Patricia Ryan MS RN Director VISN 8 Community Care Coordination Service Associate Chief Consultant VHA Office of Telehealth Services
|
|
|
- Scarlett Kerry Lindsey
- 5 years ago
- Views:
Transcription



1 Patricia Ryan MS RN Director VISN 8 Community Care Coordination Service Associate Chief Consultant VHA Office of Telehealth Services


2 The Existing Health Care System Tertiary Secondary Home Primary Doctor s Office Rural and Regional Health Hospitals Centers or Outpatient Clinics INREACH Referral Hospitals
3 The wider application of care and case management principles to the delivery of healthcare services using health informatics, disease management and Telehealth to facilitate access to care and to improve the health of designated individuals and populations with the specific intent of providing the right care in the right place at the right time.
4 Three major components: CCHT Care Coordination Home Telehealth CVT Clinical Video Telehealth SF Store and Forward Telehealth
5 2003: Initial funding for CCHT equipment for a small pilot group of VHA Networks (VISNs) : RFP for all VISNs in two phases Major focus on non-institutional care (NIC) and management of chronic conditions Now-More than 150 CCHT programs nationally 42,000+ patients actively enrolled currently Rural and Transformation Funding
6 CCHT may be utilized in a continuum with Primary Care Providers, clinic-based care managers and more traditional Primary Care or Specialty case managers as well as discharge planners and other disciplines involved in care. Care Coordinators are case managers who are able to leverage the use of health informatics, telehealth technologies and disease management strategies to coordinate care of patients with high risk, high cost or high utilization patterns.
7 Chronic conditions Frequents visits Enrolled at primary care clinics Telephone service in home Veteran/Caregiver accept/consent Cognitively intact, Veteran/Caregiver Veteran/Caregiver demonstrate competency using and maintaining CCHT equipment
8 Basic enrollment criteria include patients with high risk, high cost, high utilization patterns (adapted by each VISN or program for vulnerable populations) Decision support data from standard or ad hoc reports, registries, and other data sources used in some programs to help identify patients who meet the criteria above Provider consult submitted for CCHT; In some cases this is driven by policy/protocol Plan of care developed by the Care Coordinator and the Veteran in conjunction with goals & targets already identified by provider
9 Veterans living in Puerto Rico and US Virgin Islands with: DM Hgb A 1 C levels > 8% Congestive Heart Failure (CHF) Frequent Emergency Room visits High-cost/high cost/high-user SCI patients with DM diagnosis Chronic Conditions living in Rural Areas
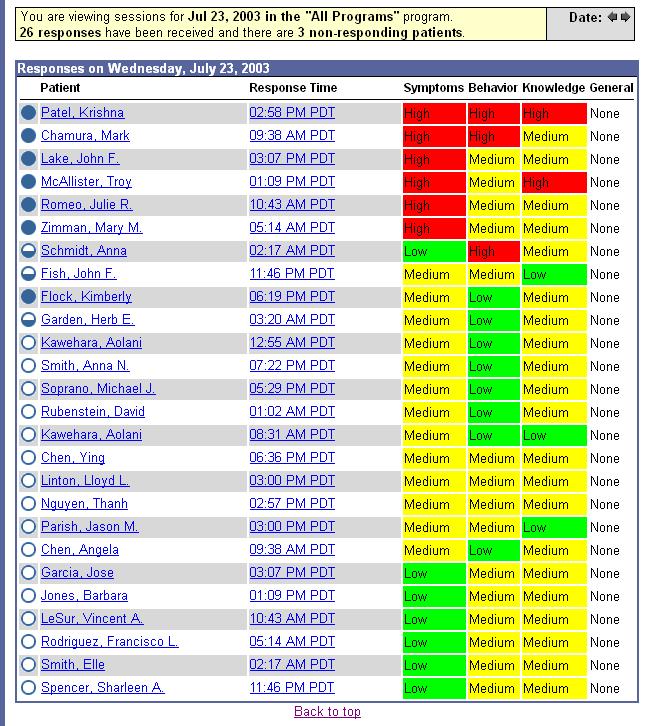
10 Monitor data daily submitted by patients using devices Triage data from vital signs, reported symptoms, question responses Contact patients with high risk responses, significant changes in condition or data elements received Identify and intervene for potential exacerbations or complications to facilitate: Just In Time care in clinic, ED/urgent care, community Provider directed interventions such as medication management Protocol-based interventions Self Management Education
11 11



12 Referrals by Medical Providers or Interdisciplinary Team Members Telehealth No Patient does not meet enrollment criteria Screening for Eligibility Criteria Enrollment Process Initiation of Care Yes Daily Tracking Process by Telehealth Technology Care Coordination Case Management Telephone Technology Mail Continues communication with Primary Provider, consult interdisciplinary team according to patient needs Patient Education Medication Compliance Diet Compliance Physical Activity Healthy Lifestyle Re-evaluation Compliance Maintenance Continued need for CCHT Management Non Compliance Goals met Discharge
 utilized on messaging devices Data submitted by")

13 Messaging devices, video monitoring, video phones, peripheral vital signs devices- all primarily POTS based currently Disease Management Protocols (DMPs) utilized on messaging devices Data submitted by patients through devices stored on vendor servers behind the VA firewall and accessed daily on VA desktop computers by Care Coordinators VistA Integration in process for selected data to transfer via HL7 messaging






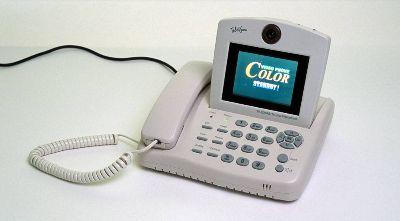

14 In Home Telehealth Technologies
15 Increased access and patient satisfaction Enhanced functional status and quality of life Increased Provider and CCHT staff satisfaction Reduced admissions and bed days of care Reduced clinic and ED visits Reduced nursing home admission rates Reduced overall costs for Veterans with history of frequent admissions and unscheduled clinic visits.
16
17 National quarterly CCHT Score Card includes data per VISN on census, NIC ADC, categories of care, utilization, performance measure and monitors, patient satisfaction, VR-12 summary data and other data elements. Outcomes published 12/08: Diabetes 8,954 pts nationally / utilization 20.4% Reduction of BDOC = 47% Patient satisfaction = 85%
18 Reductions in Utilization by Condition Monitored Condition Number Of Patients %Reduction Diabetes 8, % HTN 7, % CHF 4, % COPD 1, % Depression % PTSD % Other mental health % Single condition 10, % Multiple conditions 6, % Darkins A, Ryan P, Kobb R, Foster L, Edmonson E, Wakefield B, Lancaster B. Care coordination/home telehealth: The systematic implementation of health informatics, home telehealth, and disease management to support the care of veterans with chronic conditions. Telemed J E Health 2008;14:10,


19 Neale R. Chumbler, Ph.D. VA HSR&D Center of Excellence for Implementing Evidence-based Practice, Indianapolis VAMC; Department of Sociology, Indiana University School of Liberal Arts
20 Patients with diabetes enrolled in VA CCHT program at 4 VAMCs in a Southeast VISN Rigorous quasi-experimental design that used propensity scores to compensate for differences between CCHT program and comparison group 1. Diabetes patients enrolled in VA CCHT & prospectively followed (n=387). 2. Comparison group --- Matched comparison group (n = 387).
21 Unless closely monitored, diabetes can be associated with serious complications, including mortality & increased preventable service visits. 1) 12 months SF 36V---Physical functioning; bodily pain; social functioning 2) 24 mos. Significant reductions (by 25%, p =.02) Chumbler et al., 2005; Barnett et al., 2006;
22 Followed cohort over 4 years Quasi-experimental design More deaths in control group (n = 102, 26%) vs. CCHT group (n = 75, 19%, p =.02). Multivariate Analyses Controlled for demographic and clinical variables CCHT group --- Reduced 4-year all-cause mortality (HR = 0.7, 95% CI,.5-.9, p =.01) Chumbler et al., 2009
23 Patients with diabetes are 2 to 5 times more likely to be admitted for inpatient care than patients without diabetes Many studies found that hospitalizations for ambulatory care sensitive conditions (ACSCs) could be prevented if timely and appropriate care were accessible to patients We applied AHRQ s Preventable Quality Indicators (PQIs) to VA national databases to calculate preventable hospitalization use PQIs set of measures used with hospital inpatient data to identify 14 categories of ACSCs (e.g., asthma; uncontrolled diabetes; urinary infection) Donner 2008; Jia et al., 2009
24 Primary Research Question: Is the CCHT program for diabetes associated with less preventable hospital use during 4 year follow-up During initial 18 months of follow-up, CCHT enrollees with diabetes were less likely to be admitted for a preventable hospitalization (after adjusting for demographic and clinical characteristics) Over the 4-year period, control group patients had significantly higher frequency of diabetes long-term complications, lower limb amputation, and uncontrolled diabetes Jia et al., 2009
25 First study to assess specific types of inpatient utilization that were potentially preventable Illustrates the accessibility benefits of telehealth service as an attempt to offer timely and essential monitoring of patients Jia et al., 2009
26 Substantiates the importance of having a nurse use home messaging device to manage diabetes symptoms and conditions in a preventative manner, necessitating more advanced interventions
27 Barnett, TE., Chumbler NR, Vogel WB, Beyth RJ, Qin H, & Kobb R The effectiveness of a care coordination/hometelehealth program for veterans with diabetes: A two-year follow-up. The American Journal of Managed Care 12(8): Bates DW & Bitton A The future of health information technology in the patient centered medical home. Health Affairs 29(4): Chumbler NR, Haggstrom DH, Saleem, J. Implementation of health information technology in VHA to support transformational change: Telehealth and personal health records Apr. 23. [Epub ahead of print]. Medical Care.
28 Chumbler, NR, Chuang, HC, Wu, SS, Wang, X, Kobb, R, Haggstrom, D, Jia, H Mortality Risk for Diabetes Patients in a Care Coordination/Home-Telehealth Program. Journal of Telemedicine and Telecare 15: Chumbler, NR, Neugaard B, Ryan P, Kobb R, Qin H, & Joo Y Assessment of health services utilization and healthrelated quality of life in veterans with Diabetes enrolled in a VHA Community-Care Coordination Service program. Evaluation and the Health Professions 28: Jia H, Chuang H, Wu SS, Wang X, Chumbler NR Longterm impact of home telehealth service on preventable hospitalization use. Journal of Rehabilitation Research and Development 46(5):


29 Dana J. Cervone, APRN, PMHNP-BC VACT Healthcare System May 12 th, 2010


30 Assist the MH Clinician in managing the complex veteran (High Risk, High Use, High Cost) Provide Cost Effective Interdisciplinary team care approach Reduce/Prevent relapse/decompensation Reduce need for future acute hospitalizations Reduce ED presentations or unscheduled visits to Primary Psych Clinician Encourage increased self-management for Veterans with Chronic Mental Illness
31 Inclusions Exclusions Referral from MH Clinician Primary Psychiatric Dx. (Depression, Substance Abuse, PTSD, Schizophrenia, Bipolar) Housing with phone line (cellular / computer access) Psychiatrically stable enough for enrollment Unable to use basic technology Declined by patient Deemed to be clinically inappropriate by the MH Provider or Treatment Team and the Care Coordinator
32 Number and duration of admissions to inpatient unit in last year Number of presentations to PER in last year Multiple self harm attempts/gestures History of multiple unscheduled clinic visits or no-shows in the last year
33
34 Current average daily census of 96 with 94.8% meeting NIC-A criteria ( Exceeding Performance Measure at %) Increased Efficiency resulting in an increased caseload from veterans in 2008 to in Provider satisfaction at 100% in 2009, up from 70% the preceding year.
35 We reviewed 76 Veterans in the CCHT-TMH program. ED Visits in Psychiatry ED WHAV decreased after the patient was enrolled in the CCHT-TMH program. 62% or 47 ED visits were reported 6 months prior to enrollment Only 27% or 16 ED visits were reported 6 months after enrollment. Extract from Vista AAH ACRP Ad Hoc Report: Clinic Name PSYCHIATRY ER WHAV.
36 We reviewed 76 Veterans in the CCHT-TMH program. Admissions in 1-8WPSY decreased after the patient was enrolled in the CCHT-TMH program. 55% or 42 admissions were reported 6 months prior to enrollment 8% or 6 admissions were reported 6 months after enrollment. Extract from Vista Patient Movement Report Menu: Ward Admission Report and Transferred to Ward Report for 1-8WPSY
 (689) VA Connecticut")
 Veterans")


37 30 Day Readmission Rate for (V01) (689) VA Connecticut HCS, CT, Acute Psych (Fiscal Year in All Dates) 30 Day Readmission Rate for Veterans involved in Telemental Health Program 30 Day Readmission Rates from Pro-Clarity DSS Data Cubes
38
Telehealth in the Veterans Health Administration. Mary C. Foster, DNP, Telehealth Program Manager Mid-Atlantic Health Care Network January 27, 2016
 Telehealth in the Veterans Health Administration Mary C. Foster, DNP, Telehealth Program Manager Mid-Atlantic Health Care Network January 27, 2016 The Vision For Telehealth In VA Patient Focused Makes
Telehealth in the Veterans Health Administration Mary C. Foster, DNP, Telehealth Program Manager Mid-Atlantic Health Care Network January 27, 2016 The Vision For Telehealth In VA Patient Focused Makes
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2
 Program Grantees: Part 2") SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
Suicide Among Veterans and Other Americans Office of Suicide Prevention
 Suicide Among Veterans and Other Americans 21 214 Office of Suicide Prevention 3 August 216 Contents I. Introduction... 3 II. Executive Summary... 4 III. Background... 5 IV. Methodology... 5 V. Results
Suicide Among Veterans and Other Americans 21 214 Office of Suicide Prevention 3 August 216 Contents I. Introduction... 3 II. Executive Summary... 4 III. Background... 5 IV. Methodology... 5 V. Results
VHA Transformation to a Patient Centered Medical Home Model of Care
 VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
The Future of Home Health is Here
 The Future of Home Health is Here How Home Health Agencies Can Bridge the Care Gap for ACOs and Hospital Networks The Future of Home Health is Here How Home Health Agencies Can Bridge the Care Gap for
The Future of Home Health is Here How Home Health Agencies Can Bridge the Care Gap for ACOs and Hospital Networks The Future of Home Health is Here How Home Health Agencies Can Bridge the Care Gap for
In Press at Population Health Management. HEDIS Initiation and Engagement Quality Measures of Substance Use Disorder Care:
 In Press at Population Health Management HEDIS Initiation and Engagement Quality Measures of Substance Use Disorder Care: Impacts of Setting and Health Care Specialty. Alex HS Harris, Ph.D. Thomas Bowe,
In Press at Population Health Management HEDIS Initiation and Engagement Quality Measures of Substance Use Disorder Care: Impacts of Setting and Health Care Specialty. Alex HS Harris, Ph.D. Thomas Bowe,
Results from the Iowa Medicaid Congestive Heart Failure Population Disease Management
 EXECUTIVE SUMMARY Study Validates Use of Technology-Based Remote Monitoring Platform to Reduce Healthcare Utilization and Cost Results from the Iowa Medicaid Congestive Heart Failure Population Disease
EXECUTIVE SUMMARY Study Validates Use of Technology-Based Remote Monitoring Platform to Reduce Healthcare Utilization and Cost Results from the Iowa Medicaid Congestive Heart Failure Population Disease
Disease Management at Anthem West Or: what have we learned in trying to design these programs?
 Disease Management at Anthem West Or: what have we learned in trying to design these programs? Lisa M. Latts, MD, MSPH Regional Medical Director May 12, 2003 Anthem Inc. Anthem Inc. Headquarters: Indianapolis
Disease Management at Anthem West Or: what have we learned in trying to design these programs? Lisa M. Latts, MD, MSPH Regional Medical Director May 12, 2003 Anthem Inc. Anthem Inc. Headquarters: Indianapolis
A Path to Self-actualization:
 A Path to Self-actualization: Maximizing Quality of Life for People with Chronic Disease Lisa Bujno, APRN Associate Chief Nurse, Quality and Performance White River Junction VAMC May 12, 2015 May 12, 2015
A Path to Self-actualization: Maximizing Quality of Life for People with Chronic Disease Lisa Bujno, APRN Associate Chief Nurse, Quality and Performance White River Junction VAMC May 12, 2015 May 12, 2015
1331 Garden Highway Sacramento, CA
 Fiscal Impact of AB 415: Potential Cost Savings from Expansion of Telehealth Matthew Newman & Trisha McMahon, Blue Sky Consulting September 30, 2011 A fiscal analysis of AB 415, The Telehealth Advancement
Fiscal Impact of AB 415: Potential Cost Savings from Expansion of Telehealth Matthew Newman & Trisha McMahon, Blue Sky Consulting September 30, 2011 A fiscal analysis of AB 415, The Telehealth Advancement
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Department of Veterans Affairs VHA DIRECTIVE Veterans Health Administration Washington, DC December 7, 2005
 Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
HIDD 101 HOSPITAL INPATIENT AND DISCHARGE DATA IN NEW MEXICO
 HIDD 101 HOSPITAL INPATIENT AND DISCHARGE DATA IN NEW MEXICO Health Information System Act (24-14A-1, et seq. NMSA 1978) Provides authority for the Department of Health to collect health data. NMDOH had
HIDD 101 HOSPITAL INPATIENT AND DISCHARGE DATA IN NEW MEXICO Health Information System Act (24-14A-1, et seq. NMSA 1978) Provides authority for the Department of Health to collect health data. NMDOH had
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health
 Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Telemedicine/Telehealth
 Telemedicine/Telehealth Technology Tools for Enhanced Clinical Support June 2016 Once upon a very different time, doctors arrived at one s doorstep carrying a black bag packed with a thermometer, a stethoscope,
Telemedicine/Telehealth Technology Tools for Enhanced Clinical Support June 2016 Once upon a very different time, doctors arrived at one s doorstep carrying a black bag packed with a thermometer, a stethoscope,
Mental Health at Mercy Health: Treating the Whole Person. David E. Blair, MD Mercy Health Physician Partners President and CMO
 Mental Health at Mercy Health: Treating the Whole Person David E. Blair, MD Mercy Health Physician Partners President and CMO Trinity Health s 22-state diversified system today $17.6B In Revenue 1.3M Attributed
Mental Health at Mercy Health: Treating the Whole Person David E. Blair, MD Mercy Health Physician Partners President and CMO Trinity Health s 22-state diversified system today $17.6B In Revenue 1.3M Attributed
Hospital Discharge Data, 2005 From The University of Memphis Methodist Le Bonheur Center for Healthcare Economics
 Hospital Discharge Data, 2005 From The University of Memphis Methodist Le Bonheur Center for Healthcare Economics August 22, 2008 Potentially Avoidable Pediatric Hospitalizations in Tennessee, 2005 Cyril
Hospital Discharge Data, 2005 From The University of Memphis Methodist Le Bonheur Center for Healthcare Economics August 22, 2008 Potentially Avoidable Pediatric Hospitalizations in Tennessee, 2005 Cyril
Policies for Controlling Volume January 9, 2014
 Policies for Controlling Volume January 9, 2014 The Maryland Hospital Association Policies for controlling volume Introduction Under the proposed demonstration model, the HSCRC will move from a regulatory
Policies for Controlling Volume January 9, 2014 The Maryland Hospital Association Policies for controlling volume Introduction Under the proposed demonstration model, the HSCRC will move from a regulatory
Veterans Health Administration: Surveillance of Cardiovascular Disease, Diabetes Mellitus, and Chronic Obstructive Pulmonary Disease
 Veterans Health Administration: Surveillance of Cardiovascular Disease, Diabetes Mellitus, and Chronic Obstructive Pulmonary Disease Paul D. Varosy, MD Director of Cardiac Electrophysiology VA Eastern
Veterans Health Administration: Surveillance of Cardiovascular Disease, Diabetes Mellitus, and Chronic Obstructive Pulmonary Disease Paul D. Varosy, MD Director of Cardiac Electrophysiology VA Eastern
Statistical Analysis Plan
 Statistical Analysis Plan CDMP quantitative evaluation 1 Data sources 1.1 The Chronic Disease Management Program Minimum Data Set The analysis will include every participant recorded in the program minimum
Statistical Analysis Plan CDMP quantitative evaluation 1 Data sources 1.1 The Chronic Disease Management Program Minimum Data Set The analysis will include every participant recorded in the program minimum
Forces Shaping Integrated Care. Presenters OBJECTIVES. Care Coordination in Integrated Care: Development of a Role for Psychiatric RNs
 Care Coordination in Integrated Care: Development of a Role for Psychiatric RNs APNA 29 th Annual Conference Lake Buena Vista, Florida Session #3022 October 30, 2015 Presenters Joyce Shea, DNSc, PMHCNS
Care Coordination in Integrated Care: Development of a Role for Psychiatric RNs APNA 29 th Annual Conference Lake Buena Vista, Florida Session #3022 October 30, 2015 Presenters Joyce Shea, DNSc, PMHCNS
Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies
 Improvement Strategies") Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies 1. What efforts and/or strategies have you put in place to improve your plans performance on the Follow-Up After Hospitalization
Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies 1. What efforts and/or strategies have you put in place to improve your plans performance on the Follow-Up After Hospitalization
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES
 EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Risk Stratification: Necessary Tool for Value-Based Payments
 Risk Stratification: Necessary Tool for Value-Based Payments Presenters: Jolene Rasmussen, Texas Council of Community Centers Tim Markello, Gulf Coast Center Mary Duffy, Bluebonnet Trails Community Services
Risk Stratification: Necessary Tool for Value-Based Payments Presenters: Jolene Rasmussen, Texas Council of Community Centers Tim Markello, Gulf Coast Center Mary Duffy, Bluebonnet Trails Community Services
Innovations in Expanding Primary Care Capacity: Moving Away from Visit Based Care for Medicare Beneficiaries
 Innovations in Expanding Primary Care Capacity: Moving Away from Visit Based Care for Medicare Beneficiaries IOM 9/22/11 Kathy Duckett RN, BSN Director of Clinical Programs Partners Healthcare at Home
Innovations in Expanding Primary Care Capacity: Moving Away from Visit Based Care for Medicare Beneficiaries IOM 9/22/11 Kathy Duckett RN, BSN Director of Clinical Programs Partners Healthcare at Home
Behavioral Health Division JPS Health Network
 Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
UTILIZING TELEHEALTH SERVICES TO IMPROVE ACCESS TO QUALITY CARE IN RURAL SETTINGS
 UTILIZING TELEHEALTH SERVICES TO IMPROVE ACCESS TO QUALITY CARE IN RURAL SETTINGS Charles Gizara, MS, BSN, RN, CCM Director Integrated Care Management Jennifer Light, RN Telehealth Coordinator Goals /
UTILIZING TELEHEALTH SERVICES TO IMPROVE ACCESS TO QUALITY CARE IN RURAL SETTINGS Charles Gizara, MS, BSN, RN, CCM Director Integrated Care Management Jennifer Light, RN Telehealth Coordinator Goals /
UCARE MODEL OF CARE SUMMARY FOR MH-TCM (February 2009)
") UCARE MODEL OF CARE SUMMARY FOR MH-TCM (February 2009) The UCare Model of Care for Mental Health Targeted Case Management is designed to provide care for the child member and their families and adult members,
UCARE MODEL OF CARE SUMMARY FOR MH-TCM (February 2009) The UCare Model of Care for Mental Health Targeted Case Management is designed to provide care for the child member and their families and adult members,
HealthPartners SNBC Inspire
 Click to edit Master title style HealthPartners SNBC Inspire March 28 & 30, 2017 Agenda New Team Members DHS SNBC Audit 6 Month Follow Up Calls Benefit Exception Inquiry Form Adjustments HealthPartners
Click to edit Master title style HealthPartners SNBC Inspire March 28 & 30, 2017 Agenda New Team Members DHS SNBC Audit 6 Month Follow Up Calls Benefit Exception Inquiry Form Adjustments HealthPartners
VHA Mental Health Program Office Update VA Psychologist Leader Conference
 VHA Mental Health Program Office Update VA Psychologist Leader Conference Wendy Tenhula, PhD Acting Deputy Chief Consultant for Specialty Mental Heath David Carroll, PhD Executive Director, Office of Mental
VHA Mental Health Program Office Update VA Psychologist Leader Conference Wendy Tenhula, PhD Acting Deputy Chief Consultant for Specialty Mental Heath David Carroll, PhD Executive Director, Office of Mental
Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014
 Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014 Data analysis at a population level Implications for our care model Facilitated discussion Population management
Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014 Data analysis at a population level Implications for our care model Facilitated discussion Population management
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Behavioral Health Initial Review Form
 Behavioral Health Initial Review Form https://providers.amerigroup.com This form is for inpatients, the Partial Hospitalization Program and the Intensive Outpatient Program. Please submit this form on
Behavioral Health Initial Review Form https://providers.amerigroup.com This form is for inpatients, the Partial Hospitalization Program and the Intensive Outpatient Program. Please submit this form on
Southwest Texas Regional Advisory Council
 Executive Summary In 1989, the Texas legislature identified a need to ensure trauma resources were available to every person in Texas. The Omni Rural Health Care Rescue Act, directed the Bureau of Emergency
Executive Summary In 1989, the Texas legislature identified a need to ensure trauma resources were available to every person in Texas. The Omni Rural Health Care Rescue Act, directed the Bureau of Emergency
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
VA Connects: Telemental Health Regional Center
 VA Connects: Telemental Health Regional Center Martin P. Paulus, M.D. 1 Steven R. Thorp, Ph.D., ABPP 2 Kathryn E. Williams, Ph.D. 3 1 VA San Diego Healthcare System, Center of Excellence for Stress and
VA Connects: Telemental Health Regional Center Martin P. Paulus, M.D. 1 Steven R. Thorp, Ph.D., ABPP 2 Kathryn E. Williams, Ph.D. 3 1 VA San Diego Healthcare System, Center of Excellence for Stress and
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
2016 Complex Case Management. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
Overview of Six Texas Demonstrations
 Texas Case Study: Document 2 Overview of Six Texas Demonstrations The chart below provides an overview of six Texas demonstrations. Where possible, the chart indicates the purpose of the demonstration,
Texas Case Study: Document 2 Overview of Six Texas Demonstrations The chart below provides an overview of six Texas demonstrations. Where possible, the chart indicates the purpose of the demonstration,
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs
 2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling
 Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Hot Spotter Report User Guide
 PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Exploring telehealth options for outreach services: CheckUP project
 Exploring telehealth options for outreach services: CheckUP project Dr Liam Caffery Centre for Online Health The University of Queensland Abbreviations ABF Activity-based Funding AHW Aboriginal Health
Exploring telehealth options for outreach services: CheckUP project Dr Liam Caffery Centre for Online Health The University of Queensland Abbreviations ABF Activity-based Funding AHW Aboriginal Health
The Career Path of a Chief Nursing Officer: The Impact of Nursing Leadership at the Veterans Health Administration Cathy Rick, RN PhD (h), NEA-BC,
, NEA-BC,") The Career Path of a Chief Nursing Officer: The Impact of Nursing Leadership at the Veterans Health Administration Cathy Rick, RN PhD (h), NEA-BC, FACHE, FAAN 1 Conflict of Interest Disclosure Cathy Rick,
The Career Path of a Chief Nursing Officer: The Impact of Nursing Leadership at the Veterans Health Administration Cathy Rick, RN PhD (h), NEA-BC, FACHE, FAAN 1 Conflict of Interest Disclosure Cathy Rick,
Chapter VII. Health Data Warehouse
 Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Integrated Mental Health Care. Questions
 Integrated Mental Health Care Closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Questions Due to the large number of participants, it is not practical to take questions over
Integrated Mental Health Care Closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Questions Due to the large number of participants, it is not practical to take questions over
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Alpert Medical School of Brown University Clinical Psychology Internship Training Program Rotation Description
 Rotation Title: Neuropsychology Track Neuropsychological Assessment Rotation Location: VA Medical Center Rotation Supervisor(s): Stephen Correia, Ph.D. (Primary Supervisor) Megan Spencer, Ph.D. Donald
Rotation Title: Neuropsychology Track Neuropsychological Assessment Rotation Location: VA Medical Center Rotation Supervisor(s): Stephen Correia, Ph.D. (Primary Supervisor) Megan Spencer, Ph.D. Donald
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Medical Management Program
 Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent Fraud, Waste and Abuse in its programs. The Molina
Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent Fraud, Waste and Abuse in its programs. The Molina
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018
 Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Access to Psychiatric Inpatient Care: Prolonged Waiting Periods in Medical Emergency Departments. Data Report for
 Access to Psychiatric Inpatient Care: Prolonged Waiting Periods in Medical Emergency Departments Data Report for 2012-2014 Prepared by: Jennifer D. Dudek, MPH 150 North 18 th Avenue, Suite 320 Phoenix,
Access to Psychiatric Inpatient Care: Prolonged Waiting Periods in Medical Emergency Departments Data Report for 2012-2014 Prepared by: Jennifer D. Dudek, MPH 150 North 18 th Avenue, Suite 320 Phoenix,
Telemedicine and Health Reform. Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center
 Telemedicine and Health Reform Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center 1 telehealthresourcecenters.org Links to all TRCs National Webinar Series Reimbursement,
Telemedicine and Health Reform Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center 1 telehealthresourcecenters.org Links to all TRCs National Webinar Series Reimbursement,
Section 7. Medical Management Program
 Section 7. Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent fraud, waste and abuse in its programs.
Section 7. Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent fraud, waste and abuse in its programs.
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring
 Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum. May 2015 avalere.com
 Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
MAGELLAN UNIVERSAL SERVICES LIST - Includes Preferred HIPAA Compliant Codes. UB-04 Revenue Codes
 Service Name & Detailed Magellan Description (see column heading explanations at end of this document) MAGELLAN UNIVERSAL SERVICES LIST - Includes Preferred HIPAA Compliant Codes Codes Used to Determine
Service Name & Detailed Magellan Description (see column heading explanations at end of this document) MAGELLAN UNIVERSAL SERVICES LIST - Includes Preferred HIPAA Compliant Codes Codes Used to Determine
Leveraging Your Facility s 5 Star Analysis to Improve Quality
 Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
What Counts in Mental Health and What We Are Counting? Our Performance Measures and Other Metrics
 What Counts in Mental Health and What We Are Counting? Our Performance Measures and Other Metrics Dan Kivlahan, PhD Acting National Mental Health Program Director, Addictive Disorders Katy Lysell, Psy.D.,
What Counts in Mental Health and What We Are Counting? Our Performance Measures and Other Metrics Dan Kivlahan, PhD Acting National Mental Health Program Director, Addictive Disorders Katy Lysell, Psy.D.,
Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care. Opportunity Statement
 to Improve Functional Outcomes and Reduce Readmissions and Burden of Care. Opportunity Statement") Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care Robert D. Rondinelli, MD, PhD Paulette Niewczyk, MPH, PhD AlphaFIM, FIM, SigmaFIM,
Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care Robert D. Rondinelli, MD, PhD Paulette Niewczyk, MPH, PhD AlphaFIM, FIM, SigmaFIM,
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
The Drive Towards Value Based Care
 The Drive Towards Value Based Care Thursday, March 3, 2016 Michael Aratow, MD, FACEP Chief Medical Information Officer, San Mateo Medical Center Gaurav Nagrath, MBA, Sr. Strategist, Population Health Research
The Drive Towards Value Based Care Thursday, March 3, 2016 Michael Aratow, MD, FACEP Chief Medical Information Officer, San Mateo Medical Center Gaurav Nagrath, MBA, Sr. Strategist, Population Health Research
Effectiveness of Health Coaching on Health Outcomes and Health Services Utilization and Costs
 Effectiveness of Health Coaching on Health Outcomes and Health Services Utilization and Costs BHAC Conference April 22, 2013 Mary Jo Kreitzer PhD, RN, FAAN Mary Jo Kreitzer, PhD Yvonne Jonk, PhD Karen
Effectiveness of Health Coaching on Health Outcomes and Health Services Utilization and Costs BHAC Conference April 22, 2013 Mary Jo Kreitzer PhD, RN, FAAN Mary Jo Kreitzer, PhD Yvonne Jonk, PhD Karen
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
In Arkansas 02/20/2014 1
 In Arkansas 02/20/2014 1 Procedures for Determination of Medical Need for Nursing Home Services I. Medical Need Assessments A. Nursing Facility Procedures B. OLTC Procedures II. Pre-Admission Screening
In Arkansas 02/20/2014 1 Procedures for Determination of Medical Need for Nursing Home Services I. Medical Need Assessments A. Nursing Facility Procedures B. OLTC Procedures II. Pre-Admission Screening
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
Evidence Tables and References 6.4 Discharge Planning Canadian Best Practice Recommendations for Stroke Care Update
 Evidence Tables and References 6.4 Discharge Planning Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Last Updated: June 21, 2013 Table of Contents Search Strategy... 2 What existing
Evidence Tables and References 6.4 Discharge Planning Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Last Updated: June 21, 2013 Table of Contents Search Strategy... 2 What existing
Program Evaluation of Veteran Outcomes and Project Implementation. Program Evaluation and Resource Center (PERC) Mental Health Operations
 Mental Health Operations") Program Evaluation of Veteran Outcomes and Project Implementation Program Evaluation and Resource Center (PERC) Mental Health Operations MAY 2014 Part 1: Monitoring Veteran Outcomes WHO: Veterans being
Program Evaluation of Veteran Outcomes and Project Implementation Program Evaluation and Resource Center (PERC) Mental Health Operations MAY 2014 Part 1: Monitoring Veteran Outcomes WHO: Veterans being
CMS-0044-P; Proposed Rule: Medicare and Medicaid Programs; Electronic Health Record Incentive Program Stage 2
 May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
Outcomes for Iowa Medicaid Chronic Condition Health Home Program Enrollees. Policy Report. SFYs February 2017
 Policy Report February 2017 Outcomes for Iowa Medicaid Chronic Condition Health Home Program Enrollees Ss 2012-2015 Elizabeth Momany Assistant Director, Health Policy Research Program* Associate Research
Policy Report February 2017 Outcomes for Iowa Medicaid Chronic Condition Health Home Program Enrollees Ss 2012-2015 Elizabeth Momany Assistant Director, Health Policy Research Program* Associate Research
Health Center Program Update
 Health Center Program Update NACHC Policy & Issues Forum March 14, 2018 Jim Macrae Associate Administrator, Bureau of Primary Health Care (BPHC) Health Resources and Services Administration (HRSA) 3/22/2018
Health Center Program Update NACHC Policy & Issues Forum March 14, 2018 Jim Macrae Associate Administrator, Bureau of Primary Health Care (BPHC) Health Resources and Services Administration (HRSA) 3/22/2018
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care
 Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Long-Stay Alternate Level of Care in Ontario Mental Health Beds
 Health System Reconfiguration Long-Stay Alternate Level of Care in Ontario Mental Health Beds PREPARED BY: Jerrica Little, BA John P. Hirdes, PhD FCAHS School of Public Health and Health Systems University
Health System Reconfiguration Long-Stay Alternate Level of Care in Ontario Mental Health Beds PREPARED BY: Jerrica Little, BA John P. Hirdes, PhD FCAHS School of Public Health and Health Systems University
2016 Mommy Steps Program Descriptions
 2016 Mommy Steps Program Descriptions Our mission is to improve the health and quality of life of our members Mommy Steps Program Descriptions I. Purpose Passport Health Plan (Passport) has developed approaches
2016 Mommy Steps Program Descriptions Our mission is to improve the health and quality of life of our members Mommy Steps Program Descriptions I. Purpose Passport Health Plan (Passport) has developed approaches
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill
 Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL
 HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
New York State Medicaid Value Based Payment: Data Driven Strategies. Bundled Payment Summit June 27, 2017
 New York State Medicaid Value Based Payment: Data Driven Strategies Bundled Payment Summit June 27, 2017 Panelists Moderator Paloma Hernandez Anthony Thompson Marc Berg President and CEO Urban Health Plan
New York State Medicaid Value Based Payment: Data Driven Strategies Bundled Payment Summit June 27, 2017 Panelists Moderator Paloma Hernandez Anthony Thompson Marc Berg President and CEO Urban Health Plan
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Ambulatory-care-sensitive admission rates: A key metric in evaluating health plan medicalmanagement effectiveness
 Milliman Prepared by: Kathryn Fitch, RN, MEd Principal, Healthcare Management Consultant Kosuke Iwasaki, FIAJ, MAAA Consulting Actuary Ambulatory-care-sensitive admission rates: A key metric in evaluating
Milliman Prepared by: Kathryn Fitch, RN, MEd Principal, Healthcare Management Consultant Kosuke Iwasaki, FIAJ, MAAA Consulting Actuary Ambulatory-care-sensitive admission rates: A key metric in evaluating
Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through Telemedicine
 PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
Legal 2000 The Nevada Process of Civil Commitment
 Legal 2000 The Nevada Process of Civil Commitment Some Proposed Amendments Lesley R. Dickson, M.D. President, Nevada Psychiatric Association June 17, 2008 LEGAL 2000 The Nevada Process of Civil Commitment
Legal 2000 The Nevada Process of Civil Commitment Some Proposed Amendments Lesley R. Dickson, M.D. President, Nevada Psychiatric Association June 17, 2008 LEGAL 2000 The Nevada Process of Civil Commitment
Understanding and Identifying Target Populations for Integrated Care
 Understanding and Identifying Target Populations for Integrated Care W.Wodchis, X.Camacho, I. Dhalla, A. Guttman, B.Lin, G.Anderson Leveraging the Culture of Performance Excellence in Ontario s Health
Understanding and Identifying Target Populations for Integrated Care W.Wodchis, X.Camacho, I. Dhalla, A. Guttman, B.Lin, G.Anderson Leveraging the Culture of Performance Excellence in Ontario s Health
SUMMARY OF THE STATE GRANT OPPORTUNITIES IN THE PATIENT PROTECTION AND AFFORDABLE CARE ACT: H.R (May 24, 2010)
") National Conference of State Legislatures 444 North Capitol Street, N.W., Suite 515 Washington, D.C. 20001 SUMMARY OF THE STATE GRANT OPPORTUNITIES IN THE PATIENT PROTECTION AND AFFORDABLE CARE ACT: H.R.
National Conference of State Legislatures 444 North Capitol Street, N.W., Suite 515 Washington, D.C. 20001 SUMMARY OF THE STATE GRANT OPPORTUNITIES IN THE PATIENT PROTECTION AND AFFORDABLE CARE ACT: H.R.