BC Pediatric Early Warning System (PEWS) for Emergency and Urgent Care Settings. Regional Workshops 2018
|
|
|
- Maud Crawford
- 5 years ago
- Views:
Transcription

1 BC Pediatric Early Warning System (PEWS) for Emergency and Urgent Care Settings Regional Workshops
2 By the end of this session you will be able to... Understand PEWS and explain reasons for using PEWS in ED Describe each of the components BC PEWS ED Practice using the components of BC PEWS ED through case scenarios Plan for implementation at your site Identify & review supports and resources available to assist in implementing BC PEWS ED 2
3 1 Child Health BC 3





4 Child Health BC Network Ministry of Health Ministry of Child/Family Development Ministry of Education Government Ministries Provincial Health Authorities Fraser Interior Island Northern Van-Coastal PHSA First Nations Professional Societies Academic Partners BC Pediatric Society DOBC: Society of GPs BC Principals, Vice Principals UBC Departments of Pediatrics, Surgery Canadian Child Health Coalition 4
")

5 Examples of CHBC Initiatives Tiers of Service systems planning Provincial Asthma Guidelines Concussion Awareness Training Tool (CATT) Lifetime Prevention Schedule Is Good Good Enough - Child Health Indicators report Hip Surveillance for Children with Cerebral Palsy 5


6 6 Six Tiered System of Service
7 2 Why PEWS for ED in BC? 7
8 Why PEWS? Failure to identify & intervene early with clinical deterioration is a source of substantive unintended harm including death, disability, prolonged stay &/or readmission ~63 to 89% of children do not survive cardiac arrest & morbidity in survivors remains high. Yet children may demonstrate symptom deterioration up to 24 hours prior to cardiopulmonary arrest To maximize early recognition of clinical deterioration, Pediatric Early Warning Systems (PEWS) have been implemented internationally with a substantial and growing body of evidence supporting their use PEWS identifies abnormal physiology quickly and when tracked across time offers early warning of deterioration. Combined with escalation guidelines, PEWS encourages timely mitigation 8


9 Why PEWS? Early Recognition Early Intervention Improved outcomes 9
10 A Case for Change PEWS identified as a high priority by Health Authorities: Concerning critical incidents in both the inpatient & emergency department settings related to failure to identify risk/deterioration Setting a standard for care & communication based on evidence addresses: Complexity in identification of deterioration risk in children (vital signs ranges, compensation) Diversity of knowledge, skills & experience levels of providers across the province Issues of high cognitive load in busy ED with intermittent high patient loads, diverse diagnoses, multiple handovers, intense time pressures 10
11 The Evidence Extensive literature exists for the use of PEWS with inpatients; less but growing evidence for ED: o PEWS scores demonstrated high inter-rater & intra-rater reliability o PEWS can be integrated in routine patient evaluation & performed rapidly in the busy ED setting (less than 90 seconds) o PEWS is a good predictor of ICU admission (medical illness) o PEWS cannot replace the triage tool o There are several reported positive associations with the use of PEWS in the ED including: Assists generalist nurses (low volume pediatrics) to accurately assess children and plan interventions Provides a baseline for monitoring deterioration Ensures patients have a full set of observations taken, recorded and repeated as clinically necessary 11
. Richmond ED relies on general health providers, who see predominately adults, but also care for children.")
12 Richmond Hospital ED Pilot Research To guide provincial planning, a oneyear pilot was conducted at Richmond Hospital to research the use of PEWS in a general emergency department. ED has approximately 6800 paediatric visits annually (12% of total visits). Richmond ED relies on general health providers, who see predominately adults, but also care for children. 12
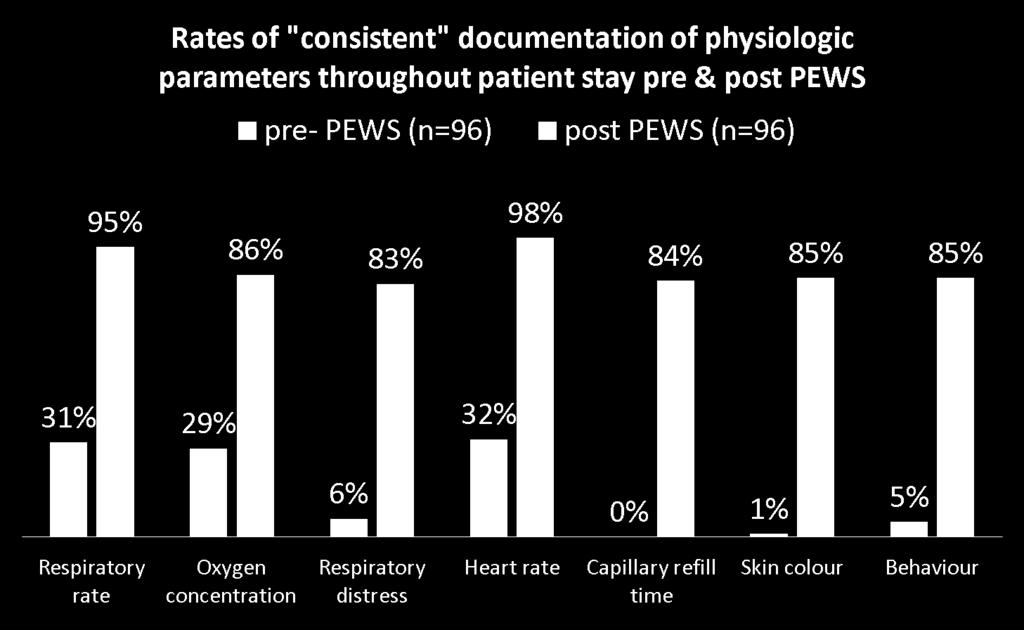
13 Results of PEWS in ED pilot Overall results were very positive and include: Health providers report high levels of change in knowledge & confidence in caring for pediatric patients. Health providers improved communication between team members. At Triage: With the use of PEWS at triage, documentation of physiological parameters increased by 75%. Canadian Triage and Acuity Scale (CTAS) assignment was more accurate because the pediatric assessment was more thorough. 13

14 14 Assessment & Documentation

15 Perceived Value of PEWS System allows a better "snapshot" look of how acutely a child needs intervention and I feel it prompts me to intervene sooner than without a PEWS score - RN 15
16 BC PEWS ED: A provincial approach To develop and implement a standardized provincial approach for the identification of children and youth who present at the ED who may be at risk for deterioration. System will be based on: Best available evidence Results of the Richmond Hospital Emergency Department pilot, and Provincial consensus 16
17 Provincial Consensus Consensus reached on the following: 1.Implement PEWS in ED in a standardized manner across the province 2.Implement at triage & with every full set of vitals 3.Use a standardized escalation aid 4.Use standardized documentation including: Pediatric Emergency Nursing Record (ENAR) PEWS Vital Sign Record 5.There are no exclusion criteria. PEWS will be completed on every pediatric patient presenting in ED (except CTAS 1 or patients requiring immediate treatment) 17

18 18 WHY DO WE NEED EARLIER WARNING OF COMPROMISE?
19 3 Components of BC PEWS ED Child Health BC has been working with Health Authorities to develop a PEWS system that will work across the province for the ED environment 19
20 Components of BC PEWS ED PEWS Score Standardized pediatric emergency nursing record Tools to promote Situational Awareness Escalation Aid Communication Framework (SBAR) 20
21 Validated Scoring Tool: Brighton Score can range between 0 and 13. Higher PEWS scores associated with higher risk of clinical deterioration Behaviour Brighton Pediatric Early Warning Score SCORE Playing Sleeping Irritable Lethargic &/OR Appropriate Confused &/OR Reduced response to pain Respiratory Cardiovascular Within normal parameters No recession or tracheal tug Pink &/OR capillary refill 1-2 seconds 10 above normal parameters, Using accessory muscles, &/OR 30+% FiO2 or 4+ liters/min Pale &/OR capillary refill 3 seconds >20 above normal parameters recessing/retractions, tracheal tug &/OR 40+% FiO2 or 6+liters/min Grey &/OR capillary refill 4 seconds Tachycardia of 20 above normal rate. 5 below normal parameters with sternal recession/retractions, tracheal tug or grunting &/OR 50% FiO2 or 8+liters/min Grey and mottled or capillary refill 5 seconds or above OR Tachycardia of 30 above normal rate or bradycardia Q 20 minutes bronchodilators &/OR persistent vomiting following surgery (2 points each) (Monaghan, 2005) TOTAL PEWS SCORE Monaghan A. Detecting and managing deterioration in children. Paediatr Nurs. 2005; 17:2-5 21

22 PEWS score PEWS Scoring Legend Age- specific vital signs norms based on CTAS
23 PEWS Score The PEWS Vital Sign record (inserts for ENAR or trauma record) are divided into 6 age ranges to accommodate for vital signs differences in pediatric patients: 0-3 months 4-6 years 4-11 months 7-11 years 1-3 years 12+ years 23
 or mode of oxygen delivery device; no score Record level of respiratory distress by using a Calculate and record the Respiratory PEWS Score: Take the HIGHEST")
24 Scoring Respiratory Category AIRWAY BREATHING PEWS Scoring Legend 99 RA Record respiration rate using a and connect with a line Record supplemental O2 % or L/min concentration Record but do not score O2 saturation % Record RA (room air) or mode of oxygen delivery device; no score Record level of respiratory distress by using a Calculate and record the Respiratory PEWS Score: Take the HIGHEST score (max 3) Respiratory Category Parameter Scoring Range Respiratory Rate Oxygen Saturation not scored Supplemental O Respiratory Distress
25 Refer to the CTAS definitions for full description, Key indicators include but are not limited to: Mild: No obvious WOB tachypnea, dyspnea Scoring Respiratory Category Moderate: Increased WOB, restlessness/anxiety, tachypnea, retractions, increased expiratory phase Severe: Excessive WOB, cyanosis, decreased mental status, tachycardia, bradycardia, upper airway obstruction, absent or decreased breath sounds. 25

26 Scoring Cardiovascular Category If a vital sign lands on a line, score up (e.g. score as 2) Record Heart Rate using a and connect with a line CIRCULATION Record Blood Pressure ; recording MAP numerically PEWS Scoring Legend Cardiovascular Category Record Capillary Refill Time using a Record Skin Colour using a Calculate and record the Cardiovascular PEWS Score: Take the HIGHEST score (max 3) Parameter Scoring Range Rate ** Blood Pressure/MAP Not scored Capillary Refill Time Skin Colour Record but do not score Blood Pressure and MAP *There is NO score of 1 for Heart Rate 25

27 26 Scoring HHHF Therapy
28 Scoring Behaviour Category Behaviour Category DISABILITY Indicate the assessed patient behavior using a PEWS Scoring Legend Calculate and record the Behaviour PEWS Score: Take the HIGHEST score (max 3) Behaviour Sleeping refers to any period of sleeping. 27
29 Scoring Other factors and total PEWS OTHER FACTORS PEWS Scoring Legend Enter if applicable; score 2 points each Persistent vomiting following surgery 2 Bronchodilator every 20 minutes 2 Calculate and record the TOTAL Pediatric Early Warning Score: Add the Respiratory + Cardiovascular + Behavior + Other factors Category scores together= Total PEWS (0-13 maximum) 28
30 Situational Awareness in ED Perceive/recognize risk for children in a busy ED Understand meaning/significance Anticipate/ predict future state/events Decision Action Based on Endsley s model of SA 29


31 Situational Awareness Factors Cincinnati Children s found these factors to be 100% sensitive predictors of serious deterioration. Addressing all five on a regular basis helped teams improve predicting & preventing deterioration Caregiver Concern Unusual Therapy Watcher Patient PEWS Score 2+ Communication Breakdown 30

32 Situational Awareness Factors Parent/Family/Caregiver: This factor is not the same as presenting complaint or frustration over wait times. It indicates increasing concern expressed regarding a child s condition, a worsening or changing state. Parents offer valuable insight into their child s normal state, pain and comfort. Watcher Patient: A patient you identify as requiring more frequent observation Most commonly used factor. Can capture risk not captured solely by score e.g. surgical risk, abnormal labs or neurovital signs and mental health concerns. 31
33 Situational Awareness Factors Communication Breakdown: a lack of clarity, break or difficulty in communication e.g. in treatment decisions, reporting of results, patient planning, designation of responsibilities, language barriers. Unusual Therapy: unusual Therapy: unfamiliarity with a medication or protocol in the department or by the health care provider (e.g. new and/or low frequency and high risk medication or process). Applying the unusual therapy bring increased awareness to patient care, support and planning. PEWS score 2 or higher: should trigger increased awareness, notification, assessment and resource review. 32

34 Situational Awareness Why use SA? SA identifies additional risks and influences the escalation of: care support increased monitoring observation Includes and goes beyond elevated PEWS score How to promote SA in ED? Posters throughout ED Document risk Regular reporting/ debriefing 34

35 34 Escalation Aid
36 Standardizing Communication (SBAR) What is SBAR? SBAR (Situation- Background-Assessment- Recommendation) technique provides a framework for communication between members of the health care team about a patient's condition Situation: S Background: B Assessment: A Recommendation: R What is the situation you are calling about? I am (name), a nurse on ward (X) I am calling about (patient X) I am calling because I am concerned that (e.g. BP is low/high, pulse is XX, temperature is XX, PEWS score is X) Pertinent Information & Relevant History Patient (X) was admitted on (XX date) with (e.g. respiratory infection) They have had (X procedure/investigation/operation) Patient (X) s condition has changed in the last (XX mins) Their last set of vital signs were (XXX) What do you think the problem is? I think the problem is (XXX) and I have (e.g. applied oxygen/given analgesia, stopped the infusion) OR I am not sure what the problem is but the patient (X) is deteriorating OR I don t know what s wrong but I am really worried What do you want to happen? I need you to Come to see the child in the next (XX mins) AND Is there anything I need to do in the meantime? (give a normal saline bolus/repeat vitals/start antibiotics) Ask receiver to repeat key information to ensure understanding 36
37 4 Case Study 1 36

38 Case Scenarios Scenarios are simulated. Specific timelines, routines, and practices are not intended to reflect individual sites or real cases but to teach the PEWS system. 38
39 Case 1 Scenario Objective: To review the components of the PEWS system through a scenarios based activity which includes: Practicing documentation of PEWS observations Calculating the PEWS score Identifying Situational Awareness Factors Reviewing SBAR Reviewing Escalation Aid recommendations 38
40 Case 1 Patient: Baby Boy Sidhu Age: 14 days Accompanied by: Mother & Father Presenting Complaint: Nasal congestion, cough, decreased feeding and increasing difficulty with feeding (5 short breast feeds last 24 hours), sleeping long periods, diapers don t appear as wet or heavy as normal Caregiver concern in addition to presenting complaint: No Relevant Past Medical History: SVD, Primip, Discharged at 24 hours, breast feeding, gaining weight 39

41 Case 1 Presents at Triage at: 23:00 Sleeping in mums arms Moderate work of breathing (tachypnea/use of accessory muscles) Pink peripherally and centrally Apply the Pediatric Assessment Triangle: Appearance: Work of Breathing: Circulation: looks well, or unwell? J Emerg Nurs Mar; 39(2):
42 Case 1 Respiratory Category Respiratory rate 65 Oxygen Saturation % 95 Supplemental oxygen delivered Mode of Delivery RA Respiratory Distress Mod PEWS Score for Respiratory Cardiovascular Category Heart Rate 170 Blood Pressure 70/55 MAP 62 Capillary Refill Time 2 Skin Colour Pink PEWS Score for Cardiovascular Behaviour Category Playing/Appropriate Sleeping Irritable Lethargic/Confused Reduced response to pain PEWS Score for Behaviour Other Factors Persistent vomiting following surgery 1. Select the correct aged PEWS VS record 2. PEWS Scoring document the PEWS observations calculate the PEWS score Bronchodilator every 20 minutes Total PEWS Score ( R + C+ B + O) (max 13) 41
43 Case 1 Situational Awareness Factors: Using your clinical judgment from the scenario above and PEWS observations and VS, what Situational Awareness factors would you apply? Enter the time of escalation if applicable and make any additional documentation in nurses notes. 43
44 Additional information Patient weight: 4200 gm Patient temperature: 36.5 Axilla Case 1 **Documentation of the patient s weight and temperature is an important step in pediatric assessment and may happen at triage or at admission Determining level of patient acuity 1.The patients CTAS score is determined. When assigning the CTAS score consider the CTAS guidelines, the PEWS score and Situational Awareness factors 2.Refer to escalation aid used at your site 3.Prepare patient for admission and further assessment The Physician has been paged in response to the nursing assessment findings regarding the patients condition and corresponding PEWS score and CTAS assignment 44
45 Case 1 Admission and Transfer of the Patient to the ED The baby and his parents are now transferred to the emergency stretcher area. The admitting RN report is received and you now complete the primary and secondary assessment including PEWS observations and document in the paper or electronic health record. Additional Information: Time: 23:15 Patient Temperature: 36.8 Celsius Axilla 45
46 Case 1 Respiratory Category Respiratory rate 68 Oxygen Saturation % 93 Supplemental oxygen delivered 1/2 L Mode of Delivery NP Respiratory Distress Mod PEWS Score for Respiratory Cardiovascular Category Heart Rate 178 Blood Pressure 72/58 MAP 60 Capillary Refill Time 3 Skin Colour Pale PEWS Score for Cardiovascular Behaviour Category Playing/Appropriate Sleeping Irritable Lethargic/Confused Reduced response to pain PEWS Score for Behaviour Other Factors Persistent vomiting following surgery PEWS Scoring document the PEWS observations calculate the PEWS score Bronchodilator every 20 minutes Total PEWS Score ( R + C+ B + O) (max 13) 46
47 Case 1 Situational Awareness Factors: Using your clinical judgment from the scenario above and PEWS observations and VS, what Situational awareness factors would you apply? Enter the time of escalation if applicable and make any additional documentation in nurses notes. 47
48 Case 1 Applying clinical knowledge, what information does the VS trending show? Refer to the Escalation Aid used at your site for the recommended actions to consider Where does Baby Sidhu s score fall in the escalation zone? What are the next steps? What tool can help frame your conversation with the physician 48
49 Case 1 Time: 23:30 Seen by: Physician Orders: Routine labs, VS q30 mins, full Cardio-Respiratory monitoring, maintain oxygen saturations above 94%, NGT feeds, gently suction nares PRN Results: Normal electrolytes, elevated WC, elevated CO2 Nursing Actions: RN elevates HOB, uses nasal aspirator and gently suction nares for large amount of secretions. Baby is settled into crib. Family reassured 49
50 Case 1 Respiratory Category Respiratory rate 58 Oxygen Saturation % 96 Supplemental oxygen delivered 1/2 L Mode of Delivery NP Respiratory Distress Mod PEWS Score for Respiratory Cardiovascular Category Heart Rate 160 Blood Pressure MAP Capillary Refill Time 3 Skin Colour Pale PEWS Score for Cardiovascular Behaviour Category Playing/Appropriate Sleeping Irritable Lethargic/Confused Reduced response to pain PEWS Score for Behaviour Other Factors Persistent vomiting following surgery PEWS Scoring document the PEWS observations calculate the PEWS score 50 Bronchodilator every 20 minutes Total PEWS Score ( R + C+ B + O) (max 13)
51 Case 1 Situational Awareness Factors: Using your clinical judgment from the scenario above and PEWS observations and VS, what Situational Awareness factors would you apply? Enter the time of escalation if applicable and make any additional documentation in nurses notes. 51
52 Case 1 Refer to the Escalation Aid used at your site for the recommended actions to consider Where does Baby Sidhu s score fall in the escalation zone? Apply your clinical assessment skills and clinical judgement Refer to the corresponding score in the escalation aid for considerations and recommendations in managing the patients care. 52
53 Case 1 Learning points from Case I Neonates are at increased risk of deterioration due to age and can deteriorate rapidly Visual trending of HR and RR aids in recognizing deterioration along with colour and any response to treatment Capillary refill time is a good indicator of perfusion and cardiac output Consider the ED environment: extra stimulation and handling can cause an increase in some vital signs 53
54 4 Case Study 2 53
55 Case 2 Scenario Objective: To review the components of the PEWS system through a scenarios based activity which includes: Practicing documentation of PEWS observations Calculating the PEWS score Identifying Situational Awareness factors Reviewing SBAR Reviewing Escalation Aid recommendations 55
56 Case 2 Patient: Jamal Age: 9 years old Accompanied by: Mother Presenting Complaint: Abdominal pain, vomiting, fever, lethargy, feeling unwell, his lips are dry, pale, breathing slightly fast Caregiver concern in addition to presenting complaint: Yes Relevant Past Medical History: Jamal had a ruptured appendix 10 days ago and was discharged from hospital 48 hours ago. He has been vomiting the past 8 hours with increasing frequency 2-3 times an hour now mostly bilious. He is unable to keep any amounts of fluids down. Mum is very concerned as Jamal is looking much worse in the past two hours. 56
57 Case 2 Presents at Triage at: 13:00 Lethargic, responds to questions breathing shallow and fast pale with sunken eyes Apply the Pediatric Assessment Triangle: Appearance: Work of Breathing: Circulation: looks well, or unwell? J Emerg Nurs Mar; 39(2):
58 Case 2 Respiratory Category Respiratory rate 36 Oxygen Saturation % 96 Supplemental oxygen delivered Mode of Delivery RA Respiratory Distress mild PEWS Score for Respiratory Cardiovascular Category Heart Rate 140 Blood Pressure 105/68 MAP 72 Capillary Refill Time 3 Skin Colour Pale PEWS Score for Cardiovascular Behaviour Category Playing/Appropriate Sleeping Irritable Lethargic/Confused Reduced response to pain PEWS Score for Behaviour Other Factors Persistent vomiting following surgery 1. Select the correct aged PEWS record 2. PEWS Scoring document the PEWS observations calculate the PEWS score Bronchodilator every 20 minutes Total PEWS Score ( R + C+ B + O) (max 13) 58
59 Situational Awareness Factors: Using your clinical judgment from the scenario above and PEWS observations and VS, what Situational awareness factors would you apply? Case 2 Enter the time of escalation if applicable and make any additional documentation in nurses notes. 59
60 Case 2 Additional information Patient weight: 26 kg Patient temperature: 38 Oral **Documentation of the patient s weight and temperature is an important step in pediatric assessment and may happen at Triage or at admission Determining level of patient acuity 1. The patients CTAS score is determined. When assigning the CTAS score consider the CTAS guidelines, the PEWS score and situational awareness factors 2. Refer to escalation aid used at your site 3. Prepare patient for admission and further assessment 60
61 Case 2 Admission and Transfer of the Patient to the ED Jamal and his parents are now transferred to the emergency stretcher area. The physician is present and assessing the patient as you complete the primary assessment (secondary as able) including PEWS observations and document accordingly in the paper or electronic health record. Additional Information: Time: 13:15 Patient Temperature: 38 Celsius Oral 61

62 Case 2 PEWS Scoring document the PEWS observations calculate the PEWS score 62
63 Case 2 Situational Awareness Factors: Using your clinical judgment from the scenario above and PEWS observations and VS, what Situational Awareness factors would you apply? Enter the time of escalation if applicable and make any additional documentation in nurses notes. 63
64 Case 2 What factors could influence the PEWS score? Looking at the overall assessment as well as the PEWS score, what are some of the other indications of de-compensation which are evident? Refer to the escalation aid used at your site for the recommended actions to consider Where does Jamal s PEWS score fall in the escalation aid zone? Apply your clinical assessment skills and clinical judgement Refer to the corresponding score in the escalation aid for considerations and recommendations in managing the patients care 64
65 Case 2 Scenario details: review the following scenario information and refer back to it for planning of care Time: 1330 Orders: Normal saline bolus, IV fluids, appropriate labs (chemistry, complete blood count microbiology), VS and PEWS observations q15 mins, Medications: Tylenol, antiemetic appropriate doses for age Consult: Surgical, Jamal continues to vomit Nursing Actions: IV started, IV bolus and maintenance fluids commenced, nursing documentation as per HA and professional standards Time: 13:45 Patient Temperature: 37.8 Celsius Oral 65

66 Case 2 PEWS Scoring document the PEWS observations calculate the PEWS score 66
67 Case 2 Situational Awareness Factors: Using your clinical judgment from the scenario above and PEWS observations and VS, what Situational Awareness factors would you apply? Enter the time of escalation if applicable and make any additional documentation in nurses notes. 67
68 Case 2 Refer to the escalation aid used at your site for the recommended actions to consider Where does Jamal s PEWS score fall in the escalation aid zone? What tool can by used to frame your conversation with the Physician? What are the next steps? 68
69 Case 2 Learning points from scenario 1. Persistent vomiting following surgery refers to: vomiting more than usual following surgery assess the child frequently for signs of dehydration (tachypnea, tachycardia, perfusion-cap refill time, narrow pulse pressure, low urine output), changes in mental status 2. Screening for Sepsis: A child with a critically high heart rate should be screened for sepsis 3. A PEWS score may not always reflect continuing deterioration if the maximum score within the category has already been reached. Always review the vital sign norms individually and trending patterns in the clinical assessment 69
70 4 Case Study 3 69
71 Case 3 Scenario Objective: To review the components of the PEWS system through a scenarios based activity which includes: Practicing documentation of PEWS observations Calculating the PEWS score Identifying Situational Awareness Factors Reviewing SBAR Reviewing Escalation Aid recommendations 71
72 Case 3 Patient: Yuko Age: 12 years old Accompanied By: Home stay parent Presenting Complaint: Neck pain for last 8-12 hours, lethargy-has been lying on the couch holding her head and neck supported on a pillow, no appetite all day. Caregiver Concern in addition to presenting complaint: Yuko has recently come from Japan as a home stay student. English is a second language and communication is very limited. Relevant Past Medical History: Unknown, home stay mum is contacting the school and family in Japan 72
73 Case 3 Presents at Triage at: 2000 Quietly leaning on the desk holding her chin in her hands, appears withdrawn and anxious Pink centrally but pale No work of breathing Apply the Pediatric Assessment Triangle: Appearance: Work of Breathing: Circulation: looks well, or unwell? J Emerg Nurs Mar; 39(2):
74 Case 3 Respiratory Category Respiratory rate 16 Oxygen Saturation % 97 Supplemental oxygen delivered Mode of Delivery RA Respiratory Distress None PEWS Score for Respiratory Cardiovascular Category Heart Rate 100 Blood Pressure 102/70 MAP 76 Capillary Refill Time 3 Skin Colour Pale PEWS Score for Cardiovascular Behaviour Category Playing/Appropriate Sleeping Irritable Lethargic/Confused Reduced response to pain PEWS Score for Behaviour Other Factors Persistent vomiting following surgery Bronchodilator every 20 minutes Total PEWS Score ( R + C+ B + O) 1. Select the correct aged PEWS record 2. PEWS Scoring document the PEWS observations calculate the PEWS score 74
75 Situational Awareness Factors: Using your clinical judgment from the scenario above and PEWS observations and VS, what Situational Awareness factors would you apply? Case 3 Enter the time of escalation if applicable and make any additional documentation in nurses notes. 75
76 Case 3 Additional information Patient weight: 45 kg Patient temperature: 38 Oral **Documentation of the patient s weight and temperature is an important step in pediatric assessment and may happen at Triage or at admission Determining level of patient acuity 1. The patients CTAS score is determined. When assigning the CTAS score consider the CTAS guidelines, the PEWS score and situational awareness factors 2. Refer to escalation aid used at your site 3. Prepare patient for admission and further assessment 76
77 Case 3 Admission and Transfer of the Patient to the ED Yuko is now transferred to the ambulatory area. It is a very busy evening in the ED As the admitting RN report is received and you now complete the primary and secondary assessment including PEWS observations and document accordingly in the paper or electronic health record. Additional Information: Time: 20:30 Patient Temperature: 38.2 Celsius Oral 77
78 Case 3 Respiratory Category Respiratory rate 28 Oxygen Saturation % 95 Supplemental oxygen delivered Mode of Delivery RA Respiratory Distress mild PEWS Score for Respiratory Cardiovascular Category Heart Rate 120 Blood Pressure 97/70 MAP 78 Capillary Refill Time 3 Skin Colour pale PEWS Score for Cardiovascular Behaviour Category Playing/Appropriate Sleeping Irritable Lethargic/Confused Reduced response to pain PEWS Score for Behaviour Other Factors Persistent vomiting following surgery PEWS Scoring document the PEWS observations calculate the PEWS score 78 Bronchodilator every 20 minutes Total PEWS Score ( R + C+ B + O) (max 13)
79 Situational Awareness Factors: Case 3 Using your clinical judgment from the scenario above and PEWS observations and VS, what Situational Awareness factors would you apply? Enter the time of escalation if applicable and make any additional documentation in nurses notes. 79
80 Case 3 Are there other factors to consider that may contribute to Yuko s increased PEWS score in the ED environment? Refer to the escalation aid used at your site for the recommended actions to consider Where does Yuko s PEWS score fall in the escalation aid zone? What are the next steps? 80
81 Case 3 Time: 2100 Seen by: Emergency Room Physician Orders received: Tylenol for neck pain, IV fluids, Neck Xray, CBC, VS q1 hour Nursing Actions: Tylenol administered (appropriate 2130), Labs drawn; IV commenced at maintenance, Patient sent to
82 Case 3 Additional scenario information: Radiology calls for RN to collect Yuko from the Radiology Department. Yuko has vomited during procedure and is complaining of a severe headache and appears confused. You return with to the ED with her and repeat her PEWS observations. Her home stay mother is very concerned with this rapid deterioration since arrival. Time: 2200 Patient Temperature: 39 C Tympanic 82
83 Case 3 Respiratory Category Respiratory rate 12 Oxygen Saturation % 86 Supplemental oxygen delivered 8 Mode of Delivery M Respiratory Distress severe PEWS Score for Respiratory Cardiovascular Category Heart Rate 70 Blood Pressure 97/70 MAP 78 Capillary Refill Time 5 Skin Colour mottled PEWS Score for Cardiovascular Behaviour Category Playing/Appropriate Sleeping Irritable Lethargic/Confused Reduced response to pain PEWS Score for Behaviour Other Factors Persistent vomiting following surgery PEWS Scoring document the PEWS observations calculate the PEWS score 83 Bronchodilator every 20 minutes Total PEWS Score ( R + C+ B + O) (max 13)

84 Situational Awareness Factors: Case 3 Using your clinical judgment from the scenario above and PEWS observations and VS, what Situational Awareness factors would you apply? Enter the time of escalation if applicable and make any additional documentation in nurses notes. 84
85 Case 3 Refer to the escalation aid used at your site for the recommended actions to consider Where does Yuko s PEWS score fall in the escalation aid zone? What are the next steps? Referring to the Vital Signs information, what other tools should a RN consider using? 85
86 Case 3 Learning points from scenario A full clinical assessment must accompany a PEWS score Consider the vital signs and clinical impression that contribute to the PEWS score and not just the score alone Tracking and trending by visually joining HR and RR by a line helps to visually identify changes over time If a value lands on the line apply the higher score Normal capillary refill time is less than 2 seconds; a drop in BP is a late and ominous sign 86
87 Key points about PEWS It is a complete system-not just a score Apply first at triage & then with all subsequent assessments (frequency will vary with patient condition, orders and site protocols) Use for all patients regardless of acuity/ CTAS (do not delay treatment to do a score if treatment is required) It is a support for clinical decision making PEWS is not a substitute for clinical judgement. If a PEWS score or escalation action does not make sense in context, document clinical reasoning & repeat 86
88 5 Site Implementation Planning 87
89 Implementation planning Using the worksheet provided work with your team to identify: Where will forms and resources be housed? What will be your daily management plan? How will you ensure nurses are using the scoring and ENAR correctly? How will you encourage your healthcare team to engage patient s and families? Where will you hang the situational awareness posters? Where will you put your supporting resources (Braden Q, falls, pain etc.) e.g. ring with the clipboard? resource binders? 89
90 Trainer s Next Steps Track staff completion of online modules Book your in-person site training sessions to ensure you capture all staff who will be using the system Continue to finalize the implementation plan for your agency Access and review all PEWS resources 90
91 Additional Trainer Resources Education Support Tools Available on the child health BC website: Situational Awareness Poster 2 page Overview of PEWS Frequently Asked Questions SBAR tool PEWS Lanyard Card Pediatric Vital Sign Lanyard Card PEWS Nursing PowerPoint Provincial PEWS Education Lesson Plan PEWS Education Session Evaluation Physician Orientation Video Leadership PowerPoint Case Studies Quality Improvement Tools Edu-quicks 91
92 6 Who to contact? 91
SITE APPLICABILITY This practice applies to all pediatric patient care areas that have been designated by your health authority.
 GUIDELINE PURPOSE To provide guidance and direction for the use of the Pediatric Early Warning System (PEWS). The PEWS system supports the recognition, mitigation, notification, and response to the pediatric
GUIDELINE PURPOSE To provide guidance and direction for the use of the Pediatric Early Warning System (PEWS). The PEWS system supports the recognition, mitigation, notification, and response to the pediatric
Provincial Pediatric Early Warning System (PEWS) Clinical Decision Support Tool. Guideline Purpose. Practice Level / Competencies.
 Clinical Decision Support Tool. Guideline Purpose. Practice Level / Competencies.") Guideline Purpose To provide guidance and direction for the use of the British Columbia Pediatric Early Warning System (BC PEWS). The PEWS system supports the early recognition, mitigation, notification,
Guideline Purpose To provide guidance and direction for the use of the British Columbia Pediatric Early Warning System (BC PEWS). The PEWS system supports the early recognition, mitigation, notification,
Provincial Pediatric Early Warning System (PEWS) Clinical Decision Support Tool. Guideline Purpose. Practice Level / Competencies.
 Clinical Decision Support Tool. Guideline Purpose. Practice Level / Competencies.") Guideline Purpose To provide guidance and direction for the use of the British Columbia Pediatric Early Warning System (BC PEWS). The PEWS system supports the early recognition, mitigation, notification,
Guideline Purpose To provide guidance and direction for the use of the British Columbia Pediatric Early Warning System (BC PEWS). The PEWS system supports the early recognition, mitigation, notification,
Paediatrics. PEWS & Deteriorating Patients Linda Clerihew
 Paediatrics PEWS & Deteriorating Patients Linda Clerihew SPSP 2007 SPSPP 2010 McQIC 2013 Aim 30% reduction in avoidable harm measured by the Paediatric Serious Harm Key Indicators by December 2015 Measuring
Paediatrics PEWS & Deteriorating Patients Linda Clerihew SPSP 2007 SPSPP 2010 McQIC 2013 Aim 30% reduction in avoidable harm measured by the Paediatric Serious Harm Key Indicators by December 2015 Measuring
Irish Paediatric Early Warning System (PEWS)
") Irish Paediatric Early Warning System (PEWS) Learning Outcomes By the end of the session, you will be able to: Discuss the importance of clinical judgement and individualised assessment Discuss the use
Irish Paediatric Early Warning System (PEWS) Learning Outcomes By the end of the session, you will be able to: Discuss the importance of clinical judgement and individualised assessment Discuss the use
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool
 Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
The ROHNHSFT Experience: Implementing BWCH PEWS
 The ROHNHSFT Experience: Implementing BWCH PEWS Alison Warren Clinical Matron for Children and Young Peoples Services The Royal Orthopaedic Hospital NHS Foundation Trust RGN, RSCN, ENB 415 & 998 PG Cert
The ROHNHSFT Experience: Implementing BWCH PEWS Alison Warren Clinical Matron for Children and Young Peoples Services The Royal Orthopaedic Hospital NHS Foundation Trust RGN, RSCN, ENB 415 & 998 PG Cert
NHS LOTHIAN Standard Operating Procedure: EHSCP Physiological Observations of Patients in the Community Setting
 NHS LOTHIAN Standard Operating Procedure: EHSCP Physiological Observations of Patients in the Community Setting 1. Introduction To standardise the type and frequency of observations to be taken on adult
NHS LOTHIAN Standard Operating Procedure: EHSCP Physiological Observations of Patients in the Community Setting 1. Introduction To standardise the type and frequency of observations to be taken on adult
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
Los Angeles Medical Center Policies and Procedures
 Section: OPERATIONS Title: GUIDELINES FOR RAPID RESPONSE TO CHANGES IN A PATIENT S CONDITION Approved by: POLICY & PROCEDURE COMMITTEE 10/09 MEDICAL EXECUTIVE COMMITTEE 10/09 REFERENCES: Institute for
Section: OPERATIONS Title: GUIDELINES FOR RAPID RESPONSE TO CHANGES IN A PATIENT S CONDITION Approved by: POLICY & PROCEDURE COMMITTEE 10/09 MEDICAL EXECUTIVE COMMITTEE 10/09 REFERENCES: Institute for
These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in
 These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in the UK and beyond. 1 The first EWS was devised in 1997
These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in the UK and beyond. 1 The first EWS was devised in 1997
Early Warning Score Procedure
 Procedure Contents Purpose... 2 Scope/Audience... 2 Associated documents... 3 Definitions... 4 Adult patients... 4 Maternity patients... 4 Paediatric patients... 4 Equipment... 5 Education and training
Procedure Contents Purpose... 2 Scope/Audience... 2 Associated documents... 3 Definitions... 4 Adult patients... 4 Maternity patients... 4 Paediatric patients... 4 Equipment... 5 Education and training
Subacute Care. 1. Define important words in the chapter. 2. Discuss the types of residents who are in a subacute setting
 175 26 Subacute Care 1. Define important words in this chapter 2. Discuss the types of residents who are in a subacute setting 3. List care guidelines for pulse oximetry 4. Describe telemetry and list
175 26 Subacute Care 1. Define important words in this chapter 2. Discuss the types of residents who are in a subacute setting 3. List care guidelines for pulse oximetry 4. Describe telemetry and list
Policies and Procedures. I.D. Number: 1145
 Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
Title Protocol for the Management of Chest Wall Injuries (over 12 years of age) in MIU s and WIC s.
 in MIU s and WIC s.") Document Control Title Protocol for the Management of Chest Wall Injuries (over 12 years of age) in MIU s and WIC s. Author Author s job title Professional Lead, Minor Injuries Unit Directorate Department
Document Control Title Protocol for the Management of Chest Wall Injuries (over 12 years of age) in MIU s and WIC s. Author Author s job title Professional Lead, Minor Injuries Unit Directorate Department
DETERIORATING PATIENT POLICY GENERAL POLICY NO. 50
 DETERIORATING PATIENT POLICY GENERAL POLICY NO. 50 Applies to: Committee for Approval Date of Approval September 2012 Date Ratified: September 2012 Review Date: September 2015 Name of Lead Manager Version:
DETERIORATING PATIENT POLICY GENERAL POLICY NO. 50 Applies to: Committee for Approval Date of Approval September 2012 Date Ratified: September 2012 Review Date: September 2015 Name of Lead Manager Version:
Wessex Regional All Cause Deterioration (including Sepsis) Guidance
 Guidance") Wessex Regional All Cause Deterioration (including Sepsis) Guidance For Adult ( 16 non-pregnant) patients WACDG v1 11 th May 2018 Guidance includes models for the following healthcare settings Hospital
Wessex Regional All Cause Deterioration (including Sepsis) Guidance For Adult ( 16 non-pregnant) patients WACDG v1 11 th May 2018 Guidance includes models for the following healthcare settings Hospital
Assessment and Reassessment of Patients
 Approved by: Assessment and Reassessment of Patients Senior Director, Operations, Emergency, Medicine, Critical Care & Respiratory - GNCH Senior Director, Operations, Emergency, Medicine, Critical Care
Approved by: Assessment and Reassessment of Patients Senior Director, Operations, Emergency, Medicine, Critical Care & Respiratory - GNCH Senior Director, Operations, Emergency, Medicine, Critical Care
Sepsis guidance implementation advice for adults
 Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE OBSTETRICAL TRIAGE ACUITY SCALE (OTAS) SCOPE Provincial: Women s and Infant s Health APPROVAL AUTHORITY Vice-President, Research, Innovation & Analytics SPONSOR Maternal Newborn Child & Youth, Strategic
TITLE OBSTETRICAL TRIAGE ACUITY SCALE (OTAS) SCOPE Provincial: Women s and Infant s Health APPROVAL AUTHORITY Vice-President, Research, Innovation & Analytics SPONSOR Maternal Newborn Child & Youth, Strategic
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
General Practice Triage: An update for Reception & Clinical Staff
 General Practice Triage: An update for Reception & Clinical Staff October 2017 Magali De Castro Clinical Director, HotDoc This update will cover Essential components of a robust triage system Accreditation
General Practice Triage: An update for Reception & Clinical Staff October 2017 Magali De Castro Clinical Director, HotDoc This update will cover Essential components of a robust triage system Accreditation
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Shock - Hypovolaemia
 Shock - Hypovolaemia Research Staff: Participants should be asked to arrive dressed as they would for clinical placement. That is, in uniform, hair and jewellery appropriate, note pad, pen, watch, stethoscope,
Shock - Hypovolaemia Research Staff: Participants should be asked to arrive dressed as they would for clinical placement. That is, in uniform, hair and jewellery appropriate, note pad, pen, watch, stethoscope,
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart
 Observation Chart") CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY
 POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
Antimicrobial Stewardship in Continuing Care. Nursing Home Acquired Pneumonia Clinical Checklist
 Antimicrobial Stewardship in Continuing Care Nursing Home Acquired Pneumonia Clinical Checklist March 2015 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis
Antimicrobial Stewardship in Continuing Care Nursing Home Acquired Pneumonia Clinical Checklist March 2015 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Chan Man Yi, NC (Neonatal Care) Dept. of Paed. & A.M., PMH 16 May 2017
 Dept. of Paed. & A.M., PMH 16 May 2017") The implementation of an integrated observation chart with Newborn Early Warning Signs (NEWS) to facilitate observation of infants at risk of clinical deterioration Chan Man Yi, NC (Neonatal Care) Dept.
The implementation of an integrated observation chart with Newborn Early Warning Signs (NEWS) to facilitate observation of infants at risk of clinical deterioration Chan Man Yi, NC (Neonatal Care) Dept.
National Quality Improvement Project 2018/2019 Vital Signs in Adult Information Pack
 National Quality Improvement Project 2018/2019 Vital Signs in Adult Information Pack Introduction... 3 Methodology... 4 Inclusion criteria... 4 Exclusion criteria... 4 Flow of data searches to identify
National Quality Improvement Project 2018/2019 Vital Signs in Adult Information Pack Introduction... 3 Methodology... 4 Inclusion criteria... 4 Exclusion criteria... 4 Flow of data searches to identify
Document #: WR
 Rapid Response Team (RRT) Policy Northwest Network Effective Date: 2/8/2018 Version #: 2 Document #: WR.387.149 Patient Care Next Review: 2/8/2021 Page #: 1 of 7 SCOPE: All PeaceHealth St. Joseph Center
Rapid Response Team (RRT) Policy Northwest Network Effective Date: 2/8/2018 Version #: 2 Document #: WR.387.149 Patient Care Next Review: 2/8/2021 Page #: 1 of 7 SCOPE: All PeaceHealth St. Joseph Center
Monday, August 15, :00 p.m. Eastern
 Monday, August 15, 2016 2:00 p.m. Eastern Dial In: 888.863.0985 Conference ID: 34874161 Slide 1 Speakers Deb Kilday, MSN, RN Senior Performance Partner Performance Services Quality & Safety Premier, Inc.
Monday, August 15, 2016 2:00 p.m. Eastern Dial In: 888.863.0985 Conference ID: 34874161 Slide 1 Speakers Deb Kilday, MSN, RN Senior Performance Partner Performance Services Quality & Safety Premier, Inc.
Simulation Design Template
 Simulation Design Template Date: May 7/8, 2008 File Name: Discipline: RN, Charge nurse, medical radiology, pharmacy tech, social work, medicine (whatever is available at the institution) Student Level:
Simulation Design Template Date: May 7/8, 2008 File Name: Discipline: RN, Charge nurse, medical radiology, pharmacy tech, social work, medicine (whatever is available at the institution) Student Level:
PROCEDURAL SEDATION AND ANALGESIA: HOSPITAL-WIDE POLICY
 CLINICAL PRACTICE POLICY PAGE: 1 OF 6 PURPOSE: These policies will allow clinicians to provide their patients with the benefits of procedural sedation and analgesia while minimizing the associated risks.
CLINICAL PRACTICE POLICY PAGE: 1 OF 6 PURPOSE: These policies will allow clinicians to provide their patients with the benefits of procedural sedation and analgesia while minimizing the associated risks.
DRAFT. WORKING DRAFT Nursing associate skills annexe. Part of the draft standards of proficiency for nursing associates. Page 1
 WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
N: Emergency Nursing. Alberta Licensed Practical Nurses Competency Profile 135
 N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
Policies and Procedures. ID Number: 1138
 Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Keep watch and intervene early
 IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
This matter was initiated by a letter from the complainant received on March 20, A response from Dr. Justin Clark was received on May 11, 2017.
 COLLEGE OF PHYSICIANS AND SURGEONS OF NOVA SCOTIA SUMMARY OF DECISION OF INVESTIGATION COMMITTEE C Dr. Justin Clark License Number: 016409 Investigations Committee C of the College of Physicians and Surgeons
COLLEGE OF PHYSICIANS AND SURGEONS OF NOVA SCOTIA SUMMARY OF DECISION OF INVESTIGATION COMMITTEE C Dr. Justin Clark License Number: 016409 Investigations Committee C of the College of Physicians and Surgeons
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE RESTRAINT AS A LAST RESORT - CRITICAL CARE SCOPE Provincial: Critical Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating Officer, Glenrose Rehabilitation Hospital
TITLE RESTRAINT AS A LAST RESORT - CRITICAL CARE SCOPE Provincial: Critical Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating Officer, Glenrose Rehabilitation Hospital
Activation of the Rapid Response Team
 Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
SBAR Communication Tool. Anne Marie Oglesby RGN., MSc. Health Care (Risk Management & Quality) Clinical Risk Advisor, Clinical Indemnity Scheme
 Clinical Risk Advisor, Clinical Indemnity Scheme") SBAR Communication Tool Anne Marie Oglesby RGN., MSc. Health Care (Risk Management & Quality) Clinical Risk Advisor, Clinical Indemnity Scheme Background Communication Tools What is SBAR SBAR in action
SBAR Communication Tool Anne Marie Oglesby RGN., MSc. Health Care (Risk Management & Quality) Clinical Risk Advisor, Clinical Indemnity Scheme Background Communication Tools What is SBAR SBAR in action
Merced College Registered Nursing 34: Advanced Medical/Surgical Nursing and Pediatric Nursing
 Merced College Registered Nursing 34: Advanced Medical/Surgical Nursing and Pediatric Nursing Course Description, Student Learning Outcomes and Competencies, Clinical Evaluation Tool, and Clinical Activities
Merced College Registered Nursing 34: Advanced Medical/Surgical Nursing and Pediatric Nursing Course Description, Student Learning Outcomes and Competencies, Clinical Evaluation Tool, and Clinical Activities
NURSING DIAGNOSIS: Risk for fluid volume deficit related to frequent urination.
 NURSING CARE PLAN NURSING DIAGNOSIS: Risk for fluid volume deficit related to frequent urination. Goal: Provision of fluid balance. Demonstrate adequate hydration as evidenced by stable vital signs, palpable
NURSING CARE PLAN NURSING DIAGNOSIS: Risk for fluid volume deficit related to frequent urination. Goal: Provision of fluid balance. Demonstrate adequate hydration as evidenced by stable vital signs, palpable
FALLS RISK REDUCTION & MANAGEMENT OF INPATIENT FALLS - STANDARDS
 STANDARDS TO BE MET 1. Safe Mobilisation and Falls Prevention Assessment 1.1 The multidisciplinary team will: a) Conduct the Safe Mobilisation and Fall Prevention Assessment; b) Initiate appropriate interventions
STANDARDS TO BE MET 1. Safe Mobilisation and Falls Prevention Assessment 1.1 The multidisciplinary team will: a) Conduct the Safe Mobilisation and Fall Prevention Assessment; b) Initiate appropriate interventions
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
End Of Life Decision Making - Who s Decision Is It Anyway?
 End Of Life Decision Making - Who s Decision Is It Anyway? Kara Livy RN MN NP Critical Care Nurse Practitioner Royal Alexandra Hospital Edmonton, Alberta Kara.livy@albertahealthservices.ca End-Of-Life
End Of Life Decision Making - Who s Decision Is It Anyway? Kara Livy RN MN NP Critical Care Nurse Practitioner Royal Alexandra Hospital Edmonton, Alberta Kara.livy@albertahealthservices.ca End-Of-Life
National Early Warning Score (ViEWS) System. Recommendations for Audit. February 2012
 System. Recommendations for Audit. February 2012") National Early Warning Score (ViEWS) System Recommendations for Audit February 2012 Version 3 Acknowledgement: The National Early Warning Score and associated Education Programme Audit and Evaluation sub-group
National Early Warning Score (ViEWS) System Recommendations for Audit February 2012 Version 3 Acknowledgement: The National Early Warning Score and associated Education Programme Audit and Evaluation sub-group
Disclosure of Proprietary Interest. HomeTown Health HCCS
 HomeTown Health HCCS Hospital Consortium Project: Track 2 Clinical Documentation Program: E ssentials and Took Kits Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
HomeTown Health HCCS Hospital Consortium Project: Track 2 Clinical Documentation Program: E ssentials and Took Kits Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
ESSENTIAL NEWBORN CARE: INTRODUCTION
 ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
Brief Summary. Educational Rationale. Learning Objectives: Nurse. Learning Objectives: Doctor
 Simulation Scenario Title Bacterial meningitis Version 10 Target Audience FY doctors & student nurses Run time 10-15 mins Authors Niamh Feely, Andrew Smith, Udesh Naidoo, Paul Wilder, Mark Loughrey Last
Simulation Scenario Title Bacterial meningitis Version 10 Target Audience FY doctors & student nurses Run time 10-15 mins Authors Niamh Feely, Andrew Smith, Udesh Naidoo, Paul Wilder, Mark Loughrey Last
Policy Review Sheet. Review Date: 14/10/16 Policy Last Amended: 19/10/17. Next planned review in 12 months, or sooner as required.
 Category: Care Management Sub-category: Care Practice Page: 1 of 10 Policy Review Sheet Review Date: 14/10/16 Policy Last Amended: 19/10/17 Next planned review in 12 months, or sooner as required. Note:
Category: Care Management Sub-category: Care Practice Page: 1 of 10 Policy Review Sheet Review Date: 14/10/16 Policy Last Amended: 19/10/17 Next planned review in 12 months, or sooner as required. Note:
Thursday, July 17, :30 a.m. Eastern
 Thursday, July 17, 2014 11:30 a.m. Eastern Dial-In: 1.888.863.0985 Conference ID: 62918492 Slide 1 Robyn D Oria MA, RNC, APC, is the Executive Director at the Central Jersey Family Health Consortium in
Thursday, July 17, 2014 11:30 a.m. Eastern Dial-In: 1.888.863.0985 Conference ID: 62918492 Slide 1 Robyn D Oria MA, RNC, APC, is the Executive Director at the Central Jersey Family Health Consortium in
Procedure REFERENCES. Protecting 5 Million Lives from Harm Campaign, Institute for Health Care Improvement (IHI), 2007.
, 2007.") Title: Nursing Chain of Command for Deterioration of Patient Condition and/or Medical Follow-up DESCRIPTION/OVERVIEW This procedure provides patient care staff guidance for ensuring effective communication
Title: Nursing Chain of Command for Deterioration of Patient Condition and/or Medical Follow-up DESCRIPTION/OVERVIEW This procedure provides patient care staff guidance for ensuring effective communication
Predictive Analytics and the Impact on Nursing Care Delivery
 Predictive Analytics and the Impact on Nursing Care Delivery Session 2, March 5, 2018 Whende M. Carroll, MSN, RN-BC - Director of Nursing Informatics, KenSci, Inc. Nancee Hofmeister, MSN, RN, NE-BC Senior
Predictive Analytics and the Impact on Nursing Care Delivery Session 2, March 5, 2018 Whende M. Carroll, MSN, RN-BC - Director of Nursing Informatics, KenSci, Inc. Nancee Hofmeister, MSN, RN, NE-BC Senior
Clinical Skills Passport for Relief and Temporary Staff in Neonatal Units
 Clinical Skills Passport for Relief and Temporary Staff in Neonatal Units This work is drawn from the Scottish Neonatal Nurses Group document The Competency Framework and Core Clinical Skills for Neonatal
Clinical Skills Passport for Relief and Temporary Staff in Neonatal Units This work is drawn from the Scottish Neonatal Nurses Group document The Competency Framework and Core Clinical Skills for Neonatal
Acutely ill patients in hospital
 Issue date: July 2007 Acutely ill patients in hospital Recognition of and response to acute illness in adults in hospital Developed by the Centre for Clinical Practice at NICE Contents Key priorities for
Issue date: July 2007 Acutely ill patients in hospital Recognition of and response to acute illness in adults in hospital Developed by the Centre for Clinical Practice at NICE Contents Key priorities for
A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs.
 6. Referral process Key findings A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs. Consultant physicians had no knowledge or input into
6. Referral process Key findings A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs. Consultant physicians had no knowledge or input into
RECOMMENDATION FOR CONSIDERATION
 Board Meeting Date: June 15, 2016 RECOMMENDATION FOR CONSIDERATION Subject: Critical Care Transfer of Care Data Elements and Form VTR#: 0616-04 Committee/Task Force: Critical Care Transport Task Force
Board Meeting Date: June 15, 2016 RECOMMENDATION FOR CONSIDERATION Subject: Critical Care Transfer of Care Data Elements and Form VTR#: 0616-04 Committee/Task Force: Critical Care Transport Task Force
Modified Blalock Taussig Shunt
 Patient Information Service Bristol Royal Hospital for Children Modified Blalock Taussig Shunt - Information for parents and staff Respecting everyone Embracing change Recognising success Working together
Patient Information Service Bristol Royal Hospital for Children Modified Blalock Taussig Shunt - Information for parents and staff Respecting everyone Embracing change Recognising success Working together
PATIENT RIGHTS, PRIVACY, AND PROTECTION
 REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
ADMISSION CARE PLAN. Orient PRN to person, place, & time
 ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
Recognizing and Reporting Acute Change of Condition
 Recognizing and Reporting Acute Change of Condition Welcome to the Elizabeth McGowan Training Institute Cell Phones and Pagers Please turn your cell phones off or turn the ringer down during the session.
Recognizing and Reporting Acute Change of Condition Welcome to the Elizabeth McGowan Training Institute Cell Phones and Pagers Please turn your cell phones off or turn the ringer down during the session.
Family/Caregiver Education Checklist Return Demonstration of Knowledge FIRST 24 HOURS
 of Knowledge FIRST 24 HOURS The following checklists will be completed by a PDN RN or LPN to ensure family/caregiver s skill level is adequate to safely take care of their child independently Teaching
of Knowledge FIRST 24 HOURS The following checklists will be completed by a PDN RN or LPN to ensure family/caregiver s skill level is adequate to safely take care of their child independently Teaching
Chapter 11 Assessment of the Medical Patient DOT Directory
 Chapter 11 Assessment of the Medical Patient U.S. Objectives U.S. Objectives are covered and/or supported by the PowerPoint Slide Program and Notes for Emergency Care, 11th Ed. Please see the Chapter 11
Chapter 11 Assessment of the Medical Patient U.S. Objectives U.S. Objectives are covered and/or supported by the PowerPoint Slide Program and Notes for Emergency Care, 11th Ed. Please see the Chapter 11
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
NUR 181 PHYSICAL ASSESSMENT PREPARATION FOR UNIT 1 MODULE
 NUR 181 PHYSICAL ASSESSMENT PREPARATION FOR UNIT 1 MODULE This Module is intended to give you a head start as you begin the Physical Assessment course in the Bergen Community College Nursing Program. The
NUR 181 PHYSICAL ASSESSMENT PREPARATION FOR UNIT 1 MODULE This Module is intended to give you a head start as you begin the Physical Assessment course in the Bergen Community College Nursing Program. The
Inguinal hernia repair integrated care pathway (ICP)
") Name Ward Hosp no DOB Affix patient label Inguinal hernia repair integrated care pathway (ICP) Inclusion criteria Patients undergoing inguinal hernia repair aged under 3 months corrected gestational age
Name Ward Hosp no DOB Affix patient label Inguinal hernia repair integrated care pathway (ICP) Inclusion criteria Patients undergoing inguinal hernia repair aged under 3 months corrected gestational age
Patient Controlled Analgesia Guidelines
 Patient Controlled Analgesia Guidelines Date: August 2005 Ref : PCD005 Vers : 2 Policy Profile Policy Reference Number PCD005 Version 2 Status Approved Trust Lead Director of Nursing/Acute Pain Team Implementation
Patient Controlled Analgesia Guidelines Date: August 2005 Ref : PCD005 Vers : 2 Policy Profile Policy Reference Number PCD005 Version 2 Status Approved Trust Lead Director of Nursing/Acute Pain Team Implementation
Title Audit of Compliance with the Irish Paediatric Early Warning System National Clinical Guideline No. 12.
 1 QUALITY ASSURANCE AND VERIFICATION DIVISION HEALTHCARE AUDIT SUMMARY REPORT Title Audit of Compliance with the Irish Paediatric Early Warning System National Clinical Guideline No. 12. Number QAV008/2016
1 QUALITY ASSURANCE AND VERIFICATION DIVISION HEALTHCARE AUDIT SUMMARY REPORT Title Audit of Compliance with the Irish Paediatric Early Warning System National Clinical Guideline No. 12. Number QAV008/2016
RECOGNISING AND RESPONDING TO EARLY DETERIORATION OF ACUTELY ILL PATIENTS ON THE WARDS. Presented by Primary Health Care Team
 RECOGNISING AND RESPONDING TO EARLY DETERIORATION OF ACUTELY ILL PATIENTS ON THE WARDS Presented by Primary Health Care Team 2013/2014 Aims of Session Any patient in hospital may become acutely ill, however,
RECOGNISING AND RESPONDING TO EARLY DETERIORATION OF ACUTELY ILL PATIENTS ON THE WARDS Presented by Primary Health Care Team 2013/2014 Aims of Session Any patient in hospital may become acutely ill, however,
Temporary Exclusion for Health Reasons (Including Medications and Special Diets) Policy
 Policy") Temporary Exclusion for Health Reasons Policy Rationale: Head Start Performance Standard 45 CFR Section 1304.22 (b)(i) Policy: To ensure the health and safety of our children, staff and volunteers, children
Temporary Exclusion for Health Reasons Policy Rationale: Head Start Performance Standard 45 CFR Section 1304.22 (b)(i) Policy: To ensure the health and safety of our children, staff and volunteers, children
Patient Safety: Fall Prevention. Unlicensed Assistive Personnel
 Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis
 Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Importance of Effective Training and Support During the Preceptorship period
 Importance of Effective Training and Support During the Preceptorship period Alison Dinning Inter professional Education lead Nursing Development Student nurse retention in East Midlands 4.2 million wasted
Importance of Effective Training and Support During the Preceptorship period Alison Dinning Inter professional Education lead Nursing Development Student nurse retention in East Midlands 4.2 million wasted
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition
 Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Irish Children s Triage System (ICTS) Project
 Project") Irish Children s Triage System (ICTS) Project Presented by Ruth Devers CNM3 Children's University Hospital Temple St Mary Tumelty CNM3 National Children's Hospital, Tallaght Bridget Conway CNM3 Our Lady's
Irish Children s Triage System (ICTS) Project Presented by Ruth Devers CNM3 Children's University Hospital Temple St Mary Tumelty CNM3 National Children's Hospital, Tallaght Bridget Conway CNM3 Our Lady's
9/17/2018. Place of Service Type of Service Patient Status
 Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Triage of children in the
 Triage of children in the emergency department Jocelyn Gravel MD, MSc Emergency department CHU Sainte-Justine June 7 th 2011 Disclosure No financial relationship to disclose or potential conflicts of interest
Triage of children in the emergency department Jocelyn Gravel MD, MSc Emergency department CHU Sainte-Justine June 7 th 2011 Disclosure No financial relationship to disclose or potential conflicts of interest
Simulation Design Template. Date: May 7, 2008 File Name: Group 4
 Simulation Design Template Date: May 7, 2008 File Name: Group 4 Discipline: Nursing, medicine, radiology, EMT, possible consultant (specialist ie neurosurgeon via conference call), possible social work/pastoral
Simulation Design Template Date: May 7, 2008 File Name: Group 4 Discipline: Nursing, medicine, radiology, EMT, possible consultant (specialist ie neurosurgeon via conference call), possible social work/pastoral
An avoidable death of a three-year-old child from sepsis
 An avoidable death of a three-year-old child from sepsis A report by the Health Service Ombudsman for England on an investigation into a complaint from Mr and Mrs Morrish about The Cricketfield Surgery,
An avoidable death of a three-year-old child from sepsis A report by the Health Service Ombudsman for England on an investigation into a complaint from Mr and Mrs Morrish about The Cricketfield Surgery,
A Practical Framework for Measuring Higher-Order Cognitive Constructs: An Application to Measuring Nursing Clinical Judgment
 A Practical Framework for Measuring Higher-Order Cognitive Constructs: An Application to Measuring Nursing Clinical Judgment Ada Woo, PhD National Council of State Boards of Nursing 1 Outline Background
A Practical Framework for Measuring Higher-Order Cognitive Constructs: An Application to Measuring Nursing Clinical Judgment Ada Woo, PhD National Council of State Boards of Nursing 1 Outline Background
Protocol/Procedure XX. Title: Procedural Sedation/Moderate Sedation
 Protocol/Procedure XX Title: Procedural Sedation/Moderate Sedation A. DEFINITION Procedural Moderate Sedation/Analgesia is a drug-induced depression of consciousness during which patients respond purposefully
Protocol/Procedure XX Title: Procedural Sedation/Moderate Sedation A. DEFINITION Procedural Moderate Sedation/Analgesia is a drug-induced depression of consciousness during which patients respond purposefully
Preparing for Death: A Guide for Caregivers
 Preparing for Death: A Guide for Caregivers Preparing for Death As a person is dying, their body will go through a number of physical changes as it slows down and moves toward the final stages of life.
Preparing for Death: A Guide for Caregivers Preparing for Death As a person is dying, their body will go through a number of physical changes as it slows down and moves toward the final stages of life.
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Anesthesia
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Anesthesia 1. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation.
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Anesthesia 1. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation.
All About Your Peripherally Inserted Central Catheter (PICC)
") All About Your Peripherally Inserted Central Catheter (PICC) General Information Intravenous (IV) therapy is the delivery of fluid directly into a vein. An intravenous catheter is a hollow tube that is
All About Your Peripherally Inserted Central Catheter (PICC) General Information Intravenous (IV) therapy is the delivery of fluid directly into a vein. An intravenous catheter is a hollow tube that is
Proactive Care Team Contingency Plan Original completed: Patient Details. Frameworki Number: First Name: Margaret Lives Alone: Yes No
 Proactive Care Team Contingency Plan Original completed: Patient Details Surname: Jones NHS Number: Frameworki Number: First Name: Margaret Lives Alone: Yes No Known As: Maggie Key safe: Yes No Number
Proactive Care Team Contingency Plan Original completed: Patient Details Surname: Jones NHS Number: Frameworki Number: First Name: Margaret Lives Alone: Yes No Known As: Maggie Key safe: Yes No Number
Acute Care Workflow Solutions
 Acute Care Workflow Solutions 2016 North American General Acute Care Workflow Solutions Product Leadership Award The Philips IntelliVue Guardian solution provides general floor, medical-surgical units,
Acute Care Workflow Solutions 2016 North American General Acute Care Workflow Solutions Product Leadership Award The Philips IntelliVue Guardian solution provides general floor, medical-surgical units,