An Introduction to Quality Improvement Day 2
|
|
|
- Raymond Marshall
- 5 years ago
- Views:
Transcription
1
2 An Introduction to Quality Improvement Day 2
3 QUALITY IMPROVEMENT SCIENCE

4 Deming s Lens of Improvement Appreciation of a system Theory of Knowledge Psychology Understanding Variation

5 One need not be eminent in any part of profound knowledge in order to understand it and to apply it. The various segments of the system of profound knowledge cannot be separated. They interact with each other.





6
7 Development of Profound Knowledge Variation Shewhart Control Chart 1924 Design of Experiments Sir Ronald Fisher, 1925 Shewhart s 1931 and 1939 Books on Quality Control* Sampling methods Developed, H. F. Dodge Use of statistical methods to support the war effort Enumerative vs Analytic Studies in Statistics, Deming Systems Psychology Hawthorne Experiments Plant 1927 General Systems Theory Lugwig von Bertalanffy, 1949 Tavistock Institute 1951 Socio-technical System Principles of Systems Jay Forrester, 1968 Maslow Hierarchy of Needs1962 Theory of Constraints The Goal E. Goldratt, th Discipline Peter Senge 1990 Switch Dan Heath 2011 Knowledge Mind & The World Order, C.I. Lewis 1929* Lectures at The USDA, 1938, organized By Deming* How We Think Dewey, 1933 Human Side of Enterprise D. McGregor, 1960 Motivation Theory Herzberg, 1968 Double Loop Learning in Organizations Chris Argyris, 1977 Drive Daniel Pink 2009
8
9 Two Types of Knowledge Subject Matter Knowledge: Knowledge basic to the things we do in life. Professional knowledge. Subject Matter Knowledge Improvement Science Profound Knowledge: The interaction of the theories of systems, variation, knowledge, and psychology.
10 Knowledge for Improvement Subject Matter Knowledge Improvement: Learn to combine subject matter knowledge and profound knowledge in creative ways to develop effective changes for improvement. Improvement Science
11 System of Profound Knowledge Subject matter Knowledge Appreciation of a system Theory of Knowledge Psychology Understanding Variation Knowledge for Improvement
12 PSYCHOLOGY OF IMPROVEMENT
13 MOTIVATION
14 CAN T The COM-B model, Michie et al (2011)
15 WON T The COM-B model, Michie et al (2011)
")
16 One More Time: How Do You Motivate Employees? Harvard Business Review (reprint Jan, 2003)


17 Allow autonomy Enable Mastery How to motivate Create sense of purpose
18 CHANGE

19 The COM-B model, Michie et al (2011)

20 Opportunity

21 The Everett Rogers curve
22
 Chip and Dan Heath,")
23 Direct the Rider (rational) Motivate the Elephant (emotional) Chip and Dan Heath, Switch

24 Improvement in health care is 20% technical and 80% human Marjorie Godfrey, MS, RN, PhD The Dartmouth Institute for Health Policy and Clinical Practice
25 CHANGE IDEAS - INNOVATION
26 Take a Specific Aim We know what we want to improve Change ideas are the possible how s. BE CREATIVE!
 See patients even if late Patients don t have own transport Scheduling Mismatch of arrivals and resources Hospital transport is late Reliant on others for lifts Don t know how long")
27 Fishbone (Cause and Effect Diagram) Communication Fax machine doesn t work properly Dictation delays clinic, always get out of sync Late & early arrivals Culture it s accepted See early patients early (sometimes) See patients even if late Patients don t have own transport Scheduling Mismatch of arrivals and resources Hospital transport is late Reliant on others for lifts Don t know how long things take cycle times Non standardised variation in content Waiting for other professionals to finish CF Clinic Why are Patients waiting in the CF clinic? Trials PEG changes, not planned into timings Notes Scales Going to find nebuliser from the ward X ray Going to the Pharmacy if patient too unwell Pharmacy Taking patient off for a ward tour Answering the doorbell Telephone Calls Calls from the ward Service Improvement Treatments Finding Things 17 Interruptions
28 5 Whys Getting to the root cause WHY did this patient stay in hospital 111 days WHY?...because they developed hospital acquired pneumonia WHY?...because they were immobile WHY?...because they fell on the ward WHY?...because they suffered from dementia and would have been better cared for in the familiar environment of their own home
29 Review Your Process Map Input Output

30 Change Ideas Langley s Change Concepts Some Examples Eliminate waste are all processes essential? Eliminate multiple entry can this be combined? Move steps closer together Find and remove bottlenecks Do tasks in parallel Use pull systems Give people access to information Use proper measurement Smooth workflow, reduce variation Minimise handoffs passing work between depts or individuals Reduce waiting times Standardise use exactly same system Listen to customers

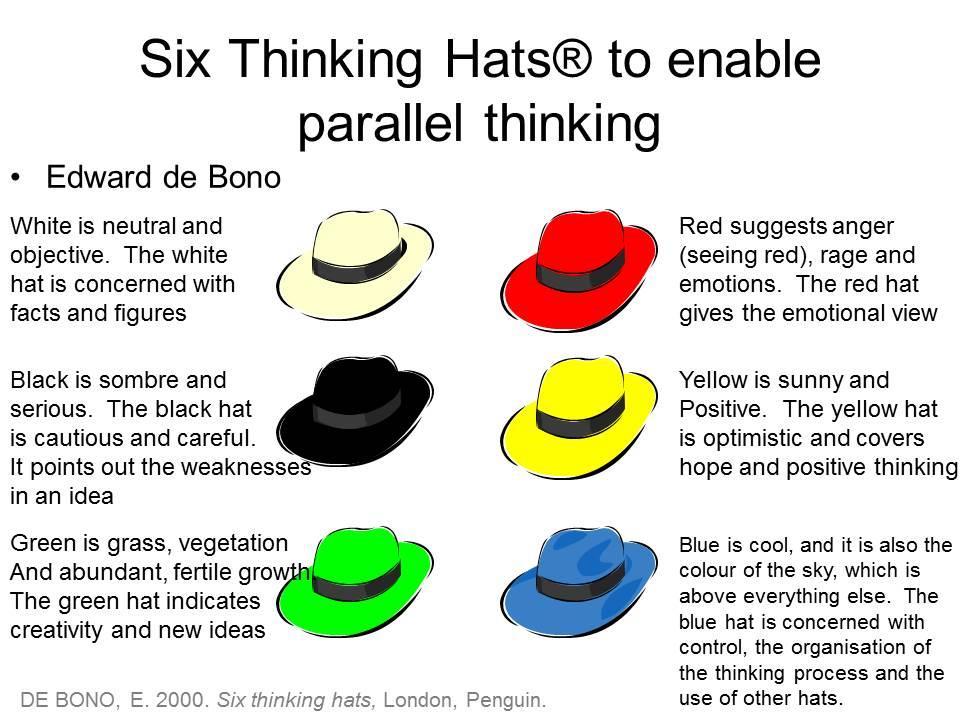
31 Meetings: Traditional Adversarial Thinking Take sides. Argue. Prove the other side wrong.
32
33 Brainstorming - Creative thinking! No idea is too big, too small or out of the question Do not judge or criticise others ideas Listen to others ideas and build on them 1. Silent period think about improvements to the process and write on a post it 2. Interactive period shout out other ideas that come to mind!
34 Multivoting Review all the ideas & merge similar ideas Vote for 1/3 ideas, use selection criteria, e.g. Ideas that can be started fast The change is reasonably low cost The effort is small compared to the impact The idea can be tested without getting permission from others Count the votes Test the top change ideas using PDSA


35
36 Time Series Data: All improvement is change, not all change is improvement.
37 Looking at Data Here are two numbers what s going on? Value 5 0 A B
38 Hold on A B Series
39 But A B Series
40 But then again A B Series
41 Erm 30 A 25 B Series

42 Here are two pie charts we wanted to decrease DNAs (no shows)
43 No Shows Hold on A B Series Weeks
44 No Shows But A B Series Weeks
45 No Shows But then again A B Series Weeks
46 What s going on with this data? Test 1 Test 2 Test 3 Test
47 What s going on with this data? Test 1 Test Series2 Series Test 3 Test Series2 15 Series Service Improvement
48 Beware of averages too Here are our two numbers (Monthly data) Value 5 0 A B
49 Here s what s happening by week 40? Weekly Data Series A B
50 Or Even Series
51 Summary One number will always be different to another plot data over time Tables take time to understand Chart your data to see what s happening Beware of averages they can be misleading
52 VARIATION
53 Profound Knowledge Understanding Variation Appreciation of a System Theory of Knowledge Psychology Understanding Variation

54 Reacting to Variation


55 William Sealy Gosset ( ) Sir Ronald Fisher ( )

56 Austin Bradford Hill
57 Sampling Water Content
58
59 Sampling Water Content TIME

60 Walter Shewhart ( ) W. Edwards Deming ( )




61 Sampling Water Content TIME
62
63 If I had to reduce my message for management to just a few words, I d say it all had to do with reducing variation. W. Edwards Deming
64 What Time is it? Write down the current time in minutes past the hour
65 Unintended variation patients vary
66 What do people call me? Dr. Downes Tom Dad Intended Variation
67 Intended and Unintended Variation
68 Shewhart s Theory of Variation Common Causes: those causes inherent in the system over time and affect all outcomes of the system Chance cause Stable over time
69 Common Cause Variation
70 Shewhart s Theory of Variation Special Causes: those causes not part of the system all the time. Arise because of specific circumstances Assignable cause Unstable process



71 Special Cause - My trip to work Upper process limit Mean Lower process limit
72 Theatre Incidents January March 2012 SSC implemented
73 Responding to Special Cause Variation Identify the cause: If positive then can it be replicated or standardised. If negative then cause needs to be eliminated
74 Theatre Incidents January March 2012 SSC implemented
75 Responding to Common Cause Variation 1. Reduce variation: make the process even more predictable or reliable (and/or) 2. Not satisfied with result: redesign process to get a better result
76 Process with special cause variation Identify the cause: if positive then can it be replicated or standardized. If negative then cause needs to be eliminated Process with common cause variation Reduce variation: make the process even more reliable Not satisfied with result: redesign process to get a better result

77 Theatre Incidents January March 2012 SSC implemented
78
79 SPC CHARTS
80 SPC, Statistical Process Control or The Control Chart Elements 1. Run chart/graph showing data, running record, time order sequence 2. A line showing the mean 3. 2 lines showing the upper and lower process control limits You only need 25 data points to set up a control chart, but 50 are better if available
81 Common cause variation - a stable process F M A M J J A S O N D J F M A M J J A S O N D Upper process limit Mean Lower process limit
82 Standard Deviation or σ In statistics, standard deviation shows how much variation exists from the mean. A low standard deviation indicates that the data points tend to be very close to the mean; high standard deviation indicates that the data points are spread out over a large range of values.

83 Standard Deviation and a normal distribution
84 PRACTICAL INTERPRETATION OF THE STANDARD DEVIATION 99.6% will be within 3 s Mean - 3s 1 in 256 Mean Mean + 3s
85 3s AND THE CONTROL CHART 3s 3s UCL Mean LCL 6s
86 Special cause variation F M A M J J A S O N D J F M A M J J A S O N D
 MEAN")
87 SPECIAL CAUSES - RULE 1 UCL Point above Upper Control Limit (UCL) MEAN LCL
88 SPECIAL CAUSES - RULE 1 UCL MEAN LCL Or point below Lower Control Limit (LCL)

89 SPECIAL CAUSES - RULE 2 UCL MEAN LCL Eight points above centre line

90 SPECIAL CAUSES - RULE 2 UCL Or eight points below centre line MEAN LCL

91 SPECIAL CAUSES - RULE 3 UCL Six points in a downward direction MEAN LCL

92 SPECIAL CAUSES - RULE 3 UCL Or six points in an upward direction MEAN LCL
93 What use is this? Evaluate and improve underlying process Is the process stable? Use data to make predictions and help planning Recognise variation Prove/disprove assumptions and (mis)conceptions Help drive improvement identify statistically significant change

94 Example
95 Annotated SPC Charts One of the most powerful tools for improvement Describe a process captured over time (as opposed to being a single sample) Reveal any trends a process might be experiencing When combined with careful annotation they track the impact of change
96 Why We Want to Annotate Our Charts 'And this is the period when the cat was away. '

97 Annotated SPC Charts




98
99 CAPACITY AND DEMAND

100 If I had to reduce my message for management to just a few words, I d say it all had to do with reducing variation. W. Edwards Deming


101 Procedure Time (Minutes) Variation & Queues 100% 80% 50% Consecutive Patients 80% rule is the most efficient balancing waiting and waste

102
103
104 Calculating the 80% rule 80% Rule = Variation x Lowest Value (Variation = High Value Low Value) Variation = 23 7 = x 0.8 = = (approx. 20min)
105 Plan Cycle Time = 20m
106 More Variable More Reliable Cycle time at 80% - PDSA 1 Role Cycle Time at 80% Lung Function 15m Weight & Nurse 10m Dietician 20m Dr 20m Others 15m
107 Patient 10 PDSA - Plan Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6 Patient 7 Patient 8 Patient 9 L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O L L L W N D D D D Dr Dr Dr Dr L L L W N D D D D Dr Dr L L L W N D D D D L L L W N D D
108 PDSA - Plan Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6 Patient 7 Patient 8 Patient 9 Patient 10 Patient 11 Patient 12 Patient 13 Patient 14 Patient 15 Patient 16 Patient 17 Patient 18 L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O L L L W N D D D D Dr Dr Dr Dr O O O

109 PDSA Do & Study

110 Demand is increasing... More slots needed...
111 80% = 21mins 3hrs = 8 Patients
112 80% = 21mins 80% = 18mins 3hrs = 8 Patients 3hrs = 10 Patients
113 80% = 21mins 80% = 18mins 80% = 14mins 3hrs = 8 Patients 3hrs = 10 Patients 3hrs = 12 Patients
114 HOW DO YOU REDUCE COMMON CAUSE VARIATION?
115 Volume drives value.
116 Capacity required = (27-7) x 80% + 7 = 23
117 Capacity required = (27-7) x 80% + 7 = 23
118
119 Capacity required = 42 (previously = 46) (4 beds less than separate units ~ 320,000)

120 Lung Cancer Clinic =
121 Lung Cancer - pooled
122 More Queuing...
123 Which is best? C S S C S C C C S C S S
124 And Finally - Which is best? S C Long S C Long C Short C Long S C Short S S

125 Quiz Example Clickers at the ready
126 THE MARSHMALLOW CHALLENGE
127
128
129 SPREAD
130 Testing Multiple cycles investigating the change idea under many different conditions What can you learn from continued testing?
131 Implementation Once a team has achieved a high degree of belief What would it really take to achieve this step
132 Confidence PDSA Cycle: Deciding on Scale of Test Engagement, Readiness to Change Current Situation Resistant (No commitment) Indifferent (some commitment) Ready (strong commitment) Low Degree of Belief that change idea will lead to Improvement Cost of failure large Cost of failure small Very Small Scale Test Very Small Scale Test Very Small Scale Test Very Small Scale Test Very Small Scale Test Small Scale Test High Degree of Belief that change idea will lead to Improvement Cost of failure large Cost of failure small Very Small Scale Test Small Scale Test Large Scale Test Small Scale Test Large Scale Test Implement Source - The Improvement Guide
133 SUSTAIN
134 When you have achieved your specific aim Building reliability into the process Restrict variation from your process Sustain improvement long term Quality Improvement - The structure PDSA SDSA Standardise Some techniques.. Assessment - 5Ps Change Ideas Define Themes

135 SOP (Standard Operating Procedures) or Playbooks Define exactly how a process works Great for new staff Reduce variation


136 Use Visual Management to build-in knowledge


137 Strategy: Use Visual Controls Which dial turns on the burner?

138 Schipol Airport, Amsterdam


139



140 Amsterdam Science Museum Amsterdam Shopping Centre Amsterdam Art Deco Cinema

141 International Spread Lausanne Olympic Museum, Switzerland
142

143


144

145 Surprise!
146 Design in reliability Make it easiest to do the process the redesigned way Don t rely on one person being able to deliver part of your process they will take leave at some point! 5S (Sort, Straighten, Shine, Standardise, Sustain) remove all old materials not required for your new process
147 The Sheffield MCA


148 We aim to help teams improve the quality and efficiency of services for patients and staff Pathway Improvement Microsystem Coaching Intensive Improvement Support Support for Large Scale Change Project Management Programme Management






149 Coaches per Cohort C1 C2 C3 C4 C5 C6 C7 869 Improvement Collaboratives Ward Outpatients Weston Park

150 Based on Dartmouth s evidence based ecoach the Coach programme translated to NHS and UK context Sheffield Faculty 6 month taught portion Experiential learning you need to coach a microsystem, learn from and report on this



151 WARD Collaborative What are we testing?

152 What are we learning? This is really hard work but results can be achieved

153 What are we learning? Leadership is essential - time and space is needed for improvement work to happen.

154 What are we learning? It s hard to coach your own team

155 What are we learning? The structured approach helps you make measurable sustainable improvements 5 P Assessment 5P The Microsystem Improvement Ramp Dartmouth Microsystem Improvement Curriculum Cause & Effect Global Specific Aim Aim Global Aim Theme Theme PDSA Change Ideas Measures Specific Aim Change Ideas Effective Meeting Skills 1 2 PDSA 2 A P Measures 1 S D A S P D Flowchart A P S D A P S D Global Aim 2 2 A P SDSA S D 3 3 A S P D Global Aim SDS A

156 What are we learning? Assess the system before deciding on solutions

157 What are we learning? Improvement work is 80% human and 20% technical - use the team & the patients knowledge and skills

158 What are we learning? Giving the team ownership of ideas and decisions - what to improve and how to improve it.

159 What are we learning? Involving patients in the work from the start is essential

160 What are we learning? Start small and build confidence.

161 What are we learning? Use measurement to show that changes are measurable improvements 50% reduction in length of stay



162 Over 160 teams have worked on microsystem improvement across STH, SCH and the care trust Geriatric and Stroke Medicine Microsystem designed a new discharge checklist and introduced reminders which reduced the average length of time to complete E-discharge from 37 to 11 hours Urology outpatients saved 37 hours of nursing time per week by redesigning how clinics run Community Stroke Microsystem reduced waiting times to see a physiotherapist by 44% Medical Photographer Microsystem increased the number of reports completed within 21 days from 56% to 97% Dermatology Microsystem & Skin Cancer Pre-operative assessment removed the FLOW Pathway reduced average time to need for 300 patient return visits and 300 surgery from 27 days to 10 days hours of nurse time each month using an electronic assessment tool Sheffield Health and Social Care Paediatric Psychology Service Microsystem Wainwright Crescent Respite care unit reduced the number of letter templates reduced average length of stay from 46 to from 80 to 9, saving up to 2 and half hours 24 days by discussing housing issues each week earlier in a patients stay

 Apply to be a Coach")
163 Want more information? Stories & case Studies Events (Open Invite) Apply to be a Coach Apply to have your team coached
164 FLOW FLOW COACHING ACADEMY



165 Flow Coaching Academy: Cohort 1
166 Length of stay for >75y medical patients


167 FLOW FLOW FLOW COACHING ACADEMY FLOW COACHING ACADEMY Shared System Understanding Participation Build a Consensus Build a Big Room Collective Creativity FLOW FLOW COACHING ACADEMY FLOW FLOW COACHING ACADEMY FLOW FLOW FLOW COACHING ACADEMY FLOW COACHING ACADEMY Rhythm & Pace Move beyond silos A forum A physical space
168 WHO SHOULD ATTEND THIS COURSE?
169
A Step-by-Step Guide to Tackling your Challenges
 Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health
 REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
Basic Knowledge of Clinical Microsystems. Success Characteristics of Great Clinical Microsystems Developing Microsystems
 Basic Knowledge of Clinical Microsystems Success Characteristics of Great Clinical Microsystems Developing Microsystems Marjorie M. Godfrey, PhD, MS, BSN Co-Director, The Dartmouth Institute Microsystem
Basic Knowledge of Clinical Microsystems Success Characteristics of Great Clinical Microsystems Developing Microsystems Marjorie M. Godfrey, PhD, MS, BSN Co-Director, The Dartmouth Institute Microsystem
Online library of Quality, Service Improvement and Redesign tools. Process templates. collaboration trust respect innovation courage compassion
 Online library of Quality, Service Improvement and Redesign tools Process templates collaboration trust respect innovation courage compassion Process templates What is it? Process templates provide a visual
Online library of Quality, Service Improvement and Redesign tools Process templates collaboration trust respect innovation courage compassion Process templates What is it? Process templates provide a visual
Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust Tel
 Lean Thinking Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust neil.westwood@institute.nhs.uk Tel 07747794976 NHS Institute for Innovation and Improvement Plan for today
Lean Thinking Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust neil.westwood@institute.nhs.uk Tel 07747794976 NHS Institute for Innovation and Improvement Plan for today
Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA
 These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
Flow Coaching Academy programme
 Flow Coaching Academy programme Professor Tom Downes, MB BS, MRCP, MBA, MPH (Harvard) Clinical Lead for Quality Improvement Sheffield Teaching Hospitals Health Foundation / IHI QI Fellow 6 th July 2018
Flow Coaching Academy programme Professor Tom Downes, MB BS, MRCP, MBA, MPH (Harvard) Clinical Lead for Quality Improvement Sheffield Teaching Hospitals Health Foundation / IHI QI Fellow 6 th July 2018
Systems Thinking. The Quality Academy Tutorial 18
 Systems Thinking The Quality Academy Tutorial 18 Learning Objectives: You Will Learn About What a system is Importance of system change in HIV care Transforming systems with the help of quality improvement
Systems Thinking The Quality Academy Tutorial 18 Learning Objectives: You Will Learn About What a system is Importance of system change in HIV care Transforming systems with the help of quality improvement
Emergency Medicine Programme
 Emergency Medicine Programme Implementation Guide 8: Matching Demand and Capacity in the ED January 2013 Introduction This is a guide for Emergency Department (ED) and hospital operational management teams
Emergency Medicine Programme Implementation Guide 8: Matching Demand and Capacity in the ED January 2013 Introduction This is a guide for Emergency Department (ED) and hospital operational management teams
Improvement Leaders Guide Improving flow Process and systems thinking
 Improvement Leaders Guide Improving flow Process and systems thinking Improvement Leaders Guides The ideas and advice in these Improvement Leaders Guides will provide a foundation for all your improvement
Improvement Leaders Guide Improving flow Process and systems thinking Improvement Leaders Guides The ideas and advice in these Improvement Leaders Guides will provide a foundation for all your improvement
Rapid Cycle Improvement
 Rapid Cycle Improvement with PDSA CPSI Forum April 30, 2009 Eileen Patterson, MCE Director - Quality Improvement Ontario Health Quality Council 1 What is it? Roots are within System of Profound Knowledge;
Rapid Cycle Improvement with PDSA CPSI Forum April 30, 2009 Eileen Patterson, MCE Director - Quality Improvement Ontario Health Quality Council 1 What is it? Roots are within System of Profound Knowledge;
NHS. Top tips to overcome the challenge of commissioning diagnostic services. NHS Improvement - Diagnostics. NHS Improvement Diagnostics CANCER
 CANCER NHS NHS Improvement Diagnostics DIAGNOSTICS HEART LUNG STROKE NHS Improvement - Diagnostics Top tips to overcome the challenge of commissioning diagnostic services Top tips to overcome the challenge
CANCER NHS NHS Improvement Diagnostics DIAGNOSTICS HEART LUNG STROKE NHS Improvement - Diagnostics Top tips to overcome the challenge of commissioning diagnostic services Top tips to overcome the challenge
Leadership. David Dalton Chief Executive
 Leadership David Dalton Chief Executive Effective Modern Leadership Leaders at all levels are crucial in creating the culture of care and compassion in the NHS. Today s effective leaders in the NHS demonstrate
Leadership David Dalton Chief Executive Effective Modern Leadership Leaders at all levels are crucial in creating the culture of care and compassion in the NHS. Today s effective leaders in the NHS demonstrate
Objective: To practice quality improvement tools by applying them to an improvement effort in an ambulatory care setting.
 Exercise 1 Objective: To practice quality improvement tools by applying them to an improvement effort in an ambulatory care setting. 1. Read the following case study. 2. Follow the instructions at the
Exercise 1 Objective: To practice quality improvement tools by applying them to an improvement effort in an ambulatory care setting. 1. Read the following case study. 2. Follow the instructions at the
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Boarding Impact on patients, hospitals and healthcare systems
 Boarding Impact on patients, hospitals and healthcare systems Dan Beckett Consultant Acute Physician NHSFV National Clinical Lead Whole System Patient Flow Project Scottish Government May 2014 Important
Boarding Impact on patients, hospitals and healthcare systems Dan Beckett Consultant Acute Physician NHSFV National Clinical Lead Whole System Patient Flow Project Scottish Government May 2014 Important
In this edition we will showcase the work of the development of a model for GP- Paediatric Hubs
 Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Elaine Andrews, Assistant Director of Nursing & Safety and Caroline Booton Quality Analyst Jill Asbury, Acting Director of Nursing
 Report to: Board of Directors Date of Meeting: 26 th October 2016 Report Title: Inpatient Falls Report Status: Mark relevant box with X Prepared by: Executive Sponsor (presenting): For information x Discussion
Report to: Board of Directors Date of Meeting: 26 th October 2016 Report Title: Inpatient Falls Report Status: Mark relevant box with X Prepared by: Executive Sponsor (presenting): For information x Discussion
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
University of Michigan Health System
 University of Michigan Health System Programs and Operations Analysis Analysis of the Discharge Process at Internal Medicine Unit B Department of Internal Medicine Final Report To: Dr. Christopher Kim,
University of Michigan Health System Programs and Operations Analysis Analysis of the Discharge Process at Internal Medicine Unit B Department of Internal Medicine Final Report To: Dr. Christopher Kim,
Delivering the Five Year Forward View. through Business Intelligence
 Delivering the Five Year Forward View through Business Intelligence Introduction The market for analytics has matured significantly in the past five years and, although the health sector in the UK has
Delivering the Five Year Forward View through Business Intelligence Introduction The market for analytics has matured significantly in the past five years and, although the health sector in the UK has
UNC2 Practice Test. Select the correct response and jot down your rationale for choosing the answer.
 UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
How to Initiate and Sustain Operational Excellence in Healthcare Delivery: Evidence from Multiple Field Experiments
 How to Initiate and Sustain Operational Excellence in Healthcare Delivery: Evidence from Multiple Field Experiments Aravind Chandrasekaran PhD Peter Ward PhD Fisher College of Business Ohio State University
How to Initiate and Sustain Operational Excellence in Healthcare Delivery: Evidence from Multiple Field Experiments Aravind Chandrasekaran PhD Peter Ward PhD Fisher College of Business Ohio State University
Transformational Patient Care Redesign Project
 Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Admissions and Planned Discharge
 Releasing Time to Care The Productive Mental Health Ward Admissions and Planned Discharge Version 1 This document is for ward leaders, lead nurses, matrons, nursing directors and directors with responsibility
Releasing Time to Care The Productive Mental Health Ward Admissions and Planned Discharge Version 1 This document is for ward leaders, lead nurses, matrons, nursing directors and directors with responsibility
TEAM ASSESSMENT PULL PROCESS CHILDREN S HEALTHCARE OF ATLANTA AT SCOTTISH RITE
 Publication Year: 2011 TEAM ASSESSMENT PULL PROCESS CHILDREN S HEALTHCARE OF ATLANTA AT SCOTTISH RITE Summary: The Team Assessment Pull Process (TAPP) is a technique to redesign emergency department patient
Publication Year: 2011 TEAM ASSESSMENT PULL PROCESS CHILDREN S HEALTHCARE OF ATLANTA AT SCOTTISH RITE Summary: The Team Assessment Pull Process (TAPP) is a technique to redesign emergency department patient
LV Prasad Eye Institute Annotated Bibliography
 Annotated Bibliography Finkler SA, Knickman JR, Hendrickson G, et al. A comparison of work-sampling and time-and-motion techniques for studies in health services research.... 2 Zheng K, Haftel HM, Hirschl
Annotated Bibliography Finkler SA, Knickman JR, Hendrickson G, et al. A comparison of work-sampling and time-and-motion techniques for studies in health services research.... 2 Zheng K, Haftel HM, Hirschl
The Power of Quality. Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center
 The Power of Quality Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center What do you think of when you hear the word quality? LEAN RCA PDSA QAPI SIX SIGMA PIP TQM 5s Objectives Transplant
The Power of Quality Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center What do you think of when you hear the word quality? LEAN RCA PDSA QAPI SIX SIGMA PIP TQM 5s Objectives Transplant
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations
 ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
CASE STUDY The Safer Patients Initiative
 CSE STUDY The Safer Patients Initiative Critical care in practice: Royal ree Hospital and the University Hospital of Wales 1. INTRODUCTION In late 4, the Health oundation funded the Institute for Healthcare
CSE STUDY The Safer Patients Initiative Critical care in practice: Royal ree Hospital and the University Hospital of Wales 1. INTRODUCTION In late 4, the Health oundation funded the Institute for Healthcare
Same day emergency care: clinical definition, patient selection and metrics
 Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
A Framework for Quality Improvement
 U019 - Integrating QI into the Derm Practice A Framework for Quality Improvement Margo Reeder, MD Assistant Professor Director of Quality Improvement UWSMPH July 30 2016 Quality is increasingly part of
U019 - Integrating QI into the Derm Practice A Framework for Quality Improvement Margo Reeder, MD Assistant Professor Director of Quality Improvement UWSMPH July 30 2016 Quality is increasingly part of
IS YOUR QAPI COP READY?
 IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
University of Michigan Health System Program and Operations Analysis. Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients
 University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
AN APPOINTMENT ORDER OUTPATIENT SCHEDULING SYSTEM THAT IMPROVES OUTPATIENT EXPERIENCE
 AN APPOINTMENT ORDER OUTPATIENT SCHEDULING SYSTEM THAT IMPROVES OUTPATIENT EXPERIENCE Yu-Li Huang, Ph.D. Assistant Professor Industrial Engineering Department New Mexico State University 575-646-2950 yhuang@nmsu.edu
AN APPOINTMENT ORDER OUTPATIENT SCHEDULING SYSTEM THAT IMPROVES OUTPATIENT EXPERIENCE Yu-Li Huang, Ph.D. Assistant Professor Industrial Engineering Department New Mexico State University 575-646-2950 yhuang@nmsu.edu
University of Michigan Comprehensive Stroke Center
 University of Michigan Comprehensive Stroke Center Improving the Discharge and Post-Discharge Process Flow Final Report Date: April 18, 2017 To: Jenevra Foley, Operating Director of Stroke Center, jenevra@med.umich.edu
University of Michigan Comprehensive Stroke Center Improving the Discharge and Post-Discharge Process Flow Final Report Date: April 18, 2017 To: Jenevra Foley, Operating Director of Stroke Center, jenevra@med.umich.edu
We plan. We achieve.
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
Targets, flow, exit block, stranded patients, red2green. What s any of this got to do with good patient care?
 Targets, flow, exit block, stranded patients, red2green. What s any of this got to do with good patient care? Lee Dowson Divisional Director of Medicine Royal Wolverhampton NHS Trust Clinical Associate
Targets, flow, exit block, stranded patients, red2green. What s any of this got to do with good patient care? Lee Dowson Divisional Director of Medicine Royal Wolverhampton NHS Trust Clinical Associate
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Faculty Session 1 Time Title Objectives Tied to others Brent James, MD. Always together w/pragmatic 1. Always together w/modelling Processes 1
 Faculty Session Time Title Objectives Tied to others Managing Clinical Processes: An Definition of processes Always together w/ Methods Introduction to Clinical QI Quality improvement as the science of
Faculty Session Time Title Objectives Tied to others Managing Clinical Processes: An Definition of processes Always together w/ Methods Introduction to Clinical QI Quality improvement as the science of
A Year in an Hour. NIHR CLAHRC Northwest London. Collaboration for Leadership in Applied Health Research and Care Northwest London
 A Year in an Hour Prof Julie Reed @julie4clahrc Collaboration for Leadership in Applied Health Research and Care The National Institute for Health Research Collaboration for Leadership in Applied Health
A Year in an Hour Prof Julie Reed @julie4clahrc Collaboration for Leadership in Applied Health Research and Care The National Institute for Health Research Collaboration for Leadership in Applied Health
The CHANGE room story
 The CHANGE room story Dr Jennifer Hill Clinical Director of Respiratory Medicine NIHR CLAHRC for Yorkshire & Humber What is the Respiratory service in Sheffield? National - Pulmonary hypertension Regional
The CHANGE room story Dr Jennifer Hill Clinical Director of Respiratory Medicine NIHR CLAHRC for Yorkshire & Humber What is the Respiratory service in Sheffield? National - Pulmonary hypertension Regional
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, Mike Williams, MPH/HSA The Abaris Group
 NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
COMPARATIVE STUDY OF HOSPITAL ADMINISTRATIVE DATA USING CONTROL CHARTS
 International Jour. of Manage.Studies.,Statistics & App.Economics (IJMSAE), ISSN 2250-0367, Vol. 7, No. I (June 2017), pp. 1-12 COMPARATIVE STUDY OF HOSPITAL ADMINISTRATIVE DATA USING CONTROL CHARTS SUCHETA
International Jour. of Manage.Studies.,Statistics & App.Economics (IJMSAE), ISSN 2250-0367, Vol. 7, No. I (June 2017), pp. 1-12 COMPARATIVE STUDY OF HOSPITAL ADMINISTRATIVE DATA USING CONTROL CHARTS SUCHETA
Improving operating room efficiency through the use of lean six sigma methodologies. Teodora O. Nicolescu
 Improving operating room efficiency through the use of lean six sigma methodologies Teodora O. Nicolescu Author detail: Teodora O. Nicolescu, MD Associate Professor Department of Anesthesiology The University
Improving operating room efficiency through the use of lean six sigma methodologies Teodora O. Nicolescu Author detail: Teodora O. Nicolescu, MD Associate Professor Department of Anesthesiology The University
Step by step measurement guide
 Step by step measurement guide The guide has been produced under a creative commons license please use the symbols shown for guidance if you wish to use or adapt the material This edited presentation has
Step by step measurement guide The guide has been produced under a creative commons license please use the symbols shown for guidance if you wish to use or adapt the material This edited presentation has
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Advanced SPC for Healthcare. Introductions
 Advanced SPC for Healthcare December 5, 20 Brent James, MD, Intermountain Healthcare James Benneyan, PhD, Northeastern University Victoria Jordan, PhD, UT MD Anderson Cancer Center Introductions Who are
Advanced SPC for Healthcare December 5, 20 Brent James, MD, Intermountain Healthcare James Benneyan, PhD, Northeastern University Victoria Jordan, PhD, UT MD Anderson Cancer Center Introductions Who are
Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship
 Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship Diane Levine, Wayne State University Allison Heacock, The Ohio State University Amy Shaheen, University of North Carolina
Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship Diane Levine, Wayne State University Allison Heacock, The Ohio State University Amy Shaheen, University of North Carolina
Online library of Quality, Service Improvement and Redesign tools. Discharge planning. collaboration trust respect innovation courage compassion
 Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
October 2, 2015 Page 1
 Run Charts, Control Charts, and SPC: Basic Power Tools for Quality Improvement James I. Hagadorn MD MSc Division of Neonatology, Department of Pediatrics University of Connecticut School of Medicine Connecticut
Run Charts, Control Charts, and SPC: Basic Power Tools for Quality Improvement James I. Hagadorn MD MSc Division of Neonatology, Department of Pediatrics University of Connecticut School of Medicine Connecticut
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Shared Decision Making: A Practice Manual for Implementers
 Shared Decision Making: A Practice Manual for Implementers Judy Chang, Douglas Conrad, Anne Renz, and Carolyn Watts University of Washington, Seattle, WA May 2011 http://depts.washington.edu/shareddm Introduction
Shared Decision Making: A Practice Manual for Implementers Judy Chang, Douglas Conrad, Anne Renz, and Carolyn Watts University of Washington, Seattle, WA May 2011 http://depts.washington.edu/shareddm Introduction
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS
 CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
Quality Improvement in Health and Social Care
 Some Fundamentals on Quality Improvement in Health and Social Care Towards a Shared Understanding EPSO, Reykjavik, 2017-09-26 Johan Thor, MD, MPH, PhD Associate Professor E-mail: johan.thor@ju.se The death
Some Fundamentals on Quality Improvement in Health and Social Care Towards a Shared Understanding EPSO, Reykjavik, 2017-09-26 Johan Thor, MD, MPH, PhD Associate Professor E-mail: johan.thor@ju.se The death
An Analysis of Waiting Time Reduction in a Private Hospital in the Middle East
 University of Tennessee Health Science Center UTHSC Digital Commons Applied Research Projects Department of Health Informatics and Information Management 2014 An Analysis of Waiting Time Reduction in a
University of Tennessee Health Science Center UTHSC Digital Commons Applied Research Projects Department of Health Informatics and Information Management 2014 An Analysis of Waiting Time Reduction in a
Releasing Time to Care The Productive Ward Programme Proposed Implementation Paper March 23rd 2009
 Releasing Time to Care The Productive Ward Programme Proposed Implementation Paper March 23rd 2009 1 CONTENTS TABLE PAGE Page 2 Page 3 Page 4 Page 6 CONTENT Contents Page Introduction & Background Benefits
Releasing Time to Care The Productive Ward Programme Proposed Implementation Paper March 23rd 2009 1 CONTENTS TABLE PAGE Page 2 Page 3 Page 4 Page 6 CONTENT Contents Page Introduction & Background Benefits
Online library of Quality, Service Improvement and Redesign tools. Reliable design. collaboration trust respect innovation courage compassion
 Online library of Quality, Service Improvement and Redesign tools Reliable design collaboration trust respect innovation courage compassion Reliable design What is it? Patients receiving the right care,
Online library of Quality, Service Improvement and Redesign tools Reliable design collaboration trust respect innovation courage compassion Reliable design What is it? Patients receiving the right care,
The Oncology Project Year 3
 The Oncology Project Year 3 Dr Alison Brewster Consultant Clinical Oncologist, Velindre Hospital Introduction to the Oncology Project Why is it important? Learning objectives Process Tutorials Patient
The Oncology Project Year 3 Dr Alison Brewster Consultant Clinical Oncologist, Velindre Hospital Introduction to the Oncology Project Why is it important? Learning objectives Process Tutorials Patient
IMPROVING RESIDENT HANDOFFS. Educating for Quality Improvement & Patient Safety
 IMPROVING RESIDENT HANDOFFS Educating for Quality Improvement & Patient Safety 1 Stephanie Reeves, DO has no relevant financial relationships with commercial interests to disclose. 2 CS&E Participant Stephanie
IMPROVING RESIDENT HANDOFFS Educating for Quality Improvement & Patient Safety 1 Stephanie Reeves, DO has no relevant financial relationships with commercial interests to disclose. 2 CS&E Participant Stephanie
Root Cause Analysis. Why things happen
 Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Quality Management Program
 Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
World Health Organization Male Circumcision Quality Assurance Workshop 2010
 Male Circumcision Quality Assurance Workshop World Health Organization 1 DAY 3 2 Giving Feedback: The Debriefing Assessment team determines information to share Relate comments to the specific standard
Male Circumcision Quality Assurance Workshop World Health Organization 1 DAY 3 2 Giving Feedback: The Debriefing Assessment team determines information to share Relate comments to the specific standard
Integrating quality improvement into pre-registration education
 Integrating quality improvement into pre-registration education Jones A et al (2013) Integrating quality improvement into pre-registration education. Nursing Standard. 27, 29, 44-48. Date of submission:
Integrating quality improvement into pre-registration education Jones A et al (2013) Integrating quality improvement into pre-registration education. Nursing Standard. 27, 29, 44-48. Date of submission:
Tips and Tools for Learning Improvement. Developing Changes
 Tips and Tools for Learning Improvement Developing Changes What are changes in improvement? Making improvement requires change. Changes are any possible solutions to problems identified by improvement
Tips and Tools for Learning Improvement Developing Changes What are changes in improvement? Making improvement requires change. Changes are any possible solutions to problems identified by improvement
Using QI tools: Action Effect Diagrams
 Using QI tools: Action Effect Diagrams Tom Woodcock Supported by and delivering for: London s NHS organisations include all of London s CCGs, NHS England and Health Education England 1 Learning Objectives
Using QI tools: Action Effect Diagrams Tom Woodcock Supported by and delivering for: London s NHS organisations include all of London s CCGs, NHS England and Health Education England 1 Learning Objectives
8/10/2015. Module 1. A Fundamental Understanding of Quality. Management and its Application to Health Care
 Module 1 A Fundamental Understanding of Quality Management and its Application to Health Care Addressing Physician Uncertainty about Payment Reform: Skills for Success in Value-Based Delivery Systems The
Module 1 A Fundamental Understanding of Quality Management and its Application to Health Care Addressing Physician Uncertainty about Payment Reform: Skills for Success in Value-Based Delivery Systems The
Quality Improvement Scorecard November 2017
 Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance
 Directorate for Health Workforce and Performance") Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance A Whole System Approach to Patient Flow for Scotland Our Quality Improvement Approach Jane Murkin Programme
Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance A Whole System Approach to Patient Flow for Scotland Our Quality Improvement Approach Jane Murkin Programme
National Programme to Prevent Central-Line Associated Bacteraemia. Project Charter October 2011 to April 2013
 National Programme to Prevent Central-Line Associated Bacteraemia Project Charter October 2011 to April 2013 1. Overview Central-Line Associated Bacteraemia (CLAB) prevention is one of the most important
National Programme to Prevent Central-Line Associated Bacteraemia Project Charter October 2011 to April 2013 1. Overview Central-Line Associated Bacteraemia (CLAB) prevention is one of the most important
Example 1: Self-Management: Development of a Self-Management form, Part 1
 PDSA examples Example 1 We have concentrated on a collection of PDSA cycles that are relatively small in focus and time span, to emphasise the importance of small, rapid tests of change. Many of these
PDSA examples Example 1 We have concentrated on a collection of PDSA cycles that are relatively small in focus and time span, to emphasise the importance of small, rapid tests of change. Many of these
2018 African Forum on Quality and Safety in Healthcare. Better Quality Through Better Measurement. Session Objectives
 2018 African Forum on Quality and Safety in Healthcare Better Quality Through Better Measurement Faculty Robert Lloyd, PhD, Vice President 20 February 2018 Session Objectives To evaluate your knowledge
2018 African Forum on Quality and Safety in Healthcare Better Quality Through Better Measurement Faculty Robert Lloyd, PhD, Vice President 20 February 2018 Session Objectives To evaluate your knowledge
Performance. Improvement in Scheduled Care Waiting List Management TOOLKIT. An Roinn Sláinte DEPARTMENT OF HEALTH. January 2013
 Performance TOOLKIT in Scheduled Care January 2013 Patient Toolkit Pathways Performance in Scheduled Care Setting the context and initiating whole systems change for the delivery of scheduled care and
Performance TOOLKIT in Scheduled Care January 2013 Patient Toolkit Pathways Performance in Scheduled Care Setting the context and initiating whole systems change for the delivery of scheduled care and
Safe medication practice what can we learn from root cause analysis and related methods?
 Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
Engaging Frontline Staff in Real-Time Improvement
 Engaging Frontline Staff in Real-Time Improvement Sharon Mann and Jennifer Phillips Session Code C6 These presenters have nothing to disclose Institute for Healthcare Improvement December 2013 2012 2013
Engaging Frontline Staff in Real-Time Improvement Sharon Mann and Jennifer Phillips Session Code C6 These presenters have nothing to disclose Institute for Healthcare Improvement December 2013 2012 2013
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Neurosurgery. Themes. Referral
 06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
University of Michigan Health System. Program and Operations Analysis. CSR Staffing Process. Final Report
 University of Michigan Health System Program and Operations Analysis CSR Staffing Process Final Report To: Jean Shlafer, Director, Central Staffing Resources, Admissions Bed Coordination Center Amanda
University of Michigan Health System Program and Operations Analysis CSR Staffing Process Final Report To: Jean Shlafer, Director, Central Staffing Resources, Admissions Bed Coordination Center Amanda
Health and care services in Herefordshire & Worcestershire are changing
 Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
Pave Your Path: Improvement Science & Helpful Techniques
 Pave Your Path These presenters have nothing to disclose Pave Your Path: Improvement Science & Helpful Techniques Cory Sevin, RN, MSN, NP Director, IHI Jane Taylor, EdD Improvement Advisory May 21, 2013
Pave Your Path These presenters have nothing to disclose Pave Your Path: Improvement Science & Helpful Techniques Cory Sevin, RN, MSN, NP Director, IHI Jane Taylor, EdD Improvement Advisory May 21, 2013
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
Seven day hospital services: case study. University Hospital Southampton NHS Foundation Trust
 Seven day hospital services: case study University Hospital Southampton NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health
Seven day hospital services: case study University Hospital Southampton NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health
Managing Elective Waiting Times A checklist for NHS health boards
 12 March 2015 Archwilydd Cyffredinol Cymru Auditor General for Wales Managing Elective Waiting Times A checklist for NHS health boards Introduction 1 The Auditor General published his report on NHS Waiting
12 March 2015 Archwilydd Cyffredinol Cymru Auditor General for Wales Managing Elective Waiting Times A checklist for NHS health boards Introduction 1 The Auditor General published his report on NHS Waiting
Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation
 Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation April 2018 Version 4.0 Document information Document purpose Document name Author Policy Specialised
Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation April 2018 Version 4.0 Document information Document purpose Document name Author Policy Specialised
PDSA and Project Presentations
 Improvement Advisor Professional Development Program Wave 42 PDSA and Project Presentations IA Wave 42 October 6, 2016 Agenda Time Topic Leader 3:00 BST Welcome and Check-In Prep for WS2 Jane 3:15 Reflect
Improvement Advisor Professional Development Program Wave 42 PDSA and Project Presentations IA Wave 42 October 6, 2016 Agenda Time Topic Leader 3:00 BST Welcome and Check-In Prep for WS2 Jane 3:15 Reflect
Quality Improvement Scorecard June 2017
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Basic Skills for CAH Quality Managers
 Basic Skills for CAH Quality Managers MARCH 20, 2014 THE BASICS OF DATA MANAGEMENT Data Management Systems COLLECTION AGGREGATION ASSESSMENT REPORTING 1 Some Data Management Terminology Objective data
Basic Skills for CAH Quality Managers MARCH 20, 2014 THE BASICS OF DATA MANAGEMENT Data Management Systems COLLECTION AGGREGATION ASSESSMENT REPORTING 1 Some Data Management Terminology Objective data
An analysis of the average waiting time during the patient discharge process at Kashani Hospital in Esfahan, Iran: a case study
 An analysis of the average waiting time during the patient discharge process at Kashani Hospital in Esfahan, Iran: a case study Sima Ajami and Saeedeh Ketabi Abstract Strategies for improving the patient
An analysis of the average waiting time during the patient discharge process at Kashani Hospital in Esfahan, Iran: a case study Sima Ajami and Saeedeh Ketabi Abstract Strategies for improving the patient
National Primary Care Cluster Event ABMU Health Board 13 th October 2016
 National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus
 University of Groningen The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
University of Groningen The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
Innovations for Integrating Quality and Safety in Education and Practice: The QSEN Project
 Innovations for Integrating Quality and Safety in Education and Practice: The QSEN Project Linda Cronenwett, PhD, RN, FAAN Principal Investigator, QSEN Gwen Sherwood, PhD, RN, FAAN Co-Investigator, QSEN
Innovations for Integrating Quality and Safety in Education and Practice: The QSEN Project Linda Cronenwett, PhD, RN, FAAN Principal Investigator, QSEN Gwen Sherwood, PhD, RN, FAAN Co-Investigator, QSEN
When going Lean, Waste is the Enemy
 When going Lean, Waste is the Enemy Eric S. Kastango, MBA, RPh, FASHP Clinical IQ, LLC March 31, 2009 Objectives Review the definition, elements and wastes of Lean Review the difference between Six Sigma
When going Lean, Waste is the Enemy Eric S. Kastango, MBA, RPh, FASHP Clinical IQ, LLC March 31, 2009 Objectives Review the definition, elements and wastes of Lean Review the difference between Six Sigma
Medical technologies guidance Published: 21 March 2018 nice.org.uk/guidance/mtg37
 Thopaz+ portable digital system for managing chest drains Medical technologies guidance Published: 21 March 2018 nice.org.uk/guidance/mtg37 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Thopaz+ portable digital system for managing chest drains Medical technologies guidance Published: 21 March 2018 nice.org.uk/guidance/mtg37 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).