Increasing efficiency in the ED: Evidence based guidelines as a driver for quality
|
|
|
- Brandon Wells
- 5 years ago
- Views:
Transcription



1 Increasing efficiency in the ED: Evidence based guidelines as a driver for quality Charles G. Macias MD, MPH Associate Professor of Pediatrics/Section of Emergency Medicine Director of the Center for Clinical Effectiveness Baylor College of Medicine/Texas Children s Hospital Houston, Texas
2 Disclosures I do not have any relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this presentation



3 Future of Emergency Care
4 June 15, 2006 Emergency medical care in the United States is on the verge of collapse As a system it provides care of variable and often unknown quality
5 One definition of quality The degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge KN Lohr, N Engl J Med, 1990
6 Scientific judgment Preference Judgment Evidence Analyze Evidence Benefits, harms and costs Decisions Outcomes Adapted from D Eddy MD, PhD
7 Decision making and quality Evidence & Scientific judgment Evaluation Recommendation Transparency: Preference values and Judgment preferences Evidence Analyze Shared Evidence baseline Benefits, Data harms and costs transformation High quality care Decisions Performance measures Outcomes
8 Why does it matter? A parallel example RCT of treatment of hypertension on the jobsite (a steel mill) versus referral to the PCP No difference in compliance between the groups Exploration of factors relating to therapy revealed specific determinants of the clinical decision to treat some, but not other, hypertensive patients: 1. The level of diastolic blood pressure. 2. The patient s age. 3.???? 4. The amount of target-organ damage.
9 A parallel example RCT of treatment of hypertension on the jobsite (a steel mill) versus referral to the PCP No difference in compliance between the groups Exploration of factors relating to therapy revealed specific determinants of the clinical decision to treat some, but not other, hypertensive patients: 1. The level of diastolic blood pressure. 2. The patient s age. 3. The year the physician graduated from medical school 4. The amount of target-organ damage.
10 The purpose of EBGs: minimizing variation Wide variations in practice are often not related to differences among patients Minimizing variations in practice can improve quality of health care delivery Variation in beliefs Variation in interpretation of evidence Variation in response when evidence is lacking Does this variation exist in emergency medicine?

11 Variation in ED practice Entity Population Study Variation Acute asthma Eastern Ontario Lougheed, Chest 2009 Systemic steroids, PEFR, referrals to asthma services Asthma admissions Ontario Lougheeed Chest fold variation in hospitalization rates for asthma influenced by variation in % ED pts admitted Trauma facility utilization California Wang Ann Emerg Med 2008 Trauma center hospitalization varied by distance of residence, presence of private insurance Periorbital cellulitis Vancouver Goldman Ped Emerg Care 2008 po vs IV antibiotics Variation in decision for hospitalization AGE PHIS Tieder Pediatrics 2009 Variation in resource use: electrolytes, stool studies, UA/Ucx, antibiotics, antiemetics Retropharyngeal abscess KID 2003 Lander Int J Pediatr Oto Variation in hospitalization; Midwest had decreased total charges and LOS 2008
12 Empowering the art of medicine Evidence based guidelines help control complexity Analytic methods to understand outcomes Divide and conquer for different personnel Reductionism to a more efficient functioning Pareto principle 80/20 rule 20% of the problems cause 80% of the trouble 80% of the benefit will come from 20% of the opportunities


13 Art is in the eye of the beholder
14 Creating EBGs: 1. Identifying the quality gaps Targeting areas for quality improvement High prevalence Marked variations in care Resource intensive care High morbidity or mortality
15
16 Team Creating EBGs: 2. Assembling a team Community or Subject Area Practitioner Leader Champion of Guideline topic Sub-specialists in the area of focus Nurses Pharmacist Other Allied Healthcare providers (RTs, OT/PT, etc.) Family / patient Clinical Effectiveness and other support Bottom-up team building and interdisciplinary care are fundamentals of quality improvement Facilitator Methodologist Librarian Data analyst and outcomes coordinator Educator
17 Creating EBGs: 3. Identifying the questions in PICO format P population In ED patients with bronchiolitis I intervention does nebulized hypertonic saline C comparison when compared to standard therapy 0 outcome of interest prevent admission, shorten ED stay, etc.

18 Creating EBGs: 4. Conducting the search

19 Creating EBGs: 5. Evaluating the Evidence Evidence hierarchy
20 Grading of Recommendations, Assessment, Development and Evaluation Recommendations Strong Weak Evidence quality High Moderate Low Very low
21 Guideline appraisal of existing guidelines AGREE (Appraisal of Guidelines Research and Evaluation) Becoming industry standard 23 item list with six domains scope and purpose stakeholder involvement rigor of development clarity and presentation applicability editorial independence
22 When the evidence is lacking Standardize (goal of a guideline) Revisit evidence frequently and rigorously Clinical/outcomes research to increase evidence base

23 EBG Complete EBG Implementation Rubenstein, J Gen Intern Med 2006

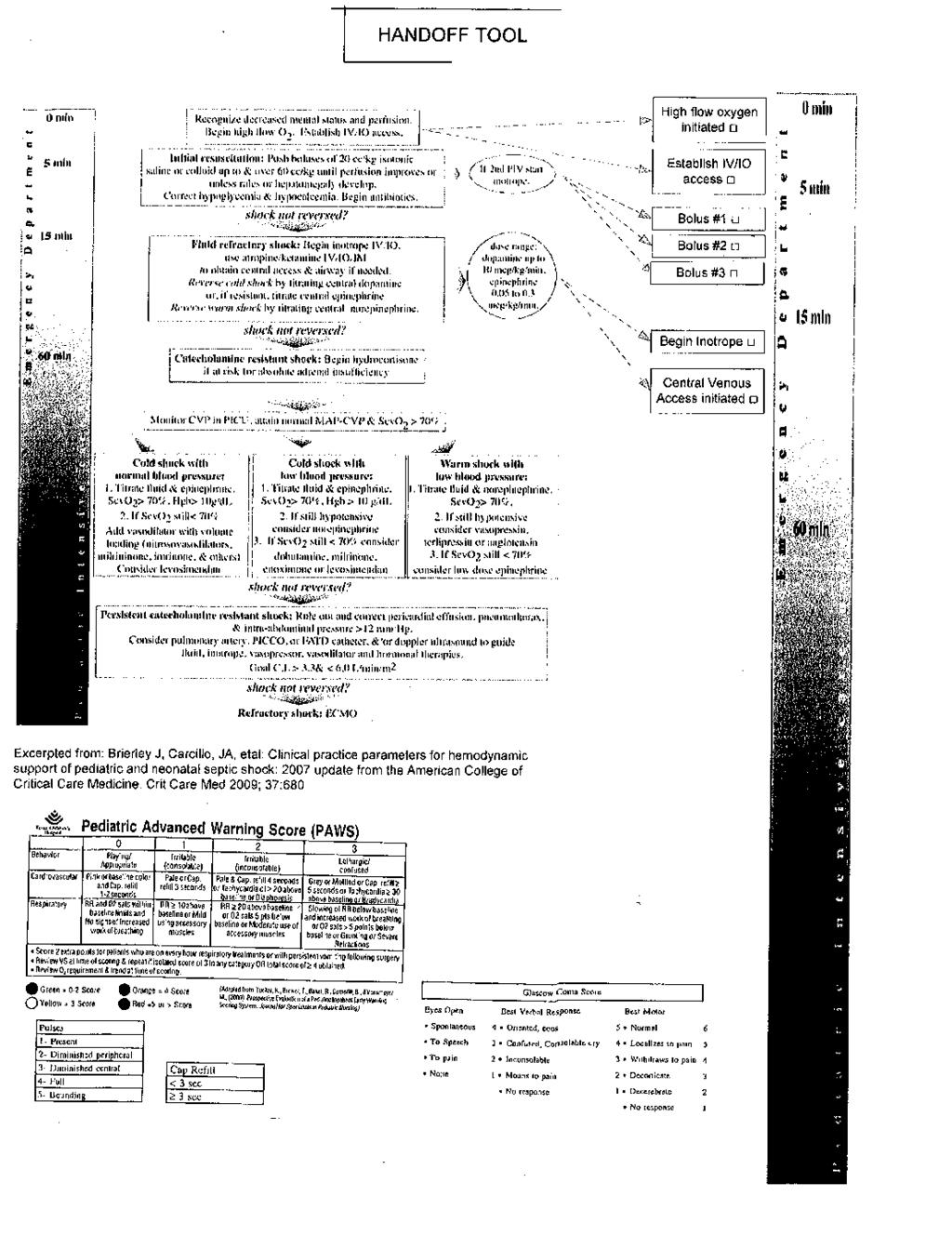
24 Age-specific goal directed therapy ER: 1 st hour fluid resuscitation and inotrope therapy Therapeutic endpoints: Threshold heart rate Normal blood pressure Capillary refill 2 sec Normal pulses Warm extremities Normal glucose and ionized calcium Monitoring Recommendations: Airway and breathing Circulation Fluid resuscitation Hemodynamic support Hydrocortisone therapy Ongoing ICU hemodynamic support Central venous oxygen saturation >70% Cardiac Index L/min/m 2 Brierley J, et al, Crit Care Med 2009 Vol. 37(1), 1-23.

25 Shock reversal resulted in better survival *p <.001 Multiple logistic regression analyses revealed time-dependent relationships between persistent shock and delayed ACCCM- PALS-directed resuscitation with poor outcome Variable Mortality Odds Ratio 95% Confidence Interval p <.001 Improved mortality by 38% Number Needed to Treat = 3.3 Duration of persistent shock (per 1-hour increment) Delay in resuscitation consistent with ACCM-PALS Guidelines (per 1-hour increment) Han et al., Pediatrics 2003
26 Evidence for goal directed therapy PI Study Population Outcome Ninis BMJ 2005 Meningococcal septic shock 22.6 adjusted mortality OR with delay in inotrope resuscitation de Oliveira Intensive Care Med 2008 Shock with continuous central venous oxygen sat monitoring RCT: Goal directed therapy via 2002 guidelines decreased mortality from 39% to 12% (NNT 3.6) Karapinar Crit Care Med 2004 Tertiary care center patients in fluid refractory shock Before/after 28 day mortality of targeted goal: 3% otherwise healthy and 9% chronically ill Maat Crit Care 2007 Referral, transport and tertiary care center Reduction in mortality rate from purpura and severe sepsis to 1% (ARR of 19%)
27 Shock management at TCH: 2009 Time to FIRST bolus: 53 min Time to THIRD bolus: 152 min Time to first antibiotic: 127 min Time to PICU: 260 min
28 The team ED: B Patel MD ED: A Perry MD ED/ID: A Cruz MD, MPH Nursing: E Wuestner RN PICU: E Williams MD Transport: J Graf MD Nursing administration: E Fredeboelling RN
29 Model for communication

30 I hate you more! Emergency center Intensive care unit Courtesy of Eric Williams MD
31

32 Triage best practice alert

33 From 53 to 23 min

34 From 152 to 67 min

35 From 127 to 37 min
36 Sample Mean Balance measures Arrival to Admit for Acuity 2 Patients UCL= _ X= LCL= Week Tests performed with unequal sample sizes
37 The outcome A reduction in morbidity A projected 38% reduction in mortality 10 year costs of sepsis related lawsuit settlements: TCH: $2.5 million (actual costs) BCM: $1.25 million (estimated costs) Total projected 10 year savings: $1.4 million Costs of lawsuits courtesy of L Sessions
38 ED Length of Stay (in mintues) LOS in ED for AGE Moving Average Chart of Length of Stay in ED Before and After Introduction of ORT 500 BEFORE AFTER UCL=257.8 _ X=221.9 LCL= ED patients with chief complaint of vomiting or diarrhea and dx of AGE, vomiting or diarrhea
39 Gains: capacity measures Time savings Total ED hours Number of patients/year 33 min 3646 hours 691 patients Goal (d): 58 min 6409 hours 1216 patients Goal (v): 91 min hours 1908 patients Financial implications: $250,000 to 1.3 million contribution to margin Financial planning and reporting: Alec King and Carolyn Smith
40 Hours Bronchiolitis measures ED LOS RSV-LOS Bronch-LOS
41 Cost savings (bronchiolitis) Calculating cost savings inpatient Use # of Admits for Bronchiolitis (2009 = 583) Calculate days saved per year based upon ALOS decrease from 2006 pre EBG year Building capacity Use 2009 data to determine variable direct cost per day ($2011) Calculate savings in $128,965 Assumption: filling beds in early days with patients with higher margin per case Calculating capacity ED Building ED capacity because of shorter LOS in ED 2006 to 2009: ED LOS decreased 2.91 hours for bronchiolitis x 1430 patients=4161 hours x avg LOS in 2009 (5.27 hrs)= 789 additional patients Could multiple by per patient revenue/margin for financial impact Contribution margin: 1.57 million Complex model with multiple caveats Financial planning and reporting: Alec King and Carolyn Smith
42 Not all EBGs are created equal Scientific judgment Preference Judgment Evidence Analyze Evidence Benefits, harms and costs Decisions Outcomes based Evidence Preference Consensus based Based based Outcomes Adapted from D Eddy MD, PhD
43 Questions? The Center for Clinical Effectiveness Knowledge translation research Process mapping/age Bronchiolitis/financial measures
44 Centers of Excellence Health Services Research Data Transformation the Center for Clinical Effectiveness Policy and Advocacy Patient Safety Education and Community Outreach Evidence Based Outcomes Center Health Information Technology Integration
45 Knowledge translation Adapted from Tugwell J Chron Dis 1985
46 Acute Gastroenteritis EBG AGE multi-disciplinary team included: P Nag MD J Tran MD C Allen MD S Patel MD M Gilger MD C Davis RN A Hope C Conkin, MS, RD EBOC specialist: Q Franklin, MS EBOC implementation specialist: E Crabtree
47
48 BEGIN Patient presents to Emergency Dept (ED). Does patient have vomiting &/ or diarrhea Flow chart of a patient with acute gastroenteritis through the TCH Emergency Department: Existing process Evaluate per clinical symptoms 4 Patient discharged home 1 3 Patient transferred to inpatient bed 2 Fellow/ Attending does pretransfer check PCA checks vital signs Patient registers Patient waiting Triage nurse does the following: Vitals What is the patient s level of dehydration? Key: solid arrow indicates yes broken arrow indicates no 1 Outcome: Time in ED 2 Outcome: Time to inpatient bed 3 Outcome: Length of stay (LOS) 4 Outcome: Revisit from ED discharge 4 Outcome: Revisit from inpatient discharge Nurse discharges patient Nurse-Nurse checkout occurs Bed approved Patient evaluated by triage nurse Severe dehydration Mild or Moderate dehydration PCA checks vital signs ED secretary requests bed Is the patient vomiting? MD does discharge orders MD does admission orders Put patient in ED room Follow TCH AGE clinical algorithm Triage nurse does the following: Give Zofran Provide gatorade/pedialyte Triage nurse does the following: Nothing or give patient gatorade/ pedialyte Decision to discharge patient Is the patient ok for discharge? Decision to admit patient Patient waiting Patient put in ED room Patient evaluated by nurse Patient evaluated by Medical student Patient evaluated by ED resident Patient evaluated by ED fellow Patient evaluated by ED attending Process map before EBG Modified: 7/21/2009
49 EBG leverage points
50
51 The ORT tracking sheet Texas Children s Hospital Emergency Department Oral Rehydration Therapy Tracking Sheet For Parents Texas Children s Hospital Emergency Department Oral Rehydration Therapy Tracking Sheet Nurse/Physician Documentation Area Parents: Your child has been vomiting and/or has diarrhea and needs clear fluid by a syringe. Your child needs small frequent amounts so they will not vomit. Follow the 5 steps below. 1. Give your child ½ of a syringe, then wait 5 minutes. 2. Give your child 1 full syringe, then wait 5 minutes. 3. Give your child 2 full syringes, then wait 5 minutes. * If your child vomits, wait 10 minutes times and start again. If your child vomits 3.,tell a nurse 4: If your child does not vomit, then give your child 3 full syringes every 5 minutes. * Please mark a box below for every syringe your child takes. Number of syringes taken. Mark a box with an X for each syringe taken. Patient Sticker: Weight kg Fluid Pedialyte (if < 1 year old) Gatorade (if > 1 year old) Patient Age: (in months if < 3 years old, and in years if > 3 years old) Triage assessment of dehydration In ED room assessment of dehydration Patient received ondansetron (zofran) Patient received intravenous fluid Nurse Documentation Area Time Gorelick Score HR Signature of nurse verifying the above documentation upon final disposition: Resident assessment of dehydration NP/PA/Fellow/ Attending assessment of dehydration Physician Documentation Area Resident, NP/PA/Fellow/Attending Time Gorelick Score HR Total amount of fluid PO: cc Total episodes of emesis: Total episodes of diarrhea: Gorelick score (long form) Poor overall appearance Sunken eyes Decreased skin elasticity 5. Please come back to the nurse in 90 minutes at : for them to check on your child. Capillary refill > 2 seconds Abnormal respirations Decreased urine output Absent tears Abnormal radial pulse Dry mucous membranes Tachycardia (HR >150) < 7 points $ No /Mild/ Moderate dehydration 7 points $ Severe dehydration
52 BEGIN Patient presents to Emergency Dept (ED). Patient registers Patient waiting Flow chart of a patient with acute gastroenteritis through the TCH Emergency Deparment Does patient have vomiting &/ or diarrhea Triage nurse does the following: Vitals Assess dehydration (Gorelick score)** What is the patient s level of dehydration? Evaluate per clinical symptoms Key: solid arrow indicates yes broken arrow indicates no ** New process 1 Outcome: Time in ED 2 Outcome: Time to inpatient bed 3 Outcome: Length of stay (LOS) 4 Outcome: Revisit from ED discharge 4 Outcome: Revisit from inpatient discharge 4 Patient discharged home 1 Nurse discharges patient 3 Patient transferred to inpatient bed 2 Collect ORT tracking sheet Fellow/ Attending does pretransfer check PCA checks vital signs Nurse-Nurse checkout occurs Bed approved Patient evaluated by triage nurse Severe dehydration Mild or Moderate dehydration PCA checks vital signs ED secretary requests bed Is the patient vomiting? MD does discharge orders MD does admission orders Put patient in ED room Follow TCH AGE clinical algorithm Triage nurse does the following: Give Zofran Provide patient education on ORT Initiate ORT Give ORT tracking sheet** Triage nurse does the following: Provide patient education on ORT Initiate ORT Give ORT tracking sheet** Decision to discharge patient Is the patient ok for discharge? Decision to admit patient Patient waiting Patient put in ED room Patient evaluated by nurse Patient evaluated by Medical student Patient evaluated by ED resident Patient evaluated by ED fellow Patient evaluated by ED attending Bedside nurse does the following: Assesses dehydration (Gorelick score)** Monitors progress on ORT tracking sheet** Reemphasizes patient education on ORT ED Fellow does the following: Assesses dehydration (Gorelick score)** Monitors progress on ORT tracking sheet** Reemphasizes patient education on ORT Determines patient disposition Process map after EBG Modified: 5/9/2009
53 ED Length of Stay (in mintues) LOS in ED for AGE Moving Average Chart of Length of Stay in ED Before and After Introduction of ORT 500 BEFORE AFTER UCL=257.8 _ X=221.9 LCL= ED patients with chief complaint of vomiting or diarrhea and dx of AGE, vomiting or diarrhea
54 Gains: capacity measures Time savings Total ED hours Number of patients/year 33 min 3646 hours 691 patients Goal (d): 58 min 6409 hours 1216 patients Goal (v): 91 min hours 1908 patients Financial implications: $250,000 to 1.3 million contribution to margin Financial planning and reporting: Alec King and Carolyn Smith
55 Bronchiolitis EBG Multi-disciplinary team included: Y Han MD M McPherson MD B Hogan MD R Moore MD R Wolf RN S Iniquez RCP S Kim PharmD C Jones, EBOC specialist
56 Phase 1: Implementation focus on ED ED Visits for Bronchiolitis Total
57 Bronchiolitis Disposition from ED 80% 70% 60% 50% 40% 30% 20% 10% 0% % discharged % admitted No change in severity by CRS score
58 Hours Bronchiolitis measures ED LOS RSV-LOS Bronch-LOS
59 percentage use Bronchiolitis measures Bronchiolitis measures across the continuum IV Abx Epi Bronchodilator CXR Steroid
60 Cost savings (bronchiolitis) Calculating cost savings inpatient Use # of Admits for Bronchiolitis (2009 = 583) Calculate days saved per year based upon ALOS decrease from 2006 pre EBG year Building capacity Use 2009 data to determine variable direct cost per day ($2011) Calculate savings in $128,965 Assumption: filling beds in early days with patients with higher margin per case Calculating capacity ED Building ED capacity because of shorter LOS in ED 2006 to 2009: ED LOS decreased 2.91 hours for bronchiolitis x 1430 patients=4161 hours x avg LOS in 2009 (5.27 hrs)= 789 additional patients Could multiple by per patient revenue/margin for financial impact Contribution margin: 1.57 million Complex model with multiple caveats Financial planning and reporting: Alec King and Carolyn Smith
61 Objectives 1. To define the role of evidence based guidelines in medical decision making. 2. To describe strategies for the effective creation and implementation of guidelines. 3. To understand the relationship of evidence based guidelines to quality improvement. 4. To discuss strategies for linking measures and outcomes to guideline implementation. This discussion will focus on the merger of science and operations, both critical for high quality health care delivery.
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016
 Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Managing Population Health with Science, Analytics, and Quality Improvement
 Managing Population Health with Science, Analytics, and Quality Improvement Charles G Macias MD, MPH Chief Clinical Systems Integration Officer Texas Children s DISCLAIMER: The views and opinions expressed
Managing Population Health with Science, Analytics, and Quality Improvement Charles G Macias MD, MPH Chief Clinical Systems Integration Officer Texas Children s DISCLAIMER: The views and opinions expressed
Integrating Evidence- Based Pediatric Prehospital Protocols into Practice
 Integrating Evidence- Based Pediatric Prehospital Protocols into Practice Manish I. Shah, MD Assistant Professor of Pediatrics Program Director, EMS for Children State Partnership Texas Objectives To provide
Integrating Evidence- Based Pediatric Prehospital Protocols into Practice Manish I. Shah, MD Assistant Professor of Pediatrics Program Director, EMS for Children State Partnership Texas Objectives To provide
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
A Practical Framework for Measuring Higher-Order Cognitive Constructs: An Application to Measuring Nursing Clinical Judgment
 A Practical Framework for Measuring Higher-Order Cognitive Constructs: An Application to Measuring Nursing Clinical Judgment Ada Woo, PhD National Council of State Boards of Nursing 1 Outline Background
A Practical Framework for Measuring Higher-Order Cognitive Constructs: An Application to Measuring Nursing Clinical Judgment Ada Woo, PhD National Council of State Boards of Nursing 1 Outline Background
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING
 SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING Dr. Duncan Hargreaves QI Fellow Worthing Hospital Allied Health Sciences Network 2017 SEPSIS IMPROVEMENT AT WSHFT QUESTcollaboration ->
SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING Dr. Duncan Hargreaves QI Fellow Worthing Hospital Allied Health Sciences Network 2017 SEPSIS IMPROVEMENT AT WSHFT QUESTcollaboration ->
ASCO s Quality Training Program
 ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
EMR Surveillance Intervenes to Reduce Risk Adjusted Mortality March 2, 2016 Katherine Walsh, MS, DrPH, RN, NEA-BC Vice President of Operations,
 EMR Surveillance Intervenes to Reduce Risk Adjusted Mortality March 2, 2016 Katherine Walsh, MS, DrPH, RN, NEA-BC Vice President of Operations, Houston Methodist Hospital Michael Rothman, PhD, Chief Science
EMR Surveillance Intervenes to Reduce Risk Adjusted Mortality March 2, 2016 Katherine Walsh, MS, DrPH, RN, NEA-BC Vice President of Operations, Houston Methodist Hospital Michael Rothman, PhD, Chief Science
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE
 EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
APPLICATION FORM. Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes. Director of Quality
 APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
abstract QUALITY REPORT
 Implementation of an Inpatient Pediatric Sepsis Identification Pathway Chanda Bradshaw, MD, Ilyssa Goodman, MD, Rebecca Rosenberg, MD, MPH, Christopher Bandera, MD, Arthur Fierman, MD, Bret Rudy, MD BACKGROUND
Implementation of an Inpatient Pediatric Sepsis Identification Pathway Chanda Bradshaw, MD, Ilyssa Goodman, MD, Rebecca Rosenberg, MD, MPH, Christopher Bandera, MD, Arthur Fierman, MD, Bret Rudy, MD BACKGROUND
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
MEDICAL DIRECTIVE Critical Care Outreach Team (CCOT) Abdominal Pain
 Abdominal Pain") Authorizing physician(s) Intensivists who are part of the Critical Care Physician Section Authorized to who CCOT Responders (RRTs and RNs) that have the knowledge, skill and judgment and who have successfully
Authorizing physician(s) Intensivists who are part of the Critical Care Physician Section Authorized to who CCOT Responders (RRTs and RNs) that have the knowledge, skill and judgment and who have successfully
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Respiratory Clinical Review of Patients with Community Acquired Pneumonia
 Respiratory Clinical Review of Patients with Community Acquired Pneumonia DrPeter Wu Staff Specialist Department of Respiratory & Sleep Medicine Westmead Hospital Western Sydney Local Health District How
Respiratory Clinical Review of Patients with Community Acquired Pneumonia DrPeter Wu Staff Specialist Department of Respiratory & Sleep Medicine Westmead Hospital Western Sydney Local Health District How
5/9/2015. Disclosures. Improving ICU outcomes and cost-effectiveness. Targets for improvement. A brief overview: ICU care in the United States
 Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Early Management Bundle, Severe Sepsis/Septic Shock
 Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Supplementary Online Content
 Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
Presenters. Tiffany Osborn, MD, MPH. Laura Evans, MD MSc. Arjun Venkatesh, MD, MBA, MHS
 Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Clinical Operations in a Service Line Model
 Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line Development Jill Castaneda Project Manager,
Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line Development Jill Castaneda Project Manager,
National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI)
") October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
Observation Unit. Romil Chadha
 Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
The impact of nighttime intensivists on medical intensive care unit infection-related indicators
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 The impact of nighttime intensivists on medical intensive care unit infection-related indicators Abhaya Trivedi
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 The impact of nighttime intensivists on medical intensive care unit infection-related indicators Abhaya Trivedi
Patient Safety and Quality Measures for CRRT: The UAB Experience. Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012
 Patient Safety and Quality Measures for CRRT: The UAB Experience Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012 Quality Healthcare Quality is the extent to which health services for
Patient Safety and Quality Measures for CRRT: The UAB Experience Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012 Quality Healthcare Quality is the extent to which health services for
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
ICU Research Using Administrative Databases: What It s Good For, How to Use It
 ICU Research Using Administrative Databases: What It s Good For, How to Use It Allan Garland, MD, MA Associate Professor of Medicine and Community Health Sciences University of Manitoba None Disclosures
ICU Research Using Administrative Databases: What It s Good For, How to Use It Allan Garland, MD, MA Associate Professor of Medicine and Community Health Sciences University of Manitoba None Disclosures
Launching an Enterprise Data Warehouse to Rapidly Reduce Waste in Asthma Care
 Success Story Launching an Enterprise Data Warehouse to Rapidly Reduce Waste in Asthma Care HEALTHCARE ORGANIZATION Children s Hospital TOP RESULTS Decreased average length of stay by 11 hours Achieved
Success Story Launching an Enterprise Data Warehouse to Rapidly Reduce Waste in Asthma Care HEALTHCARE ORGANIZATION Children s Hospital TOP RESULTS Decreased average length of stay by 11 hours Achieved
Bronchiolitis and Hypoxia: Discharge on Oxygen from the ED is a viable alternative to hospital admission
 Bronchiolitis and Hypoxia: Discharge on Oxygen from the ED is a viable alternative to hospital admission Lalit Bajaj MD, MPH Associate Professor of Pediatrics and Emergency Medicine Medical Director, Clinical
Bronchiolitis and Hypoxia: Discharge on Oxygen from the ED is a viable alternative to hospital admission Lalit Bajaj MD, MPH Associate Professor of Pediatrics and Emergency Medicine Medical Director, Clinical
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Clinical Safety & Effectiveness Cohort # 8
 Clinical Safety & Effectiveness Cohort # 8 1 IMPROVING THE TIMELINESS OF PARACENTESIS: IMPACT OF A PROCEDURE TEAM DATE Educating for Quality Improvement & Patient Safety FINANCIAL DISCLOSURE Patricia Wathen,
Clinical Safety & Effectiveness Cohort # 8 1 IMPROVING THE TIMELINESS OF PARACENTESIS: IMPACT OF A PROCEDURE TEAM DATE Educating for Quality Improvement & Patient Safety FINANCIAL DISCLOSURE Patricia Wathen,
Painful Infusions of Potassium A Potassium Protocol. Eve Holderman, BSN, RN, CPAN October 21, 2017 NYSPANA State Conference
 Painful Infusions of Potassium A Potassium Protocol Eve Holderman, BSN, RN, CPAN October 21, 2017 NYSPANA State Conference Objective To identify strategies for intervention when the patient experiences
Painful Infusions of Potassium A Potassium Protocol Eve Holderman, BSN, RN, CPAN October 21, 2017 NYSPANA State Conference Objective To identify strategies for intervention when the patient experiences
IMPACT OF RN HYPERTENSION PROTOCOL
 1 IMPACT OF RN HYPERTENSION PROTOCOL Joyce Cheung, RN, Marie Kuzmack, RN Orange County Hypertension Team Kaiser Permanente, Orange County Joyce.m.cheung@kp.org and marie-aline.z.kuzmack@kp.org Cell phone:
1 IMPACT OF RN HYPERTENSION PROTOCOL Joyce Cheung, RN, Marie Kuzmack, RN Orange County Hypertension Team Kaiser Permanente, Orange County Joyce.m.cheung@kp.org and marie-aline.z.kuzmack@kp.org Cell phone:
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
2018 DOM HealthCare Quality Symposium Poster Session
 Winner - Outstanding Faculty Project Author Hillary Lum, MD, Faculty Division/Department Geriatric Medicine / Department of Medicine UCHealth Patient use of a Medical Power of Attorney via My Health Connection
Winner - Outstanding Faculty Project Author Hillary Lum, MD, Faculty Division/Department Geriatric Medicine / Department of Medicine UCHealth Patient use of a Medical Power of Attorney via My Health Connection
Goals today 6/14/2011. Disclosures, 2004-May Sepsis A Medical Emergency. Jim O Brien, MD, MSc So what is sepsis anyway?
 Jim O Brien, MD, MSc James.OBrien@osumc.edu Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Jim O Brien, MD, MSc James.OBrien@osumc.edu Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Barriers to Early Rehabilitation in Critically Ill Patients. Shannon Goddard, MD Sunnybrook Health Sciences Centre
 Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
Partnering with the Care Management Department. Medical Staff and Allied Health Practitioner Orientation
 Partnering with the Care Management Department Medical Staff and Allied Health Practitioner Orientation 10/2015 Department of Care Management Medical Directors of Care Coordination Inpatient Case Managers
Partnering with the Care Management Department Medical Staff and Allied Health Practitioner Orientation 10/2015 Department of Care Management Medical Directors of Care Coordination Inpatient Case Managers
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
St. Vincent s Health System Page 1 of 8. Nursing Administration HOSPITAL SHARED POLICY?
 St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
Select Medical TRANSITIONS OF CARE & CARE COORDINATION
 Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways
 For Patients not eligible for other TICKER Clinical Pathways") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
BC Pediatric Early Warning System (PEWS) for Emergency and Urgent Care Settings. Regional Workshops 2018
 for Emergency and Urgent Care Settings. Regional Workshops 2018") BC Pediatric Early Warning System (PEWS) for Emergency and Urgent Care Settings Regional Workshops 2018 1 By the end of this session you will be able to... Understand PEWS and explain reasons for using
BC Pediatric Early Warning System (PEWS) for Emergency and Urgent Care Settings Regional Workshops 2018 1 By the end of this session you will be able to... Understand PEWS and explain reasons for using
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Emergency Medical Services: More Than Just a Ride to the Hospital
 Emergency Medical Services: More Than Just a Ride to the Hospital Manish I. Shah, MD, MS Prehospital Domain Lead EMS for Children Innovation and Improvement Center Associate Professor Department of Pediatrics
Emergency Medical Services: More Than Just a Ride to the Hospital Manish I. Shah, MD, MS Prehospital Domain Lead EMS for Children Innovation and Improvement Center Associate Professor Department of Pediatrics
Study Title: Optimal resuscitation in pediatric trauma an EAST multicenter study
 Study Title: Optimal resuscitation in pediatric trauma an EAST multicenter study PI/senior researcher: Richard Falcone Jr. MD, MPH Co-primary investigator: Stephanie Polites MD, MPH; Juan Gurria MD My
Study Title: Optimal resuscitation in pediatric trauma an EAST multicenter study PI/senior researcher: Richard Falcone Jr. MD, MPH Co-primary investigator: Stephanie Polites MD, MPH; Juan Gurria MD My
NHS LOTHIAN Standard Operating Procedure: EHSCP Physiological Observations of Patients in the Community Setting
 NHS LOTHIAN Standard Operating Procedure: EHSCP Physiological Observations of Patients in the Community Setting 1. Introduction To standardise the type and frequency of observations to be taken on adult
NHS LOTHIAN Standard Operating Procedure: EHSCP Physiological Observations of Patients in the Community Setting 1. Introduction To standardise the type and frequency of observations to be taken on adult
South London Neonatal Network Hypoxic Ischemic Encephalopathy Transfer Guidelines. Version 1.0
 South London Neonatal Network Hypoxic Ischemic Encephalopathy Transfer Guidelines Version 1.0 Ratified: 28 th August 2018 Date for Review: 28 th August 2019 Suzanne.sweeney@uclpartners.com South London
South London Neonatal Network Hypoxic Ischemic Encephalopathy Transfer Guidelines Version 1.0 Ratified: 28 th August 2018 Date for Review: 28 th August 2019 Suzanne.sweeney@uclpartners.com South London
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
Thank you for joining us today!
 Thank you for joining us today! Please dial 1.800.732.6179 now to connect to the audio for this webinar. To show/hide the control panel click the double arrows. 1 Emergency Room Overcrowding A multi-dimensional
Thank you for joining us today! Please dial 1.800.732.6179 now to connect to the audio for this webinar. To show/hide the control panel click the double arrows. 1 Emergency Room Overcrowding A multi-dimensional
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Wired to Save Lives: A Virtual Hospital Experience
 Wired to Save Lives: A Virtual Hospital Experience Donald J. Kosiak, MD, MBA, FACEP, CPE Vice President for Medical Development Thursday, March 3 rd -- 11:30am Conflict of Interest Donald Kosiak, MD Has
Wired to Save Lives: A Virtual Hospital Experience Donald J. Kosiak, MD, MBA, FACEP, CPE Vice President for Medical Development Thursday, March 3 rd -- 11:30am Conflict of Interest Donald Kosiak, MD Has
Section: Emergency Department Application: Medical Center. Contact Person: Director, Emergency Services. Approved:
 Subject: Triage of Patients Core X General Recommended: Section: Emergency Department Application: Medical Center Contact Person: Director, Emergency Services Approved: Policy Number: ED 101 Date of Issue:
Subject: Triage of Patients Core X General Recommended: Section: Emergency Department Application: Medical Center Contact Person: Director, Emergency Services Approved: Policy Number: ED 101 Date of Issue:
COPD Management in the community
 COPD Management in the community Anne Jones Independent Respiratory Nurse Consultant RN,BSc(Hons),PGDip(RespMed)/MA Content of session Will consider the impact of COPD COPD Strategy recommendations and
COPD Management in the community Anne Jones Independent Respiratory Nurse Consultant RN,BSc(Hons),PGDip(RespMed)/MA Content of session Will consider the impact of COPD COPD Strategy recommendations and
Emergency. Best Critical Care Practices
 Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Jim O Brien, MD, MSc James.OBrien@osumc.edu Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Jim O Brien, MD, MSc James.OBrien@osumc.edu Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Predictive Analytics and the Impact on Nursing Care Delivery
 Predictive Analytics and the Impact on Nursing Care Delivery Session 2, March 5, 2018 Whende M. Carroll, MSN, RN-BC - Director of Nursing Informatics, KenSci, Inc. Nancee Hofmeister, MSN, RN, NE-BC Senior
Predictive Analytics and the Impact on Nursing Care Delivery Session 2, March 5, 2018 Whende M. Carroll, MSN, RN-BC - Director of Nursing Informatics, KenSci, Inc. Nancee Hofmeister, MSN, RN, NE-BC Senior
Fundamental Critical Care Support (FCCS)
") Provided By: Fundamental Critical Care Support (FCCS) Center for Advanced Medical Learning and Simulation (CAMLS) 124 S. Franklin, Tampa, Florida 33602 Needs Statement and Educational Gap: Early identification
Provided By: Fundamental Critical Care Support (FCCS) Center for Advanced Medical Learning and Simulation (CAMLS) 124 S. Franklin, Tampa, Florida 33602 Needs Statement and Educational Gap: Early identification
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems NPSS Asheville, NC
 Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Assessment and Reassessment of Patients
 Approved by: Assessment and Reassessment of Patients Senior Director, Operations, Emergency, Medicine, Critical Care & Respiratory - GNCH Senior Director, Operations, Emergency, Medicine, Critical Care
Approved by: Assessment and Reassessment of Patients Senior Director, Operations, Emergency, Medicine, Critical Care & Respiratory - GNCH Senior Director, Operations, Emergency, Medicine, Critical Care
Hospital Clinical Documentation Improvement
 Hospital Clinical Documentation Improvement March 2016 Clinical Documentation Improvement (CDI) is a team approach to improving documentation practices through ongoing education, concurrent chart review
Hospital Clinical Documentation Improvement March 2016 Clinical Documentation Improvement (CDI) is a team approach to improving documentation practices through ongoing education, concurrent chart review
Next Gen Training. Why is Next Gen So Important? Step-by-Step Vitals Entry Scenarios and Mock Work-ups
 Next Gen Training Why is Next Gen So Important? Step-by-Step Vitals Entry Scenarios and Mock Work-ups Why is Next Gen So Important? Better for the VFC: All the necessary info can be accessed from any VFC
Next Gen Training Why is Next Gen So Important? Step-by-Step Vitals Entry Scenarios and Mock Work-ups Why is Next Gen So Important? Better for the VFC: All the necessary info can be accessed from any VFC
MEDICATION ADMINISTRATION: BELOW THE DRIP CHAMBER
 KINGSTON GENERAL HOSPITAL MEDICATION ADMINISTRATION: BELOW THE DRIP CHAMBER LEARNING GUIDE FOR REGISTERED NURSES AND REGISTERED PRACTICAL NURSES Prepared by: Nursing Education Date: 2001 November Revised:
KINGSTON GENERAL HOSPITAL MEDICATION ADMINISTRATION: BELOW THE DRIP CHAMBER LEARNING GUIDE FOR REGISTERED NURSES AND REGISTERED PRACTICAL NURSES Prepared by: Nursing Education Date: 2001 November Revised:
STANDARDIZED PROCEDURE ALLOGENEIC /AUTOLOGOUS HEMATOPOIETIC STEM CELL INFUSION (Adult, Peds)
") STANDARDIZED PROCEDURE I. Definition: The infusion of allogeneic /autologous hematopoietic progenitor cells as a part of hematopoetic stem cell transplant or donor lymphocyte infusion. II. Background Information
STANDARDIZED PROCEDURE I. Definition: The infusion of allogeneic /autologous hematopoietic progenitor cells as a part of hematopoetic stem cell transplant or donor lymphocyte infusion. II. Background Information
Valorie Sweigart, DNP g, Samuel Shartar, RN, CEN Emory Healthcare
 Valorie Sweigart, DNP g, Samuel Shartar, RN, CEN Emory Healthcare Why build Principles of observational medicine ROI ED Hospital Clinical implications Define intended d use Open, closed or mixed use Impact
Valorie Sweigart, DNP g, Samuel Shartar, RN, CEN Emory Healthcare Why build Principles of observational medicine ROI ED Hospital Clinical implications Define intended d use Open, closed or mixed use Impact
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
PG snapshot Nursing Special Report. The Role of Workplace Safety and Surveillance Capacity in Driving Nurse and Patient Outcomes
 PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs.
 6. Referral process Key findings A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs. Consultant physicians had no knowledge or input into
6. Referral process Key findings A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs. Consultant physicians had no knowledge or input into
Stampede Sepsis: A Statewide Collaborative
 Stampede Sepsis: A Statewide Collaborative Kentucky Sepsis Summit August 24, 2016 T E R I H U L E T T, R N, B S N, C I C, F A P I C P R O G R A M M A N A G E R, I N F E C T I O N P R E V E N T I O N CHA
Stampede Sepsis: A Statewide Collaborative Kentucky Sepsis Summit August 24, 2016 T E R I H U L E T T, R N, B S N, C I C, F A P I C P R O G R A M M A N A G E R, I N F E C T I O N P R E V E N T I O N CHA
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES
 CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES Manual Subject Emergency Medical Services Administrative Policies and Procedures First Responder Prehospital Care Report - BLS Policy Page 1 of 13 References
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES Manual Subject Emergency Medical Services Administrative Policies and Procedures First Responder Prehospital Care Report - BLS Policy Page 1 of 13 References
Private Duty Nursing (PDN) Eligibility Determination Workshop. A refresher course for current PIHP Nurses and initial training for new PIHP Nurses
 Eligibility Determination Workshop. A refresher course for current PIHP Nurses and initial training for new PIHP Nurses") Private Duty Nursing (PDN) Eligibility Determination Workshop A refresher course for current PIHP Nurses and initial training for new PIHP Nurses Presenters: Linda Fletcher, RN, MS, CPNP Deb Ziegler, HSW
Private Duty Nursing (PDN) Eligibility Determination Workshop A refresher course for current PIHP Nurses and initial training for new PIHP Nurses Presenters: Linda Fletcher, RN, MS, CPNP Deb Ziegler, HSW
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
DMAT Intermediate Triage Lecture Notes Keith Conover, M.D., FACEP 1.0 7/11/14 Objectives: Describe the differences between START triage and ESI
 DMAT Intermediate Triage Lecture Notes Keith Conover, M.D., FACEP 1.0 7/11/14 Objectives: Describe the differences between START triage and ESI triage, both in terms of levels and context in which they
DMAT Intermediate Triage Lecture Notes Keith Conover, M.D., FACEP 1.0 7/11/14 Objectives: Describe the differences between START triage and ESI triage, both in terms of levels and context in which they
Do protocols & guidelines improve care? Prof Dr Marc Sabbe Emergency Department, UZLeuven KULeuven, Belgium
 Do protocols & guidelines improve care? Prof Dr Marc Sabbe Emergency Department, UZLeuven KULeuven, Belgium Content Is there a problem? Definitions When do we need guidelines & protocols? Advantages &
Do protocols & guidelines improve care? Prof Dr Marc Sabbe Emergency Department, UZLeuven KULeuven, Belgium Content Is there a problem? Definitions When do we need guidelines & protocols? Advantages &
Cost-effective critical care: What does it look like?
 Cost-effective critical care: What does it look like? Scott D. Halpern, M.D., Ph.D. Associate Professor of Medicine, Epidemiology, and Medical Ethics & Health Policy Director, Fostering Improvement in
Cost-effective critical care: What does it look like? Scott D. Halpern, M.D., Ph.D. Associate Professor of Medicine, Epidemiology, and Medical Ethics & Health Policy Director, Fostering Improvement in
Policy for Admission to Adult Critical Care Services
 Policy Number: CCaNNI 008 Title: Policy for Admission to Adult Critical Care Services Operational Date: Review Date: December 2009 December 2012 Type of Document: EQIA Screening Date: Corporate x Clinical
Policy Number: CCaNNI 008 Title: Policy for Admission to Adult Critical Care Services Operational Date: Review Date: December 2009 December 2012 Type of Document: EQIA Screening Date: Corporate x Clinical
IN EFFORTS to control costs, many. Pediatric Length of Stay Guidelines and Routine Practice. The Case of Milliman and Robertson ARTICLE
 Pediatric Length of Stay Guidelines and Routine Practice The Case of Milliman and Robertson Jeffrey S. Harman, PhD; Kelly J. Kelleher, MD, MPH ARTICLE Background: Guidelines for inpatient length of stay
Pediatric Length of Stay Guidelines and Routine Practice The Case of Milliman and Robertson Jeffrey S. Harman, PhD; Kelly J. Kelleher, MD, MPH ARTICLE Background: Guidelines for inpatient length of stay
Clinical Operations in a Service Line Model
 These presenters have nothing to disclose. Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line
These presenters have nothing to disclose. Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line
Mercy Virtual. Transforming Medicine and Value Through Virtual Care. Randall S Moore, MD, MBA. Orlando, FL. September, 2017
 Mercy Virtual Transforming Medicine and Value Through Virtual Care Randall S Moore, MD, MBA Orlando, FL September, 2017 The opinions expressed are those of the presenter and do not necessarily state or
Mercy Virtual Transforming Medicine and Value Through Virtual Care Randall S Moore, MD, MBA Orlando, FL September, 2017 The opinions expressed are those of the presenter and do not necessarily state or
Managing Hospital Costs in an Era of Uncertain Reimbursement A Six Sigma Approach
 Managing Hospital Costs in an Era of Uncertain Reimbursement A Six Sigma Approach Prepared by: WO L December 8, 8 Define Problem Statement As healthcare costs continue to outpace inflation and rise over
Managing Hospital Costs in an Era of Uncertain Reimbursement A Six Sigma Approach Prepared by: WO L December 8, 8 Define Problem Statement As healthcare costs continue to outpace inflation and rise over
Overview. Dr Stephen Gulliford & AKI Specialist Nurse Suzanne Wilson Page 1
 Improving Patient Safety and Reducing Harm through the Development of an Acute Kidney Injury Specialist Service at Wrightington, Wigan and Leigh NHS Foundation Trust Overview Acute Kidney Injury (AKI)
Improving Patient Safety and Reducing Harm through the Development of an Acute Kidney Injury Specialist Service at Wrightington, Wigan and Leigh NHS Foundation Trust Overview Acute Kidney Injury (AKI)
Our Sepsis Improvement Journey
 A25 Our Sepsis Improvement Journey Driving Value through Collaboration December 6, 2016 9:30 10:45 am #IHIFORUM Session Objectives P2 To describe how our organization reduced sepsis mortality, saved lives
A25 Our Sepsis Improvement Journey Driving Value through Collaboration December 6, 2016 9:30 10:45 am #IHIFORUM Session Objectives P2 To describe how our organization reduced sepsis mortality, saved lives
RECOMMENDATION FOR CONSIDERATION
 Board Meeting Date: June 15, 2016 RECOMMENDATION FOR CONSIDERATION Subject: Critical Care Transfer of Care Data Elements and Form VTR#: 0616-04 Committee/Task Force: Critical Care Transport Task Force
Board Meeting Date: June 15, 2016 RECOMMENDATION FOR CONSIDERATION Subject: Critical Care Transfer of Care Data Elements and Form VTR#: 0616-04 Committee/Task Force: Critical Care Transport Task Force
Christian Brothers Risk Management Services. Nursing Home & Health Care Ministry Documentation: Are you open for a lawsuit?
 2013 Spring Webinar Series 2013 Christian Brothers Services, Romeoville, IL. All Rights Reserved. No part of this presentation may be reproduced, stored in a retrieval system, or transmitted by any means
2013 Spring Webinar Series 2013 Christian Brothers Services, Romeoville, IL. All Rights Reserved. No part of this presentation may be reproduced, stored in a retrieval system, or transmitted by any means
Can Improvement Cause Harm: Ethical Issues in QI. William Nelson, PhD Greg Ogrinc, MD, MS Daisy Goodman, CNM. DNP, MPH
 Session Code A4, B4 The presenters have nothing to disclose Can Improvement Cause Harm: Ethical Issues in QI William Nelson, PhD Greg Ogrinc, MD, MS Daisy Goodman, CNM. DNP, MPH December 6, 2016 #IHIFORUM
Session Code A4, B4 The presenters have nothing to disclose Can Improvement Cause Harm: Ethical Issues in QI William Nelson, PhD Greg Ogrinc, MD, MS Daisy Goodman, CNM. DNP, MPH December 6, 2016 #IHIFORUM
CGS Administrators, LLC Clinical Hospice Documentation from CGS Missouri Hospice & Palliative Care Assoc. October 3, 2016
 Missouri Hospice & Palliative Care Conference Reviewer s decision is reliant upon documentation Results in a full denial for the submission Documentation must be legible Medical necessity is always based
Missouri Hospice & Palliative Care Conference Reviewer s decision is reliant upon documentation Results in a full denial for the submission Documentation must be legible Medical necessity is always based
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Paediatrics. PEWS & Deteriorating Patients Linda Clerihew
 Paediatrics PEWS & Deteriorating Patients Linda Clerihew SPSP 2007 SPSPP 2010 McQIC 2013 Aim 30% reduction in avoidable harm measured by the Paediatric Serious Harm Key Indicators by December 2015 Measuring
Paediatrics PEWS & Deteriorating Patients Linda Clerihew SPSP 2007 SPSPP 2010 McQIC 2013 Aim 30% reduction in avoidable harm measured by the Paediatric Serious Harm Key Indicators by December 2015 Measuring