THE HOSPICE REGULATORY MERRY-GO-ROUND
|
|
|
- Stephany Bond
- 5 years ago
- Views:
Transcription


1 THE HOSPICE REGULATORY MERRY-GO-ROUND

2 HAVE YOU HAD YOUR ANTIVERT TODAY? 2
3 OBJECTIVES Name a current & proposed change in reimbursement for hospice. Define the impact of not using Debility & Adult Failure to Thrive as primary diagnoses. Describe two potential repercussions to the hospice industry from the growth of managed care in healthcare. Identify the steps that a hospice should take to stabilize their program in this environment. 3

4 WHY IS HOSPICE ON THE ENFORCEMENT RADAR SCREEN?
5 WHY THE INCREASED SCRUTINY FOR HOSPICE? Over 1.5 million Medicare patients per year ALOS continues to grow 71.8 days The number of proprietary hospice programs is increasing Majority of hospice programs are proprietary Percentage of non-cancer patients continues to increase Use of GIP is increasing with longer lengths of stay Expenditures for the Medicare hospice benefit have increased approximately $1 billion per year Source: NHPCO s Facts & Figures 2013 Edition
6 WHY IS HOSPICE ON THE ENFORCEMENT RADAR SCREEN? Data Mining Whistleblowers Budget pressure Audit contractors (ZPIC, MIC, RAC) Law enforcement (DOJ, OIG, Ags, MFCU) have experience with hospice investigations OIG audits & reports

7 INCREASED REGULATORY SCRUTINY 7

8 WHO S LOOKING AT HOSPICE 8
9 MEDICARE CONTRACTORS CA & NV Medicare Administrative Contractor (MAC) National Government Services Comprehensive Error Rate Testing (CERT) Review Contractor (RC) AdvanceMed Corp. Recovery Auditor (RA) HealthDataInsights HDI Zone Program Integrity Contractor (ZPIC) Safeguard Services, LLC
10 MEDICARE CONTRACTORS CA & NV, CONT D State Medicaid Auditors- Medi-Cal DHHS Payment Error Rate Measurement (PERM) Review Contractor (RC) A+ Government Solutions Medicaid Integrity Contractor (MIC) Review MIC AdvanceMed

11 ZONE PROGRAM INTEGRITY CONTRACTORS 11
12 ZPICS ZONE PROGRAM INTEGRITY CONTRACTORS Safeguard Services, LLC California & Nevada Paid on a contractual basis rather than a contingency fee like RAs. Fraud detection and deterrence Statistics sampling and extrapolation of damages 12
13 ZPIC AUDITS ACTIVE IN HOSPICE Focus on: Length of Stay (LOS) Non-CA diagnosis SNF care Readmits after discharge Higher levels of care GIP & Continuous Care Technical and clinical compliance Medical necessity 13
14 HOW ZPIC AUDITS WORK Use data mining to target their investigations They establish a Relevant Time Frame (RTF), then request a sample of clinical records from the RTF All denials associated with the sample are then factored into a Charge Denial Rate (CDR) The CDR (% of ALL denials in sample) may be applied to all claims submitted for ALL patients during the RTF without further record review 14

15 ZPIC TORNADO EFFECT Potential for complete financial devastation Several hospices have had to close due to ZPIC audits 15
16 RANGE OF HOSPICE ZPIC CLAIMS In Safeguard Services, LLC region $0.00 to $112.8 million in hospice repayments Difference was in the eligibility documentation and medical necessity
17 UNIFIED PROGRAM INTEGRITY CONTRACTOR (UPIC) ZPIC & MAC to merge Focus will be on both Medicare & Medicaid integrity issues MAC would take on a broader role in program integrity activities Medicaid Integrity Contractors will be phased out Recovery Auditors will remain in place Medicare & Medicaid data will be a unified database 17

18 FOR WHAT ARE THEY LOOKING? 18
19 UNDERSTANDING ERRORS, WASTE, FRAUD & ABUSE Mistakes Inefficiencies Bending the rules Intentional deception Error Waste Abuse Fraud Incorrect coding Medically unnecessary service Improper billing practices (e.g., upcoding) Billing for services that were not provided 19
20 Subpart A General Provisions and Definitions Subpart B Duration of Benefits Eligibility, Election, Subpart C Conditions of Participation: Patient Care Subpart D Conditions of Participation - Organizational Environment Subpart E - Reserved Subpart F Covered Services Subpart G Care Payment for Hospice

21 THE OFFICE OF INSPECTOR GENERAL 21
22 OIG S FOCUS ON HOSPICE Coverage requirements for hospice patients residing in nursing homes Medicare hospices that focus on nursing facility residents ( high percentage hospices ) Marketing practices with nursing facilities Compliance with Medicaid reimbursement requirements GIP appropriateness Hospital-to-GIP transfers Duplicate drug claims (including non-covered but hospice-related medications)
23 OIG REPORT A JUNE 2012 During CY09 Medicare Part D paid over $33 Million for drugs of hospice patients These drugs included: Analgesics antiemetics laxatives anti-anxiety drugs, as well as prescription drugs used to treat COPD and ALS OIG urged the education of Part D providers, hospices & pharmacies regarding proper hospice medication coverage Require Part D plan sponsors to develop controls to prevent paying for drugs that hospice should be covering 23
24 CMS PART D PROGRAM INTEGRITY MEMO AUGUST 2013 Deduct from pharmacy s payments for analgesics provided to beneficiaries on hospice Pharmacies should seek payment from hospice There is no instruction regarding potentially unrelated analgesics Directs Part D plan sponsors to recoup payments back to 2011 Hospices are beginning to receive notices from pharmacies requesting repayment for analgesics previously paid for by Part D 24
25 WHAT HOSPICES NEED TO DO REGARDING PART D REPAYMENT Check the patient s medical record to determine whether the drugs were related to the terminal illness & indicated on the POC If related, determine if they were provided by & paid for by the hospice If they were related and not paid for, the hospice should reimburse the pharmacy If the drug was unrelated & there is documentation to support why it is not related, share that documentation with the pharmacy & Part D plan sponsor & indicate that the hospice was not the responsible party If you become aware of Part D blocking all drugs due to hospice, alert CHAPCA & NHPCO 25
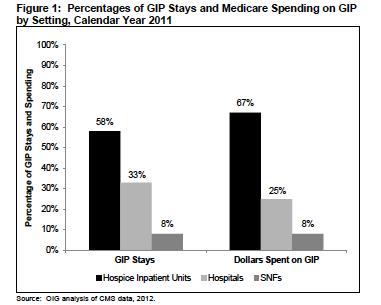
26 OIG ISSUES REPORT ON GIP MAY 3, 2013 Medicare expenditures for GIP in 2011: $1.1 Billion 23% of beneficiaries received GIP during their stay in hospice 33% of beneficiary GIP stays exceeded 5 days 11% lasted 10 days or more 26
27 27
28 28
29 GIP CRACKDOWN The Federal government recently reached a $2.7 million settlement with a hospice for allegedly billing Medicare for GIP when beneficiaries actually received routine home care, which has a lower reimbursement rate 29
30 OIG S CONCERN OVER LACK OF GIP 25% of hospices provided little to no GIP, respite, or continuous care 429 hospices only provided routine homecare in 2011 These hospices may become the focus of scope-of-service and quality concerns Companion study by OIG on medical record review of 2012 claims and clinical eligibility of GIP 30
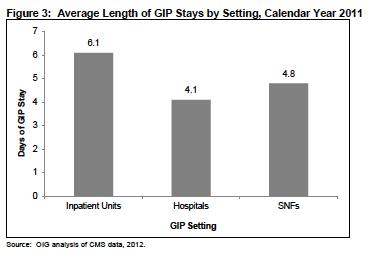
31 OIG REQUESTS GIP RECORDS Spring many hospice providers received requests for GIP records Random sample of records from several hundred providers throughout the country Includes GIP provided in hospitals, SNFs, and in hospice inpatient units The purpose of the review is to assess the appropriateness of GIP provided in different settings Evaluating GIP in hospice IPUs, SNFs & hospitals 31

32 PAYMENT RELATED RISK 32

33 MAJOR RISK AREAS Technical Risks Clinical Risks 33
34 MAJOR TECHNICAL RISKS Election Statement Certification & Recertification Plan of Care 34

35 MAJOR CLINICAL RISKS Eligibility for hospice & General Inpatient/Continuous Care Discharges & Revocations Related vs. Not Related to the terminal illness 35

36 CERTIFICATION OF TERMINAL ILLNESS 36
37 CAUTIONS REGARDING THE TECHNICAL REQUIREMENTS FOR CERTIFICATION Certification of Terminal Illness and Recertification Adhere to oral and written CTI requirements Example - Hospice admits 6/1 and fails to obtain oral certs, written certs are not received from both physicians until 6/22 - Therefore, cannot bill 6/1-6/21 Physicians must date their own signatures Print physician name under signature or have a signature identification log 37
38 ISSUES REGARDING THE TECHNICAL REQUIREMENTS FOR CERTIFICATION Physician Narrative Statement The physician must include a brief narrative explanation of the clinical findings that supports a life expectancy of 6 months or less, as evidenced by Only the certifying physician can complete the narrative Be careful if the F2F is done between days out, that the narrative is not written and recertification signed any earlier than 15 days prior to the start of the benefit period F2F must occur prior to the physician recertification 38
39 DISCHARGE DUE TO MISSED F2F Patient not considered terminally ill for Medicare CMS requires Hospice to discharge the patient but can re-admit once the F2F encounter occurs CMS also expects hospice to continue to care for the patient at its own expense until the required F2F occurs Once the F2F and recertification is completed, the pt may then be readmitted to hospice The patient starts a new benefit period The hospice generates new orders, initial and comprehensive assessments and care plans 39
40 CLINICAL ELIGIBILITY D O C U M E N T I N G M E D I C A L N E C E S S I T Y F O R H O S P I C E C A R E 40

41 #1 Hospice Risk Area Does the patient meet clinical criteria? 41
42 GREATEST RISK, THE TRIPLE THREAT Long Length of Stay Non-CA Diagnoses Facility Based Care 42
43 ALLEGED LACK OF MEDICAL NECESSITY On February 15, 2012, hospice company XYZ, Inc., agreed to pay $25 million to resolve allegations that it submitted false claims to federal programs for medically unnecessary continuous home care services billed at a higher rate than routine care services. As a result, XYZ, Inc., entered into a Corporate Integrity Agreement (CIA) with HHS/OIG
44 MEDICAL NECESSITY = REASONABLE & NECESSARY Documentation is integral to supporting the medical necessity for the service The most clear cut way to support medical necessity in an audit is documenting medical decision-making Complete documentation of the IDG thought process, including issues being ruled out will support medical necessity and higher levels of services billed Not furnished primarily for the convenience of the patient, the attending physician, or another physician or supplier 44
45 MEDICAL NECESSITY For medical review purposes Each claim billed stands alone & requires sufficient support of the ongoing medical necessity of the hospice services being provided Medical necessity is identified in the initial and ongoing comprehensive assessments The plan of care should be developed based on the initial & updated assessments All interventions must be in direct response to the established plan of care 45
46 DON T LET THIS HAPPEN TO YOU There was no indication in the submitted documentation that the beneficiary s life expectancy was 6 months or less. There was no documentation of co morbidities that would have contributed to a short life expectancy. The documentation shows that the patient required full time custodial care, but not the services of Hospice. -Comments extracted from a de-identified ZPIC finding

47 DEBILITY & ADULT FAILURE TO THRIVE F Y H O S P I C E W A G E I N D E X A N D P A Y M E N T R A T E U P D A T E ; [ CMS P] 47
48 DEBILITY & ADULT FAILURE TO THRIVE CMS clarified that debility and adult failure to thrive SHOULD NOT be used as principal hospice diagnoses on the hospice claim form Claims will be returned to the provider (RTP) beginning Oct. 1, 2014 for a more definitive principal diagnosis Debility and adult failure to thrive could be listed on the hospice claim as secondary or related comorbid diagnoses CMS expects providers to code the most definitive, contributory terminal diagnosis in the principal diagnosis field with all other related conditions in the additional diagnoses fields 48
49 ICD-9 CODES TO AVOID USING AS THE TERMINAL DIAGNOSIS: Abnormal weight loss Failure to thrive Adult failure to thrive Malaise and fatigue Debility, unspecified Cachexia Other ill-defined conditions Other unknown & unspecified cause of morbidity or mortality Along with any other code in the 780 through 799 rangebut they may be listed as RELATED conditions
50 IDENTIFY THE PRINCIPLE HOSPICE DIAGNOSIS Discuss patient s condition with the physician or medical director to determine the correct primary diagnosis And document: Secondary conditions: Caused by, the primary hospice diagnosis (e.g., intractable HTN in a patient with renal CA) Related Co-morbid conditions: Separate conditions that directly contribute to the burden of illness and resulting 6-month life expectancy Debility and AFTT can be utilized as secondary or related co-morbid conditions as they are likely to contribute to a life expectancy of 6 months or less and should be considered in determining eligibility 50
51 IDENTIFY THE PRINCIPLE HOSPICE DIAGNOSIS Unrelated Comorbid conditions: unrelated to, or separate and distinct from, the primary hospice diagnosis These may add to the burden of illness and should be identified and documented in the hospice record They should not be included on the hospice claims form 51
52 All Diagnoses Primary Diagnosis or Co-Morbid Conditions that Influence Prognosis Listed on Claim Pay Co-Morbid Conditions that Do Not Influence Prognosis Not Listed on Claim Don t Pay
53 PRIOR PRIMARY DIAGNOSIS - DEBILITY Primary and Secondary Diagnosis Primary Code: 332.0, Parkinson s disease Other (secondary) codes: , dysphagia Other codes: , weight loss Other codes: 458.0, orthostatic hypotension Other codes: V12.61, history of pneumonia Other codes: V85.0, adult BMI below 19 53
54 DIAGNOSIS REPORTING REQUIREMENTS ON CLAIM FORM List the primary hospice diagnosis List all related other diagnoses Do not list unrelated co-morbidities But be sure to list them in the clinical record The hospice claim includes a field for the patient s principal hospice diagnosis, and allows for up to 17 additional diagnoses on the paper UB-04 claim, and up to 24 additional diagnoses on the 837I 5010 electronic claim
55 WHAT DOES HOSPICE NEED TO DO? New Admissions Cease the use of debility, AFTT & other ill-defined conditions as a primary hospice diagnosis for newly admitted patients Select a primary diagnosis that is most contributory to the patient s terminal disease trajectory and requires end-of-life palliative interventions Use other health conditions (including debility, AFTT, etc) to support the prognosis as needed 55
56 WHAT DOES HOSPICE NEED TO DO? New Admissions (Cont d) Include all prognosis-impacting conditions on the claims form Cover all medications & treatments for diagnoses supporting the 6 month prognosis If a medication is unrelated, have the medical director or hospice physician document why in the record 56
57 WHAT DOES HOSPICE NEED TO DO? Current Patients with a Primary Diagnosis of Debility or AFTT Perform a census analysis to identify all patients that fall into the ICD-9 category of Symptoms, Signs and Ill-defined conditions (ICD ) Have your medical director or hospice team physician review each patient s clinical record to identify an alternative primary diagnosis 57
58 TIPS IN SELECTING THE PRIMARY DIAGNOSIS Use the plan of care (POC) to see what body system requires the greatest amount of palliative interventions Use the drug profile to identify the issues being treated Ask yourself, if the patient died tomorrow, what cause of death would be listed on the death certificate 58
59 CHANGING THE PRIMARY DIAGNOSIS Obtain a physician order for the new diagnosis Obtain a new physician note that supports eligibility for the new diagnosis Ensure that the new diagnosis is supported by documentation in the clinical record Develop a new POC based on an updated comprehensive assessment Update the drug profile with appropriate designations of related/covered or unrelated/noncovered Have hospice physician document the reason for non-related medications Change billing codes 59
60 CHANGING THE PRIMARY DIAGNOSIS It is not necessary to cancel any claims already processed with the original diagnosis The diagnosis can be changed on the next claim, or an adjustment may be made to a prior claim if needed If the patient has no clear alternate diagnosis that can be supported by clinical documentation, and the POC has not changed over time to reflect end-of-life symptom management, consideration should be given to discharge the patient 60
61 EDUCATIONAL NEEDS FOR CHANGING THE PRIMARY DIAGNOSIS Educate all attending physicians, explaining the reason for the changes & involve them in the determination of the primary diagnosis Discuss these changes with staff and referral sources, including contracted nursing facilities and assisted living facilities Be cautious of physicians finding the next easiest diagnosis to assign their hospice patient referrals (e.g. Alzheimer s) as the diagnosis must meet the LCD guidelines 61
62 ICD-10 ICD 10 will replace the ICD 9 on October 1, 2014 A critical issue associated with the transition to ICD 10 involves the matter of crosswalking between ICD 9 and ICD 10 code sets Obtain a 2014 coding book with the conversion tables Send someone from your agency to training. Many of the rules will be different 62
63 ICD-10 Even veteran coders will need to start from scratch Coders need to brush up on anatomy & physiology as diagnosis coding will require more specificity of site of disease processes, including site and side of body for wound and fracture codes ICD-10 is owned by the World Health Organization, they will be providing guidance on use of ICD-10 codes It may be time to consider an external contracted coding company to assist in coding and billing 63
64 ICD-10 RESOURCES General ICD-10 information tm ICD-10-CM files, information, and General Equivalence Mappings (GEM) between ICD-10- CM and ICD-9-CM m.htm CMS Educational Tools
65 DISCHARGE NOTIFICATION ABN / NOMNC / DENC 65
66 FORM ACRONYMS ABN Advance Beneficiary Notice of Noncoverage - CMS-R-131 Form (03/11) NOMNC Notice of Medicare Non Coverage - CMS Form (revised and effective on May 1, 2012) DENC Detailed Explanation of Non Coverage - CMS Form (revised and effective on May 1, 2012) 66

67 What Notices and Why? Generic NOMNC When Hospice services are being terminated. Services will not continue no further action Services will continue ABN is provided DENC if appealing
68 WHEN TO ISSUE AN ABN 1. Ineligibility because the patient is no longer terminally ill 2. Specific items or services that are billed separately from the hospice per diem rate, such as physician services are not reasonable and necessary 3. The hospice level of care (GIP & Continuous Care) is no longer medically necessary should only issue if patient/representative refuse to decrease level of care and wish to appeal 68
69 CR DEMAND BILLING OF GIP LEVEL OF CARE CMS Publication Claims Processing Manual, Chapter 1 General Billing Requirements, section Outpatient Billing with an ABN (Occurrence Code 32) Occurrence Code 32 is reported on the claim with the date the ABN was provided to the beneficiary The services in question are submitted as covered services and when billing for both ABN related and non- ABN related services, the hospice appends the GA modifier to the line item(s) related to the ABN Medicare may require suspension of any claims using occurrence code 32 for medical review of covered charges associated with an ABN If the GIP coverage is denied the MAC is directed to pay at the Routine Home Care rate 69
70 WHEN ABNS ARE NOT REQUIRED FOR HOSPICE 1. Revocations 2. Transfers 3. Respite care beyond 5 consecutive days 4. Emergent care not approved/coordinated by hospice 5. Medications, DME, or supplies that may be related to the terminal illness; are deemed not part of the hospice palliative plan of care 70
71 ABN/NOMNC/DENC RESOURCES CMS, Change Request 7903, Expedited Determinations for Provider Service Terminations. May 24, Guidance/Guidance/Transmittals/Downloads/R2711CP.pdf CMS, Medicare Claims Processing Manual, Chapter 30 - Financial Liability Protections, page Guidance/Guidance/Manuals/downloads/clm104c30.pdf 71
72 HOSPICE QUALITY REPORTING PROGRAM Hospices should currently be collecting data for the QAPI Structural Measure and NQF 0209/Pain measure for all of 2013 Data submission deadline for 2013 data is April 1, % market basket financial penalty FY 2015 if not submitted In calendar year 2014: the QAPI structural measure and NQF #0209/Pain measure will be discontinued. Reminder: CoP QAPI requirements remain the same 72
73 HOSPICE ITEM SET (HIS) Proposed to begin the use and submission of HIS on July 1, 2014 Electronic data submission on admission and discharge of every patient on or after 7/1/ new quality measures Hospices who fail to report quality data via the HIS system in 2014 will have a 2% market basket reduction for FY2016 (10/1/2015) 73
74 HOSPICE ITEM SET MEASURES NQF #1617 Patients Treated with an Opioid who are given a bowel regimen NQF #1634 Pain Screening NQF #1637 Pain Assessment NQF #1638 Dyspnea Treatment NQF #1639 Dyspnea Screening NQF #1641 Treatment Preferences NQF #1647 Beliefs/Values Addressed (if desired by the patient) (modified) 74
75 MEASURES Specifications of proposed measures are found at: National Quality Forum (NQF) Final Report on Palliative and End of Life Measures d_end-of-life_care.aspx#t=1&s=&p= 75
76 EXPERIENCE OF CARE SURVEY Post-death family caregiver survey Proposed start date: CY2015 January March 2015 dry run for at least 1 month to test conditions before public reporting of the data Mandatory compliance with continuous monthly data beginning April 1, 2015 through December 2015 for FY 2017 payment update Fewer than 50 deaths in 2014: exempt 76
77 HOSPICE EXPERIENCE OF CARE SURVEY 3 versions determined by location of death: Home Nursing Home Inpatient care Focuses on the patient/caregiver experience of care, rather than patient satisfaction Includes questions about provider communication and care plus patient and family characteristics Hospices must contract with a vendor for survey administration and quarterly data submission 77
78 CR 8358 ADDITIONAL DATA REPORTING REQUIREMENTS FOR HOSPICE CLAIMS Hospice staff visit data for GIP level of care Skilled nursing facilities (site of service HCPCS code Q5004) Hospitals (site of service HCPCS codes Q5005, Q5007, Q5008) NPI Number of Facility where Hospice Patient is Receiving Services Visits on Date of Death Injectable and Non-injectable Prescription Drugs Infusion Pumps 78
79 HOSPICE PAYMENT REFORM Current models being studied by Abt Associates: MedPAC recommended U-shaped model Tiered model Short stay add-on, similar to home Health Low Utilization Payment Amount (LUPA) Case-mix model Rebasing the Routine HC rate Site of service adjustment for hospice patients in nursing facilities 79
80 CMS HEALTHCARE INNOVATION AWARDS CMS is soliciting proposals Under Category 1 - Models that are designed to rapidly reduce Medicare, Medicaid, and/or CHIP costs in outpatient and/or post-acute settings CMS specifically stated during a recent Webinar that proposals designed to reduce hospice spending were being sought What is CMS goal? To further limit access to hospice care? Are they seeking ways to change the payment structure? Could it actually lead to greater access to hospice? The stated goal of this round of funding is to propose new payment and service delivery models that will provide better health, better health care, and lower costs through improved quality 80
81 FINAL LTC RULES FOR HOSPICE CARE M E D I C A R E & M E D I C A I D : R E Q U I R E M E N T S F O R L T C F A C I L I T I E S ;, H O S P I C E S E R V I C E S ; F I N A L R U L E 78 F E D E R A L R E G I S T E R ( 6 / 2 7 / 1 3 ) P P
82 LTC FACILITY FINAL RULE ON HOSPICE CARE IN NURSING HOMES Effective 8/26/13 Provided complimentary regulations for the LTC industry regarding how hospice patient s care should be provided in a LTC facility Includes the following requirements: Contract language Collaboration Plan of Care Training Update your contracts & training materials with the new requirements 82
83 HIPAA OMNIBUS RULE Published 1/25/13 Compliance deadline was 9/23/13 Items needing hospice action include: Conduct a risk analysis of security of PHI Assure encryption specifications Update policies & procedures Update staff training 83

84 CALIFORNIA UPDATES 84
85 CDPH - NEW CA HOSPICE FACILITY LICENSE Effective Jan 1, 2013 Hospice inpatient units/homes were previously licensed as CLHF, Special Hospital: Hospice or SNF Allows a licensed and Medicare certified hospice provider to operate a hospice inpatient facility Providers will have the option to operate a hospice facility within the physical plant of another licensed facility; hospital or SNF If the facility represents itself to be a hospice and uses the word hospice facility, or hospice home, it must be licensed as a hospice facility 85
86 HOSPICE FACILITY LICENSE Max of 24 beds Must have an RN 24 hr./day Only a licensed hospice can apply for a hospice facility license A HHA licensed hospice must first apply for a hospice program license Licensing fee will be the same as CLHF for the 1 st year, $312/bed Hospices are required to follow Medicare COP Hospices that provides inpatient care directly 86
87 HOSPICES OPERATING CLHF Hospices that operate a CLHF may continue to do so if they remove hospice from the name and do not represent themselves as a hospice If GIP is going to be provided, the hospice must be licensed as a hospice facility Hospices may convert to new license by submitting an application and fee to Central Applications Unit (CAU) of CDPH. Once the completed application has been approved and surveys are performed (if required), the CDPH will issue the license accordingly 87
88 NEW HOSPICE FACILITIES All new facilities that are in process of building a Hospice facility must apply for an initial license This is causing some confusion with the District Offices and CHAPCA is working with CDPH to clarify the process Hospices will need to submit their applications directly to the District Office of CDHP for review and approval of the application CAU will not process these applications 88
89 CDHS - UPDATED MEDI-CAL ALL PLAN LETTER Due to be published 10/28/13 Clarifies the following: There is no pre-authorization for hospice services, except for the GIP level of care Room & board (R & B) is to be billed through the hospice and is not considered LTC, therefore the Plan is responsible for payment for R & B the entire length of hospice election Plans must pay hospice at the Medicaid published rates, at a minimum Identifies the Concurrent Hospice & Curative Care for Children program as well as the California Children Services for Life Limiting Condition program 89
90 THE HEALTHCARE ENVIRONMENT Healthcare Reform Budget crisis Sequestration & decreasing reimbursements Expanding managed care products Dual eligible demonstration projects Increasing mergers and acquisitions Increasing regulations and reporting requirements An aging society Decreasing availability of healthcare personnel 90

91 WHERE ARE THE GOOD OLE DAYS 91


92 NO WORRIES, I HAVE EVERYTHING UNDER CONTROL 92

93 ALL SYSTEMS NEED MAINTENANCE 93
94 STEPS TO PROTECT YOUR PROGRAM 94
95 FALSE CLAIMS ACT Providers must report and return overpayments (accidentally or otherwise) to Medicare/Medi-Cal within 60 days of identifying the overpayment Under PPACA, failure to return an overpayment within 60 days exposes a provider to liability under the FCA 95
96 AUDIT CURRENT RECORDS Do not do retro-active review, you will be held to the self-reporting rules Hold current claims while reviewing current documentation Adjust claims based on the audit results Evaluate: Technical compliance Clinical eligibility Medical necessity Higher levels of care Proper discharge notification 96
97 COMPLIANCE Follow the Medicare Statutes, Regulations (Conditions of Coverage & Conditions of Participation) Admit patients who are eligible and qualify under the LCD guidelines Cease the use of Debility & AFTT Document progressive decline Follow certification and recertification regulations carefully, including required physician narratives and face-to-face encounters for the 3 rd and subsequent benefit periods Assure your physician narratives are legible & clinically support the 6-month terminal prognosis 97
98 COMPLIANCE CONT D Update contracts for HIPAA and LTC rule compliance Assure that your NOMNC, ABN & DENC are provided to patients in a timely manner Train staff well on all of the changing rules and regulations Monitor all mail Respond to ADRs and Audits timely & thoroughly If you become aware of an overpayment, repay it within 6o days Always alert your attorney of audits & overpayments Have strong QAPI & Corporate compliance programs 98

99 99

100 QUESTIONS 100
101 PRESENTER Holly Swiger, PhD, MPH, PHN, RN Swiger Consulting at Stellar Concepts, Inc. 101
2014 HOSPICE REGULATORY UPDATE
 2014 HOSPICE REGULATORY UPDATE Holly Swiger, PhD, MPH, PHN, RN Stellar Concepts, Inc. WHISTLEBLOWERS MARCH 13, 2014 Hospice company to pay $3.92 million to settle false claims allegations; two whistleblowers
2014 HOSPICE REGULATORY UPDATE Holly Swiger, PhD, MPH, PHN, RN Stellar Concepts, Inc. WHISTLEBLOWERS MARCH 13, 2014 Hospice company to pay $3.92 million to settle false claims allegations; two whistleblowers
General Inpatient Level of Care: Managing Risks
 General Inpatient Level of Care: Managing Risks THE CAROLINAS CENTER, 2015 1 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org THE CAROLINAS
General Inpatient Level of Care: Managing Risks THE CAROLINAS CENTER, 2015 1 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org THE CAROLINAS
Hospice House Network Inpatient Conference
 Hospice House Network Inpatient t Conference Trends & Recent Developments in Hospice General Inpatient Care Policy and Enforcement June 7, 2013 1 www.morganlewis.com Presented by Howard J. Young, Esq.
Hospice House Network Inpatient t Conference Trends & Recent Developments in Hospice General Inpatient Care Policy and Enforcement June 7, 2013 1 www.morganlewis.com Presented by Howard J. Young, Esq.
Automating documentation helps hospice agencies withstand greater scrutiny
 White Paper Automating documentation helps hospice agencies withstand greater scrutiny Documenting care plan, procedures key to staying in regulatory compliance Abstract The importance of strong documentation
White Paper Automating documentation helps hospice agencies withstand greater scrutiny Documenting care plan, procedures key to staying in regulatory compliance Abstract The importance of strong documentation
4/20/2015. NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals. Today s Objectives. Background
 NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Consulting Services Pamela Meliso, JD, MPH Director of Consulting Services Today
NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Consulting Services Pamela Meliso, JD, MPH Director of Consulting Services Today
The Concerns. Hospice Care in The Nursing Home NHPCO MLC All Rights Reserved 1.
 Hospice Care in The Nursing Home Navigating The Regulatory Challenges Roseanne Berry, MSN, RN Consultant/Educator R&C Healthcare Solutions & Hospice Fundamentals 480 650 5604 roseanne@rchealthcaresolutions.com
Hospice Care in The Nursing Home Navigating The Regulatory Challenges Roseanne Berry, MSN, RN Consultant/Educator R&C Healthcare Solutions & Hospice Fundamentals 480 650 5604 roseanne@rchealthcaresolutions.com
Medical Review: Past, Present and Future
 Medical Review: Past, Present and Future HPCAI Fall Conference Annette Lee of Provider Insights, Inc. 11/5/2013 1 Progressive Corrective Action (PCA) Process designed by CMS, ensures a logical, fair methodology
Medical Review: Past, Present and Future HPCAI Fall Conference Annette Lee of Provider Insights, Inc. 11/5/2013 1 Progressive Corrective Action (PCA) Process designed by CMS, ensures a logical, fair methodology
Tracey L. Klein, J.D
 Heather L. Fields, CHC, CCEP 414-298-8166 hfields@reinhartlaw.com Tracey L. Klein, J.D. 414-298-8156 tklein@reinhartlaw.com Karla H. Pinkerton, J.D., MPH 608-229-2238 kpinkerton@reinhartlaw.com Heather
Heather L. Fields, CHC, CCEP 414-298-8166 hfields@reinhartlaw.com Tracey L. Klein, J.D. 414-298-8156 tklein@reinhartlaw.com Karla H. Pinkerton, J.D., MPH 608-229-2238 kpinkerton@reinhartlaw.com Heather
Responding to Today s Health Care Regulatory Environment
 Responding to Today s Health Care Regulatory Environment St. Joseph s Health Michael R. Holper SVP, Compliance and Audit Services October 26, 2016 2014 Trinity Health. All Rights Reserved. 1 We operate
Responding to Today s Health Care Regulatory Environment St. Joseph s Health Michael R. Holper SVP, Compliance and Audit Services October 26, 2016 2014 Trinity Health. All Rights Reserved. 1 We operate
HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc.
 HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. www.targetedprobe&educate.com Targeted Probe and Educate October 1, 2017 Targets providers based on data Can
HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. www.targetedprobe&educate.com Targeted Probe and Educate October 1, 2017 Targets providers based on data Can
ELIGIBILITY & CERTIFICATION THE CONTINUING SAGA
 1 ELIGIBILITY & CERTIFICATION THE CONTINUING SAGA Hospice Fundamentals Charlene Ross, MSN, MBA, RN Consultant / Educator 2 What You Will Learn Today The regulatory requirements of certification, recertification
1 ELIGIBILITY & CERTIFICATION THE CONTINUING SAGA Hospice Fundamentals Charlene Ross, MSN, MBA, RN Consultant / Educator 2 What You Will Learn Today The regulatory requirements of certification, recertification
Annual Leadership Institute August 25, Triple Check: A Process for Preventing False Claims
 Annual Leadership Institute August 25, 2016 Triple Check: A Process for Preventing False Claims 1 Your presenter today is: Sophie A. Campbell, MSN, RN, CRRN, RAC-CT, CNDLTC Director, Clinical Advisory
Annual Leadership Institute August 25, 2016 Triple Check: A Process for Preventing False Claims 1 Your presenter today is: Sophie A. Campbell, MSN, RN, CRRN, RAC-CT, CNDLTC Director, Clinical Advisory
10/22/2012. Discharge, Revocation and Transfer: Process, ABN and Appeals. Discharge the regulations. Objectives for Today s Session
 Discharge, Revocation and Transfer: Process, ABN and Appeals Jennifer Kennedy, MA, BSN, CHC, LNC National and Palliative Care Organization Patricia Smith Putzbach, RN, BSN, MBA, CHPN Life Choice Discharge
Discharge, Revocation and Transfer: Process, ABN and Appeals Jennifer Kennedy, MA, BSN, CHC, LNC National and Palliative Care Organization Patricia Smith Putzbach, RN, BSN, MBA, CHPN Life Choice Discharge
Using SNF Data to Manage Federal & State Audit Initiatives
 Using SNF Data to Manage Federal & State Audit Initiatives 2012 OIG & GAO Reports In 2009 OIG estimated that 47% of claims had misreported information on the MDS that caused significant errors in Billing
Using SNF Data to Manage Federal & State Audit Initiatives 2012 OIG & GAO Reports In 2009 OIG estimated that 47% of claims had misreported information on the MDS that caused significant errors in Billing
State of California Health and Human Services Agency Department of Health Care Services
 State of California Health and Human Services Agency Department of Health Care Services TOBY DOUGLAS Director EDMUND G. BROWN JR. Governor DATE: OCTOBER 28, 2013 ALL PLAN LETTER 13-014 SUPERSEDES ALL PLAN
State of California Health and Human Services Agency Department of Health Care Services TOBY DOUGLAS Director EDMUND G. BROWN JR. Governor DATE: OCTOBER 28, 2013 ALL PLAN LETTER 13-014 SUPERSEDES ALL PLAN
MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY
 MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY On April 29, 2013, the Centers for Medicare & Medicaid
MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY On April 29, 2013, the Centers for Medicare & Medicaid
STATE HOSPICE ORGANIZATION AND PALMETTO GBA COALITION MEETING SUMMARY
 STATE HOSPICE ORGANIZATION AND PALMETTO GBA COALITION MEETING SUMMARY For meeting held on August 19, 2010 Included in this report: NCLOS audits update on status Various other audit types (ZPIC) Palmetto
STATE HOSPICE ORGANIZATION AND PALMETTO GBA COALITION MEETING SUMMARY For meeting held on August 19, 2010 Included in this report: NCLOS audits update on status Various other audit types (ZPIC) Palmetto
6/25/2013. Knowledge and Education. Objectives ZPIC, RAC and MAC Audits. After attending this presentation, the attendees will be able to :
 Objectives ZPIC, RAC and MAC Audits Approach After attending this presentation, the attendees will be able to : 1. Understand the different types of audits related to reimbursement: ZPIC, RAC, and MAC
Objectives ZPIC, RAC and MAC Audits Approach After attending this presentation, the attendees will be able to : 1. Understand the different types of audits related to reimbursement: ZPIC, RAC, and MAC
Hospices Under the Microscope: Are You Prepared for ZPICs? Medicare Integrity Programs. Objectives. Fraud or Abuse? 3/3/2014
 Hospices Under the Microscope: Are You Prepared for ZPICs? Paula G. Sanders, Esquire Principal & Chair Health Care Practice Post & Schell, PC Diane Baldi, RN CHPN Chief Executive Officer Hospice of the
Hospices Under the Microscope: Are You Prepared for ZPICs? Paula G. Sanders, Esquire Principal & Chair Health Care Practice Post & Schell, PC Diane Baldi, RN CHPN Chief Executive Officer Hospice of the
The Monthly Publication of the National Hospice and Palliative Care Organization
 The Monthly Publication of the National Hospice and Palliative Care Organization Print-friendly PDF From September 2012 Issue A Hospice Provider s Guide to Live Discharges By Jennifer Kennedy, MA, BSN,
The Monthly Publication of the National Hospice and Palliative Care Organization Print-friendly PDF From September 2012 Issue A Hospice Provider s Guide to Live Discharges By Jennifer Kennedy, MA, BSN,
Medicare Regulations and Rules Update What Should You Know?
 Medicare Regulations and Rules Update What Should You Know? Presenters: Gary Massey, CPA & Emily Wetsel, CPA Investment advisory services are offered through CliftonLarsonAllen Wealth Advisors, LLC, an
Medicare Regulations and Rules Update What Should You Know? Presenters: Gary Massey, CPA & Emily Wetsel, CPA Investment advisory services are offered through CliftonLarsonAllen Wealth Advisors, LLC, an
NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals
 NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Home Care & Hospice Services Pamela Meliso, JD, MPH Director of Consulting &
NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Home Care & Hospice Services Pamela Meliso, JD, MPH Director of Consulting &
Objectives. The Alphabet Soup Of Hospice Scrutiny
 Leadership And The Interdisciplinary Group: Overcoming Organizational Challenges In A Time of Change Alphabet Soup For The Hospice Soul: Understanding The Impact Of RHHI, MAC, RAC, CMS, OIG, FBI and DOJ
Leadership And The Interdisciplinary Group: Overcoming Organizational Challenges In A Time of Change Alphabet Soup For The Hospice Soul: Understanding The Impact Of RHHI, MAC, RAC, CMS, OIG, FBI and DOJ
Medicare Part A Update
 Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
HOMECARE AND HOSPICE REIMBURSEMENT
 Hospice Modeling Hospice Changes to Prepare for Medicare Reimbursement and Care Delivery Reform Robert J. Simione Managing Principal Simione Healthcare Consultants, LLC HOMECARE AND HOSPICE REIMBURSEMENT
Hospice Modeling Hospice Changes to Prepare for Medicare Reimbursement and Care Delivery Reform Robert J. Simione Managing Principal Simione Healthcare Consultants, LLC HOMECARE AND HOSPICE REIMBURSEMENT
The OIG and Hospice in Nursing Facilities: Past, Present and Future
 The OIG and Hospice in Nursing Facilities: Past, Present and Future Heather P. Wilson, Ph.D. Weatherbee Resources, Inc. Howard Young, Esq. Morgan Lewis & Bockius, LLP March 30, 2012 Objectives Name three
The OIG and Hospice in Nursing Facilities: Past, Present and Future Heather P. Wilson, Ph.D. Weatherbee Resources, Inc. Howard Young, Esq. Morgan Lewis & Bockius, LLP March 30, 2012 Objectives Name three
CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness. October 12, 2009
 Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness October 12, 2009 Betty B. Bibbins, MD, CHC, FACOG, C-CDI, C CDI, CPEHR, CPHIT President & Chief
Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness October 12, 2009 Betty B. Bibbins, MD, CHC, FACOG, C-CDI, C CDI, CPEHR, CPHIT President & Chief
THE ART OF DIAGNOSTIC CODING PART 1
 THE ART OF DIAGNOSTIC CODING PART 1 Judy Adams, RN, BSN, HCS-D, HCS-O June 14, 2013 2 Background Every health care setting has gone through similar changes in the need to code more thoroughly. We can learn
THE ART OF DIAGNOSTIC CODING PART 1 Judy Adams, RN, BSN, HCS-D, HCS-O June 14, 2013 2 Background Every health care setting has gone through similar changes in the need to code more thoroughly. We can learn
Connecticut Medical Assistance Program. Hospice Refresher Workshop
 Connecticut Medical Assistance Program Hospice Refresher Workshop Training Topics What s New in 2015? Electronic Messaging Claim Adjustments Messages Archived Proposed Changes in Hospice Rates Fiscal Year
Connecticut Medical Assistance Program Hospice Refresher Workshop Training Topics What s New in 2015? Electronic Messaging Claim Adjustments Messages Archived Proposed Changes in Hospice Rates Fiscal Year
Medicare Noncoverage Notices
 March 2014 This job aid is intended to assist home health and hospice clinicians in: Understanding and complying with regulations for issuing required Medicare notices at the time of termination and change
March 2014 This job aid is intended to assist home health and hospice clinicians in: Understanding and complying with regulations for issuing required Medicare notices at the time of termination and change
Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule
 Calendar Year (CY) 2013 Final Rule") Last updated 11/13/12 Contact: Advocacy@apta.org Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule Introduction COMPREHENSIVE SUMMARY On November 2, 2012, the Centers
Last updated 11/13/12 Contact: Advocacy@apta.org Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule Introduction COMPREHENSIVE SUMMARY On November 2, 2012, the Centers
Overview of the Hospice Proposed Rule
 HOSPICE Overview of Hospice Payment Reform Robert J. Simione Managing Principal Simione Healthcare Consultants On April 29, 2013 CMS issued the proposed rule that would update FY 2014 Medicare payment
HOSPICE Overview of Hospice Payment Reform Robert J. Simione Managing Principal Simione Healthcare Consultants On April 29, 2013 CMS issued the proposed rule that would update FY 2014 Medicare payment
October Hospice Fundamentals All Rights Reserved 1. ABNs: The Why, The What & The When. The Plan
 ABNs: The Why, The What & The When Subscriber Webinar The Plan CMS Benefit Notices Initiative The Advance Beneficiary Notice of Noncoverage (ABN) The Uses: Statutory & Voluntary The Form The Difficulties
ABNs: The Why, The What & The When Subscriber Webinar The Plan CMS Benefit Notices Initiative The Advance Beneficiary Notice of Noncoverage (ABN) The Uses: Statutory & Voluntary The Form The Difficulties
Topics. Overview of the Medicare Recovery Audit Contractor (RAC) Understanding Medicaid Integrity Contractor
 Understanding Medicaid Integrity Contractor") RACS, ZPICS & MICS John Falcetano, CHC-F, CCEP-F, CHPC, CHRC, CIA Chief Audit and Compliance Officer University Health Systems of Eastern Carolina jfalceta@uhseast.com Topics Overview of the Medicare Recovery
RACS, ZPICS & MICS John Falcetano, CHC-F, CCEP-F, CHPC, CHRC, CIA Chief Audit and Compliance Officer University Health Systems of Eastern Carolina jfalceta@uhseast.com Topics Overview of the Medicare Recovery
2017 OIG Work Plan and Current Compliance Topics - Home Health and Hospice
 HCCA Web Conference November 20, 2015 2017 OIG Work Plan and Current Compliance Topics - Home Health and Hospice Bill Musick, BS, MBA, CHC, CHCP Senior Associate & Consulting Projects Manager Your trusted
HCCA Web Conference November 20, 2015 2017 OIG Work Plan and Current Compliance Topics - Home Health and Hospice Bill Musick, BS, MBA, CHC, CHCP Senior Associate & Consulting Projects Manager Your trusted
Medicare Hospice Billing 2015 & Beyond!
 Medicare Hospice Billing 2015 & Beyond! Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. Sequential Claim Billing The NOE must be in S/LOC P B9997 prior to submitting the first
Medicare Hospice Billing 2015 & Beyond! Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. Sequential Claim Billing The NOE must be in S/LOC P B9997 prior to submitting the first
Home Health, Hospice, and Nursing Facility. Indiana Health Coverage Programs DXC Technology October 2017
 Home Health, Hospice, and Nursing Facility Indiana Health Coverage Programs DXC Technology October 2017 Agenda Billing Tips Home Health Hospice Nursing Facility Claim Form Update Helpful Tools Questions
Home Health, Hospice, and Nursing Facility Indiana Health Coverage Programs DXC Technology October 2017 Agenda Billing Tips Home Health Hospice Nursing Facility Claim Form Update Helpful Tools Questions
Certified Ophthalmic Executive (COE) Review Day
 Review Day") Certified Ophthalmic Executive (COE) Review Day Compliance Plan & Chart Audits Financial Disclosure The instructor acknowledges a financial interest in the subject matter of this presentation. Presented
Certified Ophthalmic Executive (COE) Review Day Compliance Plan & Chart Audits Financial Disclosure The instructor acknowledges a financial interest in the subject matter of this presentation. Presented
4/17/2017 OBJECTIVES FEDERAL REQUIREMENTS. Having the Difficult Conversation: We need to Discharge You from Hospice
 Having the Difficult Conversation: We need to Discharge You from Hospice Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Identify the regulatory requirements
Having the Difficult Conversation: We need to Discharge You from Hospice Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Identify the regulatory requirements
Table of Contents. 1.0 Description of the Procedure, Product, or Service Definitions Hospice Terminal illness...
 Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 1.1.1 Hospice... 1 1.1.2 Terminal illness... 1 2.0 Eligibility Requirements... 1 2.1 Provisions... 1 2.1.1
Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 1.1.1 Hospice... 1 1.1.2 Terminal illness... 1 2.0 Eligibility Requirements... 1 2.1 Provisions... 1 2.1.1
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512)
") NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
FRAUD AND ABUSE IN HOSPICE: Under the Microscope Weatherbee Hospice Regulatory Boot Camp. Howard J. Young, Esq.
 FRAUD AND ABUSE IN HOSPICE: Under the Microscope Weatherbee Hospice Regulatory Boot Camp Howard J. Young, Esq. Morgan Lewis & Bockius Hospice Services Doing Good skilled nursing services drugs and biologicals
FRAUD AND ABUSE IN HOSPICE: Under the Microscope Weatherbee Hospice Regulatory Boot Camp Howard J. Young, Esq. Morgan Lewis & Bockius Hospice Services Doing Good skilled nursing services drugs and biologicals
NHPCO Regulatory Recap for Activity from August 2011 Volume 1, Issue No.8
 NHPCO Regulatory Recap for Activity from August 2011 Volume 1, Issue No.8 To: NHPCO Membership From: NHPCO Regulatory Team IN THIS ISSUE: CMS Help Prevent Fraud Campaign CMS Provider Compliance Group Outreach
NHPCO Regulatory Recap for Activity from August 2011 Volume 1, Issue No.8 To: NHPCO Membership From: NHPCO Regulatory Team IN THIS ISSUE: CMS Help Prevent Fraud Campaign CMS Provider Compliance Group Outreach
Home Care and Hospice: Payment and Reimbursement Update: AHLA Institute on Medicare and Medicaid Payment Issues
 Home Care and Hospice: Payment and Reimbursement Update: 2014 AHLA Institute on Medicare and Medicaid Payment Issues William A. Dombi Vice President for Law National Association for Home Care & Hospice
Home Care and Hospice: Payment and Reimbursement Update: 2014 AHLA Institute on Medicare and Medicaid Payment Issues William A. Dombi Vice President for Law National Association for Home Care & Hospice
Recovery Audit Contractors: AHA Perspective. Elizabeth Baskett, Policy, AHA February 23, 2012
 Recovery Audit Contractors: AHA Perspective Elizabeth Baskett, Policy, AHA February 23, 2012 Agenda Lay of the Land = Audit Overload RACs (Medicare & Medicaid) MACs ZPICs and OIG and DOJ, oh my! AHA and
Recovery Audit Contractors: AHA Perspective Elizabeth Baskett, Policy, AHA February 23, 2012 Agenda Lay of the Land = Audit Overload RACs (Medicare & Medicaid) MACs ZPICs and OIG and DOJ, oh my! AHA and
Palmetto GBA Hospice Coalition Questions and Answers
 Palmetto GBA Hospice Coalition Questions and Answers September 23, 2008 To: Hospice Coalition Members From: Palmetto GBA Provider Education Date: September 23, 2008 Location: Palmetto GBA Attachment A:
Palmetto GBA Hospice Coalition Questions and Answers September 23, 2008 To: Hospice Coalition Members From: Palmetto GBA Provider Education Date: September 23, 2008 Location: Palmetto GBA Attachment A:
Medicare Fraud & Abuse: Prevention, Detection, and Reporting ICN
 Medicare Fraud & Abuse: Prevention, Detection, and Reporting ICN 908103 1 Disclaimers This presentation was current at the time it was published or uploaded onto the web. Medicare policy changes frequently
Medicare Fraud & Abuse: Prevention, Detection, and Reporting ICN 908103 1 Disclaimers This presentation was current at the time it was published or uploaded onto the web. Medicare policy changes frequently
Palmetto GBA Hospice Coalition Questions August 7, 2001
 Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
Hospice Program Integrity Recommendations
 Hospice Program Integrity Recommendations Projected increases in the elderly population and the number of Medicare beneficiaries will likely result in continued growth in utilization of hospice services.
Hospice Program Integrity Recommendations Projected increases in the elderly population and the number of Medicare beneficiaries will likely result in continued growth in utilization of hospice services.
RECENT INVESTIGATION AND ENFORCEMENT TRENDS
 RECENT INVESTIGATION AND ENFORCEMENT TRENDS Texas and New Mexico Hospice Organization Mark S. Armstrong Member of the Firm EPSTEIN, BECKER & GREEN, P.C. Houston, Texas 2014 Epstein Becker & Green, P.C.
RECENT INVESTIGATION AND ENFORCEMENT TRENDS Texas and New Mexico Hospice Organization Mark S. Armstrong Member of the Firm EPSTEIN, BECKER & GREEN, P.C. Houston, Texas 2014 Epstein Becker & Green, P.C.
Hospice Discharges. Legacy Hospice
 Hospice Discharges Legacy Hospice Live Discharges Once a Medicare beneficiary elects the hospice benefit, hospice may not automatically or routinely d/c the beneficiary at it s discretion, even if the
Hospice Discharges Legacy Hospice Live Discharges Once a Medicare beneficiary elects the hospice benefit, hospice may not automatically or routinely d/c the beneficiary at it s discretion, even if the
National Hospice and Palliative Care OrganizatioN. Facts AND Figures. Hospice Care in America. NHPCO Facts & Figures edition
 National Hospice and Palliative Care OrganizatioN Facts AND Figures Hospice Care in America 2017 Edition NHPCO Facts & Figures - 2017 edition Table of Contents 2 Introduction 2 About this report 2 What
National Hospice and Palliative Care OrganizatioN Facts AND Figures Hospice Care in America 2017 Edition NHPCO Facts & Figures - 2017 edition Table of Contents 2 Introduction 2 About this report 2 What
How to Overhaul your Internal Structure to be Prepared for the New Home Health CoPs. Program Objectives
 How to Overhaul your Internal Structure to be Prepared for the New Home Health CoPs 2015 NAHC Annual Meeting 106 October 28, 4:30 5:30 p.m. Nashville, Tennessee Kathleen Spooner, RN, CMC Kathleen A. Hessler,
How to Overhaul your Internal Structure to be Prepared for the New Home Health CoPs 2015 NAHC Annual Meeting 106 October 28, 4:30 5:30 p.m. Nashville, Tennessee Kathleen Spooner, RN, CMC Kathleen A. Hessler,
The Hospice/Nursing Home Partnership: How to do it Right! Background: Barrier vs. Collaboration
 The Hospice/Nursing Home Partnership: How to do it Right! National Hospice and Palliative Care Organization 29 th Management and Leadership Conference Connie A. Raffa, J.D., LL.M. March 27, 2014 raffa.connie@arentfox.com
The Hospice/Nursing Home Partnership: How to do it Right! National Hospice and Palliative Care Organization 29 th Management and Leadership Conference Connie A. Raffa, J.D., LL.M. March 27, 2014 raffa.connie@arentfox.com
Having the Difficult Conversation: We need to Discharge You from Hospice
 Having the Difficult Conversation: We need to Discharge You from Hospice Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Identify the regulatory requirements
Having the Difficult Conversation: We need to Discharge You from Hospice Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Identify the regulatory requirements
Proposed Fraud & Abuse Rule Implementing ACA Provisions. Ivy Baer October 26, 2010
 Proposed Fraud & Abuse Rule Implementing ACA Provisions Ivy Baer ibaer@aamc.org 202-828-0499 October 26, 2010 Comments Due November 16, 2010 To submit: Refer to: CMS-6028-P http://www.regulations.gov 2
Proposed Fraud & Abuse Rule Implementing ACA Provisions Ivy Baer ibaer@aamc.org 202-828-0499 October 26, 2010 Comments Due November 16, 2010 To submit: Refer to: CMS-6028-P http://www.regulations.gov 2
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
Auditing and Monitoring Focusing Your Resources
 Auditing and Monitoring Focusing Your Resources Subscriber Webinar June 13, 2014 Today s Plan Why a hospice should devote resources to auditing and monitoring Setting priorities Guidelines for developing
Auditing and Monitoring Focusing Your Resources Subscriber Webinar June 13, 2014 Today s Plan Why a hospice should devote resources to auditing and monitoring Setting priorities Guidelines for developing
Medicare Recovery Audit Contractors. Chicago, IL August 1, 2008
 Medicare Recovery Audit Contractors Chicago, IL August 1, 2008 1 Recovery Audit Contractors Demo Summary National Rollout AHA Strategy AHA RACTrac Overview 2 Recovery Audit Contractors Medicare Modernization
Medicare Recovery Audit Contractors Chicago, IL August 1, 2008 1 Recovery Audit Contractors Demo Summary National Rollout AHA Strategy AHA RACTrac Overview 2 Recovery Audit Contractors Medicare Modernization
Hot Off the Press! The FY2017 Final Rule & Its Implications for Hospices. Presenter. Objectives 08/31/16
 Hot Off the Press! The FY2017 Final Rule & Its Implications for Hospices August 31, 2016 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org
Hot Off the Press! The FY2017 Final Rule & Its Implications for Hospices August 31, 2016 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org
Recovery Audit Contractors (RACs) and Medicare. The Who, What, When, Where, How and Why?
 and Medicare. The Who, What, When, Where, How and Why?") Recovery Audit Contractors (RACs) and Medicare The Who, What, When, Where, How and Why? 1 Agenda What is a RAC? Will the RACs affect me? Why RACs? What does a RAC do? What are the providers options? What
Recovery Audit Contractors (RACs) and Medicare The Who, What, When, Where, How and Why? 1 Agenda What is a RAC? Will the RACs affect me? Why RACs? What does a RAC do? What are the providers options? What
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #51 Navigating Health Care Reform: Creating a Road Map for Success Thursday, August 8 8:15 to 9:45 a.m. Regency
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #51 Navigating Health Care Reform: Creating a Road Map for Success Thursday, August 8 8:15 to 9:45 a.m. Regency
FY 2017 Hospice Proposed Rule. Hospice Regulatory Review May Webinar Agenda. Hospice Regulatory Review
 Hospice Regulatory Review May 2016 Presented by: Deanna Loftus, Director of Regulatory Compliance Liz Silva, Director of Hospice Webinar Agenda CY 2017 Proposed Rule o New Payment Rates o Diagnosis Code
Hospice Regulatory Review May 2016 Presented by: Deanna Loftus, Director of Regulatory Compliance Liz Silva, Director of Hospice Webinar Agenda CY 2017 Proposed Rule o New Payment Rates o Diagnosis Code
More than a Century of Legal Experience
 Advanced Beneficiary Notice (ABN) and Hospital Issued Notice of Non Coverage(HINN): To Issue, or Not to Issue an ABN or HINN July 30, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience
Advanced Beneficiary Notice (ABN) and Hospital Issued Notice of Non Coverage(HINN): To Issue, or Not to Issue an ABN or HINN July 30, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience
FRAUD AND ABUSE IN HOSPICE: Under the Microscope Weatherbee Hospice Regulatory Boot Camp. Howard J. Young, Esq.
 FRAUD AND ABUSE IN HOSPICE: Under the Microscope Weatherbee Hospice Regulatory Boot Camp Howard J. Young, Esq. Morgan Lewis & Bockius Hospice Services Doing Good skilled nursing services drugs and biologicals
FRAUD AND ABUSE IN HOSPICE: Under the Microscope Weatherbee Hospice Regulatory Boot Camp Howard J. Young, Esq. Morgan Lewis & Bockius Hospice Services Doing Good skilled nursing services drugs and biologicals
Medicare and Medicaid Audit Defense & Appeals: From RACs to ZPICs September 7, 2012 Skokie, IL
 Midwest Home Health Summit Best Practices Conference Series Medicare and Medicaid Audit Defense & Appeals: From RACs to ZPICs September 7, 2012 Skokie, IL Michael T. Walsh Principal Kitch Attorneys & Counselors
Midwest Home Health Summit Best Practices Conference Series Medicare and Medicaid Audit Defense & Appeals: From RACs to ZPICs September 7, 2012 Skokie, IL Michael T. Walsh Principal Kitch Attorneys & Counselors
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
April Hospice Fundamentals All Rights Reserved 1. The Certification/ Recertification Process: No Room for Error. What You Will Learn Today
 The Certification/ Recertification Process: No Room for Error Subscriber Webinar What You Will Learn Today Regulatory requirements Election of the Medicare Hospice Benefit Certification Recertification
The Certification/ Recertification Process: No Room for Error Subscriber Webinar What You Will Learn Today Regulatory requirements Election of the Medicare Hospice Benefit Certification Recertification
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL
 Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN. Post Acute Provider Specific Sections from OIG Work Plans
 HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
CDx ANNUAL PHYSICIAN CLIENT NOTICE
 CDx ANNUAL PHYSICIAN CLIENT NOTICE - 2018 CDX Diagnostics is providing this annual notice in accordance with the recommendations made by the Office of Inspector General (OIG) as part of our CDx Compliance
CDx ANNUAL PHYSICIAN CLIENT NOTICE - 2018 CDX Diagnostics is providing this annual notice in accordance with the recommendations made by the Office of Inspector General (OIG) as part of our CDx Compliance
Improving Medicaid Program Integrity: State Strategies to Combat Fraud and Abuse
 Improving Medicaid Program Integrity: State Strategies to Combat Fraud and Abuse March 6, 2013 Overview New York's Experience Role of Medicaid Program Integrity: Florida s Approach Medicaid Anti-Fraud
Improving Medicaid Program Integrity: State Strategies to Combat Fraud and Abuse March 6, 2013 Overview New York's Experience Role of Medicaid Program Integrity: Florida s Approach Medicaid Anti-Fraud
National Update : 2013 HEALTH CARE REFORM. Insurance reforms through the ACA Delivery reforms New delivery models under study
 National Update : 2013 Mary St. Pierre, RN, BSN, MGA m 1 HEALTH CARE REFORM Insurance reforms through the ACA Delivery reforms New delivery models under study Chronic care management Transitions in care
National Update : 2013 Mary St. Pierre, RN, BSN, MGA m 1 HEALTH CARE REFORM Insurance reforms through the ACA Delivery reforms New delivery models under study Chronic care management Transitions in care
Pharmacy Compliance: Beyond Med Errors. Overview
 Pharmacy Compliance: Beyond Med Errors Daniel P. Fitzgerald, Senior Attorney Litigation & Regulatory Law Department Walgreen Co. James S. Mathis, Esq., Nashville, TN Overview Med Errors & Controlled Substances
Pharmacy Compliance: Beyond Med Errors Daniel P. Fitzgerald, Senior Attorney Litigation & Regulatory Law Department Walgreen Co. James S. Mathis, Esq., Nashville, TN Overview Med Errors & Controlled Substances
Zone Program Integrity Program & Recovery Audit Contractors
 Zone Program Integrity Program & Recovery Audit Contractors Advance Planning and Responsive Tools. AHLA Long Term Care and the Law Program Feb 26, 2013 Presented by: Brain Daucher Esq. Sheppard Mullin
Zone Program Integrity Program & Recovery Audit Contractors Advance Planning and Responsive Tools. AHLA Long Term Care and the Law Program Feb 26, 2013 Presented by: Brain Daucher Esq. Sheppard Mullin
Department of Health and Human Services. Centers for Medicare & Medicaid Services. Medicaid Integrity Program
 Department of Health and Human Services Centers for Medicare & Medicaid Services Medicaid Integrity Program California Comprehensive Program Integrity Review Final Report Reviewers: Jeff Coady, Review
Department of Health and Human Services Centers for Medicare & Medicaid Services Medicaid Integrity Program California Comprehensive Program Integrity Review Final Report Reviewers: Jeff Coady, Review
Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services (CMS) Transmittal 2867 Date: February 5, 2014
 Centers for Medicare & Medicaid Services (CMS) Transmittal 2867 Date: February 5, 2014") CS anual System Pub 100-04 edicare Claims Processing Department of Health & Human Services (DHHS) Centers for edicare & edicaid Services (CS) Transmittal 2867 Date: February 5, 2014 Change Request 8569
CS anual System Pub 100-04 edicare Claims Processing Department of Health & Human Services (DHHS) Centers for edicare & edicaid Services (CS) Transmittal 2867 Date: February 5, 2014 Change Request 8569
Enforcement Trends and Compliance: Hospice and Home Health
 Enforcement Trends and Compliance: Hospice and Home Health HCCA Healthcare Enforcement Compliance Institute October 25, 2016 1 Agenda Overview of Recent Enforcement Trends False Claims Act Litigation Developments
Enforcement Trends and Compliance: Hospice and Home Health HCCA Healthcare Enforcement Compliance Institute October 25, 2016 1 Agenda Overview of Recent Enforcement Trends False Claims Act Litigation Developments
Enforcement Trends and Compliance: Hospice and Home Health
 Enforcement Trends and Compliance: Hospice and Home Health HCCA Healthcare Enforcement Compliance Institute October 25, 2016 1 Agenda Overview of Recent Enforcement Trends False Claims Act Litigation Developments
Enforcement Trends and Compliance: Hospice and Home Health HCCA Healthcare Enforcement Compliance Institute October 25, 2016 1 Agenda Overview of Recent Enforcement Trends False Claims Act Litigation Developments
Medicare Administrative Contractors and the Medical Review Process. Medicare Administrative Contractors (MAC) Audits
 Audits") Medicare Administrative Contractors and the Medical Review Process Roseanne Berry, MSN, RN Charlene Ross, MBA, MSN, RN Ask the Experts February 10, 2012 Medicare Administrative Contractors (MAC) Audits
Medicare Administrative Contractors and the Medical Review Process Roseanne Berry, MSN, RN Charlene Ross, MBA, MSN, RN Ask the Experts February 10, 2012 Medicare Administrative Contractors (MAC) Audits
Chapter 15. Medicare Advantage Compliance
 Chapter 15. Medicare Advantage Compliance 15.1 Introduction 3 15.2 Medical Record Documentation Requirements 8 15.2.1 Overview... 8 15.2.2 Documentation Requirements... 8 15.2.3 CMS Signature and Credentials
Chapter 15. Medicare Advantage Compliance 15.1 Introduction 3 15.2 Medical Record Documentation Requirements 8 15.2.1 Overview... 8 15.2.2 Documentation Requirements... 8 15.2.3 CMS Signature and Credentials
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability
 Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
PROPOSED RULE: MEDICARE PROGRAM; HOME HEALTH PROSPECTIVE PAYMENT SYSTEM RATE UPDATE FOR CY 2013 SUMMARY. July 17, 2012
 PROPOSED RULE: MEDICARE PROGRAM; HOME HEALTH PROSPECTIVE PAYMENT SYSTEM RATE UPDATE FOR CY 2013 SUMMARY July 17, 2012 On July 6, 2012, the Centers for Medicare & Medicaid Services (CMS) made public a proposed
PROPOSED RULE: MEDICARE PROGRAM; HOME HEALTH PROSPECTIVE PAYMENT SYSTEM RATE UPDATE FOR CY 2013 SUMMARY July 17, 2012 On July 6, 2012, the Centers for Medicare & Medicaid Services (CMS) made public a proposed
Riding Herd on Fraud, Waste and Abuse
 Riding Herd on Fraud, Waste and Abuse Dan McCullough Judi McCabe Juanita Henry Kim Hrehor 1 Taking Stock: Surveying the Landscape of Fraud, Waste and Abuse 2 How Big is the Problem? The simple truth is
Riding Herd on Fraud, Waste and Abuse Dan McCullough Judi McCabe Juanita Henry Kim Hrehor 1 Taking Stock: Surveying the Landscape of Fraud, Waste and Abuse 2 How Big is the Problem? The simple truth is
Chapter 11 Section 3. Hospice Reimbursement - Conditions For Coverage
 Hospice Chapter 11 Section 3 Issue Date: February 6, 1995 Authority: 32 CFR 199.4(e)(19) 1.0 APPLICABILITY This policy is mandatory for reimbursement of services provided by either network or nonnetwork
Hospice Chapter 11 Section 3 Issue Date: February 6, 1995 Authority: 32 CFR 199.4(e)(19) 1.0 APPLICABILITY This policy is mandatory for reimbursement of services provided by either network or nonnetwork
2013 OIG Work Plan. Scott McBride Baker & Hostetler LLP 1000 Louisiana, Suite 2000 Houston, Texas
 2013 OIG Work Plan Scott McBride Baker & Hostetler LLP 1000 Louisiana, Suite 2000 Houston, Texas 77002 713.646.1390 smcbride@bakerlaw.com Webinar Essentials * Session is currently being recorded, and will
2013 OIG Work Plan Scott McBride Baker & Hostetler LLP 1000 Louisiana, Suite 2000 Houston, Texas 77002 713.646.1390 smcbride@bakerlaw.com Webinar Essentials * Session is currently being recorded, and will
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
Adapting Your Medical Necessity Compliance Program In An Evolving Regulatory Environment
 Adapting Your Medical Necessity Compliance Program In An Evolving Regulatory Environment Joydip Roy MD Vice President of Compliance and Physician Education Adapting Your Medical Necessity Compliance Program
Adapting Your Medical Necessity Compliance Program In An Evolving Regulatory Environment Joydip Roy MD Vice President of Compliance and Physician Education Adapting Your Medical Necessity Compliance Program
One Year Later THE IMPACT OF HEALTH CARE REFORM on Health Care Provider Audits and Compliance Programs
 24 Health Care Law One Year Later THE IMPACT OF HEALTH CARE REFORM on Health Care Provider Audits and Compliance Programs By Andrew B. Wachler, Jennifer Colagiovanni, and Christopher J. Laney FAST FACTS:
24 Health Care Law One Year Later THE IMPACT OF HEALTH CARE REFORM on Health Care Provider Audits and Compliance Programs By Andrew B. Wachler, Jennifer Colagiovanni, and Christopher J. Laney FAST FACTS:
2016 Hospice Regulatory Blueprint for Action. Hospice Association of America 228 Seventh Street, SE Washington DC
 2016 Hospice Regulatory Blueprint for Action Hospice Association of America 228 Seventh Street, SE Washington DC 20003-4306 HOSPICE ASSOCIATION OF AMERICA 2016 REGULATORY BLUEPRINT FOR ACTION TABLE OF
2016 Hospice Regulatory Blueprint for Action Hospice Association of America 228 Seventh Street, SE Washington DC 20003-4306 HOSPICE ASSOCIATION OF AMERICA 2016 REGULATORY BLUEPRINT FOR ACTION TABLE OF
CY 2016 Hospice Proposed Rule. HEALTHCAREfirst 5/13/2015. Hospice Regulatory Update FY Hospice Regulatory Review May 2015.
 Hospice Regulatory Review May 2015 Presented by: Deanna Loftus Director of Regulatory Compliance Webinar Agenda CY 2016 Proposed Rule o New Payment Rates o New Service Intensity Add-On o HQRP Updates o
Hospice Regulatory Review May 2015 Presented by: Deanna Loftus Director of Regulatory Compliance Webinar Agenda CY 2016 Proposed Rule o New Payment Rates o New Service Intensity Add-On o HQRP Updates o
How to Survive Audits By Accurately Documenting Medical Necessity. Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus
 How to Survive Audits By Accurately Documenting Medical Necessity Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus How to Survive Audits By Accurately Documenting Medical
How to Survive Audits By Accurately Documenting Medical Necessity Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus How to Survive Audits By Accurately Documenting Medical
Chapter 30, Medicaid Hospice Program 07/19/13
 Chapter 30, Medicaid Hospice Program 07/19/13 30.4. Definitions. The following words and terms, when used in this chapter, shall have the following meanings, unless the context clearly indicates otherwise.
Chapter 30, Medicaid Hospice Program 07/19/13 30.4. Definitions. The following words and terms, when used in this chapter, shall have the following meanings, unless the context clearly indicates otherwise.
Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule
![Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule](/thumbs/73/68786685.jpg "Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule") Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule TABLE OF CONTENTS Issue Page I. Introduction and Background
Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule TABLE OF CONTENTS Issue Page I. Introduction and Background
Government Focus in Home Health
 Government Focus in Home Health November 8, 2011 Cheryl Golden Director Deloitte & Touche LLP Contents Current Regulatory Focus in Home Health Government Programs HHS OIG Work Plan 2012 Auditing and Monitoring
Government Focus in Home Health November 8, 2011 Cheryl Golden Director Deloitte & Touche LLP Contents Current Regulatory Focus in Home Health Government Programs HHS OIG Work Plan 2012 Auditing and Monitoring
2017 National Training Program
 2017 National Training Program Module 10 Medicare and Medicaid Fraud, Waste, and Abuse Prevention Contents Lesson 1 Fraud, Waste, and Abuse Overview... Lesson 2 CMS Fraud and Abuse Strategies... Lesson
2017 National Training Program Module 10 Medicare and Medicaid Fraud, Waste, and Abuse Prevention Contents Lesson 1 Fraud, Waste, and Abuse Overview... Lesson 2 CMS Fraud and Abuse Strategies... Lesson
AHLA. Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions
 AHLA Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Joan C. Ragsdale CEO MedManagement LLC Vestavia,
AHLA Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Joan C. Ragsdale CEO MedManagement LLC Vestavia,
The Medicare Hospice Benefit. What Does It Mean to You and Your Patients?
 The Medicare Hospice Benefit What Does It Mean to You and Your Patients? The Medicare Hospice Benefit By the time Congress established the Medicare Hospice Benefit in 1982, hundreds of organizations in
The Medicare Hospice Benefit What Does It Mean to You and Your Patients? The Medicare Hospice Benefit By the time Congress established the Medicare Hospice Benefit in 1982, hundreds of organizations in
Medicare Consolidate Billing & Overview
 Medicare Consolidate Billing & Overview Julie Kearney, Kearney & Associates Consolidated Billing The Balanced Budget Act of 1997, Congress mandated that payment for the majority of services provided to
Medicare Consolidate Billing & Overview Julie Kearney, Kearney & Associates Consolidated Billing The Balanced Budget Act of 1997, Congress mandated that payment for the majority of services provided to