3 rd Quarter MSHO/MSC+ Care Coordination Training
|
|
|
- Alaina Atkins
- 5 years ago
- Views:
Transcription

1 3 rd Quarter MSHO/MSC+ Care Coordination Training Internal Care Coordinators & Care Systems: September 21 st, 2016 Recorded WebEx: September 28 th, 2016
2 Agenda Welcome/Introductions American Cancer Society-Bobbi Jo Glood/Jennifer Andersen STARS-Cindy Radke Model of Care-Bobbi Jo Glood/Jennifer Andersen PCA/EW Updates-Esther Versalles-Hester Care Coordination Update-Bobbi Jo Glood/Jennifer Andersen Silver Sneakers-refer to the posted WebEx on the UCare website.
3 Stars September, 2016



4 Medication Adherence Helps numerous Star measures *Blood Pressure Control *Diabetes Care Blood Sugar Control *Part D Medication Adherence for Cholesterol *Plan all cause readmissions
5 Interventions Late to refill letters sent August. August newsletter article. Work with members to identify reasons for non adherence.
6 Part C logs Continue to see assessment dates prior to date converted to MSHO. Remember to do product changes!!!! First year we can count refusals and unable to reach as long as completed within designated timeframes. Data validation in be prepared when file requests happen!
7 Other Star Measures? Care of Older Adult MSHO only measures Functional status assessment Pain Screening Medication Review Requests for data occur during HEDIS season beginning of Requests for HRA assessments- Care Plans- Any ability to pull medication reviews from EMR systems. Will be presenting more on these measures in December meeting and introduce our Quality Manager for HEDIS Chelsey!
8 Parting remarks Continue to work with MSHO members to close gaps in care. Work hard to close gaps before the end of the year! What can UCare do to assist? Remember the incentives offered!
9 Cancer Prevention and Early Detection Angie Rolle State Health Systems Sr Director American Cancer Society
10 Overview of Presentation Tobacco Cessation Cancer Screening Breast Cervical Colorectal 10
11 Tobacco Use is linked to 1 in 3 cancer deaths 90 percent of all lung cancers Increased risk of 14 other cancers including breast, cervical and colon 11
12 When talking to a smoker Talk about health benefits of quitting, especially immediate impact Consider the cost argument, cigarettes are not cheap Acknowledge that it is hard to quit but offer support and be patient with them 12
13 Immediate benefits of quitting 20 minutes after quitting Your heart rate and blood pressure drop. 12 hours after quitting The carbon monoxide level in your blood drops to normal. 2 weeks to 3 months after quitting Your circulation improves and your lung function increases. 13
14 Mid-term Benefits 1 year after quitting The excess risk of coronary heart disease is half that of a continuing smoker's. 2-5 years after quitting Stroke risk can fall to that of a non-smoker 5 years after quitting Risk of cancer of the mouth, throat, esophagus, and bladder are cut in half. Cervical cancer risk falls to that of a nonsmoker. 14
15 Long term benefits of quitting 10 years after quitting The risk of dying from lung cancer is about half that of a person who is still smoking. The risk of cancer of the larynx and pancreas decreases. 15 years after quitting The risk of coronary heart disease is that of a non-smoker's. 15
16 Consider the cost We all know that smoking causes a range of health problems, but have you thought about how it affects your wallet? Cigarettes and/or tobacco breath mints and cough drops cleaning expenses clothes, home, and car. Long term costs of doctor visits 16
17 Advice: Make a Plan Pick the date and mark it on your calendar. Tell friends/family about your quit day. Stock up on oral substitutes sugarless gum, carrot sticks, or hard candy. Think back to your past attempts to quit. Try to figure out what worked and what didn t work for you. 17
18 Ucare Quitline UCare members can get free help to quit smoking or chewing tobacco with the tobacco quit line. Counselors at the tobacco quit line are there to help Ucare members kick the habit. Nicotine patches, gum, or lozenges are also available to eligible UCare members at no charge when they call the tobacco quit line. Call the tobacco quit line at TTY/hearing impaired: The tobacco quit line hours are 7 a.m. to 10 p.m., Monday through Friday, and 10 a.m. to 4 p.m. on Saturdays. 18
19 Cancer Screening Benefits Screening offers the opportunity to detect cancers before symptoms appear Earlier stages are often more treatable Some cancer screenings can find problems before they become cancer 19
20 Cancer Screening Recommendations Breast, cervical and colon tests have broad support as cancer screenings Lung cancer screening is recommended for a small group of former smokers The value of current prostate cancer tests is a matter of debate 20


21 21
22 Breast Cancer and Age Nearly 8 out of 10 breast cancers occur in women older than age 50 A woman who is 70 is almost twice as likely to develop breast cancer in the next year as a woman who is
23 Breast Cancer and Family History Your risk is greater if a close relative has had breast cancer But only 20-30% of women with breast cancer have a family member with this disease. 23

24 24
25 Breast screening saves lives Over 98% of women diagnosed with breast cancer in localized stage were alive 5 years later Mammography screening can help women detect breast cancer in this early stage 25
26 Colon Screening 90% of men and women diagnosed with localized colon cancer are alive 5 years later Less than half of colon cancers are diagnosed in this early, more treatable stage 26

27 Why Test? There are two aims of testing: 1. Prevention Find and remove polyps to prevent cancer 2. Early Detection Find cancer in the early stages, when best chance for a cure
28 Benefits of Early Detection Survival Rates by Disease Stage* 5-yr Survival % 70.4% 12.5% Local Regional Distant Stage of Detection
29 Decrease in Incidence Decline due to: Screening polyp removal prevention Recent study estimates that screening has prevented approximately 550,000 cases of colorectal cancer in the US over the past three decades

30 Colonoscopy
31 Colonoscopy Limitations Greater patient requirements for successful completion Requires a bowel prep and facility visit, and often a preprocedure specialty office visit Access Limited by insurance status, local resources Patient preference Many individuals don t want an invasive test or a test that requires a bowel prep 31

32 What about stool tests?
33 Stool Test Types A) Tests that detect blood (Fecal Occult Blood Tests) Recommended by ACS, USPSTF and all major screening guidelines Two types (but multiple brands, variable performance) Guaiac based FOBT Immunochemical (FIT) B) Tests that detect aberrant DNA One test (Cologuard) available in U.S. Combines DNA mutation test with FIT Recently added to USPTF recommendations

34 Guaiac Tests Specific for human blood and for lower GI bleeding Results not influenced by foods or medications Some types require only 1 or 2 stool specimens Higher sensitivity than older forms of guaiac based FOBT Costs more than guaiac tests (but higher reimbursement)


35 Fecal Immunochemical Tests (FIT) Specific for human blood and for lower GI bleeding Results not influenced by foods or medications Some types require only 1 or 2 stool specimens Higher sensitivity than older forms of guaiac based FOBT Costs more than guaiac tests (but higher reimbursement)
36 Advantages of stool tests Less expensive No bowel preparation. Done in privacy at home. No need for time off work or assistance getting home after the procedure. Non invasive no risk of pain, bleeding, perforation Limits need for colonoscopies required only if stool blood testing is abnormal. 36
37 Inadomi, Arch Intern Med 2012 Patient Preferences
38 Many patients prefer stool tests Diverse sample of 323 adults given detailed side by side description of FOBT and colonoscopy (DeBourcy et al. 2007) 53% preferred FOBT Almost half felt very strongly about their preference 212 patients at 4 health centers rated different screening options with different attributes (Hawley et al. 2008) 37% preferred colonoscopy 31% preferred FOBT Nationally representative sample of 2068 VA patients given brief descriptions of each screening mode (Powell et al. 2009) 37% preferred colonoscopy 29% preferred FOBT
. Provides state-of-the-science information about guaiac and immunochemical FOBT, test performance and characteristics of high quality screening programs. Available at www.cancer.")
39 High Quality Stool Testing Clinicians Reference: FOBT One page document designed to educate clinicians about important elements of colorectal cancer screening using fecal occult blood tests (FOBT). Provides state-of-the-science information about guaiac and immunochemical FOBT, test performance and characteristics of high quality screening programs. Available at
40 Encourage Members to Talk to their doctor I m over 50, how soon can I get tested for colon cancer? I understand that there is more than one type of test for colon cancer. Should I consider a stool test? Is there a particular stool test that you would recommend?

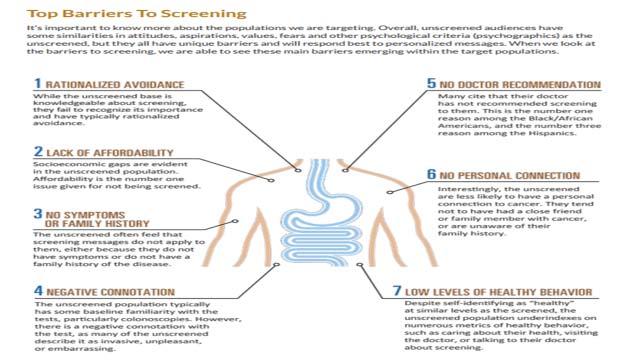
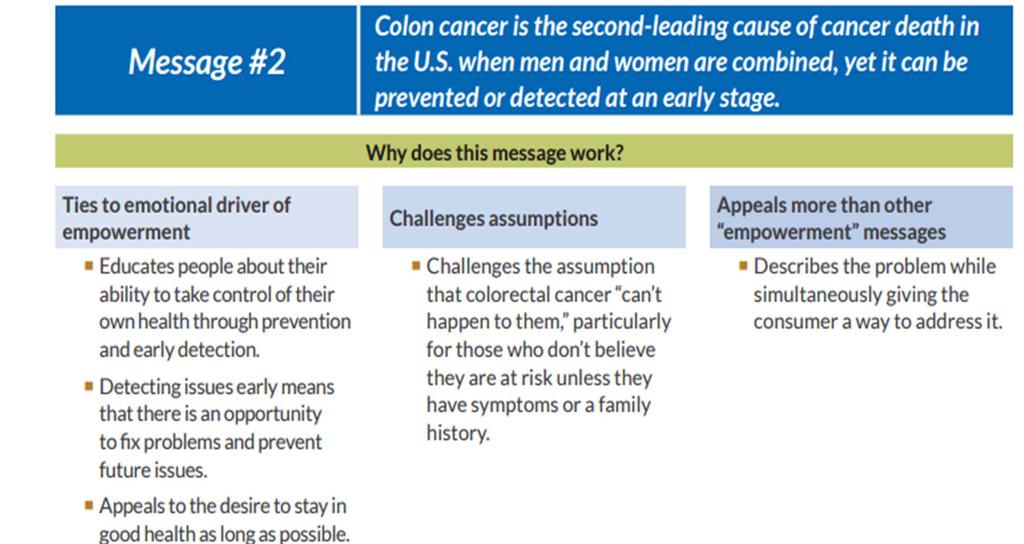
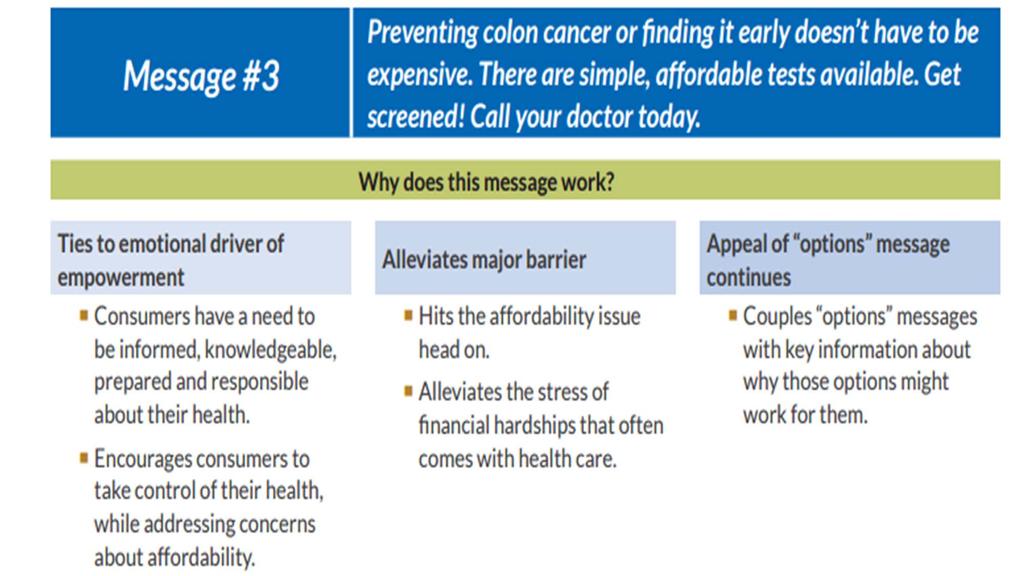
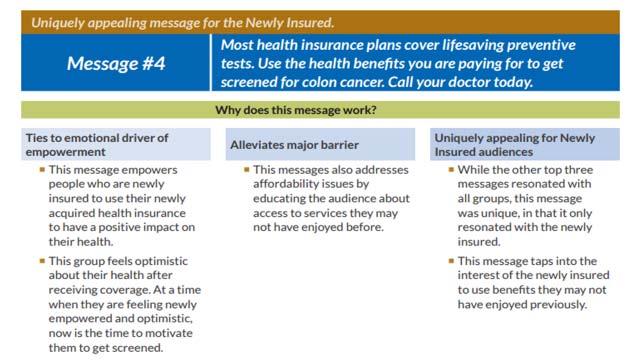
41 Effective Messaging
42


43
44
45
46

47
48 When someone receives a cancer diagnosis they often have questions.
49 How can ACS help? Phone help: On the internet: Information Emotional Support Day-to-Day Help
50

51 Hope Lodge

52 Road To Recovery
53 UCare MSHO Model of Care 2016

54 UCare MSHO Model of Care Overall goal of the MOC: Drive improvements in health outcomes and quality of life for members. UCare s MOC is designed to: Increase access to affordable, cost-effective health care. Improve coordination of care. Ensure seamless transitions of care. Manage costs.
55 UCare s SNP Population MSHO serves over 10,000 special needs dual eligibles The majority (70%) are women. 31% are minorities. 82% live in the community, 18% are institutionalized. >1 out of 3 members has 2-4 chronic conditions. >1 in 10 has 10+ chronic conditions. Top five most frequent health issues are: Hypertension (77%). Disorders of Lipid Metabolism (51%). Rheumatoid Arthritis /Osteoarthritis (44%). Diabetes (40%). Depression (37%).




56 UCare Care Coordination Care Coordination is the cornerstone of the MSHO Care Model. All MSHO members receive care coordination. Integrates Medicaid and Medicare services Includes MLTSS services. Care Coordinators are Qualified Professionals RNs and SWs. Coordinate member services, act as central point of contact.
57 UCare Care Coordination Care coordination consists of: Face to face Health Risk Assessment (HRA) Initially, annually, or if there is a change in condition. Development of an Individualized Care Plan (ICP) Ongoing coordination of full range of Medical services Behavioral health services Managed Long Term Supports and Services (MLTSS). Facilitation of communication (member, family, Interdisciplinary Care Team ICT). Care transition management.
58 Tailored Benefits and Services Extra benefits and services to promote healthy lifestyle, preventive care, safety. Health promotion programs (fitness, mammogram incentive, smoking cessation, UCare 24/7 Nurse Advice Line). Comprehensive medication reviews. Culturally competent staff Bilingual associate care managers, care coordinators, Customer Service reps, county and care system liaisons, providers. Care coordinators hired internally or contracted through counties, care systems, agencies. UCare model favors local level care coordination.



59 Provider Network Provider network meets the comprehensive needs of our members, including: 13,000+ primary care physicians. 15,000+ specialists. 9,800+ primary and specialty clinics dental providers. Critical access hospitals, geriatric services and nursing homes, DME, behavioral health, lab and X-ray, open access network. No referral required to contracted providers. Use DHS Tier 1 providers for MLTSS. Clinical practice guidelines available to providers. Model of Care training offered annually. Face to face or WebEx.


60 Quality Measurement & Performance Improvement UCare collects and analyzes data and reports from a variety of sources to: Evaluate the Model of Care. Identify improvements. Monitor and measure health outcomes.
61 UCare MOC Performance Goals Goal and Performance Measure Areas: Provider access. Member satisfaction. Care coordination HRA and care plan goals. Transition of care, preventive care, quality of health. HEDIS and Star measures : Breast cancer and colon cancer screening. Routine diabetic care. Depression medication adherence.
62 Data Sources for MOC Review UCare collects and analyzes data and reports from a variety of sources to evaluate the Model of Care and identify improvements based on these outcomes: Provider Geo Access survey. CMS Stars and HEDIS. Care coordination surveys. Analysis of enrollment and CC assignment data. Care plan and care transition audits. Clinical practice guideline claims review. MOC training for providers and CCs. Complaint reporting related to care coordination. Other data and ad hoc reporting.



63 Model of Care Challenges Member demographics present significant challenges: Age. Geographic location. Lack of integration of Medicare & Medicaid Services. Ethnicity, language barriers and cultural beliefs (many are immigrants). Lack of general and specialized transportation. Difficulty obtaining dental services. Vision and hearing impairments.
64 Challenges, cont. Multiple diseases and comorbidities. High medication use and side effects. Mental health and cognitive problems. Need for caregiver/caregiver support. End of life care needs. Low socioeconomic status combined with poor health literacy. Lack of provider engagement with care coordinator. Difficulty in getting providers to order tests or procedures that meet quality and Stars measures. Lack of available MLTSS providers.


65 How UCare Meets Challenges Extra benefits and services Medical and EW transportation Strong and Stable Kit, Silver Sneakers, Health Promotion Incentives. Interpreter services, bilingual staff. 24 hour Nurse Line. Culturally specific transportation when able. MLTSS. Caregiver training. Preventive care screening reminders. Align members with community resources. Mobile Dental Unit





66 MLTSS Services MLTSS Services designed to help members live independently: EW transportation. Homemaking. Meals on Wheels. PERS. ADC. Customized Living. Relocation services. PCA.
67 Clinical Liaison Staff to Meet Member Needs Works with Hmong members with complex medical/mental conditions, provides education to Hmong community- mbrs. and families. Diverse UCare staff Customer Service, and care coordination staff from diverse backgrounds. Somali, Hmong, Hispanic interpreters. Community support- community health workers, community sponsorships.
68 Member Outreach Efforts Call campaigns for preventive care Colon and breast cancer screening. Mobile Mammography. In-home osteoporosis screening. Diabetes care. Health coach calls for gaps in care. Partnership with WellShare International that started April 2016


 Collaboration on audit")
69 Collaboration With Other Health Plans Collaborative Care Plan Transition of Care Process and Logs PIPs Depression Medication Adherence Work on assessment processes (MnCHOICES) Collaboration on audit processes and forms.


70 Successes Continual shift to community living. High levels of satisfaction with care coordination. Successful outreach for preventive care.
71 Shift to Community Living Community 73% 77% 80% 82% Institutional 27% 23% 20% 18%


72 Member Satisfaction with Care Coordination 97% are satisfied with their CC. 89% know who there CC is and how to contact them. 93% state their CC is respectful to them and their needs. 72% depend on their CC to assist with their health care needs. 89% Feel their CC has helped them maintain or improve their overall health. 85% feel their CC makes it easier for them to get care or services to remain safely at home.
73 Success With Member Outreach 100+ women received mammograms in last 18 months through local events. Increase in women receiving mammogram incentive vouchers. 278 in in in members returned colon cancer screening kits.
74 Summary Care Coordination is foundation of care model. UCare offers benefits and services designed to meet unique member needs. UCare meets challenges through innovative services, partnerships. Many successes.
75 PCA and EW Updates Presented by: Esther Versalles-Hester
76 PCA Updates UCare continues to engage Care System case managers with transition of the PCA assessment process. In the process of developing guidance and criteria to ensure compliance with DHS requirements. Due to delays with CFSS and MnCHOICE implementation, MCO s are engaging DHS in conversations regarding the current PCA process and expectations. DHS will be gathering data on the PCA assessment outcome for CFSS readiness.
77 Provider contract termination UCare notifies the assigned care system via authorization report in order for the case manager to assist in the transition process. It is vital that the report is processed expeditiously to avoid service interruption. CM s are reminded to contact the member or the RP to assist in securing a new provider. This includes EW services as well. UCare ends the current authorization on the provider contract term date and notifies the member via US mail.
78 EW Reminders All EW services require authorization for claims payment purpose. Please submit DTR s timely. UCare is required to provide an advance 14 day notice to the member and the provider of service reduction termination or denial. Please use current version (revised 5/2016) of the WSAF that includes drop down box for specific services. Verify provider NPI/UMPI and fax number prior to WSAF submission. UCare has received calls from the provider that the fax number listed on the WSAF is incorrect. Homemaker services that exceed greater than 5 hrs a week require care system supervisor approval. With the exception of PCA and Chore services, homemaking does not have flexible use and must be based on member plan of care and need not want. Change of EW providers. Please notify UCare via the WSAF when a member switches from one EW provider to another.
79 DME services covered under EW Case managers must ensure and document in the community support plan before purchase of the equipment or supply that the item meets all of the following criteria: Cannot be funded through any other source. If an item is never covered by MA, it is not necessary to seek a written denial from MA. If an item may be covered by MA, the medical supplier must seek authorization from UCare before seeking authorization of coverage under the EW program Specified in a community support plan as necessary to avoid institutionalization Meant for the sole use of the recipient Either medically necessary (appropriate and effective for the medical needs and health and safety of the recipient); or remedially necessary (appropriate to assist a recipient in increased independence and integration in their environment or community) Appropriate and effective for the medical needs, diagnosis, and condition of the recipient Of an acceptable quality Timely (that is, the accommodation is provided at the time it is needed) The most cost-effective health service available to meet the medical needs of the recipient An effective and appropriate use of MA waiver funds Cannot be funded through any other source.
80 EW Approval Reminders Example: Wheelchairs, Walkers, Lift Chairs, Canes, Hospital Beds. Most DME are covered benefits under Medicare and Medicaid and may require a physicians order. However, under the medical benefit, DME under $500 does not require an authorization from UCare. CM must exhaust all other payer sources i.e. Medicare or MA benefits prior to approving under the EW benefit. UCare has recently experienced issues with DME items that meet Medicare/MA criteria for which the CM is approving under EW. Questions on whether an item meets Medicare or Medicaid criteria can be submitted to the clinical services liaison for assistance.
81 Questions???? Please contact the Clinical Liaison at Or Esther Versalles-Hester at or
82 Care Coordination Updates Bobbi Jo Glood and Jennifer Andersen


83 Advanced Directives The CC must document on an annual basis that they addressed or discussed advance directives with the member. If an advance directive was not discussed, document the reason.
84 Advance Directives resource Fairview Health Services is a partner with Honoring Choices Minnesota, which brings health care systems together to promote the benefits of advance care planning. You can find Health Care Directives written in Hmong, Somali, Russian, and Spanish Website: mmitment/involvement/honoringchoices/index.h tm


85 UCare Mobile Dental Clinic The UCare Mobile Dental Clinic is returning to Minnesota roads this fall to serve eligible UCare members with preventive dental coverage. After a seven-month hiatus, the wheel-chair accessible clinic will be back in action beginning Aug. 29 in Roseville, Minn. It will offer care in 2016 at five Twin Cities metro area sites and also visit four sites in Greater Minnesota (here s the 2016 schedule). The 2017 service schedule will be available later this year.


86 Updated Requirements Grids For MSHO and MSC+: Updated as of to reflect changes related to Person Centered Planning and the addition of the Transitional Health Risk Assessment Form. Changes are highlighted in yellow.
87 My Move Plan Summary To help with the process of moving, DHS created the My Move Plan Summary, DHS-3936 to support MSHO and MSC+ members. This only applies to members who are open to EW. Requirements The Person-Centered, Informed Choice and Transition Protocol (PDF) requires care coordinators and support planners, to work together with the member who is moving to create this summary. If a member indicates Prefer to live somewhere else, or Don t know on question E.13 of the DHS-3428/LTCC, the care coordinator is required to complete the My Move Plan Summary document. Care Coordinator roles and responsibilities When using the My Move Plan Summary, the care coordinator should: Initiate the document s creation Build and share the summary with the member Inform the member about the process, including any changes to the plan Refer to the document throughout the move Update the document when it needs modification or changes Sign and keep a copy of the completed document in the member s file. This document can be found on the DHS edocs website.
88 DHS Bulletin-Comprehensive Policy on EW residential services This bulletin has been re-issued to include Person Centered Planning, new CL rates and the monthly-to-daily rate. There are no new policies. This bulletin can be found on the DHS website
89 Updated DHS forms DHS has updated the following forms and they can be located on the edocs website. LTC Screening Document-DHS-3427 LTCC assessment form-dhs-3428 Please download and use the new versions.
90 Updated MMIS manuals DHS has updated the following MMIS manuals as of July 2016, please begin to refer to the new manuals and destroy any old copies. DHS-4625: The Instructions for Completing and Entering the LTCC Screening Document and Service Agreement into MMIS DHS-5020A: The Instructions for Completing and Entering the LTCC Screening Document into MMIS for the SNBC Program DHS-4669: The Instructions for Completing and Entering the LTCC Screening Document into MMIS for the MSHO and MSC+ Programs
91 Access & Password reset requests for MMIS Please begin to send your access and password reset requests to Bobbi Jo Glood & Jennifer Andersen via the .
92 DHS Best Practice Care Coordination Learning Day This Learning Day is Thursday, Sept. 29, from 8 a.m. to 4:30 p.m. at the Radisson Blu-Mall of America. You can either attend it in person or view it via Webinar. The event informs MSHO, MSC+ and SNBC care coordinators about new care coordination requirements and strategies for effective care coordination. Registration will open Aug. 17, 2016, and can be completed on the DHS website. During the registration process, you will be prompted to choose between on-site attendance or participation via Webinar.
93 Tidbits & Reminders Change in Care Coordination Delegate and Waiver Service Approval Forms We have learned that we have been receiving requests on our UCare Waiver Service Approval Form to end authorizations due to a change in care coordination delegate. Please note that we do not end authorizations due to this type of change. Authorizations will remain in place to avoid claim denials. If you have questions, please contact clinicalliaison@ucare.org. Part C Logs MSHO/MSC+ care coordinators are reminded that Part C logs are due on or before the 10 th of every month for the previous month s activity. If the 10 th of the month falls on a weekend, it is preferred that you submit your logs before the 10 th. All Excel spreadsheets must be ed to UCare at assessmentreporting@ucare.org care coordination satisfaction survey Thanks to all care coordinators who completed the annual UCare Care Coordination Satisfaction Survey! Your feedback helps us identify areas in which we can improve our current processes. We will be presenting the findings at the December quarterly


 Tool questions DHS has a new email address for RS")
94 Tidbits & Reminders continued DHS-LTCC and Collaborative Care Plan Training If you were unable to attend the LTCC and Collaborative Care Plan Training on June 23, 2016, DHS has archived this training for viewing at a later date. This training provides valuable information on the updated LTCC and Collaborative Care Plan that became effective July 1, New DHS address for Residential Services (RS) Tool questions DHS has a new address for RS Tool questions, EWRShelp@state.mn.us. Please use this address rather than ing individuals at DHS directly to ensure that your questions are answered promptly.
95 Silver Sneakers
3 rd Quarter MSHO/MSC+ Care Coordination Training
 3 rd Quarter MSHO/MSC+ Care Coordination Training Care Systems & UCare Care Coordinators: September 13 th, 2017 Recorded WebEx: September 14 th, 2017 Agenda STARS Cindy Radke Bus Pass Transportation Jeremy
3 rd Quarter MSHO/MSC+ Care Coordination Training Care Systems & UCare Care Coordinators: September 13 th, 2017 Recorded WebEx: September 14 th, 2017 Agenda STARS Cindy Radke Bus Pass Transportation Jeremy
All related UCare forms can be found, HERE, all DHS forms can be found HERE, all DHS Bulletins can be found HERE.
 Minnesota Senior Health Options (MSHO) Care Coordination (CC) and Minnesota Senior Care Plus (MSC+) Community Case Management (CM) Requirements Updated 1.1.18 All Minnesota Senior Health Options (MSHO)
Minnesota Senior Health Options (MSHO) Care Coordination (CC) and Minnesota Senior Care Plus (MSC+) Community Case Management (CM) Requirements Updated 1.1.18 All Minnesota Senior Health Options (MSHO)
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
1 st Quarter MSHO/MSC+ Care Coordination Training March 13 th -Care Systems and Internal Care Coordinators March 14 th -Recorded WebEx
 1 st Quarter MSHO/MSC+ Care Coordination Training 2018 March 13 th -Care Systems and Internal Care Coordinators March 14 th -Recorded WebEx Agenda CAHPS Survey Emily Eckhoff Behavioral Health Malanie Blanchard
1 st Quarter MSHO/MSC+ Care Coordination Training 2018 March 13 th -Care Systems and Internal Care Coordinators March 14 th -Recorded WebEx Agenda CAHPS Survey Emily Eckhoff Behavioral Health Malanie Blanchard
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
At EmblemHealth, we believe in helping people stay healthy, get well and live better.
 At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
Special Needs Program Training. Quality Management Department
 10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
1. What is your ethnic origin? (Check one) 2. What is your gender? 3. What is your age? Page 1. nmlkj. nmlkj. nmlkj. nmlkj. nmlkj. nmlkj. nmlkj.
 2. What is your gender? 3. What is your age? Page 1. nmlkj. nmlkj. nmlkj. nmlkj. nmlkj. nmlkj. nmlkj.") 1. What is your ethnic origin? (Check one) White Asian/Pacfic Island American Indian Black Hispanic 2. What is your gender? Female Male 3. What is your age? 18 to 24 55 to 64 25 to 34 65 to 74 35 to 44
1. What is your ethnic origin? (Check one) White Asian/Pacfic Island American Indian Black Hispanic 2. What is your gender? Female Male 3. What is your age? 18 to 24 55 to 64 25 to 34 65 to 74 35 to 44
MCS Model of Care For Special Needs Plans (SNP) Annual training for delegated entities and facilities
 Annual training for delegated entities and facilities") 2018 MCS Model of Care For Special Needs Plans (SNP) Annual training for delegated entities and facilities Quality Department CAN_2790318S CMS Requirements The Centers of Medicare & Medicaid Services (CMS)
2018 MCS Model of Care For Special Needs Plans (SNP) Annual training for delegated entities and facilities Quality Department CAN_2790318S CMS Requirements The Centers of Medicare & Medicaid Services (CMS)
UCare Connect + Medicare Care Coordination Requirement Grid Updated
 UCare Connect + Medicare Care Coordination Requirement Grid Updated 1.1.18 The assigned Care Coordinator (CC) must meet the required definition of a qualified professional. Care coordination services incorporate
UCare Connect + Medicare Care Coordination Requirement Grid Updated 1.1.18 The assigned Care Coordinator (CC) must meet the required definition of a qualified professional. Care coordination services incorporate
HouseCalls Objectives
 Overview Agenda Overview Objectives Background Case studies Member Experience Primary Care Provider Experience Referrals and Follow-up Influence on Centers for Medicare & Medicaid Services (CMS) Star Ratings
Overview Agenda Overview Objectives Background Case studies Member Experience Primary Care Provider Experience Referrals and Follow-up Influence on Centers for Medicare & Medicaid Services (CMS) Star Ratings
CareMore Special Needs Plans Model of Care. Annual Evaluation 2015 Performance
 CareMore Special Needs Plans Model of Care Annual Evaluation 2015 Performance The Special Needs Plans (SNPs) Medicare SNPs are a type of Medicare Advantage Plan (like an HMO or PPO). Medicare SNPs limit
CareMore Special Needs Plans Model of Care Annual Evaluation 2015 Performance The Special Needs Plans (SNPs) Medicare SNPs are a type of Medicare Advantage Plan (like an HMO or PPO). Medicare SNPs limit
Model of Care Scoring Guidelines CY October 8, 2015
 Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
OneCare Model of Care
 OneCare Model of Care Note: Content of this course was current at the time it was published. As Medicare policy changes frequently, check with your immediate supervisor regarding recent updates. 2018 Learning
OneCare Model of Care Note: Content of this course was current at the time it was published. As Medicare policy changes frequently, check with your immediate supervisor regarding recent updates. 2018 Learning
QUALITY IMPROVEMENT PROGRAM
 QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
2015 Quality Improvement Work Plan Summary
 2015 Quality Improvement Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how
2015 Quality Improvement Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how
2018 PROVIDER TOOLKIT
 1100 Circle 75 Parkway Suite 1100 Atlanta, GA 30339 2018 PROVIDER TOOLKIT Understanding the Centers for Medicare and Medicaid (CMS) Stars Rating System What is CMS Quality Star Ratings program? CMS evaluates
1100 Circle 75 Parkway Suite 1100 Atlanta, GA 30339 2018 PROVIDER TOOLKIT Understanding the Centers for Medicare and Medicaid (CMS) Stars Rating System What is CMS Quality Star Ratings program? CMS evaluates
(Referred to as the Care Plan Data Collection Guide in the DHS Triennial Compliance Assessment (TCA) conducted by the Minnesota Department of Health)
 conducted by the Minnesota Department of Health)") Minnesota Department of Human Services Managed Care (MSHO MSC+) Elderly Waiver Care Planning Audit (as required under 7.1.4.D., 7.8.3, 9.3.7 of the 2016 MSHO/MSC+ contract) 2017 Audit Protocol (Final 7.17.2017)
Minnesota Department of Human Services Managed Care (MSHO MSC+) Elderly Waiver Care Planning Audit (as required under 7.1.4.D., 7.8.3, 9.3.7 of the 2016 MSHO/MSC+ contract) 2017 Audit Protocol (Final 7.17.2017)
2013 MSHO Model of Care Training
 2013 MSHO Model of Care Training 1 MSHO Model of Care Training - Overview MSHO Overview Model of Care Definition Model of Care Training Requirement Model of Care Components Measurable Goals Staff Structure
2013 MSHO Model of Care Training 1 MSHO Model of Care Training - Overview MSHO Overview Model of Care Definition Model of Care Training Requirement Model of Care Components Measurable Goals Staff Structure
Passport Advantage (HMO SNP) Model of Care Training (Providers)
 Model of Care Training (Providers)") Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Your health comes first
 Your health comes first Here are the many ways we re working to ensure the quality of your care At Amerigroup, our focus is on you. We want to help you get and stay healthy. That s why we have many programs
Your health comes first Here are the many ways we re working to ensure the quality of your care At Amerigroup, our focus is on you. We want to help you get and stay healthy. That s why we have many programs
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plan Model of Care Chinese Community Health Plan
 Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
INSTRUCTIONS FOR INSPIRE (SNBC) CARE PLAN
 CARE PLAN") INSTRUCTIONS FOR INSPIRE (SNBC) CARE PLAN INFORMATION ABOUT ME 1. Name: Enter member s name. 2. My DOB: Enter member s date of birth. 3. Health Plan ID Number: Enter member s HealthPartners Member ID number.
INSTRUCTIONS FOR INSPIRE (SNBC) CARE PLAN INFORMATION ABOUT ME 1. Name: Enter member s name. 2. My DOB: Enter member s date of birth. 3. Health Plan ID Number: Enter member s HealthPartners Member ID number.
Wellness Guide for LCRA Retirees
 2016 Wellness Guide for LCRA Retirees Contents 2 How the EmPOWER program works 3 How to register 3 Text message reminders 4 Member health assessment 4 Biometric screening 5 Earning points and saving money
2016 Wellness Guide for LCRA Retirees Contents 2 How the EmPOWER program works 3 How to register 3 Text message reminders 4 Member health assessment 4 Biometric screening 5 Earning points and saving money
Welcome to BCHC Your Medical Home
 START HERE 1 Welcome to BCHC Your Medical Home Thank you for choosing Berks Community Health Center (BCHC) as your medical home. This booklet gives you information about being a patient at BCHC and what
START HERE 1 Welcome to BCHC Your Medical Home Thank you for choosing Berks Community Health Center (BCHC) as your medical home. This booklet gives you information about being a patient at BCHC and what
Quality Program Transparency and Accountability Report
 Quality Program Transparency and Accountability Report Compiled and submitted by Chelsey Doepner Quality Improvement Specialist cdoepner@ucare.org 612-294-5674 September 1, 2015 2015 Quality Program Transparency
Quality Program Transparency and Accountability Report Compiled and submitted by Chelsey Doepner Quality Improvement Specialist cdoepner@ucare.org 612-294-5674 September 1, 2015 2015 Quality Program Transparency
Passport Advantage Provider Manual Section 8.0 Quality Improvement
 Passport Advantage Provider Manual Section 8.0 Quality Improvement Table of Contents 8.1 Quality Improvement Program 8.2 Clinical Practice Guidelines 8.3 Star s 8.4 Quality of Care Concerns 8.3 Practitioner
Passport Advantage Provider Manual Section 8.0 Quality Improvement Table of Contents 8.1 Quality Improvement Program 8.2 Clinical Practice Guidelines 8.3 Star s 8.4 Quality of Care Concerns 8.3 Practitioner
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Asthma Disease Management Program
 Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
SPECIAL NEEDS PLAN. Model of Care Training
 SPECIAL NEEDS PLAN Model of Care Training WHAT IS A SNP? The Medicare Modernization Act of 2003 established Special Needs Plans (SNP). Centers Plan for Healthy Living (CPHL) participates in two types of
SPECIAL NEEDS PLAN Model of Care Training WHAT IS A SNP? The Medicare Modernization Act of 2003 established Special Needs Plans (SNP). Centers Plan for Healthy Living (CPHL) participates in two types of
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
P. R. E. P. Prevention Reward Employee Program. Tolleson Union High School District Plan Document
 P. R. E. P. Prevention Reward Employee Program Tolleson Union High School District Plan Document 2013-2014 ii Table of Contents Table of Contents 1 Welcome to P.R.E.P. 1 Program Overview. 2 Eligibility.
P. R. E. P. Prevention Reward Employee Program Tolleson Union High School District Plan Document 2013-2014 ii Table of Contents Table of Contents 1 Welcome to P.R.E.P. 1 Program Overview. 2 Eligibility.
From Fragmentation to Integration: Bringing Medical Care and HCBS Together. Jessica Briefer French Senior Research Scientist
 From Fragmentation to Integration: Bringing Medical Care and HCBS Together Jessica Briefer French Senior Research Scientist 1 Integration: The Holy Grail? An act or instance of combining into an integral
From Fragmentation to Integration: Bringing Medical Care and HCBS Together Jessica Briefer French Senior Research Scientist 1 Integration: The Holy Grail? An act or instance of combining into an integral
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare
 Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Frequently Asked Questions: HEDIS Clinical Quality Validation (Previously named HEDIS Attestations)
") December 2017 Frequently Asked Questions: HEDIS Clinical Quality Validation (Previously named HEDIS Attestations) HEDIS and Medicare Stars: A Florida Blue Health Care Quality Program 1. What is HEDIS?
December 2017 Frequently Asked Questions: HEDIS Clinical Quality Validation (Previously named HEDIS Attestations) HEDIS and Medicare Stars: A Florida Blue Health Care Quality Program 1. What is HEDIS?
Best Practices. SNP Alliance. October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees
 SNP Alliance Best Practices October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees Commonwealth Care Alliance is a Massachusetts-based non-profit,
SNP Alliance Best Practices October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees Commonwealth Care Alliance is a Massachusetts-based non-profit,
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
Elderly Waiver/Alternative Care Programs. Lisa Rotegard Manager Aging and Adult Services MN Department of Human Services
 Elderly Waiver/Alternative Care Programs Lisa Rotegard lisa.rotegard@state.mn.us Manager Aging and Adult Services MN Department of Human Services 1 Who is Eligible for EW? Age 65 or older Eligible for
Elderly Waiver/Alternative Care Programs Lisa Rotegard lisa.rotegard@state.mn.us Manager Aging and Adult Services MN Department of Human Services 1 Who is Eligible for EW? Age 65 or older Eligible for
Health HAPPEN. Make. Prepare now to stay healthy during flu season. Inside
 Inside How to lower your blood pressure Make Health HAPPEN Quarter 3, 2017 www.myamerigroup.com/medicare Prepare now to stay healthy during flu season Influenza, also known as the flu, can make you feel
Inside How to lower your blood pressure Make Health HAPPEN Quarter 3, 2017 www.myamerigroup.com/medicare Prepare now to stay healthy during flu season Influenza, also known as the flu, can make you feel
HOSPICE POLICY UPDATE
 #02-56-13 Bulletin June 24, 2002 Minnesota Department of Human Services # 444 Lafayette Rd. # St. Paul, MN 55155 OF INTEREST TO County Directors Administrative contacts AC, EW, CAC, CADI, TBI DD Waiver
#02-56-13 Bulletin June 24, 2002 Minnesota Department of Human Services # 444 Lafayette Rd. # St. Paul, MN 55155 OF INTEREST TO County Directors Administrative contacts AC, EW, CAC, CADI, TBI DD Waiver
Menu Item: Population Management
 Cover Page Menu Item: Population Management Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
Cover Page Menu Item: Population Management Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
An RHC Patient Centered Medical Home Experience
 An RHC Patient Centered Medical Home Experience NARHC October 19, 2017 Kate Hill, RN The Compliance Team MACRA Recognition TCT Recognized for it s PCMH Program Today s Objectives Understand the difference
An RHC Patient Centered Medical Home Experience NARHC October 19, 2017 Kate Hill, RN The Compliance Team MACRA Recognition TCT Recognized for it s PCMH Program Today s Objectives Understand the difference
Special Needs Plan (SNP) Model of Care Training 2018
 Model of Care Training 2018") Special Needs Plan (SNP) Model of Care Training 2018 Table of Contents Training Overview Pg. 1 Denver Health Medical Plan s (HMO SNP) MOC Annual Training Pg. 2 Special Needs Plans (SNPs) Pg. 2 Special
Special Needs Plan (SNP) Model of Care Training 2018 Table of Contents Training Overview Pg. 1 Denver Health Medical Plan s (HMO SNP) MOC Annual Training Pg. 2 Special Needs Plans (SNPs) Pg. 2 Special
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Medicare: 2017 Model of Care Training 12/14/201 7
 Medicare: 2017 Model of Care Training 12/14/201 7 What is the Model of Care? The Model of Care (MOC) is Allwell s plan for delivering our integrated care management program for members with special needs.
Medicare: 2017 Model of Care Training 12/14/201 7 What is the Model of Care? The Model of Care (MOC) is Allwell s plan for delivering our integrated care management program for members with special needs.
Frequently Asked Questions: HEDIS Attestations
 November 2016 Frequently Asked Questions: HEDIS Attestations What is HEDIS? (Healthcare Effectiveness Data and Information Set) HEDIS stands for Healthcare Effectiveness Data and Information Set which
November 2016 Frequently Asked Questions: HEDIS Attestations What is HEDIS? (Healthcare Effectiveness Data and Information Set) HEDIS stands for Healthcare Effectiveness Data and Information Set which
Model of Care. Quality Department 2017
 Model of Care Quality Department 2017 1 Objectives Understand the four (4) Model of Care elements, aimed at improving healthcare for D-SNP members. Learn about the Model of Care that MCS offers to their
Model of Care Quality Department 2017 1 Objectives Understand the four (4) Model of Care elements, aimed at improving healthcare for D-SNP members. Learn about the Model of Care that MCS offers to their
Checklist for Ocean County Community Health Improvement Plan Implementation of Strategies- Activities for Ocean County Health Centers: CHEMED & OHI
 Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Steps for Success. Personal Care Assistance
 Steps for Success Personal Care Assistance Why are you here? An overview of: PCA Program guidelines Eligibility Covered services How a person gets services 2 Why are you here? Program policy requirements
Steps for Success Personal Care Assistance Why are you here? An overview of: PCA Program guidelines Eligibility Covered services How a person gets services 2 Why are you here? Program policy requirements
How Care Management Can Help You. Disease Management Program
 Florida 2015 ISSUE II How Care Management Can Help You Got a question or concern about your health? Care Management helps members with special needs. It pairs a member with a care manager. The care manager
Florida 2015 ISSUE II How Care Management Can Help You Got a question or concern about your health? Care Management helps members with special needs. It pairs a member with a care manager. The care manager
MODEL OF CARE TRAINING 2018
 MDEL F CARE TRAINING 2018 Content Introduction to SNP SNP Model of Care CHMP SNP population and vulnerable population SNP Benefit Roles and Responsibility HRA ICT Team Care Transition process Provider
MDEL F CARE TRAINING 2018 Content Introduction to SNP SNP Model of Care CHMP SNP population and vulnerable population SNP Benefit Roles and Responsibility HRA ICT Team Care Transition process Provider
Quality: Finish Strong in Get Ready for October 28, 2016
 Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Community Health Improvement Plan
 Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance
 Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance Joan Valentine, MSA, RN Executive Vice President Visiting Physicians Association David
Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance Joan Valentine, MSA, RN Executive Vice President Visiting Physicians Association David
Molina Medicare Model of Care. Healthcare Services Molina Healthcare 2016
 Molina Medicare Model of Care Healthcare Services Molina Healthcare 2016 MHTPS_MOCTRN_062016 1 Molina s Mission Our mission is to provide quality health services to financially vulnerable families and
Molina Medicare Model of Care Healthcare Services Molina Healthcare 2016 MHTPS_MOCTRN_062016 1 Molina s Mission Our mission is to provide quality health services to financially vulnerable families and
UCare Connect Care Coordination Requirement Grid Updated effective
 UCare Connect Care Coordination Requirement Grid Updated 8.1.18 effective 9.1.18 The assigned Care Coordinator (CC) must meet the required definition of a qualified professional. Care coordination services
UCare Connect Care Coordination Requirement Grid Updated 8.1.18 effective 9.1.18 The assigned Care Coordinator (CC) must meet the required definition of a qualified professional. Care coordination services
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Connecticut Department of Public Health
 Connecticut Department of Public Health Request for Proposal October 2008 RFP # 2009-4548 The Connecticut Department of Public Health s (DPH) Comprehensive Cancer Program is pleased to announce the availability
Connecticut Department of Public Health Request for Proposal October 2008 RFP # 2009-4548 The Connecticut Department of Public Health s (DPH) Comprehensive Cancer Program is pleased to announce the availability
Molina Medicare Model of Care
 Molina Medicare Model of Care Provider Network Molina Healthcare 2018 1 Molina s Mission and Vision Our Vision: We envision a future where everyone receives quality health care Our Mission: To provide
Molina Medicare Model of Care Provider Network Molina Healthcare 2018 1 Molina s Mission and Vision Our Vision: We envision a future where everyone receives quality health care Our Mission: To provide
A Guide to Accessing Quality Health Care
 A Guide to Accessing Quality Health Care Spring 2015 MolinaHealthcare.com 37894DM0115 Molina Healthcare s Quality Improvement Plan and Program Your health care is important to us. We want to hear how we
A Guide to Accessing Quality Health Care Spring 2015 MolinaHealthcare.com 37894DM0115 Molina Healthcare s Quality Improvement Plan and Program Your health care is important to us. We want to hear how we
2016 Complex Case Management. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015
 MODEL OF CARE TRAINING 2015") SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
Update! Frequently Asked Questions: HEDIS Clincal Quality Validation (previously named HEDIS Attestations)
") March 2018 Update! Frequently Asked Questions: HEDIS Clincal Quality Validation (previously named HEDIS Attestations) 1. What is HEDIS? (Healthcare Effectiveness Data and Information Set) HEDIS stands
March 2018 Update! Frequently Asked Questions: HEDIS Clincal Quality Validation (previously named HEDIS Attestations) 1. What is HEDIS? (Healthcare Effectiveness Data and Information Set) HEDIS stands
Triennial Compliance Assessment. HealthPartners. Performed under Interagency Agreement for: Minnesota Department of Human Services
 Triennial Compliance Assessment Of HealthPartners Performed under Interagency Agreement for: Minnesota Department of Human Services By Minnesota Department of Health (MDH) Managed Care Systems Section
Triennial Compliance Assessment Of HealthPartners Performed under Interagency Agreement for: Minnesota Department of Human Services By Minnesota Department of Health (MDH) Managed Care Systems Section
CMS Mandated Training
 CMS Mandated Training Brand New Day Models of Care PRINT Your Name: SIGN Your Name: Print Today s Date: F:\QM\COMPLIANCE\COMPLIANCE TRAINING\MOC\BRAND NEW DAY MOC TRAINING.docx Brand New Day Medicare Mandated
CMS Mandated Training Brand New Day Models of Care PRINT Your Name: SIGN Your Name: Print Today s Date: F:\QM\COMPLIANCE\COMPLIANCE TRAINING\MOC\BRAND NEW DAY MOC TRAINING.docx Brand New Day Medicare Mandated
Sage Medical Center New Patient Forms
 Sage Medical Center New Patient Forms Patient Name: DOB: Providers and Suppliers of Your Medical Care: Please list all providers and suppliers of your medical care such as primary care physicians, specialty
Sage Medical Center New Patient Forms Patient Name: DOB: Providers and Suppliers of Your Medical Care: Please list all providers and suppliers of your medical care such as primary care physicians, specialty
HealthPartners SNBC Inspire
 Click to edit Master title style HealthPartners SNBC Inspire March 28 & 30, 2017 Agenda New Team Members DHS SNBC Audit 6 Month Follow Up Calls Benefit Exception Inquiry Form Adjustments HealthPartners
Click to edit Master title style HealthPartners SNBC Inspire March 28 & 30, 2017 Agenda New Team Members DHS SNBC Audit 6 Month Follow Up Calls Benefit Exception Inquiry Form Adjustments HealthPartners
ProviderReport. Managing complex care. Supporting member health.
 ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
Are your patients up to date?
 SUMMER 2014 Are your patients up to date? As your patients physician, you can play a big part in keeping them on track for preventive screenings. You have a stronger influence on the health of your patients
SUMMER 2014 Are your patients up to date? As your patients physician, you can play a big part in keeping them on track for preventive screenings. You have a stronger influence on the health of your patients
Guide to Accessing Quality Health Care Spring 2017
 Guide to Accessing Quality Health Care Spring 2017 MolinaHealthcare.com 5771749DM0217 MyMolina MyMolina is a secure web portal that lets you manage your own health from your computer. MyMolina.com is easy
Guide to Accessing Quality Health Care Spring 2017 MolinaHealthcare.com 5771749DM0217 MyMolina MyMolina is a secure web portal that lets you manage your own health from your computer. MyMolina.com is easy
Health Home Flow Hypothetical Patient Scenario
 Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015
 Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
P.R.E.P. Prevention Reward Employee Program
 P.R.E.P. Prevention Reward Employee Program Plan Document 2015-2016 ii Table of Contents Table of Contents 1 Welcome to P.R.E.P. 1 Program Overview 2 Eligibility 2 How to Participate 2 2 Completing your
P.R.E.P. Prevention Reward Employee Program Plan Document 2015-2016 ii Table of Contents Table of Contents 1 Welcome to P.R.E.P. 1 Program Overview 2 Eligibility 2 How to Participate 2 2 Completing your
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Medicare: 2017 Model of Care Training 4/13/2017
 Medicare: 2017 Model of Care Training Training Objectives This course will describe how MHS Health Wisconsin Medicare Advantage and its contracted providers work together to successfully deliver the Model
Medicare: 2017 Model of Care Training Training Objectives This course will describe how MHS Health Wisconsin Medicare Advantage and its contracted providers work together to successfully deliver the Model
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Exclusively for Health Advocate Members. All-in-1 Benefit. Benefits Gateway Personal Dashboard Healthcare Help Wellness Support EAP+Work/Life
 Exclusively for Health Advocate Members All-in-1 Benefit Benefits Gateway Benefits Gateway Connect to the right benefit Welcome to HealthAdvocate Health Advocate is a service provided by your employer
Exclusively for Health Advocate Members All-in-1 Benefit Benefits Gateway Benefits Gateway Connect to the right benefit Welcome to HealthAdvocate Health Advocate is a service provided by your employer
Health First Wellness Incentive
 Health First Wellness Incentive The Health First Wellness Incentive has been set up as a reward for taking steps to either maintain or obtain a healthy lifestyle. Taking healthy actions and becoming a
Health First Wellness Incentive The Health First Wellness Incentive has been set up as a reward for taking steps to either maintain or obtain a healthy lifestyle. Taking healthy actions and becoming a
Blue Advantage (PPO) SM 2018 Quality+Partnerships
 SM 2018 Quality+Partnerships") Blue Advantage (PPO) SM 2018 Quality+Partnerships Your Partner in Quality Care BlueCross BlueShield of Tennessee is committed to ensuring our members have access to a network of high quality providers.
Blue Advantage (PPO) SM 2018 Quality+Partnerships Your Partner in Quality Care BlueCross BlueShield of Tennessee is committed to ensuring our members have access to a network of high quality providers.
Assistance. Improving. Consumer Health. Strategies for
 Assistance Strategies for Improving Consumer Health A resource to help educate consumers about available preventive health incentives and eliminating barriers to receiving care www.bhpi.org www.healthsharesolutions.org
Assistance Strategies for Improving Consumer Health A resource to help educate consumers about available preventive health incentives and eliminating barriers to receiving care www.bhpi.org www.healthsharesolutions.org
2018 Medicare Advantage Dual Eligible Special Needs Plan (DSNP), Chronic Special Needs Plan ESRD (CSNP ESRD) & Model of Care (MOC) Overview
, Chronic Special Needs Plan ESRD (CSNP ESRD) & Model of Care (MOC) Overview") 2018 Medicare Advantage Dual Eligible Special Needs Plan (DSNP), Chronic Special Needs Plan ESRD (CSNP ESRD) & Model of Care (MOC) Overview Medicare Advantage (MA) Program Part C Medicare Advantage Medicare
2018 Medicare Advantage Dual Eligible Special Needs Plan (DSNP), Chronic Special Needs Plan ESRD (CSNP ESRD) & Model of Care (MOC) Overview Medicare Advantage (MA) Program Part C Medicare Advantage Medicare
Medicare Advantage Star Ratings
 Medicare Advantage Star Ratings December 2017 The Star Rating System measures how well Medicare Advantage (MA) and its prescription drug plans perform for consumers. As an integrated health system, Presbyterian
Medicare Advantage Star Ratings December 2017 The Star Rating System measures how well Medicare Advantage (MA) and its prescription drug plans perform for consumers. As an integrated health system, Presbyterian
GERIATRIC SERVICES CAPACITY ASSESSMENT DOMAIN 4 ALTERNATE LIVING ARRANGEMENTS
 GERIATRIC SERVICES CAPACITY ASSESSMENT DOMAIN 4 ALTERNATE LIVING ARRANGEMENTS Table of Contents Introduction... 2 Purpose... 2 Serving Senior Medicare-Medicaid Enrollees... 2 How to Use This Tool... 2
GERIATRIC SERVICES CAPACITY ASSESSMENT DOMAIN 4 ALTERNATE LIVING ARRANGEMENTS Table of Contents Introduction... 2 Purpose... 2 Serving Senior Medicare-Medicaid Enrollees... 2 How to Use This Tool... 2
1 Title Improving Wellness and Care Management with an Electronic Health Record System
 HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
Model of Care Heritage Provider Network & Arizona Priority Care Model of Care 2018
 Model of Care Model of Care 2018 Learning Objectives Program participants will be able to: List two differences between the Complex Care Management (CCM), and Special Needs Program (SNP) programs. Identify
Model of Care Model of Care 2018 Learning Objectives Program participants will be able to: List two differences between the Complex Care Management (CCM), and Special Needs Program (SNP) programs. Identify
St. James Mercy Hospital 2012 Community Service Plan Update Executive Summary
 St. James Mercy Hospital 2012 Community Service Plan Update Executive Summary Hospitals in New York State (NYS) are required by the Department of Health to create and publicly distribute an annual Community
St. James Mercy Hospital 2012 Community Service Plan Update Executive Summary Hospitals in New York State (NYS) are required by the Department of Health to create and publicly distribute an annual Community
My Complete Medications List
 Pharmacy Features 1 My Complete Medications List 2 My HealtheVet: Get Care Get Care: Care Givers Treatment Facilities My Coverage Health insurance Health Calendar To-Do s Wellness Reminders 3 My HealtheVet:
Pharmacy Features 1 My Complete Medications List 2 My HealtheVet: Get Care Get Care: Care Givers Treatment Facilities My Coverage Health insurance Health Calendar To-Do s Wellness Reminders 3 My HealtheVet:
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
UPMC Health Plan. Value Based Insurance Design (VBID) Spark Your Health
 Spark Your Health") UPMC Health Plan Value Based Insurance Design (VBID) Spark Your Health Value Based Insurance Design (VBID) Spark Your Health Medicare Advantage Summit April 6, 2017 Helene Weinraub 1 The statements contained
UPMC Health Plan Value Based Insurance Design (VBID) Spark Your Health Value Based Insurance Design (VBID) Spark Your Health Medicare Advantage Summit April 6, 2017 Helene Weinraub 1 The statements contained
Meet DEAN & EDNA: The Application of HHQI Resources in the Reduction of Avoidable Hospitalizations
 Meet DEAN & EDNA: The Application of HHQI Resources in the Reduction of Avoidable Hospitalizations Cindy Sun, MSN, RN Objectives At the conclusion of this session, the participant will be able to: Access
Meet DEAN & EDNA: The Application of HHQI Resources in the Reduction of Avoidable Hospitalizations Cindy Sun, MSN, RN Objectives At the conclusion of this session, the participant will be able to: Access
Rethinking annual assessments: Identifying and closing gaps in care
 Rethinking annual assessments: Identifying and closing gaps in care Expert presenters Curtis A. Mock, MD, MBA, National Medical Director, Complex Population Management Annual in-home assessments provide
Rethinking annual assessments: Identifying and closing gaps in care Expert presenters Curtis A. Mock, MD, MBA, National Medical Director, Complex Population Management Annual in-home assessments provide
KyHealth Choices. Presentation to Medicaid Congress June 15, Mark D. Birdwhistell Secretary, Cabinet for Health and Family Services
 KyHealth Choices Presentation to Medicaid Congress June 15, 2007 Mark D. Birdwhistell Secretary, Cabinet for Health and Family Services Agenda Background & Vision for Kentucky Medicaid Comprehensive Medicaid
KyHealth Choices Presentation to Medicaid Congress June 15, 2007 Mark D. Birdwhistell Secretary, Cabinet for Health and Family Services Agenda Background & Vision for Kentucky Medicaid Comprehensive Medicaid
National Resource Center on Native American Aging at the UNDSMHS Center for Rural Health
 Assessing Elder Needs How to Measure Benefits and Develop Links to Long-term Care Alan Allery, Ph.D. Richard L. Ludtke, PhD Leander R. McDonald, PhD National Resource Center on Native American Aging at
Assessing Elder Needs How to Measure Benefits and Develop Links to Long-term Care Alan Allery, Ph.D. Richard L. Ludtke, PhD Leander R. McDonald, PhD National Resource Center on Native American Aging at
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically