State of New Hampshire
|
|
|
- Patrick Price
- 5 years ago
- Views:
Transcription

1 State of New Hampshire ADVERSE EVENT REPORTING 2015 REPORT Provided by New Hampshire Department of Health and Human Services Office of Operations Support Bureau of Licensing & Certification November 18, 2016 Adverse Event Report Hospitals & Ambulatory Surgery Centers In 2010, the state of New Hampshire enacted RSA which adopted the National Quality Forum s Serious Reportable Events and added a specific event related to the transmission of blood borne pathogens. The law requires hospitals and ambulatory surgery centers to report any of these events should they occur in their facility. There are twenty-nine (29) NQF Serious Reportable Events (SREs) structured around seven categories: surgical, product or device, patient protection, care management, environmental, radiologic events and potential criminal. This report is submitted in accordance with New Hampshire law (NHRSA ) which requires an annual report to the Legislature. The Bureau of Licensing and Certification submits the annual report to the Legislature that includes the aggregate number and type of adverse events by facility for the prior calendar year. Lessons learned from the root cause(s) and corrective action plan(s) for each reported adverse event are also included. The Bureau and the healthcare organizations work together to continuously improve patient safety.
2 National Quality Forum : The National Quality Forum (NQF) is a not-for-profit nonpartisan, membership based organization that works to catalyze improvement in healthcare. This status allows the federal government to rely on NQF-defined measures or healthcare practices as the best, evidence-based approaches to improving care. Sometimes referred to as never events, the NQF list has increasingly become the basis for state mandatory reporting systems. The list of NQF serious reportable events (SREs) is intended to capture events that are clearly identifiable and measurable, and largely preventable. Definition of Adverse Event: Adverse events are outcomes determined to be unrelated to the natural course of the patient s illness or underlying condition, or the proper treatment of that illness or underlying condition. The law further characterizes an adverse event according to the NQF SREs: SURGICAL OR INVASIVE PROCEDURE EVENTS Surgery or other invasive procedure performed on the wrong site Surgery or other invasive procedure performed on the wrong patient Wrong surgical or other invasive procedure performed on a patient Unintended retention of a foreign object in a patient after surgery or other invasive procedure Intraoperative or immediately postoperative/post procedure death in an ASA (American Society Anesthesiologist) Class 1 patient PRODUCT OR DEVICE EVENTS Patient death or serious injury associated with the use of contaminated drugs, devices, or biologics provided by the healthcare setting Patient death or serious injury associated with the use or function of a device in patient care, in which the device is used or functions other than as intended Patient death or serious injury associated with intravascular air embolism that occurs while being cared for in a healthcare setting PATIENT PROTECTION EVENTS Discharge or release of a patient/resident of any age, who is unable to make decisions, to other than an authorized person Patient death or serious injury associated with patient elopement (disappearance) Patient suicide, attempted suicide, or self-harm that results in serious injury, while being cared for in a healthcare setting CARE MANAGEMENT EVENTS Patient death or serious injury associated with a medication error (e.g., errors involving the wrong drug, wrong dose, wrong patient, wrong time, wrong rate, wrong preparation, or wrong route of administration) Patient death or serious injury associated with unsafe administration of blood products Page 2
3 Maternal death or serious injury associated with labor or delivery in a low-risk pregnancy while being cared for in a healthcare setting Death or serious injury of a neonate associated with labor or delivery in a low-risk pregnancy Patient death or serious injury associated with a fall while being cared for in a healthcare setting Any Stage 3, Stage 4, and unstageable pressure ulcers acquired after admission/presentation to a healthcare setting Artificial insemination with the wrong donor sperm or wrong egg (updated) Patient death or serious injury resulting from the irretrievable loss of an irreplaceable biological specimen Patient death or serious injury resulting from failure to follow up or communicate laboratory, pathology, or radiology test results ENVIRONMENTAL EVENTS Patient or staff death or serious injury associated with an electric shock in the course of a patient care process in a healthcare setting Any incident in which systems designated for oxygen or other gas to be delivered to a patient contain no gas, the wrong gas, or are contaminated by toxic substances Patient or staff death or serious injury associated with a burn incurred from any source in the course of a patient care process in a healthcare setting Patient death or serious injury associated with the use of physical restraints or bedrails while being cared for in a healthcare setting RADIOLOGIC EVENTS Death or serious injury of a patient or staff associated with the introduction of a metallic object into the M RI area POTENTIAL CRIMINAL EVENTS Any instance of care ordered by or provided by someone impersonating a physician, nurse, pharmacist, or other licensed healthcare provider Abduction of a patient/resident of any age Sexual abuse/assault on a patient or staff member within or on the grounds of a healthcare setting Death or serious injury of a patient or staff from physical assault (battery) within or on the grounds of a healthcare setting The state law also had the following addition to the RSA 151:38: The exposure of a patient to a non-aerosolized blood borne pathogen by a health care worker's intentional, unsafe act. An act by hospital or ambulatory surgery center staff resulting in an infection or disease shall be considered to be purposefully unsafe if it meets all of the following criteria: (1) There was an intentional act or reckless behavior; (2) No reasonable person with similar qualifications, training, and experience would have acted the same way under similar circumstances; and (3) There were no extenuating circumstances that could justify the act. Page 3
4 Page 4
5 Page 5
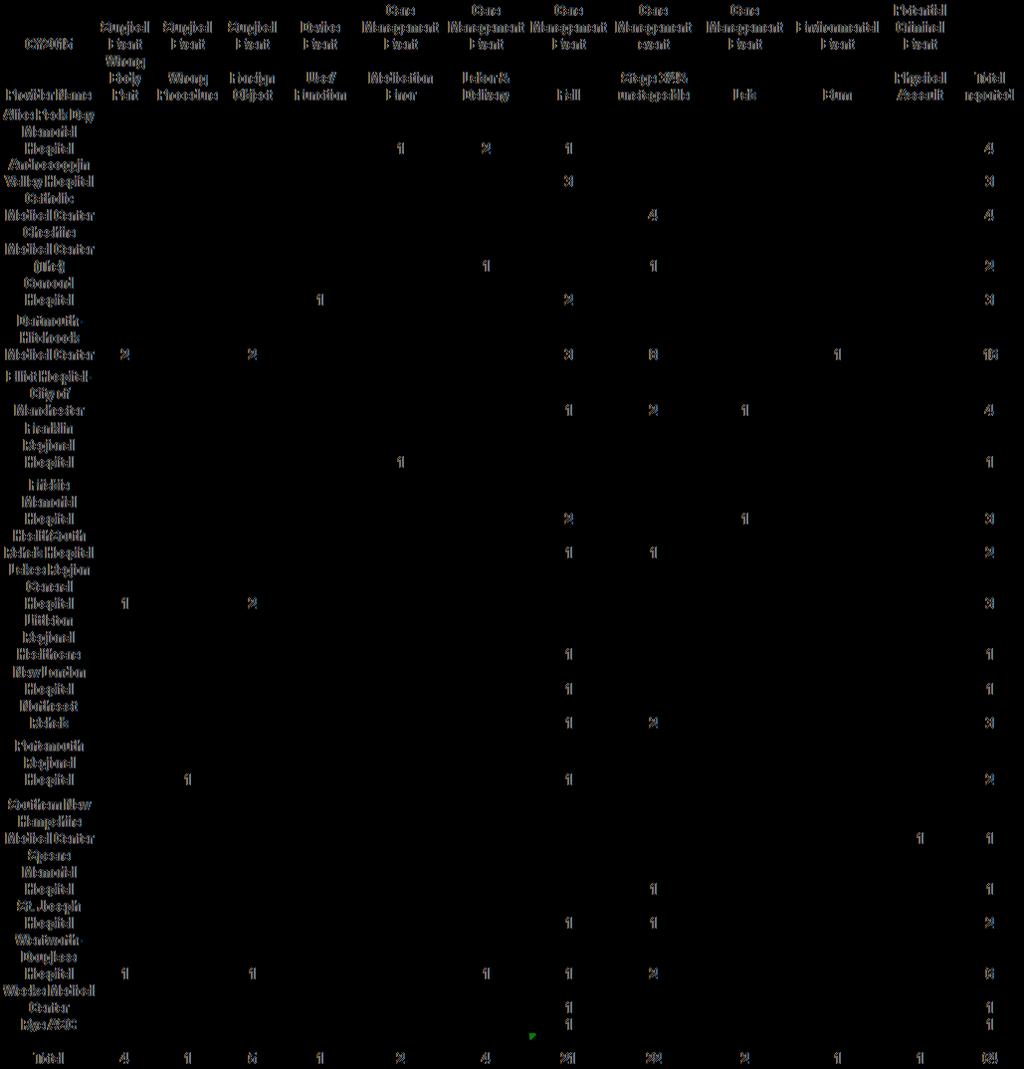
6 Hospital 2015 Adverse Events ICU Beds Staffed Beds Admission s Patient Days Inpatient Surgeries Outpatient Surgeries ALICE PECK DAY MEMORIAL HOSPITAL ,288 4, ,574 ANDROSCOGGIN VALLEY HOSPITAL ,459 5, ,419 CATHOLIC MEDICAL CENTER ,566 55,661 4,161 5,480 CHESHIRE MEDICAL CENTER (THE) ,667 19, ,330 CONCORD HOSPITAL ,647 58,220 3,609 6,684 COTTAGE HOSPITAL , DARTMOUTH-HITCHCOCK MEDICAL CENTER , ,887 8,553 11,001 ELLIOT HOSPITAL CITY OF MANCHESTER ,104 64,417 3,024 5,190 EXETER HOSPITAL INC ,892 19,871 1,442 4,679 FRANKLIN REGIONAL HOSPITAL ,196 7, ,168 FRISBIE MEMORIAL HOSPITAL ,290 15,580 1,187 6,113 HUGGINS HOSPITAL , ,372 LAKES REGION GENERAL HOSPITAL ,614 23,863 1,686 8,125 LITTLETON REGIONAL HEALTHCARE ,623 5, ,598 MEMORIAL HOSPITAL ,631 6, ,728 MONADNOCK COMMUNITY HOSPITAL ,474 4, ,273 NEW LONDON HOSPITAL ,250 5, ,479 PARKLAND MEDICAL CENTER ,530 13, ,344 PORTSMOUTH REGIONAL HOSPITAL ,381 40,234 2,289 2,359 SOUTHERN NEW HAMPSHIRE MEDICAL CENTER ,909 34,307 1,173 3,627 SPEARE MEMORIAL HOSPITAL ,344 5, ST JOSEPH HOSPITAL ,261 25,118 1,117 2,537 UPPER CT VALLEY HOSPITAL , VALLEY REGIONAL HOSPITAL, INC , WEEKS MEDICAL CENTER , WENTWORTH-DOUGLASS HOSPITAL ,269 27,108 1,301 5,609 CROTCHED MOUNTAIN REHAB , HAMPSTEAD REHAB ,689 17, HEALTHSOUTH REHAB , NEW HAMPSHIRE HOSPITAL ,009 57, NORTHEAST REHAB ,266 38, RYE ASC Note: Data is reported based on the hospitals Fiscal Year Data Source: AHA Survey 2015 & hospitals Data Date: 10/17/2016 Compiled By: Foundation for Healthy Communities (FHC) Page 6
7 Page 7
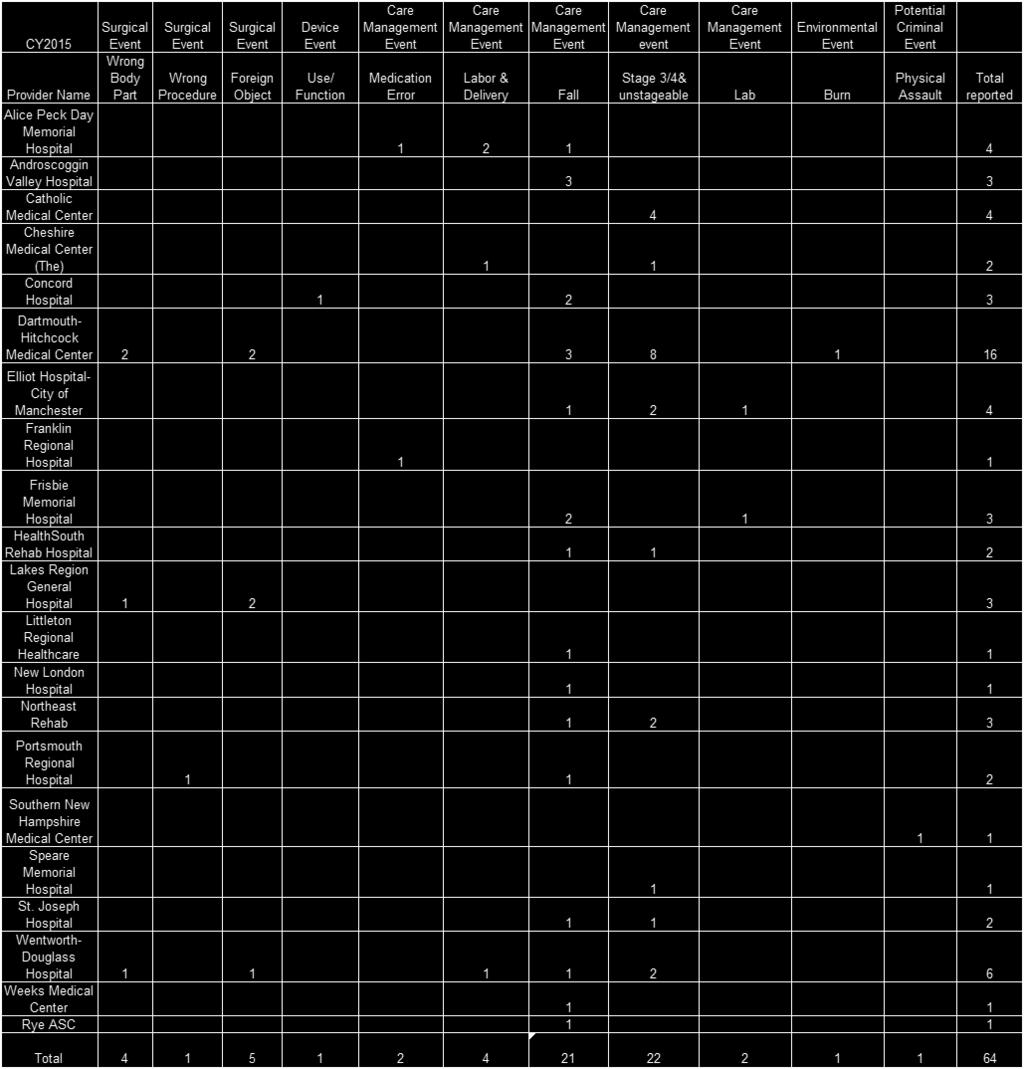
8 Requirements: Reporting Any hospital or ambulatory surgical center facility must notify the New Hampshire Department of Health and Human Services within 15 working days after the discovery of the event. The notification shall be filed in a format specified by the Department and shall not include any identifying information of the healthcare professionals, facility employees, or patients involved. The notification should include a brief description of the event. Within 60 days the facility needs to submit a credible root cause analysis and corrective action plan (CAP). What happened in 2015? It is important to note that no consumer complaints were received by the Department concerning the 64 adverse events reported. Complaints and adverse events are handled by Health Facilities Administration-Certification (HFA-C) as two distinct actions. The Department is responsible for the health, safety and well-being of New Hampshire's citizens. HFA-C evaluates facilities in determining that the facilities are in compliance with patient safety, quality assurance and federal and state regulatory laws. RSA 151:40 establishes that failure of a facility to report timely, adverse events to include root cause analysis and plans of correction, be subject to disciplinary actions. During the calendar year 2015 no disciplinary actions were required for late reporting. In order to answer the question, "How do you know the reporting facility did what they said they were going to do to correct the problem?" HFA-C sampled over 10% of the adverse events and asked for and received specific performance data to be submitted as a follow up to their CAP. All facilities sampled provided performance information. It was concluded that the hospitals followed through with actions to correct the problems. Unpreventable / Unavoidable Harm According to NQF, to qualify for the list of SREs an event must be largely, if not entirely, preventable in addition to other criteria. All hospitals and ASCs report Adverse Events as required by law. Upon completion of a detailed root cause analysis, they may occasionally find that, despite adoption of evidence based protocols and strict adherence to established standards of care, an optimal outcome is not achieved and harm still occurs. Individuals may have clinical conditions that can create a complex set of processes that lead to an event, despite providing the best prevention and/or treatment known. The goal of patient care is to do all that is possible and learn from all events, whether or not a reported event was considered unavoidable. Serious Reportable Events / Adverse Events Since January 2010, NH hospitals and ASCs have been reporting adverse events to the Bureau of Health Facilities Certification as required by RSA 151: 38. The law was revised in It is important to note that changes and additions to the list of SREs, including changes in definitions, resulted in an increased number of reports in This was particularly evident in the category of pressure ulcers, whose definition was expanded to include unstageable, which resulted in a doubling of pressure ulcer reports between 2013 and 2014, from 11 to 22. The number of reportable events of pressure ulcers stabilized in It is worthy to note there was a 12% decrease in total adverse events in Organizations have scrutinized their root cause analyses to determine opportunities to Page 8



9 improve the quality of care that patients receive within their hospitals. Over the years of reporting, organizations have worked to improve identified weaknesses in systems of patient care. Page 9
10 Comparison by Events SURGICAL OR INVASIVE PROCEDURE EVENTS Wrong site Wrong patient Wrong procedure Unintended retention of a foreign object Intraoperative or immediately postoperative death of ASA Class 1 patient PRODUCT OR DEVICE EVENTS Use of contaminated drugs, biologics or device Misuse/malfunction of a device Air embolism PATIENT PROTECTION EVENTS Release of a patient of any age, who is unable to make decisions, to the wrong person Patient elopement Patient suicide, attempted suicide, or self-harm CARE MANAGEMENT EVENTS Death or serious injury due to a medication error Death or serious injury due to unsafe transfusion practices Maternal death or serious injury In a low-risk pregnancy, labor or delivery Death or serious injury of a neonate in a low risk pregnancy, labor or delivery Death or serious injury associated with a fall Stage 3 or 4 or unstageable pressure ulcers acquired after admission Artificial insemination with the wrong donor sperm or donor egg Death or serious injury from irretrievable loss of an irreplaceable biological specimen Death or serious injury from failure to follow up or communicate laboratory, pathology, or radiology test results ENVIRONMENTAL EVENTS Death or serious injury associated with an electric shock Wrong gas, no gas or contamination in patient gas line Patient or staff death or serious injury associated with a burn Death or serious injury associated with the use of physical restraints or bedrails RADIOLOGIC EVENTS Page 10
11 Death or serious injury if a patient or staff with the introduction of a metallic object into the MRI POTENTIAL CRIMINAL EVENTS Care ordered by or provided by someone impersonating an MD, RN, Pharmacist or other LIP (Licensed Independent Practitioner) Abduction of a patient of any age Sexual abuse/assault of a patient or staff member Death or serious Injury of a patient or staff from physical assault (battery) TOTAL What are NH hospitals doing about Serious Reportable Events? In analyzing the events reported in 2015 it should be noted that there were three major areas responsible for 83% of the events reported. These areas were as follows: Falls 33% Pressure Ulcers 34% Surgical Events 16% In consideration of the fact that these event types represent 83% of the total events it is important that we focus on these and address what the NH hospitals are doing to prevent them from occurring. Falls with Injury Problem Summary: A fall is defined a sudden, unintentional change in position causing an individual to land at a lower level, on an object, the floor, on the ground, other than as a consequence of a sudden onset of paralysis epileptic seizures, or overwhelming external forces. Falls in a hospital can, and often do, complicate the hospital stay and keep the patient from returning to the community. Many falls that occur are injury free and would not be considered an adverse event. However, for the few who suffer from injuries it may mean additional testing and an increased duration of stay in the hospital. The majority of falls occur when patients are moving to and from the bathroom or attempting to get up from the commode on their own. Patients who suffer serious injury are typically over the age of 60 and suffer from several chronic diseases and conditions that impact balance, strength, and mobility due to the medications or because of their medical condition. Page 11

12 Contributing Factors: Many factors over the years have been identified by NH hospitals. These include but may not be limited to the following: Advanced age of hospitalized patients Physical challenges with mobility and oxygenation impairments History of falls in the past several months prior to admission Adults who fall while walking to bathroom may not call the nurse because: They don t remember to call the nurse They are adults who have independently toileted themselves up until recently Since men void while standing they can experience a sudden decrease in blood pressure when standing which may lead to disorientation Patients admitted to hospitals are much more ill and present with complicated care issues Medical conditions may impact mobility such as impaired blood flow to lower legs Medications may interfere with mobility and judgment, such as post-operative pain medications History of Substance abuse - alcohol or non-prescribed medications - many may have self- medicated in lieu of seeking medical help or because medical support was too expensive Strategies in place in NH hospitals include but are not limited to: Focus on patient rounding to see and determine the safety and comfort of patients at least every hour Page 12
13 Completion of a Fall Risk Assessment upon admission, updated every shift and re-evaluated after every fall Staff debriefing (discussion) after every fall to determine contributing factors and how events occurred in an attempt to learn how to better provide the patient care to prevent further falls Dedicated resources to a sitter program to provide human companionship and help alert nurses in a timely manner when a patient is trying to move creating a fall risk Use of family visitors to help keep patients calm and alert staff of activity that may be a falls risk Use of motion sensors - pads and alarms activated by patient movement that alert staff to movement Fall Prevention Teams interdisciplinary team to review and discuss ways to prevent falls and reduce injury Gait Belts Used to help maintain balance and give staff more control if patient demonstrates weakness while walking to help lower patients to the floor instead of patients falling to the floor Plan Moving Forward: Link specific interventions to prevent a fall to the fall risk assessment score Staff education refresher on fall prevention including the intent of assessment and making changes in interventions as needed to address the changing fall risk of the patient Expand the act of purposeful rounding to include toileting at least hourly. Current standard is to ask the patient but in high risk cases we may need to trial a new standard of actually taking patients to the bathroom Revitalize fall prevention teams, rotating new staff and clinicians into committees for a fresh approach in reviewing the events Re-evaluate and improve use of sitter programs and incorporate patient family engagement in the process Expand risk assessments upon hospital admission to include a history of falls at home as well as assessing for signs of falls such as bruising Conclusion: Over the next 10 years the population of NH Seniors (age 65+) is expected to double to 325,000 people. Many may have multiple medical conditions and changing mentation. The typical patient will be on no fewer than 8-10 routine medications, many that may interfere with mobility. Hospitals in New Hampshire will continue to assist patients and their families with falls prevention during the hospital stay. Hospitals will educate patients and their families while in their care about a patient s high risk areas and work with them for a safe discharge/ return to home and community. Hospital Acquired Pressure Ulcers Adverse Events Problem Summary: Pressure ulcers, also more commonly referred to as bedsores, decubitus ulcers or pressure sores are skin lesions which can be caused by friction, humidity, temperature, continence, medication, shearing force, age and unrelieved pressure. Patients prone to pressure ulcers are those who sit or lie down in one position for more than 2 hours at a time. In addition, poor nutrition and dehydration, and medical conditions that cause poor blood circulation to extremities, such as diabetes can cause pressure ulcers. Inadequate performance of proper skin inspections, Page 13

14 infrequent repositioning, and inability to maintain clean, dry skin can contribute to the development of a hospital acquired pressure ulcer. However not all pressure injuries are preventable. The skin is an organ just like the heart and lungs. Sometimes overwhelming illness contributes to the failure of the underlying skin tissue and despite excellent care the tissue breakdown will progress to a pressure injury. The most common areas for pressure ulcers include hips, backs, ankles, and buttocks. Contributing Factors: Many factors over the years have been identified by NH hospitals. These include but may not be limited to the following: Lack of thorough skin inspection/assessment Incomplete skin inspections Inaccurate staging of pressure ulcers Poor communications between staff and providers Not repositioning every 2 hours to relieve pressure Attention to addressing and improving hydration and nutritional status Clinical lapses in diabetes management leading to uncontrolled high blood sugars High risk medical conditions and history including: Diabetes, Smoking, Chronic Obstructive Pulmonary Disease, Vascular Disease, bed or chair bound patients, bladder and/or bowel incontinence, and poor hygiene Wearing constrictive clothing or shoes that can cause sores to form on feet and lower legs Operative procedures which necessitate the patient s position be maintained in a single place for extended periods of time Page 14
15 Strategies in place in NH hospitals include but are not limited to: Skin Assessment upon admission to identify pressure injuries at the time of admission so that prompt care can be initiated and reassessed every shift to detect early development of pressure injuries to prevent progression Use of Braden Scale for predicting pressure ulcer risk to determine other risk factors such as poor nutrition, dehydration, and hygiene issues so that high risk patients can be promptly identified and preventative interventions can be implemented before a pressure injury occurs Use of smooth soft surfaces and special pads for surgical patients undergoing lengthy procedures Development of protocols for cleaning and treating wounds Enhanced protocols for wound debridement (removal of dead tissue to allow for healing) Use of specifically designed dressings that can enhance wound healing Education/training on wound care at orientation of clinical staff with refresher classes offered at least every 2 years Plan Moving Forward : Training and education on skin inspection/assessment and documentation of any sign of pressure ulcer development Provider engagement in early detection and planning for risk of skin breakdown during hospitalization Family Engagement teaching family members the importance of nutrition, hydration, and disease management in prevention of wounds developing in the home Adoption of new evidence based practices including new wound care treatments for faster healing Engagement of local provider practices and home care agencies in inspections, assessments, and preventative treatment and patient/family education Consider appointment of wound care experts or a specialized team that can assist in cases of difficult evaluations or difficult patient issues requiring special prevention techniques/treatment Involvement of wound care specialists earlier in the assessment/documentation. Conclusion: All NH hospitals are chasing zero meaning they are striving for NO hospital acquired pressure ulcers. Since many wounds can begin in the community setting, reaching out to services that can influence prevention before and after hospitalization is being considered as part of efforts to reduce harm in NH communities. Problem Summary: Surgical or Invasive Procedure Adverse Events Surgical interventions in modern medicine take many different forms. Some are minor procedures performed in an office or bedside setting, taking a single clinician no more than a few minutes to complete. Others are highly complex Page 15


16 invasive procedures requiring a team of 10 or more experts in a traditional operating room where a single surgery may take anywhere from 1-30 hours and requires hundreds of instruments and a variety of technical equipment. More procedures are being done in highly technical settings designed for minimally invasive procedures such as interventional radiology, cardiology, and endoscopy suites and ambulatory surgery centers. Highly complex procedures can now be safely performed in these settings due to advances in the use of robotics, scopes, and procedural imaging. NH hospitals and ASCs are working to prevent surgical errors in all these settings through the use of checklists, team time outs, and briefings. Despite these efforts, surgical and procedural errors do occasionally happen. These errors include surgical instruments or objects such as sponges unintentionally left behind in the patient; the side, site or procedure is different than what was intended; or if a procedure is done correctly but was completed on the wrong patient. Contributing Factors: Many factors over the years have been identified by NH hospitals and ASCs. These include but may not be limited to the following: Frequent hand-offs of information during the continuum of care from the time of the original diagnosis of the issue requiring surgery to the actual team preforming the procedure; vital information is sometimes misrepresented or lost completely as it is handed off along the way Complexity of the environment and the systems in use may divert attention and concentration of the surgeon and other team members at key points Page 16
17 Inconsistent organizational expectations for training and orientation to surgical safety, time out, briefings and use of checklist in all settings where procedures occur Strategies in place in NH hospitals and ASCs include but are not limited to: Organizational Leadership engaged in prevention of harm and establishing expectations for organizational performance Full investigations of near miss events to understand failures and improve reliability of systems before an error causing harm occurs Engagement of Medical Staff by incorporation of time out/checklist performance into the provider performance evaluation process Time outs or briefings that invite all members of the team, regardless of role, to be mindful of potential problems or errors, increase the likelihood of anyone on the team speaking up when a potential problem is detected Verification of information in surgical plan with sources of truth such as pathology reports, imaging reports, and consultations in order to catch prior communication lapses Patient engagement in development of patient safety steps regarding surgical preparations and communication about the process Include the patient in the safety checks, together with the goals of the procedure from the patient s perspective, to get all team members unified on the plan of care Plan Moving Forward: Continue to educate staff in the use of the checklist and time out process including the inherent limitations of these tools to prevent all surgical errors Continue to foster a safe culture that encourages staff to speak up and stop the process if they suspect a problem, by training the surgeon in leadership methods that invite team communication and collaboration Enhance high reliability performance of the surgical team by including the patient s goals of care in the safety checks or briefings Extend surgical safety concepts and processes to all non-operating room procedural areas Explore and consider the implementation of pauses during the procedure prior to critical steps to assure all team members understand the plan and their role in executing it Track and trend near miss events to improve systems and processes before actual error occurs When a surgical error causing harm occurs, continue to develop methods for supporting the affected patient and family as well as the team members involved in the error NH hospitals and ASCs continue to work collaboratively to establish safe surgical practices Page 17
18 Conclusion: Surgical events are overwhelming to patients, families and the healthcare team involved with an error. Strong leadership during the surgical time out reinforces the important role of each team member in ensuring patient safety. Each team member must verbally state their name and purpose of the surgery and discuss any concerns before the surgery. With collaboration among team members, each member has a vested interest in the patient s outcome. Fostering communication among team members has helped reduce surgical events this year. Summary The continued goal for the NH hospitals and ASCs is to utilize their root cause analyses and to make corrective action plans (CAPs) that can enhance patient safety. The Hospitals and the ASCs remain committed to educate their personnel and professional staff about patient safety to promote the best outcomes for their patients. Acknowledgements: The Department's Adverse Event Reporting Staff would like to thank the many staff at New Hampshire's hospitals and ASCs for their prompt reporting of events, root cause analyses and corrective action plans. The assistance of members of the NH Health Care Quality Assurance Commission and staff of the Foundation for Healthy Communities is also acknowledged. Questions concerning this report may be directed to: michael.fleming@dhhs.nh.gov Page 18
Preventing Serious Reportable Events in Health Care
 Preventing Serious Reportable Events in Health Care The National Quality Forum (NQF), a coalition of public and private healthcare sector leaders who are focused on improving healthcare quality and patient
Preventing Serious Reportable Events in Health Care The National Quality Forum (NQF), a coalition of public and private healthcare sector leaders who are focused on improving healthcare quality and patient
Serious Reportable Events in Healthcare 2011 Update
 Serious Reportable Events in Healthcare 2011 Update July 19, 2011 1 Overview Purpose 2002, 2006, 2011 Facilitate uniform, comparable public reporting Enable systematic learning Ensure currency & appropriateness
Serious Reportable Events in Healthcare 2011 Update July 19, 2011 1 Overview Purpose 2002, 2006, 2011 Facilitate uniform, comparable public reporting Enable systematic learning Ensure currency & appropriateness
Serious Reportable Events Madeleine Biondolillo, MD Associate Commissioner Public Health Council August 2014
 Serious Reportable Events 2011-2013 Madeleine Biondolillo, MD Associate Commissioner Public Health Council August 2014 1 Overview Background Serious Reportable Events Quality Improvement Initiative Outcomes
Serious Reportable Events 2011-2013 Madeleine Biondolillo, MD Associate Commissioner Public Health Council August 2014 1 Overview Background Serious Reportable Events Quality Improvement Initiative Outcomes
Financial Disclosure. Learning Objectives: Preventing and Responding to Sentinel Events in Surgery 10/13/2015
 Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
VERMONT2008 Patient Safety, Surveillance, and Improvement System
 VERMONT2008 Patient Safety, Surveillance, and Improvement System Report to the Legislature on Act 215 (2006), 18 V.S.A. 1913(e) 108 Cherry Street, PO Box 70 Burlington, VT 05402 1.802.863.7341 healthvermont.gov
VERMONT2008 Patient Safety, Surveillance, and Improvement System Report to the Legislature on Act 215 (2006), 18 V.S.A. 1913(e) 108 Cherry Street, PO Box 70 Burlington, VT 05402 1.802.863.7341 healthvermont.gov
POLICIES AND PROCEDURE MANUAL
 POLICIES AND PROCEDURE MANUAL Policy: MP209 Section: Medical Benefit Policy Subject: Medical Error Never Events, Hospital Acquired Conditions, and Hospital Readmission Review I. Policy: Medical Error Never
POLICIES AND PROCEDURE MANUAL Policy: MP209 Section: Medical Benefit Policy Subject: Medical Error Never Events, Hospital Acquired Conditions, and Hospital Readmission Review I. Policy: Medical Error Never
Serious Reportable Events (SREs) Transparency & Accountability are Critical to Reducing Medical Errors
 Transparency & Accountability are Critical to Reducing Medical Errors") Serious Reportable Events (SREs) Transparency & Accountability are Critical to Reducing Medical Errors Tens of thousands of lives are forever changed each year as a result of healthcare errors. There is
Serious Reportable Events (SREs) Transparency & Accountability are Critical to Reducing Medical Errors Tens of thousands of lives are forever changed each year as a result of healthcare errors. There is
EXPERIENCE OF NH HOSPITALS: FALLS DATA NH FALLS RISK REDUCTION TASK FORCE ANNUAL DATA MEETING MARCH 7, 2017 PRESENTED BY: ANNE DIEFENDORF FOUNDATION
 EXPERIENCE OF NH HOSPITALS: FALLS DATA NH FALLS RISK REDUCTION TASK FORCE ANNUAL DATA MEETING MARCH 7, 2017 PRESENTED BY: ANNE DIEFENDORF FOUNDATION FOR HEALTHY COMMUNITIES Objectives Review 2015 NH Adverse
EXPERIENCE OF NH HOSPITALS: FALLS DATA NH FALLS RISK REDUCTION TASK FORCE ANNUAL DATA MEETING MARCH 7, 2017 PRESENTED BY: ANNE DIEFENDORF FOUNDATION FOR HEALTHY COMMUNITIES Objectives Review 2015 NH Adverse
Sample Reportable Events
 Sample Reportable Events This list serves as a guideline of event types typically reported through the ERS (Event Reporting System), online event reporting software. These examples come from hospitals
Sample Reportable Events This list serves as a guideline of event types typically reported through the ERS (Event Reporting System), online event reporting software. These examples come from hospitals
SERIOUS REPORTABLE EVENTS IN HEALTHCARE 2011 UPDATE: A CONSENSUS REPORT
 DRAFT DRAFT DRAFT NATIONAL QUALITY FORUM SERIOUS REPORTABLE EVENTS IN HEALTHCARE 2011 UPDATE: A CONSENSUS REPORT DRAFT REPORT FOR VOTING DRAFT DRAFT DRAFT NATIONAL QUALITY FORUM SERIOUS REPORTABLE EVENTS
DRAFT DRAFT DRAFT NATIONAL QUALITY FORUM SERIOUS REPORTABLE EVENTS IN HEALTHCARE 2011 UPDATE: A CONSENSUS REPORT DRAFT REPORT FOR VOTING DRAFT DRAFT DRAFT NATIONAL QUALITY FORUM SERIOUS REPORTABLE EVENTS
New Hampshire Insurance Department. Report on Hospital Tiering for the HealthFirst Standard Benefit Design. For Calendar year 2011.
 New Hampshire Insurance Department Report on Hospital Tiering for the HealthFirst Standard Benefit Design For Calendar year 2011 November 30, 2010 Introduction HealthFirst was first offered during calendar
New Hampshire Insurance Department Report on Hospital Tiering for the HealthFirst Standard Benefit Design For Calendar year 2011 November 30, 2010 Introduction HealthFirst was first offered during calendar
GENERAL ADMINISTRATIVE POLICY: ADVERSE EVENT REPORTING TO CALIFORNIA DEPARTMENT OF PUBLIC HEALTH (CDPH)
") GENERAL ADMINISTRATIVE POLICY: ADVERSE EVENT REPORTING TO CALIFORNIA DEPARTMENT OF PUBLIC HEALTH (CDPH) Effective Date: 02/12 Page No. 1 of 7 I. PURPOSE To comply with mandated reporting requirements of
GENERAL ADMINISTRATIVE POLICY: ADVERSE EVENT REPORTING TO CALIFORNIA DEPARTMENT OF PUBLIC HEALTH (CDPH) Effective Date: 02/12 Page No. 1 of 7 I. PURPOSE To comply with mandated reporting requirements of
Subject: Hospital-Acquired Conditions (Page 1 of 5)
") Subject: Hospital-Acquired Conditions (Page 1 of 5) Objective: I. To facilitate safe patient care for all Health Share/Tuality Health Alliance (THA) members. II. To encourage and support provider efforts
Subject: Hospital-Acquired Conditions (Page 1 of 5) Objective: I. To facilitate safe patient care for all Health Share/Tuality Health Alliance (THA) members. II. To encourage and support provider efforts
A new freedom of choice for the state where freedom means everything.
 A new freedom of choice for the state where freedom means everything. Anthem HMO Blue New England Choice 04110NHMENABS 04/15 For Large Group only Choose your doctors and your hospitals all across New England.
A new freedom of choice for the state where freedom means everything. Anthem HMO Blue New England Choice 04110NHMENABS 04/15 For Large Group only Choose your doctors and your hospitals all across New England.
Any other findings required by other provisions of law as precondition to adoption or effectiveness of rule? Yes No If Yes, explain:
 RULE-MAKING ORDER Agency: Health Care Authority, Medicaid Program CR-103P (May 2009) (Implements RCW 34.05.360) Permanent Rule Only Effective date of rule: Permanent Rules 31 days after filing. Other (specify)
RULE-MAKING ORDER Agency: Health Care Authority, Medicaid Program CR-103P (May 2009) (Implements RCW 34.05.360) Permanent Rule Only Effective date of rule: Permanent Rules 31 days after filing. Other (specify)
ETHICAL CONSIDERATIONS THAT ARISE IN LONG TERM CARE PART 2 REPORTING OBLIGATIONS
 ETHICAL CONSIDERATIONS THAT PART 2 REPORTING OBLIGATIONS Brian D. Pagano, Esq Burns White LLC bdpagano@burnswhite.com Event: Different Types of Events A discrete, auditable, and clearly defined occurrence.
ETHICAL CONSIDERATIONS THAT PART 2 REPORTING OBLIGATIONS Brian D. Pagano, Esq Burns White LLC bdpagano@burnswhite.com Event: Different Types of Events A discrete, auditable, and clearly defined occurrence.
POLICY NAME POLICY # Sentinel, Adverse Event and Near Miss. CSP Reporting and Investigation
 Purpose To outline a reporting system that promotes client safety by learning from experiences and utilizing the results of investigations and data analysis to prepare and disseminate recommendations for
Purpose To outline a reporting system that promotes client safety by learning from experiences and utilizing the results of investigations and data analysis to prepare and disseminate recommendations for
Consumers Union/Safe Patient Project Page 1 of 7
 Improving Hospital and Patient Safety: An overview of recently passed legislation and requirements towards improving the safety of California s hospital patients June 2009 Background Since 2006 several
Improving Hospital and Patient Safety: An overview of recently passed legislation and requirements towards improving the safety of California s hospital patients June 2009 Background Since 2006 several
Barriers to People Receiving the Right Care
 Barriers to People Receiving the Right Care July 19, 2017 Executive Summary This report identifies barriers to people receiving the right care at the right time throughout New Hampshire. Hospital patients
Barriers to People Receiving the Right Care July 19, 2017 Executive Summary This report identifies barriers to people receiving the right care at the right time throughout New Hampshire. Hospital patients
(1) Provides a brief overview of CMS Medicare payment policy for selected HACs;
 Provides a brief overview of CMS Medicare payment policy for selected HACs;") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-26-12 Baltimore, Maryland 21244-1850 Center for Medicaid and State Operations SMDL #08-004
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-26-12 Baltimore, Maryland 21244-1850 Center for Medicaid and State Operations SMDL #08-004
Information on How to Prevent Pressure Ulcers ( Bedsores ) for Patients, Relatives and Carers in Hospital and in the Community
 for Patients, Relatives and Carers in Hospital and in the Community") Information on How to Prevent Pressure Ulcers ( Bedsores ) for Patients, Relatives and Carers in Hospital and in the Community Tissue Viability Team Community & Therapy Services This leaflet has been designed
Information on How to Prevent Pressure Ulcers ( Bedsores ) for Patients, Relatives and Carers in Hospital and in the Community Tissue Viability Team Community & Therapy Services This leaflet has been designed
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
SKILLED NURSING HOME RISK MONITOR METRICS
 The Risk Monitor offers three views: FACILITY 1st column, total number year-to-date (calculated by the system, from January and including the current month); 2nd column, actual numbers submitted by your
The Risk Monitor offers three views: FACILITY 1st column, total number year-to-date (calculated by the system, from January and including the current month); 2nd column, actual numbers submitted by your
Patient Safety (PS) 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.
 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.") Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
Understand nurse aide skills needed to promote skin integrity.
 Unit B Resident Care Skills Essential Standard NA5.00 Understand nurse aide s role in providing residents hygiene, grooming, and skin care. Indicator Understand nurse aide skills needed to promote skin
Unit B Resident Care Skills Essential Standard NA5.00 Understand nurse aide s role in providing residents hygiene, grooming, and skin care. Indicator Understand nurse aide skills needed to promote skin
SURGICAL SAFETY CHECKLIST
 SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
New Mexico DDSD General Events Report (GER) Guide
 Guide") New Mexico DDSD General Events Report (GER) Guide GER APPLICABILITY: All events that occur during delivery of Supported Living, Family Living, Intensive Medical Living, Customized In-Home Supports, Customized
New Mexico DDSD General Events Report (GER) Guide GER APPLICABILITY: All events that occur during delivery of Supported Living, Family Living, Intensive Medical Living, Customized In-Home Supports, Customized
Required Organizational Practices Resources for 2016
 Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
The Joint Commission and Facility Design: A Partnership for Patient Safety and Quality Care
 The Joint Commission and Facility Design: A Partnership for Patient Safety and Quality Care A Webinar Presentation for the AIA AAH 8 January 2013 1 Topic 1: Driving Safety through Good Design Presenter:
The Joint Commission and Facility Design: A Partnership for Patient Safety and Quality Care A Webinar Presentation for the AIA AAH 8 January 2013 1 Topic 1: Driving Safety through Good Design Presenter:
Effective Date: August 31, 2006 SUBJECT: PRESSURE SORE (DECUBITUS ULCER), PREVENTION AND TREATMENT
, PREVENTION AND TREATMENT") COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION - Treatments POLICY NUMBER: 420 Effective Date: August 31, 2006 SUBJECT: PRESSURE SORE (DECUBITUS ULCER), PREVENTION AND TREATMENT 1.
COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION - Treatments POLICY NUMBER: 420 Effective Date: August 31, 2006 SUBJECT: PRESSURE SORE (DECUBITUS ULCER), PREVENTION AND TREATMENT 1.
ADVERSE HEALTH EVENTS IN MINNESOTA
 S E C O N D ANNUAL F EBRUARY 2006 TABLE OF CONTENTS Introduction.................................................. 3 Background................................................... 4 How to use this report.........................................
S E C O N D ANNUAL F EBRUARY 2006 TABLE OF CONTENTS Introduction.................................................. 3 Background................................................... 4 How to use this report.........................................
Contact Hours (CME version ONLY) Suggested Target Audience. all clinical and allied patient care staff. all clinical and allied patient care staff
 Suggested Target Audience. all clinical and allied patient care staff. all clinical and allied patient care staff") 1 Addressing Behaviors That Undermine a Culture of Safety PA CE CME FL 8/31/2016 2 2 7 3 43 1.0 1.0 1.0 all staff Sentinel Event Alert, Issue 40: Behaviors that undermine a culture of safety 2 Adverse
1 Addressing Behaviors That Undermine a Culture of Safety PA CE CME FL 8/31/2016 2 2 7 3 43 1.0 1.0 1.0 all staff Sentinel Event Alert, Issue 40: Behaviors that undermine a culture of safety 2 Adverse
New Jersey Department of Health Report Preparation Team. Abate Mammo, PhD, Acting Executive Director Healthcare Quality and Informatics
 2012 Summary Report New Jersey Department of Health Report Preparation Team Abate Mammo, PhD, Acting Executive Director Healthcare Quality and Informatics Emmanuel Noggoh, Director Health Care Quality
2012 Summary Report New Jersey Department of Health Report Preparation Team Abate Mammo, PhD, Acting Executive Director Healthcare Quality and Informatics Emmanuel Noggoh, Director Health Care Quality
Clinical Policy Title: Provider preventable conditions and hospital acquired conditions
 Clinical Policy Title: Provider preventable conditions and hospital acquired conditions Clinical Policy Number: 18.04.04 Effective Date: July 1, 2016 Initial Review Date: January 20, 2016 Most Recent Review
Clinical Policy Title: Provider preventable conditions and hospital acquired conditions Clinical Policy Number: 18.04.04 Effective Date: July 1, 2016 Initial Review Date: January 20, 2016 Most Recent Review
Patient Safety Course Descriptions
 Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
The Joint Commission:
 The Joint Commission: Over a century of quality and safety 1910-1913 Ernest Codman, M.D. proposes the end result system of hospital standardization. American College of Surgeons is founded. The end result
The Joint Commission: Over a century of quality and safety 1910-1913 Ernest Codman, M.D. proposes the end result system of hospital standardization. American College of Surgeons is founded. The end result
TrainingABC Patient Rights Made Simple Support Materials
 TrainingABC 2017 Patient Rights Made Simple Support Materials Video Transcript The Patient Bill of Rights is a list of rights first developed in 1973 and then revised in 1992, by the American Hospital
TrainingABC 2017 Patient Rights Made Simple Support Materials Video Transcript The Patient Bill of Rights is a list of rights first developed in 1973 and then revised in 1992, by the American Hospital
Pressure Injuries. Care for Patients in All Settings
 Pressure Injuries Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a pressure injury. The scope of the standard
Pressure Injuries Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a pressure injury. The scope of the standard
How to Prevent Pressure Ulcers. Advice for Patients and Carers
 How to Prevent Pressure Ulcers Advice for Patients and Carers This booklet contains the best advice currently available to help people avoid getting a pressure ulcer. It is for people who are at risk
How to Prevent Pressure Ulcers Advice for Patients and Carers This booklet contains the best advice currently available to help people avoid getting a pressure ulcer. It is for people who are at risk
Pressure Ulcers ecourse
 Pressure Ulcers ecourse Module 5.8: Pressure Ulcer Surgery Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Module 5.8: Pressure
Pressure Ulcers ecourse Module 5.8: Pressure Ulcer Surgery Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Module 5.8: Pressure
Challenge Scenario. Featured TAG TOPIC SCENARIO NOTES F314
 TAG TOPIC Give residents proper treatment to prevent new bed (pressure) sores or heal existing bed sores. SCENARIO In this scenario, the facility failed to ensure that residents who were admitted without
TAG TOPIC Give residents proper treatment to prevent new bed (pressure) sores or heal existing bed sores. SCENARIO In this scenario, the facility failed to ensure that residents who were admitted without
Initial Pool Process: Resident Interview
 Initial Pool Process: Resident Interview Care Area Probes Response Options Choices Are you able to make choices about your daily life that are important to you? I d like to talk to you about your choices.
Initial Pool Process: Resident Interview Care Area Probes Response Options Choices Are you able to make choices about your daily life that are important to you? I d like to talk to you about your choices.
New Mexico DDSD General Events Report (GER) Guide
 Guide") New Mexico DDSD General Events Report (GER) Guide APPLICABILITY: All DDW Participants age 21 and older plus DDW Participants age 18-21 who receive Supported Living or Family Living See definitions and
New Mexico DDSD General Events Report (GER) Guide APPLICABILITY: All DDW Participants age 21 and older plus DDW Participants age 18-21 who receive Supported Living or Family Living See definitions and
Appendix 5. Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to the Safeguarding Adults Procedures
 Appendix 5 Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to the Safeguarding Adults Procedures Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to
Appendix 5 Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to the Safeguarding Adults Procedures Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to
CAMH February 2005 Update HIGHLIGHTS
 CAMH February 2005 Update HIGHLIGHTS STANDARD UP 1. How to Use Manual Multiple changes to scoring, category changes and Measure of Success (MOS) designation removed 2. Accreditation Policies & Procedures
CAMH February 2005 Update HIGHLIGHTS STANDARD UP 1. How to Use Manual Multiple changes to scoring, category changes and Measure of Success (MOS) designation removed 2. Accreditation Policies & Procedures
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM
 Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
sample Pressure Sores Prevention & Awareness Copyright Notice This booklet remains the intellectual property of Redcrier Publications L td
 First name: Surname: Company: Date: Pressure Sores Prevention & Awareness Please complete the above, in the blocks provided, as clearly as possible. Completing the details in full will ensure that your
First name: Surname: Company: Date: Pressure Sores Prevention & Awareness Please complete the above, in the blocks provided, as clearly as possible. Completing the details in full will ensure that your
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition
 Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Inspection Protocol Skin and Wound Care. Definition / Description. Use. Resident-related Triggered
 Resident-related Triggered Home Name: Inspection Number: (hard copy use only) Date: Inspector ID: Definition / Description Altered skin integrity: The potential or actual disruption of epidermal or dermal
Resident-related Triggered Home Name: Inspection Number: (hard copy use only) Date: Inspector ID: Definition / Description Altered skin integrity: The potential or actual disruption of epidermal or dermal
Accreditation Program: Long Term Care
 ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
Healthcare Risk Control
 Topics Covered 2016 Administrative Support Services Healthcare Advertising and Marketing Media Relations Social Media in Healthcare Critical Care Clinical Alarms Invasive Lines Pulse Oximetry Risk Management
Topics Covered 2016 Administrative Support Services Healthcare Advertising and Marketing Media Relations Social Media in Healthcare Critical Care Clinical Alarms Invasive Lines Pulse Oximetry Risk Management
Auckland District Health Board Summary 1 July 2011 to 30 June 2012 Serious and Sentinel Events
 DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
WPSC Teleconference Avoiding Never Events. Linda Furkay, PhD, RN Patient Safety Adverse Event Officer
 Linda Furkay, PhD, RN Patient Safety Adverse Event Officer Share Findings from adverse events surgical errors, pressure ulcers, & falls Successful patient safety strategies here in Washington & from other
Linda Furkay, PhD, RN Patient Safety Adverse Event Officer Share Findings from adverse events surgical errors, pressure ulcers, & falls Successful patient safety strategies here in Washington & from other
New data from Minnesota hospitals offers more insight into preventing
 Patient safety Preventing pressure ulcers: New lessons from Minnesota New data from Minnesota hospitals offers more insight into preventing pressure ulcers during long surgical procedures. Data collected
Patient safety Preventing pressure ulcers: New lessons from Minnesota New data from Minnesota hospitals offers more insight into preventing pressure ulcers during long surgical procedures. Data collected
Appendix Five Decision Pathway Pressure Ulcers and safeguarding Adults (A3 format)
") Appendix Five Decision Pathway Pressure Ulcers and safeguarding Adults (A3 format) Pressure ulcer is observed. Concern is raised that a person has significant skin damage. Category / Grade 3 and 4 or Multiple
Appendix Five Decision Pathway Pressure Ulcers and safeguarding Adults (A3 format) Pressure ulcer is observed. Concern is raised that a person has significant skin damage. Category / Grade 3 and 4 or Multiple
3/12/2015. Session Objectives. RAI User s Manual. Polling Question
 Session Objectives MDS 3.0 Coding Challenges: Questions, Answers, and Explanations Jen Pettis, BS, RN, WCC Associate March 19, 2015 Upon completion of the program, the participate will: Describe the four
Session Objectives MDS 3.0 Coding Challenges: Questions, Answers, and Explanations Jen Pettis, BS, RN, WCC Associate March 19, 2015 Upon completion of the program, the participate will: Describe the four
Pressure Ulcer Prevention
 Information for patients This leaflet can be made available in other formats including large print, CD and Braille and in languages other than English, upon request. This leaflet has been adapted from
Information for patients This leaflet can be made available in other formats including large print, CD and Braille and in languages other than English, upon request. This leaflet has been adapted from
HealthStream Ambulatory Regulatory Course Descriptions
 This course covers three related aspects of medical care. All three are critical for the safety of patients. Avoiding Errors: Communication, Identification, and Verification These three critical issues
This course covers three related aspects of medical care. All three are critical for the safety of patients. Avoiding Errors: Communication, Identification, and Verification These three critical issues
ADVERSE HEALTH EVENTS IN MINNESOTA HOSPITALS
 JANUARY 2005 ADVERSE HEALTH EVENTS IN MINNESOTA HOSPITALS FIRST ANNUAL PUBLIC REPORT 3 ADVERSE HEALTH EVENTS IN MINNESOTA HOSPITALS MDH 2 0 0 5 TABLE OF CONTENTS 2 HOW TO USE THIS REPORT 3 SELECTED SAFETY
JANUARY 2005 ADVERSE HEALTH EVENTS IN MINNESOTA HOSPITALS FIRST ANNUAL PUBLIC REPORT 3 ADVERSE HEALTH EVENTS IN MINNESOTA HOSPITALS MDH 2 0 0 5 TABLE OF CONTENTS 2 HOW TO USE THIS REPORT 3 SELECTED SAFETY
Cynthia M. Kirchner, MPH, Director, Quality Improvement. Emmanuel Noggoh, Director, Health Care Quality Assessment
 2010 Summary Report Office of Health Care Quality Assessment Report Preparation Team Cynthia M. Kirchner, MPH, Director, Quality Improvement Emmanuel Noggoh, Director, Health Care Quality Assessment Mary
2010 Summary Report Office of Health Care Quality Assessment Report Preparation Team Cynthia M. Kirchner, MPH, Director, Quality Improvement Emmanuel Noggoh, Director, Health Care Quality Assessment Mary
Towards Quality Care for Patients. Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care
 Towards Quality Care for Patients Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care National Department of Health 2011 National Core Standards for Health Establishments in South
Towards Quality Care for Patients Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care National Department of Health 2011 National Core Standards for Health Establishments in South
Preventing Falls in the Home
 ~ VOLUME I ISSUE V LESSON PLAN ~ OBJECTIVES Upon completion of this program, the home health aide will be able to:» Identify four variables that increase the likelihood of falls» List three common hazards
~ VOLUME I ISSUE V LESSON PLAN ~ OBJECTIVES Upon completion of this program, the home health aide will be able to:» Identify four variables that increase the likelihood of falls» List three common hazards
SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER. Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow
 SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow I. Clinical Mission of the North Carolina Jaycee Burn Center The clinical
SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow I. Clinical Mission of the North Carolina Jaycee Burn Center The clinical
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager
 Ratchada Prakongsai Senior Manager") Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
GENERAL HOSPITAL ORIENTATION Revised: January 2013 EE Intl Hosp Ort
 GENERAL HOSPITAL ORIENTATION 2013-2014 1 GOOD SAMARITAN HOSPITAL MANDATORY EDUCATION CLASSES ATTENDANCE OR SELF-LEARNING MODULE ACKNOWLEDGEMENT Organizational Mission, Vision, and Goals Cultural Diversity
GENERAL HOSPITAL ORIENTATION 2013-2014 1 GOOD SAMARITAN HOSPITAL MANDATORY EDUCATION CLASSES ATTENDANCE OR SELF-LEARNING MODULE ACKNOWLEDGEMENT Organizational Mission, Vision, and Goals Cultural Diversity
The Criminalization of Adverse Events. Joy Schank, MSN Caroline E. Fife, MD,
 The Criminalization of Adverse Events Joy Schank, MSN Caroline E. Fife, MD, Patient wanted to die at home and niece agreed to care for her Advanced Alzheimer s Called 911 Cause of death: Sepsis due to
The Criminalization of Adverse Events Joy Schank, MSN Caroline E. Fife, MD, Patient wanted to die at home and niece agreed to care for her Advanced Alzheimer s Called 911 Cause of death: Sepsis due to
Chapter 14. Body Mechanics and Safe Resident Handling, Positioning, and Transfers
 Chapter 14 Body Mechanics and Safe Resident Handling, Positioning, and Transfers Body Mechanics Body mechanics means using the body in an efficient and careful way. It involves: Good posture Balance Using
Chapter 14 Body Mechanics and Safe Resident Handling, Positioning, and Transfers Body Mechanics Body mechanics means using the body in an efficient and careful way. It involves: Good posture Balance Using
Recommendations and Guidance for Application of the Adverse Health Event Definitions
 Recommendations and Guidance for Application of the Adverse Health Event Definitions March 2017 The MHA Patient Safety Registry Advisory Committee has been working on recommendations for definitional questions
Recommendations and Guidance for Application of the Adverse Health Event Definitions March 2017 The MHA Patient Safety Registry Advisory Committee has been working on recommendations for definitional questions
Attachment A - Comparison of OASIS-C (Current Version) to OASIS-C1 (Proposed Data Collection)
 to OASIS-C1 (Proposed Data Collection)") Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
Medicare Won t Pay for Medical Errors
 Medicare Won t Pay for Medical Errors By KEVIN SACK October 1, 2008 New York Times ST. PAUL If an auto mechanic accidentally breaks your windshield while trying to repair the engine, he would never get
Medicare Won t Pay for Medical Errors By KEVIN SACK October 1, 2008 New York Times ST. PAUL If an auto mechanic accidentally breaks your windshield while trying to repair the engine, he would never get
Examples of enforcement letters to Adult Family Homes certified to care for people with Developmental Disabilities in Washington State
 Examples of enforcement letters to Adult Family Homes certified to care for people with Developmental Disabilities in Washington State Repeated, uncorrected violations highlighted All information retrieved
Examples of enforcement letters to Adult Family Homes certified to care for people with Developmental Disabilities in Washington State Repeated, uncorrected violations highlighted All information retrieved
Department of Defense INSTRUCTION. SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP)
 Patient Safety Program (PSP) (MHSPSP)") Department of Defense INSTRUCTION NUMBER 6025.17 August 16, 2001 SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP) ASD(HA) References: (a) Sections 742 and 754 of the Floyd D.
Department of Defense INSTRUCTION NUMBER 6025.17 August 16, 2001 SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP) ASD(HA) References: (a) Sections 742 and 754 of the Floyd D.
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Abdomino-perineal Resection/Excision of the Rectum
 Abdomino-perineal Resection/Excision of the Rectum What is an Abdomino-perineal Resection/Excision of Rectum? An Abdomino-perineal Resection/Excision of Rectum is the surgical removal of part of the large
Abdomino-perineal Resection/Excision of the Rectum What is an Abdomino-perineal Resection/Excision of Rectum? An Abdomino-perineal Resection/Excision of Rectum is the surgical removal of part of the large
Update on the Maryland Patient Safety Program
 Update on the Maryland Patient Safety Program Department of Heath and Mental Hygiene Wendy Kronmiller, Director Renee Webster, Assistant Director Anne Jones RN, Nurse Surveyor Third Annual Maryland Patient
Update on the Maryland Patient Safety Program Department of Heath and Mental Hygiene Wendy Kronmiller, Director Renee Webster, Assistant Director Anne Jones RN, Nurse Surveyor Third Annual Maryland Patient
Immunizations Criminal Background check Infection Control HIPPA Health Insurance Portability and Accountability Act
 Reedsburg Area Senior Life Center Welcome to Reedsburg Area Senior Life Center for your clinical! We hope you will have a positive and rewarding learning experience. If you have any questions during your
Reedsburg Area Senior Life Center Welcome to Reedsburg Area Senior Life Center for your clinical! We hope you will have a positive and rewarding learning experience. If you have any questions during your
E: Nursing Practice. Alberta Licensed Practical Nurses Competency Profile 51
 E: Nursing Practice Alberta Licensed Practical Nurses Competency Profile 51 Competency: E-1 Critical Thinking E-1-1 E-1-2 E-1-3 Demonstrate knowledge and ability to apply critical thinking concepts throughout
E: Nursing Practice Alberta Licensed Practical Nurses Competency Profile 51 Competency: E-1 Critical Thinking E-1-1 E-1-2 E-1-3 Demonstrate knowledge and ability to apply critical thinking concepts throughout
Patient Falls Metric (2018)
") Patient Falls Metric (2018) Falls Unintentionally coming to rest on the ground, floor or other lower surface (NPSA 2010) Include all slips, trips and falls e.g. if a patient is found on the floor, lowered
Patient Falls Metric (2018) Falls Unintentionally coming to rest on the ground, floor or other lower surface (NPSA 2010) Include all slips, trips and falls e.g. if a patient is found on the floor, lowered
GENERAL EVENTS REPORTING REQUIREMENTS
 GENERAL EVENTS REPORTING REQUIREMENTS DDSD is pleased to introduce the revised General Events Reporting (GER) requirements. There are two important changes related to medication error reporting: 1. Effective
GENERAL EVENTS REPORTING REQUIREMENTS DDSD is pleased to introduce the revised General Events Reporting (GER) requirements. There are two important changes related to medication error reporting: 1. Effective
PRESSURE ULCER PREVENTION SIMPLIFIED
 10 PRESSURE ULCER PREVENTION SIMPLIFIED This simplified leaflet is intended to give you information about pressure ulcer and aid your clinical practice PRESSURE ULCER PREVENTION SIMPLIFIED Pressure ulcer
10 PRESSURE ULCER PREVENTION SIMPLIFIED This simplified leaflet is intended to give you information about pressure ulcer and aid your clinical practice PRESSURE ULCER PREVENTION SIMPLIFIED Pressure ulcer
QUESTIONS PERTINENT TO PRODUCT SELECTION:
 QUESTIONS PERTINENT TO PRODUCT SELECTION: Impact on patient outcomes Impact on patient/staff safety Economic considerations Use the following pages to help facilitate discussion with vendors, write your
QUESTIONS PERTINENT TO PRODUCT SELECTION: Impact on patient outcomes Impact on patient/staff safety Economic considerations Use the following pages to help facilitate discussion with vendors, write your
Sentinel Event Data. Root Causes by Event Type Copyright, The Joint Commission
 Sentinel Event Data Root Causes by Event Type 2004 2014 Joint Commission Root Cause Information www.jointcommission.org/sentinel_event_policy_and_procedures/ Sentinel Events are reported to The Joint Commission
Sentinel Event Data Root Causes by Event Type 2004 2014 Joint Commission Root Cause Information www.jointcommission.org/sentinel_event_policy_and_procedures/ Sentinel Events are reported to The Joint Commission
Patient Safety. If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator Updated:
 Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
National Patient Safety Goals Effective January 1, 2016
 National Patient Safety Goals Effective January 1, 2016 Goal 1 Improve the accuracy of patient identification. NPSG.01.01.01 Home are Accreditation Program Use at least two patient identifiers when providing
National Patient Safety Goals Effective January 1, 2016 Goal 1 Improve the accuracy of patient identification. NPSG.01.01.01 Home are Accreditation Program Use at least two patient identifiers when providing
Provider Rate Table Residential Habilitation Services in a Licensed Facility Effective April 1, 2011
 Provider Table Residential Habilitation Services in a Licensed Facility Effective April 1, 2011 Residential Habilitation Services - s with April 1, 2011 Reductions Without Geographic Factor With Geographic
Provider Table Residential Habilitation Services in a Licensed Facility Effective April 1, 2011 Residential Habilitation Services - s with April 1, 2011 Reductions Without Geographic Factor With Geographic
National Patient Safety Goals
 III. PATIENT SAFETY National Patient Safety Goals The National Patient Safety Goals for Hospital, Laboratory and Home Health Programs have been developed to improve patient safety. Ask your Volunteer Office
III. PATIENT SAFETY National Patient Safety Goals The National Patient Safety Goals for Hospital, Laboratory and Home Health Programs have been developed to improve patient safety. Ask your Volunteer Office
The Leapfrog Hospital Survey Scoring Algorithms. Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey
 The Leapfrog Hospital Survey Scoring Algorithms Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey 2017 Leapfrog Hospital Survey Scoring Algorithms Table of Contents 2017 Leapfrog Hospital
The Leapfrog Hospital Survey Scoring Algorithms Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey 2017 Leapfrog Hospital Survey Scoring Algorithms Table of Contents 2017 Leapfrog Hospital
A Patient s Guide to Pressure Ulcer Prevention
 A Patient s Guide to Pressure Ulcer Prevention This leaflet has been written to give you information, which may help you to understand the care delivered, to prevent pressure ulcer development during your
A Patient s Guide to Pressure Ulcer Prevention This leaflet has been written to give you information, which may help you to understand the care delivered, to prevent pressure ulcer development during your
Based on the comprehensive assessment of a resident, the facility must ensure that:
 7. QUALITY OF CARE Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental and psychosocial wellbeing,
7. QUALITY OF CARE Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental and psychosocial wellbeing,
Medical Staff Rules & Regulations Last Updated: October University Hospital Medical Staff. Rules & Regulations
 University Hospital Medical Staff Rules & Regulations 1 UNIVERSITY HOSPITAL MEDICAL STAFF RULES AND REGULATIONS The Medical Staff shall adopt Rules and Regulations as may be necessary to implement the
University Hospital Medical Staff Rules & Regulations 1 UNIVERSITY HOSPITAL MEDICAL STAFF RULES AND REGULATIONS The Medical Staff shall adopt Rules and Regulations as may be necessary to implement the
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Queen Elizabeth Medical Centre Edgbaston, Birmingham, B15 2TH
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Queen Elizabeth Medical Centre Edgbaston, Birmingham, B15 2TH
SAMPLE Bariatric Surgery Program Survey for Facilities and Surgeons
 I. Facility Section (to be completed by the facility s risk and/or quality department) Facility Name: Address: Date: Contact Person: Directions Please check the appropriate yes or no answer boxes where
I. Facility Section (to be completed by the facility s risk and/or quality department) Facility Name: Address: Date: Contact Person: Directions Please check the appropriate yes or no answer boxes where
ADVERSE HEALTH EVENTS IN MINNESOTA
 ADVERSE HEALTH EVENTS IN MINNESOTA 13 TH ANNUAL PUBLIC REPORT FEBRUARY 2017 HEALTH POLICY ADVERSE HEALTH EVENTS IN MINNESOTA ANNUAL REPORT, FEBRUARY 2017 Adverse Health In Minnesota Annual Report February
ADVERSE HEALTH EVENTS IN MINNESOTA 13 TH ANNUAL PUBLIC REPORT FEBRUARY 2017 HEALTH POLICY ADVERSE HEALTH EVENTS IN MINNESOTA ANNUAL REPORT, FEBRUARY 2017 Adverse Health In Minnesota Annual Report February
NHS HIGHLAND. Significant Event Report
 ` NHS HIGHLAND Significant Event Report Report to - Quality & Patient Safety Raigmore Management Team of Findings from Significant Event Review Meeting QPS040 26/10/2011 1.0 Outline of Significant Event
` NHS HIGHLAND Significant Event Report Report to - Quality & Patient Safety Raigmore Management Team of Findings from Significant Event Review Meeting QPS040 26/10/2011 1.0 Outline of Significant Event
What you can do to help stop the spread of MRSA and other infections
 MRSA wash it away As a patient it is important that you get better quickly and stay well. This leaflet gives you information about MRSA and other health care associated infections, so that you know what
MRSA wash it away As a patient it is important that you get better quickly and stay well. This leaflet gives you information about MRSA and other health care associated infections, so that you know what
Fundamentals of Care. Do you receive care Do you know what to expect? Do you provide care? Quality of care for adults
 Fundamentals of Care Do you receive care Do you know what to expect? Do you provide care? Quality of care for adults Foreword by Jane Hutt, Minister for Health and Social Services The twelve aspects of
Fundamentals of Care Do you receive care Do you know what to expect? Do you provide care? Quality of care for adults Foreword by Jane Hutt, Minister for Health and Social Services The twelve aspects of
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Introduction to Perioperative Nursing
 C H A P T E R 1 Introduction to Perioperative Nursing LEARNER OBJECTIVES 1. Define the three phases of the surgical experience. 2. Describe the scope of perioperative nursing practice. 3. Discuss application
C H A P T E R 1 Introduction to Perioperative Nursing LEARNER OBJECTIVES 1. Define the three phases of the surgical experience. 2. Describe the scope of perioperative nursing practice. 3. Discuss application