Patient Driven Payment Model 101
|
|
|
- Solomon Shields
- 5 years ago
- Views:
Transcription

1 Patient Driven Payment Model 101 MARK MCDAVID, OTR, RAC-CT Presented by
2 Why a New Payment Model? MedPAC has raised concerns about: Provider advantage Payment inequities for different patient types Patient selection being driven by payment Concerns about overutilization of therapy MedPAC has been focused on PAC payment reform Aligning cost and payment Equitable payments across patient groups Pay for performance 2
3 OIG Reports Over the Years Questionable billing by skilled nursing facilities (December 2010) Inappropriate Payments to Skilled Nursing Facilities Cost Medicare More Than a Billion Dollars in 2009 (November 2012) The Medicare Payment System for Skilled Nursing Facilities Needs to be Reevaluated (September 2015) 3
4 CMS Goals Limit complexity of the new payment system 66 Payment categories vs 28,800 Address financial incentives described by MedPAC, OIG, and CMS Payment model accuracy that will compensate facilities based on complexity of the patient 4
5 Acumen CMS Contractor Previous (current) PPS System Therapy Nursing Non-case mix Index Maximized Proposed PPS System PT Component OT Component ST Component Non-therapy ancillary component Nursing component Non-case mix component Not Index Maximized 5
6 Patient Driven Payment Model (PDPM) CMS Proposes Complete overhaul of the Medicare A payment system (replacing RUGs-IV) On April 27, 2018 CMS released a SNF PPS Proposed Rule for FY 2019 that included the PDPM for FY 2020 Comments were due to CMS by June 26, 2018 by 5pm 6
7 PDPM 6 Components CMS Proposes 5 case-mix adjusted components and 1 non case-mix adjusted component. Physical Therapy Component Occupational Therapy Component Speech-Language Pathology Component Nursing Component Non-Therapy Ancillary Component Non Case-mix Component (room and board, admin cost, capital-related costs) + wage adjustment 7
8 Patient Driven Payment Model PT Component SLP Component Nursing Component NTA Component OT Component Resident Non Case-Mix Component 8

9 Patient Driven Payment Model Note: All residents would be classified into PT, OT, and SLP classification regardless of whether they are on therapy case load (likely being assigned the lowest CMI for the these components). 9
10 Physical and Occupational Therapy Case-Mix Classification 10
11 PT and OT Components Unlike RCS-I, in the PDPM the PT and OT Components are calculated together but paid separately based on the casemix. Drivers of PT and OT component Primary reason for skilled stay Function score 11
12 PT and OT Components I8000 ICD-10-CM will classify the patient into one of the 4 Clinical Categories. Multiple ICD-10-CM codes will point to more than one Clinical Category In these cases, the Clinical Category will be further delineated by including the ICD-10-PCS (procedure code) on the second line of I8000 This is due to post-surgical patient needs may be much different than non-surgical patients 12
13 4 PT/OT Clinical Categories Major Joint Replacement or Spinal Injury Non-Orthopedic Surgery and Acute Neurologic Other Orthopedic Medical Management 13
14 PT and OT Functional Score CMS Proposes to use 10 Section GG items to calculate the PT and OT Function Score. This includes 4 late loss ADLs and 2 early loss ADLs Two bed mobility items Three transfer items One eating items One toileting item One oral hygiene item Two walking items GG goes from a 6-point scale (with 3 not attempted codes) to 0-4 point scale for Function Score purposes 14
15 PT and OT Functional Score Construction (Except walking) Responses Score 05, 06 Set-up assistance, Independent 4 04 Supervision or touching assistance 3 03 Partial/moderate assistance 2 02 Substantial/maximal assistance 1 01, 07, 09, 88 Dependent, Refused, N/A, Not Attempted 0 More Care Needed Table 16 CMS 1696-P 15
16 PT and OT Functional Score Construction for Walking Items Responses Score 05, 06 Set-up assistance, Independent 4 04 Supervision or touching assistance 3 03 Partial/moderate assistance 2 02 Substantial/maximal assistance 1 01, 07, 09, 88 Dependent, Refused, N/A, Not Attempted, Resident Cannot Walk* *Coded based on response to GG0170H1 (Does the resident walk?) 0 More Care Needed Table 17 CMS 1696-P 16
17 Proposed Section GG Items Included in PT and OT Function Measure Section GG Item Score GG0130A1 Self-care: Eating 0-4 GG0310B1 Self-care: Oral Hygiene 0-4 GG0130C1 Self-care: Toileting Hygiene 0-4 GG0170B1 Mobility: Sit to lying 0-4 (avg of GG0170C1 Mobility: Lying to sitting on side of 2 items) bed GG0170D1 GG0170E1 GG0170F1 Mobility: Sit to stand Mobility: chair/bed-to-chair transfer Mobility: Toilet transfer 0-4 (avg of 3 items) GG0170J1 Mobility: Walk 50 feet with 2 turns 0-4 (avg of GG0170K1 Mobility: Walk 150 feet 2 items) 17 Table 18 CMS 1696-P
18 PT and OT Case-mix Classification Groups Clinical Category Major Joint Replacement or Spinal Surgery Section GG Function Score PT OT Case- Mix Group PT Case- Mix Index OT Case- Mix Index 0-5 TA TB TC TD TE Other Orthopedic 6-9 TF TG Partial Table 21 CMS 1696-P 24 TH
19 PT and OT Case-mix Classification Groups Clinical Category Medical Management Section GG Function Score PT OT Case- Mix Group PT Case- Mix Index OT Case- Mix Index 0-5 TI Tj TK TL Non-Orthopedic Surgery and Acute Neurologic 19 Partial Table 21 CMS 1696-P 0-5 TM TN TO TP


20 Speech Language Pathology Case-Mix Classification 20
21 SLP Component 5 Characteristics that will impact the SLP Component Acute Neurologic or Non-Neurologic SLP-Related Comorbidity Cognitive Impairment Mechanically Altered Diet Swallowing Disorder 21
22 SLP Component Acute Neurologic or Non-Neurologic Determined by I8000 SLP-Related Comorbidity Also determined by I
23 SLP-Related Comorbidities Aphasia CVA, TIA, or Stroke Hemiplegia or Hemiparesis Traumatic Brain Injury Tracheostomy Care (while a resident) Ventilator or Respirator (while a resident) Laryngeal Cancer Apraxia Dysphagia ALS Oral Cancers Speech and Language Deficits Table 22 CMS 1696-P 23
24 Cognitive Functional C Score (CFS) CMS Proposes blending BIMS and CPS to get a CFS score CFS Cognitive Scale BIMS Score CPS Score 1. Cognitively Intact Mildly Impaired Moderately Impaired Severely Impaired Table 20 CMS P 24
25 SLP Component Mechanically Altered Diet Determined by K0510C2 Swallowing Disorder Determined by K0100Z 25
26 Presence of Acute Neurologic Condition, SLP-Related Comorbidity, or Cognitive Impairment 12 SLP Case-Mix Groups Mechanically Altered Diet or Swallowing Disorder Case-Mix Group Case-Mix Index None Neither SA 0.68 None Either SB 1.82 None Both SC 2.66 Any one Neither SD 1.46 Any one Either SE 2.33 Any one Both SF 2.97 Any two Neither SG 2.04 Any two Either SH 2.85 Any two Both SI 3.51 Any three Neither SJ 2.98 Any three Either SK 3.69 Any three Both SL Table 23 CMS-1696-P


27 Nursing Case-Mix Classification Proposed 27
28 25 Nursing Indexes CMS Proposes to use a modified version of the RUG-IV Nursing Categories CMS reduced the number of Nursing RUGs from 43 to 25. This was accomplished by collapsing case-mix groups that have contiguous ADL scores when those RUGs were defined by similar clinical traits We will look at Table 26 in a few slides. 28
29 25 Nursing Indexes CMS Proposes to use a modified version of the RUG-IV Nursing Categories Nursing will also use Section GG to capture the Nursing Function Score Using the same methodology as for the PT and OT component. 0-4 point scale Average bed mobility and transfers 29
30 Section GG items for Nursing Section GG Item Table 25 CMS 1696-P Score GG0130A1 Self-care: Eating 0-4 GG0130C1 Self-care: Toileting Hygiene 0-4 GG0170B1 Mobility: Sit to lying 0-4 (avg of GG0170C1 Mobility: Lying to sitting on side of 2 items) bed GG0170D1 GG0170E1 GG0170F1 Mobility: Sit to stand Mobility: chair/bed-to-chair transfer Mobility: Toilet transfer 0-4 (avg of 3 items) 30
31 PDPM Nursing Index 25 Indexes RIG-IV Nursing RUG 31 ES3 ES2 Extensive Services Trach and Vent Trach or Vent Clinical Condition Depres sion # of Restorative Nursing Services GG-based Function Score PDPM Nursing Case-Mix Group *e.g. septicemia, respiratory therapy and more see full chart Partial Table 26 CMS 1696-P Nursing Case- Mix Index ES ES ES1 Infection ES HE2/HD Serious medical condition* Yes HDE HE1/HD1 --- same No HDE HC2/HB2 --- Same Yes HBC HC1/HB1 --- Same No HBC1 1.85
32 HIV/AIDS add-on Due to significant increase in nursing cost to care for HIV/AIDS pts, the facility will get an 18% increase in the Nursing Component This would be applied based on the presence of ICD-10-CM code B20 on the SNF claim 32
33 Non-Therapy Ancillary Case-Mix Classification 33
34 50 Conditions & Extensive Services Used for NTA Classification Condition/Extensive Services Partial Table 27 CMS P Source Points HIV/Aids SNF Claim 8 Parenteral IV feeding: High MDS Item O0100H2 7 Special Treatments/ Programs: IV Meds Postadmit Special Treatments/ Programs: Vent or Resp Post-admit MDS Item O0100I2 5 MDS ItemO010F2 4 Endocarditis MDS Item I
35 NTA Case-Mix Classification Groups NTA Score Range NTA Group NTA Case-Mix Index 12+ NA NB NC ND NE NF 0.72 Partial Table 28 CMS 1696-P 35
36 36 Non Case-Mix Component

37 Non Case-Mix Component Flat rate Non case-mix adjusted 37
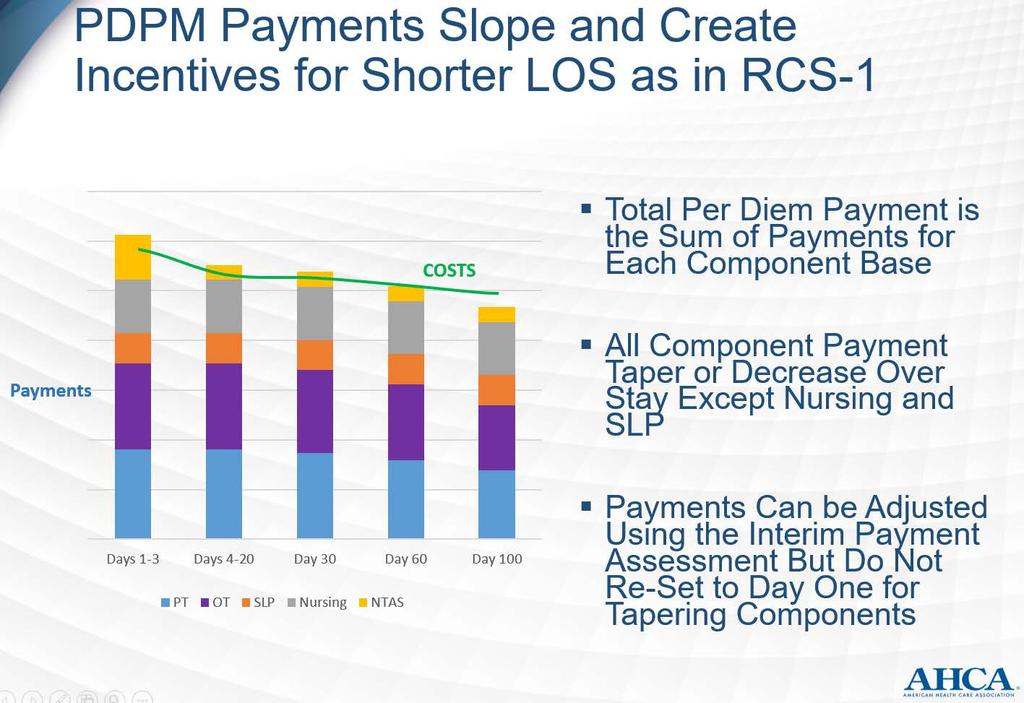
38 Variable Per Diem Adjustment Factor 38


39 Variable Per Diem Adjustment Factor Adjustment Factor PT and OT: After day 20, drop 2% every 7 days. Of interest, if the patient is in the facility on days , the adjustment factor for PT and OT is

40 NTA Adjustment Factor Medicare Payment Days Adjustment Factor Table 31 CMS 1696-P 40

 SNF Part A Discharge")
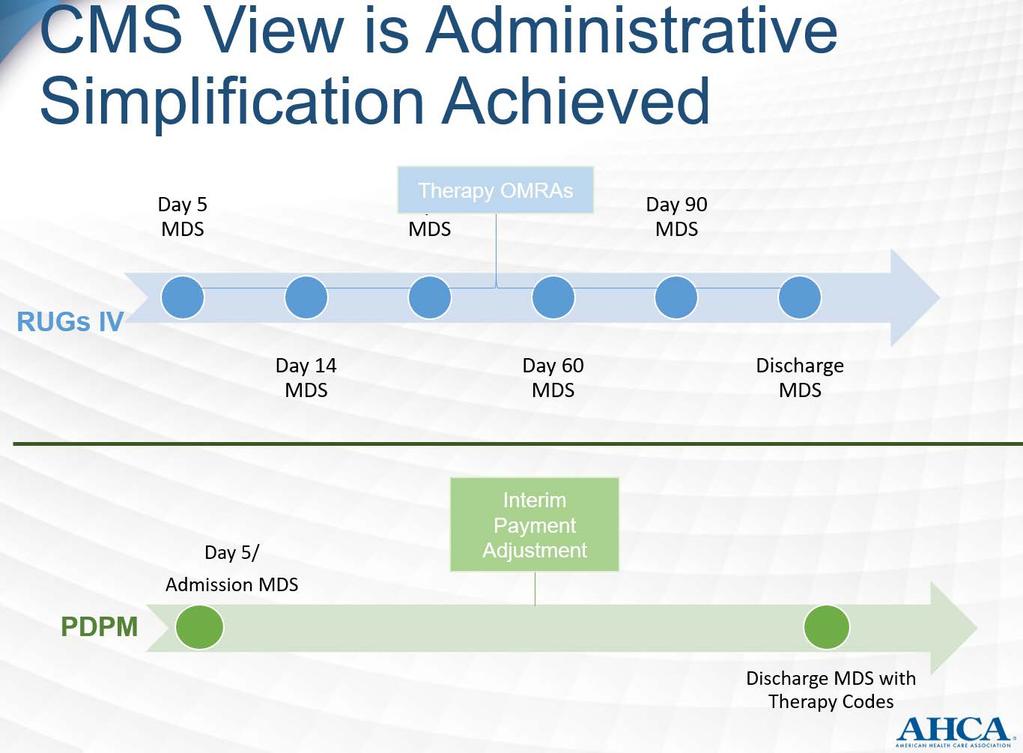
41 Assessments (MDS) to be completed Only three types of assessments 5-Day Scheduled Assessment Interim Payment Assessment (IPA) SNF Part A Discharge Assessment 41


42 5-Day Scheduled Assessment Grace Days Remove the label grace days so that the 5-day PPS schedule will be days 1-8 vs days 1-5 with grace days of
43 Interim Payment Assessment Requirements (1) There is a change in the resident s classification in at least one of the first tier classification criteria for any of the components under the proposed PDPM (which are those clinical or nursing payment criteria identified in the first column in Tables 21, 23, 26, and 27 PT/OT, SLP, Nursing, NTA) such that the resident would be classified into a classification group for that component that differs from that provided by the 5-day scheduled PPS assessment, and the change in classification group results in a change in payment either in one particular payment component or in the overall payment for the resident; and (2) The change(s) are such that the resident would not be expected to return to his or her original clinical status within a 14-day period. 43


44 Interim Payment Assessment Requirements - In addition, we propose that the Assessment Reference Date (ARD) for the IPA would be no later than 14 days after a change in a resident s first tier classification criteria is identified. The IPA is meant to capture substantial changes to a resident s clinical condition and not every day, frequent changes. We believe 14 days gives the facility an adequate amount of time to determine whether the changes identified are in fact routine or substantial. - Missed or late IPAs will be treated as missed or late unscheduled assessments 44


45 PPS Discharge Assessment Must be completed on all PPS discharges Adding a modified Section O to this assessment 45
46 Modified Section O MDS Item Number O0400A5 O0400A6 O0400A7 O0400A8 O0400A9 O0400A10 Item Name Special Treatments, Procedures and Programs: Speech-Language Pathology and Audiology Services: Therapy Start Date Special Treatments, Procedures and Programs: Speech-Language Pathology and Audiology Services: Therapy End Date Special Treatments, Procedures and Programs: Speech-Language Pathology and Audiology Services: Total Individual Minutes Special Treatments, Procedures and Programs: Speech-Language Pathology and Audiology Services: Total Concurrent Minutes Special Treatments, Procedures and Programs: Speech-Language Pathology and Audiology Services: Total Group Minutes Special Treatments, Procedures and Programs: Speech-Language Pathology and Audiology Services: Total Days 46 Partial Table 35 CMS-1696-P


47 Decrease in Provider Burden CMS Proposes The PDPM model will save providers $200M per year or $2B over 10 years 47
48 48




49 PDPM Modes of Therapy Group and Concurrent Therapy Limits to 25% combined Most services provided on an individual basis 49
50 PDPM Modes of Therapy Group and Concurrent minutes counted in full vs ¼ and ½ respectively CMS will use the Discharge Assessment to monitor Group and Concurrent utilization. Should a provider exceed this limitation, a non-fatal warning edit will appear on the validation report after submission to the QIES ASAP system CMS may consider future proposals to address abuses of this policy or flag providers for additional review 50
 if the")

51 PDPM Interrupted Stays Payment calendar continues (using adjustment factors) if the resident is discharged from a SNF and returns to the same SNF within 3 midnights. Eval implications? 51
52 PDPM Per Diem PT and OT Rate SLP Rate Nursing Rate NTA Rate Non-Case-Mix Rate Base Rate x PT and OT CMI x Adjustment Factor Base Rate x SLP CMI Nursing Rate x Nursing CMI Base Rate x NTA CMI x Adjustment Factor Non-Case Mix Rate $$$ + $$$ + $$$ + $$$ + $$$ + $$$ 52 Total Per Diem
53 Hip Replacement Example Mr. B had a hip replacement and was sent for rehab at our SNF. His case-mix groups are as follows: PT and OT case-mix group TA SLP case-mix group SA Nursing PDPM case-mix group CDE2 Non-therapy ancillary NE Non case-mix flat rate 53
54 Hip Replacement Example Case-mix group Case-mix Index TB TB SA CDE2 NE Urban PT OT SLP Nursing NTA Non case-mix Per diem $ $ $ $ $ 78.05x3 $ Subtotal $ $ $ $ $ $ Urban - *Note: these rates are not wage index adjusted Days Per Diem 1-3 $ $ $
55 Hip Replacement Example Case-mix group Case-mix Index TB TB SA CDE2 NE Rural PT OT SLP Nursing NTA Non case-mix Per diem $ $ $ $ $ 74.56x3 $ Subtotal $ $ $ $ $ $ Rural - *Note: these rates are not wage index adjusted Days Per Diem 1-3 $ $ $


56 Joint Replacement/Medically Complex Extremely ill patient with multiple comorbidities (joint replacement, dysphagia and mech altered diet, septicemia, depressed, 0-5 on GG, 12+ on NTA): PT and OT case-mix group TA SLP case-mix group SC Nursing PDPM case-mix group HDE2 Non-therapy ancillary NA Non case-mix flat rate 56
57 Joint Replacement/Medically Complex Case-mix group Case-mix Index TA TA SC HDE2 NA Urban PT OT SLP Nursing NTA Non case-mix Per diem $59.33 $55.23 $22.15 $ $78.05 x3 $92.63 Subtotal $90.77 $82.29 $58.91 $ $ $ Urban - *Note: these rates are not wage index adjusted - Show AANAC Handout Days Per Diem 1-3 $ $ $
58 58
59 Now What? Industry Changes? The usual contract therapy contract will no longer work Part B will continue as is Part A portion of contract What do we go to next? Pay contract based on hourly rate of time on-site? Same as above with productivity minimum? Pay contractor a percentage of the PT/OT and ST rates? 59
60 Now What? Industry Changes? Therapy utilization? Assume that therapy utilization will decrease May mean that there is a decreased demand for therapists nationwide. Therapist salaries? Is this PPS lite for the therapy portion of the industry? Could in-house therapy be an option or a reality for your facility? 60
61 Some Concerns About the Model Rationing of therapy. PT and OT limited clinical categories why not use comorbidities like the SLP component? PT and OT cognition removed from this calculation concerns Modified Section O on discharge assessment seen as helpful to the therapy community. How will it be handled if one discipline misses a few days? (sick therapist, holiday, staffing issues) 61
62 Some Concerns About the Model Use of Section GG seen as a good thing, but usual performance to drive resource allocation? PDPM is based on statistical analysis and on projection that has not been tested. Need a demonstration project and possible phased-in roll out system. Unknowns about the IPA probably won t know specifics until the draft RAI comes out in January 2019 Auditors may try to apply rules that do not apply to this model well after the fact (paid for SLP, but didn t provide it to a specific patient, auditor may try to take those funds back) 62


63 Who we are and who we serve: SNF Rehab Agency Legal SNF In-house Contract conversion Contract therapy company audits 63
64 What will PDPM look like for SimpleLTC customers? Currently reviewing PDPM details and product options SimpleAnalyzer will include PDPM views/analytics Product vision Possible RUG analytics tool (pre-pdpm) to include Case Mix Index analysis Possible cross-integration of analytics from RUG to PDPM What are my RUG reimbursements now? How might my reimbursements be different under PDPM? How will my CMI affect this? Look for product announcements coming soon


65 Now that we have opened Pandora s box, what questions do you have about PDPM? 21 Page synopsis on our website Mark McDavid, OTR/L RAC-CT Seagrove Rehab Partners mark@ www. 65
6/12/2017. The Rumor is True: A New PPS Payment System is on the Horizon Presented by: RKL, LLP Senior Living Services Consulting Group
 The Rumor is True: A New PPS Payment System is on the Horizon Presented by: RKL, LLP Senior Living Services Consulting Group 1 Speaker Introductions Stephanie Kessler, RAC-CT Partner 717.885-5724 skessler@rklcpa.com
The Rumor is True: A New PPS Payment System is on the Horizon Presented by: RKL, LLP Senior Living Services Consulting Group 1 Speaker Introductions Stephanie Kessler, RAC-CT Partner 717.885-5724 skessler@rklcpa.com
What Every Administrator Needs to Know About the PROPOSED Patient Driven Payment Model (PDPM)
") What Every Administrator Needs to Know About the PROPOSED Patient Driven Payment Model (PDPM) Presented by: Robin L. Hillier, CPA, STNA, LNHA, RAC-MT robin@rlh-consulting.com (330) 807-2850 PDPM Overview
What Every Administrator Needs to Know About the PROPOSED Patient Driven Payment Model (PDPM) Presented by: Robin L. Hillier, CPA, STNA, LNHA, RAC-MT robin@rlh-consulting.com (330) 807-2850 PDPM Overview
Proposed RCS-1 & It s Impact on Therapy Services- Will it Happen? Krista Olson, MS,CCC-SLP
 Proposed RCS-1 & It s Impact on Therapy Services- Will it Happen? Krista Olson, MS,CCC-SLP Objectives: What is RCS-1? Why the proposed change in payment system? Differences between RCS-1 and current PPS
Proposed RCS-1 & It s Impact on Therapy Services- Will it Happen? Krista Olson, MS,CCC-SLP Objectives: What is RCS-1? Why the proposed change in payment system? Differences between RCS-1 and current PPS
Objectives 9/18/2018. Patient Driven Payment Model(PDPM) Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018
 Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018") Patient Driven Payment Model(PDPM) Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018 Mission: The trusted voice for aging. Objectives List the five(5) case mix components
Patient Driven Payment Model(PDPM) Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018 Mission: The trusted voice for aging. Objectives List the five(5) case mix components
CMS (Medicare), Patient Driven Payment Model PDPM. Presented by: Cindy Gensamer, MBA, HSE, LNHA Vice President Absolute Rehabilitation
, Patient Driven Payment Model PDPM. Presented by: Cindy Gensamer, MBA, HSE, LNHA Vice President Absolute Rehabilitation") CMS (Medicare), Patient Driven Payment Model PDPM Presented by: Cindy Gensamer, MBA, HSE, LNHA Vice President Absolute Rehabilitation What is it? PDPM Released in Final Rule 7-31-18 Effective 10-1-19 Patient
CMS (Medicare), Patient Driven Payment Model PDPM Presented by: Cindy Gensamer, MBA, HSE, LNHA Vice President Absolute Rehabilitation What is it? PDPM Released in Final Rule 7-31-18 Effective 10-1-19 Patient
2/20/2018. Resident Classification System RCS-1. CMS Proposal
 Resident Classification System RCS-1 CMS Proposal Resident Classification System I (RCS-I) Complete overhaul of the Medicare A payment system (replacing RUGs-IV) On April 27, 2017 CMS released an Advance
Resident Classification System RCS-1 CMS Proposal Resident Classification System I (RCS-I) Complete overhaul of the Medicare A payment system (replacing RUGs-IV) On April 27, 2017 CMS released an Advance
8/27/2018. PDPM Strategies to Thrive Under the SNF Medicare Reimbursement Overhaul. Objectives. PDPM Introduction
 PDPM Strategies to Thrive Under the SNF Medicare Reimbursement Overhaul Presented by: Cindy Gensamer Vice President, Absolute Rehabilitation & Consulting Services, Inc. Brady Dalrymple Business Owner,
PDPM Strategies to Thrive Under the SNF Medicare Reimbursement Overhaul Presented by: Cindy Gensamer Vice President, Absolute Rehabilitation & Consulting Services, Inc. Brady Dalrymple Business Owner,
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I
 Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I ZIMMET HEALTHCARE 2018
 Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model
 and the MDS: A Total Evolution of the SNF Payment Model") Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
SNF proposed rule revisions to case-mix methodology
 SNF proposed rule revisions to case-mix methodology Comments due: August 25, 2017 CMS intent to propose case-mix refinements in the FY 2019 SNF PPS proposed rule Summary of changes Goals of the change:
SNF proposed rule revisions to case-mix methodology Comments due: August 25, 2017 CMS intent to propose case-mix refinements in the FY 2019 SNF PPS proposed rule Summary of changes Goals of the change:
Patient-Driven Payment Model
 Patient-Driven Model Why a New System? Top 10 RUGs in 2015 Comprise 90% of SNF Days and 92% of SNF s RUG RUG Description Total Days 2015 Distinct Beneficiaries Per RUG Per Day Per Beneficiary Total Percent
Patient-Driven Model Why a New System? Top 10 RUGs in 2015 Comprise 90% of SNF Days and 92% of SNF s RUG RUG Description Total Days 2015 Distinct Beneficiaries Per RUG Per Day Per Beneficiary Total Percent
& Reward. Opportunity, Risk. HealthPRO Heritage National healthcare solutions firm specializing in Care ReDesign for top of market clients 9/5/2018
 Opportunity, Risk & Reward Care Redesign Cross Continuum Connections Built on a Foundation of Clinical Innovation Elisa Bovee, MS OTR/L, Vice President of Clinical Strategies 2017 LeadingAge New York Annual
Opportunity, Risk & Reward Care Redesign Cross Continuum Connections Built on a Foundation of Clinical Innovation Elisa Bovee, MS OTR/L, Vice President of Clinical Strategies 2017 LeadingAge New York Annual
The Shift is ON! Goodbye PPS, Hello RCS
 The Shift is ON! Goodbye PPS, Hello RCS Presented By Maureen McCarthy, RN, BS, RAC-MT, QCP-MT President/CEO Maureen McCarthy, RN, BS, RAC-MT, QCP-MT Maureen is the President of Celtic Consulting, LLC and
The Shift is ON! Goodbye PPS, Hello RCS Presented By Maureen McCarthy, RN, BS, RAC-MT, QCP-MT President/CEO Maureen McCarthy, RN, BS, RAC-MT, QCP-MT Maureen is the President of Celtic Consulting, LLC and
Goodbye PPS: Hello RCS!
 Disclosure of Commercial Interests I consult for the following organizations: Celtic Consulting LLC President, CEO Celtic Consulting is a Long-Term Care advisory firm, focused on providing one-on-one oversight
Disclosure of Commercial Interests I consult for the following organizations: Celtic Consulting LLC President, CEO Celtic Consulting is a Long-Term Care advisory firm, focused on providing one-on-one oversight
Medicare Skilled Nursing Facility Prospective Payment System
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Program Year: FY2019 August 2018 1 TABLE OF CONTENTS Overview and Resources... 2 SNF Payment Rates... 2 Wage Index and Labor-Related
CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1)
") CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1) Ohio Health Care Association Mike Cheek, Senior Vice President, Reimbursement Policy October 3, 2017 Background 1 FY18
CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1) Ohio Health Care Association Mike Cheek, Senior Vice President, Reimbursement Policy October 3, 2017 Background 1 FY18
RCS-1. (Resident Classification System-Version 1) New Medicare payment system: What to Expect!
 New Medicare payment system: What to Expect!") RCS-1 (Resident Classification System-Version 1) New Medicare payment system: What to Expect! Presented by: Patricia J. Boyer Director of Clinical Services Wipfli LLP Wipfli LLP 10000 Innovation Drive,
RCS-1 (Resident Classification System-Version 1) New Medicare payment system: What to Expect! Presented by: Patricia J. Boyer Director of Clinical Services Wipfli LLP Wipfli LLP 10000 Innovation Drive,
MEDICARE PART A SNF PROSPECTIVE PAYMENT SYSTEM
 MEDICARE PART A SNF PROSPECTIVE PAYMENT SYSTEM MDS 3.0 Captured Services as Qualifiers for Medicare Part A RUG-IV Grouper REHABILITATION Base Rates Urban Unadjusted AWI = 1.0000 ADL END 10/1/2017 INDEX
MEDICARE PART A SNF PROSPECTIVE PAYMENT SYSTEM MDS 3.0 Captured Services as Qualifiers for Medicare Part A RUG-IV Grouper REHABILITATION Base Rates Urban Unadjusted AWI = 1.0000 ADL END 10/1/2017 INDEX
Countdown to MDS Section GG: Collaboration Between Nursing and Therapy
 Countdown to MDS Section GG: Collaboration Between Nursing and Therapy Presented in Collaboration with NASL: Joanne M. Wisely, MA CCC/SLP, VP Legislative Advocacy Genesis Rehab Services/Respiratory Health
Countdown to MDS Section GG: Collaboration Between Nursing and Therapy Presented in Collaboration with NASL: Joanne M. Wisely, MA CCC/SLP, VP Legislative Advocacy Genesis Rehab Services/Respiratory Health
Federal FY2019 SNF PPS Proposed Rule, SNF Value-Based Purchasing Program, and SNF Quality Reporting Program Analysis
 Federal FY2019 SNF PPS Proposed Rule, SNF Value-Based Purchasing Program, and SNF Quality Reporting Program Analysis Part I: Update to the SNF VBP and QRP Programs Part II: Payment Updates Part III: Patient-Driven
Federal FY2019 SNF PPS Proposed Rule, SNF Value-Based Purchasing Program, and SNF Quality Reporting Program Analysis Part I: Update to the SNF VBP and QRP Programs Part II: Payment Updates Part III: Patient-Driven
CMS Requirements of Participation Facility Assessment
 HEALTHCARE I N S I G H T S May 2017 THE NEWSLETTER FROM LOEB & TROPER FOR NURSING HOMES AND HOME CARE AGENCIES CONTENTS CMS Requirements of Participation Facility Assessment Managed Care Contracts and
HEALTHCARE I N S I G H T S May 2017 THE NEWSLETTER FROM LOEB & TROPER FOR NURSING HOMES AND HOME CARE AGENCIES CONTENTS CMS Requirements of Participation Facility Assessment Managed Care Contracts and
Dazed and Confused: Initial Results from the IRF QRP Data
 Dazed and Confused: Initial Results from the IRF QRP Data Troy Hillman Manager, Analytical Services Uniform Data System for Medical Rehabilitation 2017 Uniform Data System for Medical Rehabilitation, a
Dazed and Confused: Initial Results from the IRF QRP Data Troy Hillman Manager, Analytical Services Uniform Data System for Medical Rehabilitation 2017 Uniform Data System for Medical Rehabilitation, a
2014 AANAC 9_30_ AANA C AANA
 2013 2014 AANAC AANAC 9_30_14 Expert Advisory Panel Guests Deb Myhre, RN, RAC-MT, C-NE Mark McDavid, OTR, RAC-CT Requirements for Successful Completion 1 Contact hour will be awarded for this continuing
2013 2014 AANAC AANAC 9_30_14 Expert Advisory Panel Guests Deb Myhre, RN, RAC-MT, C-NE Mark McDavid, OTR, RAC-CT Requirements for Successful Completion 1 Contact hour will be awarded for this continuing
Seema Verma Centers for Medicare & Medicaid Services Department of Health and Human Services Attn: CMS-1696-P P.O. Box 8016 Baltimore, MD
 June 26, 2018 Seema Verma Centers for Medicare & Medicaid Services Department of Health and Human Services Attn: CMS-1696-P P.O. Box 8016 Baltimore, MD 21244-1850 Re: CMS-1696-P Medicare Program; Prospective
June 26, 2018 Seema Verma Centers for Medicare & Medicaid Services Department of Health and Human Services Attn: CMS-1696-P P.O. Box 8016 Baltimore, MD 21244-1850 Re: CMS-1696-P Medicare Program; Prospective
Chances are.. Based on my experience MDS 3.0 Update for Long Term Care PRESENTED BY 2/13/2017. New focus on Data by CMS and Regulatory Agencies
 PRESENTED BY 2017 MDS 3.0 Update for Long Term Care LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@tatci.com New focus on Data by CMS and Regulatory
PRESENTED BY 2017 MDS 3.0 Update for Long Term Care LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@tatci.com New focus on Data by CMS and Regulatory
Sneak Peak: MDS 3.0 Changes & New QRP s. Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma
 Sneak Peak: MDS 3.0 Changes & New QRP s Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma Disclaimer These materials, including any medical literature
Sneak Peak: MDS 3.0 Changes & New QRP s Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma Disclaimer These materials, including any medical literature
June 26, Dear Ms. Verma:
 Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 RE: CMS 1696 Medicare Program; Prospective Payment
Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 RE: CMS 1696 Medicare Program; Prospective Payment
Section GG GG 1. MDS Coding Essentials: Section GG and Function. MDS Essentials. Section GG Assessment Types. Content 4/24/2017.
 Section GG GG 1 MDS Coding Essentials: SECTION GG: FUNCTIONAL ABILITIES AND GOALS Intent: This section assesses the need for assistance with self care and mobility activities. Sections GG and K 1 4 MDS
Section GG GG 1 MDS Coding Essentials: SECTION GG: FUNCTIONAL ABILITIES AND GOALS Intent: This section assesses the need for assistance with self care and mobility activities. Sections GG and K 1 4 MDS
Medicare Program; Prospective Payment System and Consolidated Billing for Skilled. AGENCY: Centers for Medicare & Medicaid Services (CMS), HHS.
, HHS.") This document is scheduled to be published in the Federal Register on 05/04/2017 and available online at https://federalregister.gov/d/2017-08519, and on FDsys.gov DEPARTMENT OF HEALTH
This document is scheduled to be published in the Federal Register on 05/04/2017 and available online at https://federalregister.gov/d/2017-08519, and on FDsys.gov DEPARTMENT OF HEALTH
Get A Seat at the Table
 Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Attachment C: Itemized List of OASIS Data Elements
 Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS)
") CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS) 6.1 Background The Balanced Budget Act of 1997 included the implementation of a Medicare Prospective Payment System (PPS)
CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS) 6.1 Background The Balanced Budget Act of 1997 included the implementation of a Medicare Prospective Payment System (PPS)
Changes to the RAI manual effective October 1, 2013
 Changes to the RAI manual effective October 1, 2013 CMS released on Friday, September 27 an updated version of the RAI manual that became effective October 1, 2013. The manual is found here> http://www.cms.gov/medicare/quality-initiatives-patient-assessment-
Changes to the RAI manual effective October 1, 2013 CMS released on Friday, September 27 an updated version of the RAI manual that became effective October 1, 2013. The manual is found here> http://www.cms.gov/medicare/quality-initiatives-patient-assessment-
National Association for the Support of Long Term Care
 Seema Verma, Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Hubert H. Humphrey Building, Room 445-G 200 Independence Avenue, SW Washington, D.C. 20201
Seema Verma, Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Hubert H. Humphrey Building, Room 445-G 200 Independence Avenue, SW Washington, D.C. 20201
AVOID FINANCIAL PENALTIES BY PREPARING FOR MDS 3.0 UPDATE
 AVOID FINANCIAL PENALTIES BY PREPARING FOR MDS 3.0 UPDATE SNF QRP Quality Measures or Not? August 25, 2016 Carol Smith, RN,BSN, RAC-CT Managing Consultant csmith@bkd.com Suzy Harvey, RN-BC, RAC-CT Managing
AVOID FINANCIAL PENALTIES BY PREPARING FOR MDS 3.0 UPDATE SNF QRP Quality Measures or Not? August 25, 2016 Carol Smith, RN,BSN, RAC-CT Managing Consultant csmith@bkd.com Suzy Harvey, RN-BC, RAC-CT Managing
Pitch Perfect: Selling Your Services to LTC Facilities
 Pitch Perfect: Selling Your Services to LTC Facilities Lou Ann Brubaker, President Brubaker Consulting www.brubakerconsulting.com 301 535 5449 brubak97@aol.com Linkedin Disclosure Lou Ann Brubaker is the
Pitch Perfect: Selling Your Services to LTC Facilities Lou Ann Brubaker, President Brubaker Consulting www.brubakerconsulting.com 301 535 5449 brubak97@aol.com Linkedin Disclosure Lou Ann Brubaker is the
June 22, Submitted electronically
 June 22, 2018 Seema Verma, MPH Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G Attn: CMS-1696-P Hubert Humphrey Building 200 Independence Ave,
June 22, 2018 Seema Verma, MPH Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G Attn: CMS-1696-P Hubert Humphrey Building 200 Independence Ave,
COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES
 COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES WOULD YOU COMPLETE A SIGNIFICANT CHANGE IN STATUS ASSESSMENT? Example
COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES WOULD YOU COMPLETE A SIGNIFICANT CHANGE IN STATUS ASSESSMENT? Example
100 Days Out: What's Changing with the MDS 3.0 Item Set on October 1, 2018
 100 Days Out: What's Changing with the MDS 3.0 Item Set on October 1, 2018 June 22, 2018 Learning Objectives/Outcomes Locate the current DRAFT MDS 3.0 Item Sets as well as the Item Set Change History document
100 Days Out: What's Changing with the MDS 3.0 Item Set on October 1, 2018 June 22, 2018 Learning Objectives/Outcomes Locate the current DRAFT MDS 3.0 Item Sets as well as the Item Set Change History document
Division of Health Care Financing and Policy
 Division of Health Care Financing and Policy Presentation to the Legislative Subcommittee on Post Acute Care in Nevada February 2016 1 Topics of Discussion Post acute care-types of services Current rate
Division of Health Care Financing and Policy Presentation to the Legislative Subcommittee on Post Acute Care in Nevada February 2016 1 Topics of Discussion Post acute care-types of services Current rate
The Finalized MDS 3.0 RAI Manual: What you need to know about the new item set, new section, and more!
 The Finalized MDS 3.0 RAI Manual: What you need to know about the new item set, new section, and more! Presented by: Amy Franklin RN, RAC-MT, DNS-MT, QCP-MT AANAC Curriculum Development Specialist 1 Faculty
The Finalized MDS 3.0 RAI Manual: What you need to know about the new item set, new section, and more! Presented by: Amy Franklin RN, RAC-MT, DNS-MT, QCP-MT AANAC Curriculum Development Specialist 1 Faculty
Historical Document: Transition Occured to RUG - IV - 01/01/2012. RUG IV & MN Case Mix. Objectives. Why RUG IV? 11/21/2011
 RUG IV & MN Case Mix November 2011 James Sims, Principal Planner Marci Martinson, Case Mix Review Director Objectives O By the end of this session the participant will be able to: O State the reasons for
RUG IV & MN Case Mix November 2011 James Sims, Principal Planner Marci Martinson, Case Mix Review Director Objectives O By the end of this session the participant will be able to: O State the reasons for
Indiana Medicaid Reimbursement Update Tysen Adams, CPA Deborah Lake, RN, RAC-CT Senior Managing Consultants BKD, LLP
 Indiana Medicaid Reimbursement Update Tysen Adams, CPA Deborah Lake, RN, RAC-CT Senior Managing Consultants BKD, LLP Agenda 5 To 8 Year Long-Term Care Plan Value Based Purchasing Issues Proposed Report
Indiana Medicaid Reimbursement Update Tysen Adams, CPA Deborah Lake, RN, RAC-CT Senior Managing Consultants BKD, LLP Agenda 5 To 8 Year Long-Term Care Plan Value Based Purchasing Issues Proposed Report
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW OHA Finance/PFS Webinar Series. May 10, 2016
 MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
AANAC Education Advancement. MDS Essentials: An Introduction. Learning Objectives 3/22/2017. Education Advancement
 AANAC Education Advancement MDS Essentials: An Introduction to MDS 3.0 We want to provide you with the right education at the right time in your career path Consider the following to identify your needs:
AANAC Education Advancement MDS Essentials: An Introduction to MDS 3.0 We want to provide you with the right education at the right time in your career path Consider the following to identify your needs:
Equalizing Medicare Payments for Select Patients in IRFs and SNFs
 Equalizing Medicare Payments for Select Patients in IRFs and SNFs Doug Wissoker Bowen Garrett A report by staff from the Urban Institute for the Medicare Payment Advisory Commission The Urban Institute
Equalizing Medicare Payments for Select Patients in IRFs and SNFs Doug Wissoker Bowen Garrett A report by staff from the Urban Institute for the Medicare Payment Advisory Commission The Urban Institute
The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform. Summary
 Reform. Summary") Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Medicare Part A Update
 Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
Medi-Pak Advantage: Reimbursement Methodology
 Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
Data Stewardship: Essential Skills for Long Term Care Facility Managers
 Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Inpatient Rehabilitation Program Information
 Inpatient Rehabilitation Program Information The Inpatient Rehabilitation Program at TIRR Memorial Hermann The Woodlands has a team of physicians, therapists, nurses, a case manager, neuropsychologist,
Inpatient Rehabilitation Program Information The Inpatient Rehabilitation Program at TIRR Memorial Hermann The Woodlands has a team of physicians, therapists, nurses, a case manager, neuropsychologist,
Development of Updated Models of Non-Therapy Ancillary Costs
 Development of Updated Models of Non-Therapy Ancillary Costs Doug Wissoker A. Bowen Garrett A memo by staff from the Urban Institute for the Medicare Payment Advisory Commission Urban Institute MedPAC
Development of Updated Models of Non-Therapy Ancillary Costs Doug Wissoker A. Bowen Garrett A memo by staff from the Urban Institute for the Medicare Payment Advisory Commission Urban Institute MedPAC
Outcomes Measurement in Long-Term Care (LTC)
") ASHA Short Course Outcomes Measurement in Long-Term Care (LTC) Bill Goulding, MS/CCC-SLP November 19, 2012 How Do We Show Value? Easy to measure! Not so easy! V $$$ A L Impact? Cost U Benefit E What do
ASHA Short Course Outcomes Measurement in Long-Term Care (LTC) Bill Goulding, MS/CCC-SLP November 19, 2012 How Do We Show Value? Easy to measure! Not so easy! V $$$ A L Impact? Cost U Benefit E What do
Clinical and Compliance Bulletin
 Clinical and Compliance Bulletin 877.799.9595 www.evergreenrehab.com 2011 Quarter 3 Coding Corner FAQ 1. How do I bill for group speech therapy treatment? There are two group therapy CPT codes that are
Clinical and Compliance Bulletin 877.799.9595 www.evergreenrehab.com 2011 Quarter 3 Coding Corner FAQ 1. How do I bill for group speech therapy treatment? There are two group therapy CPT codes that are
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2016
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2016 August 2015 Table of Contents Overview and Resources... 2 SNF Payment Rates... 2 Effect of Sequestration...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2016 August 2015 Table of Contents Overview and Resources... 2 SNF Payment Rates... 2 Effect of Sequestration...
What s New with the NYS OMIG Audit Process. NYSHFA Nurse Leadership Conference April 23, Disclosure
 What s New with the NYS OMIG Audit Process NYSHFA Nurse Leadership Conference April 23, 2015 Disclosure Information contained in this program has been collected and collated by Zimmet Healthcare Services
What s New with the NYS OMIG Audit Process NYSHFA Nurse Leadership Conference April 23, 2015 Disclosure Information contained in this program has been collected and collated by Zimmet Healthcare Services
Executive Summary. This Project
 Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
CRS Report for Congress Received through the CRS Web
 CRS Report for Congress Received through the CRS Web Order Code RS20386 Updated April 16, 2001 Medicare's Skilled Nursing Facility Benefit Summary Heidi G. Yacker Information Research Specialist Information
CRS Report for Congress Received through the CRS Web Order Code RS20386 Updated April 16, 2001 Medicare's Skilled Nursing Facility Benefit Summary Heidi G. Yacker Information Research Specialist Information
RURAL HEALTH RESEARCH POLICY ANALYSIS CENTER. A Primer on the Occupational Mix Adjustment to the. Medicare Hospital Wage Index. Working Paper No.
 N C RURAL HEALTH RESEARCH & POLICY ANALYSIS CENTER A Primer on the Occupational Mix to the Medicare Hospital Wage Index Working Paper No. 86 September, 2006 725 MARTIN LUTHER KING JR. BLVD. CB #7590 THE
N C RURAL HEALTH RESEARCH & POLICY ANALYSIS CENTER A Primer on the Occupational Mix to the Medicare Hospital Wage Index Working Paper No. 86 September, 2006 725 MARTIN LUTHER KING JR. BLVD. CB #7590 THE
Discharge to Community Measure
 The Discharge to Community Measure determines the percentage of all new admissions from a hospital who are discharged back to the community and remain out of any skilled nursing center for the next 30
The Discharge to Community Measure determines the percentage of all new admissions from a hospital who are discharged back to the community and remain out of any skilled nursing center for the next 30
Percentage of Short-Stay Residents who were Re-hospitalized after a Nursing Home Admission
 Table 1. Percentage of Short-Stay Residents who were Re-hospitalized after a Nursing Home Admission Measure Description Numerator and Window Numerator Exclusions Covariates The percent of short-stay residents
Table 1. Percentage of Short-Stay Residents who were Re-hospitalized after a Nursing Home Admission Measure Description Numerator and Window Numerator Exclusions Covariates The percent of short-stay residents
August 25, Dear Ms. Verma:
 Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
RAPID RUG GUIDE RUG-III, VERSION GROUPER Effective for Assessments With an ARD on or After 10/1/2013
 RAPID RUG GUIDE RUG-III, VERSION 5.20 34-GROUPER Effective for Assessments With an ARD on or After 10/1/2013 Step 1: Calculation To calculate the score of Bed Mobility (G0110A), Transfer (G0110B) and Toilet
RAPID RUG GUIDE RUG-III, VERSION 5.20 34-GROUPER Effective for Assessments With an ARD on or After 10/1/2013 Step 1: Calculation To calculate the score of Bed Mobility (G0110A), Transfer (G0110B) and Toilet
State of Kansas Department of Social and Rehabilitation Services Department on Aging Kansas Health Policy Authority
 State of Kansas Department of Social and Rehabilitation Services Department on Aging Kansas Health Policy Authority Notice of Proposed Nursing Facility Medicaid Rates for State Fiscal Year 2010; Methodology
State of Kansas Department of Social and Rehabilitation Services Department on Aging Kansas Health Policy Authority Notice of Proposed Nursing Facility Medicaid Rates for State Fiscal Year 2010; Methodology
Revised Section GG 8/28/2018. Why does it matter now? Importance of Section GG. Started in Revisions effective Oct. 1, 2018
 Revised Section GG Arbor Rehabilitation Approach Fall 2018 Why does it matter now? Started in 2016 Revisions effective Oct. 1, 2018 Increased areas for data collection Significantly increased importance!
Revised Section GG Arbor Rehabilitation Approach Fall 2018 Why does it matter now? Started in 2016 Revisions effective Oct. 1, 2018 Increased areas for data collection Significantly increased importance!
Medicare PPS Report. Self Guided Tutorial
 Medicare PPS Report Self Guided Tutorial 1 Tutorial Objectives After completing this tutorial, you will be able to: Identify the purpose of the Medicare PPS Report Access the Medicare PPS Report Customize
Medicare PPS Report Self Guided Tutorial 1 Tutorial Objectives After completing this tutorial, you will be able to: Identify the purpose of the Medicare PPS Report Access the Medicare PPS Report Customize
G-Codes Functional Reporting: Are You Compliant
 G-Codes Functional Reporting: Are You Compliant Presented by: HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. HHI PPS & Case Mix Onsite Chart Audits MMQ Audits Seminars Consulting
G-Codes Functional Reporting: Are You Compliant Presented by: HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. HHI PPS & Case Mix Onsite Chart Audits MMQ Audits Seminars Consulting
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals
 Rural Hospitals under 100 Beds and Critical Access Hospitals") SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
Value Based Care in LTC: The Quality Connection- Phase 2
 Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Medicare Inpatient Psychiatric Facility Prospective Payment System
 Medicare Inpatient Psychiatric Facility Prospective Payment System Payment Rule Brief PROPOSED RULE Program Year: FFY 2016 Overview and Resources On April 24, 2015, the Centers for Medicare and Medicaid
Medicare Inpatient Psychiatric Facility Prospective Payment System Payment Rule Brief PROPOSED RULE Program Year: FFY 2016 Overview and Resources On April 24, 2015, the Centers for Medicare and Medicaid
Acute Care to Rehab & Complex Continuing Care (CCC) Referral
 Referral") o General Rehabilitation Low Intensity Rehabilitation (GRH, SJHCG) o (CMH, GRH, SJHCG) o Chronic Assisted Ventilator (GRH only) o o Ischemic o Hemorrhagic Stroke Rehab: Program Readiness Date: Complex
o General Rehabilitation Low Intensity Rehabilitation (GRH, SJHCG) o (CMH, GRH, SJHCG) o Chronic Assisted Ventilator (GRH only) o o Ischemic o Hemorrhagic Stroke Rehab: Program Readiness Date: Complex
Navigating the New CMS Quality Measures
 Navigating the New CMS Quality Measures Dawn Murr-Davidson RN, BSN Director of Quality Initiatives Pennsylvania Health Care Association 1 Objectives Discuss the CMS Nursing Home Compare new quality measures
Navigating the New CMS Quality Measures Dawn Murr-Davidson RN, BSN Director of Quality Initiatives Pennsylvania Health Care Association 1 Objectives Discuss the CMS Nursing Home Compare new quality measures
Chapter 6 Section 3. Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment)
") Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Understanding the PEPPER
 Understanding the PEPPER and What It Means to Your IRF FIM, UDS-PRO, and UDSMR are trademarks of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc. Sue Gehrman,
Understanding the PEPPER and What It Means to Your IRF FIM, UDS-PRO, and UDSMR are trademarks of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc. Sue Gehrman,
Department of Veterans Affairs VHA DIRECTIVE Veterans Health Administration Washington, DC December 7, 2005
 Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
5/11/2017. Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC. It s official!
 Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC It s official! 2 1 Capturing the services and resident characteristics provided to Medicare A residents in specific timeframes. Determining the Medicare payment
Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC It s official! 2 1 Capturing the services and resident characteristics provided to Medicare A residents in specific timeframes. Determining the Medicare payment
11/18/2013 MDS 3.0 RAI MANUAL CHAPTER 1 RAI MANUAL CHAPTER 1 1.8, 1-16, 1-17, I-18
 MDS 3.0 CHANGES EFFECTIVE 10-1-2013 RAI MANUAL CHAPTER 1 1.8, 1-16, 1-17, I-18 Support Agency Contractors to assist in accomplishment of a CMS function. To assist another Federal or SA.for purposes of
MDS 3.0 CHANGES EFFECTIVE 10-1-2013 RAI MANUAL CHAPTER 1 1.8, 1-16, 1-17, I-18 Support Agency Contractors to assist in accomplishment of a CMS function. To assist another Federal or SA.for purposes of
Framework for Post-Acute Care: Current and Future Issues for Providers
 Framework for Post-Acute Care: Current and Future Issues for Providers Alan G. Rosenbloom Alliance for Quality Nursing Home Care March 2012 Overview of Presentation Post-Acute Care: Background and Trends
Framework for Post-Acute Care: Current and Future Issues for Providers Alan G. Rosenbloom Alliance for Quality Nursing Home Care March 2012 Overview of Presentation Post-Acute Care: Background and Trends
RUG-III V ERSION 5.20 CALCULATION WORKSH E E T 34 GROUP MOD E L F OR MDS 3.0
 RUG-III V ERSION 5.20 CALCULATION WORKSH E E T 34 GROUP MOD E L F OR MDS 3.0 This RUG-III Version 5.20 calculation worksheet is a step-by-step walk through to manually determine the appropriate RUG-III
RUG-III V ERSION 5.20 CALCULATION WORKSH E E T 34 GROUP MOD E L F OR MDS 3.0 This RUG-III Version 5.20 calculation worksheet is a step-by-step walk through to manually determine the appropriate RUG-III
Interdisciplinary Rehabilitation for Stroke
 Interdisciplinary Rehabilitation for Stroke Jessica Berry, MD Natasa Miljkovic, MD, PhD Antonette Murphy, RN, BSN, Clinician Kelly Vitti, PT, GCS, NCS Role of the PM&R Physician Consultation in acute care
Interdisciplinary Rehabilitation for Stroke Jessica Berry, MD Natasa Miljkovic, MD, PhD Antonette Murphy, RN, BSN, Clinician Kelly Vitti, PT, GCS, NCS Role of the PM&R Physician Consultation in acute care
Prior Authorization form for Post-Acute Care Admission and Recertification for SNF,LTAC and Rehab
 Prior Authorization form for Post-Acute Care Admission and Recertification for SNF,LTAC and Rehab (Required for all Rehab, SNF, LTAC admits) Providers must request authorization for initial admissions
Prior Authorization form for Post-Acute Care Admission and Recertification for SNF,LTAC and Rehab (Required for all Rehab, SNF, LTAC admits) Providers must request authorization for initial admissions
Determining the Appropriate Inpatient Rehabilitation Candidate
 Determining the Appropriate Inpatient Rehabilitation Candidate Brandi Damron, OTR/L, MBA Program Director Norton Community Hospital Inpatient Rehab Unit Objectives Discuss the preadmission process limitations
Determining the Appropriate Inpatient Rehabilitation Candidate Brandi Damron, OTR/L, MBA Program Director Norton Community Hospital Inpatient Rehab Unit Objectives Discuss the preadmission process limitations
Regulatory Compliance Risks. September 2009
 Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
RUG-III VERSION 5.2 CALCULATION WORKSHEET 34 GROUP MODEL
 RUG-III VERSION 5.2 CALCULATION WORKSHEET 34 GROUP MODEL This RUG-III Version 5.2 calculation worksheet is a step-by-step walk through to manually determine the appropriate RUG-III classification based
RUG-III VERSION 5.2 CALCULATION WORKSHEET 34 GROUP MODEL This RUG-III Version 5.2 calculation worksheet is a step-by-step walk through to manually determine the appropriate RUG-III classification based
NORTH DAKOTA LEVEL OF CARE FORM INSTRUCTIONS TO BE USED WITH LOC FORM ND
 For this section, select which type of LOC screen is to be reviewed Requested Screen Type NORTH DAKOTA LEVEL OF CARE FORM INSTRUCTIONS Nursing Facility Swingbed CMFN PACE MFP Provisional MFP Final Tech.
For this section, select which type of LOC screen is to be reviewed Requested Screen Type NORTH DAKOTA LEVEL OF CARE FORM INSTRUCTIONS Nursing Facility Swingbed CMFN PACE MFP Provisional MFP Final Tech.
Maximizing your Medicaid Rate
 Maximizing your Medicaid Rate RICK HOLLOWAY, ADMINISTRATOR IDAHO STATE VETERANS HOME-BOISE OCTOBER 6, 2016 Outline and Objectives Can you impact your Medicaid rate What goes into your Medicaid rate What
Maximizing your Medicaid Rate RICK HOLLOWAY, ADMINISTRATOR IDAHO STATE VETERANS HOME-BOISE OCTOBER 6, 2016 Outline and Objectives Can you impact your Medicaid rate What goes into your Medicaid rate What
11/23/2011. Proactive vs. Reactive Relationship
 Overview Focus on Resident Voice Assessment Schedule EOT OMRA and New Resumption Items New PPS Assessment: COT OMRA CMS Clarifications Coding New Quality Measures Draft MDS and Care Planning as Risk Management
Overview Focus on Resident Voice Assessment Schedule EOT OMRA and New Resumption Items New PPS Assessment: COT OMRA CMS Clarifications Coding New Quality Measures Draft MDS and Care Planning as Risk Management
Maximizing your Medicaid Rate
 Maximizing your Medicaid Rate RICK HOLLOWAY, ADMINISTRATOR IDAHO STATE VETERANS HOME-BOISE APRIL 26, 2017 Outline and Objectives Can you impact your Medicaid rate What goes into your Medicaid rate What
Maximizing your Medicaid Rate RICK HOLLOWAY, ADMINISTRATOR IDAHO STATE VETERANS HOME-BOISE APRIL 26, 2017 Outline and Objectives Can you impact your Medicaid rate What goes into your Medicaid rate What
Clinical RUG-IV. RUG Qualifiers & Length of Stay. Part 1. for clients of: Content developed and presented by:
 Clinical RUG-IV RUG Qualifiers & Length of Stay Part 1 for clients of: www.teamtsi.com 800.765.8998 Content developed and presented by: 3030 N. Rocky Point Drive, Suite 240 Tampa, FL 33607 800.275.6252
Clinical RUG-IV RUG Qualifiers & Length of Stay Part 1 for clients of: www.teamtsi.com 800.765.8998 Content developed and presented by: 3030 N. Rocky Point Drive, Suite 240 Tampa, FL 33607 800.275.6252
Payment Rule Summary. Medicare Inpatient Psychiatric Facility Prospective Payment System: Update Notice for Federal Fiscal Year 2013
 Payment Rule Summary Medicare Inpatient Psychiatric Facility Prospective Payment System: Update Notice for Federal Fiscal Year 2013 August 2012 Table of Contents Overview and Resources... 2 Inpatient Psychiatric
Payment Rule Summary Medicare Inpatient Psychiatric Facility Prospective Payment System: Update Notice for Federal Fiscal Year 2013 August 2012 Table of Contents Overview and Resources... 2 Inpatient Psychiatric
5/26/2016. What's New? What's Changed? Urgent Updates QM Manual v10. Faculty Disclosure. Requirements for Successful Completion
 What's New? What's Changed? Urgent Updates QM Manual v10 Presented by: Judi Kulus, MSN, MAT, RN, NHA, RAC-MT, DNS-CT VP of Curriculum Development jkulus@aanac.org Faculty Disclosure I have no financial
What's New? What's Changed? Urgent Updates QM Manual v10 Presented by: Judi Kulus, MSN, MAT, RN, NHA, RAC-MT, DNS-CT VP of Curriculum Development jkulus@aanac.org Faculty Disclosure I have no financial
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Stakeholder input is gathered in several ways. Patients are given the opportunity to provide feedback, the SWOT analysis is based on information from
 Strategic Plan 27 Executive Summary The following is a summary of the information shared in this Operations Review and Plan. This plan highlights operational achievements and challenges, clinical outcomes
Strategic Plan 27 Executive Summary The following is a summary of the information shared in this Operations Review and Plan. This plan highlights operational achievements and challenges, clinical outcomes
Medicare Home Health Prospective Payment System Calendar Year 2015
 Proposed Rule Summary Medicare Home Health Prospective Payment System Calendar Year 2015 August 2014 1 P age TABLE OF CONTENTS Overview, Resources and Comment Submission... 1 Home Health Payment Rates...
Proposed Rule Summary Medicare Home Health Prospective Payment System Calendar Year 2015 August 2014 1 P age TABLE OF CONTENTS Overview, Resources and Comment Submission... 1 Home Health Payment Rates...
Understanding Levels of Rehab for Effective Discharge Planning
 Understanding Levels of Rehab for Effective Discharge Planning Rose M. Turner, RN, BSN, ACM Thursday, January 22 nd, 2015 The information provided in AHC Media Webinars does not, and is not intended to
Understanding Levels of Rehab for Effective Discharge Planning Rose M. Turner, RN, BSN, ACM Thursday, January 22 nd, 2015 The information provided in AHC Media Webinars does not, and is not intended to
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play?
 Programs: What Role Should Compliance Play?") Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance