialize in that particular problem. Problem: Complex Systems with many interconnected components do NOT respond well to isolated impact. Reality: The people, families, and communities you work with are the poster child of Complex Systems. 30





31 5 Collective Impact Components 31
32 Accountable Communities for Health Emerging strategy for improving population health ACHs integrate medical care, behavioral healthcare, and social service supports to improve the social determinants that shape health and wellbeing in a geographical area Collectively engage major healthcare providers across a geographic area to operate as partners rather than competitors Focuses on the health of all residents in a geographic area rather than just a patient panel New Initiative: The California Accountable Communities for Health Initiative (CACHI) will assess the feasibility, effectiveness, and potential value of a more expansive, connected and prevention-oriented health system 32
 Earlier Intervention Primary and Secondary Prevention Moderate Conditions Primary, Coordinated Care Chronic Health/High Utilizers Downstream High Need/Chroni c Conditions")
33 Snapshot of Interventions, Entry Points, & Population Health Community Clinical Wellness Interventions Smoking, Food Upstream Prevention Screening ACES SBIRT PHQ-9 Asthma and Diabetes Community Programs (schools, CBOs) Earlier Intervention Primary and Secondary Prevention Moderate Conditions Primary, Coordinated Care Chronic Health/High Utilizers Downstream High Need/Chroni c Conditions 33
34 The Work You Do is Essential All of this is new and nobody has the all the answers! The onus is on all of us to advance integrated primary care, mental health, substance use, and other personcentered services (e.g., dental, social services, and housing system of care). 34
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
Opportunities and Issues Related to BH Services in Primary Care
 Opportunities and Issues Related to BH Services in Primary Care Roger Kathol, MD, CPE President, Cartesian Solutions, Inc. Adjunct Professor, Internal Medicine & Psychiatry, University of Minnesota Clinical
Opportunities and Issues Related to BH Services in Primary Care Roger Kathol, MD, CPE President, Cartesian Solutions, Inc. Adjunct Professor, Internal Medicine & Psychiatry, University of Minnesota Clinical
MANAGING PATIENTS WITH COMPLEX CHRONIC CONDITIONS: HIGH UTILIZERS AND CARE TRANSITIONS
 MANAGING PATIENTS WITH COMPLEX CHRONIC CONDITIONS: HIGH UTILIZERS AND CARE TRANSITIONS Karen W. Linkins, PhD Principal, Desert Vista Consulting Assumptions about You and Your Organizations You are somewhere
MANAGING PATIENTS WITH COMPLEX CHRONIC CONDITIONS: HIGH UTILIZERS AND CARE TRANSITIONS Karen W. Linkins, PhD Principal, Desert Vista Consulting Assumptions about You and Your Organizations You are somewhere
Integrating Behavioral Health Across Integrated Delivery Systems
 Integrating Behavioral Health Across Integrated Delivery Systems Speaker Lori Raney, MD, Principal, Robin Henderson, PsyD, Chief Executive, Behavioral Health Providence Medical Group May 12, 2016 HealthManagement.com
Integrating Behavioral Health Across Integrated Delivery Systems Speaker Lori Raney, MD, Principal, Robin Henderson, PsyD, Chief Executive, Behavioral Health Providence Medical Group May 12, 2016 HealthManagement.com
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective
 Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
The Business Case for Bidirectional Integrated Care Mental Health and Substance Use Services in Primary Care Settings and Primary Care Services in
 The Business Case for Bidirectional Integrated Care Mental Health and Substance Use Services in Primary Care Settings and Primary Care Services in Specialty Mental Health and Substance Use Settings Prepared
The Business Case for Bidirectional Integrated Care Mental Health and Substance Use Services in Primary Care Settings and Primary Care Services in Specialty Mental Health and Substance Use Settings Prepared
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2
 Program Grantees: Part 2") SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Stigma and Attitudes Toward Working in Integrated Care
 Stigma and Attitudes Toward Working in Integrated Care INTEGRATED CARE WORKFORCE ISSUE BRIEF #1 June 2013 PRODUCED BY: CalMHSA Integrated Behavioral Health Project Karen W. Linkins, PhD, Jennifer J. Brya,
Stigma and Attitudes Toward Working in Integrated Care INTEGRATED CARE WORKFORCE ISSUE BRIEF #1 June 2013 PRODUCED BY: CalMHSA Integrated Behavioral Health Project Karen W. Linkins, PhD, Jennifer J. Brya,
Community Health Centers (CHCs)
") Health Policy Brief May 2014 Ready for ACA? How Community Health Centers Are Preparing for Health Care Reform Nadereh Pourat, Max W. Hadler Two in five CHCs have made significant progress toward ACA readiness.
Health Policy Brief May 2014 Ready for ACA? How Community Health Centers Are Preparing for Health Care Reform Nadereh Pourat, Max W. Hadler Two in five CHCs have made significant progress toward ACA readiness.
Overview. Improving Chronic Care: Integrating Mental Health and Physical Health Care in State Programs. Mental Health Spending
 Improving Chronic Care: Integrating Mental Health and Physical Health Care in State Programs Barbara Coulter Edwards bedwards@healthmanagement.com NCSL Winter CHAPS Meeting December 4, 2006 Overview Current
Improving Chronic Care: Integrating Mental Health and Physical Health Care in State Programs Barbara Coulter Edwards bedwards@healthmanagement.com NCSL Winter CHAPS Meeting December 4, 2006 Overview Current
Person Centered Agenda
 1 Person Centered Agenda Initial Confusion Overwhelmed by Statistics and Acronyms Dramatic Engagement of Issue Extreme Interest and Curiosity Deep Sense of Relief SAMHSA S STRATEGIC INITIATIVES Leading
1 Person Centered Agenda Initial Confusion Overwhelmed by Statistics and Acronyms Dramatic Engagement of Issue Extreme Interest and Curiosity Deep Sense of Relief SAMHSA S STRATEGIC INITIATIVES Leading
Best Management Practices In Integrated Behavioral Health/Primary Care Programs
 Best Management Practices In Integrated Behavioral Health/Primary Care Programs The 2017 OPEN MINDS Strategy & Innovation Institute Wednesday, June 7, 2017 2:00pm 3:15pm Steve Ramsland, Ed.D., Senior Associate,
Best Management Practices In Integrated Behavioral Health/Primary Care Programs The 2017 OPEN MINDS Strategy & Innovation Institute Wednesday, June 7, 2017 2:00pm 3:15pm Steve Ramsland, Ed.D., Senior Associate,
Integrated Mental Health Care. Questions
 Integrated Mental Health Care Closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Questions Due to the large number of participants, it is not practical to take questions over
Integrated Mental Health Care Closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Questions Due to the large number of participants, it is not practical to take questions over
Transdisciplinary Care: Opportunities and Challenges for Behavioral Health Providers
 Transdisciplinary Care: Opportunities and Challenges for Behavioral Health Providers Virna Little Journal of Health Care for the Poor and Underserved, Volume 21, Number 4, November 2010, pp. 1103-1107
Transdisciplinary Care: Opportunities and Challenges for Behavioral Health Providers Virna Little Journal of Health Care for the Poor and Underserved, Volume 21, Number 4, November 2010, pp. 1103-1107
State Policy Report #47. October Health Center Payment Reform: State Initiatives to Meet the Triple Aim. Introduction
 Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM. Bluebonnet Trails Community Services
 TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
Specialty Behavioral Health and Integrated Services
 Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Section 2703: State Option to Provide Health Homes for Enrollees with Chronic Conditions
 Section 2703: State Option to Provide Health Homes for Enrollees with Chronic Conditions Center for Medicaid, CHIP, and Survey & Certification Centers for Medicare & Medicaid Services Background. A goal
Section 2703: State Option to Provide Health Homes for Enrollees with Chronic Conditions Center for Medicaid, CHIP, and Survey & Certification Centers for Medicare & Medicaid Services Background. A goal
Behavioral Health Division JPS Health Network
 Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
I. Coordinating Quality Strategies Across Managed Care Plans
 Jennifer Kent Director California Department of Health Care Services 1501 Capitol Avenue Sacramento, CA 95814 SUBJECT: California Department of Health Care Services Medi-Cal Managed Care Quality Strategy
Jennifer Kent Director California Department of Health Care Services 1501 Capitol Avenue Sacramento, CA 95814 SUBJECT: California Department of Health Care Services Medi-Cal Managed Care Quality Strategy
Improving Health Status through Behavioral Health Interventions
 Comorbidity in the Dual Eligible Population: Improving Health Status through Behavioral Health Interventions PREPARED FOR THE CALIFORNIA ASSOCIATION OF HEALTH PLANS 2013 SEMINAR SERIES JUNE 25, 2013 BEACON
Comorbidity in the Dual Eligible Population: Improving Health Status through Behavioral Health Interventions PREPARED FOR THE CALIFORNIA ASSOCIATION OF HEALTH PLANS 2013 SEMINAR SERIES JUNE 25, 2013 BEACON
The Future of Delivery System Reform in Medi-Cal: Moving Medi-Cal Forward
 The Future of Delivery System Reform in Medi-Cal: Moving Medi-Cal Forward Cindy Mann Partner Manatt Health July 13, 2016 Agenda 2 Project Overview Medi-Cal Today Vision for the Future of Medi-Cal Near
The Future of Delivery System Reform in Medi-Cal: Moving Medi-Cal Forward Cindy Mann Partner Manatt Health July 13, 2016 Agenda 2 Project Overview Medi-Cal Today Vision for the Future of Medi-Cal Near
Caring for the Underserved - Innovative Pharmacy Practice Integration
 Caring for the Underserved - Innovative Pharmacy Practice Integration Sarah T. Melton, PharmD, BCPP, BCACP, FASCP Associate Professor Pharmacy Practice Clinical Pharmacist, Johnson City Community Health
Caring for the Underserved - Innovative Pharmacy Practice Integration Sarah T. Melton, PharmD, BCPP, BCACP, FASCP Associate Professor Pharmacy Practice Clinical Pharmacist, Johnson City Community Health
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
The Budget: Maximizing Federal Reimbursement For Parolee Mental Health Care Summary
 The 2013-14 Budget: Maximizing Federal Reimbursement For Parolee Mental Health Care MAC Taylor Legislative Analyst MAY 6, 2013 Summary Historically, the state has spent tens of millions of dollars annually
The 2013-14 Budget: Maximizing Federal Reimbursement For Parolee Mental Health Care MAC Taylor Legislative Analyst MAY 6, 2013 Summary Historically, the state has spent tens of millions of dollars annually
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Targeting Readmissions:
 Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
INVESTING IN INTEGRATED CARE
 INVESTING IN INTEGRATED CARE The Maine Health Access Foundation s 12 year journey (2005 2016) to improve patient centered care in Maine through the Integrated Care Initiative. Table of Contents The MeHAF
INVESTING IN INTEGRATED CARE The Maine Health Access Foundation s 12 year journey (2005 2016) to improve patient centered care in Maine through the Integrated Care Initiative. Table of Contents The MeHAF
 Relationships: The Behavioral Health Consultant, Primary Care Physician, and Psychiatrist i t Healthcare Integration Webinar National Council for Community Behavioral Healthcare February 25, 2010 The Status
Relationships: The Behavioral Health Consultant, Primary Care Physician, and Psychiatrist i t Healthcare Integration Webinar National Council for Community Behavioral Healthcare February 25, 2010 The Status
Evidence Based Practice: The benefits and challenges of behavioral health services in primary care settings.
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Evidence Based Practice: The benefits and challenges of behavioral health services in primary care settings.
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Evidence Based Practice: The benefits and challenges of behavioral health services in primary care settings.
Objectives. Models of Integrated Behavioral Health Care 9/23/2015
 Models of Integrated Behavioral Health Care Carlton D. Craig, Ph.D. Vernon R. Wiehe Endowed Professor in Family Violence University of Kentucky College of Social Work Carlton.craig@uky.edu (859)-257-6657
Models of Integrated Behavioral Health Care Carlton D. Craig, Ph.D. Vernon R. Wiehe Endowed Professor in Family Violence University of Kentucky College of Social Work Carlton.craig@uky.edu (859)-257-6657
The Integration of Behavioral Health and Primary Care: A Leadership Perspective
 The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
Value-Based Payment Model Designs for Behavioral Health Services in Primary Care
 Value-Based Payment Model Designs for Behavioral Health Services in Primary Care Using collaborative depression care management as a case study due to existing evidence, experience, and measures Robert
Value-Based Payment Model Designs for Behavioral Health Services in Primary Care Using collaborative depression care management as a case study due to existing evidence, experience, and measures Robert
The Minnesota Accountable Health Model
 The Minnesota Accountable Health Model L E A R N I N G S F R O M S I M : I N T E G R AT I O N O F P R I M A R Y A N D B E H AV I O R A L H E A LT H R U R A L H E A LT H C O N F E R E N C E J U N E 2 0,
The Minnesota Accountable Health Model L E A R N I N G S F R O M S I M : I N T E G R AT I O N O F P R I M A R Y A N D B E H AV I O R A L H E A LT H R U R A L H E A LT H C O N F E R E N C E J U N E 2 0,
Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies
 Improvement Strategies") Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies 1. What efforts and/or strategies have you put in place to improve your plans performance on the Follow-Up After Hospitalization
Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies 1. What efforts and/or strategies have you put in place to improve your plans performance on the Follow-Up After Hospitalization
FOLLOW UP STUDY OF HEALTHFIRST SENIOR MEMBERS WITH DIAGNOSES OF DIABETES AND DEPRESSION
 FOLLOW UP STUDY OF HEALTHFIRST SENIOR MEMBERS WITH DIAGNOSES OF DIABETES AND DEPRESSION Deborah Brotman, MD, FACP Chief Medical Officer FEGS Health & Human Services Monday, November 4, 2013 Inspiring Success
FOLLOW UP STUDY OF HEALTHFIRST SENIOR MEMBERS WITH DIAGNOSES OF DIABETES AND DEPRESSION Deborah Brotman, MD, FACP Chief Medical Officer FEGS Health & Human Services Monday, November 4, 2013 Inspiring Success
Innovative Coordinated Care Models
 Innovative Coordinated Care Models Rachel Post, LCSW Policy Director Central City Concern Rachel Solotaroff, MD, MCR Medical Director Central City Concern 1 May 2014 Central City Concern: Who we are Providing
Innovative Coordinated Care Models Rachel Post, LCSW Policy Director Central City Concern Rachel Solotaroff, MD, MCR Medical Director Central City Concern 1 May 2014 Central City Concern: Who we are Providing
The Affordable Care Act, HRSA, and the Integration of Behavioral Health Services
 The Affordable Care Act, HRSA, and the Integration of Behavioral Health Services Indiana Council of Community Mental Health Centers Ft. Wayne, Indiana May 19, 2011 David B. Bingaman, LCSW, ACSW U.S. Department
The Affordable Care Act, HRSA, and the Integration of Behavioral Health Services Indiana Council of Community Mental Health Centers Ft. Wayne, Indiana May 19, 2011 David B. Bingaman, LCSW, ACSW U.S. Department
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH
 INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
ACOs & Chronic Care Management: Opportunities For Behavioral Health Organizations In Population Health Management
 ACOs & Chronic Care Management: Opportunities For Behavioral Health Organizations In Population Health Management The 2017 OPEN MINDS Strategy & Innovation Institute Tuesday, June 6, 2017 11:45am 1:00pm
ACOs & Chronic Care Management: Opportunities For Behavioral Health Organizations In Population Health Management The 2017 OPEN MINDS Strategy & Innovation Institute Tuesday, June 6, 2017 11:45am 1:00pm
Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it
 Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it CAPT Hernan Reyes, MD Deputy Regional Administrator, HRSA Region 6 July 13, 2016 Objectives Understand the role of HRSA within
Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it CAPT Hernan Reyes, MD Deputy Regional Administrator, HRSA Region 6 July 13, 2016 Objectives Understand the role of HRSA within
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care
 Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
PHCPI framework: Presentation Crosswalk to Service Delivery Elements
 PHCPI framework: Presentation Crosswalk to Service Delivery Elements C. Service Delivery America s Federally Qualified Health Centers (FQHC) Program David Stevens, MD, FAAFP George Washington University
PHCPI framework: Presentation Crosswalk to Service Delivery Elements C. Service Delivery America s Federally Qualified Health Centers (FQHC) Program David Stevens, MD, FAAFP George Washington University
Colorado s Health Care Safety Net
 PRIMER Colorado s Health Care Safety Net The same is true for Colorado s health care safety net, the network of clinics and providers that care for the most vulnerable residents. The state s safety net
PRIMER Colorado s Health Care Safety Net The same is true for Colorado s health care safety net, the network of clinics and providers that care for the most vulnerable residents. The state s safety net
Creating the Collaborative Care Team
 Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Integration Forum Workforce Committee
 Integration Forum Workforce Committee May 27, 2016 Phone: 866-740-1260 Access Code: 3185489 Chairs: Yumi Jarris (Georgetown University School of Medicine) Randy Wykoff (East Tennessee State University)
Integration Forum Workforce Committee May 27, 2016 Phone: 866-740-1260 Access Code: 3185489 Chairs: Yumi Jarris (Georgetown University School of Medicine) Randy Wykoff (East Tennessee State University)
THE AFFORDABLE CARE ACT: OPPORTUNITIES FOR SOCIAL WORK PRACTICE IN INTEGRATED CARE SETTINGS. Suzanne Daub, LCSW April 22, 2014
 THE AFFORDABLE CARE ACT: OPPORTUNITIES FOR SOCIAL WORK PRACTICE IN INTEGRATED CARE SETTINGS Suzanne Daub, LCSW April 22, 2014 Agenda Why integrate primary care and behavioral health? Define integrated
THE AFFORDABLE CARE ACT: OPPORTUNITIES FOR SOCIAL WORK PRACTICE IN INTEGRATED CARE SETTINGS Suzanne Daub, LCSW April 22, 2014 Agenda Why integrate primary care and behavioral health? Define integrated
INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE
 THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
Beacon Health Strategies Primary Care Provider Training
 Beacon Health Strategies Primary Care Provider Training REFERRAL AND RESOURCE GUIDE Updated June 2015 BEACON HEALTH STRATEGIES beaconhealthstrategies.com June 15, 2015 1 Agenda 1. Review Medi-Cal Managed
Beacon Health Strategies Primary Care Provider Training REFERRAL AND RESOURCE GUIDE Updated June 2015 BEACON HEALTH STRATEGIES beaconhealthstrategies.com June 15, 2015 1 Agenda 1. Review Medi-Cal Managed
Health Center Strong:
 Health Center Strong: Developing and Expressing Health Center Value Jonathan Chapman Director, CHC Advisory Services, Capital Link NHCHC National Conference and Policy Symposium May 18, 2018 1 Capital
Health Center Strong: Developing and Expressing Health Center Value Jonathan Chapman Director, CHC Advisory Services, Capital Link NHCHC National Conference and Policy Symposium May 18, 2018 1 Capital
MassHealth Initiatives:
 MassHealth Initiatives: PCMHI, DUALS, PCC/BH Integration, PCPR Dr. Julian Harris CBHI and CYF Advisory Committee Joint Meeting November 5, 2012 Our Mission To improve the health outcomes of our diverse
MassHealth Initiatives: PCMHI, DUALS, PCC/BH Integration, PCPR Dr. Julian Harris CBHI and CYF Advisory Committee Joint Meeting November 5, 2012 Our Mission To improve the health outcomes of our diverse
Mild-to-Moderate Mental Health Coverage in Medi-Cal: The Challenge and Promise of Coordination between Counties and Health Plans
 Advancing innovations in health care delivery for low-income Americans Mild-to-Moderate Mental Health Coverage in Medi-Cal: The Challenge and Promise of Coordination between Counties and Health Plans December
Advancing innovations in health care delivery for low-income Americans Mild-to-Moderate Mental Health Coverage in Medi-Cal: The Challenge and Promise of Coordination between Counties and Health Plans December
Implementing Healthcare Reform: How Are we Going to Get Paid Tomorrow?
 Implementing Healthcare Reform: How Are we Going to Get Paid Tomorrow? National Council Public Policy Committee Tuesday, June 29,2010 Dale Jarvis, CPA MCPP Healthcare Consulting, Inc. dale@mcpp.net.com
Implementing Healthcare Reform: How Are we Going to Get Paid Tomorrow? National Council Public Policy Committee Tuesday, June 29,2010 Dale Jarvis, CPA MCPP Healthcare Consulting, Inc. dale@mcpp.net.com
Brian E. Sandoval, Psy.D. Primary Care Behavioral Health Manager Yakima Valley Farm Workers Clinic
 Clinical Integration of Behavioral Health in Washington State: The Development of Practice Standards for Primary Care Service Delivery Brian E. Sandoval, Psy.D. Primary Care Behavioral Health Manager Yakima
Clinical Integration of Behavioral Health in Washington State: The Development of Practice Standards for Primary Care Service Delivery Brian E. Sandoval, Psy.D. Primary Care Behavioral Health Manager Yakima
A. PCMH Service Site: 1. Co-locate behavioral health services at primary care practice sites. All participating primary
 Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
VSHP/ Behavioral Health
 VSHP/ Behavioral Health Deb Dukes & Dr Kelly Askins The contact numbers in the presentation apply to WEST Member Services ONLY. New numbers for EAST Member Services will be published and distributed by
VSHP/ Behavioral Health Deb Dukes & Dr Kelly Askins The contact numbers in the presentation apply to WEST Member Services ONLY. New numbers for EAST Member Services will be published and distributed by
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
From Fragmentation to Integration: Bringing Medical Care and HCBS Together. Jessica Briefer French Senior Research Scientist
 From Fragmentation to Integration: Bringing Medical Care and HCBS Together Jessica Briefer French Senior Research Scientist 1 Integration: The Holy Grail? An act or instance of combining into an integral
From Fragmentation to Integration: Bringing Medical Care and HCBS Together Jessica Briefer French Senior Research Scientist 1 Integration: The Holy Grail? An act or instance of combining into an integral
Overview of Medicaid. and the 1115 Medicaid Transformation Waiver. Opportunities for Supportive Housing Providers and Tenants August 2, 2016
 Overview of Medicaid and the 1115 Medicaid Transformation Waiver Opportunities for Supportive Housing Providers and Tenants August 2, 2016 Speaker Carol Wilkins, MPP Consultant carol.wilkins.ca@gmail.com
Overview of Medicaid and the 1115 Medicaid Transformation Waiver Opportunities for Supportive Housing Providers and Tenants August 2, 2016 Speaker Carol Wilkins, MPP Consultant carol.wilkins.ca@gmail.com
Health Center Program Update
 Health Center Program Update NACHC Policy & Issues Forum March 14, 2018 Jim Macrae Associate Administrator, Bureau of Primary Health Care (BPHC) Health Resources and Services Administration (HRSA) 3/22/2018
Health Center Program Update NACHC Policy & Issues Forum March 14, 2018 Jim Macrae Associate Administrator, Bureau of Primary Health Care (BPHC) Health Resources and Services Administration (HRSA) 3/22/2018
MEDI-CAL MANAGED CARE OVERVIEW
 MEDI-CAL MANAGED CARE OVERVIEW July 2018 Sandy Damiano, PhD Deputy Director DHS Primary Health Eligibility & Enrollment Apply for Medi-Cal year round: County Department of Human Assistance (DHA) Online,
MEDI-CAL MANAGED CARE OVERVIEW July 2018 Sandy Damiano, PhD Deputy Director DHS Primary Health Eligibility & Enrollment Apply for Medi-Cal year round: County Department of Human Assistance (DHA) Online,
Evaluation of the CMSP Behavioral Health Pilot Project. Final Report. Prepared for: CMSP Governing Board. Submitted by: The Lewin Group
 Prepared for: CMSP Governing Board Submitted by: The Lewin Group Date: February 17, 2011 Table of Contents ACKNOWLEDGEMENTS... III REPORT SUMMARY... 1 A. Introduction & Background... 1 B. Evaluation Methods...
Prepared for: CMSP Governing Board Submitted by: The Lewin Group Date: February 17, 2011 Table of Contents ACKNOWLEDGEMENTS... III REPORT SUMMARY... 1 A. Introduction & Background... 1 B. Evaluation Methods...
NYS Value Based Payments (VBP):
:") NYS Value Based Payments (VBP): Provider Associations, Community Based Organizations, and Consumer Advocates Town Hall Meeting Jason Helgerson NYS Medicaid Director December 16, 2016 2 Today s Agenda Agenda
NYS Value Based Payments (VBP): Provider Associations, Community Based Organizations, and Consumer Advocates Town Hall Meeting Jason Helgerson NYS Medicaid Director December 16, 2016 2 Today s Agenda Agenda
ILLINOIS 1115 WAIVER BRIEF
 ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
9/13/2017. Integrated Behavioral Health (IBH) MHCF Focus Areas. A little about myself
 MHCF Focus Areas. A little about myself") Integrated Behavioral Health (IBH) 2017 www.mthcf.org Scott.Malloy@mthcf.org (406)451 7060 MHCF Focus Areas Three focus areas: 1. Behavioral Health o Integrated behavioral health initiative o Strengthening
Integrated Behavioral Health (IBH) 2017 www.mthcf.org Scott.Malloy@mthcf.org (406)451 7060 MHCF Focus Areas Three focus areas: 1. Behavioral Health o Integrated behavioral health initiative o Strengthening
HEALTH CARE TEAM SACRAMENTO S MENTAL HEALTH CRISIS
 Team Leader/Issue Contact: HEALTH CARE TEAM Laura Niznik Williams, UC Davis Health System, (916) 276-9078, ljniznik@ucdavis.edu SACRAMENTO S MENTAL HEALTH CRISIS Requested Action: Evaluate the Institutions
Team Leader/Issue Contact: HEALTH CARE TEAM Laura Niznik Williams, UC Davis Health System, (916) 276-9078, ljniznik@ucdavis.edu SACRAMENTO S MENTAL HEALTH CRISIS Requested Action: Evaluate the Institutions
Medi-Cal and the Safety Net California Association of Health Plans Seminar Series Medi-Cal at its Core
 Medi-Cal and the Safety Net California Association of Health Plans Seminar Series Medi-Cal at its Core August 3, 2017 Deborah Kelch Executive Director Insure the Uninsured Project 1 Safety-Net Definitions
Medi-Cal and the Safety Net California Association of Health Plans Seminar Series Medi-Cal at its Core August 3, 2017 Deborah Kelch Executive Director Insure the Uninsured Project 1 Safety-Net Definitions
Re-Engineering Healthcare Integration Programs (REHIP)
") Re-Engineering Healthcare Integration Programs (REHIP) Planning for Primary Care & Psychological Health Care Integration A DCoE-Funded Tri-Service Demonstration Project Report Documentation Page Form Approved
Re-Engineering Healthcare Integration Programs (REHIP) Planning for Primary Care & Psychological Health Care Integration A DCoE-Funded Tri-Service Demonstration Project Report Documentation Page Form Approved
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care
 An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
econsult Update: Utilizing Technology to Bridge the Integration Gap Christopher Benitez, MD Clayton Chau, MD, PhD Ricardo Mendoza, MD Gary Tsai, MD,
 econsult Update: Utilizing Technology to Bridge the Integration Gap Christopher Benitez, MD Clayton Chau, MD, PhD Ricardo Mendoza, MD Gary Tsai, MD, 2 Disclosure Drs. Benitez, Chau, Mendoza and Tsai have
econsult Update: Utilizing Technology to Bridge the Integration Gap Christopher Benitez, MD Clayton Chau, MD, PhD Ricardo Mendoza, MD Gary Tsai, MD, 2 Disclosure Drs. Benitez, Chau, Mendoza and Tsai have
Integrated Behavioral Health Services
 Integrated Behavioral Health Services Anitra Walker, LCSW Liz Frye, MD, MPH Integrated Behavioral Health Background SHLI Integrated Care Initiative started in July 2011 2 initial demonstration sites; Focus
Integrated Behavioral Health Services Anitra Walker, LCSW Liz Frye, MD, MPH Integrated Behavioral Health Background SHLI Integrated Care Initiative started in July 2011 2 initial demonstration sites; Focus
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
Behavioral Health and Alternative Payment: A (Non-Scientific) Progress Report. Stephanie Jordan Brown April 26, 2016
 Progress Report. Stephanie Jordan Brown April 26, 2016") Behavioral Health and Alternative Payment: A (Non-Scientific) Progress Report Stephanie Jordan Brown April 26, 2016 The prevalence and under-treatment of behavioral health disorders is well documented...
Behavioral Health and Alternative Payment: A (Non-Scientific) Progress Report Stephanie Jordan Brown April 26, 2016 The prevalence and under-treatment of behavioral health disorders is well documented...
RPC and OMH Collaborative Care Webinar. February 1, pm
 RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Managed Medi-Cal Behavioral Health Benefits. Alliance Board Meeting October 23, 2013
 Managed Medi-Cal Behavioral Health Benefits Alliance Board Meeting October 23, 2013 Purpose Discuss role of ACA in expanding benefits Review philosophy of integrated health care Review State policy process
Managed Medi-Cal Behavioral Health Benefits Alliance Board Meeting October 23, 2013 Purpose Discuss role of ACA in expanding benefits Review philosophy of integrated health care Review State policy process
MassHealth Restructuring Overview
 1 MassHealth Restructuring Overview State of the State, Assuring Access, Equity and Integrated Care Massachusetts League of Community Health Centers Marylou Sudders, Secretary Executive Office of Health
1 MassHealth Restructuring Overview State of the State, Assuring Access, Equity and Integrated Care Massachusetts League of Community Health Centers Marylou Sudders, Secretary Executive Office of Health
This study was funded by Mental Health Services Act funding. The study team and MRMIB wish to thank:
 Agenda Item 8.e. 9/15/10 Meeting Evaluation of Mental Health and Substance Abuse Services Provided by Health Plans in the Healthy Families Program Presented to MRMIB Board on September 15, 2010 APS Healthcare,
Agenda Item 8.e. 9/15/10 Meeting Evaluation of Mental Health and Substance Abuse Services Provided by Health Plans in the Healthy Families Program Presented to MRMIB Board on September 15, 2010 APS Healthcare,
Leveraging FQHCs in California s Behavioral Health Care Continuum
 Leveraging FQHCs in California s Behavioral Health Care Continuum Allie Budenz Associate Director of Quality Improvement California Primary Care Association abudenz@cpca.org Agenda About CPCA and FQHCs
Leveraging FQHCs in California s Behavioral Health Care Continuum Allie Budenz Associate Director of Quality Improvement California Primary Care Association abudenz@cpca.org Agenda About CPCA and FQHCs
Southern California Regional Implementation & Improvement Science Webinar Series Welcome to the Webinar
 Southern California Regional Implementation & Improvement Science Webinar Series Welcome to the Webinar Karen Coleman, PhD Research Scientist II Southern California Permanente Medical Group Thoughts about
Southern California Regional Implementation & Improvement Science Webinar Series Welcome to the Webinar Karen Coleman, PhD Research Scientist II Southern California Permanente Medical Group Thoughts about
Blending Behavioral Health and Primary Care. Cherokee Health Systems Clinical Model
 Blending Behavioral Health and Primary Care Cherokee Health Systems Clinical Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Our Mission To improve the quality
Blending Behavioral Health and Primary Care Cherokee Health Systems Clinical Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Our Mission To improve the quality
CCBHCs 101: Opportunities and Strategic Decisions Ahead
 CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
APNA 27th Annual Conference Session 3023: October 11, 2013
 Beth Phoenix, RN, PhD Aaron Miller, RN, MS, PMHNP Sherri Borden, RN, MS, ANP Matt Tierney, RN, MS, NP UCSF School of Nursing None of the presenters has any conflicts of interest to disclose Beth Phoenix,
Beth Phoenix, RN, PhD Aaron Miller, RN, MS, PMHNP Sherri Borden, RN, MS, ANP Matt Tierney, RN, MS, NP UCSF School of Nursing None of the presenters has any conflicts of interest to disclose Beth Phoenix,
2017 Quality Improvement Work Plan Summary
 Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Recovery Homes: Recovery and Health Homes under Health Care Reform
 Recovery Homes: Recovery and Health Homes under Health Care Reform 4/27/11 Richard H. Dougherty, Ph.D. DMA Health Strategies Challenges of health reform Increasing coverage Reducing costs of coverage Reducing
Recovery Homes: Recovery and Health Homes under Health Care Reform 4/27/11 Richard H. Dougherty, Ph.D. DMA Health Strategies Challenges of health reform Increasing coverage Reducing costs of coverage Reducing
Drug Medi-Cal Organized Delivery System (DMC-ODS) Waiver
 Waiver") Drug Medi-Cal Organized Delivery System (DMC-ODS) Waiver Medi-Cal Managed Care Advisory Committee Uma K. Zykofsky, LCSW Director, Behavioral Health Services Alcohol & Drug Administrator Waiver Authority
Drug Medi-Cal Organized Delivery System (DMC-ODS) Waiver Medi-Cal Managed Care Advisory Committee Uma K. Zykofsky, LCSW Director, Behavioral Health Services Alcohol & Drug Administrator Waiver Authority
Primary Care/Behavioral Health INTEGRATION. Neal Adams, MD MPH Deputy Director California Institute for Mental Health
 Primary Care/Behavioral Health INTEGRATION Neal Adams, MD MPH Deputy Director California Institute for Mental Health Why Integrate BH & PC? BH disorder burden is great BH and physical health problems are
Primary Care/Behavioral Health INTEGRATION Neal Adams, MD MPH Deputy Director California Institute for Mental Health Why Integrate BH & PC? BH disorder burden is great BH and physical health problems are
Integrating Primary Medical Care and Behavioral Health Services: The New Mexico SBIRT Experience
 Integrating Primary Medical Care and Behavioral Health Services: The New Mexico SBIRT Experience Ana Moseley, LISW, ACSW, Clinical Director Tom Peterson, Ph.D., Associate Clinical Director Arturo Gonzales,
Integrating Primary Medical Care and Behavioral Health Services: The New Mexico SBIRT Experience Ana Moseley, LISW, ACSW, Clinical Director Tom Peterson, Ph.D., Associate Clinical Director Arturo Gonzales,
Pediatric Behavioral Health: How to Improve Primary Care Coordination and Increase Access
 Population Health Advisor Pediatric Behavioral Health: How to Improve Primary Care Coordination and Increase Access Jasmaine McClain, PhD Senior Analyst, Research McClainJ@advisory.com 6 Introducing Population
Population Health Advisor Pediatric Behavioral Health: How to Improve Primary Care Coordination and Increase Access Jasmaine McClain, PhD Senior Analyst, Research McClainJ@advisory.com 6 Introducing Population
Reforming Health Care with Savings to Pay for Better Health
 Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Does The Chronic Care Model Work?
 Does The Chronic Care Model Work? A Chartbook created by the staff of: Improving Chronic Illness Care, At Group Health s s MacColl Institute Supported by The Robert Wood Johnson Foundation Grant # 48769
Does The Chronic Care Model Work? A Chartbook created by the staff of: Improving Chronic Illness Care, At Group Health s s MacColl Institute Supported by The Robert Wood Johnson Foundation Grant # 48769
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
California Program on Access to Care Findings
 C P A C February California Program on Access to Care Findings 2008 Increasing Health Care Access for the Medically Underserved in Four California Counties Annette Gardner, PhD, MPH Some of the most active
C P A C February California Program on Access to Care Findings 2008 Increasing Health Care Access for the Medically Underserved in Four California Counties Annette Gardner, PhD, MPH Some of the most active
Mental Health Care in California
 Mental Health Care in California August 20, 2014 Updated on November 24, 2014 California Program on Access to Care School of Public Health 50 University Hall Berkeley, CA 94720-7360 www.cpac.berkeley.edu
Mental Health Care in California August 20, 2014 Updated on November 24, 2014 California Program on Access to Care School of Public Health 50 University Hall Berkeley, CA 94720-7360 www.cpac.berkeley.edu
10/4/2017. County/FQHC Collaborations to Improve Behavioral Health Continuum of Care. FQHCs in SUD/SMH
 County/FQHC Collaborations to Improve Behavioral Health Continuum of Care Allie Budenz, MPA Associate Director of Quality Improvement, CPCA FQHCs in SUD/SMH California has a tri-furcated behavioral health
County/FQHC Collaborations to Improve Behavioral Health Continuum of Care Allie Budenz, MPA Associate Director of Quality Improvement, CPCA FQHCs in SUD/SMH California has a tri-furcated behavioral health