(This policy rescinds any previous publication covering the same material)
|
|
|
- Teresa Janis Adams
- 5 years ago
- Views:
Transcription
1 TITLE: Isolation Protocol and Appendices (A-E) POLICIES & PROCEDURES Joint Commission: IC, PC, EC LAST REVIEW DATE: 1/2010 RESPONSIBLE PAGE 1 of 20 AREA: Infection Control Clinical Areas EFFECTIVE DATE: 2/1994 REVISION DATE: 02/2010 (This policy rescinds any previous publication covering the same material) A. Policy: Practitioners/staff will utilize appropriate isolation to manage patients/persons with infection/communicable disease. B. Purpose: To provide a guide for isolation protocol to facilitate reduction of disease transmission, infection risk and promote safety. C. Definitions: 1. STANDARD PRECAUTIONS: Standard precautions focus on the isolation of all moist body substances from all persons. This provides a consistent approach for managing all patients as potentially infectious and capable of transmitting disease. It incorporates previous Centers for Disease Control & Prevention (CDC) recommended Universal Precautions and body substance isolation. Standard precautions identify those activities that should be considered the Standard of Practice. This category addresses everything from hand washing to handling of equipment and is designed to reduce the risk of transmission of microorganisms from both recognized and unrecognized sources. This protocol applies to all patients regardless of their infection or colonization status. It eliminates the need for signage for blood and body fluid precautions and for enteric precautions because the precautions are identical for all patients and not just those with specific diagnoses. 2. TRANSMISSION-DRIVEN PRECAUTIONS: Includes many of the diagnosis-based or category specific isolations described by the CDC. These precautions are set up according to how the organism is transmitted. Precautions for these isolations will fall into three categories: a. Airborne Precautions b. Droplet Precautions c. Stringent Contact Precautions Diseases treated under these classifications are for patients documented or suspected to be infected with highly transmissible or epidemiologically important pathogens. Such diseases require additional precautions beyond Standard Precautions to interrupt transmission. These precautions are used in addition to not instead of Standard Precautions. 3. MDROs Multidrug-resistant Organisms: Microorganisms, predominantly bacteria that are resistant to one or more classes of antimicrobial agents. Although the names of certain MDROs describe resistance to only one agent (e.g., MRSA, VRE), these pathogens are
2 D. Procedures: frequently resistant to most available antimicrobial agents. Additional organisms include certain gram-negative bacteria (GNB), including those producing extended spectrum beta-lactamases (ESBLs) and others that are resistant to multiple classes of antimicrobial agents. Persons infected or colonized with these organisms should be maintained in stringent contact isolation. Such organisms may include, but are not limited to, strains of: Escherichia coli, Klebsiella pneumoniae, Pseudomonas, Acinetobacter baumannii, Stenotrophomonas maltophilia, Burkolderia cepacia and Ralstonia pickettii. See Policy IC: Method to Flag Patient Information for Resistant, Colonizing and/or Problematic Organisms: 1. NOTIFICATION OF ISOLATION: The Infection Control Department is to be notified when a patient is placed in Transmission-Driven Isolation Precautions. Notifying Infection Control is accomplished by placing an isolation order in the Medical Record, contacting the Infection Preventionist (IP) or designate by phone, leaving a voice mail message, or by (be sure in downtime to call or ). Infection Control will use the information to: a. contact the health department when appropriate/necessary; Reporting Information to the Department of Health b. evaluate the use of isolation within the institution and facilitate protocols being properly adhered to in order to protect patients and staff; c. facilitate availability of adequate isolation supplies and equipment; d. maintain and provide a grid of all patients in such isolation to each unit manager. 2. STANDARD PRECAUTIONS: Standard Precautions focus on the isolation of all moist body substances blood, feces, urine, sputum, saliva, wound drainage, and other body fluids from all patients/persons. GUIDELINES AND GENERAL INFORMATION FOR STANDARD PRECAUTIONS AND ALL PATIENT CARE: a. Hand hygiene is the single most important technique any healthcare practitioner can do to prevent the transmission of disease. Hands and other skin surfaces of the practitioner should be cleansed immediately and thoroughly if contaminated with blood, body fluids or other moist body substances. Hand hygiene is always necessary after glove removal. See Policy: Hand Hygiene b. Gloves are to be worn for all patients when working with (or anticipating any contact with) moist body substances, nonintact skin or during any contact that represents a risk for contact transmission of organisms. They are also to be worn when handling items or surfaces soiled (or possibly soiled) with body fluids, organisms and for performing vascular access or invasive procedures. After contact with each patient, gloves should be
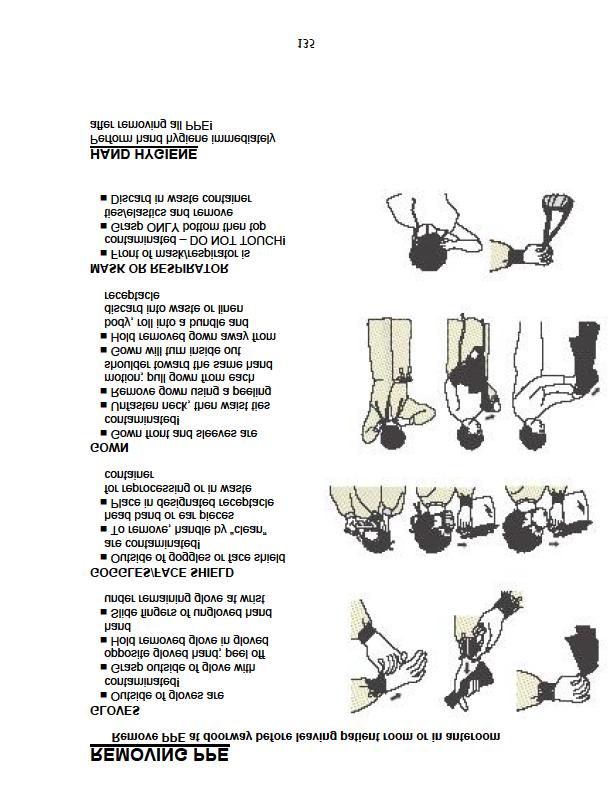
3 changed. Failure to change gloves between patient contacts is an infection control hazard. The caregiver s hands are to be cleaned immediately after the gloves are removed. c. Masks and protective eyewear or face shields are to be worn to prevent exposure of mucous membranes of the mouth, nose and eyes during procedures that are likely to generate droplets or aerosolization of blood or other body fluids. d. Gowns are to be worn to protect clothing during procedures that represent an increased risk for contact transmission, are likely to cause contact with moist body substances, or generate splashes/sprays of blood or other body fluids. The gown must be tied in the back. e. If CPR is performed, mouthpieces, resuscitation bags or other ventilation devices are available for use in all patient care areas. After use, disposable mouthpieces are to be discarded in the red biohazard containers. The resuscitation bags and masks are to be placed in a clear plastic bag and returned to Sterile Processing for disinfection and reprocessing. f. Upon completion of any procedure and prior to return to Central Sterile Processing, all soiled, reusable items are to be cleaned with soap and water to remove soil. Items used for a patient in isolation are placed in a container or clear plastic bag and label from isolation room. Reusable unit equipment must be cleaned with soap and water before disinfection with an appropriate disinfectant as per the Equipment Cleaning Reference List. g. All infectious disposable material and items are to be bagged in red plastic biohazard bags at the site of origin and discarded in the red container identified for infectious waste collection (customarily found in Soiled Utility Room). h. Blood spills are to be cleaned up with soap and water immediately. Disinfect the site/area with sodium hypochlorite (1:10 dilution of bleach to water) found in the blood spill kit. Materials used for cleaning are to be red bagged and discarded in a red infectious waste container. i. All linen that is soiled or wet with body fluids is to be placed in a moisture impervious linen bag which is found on the linen cart. j. Health care workers who have exudative or weeping dermatitis should be able to continue working if the area can be covered and remain dry. Consult with Health Services or Infection Control & Prevention for any questions. k. Laboratory specimens are to be labeled at the site of origin, in the presence of the patient, and placed in clear plastic bags with a biohazard label as they are obtained to assure the exterior container is not contaminated.
4 l. After patient use, invasive reusable equipment is to be cleaned (remove soil by wiping down with soap and water) by the user and returned to Central Sterile Processing for final disinfection. m. Equipment for use on multiple patients (phlebotomy basket, IV basket), should not be taken into the isolation room. Reusable equipment taken into the room must be disinfected before use on another patient (Example: cleansed, then disinfected with approved bleach solution.) n. At discharge or transfer, biologicals are to be removed or discarded by nursing staff i.e., when aspirators are used, discard the suction tubing, the disposable suction apparatus liner and contents in appropriate manner. 3. TRANSMISSION DRIVEN PRECAUTIONS: Guidelines for Isolation of Airborne, Droplet, and Stringent Contact Categories: a. Transmission Driven Precautions will be used for all patients suspected of having or diagnosed with airborne and/or droplet diseases, or diseases in which contact is required for transmission. i. Implementation of Transmission-Driven Precautions requires an order from the physician with the exception of MRSA, VRE, C. difficile and ESBLs. Patients with positive cultures or a code for these organisms may be placed in the appropriate transmission-driven precautions automatically. The physician must be notified of the culture. ii. An Isolation Precaution alert sign will be placed on the patient door advising everyone to see a nurse before entering the room. Immunity status will be determined and directions will be given before the individual enters. The alert sign is color coded to match the category specific isolation precaution cards. iii. Category specific Isolation Precaution Information cards are NOT to be placed on the patient s door or frame. This card will provide information as to the appropriate barrier precautions necessary. The specific disease entities are listed on the back. These cards will be kept at the nurse s station or may be placed in the top drawer of the isolation stand located outside the patient s room. b. ALL TYPES OF ISOLATION PRECAUTIONS ARE TO BE WRITTEN IN RED INK ON A WHITE ARMBAND (placed on patient), ordered in the Medical Record and circled on the CHART STICKER. Multidrug-Resistant Organisms include but are not limited to: i. Vancomycin-resistant Enterococcus (VRE) ii. Methicillin-resistant Staphylococcus aureus (MRSA) iii. Extended spectrum beta-lactamase (ESBL) iv. Multidrug-resistant gram negative bacteria (MDRGNB) v. Clostridium difficile
5 Patients with diagnosed disease entities that are antibiotic resistant or problematic, i.e. MDROs (Multidrug-Resistant Organisms) as listed above will be identified by codes placed in the hospital information system by lab personnel. The codes will appear on the patient face sheet, patient ID band and the patient labels. See Policy: IC: Method to Flag Patient Information for Resistant, Colonizing and/or Problematic Organisms: All visitors to a room with a posted isolation precaution alert sign need to stop at the nurses station for directions before entering. Visitors are required to follow the posted precautions. c. Removal from isolation status requires an order from the physician. d. A mask must be worn either by the patient or by those who are in close proximity if the patient is in Transmission-Driven Precautions due to an apparent or suspected droplet/airborne disease. Example: For patients with suspected TB, positive AFB, or a diagnosis of MTB (Mycobacterium tuberculosis), the care giver must use a particulate respirator or the patient wear a regular isolation mask during transport. See Policy IC: Respiratory Exposure Control Plan e. When an infectious process is identified, the type of isolation/precaution is to be communicated (with the exception of bloodborne pathogens) through the multiple processes stated in Part 5. Transmission Driven Isolation Setup and Communication of Isolation. f. Patients with resistant organisms (MDROs) or problem organisms which can be transmitted environmentally should be in private rooms. This includes but is not limited to VRE, MRSA or Clostridium difficile in the stool. g. Private rooms are used for patients with known transmissiondriven diseases. When a private room is not available, such as in Pediatrics or in an outbreak situation, patients infected by the same microorganism can usually share a room or area provided: i. they are not infected with other potentially transmissible microorganisms and ii. the likelihood of re-infection with the same organism is minimal The sharing of rooms in this situation is referred to as cohorting. See Part 6. Cohort System Isolation Protocol. h. Stripping and cleaning of rooms by Housekeeping, following discharge of a patient in isolation, is accomplished in the same manner as for any other patient, however, mops and cloths used in isolation rooms will be bagged and sent to the laundry for cleaning and disinfection. If the patient had a disease requiring
6 transmission- driven precautions, the sign will remain on the door until Housekeeping has cleaned the room. i. Post mortem patients to be taken to Anatomic Pathology (Morgue) - the Pathology Lab must be notified of isolation prior to transport. Place isolation sign on body of patient for autopsy. After 5:00 PM and on weekends Nursing must notify the Pathologist On call. Contact the Lab Office and personnel will give the name and pager number of the Pathologist On call. j. Transport/transfer - When it is necessary to transport a patient in isolation to another department or unit, i.e., Radiology, Surgery, Heart Lab it is important that: i. Appropriate barriers (i.e. masks, impervious dressings) are used to reduce opportunity for disease transmission. ii. Personnel in the area to which the patient is to be taken are notified of the precautions needed before the patient arrives. iii. Infected patients are informed of ways by which they can assist in preventing transmission of disease, i.e. patient wears a mask. k. AIRBORNE PRECAUTIONS (Yellow) In addition to Standard Precautions, practice the following: i. Private Airborne Infectious Isolation (A.I.I.) Rooms (negative pressure rooms) are used for patients with suspected or known TB, measles, chickenpox, disseminated Herpes zoster, smallpox, or SARS. Contact the Help Desk (Building Services) to have the A.I.I. room tested for proper air flow prior to the patient being admitted. See Policy IC: Respiratory Exposure Control Plan ii. Keep room door closed at all times to maintain negative pressure. iii. Wear respiratory protection (mask) with eye protection if you are susceptible to the disease (i.e. Varicella, Rubeola). a. Surgical mask: Measles (Rubeola), chicken pox, disseminated Herpes zoster. b. N95 Respirator mask: SARS, smallpox, novel virus, TB. For patients with TB do not re-use N95 Respirator mask if wet or soiled. SEE APPENDIX B for isolation information P.P.E. detail. iv. Limit movement/transport of the patient as much as possible. If transport is necessary, either the patient or all in his/her vicinity must wear appropriate protection (i.e. respirator for TB, SARS, and smallpox or a mask for other diseases). v. After use, the cart or wheelchair is to be cleaned and disinfected. vi. Transport of SARS, smallpox or novel virus (pandemic flu) patients will be evaluated on a case by case basis.
7 vii. viii. Avoid sharing equipment between patients. Use single-use equipment when possible. Clean and disinfect equipment before re-use if common equipment is used. Every attempt should be made to utilize single-use (disposable) equipment in cases of SARS, smallpox or Avian Influenza strains. Clean and disinfect any nondisposable equipment according to policy. l. DROPLET PRECAUTIONS (Blue) In addition to Standard Precautions the following should be practiced: i. Private Room or cohort with patients with the same microorganism with spatial separation of at least three feet. ii. Wear a mask with eye protection when working within six feet of the patient. SEE APPENDIX B for isolation information P.P.E. detail. iii. Limit movement and transport. When necessary to transport the patient between units or departments, have the patient wear a mask when possible. Care givers working within six feet of the patient should wear a mask if the patient cannot. iv. After use, the cart or wheelchair is to be cleaned and disinfected. v. Avoid sharing equipment between patients whenever possible. Utilize single-use/disposable equipment when possible. Clean and disinfect non-disposable equipment according to policy. m. STRINGENT CONTACT PRECAUTIONS (Green) In addition to Standard Precautions the following should be practiced: i. Private Room (cohort only when necessary and per policy). See Part 6. Cohort System Isolation Protocol. ii. Wear gloves when entering the room and at all times while in the patient room, providing care or otherwise. A change of gloves may be necessary after contact with material that contains the organism. iii. Gown before entering the room and at all times while in the patient room, providing care or otherwise. Remove the gloves and gown before leaving the room. Cleanse hands immediately. SEE APPENDIX B for isolation information P.P.E. detail. iv. All surfaces within the room or space are considered contaminated with organisms that are capable of being transmitted. v. Limit movement and transport. When necessary to transport the patient between units or departments, cover the patient and cart with a clean sheet. Wear clean gown and gloves for transport.
8 vi. vii. viii. After use, the cart or wheelchair must be cleansed of soil and disinfected with an approved disinfectant solution (1:10 bleach solution for C. difficile). Articles contaminated with infective material should be discarded if disposable or cleansed of soil, bagged and labeled before being sent for reprocessing. See Policy Reference List for Equipment Cleaning Unit equipment is to be cleansed of any soil and disinfected with an approved disinfectant solution (1:10 bleach solution for C. difficile). Terminal cleaning of rooms used to isolate Clostridium difficile (C. diff.) or Vancomycin Resistant Enterococcus (VRE) consists of a double clean/disinfect by Housekeeping with 1:10 bleach solution used on hightouch areas and bathrooms. 4. ISOLATION PRECAUTION SIGNAGE: a. The Appendix pages contain Isolation Information Card and sample signage for the patient s door. Signage is used with Transmission Driven isolation types Airborne, Droplet and Stringent Contact. b. This information must also be written, in RED INK, on a white arm band which is placed on the patient and circled on the chart sticker. An order for the specific isolation type should be placed in the Medical Record which will appear in Orders Tab, Rounds Report and Patient Care Summary. 5. TRANSMISSION DRIVEN ISOLATION SETUP AND COMMUNICATION OF ISOLATION: a. Obtain and document order in the Medical Record. In the case of MRSA, VRE, C. difficile, ESBL, document that a positive culture was received, the patient was placed in isolation, and the physician was notified. b. Place the appropriate color-coded isolation sign on the door or doorway of the patient s room. a. Yellow = Airborne b. Blue = Droplet c. Green = Stringent Contact c. Write the isolation category in RED INK on the following items: a. Plain white patient identiband (place on patient) i.e., Contact Precautions b. Circle on Chart Sticker d. Enter the isolation order in the Medical Record. e. Obtain isolation stand from Housekeeping at ext or Support Services f. Obtain additional YELLOW isolation gowns from the Linen Room at ext Do not deplete the supply on your linen cart. g. Obtain box of exam gloves. h. Obtain masks fluid shield for splash/spray, yellow isolation or N-95 particulate respirators as needed for respiratory protection. i. Obtain a disposable stethoscope from Central Sterile Processing or designate a stethoscope for the room. j. Obtain a disposable thermometer from C.S.P.
9 k. Place the color-coded isolation Information Card for reference in the top drawer of isolation stand or at the nurse s station. Do not place the card in view of visitors. l. Indicate the isolation category on all documentation or communication. m. Indicate the isolation category on all pre-procedural and surgical checklists. n. Always contact other areas, departments or facilities of isolation as soon as possible or well in advance of transport/transfer (i.e. EMS, funeral home staff, etc.). See Policy IC: Reporting Infections / Communicable Diseases to Referring and Receiving Healthcare Organizations o. DO NOT remove the Isolation Sign from the door when the patient leaves or transfers. Housekeeping will remove the sign and return it to the nurse in charge at the completion of cleaning and disinfection. Signs removed and returned to the nurse should be discarded. 6. COHORT SYSTEM ISOLATION PROTOCOL: a. Cohort system isolation is used for certain circumstances to separate patients with communicable disease from those without communicable disease in order to minimize disease transmission. This system is used for, but not limited to, the following situations: i. Private rooms are limited ii. Outbreak or epidemic b. Private Rooms Limited: When single-patient rooms are in short supply, apply the following principles for decisions on placement: i. Prioritize patients with conditions that may facilitate transmission for single-patient room placement. ii. Place together in the same room (cohort) patients who are infected or colonized with the same pathogen and are suitable roommates. iii. If it becomes necessary to place a patient who requires Contact Precautions in a room with a patient who is not infected or colonized with the same infectious agent: a. Avoid placing with patients who have conditions that may increase the risk of adverse outcome from infection or that may facilitate transmission (e.g., immunocompromised, open wounds). b. Verify that patients are physically separated greater than three feet apart from each other. Draw the privacy curtain between beds to minimize opportunities for direct contact. c. Change protective attire and perform hand hygiene between contacts with patients in the same room, regardless of whether one or both are in Contact Precautions. c. Outbreak or Epidemic: It is the responsibility of all staff to minimize the spread of infection by practicing good technique in hand hygiene, in procedures and isolation for every patient. To
10 further limit the spread of organisms, implementation of a cohort system may be used to minimize the spread of infection in clusters of organisms or during contagious outbreaks. i. Evaluation/investigation is justified in cases where the infection rate of any site, pathogen or site/pathogen combination has increased 2 to 2 ½ times the normal rate. ii. Outbreak evaluation/investigation is conducted by Infection Control & Prevention. Findings are discussed in Infection Control & Prevention Committee or by the Executive Committee and later taken to Infection Control & Prevention Committee. iii. Cohorting may be utilized to halt transmission and assist with investigation. Cohorting in this instance involves separating infected and/or colonized patients geographically within the unit from non-infected and/or non-colonized patients. At no time will employees assigned to a cohort group of patients care for noncohorted patients. iv. The following procedure will be used primarily in, but not limited to, such areas as Pediatrics, NICU, MICU and areas with more than one patient in isolation for an infectious disease of major public health risk (e.g., SARS, Smallpox, novel virus, epidemic/pandemic illness). v. Procedure: a. Patients with clinical symptoms and suspected infection or colonization are moved to rooms in the same geographic section of the unit and are cared for by nurses who have already been exposed or who are assigned to the cohort patients and to no patient who is not in the cohort. The assignment is to persist as long as the cohort exists in order to avoid cross-contamination to noninfected/noncolonized patients and health care workers. b. Good hand hygiene is required. Wash hands prior to care and immediately following care and/or removal of powdered gloves. Utilize the personal protective equipment indicated. c. The cohort will be terminated as soon as possible. The decision to terminate the cohort must be made by the physician who initiated it. d. Housekeeping procedures are to be followed as indicated by the type of isolation. e. Communication is a very important key in maintaining the cohort system. The charge nurse is to inform all personnel when a cohort is in effect. Patients should not leave the area unless it is absolutely necessary. If the patient must be moved for testing, etc., follow the isolation precautions indicated. f. If a patient not in the cohort develops signs/symptoms or the clinical case definition of the infection changes (qualifying other patients to be
11 placed in the cohort), communicate to the attending physician and to the Infectious Disease Physician involved to discuss adding the patient to the cohort. Siegel, J., Rhinehart, E., Jackson, M., Chiarello, L., the Healthcare Infection Control Practices Advisory Committee, Guideline for Isolation Precautions: Preventing Transmission Of Infectious Agents in Healthcare Settings, June Additional Aultman Policies for Reference Pandemic Flu Policy Patient Surge Capacity Policy 2007: Infection Directory Code Blue for Patient in Isolation Hospital Visitation During Influenza Season

12 APPENDIX A
13 APPENDIX B AIRBORNE PRECAUTIONS Visitors Report to Nurses Station Before entering Room In addition to STANDARD PRECAUTIONS: 1.) Airborne Infectious Isolation (A.I.I.) Room is to be used. 2.) Masks with eye protection are to be used by persons susceptible to the disease: a.) Surgical Mask: Measles (Rubeola), Chickenpox, Herpes zoster disseminated b.) N95 Respirator mask: SARS, Smallpox, TB, Avian Influenza Strains 3.) Keep the door to the hallway closed as much as possible. 4.) Limit transport of the patient as much as possible: if the patient must be transported, either the patient should wear a mask or the employees with him should wear a mask with eye protection. Cleanse/disinfect cart or wheelchair after use. 5.) Gloves are required to protect hands from secretions. 6.) Gowns are required to prevent contamination of clothing. 7.) HANDS MUST BE CLEANSED PER STANDARD PRECAUTIONS and POLICY. 8.) Utilize single-use/disposable equipment when possible (especially in cases of smallpox, SARS or Avian Influenza Strains). Cleanse and disinfect non-disposable equipment according to policy. Form 1577 D: 1/10 INDICATED FOR: Tuberculosis Measles (Rubeola) Varicella zoster (chickenpox) Disseminated Herpes zoster (shingles) mult. locations to include mucous membranes Smallpox Airborne and Contact S.A.R.S. (Severe Acute Respiratory Syndrome) Airborne and Contact Avian Influenza strains - Contact Infection Control for current CDC guidance Susceptible persons should not enter the room of patients known or suspected to have measles (rubeola) or Varicella (chickenpox) if other immune care givers are available. If susceptible persons must enter the room, they must wear respiratory protection. Persons immune to measles or chickenpox need not wear respiratory protection.
14 DROPLET PRECAUTIONS Visitors Report to Nurses Station Before entering Room In addition to STANDARD PRECAUTIONS, do the following: 1.) Masks with eye protection are required for those working within 6 feet of the patient. 2.) Gowns are required to prevent contamination of clothing. 3.) Gloves are required to protect hands from secretions. 4.) Place patient in a private room or cohort. Special air ventilation is not necessary. 5.) If moving/transport of the patient is necessary, the patient should wear a mask. If this is not feasible, the health care workers moving the patient will wear a mask with eye protection. Cleanse/disinfect cart or wheelchair after use. 6.) HANDS MUST BE CLEANSED PER STANDARD PRECAUTIONS and POLICY. 7.) Utilize single-use/disposable equipment when possible. Cleanse and disinfect nondisposable equipment according to policy. Form 1576 D 1/10 INDICATED FOR: Epiglottitis, Haemophilus influenzae, type b Erythema infectiosum (Parvovirus B19) Diphtheria, pharyngeal Influenza seasonal * for Pandemic influenza or novel virus contact Infection Control for current CDC guidance Measles (Rubella) Meningitis Neisseria meningitides (meningococcal) known or suspected Haemophilus influenzae, type b known or suspected Meningococcemia Meningococcal pneumonia Mumps Mycoplasma IgM Pertussis (Whooping cough) Pneumococcal pneumonia Pneumonia, Haemophilus influenzae, type b in infants and children Scarlet fever Group A streptococcus pharyngitis - infants/young children pneumonia infants/young children
15 Stringent CONTACT PRECAUTIONS Visitors Report to Nurses Station Before entering Room In addition to STANDARD PRECAUTIONS, do the following: 1.) Use a Private Room (cohort if necessary and according to policy). 2.) Gown and gloves are to be worn upon entering the room and at all times while in the room, not just while providing direct patient care. A change of gloves may be necessary after contact with material that contains the organism i.e., VRE, C. difficile. 3.) A mask with eye protection is to be used when there is potential for splash, spray or aerosolization. 4.) If the patient must be moved or transported, cover the patient and cart with clean linens. Maintain precautions to prevent transmission of organisms. Wear clean gown and gloves for transport. Cleanse and disinfect cart or wheelchair after use with appropriate disinfectant (1:10 bleach for C. difficile). 5.) HANDS MUST BE CLEANSED PER STANDARD PRECAUTIONS and POLICY. 6.) Articles contaminated with infective material should be discarded (disposable) or wiped down, bagged and labeled before being sent for decontamination and reprocessing. Unit equipment removed from the room must be cleansed (remove soil) then disinfected with appropriate disinfectant (1:10 bleach for C. difficile). Form 462 D: 1/10 INDICATED FOR: Acute respiratory infections in infants and children - (mask also) RSV, colds, bronchitis, Bronchiolitis, adenovirus, influenza, parainfluenza, Group A Streptococcus pharyngitis & pneumonia + Droplet Precautions Clostridium difficile (C. diff.) Conjunctivitis, gonococcal in newborns Diphtheria, cutaneous Group A Streptococcus Major wound, skin, burn (no dressing or dressing unable to contain drainage adequately). Herpes zoster (shingles) confined to skin surface Impetigo Multidrug-resistant Organisms (MDROs): Extended Spectrum beta-lactamase (ESBL) Methicillin-resistant Staphylococcus aureus (MRSA) Multidrug resistant gram negative bacteria (MDRGNB), i.e. Acinetobacter Vancomycin-resistant Enterococcus (VRE) Haemophilus influenzae Pediculosis Rabies Scabies Rubella congenital and other
16 APPENDIX C HOMEGOING INSTRUCTIONS FOR FAMILY AND VISITORS CLOSTRIDIUM DIFFICILE (C. DIFF) and VANCOMYCIN RESISTANT ENTEROCOCCI (VRE) 1.) Hand Cleansing - Cleanse your hands (soap and water) after contact with the patient and/or contaminated items. - Follow all soap and water hand washes with alcohol-based sanitizer, i.e., Purell to provide further protection. Allow to air dry. - Use an antibacterial soap (Dial, Hibiclens) when feasible. When washing, lather for 15 seconds. Dry hands thoroughly. 2.) Gloves - Wear gloves if you must handle stool, urine, blood, wound drainage, dressings and soiled linens. - Always wash your hands after you remove your gloves. 3.) Eating - Always wash hands before preparing, serving and/or eating food. - The patient should not prepare food for others. - Do not share dishes and utensils or food from the patient s plate. - Wash dishes with detergent and water. To be cautious, you could rinse the dishes in a mild bleach and water solution. One part bleach to 9 parts water. The bleach solution should be made fresh daily. Be sure to rinse well. 4.) Cleaning (wear gloves) - Always cleanse soiled items or surfaces with soap and water first. Disinfection can be accomplished with either the 1:10 bleach solution (for C. difficile and surfaces that can withstand bleach) or any disinfectant cleaner/cleanser used for cleaning. VRE is inactivated easily on surfaces. If you wet a surface with the disinfectant and let it air dry, that should be adequate contact time. For C. diff. it is better to scrub and rinse. - Ideally, the patient should have a bathroom to themselves. If this is not possible, clean the toilet and sink every time the patient uses them (bleach solution), especially after a bowel movement. Clean the areas daily if no stool. 5.) Waste Management - Throw away all disposable waste such as dressings, bandages, adult diapers into plastic bags and tie closed. These bags can be discarded with the regular garbage. 6.) Laundry - Wash the patients clothing and bedding separately in detergent and bleach (for C. difficile, until all diarrhea has ceased; for VRE only if linens are soiled with body substances). Revised 8/09

17 APPENDIX D
18

19 APPENDIX E
20
ISOLATION TABLE OF CONTENTS STANDARD PRECAUTIONS... 2 CONTACT PRECAUTIONS... 4 DROPLET PRECAUTIONS... 6 ISOLATION PROCEDURES... 7
 ISOLATION TABLE OF CONTENTS STANDARD PRECAUTIONS... 2 BARRIERS INDICATED IN STANDARD PRECAUTIONS... 2 PERSONAL PROTECTIVE EQUIPMENT... 3 CONTACT PRECAUTIONS... 4 RESIDENT PLACEMENT... 4 RESIDENT TRANSPORT...
ISOLATION TABLE OF CONTENTS STANDARD PRECAUTIONS... 2 BARRIERS INDICATED IN STANDARD PRECAUTIONS... 2 PERSONAL PROTECTIVE EQUIPMENT... 3 CONTACT PRECAUTIONS... 4 RESIDENT PLACEMENT... 4 RESIDENT TRANSPORT...
SECTION: PATIENT RELATED INFECTION CONTROL NUMBER: 2.1 TRANSMISSION BASED PRECAUTIONS
 University of Connecticut Health Center Page 1 of 8 SECTION: PATIENT RELATED INFECTION CONTROL NUMBER: 2.1 TRANSMISSION BASED PRECAUTIONS PURPOSE: Transmission-Based s are designed for patients documented
University of Connecticut Health Center Page 1 of 8 SECTION: PATIENT RELATED INFECTION CONTROL NUMBER: 2.1 TRANSMISSION BASED PRECAUTIONS PURPOSE: Transmission-Based s are designed for patients documented
INFECTION C ONTROL CONTROL CONTROL EDUCATION PROGRAM
 INFECTION CONTROL EDUCATION PROGRAM Isolation Precautions Isolating the disease not the patient The Purpose is To protect compromised patient from environment To prevent the spread of communicable diseases.
INFECTION CONTROL EDUCATION PROGRAM Isolation Precautions Isolating the disease not the patient The Purpose is To protect compromised patient from environment To prevent the spread of communicable diseases.
Infection Control Prevention Strategies. For Clinical Personnel
 Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Isolation Categories of Transmission-Based Precautions
 Isolation Categories of Transmission-Based Highlights Policy Statement Standard shall be used when caring for residents at all times regardless of their suspected or confirmed infection status. Transmission-Based
Isolation Categories of Transmission-Based Highlights Policy Statement Standard shall be used when caring for residents at all times regardless of their suspected or confirmed infection status. Transmission-Based
Self-Instructional Packet (SIP)
") Self-Instructional Packet (SIP) Advanced Infection Prevention and Control Training Module 4 Transmission Based Precautions February 11, 2013 Page 1 Learning Objectives Module One Introduction to Infection
Self-Instructional Packet (SIP) Advanced Infection Prevention and Control Training Module 4 Transmission Based Precautions February 11, 2013 Page 1 Learning Objectives Module One Introduction to Infection
Infection Control Prevention Strategies. For Clinical Personnel
 Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Infection Prevention and Control and Isolation Authored by: Infection Prevention and Control Department
 Infection Prevention and Control and Isolation 2015 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
Infection Prevention and Control and Isolation 2015 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
Infection Prevention Implementation and adherence to infection prevention practices are the keys to preventing the transmission of infectious diseases
 Infection Prevention Infection Prevention Implementation and adherence to infection prevention practices are the keys to preventing the transmission of infectious diseases to yourself, family members,
Infection Prevention Infection Prevention Implementation and adherence to infection prevention practices are the keys to preventing the transmission of infectious diseases to yourself, family members,
Infection Prevention and Control for Phlebotomy
 Page 1 of 10 POLICY STATEMENT: It is Sunnybrook s Policy to prevent the spread of infection within the health care institution from patient to patient, patient to staff, staff to patient by: a) providing
Page 1 of 10 POLICY STATEMENT: It is Sunnybrook s Policy to prevent the spread of infection within the health care institution from patient to patient, patient to staff, staff to patient by: a) providing
Emergency Department Isolation Precautions
 Carolinas HealthCare System Department of Infection Prevention I. SCOPE Emergency Department Isolation Precautions This policy applies to all Carolinas HealthCare System Emergency Department (ED) locations
Carolinas HealthCare System Department of Infection Prevention I. SCOPE Emergency Department Isolation Precautions This policy applies to all Carolinas HealthCare System Emergency Department (ED) locations
THE INFECTION CONTROL STAFF
 INFECTION CONTROL THE INFECTION CONTROL STAFF INTEGRIS BAPTIST V. Ramgopal, M.D., Hospital Epidemiologist Gwen Harington, RN, BSN, CIC, Infection Control Specialist Kathy Knecht, RN, Surveillance Coordinator
INFECTION CONTROL THE INFECTION CONTROL STAFF INTEGRIS BAPTIST V. Ramgopal, M.D., Hospital Epidemiologist Gwen Harington, RN, BSN, CIC, Infection Control Specialist Kathy Knecht, RN, Surveillance Coordinator
Lightning Overview: Infection Control
 Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
NEW EMPLOYEE ORIENTATION INFECTION PREVENTION AND CONTROL
 NEW EMPLOYEE ORIENTATION INFECTION PREVENTION AND CONTROL Infection Control Rev. 3/2018 Hand Hygiene Standard Precautions TOPICS Transmission-Based Precautions Personal Protective Equipment (PPE) Multiple
NEW EMPLOYEE ORIENTATION INFECTION PREVENTION AND CONTROL Infection Control Rev. 3/2018 Hand Hygiene Standard Precautions TOPICS Transmission-Based Precautions Personal Protective Equipment (PPE) Multiple
Oregon Health & Science University Department of Surgery Standard Precautions Policy
 Standard Precautions Policy 1. Policy Standard Precautions are to be followed by all employees for all patients within and entering the OHSU system. Standard Precautions are designed to reduce the risk
Standard Precautions Policy 1. Policy Standard Precautions are to be followed by all employees for all patients within and entering the OHSU system. Standard Precautions are designed to reduce the risk
INFECTION CONTROL POLICY DATE: 03/01/01 REVISED: 7/15/09 STATEMENT
 Of, INFECTION CONTROL POLICY DEPARTMENT OF RADIOLOGY DATE: 03/01/01 REVISED: 7/15/09 STATEMENT GENERAL The Department of Radiology adheres to the Duke Infection Control policies and the DUMC Exposure Control
Of, INFECTION CONTROL POLICY DEPARTMENT OF RADIOLOGY DATE: 03/01/01 REVISED: 7/15/09 STATEMENT GENERAL The Department of Radiology adheres to the Duke Infection Control policies and the DUMC Exposure Control
Infection Prevention and Control Annual Education Authored by: Infection Prevention and Control Department
 Infection Prevention and Control Annual Education 2013 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
Infection Prevention and Control Annual Education 2013 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
Infection Prevention Isolation Precautions Toolkit
 Infection Prevention Isolation Precautions Toolkit The toolkit provides: Link(s) to revised Isolation Policy on The Point Link to ICON training video and key changes to policy (NEW) Quick Review Chart
Infection Prevention Isolation Precautions Toolkit The toolkit provides: Link(s) to revised Isolation Policy on The Point Link to ICON training video and key changes to policy (NEW) Quick Review Chart
Infection Prevention and Control Annual Education 2010
 Infection Prevention and Control Annual Education 2010 Authored by: Cathy Clark, RN MPH CIC Mary Whitaker, RN CIC Bola Ogundimu, RN MPH Marie Commiskey, RN CCRN CIC Modified for affiliated schools students
Infection Prevention and Control Annual Education 2010 Authored by: Cathy Clark, RN MPH CIC Mary Whitaker, RN CIC Bola Ogundimu, RN MPH Marie Commiskey, RN CCRN CIC Modified for affiliated schools students
Department of Infection Control and Hospital Epidemiology. New Employee Orientation
 Department of Infection Control and Hospital Epidemiology New Employee Orientation Infection Control Contact Information Office 350 Parnassus Ave, Suite 510 Main Office Phone: 353-4343 Practitioner On-Call:
Department of Infection Control and Hospital Epidemiology New Employee Orientation Infection Control Contact Information Office 350 Parnassus Ave, Suite 510 Main Office Phone: 353-4343 Practitioner On-Call:
Infection Prevention and Control
 Infection Prevention and Control Infection Prevention and Control Program IPAC program consists of three healthcare professionals IPAC department is located on the 9 th floor and is available Monday to
Infection Prevention and Control Infection Prevention and Control Program IPAC program consists of three healthcare professionals IPAC department is located on the 9 th floor and is available Monday to
ISOLATION PRECAUTIONS INTRODUCTION. Standard Precautions are used for all patient care situations, but they
 ISOLATION PRECAUTIONS INTRODUCTION Standard Precautions are used for all patient care situations, but they may not always be sufficient. If a patient is known or suspected to be infected with certain pathogens
ISOLATION PRECAUTIONS INTRODUCTION Standard Precautions are used for all patient care situations, but they may not always be sufficient. If a patient is known or suspected to be infected with certain pathogens
Infection Control and Prevention On-site Review Tool Hospitals
 Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
DISEASE TRANSMISSION PRECAUTIONS AND PERSONAL PROTECTIVE EQUIPMENT (PPE)
") DISEASE TRANSMISSION PRECAUTIONS AND PERSONAL PROTECTIVE EQUIPMENT (PPE) Course Health Science Unit VII Infection Control Essential Question What must health care workers do to protect themselves and others
DISEASE TRANSMISSION PRECAUTIONS AND PERSONAL PROTECTIVE EQUIPMENT (PPE) Course Health Science Unit VII Infection Control Essential Question What must health care workers do to protect themselves and others
INFECTION CONTROL ORIENTATION TRAINING 2006
 INFECTION CONTROL ORIENTATION TRAINING 2006 INFECTION CONTROL OSHA BLOODBORNE PATHOGEN STANDARD STANDARD PRECAUTIONS RISK OF EXPOSURE TO CONTAMINATED MATERIALS USE OF PROTECTIVE EQUIPMENT FOLLOW-UP OF
INFECTION CONTROL ORIENTATION TRAINING 2006 INFECTION CONTROL OSHA BLOODBORNE PATHOGEN STANDARD STANDARD PRECAUTIONS RISK OF EXPOSURE TO CONTAMINATED MATERIALS USE OF PROTECTIVE EQUIPMENT FOLLOW-UP OF
Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings
 in Healthcare Settings") Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings : Program Goal Improve personnel safety in the healthcare environment through appropriate use of PPE. :
Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings : Program Goal Improve personnel safety in the healthcare environment through appropriate use of PPE. :
NA REVIEWED/REVISED: DATE TO BE REVIEWED: 01/31/2016 EMERGENCY MEDICAL SERVICES
 POLICY NO: 545 DATE ISSUED: 10/14/2014 DATE NA REVIEWED/REVISED: DATE TO BE REVIEWED: 01/31/2016 EMERGENCY MEDICAL SERVICES Purpose: The purpose of this policy is to state the minimum standards for infection
POLICY NO: 545 DATE ISSUED: 10/14/2014 DATE NA REVIEWED/REVISED: DATE TO BE REVIEWED: 01/31/2016 EMERGENCY MEDICAL SERVICES Purpose: The purpose of this policy is to state the minimum standards for infection
Single room with negative pressure ventilation in relation to surrounding areas
 7. Airborne/Contact Precautions 7.1 Introduction Airborne/Contact Precautions are required for patients diagnosed with, or suspected of having an infectious microorganism transmitted by the airborne and
7. Airborne/Contact Precautions 7.1 Introduction Airborne/Contact Precautions are required for patients diagnosed with, or suspected of having an infectious microorganism transmitted by the airborne and
DEPARTMENTAL POLICY. Northwestern Memorial Hospital
 Northwestern Memorial Hospital DEPARTMENTAL POLICY Subject: INFECTION CONTROL AND PREVENTION Title: ISOLATION PRECAUTIONS 1 of 8 Revision of: 04/2004 Policy # Effective Date: 01/2007 I. PURPOSE: Appropriate
Northwestern Memorial Hospital DEPARTMENTAL POLICY Subject: INFECTION CONTROL AND PREVENTION Title: ISOLATION PRECAUTIONS 1 of 8 Revision of: 04/2004 Policy # Effective Date: 01/2007 I. PURPOSE: Appropriate
IC CONTACT and CONTACT PLUS PRECAUTIONS REV. JULY 2017
 IC.04.03 CONTACT and CONTACT PLUS PRECAUTIONS REV. JULY 2017 Standard In addition to Routine Practices, Contact Precautions or Contact Plus Precautions will be used for patients known or suspected to have
IC.04.03 CONTACT and CONTACT PLUS PRECAUTIONS REV. JULY 2017 Standard In addition to Routine Practices, Contact Precautions or Contact Plus Precautions will be used for patients known or suspected to have
POLICIES & PROCEDURES. Number: Authorization: SHR Regional Infection Control Committee
 POLICIES & PROCEDURES Number: 30-40 Title: Signage Authorization: SHR Regional Infection Control Committee Source: Infection Prevention & Control Date Initiated: June 5, 2001 Date Reaffirmed: March, 2007
POLICIES & PROCEDURES Number: 30-40 Title: Signage Authorization: SHR Regional Infection Control Committee Source: Infection Prevention & Control Date Initiated: June 5, 2001 Date Reaffirmed: March, 2007
Objectives. IPC Open calls - bi-weekly series. Introduction to Infection Prevention & Control (IPC) Open Call Series
 Open Call Series") Introduction to Infection Prevention & Control (IPC) Open Call Series #4 Transmission Precautions Isolate the Organism and Not the Resident Diane Dohm MT, IP, CIC, CPHQ MetaStar Anne Haddad, MPH MPRO March
Introduction to Infection Prevention & Control (IPC) Open Call Series #4 Transmission Precautions Isolate the Organism and Not the Resident Diane Dohm MT, IP, CIC, CPHQ MetaStar Anne Haddad, MPH MPRO March
Infection Control Manual. Table of Contents
 This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
Standard Precautions must always be used in addition to Transmission Based Precautions.
 4. Airborne Precautions Airborne Precautions are recommended in addition to Standard Precautions to prevent the transmission of infections spread by very small respiratory particles which are expelled
4. Airborne Precautions Airborne Precautions are recommended in addition to Standard Precautions to prevent the transmission of infections spread by very small respiratory particles which are expelled
Standard Precautions
 Standard Precautions Speciality: Infection Control 1. Indications 1.1 Background Standard Precautions This definition broadens the coverage of the previously known Universal Precautions by recognizing
Standard Precautions Speciality: Infection Control 1. Indications 1.1 Background Standard Precautions This definition broadens the coverage of the previously known Universal Precautions by recognizing
STANDARD PRECAUTIONS POLICY Page 1 of 8 Reviewed: May 2017
 Page 1 of 8 Policy Applies to: All Mercy Staff, Credentialed Specialists, Allied Health Professionals, students, patients, visitors and contractors will be supported to meet policy requirements Related
Page 1 of 8 Policy Applies to: All Mercy Staff, Credentialed Specialists, Allied Health Professionals, students, patients, visitors and contractors will be supported to meet policy requirements Related
CPNE CLINICAL PERFORMANCE IN NURSING EXAMINATION
 22nd edition CPNE CLINICAL PERFORMANCE IN NURSING EXAMINATION Infection Control Module No part of this publication may be reproduced or distributed in any form or by any means, or stored in a database
22nd edition CPNE CLINICAL PERFORMANCE IN NURSING EXAMINATION Infection Control Module No part of this publication may be reproduced or distributed in any form or by any means, or stored in a database
8. Droplet/Contact Precautions. 8.1 Introduction
 8. Droplet/Contact Precautions 8.1 Introduction Droplet/Contact Precautions are required for patients diagnosed with, or suspected of having infectious microorganisms transmitted by the droplet route and
8. Droplet/Contact Precautions 8.1 Introduction Droplet/Contact Precautions are required for patients diagnosed with, or suspected of having infectious microorganisms transmitted by the droplet route and
Vancomycin-Resistant Enterococcus (VRE)
") Approved by: Vancomycin-Resistant Enterococcus (VRE) Vice President & Chief Medical Officer Corporate Policy & Procedures Manual VI-40 Date Approved July 14, 2016 August 12, 2016 Next Review (3 years from
Approved by: Vancomycin-Resistant Enterococcus (VRE) Vice President & Chief Medical Officer Corporate Policy & Procedures Manual VI-40 Date Approved July 14, 2016 August 12, 2016 Next Review (3 years from
Infection Prevention, Control & Immunizations
 Infection Control: This facility task must be used to investigate compliance at F880, F881, and F883. For the purpose of this task, staff includes employees, consultants, contractors, volunteers, and others
Infection Control: This facility task must be used to investigate compliance at F880, F881, and F883. For the purpose of this task, staff includes employees, consultants, contractors, volunteers, and others
ACG GI Practice Toolbox. Developing an Infection Control Plan for Your Office
 ACG GI Practice Toolbox Developing an Infection Control Plan for Your Office AUTHOR: Louis J. Wilson, MD, FACG, Wichita Falls Gastroenterology Associates, Wichita Falls, Texas INTRODUCTION: Preventing
ACG GI Practice Toolbox Developing an Infection Control Plan for Your Office AUTHOR: Louis J. Wilson, MD, FACG, Wichita Falls Gastroenterology Associates, Wichita Falls, Texas INTRODUCTION: Preventing
Principles of Infection Prevention and Control
 Principles of Infection Prevention and Control Liz Van Horne Manager, Core Competencies Senior Infection Prevention & Control Professional OAHPP Outbreak Management Workshop September 15, 2010 Objectives
Principles of Infection Prevention and Control Liz Van Horne Manager, Core Competencies Senior Infection Prevention & Control Professional OAHPP Outbreak Management Workshop September 15, 2010 Objectives
A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page
 Page 1 A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page IH0400: Contact Precautions EFFECTIVE DATE: September
Page 1 A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page IH0400: Contact Precautions EFFECTIVE DATE: September
Background of Initiative
 Outline 2 Background of Initiative 3 Development of Recommendations 4 5 6 Development and Recommendations 7 Routine Practices Based on the premise that: All patients are potentially infectious (even if
Outline 2 Background of Initiative 3 Development of Recommendations 4 5 6 Development and Recommendations 7 Routine Practices Based on the premise that: All patients are potentially infectious (even if
PRECAUTIONS IN INFECTION CONTROL
 PRECAUTIONS IN INFECTION CONTROL Standard precautions Transmission-based precautions Contact precautions Airborne precautions Droplet precautions 1 2/25/2015 WHO HAVE TO PROTECT IN HOSPITALS? Patients
PRECAUTIONS IN INFECTION CONTROL Standard precautions Transmission-based precautions Contact precautions Airborne precautions Droplet precautions 1 2/25/2015 WHO HAVE TO PROTECT IN HOSPITALS? Patients
STOP CONTACT PRECAUTIONS. Staff: Families and visitors: Please report to staff before entering. Required: - Gown & Gloves. Bed #
 CONTACT PRECAUTIONS Clean hs Clean hs with A) h foam/gel or B) soap water HOUSEER will - Gown & Gloves Point-of-Care Risk When there is a risk of splash or spray, wear face eye. For more information, refer
CONTACT PRECAUTIONS Clean hs Clean hs with A) h foam/gel or B) soap water HOUSEER will - Gown & Gloves Point-of-Care Risk When there is a risk of splash or spray, wear face eye. For more information, refer
Fall HOLLY ALEXANDER Academic Coordinator of Clinical Education MS157
 Fall 2010 HOLLY ALEXANDER Academic Coordinator of Clinical Education 609-570-3478 AlexandH@mccc.edu MS157 To reduce infection & prevent disease transmission Nosocomial Infection: an infection acquired
Fall 2010 HOLLY ALEXANDER Academic Coordinator of Clinical Education 609-570-3478 AlexandH@mccc.edu MS157 To reduce infection & prevent disease transmission Nosocomial Infection: an infection acquired
INFECTION CONTROL ORIENTATION TRAINING 2009
 INFECTION CONTROL ORIENTATION TRAINING 2009 STANDARD PRECAUTIONS BASICALLY. If it s WET and NOT YOURS, don t get any on you!! PPE And Safety Devices Are Provided!! Use them correctly to protect yourself!!
INFECTION CONTROL ORIENTATION TRAINING 2009 STANDARD PRECAUTIONS BASICALLY. If it s WET and NOT YOURS, don t get any on you!! PPE And Safety Devices Are Provided!! Use them correctly to protect yourself!!
Guidelines on Infection Prevention and Control for Cork Kerry Community Healthcare 06: Transmission Based Precautions
 Guidelines on Infection Prevention and Control for Cork Kerry Community Healthcare 06: Transmission Based Precautions This guidance document has been adopted as the policy document by: Organisation:...
Guidelines on Infection Prevention and Control for Cork Kerry Community Healthcare 06: Transmission Based Precautions This guidance document has been adopted as the policy document by: Organisation:...
2014 Annual Continuing Education Module. Contents
 This self-directed learning module contains information you are expected to know to protect yourself, our patients, and our guests. Content Experts: Infection Prevention Target Audience: All Teammates
This self-directed learning module contains information you are expected to know to protect yourself, our patients, and our guests. Content Experts: Infection Prevention Target Audience: All Teammates
Replaces: 08/11/16. Formulated: 1/2000 TRANSMISSION-BASED PRECAUTIONS
 CMHC INFECTION CONTROL Effective : 08/10/17 Page 1 of 4 POLICY: TDCJ and any medical contractors will implement Transmission-Based Precautions as needed to interrupt the transmission of potentially contagious
CMHC INFECTION CONTROL Effective : 08/10/17 Page 1 of 4 POLICY: TDCJ and any medical contractors will implement Transmission-Based Precautions as needed to interrupt the transmission of potentially contagious
The environment. We can all help to keep the patient rooms clean and sanitary. Clean rooms and a clean hospital or nursing home spread less germs.
 Infection Control Objectives: After you take this class, you will be able to: 1. List some of the reasons why residents and patients are at risk for getting infections. 2. Discuss the cycle of infection
Infection Control Objectives: After you take this class, you will be able to: 1. List some of the reasons why residents and patients are at risk for getting infections. 2. Discuss the cycle of infection
& ADDITIONAL PRECAUTIONS:
 INFECTION CONTROL GUIDELINES: STANDARD PRECAUTIONS & ADDITIONAL PRECAUTIONS: LESSON PLAN Lesson overview Time: One hour This lesson covers the guidelines developed by the U.S. Centers for Disease Control
INFECTION CONTROL GUIDELINES: STANDARD PRECAUTIONS & ADDITIONAL PRECAUTIONS: LESSON PLAN Lesson overview Time: One hour This lesson covers the guidelines developed by the U.S. Centers for Disease Control
Transmission Based Precautions (Isolation Guidelines)
") Transmission Based (Isolation Guidelines) Transmission Based (Isolation Guidelines) Contents Policy... 2 Purpose... 2 Scope/Audience... 2 Associated Documents... 2 1.1 Transmission-based... 2 1.1.1 Contact...
Transmission Based (Isolation Guidelines) Transmission Based (Isolation Guidelines) Contents Policy... 2 Purpose... 2 Scope/Audience... 2 Associated Documents... 2 1.1 Transmission-based... 2 1.1.1 Contact...
Infection Prevention & Control (IPAC):
:") Windsor Regional Hospital believes that Infection Prevention and Control is vital to patient safety. ALL persons working in the hospital have a RESPONSIBILITY to practice good infection prevention and
Windsor Regional Hospital believes that Infection Prevention and Control is vital to patient safety. ALL persons working in the hospital have a RESPONSIBILITY to practice good infection prevention and
Routine Practices. Infection Prevention and Control
 Routine Practices Infection Prevention and Control Routine Practices Elements of Routine Practices: Risk assessment + hand hygiene + personal protective equipment Environmental controls (patient placement,
Routine Practices Infection Prevention and Control Routine Practices Elements of Routine Practices: Risk assessment + hand hygiene + personal protective equipment Environmental controls (patient placement,
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY
 EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Department: Pediatrics-Hem/Onc-Module F Date Originated: 03/6/2012 Date Reviewed: 6/14, 9/12/17 Date Approved: 6/5/12 Page 1 of 8 Approved by: Department
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Department: Pediatrics-Hem/Onc-Module F Date Originated: 03/6/2012 Date Reviewed: 6/14, 9/12/17 Date Approved: 6/5/12 Page 1 of 8 Approved by: Department
- E - COMMUNICABLE DISEASES AND INFECTIOUS DISEASE CONTROL
 - E - COMMUNICABLE DISEASES AND INFECTIOUS DISEASE CONTROL Every child is entitled to a level of health that permits maximum utilization of educational opportunities. It is the policy of the Duval County
- E - COMMUNICABLE DISEASES AND INFECTIOUS DISEASE CONTROL Every child is entitled to a level of health that permits maximum utilization of educational opportunities. It is the policy of the Duval County
Infection Control and Prevention On-site Review Tool Hospitals
 Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Infection Control Policy and Procedure Manual. Post-Anesthesia Care Unit (Recovery Room) Page 1 of 6
 Page 1 of 6") (Recovery Room) Page 1 of 6 Purpose: The purpose of this policy is to establish infection prevention guidelines to prevent or minimize transmission of infections in the. Policy: All personnel will adhere
(Recovery Room) Page 1 of 6 Purpose: The purpose of this policy is to establish infection prevention guidelines to prevent or minimize transmission of infections in the. Policy: All personnel will adhere
Infection Prevention & Exposure Control Online Orientation. Kimberly Koerner RN, BSN Associate Health Nurse
 Infection Prevention & Exposure Control Online Orientation Kimberly Koerner RN, BSN Associate Health Nurse Created in 2015 Reviewed/Edited Jan 2017 Hand Hygiene Adherence to hand hygiene guidelines among
Infection Prevention & Exposure Control Online Orientation Kimberly Koerner RN, BSN Associate Health Nurse Created in 2015 Reviewed/Edited Jan 2017 Hand Hygiene Adherence to hand hygiene guidelines among
Welcome to the Cooper Infection Prevention Team
 Welcome to the Cooper Infection Prevention Team We Need YOU on the Team Healthcare Associated Infections Increase Morbidity & Mortality (Pain, Suffering and Death) CDC estimates that each year about 2
Welcome to the Cooper Infection Prevention Team We Need YOU on the Team Healthcare Associated Infections Increase Morbidity & Mortality (Pain, Suffering and Death) CDC estimates that each year about 2
INFECTION CONTROL ORIENTATION TRAINING 2006
 INFECTION CONTROL ORIENTATION TRAINING 2006 INFECTION CONTROL OSHA BLOODBORNE PATHOGEN STANDARD STANDARD PRECAUTIONS RISK OF EXPOSURE TO CONTAMINATED MATERIALS USE OF PROTECTIVE EQUIPMENT FOLLOW-UP OF
INFECTION CONTROL ORIENTATION TRAINING 2006 INFECTION CONTROL OSHA BLOODBORNE PATHOGEN STANDARD STANDARD PRECAUTIONS RISK OF EXPOSURE TO CONTAMINATED MATERIALS USE OF PROTECTIVE EQUIPMENT FOLLOW-UP OF
Cystic Fibrosis Foundation Recommendations
 Hospital Epidemiology and Infection Control Department Presenters: Sandra Kistler, RN, PHN, MSN, ICP Cystic Fibrosis Foundation Recommendations Contact Precautions for ALL patients with Cystic Fibrosis
Hospital Epidemiology and Infection Control Department Presenters: Sandra Kistler, RN, PHN, MSN, ICP Cystic Fibrosis Foundation Recommendations Contact Precautions for ALL patients with Cystic Fibrosis
Burn Intensive Care Unit
 Purpose The burn wound is especially susceptible to microbial invasion because of loss of the protective integument and the presence of devitalized tissue. Reduction of the risk of infection is of utmost
Purpose The burn wound is especially susceptible to microbial invasion because of loss of the protective integument and the presence of devitalized tissue. Reduction of the risk of infection is of utmost
PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards. Infection Prevention and Control: Personal Protective Equipment
 PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards : Personal Protective Equipment PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards 2016 PERSONAL PROTECTIVE EQUIPMENT Personal protective
PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards : Personal Protective Equipment PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards 2016 PERSONAL PROTECTIVE EQUIPMENT Personal protective
Infection Prevention and Control Guidelines for Cystic Fibrosis Patients
 AU Medical Center Policy Library Infection Prevention and Control Guidelines for Cystic Fibrosis Patients Policy Owner: Epidemiology POLICY STATEMENT Based upon best practices for the care of cystic fibrosis
AU Medical Center Policy Library Infection Prevention and Control Guidelines for Cystic Fibrosis Patients Policy Owner: Epidemiology POLICY STATEMENT Based upon best practices for the care of cystic fibrosis
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY
 EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Office of Prospective Health Infection Control Plan Date Originated: August 26, 2003 Date Reviewed: 10/22/03; 9/04/07; 03/09/10; 9/01/15; Date Approved:
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Office of Prospective Health Infection Control Plan Date Originated: August 26, 2003 Date Reviewed: 10/22/03; 9/04/07; 03/09/10; 9/01/15; Date Approved:
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY
 EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Family Medicine Physical Therapy Date Originated: February 25, 1998 Dates Reviewed: 2.25.98, 2.28.01 Date Approved: February 28, 2001 3.24.04; 9/10/13
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Family Medicine Physical Therapy Date Originated: February 25, 1998 Dates Reviewed: 2.25.98, 2.28.01 Date Approved: February 28, 2001 3.24.04; 9/10/13
A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page
 Page 1 A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page IH0200: Airborne Precautions EFFECTIVE DATE:
Page 1 A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page IH0200: Airborne Precautions EFFECTIVE DATE:
Standard Precautions (SP) & Transmission-Based Isolation Policies
 & Transmission-Based Isolation Policies") SJMHS Infection Control Policy Standard Precautions (SP) & Transmission-Based Isolation Policies Control of Communicable Disease Section Number 3 Policy Number 1.1 Effective Date: 11/63 Revised Date: 9/96,
SJMHS Infection Control Policy Standard Precautions (SP) & Transmission-Based Isolation Policies Control of Communicable Disease Section Number 3 Policy Number 1.1 Effective Date: 11/63 Revised Date: 9/96,
Personal Hygiene & Protective Equipment. NEO111 M. Jorgenson, RN BSN
 Personal Hygiene & Protective Equipment NEO111 M. Jorgenson, RN BSN Hand Hygiene the single most effective way to help prevent the spread of infections agents. (CDC, 2002.) Consistency & Compliancy 50%
Personal Hygiene & Protective Equipment NEO111 M. Jorgenson, RN BSN Hand Hygiene the single most effective way to help prevent the spread of infections agents. (CDC, 2002.) Consistency & Compliancy 50%
Infection Control in Healthcare. Facilities
 Infection Control in Healthcare Basic Principles Facilities Hand Hygiene / Respiratory Etiquette Exclusion of ill staff and visitors Standard and droplet precautions Facility-specific measures Hospitals
Infection Control in Healthcare Basic Principles Facilities Hand Hygiene / Respiratory Etiquette Exclusion of ill staff and visitors Standard and droplet precautions Facility-specific measures Hospitals
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY
 EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Department: Neurology (Hemby Lane) Date Originated: 2/20/14 Date Reviewed: 6.5.18 Date Approved: 6/3/14 Page 1 of 7 Approved by: Department Chairman Administrator/Manager
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Department: Neurology (Hemby Lane) Date Originated: 2/20/14 Date Reviewed: 6.5.18 Date Approved: 6/3/14 Page 1 of 7 Approved by: Department Chairman Administrator/Manager
Infection Control Manual. Table of Contents
 This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
Infection Control in General Practice
 Infection Control in General Practice August 2017 Magali De Castro Clinical Director, HotDoc Infection Control in General Practice This session will cover: Key infection control considerations for general
Infection Control in General Practice August 2017 Magali De Castro Clinical Director, HotDoc Infection Control in General Practice This session will cover: Key infection control considerations for general
Erlanger Infection Control Program. Resident Resident Orientation and. and
 Erlanger Infection Control Program Resident Resident Orientation Orientation and and Bloodborne Bloodborne Pathogen Pathogen Review Review 2008-2009 2009 1 Outline 1. Healthcare associated infections 2.
Erlanger Infection Control Program Resident Resident Orientation Orientation and and Bloodborne Bloodborne Pathogen Pathogen Review Review 2008-2009 2009 1 Outline 1. Healthcare associated infections 2.
OCCUPATIONAL HEALTH & SAFETY
 OCCUPATIONAL HEALTH & SAFETY Safety in the Workplace WRH recognizes health and safety as a vital component in achieving its vision, mission and values. It is committed to providing safe and harm free care
OCCUPATIONAL HEALTH & SAFETY Safety in the Workplace WRH recognizes health and safety as a vital component in achieving its vision, mission and values. It is committed to providing safe and harm free care
TRANSMISSION-BASED PRECAUTIONS
 TRANSMISSION-BASED PRECAUTIONS PRECAUTIONS Standard Precautions infection prevention practices used with all patients regardless of suspected or confirmed diagnosis. Based on the principle that all blood,
TRANSMISSION-BASED PRECAUTIONS PRECAUTIONS Standard Precautions infection prevention practices used with all patients regardless of suspected or confirmed diagnosis. Based on the principle that all blood,
Developed in response to: Best Practice Infection Prevention and Control
 Transfer of patients within MEHT Clinical Guideline Developed in response to: Best Practice Infection Prevention and Control Version Number 1.0 Issuing Directorate Corporate Governance Approved by Clinical
Transfer of patients within MEHT Clinical Guideline Developed in response to: Best Practice Infection Prevention and Control Version Number 1.0 Issuing Directorate Corporate Governance Approved by Clinical
a. Goggles b. Gowns c. Gloves d. Masks
 Scrub In A patient is isolated because of an undetermined respiratory condition. Which PPEs will healthcare professionals need before caring for the patient? a. Goggles b. Gowns c. Gloves d. Masks A patient
Scrub In A patient is isolated because of an undetermined respiratory condition. Which PPEs will healthcare professionals need before caring for the patient? a. Goggles b. Gowns c. Gloves d. Masks A patient
INTERIM INFECTION PREVENTION AND CONTROL GUIDELINES NOVEL A/H1N1 INFLUENZA
 EXECUTIVE SUMMARY: INTERIM INFECTION PREVENTION AND CONTROL GUIDELINES NOVEL A/H1N1 INFLUENZA This Infection Prevention and Control Guideline is intended for health care workers in the management of suspect
EXECUTIVE SUMMARY: INTERIM INFECTION PREVENTION AND CONTROL GUIDELINES NOVEL A/H1N1 INFLUENZA This Infection Prevention and Control Guideline is intended for health care workers in the management of suspect
Safe Care Is in YOUR HANDS
 Safe Care Is in YOUR HANDS 1 in25 patients has a Healthcare-Associated Infection Would you like to be part of prevention? It s EASY and we can start TODAY! STOP the spread of germs! Hand Hygiene Before
Safe Care Is in YOUR HANDS 1 in25 patients has a Healthcare-Associated Infection Would you like to be part of prevention? It s EASY and we can start TODAY! STOP the spread of germs! Hand Hygiene Before
Infection Control OVERVIEW
 Infection Control OVERVIEW Infections are a significant source of illness and death for nursing home residents and account for up to half of all nursing home resident transfers to hospitals. Infections
Infection Control OVERVIEW Infections are a significant source of illness and death for nursing home residents and account for up to half of all nursing home resident transfers to hospitals. Infections
INFECTION CONTROL ORIENTATION TRAINING 2004
 INFECTION CONTROL ORIENTATION TRAINING 2004 INFECTION CONTROL OSHA BLOODBORNE PATHOGEN STANDARD STANDARD PRECAUTIONS RISK OF EXPOSURE TO CONTAMINATED MATERIALS USE OF PROTECTIVE EQUIPMENT FOLLOW-UP OF
INFECTION CONTROL ORIENTATION TRAINING 2004 INFECTION CONTROL OSHA BLOODBORNE PATHOGEN STANDARD STANDARD PRECAUTIONS RISK OF EXPOSURE TO CONTAMINATED MATERIALS USE OF PROTECTIVE EQUIPMENT FOLLOW-UP OF
Newborn Nursery/Neonatal Intensive Care Unit
 Newborn Nursery/Neonatal Intensive Care Unit Ref:(a) The Association for Professionals in Infection Control and Epidemiology, Principles and Practice, 1996. (b) Hospital Epidemiology and Infection Control,
Newborn Nursery/Neonatal Intensive Care Unit Ref:(a) The Association for Professionals in Infection Control and Epidemiology, Principles and Practice, 1996. (b) Hospital Epidemiology and Infection Control,
Guidelines for the Management of C. difficile Infections in. Healthcare Settings. Saskatchewan Infection Prevention and Control Program November 2015
 Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
Urinalysis and Body Fluids
 Urinalysis and Body Fluids Unit 1 A Safety in the Clinical Laboratory Types of Safety Hazards Physical risks Sharps hazard Electrical hazard Radioactive hazard Chemical exposure risk Fire / explosive hazards
Urinalysis and Body Fluids Unit 1 A Safety in the Clinical Laboratory Types of Safety Hazards Physical risks Sharps hazard Electrical hazard Radioactive hazard Chemical exposure risk Fire / explosive hazards
Infection Prevention Checklist Section I: Policies and Practices I.1 Administrative Measures
 Infection Prevention Checklist Section I: Policies and Practices I.1 Administrative Measures Facility name:... Completed by:... Date:... A. Written infection prevention policies and procedures specific
Infection Prevention Checklist Section I: Policies and Practices I.1 Administrative Measures Facility name:... Completed by:... Date:... A. Written infection prevention policies and procedures specific
Name of Assessor Unit Date. Element Yes No Action Needed
 Figure 10.5 Checklist: Contact Precautions Name of Assessor Unit Date Element Yes No Action Needed CONTACT PRECAUTIONS GENERAL Contact Precautions are used for patients with known or suspected infections
Figure 10.5 Checklist: Contact Precautions Name of Assessor Unit Date Element Yes No Action Needed CONTACT PRECAUTIONS GENERAL Contact Precautions are used for patients with known or suspected infections
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy # 700-S01 Ebola Virus Disease Prevention and Control EBOLA VIRUS DISEASE PREVENTION AND CONTROL Effective: December 8, 2014 Replaces: October
County of Santa Clara Emergency Medical Services System Policy # 700-S01 Ebola Virus Disease Prevention and Control EBOLA VIRUS DISEASE PREVENTION AND CONTROL Effective: December 8, 2014 Replaces: October
Approval Signature: Date of Approval: December 6, 2007 Review Date:
 Personal Care Home/Long Term Care Facility Infection Prevention and Control Program Operational Directive Management of Methicillin-Resistant Staphylococcus Aureus (MRSA) Approval Signature: Supercedes:
Personal Care Home/Long Term Care Facility Infection Prevention and Control Program Operational Directive Management of Methicillin-Resistant Staphylococcus Aureus (MRSA) Approval Signature: Supercedes:
ISOLATION PRECAUTIONS AND MANAGEMENT OF MULTIDRUG-RESISTANT ORGANISMS (MDROS) IN LONG-TERM CARE FACILITIES. Evelyn Cook, RN, CIC Associate Director
 IN LONG-TERM CARE FACILITIES. Evelyn Cook, RN, CIC Associate Director") ISOLATION PRECAUTIONS AND MANAGEMENT OF MULTIDRUG-RESISTANT ORGANISMS (MDROS) IN LONG-TERM CARE FACILITIES Evelyn Cook, RN, CIC Associate Director OBJECTIVES Review Isolation Precautions Review how Multi-drug
ISOLATION PRECAUTIONS AND MANAGEMENT OF MULTIDRUG-RESISTANT ORGANISMS (MDROS) IN LONG-TERM CARE FACILITIES Evelyn Cook, RN, CIC Associate Director OBJECTIVES Review Isolation Precautions Review how Multi-drug
Everyone Involved in providing healthcare should adhere to the principals of infection control.
 Infection Control Introduction The prevention and control of infection is an integral part of the role of all health care personnel. Healthcare Associated Infections (HCAIs) affect an estimated one in
Infection Control Introduction The prevention and control of infection is an integral part of the role of all health care personnel. Healthcare Associated Infections (HCAIs) affect an estimated one in
Standard Precautions & Managing High risk cases. Tuminah Binti Jantan (SRN)
") Standard Precautions & Managing High risk cases Tuminah Binti Jantan (SRN) Outline 1. Infection risk 2. Infection control in dental practice 3. Standard precautions 4. The element of SP (sharps injury)
Standard Precautions & Managing High risk cases Tuminah Binti Jantan (SRN) Outline 1. Infection risk 2. Infection control in dental practice 3. Standard precautions 4. The element of SP (sharps injury)
Communicable Diseases and Clusters of Communicable Diseases in School
 Communicable Diseases and Clusters of Communicable Diseases in School Intended Audiences This document is intended primarily for school nurses. It is also useful for school administrators who are faced
Communicable Diseases and Clusters of Communicable Diseases in School Intended Audiences This document is intended primarily for school nurses. It is also useful for school administrators who are faced
Ebola Virus FAQs. How will the waste be handled for urine and stool of infected patients? Waste disposal will be via the sanitary sewer system.
 Ebola Virus FAQs The FAQs below are from questions received during town hall meetings and from the Premier Health email (ebolaquestions@premierhealth.com). They are arranged in categories of general questions,
Ebola Virus FAQs The FAQs below are from questions received during town hall meetings and from the Premier Health email (ebolaquestions@premierhealth.com). They are arranged in categories of general questions,
Welcome to Risk Management
 Welcome to Risk Management Risk Management is the Safety Net Report, Report, Report! Keeping Your Back Safe Follow the guidelines Associates are responsible and will be held accountable Use proper lift
Welcome to Risk Management Risk Management is the Safety Net Report, Report, Report! Keeping Your Back Safe Follow the guidelines Associates are responsible and will be held accountable Use proper lift
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY
 EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Department: Family Practice Dental Clinic Date Originated: 05-31-2006 Date Reviewed: 06-21-2006 Date Approved: Page 1 of 7 Approved by: Department Chairman
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Department: Family Practice Dental Clinic Date Originated: 05-31-2006 Date Reviewed: 06-21-2006 Date Approved: Page 1 of 7 Approved by: Department Chairman
Chapter 10. medical and Surgical Asepsis. safe, effective Care environment. Practices that Promote Medical Asepsis
 chapter 10 Unit 1 Section Chapter 10 safe, effective Care environment safety and Infection Control medical and Surgical Asepsis Overview Asepsis The absence of illness-producing micro-organisms. Asepsis
chapter 10 Unit 1 Section Chapter 10 safe, effective Care environment safety and Infection Control medical and Surgical Asepsis Overview Asepsis The absence of illness-producing micro-organisms. Asepsis