How Battle Field Experience Leads to Improvement in Orthopaedic Care BRETT COURTENAY RAAMC
|
|
|
- Jean Webster
- 5 years ago
- Views:
Transcription
1 How Battle Field Experience Leads to Improvement in Orthopaedic Care BRETT COURTENAY RAAMC
2 Outline Winners from War Medical and Munitions Technology Insurgency Warfare Medical Challenges and Solutions Case Studies Medical Advances
3 Lethality of War Wounds among US Soldiers War War in Iraq JULY 2006 and Afghanistan, No Wounded or KIA No KIA Lethality of war wounds Revolutionary War , War of ,765 2, Mexican War ,885 1, Civil War (Union Force) , , Spanish-American War World War ,404 53, World War , , Korean War ,025 33, Vietnam War ,727 47, Persian Gulf War Present DSTCMM %
4 Medicine: War and History Battle and Non Battle injuries Generally outnumber battle injuries Disease Sudan Formal Medical Corps NSW Corps Boer War Medics as combatants Nurses in the field Early surgery and delayed closure
5 20th Century World War I Orthopaedic Splintage compound Femur Mortality from 80% to 15% Blood Transfusions 1917 could only be kept 12 hours World War II Antibiotics Safe Transfusion Korea & Vietnam Golden Hour Early aggressive resuscitation

6 Florence Nightingale
7 Biography Born Florence 1820 very wealthy family 3 months training Kaiserwerth Germany 1851 Returned to run small private hospital Harley Street London Cholera very common 1854 with 38 nurses invites to Turkey to assist in British Hosp Military Hosp Crimean War Dreadful conditions
8 Achievements Cleaned up the hospital Improved everything Dramatically decreased mortality Known as the Lady with the Lamp Result of evening rounds Returned to UK as a legend Queen Victoria supporter and improved all areas but primarily nursing training
9 Quotes The very first requirement in a hospital is that it should do the sick no harm. Women have no sympathy and my experience of women is almost as large as Europe.

10
11 Lethality of Modern Warfare Type of Warfare Personal Protection Blasts aimed to Kill a lot and injure many more Medical advances Battle and Non Battle injuries
12 Injuries of Survivors


13 Body Armour

14 Loads carried by Soldiers
15 Modern Warfare Non Conventional asymmetric warfare Tactical and Strategic differences Unpredictable Exhaustion Resources Terrorism Insurgency Subversion Information operations
16 Tools of the Trade Improvised Explosive Devices (IED s) Fixed position Roadside Bombs Mobile People borne suicide bombers Vehicle borne Indirect Fire - Rockets and RPG s Direct Fire - GSW
17 Mechanism Blast Injuries Primary Injury Movement of air pressure Secondary Injury Movement of Projectiles Tertiary Injury Movement of people Quaternary Injury Miscellaneous Injuries Dead to Injured 1:4.35
18 Primary Injury Rapidly expanding blast wave Air filled organs most affected Middle Ear Lungs Colon IED 60 psi Hellfire Missile 5,000,000 psi
19 Secondary Injuries Multiple projectiles Body Armour, Ballistic helmets, Ballistic Eyewear are effective Projectiles 1800 metres per sec Unprotected areas most vulnerable Secondary missiles energized Rocks, dirt, bone fragments & clothing including additional projectiles in clothing (5mm ball bearings in the hundreds!)

20 Helmets & Eye Protection


21 Canadian SGT

22
23 Tertiary Injuries Victims projected into stationary objects Passengers in vehicles Head injuries and fractures
24 Quaternary Injuries Inhaled Pollutants Airway burns Thermal burns Crush injuries
25 Surgical Considerations Multiple patients at a time Multiple penetrating injuries Abdominal and Chest injuries Peripheral Injuries Which wounds to explore ATLS Principles
26 Australian Military Experience Sudan in 1885 March - June Infantry Battalion from NSW 700 troops Generally regarded as too late to be effective. NSW Medical Corps Volunteer Doctors and Orderlies CO MAJ William Williams Surgeon St Vincents Hospital
27 MAJ Williams Contributions NSW Medical Corps in Sudan five ambulances, two stores carts, a water cart 26 horses,,tentage, hospital equipment, and field kitchen In total 34 officers and ORs Established Resus Team MO, NO and 2 stretcher bearers basis still today Trained stretcher bearers to be at the edge of the battle as it raged to extract casualties as quickly as possible and get them to doctors working close behind the action. Modified a cart for specific use as Ambulance.
28 Military Service Training Exercises regular activity Disaster Assistance Common in our Area Papua New Guinea, Indonesia, Philippines, Pakistan Peace Keeping Bouganville, Timor, Solomon Islands, Fiji War Like Service Timor, Iraq, Afghanistan All in the last 20 years
29 Military Deployments Medical is critical but not the Mission Chain of Command Limited Control of what happens Limited resupply Unpredictable Diseases not seen in Australia General poor nutrition No facilities or services
30 Military Surgery Natural Disasters and War Like A large volume of work in a very short time with limited supplies and no short term resupply However Resus team in a FST (Role2) or Role 3 is as capable as any major ED in any major Hospital. Kandahar in to 20 CAT1 patients per day NSW has about 250 per year.
31 Challenges and Solutions Disaster Assistance Essential to do simple and effective. Easy for next person to take over without notes Do what fails well rarely second chance Very minimal resources and slow resupply Personal risks of disease and climate
32 OP SLIPPER AUS MTF Australia rotates with Dutch and Singaporean Teams Surgical Team Orthopaedic and General Surgeon Anaesthetist and Intensivist 2 Theatre RNs Theatre Technicians (Medics) Intensive Care Team 3 ICU RNs ICU Technicians (Medics)

33

34

35

36
37 Dutch Hospital Role 1 GP and general medical Dental services Physiotherapy Pathology Radiology Mortuary Pharmacy Wards Administration Theatre Complex Operating Room Intensive Care 2 beds Resuscitation 2 Cat A Recovery 2 Bays Second Resus

38


39

40
41 Modern Medical Advances Tactical Casualty Combat Care TC3 Control Haemorrhage Tourniquets issued to all One handed application Injured can apply themselves Control breathing Pneumothorax Thoracocentesis Hold fluids in most cases Damage Control Resusciation


42
43 Lessons Learnt Permissive Hypotension Rapid transfer to FST and OR where indicated Resuscitation Teams Team permitted to function Senior specialists kept back until invited to assist. Damage Control Surgery Provision of Transfusion Products Walking Blood Bank Frozen Blood Dutch Solution
44 Permissive Hypotension Minimal fluid at scene Accept BP 80mm Hg if no brain injury Airway and bleeding control All troops trained and issued with tourniquets Scoop and run rather than stay and play Transfer to FST Resus and OR capability ASAP Early and aggressive blood transfusion Rapid transfer to surgery In AFG 95% survival if pulse on arrival at FST

45
46 Resus Teams Doctor, Nurse and 2 Medics 2 Teams ready with additional 2 teams Role 2 could manage 4 CAT 1 at a time Senior MO (ICU) would monitor patients Other Specialists kept away unless necessary Permitted teams to work as a team Role 3 facility capacity for 16 CAT 1 In 2009 would handle 15 to 20 CAT 1 per day All Sydney about 250 CAT 1 per year

47

48 Damage Control Surgery The modern operation is safe for the patient. The modern surgeon must make the patient safe for the modern operation Lord Moynihan
49 Principles Multi Trauma Patient more likely die from intraoperative metabolic failure than from failure to complete operative repair Patients die from a triad of coagulopathy, hypothermia and metabolic acidosis Control of haemorrhage, prevention of contamination and protection from further injury No margin for error Decreased mortality CAT 1 from 65% to 19%
50 Parameters When to convert to Damage Control ph < 7.2 Core Temp < 32 C > Blood Volume Transfusion Early decision gives best survival.
51 Three Phases Primary Surgery Intensive Care Resuscitation Planned reoperation Principles extend to all surgery Particularly Limb saving Do basic Limb saving and revisit
52 Case Study Male 20 yrs UD possible 3 rounds of 5.56! Weapon safety problems! Rotary AME doors open and patient wet Core temp < 32 C Coagulopathic on admission Wound packed Temp in Resus on way to OT 32.8 C First ph 7.27 (in OT ABG from arterial line)

53

54
55 Resuscitation Fluids - from Injury to leaving OT 3000ml Crystalloid 600ml Colloid 14 Units Red Cells 12 Units FFP 10 Units Platelets Total Time in OT 140 minutes
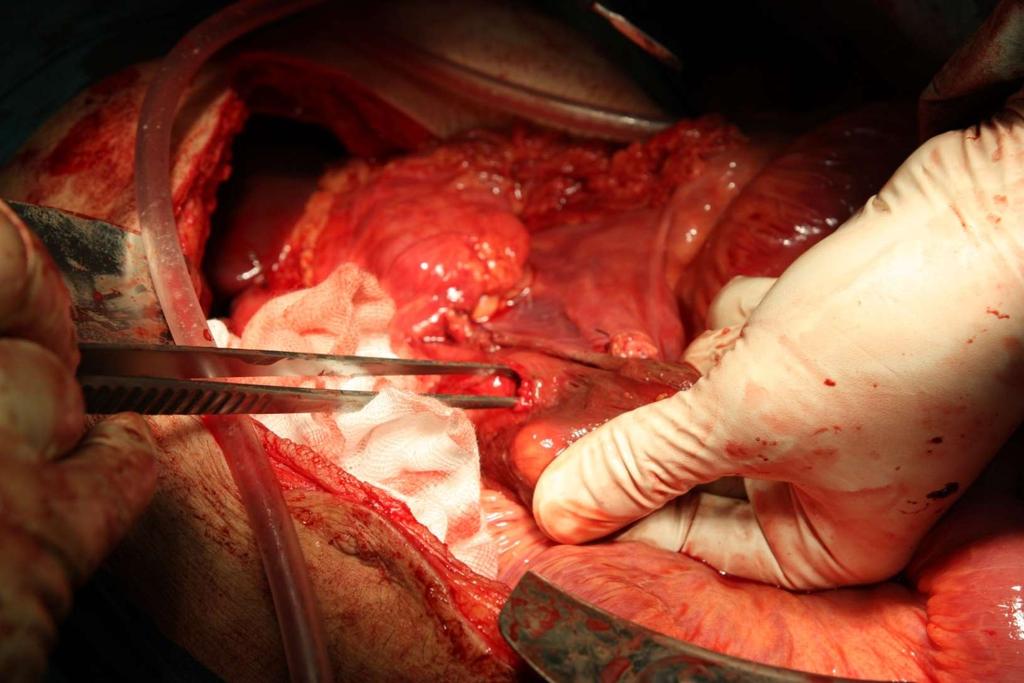
56 Findings Extensive bleeding from right iliac crest wound Extensive damage ascending colon, caecum, ileum. Laceration 2 nd /3 rd part duodenum Extended Right Hemicolectomy Bowel closed with GIA stapler No anastomosis performed
57

58
59 Intensive Care Arrived Temp 32.8 C same as pre op After laparotomy left open packed and Vac ph on admission 7.43 Temp restored to 37.2 C Blood loss dropped to 300ml per hour for 2 hours and then stopped. Transfer at 4 hours Needed to ensure Unit ready for next patient
60 Follow Up Transferred to Role 3 Principally for CT scan for spine Poor Communication 3/7 later Bowel anastomosis Plan to close abdomen Chest infection antibiotics All else good
61 Blood Solutions Walking Blood Bank Fresh blood from fellow soldiers Limited or no testing Huge pressure on mates Limited supplies Very noble but unsafe Fresh Blood from wherever Very difficult shelf life 4 weeks maximum Dutch Solution Frozen Blood
62 Dutch solution Frozen blood bank deployed in one mission Resupply as needed (less logistic requirement) All blood fully screened Blood supplied as needed by 2 person 6 units of PRBC (O-) thawed for use, rest supplied as needed All fresh RBC (frozen within 24 hours of collection) Wastage approaches zero regardless of operational tempo
63 Frozen Blood Shelf Life (stored at -80 C) All frozen on Day 1 Red Cells 10 years FFP 7 years Platelets 3 years
64 Dutch Blood Solution Frozen -70 C on day 1 collection Kept in Holland for 1 year and donor retested Shelf Life Red Cells - 10 years Plasma - 7 years Platelets - 3 Years Transported packed in dry ice Stored in -80 C freezer Reconstituted in 20 to 30 minutes Once reconstituted blood good for 2 to 3 weeks. Never short of blood and never any delay for blood.
65 In Summary Military Deployment offers unique experience Radical solutions are found Very accurate data collected and reviewed Experience shows that radical approaches works Able to demonstrate to civilian trainees and colleagues Otherwise we would stay in our comfort zone and limit progress
66 Acknowledgements All of other ADF members who helped get me there and who I worked with. To all ADF members doing the hard work who we were able to provide a high level of care to. My family left at home with only limited contact Good and regular phone calls but not able to say a lot. Personal and Family Burdens carried by the 18,000 Australians to Iraq and Afghanistan since 2001

67 Thank You
The 2013 Boston Marathon Bombings
 The 2013 Boston Marathon Bombings Lessons Learned from a Resource-Rich Urban Battlefield Presented at the 41 st Convention of the American Society of Plastic Surgical Nurses Boston, Massachusetts October
The 2013 Boston Marathon Bombings Lessons Learned from a Resource-Rich Urban Battlefield Presented at the 41 st Convention of the American Society of Plastic Surgical Nurses Boston, Massachusetts October
Update on War Zone Injuries Stan Breuer, OTD, OTR/L, CHT Colonel, United States Army
 Update on War Zone Injuries Stan Breuer, OTD, OTR/L, CHT Colonel, United States Army Disclaimer: The opinions or assertions contained herein are the private view of the author and are not to be construed
Update on War Zone Injuries Stan Breuer, OTD, OTR/L, CHT Colonel, United States Army Disclaimer: The opinions or assertions contained herein are the private view of the author and are not to be construed
Deployment Medicine Operators Course (DMOC)
") Deployment Medicine Operators Course (DMOC) The need has never been more critical to equip those who will first contact the battlefield casualty with lifesaving knowledge to improve survivability. Course
Deployment Medicine Operators Course (DMOC) The need has never been more critical to equip those who will first contact the battlefield casualty with lifesaving knowledge to improve survivability. Course
Sunrise Hospital & Medical Center Response to October 1 Mass Casualty Event. Kimberly Hatchel, DNP, MHA, RN, CENP. #VegasSTRONG
 Sunrise Hospital & Medical Center Response to October 1 Mass Casualty Event Kimberly Hatchel, DNP, MHA, RN, CENP #VegasSTRONG Level II Trauma Center About Sunrise Hospital & Medical Center 692-bed adult
Sunrise Hospital & Medical Center Response to October 1 Mass Casualty Event Kimberly Hatchel, DNP, MHA, RN, CENP #VegasSTRONG Level II Trauma Center About Sunrise Hospital & Medical Center 692-bed adult
Penn State Milton S. Hershey Medical Center. Division of Trauma, Acute Care & Critical Care Surgery
 Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Bringing Combat Medicine to the Streets of EMS. MAJ Will Smith MD, EMT-P US Army
 Bringing Combat Medicine to the Streets of EMS MAJ Will Smith MD, EMT-P US Army Disclaimers No financial or other conflicts to disclose This presentation is NOT an official position or endorsement from
Bringing Combat Medicine to the Streets of EMS MAJ Will Smith MD, EMT-P US Army Disclaimers No financial or other conflicts to disclose This presentation is NOT an official position or endorsement from
U.S. ARMY MEDICAL SUPPORT
 U.S. ARMY MEDICAL SUPPORT BY SGT FREDERICK, EVELYN CIVIL AFFAIRS TEAM 8041 MEDIC AGENDA HOSPITAL LEVELS OF CARE TRAINING FOR ALL SOLDIERS: SELF AID, Tactical Combat Casualty Care (TCCC) MEDICS: REGULAR,
U.S. ARMY MEDICAL SUPPORT BY SGT FREDERICK, EVELYN CIVIL AFFAIRS TEAM 8041 MEDIC AGENDA HOSPITAL LEVELS OF CARE TRAINING FOR ALL SOLDIERS: SELF AID, Tactical Combat Casualty Care (TCCC) MEDICS: REGULAR,
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC CONDUCT TRIAGE
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC 28542-0042 FMSO 107 CONDUCT TRIAGE TERMINAL LEARNING OBJECTIVE (1) Given multiple simulated casualties in a simulated operational
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION-EAST Camp Lejeune, NC 28542-0042 FMSO 107 CONDUCT TRIAGE TERMINAL LEARNING OBJECTIVE (1) Given multiple simulated casualties in a simulated operational
of Trauma Assembly 28 th Page 1
 Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 11 Preparing for the Next War: Pivotal Military Civilian Relationships January 16, 215 Disney s Contemporary
Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 11 Preparing for the Next War: Pivotal Military Civilian Relationships January 16, 215 Disney s Contemporary
Tactical & Hunter First Aid Workshop
 Jackson Hole Gun Club Jackson, WY July 15, 2013 Tactical & Hunter First Aid Workshop LTC Will Smith MD, Paramedic www.wildernessdoc.com Disclaimers No financial conflicts to disclose Board of Advisors
Jackson Hole Gun Club Jackson, WY July 15, 2013 Tactical & Hunter First Aid Workshop LTC Will Smith MD, Paramedic www.wildernessdoc.com Disclaimers No financial conflicts to disclose Board of Advisors
1/7/2014. Dispatch for fire at Rosslyn, VA metro station Initial dispatch as Box Alarm
 1 Dispatch for fire at Rosslyn, VA metro station Initial dispatch as Box Alarm 4 engines, 2 trucks, 1 rescue, 1 medic unit, 2 battalion chiefs, 1 EMS supervisor, 1 battalion aide First arriving units report
1 Dispatch for fire at Rosslyn, VA metro station Initial dispatch as Box Alarm 4 engines, 2 trucks, 1 rescue, 1 medic unit, 2 battalion chiefs, 1 EMS supervisor, 1 battalion aide First arriving units report
of Trauma Assembly 28 th Page 1
 Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 11 Preparing for the Next War: Pivotal Military Civilian Relationships January 16, 2015 Disney s Contemporary
Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 11 Preparing for the Next War: Pivotal Military Civilian Relationships January 16, 2015 Disney s Contemporary
COMBAT Research Study
 COMBAT Research Study Questions & Answers What is the title of this research study? The Control Of Massive Bleeding After Trauma (COMBAT): A prospective, randomized comparison of early fresh frozen plasma
COMBAT Research Study Questions & Answers What is the title of this research study? The Control Of Massive Bleeding After Trauma (COMBAT): A prospective, randomized comparison of early fresh frozen plasma
High Threat Mass Casualty 1/7/2014. Game changer..
 Changing the Paradigm: Guidelines for High Risk Scenarios E. Reed Smith, MD, FACEP Committee for Tactical Emergency Casualty Care 1 Game changer.. 2 High Threat Mass Casualty What is the traditional teaching
Changing the Paradigm: Guidelines for High Risk Scenarios E. Reed Smith, MD, FACEP Committee for Tactical Emergency Casualty Care 1 Game changer.. 2 High Threat Mass Casualty What is the traditional teaching
What is the Massive Transfusion Protocol (MTP)? Provision and mobilisation of large
? Provision and mobilisation of large") RCH Massive Transfusion Protocol medical Dr. Helen Savoia Nicole vander Linden Mary Comande What is the Massive Transfusion Protocol (MTP)? Provision and mobilisation of large amounts of blood product
RCH Massive Transfusion Protocol medical Dr. Helen Savoia Nicole vander Linden Mary Comande What is the Massive Transfusion Protocol (MTP)? Provision and mobilisation of large amounts of blood product
The Evolution of Battlefield Surgery Post Damage Control Surgery
 The Evolution of Battlefield Surgery Post- 9-11 & Damage Control Surgery LTC DUANE DUKE MD FACS Division Chief of Pediatric Surgery USU Walter Reed Surgery 19OCT2016 Disclosure I have no personal or professional
The Evolution of Battlefield Surgery Post- 9-11 & Damage Control Surgery LTC DUANE DUKE MD FACS Division Chief of Pediatric Surgery USU Walter Reed Surgery 19OCT2016 Disclosure I have no personal or professional
AAST Senior Visiting Surgeon Program
 AAST Senior Visiting Surgeon Program Landstuhl Medical Center Mary C. McCarthy, MD Professor of Surgery Wright State University School of Medicine 2007 McCarthy Objectives After participating in this activity,
AAST Senior Visiting Surgeon Program Landstuhl Medical Center Mary C. McCarthy, MD Professor of Surgery Wright State University School of Medicine 2007 McCarthy Objectives After participating in this activity,
Roles of Medical Care (United States)
") Roles of Medical Care (United States) Chapter 2 Roles of Medical Care (United States) Introduction Military doctrine supports an integrated health services support system to triage, treat, evacuate, and
Roles of Medical Care (United States) Chapter 2 Roles of Medical Care (United States) Introduction Military doctrine supports an integrated health services support system to triage, treat, evacuate, and
Department of Defense Trauma Registry
 Appendix Appendix 3 Department of Defense Trauma Registry General Evidence-based medicine allows for identification of best practices and the timely formulation of clinical practice guidelines. Unfortunately,
Appendix Appendix 3 Department of Defense Trauma Registry General Evidence-based medicine allows for identification of best practices and the timely formulation of clinical practice guidelines. Unfortunately,
Active Violence and Mass Casualty Terrorist Incidents
 Position Statement Active Violence and Mass Casualty Terrorist Incidents The threat of terrorism, specifically active shooter and complex coordinated attacks, is a concern for the fire and emergency service.
Position Statement Active Violence and Mass Casualty Terrorist Incidents The threat of terrorism, specifically active shooter and complex coordinated attacks, is a concern for the fire and emergency service.
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 401 Introduction to Tactical Combat Casualty Care TERMINAL LEARNING OBJECTIVE 1. Given a casualty in a tactical
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 401 Introduction to Tactical Combat Casualty Care TERMINAL LEARNING OBJECTIVE 1. Given a casualty in a tactical
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 13th March 2014 Compliance
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 13th March 2014 Compliance
Contents. The Event 12/29/2016. The Event The Aftershock The Recovery Lessons Learned Discussion Summary
 #OrlandoUnited: Coordinating the medical response to the Pulse nightclub shooting Christopher Hunter, M.D., Ph.D. Director, Orange County Health Services Department Associate Medical Director, Orange County
#OrlandoUnited: Coordinating the medical response to the Pulse nightclub shooting Christopher Hunter, M.D., Ph.D. Director, Orange County Health Services Department Associate Medical Director, Orange County
TCCC for All Combatants 1708 Introduction to TCCC Instructor Guide 1
 TCCC for All Combatants 1708 Introduction to TCCC Instructor Guide 1 1. Tactical Combat Casualty Care for All Combatants August 2017 Introduction to TCCC Tactical Combat Casualty Care is the standard of
TCCC for All Combatants 1708 Introduction to TCCC Instructor Guide 1 1. Tactical Combat Casualty Care for All Combatants August 2017 Introduction to TCCC Tactical Combat Casualty Care is the standard of
Medical Advances as a Result of War
 trauma medical director Michael Iwanicki, DO trauma surgeons James P. Cole, Jr., DO, FACS Vijay Nair, MD, FRCS Jeffrey Rosen, MD, FACS director, emergency, emss & trauma division Ginger Diven, RN trauma/emss
trauma medical director Michael Iwanicki, DO trauma surgeons James P. Cole, Jr., DO, FACS Vijay Nair, MD, FRCS Jeffrey Rosen, MD, FACS director, emergency, emss & trauma division Ginger Diven, RN trauma/emss
Trauma Rotation UMASS Memorial University Campus
 Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
TRAUMA CENTER REQUIREMENTS
 California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
ESCAMBIA COUNTY FIRE-RESCUE
 Patrick T Grace, Fire Chief Page 1 of 7 PURPOSE: To create a standard of operation to which all members of Escambia County Public Safety will operate at the scene of incidents involving a mass shooting
Patrick T Grace, Fire Chief Page 1 of 7 PURPOSE: To create a standard of operation to which all members of Escambia County Public Safety will operate at the scene of incidents involving a mass shooting
Tactical Combat Casualty Care. CAPT Peter Rhee, MC, USN MD, MPH, DMCC, FACS, FCCM Professor of Surgery / Molecular Cellular Biology
 Tactical Combat Casualty Care CAPT Peter Rhee, MC, USN MD, MPH, DMCC, FACS, FCCM Professor of Surgery / Molecular Cellular Biology Good medicine in bad places Tactical Care 24 man team raid Building
Tactical Combat Casualty Care CAPT Peter Rhee, MC, USN MD, MPH, DMCC, FACS, FCCM Professor of Surgery / Molecular Cellular Biology Good medicine in bad places Tactical Care 24 man team raid Building
1. Receives report from EMS and/or outlying facility. 5. Adheres to safety and universal precaution guidelines.
 Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Surgical Legacies of Modern Combat: Translating Battlefield Medical Practices into Civilian Trauma Care
 American College of Surgeons 2017. All rights reserved Worldwide. Surgical Legacies of Modern Combat: Translating Battlefield Medical Practices into Civilian Trauma Care Achieving Zero Preventa bl e Deaths
American College of Surgeons 2017. All rights reserved Worldwide. Surgical Legacies of Modern Combat: Translating Battlefield Medical Practices into Civilian Trauma Care Achieving Zero Preventa bl e Deaths
NHS Emergency Planning Guidance
 NHS Emergency Planning Guidance Planning for the development and deployment of Medical Emergency Response Incident Teams in the provision of advanced medical care at the scene of an incident NHS Emergency
NHS Emergency Planning Guidance Planning for the development and deployment of Medical Emergency Response Incident Teams in the provision of advanced medical care at the scene of an incident NHS Emergency
The Royal College of Surgeons of England
 The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY)
") July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
Disaster Preparedness for
 Disaster Preparedness for Surgeons Charles M. Little, DO FACEP Associate Professor Division of Emergency Medicine University i of Colorado Denver School of Medicine Charles.Little@ucdenver.edu Today s
Disaster Preparedness for Surgeons Charles M. Little, DO FACEP Associate Professor Division of Emergency Medicine University i of Colorado Denver School of Medicine Charles.Little@ucdenver.edu Today s
Palm Beach County Fire Rescue Standard Operating Guideline
 Palm Beach County Fire Rescue Standard Operating Guideline Operational Procedure for the Protective Element Medical Team Effective Date /DRAFT Revised Date DRAFT SCOPE: PURPOSE: AUTHORITY: This guideline
Palm Beach County Fire Rescue Standard Operating Guideline Operational Procedure for the Protective Element Medical Team Effective Date /DRAFT Revised Date DRAFT SCOPE: PURPOSE: AUTHORITY: This guideline
25 February. Prepared for: National Collegiate Emergency Medical Services Foundation. Conference 2006 Boston, Massachusetts
 25 February Prepared for: National Collegiate Emergency Medical Services Foundation Conference 2006 Boston, Massachusetts What Is Lessons Learned Information Sharing? Online since April 19, 2004 Over 20,000
25 February Prepared for: National Collegiate Emergency Medical Services Foundation Conference 2006 Boston, Massachusetts What Is Lessons Learned Information Sharing? Online since April 19, 2004 Over 20,000
Course: Acute Trauma Care Course Number SUR 1905 (1615)
") Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
Trauma. Level 2. This resident can lead a to recognize common. This resident can. accurately diagnose. team that cares for traumatic conditions and
 Page 1 of 7 Trauma Subject Name Status Employer Program Rotation Evaluation Dates Evaluated by: Evaluator Name Status Employer Program 1 (Trauma) Patient Care: Ward Care This resident is not able lead
Page 1 of 7 Trauma Subject Name Status Employer Program Rotation Evaluation Dates Evaluated by: Evaluator Name Status Employer Program 1 (Trauma) Patient Care: Ward Care This resident is not able lead
Women who ve paid the cost of war
 Women who ve paid the cost of war Women throughout history who have sacrificed everything for their country are not forgotten but thanked this Women s History Month By signing up for newly opened combat
Women who ve paid the cost of war Women throughout history who have sacrificed everything for their country are not forgotten but thanked this Women s History Month By signing up for newly opened combat
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
DISTRIBUTION RESTRICTION:
 FM 3-21.31 FEBRUARY 2003 HEADQUARTERS DEPARTMENT OF THE ARMY DISTRIBUTION RESTRICTION: Approved for public release; distribution is unlimited. FIELD MANUAL NO. 3-21.31 HEADQUARTERS DEPARTMENT OF THE ARMY
FM 3-21.31 FEBRUARY 2003 HEADQUARTERS DEPARTMENT OF THE ARMY DISTRIBUTION RESTRICTION: Approved for public release; distribution is unlimited. FIELD MANUAL NO. 3-21.31 HEADQUARTERS DEPARTMENT OF THE ARMY
Warrior Tasks and Battle Drills
 Soldier Critical Skills Warrior Tasks and Battle Drills Shoot Maintain, employ, engage with assigned weapon system Employ hand grenades Move Perform individual movement techniques Navigate from one point
Soldier Critical Skills Warrior Tasks and Battle Drills Shoot Maintain, employ, engage with assigned weapon system Employ hand grenades Move Perform individual movement techniques Navigate from one point
Right Hemicolectomy Patient Information
 Right Hemicolectomy Patient Information Page 1 of 6 Patient Information Sheet Right Hemicolectomy This leaflet has been designed to help you to understand what to expect when you are having an operation
Right Hemicolectomy Patient Information Page 1 of 6 Patient Information Sheet Right Hemicolectomy This leaflet has been designed to help you to understand what to expect when you are having an operation
Left Hemicolectomy Patient Information
 Left Hemicolectomy Patient Information Page 1 of 6 Patient Information Sheet Left Hemicolectomy This leaflet has been designed to help you to understand what to expect when you are having an operation
Left Hemicolectomy Patient Information Page 1 of 6 Patient Information Sheet Left Hemicolectomy This leaflet has been designed to help you to understand what to expect when you are having an operation
Trauma Center Pre-Review Questionnaire Notes Title 22
 This Pre-Review Questionnaire is designed to accompany the spread sheet appropriate for the Trauma Center being reviewed For use with review of Level III Trauma Center with American College of Surgeons'
This Pre-Review Questionnaire is designed to accompany the spread sheet appropriate for the Trauma Center being reviewed For use with review of Level III Trauma Center with American College of Surgeons'
STAG TRAUMA. Quality Indicators
 STAG TRAUMA Quality Indicators Document Control Document Control Version Quality Indicators V3.3.doc Date Issued 03-09-2013 Author(s) Kirsty Ward Other Related Documents Comments to Angela Khan Document
STAG TRAUMA Quality Indicators Document Control Document Control Version Quality Indicators V3.3.doc Date Issued 03-09-2013 Author(s) Kirsty Ward Other Related Documents Comments to Angela Khan Document
Nurses at War: OR Nursing in Conflict Areas
 42nd Annual Convention & Scientific Meeting Nurses at War: OR Nursing in Conflict Areas BGen Irma I Almoneda AFP (Res) OBJECTIVES: Be familiar with the nature of OR nursing practice in times of conflict;
42nd Annual Convention & Scientific Meeting Nurses at War: OR Nursing in Conflict Areas BGen Irma I Almoneda AFP (Res) OBJECTIVES: Be familiar with the nature of OR nursing practice in times of conflict;
AREA MEDICAL SUPPORT
 CHAPTER 13 AREA MEDICAL SUPPORT 13-1. Combat Zone and Communications Zone Area Medical Support Units which lack an organic HSS capability are provided routine and emergency medical treatment on an area
CHAPTER 13 AREA MEDICAL SUPPORT 13-1. Combat Zone and Communications Zone Area Medical Support Units which lack an organic HSS capability are provided routine and emergency medical treatment on an area
Emergency Medical Team (EMT) Initiative
 Initiative") Emergency Medical Team (EMT) Initiative Regional Chair Asia Pacific 2017 Surge capacity in healthcare during emergencies Groups of health professionals providing direct clinical care to populations affected
Emergency Medical Team (EMT) Initiative Regional Chair Asia Pacific 2017 Surge capacity in healthcare during emergencies Groups of health professionals providing direct clinical care to populations affected
ARLINGTON COUNTY FIRE DEPARTMENT STANDARD OPERATING PROCEDURES
 R SUBJECT: ARLINGTON COUNTY FIRE DEPARTMENT STANDARD OPERATING PROCEDURES Rescue Task Force Response SOP# A.* * /Cat * Initiated APPROVED: James Schw artz Fire Chief Revised A. PURPOSE To establish policies
R SUBJECT: ARLINGTON COUNTY FIRE DEPARTMENT STANDARD OPERATING PROCEDURES Rescue Task Force Response SOP# A.* * /Cat * Initiated APPROVED: James Schw artz Fire Chief Revised A. PURPOSE To establish policies
Example Care Pathways
 Example Care Pathways Introduction The following care pathways have been adapted from those developed to sustain provision of general surgery for children in Scotland. We have tried to avoid being too
Example Care Pathways Introduction The following care pathways have been adapted from those developed to sustain provision of general surgery for children in Scotland. We have tried to avoid being too
Interactive Trauma: Beyond the Moment of Impact
 , About the Speaker MSN, RN, CEN, CPEN, TCRN Bill is a dynamic and energetic speaker whose unique style not only provides insight to his audience but also to creates an engaging and fun atmosphere for
, About the Speaker MSN, RN, CEN, CPEN, TCRN Bill is a dynamic and energetic speaker whose unique style not only provides insight to his audience but also to creates an engaging and fun atmosphere for
Your anaesthetic for a broken hip
 Your anaesthetic for a broken hip Information to help patients, relatives and carers prepare for an anaesthetic for a broken hip First Edition 2014 www.rcoa.ac.uk/patientinfo This leaflet explains what
Your anaesthetic for a broken hip Information to help patients, relatives and carers prepare for an anaesthetic for a broken hip First Edition 2014 www.rcoa.ac.uk/patientinfo This leaflet explains what
The Challenging Scope of the. Improvised Explosive Device Battlespace. Commander ADF Counter-IED Task Force Brigadier Wayne Budd.
 The Challenging Scope of the Improvised Explosive Device Battlespace Commander ADF Counter-IED Task Force Brigadier Wayne Budd Where is the IED threat? Sweden: Suicide Attack, Stockholm, 11 December 2010
The Challenging Scope of the Improvised Explosive Device Battlespace Commander ADF Counter-IED Task Force Brigadier Wayne Budd Where is the IED threat? Sweden: Suicide Attack, Stockholm, 11 December 2010
UPMC Trauma Care System
 A Western PA Initiative 1 UPMC Trauma Care System Altoona (Level II Adult) Children s Hospital (Level I Pediatric) Hamot (Level II Adult) 2 Mercy (Level I Adult, Burn Center) Presbyterian (Level I Adult)
A Western PA Initiative 1 UPMC Trauma Care System Altoona (Level II Adult) Children s Hospital (Level I Pediatric) Hamot (Level II Adult) 2 Mercy (Level I Adult, Burn Center) Presbyterian (Level I Adult)
Use of Blood Products at a US Army Forward Surgical Team in Afghanistan, Feb 2010-Feb 2011
 Heart of America Association of Blood Banks Spring 2012 Meeting Use of Blood Products at a US Army Forward Surgical Team in Afghanistan, Feb 2010-Feb 2011 Presentation by Chris Vanfosson, MAJ, US Army
Heart of America Association of Blood Banks Spring 2012 Meeting Use of Blood Products at a US Army Forward Surgical Team in Afghanistan, Feb 2010-Feb 2011 Presentation by Chris Vanfosson, MAJ, US Army
INSTRUCTOR GUIDE FOR INTRODUCTION TO TCCC-MP
 INSTRUCTOR GUIDE FOR INTRODUCTION TO TCCC-MP 160603 1 1. Introduction to Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Combat Casualty Care is the new standard of care in prehospital
INSTRUCTOR GUIDE FOR INTRODUCTION TO TCCC-MP 160603 1 1. Introduction to Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Combat Casualty Care is the new standard of care in prehospital
Administration of blood components. Denise Watson Patient Blood Management Practitioner 11th January, 2016
 Administration of blood components Denise Watson Patient Blood Management Practitioner 11th January, 2016 Introduction British Committee for Standards in Haematology guidelines Administration process Case
Administration of blood components Denise Watson Patient Blood Management Practitioner 11th January, 2016 Introduction British Committee for Standards in Haematology guidelines Administration process Case
Decade of Service 2000s
 Decade of Service 2000s Immediately following the Sept. 11, 2001, attacks, a DAV mobile service office delivered thousands of articles of clothing and comfort kits to first responders at the Twin Towers.
Decade of Service 2000s Immediately following the Sept. 11, 2001, attacks, a DAV mobile service office delivered thousands of articles of clothing and comfort kits to first responders at the Twin Towers.
RIGHT HEMICOLECTOMY. Patient information Leaflet
 RIGHT HEMICOLECTOMY Patient information Leaflet April 2017 WHAT IS A RIGHT HEMICOLECTOMY? This is an operation that is designed to remove the right side of your large bowel. Part of the large bowel is
RIGHT HEMICOLECTOMY Patient information Leaflet April 2017 WHAT IS A RIGHT HEMICOLECTOMY? This is an operation that is designed to remove the right side of your large bowel. Part of the large bowel is
Title: ED Management of Trauma Patient Protocol
 Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Right Hemicolectomy Surgery
 Right Hemicolectomy Surgery Patient information How to contact us Oncology Department Watford General Hospital West Hertfordshire Hospitals NHS Trust Vicarage Road, Watford, Hertfordshire, WD18 0HB Tel:
Right Hemicolectomy Surgery Patient information How to contact us Oncology Department Watford General Hospital West Hertfordshire Hospitals NHS Trust Vicarage Road, Watford, Hertfordshire, WD18 0HB Tel:
Level 3 Trauma Hospital Criteria
 Level 3 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
Level 3 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
CRITICAL INCIDENT MANAGEMENT
 CRITICAL INCIDENT MANAGEMENT Dr Praveena Ali Principal Medical Officer Ministry of Health Fiji Performance Objectives Describe critical incident characteristics Discuss the characteristics of a mass casualty
CRITICAL INCIDENT MANAGEMENT Dr Praveena Ali Principal Medical Officer Ministry of Health Fiji Performance Objectives Describe critical incident characteristics Discuss the characteristics of a mass casualty
Healthcare Response to a No-Notice Incident: Las Vegas
 Access the recorded webinar here: https://register.gotowebinar.com/ recording/3579578141668518147 Speaker Bios: https://asprtracie.s3.amazonaws.com/ documents/healthcare-response-to-a-no-noticeincident-speaker-bios.pdf
Access the recorded webinar here: https://register.gotowebinar.com/ recording/3579578141668518147 Speaker Bios: https://asprtracie.s3.amazonaws.com/ documents/healthcare-response-to-a-no-noticeincident-speaker-bios.pdf
150-MC-0006 Validate the Protection Warfighting Function Staff (Battalion through Corps) Status: Approved
 Status: Approved") Report Date: 14 Jun 2017 150-MC-0006 Validate the Protection Warfighting Function Staff (Battalion through Corps) Status: Approved Distribution Restriction: Approved for public release; distribution is
Report Date: 14 Jun 2017 150-MC-0006 Validate the Protection Warfighting Function Staff (Battalion through Corps) Status: Approved Distribution Restriction: Approved for public release; distribution is
Hemostatic Damage Control Surgery Combined with Strategic Evacuation in an Intensive Care Airborne Unit Saved Life in a Critical Gun Shot Injury
 Hemostatic Damage Control Surgery Combined with Strategic Evacuation in an Intensive Care Airborne Unit Saved Life in a Critical Gun Shot Injury LtCol Johan Pillgram-Larsen, MD, Chief Consultant in Surgery,
Hemostatic Damage Control Surgery Combined with Strategic Evacuation in an Intensive Care Airborne Unit Saved Life in a Critical Gun Shot Injury LtCol Johan Pillgram-Larsen, MD, Chief Consultant in Surgery,
Recovering from a hip fracture following an accident
 South Tyneside NHS Foundation Trust Recovering from a hip fracture following an accident Providing a range of NHS services in Gateshead, South Tyneside and Sunderland. What is a hip fracture? The hip joint
South Tyneside NHS Foundation Trust Recovering from a hip fracture following an accident Providing a range of NHS services in Gateshead, South Tyneside and Sunderland. What is a hip fracture? The hip joint
Pediatric trauma: experience of a combat support hospital in Iraq B
 Journal of Pediatric Surgery (2007) 42, 207 210 www.elsevier.com/locate/jpedsurg Pediatric trauma: experience of a combat support hospital in Iraq B Rebecca McGuigan a, *, Philip C. Spinella b, Alec Beekley
Journal of Pediatric Surgery (2007) 42, 207 210 www.elsevier.com/locate/jpedsurg Pediatric trauma: experience of a combat support hospital in Iraq B Rebecca McGuigan a, *, Philip C. Spinella b, Alec Beekley
Pre-operative categorization (triaging) of emergency surgical cases. A tool for improving patient care and emergency operating room efficiency
 of emergency surgical cases. A tool for improving patient care and emergency operating room efficiency") Pre-operative categorization (triaging) of emergency surgical cases A tool for improving patient care and emergency operating room efficiency Introduction No national or provincial guidelines exist for
Pre-operative categorization (triaging) of emergency surgical cases A tool for improving patient care and emergency operating room efficiency Introduction No national or provincial guidelines exist for
AUSTRALIAN DEFENCE FORCE PUBLICATION
 AUSTRALIAN DEFENCE FORCE PUBLICATION OPERATIONS SERIES ADFP 53 HEALTH SUPPORT Commonwealth of Australia 1998 This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part
AUSTRALIAN DEFENCE FORCE PUBLICATION OPERATIONS SERIES ADFP 53 HEALTH SUPPORT Commonwealth of Australia 1998 This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part
Experience and Consequences on the Deployments of the Medical Services of the German Army in Foreign Countries Surgical Aspects
 ABSTRACT H. Gerngross, MD Military Hospital Ulm-Germany Oberer Eselsberg 40, D-89075 Ulm Several deployments supported by the german army medical services lead to new experiences concerning personal, training,
ABSTRACT H. Gerngross, MD Military Hospital Ulm-Germany Oberer Eselsberg 40, D-89075 Ulm Several deployments supported by the german army medical services lead to new experiences concerning personal, training,
The operation will take several hours and you will stay in the recovery room until you are ready to return to the ward.
 This booklet is designed to give you information about having a free flap following a lower limb injury. We hope it will answer some of the questions that you, or those who care for you, may have at this
This booklet is designed to give you information about having a free flap following a lower limb injury. We hope it will answer some of the questions that you, or those who care for you, may have at this
RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT
 CALIFORNIA TRAUMA REGULATIONS (Title 22) versus ACS RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT 2006 (Green Book) (Level I/II Trauma Centers Only) Requirement TITLE 22 ACS GREEN BOOK Trauma Medical
CALIFORNIA TRAUMA REGULATIONS (Title 22) versus ACS RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT 2006 (Green Book) (Level I/II Trauma Centers Only) Requirement TITLE 22 ACS GREEN BOOK Trauma Medical
The Israeli Experience
 E.M.S Response To Terrorism The Israeli Experience GUY CASPI Chief MCI Instructor and Director of Exercises and Operational Training MAGEN DAVID ADOM IN ISRAEL Israel National EMS and Blood Services guyc@mda.org.il
E.M.S Response To Terrorism The Israeli Experience GUY CASPI Chief MCI Instructor and Director of Exercises and Operational Training MAGEN DAVID ADOM IN ISRAEL Israel National EMS and Blood Services guyc@mda.org.il
SITUATION REPORT occupied Palestinian territory, Gaza 30 May - 3 June 2018
 TYPE OF CASUALTIES TOTAL (353) SITUATION REPORT occupied Palestinian territory, Gaza 30 May - 3 June 2018 OCCUPIED PALESTINIAN TERRITORY 3 KILLED 525 INJURED 10 TRAUMA STABILISATION POINTS 253 ESSENTIAL
TYPE OF CASUALTIES TOTAL (353) SITUATION REPORT occupied Palestinian territory, Gaza 30 May - 3 June 2018 OCCUPIED PALESTINIAN TERRITORY 3 KILLED 525 INJURED 10 TRAUMA STABILISATION POINTS 253 ESSENTIAL
Hip fracture - DHS. Your broken hip joint - some information
 Page 1 Hip Fracture - DHS Your broken hip joint - some information These notes give a guide to your stay in hospital. They also give an idea about what it will be like afterwards. They do not cover everything.
Page 1 Hip Fracture - DHS Your broken hip joint - some information These notes give a guide to your stay in hospital. They also give an idea about what it will be like afterwards. They do not cover everything.
FOR OFFICIAL USE ONLY UNTIL RELEASED BY THE SENATE ARMED SERVICES COMMITTEE STATEMENT OF COLONEL STEPHEN L. JONES, UNITED STATES ARMY COMMAND SURGEON
 FOR OFFICIAL USE ONLY UNTIL RELEASED BY THE SENATE ARMED SERVICES COMMITTEE STATEMENT OF COLONEL STEPHEN L. JONES, UNITED STATES ARMY COMMAND SURGEON UNITED STATES SOUTHERN COMMAND BEFORE THE 107 TH CONGRESS
FOR OFFICIAL USE ONLY UNTIL RELEASED BY THE SENATE ARMED SERVICES COMMITTEE STATEMENT OF COLONEL STEPHEN L. JONES, UNITED STATES ARMY COMMAND SURGEON UNITED STATES SOUTHERN COMMAND BEFORE THE 107 TH CONGRESS
Tactical Combat Casualty Care for All Combatants August (Based on TCCC-MP Guidelines ) Introduction to TCCC
 Introduction to TCCC") Tactical Combat Casualty Care for All Combatants August 2017 (Based on TCCC-MP Guidelines 170131) Introduction to TCCC Pretest Pre-Test TCCC Web Link to Video What is TCCC and Why Do I Need to Learn About
Tactical Combat Casualty Care for All Combatants August 2017 (Based on TCCC-MP Guidelines 170131) Introduction to TCCC Pretest Pre-Test TCCC Web Link to Video What is TCCC and Why Do I Need to Learn About
SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER. Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow
 SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow I. Clinical Mission of the North Carolina Jaycee Burn Center The clinical
SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow I. Clinical Mission of the North Carolina Jaycee Burn Center The clinical
Answering the Call: Combat Casualty Care Research
 Answering the Call: Combat Casualty Care Research Joint Program Committee on Combat Casualty Care Defense Health Agency Professor of Surgery Uniformed Services University Moral Test Moral test of a nation
Answering the Call: Combat Casualty Care Research Joint Program Committee on Combat Casualty Care Defense Health Agency Professor of Surgery Uniformed Services University Moral Test Moral test of a nation
Active Shooter Guideline
 1. Purpose: This procedure establishes guidelines for Monterey County Public Safety Personnel who respond to Active Shooter Incidents (ASI). The goal is to provide effective rescue and treatment procedures,
1. Purpose: This procedure establishes guidelines for Monterey County Public Safety Personnel who respond to Active Shooter Incidents (ASI). The goal is to provide effective rescue and treatment procedures,
A. Hospital demographics
 A. Hospital demographics 1. Contact details Name of the Hospital Last name of person in charge First name of person in charge City Country 2. Demographics # of inpatient beds # of operating rooms # of
A. Hospital demographics 1. Contact details Name of the Hospital Last name of person in charge First name of person in charge City Country 2. Demographics # of inpatient beds # of operating rooms # of
INTRODUCTION. Section I. SUPPORTING THE BATTLE
 CHAPTER 1 INTRODUCTION Section I. SUPPORTING THE BATTLE 1-1. General a. Warfare has changed significantly since World War II (WW II). The range, accuracy, and lethality of the modern tank gun makes it
CHAPTER 1 INTRODUCTION Section I. SUPPORTING THE BATTLE 1-1. General a. Warfare has changed significantly since World War II (WW II). The range, accuracy, and lethality of the modern tank gun makes it
Auckland District Health Board Summary 1 July 2011 to 30 June 2012 Serious and Sentinel Events
 DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
Right Hemicolectomy. Patient information - General Surgery. Right Hemicolectomy
 Right Hemicolectomy General Surgery Right Hemicolectomy Patient information - General Surgery Introduction This booklet provides information about your operation. Please do not hesitate to ask any questions
Right Hemicolectomy General Surgery Right Hemicolectomy Patient information - General Surgery Introduction This booklet provides information about your operation. Please do not hesitate to ask any questions
History of Trauma Surgery
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-disaster-medicine-and-preparedness/history-of-traumasurgery/1500/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-disaster-medicine-and-preparedness/history-of-traumasurgery/1500/
You have been admitted with a hip fracture
 Hip fracture: Information for patients and relatives You have been admitted with a hip fracture This booklet has been designed by health professionals to provide you and your relatives with the information
Hip fracture: Information for patients and relatives You have been admitted with a hip fracture This booklet has been designed by health professionals to provide you and your relatives with the information
ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221. I. Title Trauma team Activation Protocol/Roles & Responsibilities of the Trauma Team
 Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221 Subject: Trauma Team Activation Protocol/Roles & Responsibilities of the Trauma Team Trauma Coordinator UTMB respects the diverse culture
Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221 Subject: Trauma Team Activation Protocol/Roles & Responsibilities of the Trauma Team Trauma Coordinator UTMB respects the diverse culture
Battlefield Trauma Systems
 Battlefield Trauma Systems Chapter 35 Battlefield Trauma Systems Introduction A trauma system is an organized, coordinated effort in a defined geographic area that delivers the full range of care to all
Battlefield Trauma Systems Chapter 35 Battlefield Trauma Systems Introduction A trauma system is an organized, coordinated effort in a defined geographic area that delivers the full range of care to all
Trauma Readiness Training for Military Deployment: A Comparison Between a U.S. Trauma Center and an Air Force Theater Hospital in Balad, Iraq
 MILITARY MEDICINE, 176, 7:769, 2011 Trauma Readiness Training for Military Deployment: A Comparison Between a U.S. Trauma Center and an Air Force Theater Hospital in Balad, Iraq McCunn Maureen, MD * ;
MILITARY MEDICINE, 176, 7:769, 2011 Trauma Readiness Training for Military Deployment: A Comparison Between a U.S. Trauma Center and an Air Force Theater Hospital in Balad, Iraq McCunn Maureen, MD * ;
Integrated Operations for HighThreat Incidents. (Rescue Task Force) 1/24/2018. Disclaimers. Are We Paying Attention Yet?
 1/24/2018. Disclaimers. Are We Paying Attention Yet?") Integrated Operations for HighThreat Incidents (Rescue Task Force) Geoffrey L. Shapiro Director, EMS & Operational Medicine Training The George Washington University Committee for Tactical Emergency Casualty
Integrated Operations for HighThreat Incidents (Rescue Task Force) Geoffrey L. Shapiro Director, EMS & Operational Medicine Training The George Washington University Committee for Tactical Emergency Casualty
UNCLASSIFIED FY 2009 RDT&E,N BUDGET ITEM JUSTIFICATION SHEET DATE: February 2008 Exhibit R-2
 Exhibit R-2 PROGRAM ELEMENT: 0603729N PROGRAM ELEMENT TITLE: WARFIGHTER PROTECTION ADVANCED TECHNOLOGY COST: (Dollars in Thousands) Project Number & Title FY 2007 Actual FY 2008 FY 2009 FY 2010 FY 2011
Exhibit R-2 PROGRAM ELEMENT: 0603729N PROGRAM ELEMENT TITLE: WARFIGHTER PROTECTION ADVANCED TECHNOLOGY COST: (Dollars in Thousands) Project Number & Title FY 2007 Actual FY 2008 FY 2009 FY 2010 FY 2011
JOINT COMMITTEE TO CREATE A NATIONAL POLICY TO ENHANCE SURVIVABILITY FROM MASS CASUALTY SHOOTING EVENTS HARTFORD CONSENSUS II
 July 11, 2013 JOINT COMMITTEE TO CREATE A NATIONAL POLICY TO ENHANCE SURVIVABILITY FROM MASS CASUALTY SHOOTING EVENTS HARTFORD CONSENSUS II Concept to Action On April 2, 2013, representatives from a select
July 11, 2013 JOINT COMMITTEE TO CREATE A NATIONAL POLICY TO ENHANCE SURVIVABILITY FROM MASS CASUALTY SHOOTING EVENTS HARTFORD CONSENSUS II Concept to Action On April 2, 2013, representatives from a select
EMRTS Cymru Overview
 EMRTS Cymru Overview (Published 07/04/16) 1 Who are we? The Emergency Medical Retrieval and Transfer Service (EMRTS Cymru) is an exciting new service that provides consultantdelivered pre-hospital critical
EMRTS Cymru Overview (Published 07/04/16) 1 Who are we? The Emergency Medical Retrieval and Transfer Service (EMRTS Cymru) is an exciting new service that provides consultantdelivered pre-hospital critical
HOSPITALS TO ENTER PATIENTS INTO THE
 PATIENT CRITERIA FOR HOSPITALS TO ENTER PATIENTS INTO THE TRAUMA SYSTEM 1 THE ALABAMA TRAUMA SYSTEM IS UNIQUE NOT ONLY ARE THE TRAUMA HOSPITALS INSPECTED AND CERTIFIED BUT ALSO THEIR CRITICAL RESOURCES
PATIENT CRITERIA FOR HOSPITALS TO ENTER PATIENTS INTO THE TRAUMA SYSTEM 1 THE ALABAMA TRAUMA SYSTEM IS UNIQUE NOT ONLY ARE THE TRAUMA HOSPITALS INSPECTED AND CERTIFIED BUT ALSO THEIR CRITICAL RESOURCES
Chapter 1. Learning Objectives. Learning Objectives 9/11/2012. Introduction to EMS Systems
 Chapter 1 Introduction to EMS Systems Learning Objectives Define the attributes of emergency medical services (EMS) systems List 14 attributes of a functioning EMS system Differentiate the roles and responsibilities
Chapter 1 Introduction to EMS Systems Learning Objectives Define the attributes of emergency medical services (EMS) systems List 14 attributes of a functioning EMS system Differentiate the roles and responsibilities
Sudden Impact Mass Casualty Incidents Response and Planning. Charles M. Little, DO FACEP University of Colorado Denver
 Sudden Impact Mass Casualty Incidents Response and Planning Charles M. Little, DO FACEP University of Colorado Denver Can Multiple Untriaged/Untreated Battlefield Casualties Happen Here? Fort Hood, TX
Sudden Impact Mass Casualty Incidents Response and Planning Charles M. Little, DO FACEP University of Colorado Denver Can Multiple Untriaged/Untreated Battlefield Casualties Happen Here? Fort Hood, TX
Document Title: Trauma Patient Care in the Emergency Department : Pitfalls to Avoid
 Project: Ghana Emergency Medicine Collaborative Document Title: Trauma Patient Care in the Emergency Department : Pitfalls to Avoid Author(s): Jim Holliman, M.D., F.A.C.E.P. (Uniformed Services University
Project: Ghana Emergency Medicine Collaborative Document Title: Trauma Patient Care in the Emergency Department : Pitfalls to Avoid Author(s): Jim Holliman, M.D., F.A.C.E.P. (Uniformed Services University