Xtreme Makeover PCMH edition. The Miramont Story Presented by John L Bender, M.D., FAAFP May 4 th, 2013 Sonnenalp, CMS 2013 Spring Conference
|
|
|
- Grant Curtis
- 5 years ago
- Views:
Transcription
1 Xtreme Makeover PCMH edition The Miramont Story Presented by John L Bender, M.D., FAAFP May 4 th, 2013 Sonnenalp, CMS 2013 Spring Conference
2 Conflict of Interest Disclosure John L. Bender, M.D. Has no real or apparent conflicts of interest to report.
3 Learning Objectives John L. Bender, M.D. Recognize how NCQA recognition makes it possible to improve safety, efficiency, patient outcomes and profitability in the ambulatory care environment Illustrate the link between NCQA recognition and a successful Meaningful Use implementation strategy Summarize the business case for improved workflows, clinical quality and metrics (aka Registry Reporting)
4 Our story begins in Fort Collins Colorado H.G. Carlson, M.D. One of the oldest practices in Fort Collins Open 8-5 most days Paper Charts One Employee One Computer (386) 1000 patients

5

6 In a basement, paneling on the walls

7 Walls of Paper Charts
8 Move that Bus!!!

9
10 Our story today 2013 in Larimer County Colorado. 4 locations in 3 separate communities Open M-F 8-8, Saturdays providers 58 employees Electronic Charts, Patient Portal, NCQA III PCMH recognition Over 100 company computers operating in a terminal service environment and a centralized data center 30,000 patients Davies Ambulatory Award recognition from HiMSS in 2010

11 4 th fastest growing company in Northern Colorado
12 Miramont s Growth Curve year receipts volume 2001 $169, , , , , , ,449, ,940, ,616, ,505, ,356, ,804, ,000,000 4,500,000 4,000,000 year 3,500,000 3,000,000 2,500,000 2,000,000 1,500,000 1,000, ,000 0 receipts volume 2001 $169, , , , , , ,449, ,940, ,616, ,505, ,356, ,804, Miramont's Growth as measured by receipts

13 2010 HIMSS Ambulatory Award

14 2011 Colorado PCMH of the Year
15 34 primary care physicians leave practice during the same time specialty gender year of transition practice zip code event Family Medicine female closed/unable to service debt Family Medicine male Family Medicine male moved to work for Orthopedists Family Medicine male closed/unable to service debt Family Medicine male sudden death, age 52 Internal Medicine male sold/less profitable Internal Medicine male sold/less profitable Family Medicine male sold/less profitable Internal Medicine male sold/less profitable Family Medicine female closed/unable to service debt Family Medicine female closed/unable to service debt Family Medicine male closed/unable to service debt Family Medicine female closed/unable to service debt Internal Medicine male sold/less profitable Family Medicine female closed/unable to service debt Family Medicine male closed/? Internal Medicine male closed/moved to BTMG Family Medicine female I can not disclose under contract Gynecology male closed/divorce? OB/Gyn female ? OB/Gyn female ? Family Medicine female ? OB/Gyn female ? Family Medicine male unable to service debt Family Medicine male uncertain Family Medicine male offered job in Sports Medicine Family Medicine male sold/less profitable Internal Medicine female Internal Medicine male sold/less profitable Family Medicine male closed by CRMC, non profitable
16 8 are bankruptcies specialty gender year of transition practice zip code event Family Medicine female closed/unable to service debt Family Medicine male Family Medicine male moved to work for Orthopedists Family Medicine male closed/unable to service debt Family Medicine male sudden death, age 52 Internal Medicine male sold/less profitable Internal Medicine male sold/less profitable Family Medicine male sold/less profitable Internal Medicine male sold/less profitable Family Medicine female closed/unable to service debt Family Medicine female closed/unable to service debt Family Medicine male closed/unable to service debt Family Medicine female closed/unable to service debt Internal Medicine male sold/less profitable Family Medicine female closed/unable to service debt Family Medicine male closed/? Internal Medicine male closed/moved to BTMG Family Medicine female I can not disclose under contract Gynecology male closed/divorce? OB/Gyn female ? OB/Gyn female ? Family Medicine female ? OB/Gyn female ? Family Medicine male unable to service debt Family Medicine male uncertain Family Medicine male offered job in Sports Medicine Family Medicine male sold/less profitable Internal Medicine female Internal Medicine male sold/less profitable Family Medicine male closed by CRMC, non profitable
17 Hospital Movement IN the past 4 years: The number of EM physicians double, and ED utilization increases by 50%. IN the past 2 years: 250 physicians become employees of the local hospital owned medical group (600 total physicians in the county)
18 Our Product in 2002 Test results are slow Labor costs high with much non-revenue generating activity / waste No open appointments No clinical data management Barely any financial data management High variability in patient experiences from day to day Documentation illegible Unable to compete with retail clinics, urgent care, emergency departments, etc.

19 Wanting to get out of last century

20 Company Retreat August 2007
21 Ambulatory Medicine Needs to Have a Vision Where there is no vision, the people perish Proverbs 29:18
22 Positioning Statement: For local families desiring healthcare, Miramont Family Medicine is the choice that offers the most convenience and the highest value
23 Miramont Mission Statement to deliver compassionate, modern, timely healthcare in a clean, professional environment that promotes patient and staff growth, health, and happiness

24 The Restaurant with Bad Food
25 Made friends with the banker, accountant, attorney and local business leaders We decided it would take money to make money and the process starts with investing We pledged that we would make Miramont safer, more efficient, and up to date Ensure our own profitability at all times in order that we could be there for our patients for many years to come Eliminate as much as possible non-revenue generating activity Find ways to provide needed services in our house, in the free market health care system that we are given Find a better EHR (transition out of a free product we acquired in 2005) Attain NCQA recognition for a Patient Centered Medical Home

26 $1.4 million in new building in 2005
27 Every Year We Bring New Products and Services 2002 Female Provider, DEXA scanner 2003 Level 2 Laboratory, IV therapy 2004 Visiting Surgeon, 8-5 hours M-F 2005 New Building, X-ray, bilingual services 2006 Physical Therapy, Psychotherapy, After Hours 2007 INS, Coumadin clinic, Nerve Conduction studies, Saturday hours, Nurse Educator 2008 Female Physician, Colposcopy, Pain Management Specialist, Group visits, The Dispensary, Psychologist
28 Every Year We Bring New Products and Services 2009 Patient Centered Medical Home, New Website, patient portal, online registration, online scheduling requests, online bill payment, Miramont Value Plan (MVP), Allergy Testing and AIT, Second location and Third Locations, Laser Aesthetic Medicine 2010 Botox, digital Mammography, Audiology, Pediatrician, CEO level administrator, blast marketing to patient base, automated collections calls 2011DME sales, drive through pharmacy, fluoride dental treatments for children th location in Parker Colorado, self check in kiosks, Phreesia tablets, Medtronics Insulin pumps, ipro
29 THE PROCESS OF GAINING NCQA RECOGNITION or ACHIEVING MEANINGFUL USE IS A WORKFLOW REDESIGN PROCESS IN ITSELF
30 Quality Meaningful Use Basic Tenants in the PCMH/Specialist Practice Transformation: Physician Leaders who are willing to lead a team. Every person on the team must be empowered to contribute to process improvement and workflow redesign
31 Toyota Production Model The Toyota Production Model: The Toyota Way is built on two pillars, continuous improvement (kaizen), and respect for all people PDSA cycle Plan, Do, Study, Act
32 PDSA: Action Plan State the problem being addresses State the purpose of the proposed change State the specific AIM and associated measure State the action-oriented objectives What will be done!!
33 PDSA: Do State specific tasks to achieve each objective State who will do these tasks State timelines for completing tasks Who is accountable for getting things done!!
34 PDSA: Study Select qualitative and quantitative measures Complete analysis of measures Compare results with baseline values Summarize and reflect on what was learned from the data
35 PDSA: Study PDSA: Study Performance Measures Linked to Project Aims Types of Measures: How Well (efficiency) Impact (outcome) If you do not measure, you will not sustain redesign
36 PDSA: Act Determine what modifications should be made in the redesign process Prepare and plan for next test cycle to implement the modifications
37 Continuous Improvement At Miramont, we call the constant change brain damage BUT, we are not burned out, we are burned in. Even our customers are trained to look for what s new at Miramont
38 Respect for all People If there are any problems in quality... any of our employees can pull this switch to stop the production line former Toyota US President Yoshio Ishizaka Hospital equivalent: the Time Out Is there an Ambulatory Equivalent??

39 Ambulatory Checklists
40 Respect for all People The Wisdom of Crowds James Surowiecki The group will give better advice than an expert, or a guess
41 Respect for all People Who knows the weight of the Ox??
42 Respect for all People Who knows the weight of the Ox?? Answer: The crowd knows the weight!!

43 Respect for all People What is the best lifeline??

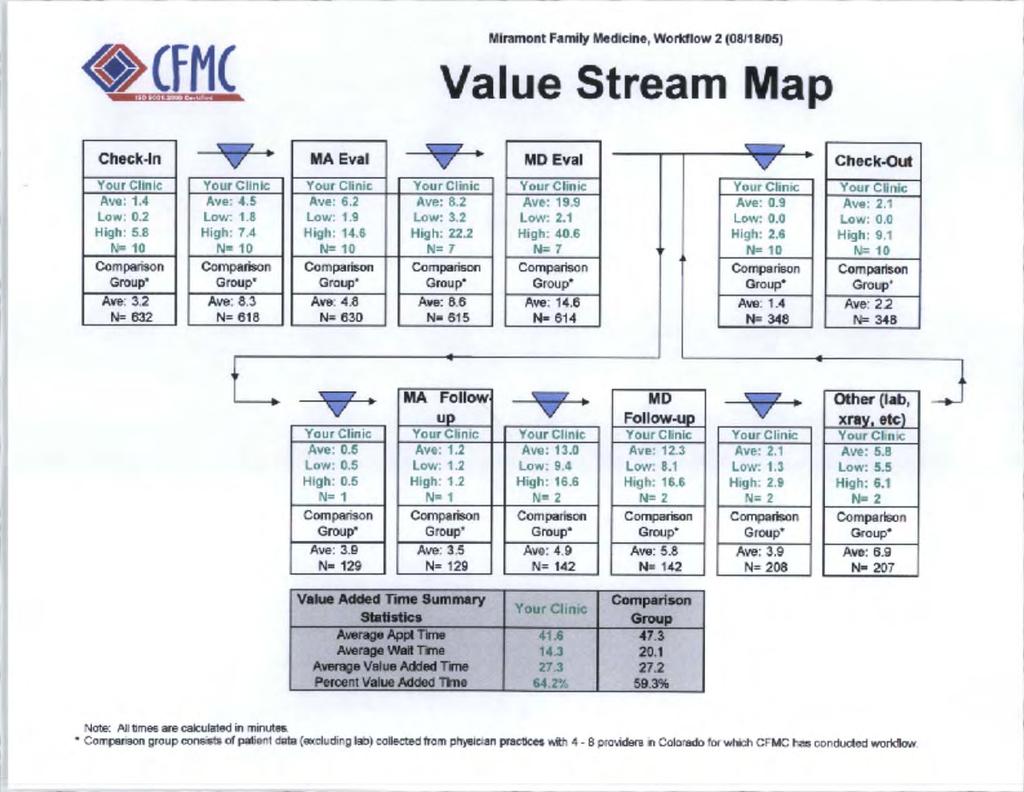
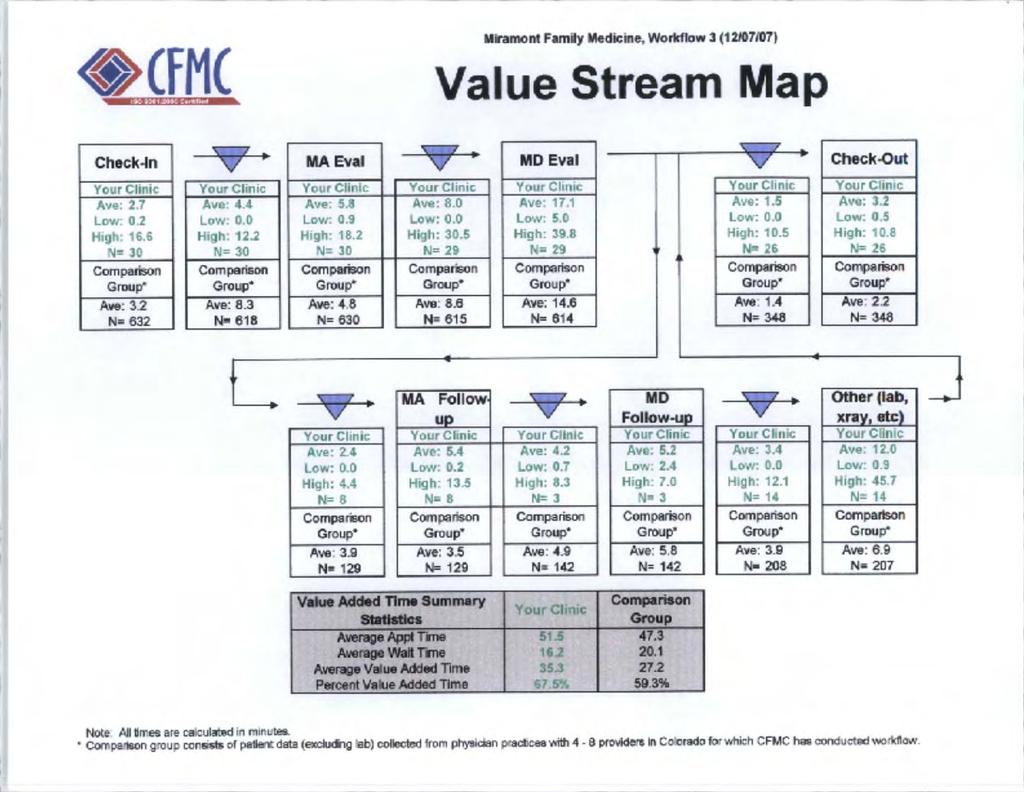
44 How to Make a Physician Owned Lab (POL) Work in Your Office: Evaluating the Costs and Benefits John L Bender, M.D., FAAFP & Amanda J. Cline, RMA
45 Old Model Physician orders test MA fills out requisition Patient given directions to local lab Patient drives to lab, has test drawn Outside lab runs test Test is reported back to physician next business day MA pulls chart to go with test Physician reviews test, signs it off, and tries to remember what he/she was looking for
46 Old Model, continued MA calls and leaves message on answering machine telling patient that results are in but unfortunately due to HIPAA cannot leave results on machine and patient will now have to call back Patient s spouse hears message, assumes the worst, and calls back three times with an urgent message asking for a return call from physician MA finally makes contact with patient, new medication is ordered, another follow-up visit is scheduled with repeat blood work ordered Receptionist refiles chart. TOTAL TIME: 20 + minutes
47 New Model Physician orders test MA draws patient Test is run in house Result is reported in room to physician and patient Decision is made for new med, result is signed off Patient schedules follow up at check-out Chart is filed TOTAL TIME: 10 minutes
48 Value Added Team We asked the Colorado Foundation for Medical Care to send the Value Added Team ( VAT ) with their stopwatches to measure our patient processing times before and after implementation. We learned that our percent value added time improved from 64.2% to 67.5%, a huge accomplishment considering that our average appointment time increased from 41 minutes in paper to 51 minutes electronically (appendix G). We now track more metrics, spend more time with our patients educating them, and waste less of their time when they are with us. Our online surveys tell us that it is easy for our patients to make appointments 97%
49
50

51 We finally know how many diabetics we have
52 A1C documentation improved over time


53 Managing population metrics for chronic disease is realistic with an EHR
54 External reporting for Fun and Profit Colorado PCMH Pilot Miramont was one of 17 clinics to participate in the Colorado Patient-Centered Medical Home (PCMH) pilot, a joint-venture between HealthTeamWorks and five of the state s major insurance payers to investigate the costs and benefits of the PCMH model in primary care. The pilot program paid PMPM (Per Member Per Month) fees to physician offices and Pay for Performance (P4P) dollars. In 2009 we received over $50, in PMPM payments, $85, for 2010, over $100,000 in 2011, and over $150,000 in The payments continued even after the pilot was complete. DARTNet - In 2010, we enrolled into the national AAFP electronic reporting research program known as DARTNet. We are currently reporting PHQ-9 data and CKD data to University Hospital in Denver, and receive some grant money for doing so.
55 External reporting for Fun and Profit. Medicaid We have grown from 1% Medicaid to 19% Medicaid as a payer source in the last 4 years; Initially receive 10% bonus on our Medicaid children for reporting to the immunization registry and performing ASQ screenings; Now we receive PMPM from regional RCCO (Regional Care Coordination Organizations) and are positioned for P4P and gainsharing next year.


56
57 External reporting for Fun and Profit PQRS - We worked with CINA (Clinical Integration Networks of America) to transform our PQRI/PQRS reporting from claims-based reporting through our clearing house to database reporting directly from our SQL server. BTE - Qualified for Bridges to Excellence monies (a recognition program available to us through the Colorado Business Group on Health) for Diabetes and Heart/Stroke metrics. Meaningful Use - We were the first or second practice in the state of Colorado to be paid Stage 1 Meaningful Use monies in May CPCI Two of 73 practices in Colorado awarded, our first payments received in November of 2012, anticipated to be worth over a million dollars over 4 years.



58

59 Coaching is Essential to Practice Transformation
60 Miramont University Lean Redesign Concepts Thanks to IPIP Consultant: Richard A. Wright MD. Mph Wright Consulting Professor of Preventive Medicine and Biometrics *Used with permission
61 Why Lean Redesign? Lean Philosophy: Eliminate Waste Waste is disrespectful of humanity because it squanders precious resources. Waste is disrespectful of the employee because it asks them to do work with no value. President of Toyota Waste is disrespectful to patients because it asks them to endure processes or procedures with no value.
62 The value of simple things Waste is everywhere in healthcare if we can harness it, there will be enough left over to care for every man, woman, and child who does not now have access to basic healthcare and we will retain a workforce who finds joy in their work!!
63 So What s Lean Redesign? A system thinking approach to redesigning linked processes called value streams, with the aim of improving efficiency, effectiveness, and overall value of services to the customer
64 Common Problems in Office Practices Long waits to get appointments Long waits to see the provider Long waits on the phone Long waits for lab results Demand exceeds provider capacity Poor clinical outcomes Lean Can Fix These Problems!! 64
65 Lean Achievements 90% reduction in wait times 90% reduction in inventory 100% increase in productivity 50% decrease in defects or errors
66 Lean System Facts Equally True for Health Care In most systems only 5% of processes add value to the customer 35% of processes are necessary but do not add value to the customer 60% of processes are both unnecessary and do not add value Therefore, elimination of waste is a major cost reduction and performance improvement strategy
67 Lean Core Ideas Determine and create value for the customer Achieve one piece flow in the value stream Eliminate the 7 speed bumps (waste) Use a root cause analysis or a proactive method to stop or prevent problems Use data to sustain improvements
68 What Leaders Must Do Create a culture for change Non-blaming environment Transparent communication Team-base engagement Staff empowerment Focus on fixing processes not people
69 Miramont Lean Redesign 4 Tools 1. Root Cause Analysis Tool 2. Value Stream Mapping Tool 3. Cycle time analysis tool 4. 5S Tool
70 Tool # 1 Root Cause Analysis Stop producing errors by stopping production when an error is detected (produce an immediate signal to the location of the error so problem-solving can start immediately. ROOT CAUSE ANALYSIS Manager goes and sees, analyzes, ask why five times By the fifth time, usually find the root cause
71 The Causes of Safety Failures Active failures Hazards Harm System factors
72 The 7 Speed Bumps of Lean Over production Excessive inventory Waiting and delays Unnecessary staff movement Unnecessary service movement Defects or errors Processing

73 Process as a Root Cause 7 Causes of Waste or MUDA
74 Lean Redesign Aphorisms and Mantras 1. Do It Right, Quickly, Safely, and Completely 2. Every System is Perfectly Designed to get the Results it Gets 3. Inefficiencies are usually due to System and Processes rather than People 4. Get Today s Work Done Today Without Yesterday s Work Being in the Way or Stopping the Flow 5. Completely Solve the Customers Problems 6. Do Not Make the Customer Wait
75 Lean Redesign Aphorisms and Mantras 1. Continuous flow increases productivity, profitability, and quality. 2. Customers don't like to wait in line: they are impatient. 3. Errors are opportunities for learning; Errors are golden nuggets to be found not garbage to be buried 4. Continuously solving root problems drives organizational learning and improvement 5. Problems are 20% cause and 80% effect
76 Lean Redesign Method Tool #2: Value Stream Mapping Tool Consultant: Richard A. Wright MD. Mph Wright Consulting Professor of Preventive Medicine and Biometrics
77 What is a Value Stream? Whenever there is a product (or service) for a customer, there is a value stream. The challenge lies in seeing it. - James Womack
78 A Value Stream is the set of all actions (both value added and non value added) required to bring a specific product or service from raw material through to the customer.
79 Potential Value Streams Administrative Processes Office Redesign usually starts here Office Visit Flow Patient Registration Space Organization Telecommunication Information Management Supplies and Inventory Charge, Billing, and Collection Medical Records
80 Potential Value Streams Clinical Processes Patient Scheduling Chronic Care Preventive Care After Hours Medications Diagnostic Tests Provider Paperwork Specialty and Primary Care Referrals
81 How to Use Mapping to Evaluate Value Streams (tool #1) 10 Sequential Steps 1. Train team on use of flow mapping methods and tools 2. Identify the value stream and where it begins and ends 3. Walk the process to identify linked processes 4. Produce the initial value stream map 5. Measure cycle/interval times in the value stream 6. Calculate cycle and TAKT times and other data 7. Walk the process again to identify flow and process-related inefficiencies 8. Produce specific process flow maps to better understand flow and risk points 9. Document process-specific actual or potential risk points 10. Use maps to focus group problem-solving or kaizen event on root causes for risk points
82 There are four symbols and shapes that you will need to be familiar with to diagram your patient process Box Activities, tasks, steps in the process Diamond Decisions Circle Start and end steps Arrow To connect each of the activities, decisions or start and end points
83 Value Stream Map Cycle and Interval Times Patient Visit Stream Patient Enters clinic Patient registered Patient Check-in Patient Sees Provider Patient Check-out Patient Scheduling Diagnostics Goes home Waiting Room Time Waiting Room Time Exam Room Wait Time Exam Room Wait Time Waiting Room Time Waiting Room Time Registration Time Intake Time Provider Time Check out Time Diagnostic Time Cycle Times

84

85 TAKT Time (tool #3) Cycle Time Analysis Tool The Pacemaker of One Piece Flow Takt time, derived from the German word Taktzeit which translates to cycle time
86 TAKT Time Calculation Delivery or production time divided by service demand Hours of operation of clinic: 8 hours x 60 min. = 480 min. Total visits per 8 hour period = 100 TAKT time = 4.8 min.
87 Grace Hill TAKT and Interval Times Minutes CYCLE Time TAKE Time Registration Check in Provider Check out Clinic Processes Scheduling Provider time is the only potential constraint in the flow
88 Imbalance in TAKT and Interval Times When Interval Times Exceed TAKT When process interval time exceeds value stream TAKT there is backlog To minimize backlog, the tendency is to pass unfinished work to next process or to speed up and produce errors Solution is to redesign process to decrease interval time or to increase staffing level to meet demand
89 Imbalance in TAKT and Interval Times When Interval Times are Less Than TAKT When process interval time is faster than TAKT Reassign staff to other areas Multitask staff
90 Registration Process Staffing Needs Sample TAKT Analysis 2 FTE actual registration clerks 510 min/day (excluding break time) 52 visits per day TAKT time = 510/52 = 9.8 min per patient Actual Interval time = 2 min per clerk IT/TT = 2/9.8 = 0.2 or 1 required FTEs Conclusion: supply exceeds demand, so there maybe excess staff capacity
91 Sort Straighten Shine Standardize Sustain The 5S of Lean (Tool #4) Method for Standardizing Processes



92 The 5S of Lean (Tool #4) Method for Standardizing Processes

93 Lean Production Cells Method for Creating One Piece Flow Kitchen Example: Sink Trash Refrigerator Micro wave Only One Cook!! Pots & Pans Stove Utensils
94 Process Redesign Pit Falls Don t buy the first answer you get Old habits are hard to break (Culture eats Strategy for breakfast) Don t start a team when you have no data Don t redefine the problem before a team does a root cause analysis Avoid Endless Data Gathering Don t Value stream map before you define the problem area
95 BLAME FREE
96 Future Plans - Keeping Current and Connecting to Others

97

98

99 Phreesia Tablets

100 Teleconferencing in remotely





101 Leveraging New IT
102 Leveraging New IT

103 Build the Medical Neighborhood
104 A Call for Courage Sometimes the opposite of Cautious is not Careless Sometimes the opposite of Cautious is Courage - John L Bender, M.D., FAAFP

105 Xtreme Makeover PCMH edition The Miramont Story Presented by John L Bender, M.D., FAAFP May 4 th, 2013 Sonnenalp, CMS 2013 Spring Conference
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012
 A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012 Introduction The Computer-Based Record Institute (CPRI) established the
A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012 Introduction The Computer-Based Record Institute (CPRI) established the
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Oregon Medical Group Team Medicine 3 April 2014
 Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Quality Improvement. Goals & Objectives. u What is Quality Health Care. u Where are the gaps in care JOHN W. RAGSDALE, III, MD JULY 2017
 Quality Improvement JOHN W. RAGSDALE, III, MD JULY 2017 DEPARTMENT OF COMMUNITY AND FAMILY MEDICINE PRIMARY CARE SEMINAR SEA PINES, SC Goals & Objectives u What is Quality Health Care u Where are the gaps
Quality Improvement JOHN W. RAGSDALE, III, MD JULY 2017 DEPARTMENT OF COMMUNITY AND FAMILY MEDICINE PRIMARY CARE SEMINAR SEA PINES, SC Goals & Objectives u What is Quality Health Care u Where are the gaps
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Patient Centered Medical Home The Road To MDH Health Care Home Certification
 Patient Centered Medical Home The Road To MDH Health Care Home Certification Determinants of Health and Their Contribution to Premature Death. Schroeder SA. N Engl J Med 2007;357:1221-1228. Practical
Patient Centered Medical Home The Road To MDH Health Care Home Certification Determinants of Health and Their Contribution to Premature Death. Schroeder SA. N Engl J Med 2007;357:1221-1228. Practical
UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION
 UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION II UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION EXECUTIVE SUMMARY Healthcare may be the only industry
UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION II UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION EXECUTIVE SUMMARY Healthcare may be the only industry
Work Design and Value Stream Mapping
 Work Design and Value Stream Mapping Jane Brock, MD, MSPH Colorado Foundation for Medical Care May 4, 2013 This material was prepared by the Colorado Foundation for Medical Care (CFMC), the Integrating
Work Design and Value Stream Mapping Jane Brock, MD, MSPH Colorado Foundation for Medical Care May 4, 2013 This material was prepared by the Colorado Foundation for Medical Care (CFMC), the Integrating
Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA
 These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
Welcome to University Family Healthcare, PA.
 Welcome to University Family Healthcare, PA. We re delighted that you have chosen us as your primary care providers. We work hard to earn your trust and to see that you have the best healthcare possible.
Welcome to University Family Healthcare, PA. We re delighted that you have chosen us as your primary care providers. We work hard to earn your trust and to see that you have the best healthcare possible.
Practical Applications on Efficiency
 Practical Applications on Efficiency Maryland MGMA September 19, 214 Owen J. Dahl, FACHE, LSSMBB Objectives To offer practical scenarios for the application of Lean Tools in YOUR practice To discuss and
Practical Applications on Efficiency Maryland MGMA September 19, 214 Owen J. Dahl, FACHE, LSSMBB Objectives To offer practical scenarios for the application of Lean Tools in YOUR practice To discuss and
How to Build a Medical Home
 How to Build a Medical Home NOTE: Make sure your computer speakers are turned ON. Audio will be streaming through your speakers. If you do not have computer speakers, call the ACCMA at 510-654-5383 for
How to Build a Medical Home NOTE: Make sure your computer speakers are turned ON. Audio will be streaming through your speakers. If you do not have computer speakers, call the ACCMA at 510-654-5383 for
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Laguna Honda Lean Transformation. Laguna Honda Strategic Performance Management November 2017
 Laguna Honda Lean Transformation Laguna Honda Strategic Performance Management November 2017 Background MAKE IT BETTER 4. 1. Performance Improvement FIX IT Do the work and make it happen 3. Create best
Laguna Honda Lean Transformation Laguna Honda Strategic Performance Management November 2017 Background MAKE IT BETTER 4. 1. Performance Improvement FIX IT Do the work and make it happen 3. Create best
August 8, :00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell
 August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
 Care Model May 12, 2016") update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Executive Summary: Davies Ambulatory Award Community Health Organization (CHO)
") Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Making Differences Matter Redesign Ambulatory Medication Reconciliation
 Making Differences Matter Redesign Ambulatory Medication Reconciliation AMGA Annual Meeting April 5 2014 Presenters Thomas N. Atkins, MD MMM,FAAFP, FACPE, CPE Steven A. Mitnick MD MBA Katherine T. Manuel,
Making Differences Matter Redesign Ambulatory Medication Reconciliation AMGA Annual Meeting April 5 2014 Presenters Thomas N. Atkins, MD MMM,FAAFP, FACPE, CPE Steven A. Mitnick MD MBA Katherine T. Manuel,
University of California, Davis Family Practice Center: Update 2014
 University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust Tel
 Lean Thinking Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust neil.westwood@institute.nhs.uk Tel 07747794976 NHS Institute for Innovation and Improvement Plan for today
Lean Thinking Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust neil.westwood@institute.nhs.uk Tel 07747794976 NHS Institute for Innovation and Improvement Plan for today
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
producing an ROI with a PCMH
 REPRINT April 2016 Emma Mandell Gray Rachel Aronovich healthcare financial management association hfma.org producing an ROI with a PCMH Patient-centered medical homes can deliver high-quality care and
REPRINT April 2016 Emma Mandell Gray Rachel Aronovich healthcare financial management association hfma.org producing an ROI with a PCMH Patient-centered medical homes can deliver high-quality care and
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18
 Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18") Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
System redesign in Primary Care
 System redesign in Primary Care A focus on Lean Anthony Behm, D.O. Chief of Staff, Erie VAMC Primary care(pc) satisfaction: up and down Satisfaction rates for PC s started dropping in the late 90 s. Physicians
System redesign in Primary Care A focus on Lean Anthony Behm, D.O. Chief of Staff, Erie VAMC Primary care(pc) satisfaction: up and down Satisfaction rates for PC s started dropping in the late 90 s. Physicians
Core Item: Hospital. Cover Page. Admissions and Readmissions. Executive Summary
 Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
YOUR HEALTH INFORMATION EXCHANGE
 YOUR HEALTH INFORMATION EXCHANGE Introduction to Health Information Exchange Healthcare organizations are experiencing substantial pressures from initiatives and reforms such as new payment models, care
YOUR HEALTH INFORMATION EXCHANGE Introduction to Health Information Exchange Healthcare organizations are experiencing substantial pressures from initiatives and reforms such as new payment models, care
Completing the Specialty Practice Assessment Tool: Guide for Behavioral Health Organizations and Divisions
 Completing the Specialty Practice Assessment Tool: Guide for Behavioral Health Organizations and Divisions Instructions: Please find below guiding questions for behavioral health organizations or divisions
Completing the Specialty Practice Assessment Tool: Guide for Behavioral Health Organizations and Divisions Instructions: Please find below guiding questions for behavioral health organizations or divisions
Lean Six Sigma DMAIC Project (Example)
") Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Kaiser Permanente QUALITY OVERVIEW OVERALL RATING : 3.4 COMPANY AT A GLANCE. Company Statistics. Accreditation Exchange Product
 QUALITY OVERVIEW Permanente As the state s largest nonprofit health plan, Permanente is committed to improving the health of our members and our state as a whole. Permanente is made up of: Foundation Hospitals
QUALITY OVERVIEW Permanente As the state s largest nonprofit health plan, Permanente is committed to improving the health of our members and our state as a whole. Permanente is made up of: Foundation Hospitals
Eligible Hours ( ) Achieving HIMSS Stage 7 and Gaining Physician Adoption of a Paperless Record CHC
 Achieving HIMSS Stage 7 and Gaining Physician Adoption of a Paperless Record CHC") Below are the sessions that qualify for CPHIMS or CAHIMS continuing education (CE) hours. Check the column for all sessions attended and total the number of hours earned each day. At the end of the form,
Below are the sessions that qualify for CPHIMS or CAHIMS continuing education (CE) hours. Check the column for all sessions attended and total the number of hours earned each day. At the end of the form,
1 Title Improving Wellness and Care Management with an Electronic Health Record System
 HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
The Power of Quality. Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center
 The Power of Quality Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center What do you think of when you hear the word quality? LEAN RCA PDSA QAPI SIX SIGMA PIP TQM 5s Objectives Transplant
The Power of Quality Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center What do you think of when you hear the word quality? LEAN RCA PDSA QAPI SIX SIGMA PIP TQM 5s Objectives Transplant
Profit = Price - Cost. TAKT Time Map Capacity Tables. Morale. Total Productive Maintenance. Visual Control. Poka-yoke (mistake proofing) Kanban.
 Kanban.") GPS Mod 22 7 Flows of Medicine MUDA MUDA Cost Reduction By Eliminating Waste Just-in-Time Profit = Price - Cost GPS Depth Study NVA/VA- Functions/Mgrs R e d e p l o y m e n t Jidoka (human automation)
GPS Mod 22 7 Flows of Medicine MUDA MUDA Cost Reduction By Eliminating Waste Just-in-Time Profit = Price - Cost GPS Depth Study NVA/VA- Functions/Mgrs R e d e p l o y m e n t Jidoka (human automation)
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination
 Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
Behavioral Health. Community Outreach Program
 Behavioral Health How do I get into Residential Treatment? You must complete a Behavioral Health intake if not already established with Behavioral Health. Our Licensed Counselors will then evaluate for
Behavioral Health How do I get into Residential Treatment? You must complete a Behavioral Health intake if not already established with Behavioral Health. Our Licensed Counselors will then evaluate for
A. DIABETES AND HEART/STROKE Data Detail
 A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
Gonzalo Paz-Soldán, MD, FAAP, CPE Executive Medical Director - Pediatrics Reliant Medical Group
 Gonzalo Paz-Soldán, MD, FAAP, CPE Executive Medical Director - Pediatrics Reliant Medical Group Describe the main characteristics of a PCMH Analyze potential benefits of becoming a PCMH Examine the criteria
Gonzalo Paz-Soldán, MD, FAAP, CPE Executive Medical Director - Pediatrics Reliant Medical Group Describe the main characteristics of a PCMH Analyze potential benefits of becoming a PCMH Examine the criteria
REPORTING METRICS FOR INTEGRATION OF PHYSICAL-BEHAVIORAL HEALTH CARE
 9/26/213 REPORTING METRICS FOR INTEGRATION OF PHYSICAL-BEHAVIORAL HEALTH CARE MARISA DERMAN, MD, MSC (OMH) M. ASHLEY HEALD, MA (UW) OBJECTIVES FOR THIS WEBINAR Review goals/ standards Review mandatory
9/26/213 REPORTING METRICS FOR INTEGRATION OF PHYSICAL-BEHAVIORAL HEALTH CARE MARISA DERMAN, MD, MSC (OMH) M. ASHLEY HEALD, MA (UW) OBJECTIVES FOR THIS WEBINAR Review goals/ standards Review mandatory
OPEN ACCESS AND REDESIGN. Kate Kubler (MSII) and Chris Soares (DSII)
 and Chris Soares (DSII)") OPEN ACCESS AND REDESIGN Kate Kubler (MSII) and Chris Soares (DSII) An opportunity for Improvement: No show rates for providers on average are 25% CHCs are offsetting high no show rates by double booking
OPEN ACCESS AND REDESIGN Kate Kubler (MSII) and Chris Soares (DSII) An opportunity for Improvement: No show rates for providers on average are 25% CHCs are offsetting high no show rates by double booking
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Patient Care: Case Study in EHR Implementation. With Help From Monkeys, Mice, and Penguins. Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007
 Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
WHITE PAPER. Transforming the Healthcare Organization through Process Improvement
 WHITE PAPER Transforming the Healthcare Organization through Process Improvement The movement towards value-based purchasing models has made the concept of process improvement and its methodologies an
WHITE PAPER Transforming the Healthcare Organization through Process Improvement The movement towards value-based purchasing models has made the concept of process improvement and its methodologies an
Overview of the EHR Incentive Program Stage 2 Final Rule published August, 2012
 I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
The content and/or presentation of the information will promote quality or improvements in healthcare and will not promote commercial interests
 Disclosure Statement: The content and/or presentation of the information will promote quality or improvements in healthcare and will not promote commercial interests UTILIZING POPULATION HEALTH DATA John
Disclosure Statement: The content and/or presentation of the information will promote quality or improvements in healthcare and will not promote commercial interests UTILIZING POPULATION HEALTH DATA John
10/10/2017. Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP
 Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP") Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Appendix 6. PCMH 2014 Summary of Changes
 Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
EHR for the PCMH A Doctor s Perspective. Medical Home Summit
 EHR for the PCMH A Doctor s Perspective Medical Home Summit Salvatore Volpe MD FAAP FACP CHCQM www.svolpemd.com March 15, 2011 Learning Objectives Why I adopted an EHR My experience: what I needed to do
EHR for the PCMH A Doctor s Perspective Medical Home Summit Salvatore Volpe MD FAAP FACP CHCQM www.svolpemd.com March 15, 2011 Learning Objectives Why I adopted an EHR My experience: what I needed to do
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Driving Business Value for Healthcare Through Unified Communications
 Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
The Quality Journey of
 The Quality Journey of New Territories West Cluster, Hong Kong Dr. T W Lee Hospital chief Executive Pok Oi Hospital New Territories West Cluster Hong Kong The Sick Hospital Medical treatment improves with
The Quality Journey of New Territories West Cluster, Hong Kong Dr. T W Lee Hospital chief Executive Pok Oi Hospital New Territories West Cluster Hong Kong The Sick Hospital Medical treatment improves with
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Kaiser Permanente: Integration, Innovation, and Transformation in Health Care
 Kaiser Permanente: Integration, Innovation, and Transformation in Health Care March 2018 Karin Cooke, MBA, Director, Kaiser Permanente International Karin.C.Cooke@kp.org kp.org/international Copyright
Kaiser Permanente: Integration, Innovation, and Transformation in Health Care March 2018 Karin Cooke, MBA, Director, Kaiser Permanente International Karin.C.Cooke@kp.org kp.org/international Copyright
Roll Out of the HIT Meaningful Use Standards and Certification Criteria
 Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
Use of Information Technology in Physician Practices
 Use of Information Technology in Physician Practices 1. Do you have access to a computer at your current office practice? YES NO -- PLEASE SKIP TO QUESTION #2 If YES, please answer the following. a. Do
Use of Information Technology in Physician Practices 1. Do you have access to a computer at your current office practice? YES NO -- PLEASE SKIP TO QUESTION #2 If YES, please answer the following. a. Do
AAWC ALERT Call for Action from Physicians
 AAWC ALERT Call for Action from Physicians The 2019 CMS Proposed Rule for the Physician Fee Schedule has multiple changes to payment & documentation requirements. See Attachment A for summary of major
AAWC ALERT Call for Action from Physicians The 2019 CMS Proposed Rule for the Physician Fee Schedule has multiple changes to payment & documentation requirements. See Attachment A for summary of major
2014 Patient Centered Medical Home (PCMH) Recognition
 Recognition") Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
The Patient Centered Medical Home: 2011 Status and Needs Study
 The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
Paying for Primary Care: Is There A Better Way?
 Paying for Primary Care: Is There A Better Way? Robert A. Berenson, M.D. Senior Fellow, The Urban Institute CHCS Regional Quality Improvement Initiative, Providence, R.I., July 25, 2007 1 Medicare Challenges
Paying for Primary Care: Is There A Better Way? Robert A. Berenson, M.D. Senior Fellow, The Urban Institute CHCS Regional Quality Improvement Initiative, Providence, R.I., July 25, 2007 1 Medicare Challenges
Guidance for Medication Reconciliation and System Integration Process
 Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
VHA Transformation to a Patient Centered Medical Home Model of Care
 VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health
 REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
PCMH and the Care of Complex High Cost Patients
 PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
2017 National Standards for Diabetes Self-Management Education and Support INTERPRETIVE GUIDANCE
 2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
Fundamentals of Health Workflow Process Analysis and Redesign: Process Analysis
 Fundamentals of Health Workflow Process Analysis and Redesign: Process Analysis Lecture 2 Audio Transcript Slide 1 Welcome to Fundamentals of Health Workflow Process Analysis and Redesign: Process Analysis.
Fundamentals of Health Workflow Process Analysis and Redesign: Process Analysis Lecture 2 Audio Transcript Slide 1 Welcome to Fundamentals of Health Workflow Process Analysis and Redesign: Process Analysis.
Medical Home Renovations: A Patient-centered Medical Home Case Study
 Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Patrick J. O Sullivan MS, MT(ASCP)SBB Florida Hospital Orlando Laboratory Operations Director
SBB Florida Hospital Orlando Laboratory Operations Director") Patrick J. O Sullivan MS, MT(ASCP)SBB Florida Hospital Orlando Laboratory Operations Director List factors that affect the need to change work processes in Microbiology Analyze process review and determine
Patrick J. O Sullivan MS, MT(ASCP)SBB Florida Hospital Orlando Laboratory Operations Director List factors that affect the need to change work processes in Microbiology Analyze process review and determine
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Lean Six Sigma in Healthcare. 4 Simple BFO s s that Change Everything
 Lean Six Sigma in Healthcare 4 Simple BFO s s that Change Everything Presented By: Joseph Duhig Senior Vice President Juran Institute, Inc. February 23, 2008 BFO s = Blinding Flashes of the Obvious 8005
Lean Six Sigma in Healthcare 4 Simple BFO s s that Change Everything Presented By: Joseph Duhig Senior Vice President Juran Institute, Inc. February 23, 2008 BFO s = Blinding Flashes of the Obvious 8005
Medical Home Summit September 20, 2011
 Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
New Patient Welcome. elrio.org
 New Patient Welcome elrio.org Welcome to EL RIO Your HEALTHCARE HOME A healthcare home is a place where healthcare professionals know your needs, history, and how to help you stay healthy. A healthcare
New Patient Welcome elrio.org Welcome to EL RIO Your HEALTHCARE HOME A healthcare home is a place where healthcare professionals know your needs, history, and how to help you stay healthy. A healthcare
ACO Practice Transformation Program
 ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
3 Ways to Increase Patient Visits
 3 Ways to Increase Patient Visits 3 Ways to Increase Patient Visits www.kareo.com kareo.com Table of Contents Introduction 03 Create an Effective Recall/Recare Program 04 Build and Manage Your Online Presence
3 Ways to Increase Patient Visits 3 Ways to Increase Patient Visits www.kareo.com kareo.com Table of Contents Introduction 03 Create an Effective Recall/Recare Program 04 Build and Manage Your Online Presence
Stage 1 Changes Tipsheet Last Updated: August, 2012
 Stage 1 Changes Tipsheet Last Updated: August, 2012 Overview CMS recently announced some changes to the Stage 1 meaningful use objectives, measures, and exclusions for eligible professionals (EPs), eligible
Stage 1 Changes Tipsheet Last Updated: August, 2012 Overview CMS recently announced some changes to the Stage 1 meaningful use objectives, measures, and exclusions for eligible professionals (EPs), eligible
Health Center Strong:
 Health Center Strong: Developing and Expressing Health Center Value Jonathan Chapman Director, CHC Advisory Services, Capital Link NHCHC National Conference and Policy Symposium May 18, 2018 1 Capital
Health Center Strong: Developing and Expressing Health Center Value Jonathan Chapman Director, CHC Advisory Services, Capital Link NHCHC National Conference and Policy Symposium May 18, 2018 1 Capital
Improving the Delivery of Troponin Results to the Emergency Department using Lean Methodology
 Organization: Anne Arundel Medical Center Solution Title: Improving the Delivery of Troponin Results to the Emergency Department using Lean Methodology Program/Project Description, Including Goals: What
Organization: Anne Arundel Medical Center Solution Title: Improving the Delivery of Troponin Results to the Emergency Department using Lean Methodology Program/Project Description, Including Goals: What
Next Gen Training. Why is Next Gen So Important? Step-by-Step Vitals Entry Scenarios and Mock Work-ups
 Next Gen Training Why is Next Gen So Important? Step-by-Step Vitals Entry Scenarios and Mock Work-ups Why is Next Gen So Important? Better for the VFC: All the necessary info can be accessed from any VFC
Next Gen Training Why is Next Gen So Important? Step-by-Step Vitals Entry Scenarios and Mock Work-ups Why is Next Gen So Important? Better for the VFC: All the necessary info can be accessed from any VFC
Staying Connected with Patient-Generated Health Data
 Staying Connected with Patient-Generated Health Data April 14, 2015 Dr. Danny Sands, Chief Medical Officer Dr. Philip Marshall, Chief Product Officer DISCLAIMER: The views and opinions expressed in this
Staying Connected with Patient-Generated Health Data April 14, 2015 Dr. Danny Sands, Chief Medical Officer Dr. Philip Marshall, Chief Product Officer DISCLAIMER: The views and opinions expressed in this
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016
 ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
J U N E TRICARE
 TRICARE Provider News JUNE 2011 TRICARE Referral and Prior Authorization Changes As a reminder, referral and prior authorization requirements for TRICARE patients changed with the start of Health Net s
TRICARE Provider News JUNE 2011 TRICARE Referral and Prior Authorization Changes As a reminder, referral and prior authorization requirements for TRICARE patients changed with the start of Health Net s
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita