MANAGING PATIENTS WITH COMPLEX CHRONIC CONDITIONS: HIGH UTILIZERS AND CARE TRANSITIONS
|
|
|
- Mervyn Higgins
- 6 years ago
- Views:
Transcription

1 MANAGING PATIENTS WITH COMPLEX CHRONIC CONDITIONS: HIGH UTILIZERS AND CARE TRANSITIONS Karen W. Linkins, PhD Principal, Desert Vista Consulting
2 Assumptions about You and Your Organizations You are somewhere in the process of thinking about and addressing the issues of high utilization and care transitions You want to get paid for this work You d like to expand you knowledge in about models that work to increase the likelihood of success for your project! 2
3 Some New Numbers 70% of outpatient visits in CA involve behavioral healthrelated issues Nearly 70% of adults with BH conditions have one or more physical health issues Only 50% of those diagnosed with a MH condition receives treatment Only 10% of those diagnosed with a SUD receives treatment
4 Root Causes of Ineffective Care Transitions and High Utilization Communication breakdowns Expectations differ between senders and receivers of patients in transition Culture does not promote successful hand-off (e.g., lack of teamwork and respect) Inadequate amount of time provided for successful hand-off Lack of standardized procedures in conducting successful hand-off 4
5 Root Causes of Ineffective Care Transitions and High Utilization Accountability breakdowns No physician or clinical entity that takes responsibility to assure that the patient s health care is coordinated across various settings and among different providers Providers especially when multiple specialists are involved fail to coordinate care or communicate effectively, which creates confusion for the patient and others responsible for transitioning the care of the patient to the next setting or provider. Lack of information re: PCP/Clinic for hospital discharge planners No confirmation that sufficient knowledge and resources will be available at home or the next setting for the patient upon discharge. 5
6 Root Causes of Ineffective Care Transitions and High Utilization Patient education breakdowns Confusing medication regimens, unclear instructions about follow-up care Patients/caregivers not included in planning process Lack sufficient understanding of the medical condition or the plan or care Stigma that affects engagement of this population 6
7 Other Challenges Clinical/Service Capacity Individuals with AOD issues, criminal justice involved no real home anywhere (medical, BH or otherwise) Workforce capacity issues (recruitment of bilingual providers) Need for Open access and capacity to serve walk in clients Gaps between referral and connection to service: no designated point of contact for follow up across agencies involved Need for specific referral criteria and priority populations 7
8 More Challenges Data Capacity for shared care planning and follow up on referrals/client goals with different EMRs Tracking outcomes and using standard measures across systems Identifying and accessing what s needed to inform decision-making (financial, clinical, administrative) labor intensive and limited data analytic capacity Providers/staff need ongoing training to understand data sharing to support care coordination is not a violation of HIPAA Need consensus on data elements to share, format, and timeframes for information exchange and communication No designated point of contact across organizations to facilitate coordination and follow up 8

9 Collective Impact is the commitment of a group of actors from different sectors to a common agenda for solving a specific social problem, using a structured form of collaboration. The Collective Impact Foundation 9


10 The Collective Impact Foundation What we know Isolated Impact: The prevailing model of health and human services in the United States. Historically promoted by payors and funders. Has resulted in the development of over 1 million US nonprofit organizations devoted to isolated impact. Isolated Impact Definition: Efforts to effectively address a health or social problem by contracting with organizations that specialize in that particular problem. Problem: Complex Systems with many interconnected components do NOT respond well to isolated impact. Reality: The people, families, and communities you work with are the poster child of Complex Systems. 10




11 5 Collective Impact Components 11
12 National Models Numerous national models for health homes that emphasize the critical importance of care coordination for complex populations, e.g., NCQA PCMH 2014 Standards SAMHSA-HRSA Health Home Framework 2703 Health Home Models across US
13 Core Element of Integrated Care: Care Coordination Care coordination involves deliberately organizing patient care activities and sharing information among all of the participants concerned with a patient's care to achieve safer and more effective care. This means that the patient's needs and preferences are known ahead of time and communicated at the right time to the right people, and that this information is used to provide safe, appropriate, and effective care to the patient. 13 Source: Agency for Health Research and Quality (AHRQ)
14 Examples of broad care coordination approaches include: Establish Accountability Teamwork Care management Medication management Health information technology Patient-centered medical home


15 Care Coordination Functions Source: CIBHS Care Coordination Collaborative; Dr. Marc Avery, AIMS Center

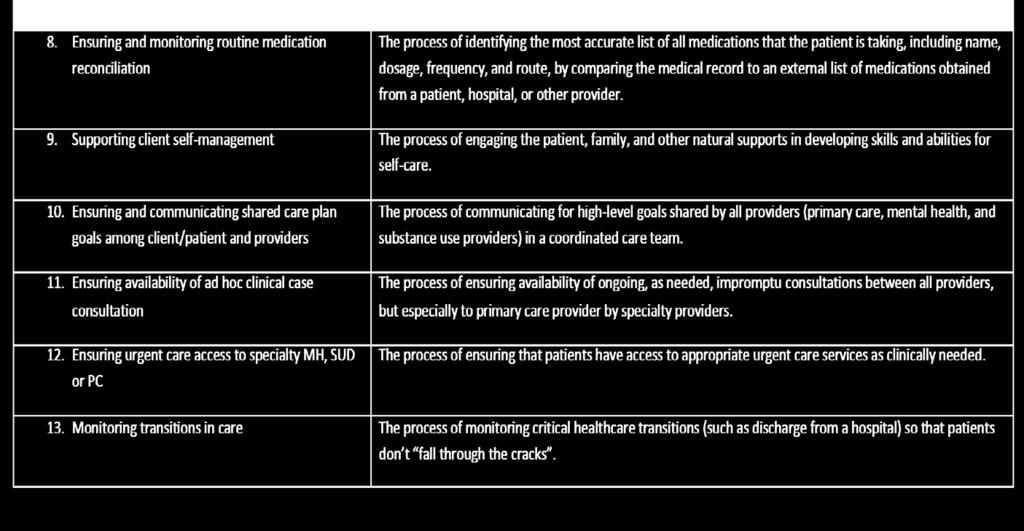
16 Care Coordination Functions (cont.)

17 #NatCon14 17
18 Activities of Integrated Behavioral Health Teams Health education materials covering the nature of the condition and the self-care, treatment and recovery Evidence driven, clinical treatment strategies Care coordination staff to coordinate and communicate between providers Psychiatric consultation and support for primary care on medication and other clinical conditions A preferred network of preferred, affiliated providers for other levels of inpatient, intermediate and specialty care Peer and recovery support Follow-up Health education Evidence driven treatment Care coordination Psychiatric consultation Network of preferred providers Peer and psychosocial support Follow-Up #NatCon14 18

19 Community Health Teams (The Vermont Blueprint for Health) Connect patients to primary care Track patients overdue for appointments or tests Help patients being discharged from hospitals Health and nutrition coaching 19 19
20 10 th Decile Project Los Angeles (CSH) Collaborative effort in LA County to connect frequent ED users to housing and appropriate care More than 25 organizations (5 Health Centers) in 6 neighborhood networks to address the needs of the top 10% highest cost, highest need Health Centers provide integrated PC/BH care Priority housing through the Coordinated Entry System for highest need individuals
,")
21 10 th Decile Project Los Angeles (CSH) Key Features: Targeting (top 10%) Triage Tool with an algorithm to identify individuals based on demographics and health status Collaboration homeless services, hospitals, and health centers Supportive Housing with rent subsidies through Section 8 or Shelter Plus Care vouchers Intensive Case Management by a health worker (sometimes at a health centers), providing management of referrals and clinical care, such as medication review (warm handoff) Care Coordination Linking individuals with primary and BH services and communicating with providers
22 Consumer Themes Providers need training on communication, listening and empathy to build trust and learn how to partner with the patient Prioritize greater attention and training on the impact of the social determinants to health as part of assessment and overall health service delivery Trained peer support specialists (by DMH) and advocates (CSH) are eager to partner with the health care sector to improve health outcomes for complex patients through outreach and system navigation This population is new to health care coverage and will need significant education on how to access services/benefits, communicate with providers, health plan and advocate for themselves Consumers want to be part of the broader health care workforce, with experience and skills to offer. They need to be part of the solution and the Team to achieve the desire outcomes of The Triple Aim 22
23 Consumer Themes (continued) Provide access to a health home in a primary care setting that s not the hospital ER Employ peers with lived experience as system navigators to work in all settings Need priority access to healthcare services (primary care, MH and SUD) and housing Bring the services to the people with whole person care staffed by integrated mobile care teams comprised of peer navigators and multi-disciplinary healthcare professionals Partner with providers that have long established, trusting relationships with homeless populations Implement one universal assessment, accessible across all providers, and data-sharing Facilitate pathways to access care through mobile integrated care teams linked to primary care, MH, SUD, housing 23
24 Priorities Make access easy, welcoming Communicate and coordinate Support the whole person Outreach and engage 24
25 Discussion Questions: How do you interface with your health plans, Beacon, the County for screening? How do you plan to increase visibility and presence in the community for outreach, engagement and follow up? What is the role of Beacon and Partnership Health Plan in care coordination efforts aimed at getting patients to the right level of care? What is the role of the hospitals and what is your current relationship with them? What is the identified target population (and N) for care coordination? Would there be a benefit for starting with a specific number of individuals to pilot test the current workflows and processes? What would it take to get dedicated staff at each agency to serve as the primary point of contact for cross-system coordination activities? How many referrals can each agency take based on caseload size and current capacity?
26 Additional Questions What screening/assessments are in place to identify MH needs of the high utilizers? Outcome measurement what tools are being used, what metrics are being tracked, frequency, populations and what is the current thinking on how to increase data analytics capacity? Is there any way that partner agencies can leverage the data analytic capacity available at the county? What is the current status of the ROI process with hospitals and other organizations? Are all providers across all agencies are on the same page?
Best Management Practices In Integrated Behavioral Health/Primary Care Programs
 Best Management Practices In Integrated Behavioral Health/Primary Care Programs The 2017 OPEN MINDS Strategy & Innovation Institute Wednesday, June 7, 2017 2:00pm 3:15pm Steve Ramsland, Ed.D., Senior Associate,
Best Management Practices In Integrated Behavioral Health/Primary Care Programs The 2017 OPEN MINDS Strategy & Innovation Institute Wednesday, June 7, 2017 2:00pm 3:15pm Steve Ramsland, Ed.D., Senior Associate,
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
LTC Discharge and Transfer Requirements. Revised October 24, 2017
 LTC Discharge and Transfer Requirements Revised October 24, 2017 OUTLINE Transitions of Care LTC Discharge and Transfer Documentation Requirements Intent of the Regulations TRANSITIONS OF CARE Understanding
LTC Discharge and Transfer Requirements Revised October 24, 2017 OUTLINE Transitions of Care LTC Discharge and Transfer Documentation Requirements Intent of the Regulations TRANSITIONS OF CARE Understanding
Stigma and Attitudes Toward Working in Integrated Care
 Stigma and Attitudes Toward Working in Integrated Care INTEGRATED CARE WORKFORCE ISSUE BRIEF #1 June 2013 PRODUCED BY: CalMHSA Integrated Behavioral Health Project Karen W. Linkins, PhD, Jennifer J. Brya,
Stigma and Attitudes Toward Working in Integrated Care INTEGRATED CARE WORKFORCE ISSUE BRIEF #1 June 2013 PRODUCED BY: CalMHSA Integrated Behavioral Health Project Karen W. Linkins, PhD, Jennifer J. Brya,
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives
 Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
CCBHC CARE COORDINATION AGREEMENTS: OVERVIEW OF LEGAL REQUIREMENTS AND CHECKLIST OF RECOMMENDED TERMS
 CCBHC CARE COORDINATION AGREEMENTS: OVERVIEW OF LEGAL REQUIREMENTS AND CHECKLIST OF RECOMMENDED TERMS Coordinating care across a spectrum of services, 29 including physical health, behavioral health, social
CCBHC CARE COORDINATION AGREEMENTS: OVERVIEW OF LEGAL REQUIREMENTS AND CHECKLIST OF RECOMMENDED TERMS Coordinating care across a spectrum of services, 29 including physical health, behavioral health, social
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH
 INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
See Protecting Access to Medicare Act (PAMA) 223(a)(2)(C), Pub. L. No (Apr. 1, 2014).
 223(a)(2)(C), Pub. L. No (Apr. 1, 2014).") CCBHC CARE COORDINATION AGREEMENTS: OVERVIEW OF LEGAL REQUIREMENTS AND CHECKLIST OF RECOMMENDED TERMS Coordinating care across a spectrum of services, 1 including physical health, behavioral health, social
CCBHC CARE COORDINATION AGREEMENTS: OVERVIEW OF LEGAL REQUIREMENTS AND CHECKLIST OF RECOMMENDED TERMS Coordinating care across a spectrum of services, 1 including physical health, behavioral health, social
DOMAIN/STEP 8: OFFER INTEGRATED, COMPLEX CARE MANAGEMENT Activities
 Phase II: Develop Integrated Complex Care Systems (Whole Health Homes) DOMAIN/STEP 8: OFFER INTEGRATED, COMPLEX CARE MANAGEMENT July - Oct 2016 Oct 2016 - Feb 2017 Feb - July 2017 Develop Complex Care
Phase II: Develop Integrated Complex Care Systems (Whole Health Homes) DOMAIN/STEP 8: OFFER INTEGRATED, COMPLEX CARE MANAGEMENT July - Oct 2016 Oct 2016 - Feb 2017 Feb - July 2017 Develop Complex Care
Medicaid Strategies: Data Sharing. csh.org. The Source for Housing Solutions. Sarah Gallagher, Director of Strategic Initiatives
 Medicaid Strategies: Data Sharing Sarah Gallagher, Director of Strategic Initiatives The Source for Housing Solutions csh.org Presentation Outline Why do we want to share data to target frequent users?
Medicaid Strategies: Data Sharing Sarah Gallagher, Director of Strategic Initiatives The Source for Housing Solutions csh.org Presentation Outline Why do we want to share data to target frequent users?
Dawn M. Graham, PhD Assistant Professor of Family Medicine Ohio University College of Osteopathic Medicine
 Dawn M. Graham, PhD Assistant Professor of Family Medicine Ohio University College of Osteopathic Medicine Jane Hamel-Lambert, PhD, MBA Associate Professor of Family Medicine Ohio University College of
Dawn M. Graham, PhD Assistant Professor of Family Medicine Ohio University College of Osteopathic Medicine Jane Hamel-Lambert, PhD, MBA Associate Professor of Family Medicine Ohio University College of
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Implementing Medicaid Behavioral Health Reform in New York
 Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York HIV Health and Human Services Planning Council of New York March 19, 2014 Agenda Goals Timeline BH Benefit
Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York HIV Health and Human Services Planning Council of New York March 19, 2014 Agenda Goals Timeline BH Benefit
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
AccessHealth Spartanburg
 TRANSFORMING COMPLEX CARE PROFILE AccessHealth Spartanburg Leveraging community partnerships to improve care for an uninsured population with complex health and social needs A ccesshealth Spartanburg (AHS)
TRANSFORMING COMPLEX CARE PROFILE AccessHealth Spartanburg Leveraging community partnerships to improve care for an uninsured population with complex health and social needs A ccesshealth Spartanburg (AHS)
Implementing Medicaid Behavioral Health Reform in New York
 Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York Conference of Local Mental Hygiene Directors November 19, 2013 Agenda Goals Timeline BH Benefit Design Overview
Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York Conference of Local Mental Hygiene Directors November 19, 2013 Agenda Goals Timeline BH Benefit Design Overview
Florida Department of Children and Families Office of Substance Abuse and Mental Health Care Coordination Rating System (Managing Entity)
") Florida Department of Children and Families Office of Substance Abuse and Mental Health Care Coordination Rating System (Managing Entity) Instructions: The checklist examines the core competencies of Care
Florida Department of Children and Families Office of Substance Abuse and Mental Health Care Coordination Rating System (Managing Entity) Instructions: The checklist examines the core competencies of Care
Whole-Community Cooperation Health by Design
 Whole-Community Cooperation Health by Design South King County Care Transitions Conference Marc Pierson June 4, 2015 From Prediction to Action Who is We? Where is Home? How long will you care? Anything
Whole-Community Cooperation Health by Design South King County Care Transitions Conference Marc Pierson June 4, 2015 From Prediction to Action Who is We? Where is Home? How long will you care? Anything
I. General Instructions
 Behavioral Health Services Mental Health (BHS-MH) A Division of Contra Costa Health Services (CCHS) Request for Qualifications Mental Health Services Act (MHSA) Master Leasing September 2013 I. General
Behavioral Health Services Mental Health (BHS-MH) A Division of Contra Costa Health Services (CCHS) Request for Qualifications Mental Health Services Act (MHSA) Master Leasing September 2013 I. General
KEY ELEMENTS STATUS EXPLAIN EVIDENCE SINGLE POINT OF ACCOUNTABILITY Serves as single point of accountability for the
 Florida Department of Children and Families Office of Substance Abuse and Mental Health Care Coordination Rating System (Provider) Instructions: The checklist examines the core competencies of Care Coordination
Florida Department of Children and Families Office of Substance Abuse and Mental Health Care Coordination Rating System (Provider) Instructions: The checklist examines the core competencies of Care Coordination
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Frequent Users Systems Engagement (FUSE)
") Frequent Users Systems Engagement (FUSE) Washtenaw County, MI April 2016 INITIATIVE OVERVIEW Bring together community partners from a variety of sectors to connect frequent users to housing, healthcare,
Frequent Users Systems Engagement (FUSE) Washtenaw County, MI April 2016 INITIATIVE OVERVIEW Bring together community partners from a variety of sectors to connect frequent users to housing, healthcare,
Making the Case and Making It Work: Integrating Behavioral Health into Primary Care
 LEARN MORE ibhpartners.org Making the Case and Making It Work: Integrating Behavioral Health into Primary Care Karen W. Linkins, PhD karen@desertvistaconsulting.com May 18, 2016 What we ll cover today
LEARN MORE ibhpartners.org Making the Case and Making It Work: Integrating Behavioral Health into Primary Care Karen W. Linkins, PhD karen@desertvistaconsulting.com May 18, 2016 What we ll cover today
Care Compact Guide Patient-Centered Specialty Care (PCSC) A Component of Medical Neighborhood Initiatives
 A Component of Medical Neighborhood Initiatives") Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
Systems Changes to Maximize the Impact of Supportive Housing on Ending Homelessness
 Systems Changes to Maximize the Impact of Supportive Housing on Ending Homelessness Matthew Doherty, Director of National Initiatives August 14, 2014 Roles of USICH Coordinates the Federal response to
Systems Changes to Maximize the Impact of Supportive Housing on Ending Homelessness Matthew Doherty, Director of National Initiatives August 14, 2014 Roles of USICH Coordinates the Federal response to
BH-TEDS What Are We Learning?
 MICHIGAN DEPARTMENT OF HEALTH & HUMAN SERVICES BH-TEDS What Are We Learning? P u t t i n g p e o p l e f i r s t, w i t h t h e g o a l o f h e l p i n g a l l M i c h i g a n d e r s l e a d h e a l t
MICHIGAN DEPARTMENT OF HEALTH & HUMAN SERVICES BH-TEDS What Are We Learning? P u t t i n g p e o p l e f i r s t, w i t h t h e g o a l o f h e l p i n g a l l M i c h i g a n d e r s l e a d h e a l t
Partnership HealthPlan of California Strategic Plan
 Partnership HealthPlan of California 2017 2020 Strategic Plan Partnership HealthPlan of California 2017 2020 Strategic Plan Message from the CEO While many of us have given up making predictions, myself
Partnership HealthPlan of California 2017 2020 Strategic Plan Partnership HealthPlan of California 2017 2020 Strategic Plan Message from the CEO While many of us have given up making predictions, myself
This report is a summary of the November 2015 Behavioral Health Stakeholder s Summit that was held in Fargo.
 This report is a summary of the November 2015 Behavioral Health Stakeholder s Summit that was held in Fargo. February 10, 2016 ADULT BEHAVIORAL HEALTH November 2015 Summary Report Exchange of information
This report is a summary of the November 2015 Behavioral Health Stakeholder s Summit that was held in Fargo. February 10, 2016 ADULT BEHAVIORAL HEALTH November 2015 Summary Report Exchange of information
Community Health Workers & Rural Health: Increasing Access, Improving Care Minnesota Rural Health Conference June 26, 2012
 Community Health Workers & Rural Health: Increasing Access, Improving Care Minnesota Rural Health Conference June 26, 2012 Joan Cleary, Interim Executive Director Minnesota Community Health Worker Alliance
Community Health Workers & Rural Health: Increasing Access, Improving Care Minnesota Rural Health Conference June 26, 2012 Joan Cleary, Interim Executive Director Minnesota Community Health Worker Alliance
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling
 Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Region 1 IDN. Integrated Delivery Network Region 1: Partnership for Integrated Care
 Region 1 IDN Integrated Delivery Network Region 1: Partnership for Integrated Care Region 1 IDN Request For Proposal Process The Region 1 IDN following a community driven process has elected to open all
Region 1 IDN Integrated Delivery Network Region 1: Partnership for Integrated Care Region 1 IDN Request For Proposal Process The Region 1 IDN following a community driven process has elected to open all
CCI Stakeholder Advisory Committee June 9, 2016 Go to: https://www.webmeeting.att.com Meeting Number: Participant Code: To join by
 CCI Stakeholder Advisory Committee June 9, 2016 Go to: https://www.webmeeting.att.com Meeting Number: 5114686455 Participant Code: 721811 To join by phone dial: 1800-230-1096 1 Contents of this presentation
CCI Stakeholder Advisory Committee June 9, 2016 Go to: https://www.webmeeting.att.com Meeting Number: 5114686455 Participant Code: 721811 To join by phone dial: 1800-230-1096 1 Contents of this presentation
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
 Care Model May 12, 2016") update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
Widespread prescribing, distribution and availability of naloxone for high risk individuals and as rescue medication 2
 Co Occurring Collaborative Serving Maine Expanding Medication Assisted Recovery Services & Building a Stronger Recovery Oriented System for SUD Treatment in Maine April 2018 Introduction: With support
Co Occurring Collaborative Serving Maine Expanding Medication Assisted Recovery Services & Building a Stronger Recovery Oriented System for SUD Treatment in Maine April 2018 Introduction: With support
Value Based Payment WHAT IS THIS ALL ABOUT?
 Value Based Payment WHAT IS THIS ALL ABOUT? 1 1 Agenda Welcome and Introductions RPC Introduction New York State s Vision Population Impacted What Does VBP Mean to Me as a BH Provider in NYS? What is Value
Value Based Payment WHAT IS THIS ALL ABOUT? 1 1 Agenda Welcome and Introductions RPC Introduction New York State s Vision Population Impacted What Does VBP Mean to Me as a BH Provider in NYS? What is Value
PCMH 2014 Quality Measurement and Improvement Worksheet
 PCMH 2014 Quality Measurement and Improvement Worksheet Purpose of the Quality Measurement and Improvement Worksheet To help practices organize the measures and quality improvement activities that are
PCMH 2014 Quality Measurement and Improvement Worksheet Purpose of the Quality Measurement and Improvement Worksheet To help practices organize the measures and quality improvement activities that are
I. General Instructions
 Contra Costa Behavioral Health Services Request for Proposals (RFP) Outpatient Mental Health Services September 30, 2015 I. General Instructions Contra Costa Behavioral Health Services (CCBHS, or the County)
Contra Costa Behavioral Health Services Request for Proposals (RFP) Outpatient Mental Health Services September 30, 2015 I. General Instructions Contra Costa Behavioral Health Services (CCBHS, or the County)
MassHealth Accountable Care Update
 MassHealth Accountable Care Update Marylou Sudders Secretary Executive Office of Health & Human Services May 16, 2018 Partnering with CHCs: In it together! Community health centers have been providing
MassHealth Accountable Care Update Marylou Sudders Secretary Executive Office of Health & Human Services May 16, 2018 Partnering with CHCs: In it together! Community health centers have been providing
A. PCMH Service Site: 1. Co-locate behavioral health services at primary care practice sites. All participating primary
 Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
A Hear from Your Peers Webinar Effective Coordination between Hospitals and CoC Homeless Assistance Providers Results in Improved Residential
 A Hear from Your Peers Webinar Effective Coordination between Hospitals and CoC Homeless Assistance Providers Results in Improved Residential Stability and Reduced Costs Webinar Format Our Webinar Format:
A Hear from Your Peers Webinar Effective Coordination between Hospitals and CoC Homeless Assistance Providers Results in Improved Residential Stability and Reduced Costs Webinar Format Our Webinar Format:
Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion. All Ohio Institute on Community Psychiatry March 25, 2017
 Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion All Ohio Institute on Community Psychiatry March 25, 2017 SBIRT Panelists: Introduction Ellen Augsperger Director of Ohio SBIRT
Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion All Ohio Institute on Community Psychiatry March 25, 2017 SBIRT Panelists: Introduction Ellen Augsperger Director of Ohio SBIRT
Specialty Behavioral Health and Integrated Services
 Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
PLACEMENT OPENINGS: Two Post-Doctoral Residency positions are available for our Integrated Behavioral Health track
 San Mateo Medical Center Medical Psychiatry Services 222 W. 39 th Ave. San Mateo, CA 94403 (650)573-2760 PLACEMENT OPENINGS: Two Post-Doctoral Residency positions are available for our Integrated Behavioral
San Mateo Medical Center Medical Psychiatry Services 222 W. 39 th Ave. San Mateo, CA 94403 (650)573-2760 PLACEMENT OPENINGS: Two Post-Doctoral Residency positions are available for our Integrated Behavioral
The Michigan Primary Care Transformation (MiPCT) Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting
 Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting") The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
Leveraging FQHCs in California s Behavioral Health Care Continuum
 Leveraging FQHCs in California s Behavioral Health Care Continuum Allie Budenz Associate Director of Quality Improvement California Primary Care Association abudenz@cpca.org Agenda About CPCA and FQHCs
Leveraging FQHCs in California s Behavioral Health Care Continuum Allie Budenz Associate Director of Quality Improvement California Primary Care Association abudenz@cpca.org Agenda About CPCA and FQHCs
econsult Update: Utilizing Technology to Bridge the Integration Gap Christopher Benitez, MD Clayton Chau, MD, PhD Ricardo Mendoza, MD Gary Tsai, MD,
 econsult Update: Utilizing Technology to Bridge the Integration Gap Christopher Benitez, MD Clayton Chau, MD, PhD Ricardo Mendoza, MD Gary Tsai, MD, 2 Disclosure Drs. Benitez, Chau, Mendoza and Tsai have
econsult Update: Utilizing Technology to Bridge the Integration Gap Christopher Benitez, MD Clayton Chau, MD, PhD Ricardo Mendoza, MD Gary Tsai, MD, 2 Disclosure Drs. Benitez, Chau, Mendoza and Tsai have
October 5 th & 6th, The Managed Care Technical Assistance Center of New York
 October 5 th & 6th, 2015 The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation, and educational resource center that offers resources to all mental health
October 5 th & 6th, 2015 The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation, and educational resource center that offers resources to all mental health
Effective Care for High-Need, High-Cost Patients: How to Maximize Prevention and Population Health Efforts
 Effective Care for High-Need, High-Cost Patients: How to Maximize Prevention and Population Health Efforts May 9, 2018 www.hcttf.org 1 Speakers Jeff Micklos Executive Director HCTTF Kelly McCracken National
Effective Care for High-Need, High-Cost Patients: How to Maximize Prevention and Population Health Efforts May 9, 2018 www.hcttf.org 1 Speakers Jeff Micklos Executive Director HCTTF Kelly McCracken National
Accessing Behavioral Health Services in Santa Barbara County: System Strengths & Needs Analysis
 Accessing Behavioral Health Services in Santa Barbara County: System Strengths & Needs Analysis Report to the Steering Committee Presented by April Howard, PhD Access Survey Team July 24, 2014 Executive
Accessing Behavioral Health Services in Santa Barbara County: System Strengths & Needs Analysis Report to the Steering Committee Presented by April Howard, PhD Access Survey Team July 24, 2014 Executive
Readmission Prevention Programs. Vice President, Strategy & Development June 6, 2017
 Readmission Prevention Programs Paul M. Duck @paulduck Vice President, Strategy & Development June 6, 2017 About Beacon Health Options Headquartered in Boston; more than 70 locations in the US and UK 5,000
Readmission Prevention Programs Paul M. Duck @paulduck Vice President, Strategy & Development June 6, 2017 About Beacon Health Options Headquartered in Boston; more than 70 locations in the US and UK 5,000
Population Health Management Tools and Strategies to Support Care Coordination An InfoMC White Paper April 2016
 Population Health Management Tools and Strategies to Support Care Coordination An InfoMC White Paper April 2016 Norris, Susan, Ph.D., Chief Clinical Officer, InfoMC Daniels, Allen S., Ed.D., Clinical Director,
Population Health Management Tools and Strategies to Support Care Coordination An InfoMC White Paper April 2016 Norris, Susan, Ph.D., Chief Clinical Officer, InfoMC Daniels, Allen S., Ed.D., Clinical Director,
Community Health Needs Assessment July 2015
 Community Health Needs Assessment July 2015 1 Executive Summary UNM Hospitals is committed to meeting the healthcare needs of our community. As a part of this commitment, UNM Hospitals has attended forums
Community Health Needs Assessment July 2015 1 Executive Summary UNM Hospitals is committed to meeting the healthcare needs of our community. As a part of this commitment, UNM Hospitals has attended forums
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
The MetroHealth System
 The MetroHealth System June 16, 2016 Presentation to Ohio Joint Medicaid Oversight Committee Dr. James Misak, Vice Chair of Community and Population Health, Department of Family Medicine Susan Mego, Executive
The MetroHealth System June 16, 2016 Presentation to Ohio Joint Medicaid Oversight Committee Dr. James Misak, Vice Chair of Community and Population Health, Department of Family Medicine Susan Mego, Executive
Building a Better Home: Transformation to a Patient Centered Health Home. Anna M. Gard, FNP-BC Association of Clinicians for the Underserved
 Building a Better Home: Transformation to a Patient Centered Health Home Anna M. Gard, FNP-BC Association of Clinicians for the Underserved A Patient Centered Health Home is not a place but an approach
Building a Better Home: Transformation to a Patient Centered Health Home Anna M. Gard, FNP-BC Association of Clinicians for the Underserved A Patient Centered Health Home is not a place but an approach
Skagit County 0.1% Behavioral Health Sales Tax Permanent Supportive Housing Program - Services Request for Proposals (RFP)
") Skagit County 0.1% Behavioral Health Sales Tax Permanent Supportive Housing Program - Services Request for Proposals (RFP) RELEASE DATE: OCTOBER 20, 2016 LETTER OF INTEREST DUE DATE: DECEMBER 19, 2017
Skagit County 0.1% Behavioral Health Sales Tax Permanent Supportive Housing Program - Services Request for Proposals (RFP) RELEASE DATE: OCTOBER 20, 2016 LETTER OF INTEREST DUE DATE: DECEMBER 19, 2017
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Care Coordination Overview. Janet Tennison, PhD UPV Standards October 8, 2013
 Care Coordination Overview Janet Tennison, PhD UPV Standards October 8, 2013 What IS Care Coordination? The deliberate, proactive organization of patient care activities between two or more participants
Care Coordination Overview Janet Tennison, PhD UPV Standards October 8, 2013 What IS Care Coordination? The deliberate, proactive organization of patient care activities between two or more participants
Brian E. Sandoval, Psy.D. Primary Care Behavioral Health Manager Yakima Valley Farm Workers Clinic
 Clinical Integration of Behavioral Health in Washington State: The Development of Practice Standards for Primary Care Service Delivery Brian E. Sandoval, Psy.D. Primary Care Behavioral Health Manager Yakima
Clinical Integration of Behavioral Health in Washington State: The Development of Practice Standards for Primary Care Service Delivery Brian E. Sandoval, Psy.D. Primary Care Behavioral Health Manager Yakima
DMC-ODS. System Transformation. Presented at DHCS 2017 Annual Conference. Elizabeth Stanley-Salazar, MPH Doug Bond Lisa Garcia, LCSW
 DMC-ODS System Transformation Presented at DHCS 2017 Annual Conference Elizabeth Stanley-Salazar, MPH Doug Bond Lisa Garcia, LCSW Objectives Understand managed care principles applied to DMC-ODS Waiver
DMC-ODS System Transformation Presented at DHCS 2017 Annual Conference Elizabeth Stanley-Salazar, MPH Doug Bond Lisa Garcia, LCSW Objectives Understand managed care principles applied to DMC-ODS Waiver
Southwest Texas Regional Advisory Council
 Executive Summary In 1989, the Texas legislature identified a need to ensure trauma resources were available to every person in Texas. The Omni Rural Health Care Rescue Act, directed the Bureau of Emergency
Executive Summary In 1989, the Texas legislature identified a need to ensure trauma resources were available to every person in Texas. The Omni Rural Health Care Rescue Act, directed the Bureau of Emergency
Attachment A INYO COUNTY BEHAVIORAL HEALTH. Annual Quality Improvement Work Plan
 Attachment A INYO COUNTY BEHAVIORAL HEALTH Annual Quality Improvement Work Plan 1 Table of Contents Inyo County I. Introduction and Program Characteristics...3 A. Quality Improvement Committees (QIC)...4
Attachment A INYO COUNTY BEHAVIORAL HEALTH Annual Quality Improvement Work Plan 1 Table of Contents Inyo County I. Introduction and Program Characteristics...3 A. Quality Improvement Committees (QIC)...4
CCBHCs 101: Opportunities and Strategic Decisions Ahead
 CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Fletcher Allen Health Care Case Study Organization Profile Located in Burlington, Fletcher Allen Health Care (FAHC) is Vermont s university
Best Practices Managing Patients with Multiple Chronic Conditions Fletcher Allen Health Care Case Study Organization Profile Located in Burlington, Fletcher Allen Health Care (FAHC) is Vermont s university
Using Big Data to improve population health: The VA Homeless Program Hotspotter initiative. NCHV Annual Meeting May, 2016
 Using Big Data to improve population health: The VA Homeless Program Hotspotter initiative NCHV Annual Meeting May, 2016 Homeless Veterans and Acute care use 40% of homeless adults went to an emergency
Using Big Data to improve population health: The VA Homeless Program Hotspotter initiative NCHV Annual Meeting May, 2016 Homeless Veterans and Acute care use 40% of homeless adults went to an emergency
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Care Coordination is More Than a Care Coordinator
 Care Coordination is More Than a Care Coordinator Jennifer P. Lundblad, PhD, MBA CA State Rural Health Association November 7, 2013 Objectives As a result of this session, participants will: Understand
Care Coordination is More Than a Care Coordinator Jennifer P. Lundblad, PhD, MBA CA State Rural Health Association November 7, 2013 Objectives As a result of this session, participants will: Understand
PROPOSED AMENDMENTS TO HOUSE BILL 4018
 HB 01-1 (LC ) //1 (LHF/ps) Requested by Representative BUEHLER PROPOSED AMENDMENTS TO HOUSE BILL 01 1 1 1 1 On page 1 of the printed bill, line, after ORS insert.0 and. In line, delete Section and insert
HB 01-1 (LC ) //1 (LHF/ps) Requested by Representative BUEHLER PROPOSED AMENDMENTS TO HOUSE BILL 01 1 1 1 1 On page 1 of the printed bill, line, after ORS insert.0 and. In line, delete Section and insert
Care Compact Guide Patient-Centered Specialty Care (PCSC) A Component of Medical Neighborhood Initiatives
 A Component of Medical Neighborhood Initiatives") Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Anthem Blue Cross and Blue Shield is the trade name of: In Colorado: Rocky Mountain Hospital and Medical
Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Anthem Blue Cross and Blue Shield is the trade name of: In Colorado: Rocky Mountain Hospital and Medical
College-wide Patient-Centered Medical Home Program Meharry Medical College
 + The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
+ The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
Quality Improvement Work Plan
 NEVADA County Behavioral Health Quality Improvement Work Plan Mental Health and Substance Use Disorder Services Fiscal Year 2017-2018 Table of Contents I. Quality Improvement Program Overview...1 A. QI
NEVADA County Behavioral Health Quality Improvement Work Plan Mental Health and Substance Use Disorder Services Fiscal Year 2017-2018 Table of Contents I. Quality Improvement Program Overview...1 A. QI
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Chronic Care Management
 Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
The Michigan Primary Care Transformation (MiPCT) Project. PGIP Meeting Update March 09, 2012
 Project. PGIP Meeting Update March 09, 2012") The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
Critical Time Intervention (CTI) (State-Funded)
 (State-Funded)") Critical Time (CTI) (State-Funded) Service Definition and Required Components Critical Time (CTI) is an intensive 9 month case management model designed to assist adults age 18 years and older with mental
Critical Time (CTI) (State-Funded) Service Definition and Required Components Critical Time (CTI) is an intensive 9 month case management model designed to assist adults age 18 years and older with mental
Adult BH Home & Community Based Services (HCBS) Foundations Webinar JUNE 29, 2016
 Foundations Webinar JUNE 29, 2016") Adult BH Home & Community Based Services (HCBS) Foundations Webinar JUNE 29, 2016 June 30, 2016 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will
Adult BH Home & Community Based Services (HCBS) Foundations Webinar JUNE 29, 2016 June 30, 2016 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will
Barry Fatland, Manager, Bridging The Gap Training Program Juan F. Gutierrez Sanin, Coordinator Bridging The Gap Training Program The Cross Cultural
 Barry Fatland, Manager, Bridging The Gap Training Program Juan F. Gutierrez Sanin, Coordinator Bridging The Gap Training Program The Cross Cultural Health Care Program www.cchcp.org Established in 1992
Barry Fatland, Manager, Bridging The Gap Training Program Juan F. Gutierrez Sanin, Coordinator Bridging The Gap Training Program The Cross Cultural Health Care Program www.cchcp.org Established in 1992
What is a Pathways HUB?
 What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
Quality Improvement Work Plan
 NEVADA County Behavioral Health Quality Improvement Work Plan Fiscal Year 2016-2017 Table of Contents I. Quality Improvement Program Overview...1 A. Quality Improvement Program Characteristics...1 B. Annual
NEVADA County Behavioral Health Quality Improvement Work Plan Fiscal Year 2016-2017 Table of Contents I. Quality Improvement Program Overview...1 A. Quality Improvement Program Characteristics...1 B. Annual
LOS ANGELES FIRE COMMISSION
 LOS ANGELES FIRE COMMISSION BOARD OF FIRE COMMISSIONERS DELIA IBARRA PRESIDENT ANDREW GLAZIER VICE PRESIDENT jimmy H. hara, m.d. REBECCA NINBURG JIMMIE WOODS-GRAY m Eft j\ 5// i ERIC GARCETTI Mayor SUE
LOS ANGELES FIRE COMMISSION BOARD OF FIRE COMMISSIONERS DELIA IBARRA PRESIDENT ANDREW GLAZIER VICE PRESIDENT jimmy H. hara, m.d. REBECCA NINBURG JIMMIE WOODS-GRAY m Eft j\ 5// i ERIC GARCETTI Mayor SUE
Housing as Health Care Webinar. Wrapping Tenancy Supports into Your Housing Strategy
 Housing as Health Care Webinar Wrapping Tenancy Supports into Your Housing Strategy National Governors Association Friday, October 28th, 2016 12-1pm EST Dial-in: 888-858-6021; Passcode 2026245354 1 Agenda
Housing as Health Care Webinar Wrapping Tenancy Supports into Your Housing Strategy National Governors Association Friday, October 28th, 2016 12-1pm EST Dial-in: 888-858-6021; Passcode 2026245354 1 Agenda
DEVELOPING A MEDICAID SUPPORTIVE HOUSING SERVICES BENEFIT
 DEVELOPING A MEDICAID SUPPORTIVE HOUSING SERVICES BENEFIT CONSIDERATIONS AND DECISION POINTS EXECUTIVE SUMMARY This tool is designed to assist States in the development of a Medicaid benefit to pay for
DEVELOPING A MEDICAID SUPPORTIVE HOUSING SERVICES BENEFIT CONSIDERATIONS AND DECISION POINTS EXECUTIVE SUMMARY This tool is designed to assist States in the development of a Medicaid benefit to pay for
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Central Ohio Primary Care (COPC) Spotlight on Innovation
 Spotlight on Innovation") Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
UPDATE ON MANAGED CARE IN NY STATE: IMPLICATIONS FOR PROVIDERS
 UPDATE ON MANAGED CARE IN NY STATE: IMPLICATIONS FOR PROVIDERS November 18, 2013 NYS OMH Behavioral Health Transition 2 Key MRT initiative to move fee-for-service populations and services into managed
UPDATE ON MANAGED CARE IN NY STATE: IMPLICATIONS FOR PROVIDERS November 18, 2013 NYS OMH Behavioral Health Transition 2 Key MRT initiative to move fee-for-service populations and services into managed
Sierra Health Foundation s Responsive Grants Program Proposers Conference Round One
 Welcome to Sierra Health Foundation s Responsive Grants Program Proposers Conference 2012 Round One Diane Littlefield Vice President of Programs and Partnerships Matt Cervantes Program Officer 2 Agenda
Welcome to Sierra Health Foundation s Responsive Grants Program Proposers Conference 2012 Round One Diane Littlefield Vice President of Programs and Partnerships Matt Cervantes Program Officer 2 Agenda
National Criminal Justice Reform Activities Important to the SUD Field. Gabrielle de la Guéronnière, Legal Action Center June 9 th, 2016
 National Criminal Justice Reform Activities Important to the SUD Field Gabrielle de la Guéronnière, Legal Action Center June 9 th, 2016 1 Work to Improve Policies Governing the Criminal Justice System
National Criminal Justice Reform Activities Important to the SUD Field Gabrielle de la Guéronnière, Legal Action Center June 9 th, 2016 1 Work to Improve Policies Governing the Criminal Justice System
Community Health Worker (CHW) Strategies and Local Public Health: Overview and Opportunities Local Public Health Association Meeting May 16, 2013
 Strategies and Local Public Health: Overview and Opportunities Local Public Health Association Meeting May 16, 2013") Community Health Worker (CHW) Strategies and Local Public Health: Overview and Opportunities Local Public Health Association Meeting May 16, 2013 Carol Berg, Board Member Joan Cleary, Executive Director
Community Health Worker (CHW) Strategies and Local Public Health: Overview and Opportunities Local Public Health Association Meeting May 16, 2013 Carol Berg, Board Member Joan Cleary, Executive Director
Agenda STATE OF TENNESSEE 12/7/2016
 STATE OF TENNESSEE Tennessee Health Link: Practice Transformation Training 12/14/2016 Agenda Overview of Tennessee Health Link Partnership between HCFA, MCOs, Navigant and Practices Introduction to Navigant
STATE OF TENNESSEE Tennessee Health Link: Practice Transformation Training 12/14/2016 Agenda Overview of Tennessee Health Link Partnership between HCFA, MCOs, Navigant and Practices Introduction to Navigant
Building a Multi-System Clinically Integrated Network
 Building a Multi-System Clinically Integrated Network 22 nd Annual AHA Leadership Summit July 2014 Valence Health Has Been Helping Provider Organizations Progress Toward Value-Based Care Since 1996 Technology-enabled
Building a Multi-System Clinically Integrated Network 22 nd Annual AHA Leadership Summit July 2014 Valence Health Has Been Helping Provider Organizations Progress Toward Value-Based Care Since 1996 Technology-enabled
Improving Health Status through Behavioral Health Interventions
 Comorbidity in the Dual Eligible Population: Improving Health Status through Behavioral Health Interventions PREPARED FOR THE CALIFORNIA ASSOCIATION OF HEALTH PLANS 2013 SEMINAR SERIES JUNE 25, 2013 BEACON
Comorbidity in the Dual Eligible Population: Improving Health Status through Behavioral Health Interventions PREPARED FOR THE CALIFORNIA ASSOCIATION OF HEALTH PLANS 2013 SEMINAR SERIES JUNE 25, 2013 BEACON
National Association of State Mental Health Program Directors Research Institute
 Goal: 100% of Consumers have access without delay to the most appropriate 24/7 emergency, crisis stabilization, inpatient or recovery bed: Lessons Learned from States with On-Line Registries of Available
Goal: 100% of Consumers have access without delay to the most appropriate 24/7 emergency, crisis stabilization, inpatient or recovery bed: Lessons Learned from States with On-Line Registries of Available
Medicaid Managed Care Readiness For Agency Staff --
 Medicaid Managed Care Readiness 101 -- For Agency Staff -- To Understand: Learning Objectives Basic principles of Managed Care as a payment vehicle for health care services The structure of the current
Medicaid Managed Care Readiness 101 -- For Agency Staff -- To Understand: Learning Objectives Basic principles of Managed Care as a payment vehicle for health care services The structure of the current
New York University Prevention Research Center
 New York University Prevention Research Center May 9, 2013 New York City, New York Sergio Matos Executive Director Community Health Worker Network of NYC President Health Innovation Associates Leading
New York University Prevention Research Center May 9, 2013 New York City, New York Sergio Matos Executive Director Community Health Worker Network of NYC President Health Innovation Associates Leading
Navigating New York State s Transition to Managed Care
 Navigating New York State s Transition to Managed Care December 3, 2014 Mary McKernan McKay, Ph.D Andrew F. Cleek, Psy.D. Meaghan E. Baier, LMSW Agenda Introduction of the Managed Care Technical Assistance
Navigating New York State s Transition to Managed Care December 3, 2014 Mary McKernan McKay, Ph.D Andrew F. Cleek, Psy.D. Meaghan E. Baier, LMSW Agenda Introduction of the Managed Care Technical Assistance
Behavioral Health Providers: The Key Element of Value Based Payment Success
 Behavioral Health Providers: The Key Element of Value Based Payment Success December 6, 2017 Presented by: Andrew Cleek, Psy.D. Meaghan Baier, LMSW Goals of the Presentation Understand the intersect between
Behavioral Health Providers: The Key Element of Value Based Payment Success December 6, 2017 Presented by: Andrew Cleek, Psy.D. Meaghan Baier, LMSW Goals of the Presentation Understand the intersect between
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Highline Health Connections: Care Navigation for Vulnerable Populations
 Highline Health Connections: Care Navigation for Vulnerable Populations WSHA Readmissions Safe Table - Feb 14, 2017 Carolyn Bonner, Director Home Health, Health Connections, Cancer Center, Sleep Center
Highline Health Connections: Care Navigation for Vulnerable Populations WSHA Readmissions Safe Table - Feb 14, 2017 Carolyn Bonner, Director Home Health, Health Connections, Cancer Center, Sleep Center
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...